An ATSB investigation into a serious hot air balloon incident in a Melbourne bayside suburb last year highlights the importance of engineering rigour in analysis, design and testing.
On the morning of 20 April 2022, a sightseeing balloon took off from Royal Park, Melbourne, with 13 passengers and a pilot on board, with the intended destination of Moorabbin Airport. It was the first flight of the balloon since its manufacture.
Travelling south-east over the Melbourne CBD, the pilot observed gaps in the balloon’s circular top vent – a panel-covered opening designed to allow the pilot to let air out of the envelope. The gaps meant the balloon was leaking air without pilot input.
The pilot was unable to seal the vent as there was a fault with the balloon’s deflation system, and a large amount of fuel had to be burned to keep the balloon aloft.
Unable to conduct a more immediate landing at Fawkner Park, the pilot opted to attempt a landing at Elwood Beach.
During the approach to the beach, and without precise altitude control, the pilot struggled to keep the balloon clear of buildings, despite almost continually burning one or two of the balloon’s three burners.
The balloon’s basket collided with two rooftops, and liquid fuel for two of the balloon’s three burners was exhausted.
The pilot continued to activate the remaining burner as the balloon descended through trees, before coming to rest outside an apartment building.
The balloon and basket sustained minor damage, and three passengers sustained minor injuries.
“The balloon’s modified deflation system leaked air once internal pressure in the envelope reached a certain point during normal operation,” ATSB Director Transport Safety Stuart Macleod said.
“At the request of the operator, the balloon manufacturer developed and approved a modification to the balloon's deflation system.
“However, the manufacturer made incorrect assumptions about the modification and subsequently did not conduct the required tests or analysis during the design phase to ensure it was safe for use.”
After the balloon was manufactured with the modified deflation system, the fault went unnoticed during the manufacturer’s production testing process because the air temperature inside the envelope was below the minimum required value.
“For reasons that could not be determined, the actual internal envelope air temperature reached during the production test was lower than recorded, and below the minimum required value.”
This discrepancy meant envelope pressure did not get high enough during the test for the fault in the modified deflation system to manifest.
The manufacturer, Kubicek Balloons, implemented several safety actions in response to the accident.
These include annual calibration of temperature sensors, an update to the production inflation test procedure, and revisions to the production quality control checklist to verify whether any balloon modifications and required tests were completed.
“This investigation highlights the importance of engineering rigour in analysis, design, and testing,” Mr Macleod said.
“Any assumptions used in the engineering analysis and design of safety critical features on aircraft must be based on sound engineering logic, subject to rigorous review to assess their validity, and documented.
“This investigation also demonstrates that robust procedures and processes must be in place to ensure measurements taken during testing are valid, accurate and reliable.”
On 28 July 2023, a Defence MRH-90 Taipan helicopter collided with water near Lindeman Island, Queensland.
The Australian Transport Safety Bureau (ATSB) provided assistance to the Defence Flight Safety Bureau (DFSB) to assist its investigation.
To facilitate this support and to provide the appropriate protections for the information, the ATSB commenced an investigation under the Transport Safety Investigation Act 2003.
The DFSB investigation was finalised and publicly released in May 2025. The investigation report is available from the DFSB website.
Any enquiries relating to the accident investigation should be directed to the Australian Defence Force.
A 737 flight crew’s response to an engine failure over the Tasman Sea earlier this year highlights the benefits of effective decision-making and management of an unexpected situation, an Australian Transport Safety Bureau investigation notes.
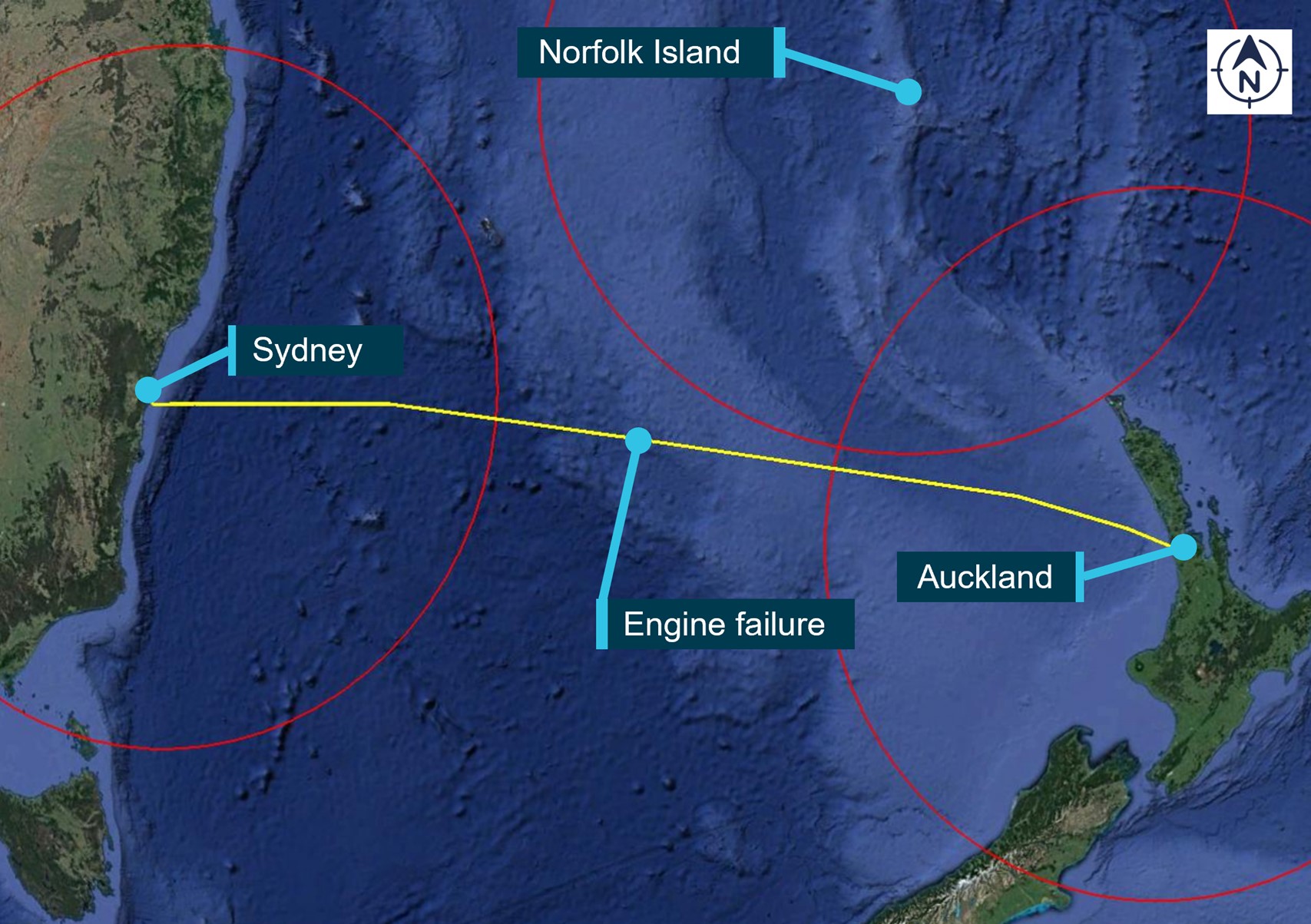
During a scheduled passenger flight from Auckland to Sydney on 18 January 2023, the left engine of a Qantas-operated Boeing 737-838 shut down uncommanded.
In response, the flight crew declared a MAYDAY to prioritise communications with air traffic control, and to ensure they were cleared for an immediate descent from 36,000 ft to 24,000 ft.
The left engine could not be restarted in-flight, and the flight crew conducted an uneventful single-engine landing at Sydney Airport about an hour later.
“A subsequent engine teardown inspection identified separation of the radial driveshaft in the engine’s inlet gearbox, which resulted in a mechanical discontinuity between the engine core and accessory gearbox,” ATSB Director Transport Safety Kerri Hughes said.
“Loss of drive to the accessory gearbox resulted in a loss of fuel pump pressure and uncommanded shutdown of the engine.”
At the time of the engine failure, the aircraft was around 150 km closer to Norfolk Island than it was to Sydney Airport. However, a diversion to Norfolk Island would have required a deviation from the aircraft’s current track, and Norfolk Island presented changeable weather and operational conditions.
“In contrast, Sydney Airport was on the aircraft’s direct route, had favourable weather conditions forecast, had an extensive emergency response, and a straight-in approach on a very long runway,” Ms Hughes noted.
“The decision to continue to Sydney ensured no additional risk was added to an already high workload situation.”
Separately, the report notes that the aircraft’s cockpit voice recorder was inadvertently overwritten during maintenance activities after the aircraft arrived at Sydney.
Since the occurrence, Qantas has enhanced its procedures to prevent inadvertent overwriting of cockpit voice recorders and flight data recorders.
A sightseeing helicopter accident as a result of a seized bearing demonstrates the importance of ensuring all aircraft parts are maintained in accordance with regulations and manufacturer guidance, an Australian Transport Safety Bureau investigation report highlights.
The Robinson R44 helicopter was being used for a sightseeing flight over Limmen National Park, NT on 16 May 2022, with a pilot and three passengers on board.
During cruise, the pilot detected vibrations and observed the engine RPM rise and then drop to zero. In response, the pilot initiated an autorotation, flaring above trees before the helicopter contacted the ground initially on the right front side, nose low. The helicopter then spun and rolled on to the left side facing the opposite way to the direction of travel.
Two of the passengers were seriously injured in the accident, while the pilot and other passenger sustained minor injuries.
An investigation by the ATSB found the helicopter’s clutch actuator lower bearing had seized, resulting in a total loss of drive from the engine to the rotor system.
“Two key findings from this investigation demonstrate the importance of following the relevant manufacturer’s maintenance procedures for all components of an aircraft,” ATSB Director Transport Safety Stuart Macleod said.
The ATSB found the seized bearing had not been maintained in accordance with the maintenance procedures.
Early in its life, the bearing had been lubricated less often than the 300 hour frequency stated in Robinson’s guidance. More recently, the maintenance organisation advised the bearing was lubricated more frequently than required.
“If a maintainer considers that additional maintenance should be conducted on any component of an aircraft, they should contact the manufacturer for engineering advice before varying from the procedure,” Mr Macleod said.
Additionally, the helicopter’s emergency locator transmitter (ELT) did not activate during the accident sequence.
The maintenance organisation advised they had not maintained the ELT since taking over maintenance of the helicopter. The operator stated they presumed it was being maintained on a 100-hourly basis.
“This serves as a reminder to operators that they should be ensuring a self-test of the ELT unit is conducted monthly, to verify it is operational.”
The report also notes findings relating to the absence of a pre-flight safety briefing, and the lack of clear guidance from the Civil Aviation Safety Authority (CASA) about brace positions for helicopters with 3-point harnesses.
“CASA has since the accident released a revised multi-part advisory circular to include information on how to brace in a helicopter with a 3-point harness,” Mr Macleod said.
On behalf of the ATSB’s Commission and staff, we welcome the appointment of Mr Peter Wilson as our Aviation Commissioner.
Mr Wilson certainly has an impressive aviation pedigree, commencing his professional piloting career with Qantas in 1985. Over the following 20 years, Mr Wilson held a number of key senior management appointments including Senior Check Captain Boeing 767, General Manager of Boeing 767 Operations and General Manager of Airbus A330 Operations.
Mr Wilson also held the senior executive appointments as Qantas’s Chief Pilot and Chief Operating Officer.
Since retiring from flying, Mr Wilson has worked as a professional consultant, served as the interim CEO and Chief Operating Officer of Tigerair and held other senior executive appointments more broadly.
We look forward to onboarding Mr Wilson over the coming days.
ATSB transport safety investigators returned to Caboolture airfield this morning to continue collecting evidence as part of their investigation into yesterday’s tragic fatal mid-air collision.
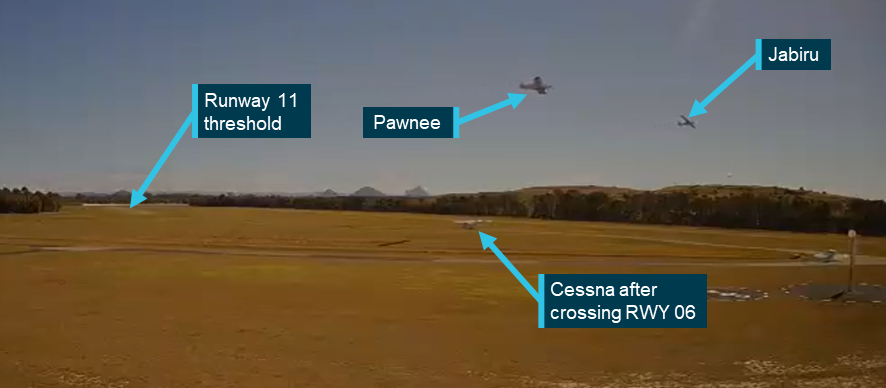
An initial analysis of a number of sources of video footage showed that the Piper Pawnee glider tug aircraft was returning to land at the airfield on runway 06, while the Jabiru J430 was in the process of taking off from runway 11.
The Pawnee was on approach to land before it commenced a go-around – an aborted landing. Go-arounds are a common and well-established practice in aviation and can be conducted for any number of reasons, but we will seek to understand why a go-around was conducted in this instance.
As well as continuing to analyse video footage, investigators will also conduct interviews with the Pawnee aircraft pilot and witnesses, download any available flight tracking data, and retrieve any avionics devices on either aircraft that may have recorded data.
On-site investigators will also use a drone to map the accident site, and look to fly indicative flightpaths of both aircraft to help build an understanding of what the pilots saw of the other aircraft.
The ATSB continues to call for any witnesses who may have seen the accident, and in particular for any pilots operating in the area who may have heard radio calls from either accident aircraft, to make contact with us via the witness form on our website.
The ATSB anticipates publishing a preliminary report, which will detail factual information established in the investigation’s evidence collection phase, in about 8 weeks' time.
A final report, detailing analysis and outlining contributing factors, will be published at the conclusion of the investigation.
However, should any critical safety issues be identified during the course of the investigation, the ATSB will immediately notify relevant parties so that appropriate safety action can be taken.
The ATSB has launched a transport safety investigation into a collision between two single-engine light aircraft at Caboolture airfield, Queensland on Friday.
It was reported that the collision occurred shortly after 10:30 am local time, when a Jabiru J430 was taking off from one runway while a Piper Pawnee was landing on a crossing runway.
Tragically, both occupants of the Jabiru were fatally injured. The Pawnee pilot was uninjured.
Investigators from the ATSB’s Brisbane office arrived on site this afternoon, while additional investigators from Canberra will be on-site tomorrow morning.
Investigators will begin gathering evidence by mapping the accident site, examining the aircraft wreckage, interviewing the surviving pilot and witnesses, and collecting relevant recorded information such as any CCTV footage and flight tracking data.
The ATSB asks anyone who witnessed the accident, or may have video footage of either aircraft at any phase of their flights, to make contact via the witness form on our website: atsb.gov.au/witness at their earliest opportunity.
The ATSB anticipates publishing a preliminary report, which will detail factual information established during the investigation’s initial evidence collection phase, in approximately 6-8 weeks.
The ATSB will publish a final report, detailing contributing factors and any identified safety issues, at the conclusion of the investigation.
However, should any critical safety issues be identified at any stage during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.
On the morning of 28 July 2023, the pilot of a Piper PA-25 Pawnee, registered VH-SPA, was in the circuit to land on runway 06 at Caboolture Airfield, Queensland. Caboolture was a non-controlled aerodrome relying on self-separation by pilots. The Pawnee was a tow aircraft for the local gliding club, and had been towing gliders from runway 06 and had previously landed on the same runway. Several other aircraft had used the intersecting runway 11 during periods where runway 06 was not being used. The windsock indicated a light wind that varied in direction, favouring runway 11 or runway 06 approximately equally.
As the Pawnee was on final approach to land, a Jabiru J430, registered VH-EDJ, commenced a take-off roll on runway 11. Approximately 16 seconds later, just prior to the Pawnee touching down, a Cessna 172, registered VH-EVR, taxied across runway 06 without stopping or making a radio call. Seeing the Cessna, the Pawnee pilot elected to conduct a go-around to avoid a potential collision with it.
While the Jabiru pilot appeared to see the Pawnee late in the sequence and attempted to evade it, the 2 aircraft collided near the runway intersection at approximately 130 ft above ground level. The Jabiru’s right wing was damaged as a result, and the aircraft collided with terrain, fatally injuring the pilot and passenger. The Pawnee was damaged, but it landed safely and its pilot was uninjured.
What the ATSB found
While in the circuit, the Pawnee pilot had made positional radio calls, and a radio call stating their intention to land and hold short of the runway intersection. Based on the Jabiru pilot's apparent unawareness of the Pawnee until just before the collision, and most witnesses not recalling hearing any calls from the Jabiru throughout the event, it is likely that the Jabiru pilot could not transmit or hear radio calls for reasons that could not be determined. Likely unaware of the landing Pawnee’s presence, the Jabiru pilot commenced take-off on runway 11 while the Pawnee was on final approach to runway 06.
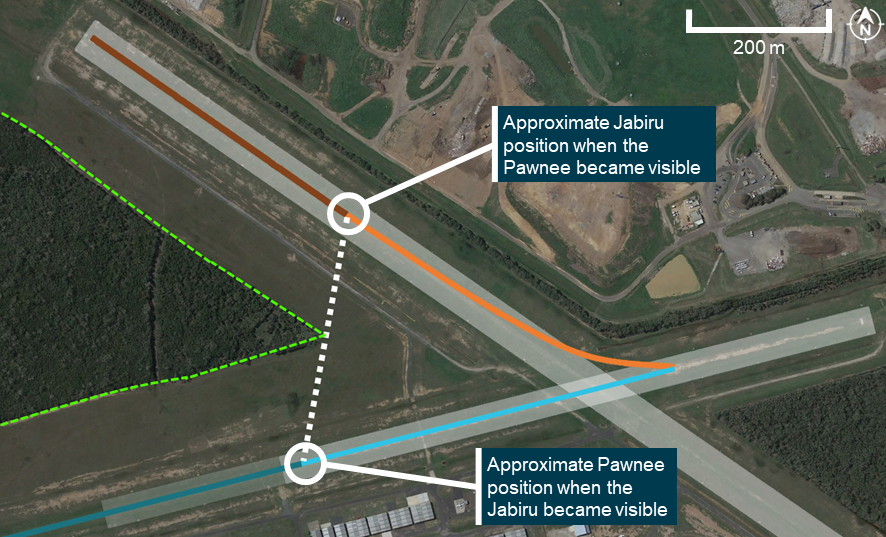
A stand of trees between the runways prevented the Pawnee and Jabiru pilots from being able to see one another’s aircraft once the Jabiru had taxied onto the runway heading. Not having heard any radio calls from the Jabiru, and unable to see it when on final approach to land, the Pawnee pilot was not aware that the Jabiru was taking off on runway 11.
The Cessna pilot had previously turned down the aircraft’s radio and not restored the volume prior to crossing runway 06. The pilot was therefore not aware of the Pawnee, and seeing the traffic on runway 11, was not expecting aircraft to be operating on runway 06.
The local gliding club regularly chose to operate on runway 06 for the first flights of the day, due to the runway’s proximity to the glider hangars, and sometimes used runway 06 later in the day when winds were light, including during periods of light traffic on runway 11/29. The use of an intersecting runway increased the collision risk as Caboolture was a non-controlled aerodrome relying on alerted see‑and‑avoid principles, exacerbated by the stand of trees blocking pilots’ sightlines.
Both the Jabiru and Pawnee pilots were familiar with the aerodrome and would have been aware of the line of sight limitations between the intersecting runways due to the stands of trees. However, the ATSB found that the aerodrome operator, the Caboolture Aero Club (CAC), did not effectively manage or inform pilots of the risk presented by trees and buildings around the airfield that prevented pilots from being able to see aircraft on intersecting runways and approach paths.
In this accident, it is likely that all 3 pilots had an understanding that runway 11 was in general use by aircraft, and therefore could be considered an active runway under applicable Civil Aviation Safety Authority (CASA) guidance for pilots using non-controlled aerodromes. However, the Pawnee pilot reasonably considered runway 06 to be an active runway through their own use of it. The ATSB found that the CASA guidance did not clearly define the term ‘active runway’, and the definition could be interpreted in different ways. Further, the guidance did not provide practical advice to pilots using a secondary runway, and in some situations, it was contrary to existing regulations.
What has been done as a result
The CAC amended the Caboolture Airfield operations manual to state that no simultaneous runway operations are permitted under any circumstances. Pilots wanting to operate on a different runway must request this and receive confirmation or acknowledgement from all aircraft taxiing or in the circuit. The manual also now states that rolling (take-off) calls must be made. A submission has been made to include the procedure in Caboolture Airfield’s En Route Supplement Australia (ERSA) entry.
CASA advised that it is in the process of improving guidance material regarding the factors and safety issues which should be considered in determining runway use. To better align with the regulations and avoid confusion, CASA is removing all references of the term 'active' when associated with a runway. CASA will also expand the guidance provided in the Part 91 Acceptable Means of Compliance and Guidance Material to assist in the industry's understanding of this issue.
Safety message
This accident demonstrates that following the existing regulations, rules of the air and associated guidance does not completely overcome the risks inherent in using multiple runways concurrently. Pilots need to carefully consider the choice of runway, not only in context of which runway might be considered ‘active’ or ‘in use’ by others, but in terms of the specific type of risks that arise when any 2 or more aircraft are going to use different runways. These risks can be heightened or alleviated by a range of factors (for example, visual obstructions) that differ widely across operations and aerodromes, and can change over time.
More generally, self-separation using alerted see-and-avoid principles carries some risk in all situations. Pilots can mitigate this to some extent by:
checking radio equipment for functionality prior to taxi
establishing two-way communication with potentially conflicting aircraft as needed
being mindful of the potential for radio communications to be missed or misinterpreted
never assuming a runway or aerodrome is safe to use simply because no other aircraft are visible.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing the collision risk around non-towered airports.
Summary video
The occurrence
Overview
On the morning of 28 July 2023, the pilot of a single-seat Piper PA-25 Pawnee, registered VH‑SPA and operated by the Caboolture Gliding Club, was towing gliders from runway 06[1] at Caboolture Airfield, Queensland. At various times, other aircraft were using the intersecting runway 11 (Figure 1).
Figure 1: Runway configuration at Caboolture Airfield
Source: Google Earth, annotated by the ATSB
As the Pawnee was on final approach to land after returning from the second glider tow, a Jabiru J430, registered VH-EDJ, with a pilot and passenger on board conducting a private flight to Dirranbandi Airport, Queensland, commenced a take-off roll on runway 11. About 16 seconds later, with the Pawnee about 200 m from touchdown, a Cessna 172, registered VH‑EVR, taxied across runway 06 without stopping or making a radio call. Seeing the Cessna, the Pawnee pilot elected to conduct a go‑around. The Pawnee began climbing at almost the same time as the Jabiru lifted off.
The 2 aircraft continued to climb on converging tracks. About 9 seconds later the Jabiru began a steep left turn in an apparent evasive manoeuvre but the 2 aircraft collided near the runway intersection, at about 130 ft above ground level.
The Jabiru’s right wing tip and aileron separated in the impact, and the aircraft collided with terrain, fatally injuring the pilot and passenger on board. The Pawnee was damaged, and the pilot returned to land without further incident.
First glider tow
At 1005 the pilot of the Pawnee took off from runway 06. It was a clear day with a 1–3 kt wind that varied between easterly and north-easterly. This was the Pawnee pilot’s first flight of the day, and the first time runway 06 had been used that day. All previous flights by other aircraft had operated on runway 11, which intersected runway 06.[2]
After the glider was released from aerotow,[3] the Pawnee pilot rejoined the circuit[4] for runway 06, and landed at 1017 without incident. Two radio calls related to this approach were recorded. The aircraft stopped short of the runway intersection, turned around and backtracked to the start of runway 06 – the runway threshold – to collect another glider.
Second glider tow and Pawnee rejoining the circuit
Caboolture Airfield was defined as an aircraft landing area (ALA), and was a non‑controlled aerodrome located within class G (non-controlled) airspace, and had a designated common traffic advisory frequency (CTAF) on which pilots made positional broadcasts when operating within the vicinity of the airport.[5] Calls were not recorded at Caboolture Airfield, but some transmissions from aircraft in flight were recorded at Caloundra Airport, an airport about 32 km to the north that used the same CTAF frequency. The ATSB identified no recordings of radio transmissions from any aircraft on the ground at Caboolture around the time of the accident and some transmissions were only partially recorded (see Recorded data).
At 1022, the Pawnee pilot took off with another glider in tow. There was a radio recording of the Pawnee pilot responding at 1024 to a radio check request from another aircraft (the original call was not recorded). At about 1027, another aircraft took off from runway 11 after making a take-off radio call on CTAF that was heard by the Pawnee pilot, but not recorded.
Meanwhile, the pilot of a Jabiru J430, registered VH‑EDJ, had just commenced taxi towards runway 11. The Jabiru had been taxied directly from the hangars next to runway 06, turning north-west onto the taxiway parallel to the runway (and facing northwest) from 1027:25.[6]
The Pawnee pilot reported that after the glider was released from aerotow, with the tow rope still attached, they made a radio call to indicate they were descending towards Caboolture to the west of the airfield. This call was not recorded.
At the time, the wind was suitable for runway 06 and there was no other traffic in the circuit or on the ground that the Pawnee pilot considered as a potential threat to a safe landing on this runway. The Pawnee pilot then joined the crosswind leg for runway 06 and made the following radio call at 1028:09 (truncated in the recording):
Caboolture traffic sierra papa alpha Pawnee is heading crosswind to runway 06 Caboolture and…
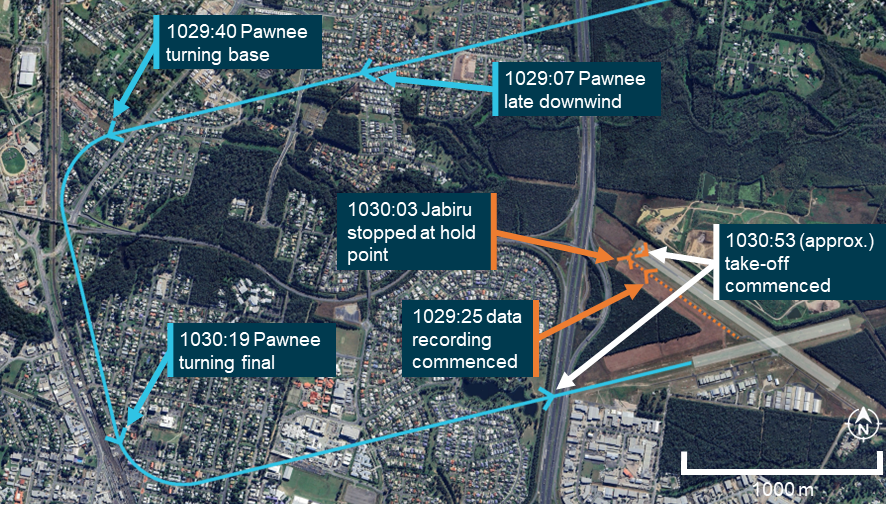
The Pawnee pilot later reported that they also communicated with the aircraft that had just departed to arrange mutual separation. The Pawnee pilot then made the following radio call at 1029:07 on the downwind leg for runway 06:
Caboolture traffic sierra papa alpha is now late downwind runway 06 Caboolture
At 1029:40 the pilot then made a radio call for the base leg, which was truncated in the recording:
Caboolture traffic, sierra papa alpha is turning base runway…
Recorded data recovered from the Jabiru showed that at 1030:02, the pilot stopped at a hold point next to runway 11, facing north-east, perpendicular to the runway. At this time there were 2 other aircraft on the ground in the vicinity of the runway 11 threshold: one ahead of the Jabiru and one in the run-up bay. The Pawnee pilot recalled that while on the base leg, and focused on the potential for other traffic in the same circuit, they saw 2 aircraft in that area but did not identify what type they were and could not recall their exact positions.
The Pawnee pilot turned onto the final leg and made another radio call at 1030:19, truncated in the recording:
Caboolture traffic, sierra papa alpha is…
According to the Pawnee pilot and several witnesses who heard the transmissions, the Pawnee pilot announced that the aircraft would be landing on runway 06 and ‘holding short’, indicating that the aircraft would not be crossing the intersection with runway 11/29 during the landing. The ATSB could not determine whether the pilot made this statement during the base call or the final call.
The Pawnee pilot reported that they intended to hold short because they did not want to cross ‘another active runway’, aware of another aircraft about to use runway 11 as well as one that had just taken off. In this case the pilot was using the term ‘active runway’ to describe a runway that is, or could soon be, in use, and considered both runway 11 and runway 06 to be active (the latter through their own use of it). The Pawnee pilot was expecting the second departing aircraft not to commence take-off until the Pawnee pilot had reported that they stopped short of the runway intersection. In general, the Pawnee pilot reported they made the hold short call to advise other traffic of their intentions. They did not expect pilots to use the intersecting runway on the basis of the hold short call, and only expected pilots to use the intersecting runway after a ‘stopped short’, or ‘clear’ call was made. The pilot reported that they had done this (radioed an intention to land and hold short with other traffic using runway 11) on many other occasions and the other aircraft had always waited until the pilot had radioed that they had stopped short and were clear of all runways.
The aircraft ahead of the Jabiru departed at about 1030:26 following an associated radio call (which was heard by the Pawnee pilot but not recorded).
Pawnee continuing final approach and Jabiru commencing take-off
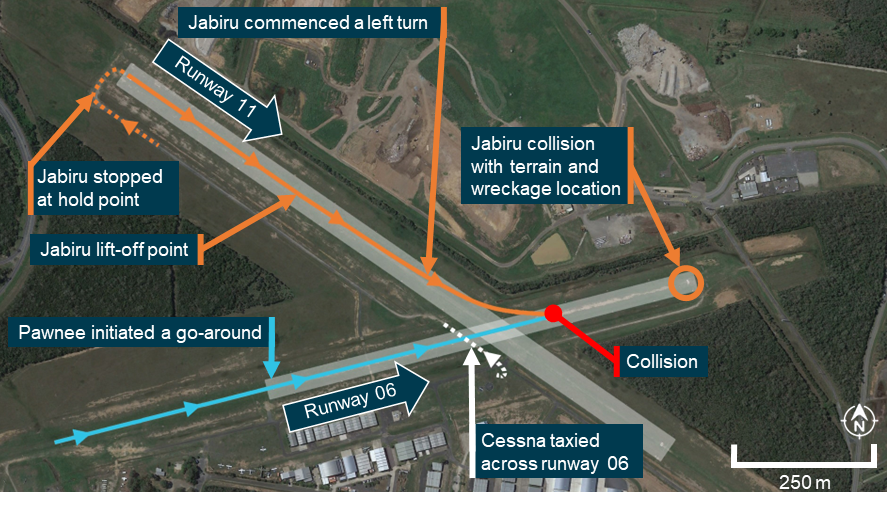
The subsequent sequence of events is illustrated in Figure 2 and Figure 3.
Figure 2: Approximate tracks of the involved aircraft based on video recordings and recorded track data
Dotted lines indicate aircraft taxiing. Source: Google Earth, annotated by the ATSB
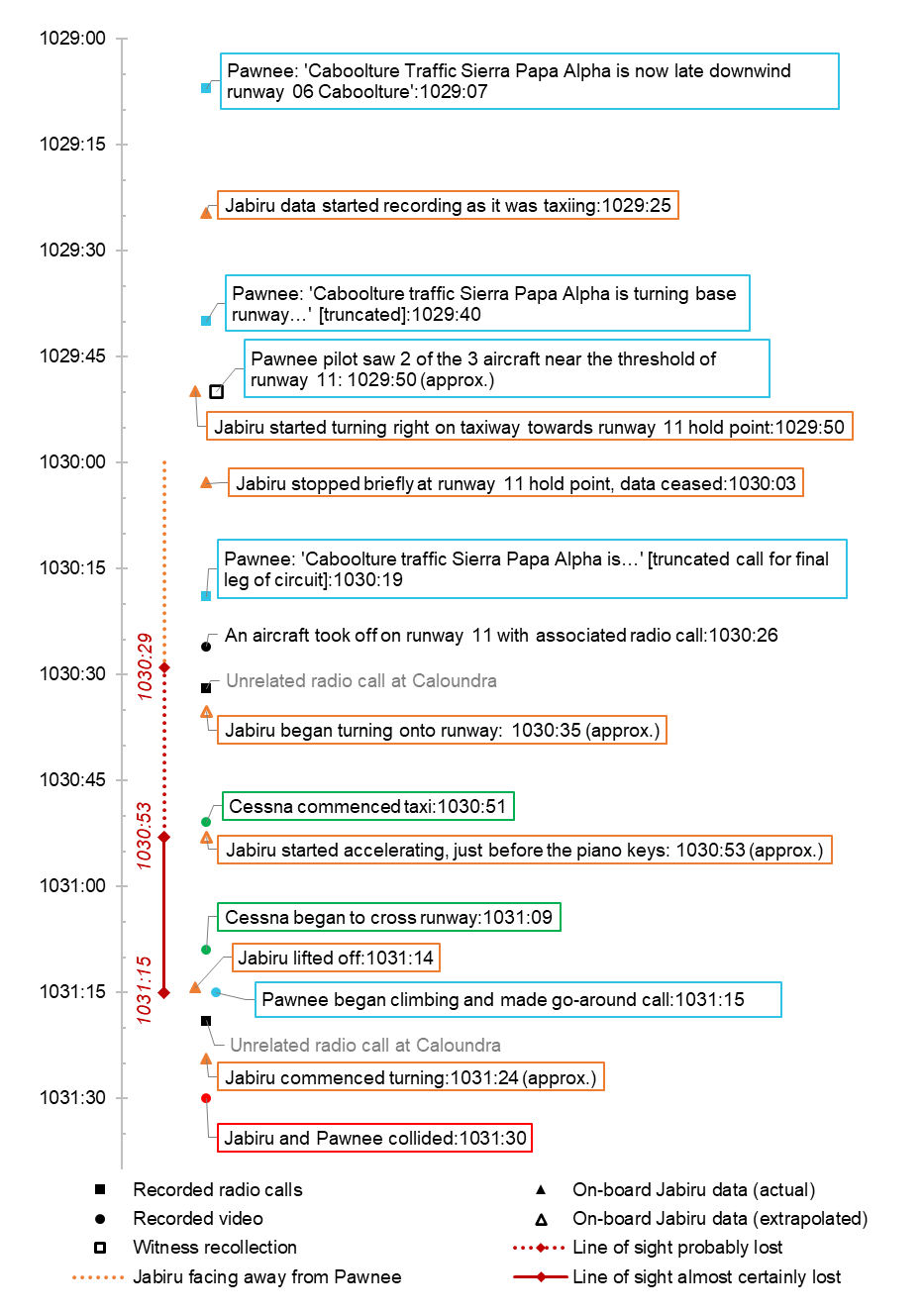
Figure 3: Sequence of events
Source: ATSB
An eyewitness stated that after waiting at the hold point, the Jabiru taxied onto the runway and immediately began the take-off roll. The recorded data was incomplete at this point, but ATSB analysis estimated that the Jabiru likely began to turn onto runway 11 at about 1030:35, establishing the runway heading a few seconds later. Take‑off would have commenced at about 1030:53. Two witnesses reported hearing the Jabiru pilot make a ‘rolling’ (take-off) call on runway 11, while 7 other witnesses, including the Pawnee pilot, stated that they did not remember hearing a rolling call. No witnesses recalled any other calls from the Jabiru.
At about the same time (1030:51), a Cessna 172, registered VH-EVR, had just commenced taxiing from a run-up bay south of the runway intersection. The aircraft was being operated by a solo student pilot who was intending to depart from runway 11. When the Cessna pilot first entered the aircraft, they heard the Pawnee making radio calls in the circuit. However, the Cessna pilot later reported having turned the radio volume down in order to concentrate on engine run-ups and pre-flight checks at the run‑up bay. As a result, the Cessna pilot did not hear the previous transmissions from the Pawnee pilot, and was not aware of it approaching runway 06 for landing. The Cessna pilot reported making a taxi call once checks were complete, and taxied onto the taxiway parallel to runway 11/29, heading towards the threshold of runway 11. At this point, the pilot realised the radio volume had not been restored and turned the volume back up.
At 1031:09, with the Pawnee about 200 m from touchdown on runway 06, the Cessna began to cross runway 06 ahead of the Pawnee. The Cessna pilot did not stop or make a radio call prior to crossing the runway. In interview, the Cessna pilot reported having been trained to stop and ‘clear’ a runway visually prior to crossing. However, the Cessna pilot had just seen an aircraft taking off from runway 11 and another (the Jabiru) lining up. With an understanding that aircraft were currently operating on runway 11, the Cessna pilot reported that they were therefore not expecting aircraft to be operating on runway 06/24, and did not look for any. In addition, due to the limited use of runway 06/24, the Cessna pilot did not always come to a complete stop before crossing.
As the Cessna began to cross the runway, the Pawnee pilot initiated a go-around,[7] unsure of the Cessna pilot’s intentions (for example, whether the Cessna was going to turn onto runway 06) and concerned about the potential for a ground collision. The Pawnee pilot reported making a radio call stating that they were going around, and said something like ‘watch out sunshine’. The order of these statements could not be determined. The radio call was not recorded, but 6 of the 10 witnesses with access to a radio reported hearing both the ‘going around’ and the ‘watch out sunshine’ parts of the call, and were relatively consistent in terms of the specific words used. Another 2 witnesses reported hearing the ‘watch out’ part of the call, but not the ‘going around’ part. At the same time, the Pawnee pilot applied full power, adopted a climb attitude and retracted one stage of flap.
Both aircraft climbing and collision
At 1031:15, the Pawnee began climbing while maintaining the runway 06 heading just as the Jabiru lifted off from runway 11 before the runway intersection. The Pawnee pilot was focusing on their climb rate, concerned about clearance between the trailing tow rope and the Cessna.[8] At about 1031:24, while the 2 aircraft were climbing at similar rates on converging tracks, the Jabiru pilot commenced a steep left turn (Figure 4). Given the steepness of the turn, and the low altitude, this was likely an attempt to avoid a collision. The Pawnee pilot reported not seeing the Jabiru until immediately after the impact, when they momentarily saw something behind the Pawnee’s left wing as they leant over to fully retract the flaps.
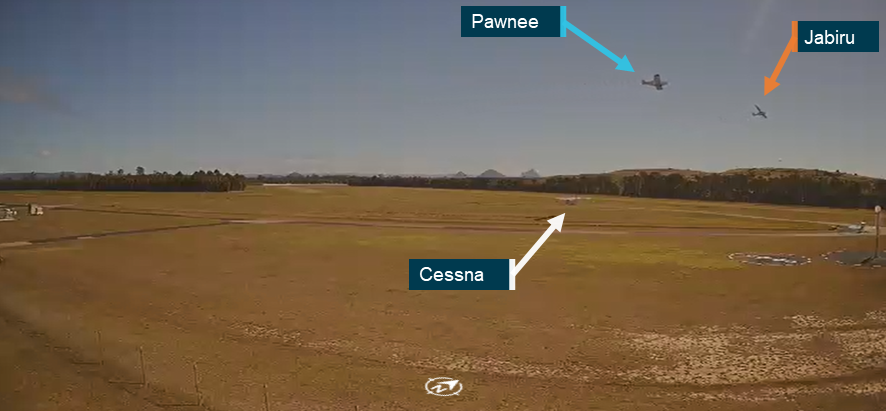
Figure 4: CCTV still image at 1031:06, from a camera south of the runway intersection, showing the 2 aircraft converging as the Jabiru turns left
Source: Caboolture Aero Club, annotated by the ATSB
At 1031:30, the 2 aircraft collided on similar tracks above runway 06, just north-east of the 06/11 intersection, at a height of about 130 ft. The leading edge of the Pawnee’s inboard left wing struck the Jabiru’s right wing at the outboard trailing edge, resulting in separation of the Jabiru’s right wing tip and part of the right aileron.
The Jabiru then rolled to the right while rapidly losing altitude. At 1031:38 it collided with terrain in a nose-down, right-wing-down attitude near the end of runway 06. The pilot and passenger were fatally injured.
The Pawnee sustained damage to its left wing in the collision but remained controllable and the pilot was uninjured.
After the collision the Pawnee pilot circled the airfield to direct first responders towards the accident site. The aircraft later landed on runway 11 without further incident.
Context
Pilot information
Jabiru VH-EDJ
The pilot of VH‑EDJ (the Jabiru) held an Air Transport Pilot Licence (aeroplane) and was a grade 2 flight instructor with multiple endorsements and ratings including as a flight instructor and for large passenger jets, having previously been an airline pilot. The pilot’s logbooks and other flight history could not be located. The pilot was reportedly experienced in general aviation and diligent with radio calls. The pilot had regularly flown at Caboolture Airfield, and held a class 2 aviation medical certificate that was valid until 30 October 2024. They were required to wear corrective lenses, but no other medical issues were listed on their licence. It could not be determined whether the pilot was using corrective lenses at the time of the accident. The ATSB could not obtain recent activity or sleep history for the pilot.
A post-mortem examination identified no significant pre-existing medical conditions (there was moderate heart disease that was considered ‘not significant enough to have caused a medical event’). Toxicology testing showed no alcohol, illicit drugs or relevant medications. Both the pilot and passenger had non-elevated levels of carbon monoxide.
Pawnee VH-SPA
The pilot of VH-SPA (the Pawnee) held a Private Pilot Licence (aeroplane) and held endorsements for glider operations and glider towing operations. The pilot was a level 3 instructor[9] with Gliding Australia, as well as a senior instructor and tow pilot examiner for Recreational Aviation Australia. They had operated as a tow pilot at Caboolture for over 20 years, and had performed 2,570 aerotow glider launches with a total flight experience of over 2,000 hours. The pilot held a class 2 aviation medical certificate that was valid until 17 July 2025. There were no relevant medical restrictions on the pilot’s licence, and they reported no medical issues or medications. The pilot also reported being well rested prior to the accident.
Cessna VH-EVR
The pilot of VH-EVR (the Cessna) was a student pilot conducting flying training at Caboolture. The pilot had commenced the process of attaining a Commercial Pilot Licence in January 2023 and did not yet hold a flight crew licence. The pilot had approximately 60 hours of flying experience. They attended Caboolture Airfield for flying training from Monday to Friday. The pilot was preparing to conduct their third solo navigation flight at the time of the occurrence. The pilot reported that runway 06/24 had been closed for approximately half of their training to date, having begun in January 2024.
Aircraft information
Jabiru VH-EDJ
The Jabiru J430 is a high-wing light aircraft. VH-EDJ had a single Jabiru 3300 piston engine and a ground-adjustable fibreglass propeller. It was constructed primarily by the pilot, first registered on 19 February 2019, and had recorded 283.7 hours total time in service at the time of the accident.
The aircraft was fitted with a Dynon SkyView SV-HDX1100 integrated touch screen avionics system, as well as an automatic dependent surveillance broadcast (ADS-B) transponder.[10] This model of transponder was capable of broadcasting the aircraft’s position (ADS-B OUT), but not receiving other positional broadcasts (ADS-B IN).
Pawnee VH-SPA
The Piper PA-25-235 Pawnee B is a low-wing single-engine aircraft. VH-SPA was powered by a Textron Lycoming O-540 piston engine with a fixed-pitch aluminium propeller. The aircraft was manufactured in 1969, and first registered in Australia in 1974. It had 10,181 hours total time in service, and had been operating as a tow aircraft at Caboolture Airfield since January 1997.
The aircraft was fitted with a basic analogue instrument suite. There was no ADS-B transponder fitted.
Wreckage and impact information
Overview
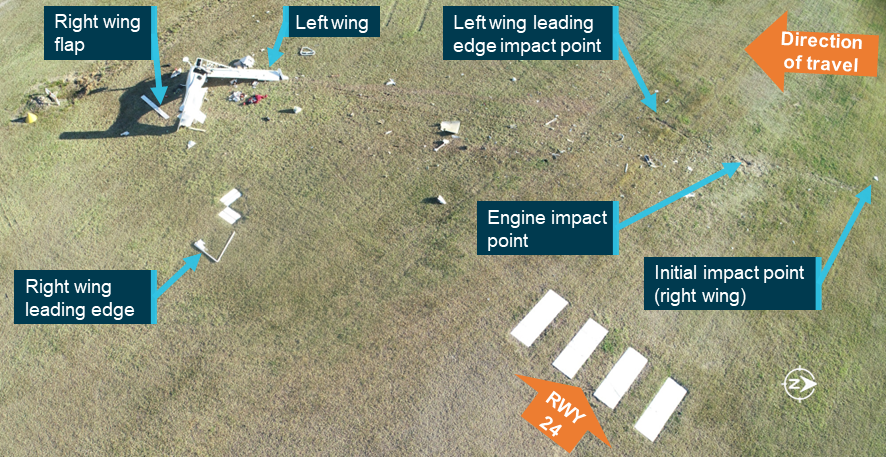
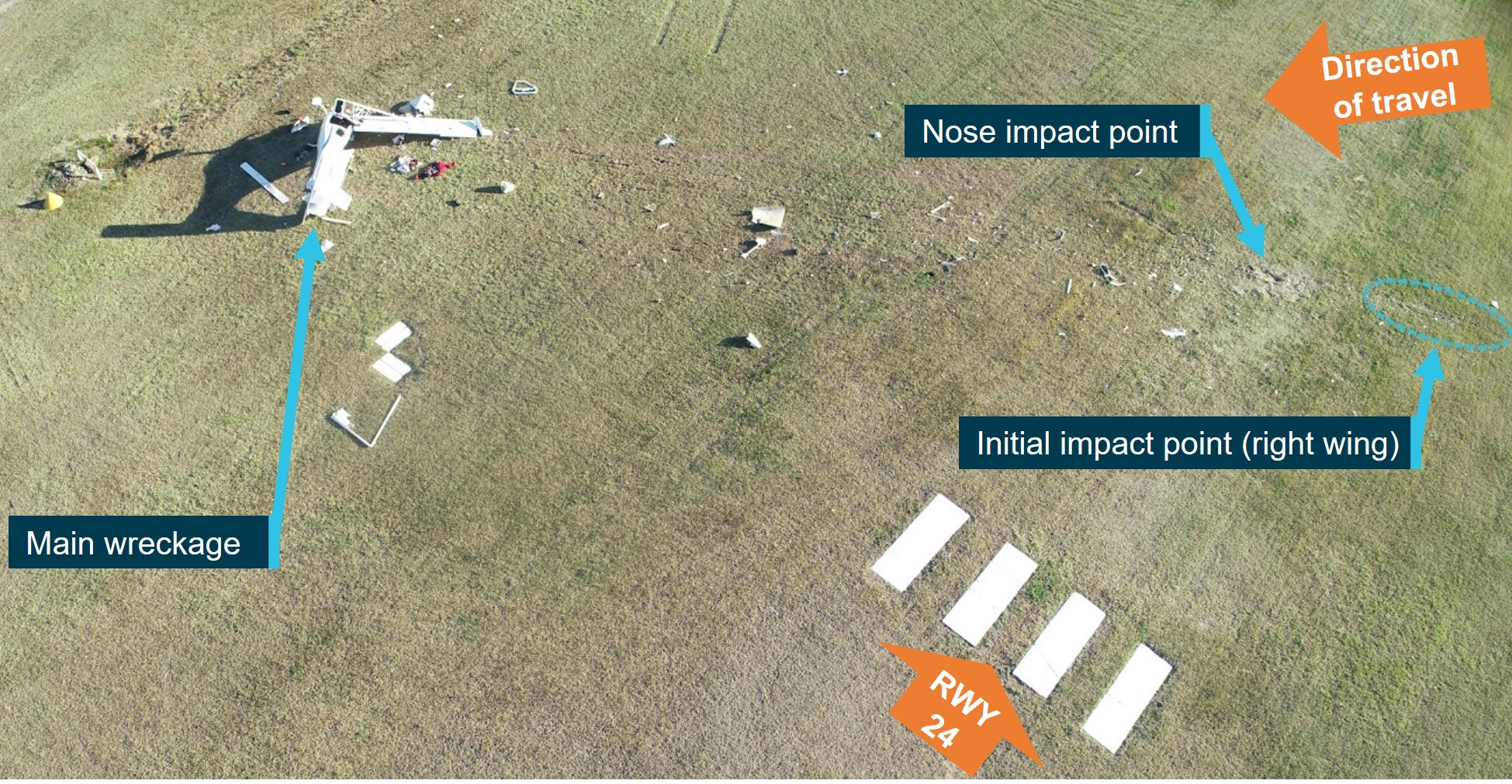
The ATSB conducted an onsite examination of the aircraft wreckage (Figure 5). The collision location and all aircraft components and wreckage were confined within the airfield. The Jabiru main wreckage site was near the threshold of runway 24, with a section of the Jabiru’s right aileron, right wing tip and associated wreckage located near the runway intersection.
Figure 5: Locations of aircraft and wreckage after the Pawnee had landed
Source: Queensland Police Service, annotated by the ATSB
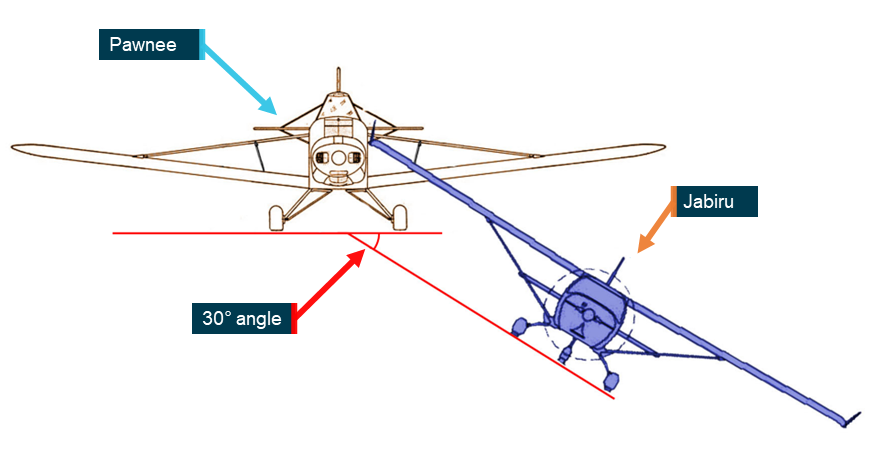
Based on the damage to each aircraft (described below), and the aileron and wing tip found near the runway intersection, the ATSB determined that the Pawnee’s left wing leading edge collided with the Jabiru’s right wing trailing edge. Damage signatures indicated that the relative angle between the 2 aircraft was about 30° in roll (Figure 6). There was no impact with the Pawnee’s propeller.
Figure 6: Approximate collision attitudes
This is a simplified diagram designed to illustrate the approximate difference in height and roll attitudes between the aircraft at the point of collision. The image does not reflect differences in pitch and yaw. Source: ATSB, Piper Aircraft and Jabiru Aircraft
Jabiru VH-EDJ
Accident site information
The Jabiru’s impact point was about 212 m beyond the separated wing tip and aileron (Figure 7). The right wing impacted the ground first, followed by the propeller and engine. The aircraft tumbled across runway 06/24 for about 42 m in a direction almost parallel to runway 11, coming to rest next to the runway threshold.
Figure 7: Jabiru wreckage trail
Source: ATSB
The rudder and elevator control surfaces were almost undamaged. They could be moved by hand after the accident, and the associated cables were continuous with all attaching hardware present. While the wing attachment points were heavily disrupted, damage to the control system appeared consistent with the midair collision and subsequent impact with terrain. Flaps were in the correct position for take-off.
The Jabiru’s engine mounts had fractured in the impact, with the control cables and fluid lines still intact. The wreckage site showed evidence of fuel spill from the wing tanks. Forward bending in the propeller blades indicated that the engine was driving the propellers at the time of impact. This, in conjunction with witness statements and video recordings indicated that the engine was producing power at the time of the accident.
There was no fire. First responders reported that both occupants were wearing shoulder and lap restraints.
Based on measurements of the ground scarring and the chord-wise symmetry of the right wing damage, it is likely that the Jabiru impacted terrain right wing first, in a nose‑down attitude of about 85°.
Based on the steep impact angle, the estimated speed, and disruption of the fuselage, the impact was not considered survivable.
Radio examination
A Microair M760-01 VHF transceiver radio was recovered from the Jabiru’s cockpit following the accident. The unit was heavily damaged and pulled away from the instrument panel, with the associated wiring still connected but damaged. The antenna and radio were still connected via a coaxial cable when the aircraft was inspected onsite, and the cable and antenna appeared undamaged. The ATSB retained the radio and some of the associated hardware (such as push-to-talk buttons) for subsequent testing. The cable and antenna were not retained. The headsets were damaged in the collision with terrain and therefore also not retained.
The radio turned on when power was applied during testing, and was selected on when recovered (a click is heard and felt at the beginning of the knob’s rotation to indicate on/off). The position of the volume knob prior to impact could not be determined as it may have moved during impact, recovery and transit. The radio was selectable between active and standby frequencies using a toggle switch, which was broken when found. The radio frequencies were set to 125.850 MHz (the CTAF frequency; see Radio communications at Caboolture Airfield) and 125.700 MHz (the area frequency). It was not possible to confirm which was selected as the active frequency prior to the collision.
Overall, the extent of damage to the radio and associated components precluded a determination of its probable functionality at the time of the accident.
Pawnee VH-SPA
The Pawnee remained intact after the collision (Figure 8). The tow rope stayed attached. Heavy impact damage occurred on the left wing leading edge, between about 0.25–1.2 metres from the wing-fuselage interface. Other impact damage was identified:
on the wing strut, directly above the damage to the leading edge
on a fuselage cowling panel located above the left wing
on the left wing lower surface, including a small piece of fibre-reinforced plastic, caught between 2 panels, which appeared consistent with the skin of the Jabiru.
Figure 8: Damage to the Pawnee’s left wing
Source: ATSB
During the ATSB examination, the rudder, aileron, and elevator controls all responded appropriately to control inputs with a full range of movement without binding or restriction. All flight control surfaces were inspected for damage, and none was found. A basic visual inspection found no obvious issues with the engine or controls. There was no visible damage to the propeller. Based on the condition of the aircraft and the location of damage, and given that the aircraft landed safely, a detailed examination of the aircraft and engine was not conducted.
The radio and headset were tested by the ATSB and found to be serviceable in both transmit and receive modes. The frequency was set to the Caboolture Airfield CTAF frequency.
Operations at non-controlled aerodromes
Aircraft landing areas
Caboolture Airfield is an aircraft landing area (ALA). ALAs are non-controlled aerodromes that are not certified by CASA. They are unregulated facilities where pilots and operators are responsible for determining whether they are suitable for their use.
In general, CASA had no requirements or regulations that specified how ALAs were to be managed and operated.[11] The regulations and guidance provided to pilots regarding right of way, radio use and rules of the air were applicable at all non-controlled aerodromes, not just ALAs.
See-and-avoid
In non-controlled airspace, pilots rely on the use of the rules of the air and ‘see‑and‑avoid’ principles to maintain separation from other aircraft sharing the airspace.
An ‘alerted’ visual search is one where the pilot is alerted to another aircraft’s presence, typically through radio communications or aircraft-based alerting systems. Broadcasting on the CTAF to any other traffic in the vicinity of a non-controlled aerodrome is known as radio-alerted see-and-avoid and assists by supporting the pilot’s situational awareness and visual lookout for traffic with the expectation of visually acquiring the subject in a particular area.
Conversely, an ‘unalerted’ search is one where reliance is entirely on the pilot searching for, and sighting, another aircraft without prior knowledge of its presence. Unalerted see‑and‑avoid relies entirely on the pilot’s ability to sight other aircraft.
Issues associated with unalerted see-and-avoid have been detailed in the ATSB research report See and Avoid(Hobbs, 1991). The report stated:
See-and-avoid can be considered to involve a number of steps. First, and most obviously, the pilot must look outside the aircraft.
Second, the pilot must search the available visual field and detect objects of interest, most likely in peripheral vision.
Next, the object must be looked at directly to be identified as an aircraft. If the aircraft is identified as a collision threat, the pilot must decide what evasive action to take. Finally, the pilot must make the necessary control movements and allow the aircraft to respond.
Not only does the whole process take valuable time, but human factors at various stages in the process can reduce the chance that a threat aircraft will be seen and successfully evaded. These human factors are not ‘errors’ nor are they signs of ‘poor airmanship’. They are limitations of the human visual and information processing system which are present to various degrees in all pilots.
The United States Federal Aviation Administration (FAA) advisory circular AC 90-48D CHG 1 Pilots’ Role in Collision Avoidance indicated that it takes unalerted pilots around 12.5 seconds to sight an aircraft and react effectively to it (Table 1).
Table 1: Reaction times for airborne collision avoidance
Event
Seconds
See object
0.1
Recognise aircraft
1.0
Become aware of collision course
5.0
Decision to turn left or right
4.0
Muscular reaction
0.4
Aircraft lag time
2.0
TOTAL
12.5
Source: Federal Aviation Administration AC 90-48D CHG 1
The ATSB research report found that an alerted search is likely to be 8 times more effective than an unalerted search, as knowing where to look greatly increases the chances of sighting traffic. Similarly, an FAA research report (Andrews 1977) suggested that unalerted pilots may take 9 times longer to react than alerted pilots.
The ATSB research report Aircraft performance and cockpit visibility study supporting investigation into the midair collision involving VH-AEM and VH-JQF, near Mangalore Airport, Victoria on 19 February 2020 (AS-2022-001) contains more information on the human performance limitations of the see-and-avoid principle.
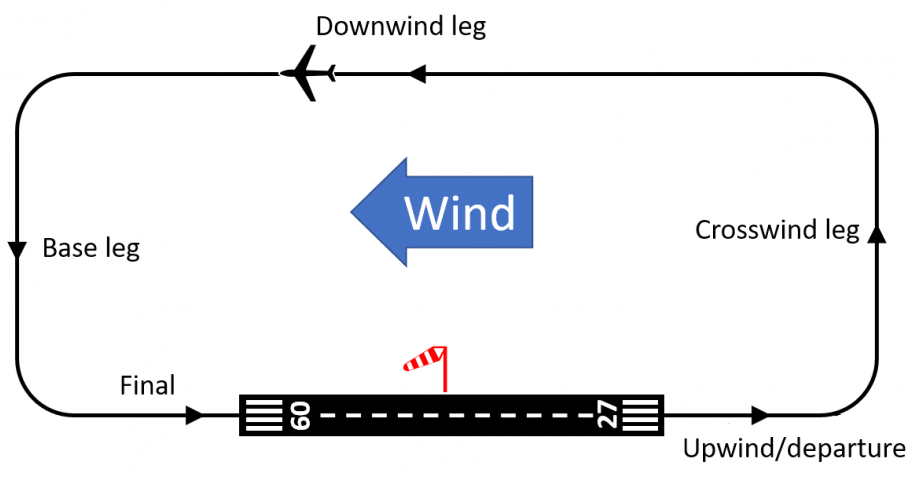
Standard circuit pattern
A circuit is the specified path to be flown by aircraft operating in the vicinity of an aerodrome (Figure 9). It comprises upwind, crosswind, downwind, base and final approach legs.
Figure 9: Standard left-hand circuit pattern
Source: SKYbrary, modified by the ATSB
Regulations and right of way
Part 91 of the Civil Aviation Safety Regulations 1998 (CASR) consolidates all of the general operating and flight rules for Australian aircraft and contains regulations detailing pilot responsibilities in relation to rules for the prevention of a collision, operating near other aircraft, right of way and operating in non-controlled airspace. These included but were not limited to the following regulations:
91.330: Right of way rules
91.335: Additional right of way rules
91.340: Right of way rules for take-off and landing
91.365: Taxiing or towing on movement area of aerodrome
91.370: Take-off or landing at non-controlled aerodrome—all aircraft
91.375: Operating on manoeuvring area, or in the vicinity, of non-controlled aerodrome—general requirements.
Right of way rules, which applied when there was a risk of collision between 2 aircraft, stated that when an aircraft is landing:
Any other aircraft (whether in flight or operating on the ground or water) must give way to the aircraft that is landing.
Regulations describing take-off and landing procedures stated that a pilot may not commence take-off until certain circumstances are met, including:
…if another aircraft is landing before the subject aircraft and is using a crossing runway—the other aircraft must have crossed, or must have stopped short of, the runway the subject aircraft is taking off from.
Regulation 91.370 prevented a pilot who is preparing to land from continuing an approach to land beyond the runway threshold if another aircraft is taking off on the same runway. These were not intended to take precedence over right of way rules, in the event of a collision risk. There was no specific regulation governing the continuation of a landing when another aircraft is taking off on a crossing runway.
When an aircraft is taxiing at an aerodrome:
the aircraft and any tow vehicle must give way…to an aircraft that is landing or on its final approach to land[12]
Land and hold short operations (LAHSO) are a set of internationally recognised procedures to allow a landing aircraft to land and hold short of a runway intersection while a crossing runway is simultaneously used by another aircraft. LAHSO is subject to stringent safety standards and training requirements, and applies only to controlled aerodromes (where aircraft in the area are directed by an air traffic controller). LAHSO procedures are therefore not applicable at a non-controlled aerodrome such as Caboolture.
In all other circumstances, including at non-controlled aerodromes, aircraft in flight or on the ground must give way to a landing aircraft as stated above.
When 2 aircraft are on converging headings at approximately the same altitude, the aircraft that has the other aircraft on its right must give way to the other aircraft.
Regulation 91.335 required that, when there is a risk of collision between 2 aircraft, the aircraft with right of way must maintain the same heading and speed until there is no longer a risk of collision. However, the regulation also stated that the avoidance of a collision takes precedence over compliance with these rules. Where an aircraft is required to give way to another aircraft, the aircraft must not be flown so that it passes ahead, or directly over, or under the other aircraft so close that there is a collision risk.
Advisory circulars
CASA published plain-language and explanatory guidance on the regulations in the form of advisory circulars (ACs) and other material. The following advisory circulars issued by CASA provided guidance to pilots operating at non-controlled aerodromes, including ALAs:
AC 91-10 - Operations in the vicinity of non-controlled aerodromes
AC 91-14 - Pilots’ responsibility for collision avoidance.
Regarding operations at non-controlled aerodromes, AC 91-14 noted that ‘rules of the air regarding right of way and rules for prevention of collisions must always be respected.’
The advisory circulars also outlined ‘alerted see-and-avoid’ principles and highlighted their importance for maintaining separation at non-controlled aerodromes. AC 91-14 gave guidance on visual searches and stressed the importance of improving a pilot’s situation awareness beyond reacting to what they can see using tools such as radio, ADS-B, and other electronic systems used for traffic avoidance. It stated:
The primary tool of alerted see-and-avoid that is common across aviation—from sport and recreational to air transport—is radio communication.
Carriage of radios
Part 91 of the CASR did not require aircraft to carry a radio when in the vicinity of uncertified aerodromes (such as Caboolture Airfield), but a radio was required in the vicinity of certified aerodromes (CASR 91.400).[13] Some aerodromes, including Caboolture, had a relevant instruction in the En Route Supplement Australia (ERSA) that required the carriage and use of a radio (see En Route Supplement Australia).
Mandatory and recommended radio calls
CASR 91.630 made certain radio calls (listed in the Part 91 Manual of Standards) mandatory for aircraft that are fitted with or carry a radio. The Part 91 Manual of Standards prescribed one type of mandatory broadcast at a non-controlled aerodrome, namely:[14]
When the pilot in command considers it reasonably necessary to broadcast to avoid the risk of a collision with another aircraft.
AC 91-10 reinforced this requirement and also stated:
Whenever pilots determine that there is a potential for traffic conflict, they should make radio broadcasts as necessary to avoid the risk of a collision or an Airprox event.
The Airservices Aeronautical Information Publication[15] stated:
In Class G [uncontrolled] airspace, pilots … should monitor the appropriate [radio] frequency and announce if in potential conflict. Pilots intercepting broadcasts from aircraft which are considered to be in potential conflict must acknowledge by transmitting own callsign and, as appropriate, aircraft type, position, actual level and intentions.
CASA recommended certain other broadcasts at a non-controlled aerodrome or dependent on traffic. AC 91-10 stated:
Pilots are reminded they are required to make all broadcasts necessary to avoid the risk of a collision with another aircraft as prescribed by Section 21.04 [Non-controlled aerodromes — prescribed broadcasts] of the Part 91 MOS. Table 5 [Recommended broadcasts in the vicinity of a non-controlled aerodrome] … contains the recommended broadcasts to achieve this requirement.
The recommended calls for non-controlled aerodromes included when a pilot:
intends to take off
is inbound to an aerodrome.
Calls that were recommended dependent on traffic included when:
a pilot intends to enter a runway, including crossing a runway
a pilot is joining a circuit
theaircraftisclearoftheactiverunway(s).
Limitations of radio communication
Positional broadcasts are a one-way communication, intended to provide a short and concise broadcast to minimise radio channel congestion. They do not imply receipt of information by other parties unless direct radio contact is made between stations to acknowledge the traffic, confirm intentions and, if required, discuss measures to provide deconfliction.
The VHF radio requires line of sight between both stations in order to function effectively. If an aircraft does not have a clear visual path direct to another in the vicinity, then the radio wave signal strength and clarity can be affected by obstacles. In some cases, terrain, vegetation or buildings can create areas that may shield or substantially reduce radio wave propagation and adversely affect broadcast signal strength and clarity.
AC 91-14 also advised:
Pilots should be mindful that transmitting information by radio does not guarantee receipt and complete understanding of that information. Many of the worst aviation accidents in history have their genesis in misunderstanding of radio calls, over-transmissions, or poor language/phraseology which undermined the value of the information being transmitted.
Without understanding and confirming the transmitted information, the potential for alerted see-and-avoid is reduced to the less safe situation of unalerted see-and-avoid.
AC 91-10 stated:
Pilots are reminded that although correct and informative radio calls play a critical role in ensuring collision avoidance in uncontrolled airspace, to ensure the safety of their aircraft they cannot assume that an absence of other radio calls means there are no nearby or conflicting aircraft…Pilots must continually look out for other aircraft, even when their broadcasts have generated no response.…
Pilots should not be hesitant to call and clarify another aircraft’s position and intentions if there is any uncertainty.
It is essential that pilots maintain a diligent lookout because other traffic may not be able to communicate by radio. For example, the other pilot may be tuned to the wrong frequency, selected the wrong radio, have a microphone failure, or have the volume turned down.
Runway use
Determination of ‘active runway’
The concept of an ‘active runway’ for non-controlled aerodromes was not defined in the regulations. The Part 91 Manual of Standards did not explicitly define the term, but referred to it in a paragraph about aircraft lighting (original emphasis):
[white strobe lights must be displayed] if the aircraft, on its way to the runway from which it will take off, or on its way from the runway on which it has landed, crosses any other runway that is in use for take-offs or landings (an active runway) — while the aircraft is crossing the active runway;
The same passage, slightly paraphrased, was also included in the CASR Part 91 Plain English Guide.[16] The following definition was provided as guidance in AC 91-10:
Active runway: The runway most closely aligned into the prevailing wind, or, in nil wind, or when predominantly all crosswind, it is the runway in use.
Landings and take-offs should be made on the active runway or the runway most closely aligned into wind.
Use of multiple runways
The advisory circular AC 91-10 made the following statements regarding ‘active’ and ‘secondary’ runways (each in separate sections):
• Pilots should be vigilant when using a runway that is not the active runway to ensure that they do not create a hazard to aircraft using the active runway.
• Landings and take-offs should be made on the active runway or the runway most closely aligned into wind.
• If a secondary runway is being used (e.g. for crosswind or low-level circuits), pilots using the secondary runway should not impede the flow of traffic using the active runway.
The CASA Visual Flight Rules Guide stated:
If a secondary runway is being used, pilots using this secondary runway should avoid impeding the flow of traffic on the active runway.
Other information on the use of runways at non-controlled aerodromes
Other than as stated above, there were no regulations or guidance applicable to the use of non-controlled aerodromes about:
determination of which runway is ‘active’, ‘secondary’ or ‘in use’ in the context of the relevant guidance
the use of runways that were not the active runway
stopping prior to entering a runway.
Caboolture Airfield information and procedures
Caboolture Airfield
As stated previously, Caboolture Airfield was a non-controlled aerodrome owned by the Queensland State Government and leased to the Caboolture Aero Club (CAC) for the aerodrome’s operation and management. It was an uncertified aerodrome, also known as an ALA. It was located about 3.5 km east of Caboolture, Queensland, with an elevation of 40 ft above mean sea level. Based on interviews with pilots familiar with Caboolture, the airfield sometimes had relatively high traffic volumes for an ALA, with a diverse traffic mix including light sport aircraft, weight shift aircraft, helicopters, gliders and warbirds. Several flight schools conducted both fixed-wing and helicopter flight training at the airfield.
Caboolture Airfield had 2 intersecting runways with magnetic orientations of 114°/294° (runway 11/29), and 065°/245° (runway 06/24). Their lengths were 1,129 m and 820 m respectively. Both runways were unsealed grass, except for a sealed portion at the beginning of runway 11.
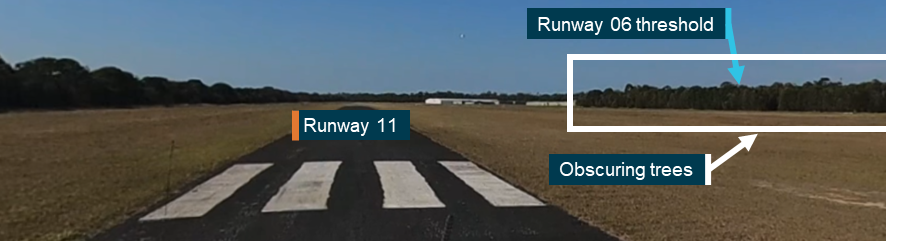
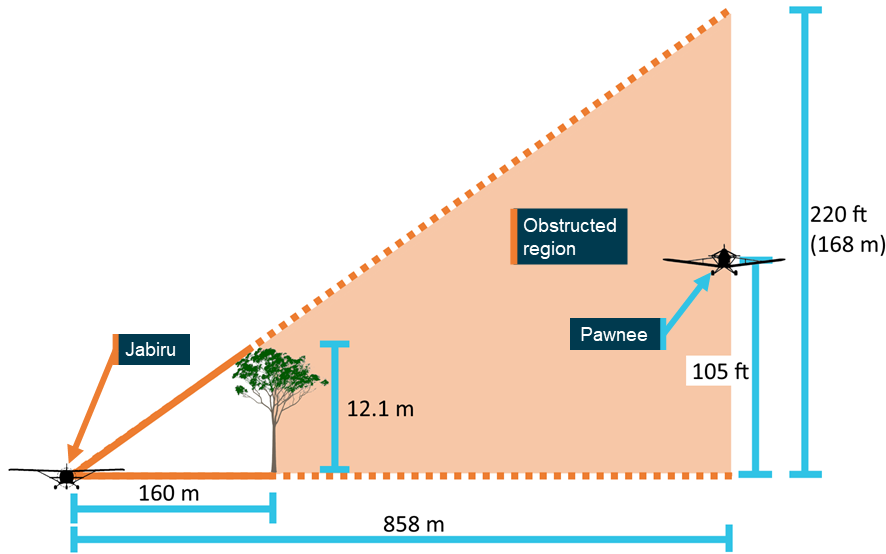
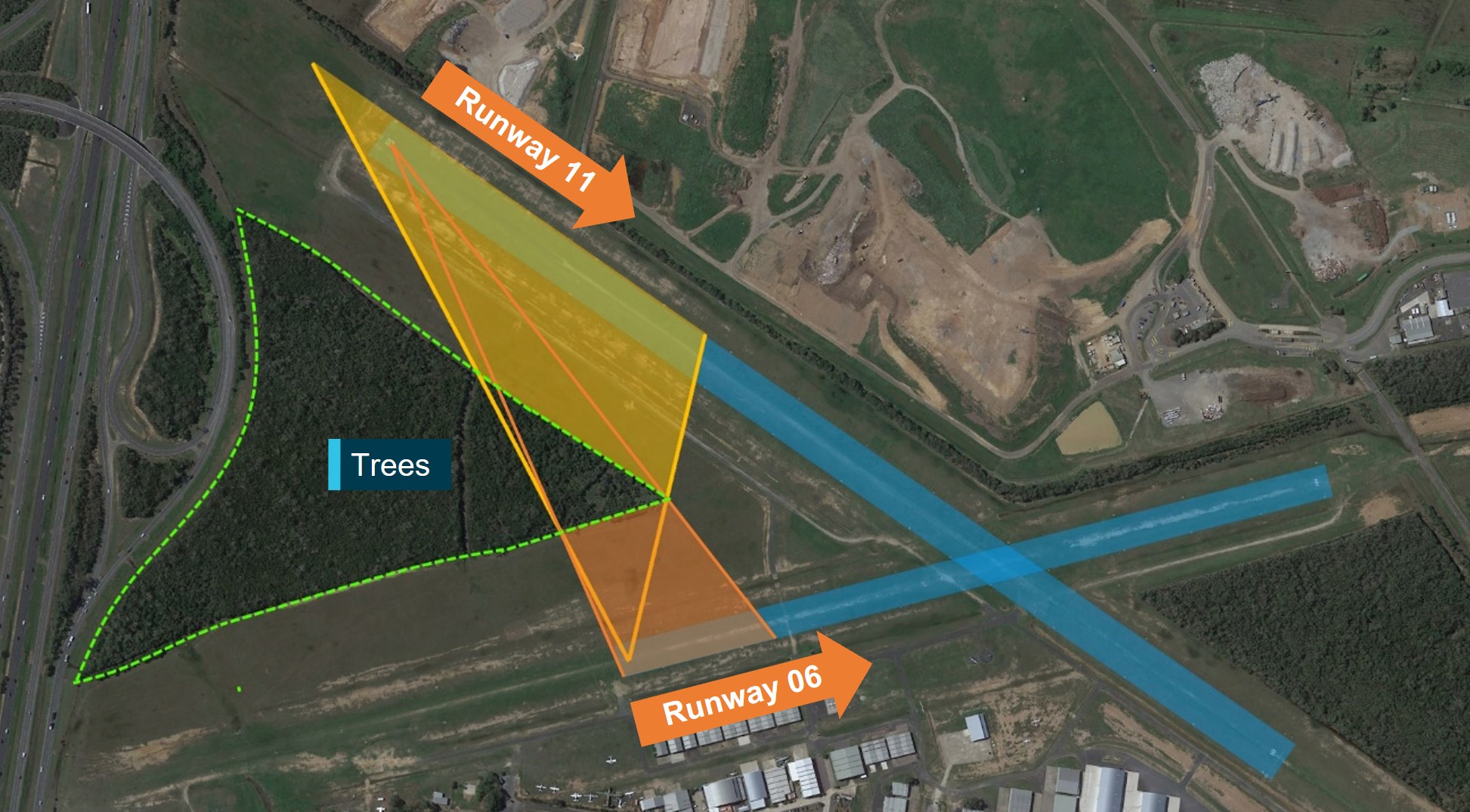
Two different stands of evergreen trees were established between the intersecting runways (Figure 10). The stand between the arrival ends of runway 06 and runway 11 was dense and it was not possible to see through it. Site measurements found that at its eastern-most point, the trees were at a height of about 9.5 m, but elsewhere, the trees were approximately 14 m high (the terrain itself is relatively flat). The northern border of the aerodrome was marked by a fence and a line of trees. Hangars, training schools and other administrative buildings stood to the south of the 2 runways. From the perspective of any of the 4 runway thresholds, the trees and buildings around Caboolture Airfield prevented pilots from being able to see either end of the intersecting runway (Figure 11 and Figure 12).
The ATSB estimated that the first 460 m of runway 11, and the first 180 m of runway 06, would not be visible from the other runway’s threshold. Visibility between the runways was significantly more affected if an aircraft was using the 250 m section prior to the runway 06 threshold (which was permitted for take-off only) (Figure 10, Figure 11, and Figure 12).
Figure 10: Obscured parts of the adjacent runway from the thresholds of runways 11 (orange) and 06 (blue) while at ground level
The shaded areas illustrate the areas that would not be visible from the threshold of the other runway. Source: Google Earth, annotated by the ATSB
Figure 11: Perspective from ground level at the threshold of runway 11
Source: ATSB
Figure 12: Perspective from ground level at the threshold of runway 06
Source: ATSB
Operations manual
Though not required to do so by regulation, the CAC maintained and published a Caboolture Airfield operations manual (available to the public on the club’s website), detailing procedures for pilots intending to operate at Caboolture Airfield. The most recent revision was 2.0, issued in March 2023. The manual did not take precedence over the CASR.
The Caboolture Airfield operations manual noted that traffic at the thresholds of runways 11 and 29 would not be visible if taking off before the threshold of runway 06 (pilots were permitted to commence take-off 250 m before the threshold of runway 06). It stated that aircraft towards the departure end of runway 06 might not be visible from before the landing threshold due to a crest in the runway.
The Caboolture Airfield operations manual stated (original emphasis):
Aircraft shall obey the standard Rule of the Air of ‘giving way to aircraft' established on final.
En Route Supplement Australia
Background
Information about controlled and non-controlled aerodromes around Australia was published in the En Route Supplement Australia (ERSA). The ERSA was part of the Airservices Australia AIP and published by Airservices Australia but the details for each aerodrome were provided by the aerodrome operator. CASR 139 required operators of certified aerodromes to ensure there was adequate aerodrome information in the ERSA. The types of information required included telephone numbers, runway specifications, lighting, visual aids, available ground services, local traffic regulations, special procedures and local precautions.
While there was no obligation for an uncertified aerodrome like Caboolture to have an ERSA entry, one had been submitted and maintained by CAC as the aerodrome operator. As a result, the CAC was considered to be an ‘aeronautical data originator’ under the regulations, and was therefore responsible for keeping the ERSA entry up to date.
ERSA information for Caboolture Airfield
The ERSA information for Caboolture Airfield noted the presence of gliding operations. It stated that trees may ‘encroach on Transitional Slopes gradients’; that is, may not meet obstacle clearance criteria that are mandated only for certified aerodromes. The effect of the trees on visibility between runways was not noted. The ERSA information advised visiting pilots to refer to the Caboolture Airfield operations manual synopsis available on the ‘aero club’ (CAC) website. This synopsis referred to a one-page appendix containing a quick reference handout with basic aerodrome and circuit information. This did not mention visibility between runways. However, as discussed in Guidance on the use of runways, the Caboolture Airfield operations manual noted visual obstructions elsewhere.
The ERSA information for Caboolture also stated: ‘Carriage and use of radio is required by the AD OPR [aerodrome operator].’ There was no regulatory requirement for pilots to follow specific aerodrome instructions of this nature that are in the ERSA, except with regard to circuit direction and at controlled aerodromes. However, according to AC 91‑10, such instructions may be considered a condition of use imposed by the aerodrome operator.
Relevant information for other aerodromes
An ATSB review of ERSA information (2024 data) identified 27 entries for non-controlled aerodromes, including 6 entries for uncertified aerodromes[18] that included information about visual obstructions between runways. ERSA entries for 4 uncertified aerodromes noted obstructions between intersecting runways or intersecting runway centrelines (where the runways themselves do not intersect but the approach and departure flight paths do). The other 2 entries were for visibility between both ends of the same runway.
The ATSB examined the relevant guidance associated with the visual obstructions. The entry for Casino required pilots to broadcast their intentions before operating on the runway, Great Lakes Airfield stated that a pilot must confirm that runways are clear prior to take-off or landing (without specifying the means to do so, but likely via radio), and 3 others required a radio to be carried and used (in a similar manner to the ERSA entry for Caboolture). None directly linked these requirements to the visual obstructions.
There were also 19 entries for certified, non-controlled aerodromes that included information about visual obstructions between runways or runway ends.[19] Of these, 9 entries stated that certain radio calls were to be considered mandatory, and all of these linked the requirement to the visual obstructions.
Guidance on the use of runways
Standard left circuits were specified at Caboolture, except for runway 29, which was a right circuit.
With regard to which runway was preferred for use, the Caboolture Airfield operations manual stated:
The active runway is the RWY [runway] most into wind and the runway being used by other aircraft at the time of your departure or inbound radio broadcast. Other runways may be used with radio notification to other traffic and with priority given to other aircraft already established in the circuit of the runway in use (the active runway) and with awareness of the Glider Launch point operations.
Regarding selection of runways by pilots, the manual stated:
The pilot in command of an aircraft has the authority to select the runway most suited to the performance and operational requirements for the safe operation of their aircraft however, with combined operations the active runway is usually the one required by aircraft with the poorest cross wind capability. These factors may be less important to pilots of fast, heavy aircraft who are more interested in the length of runway available for safe operations.
All operators at YCAB [Caboolture Airfield] are advised that any pilot selecting a runway other than the one which is clearly the ‘active’ runway (by virtue of into wind and minimum cross wind component and established circuit traffic), or that has been nominated as the ‘active’ runway by a radio information communication, then such pilot will lose all right of way privileges and shall conduct the landing or take-off procedure such as to give way to, and maintain separation from all other circuit traffic.
The manual also described the gliding operations at Caboolture, and outlined the concept of a ‘launch point’: a base of operations for unpowered aircraft such as gliders, centred around a camping trailer that acted as a mobile administrative office. The manual stated:
The launch point is usually established at a point on the airfield that minimises the time and effort required to retrieve the aircraft after landing and remain clear of the active runway so that the launch crew or parked aircraft do not impede the landing or taxiing aircraft.
The Caboolture Airfield operations manual did not state the gliding club’s general preference to use runway 06 (see Gliding club information).
Based on interviews with pilots at Caboolture, including members of the CAC, in light or variable wind conditions, there was a general preference for runway 11. There were 2 main reasons for this:
Runway 11 was the only runway with a paved section just beyond the threshold. All other runways were unsealed grass.
Although open at the time of the occurrence, runway 06/24 had been closed for resurfacing for a long period of time (see Closure of runway 06/24), so operators had developed a habit of simply not using it.
Radio communications at Caboolture Airfield
The common traffic advisory frequency (CTAF) was 125.85 MHz, which was a frequency shared with Caloundra Airport, 32 km north-north-east of Caboolture.
The Caboolture Airfield operations manual stressed the importance of radio communication at Caboolture, and required that all aircraft – including gliders – carry a VHF radio tuned to 125.85 MHz. Regarding mandatory broadcasts, the manual required pilots to make an inbound call when 10 NM from the aerodrome, or at a known geographical feature. No other mandatory calls were listed, and the manual referred readers to the CASA advisory circular AC 91-10 (see Mandatory and recommended radio calls).
The Cessna pilot stated that they were trained to always make a radio call when crossing a runway, with the exception of runway 06/24 at Caboolture, where they were told not to make a call based on instructions from the CAC. An instructor at the Cessna pilot’s flying school reported telling students to generally avoid making a runway crossing call for runway 06/24 while the runway was closed, which they also recalled was based on a change to CAC procedures. The CAC did not have a record of a directive or change in policy regarding crossing calls. Several Caboolture operators interviewed by the ATSB advised that crossing calls had been a subject of ongoing discussion at the CAC. Some questioned the benefits of making a crossing call when there was no chance of a conflict with other traffic, arguing that such calls only added more crowding on an already congested radio frequency.
Closure of runway 06/24
Runway 06/24 was closed for resurfacing in December 2021, and reopened on 6 April 2023. Because Caboolture was an uncertified aerodrome, there was no regulatory requirement for hold point markings. However, runway hold point markings had been previously present on the taxiway across runway 06/24, but they were removed when the taxiway was repaved as part of the resurfacing (Figure 13). At the time of the occurrence, these lines had not been repainted. Hold point markings were still present on runway 11/29 (Figure 14).
Figure 13: Taxiway across runway 06/24 without hold point markings
Source: ATSB
Figure 14: Hold point markings at the threshold of runway 11
Source: ATSB
Gliding club information
General information
The Caboolture Gliding Club (CGC) was responsible for all unpowered glider operations conducted at Caboolture Airfield. Gliding operations were generally conducted on Fridays, Saturdays and Sundays. The CGC headquarters was situated near the threshold of runway 06. The club also used a camping trailer as a mobile base of operations that could be towed to the launch point during gliding operations. The positioning of the base would depend on which runway the CGC deemed was most appropriate for gliding operations for a given period. All unpowered gliders were towed into the air using the Pawnee.
The process for towing gliders from runway 06 was as follows: a pilot would check for conflicting traffic on runway 11/29 via radio. If clear, the pilot would tow a glider into the air using the Pawnee, then release it from the tow rope after gaining sufficient altitude. The Pawnee pilot would then re‑join the circuit for runway 06 after it released, land while stopping short of the runway intersection, then backtrack to the launch point to pick up any other gliders for aerotow. The tow rope, which can be jettisoned in an emergency, would normally remain attached to the tow aircraft throughout.
Runway selection
Runway selection is important for towed glider take-offs as well as landings. The CGC’s documented standard operating procedures stated:
Before moving any equipment to the flight line the Duty Instructor will consult with the Tug [tow] Pilot to determine the runway to be used.
There was no other information within the procedures regarding runway selection and the procedures did not discuss potential visibility issues between runways. If the winds were favourable or sufficiently light, and traffic on runway 11/29 was light, it was common on the first flights of the day for the gliders to be towed into the air from runway 06. This prevented members from having to hand-tow the gliders long distances from the hangars to other runways. The gliders could then land on whichever runway had been selected for operation by the duty instructor in consultation with the tow pilot. The CGC would sometimes use runway 06 throughout the day, depending on the prevailing winds, including during periods when runway 11/29 was being used by other aircraft. Several members stated that if the traffic volume on the intersecting runway became too high, the tow pilot or the duty instructor would decide to move gliding operations to the runway being used by the rest of the traffic.
The CGC reported that winds, both at ground level and aloft, were an important consideration in runway selection, particularly for glider launches and landings. On the morning of the occurrence, prior to any gliding operation, CCTV footage of the windsock near the runway intersection showed that there was a light (easterly) wind favouring runways 11 and 06 approximately equally. There was enough variability in the wind that at any given time, the windsock could be seen favouring runway 11 or runway 06. The CGC had its own windsock near the end of runway 06. This was not visible on CCTV cameras but would often show a different wind direction to the other windsock. The CGC duty instructor and Pawnee pilot reported observing a north-easterly wind on the morning of the occurrence.
The duty instructor assessed that traffic on 11/29 was light, later estimating one movement every 15 minutes. Based on this, it was decided that the gliders could be safely towed from runway 06 for the first flights. According to the information they used, winds were forecast to increase down runway 06 throughout the day. It was therefore decided that gliding operations would continue on runway 06 while the conditions permitted it.
Regarding runway selection for landing prior to the accident, the Pawnee pilot stated that they selected runway 06 prior to joining the crosswind leg based on the wind conditions at the time (established by their view of the 2 windsocks at the airfield).
After the accident, the ATSB surveyed 18 pilots familiar with Caboolture Airfield (including the Pawnee and Cessna pilots) about a range of topics. The relevant responses were as follows:
When asked about simultaneous intersecting runway operations at Caboolture, most pilots reported that the CGC had used runway 06, particularly for their first flights of the day while other traffic was operating on runway 11.
Their assessment of how often intersecting runways were in use concurrently was roughly evenly distributed between ‘rare’ and ‘often’.
None of the pilots believed it was common to hear tow pilots or others make radio calls to indicate they would be holding short of the runway intersection but some had heard that occur before with tow pilots.
None of the pilots could recall a previous situation where a landing pilot made a hold short call and a second pilot took off while the first aircraft was still in the process of landing.
Recorded data
On-board recording
The Pawnee carried no flight data recording devices, and no automatic dependent surveillance broadcast (ADS-B) transponder. An ADS-B transponder was fitted to the Jabiru but the ATSB did not identify any recorded ADS-B data from the Jabiru during the accident flight.[20]
The Jabiru was fitted with a Dynon SkyView SV-HDX1100 avionics system. The system was capable of recording flight data installed in the cockpit. Flight data from the accident flight was recovered from the damaged device at the ATSB’s engineering facility in Canberra (Figure 15). The unit recorded the latter part of the Jabiru’s taxi towards the hold point for runway 11, turning onto the perpendicular taxiway from about 1029:49–1029:59, and the data terminated at 1030:03 when the Jabiru was at the hold point. This likely coincided with the Jabiru coming to a stop, as reported by a witness, while another aircraft was departing on runway 11. Assuming the Jabiru’s average taxi speed from the hold point to the runway was the same as the recorded segment, the ATSB estimated that the Jabiru would have been stopped for about 2 seconds before commencing taxi to the runway, starting to turn onto the runway heading at about 1030:35.
Figure 15: Flight data recovered from the Dynon SkyView system in the Jabiru
Source: Google Earth, ATSB
The GPS data recording was re-established at 1030:56, as the Jabiru was on the threshold markings of runway 11, rolling on the runway’s heading at 13 kt. Data showed the Jabiru accelerating and taking off, then initiating a left turn before colliding with the Pawnee at a height of approximately 130 ft.
Video recording
Video footage of the accident was recovered from a closed-circuit television (CCTV) at Caboolture Airfield. The system included several cameras on buildings south of the runway intersection, aimed in different directions. Due to the limits of resolution and distance, the CCTV did not capture movement of the Jabiru near the threshold of runway 11. The Cessna crossing runway 06, the Pawnee initiating a go-around, part of the Jabiru’s take-off and the collision itself were all visible on the recordings.
An example of the footage provided by the CCTV system is shown in Figure 16. Timestamps from the CCTV footage were adjusted to align with the times provided by the Jabiru’s recorded GPS data.
Figure 16: Still from a CCTV camera located to the south of the runway intersection
Source: Caboolture Aero Club, annotated by the ATSB
Using the CCTV recordings, the ATSB logged aircraft movements in the hour prior to the accident. From 0930 until the Pawnee took off with the first glider at approximately 1005, there were 15 movements on runway 11. While the Pawnee was airborne on the first flight, an additional aircraft landed on runway 11. The next movement was the Pawnee landing on runway 06, then taking off with the second glider at 1022.
A review of the CCTV recordings found that from 0930 until the occurrence, 9 other aircraft used the same taxiway as the Cessna to cross runway 06. Of these, 8 aircraft, including the Jabiru, did not stop before crossing.
CTAF recording
CTAF broadcasts were not recorded at Caboolture Airfield, nor were they required to be. Recorded broadcasts were recovered from Caloundra Airport, which shared the same CTAF frequency. Due to distance and line of sight limitations, radio calls on or near the ground at Caboolture were generally not recorded, and some calls from within the Caboolture Airfield circuit were only partially recorded. There may have been other radio calls from aircraft in the vicinity that were not recorded.
Recordings of radio calls made by the Pawnee pilot were assessed by the ATSB as being clear and readable. The recordings included some two-way communication, indicating that the Pawnee’s radio was functional for transmitting and receiving at the time. There was no evidence in the recording of the sound associated with simultaneous radio calls interfering with one another (often referred to as heterodyning), and no witnesses recalled hearing any such interference on the morning of the accident. Several pilots who flew at Caboolture stated that heterodyning was relatively common due to frequency congestion.
Aircraft visibility
Using CCTV footage and recorded GPS data from the Jabiru, the ATSB conducted an analysis to determine when the pilots of the Pawnee and Jabiru may have had an opportunity to see one another based on whether there was a line of sight between their relative locations and the location of trees around the airfield, and on the orientations of the 2 aircraft.
While taxiing towards the hold point near the threshold of runway 11 (facing north-east from about 1027:25 to about 1029:58), the Jabiru pilot might have been able to observe the Pawnee in the downwind or base legs of the (runway 06) circuit. Once the Jabiru had turned towards the hold point, the Pawnee was on or turning onto the base leg, putting it almost directly behind the Jabiru. Approximate positions of the Pawnee and Jabiru are shown in Figure 17.
Figure 17: Approximate positions of the Jabiru and Pawnee
Positions of the Pawnee were approximated based on CTAF transmissions, assuming a 1 NM wide circuit. The take-off time was estimated by extrapolating the Pawnee’s position backwards from when recorded data recommenced at 1030:56. Source: Google Earth, annotated by the ATSB
Without flight data for the Pawnee, and given the perspective of the camera, the Pawnee’s position and altitude could not be determined to a high degree of accuracy. For the purposes of estimating the Pawnee’s position, it was assumed that during the final approach the Pawnee maintained the same heading as runway 06, along the centreline, with a constant speed and a 3° angle of descent.
The Pawnee pilot later recalled seeing 2 aircraft near the threshold of runway 06 while the Pawnee was on the base leg of the circuit, one of which was about to take off. At this point, the Jabiru was taxiing towards the hold point near the threshold of runway 11, and a third aircraft was conducting engine run-ups in the nearby run-up bay. It could not be determined which 2 of the 3 aircraft the Pawnee pilot saw.
At the time the Jabiru had commenced its take-off roll, the Pawnee (on final approach) would have descended to about 105 ft and the trees would have obstructed line of sight from this point onwards. This was determined using a trigonometric calculation based on the assumptions described above (Figure 18). The trees would also have obscured line of sight from earlier than this, possibly from when the Pawnee descended below about 220 ft (a more precise estimate could not be made due to uncertainties about the Pawnee’s height and location on the downwind and base legs of the circuit). If the Pawnee’s descent rate had been constant throughout the final descent, it would have likely descended below 220 ft at about 1030:29, when the Jabiru was likely taxiing towards the runway.
Figure 18: Tree line obstruction height calculation when the Jabiru began its take-off roll
Not to scale. This calculation shows that the Jabiru and the Pawnee were not visible to one another when the Jabiru began rolling on runway 11. The Pawnee was estimated to be 105 ft high at this point. Assuming the Jabiru pilot’s view was 2 m above the ground, the 14.1-m trees blocked the Jabiru’s view up to 220 ft. Source: ATSB
By the time the Jabiru had turned onto the runway heading at about 1030, the Pawnee would have been behind the Jabiru and below the tree line from the perspective of the Jabiru pilot.
The trees would have prevented the 2 pilots from observing one another up until they were over their respective runways and had passed the end of the stand of trees, at approximately 1031:15. At this point, the Jabiru had only just lifted off the ground, and the Pawnee was just about to begin climbing, having almost touched down prior to commencing the go-around. The point in time that the line of sight was regained is illustrated in Figure 19. At this time, the Pawnee was about 75° to the right of the Jabiru’s heading, and the Jabiru was about 55° to the left of the Pawnee’s heading.
Figure 19: Sightlines between the 2 aircraft as they climbed from the aerodrome
Source: Google Earth, annotated by the ATSB
At this point, both of the aircraft would have been visible to each other, in the occupants’ peripheral vision if they were looking directly ahead. Objects in a person’s peripheral vision are more difficult to detect due to a number of factors including limitations from visual clutter and reduced visual acuity (Rosenholtz, 2016). During this period until the collision, there would have been very little relative movement of the aircraft in each field of view, making detection difficult.[21] Visual detection of objects is also strongly dependent on a person’s attention, head position and potential sight-blockers from the aircraft itself, such as a passenger, cockpit pillars, aircraft nose, wing struts or wings. The ATSB assessed that it was possible that the Pawnee’s structure blocked the pilot’s potential view of the Jabiru.
Related occurrences
Collisions or near collisions at non-controlled aerodromes
From 2013–2023 in Australia, there were 8 other reported collisions between 2 heavier‑than-air[22] aircraft at non-controlled aerodromes, where at least one of the aircraft involved was either in the aerodrome circuit, taking off, landing or taxiing.[23]
From 2013–2023 there were 118 reported near collisions[24] at non-controlled aerodromes. ATSB analysis indicated that, where relevant information was available, almost all of the incidents had 2 factors in common: a breakdown (or absence) of radio communication, and pilots not seeing each other’s aircraft. The following relevant types of communication issues were seen in the occurrences that were investigated:
pilots misinterpreting radio communications
one or both pilots not carrying a radio
radio equipment not functioning properly
radio transmissions not being heard
interference from other transmissions.
Over the same time period, at non-controlled aerodromes, the ATSB occurrence database was searched for any collisions, near collisions, instances of separation issues[25] or runway incursions where keywords in the occurrence summary indicated that intersecting runways were involved. The search found:
1 collision (excluding this accident)
7 near collisions
19 instances of separation issues
2 runway incursions.
The collision was investigated by the ATSB (AO-2015-023) and involved 2 aircraft landing on different runways that collided at the runway intersection. Both aircraft sustained substantial damage and the pilots were not injured. The ATSB found that although there were no visual obstructions between the 2 runways, the pilots did not see one another. One pilot reported having an awareness of the other aircraft being in the vicinity, but not seeing it due to it blending into the terrain. The other pilot reported not expecting another aircraft to be landing on the other runway. Neither pilot was using their radio.
A more recent example was a near collision in June 2023 at Mildura Airport between a Piper PA‑28 and a Bombardier DHC-8 (Dash 8). An investigation report was published on the ATSB’s website (AO‑2023‑025). Mildura was a certified, non-controlled aerodrome, and both flight crews were preparing for take-off. The Dash 8 crew believed the PA-28 was at a different aerodrome because the PA-28 pilot misidentified a runway in a previous radio call. The PA-28 pilot knew the Dash 8 was at Mildura, but believed it was still taxiing. Airport buildings prevented the PA-28 pilot from seeing the Dash-8. The Dash 8 started its take-off roll on runway 09 as the PA-28 made a rolling call on the intersecting runway 36. The Dash 8 crew did not make a rolling call, believing there to be no traffic at the airport. The Dash 8 crossed ahead of the PA-28 at the runway intersection by about 600 m.
The ATSB investigated a related runway separation occurrence at Mildura, in September 2023 between a Dash 8 and a Lancair Super ES. Both aircraft were preparing to depart, from intersecting runways. Due to communication issues as well as the buildings and topography around the airport, neither of the flight crews were aware of the other aircraft prior to the Dash 8 taking off and the Lancair giving a rolling call. The pilot of a third aircraft (behind the Lancair) heard the Dash 8’s call and advised the Lancair to hold position while the Dash 8 departed, which they did. An investigation report was published on the ATSB’s website (AO‑2023‑050).
Other incidents at Caboolture Airfield
Not including this occurrence, there have been 21 occurrences at Caboolture Airfield involving aircraft separation between 2013 and 2023. Four of these occurrences were classified as near collisions, and the others were separation issues. Three of the occurrences at Caboolture involved intersecting runway operations that were counted in the above list. These occurrences were reported, but not investigated and are summarised below:
In May 2021, the pilot of a Vans RV6 took avoiding action to pass below a Robinson R22 helicopter as both aircraft were departing on intersecting runways. The R22 crew reported not hearing radio calls from the RV6 (Near collision).
In April 2021, while on approach, the pilot of an Aeropro 2k Eurofox reported horizontal separation concerns with a tow aircraft and glider that were climbing from an intersecting runway. The pilot did not hear any radio calls from the tow aircraft or glider. The tow aircraft was not identified (Separation issues).
In May 2016, while landing on runway 30 (now runway 29), the crew of a Cessna 206 initiated a go-around to maintain separation with a Cessna 140 taking off from runway 24 (Separation issues).
Safety analysis
Introduction
While the Pawnee was on final approach to land on runway 06, the Jabiru pilot commenced a take-off on the intersecting runway 11. The Cessna taxied across runway 06 in front of the Pawnee, and the Pawnee pilot initiated a go-around to avoid a potential collision with it. While the Pawnee pilot did not see the Jabiru until immediately after the collision, the Jabiru pilot appeared to notice the Pawnee moments before the collision and turned, likely in an attempt to avoid the Pawnee. The leading edge of the Pawnee’s left wing struck the trailing edge of the Jabiru’s right wing. The Jabiru’s aileron and a section of outer wing separated as a result, and the Jabiru subsequently collided with terrain. This impact was not survivable, and the pilot and passenger were fatally injured. The Pawnee remained controllable and landed safely shortly after.
This analysis will discuss the events and conditions that led to the midair collision and/or increased safety risk.
Pilot awareness
Jabiru pilot’s awareness
The Jabiru pilot’s decision to take off as the Pawnee was on final approach indicated that either the Jabiru pilot was not aware of the Pawnee at all when commencing take-off, or had some awareness but elected to take off anyway.
As established in the Context section of this report (see Aircraft visibility), trees between the intersecting runways meant the Pawnee would not have been visible from the Jabiru for a significant part of the sequence of events, including the period leading up to the commencement of the take-off. The Jabiru pilot may have had an opportunity to see and/or hear the Pawnee during preparation for flight or taxi. However, even if the Jabiru pilot only had a general awareness of the Pawnee’s presence through seeing it earlier (such as when in the circuit), it would have been difficult to accurately project its flight path and predict its position.
The Jabiru pilot’s level of situation awareness was therefore highly dependent on whether they heard any or all of the Pawnee pilot’s radio calls. The Pawnee pilot’s account, statements from various witnesses and common traffic advisory frequency (CTAF) recordings from Caloundra Airport were all consistent (accounting for witness recollection) to determine that the Pawnee pilot made at least 4 radio calls indicating their position in the circuit for runway 06.
Examples of reasons the Jabiru pilot might not have heard and understood the Pawnee pilot’s calls include technical reasons, such as if the radio volume was turned down or other settings were incorrect, or the radio and associated equipment were not functioning correctly. No radio calls from the Jabiru were recorded, but this was as expected given the absence of other recordings from any aircraft on the ground (and the cut-off Pawnee transmissions). From a technical perspective, an examination of the Jabiru’s radio found that the device was probably functional, but it was not possible to determine the radio’s volume or other settings as well as the functionality of other components in the system such as the headset, cables and antenna. It is important to note that a problem with transmission does not necessarily indicate a problem with reception, or vice versa.
Notably, most witnesses including the Pawnee pilot did not hear any calls from the Jabiru. The Jabiru pilot was reportedly diligent in making radio calls. A pilot with their amount of experience would know the recommended calls, including when entering the runway and commencing take-off. Further, the pilot would not have been expecting a reply, so the absence of such responses would not have indicated a radio problem to the pilot. On the other hand, a pilot who sees other aircraft in the circuit area might notice the apparent absence of radio traffic (in which case they may suspect a radio issue and test it and/or discontinue the flight).
The possibility of undetermined human factors affecting the Jabiru pilot’s receipt and interpretation of the radio calls was considered. For example, there may have been some distraction preventing the pilot from hearing or understanding the calls. However, if this were the case it is unlikely that the receipt of all 4 radio calls in the circuit was affected to an extent that the Jabiru pilot was completely unaware of an aircraft in the circuit for runway 06.
Alternatively, if the Jabiru pilot was aware of another aircraft using the intersecting runway, it is possible that they heard and understood the ‘land and hold short’ call from the Pawnee, and therefore determined that it would be safe to take off, expecting the Pawnee to hold short of the intersection, or believing that one of the aircraft would pass the intersection significantly behind the other. However, the pilot had extensive flying experience and was very likely familiar with the rules of the air (which did not permit a take-off before the intersecting runway was clear), and the Pawnee pilot reported never seeing a pilot act on such a call previously.
Another possibility is that the Jabiru pilot misheard or misinterpreted radio calls from the Pawnee, and believed the Pawnee had already stopped short of the intersection (but was not visible due to the trees). This belief could have been reinforced by the other aircraft departing on runway 11 prior to the Jabiru. However, if the Jabiru pilot had been generally aware of another aircraft using the intersecting runway (whether or not the pilot thought it had landed), it is unlikely they did not then hear and react to the go-around call or alter the Jabiru’s flight path unless there were other factors involved. None of the witnesses heard any transmissions from the Jabiru after the Pawnee announced the go‑around, and the Jabiru continued on a fairly straight climbing path.
If the Jabiru pilot had initially not been aware of the Pawnee but did hear its go-around call, they probably would have then been looking out for it from that point onward until the pilot made an apparent avoidance manoeuvre about 6 seconds before the collision. There was also no radio call received by others at this time.
There were 2 occupants of the Jabiru, and the Pawnee was visible for a 9-second period before the apparent evasive manoeuvre began. This is less than, but close to, the 12.5 seconds that the United States Federal Aviation Administration determined it would take from a pilot seeing an object to evasive action beginning, if the pilot is not alerted to the other aircraft’s presence. As suggested by related research (Hobbs 1991, Andrews 1977), an alerted pilot would likely see, recognise, and react to the other aircraft much more quickly. However, visual searches and reaction times are highly variable and, in this case, the Jabiru pilot’s reaction time alone does not clearly indicate whether they would have been aware or unaware of the Pawnee before it became visible.
In summary, although other possibilities could not be completely excluded, the possibility that the Jabiru pilot was not aware of the Pawnee’s presence on runway 06 until immediately before the collision is significantly more consistent with the established evidence and expected pilot behaviour. Therefore, a problem with the Jabiru’s transmission and reception of radio calls is the simplest and most compelling explanation for the absence of radio calls from the Jabiru, the pilot’s apparent unawareness of the Pawnee until just before the collision, and consequently, the pilot’s decision to take off as the Pawnee was landing.
Ultimately, however, the reasons for the Jabiru pilot’s likely non-awareness of the Pawnee could not be established with certainty. In any case, if the Jabiru pilot was not expecting other traffic they would have been less likely to see the Pawnee when it came into view. As established above, the relative movement of the Pawnee would have been slight and the view from the Jabiru cockpit could have been impeded by the aircraft’s structure (such as its high wing, wing strut, and/or cockpit pillars).
Contributing factor
The Jabiru pilot likely unknowingly could not transmit or hear radio calls, and was probably not aware of the Pawnee being on final approach to runway 06 when they decided to commence take-off on runway 11.
The Jabiru’s steep left turn was likely an attempt by the pilot to avoid collision, indicating that they saw or became aware of the Pawnee at that time. Given that this was done immediately before the collision, the pilot’s choice to turn left (rather than right, or to descend) was probably mostly reactive rather than with consideration of factors such as the flight paths or a potential collision with the tow cable.
Pawnee pilot’s awareness
The Pawnee pilot saw aircraft near the threshold of runway 11 while on the base leg of the circuit, although it could not be determined whether the Pawnee pilot saw the Jabiru taxiing towards the hold point, or the other aircraft in the run-up bay. Due to the sightlines being obscured, the Pawnee pilot would not have been able to see the Jabiru for much longer, losing visibility after descending below about 200 ft. At this time, the Jabiru was likely taxiing towards the runway. Accordingly, it would not necessarily have been clear to the Pawnee pilot how soon the Jabiru would be commencing take-off.
At non-certified aerodromes it was recommended, but not mandated, that pilots make a radio call for take-off, and if traffic necessitated it, for entering a runway. However, the Pawnee pilot did not hear the Jabiru pilot make a radio call for entering runway 11 or for commencing the take-off.
Of the other witnesses with access to a radio, 2 reported hearing a rolling (take-off) call from the Jabiru, while 6 did not hear any Jabiru calls. These types of call are very common at busy aerodromes such as Caboolture, and (especially if not relevant to the listener at the time) could be easily misremembered, not noticed, or confused with another aircraft’s call, and people can also inadvertently construct false memories (Foster & Garry 2012).
An examination of the Pawnee’s radio following the accident found it to be functioning normally and set to the correct frequency. The CTAF recordings show that the Pawnee pilot heard and responded to calls from other aircraft, and there were no recordings of any aircraft on the ground at Caboolture Airfield. As discussed above, it is also possible that the Jabiru’s radio was not fully functional, or not set correctly.
Radio transmissions interfering with one another was considered as a possibility in this occurrence. A call from a taxiing aircraft at Caloundra Airport at 1030:32 could have hypothetically been made at the same time as an entering and rolling call from the Jabiru pilot. However, this was determined to be improbable, since none of the witnesses recalled a heterodyning sound and it is unlikely that a transmission 32 km away would be significantly stronger than one at the same aerodrome unless there was a problem with the Jabiru’s radio.
If a take-off call was not transmitted from the Jabiru, it is possible that the 2 witnesses who recalled hearing it might have mistaken the taxi call at Caloundra for a take-off call. Given the conflicting witness accounts, uncertainty over the functionality of the Jabiru’s radio, and the number of plausible scenarios, it could not be determined whether the Jabiru pilot attempted to transmit a take-off call before the Jabiru departed on runway 11.
Regardless of whether a radio call was successfully transmitted by the Jabiru, it was not heard by the Pawnee pilot. This was evidenced by the Pawnee pilot’s statement, the absence of a radio response from the Pawnee pilot, their decision to continue climbing on the runway heading during the go-around, and the absence of any evasive manoeuvres prior to the collision, any of which could be expected if the Pawnee pilot had been aware of the Jabiru taking off.
During the landing the Pawnee pilot was aware of another aircraft about to take off on runway 11, but (reinforced by previous experience) was expecting the other pilot not to commence take-off until the Pawnee pilot had reported that they stopped short of the runway intersection. Having not heard an entering/rolling call, the Pawnee pilot had no indication that the other aircraft (the Jabiru) was actually taking off and no opportunity to see it until about 15 seconds before the collision (as both aircraft were climbing), because the stand of trees between runways blocked line of sight between the 2 aircraft. The ATSB assessed that it was possible that the Pawnee’s structure blocked the pilot’s potential view of the Jabiru.
In addition, there had just been a runway incursion ahead of the Pawnee pilot while in a high-workload phase of flight and they had just commenced a go-around. The Pawnee pilot was also focused on their climb rate, concerned about the clearance between the tow rope and the Cessna. The resulting distraction, surprise, and additional workload probably affected the ability of the Pawnee pilot to visually detect the Jabiru. Finally, the Jabiru would have exhibited very little relative movement in the Pawnee pilot’s field of view, making its detection more difficult.
Contributing factor
The Pawnee pilot did not hear an entering and/or rolling call from the Jabiru pilot, and it was not possible to establish from the available evidence whether a call was broadcast. In combination with the line of sight between them being blocked, the Pawnee pilot was therefore not aware that the Jabiru was taking off on the intersecting runway.
Cessna pilot’s awareness
While the Pawnee was in the circuit for runway 06, the Cessna pilot was conducting engine run-ups and pre-flight checks in the run-up bay adjacent to the runway. The pilot had turned the radio volume down in order to concentrate on the aircraft checks. Once these were completed, the Cessna pilot began taxiing towards the threshold of runway 11, and turned the radio back up. About 18 seconds after commencing taxi, the Cessna crossed runway 06/24. The radio volume being down until taxi restricted the pilot’s opportunity to be aware of any traffic operating at Caboolture, including the Pawnee intending to land on runway 06. Since the radio was not turned up until after the commencement of taxi (1030:51) the Cessna pilot would not have heard the Pawnee’s likely final call at 1030:19.
Most of the Cessna pilot’s flight training had been conducted when runway 06/24 was closed. After it was reopened, most operators at Caboolture preferred to use runway 11 provided wind conditions did not prevent it. Operators using Caboolture reported a general preference for runway 11, apart from the Caboolture Gliding Club (CGC), which preferred runway 06 for first flights. When the CGC was using runway 06, it was sometimes only for the initial glider flights, and the Cessna pilot would only have seen gliders operating on one day (Fridays) out of the 5 the pilot usually used the airfield. Consequently, the Cessna pilot was not used to seeing aircraft using runway 06.
On the morning of the occurrence, when the Cessna pilot first entered the aircraft, they heard the Pawnee pilot making radio calls in the circuit. However, during taxi and immediately prior to crossing runway 06, the Cessna pilot saw an aircraft take off from runway 11, and another aircraft (the Jabiru) lining up behind it. At that time, the Cessna pilot had an understanding that aircraft were currently operating on runway 11. Not expecting any traffic on runway 06/24, the Cessna pilot did not ‘clear’ the runway prior to crossing. The pilot also reported not coming to a complete stop before crossing the runway, and that due to the limited use of runway 06/24, they did not always come to a complete stop before crossing.
Only one of the other 9 aircraft that had taxied across runway 06 previously on that day had stopped. Although entering the runway as the Pawnee was landing contravened general flight rules, there was no obligation for the Cessna pilot to come to a full stop prior to crossing.
Contributing factor
The Cessna pilot did not hear the Pawnee pilot make a landing call, and had limited opportunity to be aware of traffic during taxi, due to having turned the radio volume down during pre-flight checks and not restoring it before taxi.
Contributing factor
Not having heard the Pawnee pilot's landing call and with most traffic using runway 11, the Cessna pilot had no expectation of an aircraft using runway 06, and taxied across the runway without stopping or looking for traffic while the Pawnee was landing. This resulted in the Pawnee commencing a go-around manoeuvre.
Pawnee pilot’s intention to hold short
While in the circuit, the Pawnee pilot was broadcasting the aircraft’s position and intentions in accordance with the alerted see-and-avoid principles used at non-controlled aerodromes. The Pawnee pilot’s radio call stating an intention to hold short of the runway intersection was not a standard call at non-controlled aerodromes, though it did not contravene any Civil Aviation Safety Authority (CASA) regulations or guidance.
Pilots using an intersecting runway would not be permitted to act contrary to the regulations on the basis of such a call because this would effectively be a type of land and hold short operation, which is not permitted at non-controlled aerodromes. In particular, if a pilot were to act upon an anticipatory ‘hold short’ radio call and take off or land on an intersecting runway under the assumption that the landing aircraft was going to hold short of the intersection, then that pilot would likely be contravening the general flight rules described in the Civil Aviation Safety Regulations. These rules require the pilot to wait until the landing aircraft has stopped short of the intersection, or crossed the intersection.
The Pawnee pilot’s aim was to provide information to other traffic at Caboolture airfield about their own intentions. However, a ‘holding short’ radio call could lead to other pilots expecting that the intersecting runway could be safely used when, in fact, there would be no certainty that the landing aircraft would be able to hold short. The possibility of a go‑around or long landing is always present. The potential for this call to have influenced the Jabiru pilot’s decision-making is discussed in Jabiru pilot’s awareness.
In the case of this accident, it was unlikely that the Jabiru pilot heard the Pawnee pilot’s hold short call (see Jabiru pilot’s awareness) so the call was probably not a factor in the Jabiru pilot’s decision to take off.
Other factor that increased risk
During the circuit call for turning onto the base leg, the Pawnee pilot stated that they would hold short of the runway intersection. While the Pawnee pilot did not intend other pilots to rely on it to avoid conflict, this call could have led to other pilots assuming that the intersecting runway could be safely used when there was no certainty that the Pawnee would be able to hold short.
Simultaneous operations at intersecting runways
Visibility between runways
A stand of trees was between the threshold of runway 06 and runway 11. The trees were between about 9 and 14 metres tall, and prevented pilots at one runway threshold from observing aircraft at the other.
The Pawnee and Jabiru pilots would have been able to observe each other’s aircraft for most of the time the Pawnee was in the circuit for runway 06. However, the ATSB analysis shows that the trees would have obstructed both pilots’ vision of each other, likely from about the time the Pawnee was on the final leg and certainly by the time the Jabiru had lined up with runway 11. Consequently, there would have been no opportunity for the Jabiru pilot to see the Pawnee landing on runway 06, or for the Pawnee pilot to see the Jabiru lining up and departing from runway 11.
Based on the analysis, there was no line of sight between the aircraft for about 46 seconds or more, until a point about 15 seconds before the collision, when the Jabiru was just lifting off and the Pawnee began climbing following the pilot’s decision to perform a go-around.
Contributing factor
A stand of trees between the intersecting runways prevented the Jabiru and Pawnee pilots from being able to observe one another, from no later than the time the Jabiru turned onto runway 11 for take-off until both aircraft had begun climbing.
Gliding club use of runway 06
Caboolture Airfield could be busy at times, involving a diverse mix of traffic including light sport aircraft, weight shift aircraft, helicopters, gliders and warbirds. It is an aircraft landing area (ALA), and therefore not subject to the same regulations imposed by CASA on certified aerodromes. However, CASA guidance about operations at non-controlled aerodromes still applied.
According to interviews, pilots using Caboolture generally preferred runway 11 due to its paved section and established habits after the runway 06/24 closure. When weather and traffic conditions permitted it, the CGC preferred to use runway 06 for its first glider launches so that gliders would not need to be hand-towed a long distance before or after a flight. The CGC sometimes used runway 06 later in the day when winds were light, including during periods of light traffic on runway 11/29.
The CGC’s preference for runway 06 even when other traffic was generally using runway 11/29 increased the risk of collision by using a runway that other pilots might not consider to be the ‘active runway’ in accordance with CASA and Caboolture Aero Club (CAC) definitions (as described in Guidance on the use of runways above). Depending on a pilot’s interpretation of the guidance and the circumstances, either runway could be considered the active runway, and operating on both concurrently would increase risk. This is further discussed in Guidance to pilots using intersecting runways.
While CGC procedures did not discuss operations on an intersecting runway, club members took various measures to minimise conflicts. Prior to take-off, tow pilots would check via radio that runway 11/29 was clear, and the CGC would only operate from runway 06 when conditions and traffic volume allowed it.
However, as demonstrated in this occurrence, the amount of traffic on the aerodrome could vary relatively quickly (there was traffic using runway 11 prior to the first glider launch, then almost no traffic on runway 11 until after the second launch). Further, there was no advice to pilots in the En Route Supplement Australia (ERSA) or Caboolture Airfield operations manual about the gliding club’s use of what might (at times) be considered a secondary runway, or in coordinating operations between pilots using different runways.
This risk of intersecting runway operations was exacerbated by the trees obstructing the pilots’ vision of certain sections of the intersecting runways. Aircraft separation was therefore reliant on radio calls being broadcast, heard, and understood by the pilots on intersecting runways. The obstruction caused by the trees was understood by CGC members. However, it was not noted in the club’s procedures. The obstruction caused by the trees was noted in the Caboolture Airfield operations manual, but only for aircraft operating before the threshold of runway 06, when in fact visibility was affected for much of the south-eastern end of the runway.
In this case, the Pawnee pilot reported selecting runway 06 for landing based on wind conditions, rather than as a result of CGC’s earlier decision or common practice.
Other factor that increased risk
The Caboolture Gliding Club had a regular practice of using runway 06 for some flights, including during periods of light traffic on runway 11/29. This increased the risk of collision as Caboolture was a non-controlled aerodrome relying on alerted see‑and‑avoid principles, and there was a stand of trees obstructing pilots' vision of intersecting runways. (Safety issue)
Use of intersecting runways
Based on the traffic being light and a favourable wind forecast, the Pawnee pilot and duty instructor for the gliding club decided to use runway 06 for the first gliding flights of the day.
Given that runway 11 was frequently used by other traffic, this meant that the glider tow aircraft and gliders would likely be using a secondary runway, increasing the risk of conflict. However, this was permissible under the Civil Aviation Safety Regulations (CASR) since Caboolture was a non-controlled aerodrome. The relevant guidance from CASA, the CGC and the CAC is discussed in the Context section of this report (see Runway use, Gliding club information and Guidance on the use of runways, respectively).
Prior to joining the circuit, the Pawnee pilot elected to land on runway 06, although there would have been a reasonable expectation that the 2 aircraft near the threshold would soon be using runway 11. This decision was reportedly based on the position of the 2 windsocks at Caboolture. While there was no way to determine exactly what the Pawnee pilot could see at the time of the decision, the wind would have favoured runways 06 and 11 fairly equally. At the time, there was no other traffic in the circuit or on the ground that the Pawnee pilot considered as a potential threat to a safe landing on 06.
The trees between the 2 runways would have blocked the Pawnee pilot’s view of the runway 11 threshold from any altitude below about 220 ft, as well as the view of the Pawnee by the occupants of the Jabiru, and the ATSB estimated the Pawnee’s height at about 100 ft when the Jabiru commenced the take-off roll.
Without having heard any further take-off calls and no longer able to see the threshold of runway 11 during the latter part of the approach, the Pawnee pilot would not have necessarily been aware that the remaining aircraft were about to take off (discussed in Pawnee pilot’s awareness). Nevertheless, the Pawnee pilot was aware of other aircraft using runway 11 more generally and considered the potential for a conflict. The Pawnee pilot considered runways 06 and 11 to both be active at the time of their approach and attempted landing.
The Pawnee pilot’s intention to stop short might have been a factor in the decision to operate on an intersecting runway, since the pilot did not intend to obstruct runway 11. Nevertheless, the decision to use runway 06 while aware of the potential for other traffic to be using runway 11 increased the risk of conflict.
Contributing factor
Based on the observed wind conditions at the time, and not anticipating any conflicting traffic, the Pawnee pilot elected to land on runway 06 even though all other traffic had been using runway 11.
Aerodrome operator guidance on visibility issues
Trees and buildings at Caboolture Airfield prevented aircraft at a given runway threshold from seeing either threshold of the intersecting runway. While aircraft are allowed to operate on intersecting runways at non-controlled aerodromes, the circumstances at Caboolture resulted in pilots being solely reliant on radio calls being made and correctly heard and interpreted to avoid traffic on intersecting runways.
The aerodrome operator, CAC, published limited information in the Caboolture Airfield operations manual about visibility between runways at Caboolture. This information was only for pilots operating from the displaced threshold of runway 06. The manual did not acknowledge that runway 11 threshold would likely not be visible from airborne aircraft on, or possibly before, the final leg of an approach to runway 06, as well as on the ground up to a point well past the threshold. Likewise, the manual did not mention similar visibility issues due to trees and buildings that pilots would have on any of the other 3 thresholds.
There was also no information in the ERSA to advise pilots of any obstructions to visibility at Caboolture Airfield. The ERSA, not an aerodrome operations manual, is the primary source of information pilots use to familiarise themselves with an aerodrome. While the ERSA entry for Caboolture Airfield included a note for pilots to refer to the aerodrome operations manual, not all pilots will do so, and the relevant information was not present in the operations manual at the time of the accident.
An ATSB review of the ERSA identified 27 aerodromes, 6 of which were uncertified, that had entries relating to visual obstructions between runways. There were 10 such aerodromes, including 1 that was uncertified, that included instructions for pilots to regard radio as calls mandatory (all the certified aerodrome entries stated that this was due to the visibility issues). Another uncertified aerodrome required pilots to confirm runways were clear before take-off or landing.
In this occurrence it is unlikely that mandated radio calls would have prevented a collision, because the Jabiru pilot probably could not transmit and hear radio calls. Additionally, a risk of collision is not eliminated if an aircraft attempting to land hears a rolling call from the intersecting runway; though the landing pilot would now be alerted to another aircraft, going around or rolling through the intersection still risks a collision. Only stopping short of the intersection would guarantee that the 2 aircraft did not collide, and this is not always feasible. If the operations manual and/or the ERSA required pilots to ensure runways are clear before landing, the Pawnee pilot likely would have radioed the 2 aircraft near the runway 11 threshold (including the Jabiru) to confirm they were not taking off. However, there is no certainty that this would have prevented the collision, particularly if the Jabiru had radio issues. A lack of response from the Jabiru could be interpreted to mean that the aircraft was not preparing to depart.
Apart from this accident, since 2016 there have been 3 other reported instances of separation concerns due to intersecting runway operations at Caboolture. The risk of a collision could be mitigated if local and visiting pilots were informed of the visibility hazards, and guidance or procedures were provided for their management.
Other factor that increased risk
The Caboolture Aero Club did not effectively manage or inform pilots of the risk presented by trees and buildings around the airfield that prevented pilots from being able to see aircraft on intersecting runways and approach paths. (Safety issue)
Guidance on intersecting runways at non‑controlled aerodromes
In addition to the regulations and right of way rules applicable at non-controlled aerodromes (including both certified and uncertified aerodromes), CASA provided guidance to pilots at these aerodromes regarding runway selection. This guidance was framed in terms of an ‘active runway’ and a ‘secondary runway’.
The following sections discuss how the concept of an ‘active runway’ is subject to different interpretations by pilots, as well as how the idea of an ‘active’ and ‘secondary’ runway can conflict with CASR regulations. Finally, they discuss the available guidance to pilots regarding runway selection at non-controlled aerodromes, and provide examples of recent occurrences where additional guidance could have provided a substantial improvement to risk controls.
Determination of active runway
CASA provided 4 official publications that described the concept of an ‘active runway’:
part 91 Manual of Standards (MOS)
CASR Part 91 Plain English Guide
advisory circular AC 91-10 - Operations in the vicinity of non-controlled aerodromes
CASA Visual Flight Rules Guide.
Although each definition had different elements and was subject to varying interpretations, they each suggested that a runway is active if it is ‘in use’ and/or one most closely aligned into the prevailing wind. The MOS and associated guide informed pilots to use strobes when their aircraft ‘… crosses any other runway that is in use for take-offs and landings (an active runway)’, implying that more than one runway could be active at a time. The other 2 documents indicated that only one runway could be active. AC 91-10 implied that a runway is always active if it is into wind, even if aircraft are operating on another runway. Further, there was no formal definition or further guidance to describe what makes a runway ‘in use’. There are various possible circumstances that might cause a runway to become ‘in use’, including when an aircraft:
is either on the runway or above it, in the process of landing or taking off
is holding at, or taxiing to a runway with the intention of using it
is on final approach to a runway
has entered the circuit for a runway.
In addition, there was no information about when the ‘in use’ period would end, whether that was a certain time after an aircraft landed/took off, or when the circuit for that runway was empty, or some other criteria.
In the case of this accident, all 3 involved pilots likely considered runway 11 to be an active runway in the sense that it was in general use. However, the Pawnee pilot considered runway 06 to also be active through their own use of it, and also believed that they had right of way as the landing aircraft. By some CASA definitions, this would have made runway 11 the secondary runway from the perspective of the Pawnee pilot.
While this situation had the potential to cause confusion between the pilots, there was insufficient evidence to determine whether it contributed to this accident because it is not clear whether the Jabiru pilot was even aware of the Pawnee, and therefore whether the Jabiru pilot had any reason to consider which runway might be active.
Regardless, there are other potential situations where pilots at non-controlled aerodromes might have conflicting views, particularly when visibility is limited by trees, buildings or terrain or when there are radio communication issues. For example, if an aircraft is in the circuit for a runway, that pilot, having made the appropriate calls, could consider their runway active. Meanwhile, on an intersecting runway, an aircraft has recently taken off and another aircraft is waiting to depart. The waiting pilot has good reason to consider this runway active (an aircraft has just departed and they are about to depart). However, visual obstructions might prevent the 2 pilots from observing one another. If the final approach/take-off calls are not heard, or not made (neither are mandatory), both pilots would be operating on intersecting runways that they believe to be active, with no expectation of crossing traffic.
Implications of an active runway
CASA guidance stated that pilots at non-controlled aerodromes should operate on the active runway, or the runway most closely aligned into wind. However, it also acknowledged that there were situations where a secondary runway could be used. If a secondary runway was in use, CASA guidance stated that pilots on the secondary runway should not create a hazard, and should not impede the flow of traffic on the active runway.
There are 2 issues with this advice: firstly, depending on when a runway is considered ‘active’ (whenever a pilot believes it to be ‘in use’), there could be no way to use a secondary runway without impeding traffic on the active runway. If an aircraft is waiting to depart on the active runway, then an aircraft landing on the secondary runway is impeding the flow of traffic, since the departing aircraft must wait for the landing aircraft to stop, or cross the intersection in accordance with the regulations.
Conversely, if the landing aircraft (using a secondary runway) is not impeding traffic on the intersecting (active) runway because there is no traffic to impede, then that intersecting runway could be considered not active. Based on the ‘in use’ definition for active runways, the landing aircraft is now on an active runway, and the intersecting runway (not currently in use) is secondary.
The second issue with this advice is that telling pilots to not obstruct the active runway on a secondary runway is akin to giving the active runway right of way. In fact, the Caboolture Airfield operations manual states this explicitly. In certain situations, this directly conflicts with existing right of way regulations. For example, a landing aircraft has right of way over an aircraft waiting to take off on an intersecting runway. If all parties agree that the waiting aircraft is on the active runway, then right of way would be with the departing aircraft based on the guidance but with the landing aircraft based on the regulations. Unless an exemption exists, regulations take precedence over guidance material or operations manuals, but the contradiction is unhelpful and avoidable.
Guidance to pilots using intersecting runways
In addition to this accident, there have been numerous near collisions and similar incidents at non-controlled aerodromes involving intersecting runways and visual obstructions. This includes 2 recent examples at Mildura Airport (a certified aerodrome) involving large passenger aircraft operations.
Beyond instructing pilots to not obstruct traffic when using a secondary runway, CASA guidance on intersecting runway operations did not provide pilots with any actionable advice. However, there are various things that pilots operating at non-controlled aerodromes can do to minimise the risk of using an intersecting runway. Some, but not all non-controlled aerodromes with acknowledged visibility issues have provided additional guidance to pilots via the ERSA to help reduce this risk. This includes:
informing pilots of potential visual obstructions between runways
requiring pilots to broadcast their intentions before entering a runway
requiring pilots to confirm other runways are clear (such as via two-way radio communication) prior to landing/taking off.
It is important that pilots using non-controlled aerodromes are equipped with the knowledge and skills necessary to assess and manage the risks associated with the concurrent use of multiple runways. CASA is in a position to provide guidance such as this for all pilots, rather than relying on aerodrome operators to identify and mitigate risk on a case-by-case basis.
Other factor that increased risk
The Civil Aviation Safety Authority guidance for pilots using non-controlled aerodromes did not clearly define the active runway. The guidance did not provide practical advice to pilots using a secondary runway, and in some situations, it was contrary to existing regulations. (Safety issue)
Hold point markings
When runway 06/24 was resurfaced, hold point markings on the taxiways were removed. They had not been restored at the time of the accident. As an uncertified aerodrome, there was no requirement for the runways at Caboolture to have hold point markings in place, and pilots were not required to stop prior to crossing a runway if there was no conflicting traffic. The CAC operations manual did not include any reference to hold point markings.
If hold point markings had been in place at the time of the accident, it is unclear whether they would have affected the Cessna pilot’s decision to taxi across the runway without stopping. The pilot was otherwise aware that they were crossing a runway, but did not stop because they had no expectation that the runway would be in use.
Other factor that increased risk
There were no hold point markings on the taxiway crossing runway 06. Although not required at non-certified aerodromes, hold point markings can help prevent runway incursions.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the midair collision involving Jabiru J430, VH-EDJ, and Piper PA-25-235, VH-SPA, at Caboolture Airfield, Queensland on 28 July 2023.
Contributing factors
The Jabiru pilot likely unknowingly could not transmit or hear radio calls, and was probably not aware of the Pawnee being on final approach to runway 06 when they decided to commence take-off on runway 11.
The Pawnee pilot did not hear an entering and/or rolling call from the Jabiru pilot, and it was not possible to establish from the available evidence whether a call was broadcast. In combination with the line of sight between them being blocked, the Pawnee pilot was therefore not aware that the Jabiru was taking off on the intersecting runway.
The Cessna pilot did not hear the Pawnee pilot make a landing call, and had limited opportunity to be aware of traffic during taxi, due to having turned the radio volume down during pre-flight checks and not restoring it before taxi.
Not having heard the Pawnee pilot's landing call and with most traffic using runway 11, the Cessna pilot had no expectation of an aircraft using runway 06, and taxied across the runway without stopping or looking for traffic while the Pawnee was landing. This resulted in the Pawnee commencing a go-around manoeuvre.
A stand of trees between the intersecting runways prevented the Jabiru and Pawnee pilots from being able to observe one another from the time the Jabiru turned onto runway 11 for take-off until both aircraft had begun climbing.
Based on the observed wind conditions at the time, and not anticipating any conflicting traffic, the Pawnee pilot elected to land on runway 06 even though all other traffic had been using runway 11.
Other factors that increased risk
The Caboolture Gliding Club had a regular practice of using runway 06 for some flights, including during periods of light traffic on runway 11/29. This increased the risk of collision as Caboolture was a non-controlled aerodrome relying on alerted see-and-avoid principles, and there was a stand of trees obstructing pilots' vision of intersecting runways. (Safety issue)
During the circuit call for turning onto the base leg, the Pawnee pilot stated that they would hold short of the runway intersection. While the Pawnee pilot did not intend other pilots to rely on it to avoid conflict, this call could have led to other pilots assuming that the intersecting runway could be safely used when there was no certainty that the Pawnee would be able to hold short.
The Caboolture Aero Club did not effectively manage or inform pilots of the risk presented by trees and buildings around the airfield that prevented pilots from being able to see aircraft on intersecting runways and approach paths. (Safety issue)
The Civil Aviation Safety Authority guidance for pilots using non-controlled aerodromes did not clearly define the active runway. The guidance did not provide practical advice to pilots using a secondary runway, and in some situations, it was contrary to existing regulations. (Safety issue)
There were no hold point markings on the taxiway crossing runway 06. Although not required at non-certified aerodromes, hold point markings can help prevent runway incursions.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Caboolture Gliding Club had a regular practice of using runway 06 for some flights, including during periods of light traffic on runway 11/29. This increased the risk of collision as Caboolture was a non-controlled aerodrome relying on alerted see-and-avoid principles, and there was a stand of trees obstructing pilots' vision of intersecting runways.
Safety issue description: The Caboolture Aero Club did not effectively manage or inform pilots of the risk presented by trees and buildings around the airfield that prevented pilots from being able to see aircraft on intersecting runways and approach paths.
Guidance on intersecting runways at non‑controlled aerodromes
Safety issue description: The Civil Aviation Safety Authority guidance for pilots using non-controlled aerodromes did not clearly define the active runway. The guidance did not provide practical advice to pilots using a secondary runway, and in some situations, it was contrary to existing regulations.
Safety action not associated with an identified safety issue
Additional safety action taken by the Caboolture Aero Club
The CAC advised that hold point markings have been restored on the taxiway across runway 06/24.
Glossary
AC
Advisory circular
ADS-B
Automatic dependent surveillance broadcast
ALA
Aircraft landing area
CAC
Caboolture Aero Club
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CGC
Caboolture Gliding Club
CTAF
Common traffic advisory frequency
ERSA
En route supplement Australia
GPS
Global positioning system
LAHSO
Land and hold short operations
MOS
Manual of standards
Sources and submissions
Sources of information
The sources of information during the investigation included:
the Pawnee and Cessna pilots
Airwork Aviation
Caboolture Aero Club
Caboolture Gliding Club
Civil Aviation Safety Authority
Queensland Police Service
CTAF recordings from Caloundra Airport
Airservices Australia
Jabiru flight data recorder
accident witnesses
16 other pilots familiar with Caboolture Airfield
video footage of the accident flight and other photographs and videos taken on the day of the accident.
References
Andrews, J. W. (1977). Air-to-air visual acquisition performance with pilot warning instruments (PWI). Massachusetts Institute of Technology, Lincoln Laboratory, FAA Report no. FAA-RD-77-30.
Federal Aviation Administration. (2016). Pilots' Role in Collision Avoidance. Advisory Circular 90-48D.
Foster, J. L., & Garry, M. (2012). Building false memories without suggestions. The American journal of psychology, 125(2), 225-232.
Hobbs, A. (1991). Limitations of the see-and-avoid principle. Canberra: Australian Transport Safety Bureau.
Rosenholtz, R. (2016). Capabilities and Limitations of Peripheral Vision. The Annual Review of Vision Science, 2, 435-457.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Pawnee and Cessna pilots
Civil Aviation Safety Authority
Caboolture Aero Club
Caboolture Gliding Club
Airwork Aviation.
Submissions were received from the:
Pawnee and Cessna pilots
Civil Aviation Safety Authority
Caboolture Aero Club
Caboolture Gliding Club.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway numbers represent the magnetic heading closest to the runway orientation (e.g. runway 11 is oriented 114° magnetic).
[2]See Video recording for a description of the preceding flights.
[3]Aerotow: the process of a powered aircraft towing a glider into the air.
[5]See Mandatory and recommended radio calls and Radio communications at Caboolture Airfield.
[6]Further details of the Jabiru’s taxi sequence are in On-board recording.
[7]A go-around, also known as a missed approach, is an aborted landing of an aircraft that is on final approach or has already touched down.
[8]The tow rope was about 55 m long and can hang 40 ft or more below the tow aircraft.
[9]Level 3 is the highest instructor rating within Gliding Australia, and certifies instructors to train other instructors as well as glider pilots.
[10]Automatic Dependent Surveillance Broadcast (ADS-B): a means by which aircraft, aerodrome vehicles and other objects can automatically transmit or receive data such as identification, position and additional data, as appropriate, in a broadcast mode via data link.
[11]The only regulation applicable to uncertified aerodromes was regarding radio communication facilities, and the requirement for the aerodrome to carry an Aerodrome Frequency Confirmation System, depending on the frequency of scheduled air transport flights.
[12]For a runway that does not have a marked runway hold position, the aircraft giving way and any tow vehicle must not encroach upon a graded runway strip.
[13]CASR 91.400 had a provision to mandate carriage of a radio at certain designated aerodromes; as of 2025, there were no aerodromes listed as such.
[14]Some non-controlled aerodromes (not Caboolture) were in ‘mandatory broadcast areas’ where radio calls were mandatory.
[15]The Aeronautical Information Publication (AIP), published by Airservices Australia, contained aeronautical maps, charts and other aeronautical information and instructions.
[16]At the time of writing, version 4.2 (2025) was current.
[17]At the time of writing, version 8.1 (2024) was current.
[18]Casino (NSW), Great Lakes Airfield (Vic), Kyneton (Vic), Maryborough (Vic), Murray Bridge (SA), and Waikerie (SA).
[19]Information about visual obstructions between runways was also included for 2 aerodromes that had control towers but were usually only controlled during the day: Broome and Camden. They were excluded from this review.
[20]The transponder used a separate antenna system to the radio. The transponder was not examined for functionality.
[21]Over the 15-second period, Jabiru would have moved from about 45° to 55° to the left of the Pawnee’s nose. The Pawnee would have moved from about 75° to 90° to the right of the Jabiru’s nose.
[22]There were 2 additional collisions between 2 balloons, which are excluded from this data.
[23]This data includes a collision between 2 helicopters using adjacent helipads near Main Beach, Gold Coast, Queensland, on 2 January 2023 (AO-2023-001).
[24]In accordance with the ATSB’s definition, a near collision occurs when an aircraft that is airborne, taking off or landing comes into such close proximity with another aircraft, terrain, person or object where immediate evasive action was required or should have been taken.
[25]Occurrences coded as ‘separation issues’ are those in non-controlled airspace where separation is a concern, but where the definition of near collision is not met.
Preliminary report
Report release date: 08/09/2023
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On the morning of 28 July 2023, the pilot of a Piper PA-25, registered VH-SPA and operated by Caboolture Gliding Club, took off from runway 06[1] at Caboolture Airfield, Queensland, with a glider in tow. It was a clear day with light winds. This was the pilot’s second flight of the day, having previously completed one prior glider aerotow in VH-SPA. After the glider was released, the pilot of VH-SPA entered the circuit for runway 06, with the intention of landing so that the aircraft could be used to tow a third glider into the air.
Caboolture Airfield was located within class G (non-controlled) airspace, and had a designated common traffic advisory frequency (CTAF) on which pilots made positional broadcasts when operating within the vicinity of the airport. To date no recordings of radio transmissions from any aircraft on the ground at Caboolture around the time of the accident have been identified (see Recorded data). Witness recollections of radio transmissions are being collated and analysed by the ATSB.
Some transmissions from aircraft in flight were recorded. While in the circuit, the pilot of VH-SPA made several radio calls on the CTAF, the last of which was at about 1030:19 and was partially recorded. According to several witnesses who heard the transmission, the pilot announced that VH-SPA was commencing a final approach to runway 06 and stated that the aircraft would be ‘holding short’, indicating that it would not be crossing the intersection with runway 11/29.
At about 1030:44, while VH-SPA was on final approach, the pilot of a Jabiru J430, registered VH‑EDJ, began take-off on runway 11. The pilot and passenger were conducting a private flight to Dirranbandi Airport, Queensland.
Also at that time, a Cessna 172, registered VH-EVR, was being taxied at the airfield by a solo student pilot. The pilot of VH‑EVR later reported having turned the radio volume down to conduct engine run-ups near the intersection of the two runways and had not restored normal volume upon completion. As a result, the pilot of VH-EVR did not hear any transmissions from the pilot of VH‑SPA, and was not aware of the aircraft approaching runway 06.
At 1030:49, just prior to VH-SPA touching down on runway 06, VH-EVR crossed runway 06 ahead of VH-SPA in a north-west direction. The pilot of VH-SPA initiated a go-around, and made an associated radio call (according to several witnesses) which was not recorded.
At 1030:55, VH-SPA began climbing while maintaining a runway 06 heading as VH-EDJ lifted off runway 11 before the runway intersection. About 5–10 seconds later, while the aircraft were climbing on crossing tracks, the pilot of VH-EDJ commenced a left turn, likely in an attempt to avoid a collision.
At 1031:11, the two aircraft collided on similar tracks above runway 06, just north-east of the 06/11 intersection, at a height of about 200–300 feet (Figure 1).
Figure 1: Approximate tracks of VH-EDJ and VH-SPA based on video footage
Source: Google Earth, annotated by the ATSB
The leading edge of the inboard left wing of VH-SPA struck VH-EDJ’s right wing at the outboard trailing edge, resulting in separation of the right wing tip and part of the right aileron. VH-EDJ rolled to the right while rapidly losing altitude. VH-EDJ collided with terrain in a nose-down, right‑wing-down attitude near the end of runway 06. The pilot and passenger were fatally injured.
VH-SPA sustained damage to its left wing in the collision but remained flyable and the pilot was uninjured. The pilot circled the airfield to direct people towards the accident site. The aircraft landed on runway 11 without further incident.
Context
Pilot information
Both pilots involved in the collision were experienced fixed-wing pilots. They were both qualified for their respective roles, and both held valid class 2 aviation medical certificates.
The pilot of VH-EDJ held an Air Transport Pilot Licence (aeroplane) and was a grade 2 flight instructor with various instrument ratings.
The pilot of VH-SPA held a Private Pilot Licence (aeroplane) and held endorsements for glider operations and glider towing operations. The pilot was also an accredited flight instructor/examiner for both gliders and tow aircraft.
The pilot of VH-EVR was a student pilot conducting flying training at Caboolture. The pilot had completed 2 solo navigation flights and was preparing to conduct a third flight at the time of the occurrence.
Aircraft information
VH-EDJ
The Jabiru J430 is an amateur-built high-wing light aircraft. It has a single Jabiru 3300 reciprocating engine and a ground-adjustable fiberglass propeller. VH-EDJ was constructed primarily by the pilot in Australia in 2019, and first registered on 19 February 2019, with 283.7 hours total time in service.
VH-SPA
The Piper PA-25-235 Pawnee B is a low-wing single-engine aircraft. It is powered by a Textron Lycoming O-540 reciprocating engine, with a fixed-pitch aluminium propeller. VH-SPA was manufactured in 1969, and first registered in Australia on 23 August, 1974. It had 10,181 hours total time in service and had been operating as a tow aircraft at Caboolture airfield since January 1997.
Wreckage and impact information
The ATSB conducted an on-site examination of the aircraft wreckage. The right wing of VH-EDJ collided with the ground forward of the threshold marking for runway 24. The nose then struck the ground, and the aircraft tumbled to a stop 45 metres from the initial impact point (Figure 2).
Figure 2: Wreckage and impact point of VH-EDJ
Source: ATSB
VH-EDJ came to rest right-side down, and was later disturbed by first responders attempting to reach the pilot and passenger. First responders reported both the pilot and passenger were wearing seatbelts. The right wing tip and a section of the right aileron was recovered near the intersection of runway 11/06, near the point at which the two aircraft collided.
VH-SPA sustained impact damage to the leading edge of its left wing as a result of the collision (Figure 3).
Figure 3: Damage to VH-SPA following the collision with VH-EDJ
Source: ATSB
Airfield information and procedures
Caboolture Airfield was an aircraft landing area,[2] located about 3.5 km east of Caboolture, Queensland. It had an elevation of 40 ft above mean sea level, and two intersecting runways with magnetic orientations of 114°/294° (runway 11/29), and 065°/245° (runway 06/24). Their lengths were 1,129 m and 820 m respectively. Both runways were unsealed grass, except for a sealed portion at the beginning of runway 11. Trees about 10–14 m high between the intersecting runways obscured parts of adjacent runways (Figure 4).
Figure 4: Obscured parts of the adjacent runway from the thresholds of runways 11 (orange) and 06 (yellow)
Source: Google Earth, annotated by the ATSB
The carriage and use of a radio was required by the aerodrome operator for all aircraft operating at Caboolture Airfield. As a non-controlled aerodrome, separation was maintained by ‘alerted see‑and-avoid’ principles guided by Civil Aviation Safety Authority (CASA) advisory circulars AC 91-10 Operations in the vicinity of non-controlled aerodromesand AC 91-14 Pilots’ responsibility for collision avoidance. These stated that pilots should broadcast position and intention so that nearby traffic would have an awareness of the aircraft and be able to plan accordingly.
Recorded data
VH-SPA carried no flight data recording devices, and no automatic dependent surveillance broadcast (ADS-B) transponder. An ADS-B transmitter was fitted to VH-EDJ but no data on the accident flight was available. Two data recording devices were recovered from VH-EDJ for later examination.
Video footage of the accident was recovered from a closed-circuit television system installed at Caboolture Airfield.
Common traffic advisory frequency (CTAF) broadcasts were not recorded at the airfield. Caloundra Airport, 32 km north-north-east of Caboolture, operated on the same CTAF frequency and recorded all transmissions received there. Due to distance and line-of-sight limitations, radio calls on or near the ground at Caboolture were generally not received, but some calls from within the Caboolture Airfield circuit were received and recorded. Recordings of radio calls made by the pilot of VH-SPA indicated that the aircraft’s radio was functional for transmitting and receiving.
Further investigation
To date, the ATSB has:
examined both aircraft and the accident site
recovered aircraft components, including the radio from VH-EDJ (which was damaged in the accident), and other items for further examination
interviewed relevant parties, including eyewitnesses and witnesses with access to common traffic advisory frequency (CTAF) transmissions
collected aircraft, pilot, aerodrome and operator documentation
analysed video recordings and CTAF transmissions.
The investigation is continuing and will include:
examination of aircraft components and other items recovered from the accident site
further review of aircraft, pilot, aerodrome and operator documentation
further analysis of video recordings and CTAF transmissions
analysis of aircraft flight paths, with particular attention given to potential visibility restrictions
a review of similar occurrences
analysis of procedures at non-controlled aerodromes with intersecting runways
interviews with other pilots familiar with Caboolture Airfield.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Runway numbers represent the magnetic heading closest to the runway orientation (e.g. runway 11 is oriented 114º magnetic).
[2] An aircraft landing area is an aerodrome that has not been certified by CASA. These aerodromes are non-controlled, unregulated facilities. It is the responsibility of pilots and operators to determine whether these aerodromes are suitable for use.
The ATSB occurrence data reported by industry identified a trend towards a heightened exposure to risk in the commercial ballooning sector, compared with other forms of non‑scheduled passenger carrying commercial aviation. This study incorporates a detailed analysis of the data and aims to identify key areas of focus for safety improvements, with an intent to reduce passenger injuries.
What the ATSB found
The ATSB found that over the period 2014–2022, commercial ballooning carried a higher risk to fare paying passengers compared with similar operations in small aeroplanes and helicopters. Specifically, a commercial ballooning flight was more likely to have a:
reported occurrence – especially a serious incident or accident
passenger sustain an injury.
The ATSB also found that minor injuries, serious injuries, serious incidents and accidents were all more likely to occur during landing than any other phase of flight, and wind was the most common factor reported to have contributed to these occurrences.
Also identified, was that between 2014 and 2022 there was a significant increase in balloons with an envelope size above 400,000 cubic ft on the Civil Aviation Safety Authority’s aircraft register. This reflected an increase in the number of balloons capable of carrying the maximum passenger limit of 24 per flight, thereby increasing overall exposure to risk.
Safety message
Balloons are distinct from other aircraft, in that they travel by moving with the wind. Directional control is achieved using differing wind directions at different altitudes. As such, balloon pilots should use all available information sources, including approved Bureau of Meteorology products, to ensure they understand the weather, particularly the wind, and its influence on flight safety. Accurate weather assessment is critical for safe go/no-go decisions. Pilots should also apply threat and error management by anticipating risks such as powerlines and poor visibility, and prioritising safety over logistical pressures in adverse conditions.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing passenger injuries in commercial ballooning operations.
Reducing accident rates and passenger injuries in balloon operations requires effective safety practices. Although not required by legislation for balloon operators, implementing a Safety Management System (SMS) provides a structured approach to identifying and managing risks.
Recommended risk controls to reduce passenger injury risks include:
thorough passenger safety briefings and visual safety cards
ensuring correct brace/landing positions
clear emergency instructions
seating or positioning to minimise passenger contact injuries.
Introduction
Background
The ATSB occurrence statistics report for the 10-year period 2010–2019 (AR-2020-047) identified 19 accidents involving commercial balloon operations. These accidents resulted in 1 fatality and 19 serious injuries. Over the same period there were 70 minor injuries involving commercial balloon operations reported to the ATSB.
The report also found the following rates of accidents per million hours flown for the 5‑year period 2014–2019:[1]
291.2 for commercial ballooning operations
26.3 for non-scheduled commercial aeroplane operations
20.9 for non-scheduled commercial helicopter operations.
In addition to attempting to reduce the accident rate, one of the ATSB’s SafetyWatch priorities is to reduce passenger injuries in commercial ballooning operations.
This study benchmarks ballooning operations against other similar operations in Australia, to identify any systemic areas of concern. The results of this work will form the basis of the ballooning safety watch initiative, and identify what further investigation, research and education work may be required for this sector of aviation operations.
Any systemic safety concerns identified will be shared with industry to promote a generative safety culture, encourage further reporting of occurrences, and drive future safety action.
Safety study goals
This safety study expands the understanding of the risks of Australian commercial ballooning, namely balloon transport operations, to the fare paying passenger compared with other similar operations in an aeroplane or helicopter.
The goals of this study were to:
define what a similar operation for a fare paying passenger was in an aeroplane or helicopter to provide a valid basis for comparison
provide a rate analysis of balloon occurrences against similar operations in an aeroplane or helicopter
provide a statistical description of balloon occurrences, including the severity of injuries and safety factors involved
identify commonalities between all balloon occurrences
compare balloon occurrences by location and envelope size
identify and analyse the risks for a fare paying passenger for a flight in a commercially-operated balloon.
Balloon transport operations
Part 131 of the Civil Aviation Safety Regulations (CASR) sets out specific requirements for operating balloons and hot air airships, known in industry as ‘Part 131 aircraft’.
The CASR dictionary defines a balloon as an unpowered, lighter-than-air aircraft. A free balloon is defined as a balloon that is intended for flight without being permanently tethered.
A manned free balloon is defined as one equipped:
to carry one or more people
with controls that enable the altitude of the balloon to be controlled.
For the purposes of the safety study, the term balloon will refer to a ‘manned free balloon’.
The focus of this study was balloon transport operations, defined in CASR 131.010 as:
a passenger transport operation conducted using a Part 131 aircraft that is a registered aircraft or a foreign registered aircraft; and
conducted for hire or reward; and
undertaken wholly within Australia; and
not undertaken as part of a flight into or out of Australian territory.
This does not include training, specialised or recreational operations as defined by the CASR.
Commercial ballooning is a flying operation that takes part in a manned free balloon carrying fare paying passengers for the purpose of a joy flight or sightseeing. As such, valid comparable operations were passenger transport operations classified as a joyflights/sightseeing flight in a Part 135 small aeroplane or a Part 133 rotorcraft subset (helicopter).
Methods and sources
Overview
To allow comparison between the different aircraft types and operations, this study used reported occurrence records of aviation incidents, serious incidents, and accidents from the ATSB national aviation occurrence database. Aircraft activity data was collected from the Bureau of Infrastructure, Transport and Research Economics (BITRE) Australian aircraft activity survey, which is conducted annually and made publicly available online.
Data analysis
The collected data sets for balloons, aeroplanes and helicopters were used to conduct:
a rate analysis of reported occurrences of commercial ballooning against aeroplane and helicopter operations
an injury rate comparison.
The following analysis of balloon data from the ATSB national occurrence database was conducted:
occurrences by phase of flight
serious incidents and accidents by phase of flight
serious injuries by phase of flight
safety factors identified for serious incidents and accidents
occurrences by location.
A comparison was also conducted of the Bureau of Meteorology weather package services by location to occurrence locations, together with analysis of balloon envelope size changes over the years 2014–2022 inclusive.
ATSB national aviation occurrence database
Occurrence data is reported to the ATSB from industry through the mandatory occurrence reporting requirements of the Transport Safety Investigation Act 2003 and stored in the national aviation occurrence database. This stored data contains information including:
aircraft type
registration
location
time of occurrence
number of injuries
injury level
occurrence class (incident, serious incident, accident)
occurrence summary.
A publicly-available search engine allows users to search the database using multiple parameters including: time period, location, type of occurrence and type of aircraft.
In classifying occurrences, the ATSB used the following definitions:
Accident: an occurrence involving an aircraft where:
a person dies or suffers serious injury
the aircraft is destroyed, or is seriously damaged
any property is destroyed or seriously damaged.
Serious incident: an incident involving circumstances indicating that an accident nearly occurred (ICAO Annex 13).
Incident:an occurrence, other than an accident, associated with the operation of an aircraft which affects or could affect the safety of operation (ICAO Annex 13).
BITRE Australian aircraft activity survey
Survey data
The annual BITRE Australian aircraft activity survey and associated statistical report covers all Australian (VH-) registered aircraft used in the commercial air transport and general aviation sectors of the Australian aviation industry.
The survey is completed annually by operators, and the following data is collected:
aircraft registration
postcode of aircraft base (balloon operators indicate the postcode of the general area from which most flying was conducted)
type of activity by hours flown
type of activity by landings conducted.
The data collection allows aircraft operators to nominate the type of activity that a particular aircraft conducted over that calendar year. The survey results are merged with details from the civil aircraft register. The register gives access to additional relevant information including aircraft type, engine and fuel type, country, and year of manufacture.
Activity classification
In 2013, recommendations from the Tenth Session of the Statistics Division of the International Civil Aviation Organization (ICAO) were adopted by the ICAO Council and a new edition of the Reference Manual on the ICAO Statistics Program was published. Included within the manual was a new ICAO Classification of Civil Aviation Activities.
In 2014, BITRE adopted ICAO’s new classification and began collecting statistics in their survey to reflect this change.
In 2019, the ATSB adopted the new activity classification to align with BITRE and ICAO. The ATSB conducted a multi-year project to reclassify over 320,000 occurrences and events within the ATSB occurrence database to include the new activity classification. This reduced most of the uncertainty associated with combining/comparing the databases. These changes meant the ATSB could present more accurate, higher resolution rate data (the best measure for comparison between activities) for more activities.
In response to this change, and to enable an accurate classification comparison between balloon, aeroplane and helicopter operations, this safety study used rate and occurrence data for the years 2014–2022 inclusive.
Landings versus flight hours
BITRE provided rate data in 2 forms: flight hours per operational category and number of landings per operational category. The ATSB elected to use the number of landings (as a proxy for number of flights) rather than flight hours when comparing aircraft types.
Unlike aeroplanes and helicopters, which can record several take-offs and landings within a single hour of flight, balloon flights almost always involve only one take-off and one landing. Therefore, using flight hours would not give an accurate comparison across aircraft types. The number of landings offered a more valid and consistent measure of risk exposure between them.
BITRE flying activities
BITRE defined commercial air transport as an ‘aircraft operation involving the transport of passengers, cargo or mail for remuneration or hire’; and general aviation as an ‘aircraft operation other than a commercial air transport operation’.
The Australian aircraft activity survey had the following relevant flying activities:
general aviation
sport and pleasure flying
joyflights/sightseeing charters. Flying involving the carriage of passengers for joyflight or sightseeing purposes that take off and land at the same location
commercial aviation
non-scheduled
passenger transport charters. Flying involving the carriage of passengers by the aircraft operator or his/her employees for hire or reward (but excluding scheduled airline operations).
A review of initial data collected from BITRE identified that commercial balloon flights had been recorded as either a joyflights/sightseeing charters activity or a passenger transport charters activity. Therefore, for the purpose of this analysis, data from both aircraft activity types was used to capture all commercial balloon transport operations (‘commercial ballooning’).
Similarly, it was possible that aeroplanes and helicopter operators also recorded joyflights/sightseeing charters as passenger transport charters and not joyflights/sightseeing charters.
As such, this study analysed the data with the passenger transport charters aircraft activity type included and then excluded for aeroplanes and helicopters for the comparison with commercial ballooning.
Collected data
Australian aircraft activity survey data 2014–2022
The following data was collected from BITREAustralian aviation activity surveys for the years 2014–2022 inclusive:
balloon landings logged as joyflights/sightseeing and passenger transport charters
aeroplane and helicopter landings logged as joyflights/sightseeing and passenger transport charters
aeroplane and helicopter landings logged as joyflights/sightseeing charters only.
Results of the aircraft activity surveys conducted between 2014 and 2022 showed that there were:
68,433 commercial ballooning landings (Figure 1)
2,190,607 aeroplane joyflights/sightseeing and passenger transport landings (Figure 2)
1,795,332 helicopter joyflights/sightseeing and passenger transport landings combined (Figure 2)
Figure 4: Commercial ballooning reported occurrences per year (2014–2022)
Source: ATSB
Figure 5: Aeroplane and helicopter joyflights/sightseeing and passenger transport reported occurrences per year (2014–2022)
Source: ATSB
Figure 6: Aeroplane and helicopter joyflights/sightseeing reported occurrences by year (2014–2022)
Source: ATSB
Reported occurrence rate comparison
The ATSB used reported occurrence data and activity survey data (2014–2022) to obtain an occurrence rate comparison between commercial ballooning and combined aeroplane and helicopter operations.
The 4 rate analyses were:
occurrence rate (comparison 1)
serious incident and accident rates (comparison 2)
injury rate (comparison 3)
serious injury rate (comparison 4)
Two comparisons were conducted for each rate analysis:
commercial ballooning versus aeroplane and helicopter joyflights/sightseeing and passenger transport activities (comparison X.1)
commercial ballooning versus aeroplane and helicopter joyflights/sightseeing (only) (comparison X.2).
Occurrence rate comparison
Comparison 1.1 – reported occurrence rate comparison between commercial ballooning and joyflights/sightseeing and passenger transport in an aeroplane and helicopter
Commercial ballooning reported occurrence rate
68,433 landings
79 reported occurrences
115.4 reported occurrences per 100,000 landings.
For the period 2014–2022, the commercial ballooning reported occurrence rate was 115.4 occurrences per 100,000 landings.
Aeroplane joyflights/sightseeing and passenger transport reported occurrence rate
2,190,607 landings
1,658 occurrences
75.7 per 100,000 landings.
For the period 2014–2022, the aeroplane joyflights/sightseeing and passenger transport reported occurrence rate was 75.7 occurrences per 100,000 landings.
Helicopter joyflights/sightseeing and passenger transport reported occurrence rate
1,795,332 landings
618 occurrences
34.4 per 100,000 landings.
For the period 2014–2022, the helicopter joyflights/sightseeing and passenger transport reported occurrence rate was 34.4 occurrences per 100,000 landings.
ATSB finding
A commercial balloon flight was 1.5 times more likely to have a reported occurrence than a comparable joyflights/sightseeing and passenger transport activity in an aeroplane and 3.4 times more likely than a helicopter.
Comparison 1.2 – reported occurrence rate comparison between commercial ballooning and a joyflights/sightseeing activity in an aeroplane and helicopter aircraft
Commercial ballooning reported occurrence rate
For the period 2014–2022, the commercial ballooning reported occurrence rate was 115.4 occurrences per 100,000 landings.
For the period 2014–2022, the helicopter joyflights/sightseeing reported occurrence rate was 12.5 occurrences per 100,000 landings.
ATSB finding
A commercial balloon flight was 4.2 times more likely to have a reported occurrence than a comparable joyflights/sightseeing activity in an aeroplane and 9.2 times more likely than a helicopter.
Serious incident and accident rates
Analysis of serious incident and accident data 2014–2022, found:
Figure 7: Commercial ballooning serious incident and accidents per year (2014–2022)
Source: ATSB
Figure 8: Aeroplane joyflights/sightseeing and passenger transport serious incidents and accidents per year (2014–2022)
Source: ATSB
Figure 9: Helicopter joyflights/sightseeing and passenger transport serious incidents and accidents per year (2014–2022)
Source: ATSB
Figure 10: Aeroplane joyflights/sightseeing serious incidents and accidents per year (2014–2022)
Source: ATSB
Figure 11: Helicopter joyflights/sightseeing serious incidents and accidents per year (2014–2022)
Source: ATSB
Serious incident and accident rate comparison
Comparison 2.1 – comparison between commercial ballooning and a joyflights/sightseeing and passenger transport activity in an aeroplane and helicopter
Commercial ballooning serious incident and accident rate
68,433 commercial balloon landings
23 serious incidents + 15 accidents = 38 total
55.5 serious incidents and accidents per 100,000 landings.
Commercial ballooning had 55.5 serious incidents or accidents per 100,000 landings.
Aeroplane joyflights/sightseeing and passenger transport serious incident or accident rate
2,190,607 landings
86 serious incidents and 50 accidents = 136 total
6.2 serious incidents and accidents per 100,000 landings.
Aeroplane joyflights/sightseeing and passenger transport had a serious incident or accident rate of 6.2 per 100,000 landings.
Helicopter joyflights/sightseeing and passenger transport serious incident or accident rate
1,795,332 landings
23 serious incidents and 16 accidents = 39 total
2.2 serious incidents and accidents per 100,000 landings.
Helicopter joyflights/sightseeing and passenger transport had a serious incident or accident rate of 2.2 per 100,000 landings.
ATSB finding
A serious incident or accident was 8.9 times more likely to occur on a commercial balloon flight than a joyflights/sightseeing or passenger transport activity in an aeroplane and 25.6 times more likely than in a helicopter.
Comparison 2.2 – comparison between commercial ballooning and a joyflights/sightseeing activity in an aeroplane and helicopter
Commercial ballooning serious incident or accident rate
Commercial ballooning had 55.5 serious incidents or accidents per 100,000 landings.
Aeroplane joyflights/sightseeing serious incident or accident rate
260,506 landings
15 serious incidents and 12 accidents = 27 total
10.4 serious incidents and accidents per 100,000 landings.
Aeroplane joyflights/sightseeing had a serious incident or accident rate of 10.4 per 100,000 landings.
Helicopter joyflights/sightseeing serious incident or accident rate
496,867 landings
9 serious incidents and 4 accidents = 13 total
2.6 serious incidents and accidents per 100,000 landings.
Helicopter joyflights/sightseeing had a serious incident or accident rate of 2.6 per 100,000 landings.
ATSB finding
A serious incident or accident was 5.4 times more likely to occur on a commercial balloon flight than a joyflights/sightseeing activity in an aeroplane and 21.2 times more likely than a helicopter.
Reported injuries
Analysis of injury data in the reported occurrences 2014–2022, found:
no fatalities involving commercial balloon flights
24 fatalities involving aeroplane joyflights/sightseeing and passenger transport activities
8 fatalities involving helicopter joyflights/sightseeing and passenger transport activities
7 (of the 32) fatalities occurred in aeroplane and helicopter joyflights/sightseeing activities.
36 minor injuries and 10 serious injuries involving aeroplanes conducting joyflights/sightseeing and passenger transport activities combined (Figure 13)
17 minor injuries and 9 serious injuries involving helicopters conducting joyflights/sightseeing and passenger transport activities (Figure 14)
12 minor injuries and 2 serious injuries involving aeroplanes conducting joyflights/sightseeing activities (Figure 15)
3 minor injuries and 5 serious injuries involving helicopters conducting joyflights/sightseeing activities (Figure 16).
Figure 12: Reported commercial ballooning injuriesper year (2014–2022)
Source: ATSB
Figure 13: Reported aeroplane joyflights/sightseeing and passenger transport injuries per year (2014–2022)
Source: ATSB
Figure 14: Reported helicopter joyflights/sightseeing and passenger transport injuries per year (2014–2022)
Source: ATSB
Figure 15: Reported aeroplane joyflights/sightseeing injuries per year (2014–2022)
Source: ATSB
Figure 16: Reported helicopter joyflights/sightseeing injuries per year (2014–2022)
Source: ATSB
Injury rate comparison
Comparison 3.1 – comparison between commercial ballooning and joyflights/sightseeing and passenger transport activity in an aeroplane and helicopter
Commercial ballooning total injury rate
68,433 landings
76 total injuries (no fatalities)
111.1 injuries per 100,000 landings.
Commercial ballooning had an injury rate of 111.1 injuries per 100,000 landings.
Aeroplane joyflights/sightseeing and passenger transport total injury rate
2,190,607 landings
70 total injuries including fatalities
3.2 injuries per 100,000 landings.
Aeroplane joyflights/sightseeing and passenger transport had an injury rate of 3.2 injuries per 100,000 landings.
Helicopter joyflights/sightseeing and passenger transport total injury rate
1,795,332 landings
34 total injuries including fatalities
1.9 per 100,000 landings.
Helicopter joyflights/sightseeing and passenger transport had an injury rate of 1.9 injuries per 100,000 landings.
ATSB finding
A person was 34.7 times more likely to sustain an injury on a commercial balloon flight than in an aeroplane on a joyflights/sightseeing and passenger transport charter activity and 58.5 times more likely than in a helicopter.
Comparison 3.2 – comparison between commercial ballooning and a joyflights/sightseeing activity in an aeroplane and helicopter
Commercial ballooning total injury rate
For the period 2014–2022, the commercial ballooning injury rate was 111.1 injuries per 100,000 landings.
Aeroplane joyflights/sightseeing total injury rate
260,506 landings
21 total injuries including fatalities
8.1 per 100,000 landings.
Aeroplane joyflights/sightseeing had an injury rate of 8.1 injuries per 100,000 landings.
Helicopter joyflights/sightseeing total injury rate
496,867 landings
8 total injuries (no fatalities recorded)
1.6 per 100,000 landings.
Helicopter joyflights/sightseeing had an injury rate of 1.6 injuries per 100,000 landings.
ATSB finding
A person was 13.7 times more likely to sustain an injury on a commercial balloon flight than a joyflights/sightseeing activity in an aeroplane and 69.4 times more likely than in a helicopter.
Serious injury rate comparison
Comparison 4.1 – comparison between commercial ballooning and a joyflights/sightseeing and passenger transport activity in an aeroplane and helicopter
Commercial ballooning serious injury rate
68,433 balloon landings
18 serious injuries
26.3 serious injuries per 100,000 landings.
Commercial ballooning had a serious injury rate of 26.3 injuries per 100,000 landings.
Aeroplane joyflights/sightseeing and passenger transport serious injury rate
2,190,607 landings
10 serious injuries
0.5 serious injuries per 100,000 landings.
Aeroplane joyflights/sightseeing and passenger transport had a serious injury rate of 0.5 injuries per 100,000 landings.
Helicopter joyflights/sightseeing and passenger transport serious injury rate
1,795,332 landings
9 serious injuries
0.5 serious injuries per 100,000 landings.
Helicopter joyflights/sightseeing and passenger transport had a serious injury rate of 0.5 injuries per 100,000 landings.
ATSB finding
A person was 57.2 times more likely to sustain a serious injury on a commercial balloon flight than a joyflights/sightseeing and passenger transport charter activity in an aeroplane and 52.6 times more likely than in a helicopter.
Comparison 4.2 – comparison between commercial ballooning and a joyflights/sightseeing activity in aeroplane and helicopter
Commercial ballooning serious injury rate
For the period 2014–2022, the commercial ballooning serious injury rate was 26.3 serious injuries per 100,000 landings.
Helicopter joyflights/sightseeing had a serious injury rate of 1.0 injuries per 100,000 landings.
ATSB finding
A person was 34.2 times more likely to sustain a serious injury on a commercial balloon flight than a joyflights/sightseeing activity in an aeroplane and 26.0 times more likely than in a helicopter.
Occurrence categories
Commercial ballooning occurrence categories
Figure 17 shows the occurrence rate per most common commercial ballooning occurrence categories for the period 2014–2022.[2] Collision with terrain was the most common with 38.0 occurrences per 100,000 flights, followed by hard landings (16.1), cabin injuries (13.2) and wirestrikes (13.2).
Figure 17: Commercial ballooning occurrence rate per most common occurrence categories (2014–2022)
Source: BITRE and ATSB
Aeroplane and helicopter occurrence categories
The most common aeroplane and helicopter occurrence categories for joyflights/sightseeing and passenger transport combined are displayed in Figure 18 and Figure 19 respectively. Aeroplane occurrences involving a birdstrike had a rate of 16.3 occurrences per 100,000 flights, this was followed by diversion/returns (16.0), and a landing gear/indication (12.6). An engine failure or malfunction had an occurrence rate of 6.3 per 100,000 flights. Helicopters’ most common occurrence category was diversion/returns at 9.0 per 100,000 flights, followed by warning devices (5.8) and birdstrikes (5.2).
Figure 18: Aeroplane joyflights/sightseeing and passenger transport occurrence rate per most common occurrence categories (2014–2022)
Source: BITRE and ATSB
Figure 19: Helicopter joyflights/sightseeing and passenger transport occurrence rate per most common occurrence categories (2014–2022)
Source: BITRE and ATSB
Figure 20 and Figure 21 display the most common aeroplane and helicopter occurrence categorisations for joyflights/sightseeing only. Aircraft separation was the most common category with 0.7 per 100,000 flights, followed by engine failure or malfunction (0.6) and air-ground-air (communications) at 0.6. Helicopters’ most common occurrence category was a birdstrike at 0.9 per 100,000 flights, followed by forced/precautionary landing (0.8) and engine failure or malfunction (0.6).
Figure 20: Aeroplane joyflights/sightseeing occurrence rate per most common occurrence categories (2014–2022)
Source: BITRE and ATSB
Figure 21: Helicopter joyflights/sightseeing occurrence rate per most common occurrence categories (2014–2022)
Source: BITRE and ATSB
Commercial ballooning occurrences
Flight phase analysis
The following analysis of the 79 balloon occurrences identified the phases of flight in which:
the occurrences happened
the serious incidents and accidents occurred
people sustained injuries.
Additionally, the occurrence categories and the key safety factors that contributed to, or increased the risk of, an occurrence were extracted from the ATSB occurrence database and analysed.
Occurrence phases of flight
For the period 2014–2022, Figure 22 shows the number of occurrences per phase of flight for the 79 commercial ballooning occurrences reported to the ATSB. The majority (43 of 79, or 54%) occurred in the landing phase and a further 19% occurred during the approach phase, equalling a combined 73%.
Figure 22: Commercial ballooning occurrences per phase of flight (2014–2022)
Source: ATSB
ATSB finding
A commercial ballooning reported occurrence was more likely to occur during landing than any other flight phase.
Phases of flight of serious incidents and accidents
The reported occurrence data 2014–2022 inclusive identified 23 serious incidents and 15 accidents involving commercial ballooning. Figure 23 shows a breakdown of these serious incidents and accidents with respect to phase of flight.
Figure 23: Commercial ballooning serious incidents and accidents per phase of flight (2014–2022)
Source: ATSB
Proportionally:
11 out of 23 (48%) serious incidents occurred during the landing phase
7 out of 23 (30%) serious incidents occurred during the approach phase
10 out of 15 (67%) accidents occurred during the landing phase
1 out of 15 (7%) accidents occurred during the approach phase.
ATSB finding
A commercial ballooning serious incident or accident was more likely to occur during landing than any other flight phase.
Injuries sustained in each phase of flight
For the period 2014–2022, the ATSB occurrence database recorded 58 minor injuries, and 18 serious injuries sustained in commercial ballooning. Figure 24 shows the number of minor and serious injuries sustained in each phase of flight with phases that recorded no injuries omitted.
Figure 24: Commercial ballooning injuries by phase of flight (2014–2022)
Source: ATSB
The data identified that 47 (81%) of the minor injuries and 15 (83%) of the serious injuries occurred during landing, significantly higher than all other phases of flight.
The percentage of injuries that occurred during landing was higher than the percentages of balloon occurrences (55%), serious incidents (48%) and accidents (67%) that occurred during the landing phase of flight.
This is likely due to the nature of a balloon occurrence where an injury has occurred. For an injury to occur, a collision with an object, such as a tree or powerline, or the ground itself is usually required. This is also reflected with 7% of minor injuries occurring during the approach phase, and 10% of minor injuries and 17% of serious injuries occurring when the balloon is inflated and stationary on the ground (standing phase).
ATSB finding
A minor or serious injury on a commercial ballooning flight was most likely to occur during the landing phase of flight.
Types of injuries in commercial ballooning
Severity of injuries was recorded in the ATSB occurrence database, but details of the injuries sustained were limited, especially if the related occurrence was not investigated by the ATSB. Additionally, details of the type of basket fitted to the balloons was not captured in the occurrence database. As a result, no correlation could be made between injuries and basket type. From the available information, there were some minor injuries due to collisions with trees. Layover and hard landings contributed to the largest number of serious injuries. These resulted from balloon passengers being unrestrained within the basket and, in some occurrences, adopting an incorrect landing position. These injuries were mainly flail-type, due to collisions with other passengers, and lower limb and spinal injuries from deceleration. No fatalities occurred during ballooning operations conducted between 2014–2022.
Common reported occurrence safety factors
The safety factors recorded for the 79 commercial balloon occurrences reported to the ATSB in the period 2014–2022, were extracted from the database. The 4 leading safety factors are listed in Table 1, along with the associated injury count. 75 of the 79 occurrences identified at least 1 of these 4 leading safety factors. The most common safety factor was ‘wind’, a safety factor in 44.3% of all occurrences. Injuries were also most prevalent when wind was identified as a safety factor. The second most common was ‘assessing and planning’, which was a safety factor in 19% of occurrences, and aircraft handling also at 19% and monitoring and checking in 12.7% of all occurrences. Most occurrences had multiple safety factors. For example, wind and planning coexisted where pilots had not obtained accurate wind information during pre-flight preparation.
Aviation safety factor types that were identified were:
Wind: Situations where the direction or magnitude of wind had influenced aircraft performance, or the ability of the pilot to control the aircraft. May have also included situations where wind influenced performance of ground personnel.
Assessing and planning: Problems associated with assessment and planning activities, including briefings conducted as part of planning for a particular task. For example, pre-take-off briefings, landing position briefings.
Aircraft handling: Direct manipulation of aircraft flight path and configuration. Direct manipulation referred to actions having a relatively immediate change of flight parameters or configuration.
Monitoring and checking: Flight crew actions associated with maintaining awareness of system states (e.g. fuel, engine temperature), environmental states (e.g. weather), traffic disposition and other relevant variables.
Of the 79 balloon occurrences reported to the ATSB between 2014 and 2022, 35 (44%) attributed wind as a safety factor, and 15 (19%) attributed assessing and planning as a safety factor resulting in 8 serious incidents and 5 accidents associated with wind, and 7 serious incidents and 3 accidents associated with assessing and planning.
Occurrence review
A review of the occurrences (Appendix B – Balloon occurrences 2014–2022) identified that 44% had a wind contribution and 33% were categorised as a collision with terrain with 14% categorised as a hard landing. It was found that wind contributed in different ways. Strong winds on the ground necessitate a ‘layover’ landing, in which the basket is dragged on its side until the balloon deflates, with little directional control. These resulted in collisions with trees or other obstacles within the landing area.
In addition to impact with obstacles, occupants sustained injuries in layover landings when they did not adopt the required brace position, were unable to hold on/brace effectively and were ejected from the basket or were injured by impact with other occupants. In one occurrence, AO-2018-016, the pre-flight safety briefing was ineffective in ensuring that all passengers understood the briefing and as a result the passengers did not adopt the required landing position during a hard landing, resulting in 4 serious injuries and 7 minor injuries.
Strong winds also increased the approach distance and resulted in collisions with powerlines or trees when the pilot did not allow sufficient distance in which to manoeuvre the balloon. This was also influenced by balloon size, as larger balloons were less manoeuvrable and therefore required more obstacle clearance margin.
Pre-flight planning includes a review of the winds at different altitudes to determine approach launch and expected landing sites. When this was not done adequately, or the wind differed from expected or changed during the flight, this resulted in occurrences due to landing in unplanned locations, where the pilot did not have adequate information about the hazards.
Managing vertical descent rate relies on pilots using winds and temperatures at different heights. In one occurrence, climbing into a temperature inversion resulted in unexpected sink. In others, hard landings resulted from mismanagement of the balloon vents, delayed application of heat, or attempting to land in a confined area. Gusty conditions also resulted in hard impacts and associated injuries due to the limited cushioning of the basket.
In one occurrence, the wind was stronger than expected and the balloon overflew all suitable landing sites. This resulted in the balloon drifting over water, where the pilot elected to offload the passengers onto a boat while there was sufficient gas remaining to control the descent and passenger transfer.
In several occurrences, launching in the early morning resulted in the rising sun affecting the pilot’s visibility and subsequent impact with obstacles. Fog was another factor that reduced a pilot’s visibility and resulted in impact with obstacles during approach.
Occurrence locations
As the ATSB occurrence data included location, geographical data for Australian balloon occurrences between 2014–2022 was extracted from the database and plotted using Google Earth (Figure 25).
Balloon weather packages
CASR Part 131 requires balloon operators to obtain a weather forecast from an authorised source, such as the Bureau of Meteorology, valid for a period extending 2 hours beyond their landing time. Since October 2020, the Bureau of Meteorology provided balloon weather packages, available through the Bureau of Meteorology website, containing a compilation of relevant information for balloon flight planning. The weather packages replaced a previous recorded phone service for balloon pilots and a text-based product for Alice Springs. The packages have standardised and automated weather information for 21 locations around Australia that are frequently used by balloonists (Figure 25).
Most of the information provided in the product can be found in other aviation weather products, including area and aerodrome forecasts and observations. The unique components of the package are model meteograms (which give time series of wind and humidity at different levels in the atmosphere), ‘F160 forecasts’ (which show the vertical distribution of wind and temperature) and a wind profiler time series. These products assist the pilot in determining cloud and wind at different heights throughout the period of the forecast.
Source: Google Earth and Bureau of Meteorology, annotated by the ATSB
Occurrences by weather package location
Comparison of the occurrence and weather package locations identified that 77 of the 79 occurrences were geographically located within a 40 km radius of the nearest central point of a balloon weather package location. The remaining 2 occurrences were located about 75 km and 200 km from the nearest respective weather package areas.
The availability of a weather package did not relate to the number of occurrences or their contributing factors.
Injuries by factor and by weather package location
Table 2 shows the number of occurrences by weather package location where wind was identified as a safety factor and the number of those that resulted in serious and/or minor injuries (regardless of how many people were injured). Canberra, Sydney, and Alice Springs had zero injuries in all occurrences. The locations with the highest percentage of injuries per occurrence with wind as a safety factor, were Avon Valley (67%) and the Hunter Valley (50%).
Table 2: Wind occurrences with an injury by location
Nearest weather package location
Wind occurrence
Wind occurrence with injury
Serious injury occurrence
Minor injury occurrence
Occurrences with injuries
Melbourne (Vic)
13
3
2
2
23%
Yarra Valley (Vic)
5
2
0
2
40%
Hunter Valley (NSW)
2
1
0
1
50%
Gold Coast/Ipswich (Qld)
6
2
1
2
33%
Avon Valley (WA)
3
2
1
2
67%
Balloon envelope size
The Civil Aviation Safety Authority (CASA) maintains a register of all VH-registered aircraft. This register includes the type of aircraft, manufacturer, model, and the registration holder of all VH-registered aircraft. However, the database does not include the type of basket that is used nor the number of passengers that the balloon can carry. The ATSB collected end of calendar year registers from 2014 to 2022 and extracted VH‑registered balloon data. The total number of VH-registered balloons by year is shown in Figure 26. This data includes private balloons.
Figure 26: Total number of VH-registered balloons per year (2014–2022)
Source: CASA, annotated by the ATSB
Due to the aircraft register not recording envelope size, the designated model of each balloon was extracted from the database and cross-referenced with manufacturer data to determine the envelope size. Between 2014 and 2022, the total number of VH-registered balloons on the Australian civil aircraft register increased from 386 to 429, an 11% increase. The increase in the number of VH-registered balloons over 400,000 cubic ftis shown in Figure 27.
Figure 27: Number of VH-registered balloons over 400,000 cubic ft per year (2014–2022)
Source: CASA, annotated by the ATSB
At the end of calendar year 2014 there were 25 balloons over 400,000 cubic ft. By the end of 2022 this number had increased to 51, an increase of 104%, with a breakdown as shown in Table 3:
Table 3: VH‑registered balloons over 400,000 cubic ft
Envelope size (cubic ft)
2014
2022
Increase
400,000 to 449,999
13
25
92%
450,000 to 499,999
12
20
67%
>= 500,000 (2016 onwards)
0
6
500%
from 2016
Over the safety study period, there was an 11% increase in total VH-registered balloons. This increase included a 92% increase in balloons between 400,000 and 449,000 cubic ft, and a 67% increase in balloons between 450,000 and 499,000 cubic ft. One balloon above 500,000 cubic ft was first registered in 2016, increasing to a total of 6 by the end of 2022.
CASR Part 131 Manual of Standards, Chapter 25.03, specified that the maximum number of passengers permitted per flight was 24. To carry this number, a balloon must have a minimum volume of 450,000 cubic feet (Cameron Balloons Ltd, 2025). During the safety study period, there was a 116% increase in balloon envelopes exceeding 450,000 cubic feet. This growth indicates a rise in the number of balloons capable of carrying the maximum passenger load on a single flight.
ATSB finding
Over the safety study period, from 2014–2022, there was a significant increase in balloons with an envelope size above 400,000 cubic ft on the CASA aircraft register, and as a result, an increase in the number of balloons capable of carrying the maximum number of passengers per flight.
Occurrences by balloon envelope size
Using the same methodology to determine envelope size as above, the balloon sizes of all occurrences was extracted from the occurrence data. This data was then compared against occurrences and injuries and displayed in Table 4, identifying that:
balloons with an envelope size of 240,000 cubic ft had the highest number of occurrences with a total of 34, these occurrences resulted in 8 minor injuries and 2 serious injuries
balloons with an envelope size of 350,000 cubic ft had the highest number of serious injuries, with a total of 6 with an associated 12 minor injuries over 6 occurrences
there were 2 occurrences involving balloons with an envelope size of 525,000 cubic ft, with 2 serious injuries and 13 minor injuries
balloons above 400,000 cubic ft had a combined total of 23 occurrences out of 79 (29%), 34 out of 58 minor injuries (59%), and 9 out of 18 serious injuries (50%).
Table 4: Occurrences and injuries by balloon size 2014–2022
Envelope size (1,000 ft3)
Occurrences
Minor injuries
Serious injuries
unknown
1
0
0
90
1
0
0
105
1
0
0
120
2
0
0
210
1
0
0
240
34
8
2
275
1
3
0
300
4
1
1
340
1
0
0
350
6
12
6
400
6
11
4
425
8
4
2
450
11
6
0
525
2
13
3
Total
79
58
18
Figure 28: Average injuries per occurrence by balloon envelope size (2014–2022)
Source: ATSB
The following was identified with wind as a safety factor (Figure 29):
the 240,000 cubic ftballoons had the highest number of occurrences with 6 minor injuries and 2 serious injuries from 19 wind-related occurrences
the 350,000 cubic ftballoons had the highest number of serious injuries with 4 serious injuries from 4 wind-related occurrences
the 350,000, 400,000 and 425,000 cubic ft balloons had 7 serious injuries, 23 minor injuries out of 9 occurrences combined.
Figure 29: Safety factor of wind by balloon size
Source: ATSB
Civil Aviation Safety Regulations Part 131 exposition requirements
In December 2021 a regulatory change came into effect for ballooning, with the introduction of CASR Part 131 Balloons and hot air airships. These changes were not fully implemented until November 2024, when the Part 131 Manual of Standards commenced.
There are 21 CASR Part 131 AOC holders in Australia. A requirement for the issue of a Part 131 Air Operator’s Certificate (AOC), is for balloon transport operators to produce a CASA‑approved company exposition. Included within the exposition is the following requirement as per CASR Part 131:
131.195 Content of exposition
(h) details of each plan, process, procedure, program and system implemented by the operator to safely conduct and manage the operator’s balloon transport operations in compliance with the civil aviation legislation.
Note: The plans, processes, procedures, programs and systems mentioned in paragraph (h) may be set out in one or more operator manuals.
Australian air transport aeroplane and helicopter AOC holders are also required to maintain a CASA-approved exposition and require a separate safety management system as per CASR Part 119. There is no current requirement for a Part 131 AOC holder to maintain a separate safety management system.
CASA advised the ATSB that it reserved the requirement for Balloon AOC holders to have an SMS in the drafting of Part 131. CASA also assessed that the transition to CASR Parts 91 and 131 was sufficient regulatory change for operators to manage at that time. Since the commencement of Part 131, CASA reported concentrating on implementing the Part 131 MOS and giving operators time to produce a compliant exposition. CASA also advised that the next tranche of work will be the transitioning of balloon pilot licensing to CASRs, followed by the transition of continuing airworthiness and maintenance requirements into Part 131. Inclusion of an SMS for balloon transport operators has not been scheduled at this time.
Summary
The data showed that a commercial balloon flight was 1.5 to 4 times more likely to have a reported occurrence than a comparable joyflights/sightseeing and passenger transport activity in an aeroplane, and about 3 to 9 times more likely than in a helicopter. These occurrences were coded as incidents, serious incidents or accidents, depending on the severity of injuries and aircraft damage. The data showed that a serious incident or accident was about 6 to 9 times more likely to occur during a commercial balloon flight than a comparable aeroplane flight and 21 to 25 times more likely than during a helicopter flight.
The data also showed a difference between the most common occurrence categories for balloons, compared with aeroplanes and helicopters. Commercial balloons were more likely to have a collision with terrain, hard landing, cabin injury or wirestrike. Aeroplanes and helicopters were more likely to have a birdstrike, diversion, forced/precautionary landing or engine failure/malfunction.
The balloon occurrences and associated injuries usually happened during approach and landing. The effect of wind was identified as a contributing safety factor to most occurrences. However, as the number of flights per region was not collected from operators, a correlation between the availability of detailed weather information and wind‑related occurrences could not be determined. Assessing and planning, aircraft handling, and monitoring and checking were also identified as common safety factors. The combination of wind-related pilot planning and decision-making, and aircraft handling in those conditions, resulted in most of the occurrences and injuries.
There were no fatalities in commercial ballooning during the 2014–2022 period, while aeroplane and helicopter joyflights/sightseeing activities resulted in 7 fatalities, and a further 24 fatalities occurred in aeroplane and helicopter passenger transport activities. However, passengers in commercial balloon flights were 14 to 35 times more likely to sustain an injury than in an aeroplane and 60 to 70 times more likely than in a helicopter.
Overall, a passenger in a commercial balloon flight was at significantly greater risk of minor or serious injury than in a similar aeroplane or helicopter flight, but unlikely to be fatally injured. Additionally, the number of passengers exposed to the risk in a single occurrence has increased with the increase in balloon size being used for commercial passenger flights. However, there was no apparent link between larger balloons and the number of ballooning-related injuries.
Injury data showed the magnitude of passenger injury risk in balloon flights compared with aeroplane and helicopter flights. While 99.7% of aeroplane and 99.8% of helicopter joyflights/sightseeing and passenger transport incidents, and 100% of both aeroplane and helicopter incidents in joyflights/sightseeing activities resulted in no injuries, only 71% of balloon incidents were injury-free.
Similarly, 95% of aeroplane and 100% of helicopter joyflights/sightseeing and passenger transport serious incidents had no injuries, and 100% of both aeroplane and helicopter joyflights/sightseeing serious incidents reported no injuries, only 83% of balloon serious incidents were injury‑free.
Furthermore, 62% of aeroplane and 38% of helicopter joyflights/sightseeing and passenger transport flight accidents had no injuries, and 25% of aeroplane and 50% of helicopter joyflights/sightseeing accidents had no injuries. 27% of balloon accidents reported no injuries. This shows that joyflights/sightseeing passengers in a balloon were slightly less likely to be injured in an accident than in an aeroplane, but more likely to be injured than in a helicopter. Furthermore, balloon passengers were more likely to be injured in an accident than aeroplane or helicopter passengers in a passenger transport accident.
The increased injury risk for balloon passengers is likely due to balloon passengers being unrestrained in an open basket. Fewer injuries per accident for aeroplanes and helicopters shows that these aircraft sustain greater damage with fewer injuries to occupants than balloons. From the available injury information, the majority of the balloon accident injuries consisted of lower limb injuries from terrain collisions, and flail type injuries from passengers colliding with each other.
A collection of more detailed injury data would allow further analysis of the mechanism of injuries, with the aim of identifying possible ways to improve passenger safety in commercial balloon flights. Passengers are therefore encouraged to provide detailed injury information in ATSB occurrence notifications. Prior to a balloon flight, passengers should be informed of the injury risks, as balloons do not have the restraint systems or impact reduction engineering afforded to passengers in aeroplanes or helicopters.
Although not a legislative requirement, an SMS can assist balloon operators to employ a structured approach to managing risk. This study identified several hazards applicable to balloon operations in Australia, such as wind, pre-flight planning, and passenger position during landings. However, there will be additional hazards applicable to specific locations or types of operation that individual operators will be aware of. Structured identification and treatment of these hazards should result in a reduction of occurrences and injuries in commercial ballooning operations.
detailed passenger safety briefings and visual cards
ensuring passengers can adopt the appropriate brace or landing position
clear instructions to passengers in an emergency
positioning of passengers to reduce injuries resulting from contact between them.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
From the evidence available, the following findings are made with respect to the Australian balloon transport operation occurrences between 2014–2022:
ATSB findings
A commercial balloon flight was 1.5 times more likely to have a reported occurrence than a comparable joyflights/sightseeing and passenger transport activity in an aeroplane and 3.4 times more likely than a helicopter.
A commercial balloon flight was 4.2 times more likely to have a reported occurrence than a comparable joyflights/sightseeing activity in an aeroplane and 9.2 times more likely than a helicopter.
A serious incident or accident was 8.9 times more likely to occur on a commercial balloon flight than a joyflights/sightseeing or passenger transport activity in an aeroplane and 25.6 times more likely than in a helicopter.
A serious incident or accident was 5.4 times more likely to occur on a commercial balloon flight than a joyflights/sightseeing activity in an aeroplane and 21.2 times more likely than a helicopter.
A person was 34.7 times more likely to sustain an injury on a commercial balloon flight than in an aeroplane on a joyflights/sightseeing and passenger transport charter activity and 58.5 times more likely than in a helicopter.
A person was 13.7 times more likely to sustain an injury on a commercial balloon flight than a joyflights/sightseeing activity in an aeroplane and 69.4 times more likely than in a helicopter.
A person was 57.2 times more likely to sustain a serious injury on a commercial balloon flight than a joyflights/sightseeing and passenger transport charter activity in an aeroplane and 52.6 times more likely than in a helicopter.
A person was 34.2 times more likely to sustain a serious injury on a commercial balloon flight than a joyflights/sightseeing activity in an aeroplane and 26.0 times more likely than in a helicopter.
A commercial ballooning reported occurrence was more likely to occur during landing than any other flight phase.
A commercial ballooning serious incident or accident was more likely to occur during landing than any other flight phase.
A minor or serious injury on a commercial ballooning flight was most likely to occur during the landing phase of flight.
Of the 79 balloon occurrences reported to the ATSB between 2014 and 2022, 35 (44%) attributed wind as a safety factor, and 15 (19%) attributed assessing and planning as a safety factor resulting in 8 serious incidents and 5 accidents associated with wind, and 7 serious incidents and 3 accidents associated with assessing and planning.
Over the safety study period, from 2014–2022, there was a significant increase in balloons with an envelope size above 400,000 cubic ft on the CASA aircraft register, and as a result, an increase in the number of balloons capable of carrying the maximum number of passengers per flight.
Glossary
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
BITRE
Bureau of Infrastructure, Transport and Research Economics
BOM
Bureau of Meteorology
ICAO
MOS
SMS
International Civil Aviation Organization
Manual of Standards
Safety management system. A systematic approach to organisational safety encompassing safety policy and objectives, risk management, safety assurance, safety promotion, third party interfaces, internal investigation and SMS implementation.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Civil Aviation Safety Authority
Bureau of Infrastructure, Transport and Research Economics
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
Bureau of Infrastructure, Transport and Research Economics.
Submissions were received from:
Civil Aviation Safety Authority
Bureau of Infrastructure, Transport and Research Economics.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
A helicopter accident in Arnhem Land highlights the risks to VFR pilots of flying after last light, and the potentially fatal consequences of survivable accidents in remote locations, an ATSB investigation report details.
The pilot of a Robinson Helicopter Company R22 had been part of a multi-vehicle animal mustering operation in the Arafura Swamp, south of Ramingining, Northern Territory, on 14 November 2022.
After the mustering had concluded for the day, members of the mustering operation began departing the swamp and it was expected the pilot would depart shortly to pick up another member of the group, before continuing to the camp.
However, when other members of the mustering operation arrived at camp, the pilot and helicopter were not there.
Realising that the pilot was missing and becoming increasingly concerned about the pilot’s welfare, the mustering group subsequently commenced a search using land vehicles, before organising an aerial search the following morning.
The wreckage of the helicopter was subsequently located at about 1300 on 15 November, about 6 km from the mustering camp. The pilot was found deceased outside the aircraft, and the helicopter was destroyed.
The pilot held a Commercial Pilot Licence (Helicopter), but was not qualified for flight in non-visual conditions, and the helicopter was not equipped for night flight.
On the evening of 14 November last light occurred at 1858. Considering the location of the accident site, the pilot probably flew easterly from the camp, facing away from the setting sun. There was no ground-based lighting in the area, and cloudy conditions associated with a nearby storm may have also reduced visibility.
“The ATSB investigation found that the accident flight occurred after nautical twilight and in dark night conditions. The pilot likely became spatially disoriented, leading to a collision with terrain,” said ATSB Director Transport Safety Dr Stuart Godley.
ATSB research and investigation reports regularly refer to the dangers of flying after last light without the appropriate qualifications and equipment to do so.
“Dark night conditions provide no useable external visual cues and in these environments all VFR pilots, including those with endorsement to operate under the night VFR, will experience an increased risk of spatial disorientation,” said Dr Godley.
“The ATSB encourages all VFR pilots to take note of the tragic consequences associated with dark night flight in this accident.
“Landing 10 minutes before last light provides a reliable method for VFR pilots to ensure they have the necessary visual cues.”
A pathologist’s report found that the injuries sustained by the pilot in the collision were probably not fatal, and that the pilot probably succumbed to environmental exposure.
After the collision, it is likely the pilot manoeuvred out of the seat belt, outside of the damaged helicopter which was laying on its side. With injuries reducing the pilot’s mobility, the pilot likely planned to wait for rescue. The day time conditions were hot and humid.
While the helicopter was equipped with a manually activated personal locator beacon, the beacon was secured to the inside of the helicopter, and the pilot was probably unable to access it once outside the helicopter after the collision.
The ATSB found that the combination of the personal locator beacon not being activated and authorities not being notified when the aircraft was missing resulted in a delay to the pilot being located before succumbing to environmental exposure after sustaining survivable injuries in the accident.
Dr Godley noted that the investigation highlights how remote locations can present an increased risk of fatal consequences from otherwise survivable accidents.
“Pilots operating in remote locations should carefully consider the use and location of equipment such as a personal locator beacon, to maximise the likelihood it will be accessible to them in the event of an accident,” he said.