The Australian Transport Safety Bureau has discontinued its investigation into a light aircraft collision with terrain in Queensland’s Clarke Ranges, after determining the pilot was not qualified to conduct the accident flight.
On 2 April 2023, a pilot and passenger departed from Natal Downs Station for a private flight to the Lakeside Airpark, south of the Whitsundays, in a Piper Cherokee single-engine light aircraft.
A search and rescue operation commenced after the aircraft failed to arrive and, the following day, wreckage was located on a steep slope at an elevation of 1,913 ft. The pilot and passenger were fatally injured, and the aircraft was destroyed.
A discontinuation notice published today on the ATSB’s website notes the aircraft departed in good weather for visual flight, but flew into poor conditions, including low cloud around the Clarke Ranges, where the topography was substantially more rugged and elevated than the coastal or inland portions of the planned route.
Evidence gathered from the accident site suggested the aircraft impacted the ground intact.
A review of records established the pilot did not hold an aeroplane pilot’s licence (either a Recreational Pilot Licence or Private Pilot Licence) required to conduct the flight.
Records from the flying school where the pilot trained showed they had completed 30.4 hours of flight instruction between November 2021 and November 2022, including 2.9 hours on the Piper Cherokee.
On that basis, the ATSB determined there was limited safety benefit in continuing to direct resources at this investigation when compared with other priorities.
“Licencing regulations administered by the Civil Aviation Safety Authority are designed to ensure pilots are properly trained and qualified to manage challenges likely to be encountered during flying operations,” ATSB Chief Commissioner Angus Mitchell said.
“This includes training intended to teach pilots to identify and manage situations presented by adverse weather, both at the pre-flight planning phase and during flight.
“When pilots operate outside the licensing regulations, they remove built-in safety defences,” Mr Mitchell said.
Despite the investigation being discontinued, Mr Mitchell emphasised some important safety lessons.
“This accident highlights the importance of following the standards for the operation and maintenance of aircraft to ensure the safety of flight, and further demonstrates that weather continues to remain one of the most significant causes of accidents in general aviation,” he said.
“The ATSB encourages all pilots, regardless of qualification or experience level, to develop the knowledge and skills required to avoid unintentional operations into adverse weather.”
On the morning of 27 June 2023, the pilot of a Robinson Helicopter R22 Beta II, registered VH‑PSC and operated by Top End Mustering, was conducting mustering operations in company with a second R22 registered VH-RCS, on Limbunya Station, Northern Territory.
After not hearing from the pilot of VH-PSC for some time, the pilot of VH-RCS attempted to contact VH-PSC with no response received, and the ground mustering crew stated that they had no recent communication either. Subsequently, the pilot of VH-RCS commenced a search and shortly after located the wreckage of VH-PSC. The helicopter was destroyed, and the pilot had sustained fatal injuries.
What the ATSB found
The ATSB found that, for reasons that could not be determined, VH-PSC collided with terrain in a nose and right-side down orientation. The site and wreckage examination identified signatures consistent with low rotor energy and low-to-nil engine power.
There was no evidence of any flight control or mechanical system abnormality that would have prevented the helicopter from operating normally. In addition, in the absence of an identified problem with the helicopter, the reason for the loss of control could not be determined.
The ATSB also identified that the maintenance release contained no endorsements for daily inspection certification, hours flown, total time‑in‑service or engine oil uplift. This was despite VH‑PSC being operated daily since its issue 13 days prior. A scheduled 25-hour engine oil and filter change had reportedly been conducted, however, had not been certified on the maintenance release. Further, the absence of recorded operating hours increased the risk of the helicopter having been operated beyond other scheduled maintenance requirements.
Safety message
Routine low-level flight brings several significant complexities to a helicopter operation including management of emergencies and the conduct of forced landings. Time to respond and the availability of suitable forced landing areas may also be significantly reduced. Main rotor energy management is an important element of maintaining control and safely landing a helicopter.
Aircraft owners and pilots should ensure that the maintenance release is updated at the end of each day’s flying. This will allow all pilots to be aware of the operational status of the aircraft and to avoid unintentional flight beyond scheduled maintenance. In addition, engine oil uplift records assist with trend monitoring of engine condition.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
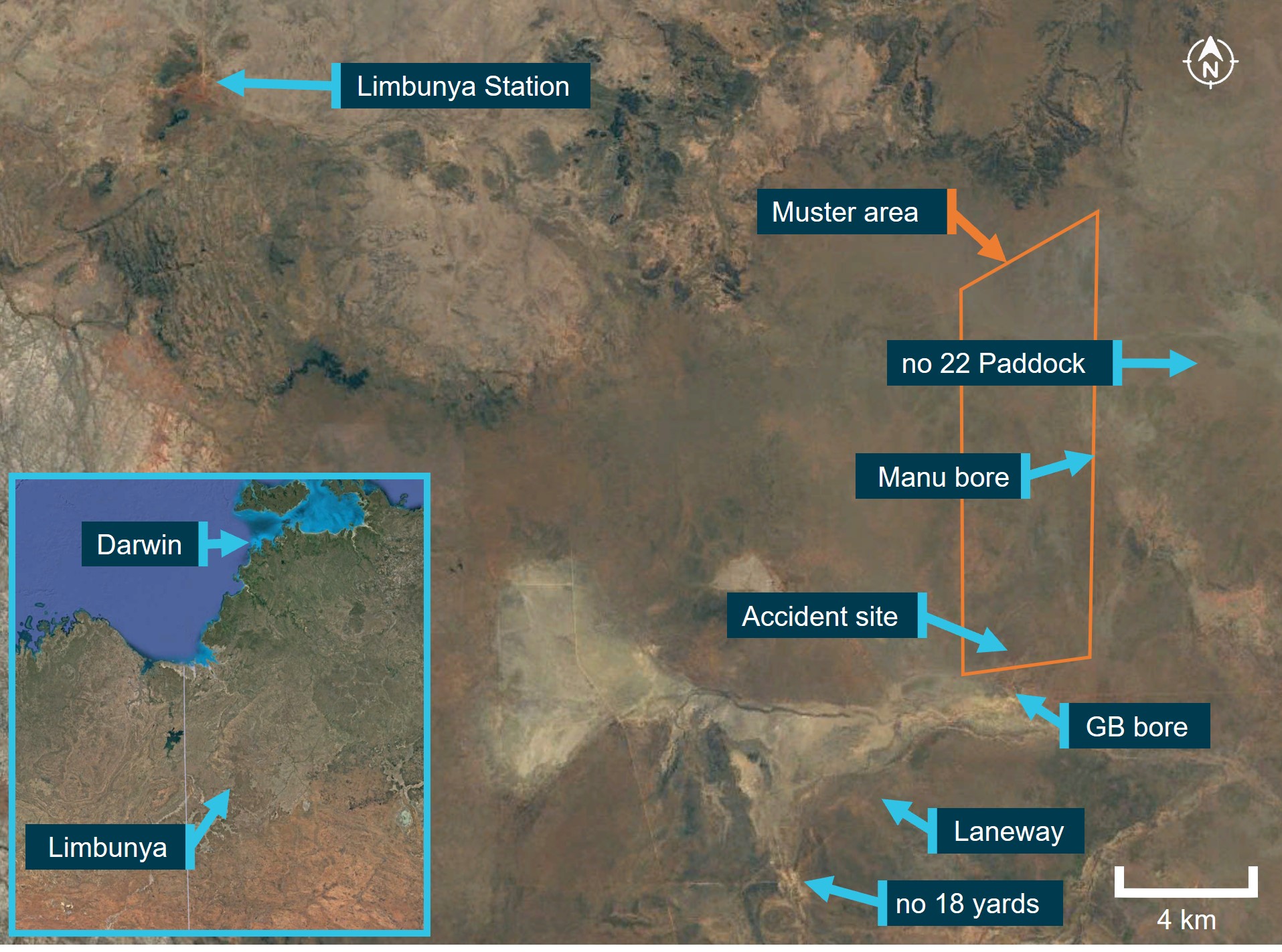
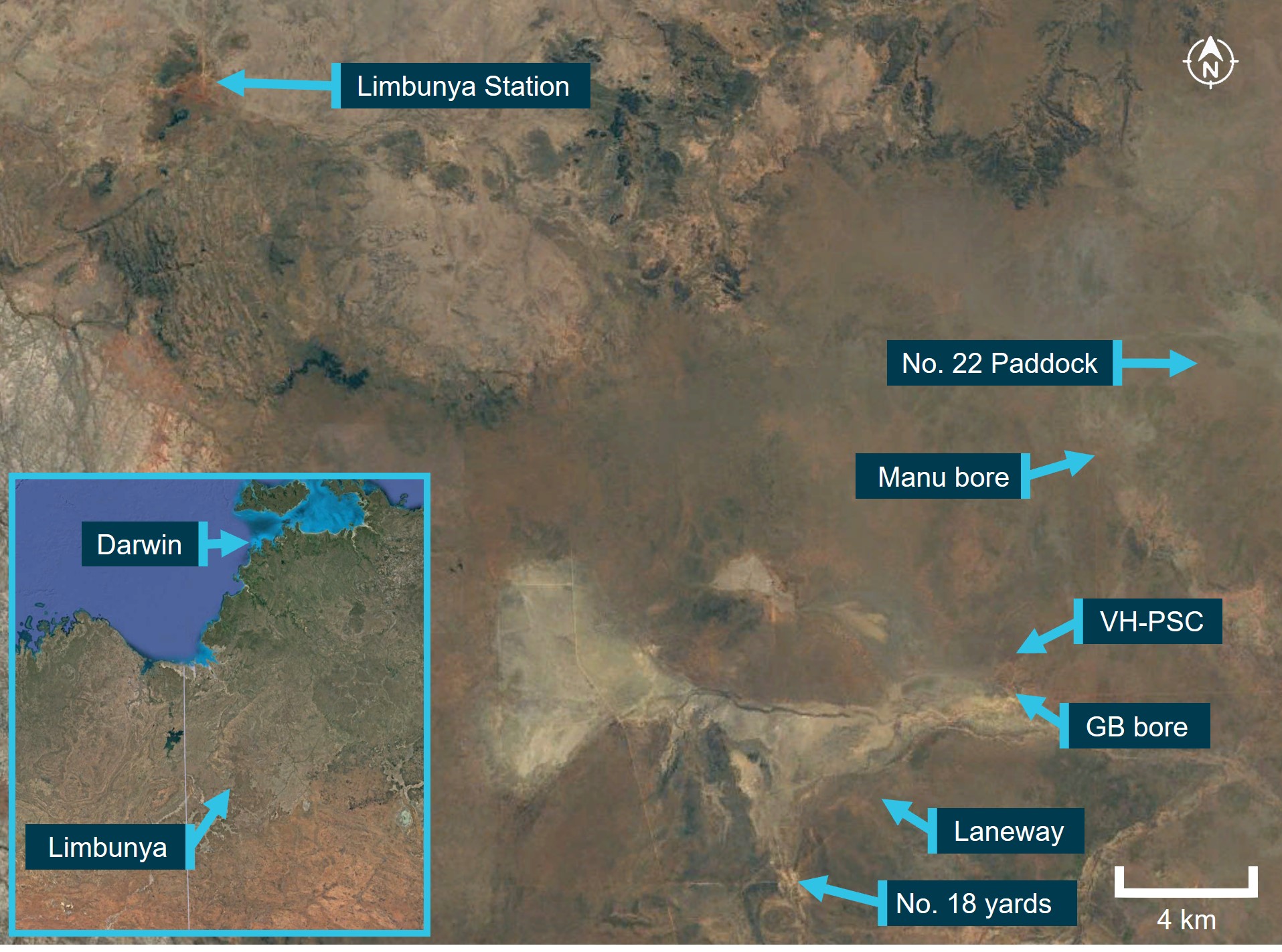
On 27 June 2023, at about 0700 local time,[1] the pilot of a Robinson Helicopter R22 Beta II, registered VH‑PSC (PSC), and operated by Top End Mustering, departed Limbunya Station, Northern Territory, in company with a second R22 registered VH‑RCS (RCS). Their task was to muster stock in a small paddock to the north of ‘GB’ bore, about 29 km to the south-east of the station homestead. In addition, they were to assist the ground mustering crew (on horseback and motorcycles) to move stock that had been mustered the previous day from ‘no 22’ paddock into the GB bore holding yards, to the ‘no 18’ yards (Figure 1). RCS was working the western side of the paddock, with PSC working down the eastern side. The helicopter pilots could communicate with each other via very high frequency (VHF) or ultra high frequency (UHF) band radios, and with the ground mustering crew via UHF.
The helicopters arrived at the northern end of the paddock at about 0730 and began pushing cattle south towards the GB bore holding yards. The pilot of PSC then supported the ground mustering crew in moving stock from the yards into a fenced laneway. The laneway would guide the stock to the no 18 holding yards that were located about 8 km to the south‑west.
At about 0915, when the cattle were moving along the laneway under the control of the ground mustering crew, the pilot of PSC was released from that task, and returned to assist the pilot of RSC with completing the mustering task.
At about 0930, the pilot of RCS diverted to Manu bore to refuel the helicopter from drum stock. After refuelling, the pilot of RCS departed back to the small paddock, and at about 0945 acknowledged a departure call from the pilot of PSC, on VHF radio, who had also completed refuelling at Manu bore.
Following a period of radio silence, the pilot of RCS contacted the head musterer at about 1000, via UHF, to enquire if they had been in contact with the pilot of PSC. The head musterer advised that no contact had occurred since about 0915. Having received no replies from PSC to their radio calls, the pilot of RCS commenced searching the area around Manu bore, and then progressed the search towards GB bore.
After about 15 to 20 minutes, the pilot of RCS located the wreckage of PSC. The helicopter was destroyed, and the pilot had sustained fatal injuries. There were no witnesses to the accident.
Figure 1: Limbunya Station and operational area
Source: Google Earth, annotated by the ATSB
Context
Pilot information
Qualifications and experience
The pilot held a Commercial Pilot Licence (Aeroplane) since 1985, a Commercial Pilot Licence (Helicopter) since 1986 and a valid Class 1 Aviation Medical Certificate. The pilot also held helicopter gas turbine engine and night visual flight rules ratings. Additionally, the pilot held a low‑level aerial mustering (aeroplane and helicopter) rating and helicopter sling operations, valid until 3 April 2025.
On 3 April 2023, the pilot underwent a flight review in an R22, with a helicopter low-level flight review and a company pilot proficiency check also conducted at the same time, at Kununurra, Western Australia. The pilot demonstrated proficiency with emergency procedures and the instructor’s handwritten flight review note stated, ‘all to a good standard. Placed a lot of emphasis on power management’.
The last entry in the pilot’s helicopter logbook was dated 10 July 2021, almost 2 years prior to the accident, with a total helicopter aeronautical experience of 12,288.1 hours. Using several sources of information, the ATSB calculated the pilot had about 14,000 flying hours on helicopters at the time of the accident, including over 3,000 hours on the R22 helicopter type.
Recent history
The pilot relocated to Kununurra and had been operating the R22, R44 and Bell 206-series helicopters across north-western Australia since 3 April 2023. The pilot had operated several helicopters most days from 5 June 2023, and VH-PSC (PSC) exclusively since 21 June 2023.
On 25 June, the pilot ferried PSC to Limbunya Station, arriving around 1800. On 26 June, the pilot conducted mustering operations at the station, with 2 other company R22 helicopters, from about 0630 until about 1300.
The second helicopter pilot and several members of the ground mustering team reported the pilot was in good spirits at dinner the night before the accident and retired to their room about 2130.
The ATSB considered whether the pilot’s activity in the preceding days and months may have led to them being fatigued at the time of the accident. A review of the pilot’s diary indicated they had operated a helicopter for all but 19 days in the preceding 90 days, totalling over 340 hours of duty time.[2] The diary indicated over 170 hours in the preceding 30 days and about 47 hours in the 7 days prior to the accident. The accident occurred on the 14th consecutive day of duty. However, the ATSB noted a short ferry flight on 25 June, the pilot being relieved from duty about midday on 26 June and being on duty for less than 5 hours on the day of the accident. It was possible that the months of extensive work time coupled with high workload operations had the potential to produce cumulative fatigue. However, noting the workload and opportunity for rest in the preceding days, there was insufficient evidence to establish if the pilot was likely experiencing a level of acute fatigue known to affect performance at the time of the accident.
Helicopter information
General
VH-PSC was a Robinson Helicopter Company (RHC) R22 Beta II helicopter, serial number 4429, powered by a Textron Lycoming O-360-J2A, 4-cylinder carburetted piston engine (Figure 2). It was manufactured in the United States in December 2008 and first registered in Australia in January 2009.
The R22 has 2 seats, with the pilot flying from the right seat, and each seat was fitted with a seatbelt and inertia reel shoulder strap, similar to those used in motor vehicles. The helicopter was not fitted with an optional cabin heating system.[3] Typical for mustering activities, the helicopter was being operated with both doors removed.
Figure 2: VH-PSC
Source: Operator
Systems information
Rotor drive system
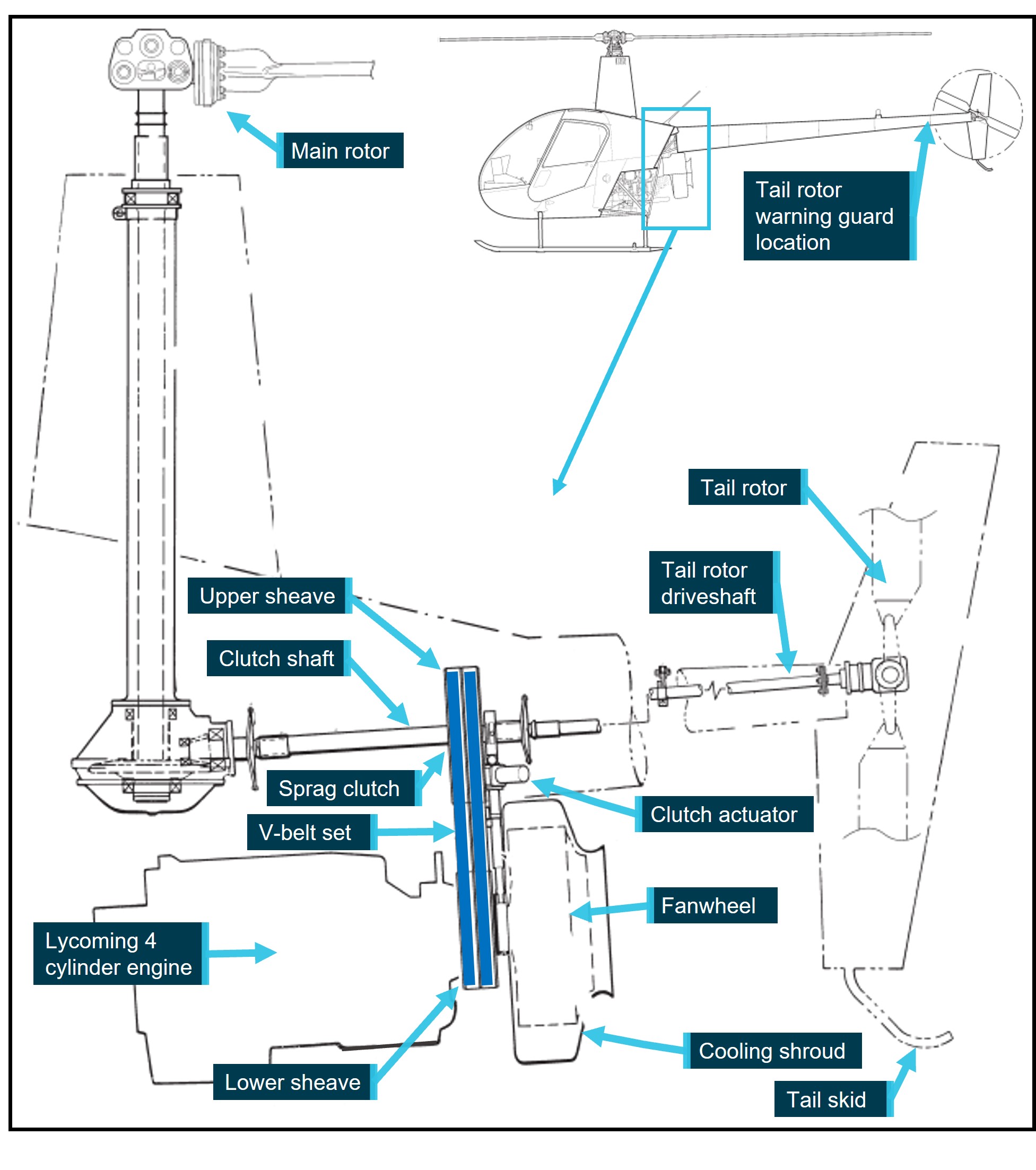
The rotor drive system on the R22 helicopter uses 2 reinforced rubber drive belts (V-belts). The drive belts are double-banded and fitted to upper and lower multi-grooved sheaves. The upper sheave has an overrunning sprag clutch (freewheeling unit)[4] in its hub, which the clutch shaft passes through. The clutch shaft transmits power forward to the main rotor gearbox and aft to the tail rotor driveshaft. The lower sheave is attached directly to the engine crankshaft.
The upper sheave is moved, relative to the lower sheave, by means of an electric clutch actuator, thereby controlling the tension on the drive belts. This allows the engine to be unloaded during startup (drive belts slack) without the rotor system engaged, and then tensioned to allow engine power to be transmitted to the rotor drive (Figure 3).
The fanwheel utilised on the R22 is a commercial product, modified by RHC. Its purpose is to direct cooling air onto the engine. It is constructed of steel, and is comprised of 8 cooling vanes welded to the rear plate (on the engine side) and a support ring on the outer side. The assembly mounts onto the fan shaft, behind the lower sheave, and is enclosed in a fibreglass shroud.
The tail rotor was fitted with a visual warning guard located on the underside of the tailcone, just forward of the tail rotor. Painted with red and white stripes, it provides a visual warning of the tail rotor disc, which can be difficult to see when operating.
Figure 3: Diagram of the R22 rotor drive system
Source: Robinson Helicopter Company, annotated by the ATSB
Low rotor revolutions per minute (RPM) warning
A ‘low RPM’ warning light will illuminate, with an associated horn, when rotor RPM is at or below 97%, regardless of engine RPM.
Fuel system
The fuel system consists of a main tank (left side, when looking from the rear of the helicopter, 69 L) and an auxiliary tank (right side, 37 L). Fuel is gravity-fed via a gascolator to the carburettor.
Engine governor system
Under normal conditions, the governor senses engine RPM and makes adjustments to the throttle control to maintain a constant engine RPM, which leads to a constant rotor RPM in flight. The governor can be selected on or off using the toggle switch on the right seat’s collective.[5] The R22 pilot’s operating handbook (POH) stated that the governor may not prevent over- or under-speed conditions generated by aggressive flight manoeuvres. In the event of malfunction, the pilot can override the governor and manipulate the throttle to maintain engine RPM, until the governor can be selected off, or rendered inoperative by pulling the circuit breaker.
Given the dynamic nature of mustering operations, when compared to flying in cruise (normal flight conditions), the pilot was likely not relying on the governor.
Carburettor heat system
The helicopter was fitted with a carburettor heat system, which directed hot air collected from a scoop installed on the engine exhaust system, via a duct, to the engine induction air box. Within the air box was a sliding guillotine-type valve to proportion the mix of cool and heated air. The pilot could monitor the temperature of the carburettor air using the carburettor air temperature gauge on the instrument panel console.[6] The carburettor heat control knob was situated aft and rear of the cyclic,[7] with ‘down’ being no heat and ‘up’ providing full heat, or anywhere in between as selected by the pilot. This heated air prevented the temperature within the carburettor from dropping to, or below, the freezing point of water.
The helicopter also had a carburettor heat assist system, which automatically applied carburettor heat when lowering the collective, generally for descent, to reduce pilot workload. The pilot could override the heat assist. In addition, a latch was provided at the carburettor heat control knob to lock the heat assist off when not required.
Fuel rotary pump
The operator reported that each helicopter would carry a drum fuel pump, which could be broken down into components with the suction tube (standpipe) capable of being separated into 3 sections. The operator advised the fuel pump components could be stored under the left (passenger) seat or optionally store some, or all, of the pump components in the left seat footwell.
The pilot of RCS used their pump for refuelling from the drum stock at Manu bore.
Airworthiness and maintenance
General
A periodic inspection of the helicopter was to be conducted every 100 hours or 12 months, whichever came first. In addition, the helicopter was subject to an overhaul every 2,200 hours or 12 years. On 15 June 2023, the helicopter underwent a 100-hourly/annual inspection, during which the engine was replaced with a newly overhauled unit.[8] As part of the periodic inspection, the exhaust system was certified as being visually inspected and pressure tested. A new maintenance release was issued at this time, which stated that the helicopter had accrued 6,300.2 hours total time‑in‑service.
Maintenance release
The maintenance release (MR) is a legal document that is part of the ongoing airworthiness requirements of an aircraft and is divided into several parts. Part 1 details any scheduled maintenance that will be required to be completed during the MR period of validity. When a maintenance task has been completed it can be certified for in Part 2 of the MR, or in the aircraft maintenance logbook. The person who performed the maintenance, or the certificate of registration holder is then required to clear the entry in Part 1, making note if the certification was logged in Part 2 or the aircraft logbook. Part 3 of the MR is used to certify for the daily inspection of the aircraft, for recording the daily total flight time, calculating the total time-in-service at the end of each day’s flying and for tracking other events, such as engine oil uplift. The regulations state that, if the certificate of registration holder, the pilot in command or the operator becomes aware the aircraft may be operated beyond any maintenance requirement noted in Part 1, then they must make ‘an endorsement signed by him or her setting out the facts of the situation and stating that the aircraft is unairworthy, and thereupon the maintenance release ceases to be in force’.
The current MR was located at the accident site. An endorsement, in Part 1 of the MR, included that an engine oil and filter change was required at 25, 50 and 75 hours post engine change. Since its issue on 15 June 2023, there were no endorsements for daily inspection certification, hours flown, total time-in-service or engine oil uplift.
Pilot approved maintenance
The civil aviation regulations permitted the pilot to perform some maintenance including changing oil filters and changing or replenishing engine oil. Further, the regulations required that ‘a person who carries out maintenance … must ensure that completion of the maintenance is certified in accordance with … the CASA [Civil Aviation Safety Authority] system of certification of completion of maintenance’.
Engine oil and filter maintenance
Following fitment of any new, rebuilt or overhauled engine, RHC required Lycoming service bulletin 480 be complied with. The bulletin required an oil and filter change after the first 25 hours of engine operation and then an oil and filter change, along with suction screen inspection and cleaning, every 50 hours of operation, or 4 months, whichever came first.[9] In addition, the filter was to be cut open and the filter element carefully inspected for metal contamination. Further, oil uplift was to be recorded to enable monitoring of oil consumption.[10]
A text message from the pilot to the operator on 19 June 2023 stated that the 25-hour oil change on PSC had been conducted. The pilot also commented that the filter looked ‘pretty clean’ and that they had bagged the element (filter) with the intent to provide it to the operator the next day. The MR had not been endorsed to show this inspection had been completed. Neither the operator, or the maintainer, could locate the filter element to verify whether the maintenance had taken place. Text messages to the operator, which aligned with the pilot’s diary, indicated the helicopter may have accumulated an additional 25 hours following the first oil and filter change, prior to 27 June 2023. However, there were no records indicating the 50-hour oil and filter change had become due, nor if it was completed.
Weight and balance
There were no records to indicate fuel quantity onboard PSC following the refuel. The ATSB calculated the helicopter weight for ‘full fuel’ and for the quantity of fuel drained from PSC at the accident site. Both calculations determined that the helicopter was being operated within the approved weight and balance envelope.
Meteorological information
Witnesses in the area and the pilot of RCS reported that the weather conditions at the time of the accident consisted of overcast[11] cloud well above their operating height with no precipitation, a temperature of about 20–25 °C, and a slight breeze.
The weather station at Limbunya recorded precipitation only. The nearest Bureau of Meteorology station was located at Victoria River Downs, about 144 km to the north-east. At about the time of the accident, the temperature recorded was 27 °C and the dewpoint[12] was 15 °C. The wind was about 5 kt, variable between north and east-north-east. The graphical area forecast showed the accident site shared similar conditions with Victoria River Downs. The forecast grid point temperature was 2 °C lower. The actual temperature and dew point data was not available for the accident site.
According to the Civil Aviation Safety Authority Carburettor icing probabilitychart, the temperature and dewpoint at Victoria River Downs were on the edge of the ‘serious icing – descent power’ and ‘moderate icing – cruise power’ envelopes. Carburettor ice is formed when the normal process of vaporising fuel in a carburettor cools the carburettor throat so much that ice forms from the moisture in the airflow, which can restrict airflow to the engine. This is more likely to occur at low engine power settings, and may result in reduced power output, rough running and in some cases engine failure. The pilot of RCS advised the ATSB that their assessment of the local conditions was they were not conducive to carburettor icing. Therefore, they did not use carburettor heat and did not encounter any adverse effects to engine operation.
Recorded information
Flight data
The helicopter was not fitted with a flight data recorder or cockpit voice recorder, nor was it required to be. In addition, the operator did not utilise electronic tracking of the helicopter.
The ATSB obtained flight tracking data from the OzRunways application installed on the pilot’s mobile phone. The application was using the mobile telephone network to transmit data to the OzRunways[13] servers every 5 seconds, which included the current position, track, groundspeed and truncated altitude in increments of 100 ft.
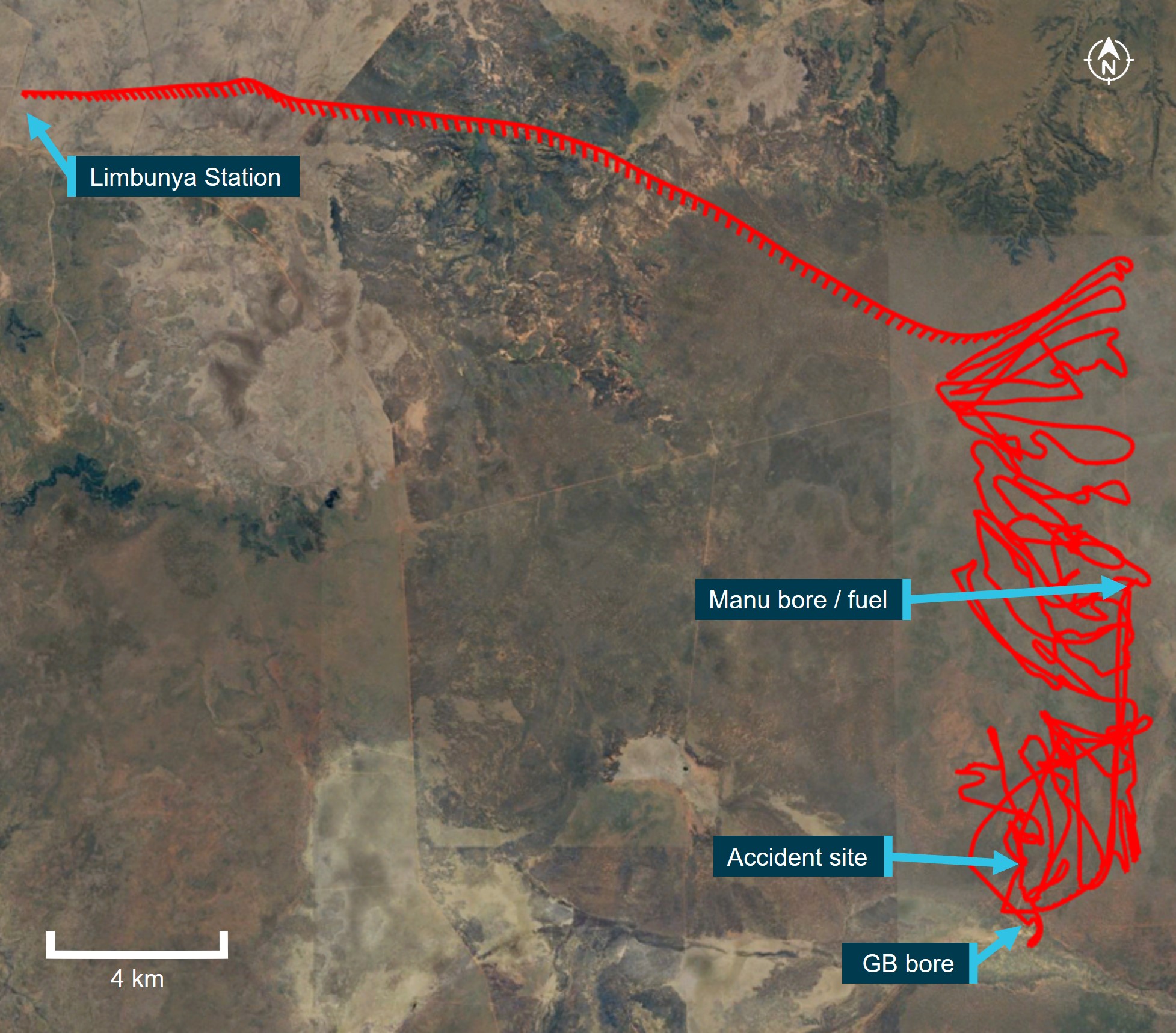
The recorded data showed PSC being operated in a manner consistent with the other pilot’s description of the mustering activities that day. Following the departure from the station homestead, the helicopter was flown direct to the northern end of the paddock and then systematically flown back and forth within the operational area, while gradually heading south to the designated holding area (Figure 4).
The flight profile data showed PSC was operated generally about 300 ft (100 m) above the ground, with extremities between 80 and 800 ft above terrain. Following the refuel, the data showed the helicopter being operated slightly higher than before the refuel. However, this was consistent with the bulk of the cattle having been mustered and the requirement to go to a higher altitude to identify isolated cattle through the timber. The final data points showed a descent of about 750 ft (230 m), followed by about 30 seconds of relatively level flight between 180–345 ft (55–105 m), before the data ceased.
There were several periods of no data being recorded during the day, of between 5 and 10 minutes.[14] The tracking data stopped short of the accident site,[15] at 1011, which prevented analysis of the final stages of flight. It could not be determined if this lack of recorded data was consistent with earlier dropouts, or due to the collision with terrain interrupting normal function.
Figure 4: VH-PSC track data
Image source: OzRunways and Google Earth, annotated by the ATSB
Helicopter recording devices
RHC introduced cockpit video cameras and engine monitoring units/governor (EMU), which are standard on new R22, R44 and R66 helicopters. The forward-facing camera records video (encompassing a view through the windshield, pilot controls and the instrument panel), intercom audio, radio transmission and GPS data. The cameras are an optional retrofit to most in-service helicopters.
The EMU monitors engine speed, rotor speed, engine oil temperature, cylinder head temperature, manifold pressure, ambient pressure, and outside air temperature. If the EMU detects an engine or rotor parameter outside of operating limits, an exceedance record is created and the data is stored.
These recording devices could assist with occurrence investigations by allowing investigators to understand the circumstance/s that precede an accident, particularly when there are no survivors or witnesses. In turn, this aids the identification of important safety issues. VH-PSC was not equipped with a cockpit camera nor EMU, nor was it required.
Wreckage and impact information
Wreckage distribution
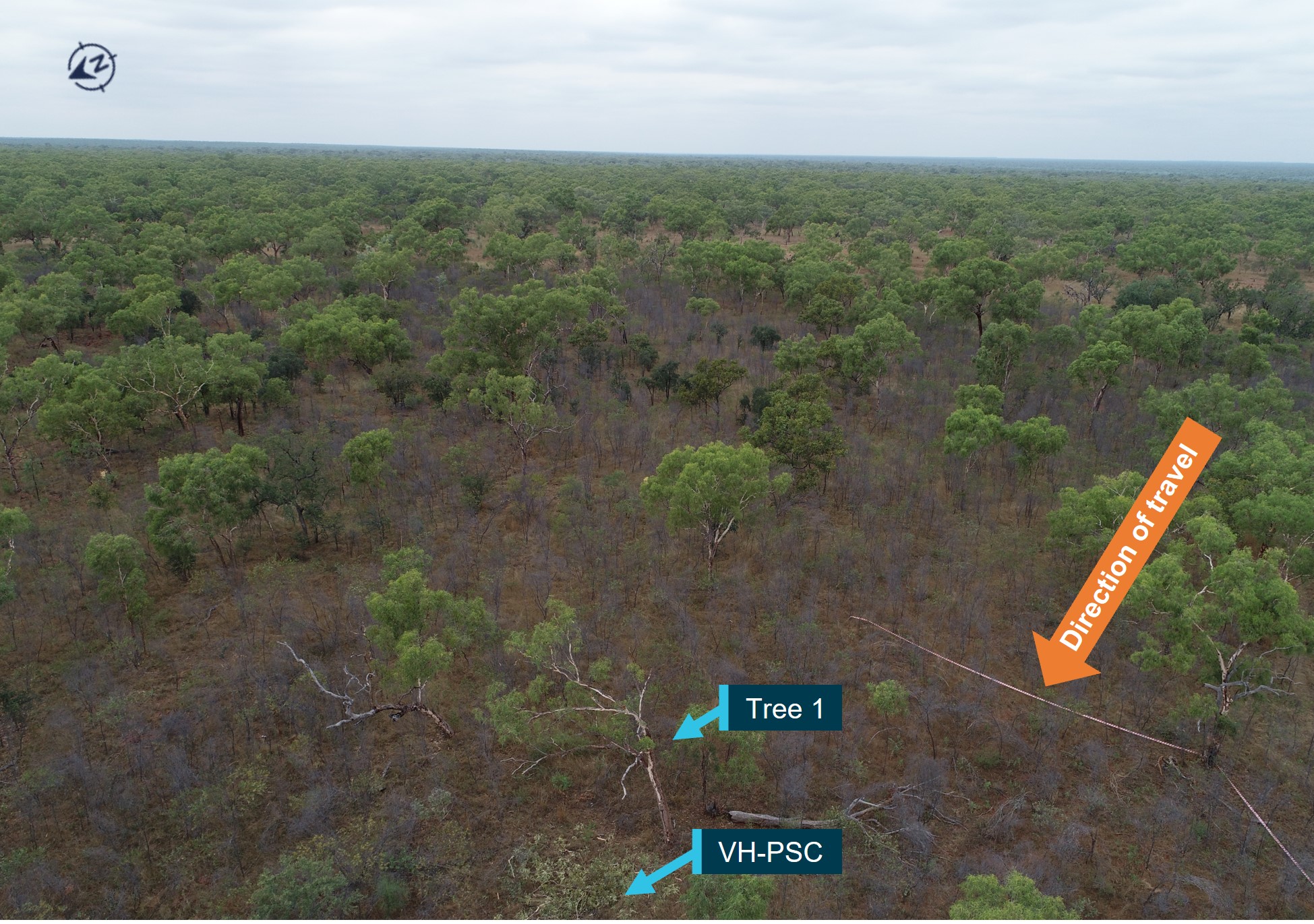
The accident site was located in an area that was flat and moderately wooded (Figure 5). There were no power lines or wires in the surrounding area. The helicopter collided with several branches of a tree (Tree 1) about mid height (5.7 m above the ground). The forward fuselage then impacted terrain in a nose-down, right side low attitude at the base of the second tree (Tree 2). The descent angle through the trees was calculated to be 45–48°. There was a short wreckage trail of about 18 m, on an approximate north-west heading. All helicopter parts were present at the accident site and there was no evidence of an in-flight break-up or a post-impact fire.
Figure 5: Site location, showing surrounding vegetation
Source: ATSB
The stabiliser assembly, with branch impact damage, was located just prior to Tree 2, the base of which exhibited impact damage and black paint transfer consistent with the landing gear. Pieces of windshield, the instrument panel and other forward fuselage components were located in the impact zone at the base of Tree 2. Fallen foliage was cleared from around Tree 2, and a distinct main rotor blade (MRB) ground scar was identified, with tip components embedded at the start. The fuselage came to rest, upright and to the right of a small tree, with the detached tailcone assembly nearby (Figure 6). The outboard section of the other MRB (MRB tip) had liberated during the tree strikes and was located about 40 m to the left of the debris trail. Rotary fuel hand pump components were located in the vicinity of the fuselage.
Figure 6: Site overview
Source: ATSB
Wreckage examination
Detailed examination of the wreckage identified continuity of the flight and engine controls, with all fractures consistent with overstress failure. However, distortion to the fuselage precluded determining engine control position prior to impact. There was nil evidence of birdstrike found in the wreckage or the surrounding area. The examination further identified the following.
Fuselage/cabin area
The collision with terrain compressed the cabin section, resulting in significant disruption of the cockpit area, the cabin structure, and the underfloor flight control mechanism. Police site images showed that the pilot was found to be wearing their seat belt at the time of the accident. Further, tearing of the seat belt webbing was very likely a result of the forces generated by the pilot restrained by the seat belt and being propelled in the direction of impact. The quick-disconnect dual flight controls[16] were not installed for left seat operation. The copilot’s seatbelt was found to be latched with the tongue locked in the buckle.
The mixture knob was in the ‘full-rich’ position with distortion to the fuselage preventing determination of the throttle selection. The throttle and mixture controls were securely connected to the carburettor, however, both linkages had failed in overstress. There was no evidence of a restriction or blockage to any part of the air induction system. Notably, the air intake hose was in good condition and the air box filter was clear.
Main rotor assembly
The main rotor blades had not contacted the cabin or tailcone and there was no evidence of extreme teeter or mast bump.[17] Both main rotor blades remained connected to the rotor head and exhibited rearward bending distortion. All hardware associated with the rotor head, blades and flight controls was secure and both pitch links were measured and found to be within service adjustment limits.[18] The pitch links were secured to the swashplate and main rotor pitch horns, with one pitch horn exhibiting distortion consistent with the main rotor blade ground strike. Overall, the damage to the main rotor blades and head assembly was indicative of low rotational energy at impact with the ground and simultaneous strike to the upper sections of Tree 2.
Landing gear
Vegetation debris on the upper surface of the left skid, forward of the strut, along with distortion to the forward strut was consistent with impact with the base of Tree 2. Fracture of the right skid and distortion to the right side of the landing gear was consistent with the nose and right-side low, impact with the ground.
Drivetrain
Both drive belts were intact, however, the rear belt had dislodged entirely from the upper sheave and the forward belt had jumped one groove forward (with one ‘v’ still engaged) during the accident sequence. There was no evidence of rubbing on either belt or sheave outer rim.[19]
The belt-tensioning clutch actuator extension was consistent with a properly functioning actuator and a relatively new belt set.[20] There was evidence of minor rotational scoring to the actuator body. The upper sheave rear face exhibited some minor surface corrosion of about a quarter to a third of the circumference, consistent with actuator body contact during the accident sequence.
Continuity of the drive train was established, except where the tail rotor drive shaft had fractured and there was tailcone separation. The main and tail gearboxes contained sufficient oil, could be rotated and the respective chip detectors were free of contamination. The freewheeling sprag clutch engaged/disengaged as expected.
Tailcone
The tailcone was securely mounted to the fuselage but had separated where the outer skin had fractured at the forward-most frame rivet line. Distortion to the tailcone just aft of the fractured rivet line was consistent with dynamic deflection occurring at fuselage impact with terrain. This corresponded to the upper left bolt, that secures the tailcone to the upper frame, being sheared. Momentum carried the tailcone forward and it came to rest in front of the fuselage, 180° opposite normal orientation.
The horizontal stabiliser and lower vertical fin exhibited damage consistent with tree branch impact and the mount to the tailcone had fractured in overstress. There was no damage or distortion to the upper vertical fin nor tail skid.[21] The tail rotor assembly was secured to the tailcone and both tail rotor blades exhibited low-energy tree strike damage. There was a small amount of dirt on the end of the tail rotor visual warning guard, consistent with coming into contact with the ground following tailcone separation from the fuselage.
Fuel system
The fuel system was selected to ‘ON’ and the bladder-type fuel tanks contained sufficient fuel for engine operation. The fuel supply from the tanks to the carburettor was intact and no signs of obstructions were noted. In addition, fuel quality was established through testing of fuel stocks at Manu bore and the homestead, and no contamination was found.
Carburettor
The carburettor heat knob was fully down (nil heat) and the heat assist was locked out (not functioning). The carburettor heat slider was in the HEAT selection, however, disruption to the airframe resulted in the control cable pulling the slider before the cable fractured in overstress.
Governor
The governor switch was oriented toward ON, however, impact damage and distortion meant the selection prior to impact could not be determined. The governor control unit was examined and tested by RHC, while being observed by a member of the United States National Transportation Safety Board (on behalf of the ATSB). The governor was within limits for all but one parameter, the ‘duty cycle’, which recorded an exceedance of 0.89%. RHC noted:
Duty cycle is the percentage of power sent to the motor to effect required throttle response. Under normal flight conditions this slight reduction in response speed would not be observable by the pilot.
Engine and fanwheel
The onsite examination identified the engine was intact and securely attached to its mount with all engine accessories securely attached. The engine sump casing had been perforated at impact, with a loss of oil contents.
Examination of the fanwheel identified the ring aft face was perforated between 2 vanes, with the edges of the break displaced aft, and curling of the edges. There was no paint transfer nor vegetation deposits, which may have identified if the damage was from a helicopter component, or tree branch. The dimension of the peeled skin was similar to the diameter of a rotary fuel pump standpipe section.
There was no circumferential scoring or damage to the other vane segments nor the aft face of the fan ring, as would be expected with a rotating fan. Damage to the fan shroud was consistent with ground impact with a stationary fan. Therefore, damage to the fan and shroud indicated that the engine was likely not operating at the time the damage to the fanwheel occurred.
Summary
Typical signatures of high energy (the engine driving the rotor) at the time of a collision with terrain include liberation and/or fragmentation of main rotor blades, fragmentation of the fanwheel and/or shroud, fracture of the main rotor pitch links and severe deformation of driveshaft flex couplings. However, in this instance, both main rotor blades remained connected to the rotor head and only exhibited rearward bending distortion. All hardware associated with the rotor head, blades and flight controls was secure. The pitch links were secured to the swashplate and main rotor pitch horns, with one pitch horn exhibiting distortion consistent with the main rotor blade ground strike. These, and other signatures, were indicative of a collision with terrain in a low rotor energy state (engine not driving the rotor system), where the energy diminishes with main rotor contact with the trees, followed by rotor sudden stoppage at ground strike.
Post onsite examination
The magneto switch was found selected to the BOTH position with the key in the barrel. The switch was examined and tested at the ATSB’s technical facility in Canberra, Australian Capital Territory. The results of the testing indicated that the ignition switch was fully functional and other than some external, physical damage attributed to impact forces, no internal defects that may have affected magneto selection operation were identified.
In January 2024, the engine was disassembled and examined at a CASA‑authorised engine overhaul facility under the supervision of the ATSB. The engine condition was consistent with the engine’s recorded time-in-service since overhaul. No internal or external damage was identified that may have prevented the engine from operating normally prior to the accident. No defects were identified in the induction system components, core engine, or cylinder assemblies that may have affected its pre-accident operation. Both magnetos were operationally tested and returned positive results and then internally examined and resistance tested with nil defects identified.
The carburettor was bench tested and internally examined, with no issues identified.
Medical and pathological information
Medical history
The pilot was known to be health conscious, fit, did not drink alcohol or smoke (cigarettes or vapes) and did not use recreational drugs. A review of the pilot’s medical records noted no medications were prescribed between 27 June 2021 and 27 June 2023.
Due to the pilot’s age, they were required to undergo an electrocardiogram (ECG),[22] and serum lipids (cholesterol) and blood glucose testing for each Class 1 medical certificate renewal. At the pilot’s most recent medical examination (November 2022) it was identified that their cholesterol level had increased. Due to the heightened cholesterol level, the pilot underwent an ECG, a treadmill stress echocardiogram,[23] and a computed tomography (CT) coronary angiogram. Following a review by a consultant cardiologist and the CASA‑designated aviation medical examiner, the pilot’s Class 1 medical certificate was renewed.
Post-mortem and toxicology
A post-mortem examination of the pilot was conducted by a qualified pathologist, on behalf of the Northern Territory Coroner. The pathologist’s report indicated that their examination was impeded due to the elapsed time between the accident and the recovery of the pilot’s body to a suitable mortuary facility. With consideration to these limitations, the report concluded that:
the pilot succumbed to multiple blunt force injuries sustained during the accident sequence
there was no evidence of any natural disease that have may resulted in death or impaired the pilot’s ability to control the aircraft.
Toxicological testing conducted as part of the pilot’s post-mortem examination identified concentrations of alcohol at 0.078% and carboxyhaemoglobin (COHb) at 11%.
The pathologist concluded that the alcohol concentration, while higher than that permitted to operate a vehicle in Australia, was ‘not relevant to death by means of interfering with mood, judgement or coordination’. In addition, the pathologist also noted that the sample location and post‑mortem changes likely affected the alcohol concentration in this instance.
The ATSB engaged an aviation medical specialist to review the pilot’s post-mortem and toxicology examinations (discussed below). Acknowledging the limitations reported by the pathologist due to decomposition, the ATSB’s aviation medical specialist also advised that some causes of death or incapacitation were not always able to be identified post-mortem.
Carboxyhaemoglobin
Carbon monoxide is an odourless, colourless and tasteless gas formed by the incomplete combustion of carbon-containing materials. When inhaled, it preferentially binds to haemoglobin, the oxygen carrying molecule in red blood cells. This creates COHb compounds and prevents oxygen from binding to the molecule and being transported, resulting in oxygen starvation.
ATSB investigation AO-2017-118 found that the physical symptoms of carbon monoxide exposure generally start to occur at COHb levels of around 10%. However, adverse neurobehavioural and cognitive effects can occur at lower levels. These symptoms and effects can include headaches, nausea, dizziness, confusion, and disorientation. These will become more severe with increasing COHb levels and duration.
The toxicology report noted:
Samples other than unpreserved peripheral blood may be unsuitable for accurate carboxyhaemoglobin determination. Results must be interpreted with caution in instances of aged or putrefied blood samples.
Correspondence with the pathologist and the ATSB’s aviation medical specialist determined that, given the time elapsed before sample collection, the sample location, and absence of an accurate determination of fluid versus blood ratio of the sample, resulted in uncertainty as to the accuracy of the COHb concentration level at the time of the accident.
A review of the ATSB aviation occurrence database identified about 60 carbon monoxide occurrences involving aeroplanes between 2010 and 2024. In contrast, only one occurrence was recorded for helicopters between 1991 and 2023:
In 2018, during take-off, the wind blew the exhaust fumes into the cockpit of an R44 resulting in the crew receiving a carbon monoxide warning. The crew returned the helicopter to the aerodrome.[24]
In addition, no accident reports (worldwide) were identified, which discussed elevated COHb levels involving R22 helicopters.
Based on the configuration of the helicopter, with the engine below and behind the cabin, it was considered unlikely for significant exhaust gases to enter the cabin, even with both doors removed.
Pilot injury assessment
According to Campman and Luzi (2007), identifying who was in control of the aircraft at the time of impact may provide valuable insight into the events leading up to the accident. The presence or absence of certain occupant injuries could assist with this determination. In particular, those relating to the upper and lower extremities from manipulating the flight controls and by the forces transmitted through the extremities at the time of impact.
Gradwell and Rainford (2016) stated that although ‘Unequivocal control-type injuries indicate that the pilot was conscious at the time of the crash’, they also highlighted that:
…caution must be exercised in their interpretation as they are neither particularly sensitive nor specific findings. Similar injuries may be seen in passengers if they grasp a solid structure at the time of impact, and if the pilot lets go of the controls in the instant before impact, then control-type injuries will not be seen.
The ATSB’s aviation medical specialist indicated that they would have expected more bone fractures if the pilot had been manipulating the controls at the time of impact. However, it was not possible to determine if the absence of typical control-related injuries identified on the pilot were suggestive of incapacitation prior to impact or rather, letting go of the flight controls during the accident sequence.
Operational information
Mustering operations
The operator’s staff described that the helicopters were typically operated ‘at height’ so that the helicopter ‘noise’ was used to move the cattle, rather than flying low and ‘upsetting’ the cattle. In this method, the helicopters were operated about 700–900 ft above the ground, which allowed the pilots to have a good overview of the area and see down through the timber to locate cattle. They would then gradually descend the helicopter, using the noise to get the cattle moving in the desired direction, before climbing to locate other cattle. The accident pilot was described as ‘careful’ and ‘calm’, when compared with some other pilots.
Quick descent
Where a quick descent is desired, the pilot will lower the collective while simultaneously rolling off throttle, to avoid main rotor overspeed. The descent will typically be steep and in a right turn, to allow the right-seated pilot to maintain forward airspeed and visual contact with their target. The throttle will then be rolled on prior to raising the collective to arrest the descent. This technique is similar to that when practicing an autorotation. The normal procedures section of the R22 POH Practice autorotation – power recovery includes the following caution:
To avoid inadvertent engine stoppage, do not chop throttle to simulate a power failure. Always roll throttle off smoothly. Recover immediately if engine is rough or engine RPM continues to drop.
Autorotation
The R22 POH detailed that a power failure may result from either an engine or drive system failure and will usually be indicated by the low rotor RPM horn. An engine failure may be indicated by a change in noise level, nose left yaw, an oil pressure light, or decreasing engine RPM. A drive system failure may be indicated by an unusual noise or vibration, nose right or left yaw, or decreasing rotor RPM while engine RPM is increasing.
The energy to successfully land (autorotation)[25] a helicopter in an engine off condition, such as an engine failure, comes from a combination of available potential and kinetic energy in the form of height, forward speed and rotor RPM. A pilot can utilise that energy to maintain drive to the main rotor and create lift.
The R22 POH explained the steps to take to enter an autorotation when between 8–500 ft.[26] The procedure stated to lower the collective immediately to maintain rotor RPM. While in a steady descent, adjust the collective to maintain rotor RPM between 97 and 110%. If time permitted, and when an engine restart is not possible, turn off unnecessary switches and close the fuel valve. Prior to landing from an autorotation, at about 40 ft above the ground, the pilot must flare the helicopter in order to reduce forward speed and increase rotor RPM before cushioning the landing.
The conditions from which a safe autorotation could be made were specified in the height-velocity diagram in the POH. A notation on the diagram encouraged pilots to avoid operation in the shaded area. When operating in this area, a pilot may be unable to complete an autorotation landing without damage. The unshaded region of the diagram shows the combinations of airspeed and height above the ground that allows a pilot to successfully complete a landing in a full autorotation without requiring exceptional skill. Recorded data showed that, over the course of the morning, PSC had been operated both in the shaded ‘avoid’ area, as well as in the non-shaded area.
Low rotor RPM and stall
The R22, with its low rotor system mass and relatively high RPM, is described as ‘low inertia’ helicopter. In low inertia systems, rotor RPM is gained and lost very easily. Low rotor RPM occurs when drag on the rotor system exceeds the power available to drive it. Without quick and effective intervention, the rotor RPM decays, it produces less lift, and the helicopter will start to descend. Airflow over the blade changes and the condition deteriorates until one or both of the main rotor blades stall.[27] According to RHC safety notice SN-24Low RPM rotor stall can be fatal, recovery fromrotor stall is ‘virtually impossible’.
Low-rotor RPM can occur at almost any time during power-on and power-off operations and is usually the result of improperly coordinating the collective and throttle, including overpitching or a failure to quickly lower the collective in an emergency such as engine failure or power reduction.
A primary cause of fatal accidents in light helicopters is failure to maintain rotor RPM. To avoid this, every pilot must have his reflexes conditioned so he will instantly add throttle and lower collective to maintain RPM in any emergency.
The low rotor RPM warning lamp and horn will activate when the rotor RPM reduces to 97% or below. The warning lamp is located on the top of the instrument panel and the horn can be heard in the cabin and through the headset. The POH stated that ‘catastrophic rotor stall could occur if the rotor RPM ever drops below 80% plus 1% per 1,000 ft of altitude’. Further, the United States Federal Aviation Administration Helicopter Flying Handbook stated that ‘low inertia rotor systems can become unrecoverable in 2 seconds or less if the RPM is not regained immediately’.
Partial power loss
As discussed in ATSB investigation AO-2022-009, RHC previously advised that a main rotor strike to the ground, a significant tree or structure, could stall (stop) an engine when operating at low power or idle, prior to an impact with the terrain.
Safety analysis
Introduction
On the morning of 27 June 2023, 2 Robinson Helicopter Company R22 helicopters were conducting mustering operations near Limbunya Station, Northern Territory, in conjunction with a ground team on horseback and motorcycles. When the pilot of the second helicopter (VH-RCS) had not heard from the pilot of VH-PSC for some time, they commenced a search and located the accident site after about 15–20 minutes. The helicopter was destroyed, and the pilot was fatally injured.
There were no witnesses and no recorded data to accurately determine the accident sequence, including the time of the accident.
This analysis will discuss the potential reasons for engine power reduction and loss of control. It also considers some aspects associated with the maintenance release.
Occurrence events
Engine power reduction
The wreckage signatures were consistent with the main rotor being in a low energy state. Given this, the ATSB considered how much engine power was being produced at the time of the accident.
Examination of components identified some minor scoring to the drive train belt-tensioning clutch actuator body, consistent with contact with the upper sheave. The corresponding location on the sheave exhibited some minor discolouration from actuator body material deposits that had begun to corrode. While scoring would normally indicate engine rotation at impact, in this instance, the sheave discolouration extended only a quarter to one third of the circumference. This limited scoring may be more representative of a low‑energy main rotor blade being forced backward to the direction of rotation at impact with the ground, rather than engine rotation. However, the non‑rotational damage to the fanwheel was consistent with the engine not operating at the time of impact.
The ATSB considered the potential reasons for the reduction in engine power, which can be broadly categorised as:
engine and associated systems defect
fuel contamination or starvation
carburettor ice
pilot-induced (intentional).
Examination of the engine and associated systems did not identify a fault or condition, which would have prevented normal operation. Nor was any issue found with the fuel quantity or quality. While an intermittent interruption to normal operation could not be completely discounted, there was no observable evidence to indicate this may have occurred.
The meteorological conditions at the nearest Bureau of Meteorology weather station,144 km away, were on the edge of the ‘serious icing – descent power’ and ‘moderate icing – cruise power’ envelopes for carburettor icing. However, the pilot of the other R22 operating in the accident area, reported that local conditions did not require the use of carburettor heat and they did not observe any indications of the formation of carburettor ice.
The ATSB considered the possibility that the pilot intentionally reduced the throttle as part of a quick descent. Inadvertent engine stoppage could occur from the throttle being reduced too quickly, which may have occurred at a height too low to perform a successful engine off landing (autorotation) to clear ground. In addition, the collision with terrain in a nose and right-side low orientation could also be indicative of a quick descent manoeuvre, from which recovery did not occur. Alternatively, as noted by the manufacturer, if the engine was in a low-power state when the main rotor blades impacted the tree and ground, it was possible that this impact stopped the engine.
Loss of control
The ATSB considered other loss of control events that may have preceded the nose and right-side down trajectory through a tree and then the subsequent collision with terrain.
There were no indications of a collision with a bird or other object, such as a wirestrike. Based on the witness observations, there was no evidence to suggest that the weather conditions affected the pilot’s ability to maintain control of the helicopter. As discussed above, there was no observable issue identified with the helicopter nor was there any indication of mast bumping. While it was possible that a loose object in the cabin interfered with the pilot’s flight controls, the disruption to the cabin area precluded identifying any evidence of this. Regardless, this scenario did not account for the low rotor energy (engine not driving the rotor system).
While distractions can occur unexpectedly, the other R22 was not operating in the immediate area to distract the pilot. The engine reduction (if not intentional) could have potentially been a distraction and required the pilot to conduct an autorotation. However, ATSB research has shown that distraction events most often result in an incident rather than accident (ATSB, 2006).
A reduction in engine power, whether operating at low or idle power, or in the event of a complete engine stoppage, requires prompt and effective management of main rotor RPM, above 97%, in order to conduct a successful autorotation.In this instance, the trajectory and orientation of the helicopter was not consistent with what would be expected if the helicopter was being flared, to reduce the rate of descent prior to touching down during a controlled autorotation.
Conclusions
The site and wreckage signatures were consistent with an engine power reduction and loss of control. Further, it could not be determined if the engine was producing low power, or was stopped, and if this was due to an engine issue (unobserved from the wreckage examination) or pilot induced. The pilot was highly experienced in low-level helicopter operations and demonstrated their capability to an instructor during simulated emergency procedures about 3 months prior. However, as there was no recorded data available or witnesses to the final stages of the flight, the pilot’s actions leading up to the accident were unknown.
Without conclusive reasons to explain the accident sequence, the ATSB also considered if it was possible that the pilot experienced some level of incapacitation before (resulting in inadvertent throttle manipulation), or after the reduction in engine power. Incapacitation could also explain the low rotor energy and/or helicopter trajectory into terrain. The absence of a radio transmission, in the event of an autorotation, could be suggestive of an incapacitation event, but could also indicate a sudden event that the pilot did not have time to transmit.
Despite this, a comprehensive review of the pilot’s medical history and general health did not identify any pre‑existing or other condition that could have adversely affected their performance. The post‑mortem did not identify the presence of any natural disease, however, the pathologist reported limitations due to decomposition, including the elevated carboxyhaemoglobin results. Further, analysis of the flight control injuries was inconclusive. Although the ATSB’s aviation medical specialist advised that some causes of death or incapacitation were not always able to be identified post-mortem, incapacitation remained only a possibility as there was insufficient evidence to conclude probability.
Therefore, due to the limited evidence available, the ATSB was unable to determine the reason for the engine power reduction and loss of control, nor the sequence of these events.
Maintenance release no longer in force
The current maintenance release, located at the accident site, had no endorsements showing daily inspections, hours flown each day, calculation of accumulated time-in-service or certification for completion of scheduled maintenance.
The pilot’s diary indicated they had operated VH-PSC every day since the maintenance release was issued (13 days prior to the accident). Text messages between the pilot and operator indicated that the required 25-hour engine oil and filter change had been completed, despite not being certified for on the maintenance release. Without a record of the accumulated total time‑in‑service, the ATSB could not determine if the 50-hour oil and filter change had come due, nor if it had been completed.
In this instance, as the pilot was the sole operator of the helicopter, the absence of endorsements did not hinder other pilots from being aware of the serviceability status. However, the maintenance release is a legal document that is part of the ongoing airworthiness requirements for the helicopter. The lack of certification for the completion of maintenance did not contribute to the accident, however, the helicopter was being operated with a maintenance release that had ceased to be in force and was therefore considered unairworthy.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving a Robinson R22 Beta II, VH-PSC, near Limbunya Station, Northern Territory, on 27 June 2023.
Contributing factors
While conducting mustering operations, for reasons that could not be determined, there was a reduction in engine power and a loss of control.
Other findings
While not contributory to the accident, the absence of endorsements for daily inspections and nil certification for the completion of scheduled maintenance resulted in VH-PSC being operated with a maintenance release that had ceased to be in force.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the other pilot and members of the ground muster team
the operator and maintainer
Civil Aviation Safety Authority
Northern Territory Office of the Coroner
Northern Territory Police
Western Australia Police
forensic and aviation pathology specialist
Robinson Helicopter Company
Airservices Australia
Bureau of Meteorology
OzRunways data from the pilot’s phone
next of kin and friends of the pilot.
References
Campman, S.C. & Luzi, S.A. (2007). The sensitivity and specificity of control surface injuries in aircraft accident fatalities. The American Journal of Forensic Medicine and Pathology, 28(2), 111‑115.
Gradwell, D. & Rainford, D.J. (Eds.). (2016). Ernsting’s Aviation and Space Medicine (5th ed). Boca Raton, FL: CRC Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
pilot of VH-RCS
the maintenance organisation that conducted the engine overhaul
Civil Aviation Safety Authority
United States National Transportation Safety Board
Robinson Helicopter Company
Bureau of Meteorology
the pathologist and medical subject matter expert.
Submissions were received from:
Robinson Helicopter Company
the operator.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]All times provided by the pilot of RCS and members of the ground muster team were estimated (give or take 10-15 minutes each side), however, were sufficiently consistent to develop the timeline of events.
[2]The hours noted in the diary were likely a combination of flight time and duty (or on ground) time.
[3]When installed, the cabin heat system uses air warmed by a shroud surrounding the muffler, which is then directed via ducting to the cabin.
[4]The freewheeling unit automatically disengages any time the engine revolutions per minute become less than rotor revolutions per minute, allowing the rotor system to rotate free of the engine drive system.
[5]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[6]When conditions were conducive to carburettor ice, the POH required the pilot to use carburettor heat as required to keep the needle on the carburettor air temperature gauge out of the yellow arc (-15 to 5 °C). In addition, carburettor heat was to be used with power settings below 18” mercury, regardless of the indicated carburettor air temperature.
[7]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[8]As the engine had been fitted to other aircraft, its overhaul cycle did not align with PSC.
[9]Service bulletin SB 480 also noted that ‘in special circumstances’ the oil and filter change ‘can be extended not more than 5 hours while en route to a place where the oil change can be done’.
[10]High oil consumption and/or a change in oil consumption can be indicative of a developing engine issue.
[11]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘overcast’ indicates that all the sky is covered.
[12]Dewpoint: the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to predict the probability of aircraft carburettor icing or the likelihood of fog.
[13]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[14]OzRunways distinguishes one flight from another by identifying that the aircraft is conducting a flight when it is above a threshold speed. Therefore, a ‘flight’ is considered to be when the aircraft is above the threshold speed to when it drops below the threshold speed. Data may not be recorded when the aircraft is below the speed threshold. PSC likely regularly dropped below the threshold speed, probably while at low altitude moving the stock. As such, the OzRunways system thought this was the end of a flight and did not record the data. Data acquisition recommenced when the helicopter was operated above the ‘flight’ thresholds.
[15]The ATSB examined the pilot’s mobile phone in case data had been collected but not yet transmitted, however, no additional information was available.
[16]Quick-disconnect flight controls do not require use of tooling to fit and remove and can therefore be accomplished by the pilot, without the requirement for a licenced aircraft maintenance engineer.
[17]Mast bumping: contact between the main rotor hub/spindle and the rotor mast which, if excessive, could severely damage the mast, or result in the separation of the main rotor system from the helicopter. Damage from mast bumping is indicative of excessive blade flapping and/or excessive tilt of the main rotor disc relative to the mast. As documented in many investigation reports worldwide, scenarios that have been linked to mast bumping include low-g and/or low rotor revolutions per minute/rotor stall, in conjunction with delayed and/or inappropriate flight control inputs.
[18]Main rotor pitch links can be lengthened (to decrease RPM) or shortened (to increase RPM) to obtain optimum autorotation rotor RPM.
[19]Rubbing from contact between a belt and the sheave can be an indication of engine providing power to the drivetrain, however, it is also possible that a dislodged belt may not make contact with the sheave under certain circumstances.
[20]A new drive belt set had been installed during the last periodic inspection.
[21]Tail skid: A guard device attached below the lower vertical fin to protect the tail rotor blades from ground strike.
[22]An ECG detects heart problems by measuring the electrical activity generated by the heart as it contracts. ECGs from healthy hearts have a characteristic shape. If the ECG shows a different shape it could suggest a heart problem.
[23]Stress echocardiogram (stress echo) is a test to assess heart function under physical stress. It uses ultrasound waves (inaudible sound waves) to image the heart and assess its function before and immediately after the exercise to see how the heart muscle pump is working, and sometimes to measure other parameters.
[24]Effects to the flight crew, if any, were not provided to the ATSB in the occurrence notification.
[25]Autorotation is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[26]For power failure below 8 ft, the pilot was to apply right tail rotor pedal input as required to prevent yaw, allow the helicopter to settle and raise the collective just before touchdown to cushion landing.
[27]Rotor stall, similar to aerodynamic stall in aeroplanes, occurs when increasing rotor blade angle, relative to airflow (angle of attack), reaches a point where airflow separates from the rotor upper surface and becomes turbulent, reducing lift. As the helicopter descends, the upward flow of air further increases the angle of attack until the critical angle of stall in reached, resulting sudden loss of lift and a large increase in drag. The increased drag acts like a rotor brake causing the rotor RPM to rapidly decrease, further increasing the rotor stall.
Preliminary report
Report release date: 31/08/2023
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 26 of the Transport Safety Investigation Act 2003.
The occurrence
On 27 June 2023, at about 0700 local time, the pilot of a Robinson Helicopter R22 Beta, registered VH‑PSC (PSC), departed Limbunya Station, Northern Territory, in company with a second R22 registered VH‑RCS (RCS). Their task was to muster stock in a small paddock to the north of GB bore, about 29 km to the south-east of the station homestead. In addition, they were to assist the ground mustering party to move stock that had been mustered from ‘No. 22’ paddock into the GB bore holding yards the previous day, to the ‘No. 18’ yards (Figure 1).
The helicopters arrived at the northern end of the paddock at about 0730 and began pushing cattle south towards the GB bore holding yards. The pilot of PSC then supported the ground mustering party in moving stock from the yards into a fenced laneway. The laneway would guide the stock to the No. 18 holding yards, that were located about 8 km to the south‑west.
Figure 1: Limbunya Station and operational area
Source: Google Earth, annotated by the ATSB
At about 0915, when the cattle were moving along the laneway under the control of the ground mustering party, the pilot of PSC was released from that task, and returned to assist the pilot of RSC with completing the mustering task.
At about 0930, the pilot of RCS diverted to Manu bore to refuel the helicopter from drum stock. Following refuelling, the pilot departed back to the small paddock, and at about 0945 acknowledged a departure call from the pilot of PSC who had also completed refuelling at Manu bore.
At about 1000, the pilot of RCS contacted the head musterer via radio to enquire if they had been in contact with the pilot of PSC. The head musterer advised that no contact had occurred since the time PSC had been released. Having received no replies from PSC to their radio calls, the pilot of RCS commenced searching the area around Manu bore, and gradually progressed the search towards GB bore.
At about 1015, the pilot of RCS located the wreckage of PSC. The helicopter was destroyed, and the pilot had sustained fatal injuries.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) with the required ratings and endorsements to operate the accident helicopter, and a valid Class 1 Aviation Medical Certificate. The pilot had about 14,000 flying hours on helicopters, including over 3,000 hours on the R22 type. The pilot also held a Commercial Pilot Licence (Aeroplane), with about 2,500 hours logged.
Aircraft information
VH-PSC was a Robinson Helicopter Company R22 Beta helicopter, serial number 4429. It was manufactured in the United States in December 2008 and first registered in Australia in January 2009. The helicopter was fitted with a 4-cylinder Lycoming engine, model O‑360-J2A, serial number L-40927-36C-C-A. On 15 June 2023, the aircraft underwent a 100-hourly/annual inspection, during which the engine was replaced with a newly overhauled unit. A new maintenance release was issued at this time, which stated that the aircraft had accrued 6,300.2 hours total time-in-service.
Meteorological information
Witnesses in the area reported that the weather conditions at the time of the accident consisted of overcast[1] skies with no precipitation, a temperature of about 20-25 °C, and a slight breeze.
Site and wreckage information
The accident site was located in an area that was flat and moderately wooded. The helicopter collided with terrain on an approximate north-west heading. There was a short wreckage trail of about 18 m, with all helicopter parts present at the accident site and no evidence of an in-flight break-up or a post-impact fire.
One main rotor blade tip was liberated in the collision and was found about 40 m to the left of the helicopter. Examination of the flight controls and helicopter structure did not identify any pre‑existing defects. The site examination found that both fuel tanks remained intact and contained fuel. In addition, fuel quality was established through testing of fuel stocks at Manu bore and the homestead.
Recorded information
The helicopter was not fitted with a tracking unit, flight data recorder or cockpit voice recorder, nor was it required to be.
Further investigation
To date, the ATSB has examined the accident site and wreckage, collected meteorological data from the Bureau of Meteorology, collected pilot and aircraft related records, conducted interviews, and liaised with the Northern Territory Police Force.
The investigation is continuing and will include further review and analysis of:
electronic data from the pilot’s mobile phone
meteorological data
wreckage information
instruments and components collected from the accident site
aircraft maintenance history
similar occurrences.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Acknowledgements
The ATSB acknowledges the assistance provided by the Northern Territory Police Force, the management and staff at Limbunya Station, and the operator.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘overcast’ indicates that all the sky is covered.
An ATSB safety study investigation’s findings contain important lessons for safety assurance in airport planning and safeguarding. It reviews the interpretation and application of Australian and international aerodrome standards, which affect how high and how close buildings can be placed to a runway.
The investigation examined historical uncertainty around the application of the aerodrome standards, and resolution by the Essendon Fields Airport operator of ‘grandfathering’, with the acceptance of the Civil Aviation Safety Authority (CASA), to aerodrome standards from the 1970s. Those standards had been used to determine the width of the runway strip (the rectangular surface area surrounding the paved runway) for the east-west runway 08/26. This action also determined the location of the obstacle limitation surfaces (OLS) along the side of the runway strip. The planning and approval process for the Bulla Road (DFO) retail precinct at the airport in the early 2000s was considered in the context of that historical uncertainty.
“This complex investigation made nine findings pertaining to the acceptance of grandfathering in non-standard circumstances, review of safety cases, limited guidance for some safety standards, and assurance processes between federal agencies for airport planning relating to the Bulla Road Precinct,” said ATSB Chief Commissioner Angus Mitchell.
“We note that both CASA and the airport operator have maintained that there is an acceptable level of safety with the current status of the runway strip, obstacle limitation surfaces, and publication of information to pilots. It was not the role of the ATSB to do a separate risk assessment, but we have noted the type of risk information that should be taken into account by aerodrome operators and regulators.”
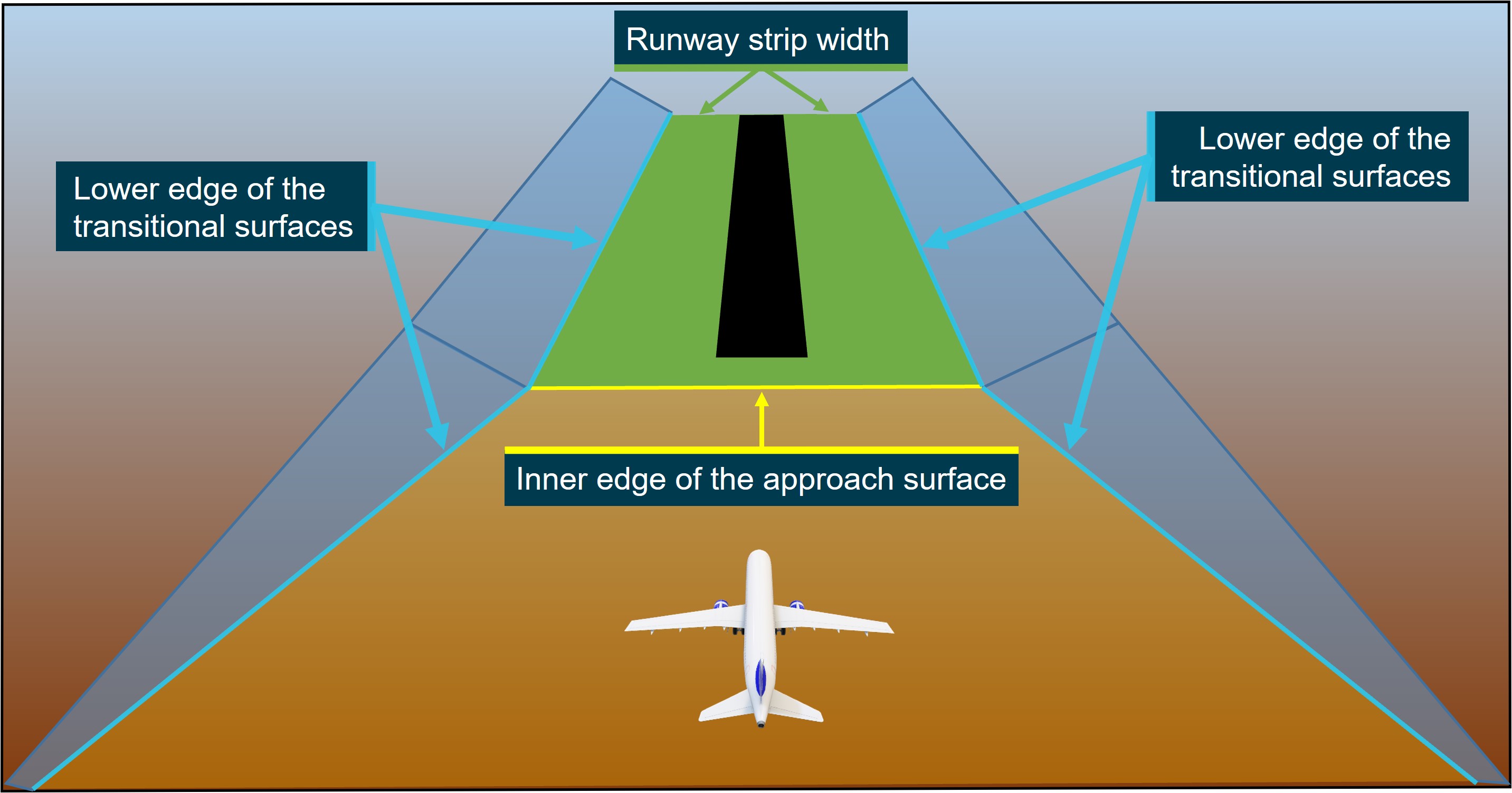
Mr Mitchell explained that the OLS are imaginary surfaces that provide a protective buffer against obstacles, such as buildings, for aircraft in the final stages of the approach to land. Any obstacles that encroach the OLS are subject to a referral to the aviation regulator for risk assessment.
From 1971, when Essendon ceased operating as an international airport, the runway 08/26 strip width was changed from 300 metres to 180 metres. The OLS around it changed with this dimension as well. The strip width was consistently published as 180 metres. However, in 2015, CASA issued an instrument to approve obstacles and require the strip width be published as 300 metres when the standards for the 180 metre strip width were not identified. The effect was that the northern portions of the retail centre buildings (which were built in 2005) infringed the runway strip and OLS down the side of the runway strip. They were notified to pilots as obstacles.
Mr Mitchell explained that the ATSB’s investigation commenced in 2018 after questions arose in another investigation as to how the buildings came to infringe the OLS. In 2019, when standards from the 1970s were identified and grandfathering occurred with the publication of a 180 metre runway strip width, the retail centre no longer infringed the runway strip or OLS.
Mr Mitchell said that the investigation had been through extensive review processes with directly involved parties, and was rescoped when grandfathering provisions were applied during the course of the investigation. Further, there were challenges with the limited information available from historical periods stretching back to the 1970s to provide context to the investigation and the need to address varying interpretations of the standards.
Separately, but in parallel to this investigation, an International Civil Aviation Organization (ICAO) taskforce has been reviewing the international standards (from which the Australian standards are derived) for the OLS. Changes have been proposed with consideration of the need to provide greater clarity on the application of the surfaces, and to reflect that modern aircraft and navigation systems have enabled reduced deviations from the intended flight path. Contracting States like Australia are considering the proposed changes.
“This investigation highlights the complex nature of airport planning and aerodrome safeguarding with the many factors that need to be considered to ensure an acceptable level of safety,” Mr Mitchell concluded.
“Aerodrome planning and aerodrome safeguarding can be further complicated when applying aerodrome standards with changing design criteria over a long historical period, as was the case at Essendon Fields Airport. It is even more challenging when there are incomplete records, limited guidance on how design criteria relate to risk, and changing interpretations of standards.”
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into the collision with terrain of a Robinson R22 helicopter during aerial mustering operations at Limbunya Station, about 500 km south of Darwin.
The ATSB is deploying investigators from its Canberra office, with experience in helicopter maintenance and engineering, to the accident site to begin the evidence collection phase of the investigation.
Over coming days investigators will examine the helicopter wreckage, survey and map the accident site with a drone, and collect any relevant components for further examination and analysis at the ATSB’s technical facilities in Canberra.
Investigators will also obtain and review any recorded data, weather information, witness reports, and aircraft operator procedures and maintenance records.
The ATSB anticipates publishing a preliminary report, which will detail factual information established during the investigation’s initial evidence collection phase, in approximately 6-8 weeks.
The ATSB will publish a final report, detailing contributing factors and any identified safety issues, at the conclusion of the investigation.
However, should any critical safety issues be identified at any stage during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.
A preliminary report has been released from an ongoing transport safety investigation into a fatal level crossing collision in South Geelong, Victoria.
The report details factual information gathered in the early evidence collection phase of the investigation, which is being conducted by the Chief Investigator, Transport Safety, who conducts rail investigations in Victoria under a collaboration agreement with the Australian Transport Safety Bureau.
The preliminary report, which contains no analysis or findings, notes that just prior to sunrise on 3 April 2023, a truck left a depot and travelled towards Barwon Terrace along an unsealed access road, which runs parallel to a railway track.
At the same time, a V/Line train with only a driver and conductor onboard was travelling along the track, in the direction of Waurn Ponds station, where it was to begin a passenger service.
As both vehicles approached the Barwon Terrace level crossing, the train driver observed the truck turning across the track ahead. In response, the driver sounded the train horn and made an emergency brake application, however, the train collided with the truck with the train travelling at about 65 km/h.
The truck was seriously damaged, and the driver was fatally injured. The train sustained minor damage, but stayed on the tracks, and the train driver and conductor were uninjured.
“Investigators attended to inspect the accident site, and have also examined operational information for the truck and train, interviewed several parties, and collected other relevant information,” Chief Investigator, Transport Safety Mark Smallwood said.
“As noted in today’s preliminary report, there was evidence of at least two routes from the unsealed road being used by road traffic to join Barwon Terrace.
“One of these routes, which was used by the truck in this collision, joins Barwon Terrace between the two boom barrier and flashing light assemblies to the north and south of the rail line.
“Our investigation is continuing, and will include review and examination of the operation of the level crossing, the operation of the vehicles involved, the layout of the unsealed road and access to the level crossing, and a review of the traffic management in place prior to, and at the time of the accident,” Mr Smallwood said.
A final report will be released at the conclusion of the investigation.
“However, should a critical safety issue be identified during the investigation, relevant parties will be immediately notified so timely safety action can be taken.”
A large bird struck the right Perspex windshield of an Air Tractor aircraft while conducting agricultural spraying near Chinchilla, Queensland, an Australian Transport Safety Bureau investigation has concluded.
On 19 September 2022, the pilot of the Air Tractor AT-502B was fatally injured after the aircraft was struck by a large bird while flying about 8 ft above ground level.
ATSB examination of the accident site indicated the aircraft flew a further 310 m, or about five seconds after the birdstrike, before colliding with the ground.
At the request of the ATSB, the Australian Centre for Wildlife Genomics at the Australian Museum analysed biological specimens of the bird from the aircraft and accident site, identifying the species as an Ardeotis australis, commonly known as an Australian bustard or Plains turkey.
The Australian bustard is Australia’s heaviest flying bird, with an average adult weight of 4.5 kg, and males weighing up to 8 kg. They are capable of flying but are mostly ground dwelling.
Prior to 2022, there were no fatal accidents in Australia on record involving civil aircraft, where a birdstrike was confirmed as a contributing factor.
“While the vast majority of birdstrikes result in nil-to-minor damage to the aircraft, and nil-to-minor injuries to occupants, these two accidents highlight the ongoing hazard birdstrikes represent,” Ms Hughes said.
“This second accident in particular highlights the ongoing hazards presented during low-level spraying operations.”
The ATSB’s final report notes recommended practices published by the Australian Aviation Wildlife Hazard Group on managing the risk of wildlife strikes.
“Practices include considering the likelihood of a wildlife strike and proximity of known wildlife characteristics such as their agility, speed, manoeuvrability, and their ability to avoid aircraft, as well as considerations such as the consequence of a potential strike,” Ms Hughes said.
The Bendix/King KAP 140 autopilot fitted in the Cessna 172R on this flight was a single-axis system. The single-axis system requires the ‘AP’ button to be depressed for 0.25 seconds to engage, and defaults to ‘ROL’ (roll) mode. The aircraft is not fitted with a wing’s leveller function and therefore, when the autopilot is engaged in roll mode, it will attempt to maintain the current position from the turn and balance co-ordinator instrument. The autopilot will not automatically disengage when the controls are manually manipulated by the pilot.
Position of autopilot
It is common practice for pilots to place a finger on the dashboard to support and assist with small changes to the throttle position as shown in Figure 1. The placement of the autopilot system made it very easy to engage by accident.
As a result of this incident the operator has implemented aircraft differences training to ensure students have knowledge over all aircraft systems and varying avionics. This training includes troubleshooting techniques specific to autopilots.
Furthermore, the operator has added an ‘In-flight controllability issues’ checklist to assist pilots during solo flight exercises.
Safety message
When acting as pilot in command, the pilot should be familiar with all the systems of the aircraft. An understanding of the autopilot system can be a useful tool for inexperienced pilots in many situations including inadvertent activation. The autopilot can also assist competently trained pilots that inadvertently enter instrument meteorological conditions (IMC) when flying under the visual flight rules (VFR). The in-flight emergency response checklist ATC IFER checklist used by Air Services Australia suggests activation of the autopilot for VFR pilots that enter IMC where the aircraft is equipped, and the pilot has been trained to use it appropriately.
This incident has many similarities to a previous investigation conducted by the ATSB, Collision with terrain involving Cessna 172, VH-ZEW, near Millbrook, Victoria on 8 September 2015 | ATSB (AO-2015-105).
The aircraft’s pilot operating handbook can also be a valuable source of information to assist pilots in understanding or recalling vital information when required.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2023-001
Occurrence date
14/03/2023
Location
Stanthorpe
State
Queensland
Occurrence class
Serious Incident
Aviation occurrence category
Loss of control
Highest injury level
None
Brief release date
26/06/2023
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
Cessna 172R
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
On the afternoon of 8 June 2023, a Regional Express Saab 340, registered VH-TRX, departed Sydney, New South Wales for an air transport flight to Merimbula, New South Wales with 3 crewmembers and 22 passengers on board.
At about 1507, the crew commenced descent into Merimbula. As icing conditions were expected during the descent, the first officer (pilot monitoring) selected the engine and wing anti-ice ON. This also activated the ice speed system, which reduced the stall warning angle of attack activation angle.
At about 1514, the crew commenced a visual approach to runway 21 at Merimbula and selected flaps to 20 degrees for the landing. During the approach in turbulent conditions, the airspeed reduced and the stall warning activated.
The captain then re‑established the required approach flight path and speed, continued the approach and the aircraft landed without further incident. The aircraft was not damaged and there were no injuries during the incident.
What the ATSB found
The ATSB found that during an approach, in turbulent conditions, the captain reduced engine power to flight idle to avoid an inadvertent flap overspeed. Due to the autopilot mode active at the time, the reduced thrust resulted in a continuous reduction in airspeed that required pilot intervention to prevent activation of the stall warning system.
Due possibly to distraction associated with the windscreen wiper setting, the airspeed continued to reduce undetected by the crew until the stall warning activated at a higher than normal margin above the stall speed.
Safety message
The approach and landing phases of a flight can have substantially increased workload when compared to other phases. Effective monitoring of aircraft and approach parameters, including performance associated with autopilot modes, and management of any distractions during these phases is essential to ensuring that an approach is safely completed.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At 1432 on 8 June 2023, a Regional Express Saab 340, registered VH-TRX (Figure 1), departed Sydney, New South Wales for an air transport flight to Merimbula, New South Wales with 3 crewmembers and 22 passengers on board.[1] The captain was acting as pilot flying, and the first officer as pilot monitoring.[2]
Figure 1: VH-TRX
Source: Ryan Hothersall
At 1507, the crew descended the aircraft from the cruising level of flight level 180.[3] As icing conditions were expected during the descent, the first officer selected the engine and wing anti-ice ON. This also activated the ice speed system, which reduced the stall warning angle of attack[4] activation angle and required the addition of 10 kt to the 116 kt landing reference airspeed[5] (see the section titled Approach speeds).
The crew elected to conduct a visual approach to runway 21 at Merimbula while using the required navigation performance instrument approach for lateral tracking to a 16 NM straight-in final approach leg.
During the approach, at 1517 with the autopilot engaged in the vertical speed mode,[6] the first officer selected flaps to 20° for the landing. At 1518:45, as the aircraft descended below 1,164 ft above mean sea level in turbulent conditions and at a speed of 143 kt, the captain reduced power to flight idle to prevent an inadvertent exceedance of the 165 kt maximum flap speed. A few seconds later, at 1518:54, speed reduced below 136 kt, the minimum speed for that segment of the approach (see the section titled Approach speeds).
The power remained at flight idle, and speed continued to reduce as the approach continued (Figure 2) with the engine anti-ice and ice speed systems selected on. The aircraft then entered a rain shower, and the captain asked the first officer to turn on the windscreen wipers. The first officer asked if they should be set to low or high and the captain asked for the high setting. The wiper activation was then delayed as the turbulence prevented the first officer from quickly making the required selection. At about the same time, with power still at flight idle, the aircraft encountered increased turbulence and at 1519:21, at a speed of 109 kt, the stall warning activated.
Figure 2: Approach flight path
Source: Google earth, annotated by ATSB
The captain responded to the stall warning by reducing the aircraft’s pitch attitude and increasing engine power and 4 seconds after the stall warning activated, speed increased above 116 kt. At 1519:29, speed increased above 126 kt and 5 seconds later increased above the minimum segment speed of 136 kt. The aircraft also descended below the desired approach path. The captain identified the low approach profile and reduced the descent rate to re‑establish the desired path.
The first officer then called for a missed approach to be conducted. The captain acknowledged the first officer’s call but elected to continue the approach because:
the approach profile had been quickly re‑established
the runway and visual approach guidance system[7] was in sight
they assessed that a missed approach would take the aircraft ‘back up into the weather’.
At 1519:55, the aircraft descended below 300 ft above aerodrome level (AAL), the stabilised approach check height for the visual approach. At that time, the approach was stable and remained so until the aircraft landed at 1520:36. The aircraft was not damaged and there were no injuries during the incident.
Context
Crew details
The captain held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The captain had over 20,000 hours of flying experience, of which over 13,000 hours were on the Saab 340.
The first officer held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer had 1,419 hours of flying experience, of which 172 hours were on the Saab 340.
The ATSB found no indicators that the flight crewmembers were experiencing a level of fatigue known to affect performance.
Stall warning system
The stall warning and identification system fitted to the Saab 340B included:
2 independent stall warning computers
2 angle of attack (AOA) sensors – one mounted on each side of the fuselage
an aural alerting system
a stick shaker device on each control column that provided a physical warning of an impending aerodynamic stall in the form of vibrations and an aural clacker sound when activated
a stick pusher device that applied forward force to the control column to reduce aircraft AOA when a stall condition was identified
a visual alerting system.
The aural alert system and stick shaker devices normally activated at 12.5° AOA while the visual alert and stick pusher activated at 19° AOA.
Operations in icing conditions
Airframe icing occurs when water droplets (cloud or liquid precipitation) at temperatures below their freezing point (supercooled) freeze on impact with aircraft surfaces. Icing conditions are only present in temperatures between 0°C and -40°C, with the highest risk of icing occurring between 0°C and -15°C. An accumulation of ice on an aircraft increases both drag and weight, reduces thrust and reduces the stall angle of attack (increases the aerodynamic stall speed). This results in smaller stall margins than for a clean (free of ice) aircraft.
The stall warning activation occurred 7 minutes after the aircraft descended out of icing conditions and, at that time, both flight crewmembers noted that the aircraft was free of ice.
Ice speed system
The ice speed system fitted to VH-TRX compensated for possible ice accumulation by lowering the stall warning stick shaker/aural alert activation AOA by about 6°. The visual alert and stick pusher activation AOA remained unchanged.
The system was activated by selecting either (or both) engine anti-ice systems on and was indicated by the illumination of a blue ICE SPEED push button on the instrument panel (Figure 3). Once activated, the ice speed system remained active even if the engine anti-ice system was subsequently selected off and needed to be deselected separately.
Figure 3: The flight deck of VH-TRX showing the ice speed system indicator
Source: Regional Express
The operator’s Flight Crew Operating Manual (FCOM) required that the ice speed system remain active for 5 minutes after leaving icing conditions or until the aircraft was free of ice, whichever occurred later. The manual also included the following caution:
Failing to increase reference speeds when the ice speed status light is illuminated reduces the margin to a stall warning indication. A stall warning may be triggered if the landing reference speed has not been corrected when the ice speed status light is illuminated.
Recovery from stall warning or stall
The FCOM for the SAAB 340 included the following procedure for recovery from a stall warning or stall:
The recommended procedure when recovering from a stall warning (stick shaker or natural buffeting) or stall in a clean or iced-up aircraft is to lower the nose approximately 5 degrees or as commanded by the stick pusher (if not restricted by proximity to ground), simultaneously apply Max power and if required roll the wings level.
This procedure also provided mandatory actions to be taken when a stall was identified:
In recovering from a low-level stall, or stall with gear or flap extended, apply standard go around procedures once a minimum of reference speed + 10 (+ 20 in icing) or stall/warning speed + 30kts is attained. Consider the possibility of a secondary stall.
Approach speeds
The base calculated reference speed for the approach was 116 kt. As the ice speed system was active, 10 kt was required to be added to the reference speed to provide the adjusted reference speed of 126 kt to be used by the crew for the landing.
For the final approach, until the 300 ft stabilisation check height, the crew was required to maintain a speed between 10 kt above the adjusted reference speed (136 kt) and 160 kt.
Meteorology
The approach was conducted in visual meteorological conditions and moderate turbulence.
At 1500, 19 minutes before the incident, the Bureau of Meteorology automatic weather station at Merimbula Airport recorded the temperature as 15° Celsius and the wind as 2 kt from 257° magnetic. Cloud cover was recorded as scattered[8] at 5,808 ft above mean sea level (AMSL), broken at 6,708 ft AMSL and overcast at 8,308 ft AMSL. Visibility was recorded as greater than 10 km in light rain.
Between 1511 and 1518, an increase in recorded wind gust speeds indicated a gust front passed over Merimbula Airport (5 km south of the incident location):
Table 1: Merimbula Airport recorded wind observations
Time
Wind direction
1 minute wind speed (kt)
1 minute wind gust (kt)
15:05
north-west
2.9
2.9
15:06
north-west
2.9
4.1
15:07
north-west
2.9
4.1
15:08
north-west
4.1
4.1
15:09
north-west
4.1
4.1
15:10
west-north-west
4.1
5.1
15:11
west-north-west
6.0
7.0
15:12
west
8.0
9.9
15:13
west
11.1
14.0
15:14
west
9.9
13.0
15:15
west
8.9
13.0
15:16
west
8.0
9.9
15:17
west
8.9
12.1
15:18
west-north-west
6.0
7.0
15:19
west-north-west
7.0
8.9
15:20
west-north-west
6.0
7.0
15:21
north-west
5.1
7.0
15:22
north-west
7.0
8.0
15:23
north-west
5.1
7.0
15:24
north-west
5.1
6.0
15:25
north-north-west
5.1
6.0
At 1530, 11 minutes after the incident, the temperature was recorded as 14° Celsius and the wind as 6 kt from 297° magnetic. Cloud cover was recorded as scattered at 3,308 ft AMSL, scattered at 5,608 ft AMSL and scattered at 7,008 ft AMSL. Visibility was recorded as greater than 10 km in light rain.
Recorded data
Analysis of flight data from VH-TRX’s flight data recorder showed that power was reduced to flight idle at 15:18:45, as the aircraft descended through 1,164 ft AMSL. Following the power reduction, the aircraft’s speed began reducing while the autopilot increased the aircraft pitch angle and wing AOA to maintain the selected descent rate. Nine seconds after the power reduction, speed reduced below 136 kt. A further 11 seconds later, speed reduced below 126 kt and 11 seconds after that, at 15:19:16, speed reduced below the base reference speed of 116 kt.
At 15:19:21, while descending though 636 ft AMSL and 34 seconds after power was reduced to flight idle, the speed slowed to 109 kt. The AOA increased to 5.9° and the stall warning activated for 1 second (Figure 4). At the same time the autopilot automatically disconnected.
Figure 4: Graphical representation of recorded flight data
Source: ATSB
Following the stall warning, the recorded angle of attack reduced by 5.6° within 2 seconds and power increased to about 50% torque within 4 seconds. At 15:19:35, 14 seconds after the stall warning, the speed increased above 136 kt and power began to be reduced to the normal approach power setting. The recorded data showed the descent rate reduced from the 830 ft per minute rate, recorded before the stall warning activation (with autopilot engaged), to about 450 ft per minute.
Audio data from the cockpit voice recorder was not available.
Decision to continue the approach
Following the stall warning activation, the first officer called for a missed approach to be conducted. The captain acknowledged the first officer’s call but elected to continue the approach.
The stall warning occurred when the aircraft was free of ice and at a height of 628 ft above the aerodrome elevation,[9] 328 ft above the stabilised approach check height of 300 ft AAL. The lowest speed recorded was 109 kt (27 kt below the minimum required speed), 21 kt above the calculated stall speed of 88 kt. Following the stall warning, the captain, acting as pilot flying, added sufficient power to increase speed above the minimum required for that phase of the approach.
The aircraft also descended below the required approach path. The captain recognised that the aircraft was low and commenced correcting it. As the aircraft descended below 300 ft AAL, it remained slightly below profile until regaining the approach path shortly after.
The actions defined in the operator’s FCOM procedure for recovery from a stall warning (see the section titled Recovery from stall warning or stall) were recommended and not mandatory. At low level, a missed approach was only mandatory in the case of an identified stall. Therefore, the captain’s actions did not contravene the operator’s procedures. Additionally, the operator’s procedures provided a mechanism for the first officer to escalate the situation if they disagreed with the captain’s decision to continue the approach.
The captain’s stated reason for the decision to continue was that the approach was restabilised, the runway and visual approach guidance system was visible, and a go-around would take the aircraft ‘back into the weather’. Therefore, the captain assessed that continuing the approach was the safest decision. The ATSB assessed that this decision was reasonable given the information available to the captain at the time and did not unduly increase risk to the flight.
Similar occurrences
In 2013, the ATSB research report Stall warnings in high capacity aircraft: The Australian context 2008 to 2012 identified that 245 stall warnings in high capacity aircraft had been reported between 2008 and 2012 in Australia. Almost all of those were low risk events of momentary duration and were responded to promptly and effectively by the flight crew to maintain control of the aircraft. However, there were also several higher risk incidents where stick shaker activation occurred on approach to land when aircraft were in a low speed, high AOA configuration. In these cases, the risk of a stall developing was increased by a lack of awareness of decreasing airspeed and increasing AOA prior to the stall warning, probably due to increased flight crew workload during this phase of flight. None of the reported occurrences resulted in an actual stall.
Safety analysis
During the descent and prior to the approach, the aircraft descended through icing conditions and the crew activated the engine anti-ice system. This also activated the ice speed system, which reduced the stall warning angle of attack activation angle. The approach was then commenced within 5 minutes of leaving icing conditions. Therefore, the ice speed system was still active as the approach commenced (as per the operator’s procedure). However, by the time of the occurrence the aircraft was operating in clear conditions and an ambient temperature well above freezing and there was no ice on the aircraft. This meant that the stick shaker/aural warning associated with an approaching stall was set to activate at an AOA of only 6° rather than the normal trigger AOA of 12.5°. That is, at a greater airspeed margin than normal above an actual (ice free) stall.
As the approach continued in turbulent conditions with the autopilot engaged, the captain, concerned that the turbulence may lead to an inadvertent exceedance of the flap limit speed, reduced power to flight idle and the aircraft speed started reducing. Due to the selected autopilot mode, the reduced thrust led to the aircraft pitch angle and wing angle of attack being automatically increased to maintain the selected descent rate. Significantly, this resulted in a further ongoing speed reduction that required pilot intervention to prevent activation of the stall warning system. While the power was selected to flight idle, the aircraft entered a rain shower and turbulence, likely associated with a gust front that was recorded passing over Merimbula Airport at about that time. At about that time, the captain asked the first officer to turn on the windscreen wipers followed by a brief discussion about the desired wiper setting.
The windscreen wiper setting discussion and subsequent minor delay in enacting the request possibly distracted the crew from effectively monitoring the airspeed and they did not identify that the speed had reduced significantly below the 136 kt minimum speed for that segment of the approach. This deceleration continued until the speed reduced to 109 kt and the stall warning system activated at the reduced ice speed system angle of attack.
The crew responded by recovering the aircraft, continuing the approach and landed the aircraft without further incident.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the stall warning activation involving a Saab 340, VH-TRX, 5 km north of Merimbula Airport, New South Wales on 8 June 2023.
Contributing factors
During an approach, in turbulent conditions, the captain reduced engine power to flight idle to avoid an inadvertent flap overspeed. Due to the autopilot mode active at the time, the reduced thrust resulted in a continuous deceleration that required pilot intervention to prevent activation of the stall warning system.
Due possibly to distraction associated with the windscreen wiper setting, the airspeed continued to reduce undetected by the crew until the stall warning activated at a higher‑than‑normal margin above the stall speed.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Regional Express
the flight crew
Bureau of Meteorology
recorded flight data from VH-TRX.
References
ATSB aviation research investigation report AR-2012-172, Stall warning in high capacity aircraft: The Australian context, Australia.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Regional Express
the flight crew
Civil Aviation Safety Authority.
Submissions were received from:
Regional Express
the captain.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The flight was operated under Civil Aviation Safety Regulations Part 121 (Air transport operations - larger aeroplanes).
[2]Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 180 equates to 18,000 ft.
[4]Angle of attack is the relative angle between the chord line of the wing and the approaching airflow.
[5]All further reference to ‘speed’ should be read as airspeed.
[6]In the vertical speed mode, the autopilot adjusted the pitch of the aircraft to maintain a selected vertical speed.
[7]Runway 21 at Merimbula was equipped with a precision approach path indicator (PAPI) lighting system.
[8]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[9]The threshold elevation of runway 21 at Merimbula was 8 ft.
Occurrence summary
Investigation number
AO-2023-030
Occurrence date
08/06/2023
Location
5 km north of Merimbula Airport
State
New South Wales
Report release date
14/08/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Stall warning
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340B
Registration
VH-TRX
Serial number
340B-287
Aircraft operator
Regional Express Pty Ltd (Rex)
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
Cargo ship was using newly planned route when it grounded on Harrington Shoal off Cape York;
Route had not been properly reviewed or approved, and planning tool contained waypoint data errors;
Duty operator monitoring vessel traffic in area was experiencing sustained elevated workload due to technical fault triggering abnormally high number of erroneous alarms and alerts.
The use of a draft voyage planning tool which included waypoint data errors plus an ongoing technical fault with the vessel monitoring and surveillance system for the Great Barrier Reef contributed to a cargo ship’s grounding on a shoal, an ATSB investigation details.
The 81-metre general cargo ship Trinity Bay grounded on Harrington Shoal, a charted feature with a depth of 0.9 metres north-west of Harrington Reef, on the morning of 19 January 2021 while conducting a regular weekly passage from Thursday Island to Cairns. Fortunately, the ship sustained only minor hull damage (some dents and paint stripping), with no injuries or pollution reported, and it was refloated on the rising tide.
The investigation report details that in an effort to address a deficiency identified during a recent internal audit, which required the use of approved routes and waypoints, the ship’s master had used a draft passage planning tool that was being trialled by the operator to plan new routes.
The planned routes from the planning tool were entered into the Trinity Bay’s electronic chart system (ECS), a navigation information system which displayed the vessel’s position and relevant nautical chart data. However, the ECS was not approved for use as the ship’s primary means of navigation and did not possess automatic route safety checking functions.
“Errors in the planning tool meant the new route took Trinity Bay dangerously close to the charted danger of Mid Rock, and then about an hour later directly over the charted danger of Harrington Shoal, where the ship grounded,” ATSB Director Transport Safety Stuart Macleod said.
“The investigation found the new passage plan was not independently verified by another of the ship’s deck watchkeeping officers, as required by the operator’s procedures, and the planned routes were entered into the electronic chart system instead of being annotated on the ship’s paper charts. In accordance with chart carriage regulations, these paper charts were the ship’s primary means of navigation, and were marked with the ship’s established previously-used routes.
“Consequently, the dangers on the newly planned route were not identified, and the monitoring of the ship’s passage was ineffective in identifying these dangers.”
The ship’s operator, Sea Swift, subsequently removed Trinity Bay’s electronic chart system from service and advised the ATSB that it was investigating the fitting of electronic chart display and information systems (ECDIS) on its ships. ECDIS is an approved navigational chart and information system that can be used in place of paper charts.
“This investigation highlights how the development and use of a detailed passage plan in accordance with the accepted principles of passage planning remains essential to safe navigation,” Mr Macleod said.
“Passage planning should be thoroughly appraised, with the route laid out and independently checked on the ship’s primary means of navigation, and then effectively monitored.”
Mr Macleod said the ATSB’s investigation also found that at the time of the grounding an ongoing technical fault in the REEFVTS (Great Barrier Reef and Torres Strait vessel traffic service) monitoring and surveillance system, meant the duty operator at the VTS Centre in Townsville was being presented with an abnormally high number of erroneous alerts and alarms. REEFVTS monitors and communicates with ships to ensure safe and efficient navigation in Torres Strait and the inner route of the Great Barrier Reef.
Among the genuine alarms received during that timeframe were warnings as Trinity Bay sailed close to Mid Rock, and again as it approached Harrington Shoal.
“Alerts associated with Trinity Bay were acknowledged by the duty operator but not followed up, due to the operator experiencing a sustained period of elevated workload, combined with a high level of expectancy that the ship was not at risk, as it frequently transited the area,” Mr Macleod said.
“Between the duty operator commencing their shift in Townsville at 0600, and when they were alerted by the ship’s master of the grounding at 0822, that operator received over 80 alerts from the REEFVTS monitoring and surveillance system, of which at least 42 were false, generated as a result of the system fault.”
Maritime Safety Queensland, which operates REEFVTS, has since implemented a software update for the system, reducing the incidence of false alarms.
Further, the reporting area covered by REEFVTS was split into two, a north and a south area operated respectively from Townsville and Gladstone, with a separate operator responsible for each area.
On 6 June 2023, the cabin crew of a QantasLink Boeing 717-200 aircraft, registered VH-NXM and operated by National Jet Systems, noticed a transient chlorine odour during the climb out of Sydney Airport, New South Wales. The cabin crew reported dizziness, mild discomfort described as pressure increasing in their head, and a metallic taste. The flight crew were advised, and the operator’s cabin air quality event procedure was completed.
About 76 minutes later, when the aircraft was on approach to Hobart Airport, Tasmania, the flight crew noticed a chlorine odour coming from the flight deck air-conditioning vents, lasting about 10 seconds. Shortly after, the captain noticed the onset of hypoxia-like symptoms and assessed themselves as unfit to continue as pilot flying.
The captain handed over pilot flying duties to the first officer and continued in the role of pilot monitoring for the remainder of the flight. The first officer, who was not experiencing any symptoms at that stage, continued the approach.
Shortly before landing, the first officer noticed that their reaction to an aircraft deviation was slowed and they started to experience cognitive difficulties. The landing was completed without further incident. After shutdown, both pilots reported a persistent headache, the captain also experienced ongoing symptoms of confusion and lethargy and attended a local hospital for medical tests.
What the ATSB found
The ATSB found that while the National Jet Systems’ cabin air quality events procedure captured the recording/reporting of odours, post-flight care of crew and maintenance actions, it did not consider the possible application of the smoke/fumes procedure or incapacitation procedure. As a result, there was an increased risk of flight crew being adversely affected by such an event during a critical stage of flight.
It was also identified that although National Jet Systems had procedures for recognition and management of pilot incapacitation, the associated training did not include the identification and response to subtle physical or cognitive incapacitation.
What has been done as a result
On 16 June 2023,National Jet Systems issued a Safety Action Notice (NJS-SAN-2023-018) reminding flight crews to consider supplemental oxygen use and the declaration of a PAN in response to a cabin air quality event.
On 2 March 2024, National Jet Systems advised the ATSB of the following safety actions taken as a result of this occurrence:
The flight crew recurrent simulator training syllabus had been updated to include in‑seat instruction specific to pilot incapacitation, followed by a practical exercise donning oxygen masks and conducting an approach, landing, and taxiing to the gate while using oxygen.
A review of smoke/fumes checklist and simulator training was undertaken.
Learnings from this occurrence have been incorporated into the newly‑introduced company A220 aircraft smoke/fumes, hypoxia, and incapacitation procedures.
A review of hypoxia training material to include specific reference to histotoxic hypoxia was undertaken, with draft content awaiting input from the Qantas chief medical officer.
Aircrew emergency procedures documentation and training pertaining to the recognition and management of crew incapacitation have been updated to include subtle and cognitive incapacitation.
Safety message
Airborne contaminants may result in the rapid onset of incapacitation, which although possibly subtle, can significantly affect the safety of flight. Physical or cognitive incapacitation can occur for many reasons and may be difficult for others, or even the sufferer of, to detect and respond to.
Flight crews should therefore be alert to the potential hazards posed by odours and fumes and not hesitate to use supplemental oxygen. The use of oxygen is a proven mitigating action in the case of environmental hazards and its rapid use ensures flight crews’ physical and mental capacity is maintained.
The occurrence
On 6 June 2023, a QantasLink Boeing 717-200 aircraft operated by National Jet Systems as QF1541 and registered VH-NXM, was conducting a scheduled passenger flight from Sydney, New South Wales to Hobart, Tasmania. On board were the captain as pilot flying (PF), first officer as pilot monitoring (PM),[1] 3 cabin crew and 54 passengers.
The aircraft departed Sydney at about 1943 local time and during the climb, the 2 cabin crew members at the front of the cabin detected a strong chlorine odour in the area of the forward galley, which was unnoticed by the flight crew. The cabin crew advised the flight crew of the odour, and once established in the cruise, the captain sought further information in accordance with company cabin air quality event procedure. The forward cabin crew reported dizziness, a feeling of pressure in the head, and a metallic taste, but that the odour had gone, and the symptoms were not increasing. The cabin crew member at the rear of the aircraft reported no odours or symptoms and stated that none of the passengers had complained of odours or appeared to be experiencing discomfort. The 2 affected cabin crew assessed themselves as fit to continue the flight. As a result, the captain elected to continue the flight to Hobart.
At about 2108, about 10 NM from Hobart Airport (Figure 1) and at an altitude of about 4,000 ft, the captain noticed a chlorine odour, which they assessed as coming from the flight deck air‑conditioning gasper vents. The first officer noticed the odour shortly after the captain but neither the captain nor first officer experienced any effects at this time. The captain and first officer reported that the odour was transient and disappeared after about 10 seconds.
About 30 seconds later, while the flight crew were configuring the aircraft for landing[2] on runway 30, the captain noticed quickly developing adverse effects on vision, mental capacity, and movement, and self-assessed as unable to safely fly the aircraft. The captain later described the symptoms as fogginess of thought, confusion, deteriorating situational awareness, weakness and tingling in the arms and legs, and narrowing of vision. The captain indicated their intention to transfer control of the aircraft to the first officer by stating ’your controls’. At that time the first officer noticed that the captain looked pale but did not appear incapacitated.
Figure 1: VH-NXM track showing approach to Hobart Airport and key events
Source: Google earth and Flight radar. Annotated by the ATSB
When about 8.5 NM from the runway at an altitude of about 3,250 ft, the first officer took over the role of PF. At the same time, the captain communicated that they were able to continue as PM with the assistance of the first officer. The first officer noted that the captain correctly actioned the commands to lower the flaps and landing gear to configure the aircraft for landing. The first officer was not experiencing negative symptoms at that stage and, as the odour was not detectable, assessed that emergency oxygen was not required.
Shortly after, the first officer noticed that the captain was struggling to read the checklist and was tripping over words, but managed to self-correct and read back air traffic control calls correctly. The first officer visually monitored the captain’s condition and ensured that no inadvertent contact was made with the flight controls.
At about 3 NM from the runway and an altitude of 1,000 ft, the first officer noted that the captain, as PM, had not made the required ‘stable’ call to confirm the aircraft was stabilised on the approach. The first officer prompted the captain with a call of ‘1,000 feet’, and the captain responded with ‘stable’. The first officer confirmed that the aircraft was stable and continued the approach. The first officer considered making a PAN[3] call, but assessed it was unnecessary due to the immediacy of landing.
At about 100 ft above the runway elevation, the first officer experienced difficulties keeping the aircraft lined up with the runway centreline. The first officer reported that the aircraft was drifting to the right of the centreline, and that their reactions to correct the drift were slower than normal. The first officer also reported feeling ‘hazy’, however these difficulties were not communicated to the captain at that time.
At about 2113, the aircraft landed at Hobart Airport and was taxied to a parking bay. The flight crew was assessed by a company medical doctor via teleconference, during which the doctor observed that the captain’s speech was noticeably affected, consistent with impairment. This resulted in the captain attending hospital for further testing.
The 2 forward cabin crew later reported the same smell on landing and again both felt similar mild symptoms. The first officer also reported a dull headache post‑flight, which lasted about 2 days.
Context
Personnel information
Flight crew information
The captain and first officer each held an air transport pilot (aeroplane) licence with a multi-engine command instrument rating and a class 1 aviation medical certificate.
At the time of the occurrence, the captain had accrued 10,670 flying hours with 5,780 of those on the Boeing 717-aircraft type. The first officer had accrued 6,984 flying hours, of which 1,614 were on the Boeing 717-aircraft type.
Post-flight medical tests
Several samples of the captain’s blood were analysed after the event to identify exposure to any toxins. The initial blood sample taken several hours after the aircraft landed found the carbon dioxide (CO2) level was slightly elevated and carbon monoxide (CO) was within the normal range. A second sample taken about an hour later showed that the levels of CO and CO2 had reduced.
Due to the time between the event and the first blood sample, and the low levels of CO and CO2 measured, the blood test results were considered to be inconclusive. The presence of an elevated CO2 level indicated the possibility of exposure to that gas, but the time, magnitude and source of the exposure could not be determined.
The first officer attended hospital the next morning for precautionary blood tests, the results showed no elevated levels of CO or CO2.
Aircraft information
Aircraft air-conditioning and pressurisation system
On Boeing 717 aircraft, pressurisation and temperature control is achieved by using bleed air from both engines. The hot, pressurised air is cooled by 2 independent pressurised air-conditioning kits (PACKs) and distributed to the flight deck and cabin. Cabin pressure is controlled by a single out‑flow valve, which is automatically modulated to open to decrease cabin air pressure and closed to increase cabin air pressure as required throughout the phases of a flight (Figure 2).
Figure 2: Simplified Boeing 717 normal air distribution
Source: Boeing. Modified and annotated by the ATSB
Typically, the left engine and left PACK are used to supply air to the flight deck and forward galley area, and the right engine and right PACK are used to supply the passenger cabin. Although, if required, either the left or right system can supply the air pressure and temperature control requirements of the entire aircraft.
The aircraft does not use recirculated cabin air, therefore air within the aircraft is completely replaced by the incoming air before being dumped overboard via the outflow valve. By controlling the flow of air through the outflow valve, the system regulates cabin air pressure throughout all phases of flight. In normal operation, pressurised air is sourced from the engine bleed air ducts, however for emergency operation, outside ram air can be selected to supply the PACKs which bypasses the engines and relies on aircraft forward movement to provide pressure.
Condensation is removed from the conditioned air by 2 independent water separators located at each PACK output manifold. Air entering the water separator is made to rotate by vanes in the inlet ducting. Centrifugal force causes the heavy water droplets to move to the outside of the separator and is collected by a coalescer bag and collector assembly, the water is then directed overboard, and the dry air continues through the system (Figure 3). The coalescer bags can be cleaned or replaced as required to prevent the build-up of contaminants and odours in the system.
Figure 3: Water separators
Source: Boeing. Modified and annotated by the ATSB
During normal operation, the system automatically controls aircraft air temperature and pressure to maintain the optimum environment inside the aircraft for comfort and safety. If required, the flight crew can manually control system temperature, airflow, and PACK bleed air source, as well as manually control aircraft pressurisation. In both manual and automatic modes, the system is protected from overheat or freezing by a series of temperature control switches and sensors.
On the incident flight, the air-conditioning and pressurisation system was operating in automatic mode, with the left PACK supplying the flight deck and forward galley area, and the right PACK supplying the passenger cabin and rear galley.
Aircraft supplementary oxygen systems
Crew emergency oxygen system
Supplemental oxygen systems are provided to supply breathable oxygen in the case that the aircraft air is not capable of supporting respiration, either due to loss of air (oxygen) pressure or environmental contaminants. They can also be used as first aid to maintain blood oxygen levels in the case of medical emergency.
The flight deck oxygen system supplies oxygen to the flight crew in the case of an emergency. The system consists of a pressurised oxygen cylinder, 3 full face masks – one located at each of the captain, first officer, and observer seated positions – and a distribution system. A single, high‑pressure gaseous oxygen supply cylinder supplies oxygen to all 3 flight deck masks.
The masks are located in stowage containers at each flight crew location. Removal of the mask from the container aligns supply valves and supplies oxygen to the mask. An inflatable harness ensures that quick donning is possible by a range of users. Integrated goggles afford protection to the eyes from smoke or other airborne irritants, and a regulator allows manual selection of oxygen supply modes for various requirements (Figure 4).
Figure 4: Flight crew oxygen masks
Source: Boeing. Modified and annotated by the ATSB
In an emergency, the pilot removes the mask from the container by grasping and pulling on the protruding regulator. The harness is inflated by squeezing 2 buttons on either side of the regulator, allowing the user to don the mask in a downward sweeping motion. Releasing the buttons deflates the harness and pulls the mask onto the pilot’s face resulting in an airtight seal between the mask and face. Oxygen supply mode is selected by way of a rotary knob on the front of the regulator to suit the emergency, and communication is enabled by an integrated dynamic microphone. The donning of the mask is designed to be completed quickly with one hand and without the need for further adjustment.
Additional portable oxygen systems, including breathing equipment, are located throughout the cabin and flight compartment, and are intended for use in medical emergencies or unexpected cabin depressurisation.
Flight crew procedures for oxygen system
Specific National Jet Systems policy and procedures for the use of supplementary or emergency oxygen by crews were dependent on the emergency.
Following a loss of cabin pressure at altitude, emergency oxygen was expected to be used promptly without the need to reference written procedures. The automatic, immediate response was required to ensure that the risk of hypoxia[4] was not realised, which might affect the flight crew’s cognitive ability and safety of flight.
Smoke, fire, or fumes on the flight deck also required an automatic response with regards to oxygen use, however the definition of smoke and fumes requiring a response rested with the flight crew’s judgement of the hazard. The procedure detailed in the Quick Reference Handbook involved the use of supplemental oxygen by the flight crew, descent to 9,000 ft, and the removal of the smoke or fumes by ventilation. National Jet Systems advised that that procedure was considered inappropriate for cabin air quality (CAQ) events (see the section titled Cabin air quality events) and it had never been used by their crews in response to a CAQ event.
The National Jet Systems Emergency Procedures Manual stipulated the administration of oxygen by a cabin crew member responding to a pilot incapacitation event, inferring that total incapacitation had occurred and the pilot was unable to apply oxygen themselves.
Lastly, the National Jet Systems B717 Pilot Handbook – Checklist procedures stated:
Crew oxygen masks must be donned and communications established when their use is required. This includes but is not limited to:
Loss of cabin pressure.
Prior to the discharge of any fire extinguisher in or near the flightdeck.
Contamination, (smoke).
The concentration of fumes or odours, either present or anticipated on the flight deck.
National Jet Systems' annual recurrent training in the use of oxygen in flight included both theory and practical assessments in the flight simulator. The training was designed to validate flight crews’ response to a loss of cabin pressure and smoke/fumes on the flight deck.
Crew use of oxygen
In this event, oxygen was not used by the cabin or flight crew. The cabin crew did not consider themselves incapacitated, and their symptoms were mild and short-lasting. During the in-flight discussion between the flight and cabin crew regarding the departure CAQ event, the captain reminded the cabin crew to use oxygen if their symptoms persisted.
The captain reported at the time they first experienced symptoms, they did not assess themselves as incapacitated and therefore there was no requirement for a go-around or declaration of a PAN, and that a go-around would have exacerbated the situation as it would have significantly extended the airborne exposure time. The captain reported that this was a CAQ event and although oxygen was available, they did not correlate flight crew use of supplemental oxygen with a CAQ event response.
At the time the captain handed over control of the aircraft, the first officer’s focus was on configuring the aircraft for landing, and the welfare of the captain. The first officer reported that they did not think oxygen was required considering the smell had ceased and symptoms were not being experienced. Further, the first officer did not consider that the captain was incapacitated as they were performing the pilot monitoring role, albeit with some prompting.
The crew reported that they had infrequently practised donning the mask during practical training. The captain further reported that in their last simulation, the mask tended to fog up, and that communicating was more difficult with it on.
The Qantas chief medical officer reported that the use of supplemental oxygen would have prevented further ingestion of any airborne contaminants present. Furthermore, had the contaminant been CO or CO2, use of oxygen was the only method able to provide rapid improvement in the crew’s condition.
Cabin air quality events
Sources of cabin air quality events
Modern aircraft air-conditioning and pressurisation systems are complex and involve significant variables in pressures, temperatures, and operating environments. Several major studies have been completed by authorities worldwide to assess the quality of cabin air and determine the source of contaminants. To date, the consensus is that aircraft cabin air quality is typical of indoor environments and considered safe. However, concerns have been raised about the possibility of contaminants which may contribute to long and/or short-term health effects. Cabin air contaminants are more likely to be detected during take-off or landing (EASA 2017).
In the 12 months preceding the incident flight, the operator recorded 28 CAQ events on Boeing 717 aircraft, 19 of which resulted in mild symptoms such as nausea, headaches, or irritated eyes or throat in the crew. Eleven of the 28 events involved reported odours during take‑off/climb and again during descent/landing. None of the recorded events affected safety of flight and were therefore categorised as innocuous by the operator.
Generally, and not specific to the Boeing 717 aircraft, known possible causes of CAQ issues include:
engine oil introduced into the airpath by leaking internal engine or auxiliary power unit compressor seals
hydraulic oil or exhaust gases introduced into the airpath from external aircraft sources
dirty or defective water separator bags or components
build-up of contaminants within the air-conditioning packs or ducting
the use of aircraft cleaning or de-icing chemicals, inadvertently introduced into the airpath
introduction of bio-effluents into the airpath in flight
external environment airborne fumes, gases or pollution
fumes from internal cabin or cargo compartment sources.
Routine inspections and maintenance of known sources of odours and fumes were conducted to reduce CAQ events. Additionally, these sources often guided the immediate action of maintenance crews in response to a CAQ event. However, the source of reported odours or fumes were often not determined.
Recent VH-NXM cabin air quality reports and maintenance
In the 6 days prior to the incident flight on 6 June 2023, maintenance records for VH-NXM documented other reports of cabin air quality issues (Table 1).
Table 1: VH-NXM CAQ events and maintenance
Date
Flights
Defect
Maintenance Action
1 June 2023
1 Flight
Forward and aft cabin crew report rotten garbage smell following application of take-off thrust, lasting 5 minutes.
Both coalescer bags replaced and cleanout of the high‑pressure ducting with auxiliary power unit bleed air carried out.
1 Flight
No CAQ Issues
2 June 2023
4 Flights
No CAQ Issues
4 June 2023
1 Flight
Chlorine smell was reported at the forward and aft galleys and the flight deck during take-off for between 3-5 minutes. Cabin crew reported mild symptoms (dizziness and shaking). The flight was diverted to Sydney.
System inspected for signs of oil leaks. Ground functional check carried out; no odours detected on ground.
1 Flight
No CAQ Issues
5 June 2023
2 Flights
No CAQ Issues
6 June 2023
1 Flight
No CAQ Issues
Incident Flight
In response to the incident flight, the following maintenance actions were completed:
inspection of air conditioning/pressurisation system ducting and associated hardware for evidence of oil or other contaminants, or unserviceability
inspection of both PACKs and water separator drain lines
inspection and replacement of both PACK coalescer bags
cleanout/burnout of pneumatic high-pressure ducting
standard troubleshooting post cabin air quality event to locate sources of oil or hydraulic fluid that may have inadvertently entered the airpath
ground testing and flight testing with particulate and air quality analysers onboard
inspection of oil replenishment records to identify notable consumption or loss
inspection of both aft toilet chemical injection systems.
The reported CAQ event could not be replicated on the ground or air by maintenance crews, therefore a definitive source of the chlorine odour was not determined.
National Jet Systems Cabin Air Quality events procedure
The National Jet Systems in-flight procedure in response to CAQ events was divided into 2 sections.
Section 1 was designed to record details of the event such as odour strength and description, time and duration of the event, and aircraft configuration at the time of the event. This was primarily intended to assist ground maintenance crews in the identification and rectification of faults during post-flight maintenance.
Section 2 was used in the case of reported crew or passenger physical symptoms resulting from the fumes event. This was to ensure post-flight medical care of crew and passengers if required, and to enable consistent recording of events and their impact on crew or passengers.
On the incident flight, both sections of the procedure were completed, and the operator was notified of the occurrence prior to arrival into Hobart.
Flight crew incapacitation
Symptoms and causes of incapacitation
Pilot incapacitation may be obvious or subtle, with symptoms ranging from total loss of function or consciousness to minor impacts on perception or executive function. Management of obvious incapacitation involves crew reacting to overt observable action or inaction. However, subtle incapacitation requires recognition of sometimes fleeting outward symptoms and reacting in a way that does not further degrade safety of flight (ICAO 2012).
The majority of reported pilot incapacitation events are caused by gastrointestinal upset, most commonly attributed to food poisoning (ATSB 2007). This type of incapacitation is characterised by clear outward symptoms and well-established responses by the crew.
Another source of pilot incapacitation is hypoxia. Hypoxia is caused by the interference in delivery of oxygen to the body. This can be the result of low oxygen pressure due to altitude, displacement of oxygen in the air by airborne contaminants, interference of oxygen in the blood due to toxins such as carbon monoxide, or restriction of blood flow due to rapid decompression, cold environment, or medical events (FAA 1991). The symptoms of hypoxia range, depending on the magnitude and speed of the source, from mild discomfort and subtle incapacitation to unconsciousness. In all cases the immediate application of supplemental oxygen will reverse the symptoms of hypoxia.
The symptoms of subtle incapacitation include degraded decision making, perception, awareness of surroundings, vision, motor control and coordination, concentration, behaviour, or memory. Symptoms can be fleeting or long lasting and difficult for others to detect; moreover, it is possible for the person experiencing the symptoms to be unaware of their presence.
This difficulty in detection is what constitutes the primary risk of this type of incapacitation, and as one of the first symptoms experienced affects cognition, it can be difficult or impossible for the person experiencing the incapacitation to recognise or respond to appropriately. Minor levels of incapacitation may be rationalised by the person suffering symptoms or by those observing; for example, difficulty maintaining altitude might be attributed to a lack of recent exposure to aircraft manual control (ICAO 2012).
Another consideration when discussing pilot incapacitation is the effect of stress on flight crews during a non-normal event, which is amplified if the event takes place during a critical stage of flight (NASA 2015):
Situational stress can adversely affect the cognition and skilled performance of pilots, as well as experts in other domains. Emergencies and other threatening situations require pilots to execute infrequently practiced procedures correctly and to use their skills and judgment to select an appropriate course of action, often under high workload, time pressure, and ambiguous indications, all of which can be stressful.
The Qantas chief medical officer asserted that the effect of stress can cause a physiological response (including hyperventilation) which is difficult to differentiate from symptoms caused by any external physical sources. In fact, the stress response itself can increase anxiety resulting in a feedback loop and severe distress for the sufferer, manifesting as physical incapacitation.
Flight crew procedures and training for crew incapacitation events
The National Jet Systems pilot incapacitation procedure involved the unaffected pilot using a cabin crew member to assist the flight crew by securing the incapacitated pilot in their seat and away from flight controls, and the application of first aid if required. The primary purpose of the procedure was to prevent inadvertent interference with the safe flight of the aircraft and to provide medical aid if necessary. The use of oxygen was stipulated in the context of first aid, if required.
Flight and cabin crews underwent recurrent practical training and assessment in the conduct of incapacitation procedures. Specific pilot incapacitation training at National Jet Systems was conducted at:
Boeing 717 Command Upgrade Training (one segment dedicated to pilot incapacitation during a simulator session)
annual practical emergency procedures training (one practical segment dedicated to pilot incapacitation, conducted with flight crew and cabin crew as a combined group, in an aircraft or synthetic trainer)
initial and 4-yearly Boeing 717 Pilot Low Visibility Procedures Take-Off Training (one exercise dedicated to a pilot incapacitation event during take-off).
The National Jet Systems Aircraft General Operating Policy & Procedure, section 5.4.8 Flight crew/cabin crew incapacitation, stated:
When a Flight Crew member becomes incapacitated in flight, as a minimum, a PAN should be declared and the aircraft should be landed at the nearest suitable airport … Any apparent incapacitation of flight crew or cabin crew should not go unnoticed.
Flight crew members should be alert to the possibility of sudden or subtle incapacitation of an operating Flight Crew member, particularly during take-off and landing manoeuvres. To protect against subtle incapacitation, Flight Crew members are required to acknowledge supporting calls. Acknowledgement is normally the word “Checked”.
National Jet Systems’ training syllabus also included relevant recurrent human factors and threat and error management training.
Two communication rule
Modern passenger aircraft use 2-pilot crews to share workload and provide redundancy in an emergency. Duties are clearly defined and split between pilot flying (PF) and pilot monitoring (PM). While the PF and PM duties can be performed by the captain or first officer, the captain retains authority on the aircraft. However, safe operation relies on the first officer monitoring the captain’s actions and challenging or intervening if necessary.
Roles are clearly defined between the PF and PM, in part to ensure that a breakdown in the system can be quickly recognised. While the PM generally handles radio calls, checklists, and monitors the status of the aircraft and PF, the PF ensures that the PM completes the appropriate checklist, checklist items and radio calls, and the PF responds with an appropriate call, usually ‘checked’. This is known as the ‘two communication rule’ and is widely used because an error or absence of a call will quickly indicate a system problem, or issue with a flight crew member (ICAO 2012).
The two communication rule is reliant on a culture on the flight deck typified by a low flight deck authority gradient[5] and a high level of situation awareness. Understanding of what should be happening at any given phase of flight is critical to the effectiveness of the rule, the adherence to standard operating procedures is therefore a key component to enable crews to quickly identify subtle incapacitation in others (ICAO 2012).
The National Jet Systems B717 Pilot Handbook, Section 11.1.1 Standard Phraseology, stated:
… The absence of a standard callout at the appropriate time may indicate a malfunction of an aircraft system or indication, or indicate the possibility of incapacitation of the other pilot.
Similar occurrences
Between 2013 and 2023, the ATSB recorded 205 flight crew incapacitation occurrences, 7 were related to cabin air quality, of which 2 took place on commercial passenger jet aircraft.
The following are summaries of notable CAQ incident investigations.
United Kingdom Air Accident Investigations Branch Airbus A320-232 G‑EUYB 09-20
On 23 September 2019, the flight crew of an Airbus A320-232 detected an odour described as a sweaty sock smell while climbing through about 10,000 ft after departing Zurich Airport. The co‑pilot stated that they had experienced similar odours on the aircraft type before but described this instance as much stronger than previously experienced. The odour lasted about 30 seconds. The crew discussed options and elected to continue the flight; the flight crew's previous experience suggested that if the smell was going to reoccur it was most likely to occur when thrust was reduced for descent so, during the cruise, they discussed their actions if the smell returned and reviewed the SMOKE/FUMES/AVNCS SMOKE checklist.
The crew detected strong acrid fumes on the flight deck while on approach to London Heathrow Airport, United Kingdom. They enacted their plan and donned oxygen masks, declared a PAN, and completed the landing.
After landing, the copilot removed their mask to check for the continued presence of the odour. It was still present, so the flight crew shut down both engines, opened the flight deck windows, and started the auxiliary power unit. Shortly after, the copilot became nauseous and vomited out the flight deck window. A cabin crew member came onto the flight deck to assist and noted a chemical smell on the flight deck. They also confirmed that there were no smells or reports of illness in the cabin.
Both flight crew attended hospital, but results were not published.
The Air Accident Investigations Branch conducted a test of the aircraft air conditioner systems on the ground with engines, auxiliary power unit, and ground power. No odours or defects were identified. A comprehensive inspection and associated aircraft systems was carried out, and no sources of the fumes was identified.
The report concluded:
While it has not been possible to positively identify the compound that was responsible for the fumes and odours experienced in G-EUYB, or any of the other recent events, a number of common factors have been identified. The majority of events occurred after the aircraft had been parked or operated in precipitation. The fumes become apparent during the later stages of the descent, sometimes preceded by a minor event during the climb phase. The generation of fumes appears to be transient; they dissipate rapidly and leave no detectable trace. No link between changes to engine power or changes in other system settings and the generation of fumes was identified.
In some cases, the presence of fumes has resulted in physiological reactions which have interfered with a flight crew member’s ability to carry out their normal duties. However, by following the smoke and fume checklist, and donning oxygen masks the flight crew were able to ensure the continued safety of the aircraft.
French Bureau d’Enquêtes et d’Analyses (BEA) 2017-0658 Airbus A320 EC‑HQJ
On 17 November 2017, the pilots of an Airbus A320 complained of an unpleasant smell and irritations while taxiing behind a Cessna Citation prior to departure from Geneva-Cointrin Airport, Sweden. During the initial climb the crew experienced nausea and dizziness, which became progressively worse as the flight continued.
During the cruise, the captain donned their supplemental oxygen mask and reported an improvement of symptoms. A short time later, the first officer donned their supplemental oxygen mask due to worsening symptoms, a PAN was declared, and the aircraft diverted to Marseilles‑Provence Airport, France. The flight crew remained on oxygen for the remainder of the flight and landed without further incident.
Blood samples were taken, and tests showed no signs of carbon monoxide poisoning, but no other toxicological tests were carried out on the blood samples. Nausea and dizziness were reported for several days following. Hair samples were taken from the flight crew and analysed, but the analysis did not find substances in quantities corresponding to a one-off significant exposure in relation with the event.
Inspection of both aircraft involved identified no relevant defects or causes of contaminated air.
The reported concluded:
Despite the wide range of actions undertaken, the investigation was not able to factually identify what caused the flight crew’s symptoms and physical discomfort. The hypothesis of them having inhaled an excessive quantity of carbon monoxide, contained in exhaust gases emanating from the Cessna Citation which had been in front of the A320, is consistent with the information collected and can explain the symptoms observed (dizziness and nausea). Nitrogen oxide and sulphur oxide compounds present in exhaust gases may also have contributed to the acrid and irritating odours smelt while taxiing. However, it cannot be excluded that the crew were intoxicated by another substance which either quickly disappeared or which was not specifically searched for in the samples taken from the aeroplane as to date, not identified, even in the most recent studies.
Toxic substances were searched for in the hair samples using the most effective, innovative techniques to date. The BEA believes that the use of these techniques on matrices such as saliva, blood or urine, sampled as quickly as possible after the symptoms, and in particular as soon as possible after landing, would increase the chances of detecting a wider range of potentially toxic substances.
Swedish Accident Investigation Board RL 2001:41e BAE 146-200 SE-DRE
On 12 November 1999, the crew of a British Aerospace BAe 146-200 were scheduled to carry out 3 return flights between Stockholm and Malmö, Sweden.
During the first flight, a cabin crew member experienced a faint feeling. On the second flight cabin crew members experienced an odd pressure in the head, nasal itching, ear pain, and the feeling of ‘moon walking’. The issue was discussed with the pilots on both occasions, and on both occasions the pilots reported feeling no symptoms.
On the third flight, the cabin crew again reported discomfort similar to the preceding flights, but more pronounced. On descent to Malmö Airport, the copilot suddenly became nauseous and donned their oxygen mask. After about 10 seconds, the captain also became nauseous and donned their oxygen mask. After a few seconds on oxygen, the copilot started to feel better, however the captain’s condition continued to deteriorate. The captain reported feeling dizzy, and having difficulty with physiological motor response, simultaneity, and in focusing. The captain started to feel better after breathing oxygen for several minutes, and the landing was completed without further incident.
No medical examinations were performed after the incident.
A comprehensive technical investigation was conducted to attempt to determine a source of foul air. This included cabin air quality tests during test flights, bleed air analysis during a test run of an engine with an identified oil leak in an engine test cell, and dismantling and inspection of the engine. Despite these efforts, a definitive explanation for the incident was not identified.
The report concluded:
Air samples taken during engine testing and aircraft test flights provided no indication of what/which chemical substances caused the symptoms.
No technical fault that can explain the incident has been found.
The location of the customer bleed port for the air-conditioning system is not optimal on the engine type.
Knowledge is lacking concerning modern lubrication oils’ characteristics at very high pressure and temperatures and their effect on human health.
Instructions are lacking concerning how crews shall act during flight when suspicion arises about contaminated cabin air.
Safety analysis
Introduction
During climb, the 2 cabin crew members in the forward galley smelt a chlorine odour and experienced associated mild symptoms, which abated after a short time, before returning again on landing. The air-conditioning system was in the normal configuration so that bleed air from the left engine and pressurised air-conditioning kit was distributed to the flight deck and forward galley, while the right side supplied the passenger cabin. Although left-side air was also being distributed to the flight deck, the flight crew did not detect odour during the climb. The crew treated the odour as a cabin air quality (CAQ) event and conducted the associated reporting actions.
Later in the flight, on approach to Hobart Airport, the flight crew noticed a chlorine odour and the captain experienced the rapid onset of symptoms of incapacitation, including cognitive impairment. The captain handed over pilot flying duties to the first officer and assumed the responsibilities of pilot monitoring.
Just before landing, the first officer reported feeling some symptoms of incapacitation but due to the proximity to landing and perceived difficulties of donning the oxygen mask, the first officer assessed that supplemental oxygen was likely to increase the risk to safety of flight. A go-around was considered, but the first officer assessed that continuing the landing was the safest overall course of action. Both flight crew members were partially incapacitated during the landing and subsequent taxi to the parking bay.
The odour and symptoms were consistent with that experienced earlier by the cabin crew, albeit with the flight crew experiencing more serious effects. The reason for the captain experiencing more debilitating effects slightly earlier than the first officer and for the cabin crew’s symptoms being subjectively milder, could not be determined. Whether a stress response to a non-normal situation in a high workload phase of flight exacerbated or contributed to the symptoms experienced by the flight crew on the incident flight was also not determined. The same aircraft had a reported CAQ event 2 days prior to the incident, in which cabin and flight crew smelt chlorine and only the cabin crew reported any symptoms, which were mild. Following the 6 June 2023 occurrence, maintenance engineers conducted an inspection of the aircraft to identify a source of the odours, none were found, and the event was not able to be reproduced on the ground or during a subsequent test flight.
Cabin air quality events procedure
Based on occurrences recorded by the ATSB and the aircraft operator, most CAQ events are short-lived and benign, with exposed crew experiencing no or mild symptoms. However, in rare cases the effects can be more serious and affect the safety of flight. Crew incapacitation may be partial or complete, and symptoms can range from the obvious, such as vomiting or loss of consciousness, to the subtle, such as mild cognitive impairment, or difficulty executing a task. In accordance with the operator’s procedures, the appropriate response depended on the extent of the effects experienced by the crew.
The history of reported CAQ events not impacting safety of flight likely influenced the intent of the operator’s CAQ event procedure, which detailed steps to report an event to assist in post-flight maintenance activities, and to assess an affected individual’s fitness to continue or return to duty. In response to the transient odour and symptoms reported during climb by the cabin crew, the flight crew completed the CAQ event procedure. Although the CAQ event procedure did not require consideration of supplemental oxygen, the captain reminded the affected cabin crew members to use supplemental oxygen if required. The CAQ event procedure did not require crews to consider actions in the event flight crews were affected by airborne contaminants.
The operator’s emergency procedure for smoke/fumes and the pilot handbook included that crew oxygen masks must be donned when concentration of fumes or odours were detected or anticipated on the flight deck. However, when the flight crew experienced the chlorine odour and more serious symptoms, they assessed it was a transient CAQ event rather than a fumes event and therefore were not required to use supplemental oxygen. Additionally, the captain’s first symptoms were likely cognitive impairment, which may have affected their judgement regarding the need for supplemental oxygen. If cognitive incapacitation is due to hypoxia or environmental contaminants, the window of opportunity to recognise and react to it can be very small before more significant cognitive effects impair decision making.
According to the operator’s medical officer, use of supplemental oxygen can have operational challenges but will not cause harm. Its use prevents further inhalation of contaminated air, preventing symptoms from worsening. In particular, it reverses the effects of hypoxia, including exposure to carbon monoxide and dioxide, and is also useful in the case of many medical emergencies.
National Jet Systems’ record of CAQ events showed 28 reported events in the 12 months prior to the incident flight, often during descent/landing preceded by events during take-off and climb. Eleven of the 28 events reported symptoms such as nausea/vomiting, headache, dizziness, or discomfort of the eyes and throat, but none of these effects impacted the safety of flight. The potential for a recurrence in the same flight was not considered in the CAQ event procedure. Additionally, the procedure did not include consideration of a CAQ issue leading to a fumes or incapacitation event.
As a result, the crew were unprepared for the subsequent fumes and incapacitation event, which occurred at a critical phase of flight, and did not use oxygen to significantly reduce the risk of both flight crew becoming partially incapacitated. The effectiveness of such preparation was demonstrated in a 2019 incident investigated by the United Kingdom Air Accident Investigations Branch. In that incident, following a mild transient CAQ event during the climb, the flight crew reviewed their smoke/fumes procedure, and discussed and planned to use oxygen if an event recurred. As a result, the flight crew quickly donned oxygen and declared a PAN when they detected fumes on approach.
Pilot incapacitation training
Multiple studies have identified gastrointestinal illness caused by food poisoning as the most common cause of pilot incapacitation. This finding has shaped pilot incapacitation training and procedures to ensure that the most prominent threat is adequately covered. The most salient features of food poisoning are obvious symptoms, the ability for the sufferer to communicate their distress, and ability to retain cognitive capacity. Training in recognition and response of pilot incapacitation has also been focused on the immediately hazardous effects of sudden and total incapacitation. The operator’s training in the use of supplemental oxygen for incapacitation focused on response to these events and did not encompass precautionary use of supplemental oxygen, or oxygen use during critical stages of flight.
The captain self-assessed as being unable to continue as pilot flying and handed over the duty to the first officer in accordance with the operator’s procedures, but did not communicate the severity of the difficulties experienced to the first officer. Although the captain knew and understood the symptoms and response to hypoxia, at the time, likely due to cognitive impairment, the captain did not recognise the hypoxia-like symptoms or identify supplemental oxygen as an appropriate response.
The National Jet Systems pilot incapacitation training focused on responding to overt or obvious incapacitation rather than the response to subtle incapacitation. The operator’s policy manual specified the flight crew’s absence of a standard call, or an acknowledgement of a standard call, as an indicator of pilot subtle incapacitation. In this case the first officer recognised that the captain had missed the stable approach call required at 1,000 ft altitude, and prompted the captain who then made the correct call.
Without the benefit of formalised training in the response to partial or cognitive incapacitation, and due to the absence of symptoms experienced by the first officer at that time, the first officer continued the landing without the use of supplemental oxygen. Additionally, the first officer assessed that the operator’s pilot incapacitation procedure and requirement to broadcast a PAN call were inappropriate in this event, as the captain was not completely incapacitated, and the aircraft was close to landing. While the proximity to landing limited the opportunity for the first officer to take any further action, the absence of training in management of subtle physical or cognitive incapacitation increased the risk of both flight crew members becoming impaired and unable to safely continue the flight.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight crew incapacitation involving Boeing 717-200, VH-NXM on approach to Hobart Airport, Tasmania on 6 June 2023.
Contributing factors
The flight crew noticed a chlorine odour during the approach to Hobart Airport. Shortly after, the captain experienced the rapid onset of symptoms of incapacitation, resulting in them handing over pilot flying duties to the first officer.
Just before landing, the first officer experienced symptoms of incapacitation, specifically slowed reaction time. Due to the impending landing, and perceived difficulties of donning the mask, supplemental oxygen was considered but not used. A go‑around was also considered but rejected following an assessment that continuing the landing was the safest course of action.
National Jet Systems’ cabin air quality events procedure focused on the recording/reporting of odours, post-flight care of crew and maintenance actions. However, it did not consider the possible application of the smoke/fumes procedure, or incapacitation procedure. As a result, there was an increased risk of flight crew being adversely affected by such an event during a critical stage of flight.(Safety issue)
Other factors that increased risk
Although National Jet Systems had procedures for recognition and management of pilot incapacitation, the associated training did not include the identification and response to subtle physical or cognitive incapacitation. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
National Jet Systems cabin air quality event procedures
Safety issue description: National Jet Systems’ cabin air quality events procedure focused on the recording/reporting of odours, post-flight care of crew and maintenance actions. However, it did not consider the possible application of the smoke/fumes procedure, or incapacitation procedure. As a result, there was an increased risk of flight crew being adversely affected by such an event during a critical stage of flight.
National Jet Systems pilot incapacitation training
Safety issue description:Although National Jet Systems contained procedures for recognition and management of pilot incapacitation, the associated training did not include the identification and response to subtle physical or cognitive incapacitation.
Glossary
CAQ
Cabin air quality
CO
Carbon monoxide
CO2
Carbon dioxide
PACK
Pressurised air-conditioning kit
PF
Pilot flying
PM
Pilot monitoring
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
National Jet Systems
Qantas chief medical officer
aircraft QAR data
Boeing Aircraft Company
Airservices Australia
Bureau of Meteorology.
References
Australian Transport Safety Bureau. (2007) Pilot Incapacitation: Analysis of Medical Conditions Affecting Pilots Involved in Accident and Incidents. 1 January 1975 to 31 March 2006. B2006/0170
Dismukes, K., Goldsmith, T. & Kochan, J. (2015). Effects of acute stress on aircrew performance: Literature review and analysis of operational aspects. National Aeronautics and Space Administration. (NASA) Report: NASA/TM-2015–218930.
European Aviation Safety Agency. (2017) CAQ Preliminary cabin air quality measurement campaign. EASA_REP_RESEA_2014_4
Federal Aviation Administration. (1991) Civilian training in high altitude flight physiology (FAA) Report: DOT/FAA/AM-91/13
International Civil Aviation Organisation. (2012). Manual of Civil Aviation Medicine (3rd ed.) ICAO Doc 8984, Montréal.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew
National Jet Systems
Civil Aviation Safety Authority
Boeing Aircraft Company
Qantas chief medical officer
United States National Transportation Safety Board
Submissions were received from:
the incident flight captain
National Jet Systems
Boeing Aircraft Company
Qantas chief medical officer
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Configuring for landing includes lowering wing flaps and slats, lowering landing gear and arming the speed brake.
[3]PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4]Hypoxia: is a physical state where sufficient oxygen is not available for the body to sustain life either due to low blood oxygen levels, or inadequate blood supply to the body.
[5]Authority gradient: the authority relationship between the captain and first officer. For example, in the case of a domineering captain and an unassertive first officer, the gradient is considered high.
Occurrence summary
Investigation number
AO-2023-026
Occurrence date
06/06/2023
Location
Hobart Airport
State
Tasmania
Report release date
16/04/2024
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Flight crew incapacitation
Occurrence class
Serious Incident
Highest injury level
Minor
Aircraft details
Manufacturer
The Boeing Company
Model
717-200
Registration
VH-NXM
Serial number
55094
Aircraft operator
National Jet Systems Pty Ltd
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes