The ATSB has launched a transport safety investigation into a fatal accident involving a Cirrus light aircraft at Gundaroo, north of Canberra, on Friday afternoon.
Transport safety investigators from the ATSB’s Canberra office were expected to arrive at the scene on Friday evening to conduct an initial assessment of the accident site.
Over coming days, investigators with experience in aircraft operations and maintenance will conduct a range of evidence-gathering activities on site including site mapping, wreckage examination, and recovery of aircraft components for further examination at the ATSB’s technical facilities in Canberra.
Investigators will also seek to interview any witnesses and involved parties, and collect relevant recorded information including flight tracking data, as well as pilot and aircraft maintenance records, and weather information.
The ATSB asks anyone who may have witnessed the accident, or may have video footage of the aircraft in any phase of its flight, to make contact via the witness form on our website: atsb.gov.au/witness at their earliest opportunity.
The ATSB anticipates publishing a preliminary report, which will detail factual information established during the investigation’s initial evidence collection phase, in approximately 6-8 weeks.
The ATSB will publish a final report, detailing contributing factors and any identified safety issues, at the conclusion of the investigation.
However, should any critical safety issues be identified at any stage during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.
A twin piston-engined charter aircraft’s forced landing on an island in the Torres Strait was likely the result of fuel starvation, an Australian Transport Safety Bureau final report details.
On 3 October 2022, a Torres Strait Air Britten-Norman BN-2 Islander with a pilot and six passengers on board was operating a flight from Saibai Island to Horn Island.
While in the cruise at about 6,000 ft, the aircraft’s engines began to surge. The pilot diverted towards Kubin Airport on Moa Island, but was unable to reach the runway and was forced to land on a road.
During the landing the aircraft impacted the ground heavily, with the rear fuselage and tail breaking away, but fortunately, there were no reported injuries.
The ATSB’s subsequent transport safety investigation found the dual engine speed fluctuations and associated power loss was probably the result of fuel starvation.
“Fuel records from earlier flights showed the pilot was using the wing tip tanks when fuel remained in the aircraft’s main tanks, which was not in accordance with the flight manual,” ATSB Director Transport Safety Dr Stuart Godley said.
“In addition, the configuration and location of the aircraft’s fuel controls and gauges were probably not conducive to rapid and accurate interpretation, with the main tank gauges and cocks located overhead the windscreen centre post and the wing tip tank contents indicators on the right side of the cockpit.”
The ATSB considered that both of these factors increased the likelihood of the wing tip tanks being inadvertently selected during part or all of the round trip, leading to the exhaustion of the wing tip tanks.
Dr Godley noted accidents involving fuel mismanagement are an ongoing safety concern to the ATSB.
“Pilots are reminded of the importance of understanding an aircraft’s fuel supply system and being familiar and proficient in its use,” he said.
“Adhering to procedures, maintaining an accurate fuel record, and ensuring appropriate tank selections are made for the phase of flight will lessen the likelihood of fuel starvation.”
Dr Godley noted that prior to the accident, in June 2022, Britten-Norman released service letter 145, which detailed an optional modification for Islander aircraft with wing tip tanks.
“The service letter details an optional modification that centralises the fuel system controls, specifically relocating the wing tip tank indicators to the overhead panel adjacent to the main tank fuel indicators, with the fuel selection switches mounted between the indicators,” he said.
“We would encourage Islander aircraft operators to consider actioning this service letter for their aircraft.”
A container ship went off its intended track towards the edge of the navigable channel in the Yarra River and struck a navigation beacon following a steering failure, an ATSB interim investigation report details.
The 277 metre CMA CGM Puccini had sailed from Swanson Dock in the Port of Melbourne on the morning of 25 May 2023 under the conduct of a pilot and initially with two tugs in attendance, the interim report from the ATSB’s on-going investigation into the serious incident details.
“Shortly after 0418, during the turn to leave Swanson Dock, the ship’s master and chief mate noticed the rudder response appeared sluggish,” ATSB Chief Commissioner Angus Mitchell said. “However, neither raised their observations with each other, or the pilot.”
About 25 minutes later, by which point it had passed under the Westgate Bridge and both tugs had been dismissed, the ship was moving at about 6.6 knots when the helmsman reported that the rudder was not responding to the steering wheel.
With its speed increasing, the ship moved further off course and tracked toward the western edge of the dredged navigable Yarra River channel.
“Despite efforts by the pilot and crew to slow the ship and correct its swing, the ship struck a navigation beacon, and its stern passed over the edge of the navigable channel,” Mr Mitchell said.
The two tugs were nearby and returned, and helped control the ship’s erratic movement. The ship was then moved to Webb Dock for inspection.
“Despite multiple, extensive inspections and tests by the ship’s engineers and two independent service engineers at Webb Dock, the erratic behaviour of the steering gear could not be replicated, and no fault was identified.”
On 26 May the ship was cleared to leave port , and it departed on 27 May for Port Botany, Sydney.
“The following day, in preparation for arrival to Port Botany, the ship’s crew again tested the steering gear,” Mr Mitchell noted.
“During this testing, the steering again began to behave erratically.”
At this time, the second engineer, who had joined the ship in Melbourne, noticed the steering system’s hydraulics were incorrectly configured. After the by-pass valve of the (non-running) pump was closed, there were no further erratic rudder responses.
The ship subsequently sailed for Brisbane on 30 May, where it berthed without incident on 1 June.
The ATSB commenced an investigation on the basis of initial reports that, despite multiple inspections, the erratic behaviour of the ship's steering on 25 May remained unexplained over the following days and the ship departed Melbourne with no problem identified.
ATSB investigators subsequently attended the ship in Brisbane on 2 June, and again in July when the ship returned to Melbourne, during which they conducted extensive testing of the steering systems, interviewed the crew, and obtained other evidence including various documents and recorded data.
Investigators also obtained evidence from the incident pilot and the pilotage provider, AMSA, and port authorities.
“As the investigation progresses, our team will verify data and evidence to confirm the order of events, analyse the ship’s steering arrangement and operation, review crew actions, and assess shipboard and CMA CGM fleetwide procedures and steering gear guidance, operation, information sharing and testing,” Mr Mitchell said.
A final report will be released at the conclusion of the investigation.
“However, should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Mr Mitchell concluded.
An incorrect position broadcast and not effectively monitoring radio calls contributed to the pilots of a King Air and Saab 340 misunderstanding the positions of the other aircraft, which led to non-standard manoeuvring before both aircraft received TCAS alerts in the circuit at Wellcamp Airport, an Australian Transport Safety Bureau investigation details.
On the morning of 21 October 2021, a Saab 340 was approaching Wellcamp, near Toowoomba, on a scheduled passenger flight from Brisbane, with two flight crew, one cabin crew, and nine passengers on board.
A Beechcraft King Air was also approaching Wellcamp, having earlier departed Roma on a charter flight with a pilot and eight passengers on board.
Approaching the circuit, the Saab flight crew announced an incorrect position on the Common Traffic Advisory Frequency (CTAF).
The ATSB found this incorrect call probably resulted in the pilot of the King Air misidentifying the Saab as another aircraft in the circuit.
“The flight crew of the Saab did not then effectively monitor the radio, resulting in them having an incorrect mental model of the King Air’s position, and not perceiving it as a threat,” ATSB Director Transport Safety Stuart Macleod said.
The pilot of the King Air then manoeuvred their aircraft opposite to the circuit traffic direction while descending into the active side of the circuit, in the vicinity of the airport, believing this manoeuvre would aid in sequencing.
“Both flight crews were unaware of the distance closing between them and, as the aircraft came closer together, both were issued traffic advisories from their traffic alert and collision avoidance system (TCAS),” Mr Macleod explained.
The Saab flight crew, who were also issued with a resolution advisory from their TCAS, followed this advisory and climbed until they were clear of conflict.
During the occurrence, separation between the aircraft reduced to 300 ft vertically and 1,000 m horizontally.
“The airspace above Wellcamp is non-controlled, with pilots responsible for self-separating,” Mr Macleod said. “It can often be busy, with a mixture of general aviation, charter, and regular public transport flights like the one the Saab was operating in this incident.
“One of the priorities of the ATSB’s SafetyWatch initiative is safety around non-controlled aerodromes, where insufficient communication between pilots is the most common cause of safety incidents like this one.
“In this case, the pilots of both aircraft had an incorrect mental model of each other’s position, and neither had positively sighted the other aircraft. The last line of defence was the TCAS, which prevented a potential collision.”
The ATSB’s final report advises pilots to use sound judgement, and to follow standard procedures and CASA guidance.
“Using standard procedures at non-towered aerodromes – unless otherwise stated in the En Route Supplement Australia – assists pilots in maintaining situational awareness and separation from other aircraft,” Mr Macleod said.
In addition, the report notes the value, demonstrated by this occurrence, of systems in addition to radio communications, such as ADS-B and TCAS.
“These additional systems serve as a valuable source of information to assist pilots’ situational awareness and decision making,” Mr Macleod concluded.
On the morning of 20 September 2023, inbound tram 6062 on route 96 was travelling south along Nicholson Street, East Melbourne towards the Victoria Parade intersection. At the same time outbound tram 6058, also on route 96, was travelling north on Nicholson Street and approached the same intersection.
At about 0952, tram 6058 followed the track, set for the right turn into Victoria Parade instead of continuing straight along Nicholson Street. As a result, the front end of tram 6058 collided with the front end of the oncoming tram 6062.
The driver of Tram 6062 and 5 passengers sustained minor injuries. Both trams derailed and sustained significant damage.
Victoria's Chief Investigator Transport Safety is conducting the investigation under the Transport Safety Investigation Act 2003 (Cth), under a collaboration agreement with the ATSB.
A preliminary report into the incident was published on the ATSB website on 22 December 2023. See below.
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
Last updated:
Preliminary report
Report release date: 22/12/2023
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
Prior to the incident
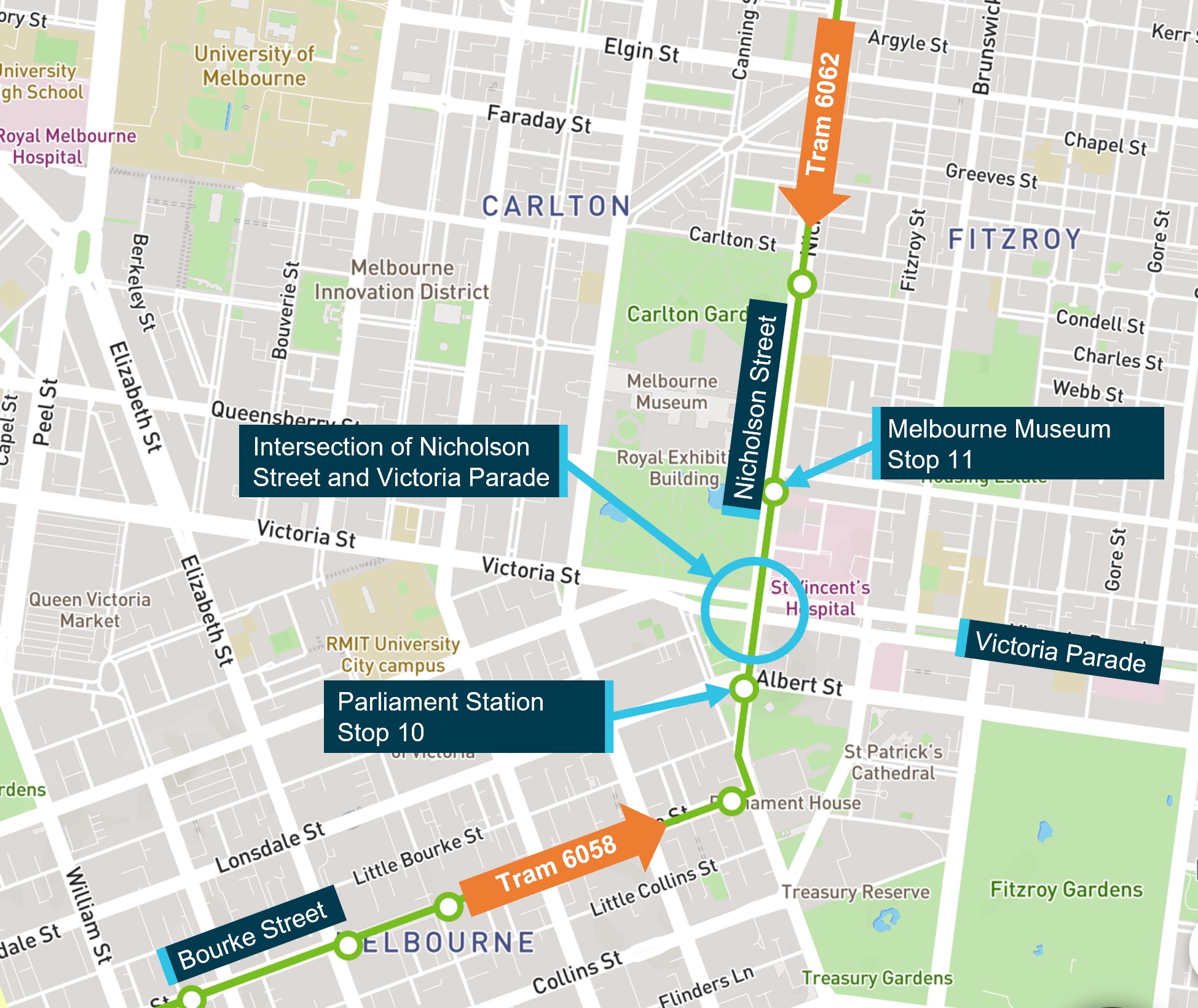
On 20 September 2023, trams 6058 and 6062 were operating on route 96 between Brunswick East and St Kilda Beach in Melbourne. Tram 6058 departed St Kilda Beach at about 0912 travelling towards Brunswick East, and tram 6062 departed Brunswick East at about 0936 travelling towards St Kilda Beach. At about 0951, both trams on parallel tracks approached the Nicholson Street intersection with Victoria Parade (Figure 1).
Figure 1: Intersection of Nicholson Street and Victoria Parade
Source: Public Transport Victoria annotated by the Office of the Chief Investigator Transport Safety
Preceding tram 6058 to the intersection was tram 6011. Tram 6011 arrived at the intersection at about 0950 and the points were switched for the tram to turn right and proceed along Victoria Parade.
The collision
After stop 11, tram 6062 proceeded south along Nicholson Street to the intersection with Victoria Parade. Traffic signals indicated that trams and road vehicles travelling south on Nicholson Street could proceed and tram 6062 commenced entering the intersection.
Tram 6058 was travelling north on Nicholson Street and in the opposite direction to tram 6062. After stopping at the Parliament Station stop (stop 10), tram 6058 proceeded up Nicholson Street towards the intersection with Victoria Parade. Traffic signals indicated that trams and road vehicles travelling north on Nicholson Street could proceed and tram 6058 commenced entering the intersection.
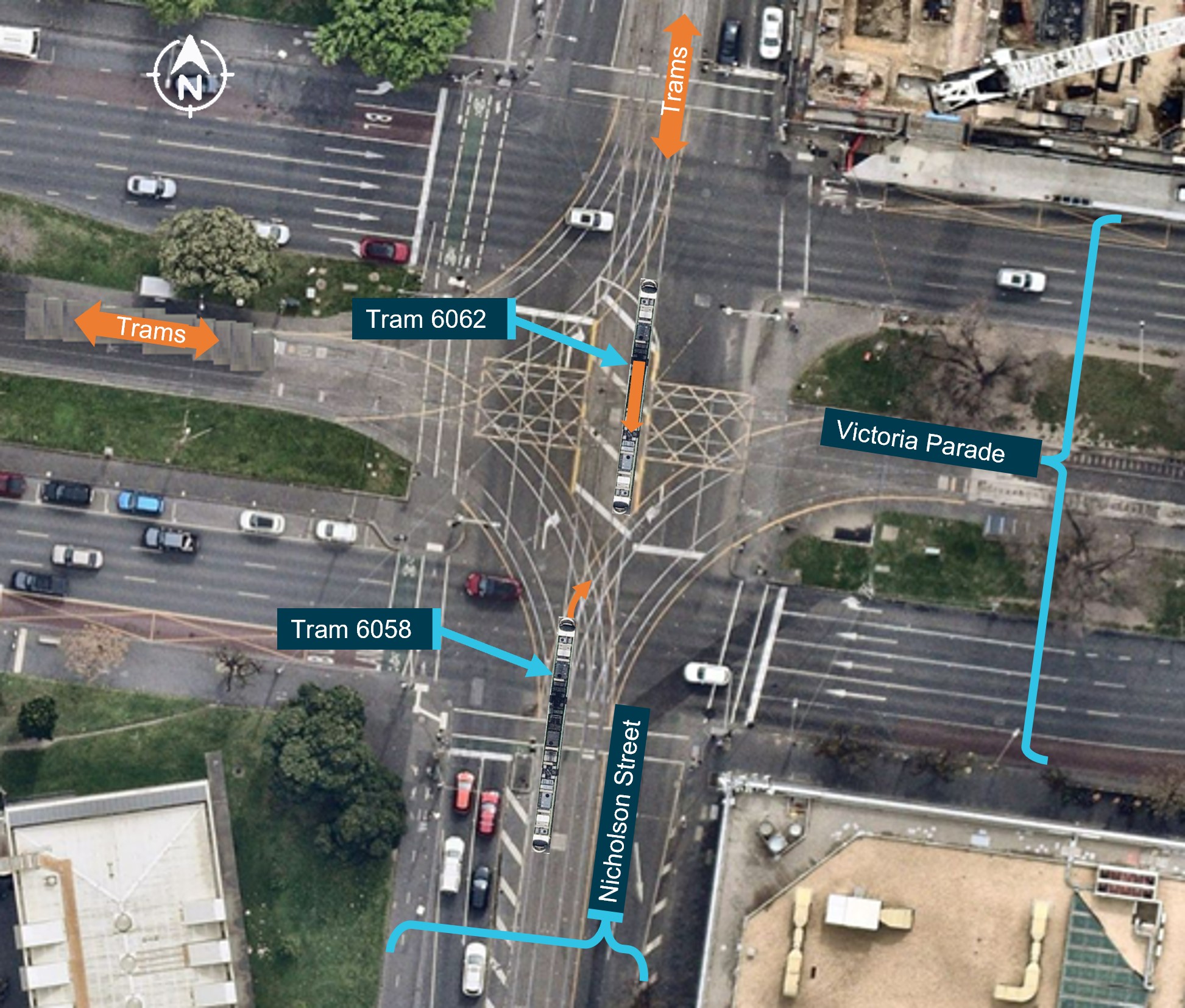
As the two trams on parallel tracks converged, tram 6058 turned to the right and into the path of tram 6062, colliding with tram 6062 at about 0952 (Figure 2). The driver of tram 6058 had expected to travel straight across the intersection.
Figure 2: Images of trams superimposed on a view of the intersection of Nicholson Street and Victoria Parade to show the paths of trams 6058 and 6062 leading to collision
The tram images superimposed on the aerial view of the intersection are not the actual trams, nor their precise locations prior to collision.
Source: Nearmap, annotated by the Office of the Chief Investigator Transport Safety
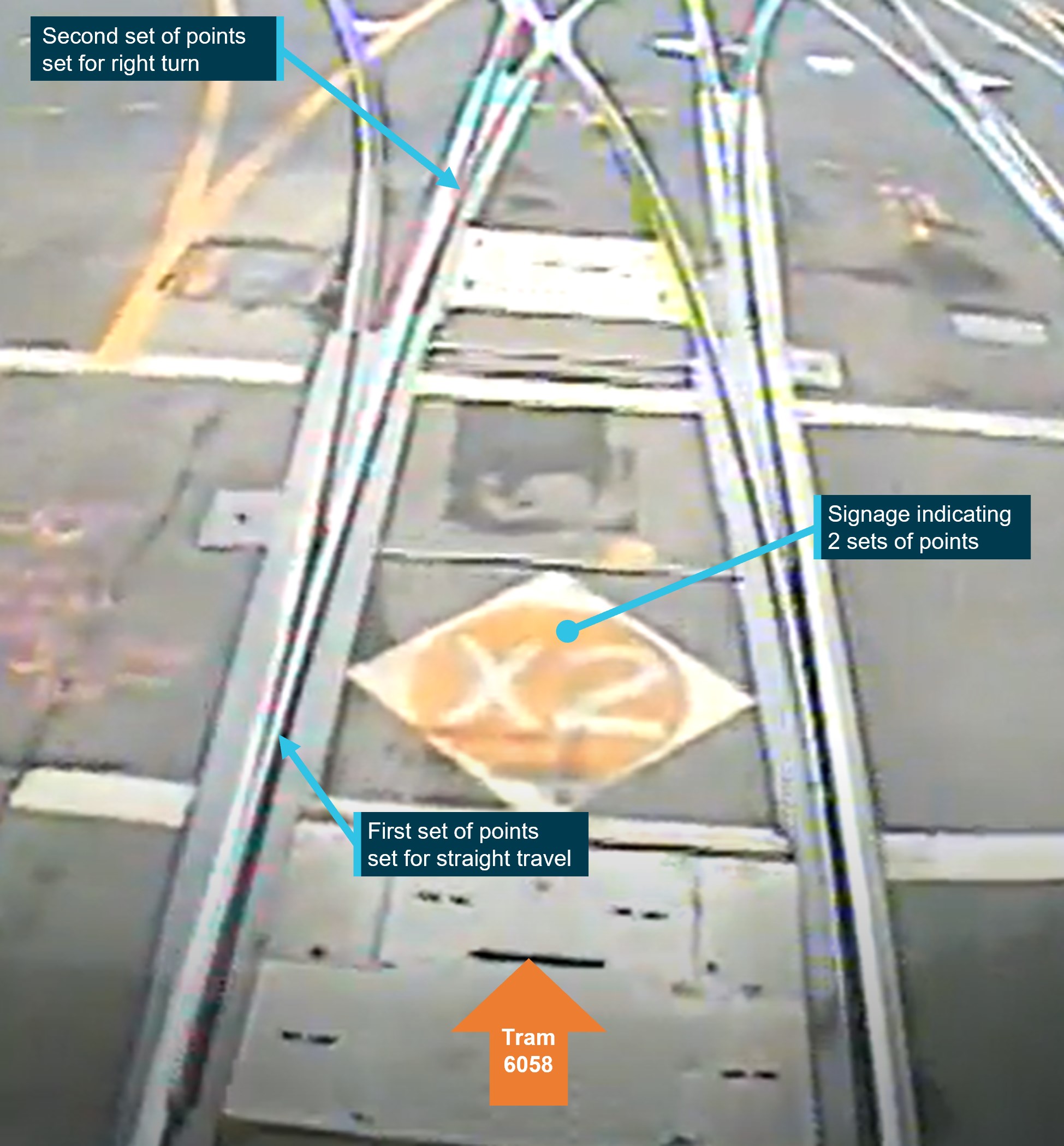
Tram 6058 had travelled through 2 sets of points. The first set of points were set for the straight, and the second set of points were set for the right turn (Figure 3).
Figure 3: Image from CCTV footage showing the settings of the 2 sets of points
Source: Yarra Trams (tram 6058 CCTV) annotated by the Office of the Chief Investigator Transport Safety.
Each tram was travelling at about 20 km/h at the time of the collision. The driver of tram 6062 and 5 passengers sustained minor injuries. Both trams derailed and sustained considerable damage to their front and right-hand panels (Figure 4).
Figure 4: Damage to tram 6058 and tram 6062
Source: Office of the Chief Investigator Transport Safety.
Context
Management of the tram network
Yarra Trams[1] was the accredited operator of the Melbourne tram network and was responsible for the operation and maintenance of rolling stock and network infrastructure. Network infrastructure was leased to Yarra Trams by the Department of Transport and Planning on behalf of the Victoria State Government.[2]
Trams
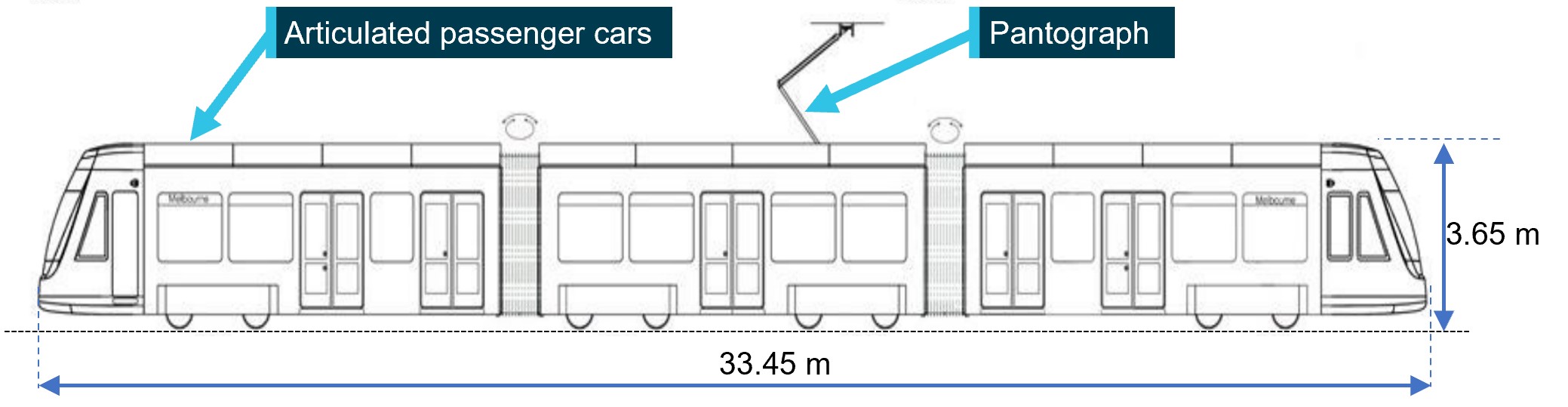
Trams 6058 and 6062 were both E2 class trams manufactured by Bombardier Transportation Australia. Each tram was comprised of 3 connected passenger units, giving a total length of about 33 m and a capacity of 64 seated and 146 standing passengers (Figure 5).[3]
Figure 5: The articulated E2 Class tram
Source: Yarra Trams, annotated by the Office of the Chief Investigator, Transport Safety.
Infrastructure
The intersection
Victoria Parade was a dual carriageway with a tram-only thoroughfare between carriageways. Nicholson Street was a two-way single carriageway south of Victoria Parade, and a dual carriageway with a tram-only thoroughfare north of the intersection.
Except for the city-circle service, normal service routes on Nicholson Street and Victoria Parade passed straight through this intersection. Trams on routes 86 and 96 travelled north and south along Nicholson Street, while trams on route 30[4] travelled east and west along Victoria Parade. City circle trams travelling north on Nicholson Street would turn left into Victoria Parade.
There was no scheduled service that required north-travelling trams on Nicholson Street to turn right into Victoria Parade. Trams would only turn right into Victoria Parade if travelling on an amended route or being directed to another location.
Signals
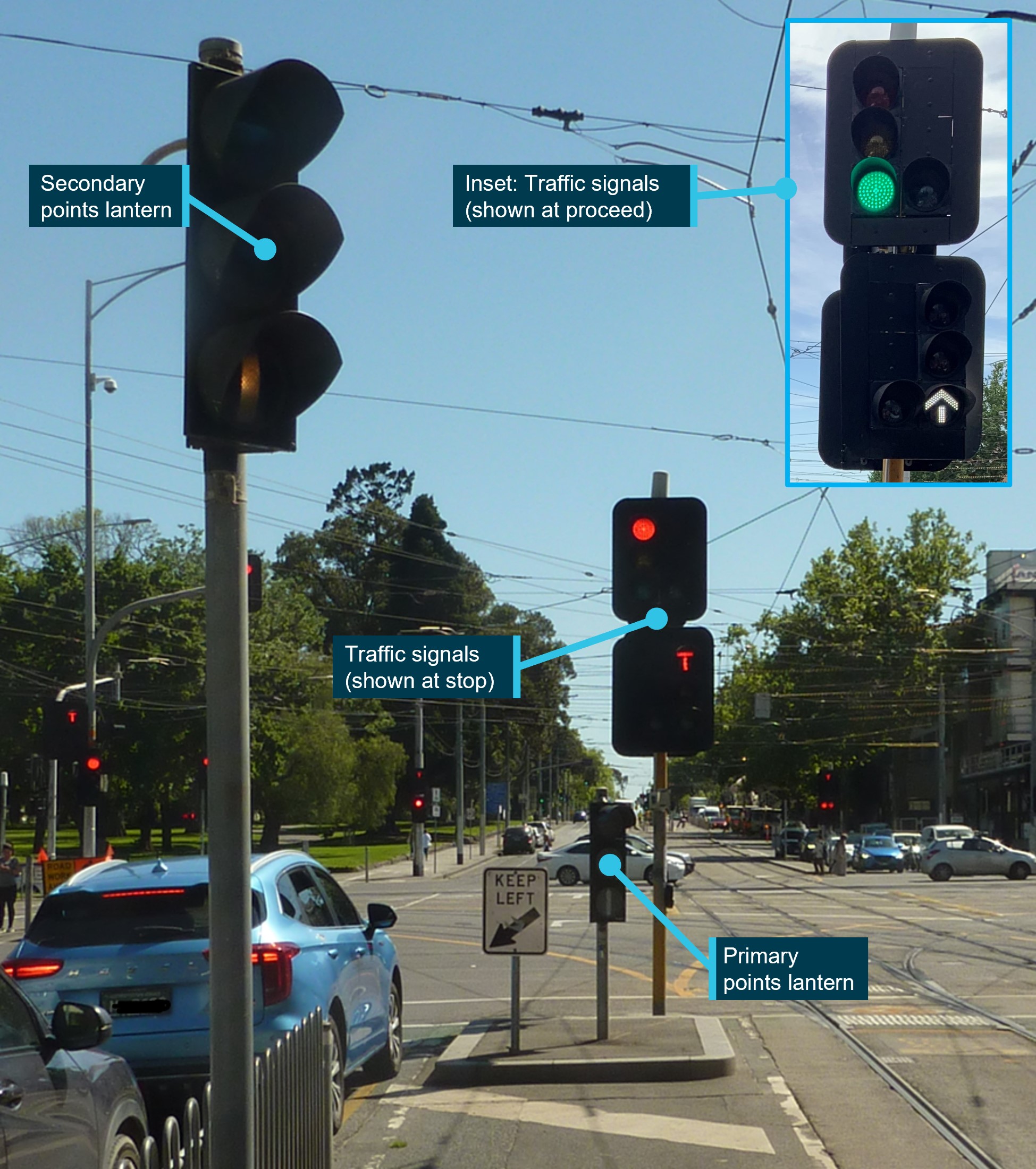
Northbound trams travelling along Nicholson Street were presented with traffic signals and primary and secondary points lanterns (Figure 6). When permitted to proceed straight, northbound trams were presented with a white arrow at 4 locations within the intersection.
Figure 6: Traffic signals at intersection when travelling north on Nicholson Street
This figure does not represent the condition of the points lanterns at various times during the sequence of events for this incident.
Source: Office of the Chief Investigator Transport Safety.
The primary points lantern had 3 lenses with each lens designed to have an unlit (nil) or lit aspect (Figure 7).[5] The central lens had 2 possible lit aspects and could indicate that the points were set to the left or to the right. The secondary points lantern was of the same configuration, however, on the day of the incident its central lens was non-operational.
Figure 7: The primary points lantern and the possible lit aspects of each lens
This figure does not represent the condition of the primary points lantern at various times during the sequence of events for this incident.
Source: Office of the Chief Investigator Transport Safety and Yarra Trams (signal aspects)
In-track equipment and surface markings
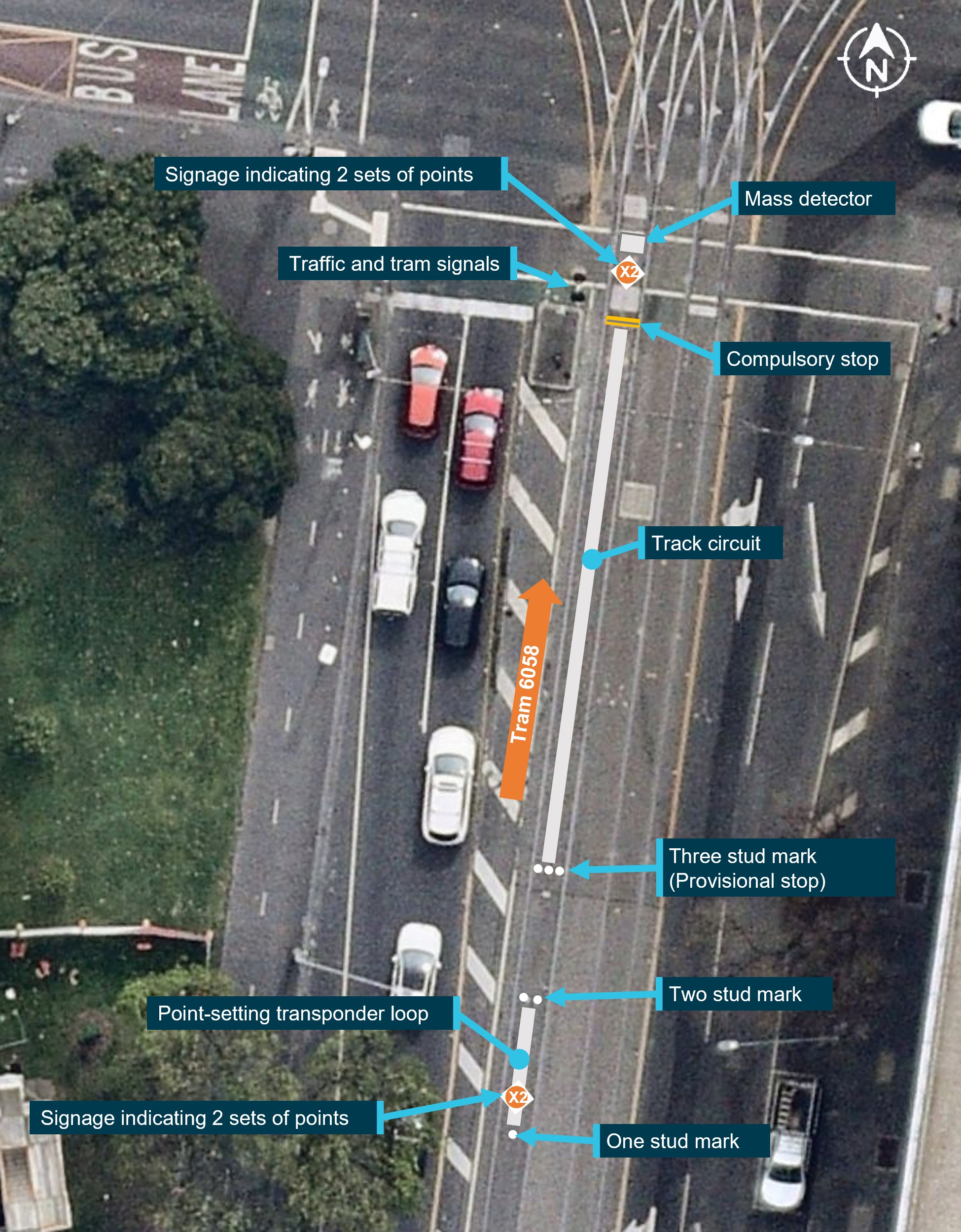
The intersection of Nicholson Street with Victoria Parade was fitted with automatic points. Travelling north on Nicholson Street and approaching the intersection, in-track equipment interfaced with trams to provide input to the operation of points, and on-ground markers provided visual cues to drivers (Figure 8).
Figure 8: Track equipment and markings on Nicholson Street travelling north
Source: Nearmap, annotated by the Office of the Chief Investigator Transport Safety
In-track equipment included (Figure 8):
a points-setting transponder loop located between the 1 and 2-stud marks that was designed to receive a (driver initiated) points-selection transmission from the tram
a track circuit located between the 3-stud mark (provisional stop) and compulsory stop that was designed to detect the presence of the tram and lock the selected points setting in position to protect against a following tram changing the position of the points
a mass detector[6] located past the compulsory stop that was also designed to protect against a change to the points position prior to the tram clearing the points.
Similar occurrence
On 19 November 2023 at about 1711, tram 6030 on route 86 was travelling north on Nicholson Street and approached the Victoria Parade intersection. It followed a tram that had earlier turned right into Victoria Parade. The driver brought the tram to a stop at the intersection and awaited traffic signals to proceed straight, and across, Victoria Parade. However, on the tram proceeding, it followed the points that had been set to the right turn for the previous tram. Realising the tram was off route, the driver immediately brought the tram to a stop without conflict to other trams or road traffic.
Further investigation
To date, investigators from the Office of the Chief Investigator Transport Safety have inspected the investigation site, conducted interviews and continue to collect evidence.
The investigation is continuing and will include the review and examination of:
operation of both trams
the function and operation of tram equipment
the operation of track infrastructure, signalling and traffic management systems
the design and arrangement of infrastructure at the intersection
the management of safety risk associated with trams deviating from their designated route
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Australian Transport Safety Bureau
About the ATSB
The ATSB is an independent Commonwealth Government statutory agency. It is governed by a Commission and is entirely separate from transport regulators, policy makers and service providers.
The ATSB’s purpose is to improve the safety of, and public confidence in, aviation, rail and marine transport through:
independent investigation of transport accidents and other safety occurrences
safety data recording, analysis and research
fostering safety awareness, knowledge and action.
The ATSB is responsible for investigating accidents and other transport safety matters involving civil aviation, marine and rail operations in Australia, as well as participating in overseas investigations involving Australian-registered aircraft and ships. It prioritises investigations that have the potential to deliver the greatest public benefit through improvements to transport safety.
The ATSB performs its functions in accordance with the provisions of the Transport Safety Investigation Act 2003 and Regulations and, where applicable, international agreements.
Rail safety investigations in Victoria
Most transport safety investigations into rail accidents and incidents in Victoria and New South Wales (NSW) are conducted in accordance with the Collaboration Agreement for Rail Safety Investigations and Other Matters between the Commonwealth Government of Australia, the State Government of Victoria, and the State Government of New South Wales. Under the Collaboration Agreement, rail safety investigations are conducted and resourced in Victoria by the Chief Investigator, Transport Safety (CITS) and in New South Wales by the Office of Transport Safety Investigations (OTSI), on behalf of the ATSB, under the provisions of the Transport Safety Investigation Act 2003.
The Chief Investigator, Transport Safety(CITS) is a statutory position established in 2006 to conduct independent, no-blame investigation of transport safety matters in Victoria. CITS has a broad safety remit that includes the investigation of rail (including tram), marine and bus incidents.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available on the ATSB website. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
[1] Yarra Trams was the trading name of the franchisee, Keolis Downer, for the operation of trams in Melbourne.
[2] Infrastructure was owned by the Victorian Rail Track Corporation (VicTrack), a State Government owned enterprise which owns railway and tram infrastructure in Victoria.
[3] The 3-unit E2 class tram was bi-directional and fitted with a driving cabin at each end.
[4] The service between Docklands to St Vincents Plaza.
[5] The aspects of the points lantern are described in the General Rules and Driving Rules, Keolis Downer, February 2017
[6]A subsurface tuned electrical circuit that detected a metal mass such as a tram.
The Australian Transport Safety Bureau has issued a safety advisory after a number of occurrences in which pedestrians were injured by rotor wash around hospital helicopter landing sites.
The notice advises medical transport operators and hospital helicopter landing site operators to engage with one another and ensure local procedures are sufficient to mitigate the risk of rotor wash associated with larger helicopters, such as the Leonardo Helicopters (AgustaWestland) AW139.
It stems from an ATSB Aviation Data and Analysis Report analysis of a series of incidents over the last five years, which considered the common factors, existing regulatory guidelines, and ways to mitigate the effects of rotor wash.
“Of the 18 helicopter rotor wash incidents reported to the ATSB in the last five years, nine occurred at hospital landing sites,” ATSB Director Transport Safety Dr Stuart Godley said.
“Six of those nine occurrences resulted in injuries to pedestrians who were within approximately 30 m of the landing site, and flight crew were not aware of the presence of pedestrians in all cases.
“In fact, in most instances, flight crew were not aware any incident had occurred at the time.”
Significantly, there were no reported occurrences of rotor wash related injuries at hospital HLS prior to the notable increase in the utilisation of AW139 for medical transport operations from 2017.
If the recommended rotor wash exclusion area for the AW139 had been applied at each HLS, it would have reduced the risk of the pedestrians being injured.
The ATSB’s report notes a range of key factors contribute to the effects of rotor wash, including the weight and size of the helicopter, the main rotor size, disc loading, prevailing winds, and flightpath.
“The flightpath is the only element that can be managed by the pilot in accordance with the operator’s procedures,” Dr Godley said.
“But as these occurrences demonstrate, pilots may be unaware of the presence of pedestrians in the vicinity, and therefore be unable to adjust their flightpath accordingly.
“As such, hospital landing site owners and helicopter owners should ensure pedestrians are not affected by rotor wash, by implementing appropriate risk controls for their landing sites, in addition to the helicopter operating procedures.”
Risk controls may include physical barriers, warning devices such as sirens, lights, high visibility warning signs, painted lines on nearby public thoroughfare to alert pedestrians to the rotor wash danger area, an inspection schedule for the landing site facility and surrounding area, and establishing a closed-loop reporting system.
Following several helicopter rotor wash incidents at hospital helicopter landing sites (HLSs) that resulted in injuries to nearby pedestrians, the ATSB compiled a list of similar incidents in the preceding 5 years. Analysis of the specific occurrences was conducted to identify the common factors, existing regulatory guidelines, and ways to mitigate the effect of rotor wash.
What the ATSB found
Of the 18 helicopter downwash incidents reported in the last 5 years, 9 were reported to have occurred at hospital HLSs. Of these, 6 occurrences resulted in injuries to pedestrians that were located within approximately 30 m of the HLS. Flight crew were not aware of the presence of pedestrians in all cases, and most flight crew were not aware of the incident at the time. Most, and possibly all of the injuries were sustained by pedestrians over the age of 75 after being exposed to rotor wash. All incidents involved AgustaWestland AW139 helicopters. If the recommended rotor wash exclusion area had been applied at each HLS, it would have reduced the risk of the pedestrians being injured.
Key factors contributing to the effects of rotor downwash include the weight of the helicopter, the main rotor size, disc loading, prevailing wind, and the flightpath. There were no reported occurrences of rotor wash related injuries at hospital HLS prior to the significant increase in the utilisation of AW139 for medical transport operations from 2017.
As part of Civil Aviation Safety Regulations Part 133 (Australian air transport operations rotorcraft), helicopter operators are required to determine information about aerodromes and determine procedures for safe operations at aerodromes. The Civil Aviation Safety Authority does not currently regulate the design and operation of heliports, including hospital HLSs, where they are not an integral part of an aerodrome certified under Civil Aviation Safety Regulations Part 139 (Aerodromes). This means that the Civil Aviation Safety Authority does not provide any formal approval for, or assurance of, HLS operational standards. The Civil Aviation Safety Authority has produced guidance material for the operators of HLSs to design, maintain, and operate their facility to the standards of certified aerodromes.
What has been done as a result
Helicopter operators involved in these incidents reported taking corrective actions to mitigate the dangers of rotor wash, which included:
immediate cessation of operations to the HLS
selection of an alternate landing area
removal of hazards in the vicinity of the HLS
operational restrictions including the number of helicopters permitted on the HLS at one time and restrictions on flightpaths used during approach and departure
marshallers put in place for arrival and departure times.
The ATSB has issued the following Safety Advisory Notice (AD-2022-001-SAN-001) with this report:
The Australian Transport Safety Bureau strongly encourages operators of hospital helicopter landing sites, and helicopter medical transport operators using those landing sites, work together to review the adequacy of existing risk controls to ensure pedestrians are adequately protected from the increased rotor wash associated with larger helicopters.
Safety message
From the identified common factors associated with rotor wash incidents, the flightpath is the only element that can be managed by the pilot in accordance with the operator’s procedures. However, pilots may be unaware of the presence of pedestrians in the vicinity of a hospital HLS. To enable the continued safe use of these facilities, hospital HLS owners and helicopter operators should ensure pedestrians are not affected by rotor wash by implementing appropriate risk controls for their HLS in addition to the helicopter operating procedures. Controls may include physical barriers, warning devices such as sirens, lights, high visibility warning signs, painted lines on nearby public thoroughfare to alert pedestrians to the rotor wash danger area, an inspection schedule for the HLS facility and surrounding area, and establishing a closed-loop reporting system.
Following several incidents at hospital helicopter landing sites (HLSs) involving injuries to nearby pedestrians from helicopter rotor wash, the ATSB initiated a review of the number and type of helicopter downwash occurrences from 2018 to 2022. The following analysis of the specific occurrences was conducted to identify the common factors, existing regulatory guidelines, and ways to mitigate the effects of rotor wash.
Rotor wash is comprised of downwash, which is the vertical component of rotor wash produced by the main rotor blades that supports the helicopter in flight, and sidewash, which is the horizontal component of rotor wash. It is influenced by environmental conditions such as air density, temperature, and altitude. However, the key factors that determine the strength of rotor wash include:
weight of the helicopter – a heavier helicopter generally produces higher downwash speeds
main rotor size – a larger rotor disc area will lower the downwash speed but a larger rotor disc is usually associated with heavier helicopters that produce higher downwash speeds
disc loading – how much weight is being carried per unit area of the rotor blades
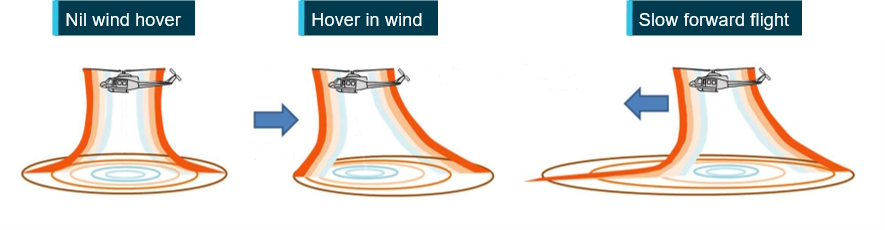
wind – the relative wind influences the movement of the rotor wash (Figure 1)
flightpath – rotor wash is concentrated underneath the helicopter as illustrated in Figure 1.
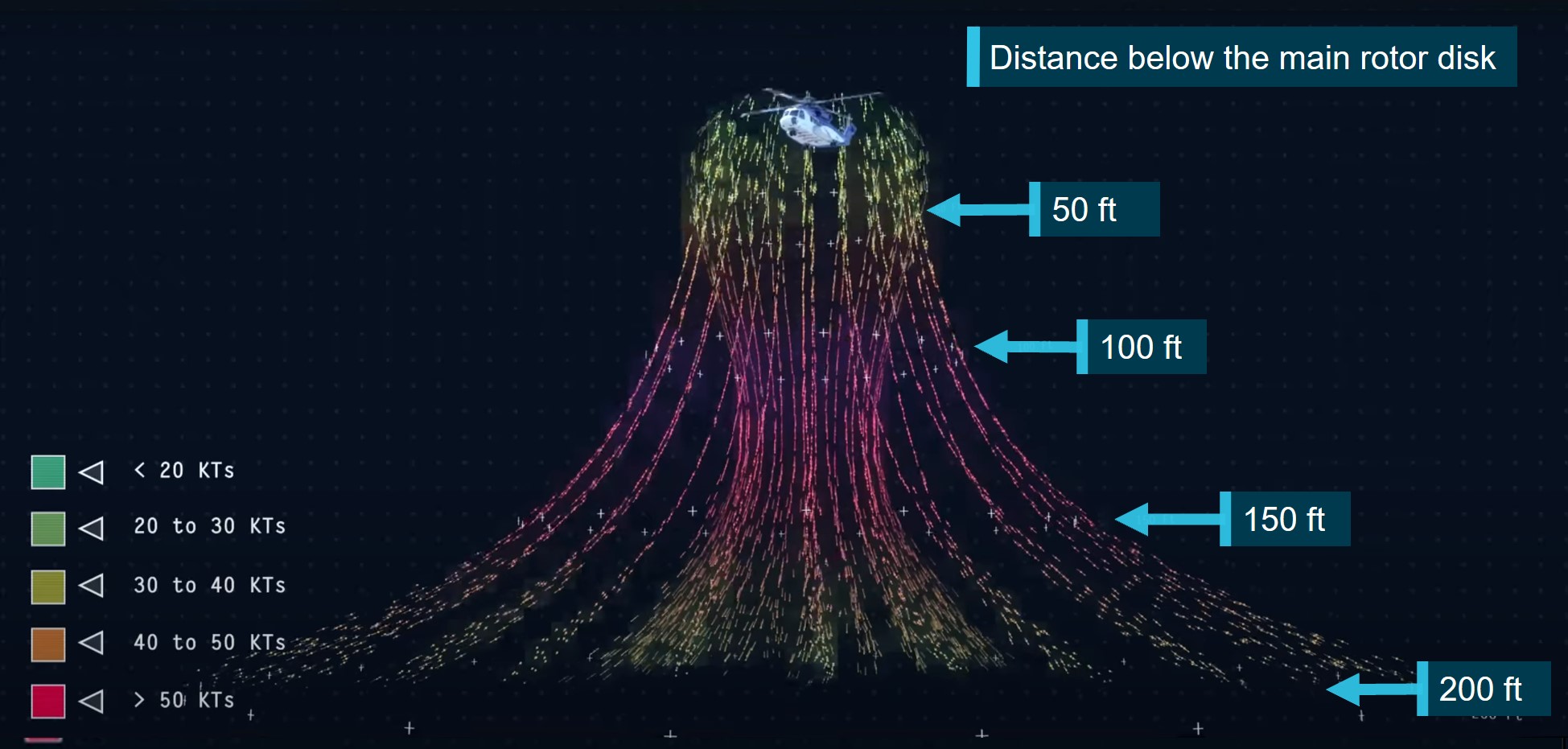
Mathematical modelling of rotor wash adjusted for the effects of open rotor flow from the main rotor blades by Airbus (2021) determined the highest velocity of this stream of air occurs from 1 to 3 rotor diameters below the rotor blades directly beneath the helicopter. Beyond this distance the high velocity airflow dissipates due to turbulence. Figure 2 is a British Petroleum model of the downwash velocities over a 200 ft vertical profile for a Sikorsky S92 helicopter. As the airflow comes under the influence of the terrain or a structure, there is a directional change and acceleration of the airflow as it transitions into sidewash as illustrated in Figure 3. Due to helicopter power requirements and the influence from the ground, rotor wash effects are most pronounced during hover, take-off, and landing where it can produce localised wind strengths greater than 100 km/h. The following figures show the rotor wash velocity in knots and a conversion table for km/h is provided at Appendix 1: Conversion tables.
Figure 2: Downwash profile of a Sikorsky S92 helicopter over 200 ft
Source: British Petroleum annotated by the ATSB
Figure 3: Sidewash profile of a Sikorsky S92 helicopter
Source: British Petroleum
Many HLSs are located inside airports at ground level, isolated from people and structures. However, hospital HLSs are often located in built-up areas or at existing hospital facilities where space permits. In Australia, they are built on the top of high-rise hospital buildings, in carparks, in public ovals and above public roads as illustrated at Appendix 3: Area of consideration. Therefore, a hospital HLS may be in an area that exposes the public to the risk of being struck by rotor wash or struck by objects propelled or dislodged by rotor wash.
The effect of rotor wash on people has been the subject of several studies, with most agreeing that 80 km/h winds represent conditions that are ‘unsuitable for walking’, and 60 km/h winds are at the ‘threshold of danger’ for the average population (Jordan and others 2008). Jordan and others (2008) also considered the effect of rotor wash on the more vulnerable groups of the population and found that in people over the age of 50, roughly half were displaced by a gust of 40 km/h. Consequently, the International Civil Aviation Organization (ICAO) heliport design work group have been working on an amendment to Document 9261 – Heliport Manual, that will incorporate a 40 km/h rotor wash speed guidance into the document.[1]
Occurrence data
Introduction
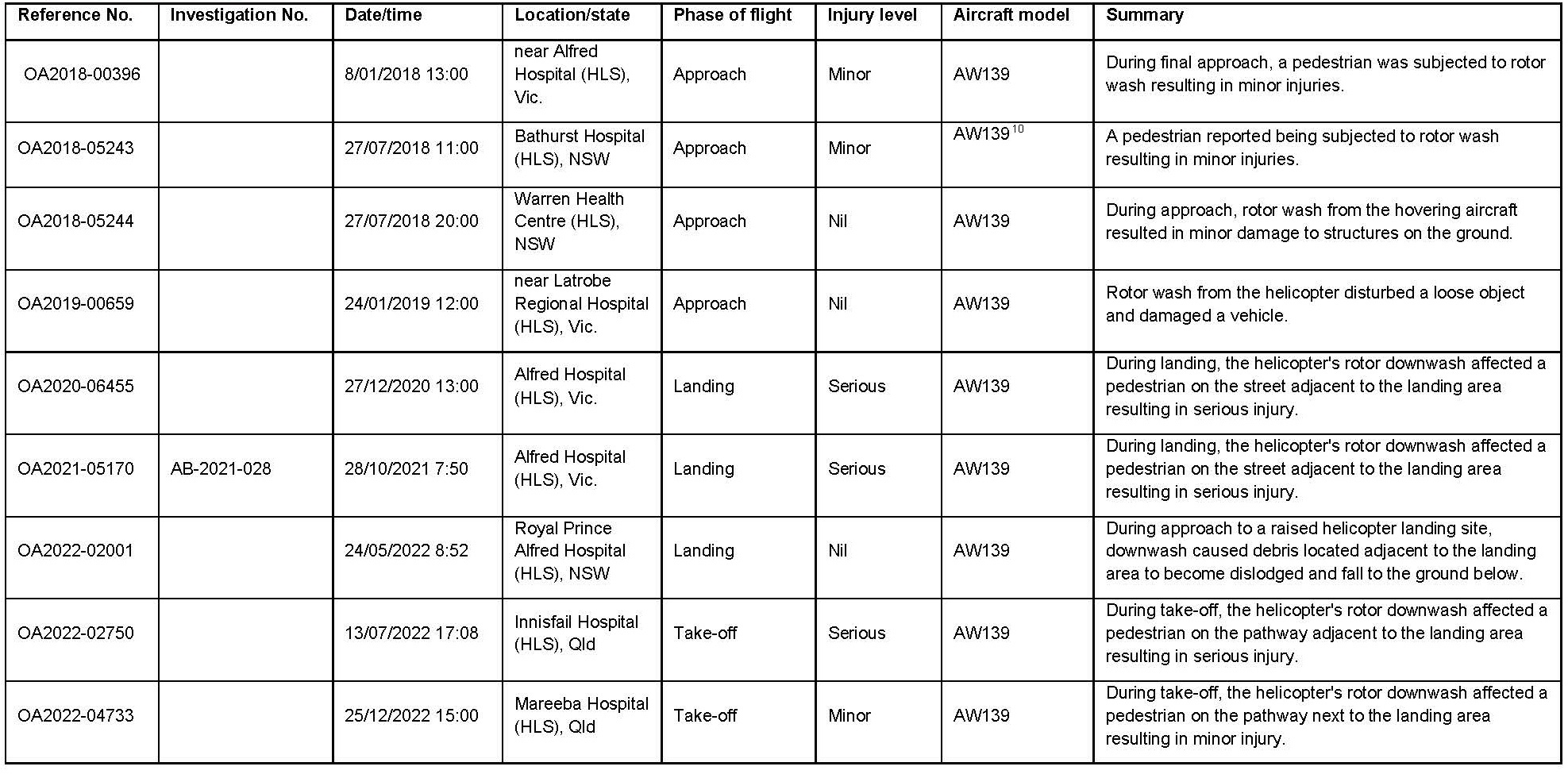
A review of the ATSB National Aviation Occurrence Database found 18 helicopter rotor wash occurrences were reported between 2018 and 2022. Of these 18 occurrences, 9 were in the immediate vicinity of a hospital HLS. A summary of each of the 9 occurrences is provided in the following section and the occurrence data is available at Appendix 2: Occurrence data.
Of the 9 rotor wash occurrences at hospital HLS:
6 resulted in injuries, 3 resulted in serious injuries and 3 resulted in minor injuries
3 resulted in damage to third party property caused by debris.
Occurrences
ATSB occurrence OA2018-00396
On 8 January 2018 at about 1300 local time, an elderly pedestrian was walking along the footpath adjacent to the Alfred Hospital HLS, Victoria, as an AgustaWestland AW139 helicopter was on approach to land. The helicopter passed overhead the pedestrian and the rotor wash was reported to have blown the pedestrian across the path and into a wall. The pedestrian sustained minor injuries (bruising) and reported they were unaware of the possible strength of the rotor wash.
ATSB occurrence OA2018-05243
On 27 July 2018 at about 1100 local time, an AgustaWestland AW139 helicopter was on approach to land at the rooftop HLS at Bathurst hospital, New South Wales. As it passed over the corner of a carpark, a pedestrian was blown over sustaining minor injuries. This HLS was situated 4 stories above ground level. The height of the helicopter during the final approach would have been consistent with the height below the main rotor disc where the strongest downwash velocities would be experienced as described by Airbus Helicopters (2021) and illustrated with Figure 2.
ATSB occurrence OA2018-05244
On 27 July 2018 at about 2000 local time, the crew of an AgustaWestland AW139 was conducting a visual approach on night vision goggles to the Health Centre HLS in Warren, New South Wales. The crew conducted a straight in approach from the east, which involved overflying a nearby caravan park. As the helicopter approached the HLS, the crew detected a large flock of birds take-flight near the HLS and entered a hover. The crew maintained the hover at 200 ft above ground level for approximately 2 minutes to allow the birds to disperse. During this time, rotor wash was reported to have affected the trees in the caravan park below, with falling branches causing minor damage to caravan park buildings and equipment.
ATSB occurrence OA2019-00659
On 24 January 2019 at about 1200 local time, an AgustaWestland AW139 was on approach to land at the Latrobe Regional Hospital, Victoria. Rotor wash from the helicopter blew a traffic barricade into the side of a vehicle parked nearby. The vehicle sustained minor damage.
ATSB occurrence OA2020-06455
On 27 December 2020 at about 1300 local time, a pedestrian was walking along the footpath adjacent to the Alfred Hospital HLS as an AgustaWestland AW139 helicopter was on approach to land. The crew altered their approach to account for the 35-knot wind on the day by tracking along the nearby park before turning towards the HLS on late final (Figure 4). As the helicopter approached the HLS, the pedestrian was blown over and sustained a broken sacrum.
On 28 October 2021 at about 1550 local time, an AgustaWestland AW139 conducted an approach to land at the Alfred Hospital HLS. The crew approached the helipad from the west, using a steep approach profile aligned with Commercial Road. As the helicopter passed overhead a pedestrian walking on the footpath about 30 m west of the HLS,[2] the pedestrian was blown over by the rotor wash and sustained serious injuries (broken bones) (Occurrence Brief AB-2021-02).
ATSB occurrence OA2022-02001
On 24 May 2022 at about 0852 local time, an AgustaWestland AW139 was on approach to the Royal Prince Alfred Hospital, NSW. During approach to the elevated HLS, the doctor onboard observed a large piece of cloth blown up behind the helicopter. Further investigation revealed that multiple lengths of shade cloth, held in place by bricks, had been dislodged by the rotor wash. It was later discovered that some of the bricks used to retain the lengths of cloth had fallen 300 ft to the ground below, with one brick found in a café and another found in an area of the hospital grounds open to the public.
ATSB occurrence OA2022-02750
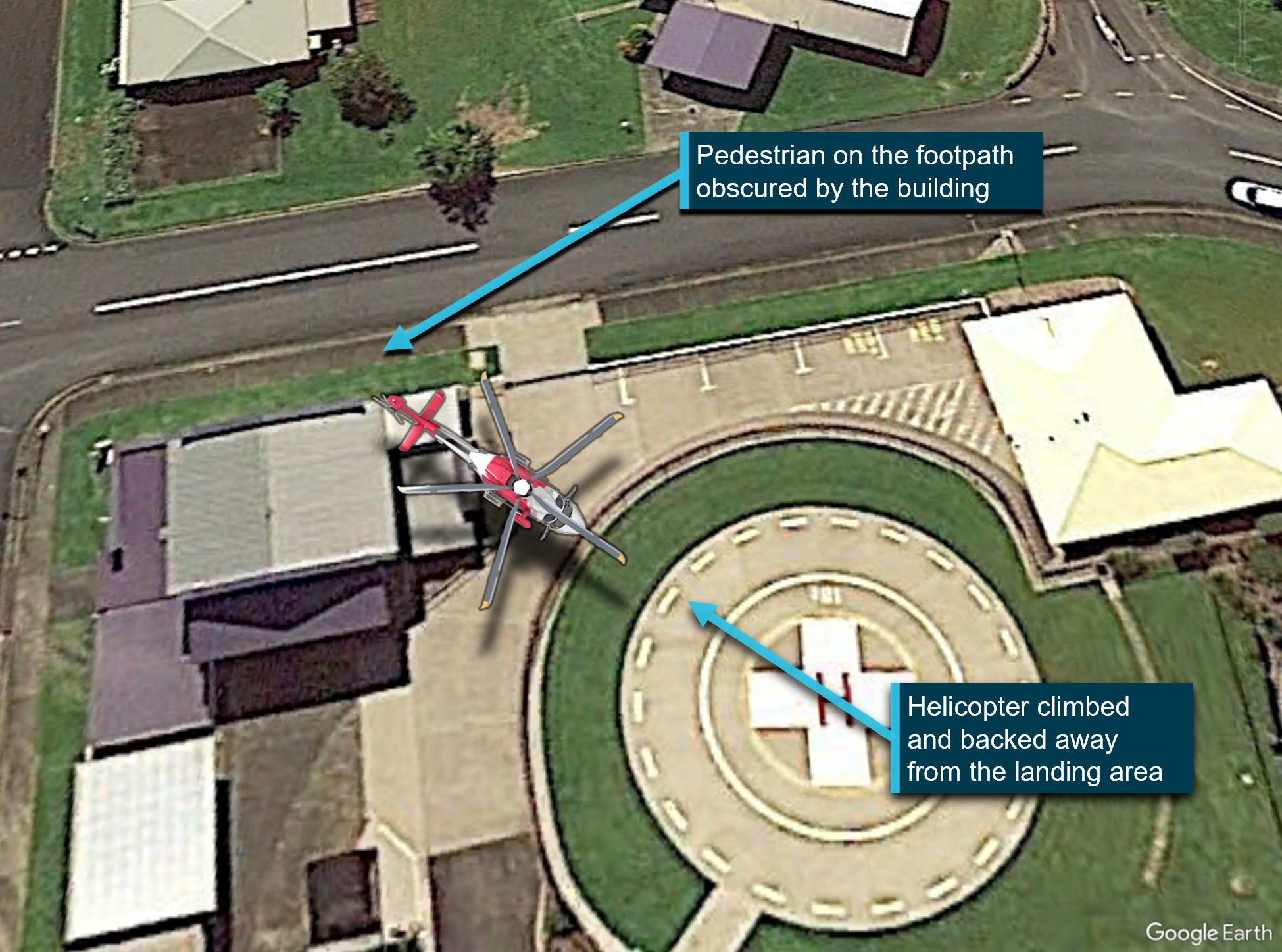
On 17 July 2022 at about 1708 local time, an AgustaWestland AW139 helicopter departed from the Innisfail Hospital HLS, Queensland. The standard departure required the helicopter to climb vertically and back away from the helipad slightly so the pilot could keep the landing area in sight in case of an abort before flying away (Figure 5). As the helicopter backed over the top of a hospital building towards the nearby roadway, a pedestrian walking on the adjacent footpath was blown over and sustained a serious head injury. The pedestrian was not visible to the crew from the helipad.
Figure 5: Approximate flight path based on operator report
Source: Google Earth annotated by the ATSB
ATSB occurrence OA2022-04733
On 25 December 2022 at about 1500 local time, the crew of an AgustaWestland AW139 commenced a take-off from the Mareeba Hospital HLS, Queensland. An elderly patient of the hospital was walking in the hospital grounds at the time and as the aircraft lifted into a low-level hover, they were blown over by the rotor wash. The patient fell to the ground and sustained minor head injuries. The crew observed the patient fall and aborted the take-off.
Medical helicopter operations and size
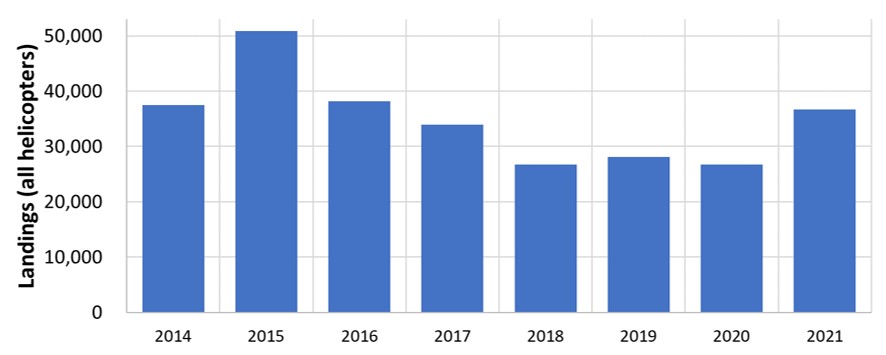
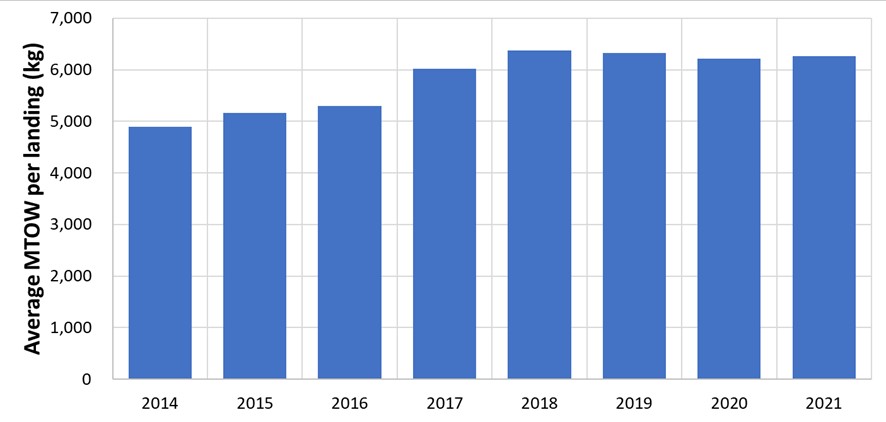
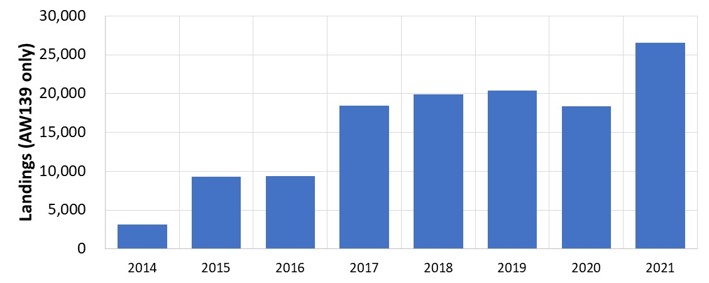
Analysis of medical transport operations (MTO) helicopter movements, from data obtained from the Bureau of Infrastructure and Transport Research Economics, indicates that the number of landings per year (Figure 6) remained relatively constant from 2014 through to 2021.
Figure 6: Number of medical transport landings 2014-21
Source: Bureau of Infrastructure and Transport Research Economics
Figure 8: Number of AW139 medical transport landing 2014-21
Source: Bureau of Infrastructure and Transport Research Economics
Common factors
Helicopter emergency medical service operations often involve time critical missions that require the crew to utilise landing areas within the grounds of hospitals. Analysis of the 9 identified occurrences found the following common factors:
most incident crews were unaware of the incident at the time of occurrence
there were no references to established rotor wash danger or exclusion areas[3]
in 5 out of the 6 injury-related events, the pedestrians age was reported to be 75 or greater, and in the 6th event, the pedestrian was reported to be using a walker
where the locations of injured pedestrians were reported, they were outside the HLS perimeter fence but within 30 m of the final approach and take‑off area (FATO) .[4]
In addition to the increase in helicopter mass, the capability of the AW139 permitted a greater number of vertical, backup, or lateral transition take-off and approach and landing options to the flight crew. The different ways the aircraft could be flown may have also been a contributing factor to the increase in rotor wash occurrences but could not be determined from the occurrence database.
Regulatory oversight and guidance
Australia
The Civil Aviation Safety Authority (CASA) does not regulate the design or operation of HLSs if they are not an integral element of an aerodrome certified under Part 139 of the Civil Aviation Safety Regulations (CASR) 1998. As hospital HLSs are not located at Part 139 certified aerodromes, CASA does not regulate their design or operation. In accordance with CASA Advisory Circular (AC) 139.R-01 v1.0 – Guidelines for Heliports – design and operation(Opens in a new tab/window), a HLS is an aerodrome intended to be used wholly or in part for the arrival, departure, and surface movement of helicopters and therefore, references to an aerodrome in this section below includes hospital HLSs.
Helicopters operating into and out of hospitals are generally medical transport operations. Medical transport operations (MTO) fall into the air transport rule set under CASR Part 133 – Australian air transport operations–rotorcraft. CASA advised the ATSB:
Part 133 requires the MTO operators to include in their exposition via regulation 133.170 of CASR procedures to determine information about aerodromes and via regulation 133.175 of CASR procedures for safety at aerodromes.
CASR 133.170 requires the MTO operator’s exposition to include information on the final approach and take‑off area (FATO) dimensions and directions for the pilot-in-command. This includes any limitations, special procedures, and restrictions the operator requires the flight crew to use at the aerodrome.
CASR 133.175 stated an operator’s procedures must include measures to ensure the safety of persons in the vicinity of the rotorcraft. The requirement to consider the effects of rotor wash is mentioned in part (b):
(b) procedures to determine the minimum distance that a person, animal or thing must be kept from the following to ensure the safety of the person, animal or thing:
(i) the rotorcraft while it is on the ground at an aerodrome with its rotors turning;
(ii) the movement area of an aerodrome while the rotorcraft is landing or taking off;
(iii) a hazard created by the downwash of the rotorcraft at an aerodrome.
In reference to CASR 133.175, CASA stated:
The assumption is these procedures and distances would also be communicated to any person responsible at a HLS location for third party person and property risk control measures, otherwise the operator would not be able to operate to the location and comply with their exposition.
the FATO and touchdown and lift-off area (TLOF)[6] are clear of all objects and animals likely to be a hazard to the helicopter, other than objects essential to the helicopter operation
no person is within 30 m of the closest point of a hovering or taxiing helicopter, other than persons who are essential to the safe conduct of the operation or the specific nature of the task and who are trained and competent in helicopter operational safety procedures
appropriate information from the owners and authorities is obtained to confirm the suitability of the HLS for the proposed operation.
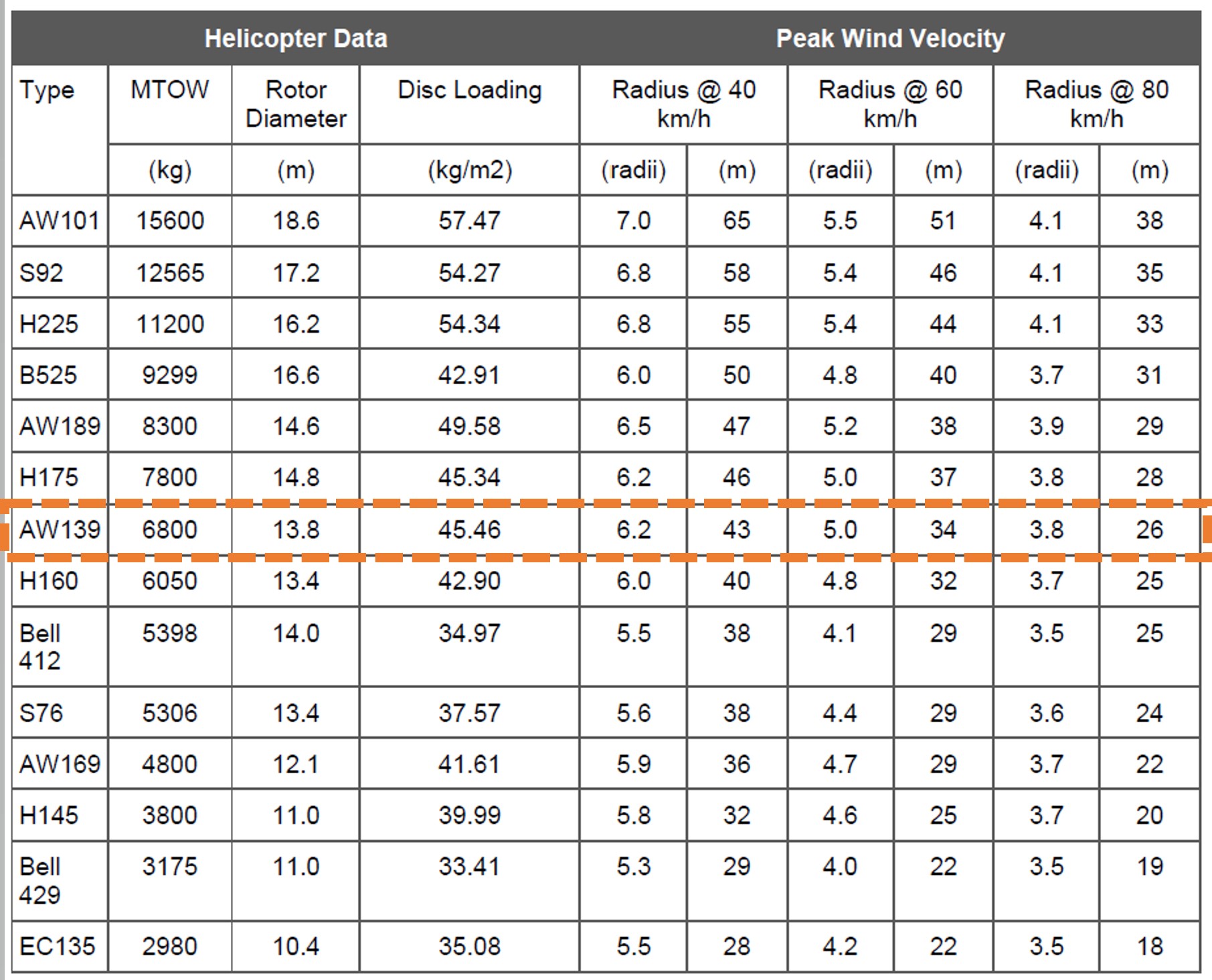
Data on rotor wash speeds has been incorporated into CASA AC 139.R-01 v1.0(Figure 9) and shows the distance from the centre of the helipad that rotor wash velocities of 40, 60 and 80 km/h can be expected for common helicopter types. The data is expressed both as a distance in metres, and as multiples of the main rotor disc radius. Figure 9 indicates that the associated strength of rotor wash increases with increased helicopter weight (MTOW). The AgustaWestland AW139, involved in all 9 rotor wash incidents described above, is highlighted and shows that beyond the recommended 30 m non-essential person exclusion area, rotor wash velocities can be expected to be between 60 and 80 km/h.
The ATSB contacted several foreign regulatory bodies to determine the oversight of hospital HLSs outside Australia. Responses were received from the United Kingdom Civil Aviation Authority (UK CAA) and Transport Canada. In addition, the guidance from the United States Federal Aviation Administration was reviewed. At the time of drafting this report the UK Air Accidents Investigation Branch had an active investigation into a fatality at the Derriford Hospital HLS, Plymouth, from a Sikorsky S92 helicopter rotor wash.
United Kingdom Civil Aviation Authority
The UK CAA advised the ATSB that every helicopter operator is responsible for approving a HLS and principal oversight by the CAA is through the review and acceptance of each operator’s operations manual landing site directory. They reported that where an elevated helipad is intended for use at night, a check flight will be conducted with the primary operator and thereafter cleared for other operators who will include it in their own landing site directory.
Hospital HLSs are not currently licensed in the UK and, with the emphasis in the Air Navigation Order (ANO) on licensing heliports only where scheduled public transport operations occur, there are only a handful of licensed heliports in the UK. New hospital HLS builds in the UK, since 2016, have been designed to the standards of UK Civil Aviation Publication (CAP) 1264 – Standards for helicopter landing areas at hospitals(Opens in a new tab/window), which incorporates sections on downwash guidance. Several recent new build HLSs, to meet a condition of their local planning authority process, have incorporated a downwash study at the pre-application stage, which takes account of the impact of rotor downwash on persons and property. However, this has been adopted by some projects as a good practice rather than as a regulatory requirement. At the time of publishing this report, it was reported that the UK CAA was poised for a further review of CAP 1264, including downwash guidance, pending the release of a final investigation report into a fatality at Derriford Hospital due to main rotor downwash from a helicopter arriving at the hospital HLS.
Utilising consultancy arrangements via their subsidiary organisation CAA International Limited, UK CAA offers a service to provide support to Hospital HLS new builds and refurbishments by undertaking feasibility studies and providing advice and support to National Health Service Trusts and their sub-contractors. CAA is currently rolling out Hospital Helipad Training Aviation Awareness courses for the benefit of Hospital HLS operational staff.
Transport Canada
Transport Canada advised that the requirement for certification is predicated in most cases on the location of the heliport being within the built-up area of a city or town, as mandated under Part 305(Opens in a new tab/window) of the Canadian Aviation Regulations 1996. Hospital HLSs may or may not meet this requirement. HLSs which are not required to be certified and whose operators wish to have the aerodrome registered and the information published in the Canada Flight Supplement, will fall under Canadian Aviation Regulation Part 301(Opens in a new tab/window), with respect to the location, markings, lighting, use and operation of the aerodrome. This differed from the available Australian guidance in that Canadian hospital HLS operators, who elected to comply with the Canadian Aviation Regulations, were required to ensure that certain minimum safety considerations were met.
Canadian Aviation Regulation 301.03(2) stated:
The Minister may refuse to register an aerodrome where the operator of the aerodrome does not meet the requirements of sections 301.05 to 301.09 [concerning warning notices, wind direction indicator, lighting, prohibitions, fire preventions] or where using the aerodrome is likely to be hazardous to aviation safety and, in such a case, shall not publish information with respect to that aerodrome.
Canadian Aviation Regulation 301.05 identified the following HLS operator responsibilities with regards to warning notices:
Where low-flying or taxiing aircraft at or in the vicinity of an aerodrome are likely to be hazardous to pedestrian or vehicular traffic, the operator of the aerodrome shall immediately:
(a) post notices warning of the hazard on any public way that is adjacent to the manoeuvring area; or
(b) where such a public way is not owned or controlled by the operator, inform the authorities responsible for placing markings on the public way that there is a hazard.
United States Federal Aviation Administration
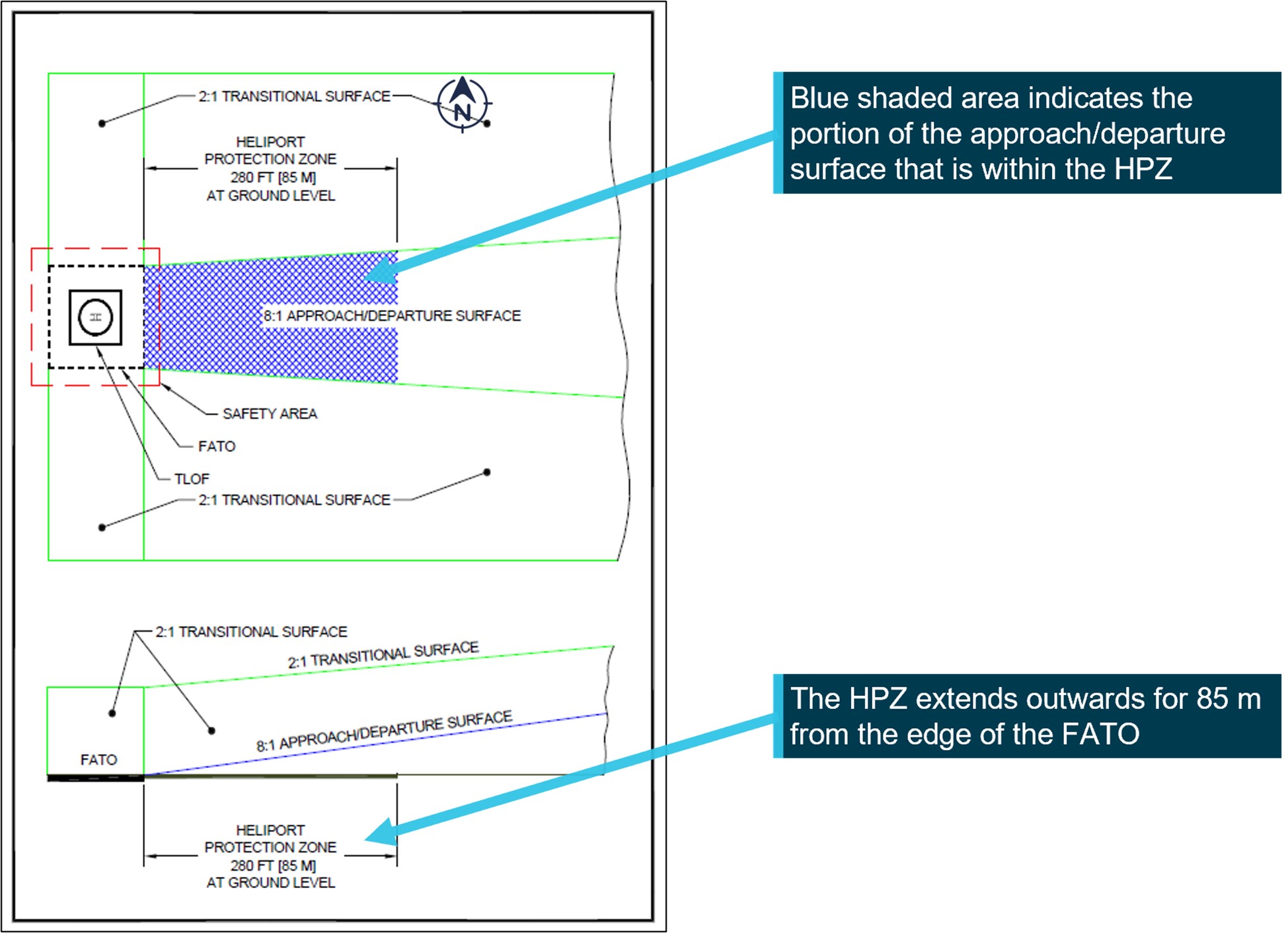
In the United States, the Federal Aviation Administration AC 150/5390-2D(Opens in a new tab/window) for heliport design recommended the establishment of a heliport protection zone (HPZ) for each approach/departure surface as illustrated in Figure 10. Starting at the edge of the FATO, the HPZ extends outwards underneath the flight path for 280 ft (85 m).
The HPZ is intended to enhance protection of people and property on the ground. This is achieved through heliport owner control over the HPZ. Such control includes clearing HPZ areas (and maintaining them clear) of incompatible objects and activities.
Source: United States Federal Aviation Administration
Managing the risk of rotor downwash at hospital HLS
Introduction
The recent increase in rotor wash incidents does not suggest that hospital HLSs are more dangerous now than they were previously, rather, the risk mitigation measures employed for previous generations of MTO helicopters are likely inadequate in managing the rotor wash hazard produced by the current generation of heavier MTO helicopters. The regulatory standards and guidance published by CASA indicate there is a shared responsibility between the HLS operator, the MTO operator, and the pilot-in-command for the safe conduct of operations to a hospital HLS.
Areas where the strength of rotor wash should be considered by hospital HLS operators, who want to comply with the Part 139 standards, should include:
public areas where pedestrians are likely to be walking
public roads and vehicle access areas
areas that contain unrestrained objects that could be propelled by rotor wash
buildings and other structures that may cause channelling and turbulence of the rotor wash.
Where the specifications cannot be met, CASA AC 139.R-01 recommends a risk assessment is conducted to identify any alternative mitigation measures to achieve an acceptable level of safety of helicopter operations at the HLS.
Understanding the risk
Where the locations of injured pedestrians were reported, they were outside the HLS perimeter fence but within 30 m of the FATO and inside the area CASA AC 91-29 recommended be kept clear of non-essential pedestrians. If the recommended rotor wash exclusion area had been applied at each HLS, it would have reduced the risk of the pedestrians being injured. However, based on the latest guidance published by CASA in AC 139.R-01 v1.0, and the research by Jordan and others (2008), the hazards associated with rotor wash at a hospital HLS should be considered further than 30 m, out to the 40 km/h rotor wash radius, to prevent injury to the elderly and vulnerable. For a HLS constructed at surface level, the distances published by CASA indicate the danger area[7]. However, for an elevated HLS, or HLS in the vicinity of structures, a rotor wash analysis should be considered to understand the nature of the risk. This can be explored with anemometers and wind vanes or with computational fluid dynamics to produce a plot of the HLS rotor wash danger area in accordance with the approach and departure flight paths for the design helicopter.[8]
Risk controls
While it is the responsibility of the HLS operator and MTO operator to identify what controls are necessary for safe operations, some generic risk controls for consideration may include an exclusion area, physical barriers, active controls, passive controls, MTO operating procedures, inspections, and a hazard reporting and tracking system as follows:
A HLS exclusion area should be in accordance with the danger area for the design helicopter as published in AC 139.R-01 v1.0, or as determined by a plot of the HLS rotor wash danger area. If this is not feasible, then an alternative strategy may need to be evaluated. Examples of hospital HLS sites in Appendix 3: Area of consideration are based on the guidance for an AgustaWestland AW139 as per Figure 11 below, which recommends an exclusion area based on a 66 m radius.
Physical barriers, such as fences and covered walkways, designed as safety barriers and/or security barriers to prevent inadvertent entry to the HLS, can provide protection to pedestrians and property from rotor wash.
Active controls can be used during helicopter operations to alert pedestrians in or near the danger area with warning lights and alarms as per Figure 12. Marshallers can be employed to restrict pedestrian access during helicopter operations.
Passive controls should include warning signs and painted/marked paths to indicate the helicopter operations danger area to the public (Transportation Research Board, 2013).
An inspection schedule can identify and secure or remove loose objects and verify the condition and serviceability of the other controls, such as the signs and barriers.
Operating procedures in accordance with CASR 133.170, should include the approved approach and departure flight paths, alternate landing sites, and the location of the danger areas for pedestrians, so flight crew can make informed decisions.
A closed-loop reporting system should be available for flight crew to alert the MTO operator and HLS operator to hazards for tracking through to closure, including any temporary or permanent controls implemented to reduce the risk.
Figure 11: HLS rotor wash regions of consideration for an AgustaWestland AW139[9]
Source: ATSB
Figure 12: HLS warning device (left) and sign (right)
Source: alamy.com
Safety action
Safety advisory notice to helicopter medical transport operators and hospital helicopter landing site operators
The Australian Transport Safety Bureau strongly encourages operators of hospital helicopter landing sites, and helicopter medical transport operators using those landing sites, work together to review the adequacy of existing risk controls to ensure pedestrians are adequately protected from the increased rotor wash associated with larger helicopters.
Sources and submissions
Sources
Civil Aviation Safety Authority
Transport Canada
United Kingdom Civil Aviation Authority
References
Airbus Helicopters (2021). Safety Promotion Notice No. 3684-P-00 Noise and downwash considerations for ground operators. Airbus Helicopters
Civil Aviation Safety Authority (2022). Advisory Circular AC 91-29 v1.1 Guidance for helicopters – suitable places to take-off and land. Civil Aviation Safety Authority.
Civil Aviation Safety Authority (2022). Advisory Circular AC 139.R-01 v1.0 Guideline for heliports – design and operation. Civil Aviation Safety Authority.
Civil Aviation Safety Authority (2019). Part 139 (Aerodromes) Manual of Standards. Australian Government.
Federal Aviation Administration (2012). Advisory Circular AC 150/5390-2C–Heliport design Federal Aviation Administration.
International Civil Aviation Organisation (2021). Document 9261:Heliport manual. International Civil Aviation Organisation.
Jordan, S. C., Johnson T., Sterling M., and Baker, C. J. (2008) Evaluating and Modelling the Response of an Individual to a Sudden Change in Wind Speed, Building and environment, Vol. 43.
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
United Kingdom Civil Aviation Authority
Transport Canada
Federal Aviation Administration
Submissions were received from:
Civil Aviation Safety Authority
United Kingdom Civil Aviation Authority
Transport Canada
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendix 1: Conversion tables
Table 1: Knots to kilometres per hour conversion table
kt
km/h
1
1.852
10
18.5
20
37.0
30
55.6
40
74.1
50
92.6
Table 2: Kilometres per hour to knots conversion table
Adapted from the guidance in AC 139.R-01. All images show a 66 m radius circle indicating the area that CASA recommended was kept clear of all loose objects and non-essential people.
Source: Google Earth annotated by the ATSB
[1] International Civil Aviation Organization Heliport design work group virtual seminar on the design and operation of heliports to provide States with updated tools based on the new amendments to Annex 14 Vol. II, updated ICAO guidance documents; and awareness of new measures.
[2]While AB-2021-028 reported this distance as 50 m west of the HLS, analysis of the details provided found that it was approximately 30 m from the HLS.
[3] Exclusion area: Term used to refer to an area from which non-essential personnel should be kept clear in accordance with AC 91-29 v1.1 and AC 139.R-01 v1.0.
[4] FATO: Final approach and take-off area. For the operation of a rotorcraft, means the area of the aerodrome:
1. from which a take-off is commenced or
2. over which the final phase of the approach to hover is completed.
[5] AC 91-29 v1.1: Supports the new Civil Aviation Safety Regulations and replaces operational information previously found in CAAP 92-2(2) and is referred to in AC139.R-01 v1.0. An advisory circular provides advice and guidance to illustrate a means, and not necessarily the only means, of complying with regulations.
[6] TLOF: Touchdown and lift-off area is the surface over which the touchdown and lift-off is conducted.
[7] Danger area: Term used to refer to an area where rotor wash velocities can be expected at or above speeds that may displace a person. (See section titled Rotor wash and Figure 9).
[8] From AC 139.R-01 v1.0: The design helicopter is a helicopter having the most demanding set of dimensions, the greatest maximum take-off weight and the most critical obstacle avoidance criteria. It may not be a single helicopter type but rather a combination of critical aspects from numerous helicopters that the heliport intends to serve.
[9] Touchdown and lift-off area (TLOF) is the surface over which the touchdown and lift-off is conducted.
Final approach and take-off area (FATO) for a rotorcraft, means the area of the aerodrome from which take-off is commenced; or, over which the final phase of the approach to hover is completed.
[10] Operator confirmed AW139 helicopter involved but was unable to confirm the registration of the aircraft.
To helicopter medical transport operators and hospital helicopter landing site operators
Medical transport operators should engage with the owners and operators of hospital helicopter landing sites to ensure local procedures are sufficient to mitigate the risk of rotorwash associated with larger aircraft.
What happened
The ATSB found that following the introduction of larger helicopters into medical transport operations, there has been an increase in rotor wash related injuries at hospital HLS.
Why did it happen
Flight crew were not aware of pedestrians in the vicinity of the hospital helicopter landing site at the time. If the recommended rotor wash exclusion area had been applied at each HLS, it would have reduced the risk of the pedestrians being injured.
: The Australian Transport Safety Bureau strongly encourages operators of hospital helicopter landing sites, and helicopter medical transport operators using those landing sites, work together to review the adequacy of existing risk controls to ensure pedestrians are adequately protected from the increased rotor wash associated with larger helicopters.
Managing the risk of rotor wash
From the identified common factors associated with rotor wash incidents, the flightpath is the only element that can be managed by the pilot in accordance with the operator’s procedures. However, pilots may be unaware of the presence of pedestrians in the vicinity of a hospital HLS. To enable the continued safe use of these facilities, hospital HLS owners and helicopter operators should ensure pedestrians are not affected by rotor wash by implementing appropriate risk controls for their HLS in addition to the helicopter operating procedures. Controls may include physical barriers, warning devices such as sirens, lights, high visibility warning signs, painted lines on nearby public thoroughfare to alert pedestrians to the rotor wash danger area, an inspection schedule for the HLS facility and surrounding area, and establishing a closed-loop reporting system.
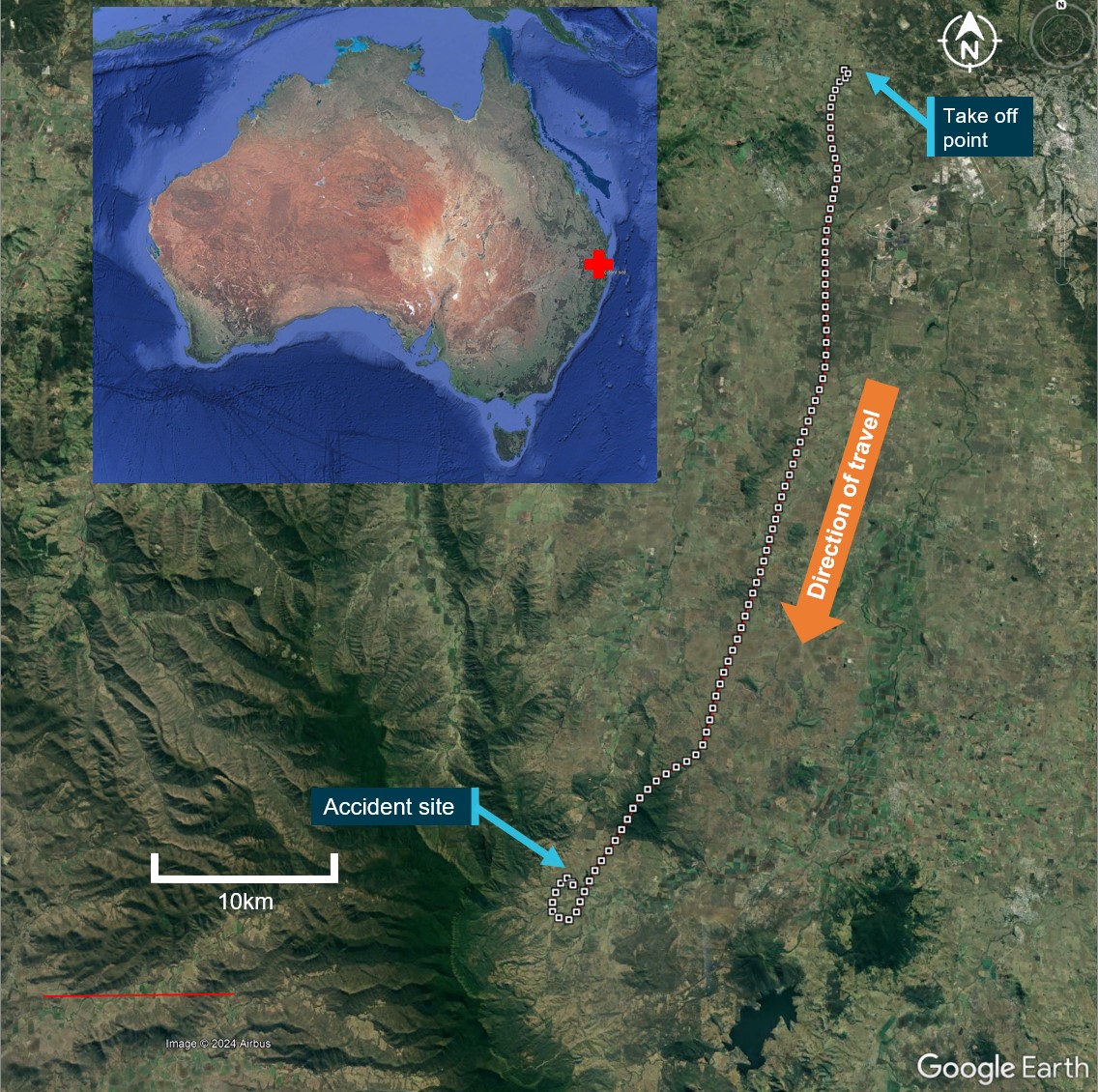
On the afternoon of 20 September 2023, the pilot of a Bell Helicopter Company 204B, registered VH‑EQW, was tasked with firefighting operations utilising a 1,230 L (Bambi Max) water bucket with a 5 m line. The helicopter departed on a 25-minute flight from a private property near Amberley, Queensland, and tracked to another property in Tarome, about 48 km to the south‑west.
While picking up a full bucket of water from the dam, the helicopter lost control, impacted the water, and subsequently sank to the bottom of the dam. The pilot extricated themselves with only minor injuries, however, the helicopter was destroyed.
What the ATSB found
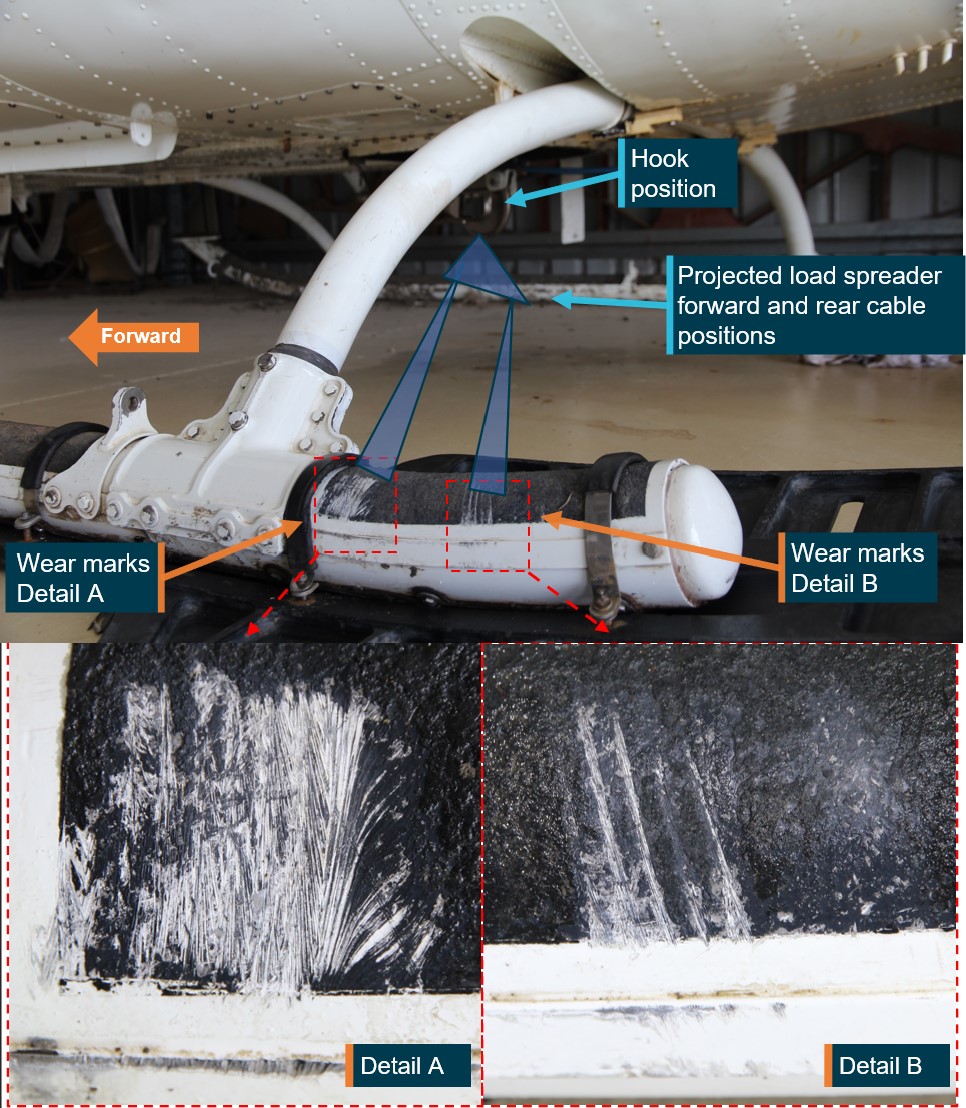
The ATSB found that the Bambi Bucket suspension cables were caught over the left rear skid when the helicopter was on approach to the dam and during the water collection into the bucket. As the load of water was lifted, it was almost certain that the helicopter’s centre of gravity moved aft and left due to the tethered weight over the left rear skid. This resulted in asymmetric lift loads, loss of control and collision with water.
The ATSB’s examination of the wreckage did not identify any pre-impact defects with the helicopter. Also, the pilot had completed helicopter underwater escape training (HUET) about 2.5 years prior to the accident.
Safety message
Conducting helicopter external load operations over water is a complex task, with the risk of an accident shown to be over twice as high as private helicopter operations. There can be a lack of visual references, visual illusions over water, limited visibility and vertical reference of the hook and external load through mirrors and bubble windows.
As shown in this accident, fouling of external load suspension cable(s) on the airframe can lead to rapid changes in weight distribution, asymmetric lift and loss of control. This investigation reinforces that correct cable positioning is vital to the safety of external lift operations. Further, this accident highlights the importance of conducting HUET to increase the occupants’ chances of post-accident survival in the event of impact with water.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
Summary of events
On the afternoon of 20 September 2023, the pilot of a Bell Helicopter Company 204B, registered VH‑EQW, was tasked with firefighting operations utilising a 1,230 L water bucket (Bambi Max) with 5 m cables.
The helicopter departed from a private property near Amberley, Queensland, on a 25-minute flight to another property near Tarome, about 48 km away (Figure 1) with the intention of uplifting water from a dam (dip site) with the water bucket slung under the helicopter for firefighting operations. The flight track data indicated that the helicopter had an average cruise ground speed of about 85 kt (78 kt indicated airspeed (IAS)), with a maximum of 93 kt (85 kt IAS).[1]
After arriving overhead the property, the pilot aligned the helicopter with the dam, descended over the water to the dip site and submerged the bucket. As the pilot began to initiate the bucket lift, control of the helicopter was lost, and it impacted the water surface and sank. The pilot sustained minor injuries, but exited and swam to shore, and the helicopter was destroyed.
Figure 1: VH-EQW flight track from the take-off point to the accident site
Source: Google Earth, modified by the ATSB
Pilot account of events
The pilot was operating the helicopter from the left seat for increased visibility from the bubble window while conducting the external load operation. The pilot recalled that, after arriving at the property at Tarome, they commenced filling their first load of water from a dam. The pilot reported that, during water collection, they heard an unusual noise and that the helicopter ‘kicked a bit’. Remaining in the hover, the pilot checked that all engine indications were normal and that the bucket and line were in the appropriate place. However, the pilot reported that something still did not feel right. As a result, they elected to dump the water from the bucket and initiate a climb out. The pilot stated that, within about 10–15 seconds, as engine power was being applied and the water was being released (dumped) from the bucket, the pilot heard what they described as a ‘loud roaring’ sound and the helicopter pitched up, yawed, rolled left, and impacted the water at low speed.
Witness observations
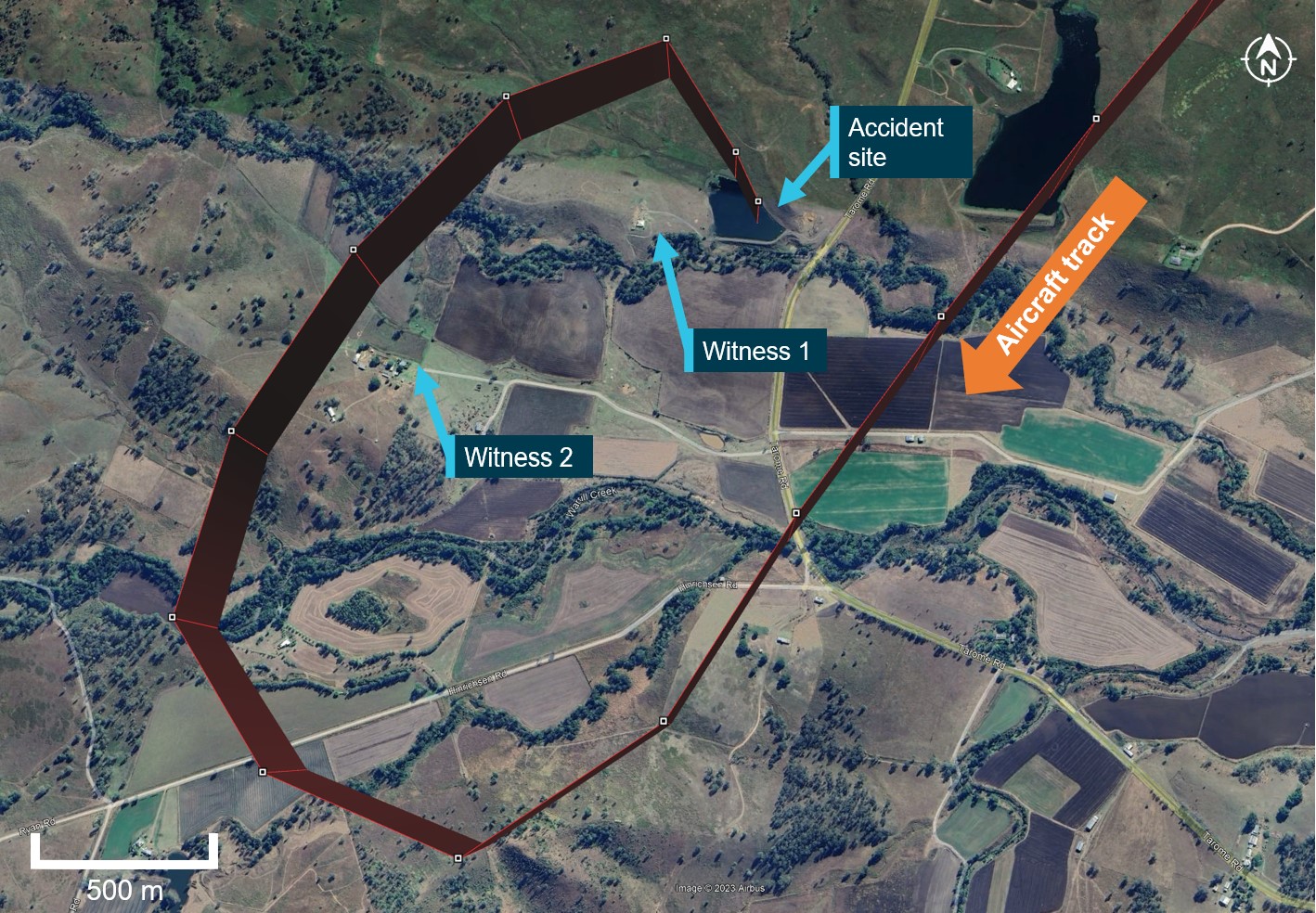
The accident was observed by 2 witnesses (Figure 2). Witness 1 observed the helicopter circle, move towards the dam on their property to collect water, and observed the entire accident sequence. They also photographed and videoed the helicopter’s movements up until moments before the accident. The witness did not see or hear anything unusual before the helicopter impacted the water. Witness 2 was on an adjacent property; they noted a definitive increase in what they thought may have been engine noise just before the accident occurred.
Figure 2: VH-EQW flight track with accident site and witness locations
Source: Google Earth, modified by the ATSB
Witness video
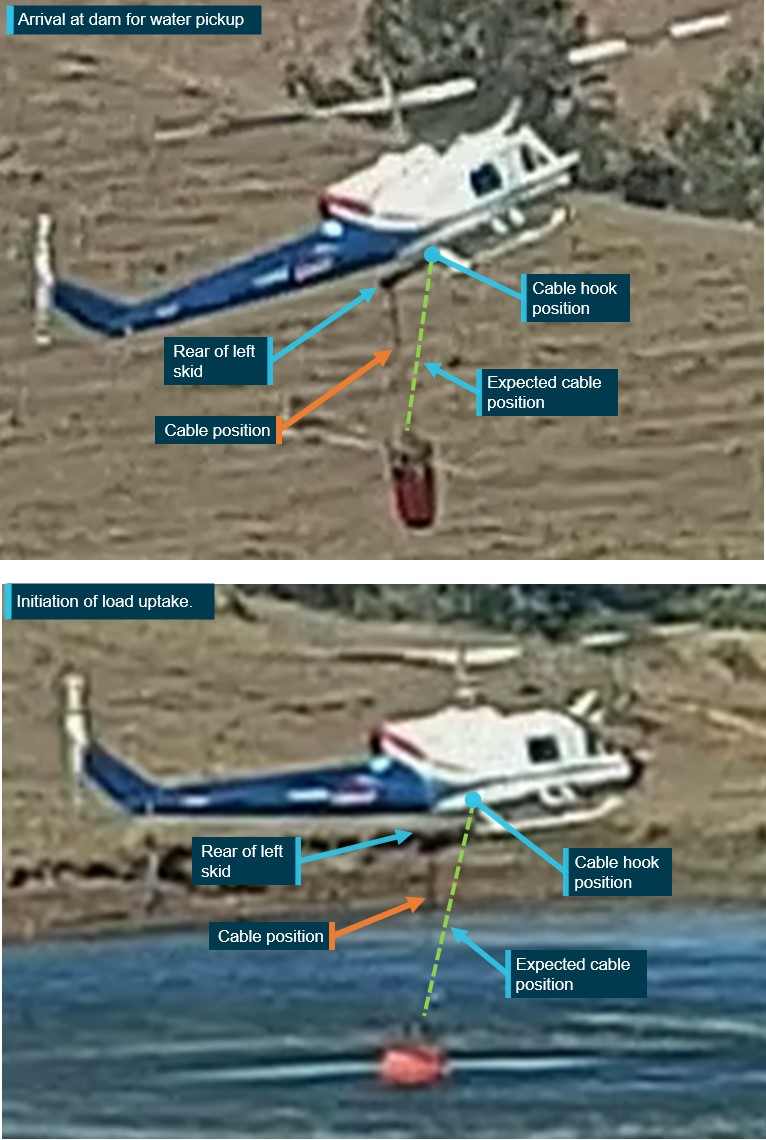
Recorded video taken by witness 1 just prior to the accident showed the helicopter on approach to the dam. It captured the water bucket suspension cable caught over the rear of the left skid when on the approach (from the start of the video – Figure 3 top) until the helicopter was initiating lift‑off with the external load of water (Figure 3 lower). The video ended as the helicopter started to take the weight of the bucket, which contained a large quantity of water. The helicopter was recorded starting to pitch up and roll left before the video stopped. There was no discernible change in sounds emanating from the helicopter for the duration of the video.
Figure 3: Sequence of water pickup from dam showing bucket cable position from approach (top) to lifting off (lower)
Source: Still photographs taken from witness video, annotated by the ATSB
Pilot egress
The pilot recalled that, after the surface impact, the helicopter almost immediately became inverted, filled with water, and sank to the bottom of the dam. The pilot stated that they removed their seatbelt and helmet and attempted to open the front left door but could not open it with either the normal or emergency release handles. The helicopter was almost fully submerged when the pilot swam to the rear of the cabin and tried to open the rear right door. They made further unsuccessful attempts to egress by kicking the helicopter windows.
The pilot then moved to the rear left door, and applying considerable force, was able to successfully open it. The pilot recalled that, when they initially attempted to open the emergency exits, they may have been trying to operate the door handles in the incorrect (opposite) direction due to the helicopter being inverted.
The pilot escaped the sinking helicopter and swam a few metres to the surface and then to the side of the dam.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) with ratings for single and gas turbine engine helicopters. Prior to the accident flight, the pilot had accumulated 2,599.4 hours of total flying experience. They had 220.8 hours total on the Bell 204/205/UH-1 helicopter. Of this, 22.8 hours was pilot in command of the Bell 204, which was accrued in the 2 months prior.
The pilot was qualified to conduct helicopter firefighting operations and had low‑level and sling operation ratings. The pilot last completed an aerial application proficiency check on 29 June 2023, which was valid until 20 June 2024, and a low-level helicopter flight review on 12 August 2023.
The pilot held a Class 1 Aviation Medical Certificate, valid to 12 June 2024, with no restrictions.
Helicopter information
General information
The Bell Helicopter Company 204B (and 205) is the civilian version of the UH-1 Iroquois. It was designed in the mid‑1950’s as a utility helicopter. The helicopter had a 2-blade main rotor and 2‑blade tail rotor and was powered by an Ozark Aeroworks T53-L-13B turboshaft engine. The helicopter was manufactured in the United States in 1965 and first registered in Australia in 2014 as VH-EQW. It had accumulated about 23,515 flight hours total time in service and had a current certificate of airworthiness and registration. The helicopter’s technical log had no outstanding defects at the time of the accident.
VH-EQW was fitted with an external load hook located directly underneath the main rotor transmission, in line with the helicopter’s centre of lift.
Bucket and suspension cable information
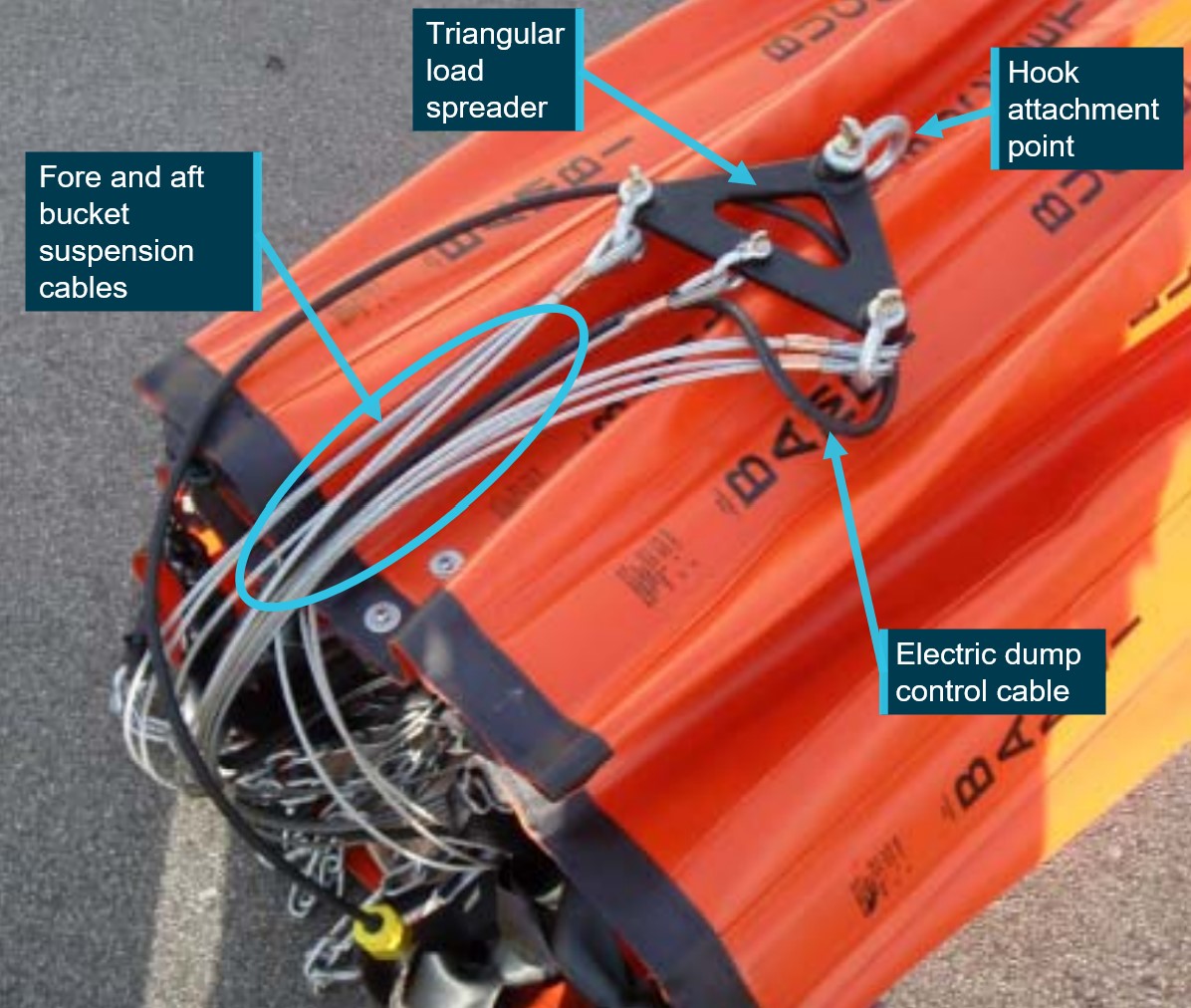
The Bambi Max water bucket fitted to VH-EQW was manufactured by SEI industries and weighed 67 kg empty and 1,300 kg when full, with a capacity of 1,230 L. The bucket was connected to the helicopter’s external load hook by several stainless steel suspension cables, separated fore and aft by a triangular spreader bar (Figure 4). A dump switch on the collective[2] was connected through a black electrical cable to control the dump valve located in the base of the bucket. The suspension cables used on the day had a length of 5.05 m and the total length including the bucket was 6.27 m.
Figure 4: Photo of exemplar Bambi Max bucket in the stored configuration showing the triangular spreader bar and suspension cables
Source: SEI industries, annotated by the ATSB
External load visibility
The helicopter was fitted with 2 rear vision mirrors that were located under each of the Perspex chin bubbles to provide visibility of the external hook, suspension cables and bucket. The bubble window fitted to the pilot’s left door also allowed for better visibility downwards and, to a limited extent, the rear of the helicopter (Figure 5). In response to this draft report, the pilot reported that the mirrors provided a full and clear view of the external hook and bucket.
Source: Operator, annotated by the ATSB
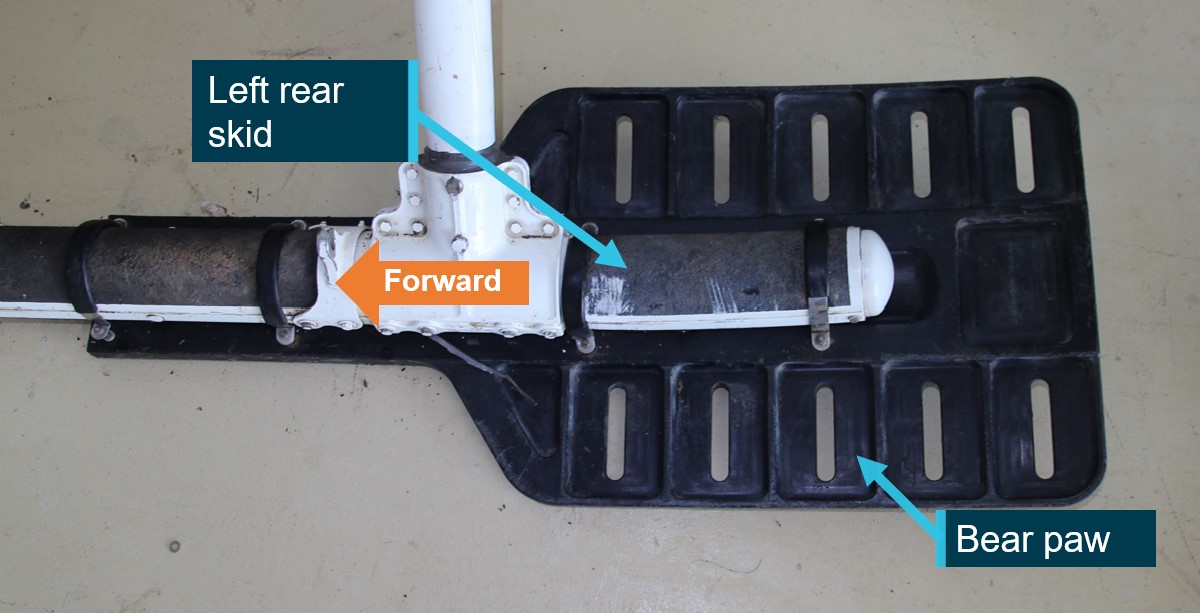
Bear paw modification
The helicopter had a pad like modification to the skids called ‘bear paws’, which are supplied as a kit of 2. The pads fit under and to the rear of each of the skids and are designed for landings off airport, on uneven or unstable terrain, helping with overall landing stability and to prevent the rear of the skids from sinking into soft surfaces. The bear paws are made from a polymer plastic and feature high impact resistance, durability and flexibility. They are secured to the skid utilising 4 metal clamps (Figure 6).
Figure 6: VH-EQW left skid with bear paw fitted
Source: ATSB
Weight and balance
The helicopter was within weight and balance limits during the transit flight to Tarome. However, when lifting the load, with the suspension cables caught over the left rear skid and a full bucket of water (weighing 1,300 kg), the load shifted significantly to the rear and to the left. In this configuration, ATSB calculations showed that the helicopter was outside its balance limitations with the addition of just a 300 kg external load and well outside the balance limitations with the addition of a full bucket of water.
Meteorological information
The weather at the time of the accident was described by the pilot as clear and calm. The Bureau of Meteorology forecast showed visibility was greater than 10 km and the wind was from the north‑west at 11 kt.
The flight was to the south-west and had a calculated tail wind component of about 3 kt. The meteorological conditions were not considered a factor in this event.
Wreckage examination
General engine and airframe examination
The helicopter was retrieved from the dam and taken to a secure facility for detailed examination. The rotor systems, drive shafts, transmissions, flight controls, exits, and engine were visually examined by the ATSB. The fuel control and overspeed governor units were removed from the engine and sent to the engine type certificate holder for functional testing. That testing did not identify any issues with the unit.
The engine drive to main rotor transmission shaft had broken out of its retaining couplings likely due to the impact. The engine manufacturer stated that the damage to the drive couplings was indicative of significant engine power driving the main rotor transmission at the time when the main rotors impacted with water, creating a sudden stoppage.
The pilot’s left front door emergency jettison system was tested and worked as designed by releasing the door from its hinges.
No pre-impact defects in the engine, flight controls or emergency exits were identified.
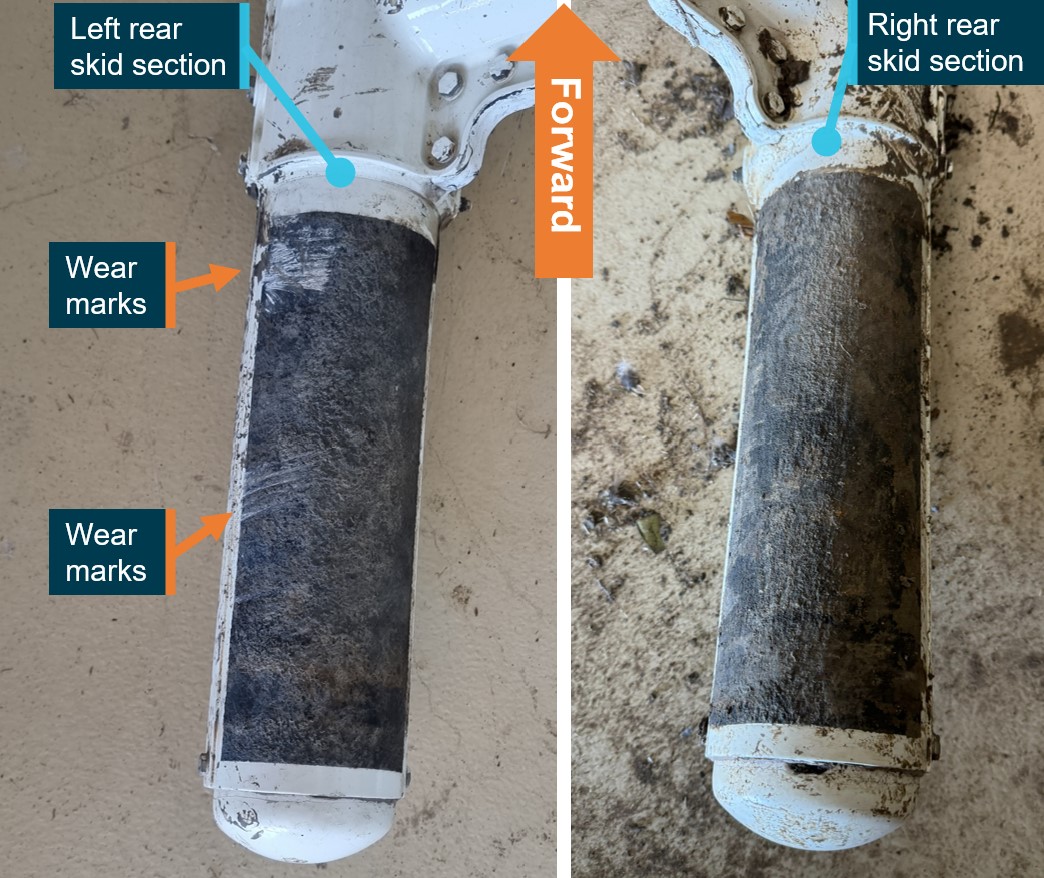
Skid examination
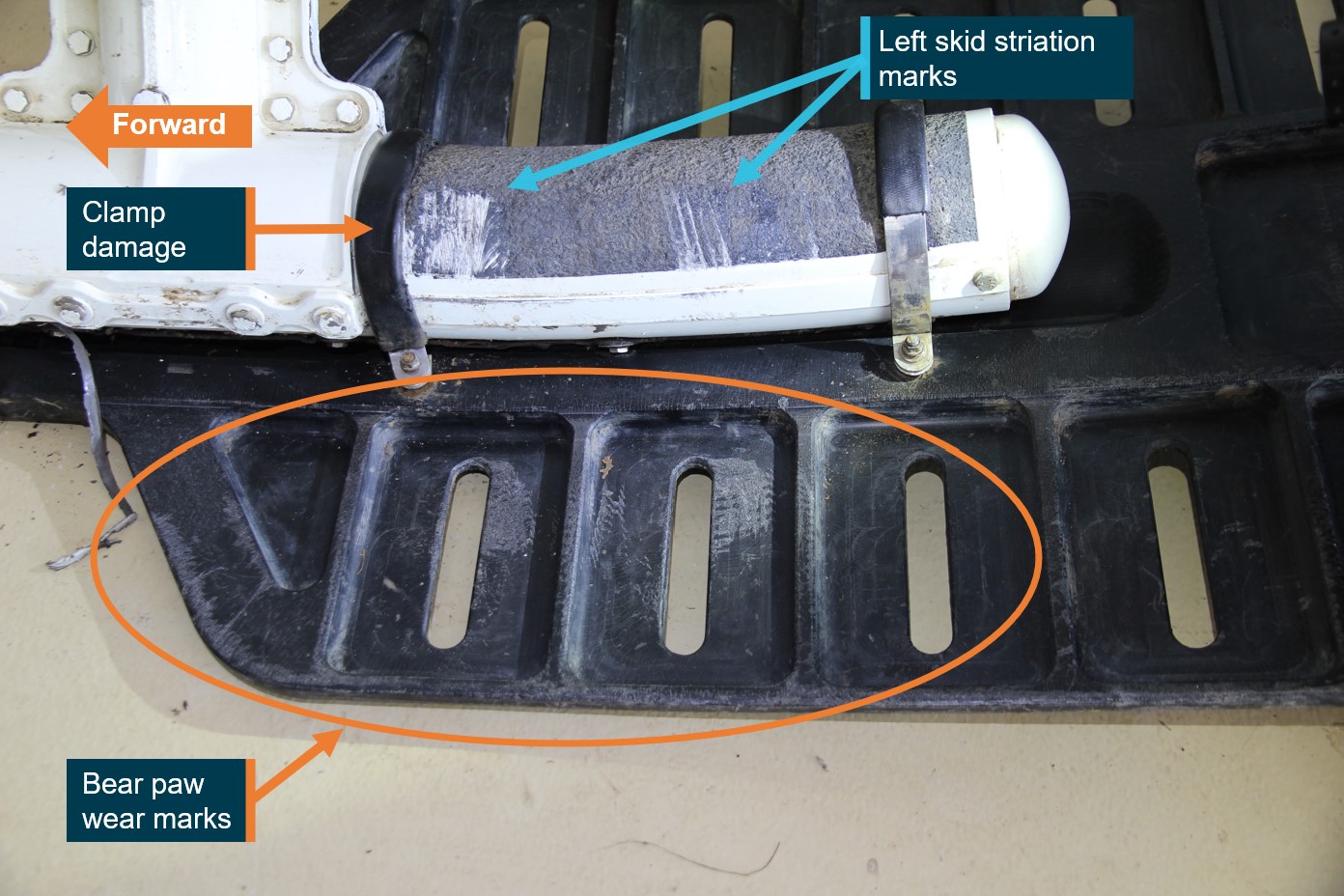
The left and right skid had their bear paw pads removed to facilitate the transport of the wreckage to the storage facility. The right skid did not have any notable damage. The left skid had several striation type wear marks at the rear of the skid (Figure 7).
Figure 7: Rear of left and right skid sections with the left skid showing wear marks
Source: ATSB
The left bear paw was refitted to the left skid to facilitate inspection as an assembly. It was noted that the bear paw had permanent deformation damage that indicated that it had rotated counterclockwise (viewed from the rear) until it had come into contact with the rear skid support. There was also damage to one of the attachment clamps, which had been forced forward at its upmost point. That clamp was directly in front of the forward set of wear marks on the rear of the skid. There was further abrasion damage that indicated the left bear paw had flexed downward under significant load on its outboard side (Figure 9).
Figure 8: Left rear skid showing corresponding skid and bear paw damage
Source: ATSB
The ATSB conducted testing with string lines and a spreader bar configured in a similar manner to the water bucket suspension cables. It was identified that, if both sets of cables were caught over the left skid, the position of the forward and rear cable positions was consistent with the locations of the striation type wear damage found on the left skid[3].
Figure 9 shows the left rear skid, viewed from an outboard direction, showing projected alignment with the hook, cable spreader and multiple bucket suspension cables. Detail A and B show close‑up wear patterns consistent with numerous stainless-steel cable wear striations that aligned with the direction of the external cargo hook attachment point.
Figure 9: Outboard of left rear skid showing hook position and likely position of spreader with forward and rear cables aligned with wear damage
Source: ATSB
Pre-flight checks with an external load
Wagtendonk (1996), in Principles of Helicopter Flight, stated that:
When a cable or strap has been attached to the helicopter hook it is most important to ensure that the cable does not pass over the skid or undercarriage leg. As the aircraft rises and the strain is taken on the load, this could cause a serious rolling sequence. Use the mirror or look directly at the cable. Sadly, non-compliance with this simple rule continues to cause problems.
Common best practice is for the bucket to be positioned at the front of the helicopter and for the suspension cables to be routed from the hook between the skids to the front. This gives the pilot the best view of the bucket during take-off and reduces the chances of the suspension cables fowling. If the cables are routed and connected from the back of the helicopter, there is potential that the cables can be caught by the skid and not seen during take-off.
The pilot reported that, during their pre-flight check, the bucket was placed at the front of the helicopter and was functionally tested.
Helicopter underwater escape training
Helicopter underwater escape training (HUET) has been in use around the world since the 1940s and is considered best practice in the overwater helicopter operating industry. HUET is designed to improve survivability after a helicopter ditches or impacts into water. Research of such accidents has shown that occupants who survive the initial impact will likely have to make an in‑water or underwater escape, as helicopters usually rapidly roll inverted post-impact due to the position and mass of the engine/s, transmission and main rotor system. The research has also shown that drowning is the primary cause of death following a helicopter accident into water.
Fear, anxiety, panic, and inaction are the common behavioural responses experienced by occupants during a helicopter accident. In addition to the initial impact, in-rushing water, disorientation, entanglement with debris, unfamiliarity with seatbelt release mechanisms and an inability to reach or open exits have all been cited as problems experienced when attempting to escape from a helicopter following an in-water accident (Rice & Greear, 1973).
HUET involves a module (replicate of a helicopter cabin and fuselage) being lowered into a swimming pool to simulate the sinking of a helicopter. The module can rotate upside down and focuses students on bracing for impact, identifying primary and secondary exit points, egressing the wreckage and surfacing. HUET is normally part of a program of graduated training that builds in complexity, with occupants utilising different seating locations, exits and visibility (via the use of ‘blackout’ goggles). This training is conducted in a controlled environment with safety divers in the water.
HUET is considered to provide individuals with familiarity with the crash environment and confidence in their ability to cope with the emergency situation (Ryack et al., 1986).Interviews with survivors from helicopter accidents requiring underwater escape frequently mention they considered that HUET was very important in their survival. Training provided reflex conditioning, a behaviour pattern to follow, reduced confusion, and reduced panic (Hytten, 1989).
The pilot conducted HUET training in March 2021, with a renewal due in 2024. The pilot reported that familiarity with the helicopter, the open area in the cabin (all seats removed) and HUET assisted with their ability to successfully escape from the sinking helicopter.
Helicopter water bucket operation accidents
The helicopter manufacturer stated that, between 1974 and 2017, there were 6 accidents involving Bell Helicopters conducting external lift operations where the suspension cable became entangled with the skids and the helicopter lost control during water uplift. Two of those accidents involved the Bell 204/205 helicopter and 4 were Bell 206s.
The Flight Safety Foundation conducted a study titled External loads, powerplant problems and obstacles challenge pilots during aerial fire-fighting operations. The study utilised data from helicopter accident reports in the United States between 1974 and 1998.
The study showed that, it was over twice as likely for a firefighting helicopter to be involved in an accident when compared to private helicopter flights. Of the 97 accidents studied, 4 instances were due to water bucket cables being caught on the skids leading to a loss of control during uplift. Further, there were 2 instances where the unloaded water bucket or external load cable came into contact with the tail/tail rotor due to excessive speed, turbulence and manoeuvring.
Two recent accidents, one in 2017 (New Zealand Transport Accident Investigation Commission report AO-2017-001) and one in 2019 (French Bureau d'Enquêtes et d'Analyses report 2019‑0023) also involved helicopter buckets coming into contact with the tail rotor. Those accidents were partly attributed to operating at airspeeds above the manufacturers’ velocity never exceed speeds.
Safety analysis
Suspension cable caught on left rear skid
Video evidence showed the Bambi Bucket suspension cables were caught over the left rear skid when the helicopter was on approach to the dam and remained attached to the skid during the water uplift. This evidence was consistent with:
The ATSB’s wreckage examination, which identified that the left rear skid and bear paw showed multiple areas of damage including striation marks indicative of contact with the bucket suspension cables.
Testing of the striation marks alignment with the fore and aft cable positions when attached to the external cargo hook with the triangular load spreader.
The video ruled out the capture of the cables over the skid during the water collection phase. However, the ATSB was unable to identify if the cables had become captured due to pre-flight bucket and cable positioning, take-off manoeuvring or during the transit flight to the dam.
Just before the video ceased, it showed the initiation of the full water bucket uplift followed by the helicopter pitching up and rolling left slightly. The ATSB weight and balance calculations concluded that any bucket weight above 300 kg (full is 1,300 kg) acting over the left rear skid, would be sufficient to move the centre of gravity outside of the helicopter’s balance limit. Therefore, it was almost certain that as the load of water was lifted, the helicopter’s centre of gravity moved aft and left as a result of the suspension cables being caught over the skid. The tethered weight created an asymmetric lifting point, which resulted in a rapid loss of control and subsequent collision with water.
Helicopter underwater escape training
The pilot conducted HUET about 2.5 years prior to the accident. This likely assisted their ability to egress the helicopter through a rear door while inverted and underwater. HUET has been shown to significantly increase the chances of survival in the event of collision with water.
No pre-impact defects
The ATSB wreckage examination did not identify any pre-impact mechanical issues with the helicopter. Further, the engine manufacturer concluded that the engine was supplying significant power to the transmission at the time of the impact with water.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control and collision with water involving Bell Helicopter Company 204B helicopter, near Tarome, Queensland, on 20 September 2023.
Contributing factors
The Bambi Bucket suspension cables were caught over the left rear skid. Consequently, as the load of water was lifted, it was almost certain that the helicopter’s centre of gravity moved aft and left, the tethered weight over the skid created an asymmetric lifting point. This resulted in a loss of control and the helicopter collided with water.
Other findings
The pilot conducted helicopter underwater escape training 2.5 years prior to the accident. This training increased the pilot's chances of survival when the helicopter became submerged in the dam.
There were no pre-impact defects identified with the helicopter.
Sources and submissions
Sources of information
The sources of information during the investigation included:
pilot
operator and chief pilot
Civil Aviation Safety Authority
Queensland Police Service
aircraft manufacturer
aircraft maintenance organisation
Airservices Australia
witnesses
video footage of the accident flight and other photographs and videos taken on the day of the accident.
References
Hytten, K. (1989). Helicopter crashing in water: Effects of simulator escape training. Acta Psychiatrica Scandinavica, Suppl. 355: 73-78. Cited in Coleshaw, S. (2010). Report for the Offshore Helicopter Safety Inquiry. Report No SC176.
Rice, E, V., & Greear, J. F. (1973). Underwater escape from helicopters. In Proceedings of the Eleventh Annual Symposium, Phoenix, AZ: Survival and Flight Equipment Association, 59-60. Cited in Brooks C., (1989). The Human Factors relating to escape and survival from helicopters ditching in water. AGRAD.
Ryack, B. L., Luria, S. M., & Smith, P. F. (1986). Surviving helicopter crashes at sea: A review of studies of underwater egress from helicopters. Aviation, Space, and Environmental Medicine, 57(6), 603-609.
Wagtendonk, W.J. (1996). Principles of Helicopter Flight, Aviation Supplies & Academics, Inc. Washington, USA.
Veillette, P. R. (1999). External loads, powerplant problems and obstacles challenge pilots during aerial fire-fighting operations (Flight Safety Foundation). https://flightsafety.org
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot
chief pilot
aircraft maintenance organisation
National Transportation Safety Board
aircraft and engine manufacturers
Civil Aviation Safety Authority.
Submissions were received from the pilot and chief pilot. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The wind information, density altitude and recorded ground speed was used to calculate the indicated airspeed.
[2]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[3]On 27 October 2024 after directly involved party submissions were completed the pilot advised that they were going to carry out their own testing and reenactments on a Bell 204 helicopter with a Bambi Bucket fitted to ascertain what had occurred.
Preliminary report
Report release date: 06/12/2023
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On the afternoon of 20 September 2023, the pilot of a Bell Helicopter Co 204B, registered VH‑EQW, was tasked with fire-fighting operations utilising a 1,200 L bucket with a short line. The helicopter departed from a private property near Amberley, Queensland, and tracked to another property in Tarome, about 26 NM (48 km) away. The pilot was operating the helicopter from the left seat for visibility while conducting the operation.
After arriving at Tarome, the pilot commenced picking up their first load of water from a dam. The pilot reported that, during water collection, they heard an unusual noise and that the helicopter ‘kicked’. Remaining in the hover, the pilot checked that all engine indications were normal and that the bucket and line were in the appropriate place. However, the pilot reported that something still did not feel right. As a result, they elected to dump the water from the bucket and initiate a climb out. Within about 10-15 seconds, as engine power was being applied, and the water was being released from the bucket, the pilot heard what they described as a ‘loud roaring’ sound and the helicopter pitched up, yawed, and subsequently had a reduction in power. The helicopter rolled left and impacted the water at low speed. The pilot sustained minor injuries and the helicopter was destroyed.
Witness observations
The accident was observed by 2 witnesses (Figure 1). ‘Witness 1’ observed the helicopter circle, move towards the dam on their property to collect water, and the entirety of the accident sequence. They photographed and videoed the helicopter’s movements up until a few seconds before the accident (Figure 2). That witness did not see or hear anything unusual before the helicopter impacted the water. ‘Witness 2’ was on an adjacent property; they noted a definitive increase in what they thought may have been engine noise just before the accident occurred.
Figure 1: VH-EQW flight track with accident site and witness locations
Source: Google Earth, modified by the ATSB
Figure 2: VH-EQW picking up water from the dam just prior the accident
Source: Supplied
Pilot egress
Almost immediately after the impact, the helicopter inverted, started to fill with water, and sink rapidly. The pilot removed their seatbelt and helmet, and attempted to open the front left door but could not open it with either the normal or emergency release handles. When the helicopter was almost fully submerged, the pilot swam to the rear of the cabin and tried to open the rear right door but could not open it either, making further attempts to get out by kicking the helicopter windows. The pilot then moved to the rear left door and, utilising considerable force, was able to successfully open it. The pilot noted in interview, that when they initially attempted to open the doors, they may have been trying to move the door handles in the incorrect (opposite) direction due to the helicopter being inverted.
The pilot escaped and swam a few metres to the surface and then to the side of the dam. The pilot stated that familiarity with the helicopter, the open area in the cabin (all seats removed) and HUET (helicopter underwater escape training) all assisted with their ability to successfully escape from the helicopter.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Helicopter) with ratings for single and gas turbine engine helicopters. Prior to the accident flight, the pilot had accumulated 2,599.4 hours of total flying experience and 220.8 hours on the Bell 204B type helicopter.
The pilot last completed an aerial application proficiency check on 29 June 2023, which was valid until 20 June 2024. The pilot was qualified to conduct helicopter fire-fighting operations and had both low‑level and sling operation ratings.
The pilot held a Class 1 Aviation Medical Certificate, valid to 12 June 2024, with no restrictions.
Aircraft information
The Bell Helicopter Company 204B is the civilian version of the UH-1 Iroquois. It was designed in the mid 1950’s as a utility helicopter. The helicopter had a 2-blade main rotor and 2-blade tail rotor and was powered by an Ozark Aeroworks T53-L-13B turboshaft engine. The accident helicopter (S/N 2038) was manufactured in the United States in 1965. The helicopter was first registered in Australia in 2014 as VH-EQW and had accumulated about 23,515 total time-in-service. It had a current airworthiness certificate and maintenance release with no outstanding defects at the time of the accident.
Wreckage examination
The helicopter was recovered from the dam and taken to a secure facility for detailed examination. The helicopter’s rotor systems, flight controls, exits, and engine were visually examined. No pre‑accident damage was identified. The pilot’s left front door emergency jettison system was tested serviceable.
Further investigation
To date, the ATSB has interviewed the pilot, the witnesses, and conducted a preliminary examination of the helicopter wreckage.
The investigation is continuing and will include review and examination of:
the pilot’s training and records
maintenance documentation
key components of the helicopter.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
The ATSB has issued a Safety Advisory Notice to both aircraft lifejacket manufacturers and national aviation certification authorities encouraging them to provide guidance to aircraft operators about how to fit a constant wear lifejacket so that it does not interfere with the proper fitment of seatbelts.
The Safety Advisory Notice has been issued as part the ATSB’s on-going investigation into the mid-air collision of two scenic flight helicopters at the Gold Coast on 2 January this year.
During the course of the investigation the ATSB has identified a potentially common lack of understanding in the broader helicopter tourism community about how ‘constant wear’ lifejackets should be worn in conjunction with seatbelts.
“Our investigators have identified that some passengers’ seatbelts in both helicopters involved in this accident were not fitted correctly, in part due to interference from their lifejackets,” said ATSB Chief Commissioner Angus Mitchell.
“However, it is very important to stress we have not attributed the outcomes from this tragic accident to the fitment of seatbelts and lifejacket interference, as the nature of the second helicopter’s collision with the sandbar would typically be non-survivable, and a range of other factors beyond seatbelts contribute to occupant safety in aircraft accidents.
“But our investigation has identified that there appears to be a broader issue across the scenic flight industry where there are misunderstandings as to how seatbelts and lifejackets should be worn.”
Mr Mitchell said an ATSB review of social media photos of passengers of helicopter tourism operations, both in Australia and internationally, established that incorrect fitment of seatbelts with constant wear pouch style lifejackets was prevalent.
Many relevant social media photos reviewed by the ATSB showed the seatbelt webbing or buckle was positioned above the lifejacket pouch or over it. This meant that the lap belt portion of the seatbelt was not low and tight across the passenger’s hips and was positioned either over the lifejacket, creating slack, or above the lifejacket, close to the passenger’s sternum increasing the risk of injury.
“This suggests there is a common lack of understanding in the helicopter tourism community, worldwide, about how to integrate constant wear lifejackets with seatbelts, so as not to reduce their effectiveness.”
Mr Mitchell said the ATSB has identified that lifejacket manufacturers and regulatory authorities have not provided any readily-available guidance to assist helicopter operators on how to position a pouch or yoke style constant wear lifejacket so as not to interfere with an aircraft seatbelt.
“Aviation lifejacket standards require operational instructions be provided in writing and on the lifejackets themselves. For constant wear lifejackets, it is reasonably foreseeable that they would be worn seated in an aircraft and while using the aircraft’s seatbelt. Yet there are no required instructions related to this in the relevant standards and the ATSB found no manufacturers opting to provide instructions.
“The ATSB encourages manufacturers of constant wear lifejackets to provide operating instructions and/or guidance material to operators of aircraft on how to wear and use a constant wear lifejacket with a seatbelt such that it does not interfere with the performance of the seatbelt during an accident,” he said.
“Further, the ATSB encourages certification authorities to modify lifejacket standards to include the requirement for instructions on how to wear constant wear lifejackets while seated and wearing a seatbelt.”