Flights after last light normalised, R22 accident investigation finds
One of Australia's largest beef cattle operations has amended procedures to ensure its helicopter pilots are not flying after last light, an ATSB investigation report details.
The safety action comes as a result of the ATSB’s investigation into a fatal Robinson R22 helicopter accident on a cattle station on Queensland’s Cape York Peninsula late last year, where the pilot was found to have flown at night, without the appropriate qualifications.
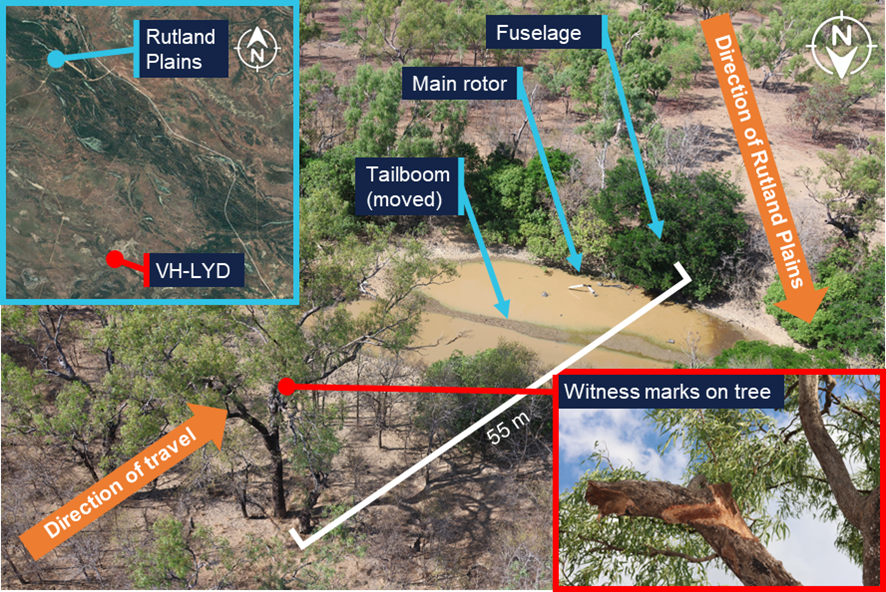
On the evening of 9 October 2025, the investigation’s final report details, the Robinson R22 Beta II was being used to guide ground vehicles tackling a bushfire on a property owned by MDH Pty Ltd, 25 km south-south-east of Kowanyama, Queensland.
At around 1920 local time, the pilot told the ground crew they would return to the station as it was getting too dark. Staff at the station lit the helipad for the R22’s arrival, but the pilot did not return.
Wreckage of the helicopter was found the next morning, and the pilot had been fatally injured.
The ATSB’s investigation concluded the helicopter’s last recorded movement was at 1929, 37 minutes after last light and 12 minutes after nautical twilight. The pilot was not qualified to fly at night, and the helicopter was not equipped for night flight.
Further, the investigation found it was normal for MDH helicopter pilots to exceed the limits of last light. An ATSB analysis of historical flight tracking data showed 39 occasions in the previous 6 months where MDH pilots flew beyond the legal minimums into night.
“Instead of observing the legal limits, pilots chose their own limits, despite none of the company’s R22 pilots being qualified for night flight, and none of its R22 helicopters being equipped for night flight,” ATSB Chief Commissioner Angus Mitchell said.
“Flying after last light was a tolerated and unmanaged risk.”
The investigation report notes MDH now requires its pilots to determine the official time of last light, and has made it a clear responsibility of the pilot and the station manager to ensure aircraft are on the ground before this time.
Mr Mitchell noted this was the fourth fatal accident of this type in Australia in the last five years.
“Flying after last light without appropriate equipment and qualifications is unsafe,” he said.
“The acceptance and normalisation of flying after last light is leading pilots to fatal accidents.”
The requirement to operate under daylight conditions, and plan to land 10 minutes before last light, provides a reliable method for ensuring there are sufficient external visual references available to safely operate an aircraft, he said.
“Pilots and the companies or landowners they work for, or contract to, must work together to avoid flight at night by unqualified, unequipped pilots,” Mr Mitchell concluded.
“Development of risk management practices in any organisation should be an ongoing activity. It should develop an ability across all parties to document operational risks and codify learnings from operations.”
The investigation report notes that pre-flight planning by MDH pilots now includes consideration of fatigue, including rest and duty times, and consideration of specific risk assessment criteria.
MDH has also implemented a pilot mentoring scheme to assist, mentor and supervise company pilots during aerial mustering operations.
Read the final report: Collision with terrain at night involving Robinson R22 Beta II, VH-LYD, 25 km south-south-east of Kowanyama, Queensland, on 9 October 2025