Flight management occurrence involving Embraer 190, VH-UYN, 20 km north-west of Alice Springs, Northern Territory, on 24 August 2023
Final report
Report release date: 02/08/2024
Executive summary
What happened
On 24 August 2023, an Alliance Airlines Embraer E190-100 IGW aircraft, registered VH-UYN, was being operated on a scheduled passenger flight, QF1960, from Darwin to Alice Springs, Northern Territory.
The flight crew were expecting to overfly and conduct a circuit to runway 12, and the aircraft was configured accordingly. During descent, ATC offered a late call for a shortened track and visual approach to the final approach fix, which the crew accepted.
As the aircraft tracked to the waypoint, the crew configured the aircraft with high drag to expedite the aircraft’s descent. However, the rate of descent was higher than the crew anticipated and attempts to arrest the rate of descent were not immediately successful.
The aircraft descended below 1,800 ft AGL with a rate of descent above 3,000 ft/min.
When the aircraft’s automation was not responding to the flight crew inputs in the way the crew anticipated, the crew disconnected the autopilot and took manual control of the aircraft.
What the ATSB found
The ATSB identified that, after accepting an ATC request at short notice to conduct a straight-in approach, the flight crew unnecessarily re‑configured the aircraft to increase drag and expedite the descent. Due to the autopilot flight mode active at the time, the aircraft pitched down to maintain airspeed at the higher drag. Shortly after, as the aircraft descended at a high vertical rate towards the selected altitude, the pilot flying made an inadvertent mode selection in the automatic flight system that went undetected by the flight crew.
Due possibly in part to their workload, the pilot flying did not identify that the aircraft was starting to automatically capture the selected altitude, and selected a higher altitude, which disarmed the altitude select mode. This resulted in the flight director resuming the high rate of descent close to terrain.
These changes were not promptly identified by the aircraft captain in their role as pilot monitoring, due in part to their focus to visually assessing the terrain clearance.
Safety message
This incident highlights how important continuous attention to the autoflight system modes displayed on the primary flight display is to situation awareness.
The ATSB reminds flight crews the importance of continually monitoring descent profiles, irrespective of the type of approach being flown and the level of automation being used.
An ICAO safety advisory on Mode Awareness and Energy State Management Aspects of Flight Deck Automation reminds pilots that if
they recognise they are uncertain about the autoflight modes or energy state, they should not allow the airplane to continue in an unstable or unpredictable flight path or energy state while attempting to correct the situation. Instead, pilots should revert to a better (usually lower) understood level or combination of automation until the aircraft resumes the desired flight path and/or airspeed. This may ultimately require that pilots turn off all automation systems and fly the aircraft manually.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On 24 August 2023, an Alliance Airlines Embraer E190-100 IGW aircraft, registered VH-UYN, was being operated on scheduled passenger flight QF1960 from Darwin to Alice Springs, Northern Territory. On board were the captain as the pilot monitoring (PM), first officer as the pilot flying (PF),[1] 2 cabin crew and 63 passengers. The weather conditions in the area were fine and suitable for operation under the visual flight rules.[2]
A trainee aerodrome controller (ADC), along with an on-the-job training instructor (OJTI), were controlling arriving and departing aircraft from the air traffic control (ATC) tower at Alice Springs Airport. The trainee ADC was providing procedural traffic separation and communicating with aircraft on the radio. The OJTI was overseeing the trainee and was ultimately responsible for ATC decisions and communications.
The en route controller had advised the trainee ADC and OJTI that the crew of VH-UYN had requested a straight-in approach to runway 12.[3] However, due to a preceding Pilatus PC-12 aircraft inbound from the north, and a helicopter arriving from the south, the trainee ADC was not comfortable offering VH-UYN this approach due to an anticipated increase in their workload. As a result, at 1617 local time, as the aircraft was passing 10,000 ft on approach to Alice Springs, the trainee ADC advised the flight crew to expect to overfly the airport and then conduct a right circuit for runway 12.
One minute later, due to preceding traffic, the trainee ADC instructed the flight crew to reduce speed to 210 kt, which the crew set in the autoflight control system (see the section titled Autoflight control system). The OJTI then assessed that if VH-UYN overflew the airport, it may result in a conflict with the helicopter arriving from the south and suggested that the trainee controller offer VH-UYN a clearance to track direct to waypoint ALDIM[4] to conduct a straight-in approach.
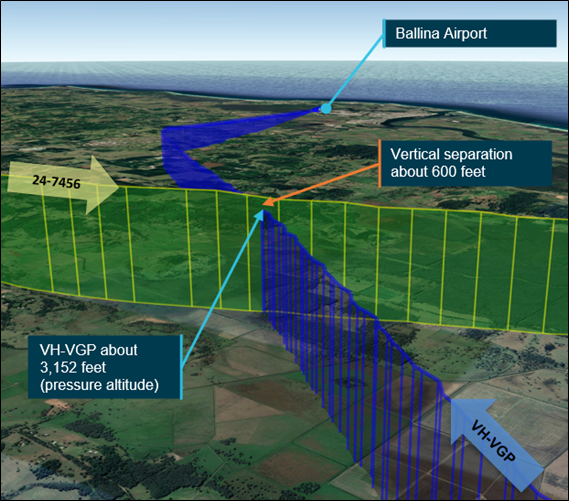
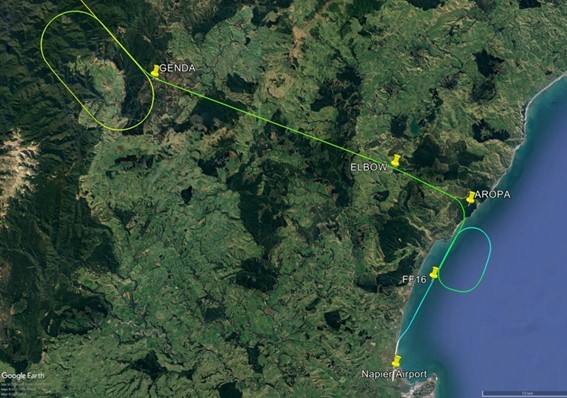
At 1621 local time, when the aircraft was passing 6,600 ft AMSL[5] and approximately 12 NM from the airport, the trainee ADC advised the flight crew that a straight-in visual approach was now available and asked if they could track direct to ALDIM, which was around 10 NM south-west of their position (Figure 1).
Figure 1: Actual and intended flight paths
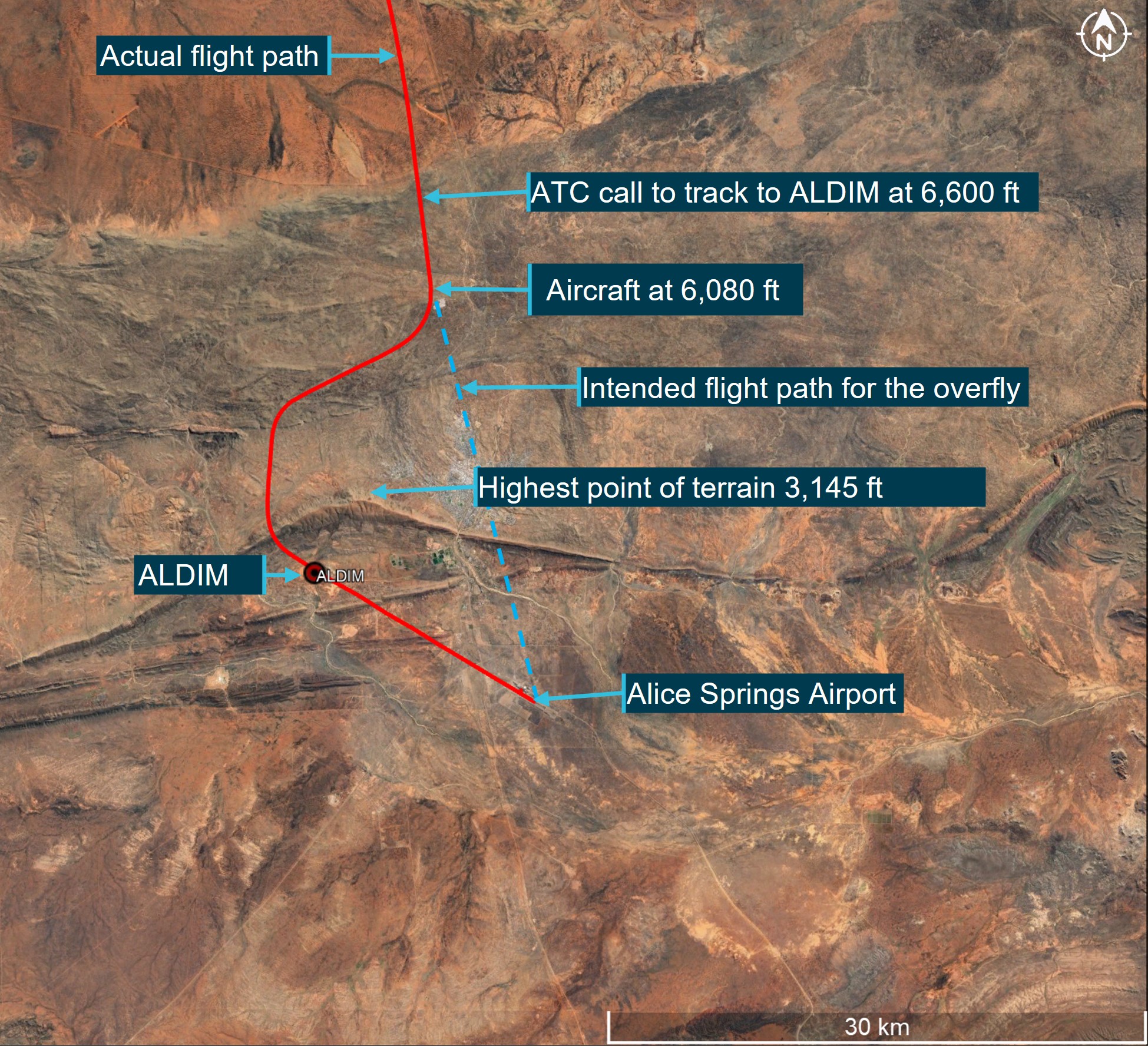
Source: Google Earth overlaid with flight data, annotated by ATSB
The PM advised ATC that they could accept the straight-in approach but would need extra track miles to configure the aircraft (as the aircraft was at a higher altitude than it normally would be for that approach). The trainee ADC cleared the crew to track right of track as required to ALDIM and cleared them for a visual approach.
During a visual approach, flight crew are required to maintain visual separation with terrain and manage the descent profile as required to intercept the final approach. Once the flight crew acknowledged the clearance, the trainee ADC and OJTI turned their attention to other traffic.
The crew initiated a turn to the west, and thirty seconds later they extended the slats to 15° then selected a target altitude of 3,300 ft AMSL (1,500 ft above aerodrome level (AAL))[6] on the guidance panel (see the section titled Altitude select mode). They then extended the flaps to position 1 (7°) and deployed the speedbrakes[7] to expedite the aircraft’s descent.
The PM suggested the PF use the flight level change (FLCH) mode in the autoflight system, which the PF selected. After FLCH was selected, the autoflight system reduced the selected speed to 175 kt before the PF manually increased it to 200 kt.
At 1622:44, passing 4,692 ft AMSL, the crew considered that the aircraft was still too high, and they extended the landing gear to add further drag to the aircraft. The crew commenced a turn towards ALDIM at this time. The PF later recalled that as the landing gear was extending, the aircraft pitched down more than expected.
About 8 seconds later, as the landing gear locked in the down position, the aircraft’s autoflight mode was changed from FLCH to flight path angle (FPA). The flight crew did not recall selecting this mode change and did not detect it. During the next 6 seconds, as the aircraft descended below 4,000 ft AMSL (1,800 ft radio altimeter height),[8] the rate of descent increased to more than 3,000 ft/min.
At 1623:00, in an attempt to reduce the observed rate of descent, the PF selected a higher altitude (from 3,300 to around 5,000 ft) on the altitude selector. However, the aircraft did not respond as the crew expected. The PF then increased the selected altitude to 8,800 ft, which also had no effect on the rate of descent (see the section titled Flight path angle mode).
The PM recalled that at this time they were looking outside to visually ensure terrain separation rather than monitoring the automation as they were aware of surrounding high terrain and an upcoming ridge line which they were required to cross. As a result, the PM was not monitoring the aircraft’s vertical speed or vertical modes during this period.
At 1623:12, as the aircraft approached 2,973 ft AMSL (1,498 ft radio altimeter height), the PM advised the PF to disconnect the autopilot and initiate a climb due to the terrain proximity. The PF disconnected the autoflight system and pitched the aircraft up to initiate a climb, leaving the autothrottle engaged and the landing gear, speedbrakes and flaps extended.
Although the rate of descent started to decrease, the thrust did not increase for 8 seconds, and the aircraft continued to descend. As thrust was eventually applied through the autothrottle, the aircraft started to climb and the crew manually reduced the aircraft’s selected speed to 185 kt.
Shortly after, the OJTI observed the aircraft on the tower situational awareness display (TSAD)[9] approximately 10 NM from the airport at approximately 3,300 ft AMSL, which the controller thought was lower than usual. The controller then looked out the window and was unable to see the aircraft above the adjacent ridge line, which the controller described as ‘alarming’, and instructed the trainee ADC to issue the flight crew a terrain safety alert[10] which was issued at 1623:40.
The PM acknowledged the alert, after which the OJTI sighted the aircraft climbing above the ridge line (at about 1,700 ft AGL). About 30 seconds after passing ALDIM, the aircraft intercepted the instrument landing system (ILS)[11] glideslope from below and the glide slope was maintained until landing.
The captain later stated that while the approach (Figure 2) was ‘untidy’, they were aware of, and visual with terrain, and did not feel that the flight was in danger at any time.
There were no EGPWS alerts or warnings.
Figure 2: Flight path over terrain
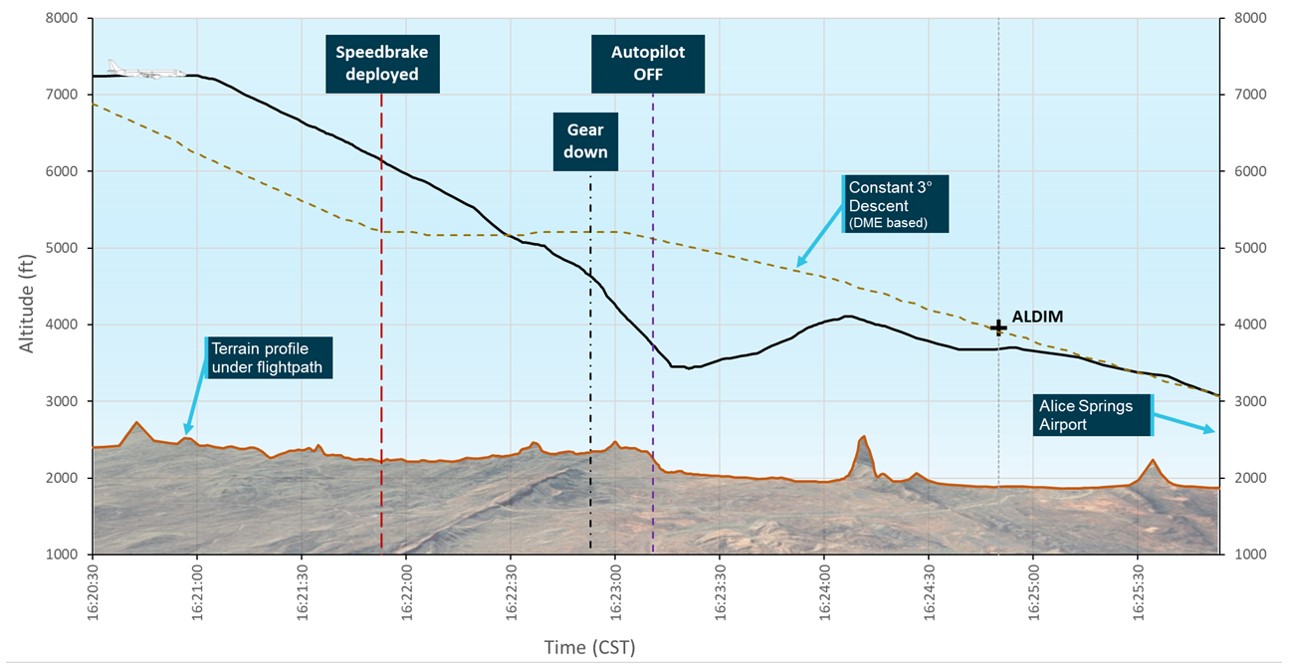
The representation of a constant 3° approach profile (brown dashed line) is based upon the DME distance from Alice Springs and is not a straight line, as may be expected for a constant 3° approach. Firstly, a 3° approach is a geometric profile, but the horizontal axis of the plot is time, so any variations in speed will distort it from a straight line. Also, the path in Figure 2 follows along the actual flight path, not a straight-in 3° approach. As such, when the aircraft is flying in a south-westerly direction, it is flying roughly tangentially to a circle centred on the DME transmitter, that is, the DME distance is not changing significantly during that period of time, so the 3° approach in Figure 2 flattens out.
Source: ATSB
Context
Flight crew
The captain and first officer each held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The captain had over 18,000 hours of flying experience, of which about 450 were on the E190 aircraft type. The first officer had over 4,300 hours of flying experience, of which about 750 were on the E190.
Both flight crew members regularly operated from Darwin to Alice Springs and were familiar with the approach and surrounding terrain. They reported feeling well rested and alert at the time of the incident and stated that there were no distractions or stressors in the cockpit prior to the incident.
Alice Springs approach
When conditions favoured a visual approach to runway 12 at Alice Springs, the captain’s preference was to conduct a straight-in ILS approach on a standard 3° profile as per the operator’s standard operating procedures, intercepting the localiser at or before waypoint ALDIM, which was the final approach fix for runway 12. An aircraft on the 3° approach profile would cross ALDIM at 3,960 ft AMSL. The minimum height at ALDIM was 3,600 ft to provide separation with the nearby ridge line, which was 3,145 ft AMSL.
While the flight crew maintained visual separation with terrain and the above minimum altitude requirements did not apply to the visual approach, it was the crew’s intention to approximately follow the approach profile and overfly ALDIM at 3,960 ft to intercept the ILS glideslope.
Aircraft
The aircraft was an ERJ 190-100 IGW, manufactured in Brazil in 2019 and issued serial number 19000095. It was registered in Australia as VH-UYN on 3 August 2021. The aircraft was fitted with 2 General Electric Company CF34-10E5 turbofan engines.
Autoflight control system
The ERJ 190 autoflight control system is controlled from the guidance panel, located on the glareshield panel in the cockpit. This panel allows either the captain or the first officer to select the flight guidance control system functions.
Flight Director
The E190 aircraft maintenance manual (AMM) stated that:
the Flight Guidance Computer System calculates the Flight Director (FD) commands that show on the primary flight display (PFD). The FD system has two categories of operation modes: vertical axis and lateral axis. The vertical FD modes supply the FD guidance commands.
Vertical flight modes
Mode selection
The autoflight control system (AFCS) has 11 modes that control the aircraft’s vertical flight path. These can either be engaged automatically by the flight management system (FMS), or by flight crew selection using the guidance panel (Figure 3).
Figure 3: E190 Guidance panel
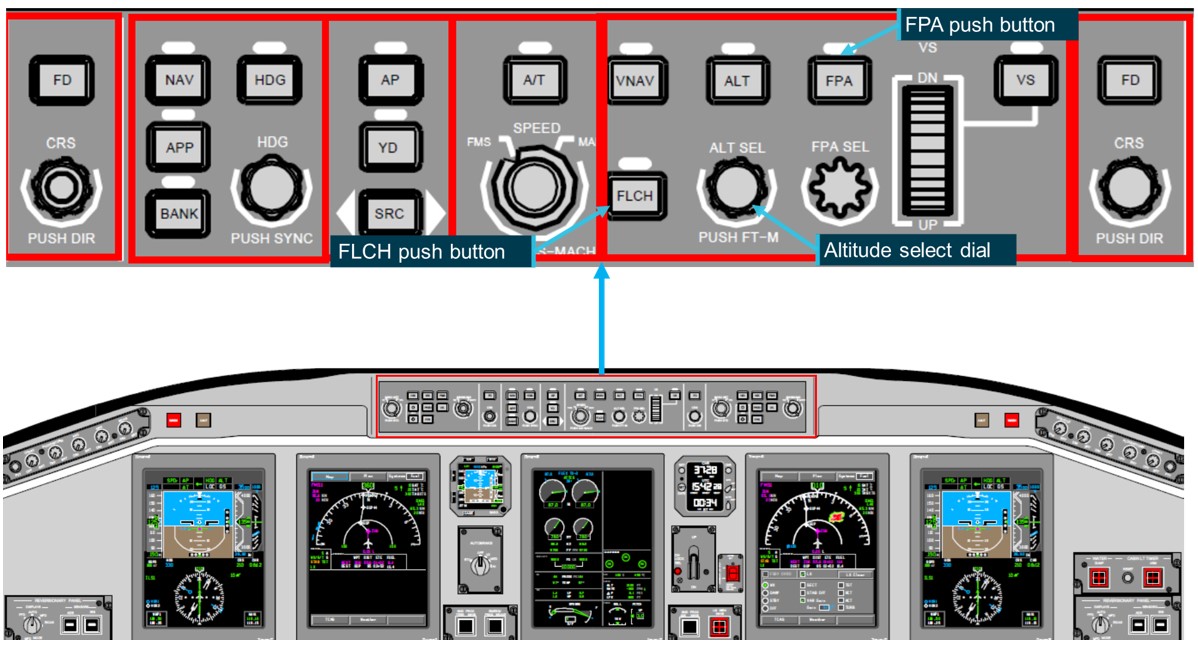
Source: Alliance Airlines training material annotated by ATSB
The engaged mode is illuminated on each primary flight display. When a flight mode change is selected by the flight crew, the active mode is displayed and flashes in reverse video with a green background for 3 seconds (Figure 4). When the FMS changes the vertical mode, the active mode flashes in magenta.
Figure 4: Automatic flight control system flight modes on the primary flight display
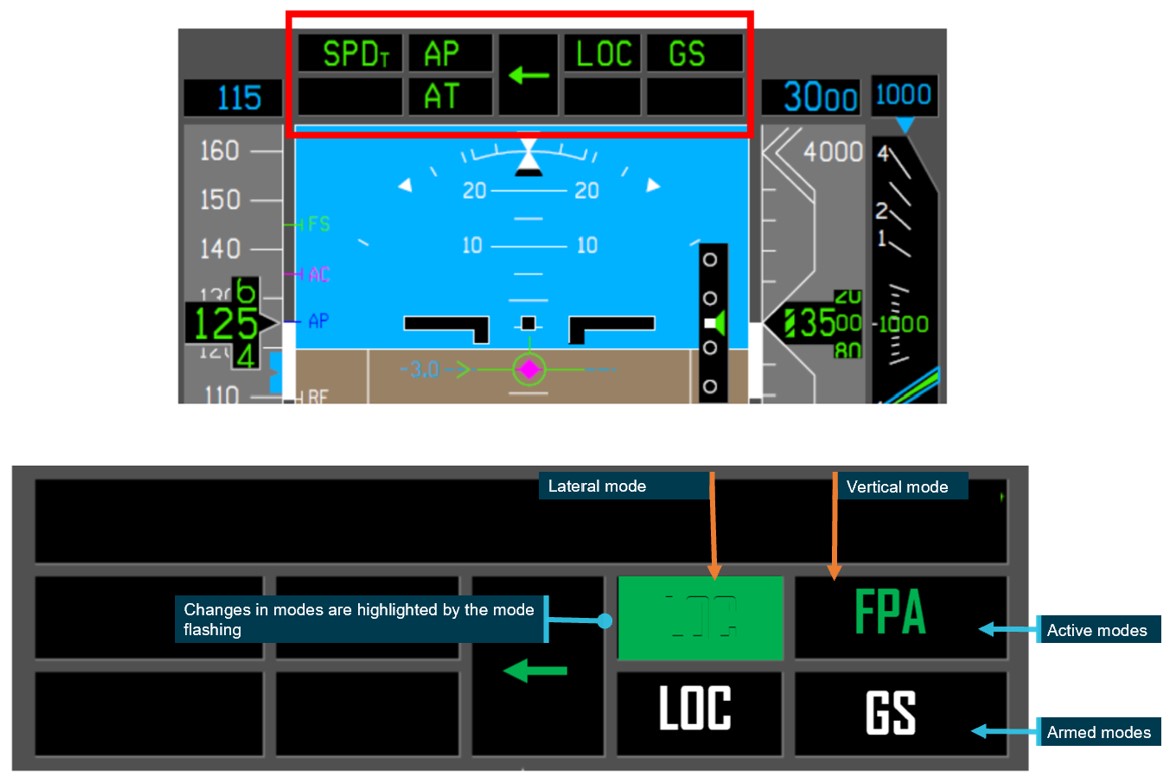
Diagram is showing the reverse video with a green background.
Source: Alliance training material annotated by ATSB
Flight level change mode
According to the operator’s E190 aircraft operations manual (AOM), FLCH mode provides commands to climb or descend to the selected altitude while holding the selected speed. The speed selected will be controlled via pitch changes through elevator inputs. The aircraft’s thrust will not be adjusted.
FLCH mode is activated by pressing the FLCH button and deactivated when another vertical mode is selected or by pressing the FLCH button again.
The aircraft manufacturer advised that the FD, while in FLCH mode, will not generate commands that could lead the aircraft to exceed the aircraft’s maximum operating limit speed (Vmo/Mmo). The FD has an overspeed protection function in which the normal acceleration limit is set to ± 0.3 G. This function tracks the selected calibrated airspeed (CAS) target within ± 5 kts or the selected Mach target within ± 0.02 Mach, depending on whether the controlling speed target is CAS or Mach.
They also advised that the FLCH mode will revert to basic mode (FPA) when an invalid condition is detected. Should this occur, the CAS message FD VERT MODE OFF would be announced and recorded in the aircraft flight data. An invalid condition is when an input parameter is considered invalid due to a sensor failure or when the parameter value exceeds the expected limits. A review of the occurrence flight data by the ATSB identified no CAS messages.
Flight path angle mode
According to the manufacturer’s E190 AMM, the FPA mode supplies guidance to keep a set flight path angle[12] reference. The operator’s E190 AOM stated that FPA:
- is the basic vertical mode (except for take-off)
- can be used for vertical navigation by selecting a higher or lower altitude on the ALTSEL and then pressing the FPA button
- becomes the active mode when:
- the autopilot is engaged and no flight director (FD) mode is selected
- the FPA button is selected on the guidance panel
- a lateral mode is selected and no vertical mode is selected
- the active vertical mode is deselected.
The pilot selects the required flight path angle using the FPA select knob on the guidance panel, however if no flight path angle is specified when FPA is selected, the FD will select and hold the current flight path angle via elevator movements. The autothrottle will adjust the thrust levers to maintain the selected airspeed.
Altitude select mode
The E190 AMM stated that:
the FD supplies flight path commands to lock on the set altitude
The aircraft manufacturer stated that when in FPA mode, as the aircraft’s altitude begins to approach the selected altitude, the mode will automatically change to ASEL until the altitude is captured and it will then change to altitude hold mode. However, ASEL mode is disarmed automatically if the selected altitude is changed. If this occurs the FD will automatically reselect FPA.
Autothrottle
The E190 AOM stated that when the FD is selected off and there are no active modes on the flight mode annunciator, the autothrottle will adjust the thrust levers to maintain the selected airspeed.
The operator’s standard operating procedures manual stated that:
The autothrottle should be used during the entire flight, engaged just prior to take-off and disengaged after touchdown or at the PF’s discretion. Pilots must always be alert and monitor the autothrottle operation checking the movement of the thrust levers in the correct direction. Normally, high level of automation induces crews to stay out of the loop, with excessive confidence on automatic flight systems.
The AOM further stated that:
The autothrottle (AT) can be overridden by moving the thrust levers in any direction without causing its disengagement. If the AT is overridden by a pilot. ‘’OVRD’ is displayed on the flight mode annunciator. When the thrust levers are released, the AT will once again return the thrust levers to their command position.
Flight data
The incident flight data from the aircraft’s quick access recorder was analysed by the ATSB and the aircraft manufacturer, Embraer (Figure 5) and (Table 1).
A review of the data identified that between the 2-minutes between 1621:13 and 1623:12 (from when the aircraft turned towards ALDIM until the autopilot was selected off), the aircraft was configured with flap and slats and flight level change (FLCH) mode was selected. Then as the landing gear locked down, flight path angle (FPA) mode was selected in the flight management system (FMS). The FMS then automatically changed to altitude select (ASEL) mode as the aircraft neared the selected altitude and while this was active, the throttle lever position increased (consistent with normal autothrottle operation) indicating the aircraft was starting to level off. However, prior to this occurring, the selected altitude was manually changed, and the flight mode reverted to FPA, and the throttle lever position automatically reduced.
The data also showed that between the first and second selection of the higher altitude in the altitude selector, the autothrottle override activated for 3 seconds. The autopilot was then intentionally disconnected, and as the speed started to reduce to the selected speed of 200 kt, the autothrottle began to increase the throttle lever angle, reducing the rate of descent. The crew then reduced the selected speed to 185 kt. This resulted in the autothrottle increasing the thrust further and the aircraft started to climb.
Figure 5: VH-UYN active flight modes on approach
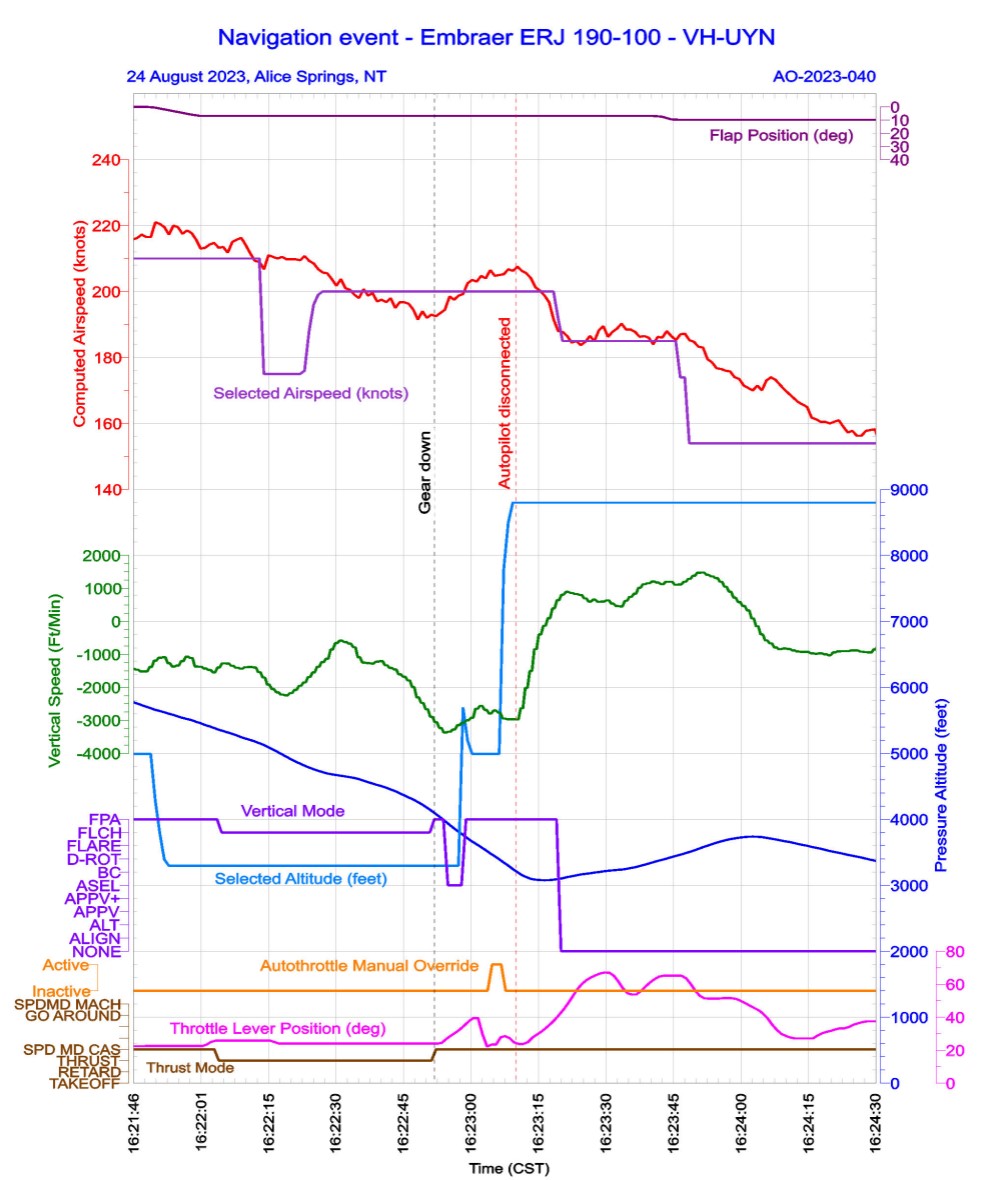
Source: ATSB
Table 1: Excerpt from QAR data for incident flight
| Time (CST) | Significant event | Vertical mode | Vertical speed (f/m) | Radio height (ft) | Altitude (ft) (AMSL) | Flight path angle (degrees) | Selected Altitude (ft) (AMSL) |
| 1621:13 | ATC cleared the aircraft for a visual approach via ALDIM | FPA | 6,600 | 4,992 | |||
| 1621:47 | Slats 15 selected | FPA | 5,995 | -5.98 | 4,992 | ||
| 1621:54 | 3,300 ft selected altitude | FPA | 5,862 | -4.75 | 3,392 | ||
| 1621:59 | Flaps 1 and speedbrakes selected | FPA | 5,760 | -4.39 | 3,392 | ||
| 1622:07 | PF selected FLCH | FLCH | -1,274 | N/A | 5,578 | -5.27 | 3,296 |
| 1622:46 | PF selected Gear down | FLCH | -1,604 | N/A | 4,392 | -11.25 | 3,296 |
| 1622:54 | Gear down and locked and crew member selected FPA (or deselected FLCH) | FPA | -3,056 | 2,290 | 4,319 | -14.77 | 3,296 |
| 1622:55 | FPA | -3,229 | 2,219 | 4,268 | -15.47 | 3,296 | |
| 1622:56 | FPA | -3,371 | 2,167 | 4,213 | -15.64 | 3,296 | |
| 1622:57 | ASEL | -3,346 | 2,100 | 4,157 | -15.29 | 3,296 | |
| 1622:58 | ASEL | -3,277 | 2,032 | 4,102 | -14.77 | 3,296 | |
| 1622:59 | ASEL | -3,145 | 1,947 | 4,051 | -14.41 | 3,296 | |
| 1623:00 | PF wound up selected altitude | ASEL | -3,075 | 1,843 | 4,003 | -14.06 | 5,696 |
| 1623:01 | FMS selected FPA | FPA | -3,000 | 1,809 | 3,951 | -13.89 | 5,200 |
| 1623:02 | FPA | -2,921 | 1,798 | 3,902 | -12.66 | 4,992 | |
| 1623:03 | FPA | -2,647 | 1,770 | 3,861 | -11.78 | 4,992 | |
| 1623:04 | FPA | -2,562 | 1,719 | 3,816 | -12.13 | 4,992 | |
| 1623:05 | FPA | -2,682 | 1,710 | 3,772 | -12.83 | 4,992 | |
| 1623:06 | Autothrottle override activated | FPA | -2,795 | 1,673 | 3,723 | -12.66 | 4,992 |
| 1623:07 | FPA | -2,701 | 1,613 | 3,680 | -12.48 | 4,992 | |
| 1623:08 | FPA | -2,766 | 1,559 | 3,633 | -13.36 | 4,992 | |
| 1623:09 | PF wound up selected altitude | FPA | -2,945 | 1,541 | 3,589 | -13.71 | 7,792 |
| 1623:10 | FPA | -2,968 | 1,517 | 3,537 | -13.71 | 8,496 | |
| 1623:11 | FPA | -2,966 | 1,519 | 3,486 | -13.71 | 8,800 | |
| 1623:12 | PF disengaged autopilot | -2,973 | 1,498 | 3,439 | -12.83 | 8,800 | |
| 1623:13 | -2,632 | 1,501 | 3,395 | -10.02 | |||
| 1623:14 | -2,017 | 1,471 | 3,363 | -7.56 | |||
| 1623:15 | -1,501 | 1,438 | 3,337 | -4.75 | |||
| 1623:16 | -844 | 1,410 | 3,325 | -2.86 | |||
| 1623:17 | -394.63 | 1,400 | 3,319 | -0.88 | |||
| 1623:18 | -132.5 | 1,381 | 3,316 | 0 | |||
| 1623:19 | 97.38 | 1,361 | 3,318 | 1.58 | |||
| 1623:40 | ATC issue safety alert ‘terrain’ | 1,128 | 1,682 | 3,325 | 5.80 |
There is a resolution difference between the recorded data and the pilot’s flight display, which only shows to the nearest 100 ft.
Company procedures
The operator’s operations policy and procedures manual stated the following values for the rate of descent below the transition altitude[13] shall not normally be exceeded:
- 3,000 ft/min down to an altitude of 3,000 ft AAL
- 2,000 ft/min down to an altitude of 2,000 ft AAL transitioning to 1,000 ft AAL
- 1,000 ft/min below 1,000 ft AAL
The decrease in recommended descent rate with altitude was to ensure increased recognition and response times in the event of an unintentional conflict with terrain.
Regarding roles and responsibilities, the operator’s manual stated that:
The PF is responsible for controlling the vertical flight path and horizontal flight path and for energy management by either:
• Supervising the auto pilot vertical and lateral modes through awareness of modes being armed or engaged, mode changes and of selected mode targets; or
• Hand flying the aircraft, with or without flight director guidance.
The PNF [PM] is responsible for:
• Systems related monitoring
• Monitoring tasks
• Performing the actions requested by the PF.
Crew training
It was an operator requirement for flight crew to monitor the automatic flight control system, and flight crew were trained to intervene, and disconnect the automation if the aircraft did not respond in the way the flight crew wanted or expected.
Workload
The PF stated that the autopilot mode changes would have been flashing on the multifunction display and while they probably saw the changes, it was likely that they did not actively absorb that information due to the high workload in the cockpit.
Research looking at unexpected changes in workload during flight has found that pilots who encounter abnormal or emergency situations experience a higher workload with an increase in the number of errors compared to pilots who do not experience these situations (Johannsen and Rouse, 1983).
Safety analysis
When ATC asked the flight crew if they could alter their flight path to conduct a straight-in approach (instead of overflying the airport), the aircraft was approximately 12 NM from the airport and passing 6,600 ft AMSL on descent. The crew accepted and, on request, were cleared to track as required to ALDIM, which was about 10 NM from the aircraft.
With the intention of crossing ALDIM between 3,600 and 4,000 ft, the crew elected to increase the rate of descent by extending slats, flaps and speedbrakes, and then selected flight level change mode (FLCH) in the flight management system to ensure the aircraft did not exceed the 210 kt speed requirement set by ATC.
When the aircraft was 5.4 NM from ALDIM and passing 4,692 ft AMSL (around 800 ft higher than the intended crossing altitude at ALDIM), the crew further increased their descent rate by extending the landing gear despite the aircraft having sufficient track miles remaining to comfortably intercept a normal descent profile.
As the aircraft was in FLCH, there were no automated thrust changes. Consequently, when the landing gear was extending and the aircraft entered a turn, the increase in drag was not offset by an increase in thrust. As a result, the aircraft pitched nose down to maintain the selected speed of 200 kt, which increased the rate of descent significantly.
Shortly thereafter, and possibly influenced by their workload, the PF inadvertently changed the selected vertical control mode to flight path angle (either by selecting FPA or deselecting FLCH). At this time, the captain’s attention was outside the cockpit, monitoring terrain clearance, and they did not detect the mode change.
As the aircraft continued to descend, the flight director entered altitude select mode to level off at 3,300 ft. The crew did not detect the mode change or that the aircraft was levelling off. Rather, in an attempt to arrest the rate of descent, the PF selected a higher altitude. In doing so, the altitude select mode was deselected, the flight director automatically reverted to FPA mode and selected the current flight path angle, which at that time was -13°. Subsequently, the PF momentarily overrode the autothrottle by manually increasing the thrust and then selected a higher altitude. The aircraft descended to 1,498 ft (AGL) during this period at a 2,973 ft/min rate of descent.
In response to the excessively high rate of descent, the flight crew turned off the autopilot and raised the nose, leaving autothrottle engaged and the selected speed unchanged. Given the aircraft’s speed was above the selected value, the autothrottle did not immediately increase thrust and the aircraft continued descending (to 1,381 ft AAL) until the speed decreased towards the selected speed. The crew then selected a lower speed and the autothrottle increased to climb power.
When the OJTI detected that the aircraft was not where they expected, they immediately instructed the trainee controller to make a terrain safety alert. However, in this case the crew had already taken action to correct the descent.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the navigation event involving Embraer E190, VH-UYN, 20 km north-west of Alice Springs, Northern Territory, on 24 August 2023.
Contributing factors
- After accepting an ATC request at short notice to conduct a straight-in approach, the flight crew unnecessarily configured the aircraft with high drag in flight level change to expedite the descent. As the aircraft pitched down to maintain airspeed, the pilot flying made an inadvertent mode selection in the automatic flight system that went undetected by the flight crew.
- Due possibly in part to their workload, the pilot flying did not identify that the aircraft was starting to automatically capture the selected altitude, and selected a higher altitude, which disarmed the altitude select mode. This resulted in the flight director resuming the high rate of descent close to terrain. These changes were not promptly identified by the pilot monitoring due in part to their focus to visually assessing the terrain clearance.
Key finding
- The air traffic controller on the job training instructor detected the unusual descent and immediately alerted the flight crew.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the captain
- the first officer
- the operator
- the aircraft manufacturer
- the controller
- Airservices Australia
- recorded data from the aircraft’s quick access recorder
References
Airservices Australia, 2023. Manual of Air Traffic Services, Version 66.4, p.294
Alliance Airlines – training material ‘automatic flight 2.0’
Alliance Airlines, 2022. E190 Aircraft Operations Manual, Volume 2, Section 3 - Automatic Flight, Issue 1.2, pp. 38-42
Alliance Airlines, 2023. Operations policy and procedures manual, v. 2.13, Chapter 7 – Approach procedures, p. 430
Alliance Airlines, 2021, Standard operating procedures manual, issue 1.1, section 4.5 – Use of autothrottle, p 45.
Embraer S.A., 2023. Embraer 190/195 Aircraft Maintenance Manual, Part 1 – Flight Guidance and Control System, pp.60-66
Johannsen, G & Rouse, WB, 1983. Studies of planning behaviour of aircraft pilots in normal, abnormal, and emergency situations. Systems, Man and Cybernetics, IEEE Transactions on, (3), pp.267-278.
International Civil Aviation Organisation Regional Aviation Safety Group – Pan America, Safety Advisory -09 ‘Mode awareness and energy state management aspects of flight deck automation’, 2022.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- flight crew
- operator
- controller
- Airservices Australia
- Civil Aviation Safety Authority
- Embraer
- Aeronautical Accidents Investigation and Prevention Centre (CENIPA), Brazil
A submission was received from:
- Embraer
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[3] Runway number: the number represents the magnetic heading of the runway.
[4] Waypoint: A specified geographical location used to define an area navigation route or the flight path of an aircraft employing area navigation. ALDIM was the final approach point on the ILS for runway 12.
[5] Above mean sea level (AMSL): The vertical distance of a level, a point, or an object considered as a point measured from mean sea level.
[6] Above aerodrome level (AAL): The elevation of the highest point of the landing area. This is usually the same as the altitude above ground level (AGL), but AAL is more precise, as in extremely hilly or mountainous areas, elevation AGL can change dramatically over small distances.
[7] Speedbrakes: spoilers are panels mounted on the upper surface of the wing that, when extended, both increase drag and decrease lift by disrupting the airflow over the wing. On the Embraer E190, the spoilers serve as ground spoilers, roll spoilers and flight spoilers (speedbrakes).
[8] A radio altimeter is an onboard electronic device capable of measuring the height of the aircraft above terrain immediately below the aircraft. The radio altimeter activates when the aircraft is within 2,500 ft of terrain.
[9] Tower Situation Awareness Display (TSAD) is used by the controller for situational awareness to assist with traffic management. The TSAD shows controllers the aircraft’s altitude and groundspeed, and depicts whether the aircraft is descending, climbing or in level flight. Controllers can use the information displayed on the TSAD for situational awareness; however, on and in the vicinity of the aerodrome, controllers are required to maintain visual observation of operations and apply procedural standards and procedures.
[10] Safety alert: the provision of advice to an aircraft when an ATS officer becomes aware that an aircraft is in a position which is considered to place it in unsafe proximity to terrain, obstructions, active restricted or prohibited areas, or another aircraft.
[11] Instrument Landing System (ILS): a precision instrument approach system which normally consists of a VHF localiser, UHF glide slope and VHF marker beacons.
[12] Flight path angle: the angle between the flight path vector, where the aircraft is going and the horizon; the aircraft's climb/descent angle.
[13] Transition altitude: When passing an altitude of 10,000 ft, aircraft transition from using the area QNH to set their altimeter to a standard setting of 1013 hPa.
Occurrence summary
| Investigation number | AO-2023-040 |
|---|---|
| Occurrence date | 24/08/2023 |
| Location | 20 km north-west of Alice Springs Airport |
| State | Northern Territory |
| Report release date | 02/08/2024 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Flight Preparation / Navigation |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Embraer-Empresa Brasileira De Aeronautica |
|---|---|
| Model | ERJ 190-100 IGW |
| Registration | VH-UYN |
| Serial number | 19000095 |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Darwin Airport, Northern Territory |
| Destination | Alice Springs Airport, Northern Territory |
| Damage | Nil |