A transport safety investigation is underway into the derailment of a passenger train between Rushall and Clifton Hill stations on 13 July 2025.
At about 2230 on 13 July 2025, a Metro Trains Melbourne passenger train travelling from Mernda station to Flinders Street Station derailed between Rushall and Clifton Hill stations.
The derailed train collided with stanchions carrying overhead wires, resulting in substantial damage to the overhead infrastructure. About 100 metres of track and one passenger car were also significantly damaged.
There were no injuries to passengers or train crew in the incident.
The Office of the Chief Investigator is investigating the incident under the Transport Safety Investigation Act 2003 (Cth) under a collaboration agreement with the Australian Transport Safety Bureau.
A preliminary report, which details factual information established in the investigation’s early evidence collection phase, was released on 3 October 2025. See below.
The final report will be released at the conclusion of the investigation. However, should a critical safety issue be identified during the investigation, the ATSB and OCI will immediately notify relevant parties so safety action can be taken.
Last updated:
Preliminary report
Report release date: 03/10/2025
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Summary video
The occurrence
Background
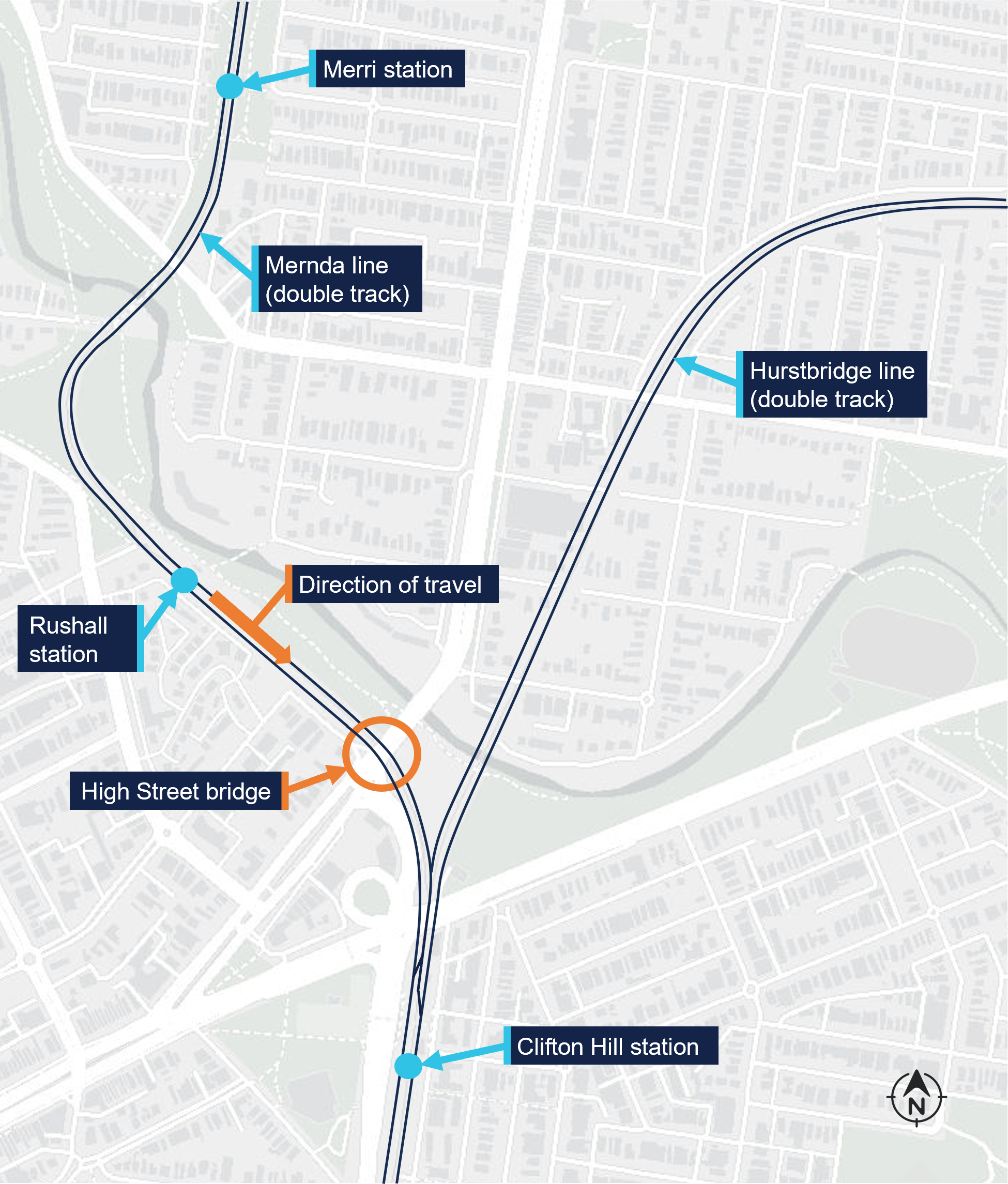
On 13 July 2025, a Metro Trains Melbourne (MTM)[1] train was providing passenger services on the Mernda and Hurstbridge lines on the metropolitan network in Melbourne, Victoria (Figure 1). The train comprised 2 coupled X’Trapolis 3-car sets.
Figure 1: Mernda and Hurstbridge lines
Source: Digital Atlas of Australia,annotated by the Office of the Chief Investigator (OCI)
That evening, it was scheduled to undertake a final round trip from Flinders Street Station (Melbourne) to Mernda and return. For this round trip, there were 2 drivers in the driving cab, the rostered driver and a principal driver.[2] The principal driver was in control of the train for this round trip as they were seeking to maintain familiarity with driving this route. The outbound journey from Melbourne to Mernda was uneventful, and the train arrived at Mernda station at about 2131.
The derailment
At about 2146, the train departed Mernda towards Melbourne as service TD1094, the final service of the evening before the line was to close for overnight maintenance. Initially the service proceeded as normal, stopping at all stations. At about 2225 the train departed Merri station and transited through a tight radius left curve before arriving at Rushall. It departed Rushall station at about 2227 travelling towards Clifton Hill (Figure 2).
Figure 2: Path of service TD1094 towards the High Street bridge
Overview of the incident area and the location of the High Street bridge. Source: Digital Atlas of Australia,annotated by OCI
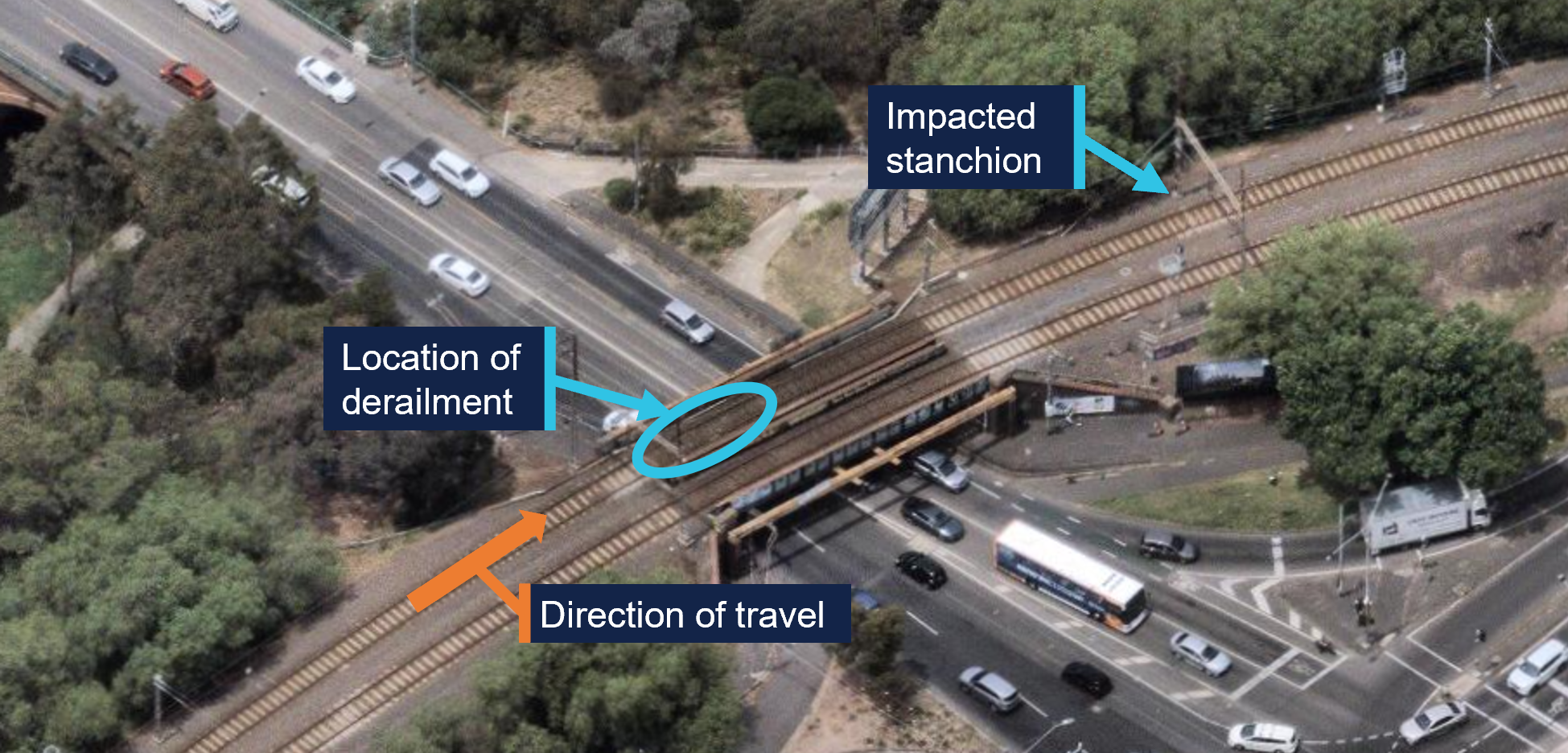
After its departure from Rushall, the train initially accelerated to about 38 km/h. The driver then reduced the train’s speed in preparation for the right curve over the High Street bridge.[3] It was this driver’s normal practice to slow to about 30 km/h for this curve, which had a 40 km/h permitted speed. At about 2228 the train was proceeding through the curve at about 28 km/h when the leading wheelset of the first bogie of the 5th car derailed on the bridge (Figure 3). The left wheel of this wheelset had climbed over the left rail toward the outside of the right curve.
Figure 3: Location of derailment on the High Street bridge
Source: Nearmap,annotated by OCI
As a result of the leading wheelset moving to the left, the right wheel dropped to the inside of the right rail. The train continued to cross the bridge with the derailed wheelset impacting rail fixtures and sleepers. Witness marks on sleepers were consistent with the initial derailment being a single axle (Figure 4).
Figure 4: Marks made on sleepers by the derailed wheels
Source: OCI
Initially the derailed wheels moved along the sleepers in close proximity to the rails. However, once off the bridge deck, the wheel path began to move further to the left until the front of the car-body and the first bogie struck a stanchion, part of an overhead wiring gantry. The impact of the front left corner of the bogie with the stanchion further rotated the bogie in an anticlockwise direction,[4] derailing its trailing axle toward the inside of the right curve and pushing the leading end of the 5th car back towards the alignment of the track.
The stanchion was substantially damaged by the impact (refer to photo at top of page) which caused the overhead wire that supplied electrical power to trains to move and lose tension. This resulted in electrical arcing between the overhead wire and the train, most probably the pantograph[5] mounted on top of the 5th car.[6]
The 2 drivers were not initially aware of the derailment. Instead, they were alerted to an issue when they heard the electrical arcing and observed the overhead wire moving in front of the train. The principal driver made a brake application, and the train was brought to a stop after travelling about 120 m in a derailed state. The train’s carriages remained connected, and the internal passenger compartment spaces were not damaged. There were no injuries to passengers or train crew.
Incident response and passenger evacuation
At 2229, after stopping the train, the principal driver made a radio call to the MTM train control centre (Metrol) informing them of a probable issue with the overhead power. In discussion, the principal driver and the Metrol train controller agreed that the principal driver would investigate further. The principal driver moved to the rear of the leading 3‑car set before alighting on the train’s left side. The other driver remained in the leading driving cab at the controls of the train.
An operator at MTM’s electrical systems control centre (Electrol) had also identified a potential electrical issue in the area at about the same time. Circuit breakers at sub‑stations supplying power to the Rushall station area had tripped. At about 2230, in response, field staff were tasked to patrol the area and look for a fault. Shortly after, the Metrol train controller notified Electrol of the train’s loss of power. Responding to the updated information, Electrol arranged for the overhead power response team to attend the incident.
Meanwhile, the principal driver proceeded back along the outside of the train and observed that that the leading bogie of the 5th car was derailed. They recalled that they attempted to call Metrol by mobile phone to inform them of the derailment, however the line was busy. They then called one of MTM’s rail incident commanders (RIC)[7] and informed them of the derailment.
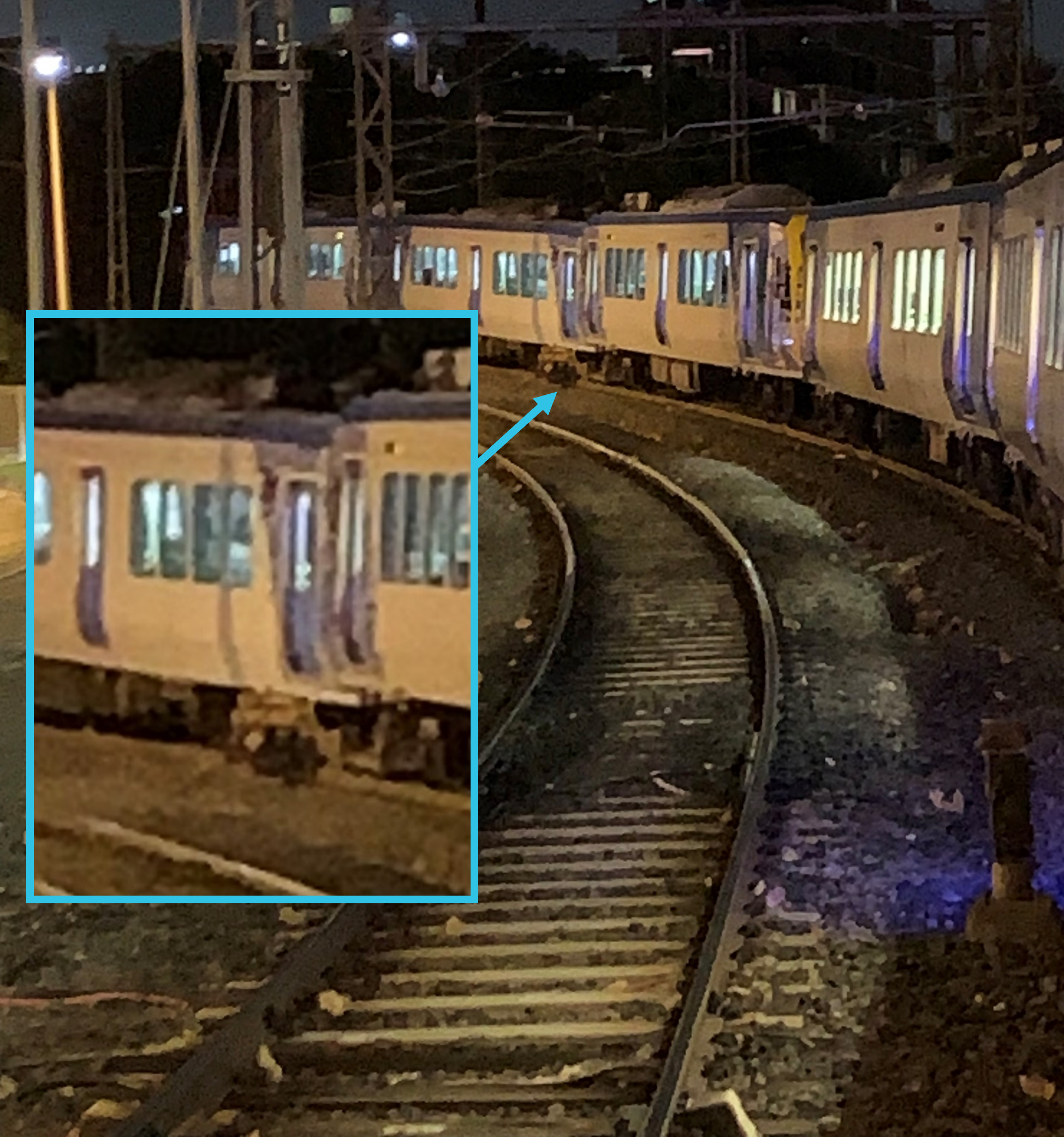
While the principal driver was inspecting the train from its left side, the driver who remained in the driving cab looked down the right side of the train and observed the trailing axle of the leading bogie on the 5th car derailed to that side (Figure 5). They reported the derailment to Metrol by train radio at 2239.
Figure 5: View of derailment from the front of the train
Source: Supplied
The RIC arrived at the incident at about 2306 and the overhead power response team arrived at about 2310. At about 2317 the RIC reported their observations to Metrol including the substantial damage to the overhead power stanchion.
There were about 30 passengers on board the train at the time of the derailment.[8] Passengers were moved into the leading car of each 3‑car set (the 1st and 4th cars) to wait until it was safe to detrain. While they waited, passengers in the 4th car repeatedly forced open the mid‑car passenger doors. However, passengers remained on board and did not self-detrain.
At about 0128 following confirmation from the overhead power response team that the site had been made safe, the RIC reported to Metrol that it was safe to detrain passengers. Passengers were detrained through the driving cab doors of the 3rd and 4th cars with no reported injuries during the evacuation.
Context
The train
Configuration
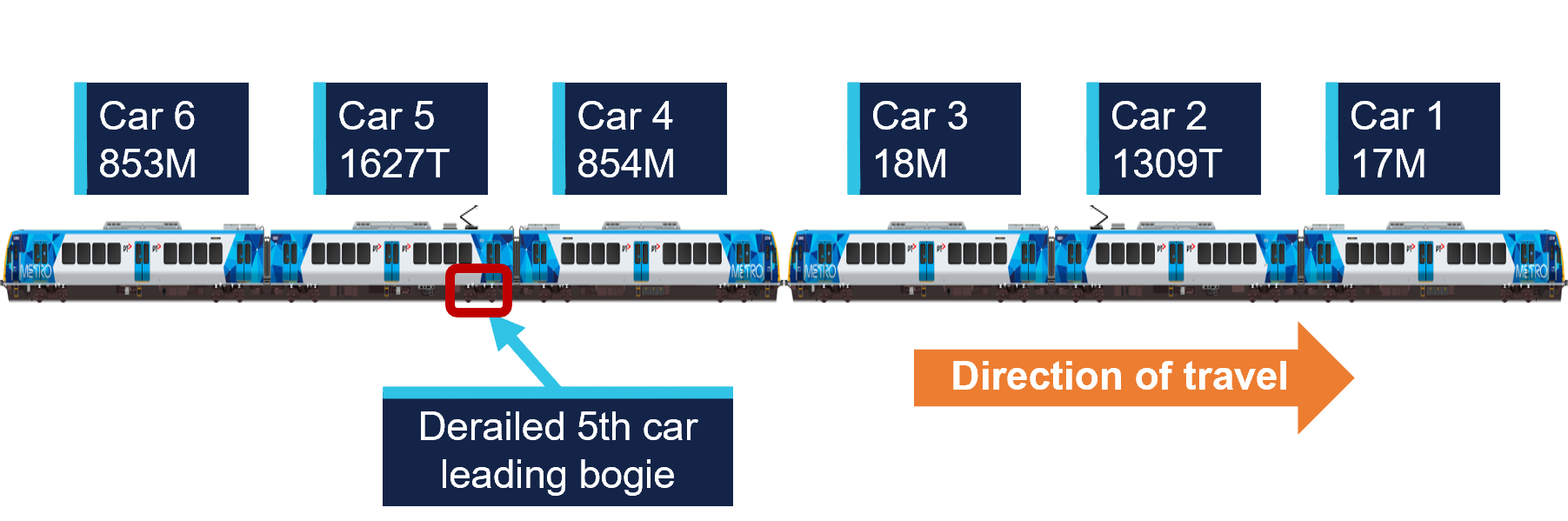
The train operating as TD1094 was a 6-car set made from 2 coupled X’Trapolis 3‑car sets.[9] The leading car‑set comprised cars 17M, 1309T and 18M and the trailing car‑set comprised cars 854M, 1627T and 853M (Figure 6).
Figure 6: Orientation of train for service TD1094
Source: MTM, modified and annotated by OCI
The motor (M) cars in each car-set incorporated a driving cab and traction motors. The trailer (T) cars were each fitted with a pantograph and associated power infrastructure that drew power from the overhead wire and distributed it to the traction motors on the motor cars. The trailer cars were not fitted with traction motors.
These car-sets had been operating together since 3 July 2025, including several services on the Mernda line up until 8 July. This train did not operate again on the Mernda line until 13 July, the day of the derailment. The derailment occurred on the fourth inbound Mernda to Melbourne trip the train had undertaken on the day.
Maintenance of derailed car-set
The most recent maintenance on the trailing 3‑car set 853M‑1627T‑854M[10] was completed on 6 June 2025. This maintenance included re‑profiling of all wheels on the 3 cars to the target (MP2) profile for the MTM passenger train fleet. At the time of the derailment, the wheels had travelled about 12,800 km since re‑profiling and measurements taken after the derailment showed that there had been little wear.
Inspection of the derailed car
Damage to the 5th car was consistent with the derailment sequence including impact damage to the leading left corner of the car‑body, bogie frame and suspension components (Figure 7). The impact with the stanchion also resulted in extreme rotation of the derailed bogie. This rotation damaged further suspension components and resulted in the rear left corner of the bogie frame impacting and piercing a battery box mounted to the underfloor of the car body. Rolling stock component testing and assessment is ongoing.
Figure 7: Impact damage to the car-body, bogie frame and suspension of the 5th car
Source: OCI
Power supply
The Melbourne metropolitan rail system is an electrified network. Trains were supplied 1500 V direct current (DC) by an overhead wire system. The power was distributed to the network in sections by sub‑stations that transformed a 22 kV alternating current (AC) electricity supply to 1500 V DC. The stanchion that was impacted during the derailment was part of a gantry that carried both the 1500 V DC overhead wire and 22 kV AC conductors, both of which were damaged during the impact.
Track
Layout
The distance from the departure end of the Rushall station platform to the start of the High Street bridge was about 220 m.[11] There were 2 parallel tracks on the bridge and the train was on the track normally used for trains travelling toward Melbourne.
Approaching the High Street bridge from Rushall, the track was tangent (straight) and uphill before transitioning to a right curve that continued over the bridge and toward Clifton Hill. Track geometry measurements taken in May 2025 (prior to the derailment) indicated the tightest radius in the right curve was about 258 m. There was also a vertical curve through the location with the bridge on a crest. Track geometry was measured following the derailment and assessment is ongoing.
Maintenance
Track maintenance on the High Street bridge was undertaken on the nights of 8 and 9 July 2025. The maintenance works included replacing 27 timber sleepers and ballast along a length of about 14 m at the Rushall end of the bridge. Additionally, both rails were replaced across the full span of the bridge (about 25 m).
Flange climb derailment
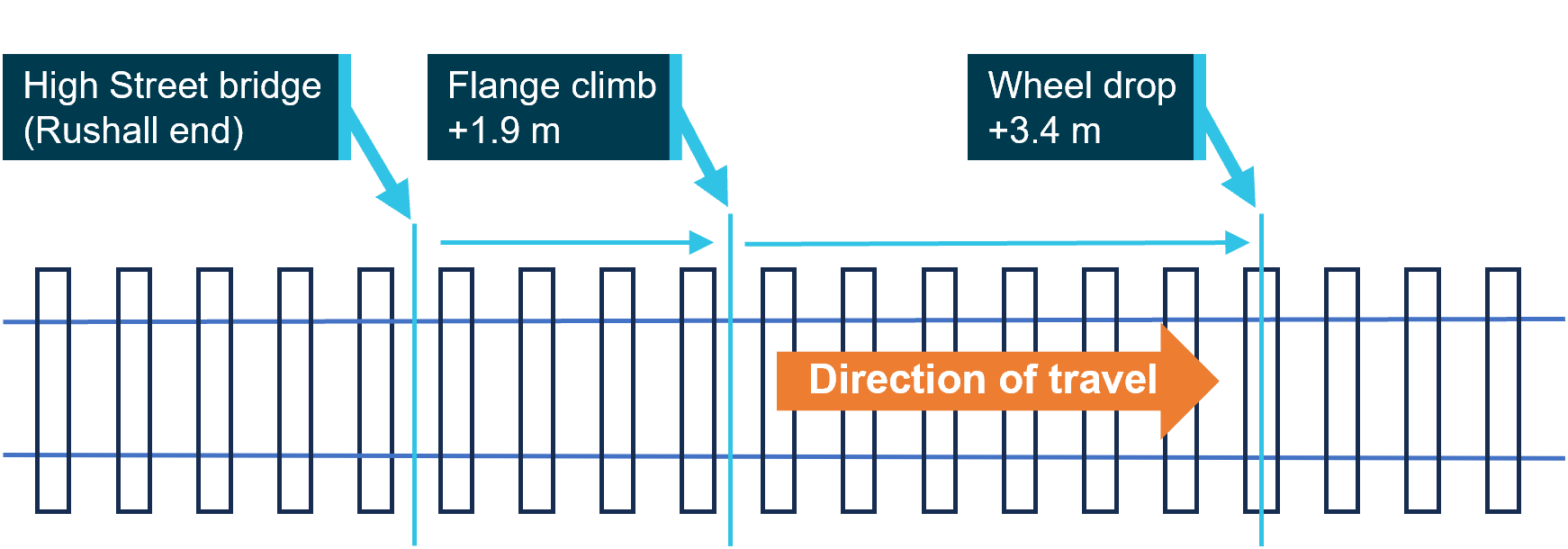
Post-derailment track inspection identified witness marks consistent with a left wheel climbing the left rail near the Rushall end of the bridge. The point of flange climb was about 1.9 m from the start of the bridge and the wheel dropped to left of the rail after travelling about 3.4 m along the top of the rail (Figure 8).
Figure 8: Distances of left wheel derailment from the Rushall end of the bridge
The derailment occurred on the High Street bridge. The approximate distances from the Rushall station end of the bridge are shown for key events. Source: OCI
The witness marks were consistent with the tip of the flange of the left leading wheel of the 5th car climbing onto the top of the rail from the inside (right) and running diagonally along the rail head before dropping to the left (Figure 9).
The presence of the wheel flange tip mark indicated that the initial derailment was by the action of flange climb. Flange climb occurs when lateral forces between the wheel and the rail exceed the capacity for vertical forces to restrain, either through excessive lateral force alone, or a combination of increased lateral force and reduced vertical force. The location of the derailment was in a tight radius curve. Therefore, the lateral force on the flange of the leading outside wheel was already high, as it was required to provide the force to turn through the curve.
Figure 9: Witness marks along the head of the left rail
The figure shows the flange climb mark made by the tip of wheel flange looking in the train’s direction of travel. The inset shows additional detail along the rail gauge corner. Source: OCI
Further investigation
To date, the following activities have been undertaken:
Inspections of the incident site
Inspections of rolling stock
Examination of track geometry and rail profile
Examination of train recorded data
Examination of maintenance records
Review of recorded communications between involved parties
Interviews with involved parties.
The investigation is continuing and will include further review and analysis of:
Factors potentially related to the flange climb derailment including:
Rolling stock wheel and suspension component condition
Track condition including geometry and maintenance practices
Wheel to rail contact conditions
The emergency response to the derailment and overhead damage.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, relevant parties will be immediately notified so appropriate and timely safety action can be taken.
Rail safety investigations in Victoria
Rail safety investigations in Victoria are conducted by the Office of the Chief Investigator (OCI) in accordance with a collaboration agreement with the ATSB.
OCI is the operational office of the Chief Investigator, Transport Safety, a statutory position established in the Transport Integration Act 2010 (Vic) to provide independent, no-blame investigation of transport safety matters in Victoria.
Under the collaboration agreement with the ATSB, OCI staff exercise powers and perform functions under the Transport Safety Investigation Act 2003 (Cth), and reports are approved for release under the TSI Act by the ATSB Commission.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
Investigations under the TSI Act do not apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings.
Under the TSI Act investigations endeavour to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
TSI Act investigations are not for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The franchisee and accredited rail transport operator of the Melbourne metropolitan rail network.
[2]At MTM, a principal driver is an experienced train driver who may provide advice and support to other drivers and conduct safety and competency training and assessment tasks. It is not unusual for principal drivers to request to drive a service when not rostered for other tasks, as was the case on this trip.
[3]The High Street bridge is sometimes also called Queens Parade bridge as the road changes name in close proximity.
[5]A pantograph is an apparatus fixed to the roof of electric trains to draw power from the overhead supply.
[6]Available evidence did not indicate arcing between overhead wires and the body of the 5th car.
[7]A RIC was the MTM site representative responsible for coordinating site actions in response to an incident.
[8]Passenger numbers were not recorded. The estimate reported is based on CCTV vision of passengers exiting into the driving cab of the 3rd and 4th cars.
[9]The Alstom X’Trapolis 100 first entered service in Melbourne in 2002, initially operating on the (then named) Hillside Trains network which included the Mernda line.
[10]Car-set 853M-1627T-854M was in the first tranche of delivered sets.
[11]The start of the bridge was at about 7.065 track km. On the Melbourne metropolitan network, track kilometres (track km) are a measure of the distance along a track from Southern Cross Station in central Melbourne.
A transport safety investigation is underway into the derailment of an MTM passenger train between Rushall and Clifton Hill stations on Sunday evening.
The derailed train collided with stanchions carrying overhead wires, resulting in substantial damage to the overhead infrastructure. About 100 metres of track and one passenger car were also significantly damaged. There were no injuries to passengers or train crew in the incident.
Victoria's Chief Investigator, Transport Safety is investigating the incident under the Transport Safety Investigation Act 2003 (Cth) under a collaboration agreement with the Australian Transport Safety Bureau (ATSB).
Investigators from the Office of the Chief Investigator (OCI) deployed to the accident site on Monday, conducting a range of evidence gathering activities.
The ATSB and OCI will release a preliminary report detailing factual information established in the investigation’s evidence-gathering phase in about two months.
A final report will be released at the conclusion of the investigation and will detail evidence, analysis and findings.
However, should a critical safety issue be identified during the investigation, the ATSB and OCI will immediately notify relevant parties so safety action can be taken.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the morning of 17 July 2024, a Bell helicopter operating under VFR[1] departed a private airfield at Creasy, Tasmania for an external sling load operation in the town of Tullah. The helicopter was crewed by 2 pilots, with the copilot as pilot flying (PF).
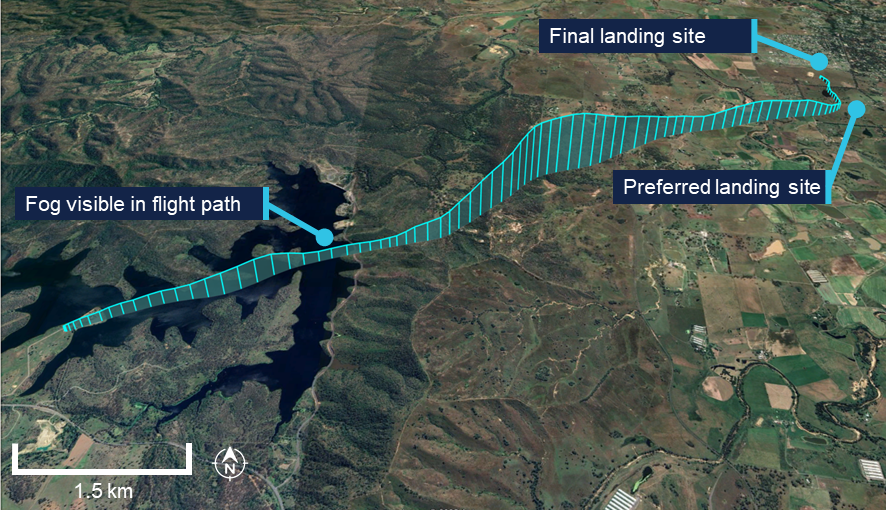
Tullah is characterised by a high ridge to the east of the town and a reservoir to the west. As the helicopter arrived over Tullah, the crew observed significant fog over most of the town, from the reservoir to the ridge.
Figure 1: Aerial image of Tullah and surrounds
Source: Google Earth, modified by the ATSB
The crew discussed the available options to land at Tullah and the pilot in command (PIC) suggested that the best option would be to approach from the west, over the reservoir, where the edge of the town was visible. The copilot did not agree with the decision to continue the flight, so the PIC took over as PF to conduct the approach.
The PIC reported that as the sun was low on the horizon and the water was glassy calm, there was a reflection of the edge of town and trees along the reservoir, reducing their depth perception. Due to a concern with possibly flying into the water, the PIC planned to conduct a slow and steep approach towards the reservoir. The PIC anticipated that they would become visual with the water at approximately 100–200 ft, aided by the rotor downwash disturbing the water surface. They would then use this as a height reference, then climb back to 500 ft to continue to the edge of town for further descent.
Video footage received by the ATSB from a third party shows the helicopter descended toward the water in fog. The PIC reported that during the descent, the rotor downwash was not visible to the crew due to the descent angle, and although the crew had the edge of the reservoir in sight, they lost visual reference with the water. At approximately 5 ft above the water, the crew identified the water surface and the PIC immediately applied power to stop the descent and initiate a climb. The PIC reported that before the descent could be arrested, the skids contacted the water. Video footage showed the helicopter making a significant splash. The helicopter subsequently climbed to 500 ft.
The crew returned the helicopter to overhead Tullah and while they considered further options for landing, conditions eventually cleared sufficiently for a landing at the edge of the town.
Safety message
Crew resource management (CRM) plays an important role in communication and decision‑making in a 2‑pilot cockpit. An informed and coordinated approach to decision‑making is essential for ensuring the most appropriate action is taken, especially in non‑normal or high workload situations.
In this instance, the controlled flight into water could have been avoided if the crew had followed effective CRM procedures when considering options for an approach over still water and with fog in the area.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 6 June 2025, the pilot of a Cirrus SR20 aircraft was conducting a private flight between Devonport Airport, Tasmania, and Moorabbin Airport, Victoria, under visual flight rules (VFR)[1] with the pilot and one passenger on board. The pilot held a private pilot licence (aeroplane).
Prior to the departure, the pilot stated that they reviewed the weather briefings accessed through an electronic flight bag application and obtained directly from the Bureau of Meteorology. After a discussion with their flight instructor, the pilot determined that forecast conditions were suitable to proceed with the flight across the Bass Strait under VFR to Moorabbin.
They also stated they made an informed decision to depart ‘as soon as possible’ due to forecast strong gusts in the vicinity of Moorabbin Airport and the end of evening civil twilight,[2] which occurred at 1736 local time.
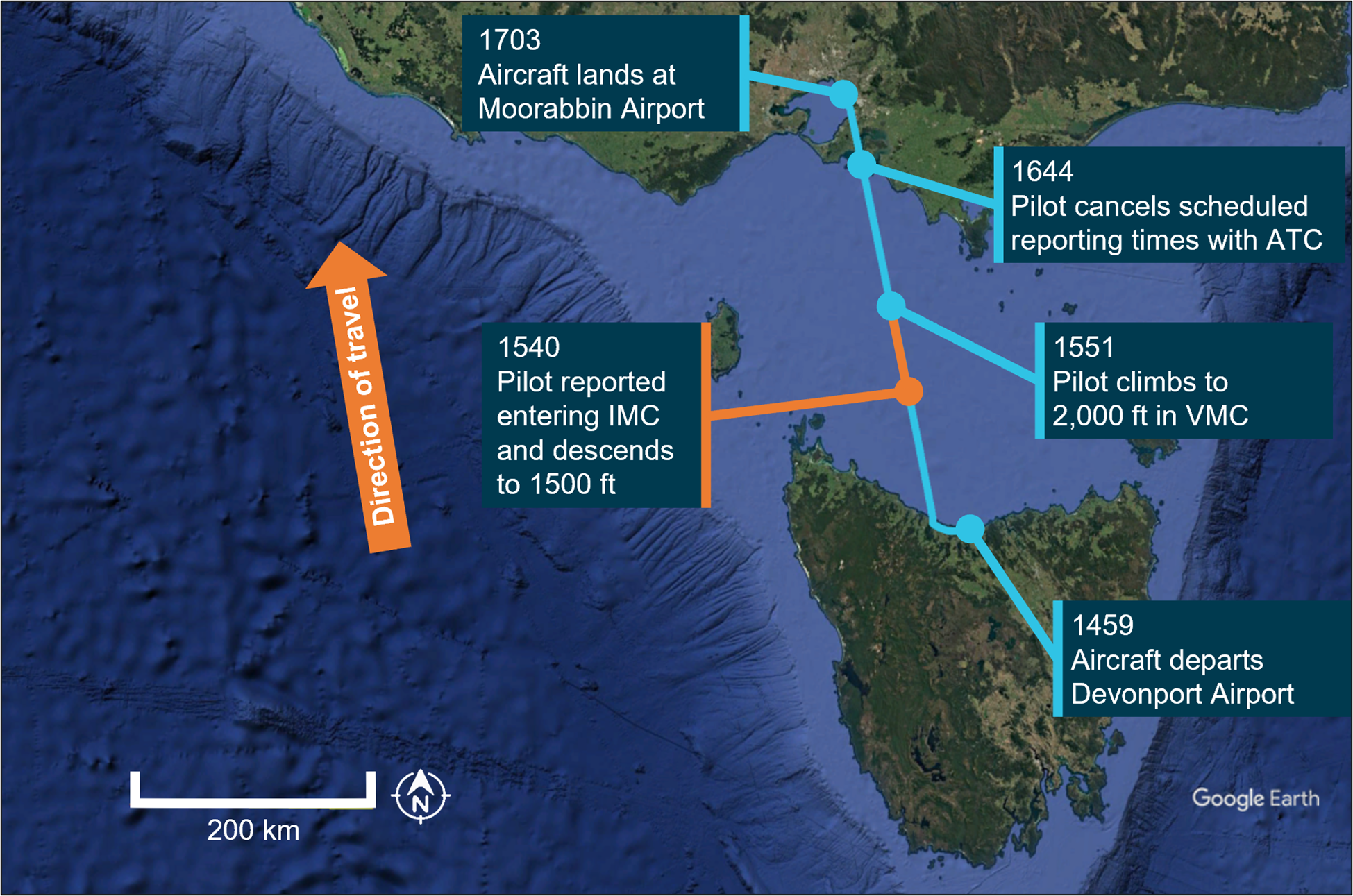
After departing Devonport at 1459, the aircraft initially proceeded on a westerly heading to conduct a brief ‘scenic’ leg (Figure 1). The pilot then made a right turn in a northerly direction toward Moorabbin Airport and climbed to 4,500 ft above mean sea level, cruising below scattered[3] cloud observed at about 5,000 ft in the vicinity of the coastline to the west of Devonport Airport.
Figure 1: Aircraft flight path and key events
Source: Google Earth, annotated by the ATSB
At about 1530, they recalled a lowering of the cloud base accompanied with a reduction in forward visibility. The pilot descended to about 2,000 ft to remain clear of cloud and immediately advised ATC of the deteriorating weather conditions and that they anticipated entering instrument meteorological conditions[4] (IMC) imminently.
At 1540, the pilot subsequently recalled entering IMC but reported being able to see below the aircraft. They immediately advised ATC and descended to 1,500 ft, at which point they regained visual meteorological conditions[5] (VMC). At 1551, confident of remaining clear of cloud, the pilot climbed back to 2,000 ft and continued the flight to Moorabbin in VMC.
The pilot recalled the autopilot was utilised throughout the flight and that scheduled reporting times were implemented at 15‑minute intervals with ATC until 1644 when they were cancelled by the pilot. The aircraft landed at Moorabbin Airport at 1703.
Safety message
Pilots operating under visual flight rules are encouraged to make conservative decisions when considering how forecast weather may affect their flight. Establishing a ‘personal minima’ is recommended for pilots to provide additional operational margins which account for factors such as weather, experience and recency.
One of the key risk controls for a visual flight rules pilot to avoid entering instrument meteorological conditions is appropriate pre‑flight preparation and planning. Pilots should always obtain up‑to‑date weather information before and during flight. While forecasts will assist in selecting the route to be flown, pilots should plan an alternate or be prepared to make necessary deviations from the planned route should actual weather conditions indicate the possibility of not being able to comply with the VFR.
For a non-instrument rated pilot, even with basic attitude instrument flying proficiency, maintaining control of an aircraft in IMC by reference to the primary flight instruments alone entails a very high workload that can result in narrowing of attention and loss of situational awareness. If entering cloud becomes unavoidable, the use of an autopilot by a suitably trained pilot can assist with maintaining the desired flight path and remove inadvertent inputs. While autopilot can be used to reduce workload, it is not infallible and should not be relied upon or used by VFR pilots as a risk mitigator to decide to fly into unsuitable conditions.
Additionally, ATC services such as Flight Following,[6] can assist the pilot with managing workload and improving situational awareness. Subject to ATC workload, information derived from Bureau of Meteorology weather radar sites can also be provided to pilots.
ATSB booklet Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions (AR-2011-050, revised 2019) provides for guidance on avoiding VFR into adverse weather. Further resources for preventing VFR into IMC can also be found on the Civil Aviation Safety Authority’s website.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]Scattered cloud is a meteorological term used in aviation to describe cloud coverage that occupies 3 to 4 oktas (eighths) of the sky.
[3]Evening civil twilight begins at sunset and ends when the geometric centre of the sun is 6 degrees below the horizon.
[4]Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules, rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[5]Visual Meteorological Conditions (VMC): weather conditions expressed in terms of flight visibility and the horizontal and vertical distance from cloud for the application of VMC criteria in various airspace classifications.
[6]Flight Following: the provision of ongoing surveillance information service which is an on request service provided to assist pilots of VFR flight within ATS surveillance system coverage in Class E and Class G Airspace, to avoid other aircraft or to assist in navigation.
On 7 February 2025, the fully laden bulk carrier FMG Nicola was departing Port Hedland under the conduct of 2 marine pilots with 3 tugs in attendance. At 1515 local time, about 5 miles into the pilotage, FMG Nicola’s main engine unexpectedly shut down. An emergency was declared, and the pilots immediately took action to control the ship’s movement while the port’s vessel traffic service mobilised additional port tugs and the ship’s engineers rectified the engine fault. The main engine was restarted at 1523, and the ship was brought back under control. Multiple tugs attended and the ship was brought clear of the channel side and taken safely to sea.
What the ATSB found
The ATSB investigation found that FMG Nicola lost propulsion because the main engine low lubricating oil pressure emergency shutdown switch erroneously activated with all system parameters otherwise normal.
Also, the investigation found that the emergency response was as per port guidance, procedures and training. The ship remained underway and kept moving and was safely navigated via the channel to sea. While the ship departed, and tracked along the edge of, the charted shipping channel, there was no evidence to show that the ship had contacted the seabed.
What has been done as a result
Pilbara Ports Authority advised that port operations have been reviewed in the areas of ship reliability and vetting, towage strategy and arrangements and pilotage and emergency response and relevant procedures have been updated. Actions taken included improved operational awareness of and training in escort towage arrangements and updating of pilotage and emergency response procedures.
The ship’s manager/operators responded to this incident by upgrading the management (testing and replacement) of main engine lubricating oil pressure switches on all ships in its fleet. This was supported by fleetwide implementation of a procedure for rapid response to main engine shutdown due to low lubricating oil pressure.
The Australian Maritime Safety Authority has updated its processes to better ensure prompt reporting of incidents to the ATSB.
Safety message
The safety of ports and ships that use them requires commitment to continued improvement and learning from incidents by port authorities, port users, facility owners and port services such as towage and pilotage. By working together, enhancing procedures and strategies, emergency situations can not only be safely managed, but lessons can be learned and used to further improve operational safety.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At 08321 on 7 February 2025, the 327 m bulk carrier FMG Nicola (cover image) completed loading 237,088 t of iron ore at its berth in Port Hedland, Western Australia. The fully laden ship had a draught of 17.51 m forward and 17.69 m aft and was due to depart its berth during the afternoon (a high water of 5.56 m was predicted for 1634).
At 1330, 2 harbour pilots, one of whom was under supervision, boarded the ship. The port authority’s marine services delivery manager (MSDM), who was also a harbour pilot, boarded to observe the departure. By 1348, the ship’s main engine and steering had been satisfactorily tested and the master-pilot information exchange was completed in readiness for departure. The pilot under supervision would conduct2 the pilotage and 4 tugs were secured to assist.
By 1412, all mooring lines had been cast off and the ship departed the berth (Figure 1). There was a 25-knot north‑north‑west wind with waves of up to 1.5 m on a 0.5 m swell in the area, including the port’s single shipping channel.
At 1442, with the ship progressing along the channel as planned, the MSDM disembarked via pilot launch. At 1446, one of the tugs was let go and returned to base.
At about 1500, FMG Nicola was turned to port to follow the channel at a speed of about 7 knots. Of the 3 tugs assisting, FMG Mako was fast at the ship’s port shoulder,3FMG Dusky at the starboard shoulder and FMG Spinner through the centre lead aft.
At 1514, as the ship approached beacons 32-33, the pilot ordered a heading4 of 334°. At about this time, FMG Mako’s master requested its towline be let go as conditions were uncomfortable due to choppy seas on the ship’s port side. The pilot concurred, and the towline was let go at 1515.
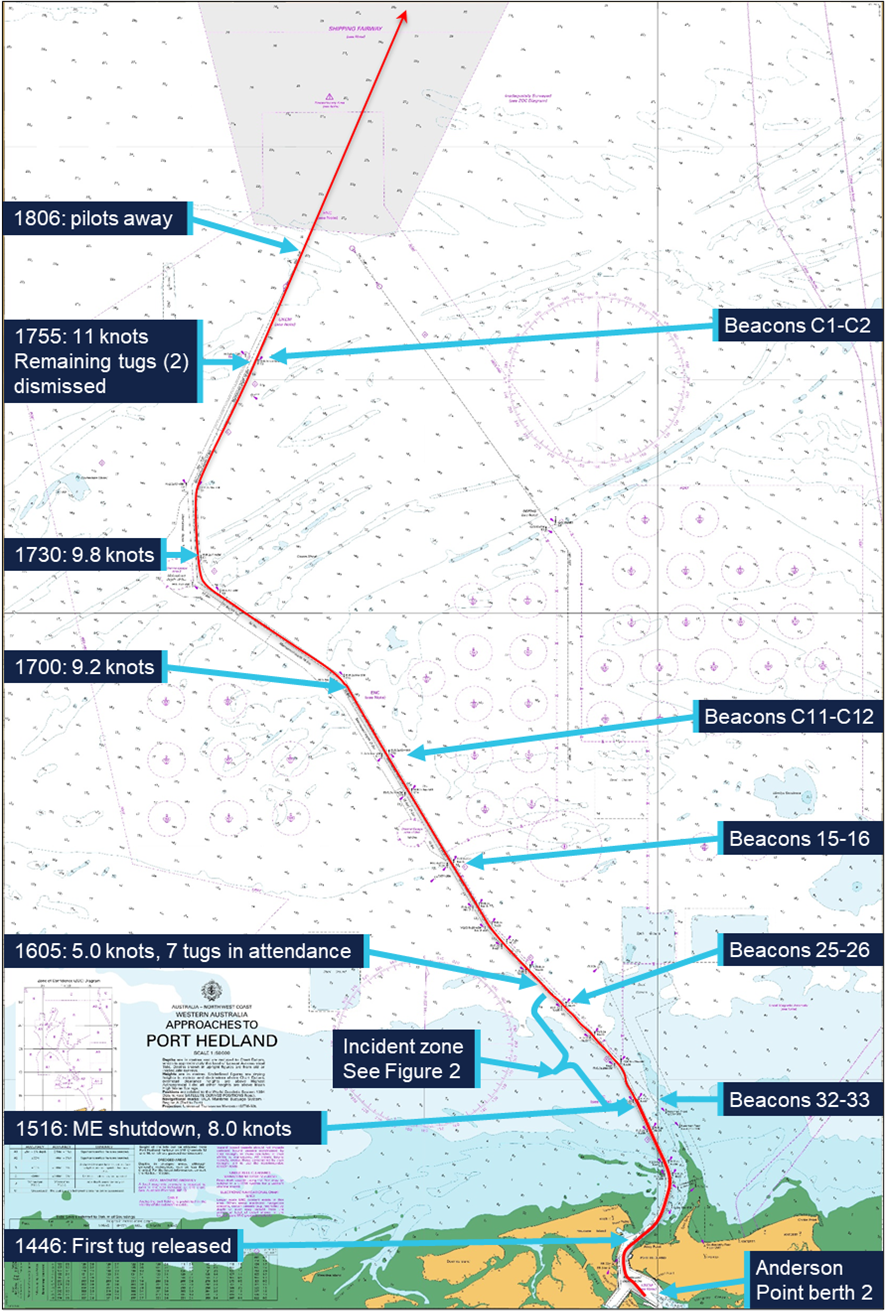
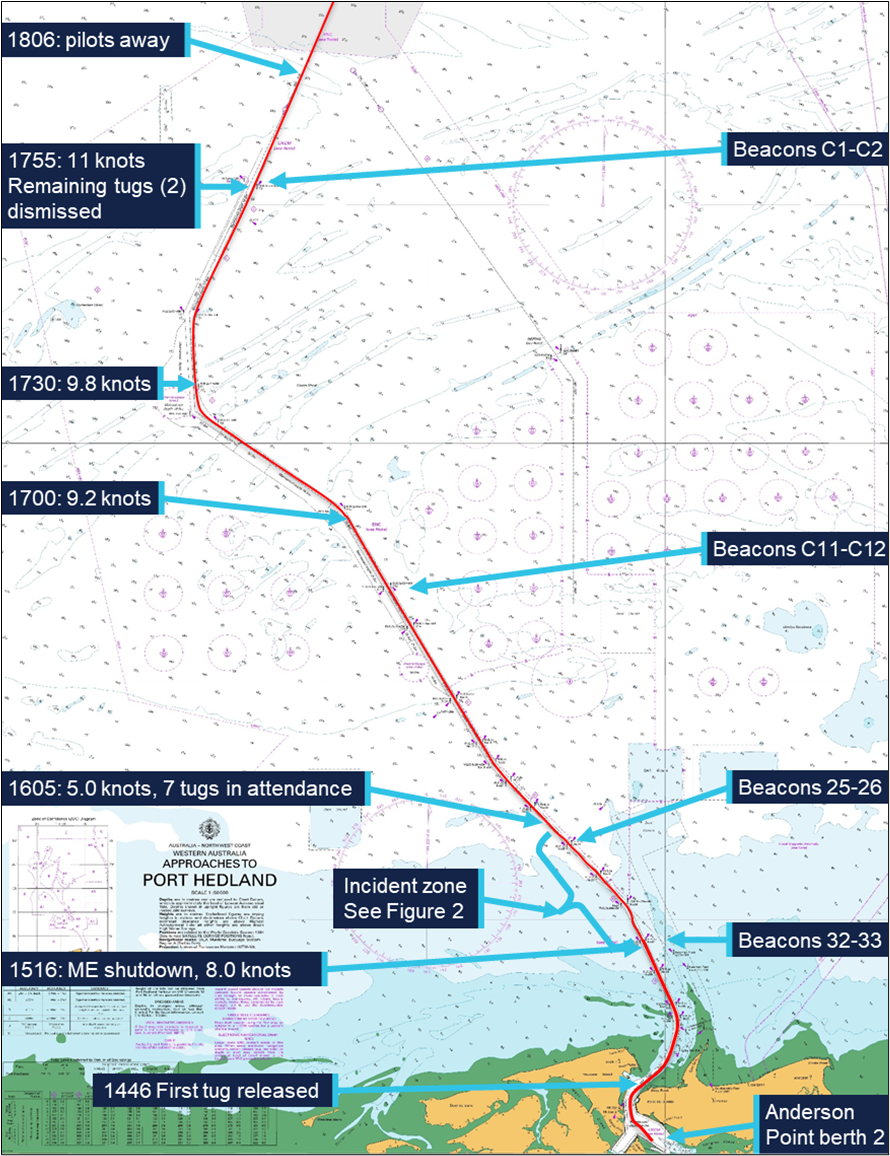
Figure 1: Overview of FMG Nicola's track through the Port Hedland shipping channel
Source: Australian Hydrographic Office, data from Australian Maritime Safety Authority
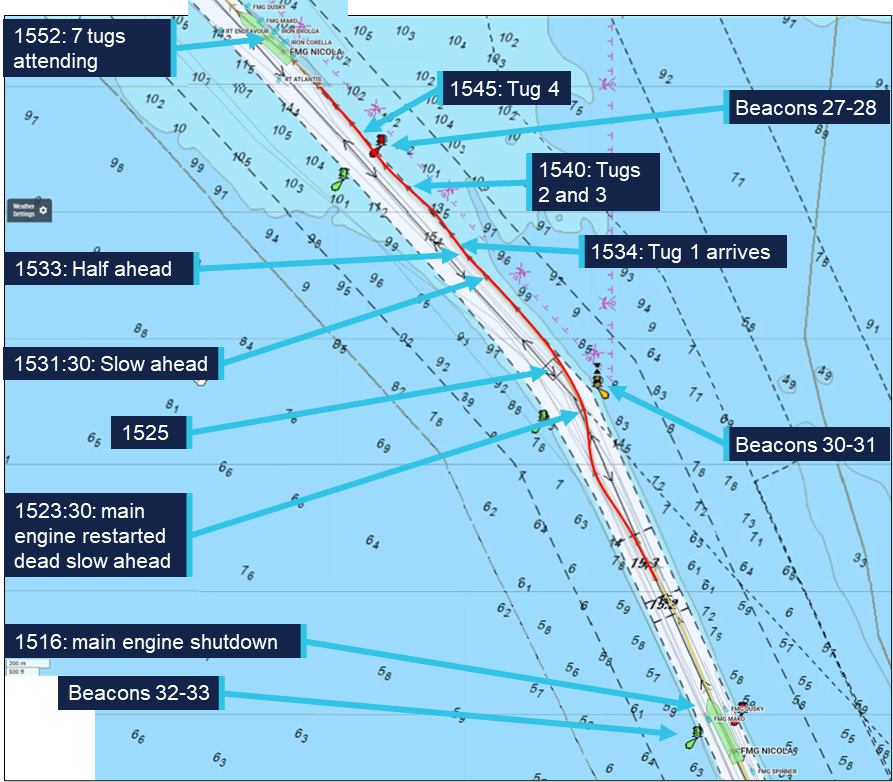
Soon after, at about 1516, FMG Nicola’s main engine suddenly shut down as the ship was passing beacons 32-33 (Figure 2). The ship’s speed was 8.3 knots; the pilot ordered the rudder midships. The pilot informed the tug masters that the ship had lost propulsion and directed them to help keep it in the channel.
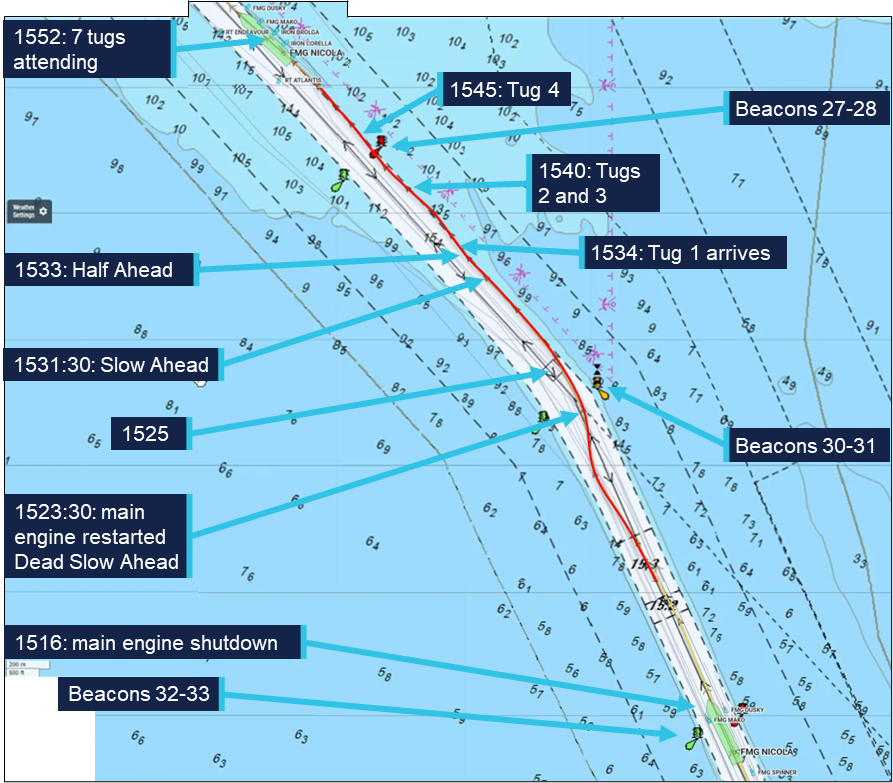
Figure 2: FMG Nicola track from about 1516 to 1552
Source: Australian Maritime Safety Authority, Marine Traffic, annotated by the ATSB
At 1518, the pilot notified Port Hedland vessel traffic service (VTS) of the emergency and requested additional tugs. The pilot gave helm orders and used the tugs to follow the channel. The ship’s speed decreased to 7.4 knots and it moved closer to the western side of the channel with a slow rate of turn of about 4° per minute to port (Figure 3).
Meanwhile, the ship’s engineers identified that the engine had shut down because the ‘main bearing and thrust bearing lubricating oil pressure low’ non‑cancellable trip had activated. The engineers determined that it had activated due to faulty operation of the pressure switch. After confirming all engine systems were operating normally, the engine trip lockout system5 was reset and, at 1523, the engine was restarted at dead slow ahead. By that time the ship had slowed to 4.8 knots.
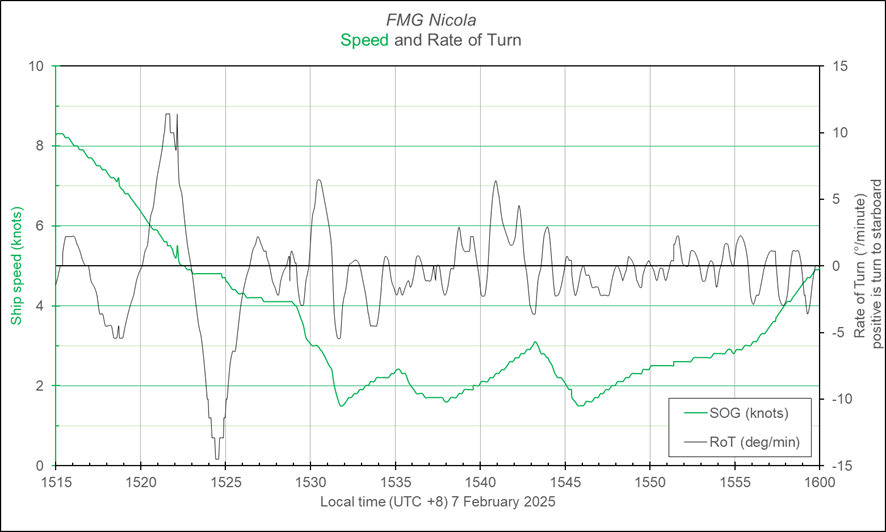
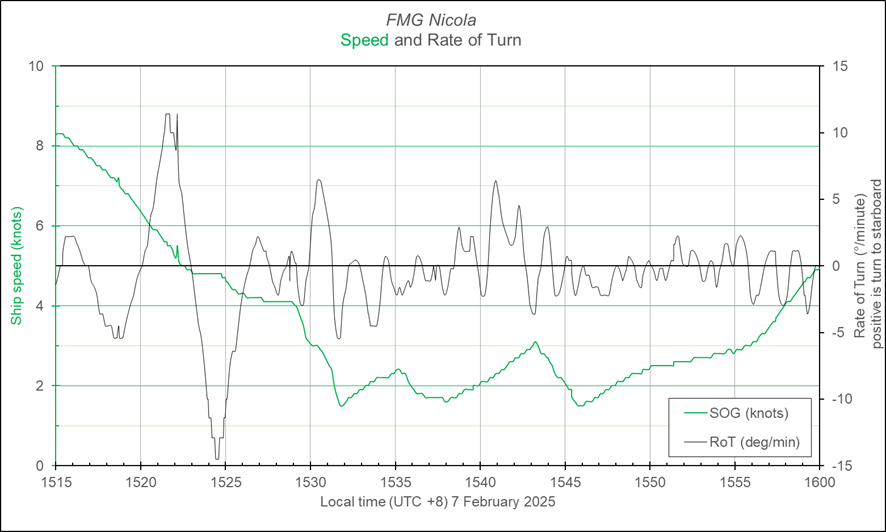
Figure 3: FMG Nicola speed and rate of turn at the time of the incident
Graph derived from Automatic Identification System data and should not be used for further analysis. Source: Australian Maritime Safety Authority, analysis by the ATSB
By about 1525, FMG Nicola had passed beacons 30-31, and, with a rate of turn 7.5° per minute to port and speed of 4.3 knots, it closed on the eastern side of the channel. Soon after, the ship stopped turning and began moving along the side of the channel, which was aligned along a 318° (T) direction there. The choppy conditions hampered the use and effectiveness of the attending tugs. The pilots and master, with assistance from VTS, assessed the situation and awaited the arrival of additional towage assets to assist the ship.
The ship continued to move along the side of the channel (Figure 2), set to starboard by the conditions and influenced by the adjacent channel side and shallower water.6 With the main engine operating and the assistance of the tugs, headway was maintained.
At 1534, the first of the additional tugs arrived and was tasked to push up on the ship’s starboard side. In the following 10 minutes, 3 more tugs arrived and assisted as required by the pilot. At 1540, the ship passed close to beacon 28 while moving along the side of the channel at a speed of 2.5 knots. At 1545, with 7 tugs in attendance (4 on starboard side, 2 on port and 1 on centre lead aft) and clear of beacon 28, FMG Nicola had slowed to 1.5 knots (main engine on half ahead, 40 rpm). Multiple port rudder orders were used to counter the set to starboard and maintain the ship’s track while avoiding the stern swinging too far to starboard into the shallows. Using the main engine and the tugs, the pilots prepared to ease the ship clear of the channel side and avoid damage to the stern, rudder and propeller.
By 1550, the ship had been moved away from the channel side. The main engine was kept at half ahead and the ship’s speed increased as it came clear of the influence of the channel side and shallow water. The tugs continued escorting the ship out the channel towards open water.
At about 1635, 3 tugs were released and a further 2 were released about 10 minutes later as the ship approached beacons C11-C12. At 1648, with the ship speed at 8.3 knots, the main engine speed was increased to full ahead (46 rpm). The remaining 2 tugs were retained and escorted the ship until it passed beacons C1-C2 to sea.
By the time the ship passed beacons C1-C2, the ship’s crew had completed inspecting and testing the main engine systems. They had also conducted an inspection, including sounding tanks and compartments, to confirm there was no ingress of water.
Shortly after, at 1806, the pilots departed the ship by helicopter and the ship continued its passage to the next port, Dongjiakou, China. During the passage, the crew inspected all ballast tanks on the starboard side and found no physical damage to the ship’s side or structure.
Context
FMG Nicola
General details
FMG Nicola was a Singapore-registered, capesize7 bulk carrier built in 2016 by Jiangsu Yangzi Xinfu Shipbuilding, China. At the time of the incident, the ship was owned and operated by Fortescue Shipping Nicola, managed by Bernhard Schulte Shipmanagement (BSM), Hong Kong, and classed with Lloyd’s Register (LR).
At the time of the incident, FMG Nicola was crewed by 23 Sri Lankan and Indian nationals, including the master, all appropriately qualified for their positions on board.
The master had 26 years of seagoing experience, all on bulk carriers, with about 4 years in command. The master joined BSM in 2015 and had completed several assignments on FMG Nicola since 2021.
The chief engineer had about 18 years of seagoing experience, with about 9 years at that rank. The chief engineer joined BSM in September 2024 and was assigned to work on FMG Nicola.
Main engine
FMG Nicola’s propulsion was provided by a 6‑cylinder, MAN‑B&W 6G80ME‑C9.5 engine developing 18,240 kW. The main engine drove a single 4‑blade, fixed‑pitch propeller, providing a service speed of 14 knots.
Lubricating oil system
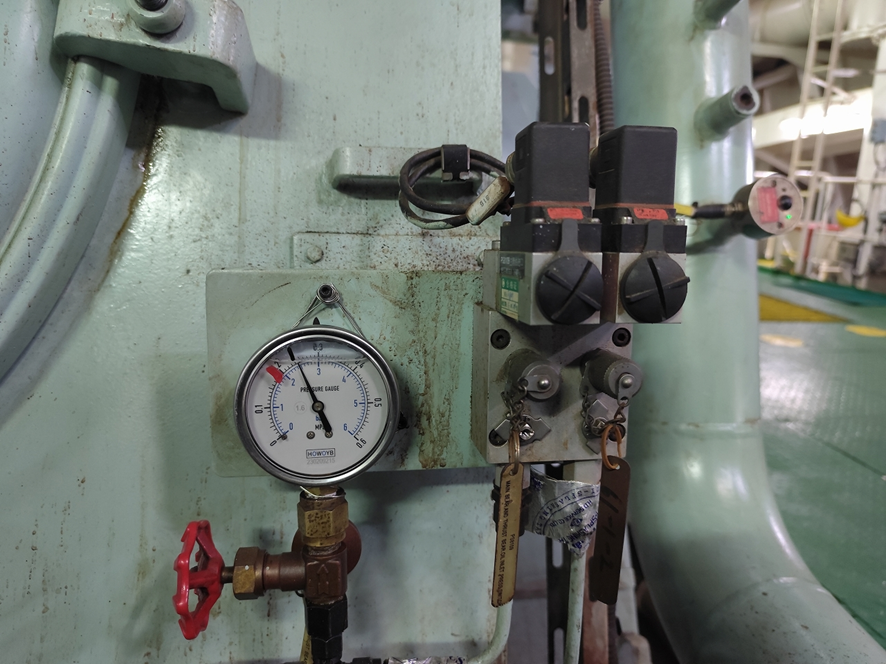
The main engine lubricating oil (LO) system was fitted with a hierarchy of oil pressure monitoring and alarm controls to limit inadvertent engine stoppage while preventing catastrophic engine damage. In addition to local, analogue indicators and pressure gauges, the LO pressure was monitored via a pressure transducer and pressure switches (Figure 4).
Signals from the sensors fed into the ship’s machinery alarm, monitoring and control system. This system provided real time, remote indication of the LO pressure. Software limits were incorporated to trigger alarms and other actions. Normal operating pressure for the system was about 250 kPa with software triggers set at:
210 kPa for standby pump start
200 kPa for low LO pressure alarm
180 kPa for main engine slow down alarm.
Figure 4: Main engine lubricating oil pressure sensing and switches
Source: Fortescue Metals Group
In addition to these triggers and alarms, the main engine LO system had a separate pressure switch set to activate at 160 kPa. This switch, independent of the oil pressure monitoring circuit, was for the main engine low LO pressure shutdown. This initiated rapid shutdown of the engine to prevent catastrophic damage due to complete loss of bearing lubricating oil.
The normal, expected, sequence of loss of LO pressure indications would follow persistently falling oil pressure: standby pump start, low pressure alarm and main engine automatic slow down prior to main engine shutdown.
The machinery monitoring system allowed for (adjustable) time delays on activation of each of these triggers. At the time of the incident, the engine LO pressure shutdown delay was set to 0.1 seconds. Following the incident, and after obtaining advice from the engine manufacturer that the delay could be increased up to 2 seconds, it was reset to 1.9 seconds.
Components of the main engine LO system were subject to regular maintenance through the ship’s planned maintenance system (PMS). The PMS records showed that the main engine pressure transmitter and pressure sensors had last been checked on 15 November 2024 (about 3 months before the incident).
Port Hedland
General information
Port Hedland, situated in the Pilbara region of Western Australia, is the world’s largest bulk export port by tonnage, handling over 500 million tonnes of cargo annually. More than 95% of this volume is iron ore, exported primarily by BHP,8 Fortescue Metals Group (FMG) and Roy Hill Infrastructure, with the port serving as the companies’ main export hub for all Pilbara output. In addition to iron ore, the port also handles exports of salt, manganese, copper concentrates, lithium minerals and livestock.
At the time of the incident, the port’s infrastructure included 19 operational berths. Eight of these berths were owned and operated by BHP, with the remaining berths owned and operated by FMG (5 berths), Roy Hill (2 berths) and Pilbara Ports Authority9 (4 berths). Shipping activity is significant, with more than 6,000 ship movements (inbound and outbound) each year.
Pilbara Ports Authority
The port was managed by the Pilbara Ports Authority (PPA), which had overarching responsibility for safety and efficiency of port operations and the environment under state legislation. The PPA’s jurisdictional responsibilities were exercised through the Port Hedland harbour master.
The harbour master’s responsibilities included the coordination of vessel traffic services, ship scheduling, pilotage and maintenance of shipping channels, navigational aids and port infrastructure. The PPA issued third‑party contracts or licences for stevedoring, towage, pilotage services and pilot transfers (helicopter and boat).
Shipping channel
Access to the port was provided by a single 22 mile10 dredged shipping channel, which allowed a single ship to traverse it at any given time. For most laden ships, particularly capesize ships, such as FMG Nicola, use of the channel was restricted by tidal conditions.
The Port Hedland navigation channel was divided into 6 zones11 based upon navigational or environmental characteristics that would impact the risk within that zone. These characteristics included location, channel alignment, bathymetry, channel slopes and sea conditions.
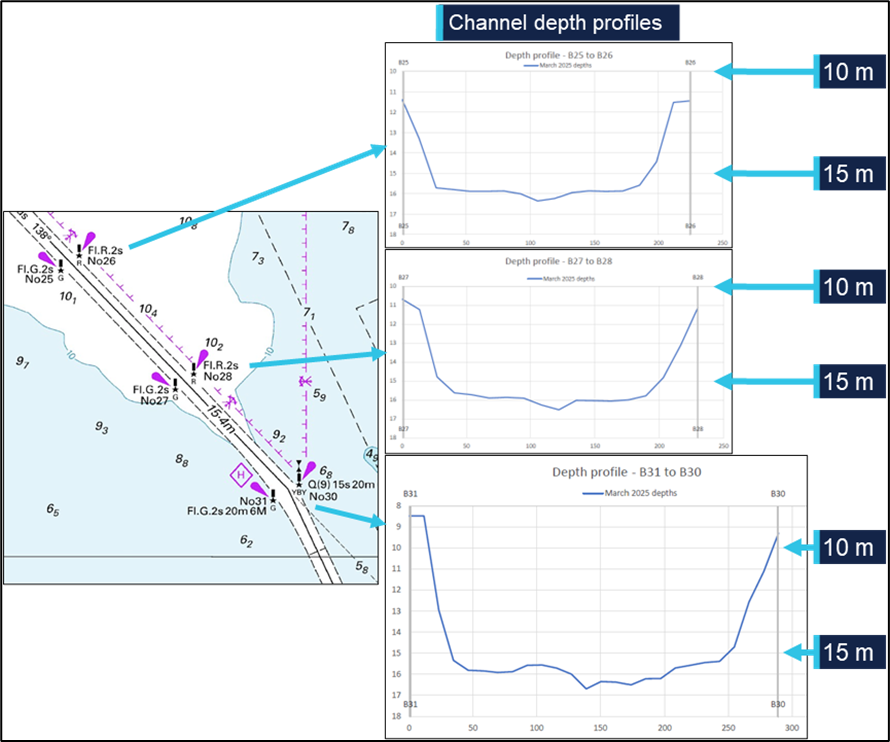
The incident took place within the 10-mile section of the channel closest to the port, an area prone to strong tidal flows and with particularly confined spaces, narrowing to a minimum width of 162 m. The channel depth in this section was maintained at about 15 m chart datum (Figure 5). The section of the channel from beacons 30-31 to 15-16 was described in the PPA documentation as:
…a relatively straight section of channel with one minor 13-degree alteration of course to starboard for outbound ships. The water adjacent to the channel is predominantly greater than 10 metres deep with scattered shoal patches…the channel batters are significantly flatter than [the channel out of the harbour].
Figure 5: Channel profile for beacons 30-31 to 25-26
Source: Australian Hydrographic Office, Pilbara Ports Authority, annotated by the ATSB
The features of the channel make the risks associated with channel blockage high. A disabled ship can strand on a falling tide as well as blocking the passage of other ships. Depending on departure times, separation between ships and the location of an incident, up to 3 additional ships could be committed to, or within, the channel and exposed to this hazard at a given time.
Escort towage strategy
Since 2013, in support of the Port Hedland port user guidelines and procedures,12 the Port Hedland escort towage strategy (ETS) had been developed and updated. Escort towage was identified as a critical mitigative control to prevent a ship grounding or colliding with fixed objects if it experienced a loss of navigation control.
The resulting ETS was intended to assist Pilbara Ports, pilots, tug masters, towage operators and other stakeholders to understand the rationale for escort towage at Port Hedland and provide guidelines to support effective escort towage operations.
Primary objectives of the ETS included:
• to assist an escorted ship to maintain manoeuvrability and navigate within water of sufficient depth to prevent a ship grounding, and the potential consequential impact of channel blockage
• to document escort towage procedures that have been identified as effective at preventing a ship grounding and potential channel blockage through research, simulation and on-water trials.
In relation to the risks associated with a loss of navigation control event, the ETS stated that:
Steering-related incidents or main engine slowdowns or failures that result in loss of navigational control are the likely root causes for a grounding incident that may lead to channel blockage at Port Hedland. Both incident types occur at Port Hedland, with engine‑related incidents far more likely than steering incidents; however, steering incidents represent the greatest risk of a channel blockage…the time available to respond to a steering incident and prevent a ship grounding is typically 60 to 90 seconds.
Engine slowdowns or failures, which are ten times (10x) more likely to occur than steering incidents, may require escort tugs to assist with steering and maintaining headway of the ship. However, the response time required for an engine slowdown or failure is typically much longer than steering failures…[and]…allows for available towage assets, including passive assets, to be positioned appropriately to assist a ship transit to an emergency anchorage…or transit to the end of the channel…with tug assistance.
The principal guidance for immediate response to a vessel emergency in the channel was to maintain channel integrity (clearance). This manifested itself as making every effort to continue the transit, with tug assistance, through the channel to a place of safety, either to anchorage or out the channel and to sea.
Pilotage
Vessels 35 m or greater in length using the main shipping channel and navigating within port limits were required to use the services of a licensed harbour pilot. Pilotage services for the port were provided by PPA through directly employed pilots as well as by third party, contracted providers.
The pilots on board FMG Nicola at the time of the incident were employed by PPA. All PPA pilots had undertaken a competency‑based pilotage training program incorporating on‑water and simulator training and competency assessments.
The supervising pilot had worked for PPA since 2023. This pilot had over 25 years of experience in the maritime industry.
The pilot under supervision joined PPA in 2024 after more than 15 years piloting a wide variety of ship types and sizes, including capesize bulkers, and larger, in an overseas port. At the time of the incident, the pilot held a level 3 authority to pilot in Port Hedland and was undertaking supervised pilotages to upgrade this authority to level 4.
Towage
Tugs in Port Hedland were operated under towage licences granted by the PPA to Pilbara Marine (a subsidiary of FMG) and BHP Towage Services (BHPTS). KOTUG operated tugs under the Pilbara Marine towage licence while Rivtow was contracted to operate the tugs under the BHPTS licence.
The 4 tugs assigned to FMG Nicola on the day of the incident were ART85‑32W class advanced rotortugs, operated by KOTUG. Each tug had a bollard pull13 of 85 t and used a hybrid propulsion arrangement with 2 azimuth thrusters forward and a third azimuth thruster aft.
The tugs which came to render assistance after FMG Nicola lost propulsion were operated by Rivtow and comprised 2 ART80‑32 rotortugs and 2 RAstar85 azimuth stern drive (ASD) tugs.
Tug release point
The port user guidelines and procedures documented the tug allocation requirements based on specified criteria. Laden outbound capsize ships required 4 tugs secured to the ship from the berth to Hunt Point, near the harbour entrance. From Hunt Point to beacons 30-31, 3 tugs were to remain tethered to the ship – a tug on each shoulder and a dedicated, active escort tug made fast through the centre lead aft. The shoulder tugs could be let go, to remain in passive escort, should conditions require, and after risk assessment by the pilot.
From beacons 30-31 to beacons 15-16 the shoulder tugs would normally be let go and move to a passive escort position off the ship’s quarters. At beacons 15-16, the tugs could be dismissed. Ships were not generally escorted to the end of the channel, except in the case of an emergency or if the ship was deemed to require escort towage until clear of port limits.
In August of 2024, to increase time for immediate response to a steering failure, the speed of capesize ships was limited to a maximum of 8.4 knots from beacons 36-37 to the end of the channel.
On the day of the incident, conditions on the exposed port shoulder of FMG Nicola were such that the master of FMG Mako requested that the tug be let go just after passing beacons 32-33. The pilot agreed to the release and the tug was let go prior to passing beacons 30-31, and just before the ship lost propulsion.
Weather
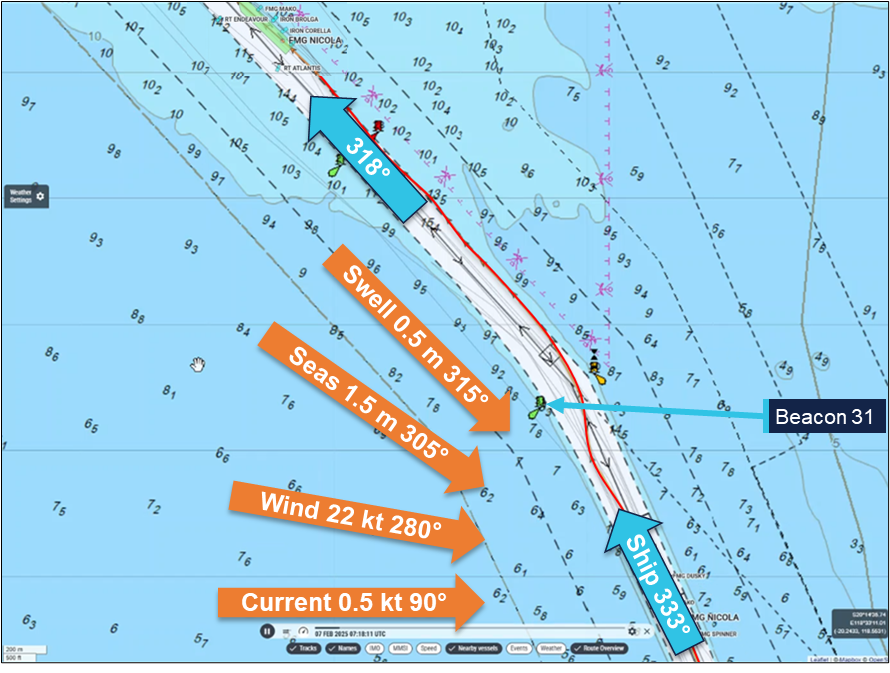
There were multiple weather monitoring stations throughout PPA’s areas of responsibility, including at beacon 31. At 1515, when FMG Nicola’s main engine shut down, the conditions recorded at beacon 31 (Figure 6) were:
Wind: 22 knots, gusting to 27 knots, from 280°
Current: 0.5 knots, towards 90°
Seas/Waves: 1.5 m, from 305°
Swell: 0.52 m, from 315°
Tide: 4.8 m rising.
Figure 6: Weather conditions (recorded at beacon 31) at 1515 hours
Source: Marine Traffic, Pilbara Ports Authority, annotated by the ATSB
Port Hedland port user guidelines and procedures stated that ‘average wind speeds ≥ 25 knots for 3 consecutive 10-minute intervals (were) considered to be the upper limit for handling vessels in the inner harbour and main shipping channel.’ Readings from beacon 31 showed the average wind speed to increase from 20 knots at 1400 to peak at 25 knots at about 1545, and remain at this level until after 1800. During this time, gusts to about 32 knots were recorded.
The 3 tugs assisting the ship out the channel all reported difficulties with the weather before and during the incident. FMG Mako was positioned at the port shoulder for the transit and exposed to the weather. While approaching beacons 30-31, the tug was let go and was directed to the port quarter to push up. In this location it was further hampered by the excessive movement of the tug in the prevailing conditions.
FMG Dusky’s master (starboard shoulder) reported that the weather was inclement which affected the effectiveness of the tug. During initial attempts to regain control of the ship, including applying braking force through FMG Dusky, one of the tug’s main engines shut down due to being overloaded. Power was quickly restored and the tug returned to full operation.
The master of FMG Spinner, at the centre lead aft position, reported the sea state as ‘poor, with a short, sharp, confused swell around 2 m’. During manoeuvring to take FMG Nicola’s stern to starboard, the tug shipped seas with sufficient force to shatter one of its bridge windows.
Post‑incident action
FMG Nicola
The ship’s managers (BSM) conducted an investigation, which focused on the cause of the main engine shutdown. Other interested parties also conducted independent investigations, which included inspections by the engine manufacturer and an underwater (dive) survey. All investigations concluded that the root cause of the main engine shutdown was an intermittent malfunction of the lubricating oil low pressure switch, which triggered an engine emergency stop despite all system parameters being normal.
The switch was replaced with a new spare on board and the operating point set to 160 kPa. In addition, the planned maintenance system routines were amended to require calibration of main engine LO pressure switches monthly and replacement of the shutdown switch reduced from 5 years to 2.5 years.
The ship’s hull inspections included an underwater survey. In summary, the survey report indicated that no evidence of hull or bilge keel damage was found and hull paintwork was intact. Similarly, no damage to the propeller and rudder was reported.
All inspections, testing and corrective actions were conducted to the satisfaction of the ship’s classification society.
Pilbara Ports Authority
Soon after being notified of the loss of propulsion, and before the ship exited the channel, PPA made a request to the master for reports into the incident and including root cause analysis and preventive measures. In addition, PPA conducted an investigation into the incident, which focused on the loss of propulsion, the effectiveness of pilotage and towage procedures, and the response.
The investigation made recommendations to various involved parties, including the ship’s operators and managers, and towage and pilotage organisations. Recommendations included updating pilotage emergency response procedures to consider loss of ship propulsion that affects steerage and optimal positioning and use of tugs. Additional training of pilots and tug masters, including on the hydrodynamic interaction between tugs and ships with low under keel clearance, was also advised.
Incident reporting
The Navigation Act 2012 required owners and masters of all vessels involved in a marine incident in Australian waters report it to the Australian Maritime Safety Authority (AMSA).14 The reporting involved a 2-step process by submitting an:
incident alert form15 as soon as ‘reasonably practicable’ (within 4 hours) after the incident either online or by email to the AMSA email address identified on the form
incident report form16 with further details within 72 hours.
Additionally, incidents were required to be reported to the ATSB in accordance with the governing legislation.17 Under this legislation, responsible persons (including the ship’s master, owner, operator or agent, the pilot, pilotage provider and VTS authority) were required to report an incident. Incident reports submitted to AMSA were forwarded to the ATSB, which allowed a responsible person to meet their Transport Safety Investigations Act reporting obligations.
Incident handling process
The AMSA Response Centre (ARC) was responsible for the receipt, assessment, triage and onward dissemination of all incident reports received by AMSA. A formal, documented procedure was followed in handling reports. All reports were assessed and classified into 4 categories:
Red – an immediately reportable emergency such as imminent danger to the vessel, life or the environment.
Orange – an immediately reportable incident that may require follow-up or prosecution, including fatalities, collision, breakaway, fire or explosion, grounding, serious pollution, damage which may affect safety of navigation, serious danger to the ship or persons, serious near miss.
Yellow – a reportable incident that may require AMSA action or investigation. This category included any incident under pilotage, environmental incidents and hazards to navigation.
Green – a reportable incident that did not meet the requirements of other categories.
Once categorised, the reports were processed as per the procedure with the levels of response and sharing of the details reducing with categories red through to green. All red and orange reports were forwarded to the ATSB. Yellow reports were forwarded to the relevant AMSA regional office and to other selected, incident-specific addresses (including the ATSB) for pollution or maritime labour convention related reports.
A process for the review of red and orange incident categorising was available for changing incident circumstances, such as severity, and for assurance and auditing purposes. Re-categorising required senior management assessment and approval.
Reporting of the incident
At 1642 on 7 February, a couple of hours after FMG Nicola’s propulsion loss, the ship’s local agent asked the master to submit the required incident reports, including the AMSA forms. Later that evening, the master emailed incident reports and supporting documents to the agent.
The following morning, 8 February, the agent forwarded the incident reports, including AMSA forms 18 and 19, and attachments, to relevant parties, including AMSA’s local office in Port Hedland. The reports were forwarded to AMSA’s incident reporting email address on 10 February.
The information in the reports indicated that the ship had not grounded and did not otherwise meet the guidelines to be categorised as red or orange. Consequently, as the incident had occurred ‘under pilotage’, it was categorised as ‘yellow’. As per procedures, the incident report documentation was not forwarded to the ATSB, but returned to the AMSA West regional office for information and review.
On 12 February, AMSA received an anonymous marine safety concern (AMSA form 355)18 of a ‘grounding event’ involving FMG Nicola that reportedly had occurred at 1412 on 8 February (the day after FMG Nicola’s departure). This report was forwarded to the AMSA West office and to AMSA’s Port Hedland office, and to the ATSB. The Port Hedland office responded that the ship’s agent and PPA had no record of a grounding event but noted there had been a stoppage of the ship’s main engine during departure (the incident reported on 10 February and categorised as ‘yellow’).
The ATSB followed up with AMSA for additional information about the anonymous report, but no further information was available. Over the following weeks, the ATSB followed up with AMSA again to check if further information, including AMSA incident report forms, was available. The ATSB was advised that no further information was available regarding a grounding, but that the ship had had a main engine failure, which did not involve grounding.
During July 2025, the ATSB became aware of media reports concerning the reported grounding of FMG Nicola while departing Port Hedland on 7 February. The ATSB followed up with AMSA and was advised that there was no information about a grounding event, other than the form 355 previously provided.
The ATSB then contacted PPA, which confirmed an incident involving a loss of the ship’s propulsion had occurred. The port authority provided copies of the incident reports and attachments that the master had submitted in February via the ship’s agent.
On 9 July 2025, after assessing the incident reports and other available information, the ATSB formally commenced this investigation.
Safety analysis
Loss of propulsion
Multiple investigations following the incident concluded that the root cause of the main engine shutdown was an intermittent malfunction of the lubricating oil (LO) low pressure switch, which triggered a main engine emergency stop, despite all system parameters being normal.
Separation between the LO shutdown system and the pressure monitoring system meant that when the shutdown switch activated, the monitoring system low LO pressure alarm was not triggered, and the pressure display did not show a fluctuation in pressure.
Inspection and testing of the shutdown pressure switch after the incident showed it to activate at 185 kPa and to operate erratically. No evidence was found to show that the failure was related to maintenance arrangements (inspection, calibration and replacement schedules); the switch had operated without any previous obvious fault.
Recovery
Following the main engine trip, the engine speed quickly dropped to zero. However, the ship’s speed fell away more slowly, due to the ship’s momentum, from 8.3 knots when the engine tripped, to 4.8 knots about 9 minutes later when the main engine was restarted.
The pilots immediately took action to control the ship’s movement and ensured steering was available. Port Hedland vessel traffic service (VTS) was notified and a ship emergency declared. In keeping with response guidelines, training and procedures, the ship was kept moving and additional assets were tasked to assist.
The ship was manoeuvred while being set to starboard and was passing between beacons 30-31 as operation of the main engine was restored. In unfavourable weather conditions, appropriate port rudder was used to manage the set to starboard and to avoid the stern swinging outside the channel and exposing the rudder and propeller to damage. Headway was maintained (minimum speed of 1.5 knots) with the main engine at half ahead (40 rpm) to keep the ship moving along the edge of the charted channel and avoid the adjacent shallow water. Beacon 28 was cleared successfully and at about 1550, 35 minutes after the initial loss of propulsion, with 7 tugs assisting, the ship was returned to the centre of the channel and safely navigated out the channel and to sea.
Inspections carried out as the ship continued to negotiate the channel and prior to departure of the pilots found no indication of water ingress or other damage. Further investigation including starboard side tank inspections, carried out at sea prior to arrival at the next port, also did not reveal any hull plating or ship structure damage. Following this, a class‑approved dive inspection found no hull or coating damage including that the bilge keels were in ‘normal’ condition.
In summary, the evidence showed that, while the ship moved along the edge of the charted channel, its hull did not contact the seabed.
Incident reporting
FMG Nicola’s loss of propulsion under pilotage met the requirements for reporting to AMSA as a marine incident. Shortly after the incident Pilbara Ports and the ship’s agent had requested incident reports from the ship’s crew, including those required by AMSA.
The morning after the incident, incident report forms were forwarded to the local Port Hedland office of AMSA. These were subsequently forwarded to the AMSA response centre. The information provided in and with the incident reports indicated that the ship lost propulsion, additional port towage assets were mobilised and the ship was safely taken to sea. The reports stated that the ship had not run aground or touched bottom. Consequently, as per AMSA procedures, the incident was assessed as being of lower severity than ‘red’ or ‘orange’ incidents and was triaged as ‘yellow’. The procedures did not require a ‘yellow’ level report to be forwarded to the ATSB.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of propulsion of FMG Nicola, Port Hedland, Western Australia, on 7 February 2025.
Contributing factors
FMG Nicola's main engine lubricating oil low pressure shutdown switch erroneously operated, causing the otherwise serviceable main engine to trip and stop.
Other factors that increased risk
The risk of grounding increased as, while maintaining headway and avoiding damage to the stern while turning, FMG Nicola tracked along the edge of the charted channel.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Pilbara Ports Authority
Pilbara Ports Authority advised the ATSB that safety action had been taken, which continued the port’s focus on machinery reliability, towage effectiveness, and structured emergency response. The actions taken were applicable to 5 areas of port operations:
Ship and machinery reliability – including increased ship vetting and inspection requirements for entry to Port Hedland.
Towage and escort strategy – assessment of tug effectiveness and limitations, defined wind and sea state thresholds, simulations and operational trials.
Tug management – guidance for pilot-tug communication protocols and tug release arrangements.
Pilotage and emergency response – procedural updates to clarify roles and responsibilities during multiple pilot pilotages and emergency situations, and to improve understanding of tug use and limitations in response to an emergency.
Training and operational awareness – to ensure that lessons learned from this incident were captured and implemented into port operations.
Safety action by FMG International
FMG International advised the ATSB that the following safety actions have been taken following this incident:
Details of the incident and investigation outcomes were distributed to the crews of sister ships of FMG Nicola.
Management of main engine lubricating oil pressure (MELOP) switches was updated:
MELOP switches were renewed on sister ships of FMG Nicola
the interval for renewal of MELOP switches was reduced from 5 years to 2.5 years on all ships in the FMG fleet
the interval for MELOP switch testing and calibration was reduced from 3 months to 1 month on all fleet vessels
after consulting with engine makers, the MELOP shutdown switch time delay was extended from 0.1 seconds to 1.9 seconds on all fleet vessels.
A procedure for resetting the MELOP shut down alarm within 1 minute has been implemented fleetwide. The procedure has also been incorporated into vessel training (drills and simulations) tools and requirements.
Safety action by the Australian Maritime Safety Authority
The Australian Maritime Safety Authority has updated incident report handling and triage procedures to better ensure the ATSB is notified of reportable marine incidents under its legislative requirements. The amended procedure requires pilotage incidents be reported to the ATSB.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Australian Maritime Safety Authority
Pilbara Ports Authority
FMG Nicola’s master, managers and Port Hedland agent
FMG International.
References
Rowe, R.W. (1996). The Shiphandler’s Guide. The Nautical Institute.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Australian Maritime Safety Authority
Maritime and Port Authority (MPA) of Singapore
Pilbara Ports Authority (PPA)
the pilots on board during the incident
FMG Nicola’s master
FMG International
Submissions were received from:
Maritime and Port Authority (MPA) of Singapore
FMG International
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^All times referred to in this report are local time, Coordinated Universal Time (UTC) + 8 hours.
^In conducting a pilotage, the pilot effectively has control of the ship’s navigation but legally only provides relevant advice to its master who remains responsible and always in command of the ship.
^A shoulder is the area where a ship’s hull form changes from the bow shape to the parallel mid body.
^The direction of the bow of a vessel expressed in degrees, either magnetic or true. All ship’s headings in this report are in degrees by gyro compass with negligible error.
^With all engine systems verified to be operating normally, the main engine trip lockout reset required return of the engine telegraph to the stop position (on the bridge and in the machinery control room (MCR)) and operating a manual reset push-button in the MCR.
^'Bank effect' and 'shallow water effect or squat' are hydrodynamic phenomena resulting from the effects of a ship transiting close to a canal bank and in shallow water respectively. When making headway, a positive pressure is developed at the ship's bow and a stronger low pressure area at its stern. This causes the stern to be pulled towards the bank. These forces intensify significantly with increased speed or shallow water, where restricted flow further reduces buoyancy and control. Constant rudder correction is required to maintain heading control of the ship. ‘The Shiphandler’s Guide’ The Nautical Institute
^Capesize ships generally have dimensions larger than that allowable for transit of Panama and Suez Canals and therefore have to sail around Cape Horn and the Cape of Good Hope.
^In 2001, BHP Limited merged with Billiton Plc to form BHP Billiton. In 2018, ‘Billiton’ was dropped from the organisation’s name, and it is now known as BHP.
^The Pilbara Ports Authority (PPA) was established on 1 July 2014, as a result of the Ports Legislation Amendment Act 2014, which consolidated 7 of Western Australia’s 8 port authorities into 4 new regional port authorities. The PPA was formed by the amalgamation of the former port authorities of Dampier and Port Hedland and also encompassed the ports of Ashburton and Varanus Island.
^Port Hedland channel zones: Zone 1 – the inner harbour and berths; Zone 2 – the inner harbour and berths to the south-west of zone 1; Zone 3 – from the outer limit of the inner harbour at Hunt Point to beacons 36-37; Zone 4 – from beacons 36-37 to 30-31; Zone 5 – from beacons 30-31 to beacons 15-16; Zone 6 – from beacons 15-16 to the termination of the channel at beacons C1-C2.
^FMG International (subsidiary of Fortescue Ltd) acted primarily as owner’s representative for Fortescue owned ore carriers, managing vessels technical and crew ship management, performed through 3rd party vessel technical/crew managers.
Interim report
Report release date: 09/10/2025
This interim report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Interim reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this interim report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
At 0832 local time on 7 February 2025, the 327 m bulk carrier FMG Nicola (image above) completed loading 237,088 t of iron ore at its berth in Port Hedland, Western Australia. The fully laden ship had a draught of 17.51 m forward and 17.69 m aft and was due to depart its berth in the afternoon (a high water of 5.56 m was predicted for 1634).
At 1330, 2 harbour pilots, one of whom was under supervision, boarded the ship. The port authority’s marine services delivery manager (MSDM), who was also a harbour pilot, boarded to observe the departure. By 1348, the ship’s main engine and steering had been satisfactorily tested and the master-pilot information exchange was completed in readiness for departure. The pilot under supervision would conduct[1] the pilotage and 4 tugs were secured to assist (see the section titled Towage).
By 1412, all mooring lines had been cast off and the ship departed the berth (Figure 1). There was a 25-knot north‑north‑west wind with waves of up to 1.5 m on a 0.5 m swell in the area, including the port’s single shipping channel.
Figure 1: Overview of FMG Nicola's track through shipping channel
Source: Australian Hydrographic Office, data from Australian Maritime Safety Authority
At 1442, with the ship progressing along the channel as planned, the MSDM disembarked via pilot launch. At 1446, one of the tugs was let go and returned to base.
At about 1500, FMG Nicola was turned to port to follow the channel at a speed of about 7 knots. Of the 3 tugs assisting, FMG Mako was fast at the ship’s port shoulder,[2]FMG Dusky at the starboard shoulder and FMG Spinner through the centre lead aft.
At 1514, as the ship approached beacons 32-33 (Figure 1), the pilot ordered a heading[3] of 334°. At about this time, FMG Mako’s master requested the pilot for its towline to be let go as there were choppy seas on the ship’s port side. The pilot concurred, and the towline was let go at 1515.
Soon after, at about 1516, FMG Nicola’s main engine suddenly shut down as it was passing beacons 32-33 (Figure 2). The ship’s speed was 8.3 knots and the pilot ordered the rudder midships. The pilot informed the tug masters that the ship had lost propulsion and directed them to help keep it in the channel.
Figure 2: FMG Nicola track from about 1516 to 1552
Source: Australian Maritime Safety Authority, Marine Traffic, annotated by the ATSB
At 1518, the pilot notified Port Hedland vessel traffic service (VTS) of the emergency and requested additional tugs. The pilot gave helm orders and used the tugs to follow the channel. The ship’s speed had decreased to 7.4 knots and it was getting closer to the western side of the channel and with a slow rate of turn of about 4° per minute to port (Figure 3).
Figure 3: FMG Nicola speed and rate of turn at the time of the incident
Graph derived from Automatic Identification System data and should not be used for further analysis. Source: Australian Maritime Safety Authority, analysis by the ATSB
Meanwhile, the ship’s engineers identified that the engine had shut down as the ‘main bearing and thrust bearing lubricating oil pressure low’ non‑cancellable trip had activated. The engineers determined that it had activated due to faulty operation of the pressure switch. After confirming all engine systems were operating normally, the engine trip lockout system[4] was reset and, at 1523, the engine was restarted at dead slow ahead.
At about 1525, FMG Nicola had passed beacons 30-31, and, with a rate of turn 7.5° per minute to port and speed of 4.3 knots, it closed on the eastern side of the channel. Soon after, the ship stopped turning and began moving along the side of the channel, which was aligned along a 318° (T) direction there.
The ship continued to move along the side of the channel (Figure 2). At 1534, the first of the additional tugs arrived and was tasked to push up on the ship’s starboard side. In the following 10 minutes, 3 more tugs arrived and assisted as required by the pilot. At 1540, the ship passed close to beacon 28 while moving along the side of the channel at a speed of 2.5 knots.
By 1550, the ship had been moved away from the channel side and its speed was increasing as the main engine speed had progressively been increased to full ahead. The tugs continued escorting the ship out the channel towards open water.
At about 1635, 3 tugs were released and a further 2 were released about 10 minutes later as the ship approached beacons C11-C12. The remaining 2 tugs were retained and escorted the ship until it passed beacons C1-C2 and to sea.
By the time the ship passed beacons C1-C2, the ship’s crew had completed inspecting and testing the main engine systems and rectified the fault. They had also conducted an inspection, including sounding compartments, to confirm there was no ingress of water.
Shortly after, at 1806, the pilots departed the ship by helicopter and the ship continued its passage to the next port, Dongjiakou, China.
During the passage, the crew inspected all ballast tanks on the starboard side and found no physical damage to the ship’s side or structure.
Context
FMG Nicola
General details
FMG Nicola was a Singapore-registered, capesize[5] bulk carrier built in 2016 by Jiangsu Yangzi Xinfu Shipbuilding, China. At the time of the incident, the ship was owned and operated by Fortescue Shipping Nicola, managed by Bernhard Schulte Shipmanagement (BSM), Hong Kong, and classed with Lloyd’s Register (LR).
At the time of the incident, FMG Nicola was crewed by 23 Sri Lankan and Indian nationals, including the master, all appropriately qualified for their positions on board.
The master had 26 years of seagoing experience, all on bulk carriers, with about 4 years in command. The master joined Bernhard Schulte Shipmanagement in 2015 and had completed several assignments on FMG Nicola since 2021.
The chief engineer had about 18 years of seagoing experience, with about 9 years at that rank. The chief engineer joined Bernhard Schulte Shipmanagement in September 2024 and was assigned to work on FMG Nicola.
Main engine
FMG Nicola’s propulsion was provided by a 6‑cylinder, MAN‑B&W 6G80ME‑C9.5 engine developing 18,240 kW. The main engine drove a single 4‑blade, fixed‑pitch propeller, providing a service speed of 14 knots.
Lubricating oil system
The main engine lubricating oil (LO) system was fitted with a hierarchy of oil pressure monitoring and alarm controls to limit inadvertent engine stoppage while preventing catastrophic engine damage. In addition to local, analogue indicators and pressure gauges, the LO pressure was monitored via a pressure transducer and pressure switches (Figure 4).
Signals from the sensors fed into the ship’s machinery alarm, monitoring and control system. This system provided real time, remote indication of the LO pressure. Software limits were incorporated to trigger alarms and other actions. Normal operating pressure for the system was about 250 kPa with software triggers set at:
210 kPa for standby pump start
200 kPa for low LO pressure alarm
180 kPa for main engine slow down alarm.
In addition to these triggers and alarms, the main engine LO system had a separate pressure switch set to activate at 160 kPa. This switch, independent of the oil pressure monitoring circuit, was for the main engine low LO pressure shutdown. This initiated rapid shutdown of the engine to prevent catastrophic damage due to complete loss of bearing lubricating oil.
Figure 4: Main engine lubricating oil pressure sensing and switches
Source: Fortescue Metals Group
The normal, expected, sequence of loss of LO pressure indications would follow persistently falling oil pressure: standby pump start, low pressure alarm and main engine automatic slow down prior to main engine shutdown.
The machinery monitoring system allowed for (adjustable) time delays on activation of each of these triggers. At the time of the incident, the engine LO pressure shutdown delay was set to 0.1 s (following subsequent advice from the engine manufacturer that the delay could be increased up to 2 s, it was reset to 1.9 s).
Components of the main engine LO system were subject to regular maintenance through the ship’s planned maintenance system (PMS). The PMS records showed that the main engine pressure transmitter and pressure sensors had last been checked on 15 November 2024 (about 3 months before the incident).
Post‑incident action
The ship’s managers (BSM) conducted an investigation, which focused on the cause of the main engine shutdown. Other interested parties also conducted independent investigations, which included inspections by the engine manufacturer and an underwater (dive) survey. All investigations concluded that the root cause of the main engine shutdown was a faulty lubricating oil low pressure switch which triggered an engine emergency stop despite all system parameters being normal.
The separation between the LO shutdown system and the pressure monitoring system meant that when the shutdown switch activated, the monitoring system low LO pressure alarm was not triggered, and the pressure display did not show a fluctuation in pressure.
Inspection and testing of the shutdown pressure switch showed it to activate at 185 kPa and to operate erratically. The switch was replaced with a new spare on board and the operating point set to 160 kPa. In addition, the planned maintenance system routines were amended to require calibration of main engine LO pressure switches monthly and replacement of the shutdown switch reduced to 2.5 years (from 5 years).
The ship’s hull inspections included an underwater survey. In summary, the survey report indicated that no evidence of hull or bilge keel damage was found and the hull paint was intact. Similarly, no damage to the propeller and rudder was reported.
All inspections, testing and corrective actions were conducted to the satisfaction of Lloyds Register, the ship’s Classification Society.
Port Hedland
General information
Port Hedland, situated in the Pilbara region of Western Australia, is the world’s largest bulk export port by tonnage, handling over 500 million tonnes of cargo annually. More than 95 per cent of this volume is iron ore, exported primarily by BHP,[6] Fortescue Metals Group (FMG) and Roy Hill Infrastructure, with the port serving as the companies’ main export hub for all Pilbara output. In addition to iron ore, the port also handles exports of salt, manganese, copper concentrates, lithium minerals and livestock.
At the time of the incident, the port’s infrastructure comprised 19 operational berths. Eight of these berths were owned and operated by BHP, with the remaining berths owned and operated by FMG (5 berths), Roy Hill (2 berths) and Pilbara Ports Authority[7] (4 berths). Shipping activity is significant, with more than 6,000 ship movements (inbound and outbound) each year.
Shipping channel
Access to the port was provided by a single 22‑mile[8] dredged channel, which allowed only one large ship to pass at a time. For most laden ships, particularly capesize ships, such as FMG Nicola, use of the channel was restricted by tidal conditions. The incident took place within the 10‑mile section of the channel closest to the port, an area prone to strong tidal flows and with particularly confined spaces, narrowing to a minimum width of 162 m and featuring steep batter slopes. The channel depth in this section was maintained at about 15 m, while adjacent waters were generally about 6 m deep.
The features of the channel described above make the risks associated with channel blockage high. A disabled ship can strand on a receding tide as well as blocking the passage of other ships. Depending on departure times, separation between ships and the location of an incident, up to 3 additional ships could be committed to, or within, the channel and exposed to this hazard at a given time.
Pilbara Ports Authority
The port was managed by the Pilbara Ports Authority (PPA), which had overarching responsibility for safety and efficiency of port operations and the environment under state legislation. The PPA’s jurisdictional responsibilities were exercised through the Port Hedland harbour master.
The harbour master’s responsibilities included the coordination of vessel traffic services, ship scheduling, pilotage and maintenance of shipping channels, navigational aids and port infrastructure. The PPA issued third‑party contracts or licences for stevedoring, towage, some pilotage services and pilot transfers (helicopter and boat).
Pilotage
Vessels 35 m or greater in length using the main shipping channel and navigating within port limits were required to use the services of a licenced harbour pilot. Pilotage services for the port were provided by PPA through directly employed pilots as well as by third‑party, contracted providers.
The pilots on board FMG Nicola at the time of the incident were employed by PPA. All PPA pilots had undertaken a competency‑based pilotage training program incorporating on‑water and simulator training and competency assessments.
The supervising pilot had worked for PPA since 2023. They had over 25 years of experience in the maritime industry, including positions as a marine pilot in Brisbane, Queensland, as an LNG loading master and as Senior Advisor Seafarer Standards with AMSA.
The pilot under supervision joined PPA in 2024 after more than 15 years as a pilot in Ningbo‑Zhoushan, China. At the time of the incident, they held a level 3 authority to pilot in Port Hedland and were undertaking supervised pilotages to upgrade this licence to level 4.
Towage
The Port of Port Hedland - Port User Guidelines and Procedures documented the tug allocation requirements based on specified criteria. Laden outbound capsize ships required 4 tugs secured to the ship from the berth to Hunt Point, near the harbour entrance. The requirement for the transit from Hunt Point to beacons 31/30 was 3 tugs.
Tugs in Port Hedland were operated under towage licences granted by the PPA to Pilbara Marine (a subsidiary of FMG) and BHP Towage Services (BHPTS). KOTUG operated tugs under the Pilbara Marine towage licence while Rivtow was contracted to operate the tugs under the BHPTS licence.
The 4 tugs assigned to FMG Nicola on the day of the incident were ART85‑32W class advanced rotortugs, operated by KOTUG. Each tug had a bollard pull[9] of 85 tonnes and used a hybrid propulsion arrangement with 2 azimuth thrusters forward and a third azimuth thruster aft.
The tugs which came to render assistance after FMG Nicola lost propulsion were operated by Rivtow and comprised of 2 ART80‑32 rotortugs and 2 RAstar85 azimuth stern drive (ASD) tugs.
Investigation into incident
Pilbara Ports Authority conducted an investigation into this incident, which focused on the loss of propulsion, the effectiveness of pilotage and towage procedures, and the response. The investigation recommended updating pilotage emergency response procedures to consider loss of ship propulsion resulting in loss of steerage and optimal positioning and use of tugs. Another recommendation was the additional training of pilots and tug masters, including on the hydrodynamic interaction between tugs and ships with low under keel clearance.
Incident reporting
The Navigation Act 2012 required owners and masters of all vessels involved in a marine incident in Australian waters report it to the Australian Maritime Safety Authority (AMSA).[10] The reporting involved a 2-step process by submitting an:
incident alert form[11] as soon as ‘reasonably practicable’ (within 4 hours) after the incident either online or by email to the AMSA email address identified on the form.
incident report form[12] with further details within 72 hours.
Additionally, incidents were required to be reported to the ATSB in accordance with the governing legislation.[13] Under this legislation, responsible persons (that in summary, included the ship’s master, owner, operator, agent, the pilot, pilotage provider and VTS authority) were required to report an incident. Incident reports submitted to AMSA are forwarded to the ATSB, which allowed a responsible person to meet their TSI Act reporting obligations.
Reporting of the incident
At 1642 on 7 February, a couple of hours after FMG Nicola’s propulsion loss, the ship’s local agent asked the master to submit the required incident reports, including the AMSA forms. Later that evening, the master emailed incident reports and supporting documents to the agent.
The following morning, 8 February, the agent forwarded the incident reports, including AMSA forms 18 and 19, and attachments to relevant parties, including AMSA’s local office in Port Hedland. The reports were forwarded to AMSA’s incident reporting email address on 10 February. The notifications submitted by FMG Nicola’s master regarding the loss of propulsion incident did not, at that time, reach the ATSB.
On 12 February, AMSA received an anonymous marine safety concern (AMSA form 355) of a ‘grounding event’ involving the ship that reportedly had occurred at 1412 on 8 February (the day after FMG Nicola’s departure). This report was forwarded to the ATSB and AMSA’s offices in Fremantle and Port Hedland. The Port Hedland office reported back that the ship’s agent and PPA had no record of a grounding event, but noted there had been a stoppage of the ship’s main engine during departure.
The ATSB immediately followed up AMSA for information about the anonymous report but no further information was reportedly available. Over the following weeks, the ATSB followed up with AMSA to check if further information, including AMSA incident report forms, had become available. The ATSB was advised no further information was available.
In July of 2025, the ATSB became aware of media reports about the grounding of FMG Nicola while departing Port Hedland on 7 February. The ATSB again followed up with AMSA and was advised that there was no information about such an incident, other than the form 355 previously provided.
The ATSB then contacted PPA, which confirmed an incident involving a loss of the ship’s propulsion had occurred. The port authority also provided copies of the incident reports and attachments that the master had submitted in February via the ship’s agent.
On 9 July 2025, after assessing the incident reports and other available information, the ATSB formally commenced an investigation into this incident and its reporting.
Further investigation
To date, the ATSB has collected evidence from relevant parties including:
The investigation is continuing and will include examination and analysis of the evidence received, including:
event sequence
corroborating data
ship track and position
response to the incident
reporting of the incident to authorities.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]In conducting a pilotage, the pilot effectively has control of the ship’s navigation but legally only provides relevant advice to its master who remains responsible and always in command of the ship.
[2]A shoulder is the area where a ship’s hull form changes from the bow shape to the parallel mid body.
[3]The direction of the bow of a vessel expressed in degrees, either magnetic or true. All ship’s headings in this report are in degrees by gyro compass with negligible error.
[4]With all engine systems verified to be operating normally, the main engine trip lockout reset required return of the engine telegraph to the stop position (on the bridge and in the machinery control room (MCR)) and operating a manual reset push-button in the MCR.
[5]Capesize ships generally have dimensions larger than that allowable for transit of Panama and Suez Canals and therefore have to sail around Cape Horn and the Cape of Good Hope.
[6]In 2001, BHP Limited merged with Billiton Plc to form BHP Billiton. In 2018, ‘Billiton’ was dropped from the organisation’s name, and it is now known as BHP.
[7]The Pilbara Ports Authority (PPA) was established on 1 July 2014, as a result of the Ports Legislation Amendment Act 2014 which consolidated 7 of Western Australia’s 8 port authorities into 4 new regional port authorities. The PPA was formed by the amalgamation of the former port authorities of Dampier and Port Hedland and also encompassed the ports of Ashburton and Varanus Island.
[14]FMG International (subsidiary of Fortescue Ltd) acted primarily as owner’s representative for Fortescue owned ore carriers, managing vessels technical and crew ship management, performed through 3rd party vessel technical/crew managers.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
At about 0800 local time on 1 June 2025, an instructor and student were conducting a training flight from Bankstown Airport, New South Wales in a Piper PA-28-151 aircraft. The aircraft was fitted with a disposable passive carbon monoxide (CO) detector.
During the pre-flight preparations, the CO detector was confirmed to show that there were no signs of carbon monoxide in the cockpit.
Shortly after take-off, while climbing through 300 ft, the instructor noticed that the CO detector had changed colour and was showing full black, indicating a high presence of carbon monoxide in the cockpit. This indication was then verified by the student pilot.
The instructor took over control of the aircraft and asked the student to open the storm window to allow fresh air into the cabin. At the advice of the instructor, the student placed their mouth and nose close to the storm window to breath from the stream of fresh air.
The flight crew requested, and ATC approved, the aircraft to rejoin the circuit and they landed back at Bankstown Airport shortly after with no further event. Prior to landing, the CO detector was noted to have changed colour to light brown, indicating that levels of carbon monoxide in the cockpit had reduced, likely due to the storm window being opened.
Once on the ground, the student pilot reported feeling no symptoms of carbon monoxide poisoning, while the instructor experienced only slight dizziness, but believed this could have been caused by adrenaline from managing the event. Blood tests conducted on both pilots detected only negligible levels of carbon monoxide in their bloodstreams.
A subsequent engineering inspection of the aircraft revealed a rubber boot seal on a nose wheel steering rod had split which was suspected of causing the CO leak. Following rectification, a check flight was performed during which no carbon monoxide was detected inside the cockpit.
Safety message
This incident serves as a salient reminder of the importance of carrying effective carbon monoxide (CO) detection equipment on board aircraft.
CO is a colourless, odourless and tasteless gas found in exhaust gases of piston engine aircraft. While passive CO detectors are commonly used in general aviation aircraft, they have limitations and rely on the pilot regularly monitoring the colour of the detector. In contrast, active electronic CO detectors are designed to attract attention through an audible alert at low CO concentrations, so are more likely to be effective. These devices are now inexpensive and widely available.
Following the fatal crash of a DHC-2 in 2017, in which the pilot was impaired due to carbon monoxide poisoning (Collision with water involving a de Havilland Canada DHC-2 Beaver aircraft, VH‑NOO, at Jerusalem Bay, Hawkesbury River, New South Wales, on 31 December 2017AO-2017-118), and a review of the effectiveness of carbon monoxide detectors by the UK Civil Aviation Authority, the ATSB launched its Know CO campaign.
These resources highlight the limitations of passive carbon monoxide detectors and strongly recommend that operators and owners of piston engine aircraft install active attention‑attracting CO detectors which provide the best opportunity of detecting carbon monoxide exposure before it can adversely impact their ability to control the aircraft.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
The ATSB’s investigation of a drone swarm accident in which more than 400 drones were lost before a planned display at Melbourne’s Docklands highlights the importance of operators using effective checklists and being familiar with all their system’s functionality and data capabilities.
The swarm of 500 Damoda Newton V2.2 drones were to be used for a light display over the water of Dockland’s Victoria Harbour on the evening of 14 July 2023.
Shortly after launching the swarm, the remote pilot in command (RPIC) identified both visually and from errors displayed on their ground control station (GCS) computer that multiple drones were out of position.
Despite the errors, the drones automatically began to move from the launch location to the show area, over the water. During this transition, further errors appeared on the GCS computer, with increasing severity.
“As the errors cascaded, drones were observed to be out of position and colliding with one another,” ATSB Chief Commissioner Angus Mitchell said.
“In response, the RPIC commanded the swarm to loiter and hold position, and attempted to return those with the most significant errors to the launch site individually.”
While multiple drones were in the loiter, the GCS computer lost connection to almost 400, with the majority descending into the harbour below.
Of the 500 drones, 427 were lost.
The ATSB’s investigation found the drones had encountered wind conditions exceeding their published capability shortly after launch, triggering collisions and a variety of technical errors.
“The wind limit exceedance was not identified by the RPIC as they were unaware that the wind speed affecting the aircraft was displayed on the GCS computer screen,” Mr Mitchell said.
The investigation noted the operator did not have a system to ensure all of its pilots could use all of the GCS software’s features, increasing the risk of show-qualified pilots failing to identify exceedances and increasing workload in the lead‑up to the show.
The operator has implemented several safety actions, including training improvements, the addition of a requirement for two CASA-approved pilots to operate every show, and for wind speed test flights using individual aircraft to take place prior to flights.
The ATSB’s final report also notes the GCS computer software did not have the functionality to actively alert a pilot to wind speed exceedances.
The manufacturer, Damoda, advised it is considering an update to enable such alerts.
“This incident demonstrates the importance of drone pilots being familiar with all functionality and data provided by relevant ground control software,” Mr Mitchell said.
“It also shows the impact human factors can have on drone operations, and how they should be actively considered and managed.”
While the risk profile may differ from that of crewed operations, Mr Mitchell noted factors such as workload and operational pressure can equally impact drone operations.
“Operators should have systems in place to ensure that pilots are familiar with system functionality, and they should ensure operational documentation, including checklists, carry the relevant prompts for flight crews to gather all necessary information to assist their decision-making process,” he said.
“Compliance with operational guidelines and limitations set or approved by the regulator are critically important to minimise risk to both the operation and the public.”
On 7 July 2025, a Kavanagh Balloons G-450, registered VH-FGC, was conducting a morning scenic flight near Beaudesert, Queensland, carrying 20 passengers and the pilot.
Shortly after launch when climbing above a ridge, the pilot identified a change in the expected wind direction and the presence of fog. The pilot considered the safest option available was to proceed to an alternate landing site in reduced visibility. However, on approach to land, a low-level wind shift changed the balloon direction. The pilot elected to conduct a landing at a different landing site rather than continue flight over populous areas.
On landing, the balloon basket was carried forward with momentum, it skipped several times before it came to a stop. However, the balloon envelope made contact with a dead tree, resulting in minor damage to the envelope. No injuries were reported.
What the ATSB found
The ATSB found that the pilot reassessed operational and safety decisions as unexpected weather impacted the flight (wind direction and fog). Ultimately the pilot was unable to avoid contact with a dead tree in the final stages of landing in reduced visibility.
However, comprehensive passenger safety briefings meant that passengers adopted brace positions prior to landing which likely prevented injury.
Safety message
The formation, movement and depth of fog is difficult to predict with accuracy, which can lead to pilots inadvertently flying into reduced visibility.
If contemplating ballooning operations in conditions conducive to fog development, even if it is not forecast, pilots are strongly encouraged to not only be aware of the possible formation of fog, but to plan for its likely effect on their flight.
This accident highlights the importance of effective safety briefings and how passengers adopting the correct body position during landing substantially reduces the likelihood and severity of injury. The pre-flight briefing is critical in ensuring passenger preparation, particularly as opportunities to reinforce this information during flight may be limited.
Pilots should use all available resources (such as passenger demonstrations and safety briefing cards) to ensure that each passenger understands the landing position and its importance.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is Reducing passenger injuries in commercial ballooning operations.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 7 July 2025, a Kavanagh Balloons G-450, registered VH-FGC, operated by Hot Air Pty Ltd was conducting a morning scenic flight near Beaudesert, Queensland.
The pilot conducted multiple weather assessments prior to the flight (see Pre-flight observations), and the balloon was set-up with the assistance of ground crew at The Overflow Estate (Figure 1).
At approximately 0623 local time, the balloon departed The Overflow Estate, at Wyaralong Dam in a north-easterly direction, carrying 20 passengers and one pilot. Based on their pre‑flight weather assessment, the pilot originally intended to land in a south-east landing site near Bromelton (Figure 1) and the ground crew had been instructed to make their way via car to assess the wind conditions near the intended landing site. However, after take‑off the balloon maintained a north-east flight path towards Woodhill and Cedar Grove.
Figure 1: Flight path overview
Source: Google Earth, annotated by the ATSB
About 13 minutes after launch, the balloon had passed over the dam when the pilot climbed the balloon over a ridge line. At about 500 ft above ground level (AGL), the pilot described encountering fog in the direction of travel (Figure 2). The pilot discounted nearby options for an early landing and considered that the safest option available, in the reduced visibility, was to select a new landing site clear of hazards in the north-east (Figure 3).
Figure 2: Fog visible after climbing a ridge at 0636
Source: Operator, annotated by the ATSB
Figure 3: Flight path details
Source: Google Earth, annotated by the ATSB
While en route to that preferred landing site, the fog thickened, before the pilot climbed the balloon above the fog (Figure 4).
Figure 4: Fog conditions below the balloon at 0640
Note: Two other balloons from a separate (unidentified) operator were visible above the fog at this time. Source: Operator
At about 0703, while on approach to the preferred landing site (Figure 3), the balloon encountered a low-level wind change at about 200 ft, increasing in strength from 4–6 kt. The wind change tracked the balloon 90 degrees left, and made landing unfeasible due to a dam and trees.
The wind shift was unexpected to the pilot as they described that surface conditions looked calm, with the fog not appearing to move. Due to ground crew traveling back from the first intended landing site, the pilot did not have information usually available via a surface wind assessment on the ground.
The pilot reconsidered the safest options available considering the reduced visibility and selected a different landing site further north, which was used infrequently by the operator, was closer to a populated area and isolated trees, but with no identified powerlines (Figure 3). The pilot burned[1] to lift the balloon over a wet area before descending towards the new landing site.
On approach, the pilot burned again to lift the balloon over a boundary fence (Figure 5) before they commenced deflation to descend for landing and instructed the passengers to adopt their pre-briefed brace positions. While approximately 5 m from the ground, the pilot visually detected a dead tree (Figure 5). In response they rapidly deflated the balloon in an attempt to stop short of the tree. The pilot further reinforced the brace instruction to the passengers. At 0709, the balloon basket touched down, however was carried forward with the balloon’s resultant air mass momentum. The basket skipped 4 times before it stopped moving (Figure 5), however the balloon envelope inertia continued until the envelope contacted a dead tree (to the left of the basket), resulting in minor damage.
Figure 5: Onboard video of the approach (left) and the final approach flight path (right)
Source: Operator and Google Earth, annotated by the ATSB
The pilot and passengers were uninjured, and due to the delayed arrival of the ground crew, the pilot sought the help of 3 volunteer passengers to recover the envelope from the tree. There was no resultant damage to the basket, however envelope damage included 15 large tears due to contact with the dead tree.
Context
Personnel information
The pilot held a commercial pilot licence (balloon), with 1,253.2 hours total flying time, of which 1,174 hours were flown as pilot in command. In the previous 90 days, the pilot had flown 40.2 hours as pilot in command, including 7.2 hours on the G-450.
The pilot held a current CASA class 2 aviation medical certificate with no conditions.
The pilot reported starting work at 0430 on the day of the occurrence, having obtained about 6 hours of sleep the night before, and an additional 30‑minute nap the previous morning. They recalled feeling fully alert at the time of the occurrence.
Aircraft information
VH-FGC was a Kavanagh Balloons G-450 manned free balloon, manufactured in 2017 by Kavanagh Balloons Australia Pty Ltd. The aircraft was certified in the manned free balloon category and operated with a valid certificate of airworthiness.
The G-450 balloon has an envelope capacity of 450,000 cubic feet and a maximum take‑off weight of 3,700 kg. At the time of the occurrence, the balloon envelope had accumulated a total time of 662.6 hours in service, while the basket had accumulated 1,614.1 hours. The basket was designed to carry a maximum of 24 passengers per basket (6 per passenger compartment).
The balloon was fuelled with 358 L of liquid petroleum gas propane at the start of the flight, with 135 L remaining at landing.
Operator information
Hot Air Pty Ltd operates in the Scenic Rim area of South East Queensland and also the Atherton Tablelands in north Queensland. The organisation has agreements in place with landowners to access several launch and landing locations in a circular pattern near Beaudesert, referred to as the operator’s flying area. The locations include private and commercial properties.
Recorded information
The balloon was equipped with the following equipment capable of recording:
a GPS which records the flight track
a ‘flight tablet’ which included an electronic Google Earth satellite map (Figure 6). The satellite map was overlaid with the operator’s flying map layer which was maintained/updated via an electronic register. The flying map included the following operational information:
launch and landing areas / property boundaries (dark blue)
sensitive zones (SZs), with restricted operation (red)
powerlines (yellow)
other relevant landowner information (white text).
An onboard camera recording the front facing view of the flight.
Figure 6: Operator flying map showing the balloon flight path
Note: Property names were blurred to maintain landowner privacy. Source: Operator, modified by the ATSB
The final landing site was designated an ‘emergency landings only’ area on the Operator flying map (Figure 6) in Woodhill. The operator occasionally used this site when necessary, but it was not used frequently.
Meteorological information
Observations for surrounding area
The Beaudesert automatic weather station (AWS) provided the air temperature (°C), dew point temperature (°C), and relative humidity (%) along with other information and showed conditions conducive to fog formation (Table 1), that is:
temperature and dew point less than 1°C difference
winds were calm
high relative humidity (above 95%)
no significant weather movement.
Table 1: Beaudesert AWS information for 7 July 2025
A local graphical area forecast was valid for a six-hour period from 0300–0900 which indicated visibility of about 300 m with scattered fog.
At 0503, the Bureau of Meteorology (BoM) issued an updated aerodrome forecast (TAF)[2] for Amberley, which indicated fog and reduced visibility of 500 m up until 0700 at which time the conditions could be expected to improve.
At 0607, the BoM issued a further update to the TAF, which forecast shallow fog with visibility of 8,000 m, and a 30% probability of fog reducing visibility to 800 m and scattered cloud at 200 ft, until 0900 that day.
Satellite imagery
Satellite imagery was obtained from the BoM, valid as of 0500. The imagery depicted areas of fog or low cloud around, but clear of the original intended area of balloon operation (see Appendix A – satellite images).
Pre-flight observations
The pilot also reviewed several sources of weather information in the preceding hours prior to launch, as required by the operator’s exposition[3] (Version 1, 11 November 2024) and CASR Part 131[4] (Table 2).
Table 2: Pilot weather observations
Approx. time
Location
Information source or method
Assessment
Previous night
Near Beaudesert
Windy.com application
Wind conditions suitable for flight.
0415
Near Beaudesert
Visibility by sight
BoM Brisbane (Mt Staplyton) Radar Loop
Visibility clear for flying area[1].
Rain showers would be clear by launch time (0623).
0430
Operator Base, Beaudesert
Visibility by sight
BoM Beaudesert AWS
BoM Brisbane (Mt Staplyton) Radar Loop
Windy.com application
NAIPS[2] account local GAF and surrounding aerodrome TAFs
Visibility clear for intended flight path.
Calm surface conditions with a temperature of 12°C.
Rain showers had cleared the flying area.
Light and variable surface winds, becoming south‑westerly 5 kt at 1000ft then westerly 16 kt at 3,000 ft.
Light winds at nearby stations, and most clear except for Amberley that indicated a chance of surface fog, however not operationally relevant being more than 48 km away from Beaudesert.
0445
Bromelton observation point
Visibility by sight
Pibal
Visibility clear for intended flight path. Fog present in the south of the flying area around Laravale, more than 14 km south of Beaudesert.
Very light southerly for 300 ft, then turning into a west‑north-westerly wind of approximately 6-8 kt before swinging back to a westerly wind of approximately 10–15 kt (as the Pibal climbed).
0530
Launch site at Wyaralong Dam
Visibility by sight
Pibal
Visibility clear for intended flight path.
No change to previous Pibal wind readings.
This location sits on elevated land and provides visibility of a proportion of the operator’s flying area.
Airservices NAIPS Internet Service (free registration required)
Based on the observations the pilot decided to depart from The Overflow Estate launch site (west of Beaudesert) with the plan to fly in a south-east direction back into their operational flying area (and towards Beaudesert).
Regulatory requirements and guidance
Balloon pilots and operators must also comply with Part 131 of the Civil Aviation Safety Regulations (CASR), pre-flight weather assessment rules in section 12.02 of the Part 131 Manual of Standards (MOS).[5]
Balloon operations can occur in Class G airspace with at least 100 m visibility below 500 ft AGL when outside 10 NM from an aerodrome (such as in the case of Beaudesert). However, CASA highly recommends that pilots and operators exercise this significant reduction in the visibility requirements with caution and only if sufficient flight preparation has taken place. Further balloon guidance is available at Advisory Circular 131-02 v4.0.
Survivability
Pre-flight passenger safety briefing
One consideration in balloon accidents is the basket tipping during landing, which can increase the risk of injury. Tipping is more likely if a basket contacts, or lands on, a tree or fence.
Passengers were provided with safety briefings and instructions prior to boarding as required by the operator’s exposition. These included:
entry/exit to the basket
remaining in the basket until instructed by crew
securing and stowing personal items
prohibited dangerous goods
use of rope handles
landing/brace positions (for normal/upright landing and emergency/hard landing).
The passengers included several foreign tourists from non-English speaking backgrounds. Verbal information was supported by physical demonstrations (of the required landing position) and graphical briefing cards with basic diagrams and translations in simplified Chinese, Japanese, Korean, and German.
One passenger reported receiving pre-flight safety information via email at multiple points leading up to the flight, which was then supported by the safety demonstration on the day of the flight.
Related occurrences
A search of the ATSB occurrence database found that in the 10 years to July 2025 there were 37 balloon hard landings, ground strikes, or collisions with terrain in Australia, resulting in 17 injuries. Of these, 13 occurrences involved contact/collision with trees.
Further information on some of these occurrences can be found in Appendix B – Related occurrences.
Safety analysis
As is often required in balloon operations, the pilot was required to reassess operational and safety decisions at multiple points before and during the flight.
This analysis will explore the assessment of weather, launch location, contingency options, and landings in reduced visibility.
Fog encountered in flight
Fog was forecast for a wide area that included the operator’s flying area and the local conditions were conducive to fog. Satellite images support the pilot’s report by confirming that fog was likely not visible in the immediate flying area when the pilot travelled to the launch site before the flight. Based on their visibility assessment and pre-flight observations, the pilot determined it was safe to fly.
However, after take-off and on climbing above the ridge line over the dam, the pilot identified fog in the direction of flight, and the balloon subsequently entered fog.
Approach to land
Once lined up and on approach to land at the preferred landing site, the balloon was affected by an unexpected low-level wind shift and tracked about 90 degrees to the left.
Subsequently, the pilot considered other landing locations and associated risks, and selected an emergency landing site, used infrequently by the operator.
Reduced visibility
Once committed to landing in the final landing area in significantly reduced visibility, the pilot visually detected a tree through the fog in front of the balloon. In an attempt to take avoiding action, they rapidly deflated the envelope to land the balloon, however due to inertia, the balloon envelope made contact with the tree and was damaged.
Comprehensive safety briefings
The passengers were provided with comprehensive safety information leading up to, and before the flight. The ground crew and pilot also ensured understanding of the brace positions prior to launch.
As a result of the proper brace position, effective briefing and re-enforced communication during landing, no injuries were sustained.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the controlled flight into terrain involving Kavanagh Balloons G-450, registration VH-FGC, 12 km north‑north-west of Beaudesert, Queensland, on 7 July 2025.
Contributing factors
After clearing a ridge line, fog was encountered in the direction of the flight path.
During the approach to land in low visibility, an unexpected low-level wind shift diverted the balloon away from the preferred clear landing area, and required the pilot to select an alternate unplanned landing site in the final stages of landing.
Due to reduced visibility, the pilot was unable to see hazardous obstacles in the final landing area and therefore unable to take timely avoiding action.
Other findings
Comprehensive passenger safety briefings meant passengers adopted brace positions prior to landing which likely prevented injury.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of the accident flight
the chief pilot of the operator
Civil Aviation Safety Authority
Bureau of Meteorology
accident witnesses
video footage of the accident flight and other photographs and videos taken on the day of the accident
recorded data from the GPS unit on the aircraft.
References
CASA (Civil Aviation Safety Authority), (2025), Part 131 Aircraft – Operations, Advisory Circular AC 131-02v4.0, CASA
CASA (Civil Aviation Safety Authority), (2025), CASR Part 131 – Guide for balloons and hot air airships, v1.2, CASA
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
the operator
Civil Aviation Safety Authority
Bureau of Meteorology.
Submissions were received from:
Civil Aviation Safety Authority
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – satellite images
High resolution visible satellite imagery
Satellite imagery was obtained from the Bureau of Meteorology and was valid at 0500 (Figure A1) showing fog/low cloud as light blue areas.
Figure A1: High resolution visible satellite imagery from 0500
Note: This imagery was not available to the pilot at the time of the event. Source: The Bureau of Meteorology, annotated by the ATSB
Appendix B – Related occurrences
Hard landing involving balloon, VH-EUA, near Yarra Glen, 8 February 2018 (AO-2018-016)
On 8 February 2018, a Kavanagh B-350 hot-air balloon, registration VH-EUA, departed Glenburn, Victoria, for a scenic charter flight with a pilot and 15 passengers on board. About 45 minutes into the flight, over the Yarra Valley, the balloon experienced a sudden wind change with associated turbulence. The pilot decided to land immediately rather than continue over rising and heavily vegetated terrain. The resulting landing was hard and fast and 11 passengers were injured, with 4 of them receiving serious injuries.
Collision with terrain involving Kavanagh E-240 Balloon, VH-LUD, near Yamanto, Queensland, on 8 October 2021 (AO-2021-042)
On 8 October 2021, a Kavanagh Balloons E-240 balloon, registered VH-LUD and operated by Floating Images Aust. Pty Ltd was conducting a morning scenic flight about 45 km south‑west of Brisbane, Queensland. On board were a pilot and 9 passengers. About 55 minutes into the flight, the pilot commenced a descent to locate a suitable landing area. During the descent, the balloon entered an area of localised fog where visibility reduced to 10 m.
The pilot continued the descent into the fog until a tree was observed in the path of the balloon. The pilot attempted to avoid the tree by initiating a climb, but the balloon collided with, and came to rest on the side of, the tree, damaging the lower part of the balloon envelope. The pilot subsequently climbed the balloon off the tree and above the fog. The flight continued to an uneventful landing in a nearby paddock that was clear of fog. There were no injuries.
Controlled flight into terrain involving Kavanagh Balloons G-525, VH-HVW, Pokolbin, New South Wales, on 30 March (AO-2018-027)
At about 0710 Eastern Daylight-saving time on 30 March 2018, a Kavanagh Balloons G‑525 balloon, registered VH-HVW (HVW) and operated by The International Balloon Flight Company (Australia), launched from a site near Pokolbin, New South Wales, for a planned 1-hour scenic flight. HVW was one of three balloons launched by the company from the same site. After climbing through fog to about 2,000 ft and realising how far the fog layer extended, the pilot of HVW, along with the other 2 pilots, decided to abort the flight and descend for a landing at the nearest suitable site. On approach to land in low‑visibility conditions, HVW collided with trees, which caused the basket to rotate 180 degrees. It then landed heavily, resulting in injuries to 16 of the 24 passengers, 3 of them serious. The pilot was uninjured and 74 of the balloon’s panels required patching or repair.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The action of activating the burner to heat the air within the balloon, increasing internal temperature and causing the balloon to rise or maintain altitude.
[2]Aerodrome forecasts are a statement of meteorological conditions expected for a specific period of time, in the
airspace within a radius of 5 NM (9 km) of the aerodrome.
[3]A CASR Part 131 Balloon Transport Operation Exposition, also known as an ‘Operations Manual’.
[4]CASR Part 131 requires balloon operators to obtain a weather forecast from an authorised source, such as the Bureau of Meteorology, valid for a period extending 2 hours beyond their landing time.
[5]The Part 131 Manual of Standards (MOS) outlines the operational standards and requirements for operators of balloons and hot air airships in Australia to ensure safety and compliance with aviation regulations.
Occurrence summary
Investigation number
AO-2025-037
Occurrence date
07/07/2025
Location
12 km north-north-west of Beaudesert
State
Queensland
Report release date
26/11/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Controlled flight into terrain (CFIT), VFR into IMC
The ATSB’s investigation of an accident involving a Cessna 206 survey aircraft in south‑east WA highlights to air work operators the importance of ensuring risks inherent to their operations are effectively managed.
The single piston-engined Cessna U206G, operated by MAGSPEC Aviation, collided with terrain during a geophysical survey flight 124 km west of Norseman on 3 March 2022, the investigation report details. Recorded data showed the flight’s first survey line commenced at 1252 local time, and the aircraft’s last recorded position occurred at 1343, in the survey area.
The wreckage and the fatally injured pilot were found five hours later, although an earlier emergency response was unlikely to have altered the outcome due to the extent of the pilot’s injuries.
“The emergency response was not initiated until 30 minutes after the aircraft's estimated time of arrival, which was 3 hours after satellite tracking had stopped and attempts to contact the pilot had been unsuccessful,” ATSB Chief Commissioner Angus Mitchell said.
“Although an earlier response was very unlikely to have altered the outcome in this tragic case, minimising the time for search and rescue and enabling emergency services to respond as quickly as possible is essential.”
Mr Mitchell said the ATSB investigation concluded control of the aircraft was likely lost at a height from which recovery was not possible during a manoeuvre to intercept the next survey line.
“While an aerodynamic stall situation is a plausible explanation for the loss of control, this could not be conclusively established due to a lack of available evidence, including no recorded data beyond the last known position of the aircraft, and no witness observations,” he said.
However, Mr Mitchell said the investigation made several findings regarding risks to aviation safety that are pertinent to air work operators.
“Air work such as mustering, spraying and geophysical survey are conducted at low levels out of operational necessity, which creates an inherently high‑risk operating environment,” he said.
“Operators are responsible for effectively managing this heightened risk with adequate and effective processes and controls.”
The investigation found MAGSPEC Aviation’s risk management processes did not include a pre-operational risk assessment to consider the generic risks and hazards common across low‑level survey operations.
“Further, a risk register was not maintained, limiting the operator’s ability to track, monitor, and mitigate all known hazards, and assess the effectiveness of the existing risk controls.”
Pilots routinely flew survey patterns using steep turns at low level, in accordance with their operator-provided training.
“Procedures or limitations specific to these manoeuvres were not included in the operations manual, increasing the risk of inconsistencies in the application of those manoeuvres and reducing the safety margins available,” Mr Mitchell observed.
Since the accident, MAGSPEC Aviation has updated its manuals and procedures, and implemented a range of other measures targeted at improving safety in its low‑level survey operations.
The investigation also identified that, while not established as contributory to the accident, the Civil Aviation Safety Authority’s regulatory oversight of the operator had not considered the operator’s primary activity of low‑level survey flights, or the processes and procedures designed to reduce the risks associated with that activity.
On 25 June 2025, the flight crew of a Jetstar Airways Airbus A321-251, VH-OYF, were conducting a scheduled passenger transport flight, JQ38, from Denpasar International Airport, Bali, Indonesia, to Sydney, New South Wales. The first officer was the pilot flying and the captain was the pilot monitoring.
During the landing at Sydney Airport, the aircraft floated for a prolonged period along the runway, was subject to a right crosswind and drifted left of the runway centreline. The captain responded by commanding a go-round which the first officer executed.
The crew proceeded to continue with the published missed approach procedure and subsequently landed without further incident.
What the ATSB found
The ATSB found that after the first officer initiated the flare manoeuvre, their control inputs resulted in a lateral deviation from the runway centreline when the aircraft floated for a prolonged period in crosswind conditions.
After the captain commanded a go-around, they inadvertently manipulated their sidestick control, which resulted in a brief period where simultaneous control inputs occurred. The crew were alerted by a ‘dual input’ generated voice message and the captain took control. There was a moment of preoccupation which resulted in the first stage of flap being retracted out of sequence, however, there were no associated flight envelope exceedances or negative effects on aircraft performance.
Safety message
Sound go-around decision-making is an effective defence against the hazards associated with low-level manoeuvring during the landing phase of flight, such as lateral runway excursions. If adequate safety margins cannot be maintained during an approach and landing, the correct and expected response is to go around.
Being go-around minded improves crew readiness and supports timely, coordinated actions during a period of high workload. This should involve crew members reviewing potential go‑around scenarios, procedures and responses prior to conducting an approach.
When flight crews are faced with the unexpected need to execute a go-around even at the final stages of landing, effective crew resource management, with clear communication between flight crew, is essential. This promotes effective teamwork when responding to disruptions and increased workload under stress, ensuring that the aircraft remains on a safe flight path and is correctly configured for the relevant phase of flight.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the evening of 25 June 2025, a Jetstar Airways Pty Limited Airbus A321-251 registered VH‑OYF was operating on a schedule passenger transport Jetstar flight, JQ38, from Denpasar International Airport, Bali, Indonesia, to Sydney, New South Wales. The flight was scheduled to arrive at Sydney Airport the following morning at 0630 AEST.[1] The operating crew included the captain, first officer, 6 cabin crew and 234 passengers. For the flight to Sydney, the first officer was the pilot flying (PF) and the captain was the pilot monitoring (PM).[2]
After departing Denpasar, the aircraft climbed to flight level (FL) 330[3] and later descended to FL310 after reaching Australian airspace due to turbulence en route. Due to the turbulence en route, the captain elected not to take any controlled rest on the nearly 6‑hour flight, while the first officer stated they would not usually take controlled rest in flight.
Prior to descent, the flight crew briefed for the arrival at Sydney, recalling that the turbulent conditions and the crosswind for the approach and landing were the main considerations.
At 0554, the flight crew commenced their descent to the west-south-west of Sydney Airport and was cleared for the approach for runway 16R[4] which was conducted in day visual meteorological conditions[5] using the autopilot. The flight crew recalled there was a 30 kt crosswind down to about 500 ft above mean sea level (AMSL) and the approach up to that point was ‘pretty normal.’ Air traffic control (ATC) advised the crew to expect an 8 kt right crosswind for landing and the first officer chose to land in the flap 3 configuration,[6] which was consistent with guidance for landing in ‘rough’ conditions. (The first officer was procedurally restricted to a maximum crosswind landing component of 20 kt).
The aircraft reached 500 ft at 0621:14 and the captain called ‘stable’ (see Stabilised approach criteria). The first officer disengaged the autopilot 5 seconds later as the aircraft approached 400 ft and recalled encountering turbulence which placed the aircraft ‘a little higher’ on the approach. At 0621:45 at 90 ft, the first officer pitched forward, which they observed resulted in a 900 ft per minute rate of descent.
At 0621:51, the first officer initiated the flare at 50 ft and reduced the thrust levers to idle at around the final approach speed (VAPP)[7] of 150 kt, which included a wind correction of 5 kt. At this point the first officer recalled they ‘over flared’. The captain also observed that the first officer applied the flare technique that was consistent with the technique for landing in the flap full configuration. The aircraft subsequently floated for a prolonged period along the runway after the first officer’s flare manoeuvre.
During the prolonged float, the aircraft was subjected to the crosswind conditions for a greater length of time. After observing the centreline deviation, the captain commanded a go-around approximately 600 m past the runway threshold, just prior to touchdown. The captain recalled they were ‘startled by the need to go around’ as the approach seemed ‘benign’ aside from the crosswind. They also reported a sudden stress response at this time as they had to rapidly transition from landing to commencing the go-around.
In response to the captain’s command, the first officer set take-off/go-around thrust at 0621:59 (Figure 1), which initiated the published missed approach procedure for the 16R GBAS landing system (GLS)[8] approach in the aircraft flight management system. The first officer also referenced their primary flight display (PFD) to command a target pitch attitude of 15° nose up.
At this point, the captain recalled they instinctively applied control inputs via their sidestick while the aircraft was just above the runway, and the crew were alerted to this by the aircraft’s ‘dual input’ voice message (see Sidestick priority logic).
The captain then engaged their sidestick pushbutton, and the first officer recalled hearing the ‘priority left’ voice message and the captain announce, ‘I have control.’ The captain subsequently took control of the thrust levers and the first officer relinquished control and became PM after the aircraft achieved a positive rate of climb. It was the role of the PM to retract the flap ‘one step’ at this point (see Go-around procedure).
Figure 1: Overview of go-around
Source: Google Earth, annotated by the ATSB
The captain announced the active flight modes on their PFD, which prompted the first officer to call ‘positive climb.’ The captain subsequently instructed the first officer to retract the landing gear, which was accomplished 42 ft above the runway at 0622:20.
At this time, the captain looked up to the flight control unit located on the cockpit glareshield to engage the autopilot. After this was actioned, they looked back to their PFD and was ‘startled’ when they noticed that the aircraft suddenly banked right and responded by disengaging the autopilot at 0622:22. They subsequently realised that the aircraft flight director was providing commands for the published missed approach procedure and subsequently re-engaged the autopilot at 0622:29.
The captain then requested flap 1, but the first officer noticed they were still configured with Flap 3 and retracted the flap by one step and announced, ‘flap 2.’ This occurred at 0622:32 when the airspeed reached 174 kt, which was below the maximum flap 3 speed of 195 kt.
They continued to follow the missed approach procedure, and the first officer advised ATC they were going around. The crew were given instructions to track for a right downwind for runway 16R at 4,000 ft. The captain recalled conducting a welfare check on the first officer, briefed the cabin manager via the interphone and made an announcement to the passengers through the public address system.
The captain elected to remain as PF for the remainder of the flight, with the first officer acting as PM. The crew then conducted a second GLS approach for runway 16R, landing at 0638 without further incident.
Context
Flight crew information
The captain held an Air Transport Pilot Licence (Aeroplane), class 1 aviation medical certificate, and had accrued 5,921 hours total flying time, 1,480 of which were in the Airbus A320 and A321 aircraft types.
The first officer held a Commercial Pilot Licence (Aeroplane), class 1 aviation medical certificate, and had 2,212 hours total flying time, 551 of which were on the Airbus A320 and A321 aircraft types.
Fatigue
The captain reported that they felt 'moderately tired' during the go-around, likely due to the back-of-the clock[9] flight, which departed Denpasar at 0057 local time in Sydney. They also stated there was limited opportunity for controlled rest during the flight and their nap prior to the flight was disrupted due to noise at the hotel. The first officer reported feeling 'ok, somewhat fresh.’
The flight crew also reported they had an adequate rest opportunity the evening prior to the flight and obtained around 6 hours sleep in the previous 24 hours and around 13–14 hours in the previous 48 hours. Their sleep during the rest opportunity was reported to be good quality and the conditions at the hotel where they spent the night were suitable and therefore conducive to obtaining restful sleep. Biomathematical modelling[10] of the flight crew’s roster for the 2 weeks leading up to the flight indicated a low likelihood of fatigue.
The ATSB considered that fatigue was unlikely to have affected the flight crew’s performance at the time of the occurrence.
Aircraft information
General
The Airbus A321-251NX is a modern, fly-by-wire aircraft, powered by 2 CFM International LEAP-1A32 turbofan engines and had seating for 232 passengers in a single-class layout.
All the flight controls are electronically actuated with the pilots using sidesticks to fly the aircraft in pitch and roll during manual flight. The 2 sidestick controllers are not coupled mechanically, and they send separate sets of signals to the flight control computers.
Sidestick priority logic
Jetstar Airways A320-A321 Flight crew operating manual (FCOM) contains the following description of the aircraft sidestick priority logic:
At all times, only one flight crewmember should fly the aircraft. However, if both flight crewmembers use their sidesticks simultaneously, their orders are algebraically added.
The flight control laws limit the combined order to the equivalent of the full deflection of one sidestick.
In this case the two green SIDE STICK PRIORITY lights on the glareshield come on and "DUAL INPUT" voice message is activated.
A flight crewmember can deactivate the other sidestick and take full control, by pressing and keeping pressed the sidestick pb (Figure 2).
A “PRIORITY LEFT” or “PRIORITY RIGHT” audio voice message is given each time priority is taken.
Figure 2: Airbus A320/A321 captain's side sidestick and sidestick pushbutton
Source: Operator, annotated by the ATSB
Post-flight maintenance
The operator reported that there were no corrective maintenance actions that were required to be carried out in relation to the occurrence. The aircraft subsequently operated a scheduled passenger service the following day.
Meteorological information
The pre‑flight briefing package provided to the flight crew from the operator’s flight dispatcher included the aerodrome forecast[11] for Sydney Airport. The forecasted weather conditions for the scheduled time of arrival 0630 local time on 26 June indicated:
wind direction of 240° at 15 kt with gusts up to 25 kt
One-minute weather data for Sydney Airport from the Bureau of Meteorology indicated a wind direction of 255° at 17 kt with gusts up 20 kt at the time of the occurrence.
Airport information
Runway 16R at Sydney Airport is oriented on a magnetic heading of 155° and has a declared length of 3,962 metres with a width of 45 metres. A precision approach path indicator system is installed and set to 3° with a threshold crossing height of 64 ft.
For daytime operations, the runway centreline, aiming point and touchdown zone markings provide visual references to assist pilots with approach and landing (Figure 3).
Figure 3: Sydney Airport runway 16R markings
Source: Google Earth, annotated by the ATSB
Recorded information
The aircraft’s quick access recorder data which captured the incident approach indicated that, as the aircraft descended below 1,000 ft, it maintained an appropriate speed and flightpath with no sustained exceedances of the stable approach criteria throughout the approach.
At 0621:59, the recorded data captured the captain’s control inputs commencing concurrently with the initiation of the go-around, while the first officer was actively manipulating their sidestick control. Simultaneous control inputs lasted for a duration of 6 seconds (Figure 4), while the aircraft’s pitch attitude remained below the aircraft’s pitch limit of 11.5° until the aircraft had climbed through about 50 ft.
The recorded data further indicated that the wind direction and speed varied following the flare manoeuvre, however the crosswind component remained well below the first officer’s operational limitation. The wind direction and speed was 315° at 13 kt with a crosswind component of 5 kt when the go-around was initiated.
Figure 4: Graphical representation of the recorded quick access data
Source: Quick access recorder from VH-OYF, annotated by the ATSB
Following the initiation of the go-around, the landing gear was retracted at 06:22:20 and 12 seconds later, the flap was retracted to the flap 2 configuration[14] at 174 kt.
Operational information
Stabilised approach criteria
Jetstar Airways A320-A321 Flight crew operating manual (FCOM) defined a stabilised approach criteria as being established on the correct lateral and vertical flight path by 1,000 ft height above airport (HAA), configured for landing, and within the stated tolerances with the required checklists completed by 500 ft HAA. The FCOM also stated that if these criteria could not be met, or if the approach became unstable below 1,000 ft HAA, a missed approach was required.
The crew reported the approach was stabilised against these criteria, which was consistent with the available recorded data.
Touchdown zone
The FCOM provided the following operational information regarding the touchdown zone:
The touchdown zone commences at 300 m (1000 ft) beyond the threshold and will not normally extend further than 600 m (2000 ft) beyond the threshold.
It is a requirement that the touchdown is planned to occur within the touchdown zone. Should it become apparent that the aircraft will touch down further than 600 m (2,000 ft) beyond the threshold, and the PIC believes that the landing is safe to continue, the PF must apply maximum reverse thrust and sufficient braking to ensure the aircraft stops within the landing distance available. If the PIC decides that a go-around is required, they will without delay, call “Go-Around”. In all cases this must be completed before the PF initiates reverse thrust.
The captain stated that runway 16R in Sydney was long enough to stop the aircraft on the runway if they had continued with the landing during the occurrence. This would have involved requesting maximum reverse and manual braking as necessary after the aircraft touched down.
The FCOM did not specifically reference runway centreline tracking during a visual approach, however the captain stated that it was their personal expectation that a deviation from the runway centreline would lead them to calling for a go-around.
Transfer of control
The operator described procedures for transfer of control within the FCOM as follows:
The pilot relinquishing control of the aircraft shall say “You have control”. The pilot assuming control shall ensure that they have clear and unobstructed access to the flight controls and, when ready, say “I have control”. Only then is the pilot relinquishing control permitted to remove their hands and feet from the flight controls.
In critical phases of flight the PIC must be alert and positioned such that they can assume immediate control of the aircraft.
Following the occurrence, the captain stated the preferable method to conduct a go‑around at low level would have been to announce ‘I have control’ and initiate the go‑around themselves. They stated that their primary consideration when conducting a go‑around at low level was to avoid the risk of tail strike.
Go-around procedure
The FCOM defined the go-around procedure for the A320/A321, which specified the task sequence, memory-based crew actions and applicable guidance relating to techniques and navigation (Figure 5).
Following the occurrence, the captain stated that although they could have taken over and landed, they believed that going around was considered the safest option. The first officer also stated, at about that time, that they were in the mindset of preparing to initiate a go-around themselves.
Related occurrences
The following ATSB investigation highlights the importance of pilots maintaining their readiness for a go-around on every approach as it is typically a period of high workload requiring effective crew coordination.
On the morning of 18 May 2018, an Airbus A320 aircraft, registered VH-VQK, was being operated on a regular public transport flight by Jetstar Airways. The flight departed from Sydney for Ballina/Byron Gateway Airport, New South Wales.
The flight crew conducted a go-around on the first approach at Ballina because the aircraft’s flight path did not meet the operator’s stabilised approach criteria. On the second approach, at about 700 ft radio altitude, a master warning was triggered because the landing gear had not been selected DOWN. The flight crew conducted a second go‑around and landed without further incident on the third approach.
The flight crew did not follow the operator’s standard procedures during the first go‑around and subsequent visual circuit at 1,500 ft. In particular, the flaps remained at flaps 3 rather than flaps 1 during the visual circuit. This created a series of distractions leading to a non‑standard aircraft configuration for a visual circuit. Limited use of available aircraft automation added to the flight crew’s workload.
Safety analysis
During the approach to Sydney airport, with the first officer acting as the pilot flying (PF), the flight crew reported experiencing a crosswind of up to 30 kt until descending through about 500 ft above mean sea level. The crew were advised by air traffic control to expect a right crosswind component of 8 kt for landing, which was within the first officer’s operational crosswind limit of 20 kt. The captain confirmed the approach was ‘stable’ at 500 ft and the first officer continued the approach as PF.
At 50 ft, the first officer initiated the flare manoeuvre prior to landing. They recalled they ‘over flared,’ and the aircraft subsequently floated for an extended period along the runway. During this time, the first officer’s control inputs did not counteract the effect of the crosswind, and the aircraft drifted left of the centreline. After observing the lateral deviation from the centreline, the captain commanded the first officer to conduct a go‑around.
This occurred just prior to the aircraft touching down when the flight crew would normally be focused on landing. The flight crew did not expect a go-around at the time and had to rapidly shift their focus to conducting the missed approach procedure. The captain recalled being ‘startled’ by the unexpected need to discontinue the landing, however they were more likely experiencing ‘surprise.’ Surprise is a cognitive-emotional response to something unexpected, which results from a mismatch between one’s mental expectations and perceptions (Rivera, Talone, Boesser, Jentsch, & Yeh, 2014). But their decision was consistent with the expectation that an approach be discontinued if the aircraft departed from the correct lateral flight path.
The unexpected change from landing to conducting a go-around close to the ground also resulted in the captain experiencing a sudden stress response at this time. When experiencing acute stress, people can respond quickly to a situation, but without conscious decision‑making (Wickens, Helton, Hollands, & Banbury, 2022). After the go‑around was commanded, there was a rapid increase in pitch attitude, engine thrust and airspeed, and in response the captain instinctively and inadvertently manipulated their sidestick while the first officer was flying, resulting in a dual-input alert.
The captain reported they only realised they had manipulated their sidestick when they heard the dual input alert. Their primary consideration during the go-around was to avoid an excessive rotation rate to avoid a tail strike, which did not occur. Additionally, operator procedures directed captains to be alert and be positioned to ‘assume immediate control of the aircraft’ during critical phases of flight.
Following the dual input alert, the captain took full control by engaging their sidestick push‑button and announced ‘I have control’, and the first officer assumed the role of pilot monitoring. A consequence of the control handover during the initial stages of the go‑around was the momentary interruption of sequential crew actions during the go‑around procedures. Interruptions typically disrupt the chain of procedure execution so abruptly that pilots turn immediately to the source of the interruption without noting the point where the procedure was suspended (Loukopoulos, Dismukes, & Barshi, 2009).
Additionally, there was a further disruption (rapid task switching) associated with the first officer and captain exchanging pilot flying and pilot monitoring roles. As a result, some of the procedural items were completed out of sequence (flap 3 retraction occurred after gear retraction).
Pilots are highly vulnerable to errors of omission when they must attend to multiple tasks. If one task becomes demanding, their attention is absorbed by these tasks demands and they can forget to switch their attention to other tasks (Loukopoulos, Dismukes, & Barshi, 2009). Although the flap retraction occurred out of sequence during the go-around, there were no associated flight envelope exceedances or negative effects on aircraft performance.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the control issues during landing and go-around involving Airbus A321, VH-OYF, at Sydney Airport, New South Wales, on 26 June 2025.
Contributing factors
During the landing after crossing the threshold, the first officer’s control inputs resulted in a lateral deviation from the runway centreline during a prolonged float.
After calling for a go-around, the captain inadvertently manipulated their sidestick while the first officer was the pilot flying, which resulted in a simultaneous control input and the go-around procedure being completed out of sequence.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Jetstar Airways Pty Limited
Bureau of Meteorology
the flight crew
recorded data from the quick access recorder from VH-OYF.
References
Loukopoulos, L., Dismukes, R., & Barshi, I. (2009). The perils of multitasking. AeroSafety World, 4(8), 18-23.
Rivera, J., Talone, A., Boesser, C., Jentsch, F., & Yeh, M. (2014). Startle and surprise on the flight deck: Similarities, differences, and prevalence. In Proceedings of the human factors and ergonomics society annual meeting (Vol. 58, No. 1, pp. 1047-1051). Sage CA: Los Angeles, CA: SAGE Publications.
Wickens, C. D., Helton, W. S., Hollands, J. G., & Banbury, S. (2022). Engineering psychology and human performance, 5th edn. Routledge, doi: 10.4324/9781003177616.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
the flight crew
Jetstar Airways Pty Limited
Bureau of Meteorology.
Submissions were received from:
the flight crew
Jetstar Airways Pty Limited.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Local time in Sydney was Australian Eastern Standard Time (AEST), which is Coordinated Universal Time (UTC) +10 hours. Times in this report are AEST unless otherwise noted.
[2]Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 330 equates to 33,000 ft.
[4]Runway numbering: the number represents the magnetic heading closest to the runway (runway 16 at Sydney Airport is oriented 155° magnetic) and R indicates the right most of 2 parallel runways.
[5]Visual meteorological conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[6]Flap 3 on the A321-251 is 21° of flap and 22° of slat extension.
[7]Final approach speed (VAPP): the VAPP is the target airspeed for the aircraft when crossing the runway threshold with the aircraft configured for landing. VAPP is equal to the lowest selectable speed with the addition of wind correction. The wind correction is limited to a minimum of 5 kt and a maximum of 15 kt.
[8]GBAS landing system (GLS): a GLS consists of a GBAS ground station located on or in the vicinity of one or more aerodromes and an aircraft subsystem. The GBAS provides data and corrections for the GNSS ranging signals over a digital VHF data broadcast to the aircraft subsystem. The aircraft subsystem translates the position signal into flight guidance similar to that provided for an ILS.
[9]Back of the clock: Work schedules that involve extended periods of night-work between midnight and dawn.
[10]A biomathematical model of fatigue predicts the effect of different patterns of work on measures such as subjective fatigue, sleep, or the effectiveness of performing work, using mathematical algorithms. Each model uses different types of inputs and assumptions and produces different types of outputs, each having limitations. The ATSB used the biomathematical modelling software SAFTE-FAST and FAID Quantum for the analysis.
[11]Aerodrome forecast (TAF): a TAF is a coded statement of meteorological conditions expected at an aerodrome and within a radius of 5 nautical miles of the aerodrome reference point.
[12]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[13]Moderate turbulence: changes to accelerometer readings of between 0.5 g and 1.0 g at the aircraft’s centre of gravity. Moderate change to aircraft attitude and/or altitude may occur but aircraft remains under positive control. Usually small changes in airspeed. Difficulty in walking. Lose objects move about.
[14]Flap 2 on the A321-251 is 14° of flap and 22° of slat extension.
Occurrence summary
Investigation number
AO-2025-036
Occurrence date
26/06/2025
Location
Sydney Airport
State
New South Wales
Report release date
27/01/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Control issues, Missed approach, Warning devices
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Airbus
Model
A321-251NX
Registration
VH-OYF
Serial number
11529
Aircraft operator
Jetstar Airways Pty Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes