Approach to incorrect runway involving Aero Commander 500-U, VH-LRI, Moorabbin Airport, Victoria, on 9 August 2025
Final report
Report release date: 28/11/2025
Investigation summary
What happened
On the afternoon of 9 August 2025, an Aero Commander 500-U, registered VH-LRI, and operated by 360° Aviation Group, was being repositioned from Bacchus Marsh Airport to Moorabbin Airport, Victoria, with a single pilot on board. At the same time, a Cessna 172, registered VH-EUE and operated by CAE Melbourne Flight Training, was being used to conduct circuit training at Moorabbin Airport with a flight instructor and a student pilot on board.
During the approach to Moorabbin, the Aero Commander crossed through the centreline of the intended runway 17R and instead aligned with the parallel runway 17L, behind the Cessna 172. Separation between the aircraft reduced as they proceeded on final before air traffic control (ATC) observed the aircraft in close proximity. ATC then instructed the Aero Commander to climb and the Cessna 172 to continue landing and the aircraft were deconflicted. The Aero Commander subsequently conducted a visual circuit and landed without further incident, and the Cessna 172 continued circuit training.
What the ATSB found
The ATSB found that the pilot of the Aero Commander configured their GPS navigation unit to provide guidance to the runway. However, due to the waypoint and track selected, the guidance provided was significantly offset from the runway’s centreline. As a result, the pilot inadvertently intercepted the final approach path of the parallel runway behind the Cessna 172.
It was also found that after identifying that the aircraft were in close proximity, air traffic control quickly issued instructions to both pilots, deconflicting the aircraft and directing them away from other traffic.
What has been done as a result
360° Aviation Group disseminated information to flight crew about the potential for misleading indications when using the aerodrome reference point for navigation at Moorabbin Airport. In addition, CAE Melbourne Flight Training advised that it was incorporating ADS-B in/out capability into the Cessna 172s in its fleet that were not currently equipped.
Safety message
Pilots are reminded of the importance of comprehensive preparation when planning a flight to an unfamiliar aerodrome. This is particularly the case when flying into a Metropolitan Class D airport due to their typical high traffic volumes, complex runway layouts, and use of local landmarks and procedures. When arriving during tower hours, advising air traffic control that you are unfamiliar with the airport alerts them to the fact that you may require additional guidance. They can also then direct extra attention to monitor your progress if their workload allows. It is also important to ask for clarification if an instruction from air traffic control is not understood, or if there is confusion or uncertainty about how the flight is progressing.
Airservices Australia publishes a number of resources for pilots operating into Class D airports. General information regarding operating in Class D airspace can be found in Operating in Class D airspace safety net and pilot safety information specific to each airport is available on the Airservices Industry Hub. The Civil Aviation Safety Authority (CASA) also publishes the Stay OnTrack series of booklets designed to help pilots flying under visual flight rules (VFR) in busy metropolitan areas.
The investigation
The occurrence
On the afternoon of 9 August 2025 an Aero Commander 500-U, registered VH-LRI and operated by 360° Aviation Group, was being repositioned from Bacchus Marsh Airport to Moorabbin Airport, Victoria, with a single pilot on board. At the same time, a Cessna 172, registered VH-EUE and operated by CAE Melbourne Flight Training, was being used to conduct circuit training[1] at Moorabbin Airport with a flight instructor and a student pilot on board (Figure 1). Both aircraft were operating under the visual flight rules (VFR).[2]
Figure 1: Aircraft flight paths

Source: Flight data overlaid on Google Earth, annotated by the ATSB
Weather conditions at the airport included clear skies, greater than 10 km visibility and a light southerly wind. At 1321, the pilot of VH-LRI contacted Moorabbin Airport air traffic control (ATC) as the aircraft approached Brighton to request a clearance to enter the control zone. The western circuit controller cleared the aircraft to enter the control zone and continue toward the airport, instructing the pilot to join an oblique base for runway 17R.[3] The controller also advised the pilot that they were ‘number 1’, indicating that there was no traffic ahead that was approaching the same runway.
The pilot of VH-LRI recalled that at this time they configured their GPS navigation unit to assist them in orienting with the runway. To achieve this, they set the destination waypoint as ‘YMMB’, the airport code for Moorabbin Airport (see the section titled Aerodrome reference point), and an inbound track of 170° corresponding to the approximate heading of runway 17R. This inbound track was 770 m offset to the east from the runway 17R extended centreline (Figure 2). They also carried an electronic flight bag (EFB) displaying navigation charts and showing the orientation of the runways.
Figure 2: Aircraft flight path relative to inbound track and runway centrelines
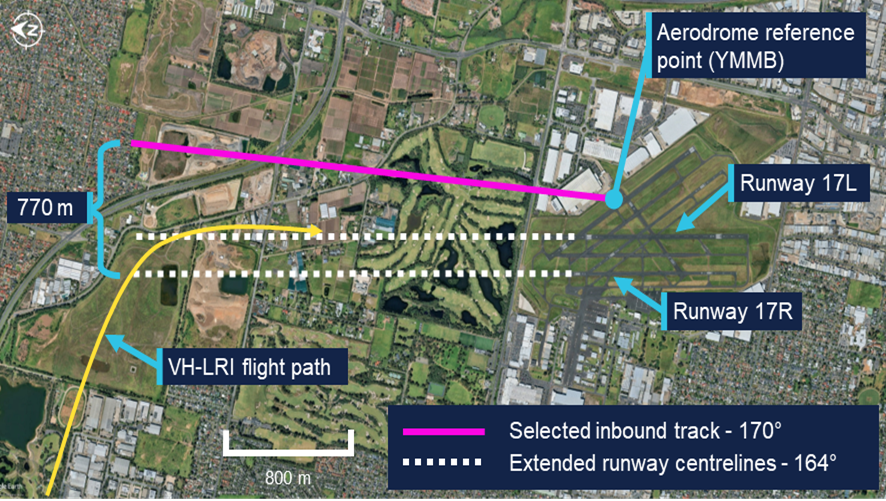
Source: Google Earth, annotated by the ATSB
At 1325, the western controller observed VH-LRI on the base leg of runway 17R and cleared the aircraft to land. By this time VH-EUE was on final approach to runway 17L. The pilot of VH-LRI recalled using a combination of visual references, and GPS navigation indications, to inform when they were approaching the centreline of runway 17R and should commence a turn to intercept the final approach course. They also recalled that, while expecting to be aligning with the western runway closest to the coast, they observed that their GPS unit was aligning them to the left of where they expected.
Approximately 12 seconds later, VH-LRI crossed the final approach course of runway 17R and turned to join final approach for runway 17L (Figure 3), aligning with the runway at 1325:26. The pilot of VH-LRI recalled that, at around that time they observed VH-EUE in front of them. Recognising that they had been advised not to expect preceding traffic they realised that they were not aligned with the correct runway.
Figure 3: VH-LRI and VH-EUE flight paths on final approach
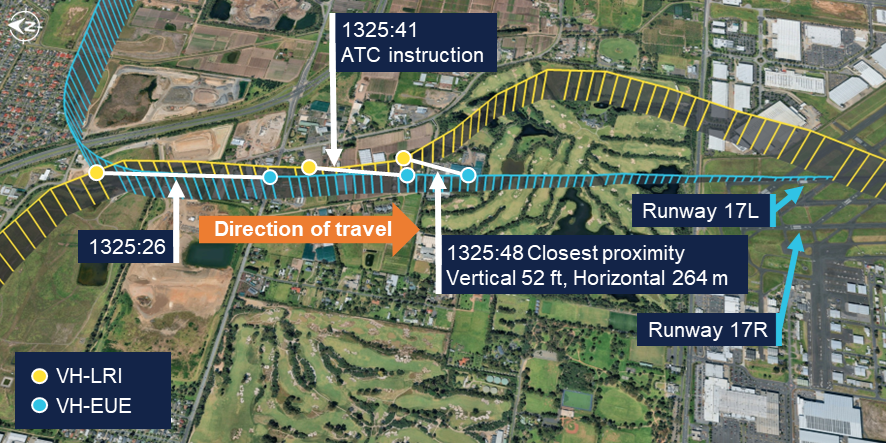
The ATSB has connected the data points from each flight at the same time to show the relative positions of the aircraft at the corresponding time. Source: Flight data overlaid on Google Earth, annotated by the ATSB
The western circuit controller reported that when looking toward the final approach area of the runways they observed that VH-LRI and VH-EUE were closer to each other than expected. They alerted the eastern circuit controller to the situation and, at 1325:41, asked the pilot of VH-LRI over the radio to confirm they were on final for runway 17R. Observing the aircraft commence a left turn, they immediately asked the pilot why they were doing so, to which the pilot responded that they were orbiting. The controller then advised the pilot that they could not orbit and instructed them to join upwind for runway 17R and climb to 1,500 ft. They further advised the pilot that there was traffic low, on short final for the other runway and to make sure they joined upwind for runway 17R. The pilot read back this instruction, discontinued the orbit and commenced a climb back toward the airport.
At the same time as the western circuit controller contacted the pilot of VH-LRI, the eastern circuit controller contacted the occupants of VH-EUE to advise that there was an aircraft in their vicinity approaching the incorrect runway. In response, the instructor of VH-EUE advised that they would go around. The controller instructed them not to go around, and instead to continue their approach, clearing them for a touch-and-go landing. The instructor read back the instruction and continued toward the runway.
During the radio exchanges, at 1325:48, the proximity between the aircraft reduced to 52 ft vertically and 264 m horizontally. While the instructor on board VH-EUE did not see VH-LRI until it had passed on their left and had commenced climbing, the pilot of VH-LRI advised that they maintained visual contact with the Cessna throughout the final approach.
Following the deconfliction, VH-LRI climbed to 1,500 ft, conducted a visual circuit for runway 17R and landed without further incident. The instructor and student on board VH‑EUE completed a touch-and-go landing and continued circuit training. The instructor reported they were not aware of the proximity of VH-LRI until reviewing flight data after the flight. They also reported that the student pilot was solely focused on operating the aircraft at the time and was not aware that any incident had occurred.
Context
Pilots
The pilot of VH-LRI held a commercial pilot licence (aeroplane) issued in 2022 and a class 1 aviation medical certificate. They had accumulated 2,058 flight hours, of which 32 hours were operating the Aero Commander 500. In the previous 90 days, the pilot had accumulated 110 flight hours. They completed an instrument proficiency check in October 2024.
The pilot advised that they had flown into Moorabbin as pilot in command once previously, approximately 9 months before. They reported that they had talked to their chief pilot and another pilot at the operator familiar with Moorabbin Airport for advice prior to the flight. They further reported that they reviewed the En Route Supplement Australia (ERSA) and satellite imagery to familiarise themselves with the runway layout and procedures at Moorabbin and considered themselves sufficiently prepared.
The flight instructor on board VH-EUE held a commercial pilot licence (aeroplane) and a class 1 aviation medical certificate. They had accumulated 1,818 flight hours, of which 1,124 hours were operating the Cessna 172. In the previous 90 days, the pilot had accumulated 82 hours. The student pilot had accumulated 18 hours, all in the Cessna 172 and all within the last 90 days.
Aircraft
Aero Commander VH-LRI
VH-LRI was an Aero Commander 500-U aircraft fitted with 2 Lycoming IO-540-E1A5 engines, each driving a Hartzell constant speed propellor. The aircraft was manufactured in 1967 and first registered in Australia in 1991. It was subsequently registered with the operator in August 2025.
At the time of the occurrence, the aircraft had accumulated 5,543 hours total time in service. The last periodic inspection was conducted in May 2025, and the maintenance release showed no outstanding items. The aircraft was equipped with both ADS-B out and in capability, including a traffic awareness and alerting system. The pilot recalled hearing the aural traffic alert activate prior to Brighton due to traffic in the area. However, they did not recall hearing any alert on approach to the airport.
Cessna 172S VH-EUE
VH-EUE was a Cessna 172S fitted with a Lycoming IO-360-L2A engine powering a McCauley propellor. The aircraft was manufactured and registered with the operator in 2006. The ATSB did not request any information on the aircraft’s maintenance history. The operator advised that the aircraft was not equipped with ADS-B out or in capability, however recorded flight data was downloaded from the aircraft’s avionics.
Moorabbin Airport
Runway layout
Moorabbin Airport has numerous runways (Figure 4), with the preferred runways being the north-south parallel runways of 17/35. Two additional parallel runways 13/31 were also available, while the shortest of the runways, runway 04/22, was not available unless operationally required. At the time of the occurrence, runways 17L and 17R were nominated as the duty runways.
Figure 4: Moorabbin Airport runway layout
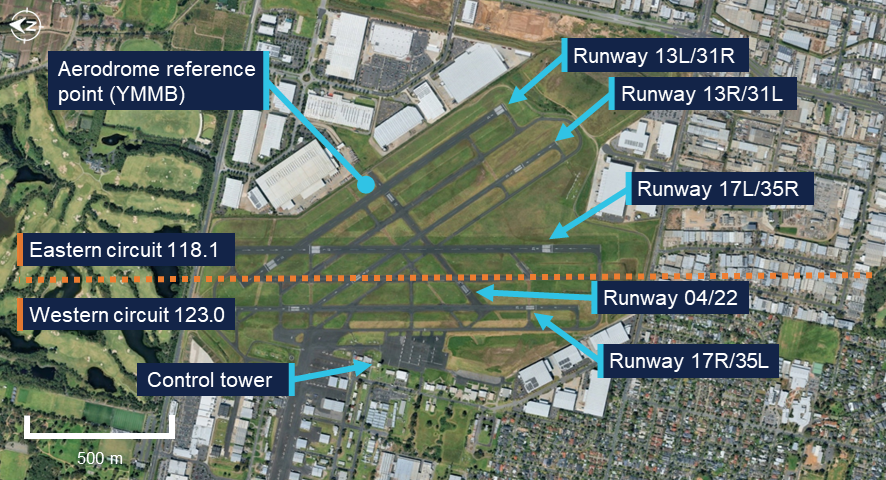
Source: Google Earth, annotated by the ATSB
The En Route Supplement Australia (ERSA) (Figure 5) contained information on the physical characteristics of each runway, including that the magnetic heading was 164° for runways 17L and 17R. The runway designations represented the magnetic heading of the runway to the nearest 10°. However, the magnetic variation at Moorabbin Airport had increased approximately 1° over the previous 40 years and therefore the magnetic heading of the runways had drifted slightly since they were originally named.
Figure 5: En Route Supplement Australia (ERSA) extract
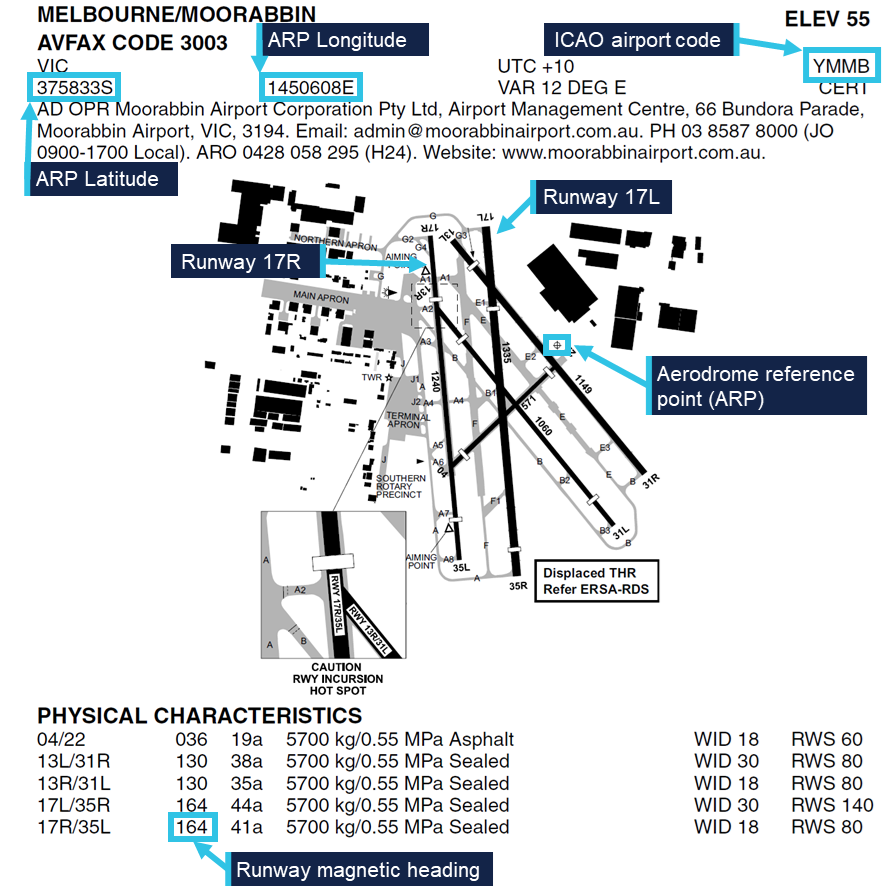
Source: Airservices Australia, annotated by the ATSB
Aerodrome reference point
The airport’s aerodrome reference point (ARP) was the designated geographical location of the airport, and the location associated with the International Civil Aviation Organisation (ICAO) airport code YMMB in aircraft navigation databases. The ARP for Moorabbin Airport was located on the eastern side of the airport, near the runway 22 threshold and 440 m away from the runway 17R centreline. This location was published in the ERSA as a latitude and longitude and shown graphically on the aerodrome plan.
Air traffic control
During tower hours, Moorabbin Airport operated as a Class D aerodrome. Pilots were required to establish and maintain 2-way communications with the tower and receive a clearance prior to entering the control zone. When operating in the airspace, aircraft operating under the visual flight rules (VFR) were given traffic information with respect to all other flights, but did not receive a separation service. Pilots were responsible for sighting and maintaining separation from other aircraft. If a pilot was unable to see, or lost sight of, other aircraft notified as traffic they were required to immediately advise ATC.
When operating parallel runways, Moorabbin Airport operated simultaneous independent circuits with each circuit utilising a different radio frequency. The eastern circuit, on runway 17L, was predominantly for circuit training and used the radio frequency 118.1 for communications between flight crew operating in the circuit and ATC. The western circuit, on runway 17R, was typically used for aircraft arriving from and departing to the west and used the radio frequency 123.0. Pilots operating in one circuit were not expected to monitor the radio frequency of the other circuit and the Aeronautical Information Package (AIP) stated that:
Operations will be regulated independently in each circuit, with an ATC clearance required to enter the opposite circuit or airspace.
At the time of the occurrence, 3 controllers were on duty in the control tower. One controller was controlling the eastern circuit while another was controlling the western circuit. A third controller was responsible for ground movements on a separate frequency. The controllers communicated with pilots in their circuit on a headset. They also had an awareness of activity in the other circuit via speakers in the tower broadcasting each frequency. In addition, the controllers were positioned physically close to each other and could communicate directly when required.
The tower was equipped with a tower situational awareness display (TSAD) which provided radar information that could be used to assist when providing control services. The western circuit controller advised that information provided by this system was limited and therefore it was not typically utilised for monitoring aircraft within the circuit area. Instead, each aircraft was monitored visually, using binoculars to assist. They further advised that at the time of the occurrence the airport was busy with multiple aircraft arriving and departing, in addition to aircraft transiting outside of the control zone to the west. There were also multiple aircraft established in the eastern circuit in addition to VH-EUE. As such, the controllers’ workload required them to direct attention to each aircraft in turn.
Related occurrences
The ATSB database contained 73 instances of aircraft approaching or landing on the incorrect runway at Moorabbin between 2015 and July 2025. During the course of this investigation the ATSB was advised of a similar occurrence that occurred on 13 August 2025 involving the same aircraft, but with a different pilot and without confliction with other traffic. The pilot of this flight advised that they had similarly configured their GPS navigation unit to provide guidance to the aerodrome reference point without realising its distance from the runway. In addition, it was reported to the ATSB that due to the high number of training flights at Moorabbin Airport, aircraft inadvertently entering into the other circuit occurred relatively regularly and was something controllers were alert for.
Safety analysis
Planning the flight to Moorabbin Airport, the pilot of VH-LRI identified that having flown there only once previously, the flight required additional planning and preparation. This included:
- consulting pilots familiar with Moorabbin Airport
- reviewing the information in the En Route Supplement Australia (ERSA)
- studying satellite imagery of the airport.
Additionally, in flight they utilised their electronic flight bag (EFB) to display the runway configuration and setup their GPS navigation to provide guidance. All of these measures were intended to improve the pilot’s situation awareness when approaching an unfamiliar aerodrome.
However, when reviewing the ERSA, the pilot did not identify that the aerodrome reference point (ARP) was located distant from the runway 17R centreline. Additionally, they did not identify that the magnetic heading of the runway differed slightly from that implied by its designation. Consequently, the inbound track configured for guidance was offset and deviated away from the runway centreline. At the point that the aircraft crossed the runway 17R centreline, the navigation unit would have indicated that the aircraft was still significantly to the right of the configured inbound track. Therefore, it is likely that the navigation indications contributed to the pilot flying through the runway centreline of 17R and joining final for 17L behind VH-EUE. VH-LRI was not advised of VH-EUE as traffic by air traffic control (ATC) as the other aircraft was operating in the eastern circuit, which required an additional clearance to enter. In addition, VH-EUE was not equipped with ADS-B out and therefore would not have been detected by a traffic awareness system.
VH-LRI was being periodically visually monitored by the western circuit controller as it approached the airport. During this time, both the eastern and western controllers’ attention was also directed to other traffic. Therefore, both controllers were likely looking away from the final approach path when VH-LRI crossed the runway 17R centreline and entered the eastern circuit. The deviation was not detected until visual contact was re‑established by the western circuit controller, by which time the aircraft was already on final approach for runway 17L.
While the distance between the aircraft reduced as they converged on the same final flightpath, as the pilot of VH-LRI reported that visual contact was maintained, there was likely no significant risk of a collision. However, upon intervention by ATC, the initial instinct of the pilot of VH-LRI was to orbit to the left, while the instructor on board VH‑EUE intended to climb. Initiation of a climb by VH-EUE would have increased the risk of collision between the aircraft, while an orbit would have placed VH-LRI in conflict with other aircraft in the eastern circuit. Therefore, the timely issuing of instructions contrary to the pilots’ intentions deconflicted the aircraft and directed them away from other traffic.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the approach to incorrect runway involving Aero Commander 500-U, VH-LRI, at Moorabbin Airport, Victoria, on 9 August 2025.
Contributing factors
- Due to unfamiliarity with the airport, the pilot of the Aero Commander configured their GPS navigation unit to provide guidance to the runway. However, due to the waypoint and track selected, the guidance was significantly offset from the runway’s centreline, resulting in the pilot inadvertently intercepting the final approach path of the parallel runway in proximity to a Cessna 172.
Other findings
- Identifying that the aircraft were in close proximity, air traffic control quickly issued instructions to both pilots, deconflicting the aircraft and directing them away from other traffic.
Safety actions
Safety action by 360° Aviation Group
360° Aviation Group disseminated information to flight crew about the potential for misleading indications when using the aerodrome reference point for navigation at Moorabbin Airport.
Safety action by CAE Melbourne Flight Training
CAE Melbourne Flight Training advised that it was incorporating ADS-B in/out capability into the Cessna 172s in its fleet that were not currently equipped.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot and operator of the Aero Commander
- the flight instructor and operator of the Cessna
- the air traffic controllers
- recorded data from aircraft avionics
- Airservices Australia
- Bureau of Meteorology.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the pilot and operator of the Aero Commander
- the flight instructor and operator of the Cessna
- the air traffic controllers
- Airservices Australia
- Civil Aviation Safety Authority.
Submissions were received from:
- the operator of the Aero Commander
- the operator of the Cessna
- Airservices Australia
- Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Circuit training: a phase of pilot training focused on take-offs and landings. It involves making approaches to the runway, touching down and then applying power to take off again.
[2] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[3] Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, or R as required for left or right when there are parallel runways.
Occurrence summary
| Investigation number | AO-2025-046 |
|---|---|
| Occurrence date | 09/08/2025 |
| Location | Moorabbin Airport |
| State | Victoria |
| Report release date | 28/11/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Aircraft separation, Depart/app/land wrong runway, Missed approach |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Aero Commander |
|---|---|
| Model | 500-U |
| Registration | VH-LRI |
| Serial number | 1690-22 |
| Aircraft operator | 360 Aircraft Pty Ltd |
| Sector | Piston |
| Operation type | Part 135 Air transport operations - smaller aeroplanes |
| Departure point | Bacchus Marsh (ALA), Victoria |
| Destination | Moorabbin Airport, Victoria |
| Damage | Nil |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 172S |
| Registration | VH-EUE |
| Serial number | 172S10224 |
| Aircraft operator | Oxford Aviation Academy (Australia) Pty Ltd |
| Sector | Piston |
| Operation type | Part 141 Recreational, private and commercial pilot flight training |
| Departure point | Moorabbin Airport, Victoria |
| Destination | Moorabbin Airport, Victoria |
| Damage | Nil |