
Final report
Report release date: 27/01/2026
Investigation summary
What happened
On 25 June 2025, the flight crew of a Jetstar Airways Airbus A321-251, VH-OYF, were conducting a scheduled passenger transport flight, JQ38, from Denpasar International Airport, Bali, Indonesia, to Sydney, New South Wales. The first officer was the pilot flying and the captain was the pilot monitoring.
During the landing at Sydney Airport, the aircraft floated for a prolonged period along the runway, was subject to a right crosswind and drifted left of the runway centreline. The captain responded by commanding a go-round which the first officer executed.
The crew proceeded to continue with the published missed approach procedure and subsequently landed without further incident.
What the ATSB found
The ATSB found that after the first officer initiated the flare manoeuvre, their control inputs resulted in a lateral deviation from the runway centreline when the aircraft floated for a prolonged period in crosswind conditions.
After the captain commanded a go-around, they inadvertently manipulated their sidestick control, which resulted in a brief period where simultaneous control inputs occurred. The crew were alerted by a ‘dual input’ generated voice message and the captain took control. There was a moment of preoccupation which resulted in the first stage of flap being retracted out of sequence, however, there were no associated flight envelope exceedances or negative effects on aircraft performance.
Safety message
Sound go-around decision-making is an effective defence against the hazards associated with low-level manoeuvring during the landing phase of flight, such as lateral runway excursions. If adequate safety margins cannot be maintained during an approach and landing, the correct and expected response is to go around.
Being go-around minded improves crew readiness and supports timely, coordinated actions during a period of high workload. This should involve crew members reviewing potential go‑around scenarios, procedures and responses prior to conducting an approach.
When flight crews are faced with the unexpected need to execute a go-around even at the final stages of landing, effective crew resource management, with clear communication between flight crew, is essential. This promotes effective teamwork when responding to disruptions and increased workload under stress, ensuring that the aircraft remains on a safe flight path and is correctly configured for the relevant phase of flight.
The investigation
The occurrence
On the evening of 25 June 2025, a Jetstar Airways Pty Limited Airbus A321-251 registered VH‑OYF was operating on a schedule passenger transport Jetstar flight, JQ38, from Denpasar International Airport, Bali, Indonesia, to Sydney, New South Wales. The flight was scheduled to arrive at Sydney Airport the following morning at 0630 AEST.[1] The operating crew included the captain, first officer, 6 cabin crew and 234 passengers. For the flight to Sydney, the first officer was the pilot flying (PF) and the captain was the pilot monitoring (PM).[2]
After departing Denpasar, the aircraft climbed to flight level (FL) 330[3] and later descended to FL310 after reaching Australian airspace due to turbulence en route. Due to the turbulence en route, the captain elected not to take any controlled rest on the nearly 6‑hour flight, while the first officer stated they would not usually take controlled rest in flight.
Prior to descent, the flight crew briefed for the arrival at Sydney, recalling that the turbulent conditions and the crosswind for the approach and landing were the main considerations.
At 0554, the flight crew commenced their descent to the west-south-west of Sydney Airport and was cleared for the approach for runway 16R[4] which was conducted in day visual meteorological conditions[5] using the autopilot. The flight crew recalled there was a 30 kt crosswind down to about 500 ft above mean sea level (AMSL) and the approach up to that point was ‘pretty normal.’ Air traffic control (ATC) advised the crew to expect an 8 kt right crosswind for landing and the first officer chose to land in the flap 3 configuration,[6] which was consistent with guidance for landing in ‘rough’ conditions. (The first officer was procedurally restricted to a maximum crosswind landing component of 20 kt).
The aircraft reached 500 ft at 0621:14 and the captain called ‘stable’ (see Stabilised approach criteria). The first officer disengaged the autopilot 5 seconds later as the aircraft approached 400 ft and recalled encountering turbulence which placed the aircraft ‘a little higher’ on the approach. At 0621:45 at 90 ft, the first officer pitched forward, which they observed resulted in a 900 ft per minute rate of descent.
At 0621:51, the first officer initiated the flare at 50 ft and reduced the thrust levers to idle at around the final approach speed (VAPP)[7] of 150 kt, which included a wind correction of 5 kt. At this point the first officer recalled they ‘over flared’. The captain also observed that the first officer applied the flare technique that was consistent with the technique for landing in the flap full configuration. The aircraft subsequently floated for a prolonged period along the runway after the first officer’s flare manoeuvre.
During the prolonged float, the aircraft was subjected to the crosswind conditions for a greater length of time. After observing the centreline deviation, the captain commanded a go-around approximately 600 m past the runway threshold, just prior to touchdown. The captain recalled they were ‘startled by the need to go around’ as the approach seemed ‘benign’ aside from the crosswind. They also reported a sudden stress response at this time as they had to rapidly transition from landing to commencing the go-around.
In response to the captain’s command, the first officer set take-off/go-around thrust at 0621:59 (Figure 1), which initiated the published missed approach procedure for the 16R GBAS landing system (GLS)[8] approach in the aircraft flight management system. The first officer also referenced their primary flight display (PFD) to command a target pitch attitude of 15° nose up.
At this point, the captain recalled they instinctively applied control inputs via their sidestick while the aircraft was just above the runway, and the crew were alerted to this by the aircraft’s ‘dual input’ voice message (see Sidestick priority logic).
The captain then engaged their sidestick pushbutton, and the first officer recalled hearing the ‘priority left’ voice message and the captain announce, ‘I have control.’ The captain subsequently took control of the thrust levers and the first officer relinquished control and became PM after the aircraft achieved a positive rate of climb. It was the role of the PM to retract the flap ‘one step’ at this point (see Go-around procedure).
Figure 1: Overview of go-around
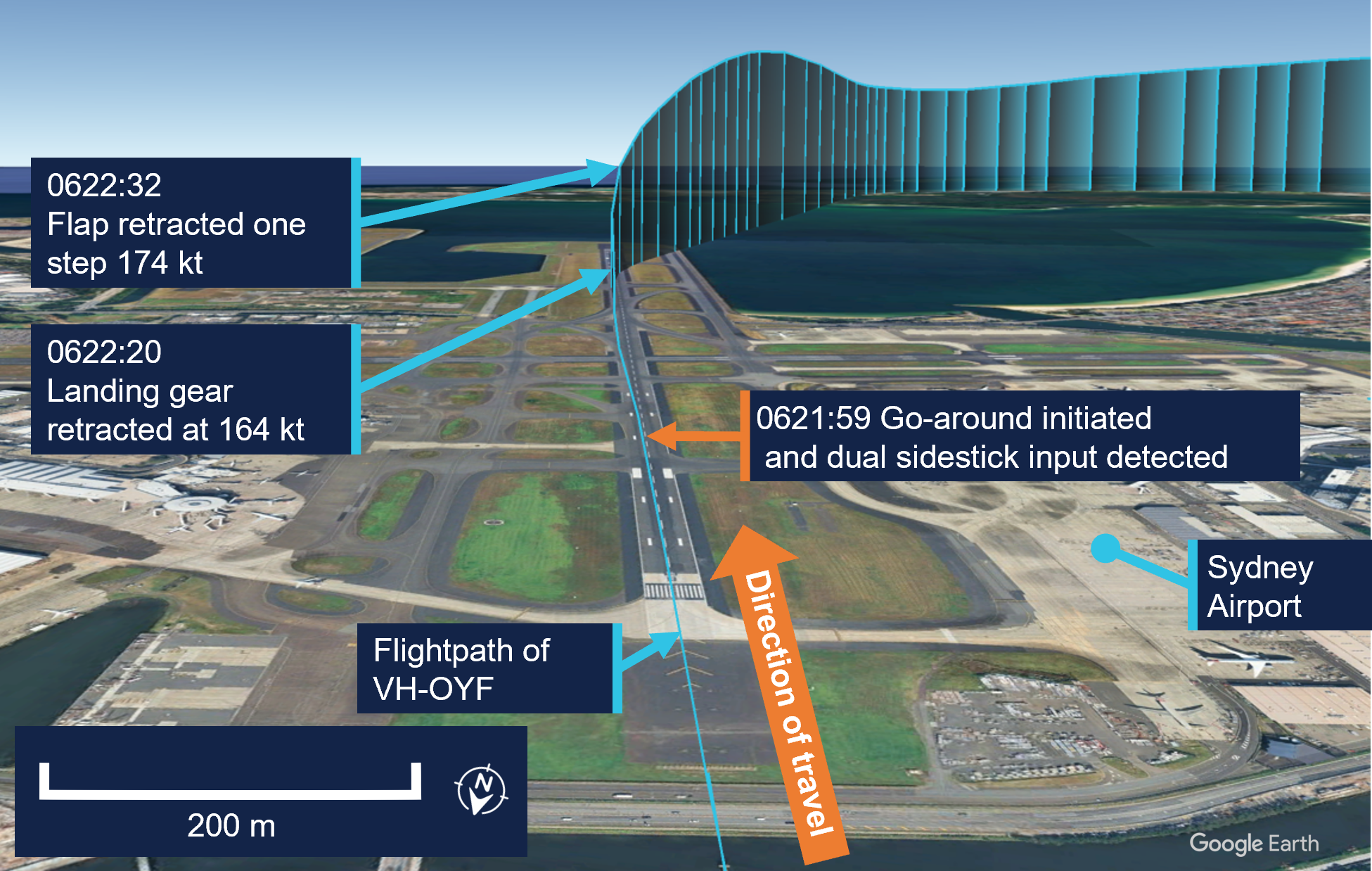
Source: Google Earth, annotated by the ATSB
The captain announced the active flight modes on their PFD, which prompted the first officer to call ‘positive climb.’ The captain subsequently instructed the first officer to retract the landing gear, which was accomplished 42 ft above the runway at 0622:20.
At this time, the captain looked up to the flight control unit located on the cockpit glareshield to engage the autopilot. After this was actioned, they looked back to their PFD and was ‘startled’ when they noticed that the aircraft suddenly banked right and responded by disengaging the autopilot at 0622:22. They subsequently realised that the aircraft flight director was providing commands for the published missed approach procedure and subsequently re-engaged the autopilot at 0622:29.
The captain then requested flap 1, but the first officer noticed they were still configured with Flap 3 and retracted the flap by one step and announced, ‘flap 2.’ This occurred at 0622:32 when the airspeed reached 174 kt, which was below the maximum flap 3 speed of 195 kt.
They continued to follow the missed approach procedure, and the first officer advised ATC they were going around. The crew were given instructions to track for a right downwind for runway 16R at 4,000 ft. The captain recalled conducting a welfare check on the first officer, briefed the cabin manager via the interphone and made an announcement to the passengers through the public address system.
The captain elected to remain as PF for the remainder of the flight, with the first officer acting as PM. The crew then conducted a second GLS approach for runway 16R, landing at 0638 without further incident.
Context
Flight crew information
The captain held an Air Transport Pilot Licence (Aeroplane), class 1 aviation medical certificate, and had accrued 5,921 hours total flying time, 1,480 of which were in the Airbus A320 and A321 aircraft types.
The first officer held a Commercial Pilot Licence (Aeroplane), class 1 aviation medical certificate, and had 2,212 hours total flying time, 551 of which were on the Airbus A320 and A321 aircraft types.
Fatigue
The captain reported that they felt 'moderately tired' during the go-around, likely due to the back-of-the clock[9] flight, which departed Denpasar at 0057 local time in Sydney. They also stated there was limited opportunity for controlled rest during the flight and their nap prior to the flight was disrupted due to noise at the hotel. The first officer reported feeling 'ok, somewhat fresh.’
The flight crew also reported they had an adequate rest opportunity the evening prior to the flight and obtained around 6 hours sleep in the previous 24 hours and around 13–14 hours in the previous 48 hours. Their sleep during the rest opportunity was reported to be good quality and the conditions at the hotel where they spent the night were suitable and therefore conducive to obtaining restful sleep. Biomathematical modelling[10] of the flight crew’s roster for the 2 weeks leading up to the flight indicated a low likelihood of fatigue.
The ATSB considered that fatigue was unlikely to have affected the flight crew’s performance at the time of the occurrence.
Aircraft information
General
The Airbus A321-251NX is a modern, fly-by-wire aircraft, powered by 2 CFM International LEAP-1A32 turbofan engines and had seating for 232 passengers in a single-class layout.
All the flight controls are electronically actuated with the pilots using sidesticks to fly the aircraft in pitch and roll during manual flight. The 2 sidestick controllers are not coupled mechanically, and they send separate sets of signals to the flight control computers.
Sidestick priority logic
Jetstar Airways A320-A321 Flight crew operating manual (FCOM) contains the following description of the aircraft sidestick priority logic:
At all times, only one flight crewmember should fly the aircraft. However, if both flight crewmembers use their sidesticks simultaneously, their orders are algebraically added.
The flight control laws limit the combined order to the equivalent of the full deflection of one sidestick.
In this case the two green SIDE STICK PRIORITY lights on the glareshield come on and "DUAL INPUT" voice message is activated.
A flight crewmember can deactivate the other sidestick and take full control, by pressing and keeping pressed the sidestick pb (Figure 2).
A “PRIORITY LEFT” or “PRIORITY RIGHT” audio voice message is given each time priority is taken.
Figure 2: Airbus A320/A321 captain's side sidestick and sidestick pushbutton
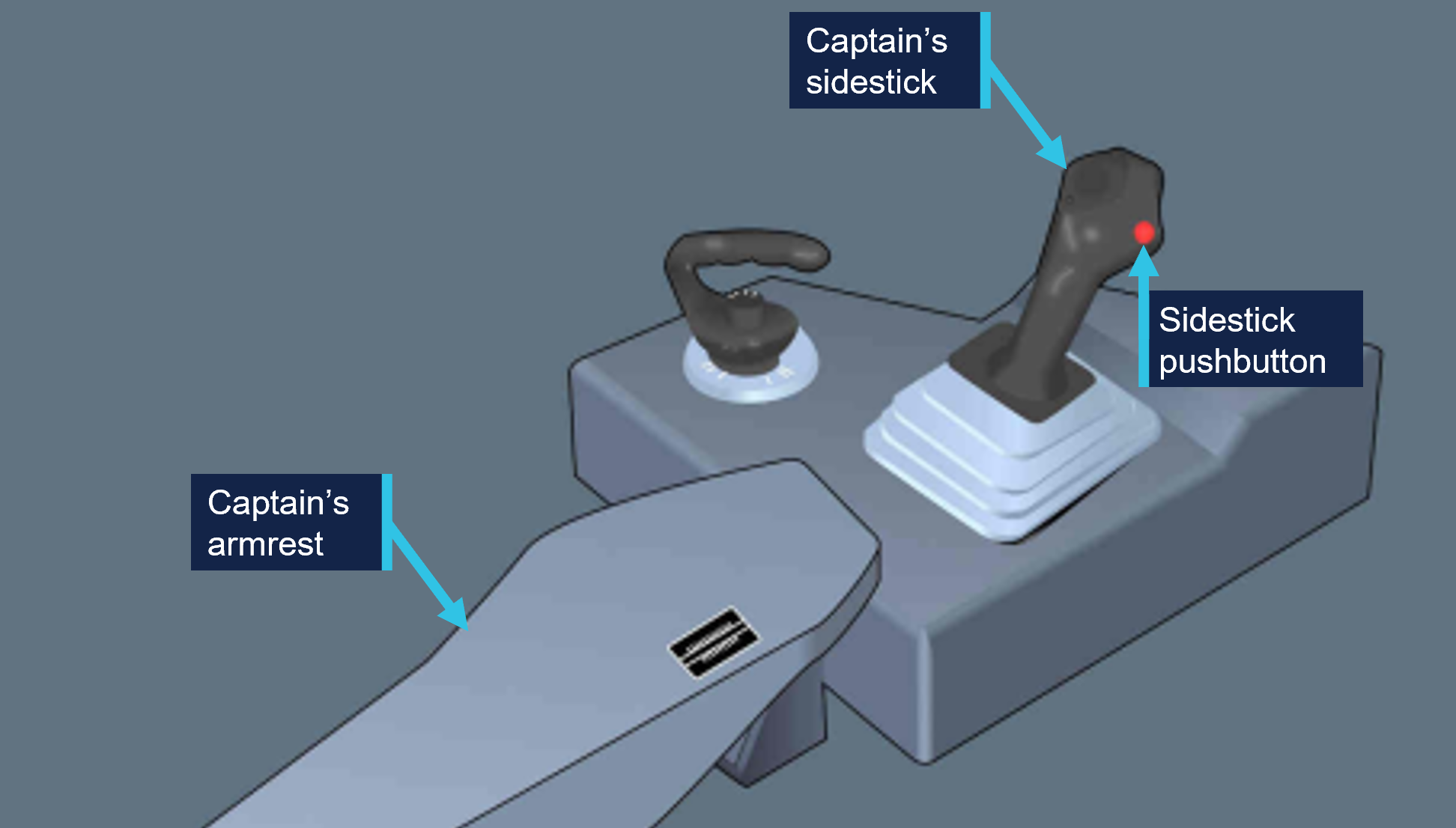
Source: Operator, annotated by the ATSB
Post-flight maintenance
The operator reported that there were no corrective maintenance actions that were required to be carried out in relation to the occurrence. The aircraft subsequently operated a scheduled passenger service the following day.
Meteorological information
The pre‑flight briefing package provided to the flight crew from the operator’s flight dispatcher included the aerodrome forecast[11] for Sydney Airport. The forecasted weather conditions for the scheduled time of arrival 0630 local time on 26 June indicated:
- wind direction of 240° at 15 kt with gusts up to 25 kt
- CAVOK[12]
- moderate turbulence[13] below 5,000 ft.
One-minute weather data for Sydney Airport from the Bureau of Meteorology indicated a wind direction of 255° at 17 kt with gusts up 20 kt at the time of the occurrence.
Airport information
Runway 16R at Sydney Airport is oriented on a magnetic heading of 155° and has a declared length of 3,962 metres with a width of 45 metres. A precision approach path indicator system is installed and set to 3° with a threshold crossing height of 64 ft.
For daytime operations, the runway centreline, aiming point and touchdown zone markings provide visual references to assist pilots with approach and landing (Figure 3).
Figure 3: Sydney Airport runway 16R markings
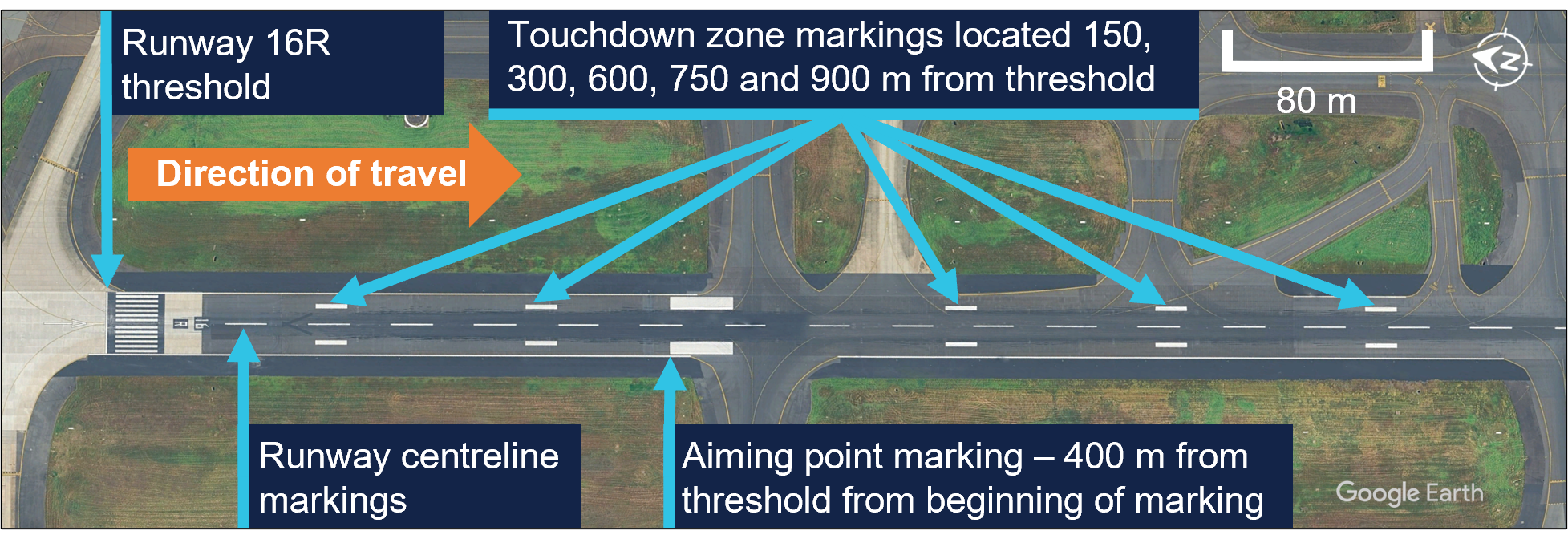
Source: Google Earth, annotated by the ATSB
Recorded information
The aircraft’s quick access recorder data which captured the incident approach indicated that, as the aircraft descended below 1,000 ft, it maintained an appropriate speed and flightpath with no sustained exceedances of the stable approach criteria throughout the approach.
At 0621:59, the recorded data captured the captain’s control inputs commencing concurrently with the initiation of the go-around, while the first officer was actively manipulating their sidestick control. Simultaneous control inputs lasted for a duration of 6 seconds (Figure 4), while the aircraft’s pitch attitude remained below the aircraft’s pitch limit of 11.5° until the aircraft had climbed through about 50 ft.
The recorded data further indicated that the wind direction and speed varied following the flare manoeuvre, however the crosswind component remained well below the first officer’s operational limitation. The wind direction and speed was 315° at 13 kt with a crosswind component of 5 kt when the go-around was initiated.
Figure 4: Graphical representation of the recorded quick access data
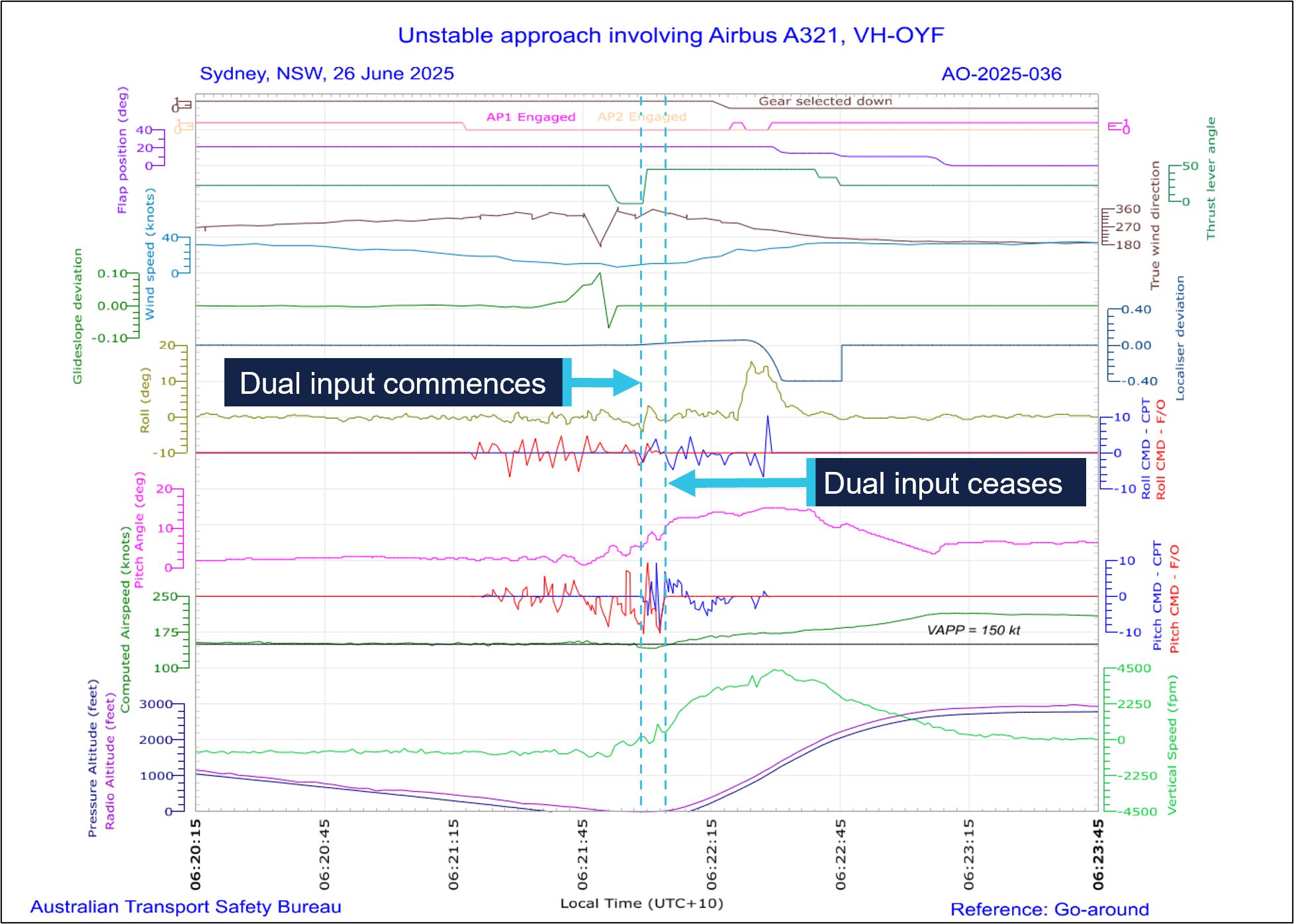
Source: Quick access recorder from VH-OYF, annotated by the ATSB
Following the initiation of the go-around, the landing gear was retracted at 06:22:20 and 12 seconds later, the flap was retracted to the flap 2 configuration[14] at 174 kt.
Operational information
Stabilised approach criteria
Jetstar Airways A320-A321 Flight crew operating manual (FCOM) defined a stabilised approach criteria as being established on the correct lateral and vertical flight path by 1,000 ft height above airport (HAA), configured for landing, and within the stated tolerances with the required checklists completed by 500 ft HAA. The FCOM also stated that if these criteria could not be met, or if the approach became unstable below 1,000 ft HAA, a missed approach was required.
The crew reported the approach was stabilised against these criteria, which was consistent with the available recorded data.
Touchdown zone
The FCOM provided the following operational information regarding the touchdown zone:
The touchdown zone commences at 300 m (1000 ft) beyond the threshold and will not normally extend further than 600 m (2000 ft) beyond the threshold.
It is a requirement that the touchdown is planned to occur within the touchdown zone. Should it become apparent that the aircraft will touch down further than 600 m (2,000 ft) beyond the threshold, and the PIC believes that the landing is safe to continue, the PF must apply maximum reverse thrust and sufficient braking to ensure the aircraft stops within the landing distance available. If the PIC decides that a go-around is required, they will without delay, call “Go-Around”. In all cases this must be completed before the PF initiates reverse thrust.
The captain stated that runway 16R in Sydney was long enough to stop the aircraft on the runway if they had continued with the landing during the occurrence. This would have involved requesting maximum reverse and manual braking as necessary after the aircraft touched down.
The FCOM did not specifically reference runway centreline tracking during a visual approach, however the captain stated that it was their personal expectation that a deviation from the runway centreline would lead them to calling for a go-around.
Transfer of control
The operator described procedures for transfer of control within the FCOM as follows:
The pilot relinquishing control of the aircraft shall say “You have control”. The pilot assuming control shall ensure that they have clear and unobstructed access to the flight controls and, when ready, say “I have control”. Only then is the pilot relinquishing control permitted to remove their hands and feet from the flight controls.
In critical phases of flight the PIC must be alert and positioned such that they can assume immediate control of the aircraft.
Following the occurrence, the captain stated the preferable method to conduct a go‑around at low level would have been to announce ‘I have control’ and initiate the go‑around themselves. They stated that their primary consideration when conducting a go‑around at low level was to avoid the risk of tail strike.
Go-around procedure
The FCOM defined the go-around procedure for the A320/A321, which specified the task sequence, memory-based crew actions and applicable guidance relating to techniques and navigation (Figure 5).
Figure 5: Jetstar Airway A320/A321 go‑around procedure below acceleration altitude
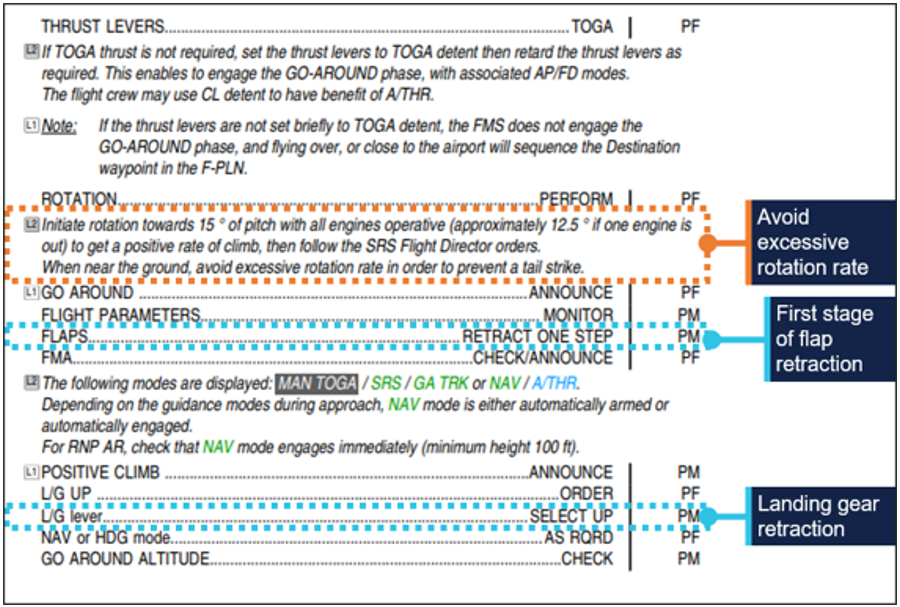
Source: Operator, annotated by the ATSB
Following the occurrence, the captain stated that although they could have taken over and landed, they believed that going around was considered the safest option. The first officer also stated, at about that time, that they were in the mindset of preparing to initiate a go-around themselves.
Related occurrences
The following ATSB investigation highlights the importance of pilots maintaining their readiness for a go-around on every approach as it is typically a period of high workload requiring effective crew coordination.
ATSB Investigation
On the morning of 18 May 2018, an Airbus A320 aircraft, registered VH-VQK, was being operated on a regular public transport flight by Jetstar Airways. The flight departed from Sydney for Ballina/Byron Gateway Airport, New South Wales.
The flight crew conducted a go-around on the first approach at Ballina because the aircraft’s flight path did not meet the operator’s stabilised approach criteria. On the second approach, at about 700 ft radio altitude, a master warning was triggered because the landing gear had not been selected DOWN. The flight crew conducted a second go‑around and landed without further incident on the third approach.
The flight crew did not follow the operator’s standard procedures during the first go‑around and subsequent visual circuit at 1,500 ft. In particular, the flaps remained at flaps 3 rather than flaps 1 during the visual circuit. This created a series of distractions leading to a non‑standard aircraft configuration for a visual circuit. Limited use of available aircraft automation added to the flight crew’s workload.
Safety analysis
During the approach to Sydney airport, with the first officer acting as the pilot flying (PF), the flight crew reported experiencing a crosswind of up to 30 kt until descending through about 500 ft above mean sea level. The crew were advised by air traffic control to expect a right crosswind component of 8 kt for landing, which was within the first officer’s operational crosswind limit of 20 kt. The captain confirmed the approach was ‘stable’ at 500 ft and the first officer continued the approach as PF.
At 50 ft, the first officer initiated the flare manoeuvre prior to landing. They recalled they ‘over flared,’ and the aircraft subsequently floated for an extended period along the runway. During this time, the first officer’s control inputs did not counteract the effect of the crosswind, and the aircraft drifted left of the centreline. After observing the lateral deviation from the centreline, the captain commanded the first officer to conduct a go‑around.
This occurred just prior to the aircraft touching down when the flight crew would normally be focused on landing. The flight crew did not expect a go-around at the time and had to rapidly shift their focus to conducting the missed approach procedure. The captain recalled being ‘startled’ by the unexpected need to discontinue the landing, however they were more likely experiencing ‘surprise.’ Surprise is a cognitive-emotional response to something unexpected, which results from a mismatch between one’s mental expectations and perceptions (Rivera, Talone, Boesser, Jentsch, & Yeh, 2014). But their decision was consistent with the expectation that an approach be discontinued if the aircraft departed from the correct lateral flight path.
The unexpected change from landing to conducting a go-around close to the ground also resulted in the captain experiencing a sudden stress response at this time. When experiencing acute stress, people can respond quickly to a situation, but without conscious decision‑making (Wickens, Helton, Hollands, & Banbury, 2022). After the go‑around was commanded, there was a rapid increase in pitch attitude, engine thrust and airspeed, and in response the captain instinctively and inadvertently manipulated their sidestick while the first officer was flying, resulting in a dual-input alert.
The captain reported they only realised they had manipulated their sidestick when they heard the dual input alert. Their primary consideration during the go-around was to avoid an excessive rotation rate to avoid a tail strike, which did not occur. Additionally, operator procedures directed captains to be alert and be positioned to ‘assume immediate control of the aircraft’ during critical phases of flight.
Following the dual input alert, the captain took full control by engaging their sidestick push‑button and announced ‘I have control’, and the first officer assumed the role of pilot monitoring. A consequence of the control handover during the initial stages of the go‑around was the momentary interruption of sequential crew actions during the go‑around procedures. Interruptions typically disrupt the chain of procedure execution so abruptly that pilots turn immediately to the source of the interruption without noting the point where the procedure was suspended (Loukopoulos, Dismukes, & Barshi, 2009).
Additionally, there was a further disruption (rapid task switching) associated with the first officer and captain exchanging pilot flying and pilot monitoring roles. As a result, some of the procedural items were completed out of sequence (flap 3 retraction occurred after gear retraction).
Pilots are highly vulnerable to errors of omission when they must attend to multiple tasks. If one task becomes demanding, their attention is absorbed by these tasks demands and they can forget to switch their attention to other tasks (Loukopoulos, Dismukes, & Barshi, 2009). Although the flap retraction occurred out of sequence during the go-around, there were no associated flight envelope exceedances or negative effects on aircraft performance.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the control issues during landing and go-around involving Airbus A321, VH-OYF, at Sydney Airport, New South Wales, on 26 June 2025.
Contributing factors
- During the landing after crossing the threshold, the first officer’s control inputs resulted in a lateral deviation from the runway centreline during a prolonged float.
- After calling for a go-around, the captain inadvertently manipulated their sidestick while the first officer was the pilot flying, which resulted in a simultaneous control input and the go-around procedure being completed out of sequence.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Jetstar Airways Pty Limited
- Bureau of Meteorology
- the flight crew
- recorded data from the quick access recorder from VH-OYF.
References
Loukopoulos, L., Dismukes, R., & Barshi, I. (2009). The perils of multitasking. AeroSafety World, 4(8), 18-23.
Rivera, J., Talone, A., Boesser, C., Jentsch, F., & Yeh, M. (2014). Startle and surprise on the flight deck: Similarities, differences, and prevalence. In Proceedings of the human factors and ergonomics society annual meeting (Vol. 58, No. 1, pp. 1047-1051). Sage CA: Los Angeles, CA: SAGE Publications.
Wickens, C. D., Helton, W. S., Hollands, J. G., & Banbury, S. (2022). Engineering psychology and human performance, 5th edn. Routledge, doi: 10.4324/9781003177616.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Civil Aviation Safety Authority
- the flight crew
- Jetstar Airways Pty Limited
- Bureau of Meteorology.
Submissions were received from:
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Local time in Sydney was Australian Eastern Standard Time (AEST), which is Coordinated Universal Time (UTC) +10 hours. Times in this report are AEST unless otherwise noted.
[2] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 330 equates to 33,000 ft.
[4] Runway numbering: the number represents the magnetic heading closest to the runway (runway 16 at Sydney Airport is oriented 155° magnetic) and R indicates the right most of 2 parallel runways.
[5] Visual meteorological conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[6] Flap 3 on the A321-251 is 21° of flap and 22° of slat extension.
[7] Final approach speed (VAPP): the VAPP is the target airspeed for the aircraft when crossing the runway threshold with the aircraft configured for landing. VAPP is equal to the lowest selectable speed with the addition of wind correction. The wind correction is limited to a minimum of 5 kt and a maximum of 15 kt.
[8] GBAS landing system (GLS): a GLS consists of a GBAS ground station located on or in the vicinity of one or more aerodromes and an aircraft subsystem. The GBAS provides data and corrections for the GNSS ranging signals over a digital VHF data broadcast to the aircraft subsystem. The aircraft subsystem translates the position signal into flight guidance similar to that provided for an ILS.
[9] Back of the clock: Work schedules that involve extended periods of night-work between midnight and dawn.
[10] A biomathematical model of fatigue predicts the effect of different patterns of work on measures such as subjective fatigue, sleep, or the effectiveness of performing work, using mathematical algorithms. Each model uses different types of inputs and assumptions and produces different types of outputs, each having limitations. The ATSB used the biomathematical modelling software SAFTE-FAST and FAID Quantum for the analysis.
[11] Aerodrome forecast (TAF): a TAF is a coded statement of meteorological conditions expected at an aerodrome and within a radius of 5 nautical miles of the aerodrome reference point.
[12] Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[13] Moderate turbulence: changes to accelerometer readings of between 0.5 g and 1.0 g at the aircraft’s centre of gravity. Moderate change to aircraft attitude and/or altitude may occur but aircraft remains under positive control. Usually small changes in airspeed. Difficulty in walking. Lose objects move about.
[14] Flap 2 on the A321-251 is 14° of flap and 22° of slat extension.
Occurrence summary
| Investigation number | AO-2025-036 |
|---|---|
| Occurrence date | 26/06/2025 |
| Location | Sydney Airport |
| State | New South Wales |
| Report release date | 27/01/2026 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Control issues, Missed approach, Warning devices |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Airbus |
|---|---|
| Model | A321-251NX |
| Registration | VH-OYF |
| Serial number | 11529 |
| Aircraft operator | Jetstar Airways Pty Limited |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Denpasar International Airport, Bali, Indonesia |
| Destination | Sydney Airport, New South Wales |
| Damage | Nil |