On 18 June 2025, a Beechcraft King Air B200, registered VH-EEL, was on descent into Bankstown Airport, New South Wales, on a passenger transport flight with the pilot and 4 passengers on board when the pilot heard a whistling noise followed by the sound of an impact coming from the rear of the aircraft. There were no abnormal indications and the aircraft was flying normally, so the pilot continued the flight.
Shortly after, the pilot was unable to reach air traffic control via radio and switched to the aircraft’s alternative radio. Communication was re‑established and the aircraft landed safely. An external inspection of the aircraft found that the VHF antenna on top of the fuselage was missing, and the vertical stabiliser was damaged.
What the ATSB found
While the top of the antenna was not recovered, the aluminium antenna base showed evidence of moisture ingress. This resulted in the antenna failing and separating from the aircraft. The exact failure mechanism could not be determined – moisture could have been absorbed by the composite skin of the antenna, reducing its strength. Alternatively, observed corrosion could have weakened the bond between structural components within the antenna, reducing stiffness and allowing cracks to develop.
Safety message
While it is not clear whether pre-existing damage was observable during antenna inspections, this occurrence is a useful reminder on the importance of vigilance while conducting routine maintenance. In addition, it serves to demonstrate the value of redundancy in safety-critical systems.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the afternoon of 18 June 2025, a Beechcraft King Air B200, registered VH-EEL, departed from Dubbo Airport, New South Wales, on a passenger transport flight to Bankstown Airport. The flight was operated by CJ Aerospace with the pilot and 4 passengers on board. It was a clear day and the aircraft was flying in visual meteorological conditions.
At approximately 1523, the aircraft was about 30 NM (55 km) from Bankstown Airport and descending through 11,000 ft when the pilot heard a whistling noise coming from the back of the aircraft. After a few seconds, the pilot reported hearing the sound of an impact towards the rear of the aircraft. The aircraft’s airspeed was approximately 280 kt at the time. There were no abnormal indications in the cockpit and the aircraft was flying normally, so the pilot continued with the flight.
The aircraft had been previously cleared by air traffic control (ATC) to descend to 5,000 ft. However, after reaching this altitude it had not been cleared for further descent, which the pilot noted to be unusual. The pilot conducted a radio check with ATC but received no response. The pilot switched the aircraft’s active VHF radio from COM 1 to COM 2, and contact with ATC was subsequently re‑established. The rest of the approach and landing proceeded without incident and the aircraft landed at Bankstown Airport at 1534.
After landing, the pilot conducted an external inspection of the aircraft and found that the VHF antenna on top of the fuselage was missing, and the vertical stabiliser was damaged (Figure 1). Further information on the damage is in Aircraft information and Antenna examination.
Figure 1: Damage to the vertical stabiliser
Source: Jet Aviation
Context
Pilot information
The pilot held a Commercial Pilot (Aeroplane) Licence, issued in December 2019, with a multi‑engine aeroplane instrument rating. At the time of the occurrence, the pilot had approximately 1,980 hours total flying experience, of which 140 hours were accrued on the King Air B200.
Aircraft information
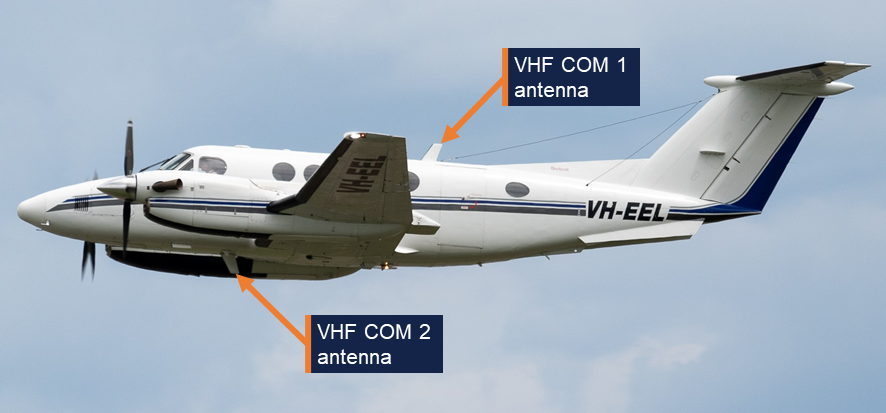
The Beechcraft King Air B200 is a pressurised, low-wing, twin turbine-engine aircraft. It has 2 VHF antennas: COM 1 is fitted on top of the fuselage, and COM 2 is underneath the fuselage (Figure 2). VH-EEL was manufactured in the United States in 2000 and registered in Australia in the same year. CJ Aerospace had been the registered operator of the aircraft since July 2021.
Figure 2: VHF antennas on VH-EEL
Source: CQ Plane Spotting
Aircraft examination
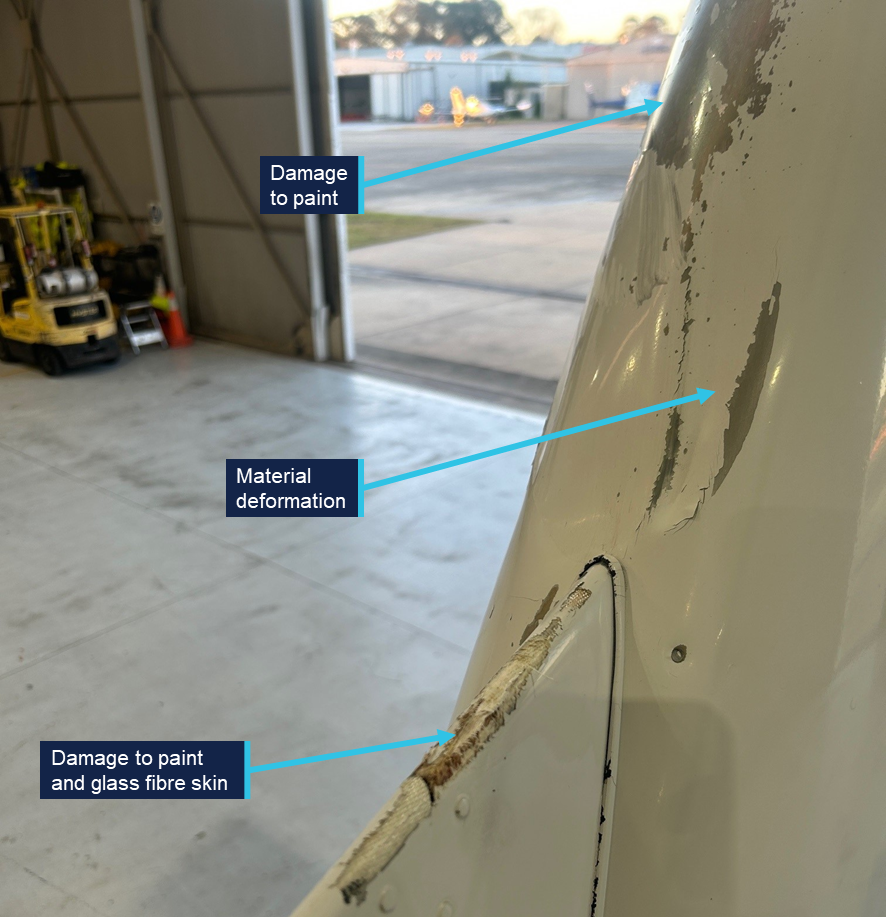
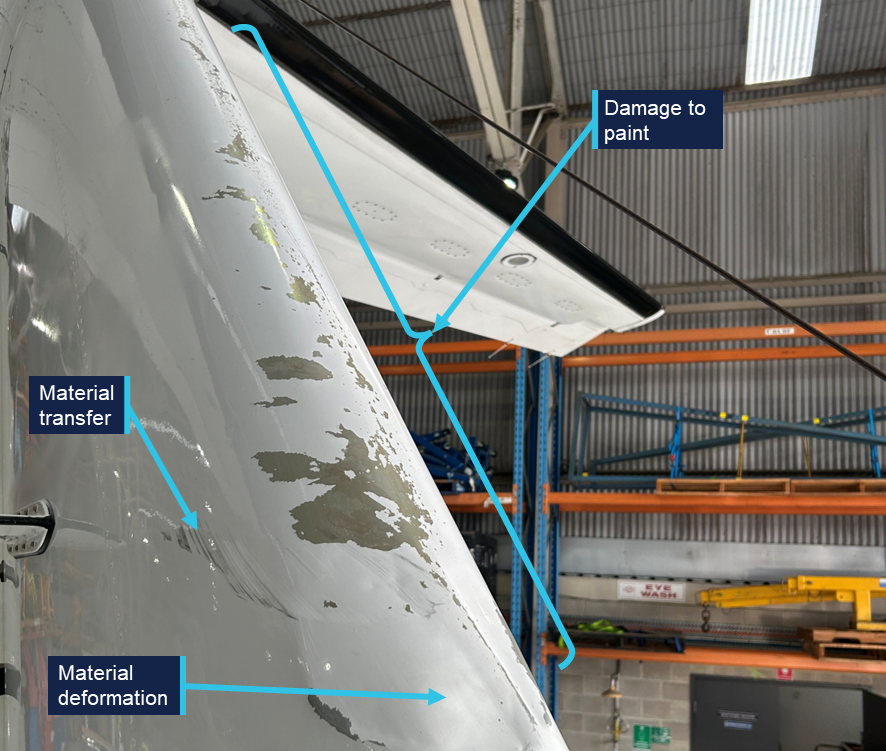
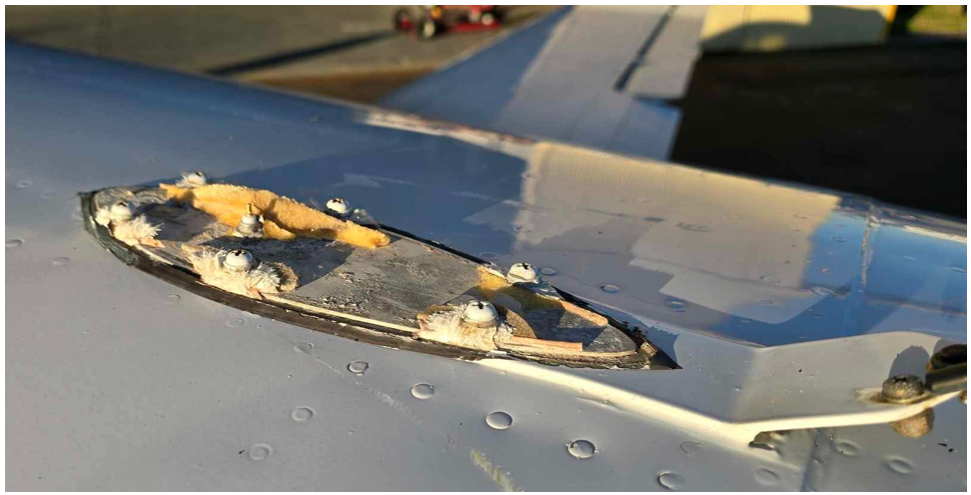
Following the occurrence, the aircraft was sent to a maintenance facility for examination and repair. The examination (not attended by the ATSB) identified that the leading edge of the vertical stabiliser had experienced deformation, and there was damage to the skin and paint on various parts of the empennage (Figure 3 and Figure 4). There also appeared to be some transfer of black material, possibly paint or rubber, onto the right side of the vertical stabiliser. The base of the antenna was still secured to the fuselage by 6 fasteners, but the glass fibre skin of the antenna had failed around each of the fasteners and separated from the aircraft (Figure 5).
Figure 3: Damage on the front of the empennage
Source: Jet Aviation, annotated by the ATSB
Figure 4: Damage on the right side of the empennage
Source: Jet Aviation, annotated by the ATSB
Figure 5: The antenna base still secured to VH-EEL
Source: Jet Aviation
Antenna examination
The detached antenna was not located. The antenna base was examined at the ATSB’s engineering facility in Canberra. The manufacturer’s label indicated that it was manufactured by the Trivec-Avant corporation. The part number was 18-40-01 and the serial number was 11514. The antenna was not original to the aircraft, and its installation date could not be determined. The Trivec-Avant corporation ceased operation in about 2011, and no technical drawings or other details could be obtained for the antenna. However, images of an antenna with the same part number were sourced online (Figure 6). It comprised a base and upper structure with an internal electrical antenna.
Figure 6: Exemplar VHF COM antenna
Source: majorjunque (eBay)
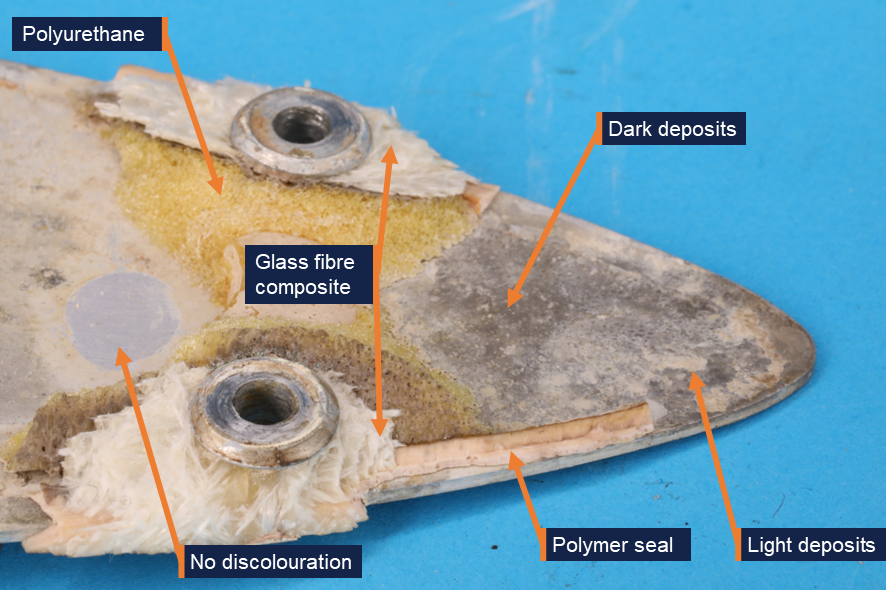
The antenna base from VH-EEL was an aluminium plate with 6 holes for fasteners and a central coaxial connection for the internal electrical antenna (Figure 7). A yellow foam adhered to the top face of the antenna was likely an expanding polyurethane product that was injected into the antenna during its construction in order to increase rigidity (Figure 8). Some fractured glass fibre composite material was observed around each of the fasteners. Fragments of a polymer seal were observed around the edges of the antenna base.
Figure 7: Antenna base from the aircraft
Source: ATSB
Both surfaces of the plate showed discoloration in several locations, identified as deposits on the surface of the metal (Figure 8). The deposits varied in colour. Samples of the dark-coloured and light-coloured deposits were scraped from the antenna using a plastic spatula and analysed for elemental composition using energy-dispersive X-ray spectroscopy (EDS). EDS analysis found that the composition of the light and dark deposits was very similar. Both predominantly contained aluminium, oxygen, and a smaller quantity of chlorine. The presence of chlorine indicated that the plate was exposed to salt water, resulting in corrosion of the aluminium plate, forming aluminium oxide.
Figure 8: Aft end of the antenna base, top face
Source: ATSB
The discolouration was not uniformly distributed over the base, and there were some regions, such as the one shown in Figure 8, where there was no evidence of deposits or discolouration. Similarly, while much of the base’s edge was discoloured, there were some regions underneath the polymer seal that appeared relatively unaffected (Figure 9).
Figure 9: Discolouration under the polymer seal, at the edge of the top face
Source: ATSB
Aircraft maintenance
The aircraft was maintained under a 4-phase inspection program over 800 flight hours or 24 calendar months. Each phase of routine maintenance was conducted sequentially every 200 hours. Inspection of the VHF antennas was conducted in Phase 3. The inspection required personnel to:
…inspect all external antennas for leading edge erosion and condition of base seals.
This was last performed on 18 October 2024 with no relevant findings recorded.
The aircraft manufacturer provided guidelines for corrosion control inspections, which were optional and to be used depending on the operating environment. Regarding antennas, the inspection stated the following:
ANTENNAS - Inspect antenna bases for proper sealing. Inspect antenna leading edges for severe erosion.
These inspections were also last carried out on 18 October 2024 with no relevant findings recorded.
Neither inspection specified whether antenna removal was necessary.
Similar occurrences
The aircraft manufacturer could not identify any previous instances of antenna separation in flight, but noted that ‘while it is rare, it is not unknown for antennas to crack at the fastener holes’.
Safety analysis
Based on the aluminium oxide and chlorine found on the surface of the VHF antenna base – a part of the antenna that should be fully enclosed and sealed – the antenna failed in flight due to pre-existing damage resulting from corrosion. The corrosion was almost certainly due to moisture ingress into the unit.
Since most of the antenna was not recovered, there was no way to determine the pathway through which moisture entered the antenna. Most of the seal surrounding the base had separated with the top half of the antenna. There was evidence of moisture under the seal in some regions, while some parts of the seal appeared to have prevented corrosion. The moisture under the seal could indicate a point of ingress, but it is possible that all the corrosion observed under the seals was due to moisture already inside the antenna, rather than evidence that the seal had been compromised.
Beyond the fact that the antenna cracked around the 6 fastener holes, the exact failure mechanism could not be determined. It is possible that corrosion weakened the bond between the polyurethane core and the base or skin of the antenna. This would have reduced the stiffness of the unit, allowing cracks to develop as it flexed during service. Alternatively, moisture could have been absorbed by the glass fibre composite skin, reducing its strength and increasing susceptibility to cracking.
Without an understanding of the mechanisms that led to moisture entering the antenna and the subsequent in-flight separation, it is not possible to determine whether any damage would have been externally visible during the relevant inspection 8 months before the occurrence. Cracking around the fastener holes might not have commenced at that point. Alternatively, damage could have been too small to detect or obscured by the paint.
One alternative possibility to pre-existing damage could not be entirely ruled out: a birdstrike or collision with a remotely piloted aircraft (RPA) could have resulted in antenna separation. However, very few birdstrikes occur above 10,000 ft, and most RPAs are not certified to fly that high. No in-flight RPA loss was reported. There was also no visual evidence of a birdstrike, and any contact with bird or RPA would likely have resulted in a loud bang precipitating the occurrence, rather than a whistling sound followed by the sound of an impact.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the antenna failure involving Beechcraft King Air B200, VH-EEL, 55 km west of Bankstown Airport, New South Wales, on 18 June 2025.
Contributing factors
During flight, pre-existing damage due to moisture ingress resulted in the VHF COM 1 antenna failing and separating from the aircraft.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
CJ Aerospace
Textron Aviation (Beechcraft)
the aircraft maintenance organisation
the maintenance organisation that examined the aircraft following the occurrence
Civil Aviation Safety Authority
Flightradar24.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
CJ Aerospace
the aircraft maintenance organisation
Civil Aviation Safety Authority
Textron Aviation (Beechcraft)
National Transportation Safety Board (United States).
There were no submissions received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Occurrence summary
Investigation number
AO-2025-031
Occurrence date
18/06/2025
Occurrence time and timezone
1523 Australian Eastern Standard Time
Location
55 km west of Bankstown Airport
State
New South Wales
Report release date
15/05/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Avionics/flight instruments, Objects falling from aircraft
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Raytheon Aircraft Company
Model
B200
Registration
VH-EEL
Serial number
BB-1697
Aircraft operator
C J Aerospace Pty Ltd
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Passenger transport charters
An incident in which a PC‑12 aeromedical aircraft struck a temporary light being used to mark a closed section of taxiway at Adelaide Airport highlights the importance of effective communication and the potential for expectation bias.
The Royal Flying Doctor Service Pilatus PC‑12 was incorrectly cleared to enter a closed section of taxiway while taxiing for a night‑time take‑off on 4 November 2024, an ATSB investigation report details.
Although the closure was detailed in a NOTAM and the ATIS (automatic terminal information service) current for Adelaide Airport at the time, the aircraft subsequently entered the taxiway and struck one of three red lights being used to denote that the section of taxiway was closed.
“The pilot knew about the taxiway closure but, when they were given clearance to enter it, assumed the works had ended early,” ATSB Director Transport Safety Stuart Macleod said.
Shortly after, the controller advised the pilot they had entered the closed taxiway and requested they stop and turn back.
An aerodrome works safety officer, in a nearby safety car, coordinated with the controller to remove the red lights from the taxiway to allow the aircraft to taxi back off the closed section. On entering the taxiway they advised they were removing debris from the taxiway.
The controller then asked the pilot if they wished to continue. After conferring with the aircraft flight nurse, the pilot assessed that the aircraft had not struck a light and advised the controller they would continue with departure.
“While the flight was uneventful, the possibility of damage meant an inspection should have been completed prior to continuing the flight,” Mr Macleod noted.
The investigation report also noted that it was Adelaide Airport’s general practice to use three red lights and no markers at night to denote a closed taxiway.
“The lighting used to identify the taxiway section as being closed was insufficient to draw the pilot’s attention at night, and the required cone markers were not in place,” Mr Macleod said.
“The use of only three red lights, in situations where there is increased background lighting such as the incident taxiway, reduced the prominence of unserviceable movement areas.”
Adelaide Airport’s method of working plan, required by CASA to ensure aerodrome works do not create a hazard to aircraft or cause confusion to pilots, did not specify a minimum number of unserviceability markers or lights to be used, the investigation found.
Moreover, CASA’s aerodrome requirements and standards (under the Part 139 Manual of Standards) did not specify that both markers and unserviceability lights were required for a closed taxiway, and did not provide adequate recommendations for lighting at aerodromes with significant background lighting.
CASA has since advised it is updating its guidance on the use of both unserviceability cones and lights to designate closed taxiways at night.
“This incident highlights the importance of effective communication, and the potential for expectation bias,” Mr Macleod concluded.
“For pilots, if you receive a clearance that contradicts a NOTAM or current ATIS information, you should question the clearance before continuing.
“For aerodrome operators, this incident reinforces that when assessing the adequacy of unserviceability lighting, consider the effects of any obscuring background lighting and increase the span of lighting if required.”
Rail operators are advised to ensure consistent application of procedures, and that checks reduce the likelihood of single‑person errors, after two Melbourne trains entered the same section of single track from opposite directions.
A final report from Victoria’s Office of the Chief Investigator (OCI), which investigates rail occurrences in Victoria under a collaboration agreement with the ATSB, details the 25 February 2024 incident.
A non-revenue (not passenger‑carrying) Metro Trains Melbourne train was travelling along a bi‑directional, single line section of track between Ferntree Gully and Upper Ferntree Gully stations, east of Melbourne, when it came to a stop at a red signal.
Another MTM train, a passenger service operating in the opposite direction, was at Upper Ferntree Gully station and scheduled to enter the single line section towards Ferntree Gully.
“The station officer at Upper Ferntree Gully believed the section between Ferntree Gully and Upper Ferntree Gully stations was clear and gave the passenger train permission to proceed into the single line section under a ‘caution order’,” Chief Investigator Mark Smallwood said.
The passenger service then proceeded into the single line section under the caution order (at below 25 km/h), and began to travel towards Ferntree Gully station, and towards the non‑revenue service which was still stopped midway along the section.
“Fortunately, the driver of the moving passenger train sighted the stationary non‑revenue train a short time later,” Mr Smallwood said.
“They brought their train to a stop about 300 m away from the stationary train.”
The OCI concluded that the station officer at Upper Ferntree Gully believed a recurring track fault was incorrectly holding the passenger train at the station, and that the single section between the two stations was clear. The non‑revenue service had arrived in the section from Ferntree Gully ahead of schedule and was not expected by the station officer.
“The investigation found that at Upper Ferntree Gully (and some other parts of the MTM network), the issuing of a caution order did not require validation by a second person,” Mr Smallwood observed.
“Checks on safety‑critical decisions should be incorporated into procedural systems to reduce the likelihood of single‑person errors.
“In addition, procedures associated with managing trains between Bayswater and Upper Ferntree Gully on the Belgrave line were inconsistently applied, and gaps in protocols and record‑keeping probably impacted the effectiveness of the systems.”
In response, operator Metro Trains Melbourne has reviewed relevant procedures and commissioned changes to signalling control circuitry to address issues identified in the investigation.
On the afternoon of 13 June 2025, a Pilatus PC‑12, registered VH‑NWI and operated by Armada Aviation, was being used to conduct a charter air transport flight from Essendon Airport, Victoria, to Launceston Airport, Tasmania. On board were a pilot and 4 passengers.
During the approach to Launceston, the aircraft deviated left from the final approach course and intercepted the extended centreline of the adjacent taxiway. The aircraft then continued towards the taxiway where a Cessna 152 (C152) was holding for departure. Approaching the taxiway, the pilot conducted a low-level right then left turn to realign with the runway, before commencing a missed approach. During the manoeuvre the aircraft passed in close proximity to the C152. Following the missed approach, the aircraft conducted a visual circuit and landed without further incident.
What the ATSB found
The ATSB found that the final approach was conducted in clear conditions almost directly into the sun, exposing the pilot to glare. Subsequently, the pilot misidentified the taxiway as the runway and aligned the aircraft with the taxiway's extended centreline. The pilot then corrected the aircraft's flight path at a low level rather than conducting an immediate missed approach. During the manoeuvre the aircraft passed in close proximity to an aircraft on the taxiway.
It was also found that after identifying that the approaching aircraft was aligned with the taxiway, the instructor on board the aircraft on the taxiway made a radio broadcast, likely alerting both the pilot and air traffic control to the situation.
What has been done as a result
Armada Aviation circulated a notice to its aircrew advising them of hazards associated with a visual approach, such as sun glare. Additionally, it made the following changes to its operating procedures:
Updated the final decision to proceed to landing to include a requirement that the runway was confirmed and clear by 400 ft above ground level, or the approach minima.
Added a top of descent safety briefing to ensure pilots brief other risks associated with the visual approach segment following an instrument approach, including lighting configuration and sun position.
Updated the checklist of the final phase of flight to include checking that the runway was confirmed and clear.
Safety message
Sun glare can reduce a pilot’s visual effectiveness even when meteorological visibility is good. When flying visually in such conditions, pilots should crosscheck against available flight and navigation instruments in conjunction with external indicators, such as airport lighting, to verify that the aircraft is on the intended flight path.
If a discrepancy is identified below an appropriate stabilised approach height, an immediate missed approach should be conducted. Low-level manoeuvring outside of the published approach and associated obstacle clearance increases the risk of collision with terrain or objects on the ground.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 13 June 2025, a Pilatus PC-12, registered VH‑NWI and operated by Armada Aviation, was being used to conduct a charter air transport flight from Essendon Airport, Victoria, to Launceston Airport, Tasmania (Figure 1). On board were a pilot and 4 passengers.
Figure 1: Occurrence flight
Source: Google Earth annotated by the ATSB
At 1511 local time, the aircraft commenced the instrument approach procedure for runway 32L[1] at Launceston. The weather at the time was predominately clear skies with few[2] clouds at 3,000 ft, variable wind up to 5 kt and visibility greater than 10 km.
At approximately the same time, the occupants (instructor and student) of a Cessna 152 (C152) on the ground at Launceston contacted air traffic control (ATC) to request taxi clearance for departure on a training flight. Due to the closure of a section of the taxiway (see Figure 4 and the section titled Construction works), the C152 was required to backtrack the runway and vacate onto taxiway A at the runway 32L threshold. The aircraft then turned 180° on the taxiway and stopped with the nose of the aircraft at holding point A. At 1515, the C152 reported to ATC that they had completed the taxi and were clear of the runway.
By this time VH‑NWI was established on the final segment of the approach, approximately 7 NM (13 km) from the runway. Shortly thereafter, ATC cleared the aircraft to land, later reporting that at this time they observed the aircraft established on the final approach. The pilot reported that throughout the final approach, they were looking into the sun and consequently they ‘couldn’t really see much at all’.
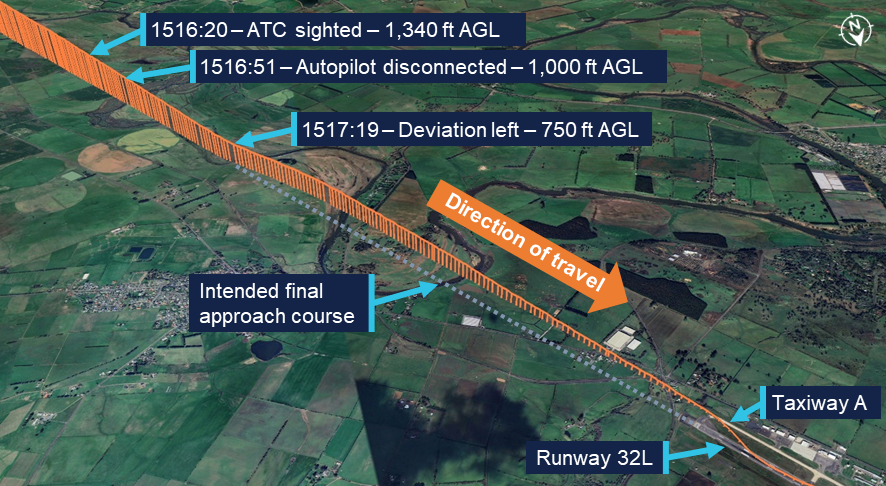
ATC reported again sighting the aircraft when it was approximately 4 NM (7 km) from the runway. At this point the aircraft was approximately 1,340 ft above ground level (AGL) and still aligned with the final approach course (Figure 2).
Figure 2: Final approach flight path
Recorded altitude resolution ± 12.5 ft, over underlying terrain elevation, rounded to nearest 5 ft. Source: ADS-B flight data overlaid on Google Earth, annotated by the ATSB
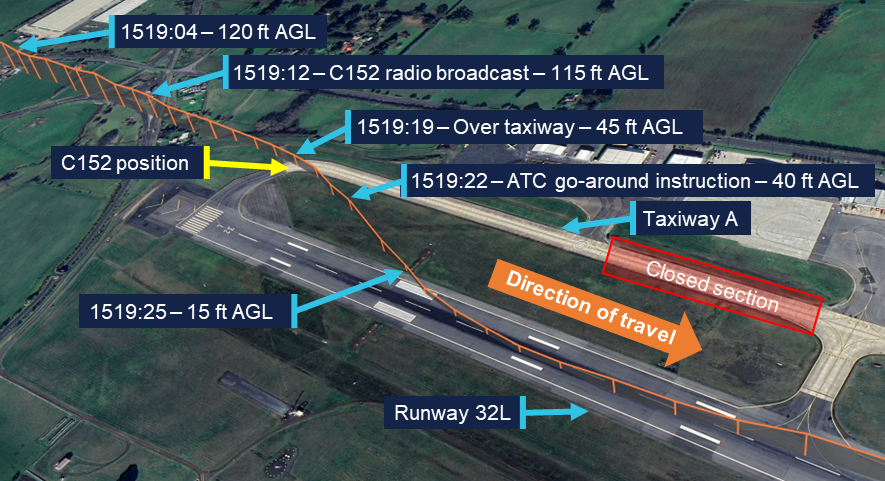
The pilot advised that, during the approach, they used the autopilot to manage the aircraft’s flight path until approximately 1,000 ft AGL. At this point they disconnected the autopilot and transitioned to looking outside. The pilot recalled that they were still looking into the sun and only seeing one feature on the ground that stood out. Identifying it as the runway, they began visually flying the aircraft towards it. Recorded flight data showed that at approximately 750 ft AGL, the aircraft began to deviate left until it intercepted the extended centreline of taxiway A. From this position the aircraft continued to descend towards the taxiway. At 1519, when the aircraft was approximately 120 ft AGL, weather cameras at the airport recorded images showing both the aircraft on final and the C152 at the holding point (Figure 3).
Figure 3: Weather camera images at 1519
Combination of 2 images: Left image camera bearing 135° (SE) at 1519:04, right image camera bearing 225° (SW) at 1519:02. Source: Bureau of Meteorology, annotated by the ATSB
The instructor on board the C152 recalled that upon looking for the approaching aircraft, they saw that it was lined up with the taxiway. At 1519:12, they made a radio broadcast on the Launceston Tower frequency advising ‘He’s landing on the taxiway’. Following the call, VH-NWI passed above and behind them. It then reappeared on their left side, after conducting a right, then left, turn to align with the runway.
A review of flight data showed that VH-NWI continued to descend as it tracked the taxiway extended centreline until 1519:16, at which point it commenced a right turn (Figure 4). During the turn, the aircraft passed over the taxiway at a height of approximately 45 ft AGL, 15 m behind holding point A, at which the C152 was positioned. Subsequently, the aircraft descended further as it flew over the grassed area between the taxiway and the runway before turning left to align with the runway centreline. During the realignment manoeuvre, the aircraft descended to approximately 15 ft AGL.
Figure 4: Low-level manoeuvre and missed approach
Recorded altitude resolution ± 12.5 ft, over underlying terrain elevation, rounded to nearest 5 ft. Source: ADS-B flight data overlaid on Google Earth, annotated by the ATSB
The pilot recalled that when not far from the runway environment they became aware that they were approaching the taxiway and in response turned the aircraft towards the runway. They further reported that they were not aware of the C152 at the holding point. While they recalled hearing a radio broadcast as they were moving towards the runway, they did not know who had made it.
ATC reported that upon hearing the broadcast from the C152 they observed VH-NWI on short final lined up with taxiway A, after which it immediately made a right turn to align with the runway. At 1519:22 they instructed the pilot to go around.[3] The pilot later reported that they heard the instruction from ATC, by which time they had decided to initiate a missed approach. Flight data recorded that the aircraft commencing a climb away from the runway at 1519:31. Following the missed approach, the pilot conducted a visual circuit and the aircraft landed without further incident. Subsequently, the C152 departed.
Context
Pilot
The pilot held an air transport pilot licence (aeroplane) issued in 2013 and a class 1 aviation medical certificate. They had accumulated 4,251 flight hours, of which 659 hours were operating the Pilatus PC‑12. In the previous 90 days, the pilot had accumulated 26 hours, all in the PC‑12. They completed an instrument proficiency check in January 2025.
The pilot reported that they had flown into Launceston Airport a number of times previously, both during the day and at night. They did not recall any prior occasion where sun glare had been an issue during final approach.
Aircraft
VH-NWI was a Pilatus PC‑12, powered by a Pratt & Whitney PT6A‑67B turbine engine driving a 4‑bladed, variable pitch Hartzell propeller. The aircraft was manufactured in 1995 and first registered in Australia in 2002. It was subsequently registered with the operator in 2014.
At the time of the incident, the aircraft had accumulated 8,674 hours total time in service. The aircraft was being maintained in accordance with the operator’s system of maintenance and the PC‑12 maintenance manual. The last periodic inspection was conducted in April 2025, and the maintenance release showed no outstanding items.
Launceston Airport
Runway environment
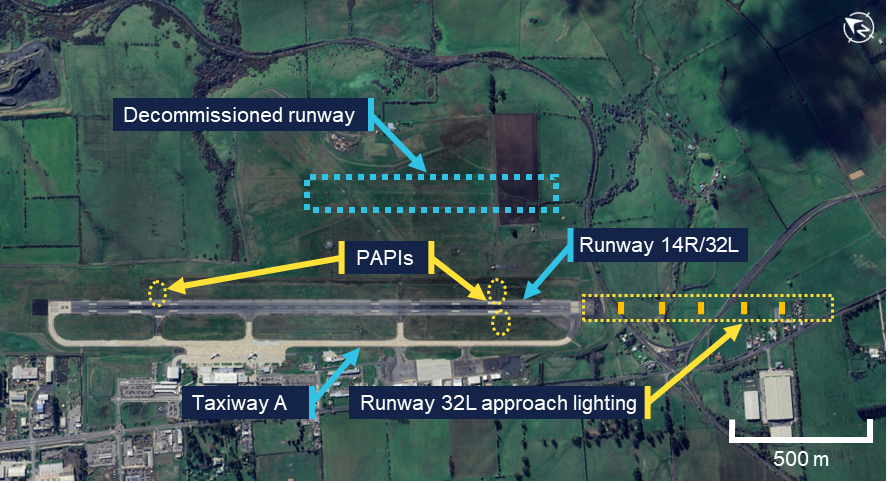
Launceston Airport had a single grooved asphalt runway 14R/32L (Figure 5). The runway was 45 m wide and approximately 2 km long with a runway heading of 313°. The airport had previously operated a parallel grass runway 14L/32R which had been decommissioned however, the remaining runway had not been renamed to remove the left / right designation. The En Route Supplement Australia (ERSA) provided information on Launceston Airport and identified the single operational runway and the decommissioned runway.
Access to the ends of the runway was via taxiway A located on the western side. The taxiway was 23 m wide and ran the length of the runway. The taxiway surface was a lighter colour compared to that of the asphalt runway.
Figure 5: Launceston Airport runway environment and lighting
Source: Google Earth, annotated by the ATSB
Aerodrome and approach lighting
Launceston Airport was equipped with runway edge lighting, approach lighting, taxiway lighting and precision approach path indicator (PAPI)[4] systems. Approach lighting was installed leading to runway 32L with a PAPI on both sides of the runway. Runway 14R had no approach lighting, and a single PAPI on the left of the runway. When activated, the intensity level of each lighting component could be set between 1–6, with 1 being the lowest intensity, and 6 being the highest. During tower hours, this setting was controlled by ATC via a panel in the control tower. Outside tower hours the settings were preset.
On the day of the occurrence, all aerodrome lighting was initially inactive. At 1331 local time, the PAPIs for both runway 14R and 32L were activated at an intensity setting of 5. At 1506, 13 minutes prior to the occurrence, the runway edge lighting, taxiway lighting and the approach lighting for runway 32L were activated with an intensity setting of 4. At the same time, the intensity of the PAPIs was reduced to 4. Airservices advised that this intensity setting was selected due to decreasing ambient light associated with winter conditions at that time of day.
The pilot could not recall whether the airport lighting was on during the first approach. During the second approach and landing, they recalled that the lighting was on and thought that it looked dim and was difficult to see.
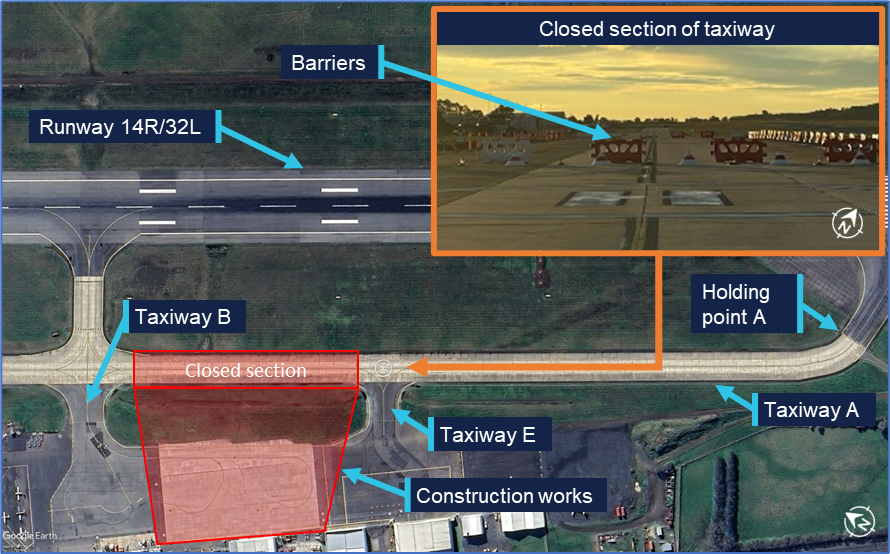
Construction works
At the time of the incident construction works were being conducted in the area adjacent to the southern apron. These works required the closure of taxiway A between taxiway B and taxiway E (Figure 6). Barriers, unserviceability markers and lighting was deployed at the ends of the closed section of taxiway to prevent access. The presence of works and the taxiway closure were advised both via NOTAM[5] and the airport’s automatic terminal information service (ATIS).[6] The pilot reported being aware that the taxiway was closed.
Figure 6: Airport construction works
Source: Google Earth, inset supplied, annotated by the ATSB
Sun effect during the approach
Sun position
At 1517, the time that the aircraft began to deviate from the final approach course, the sun was positioned 10° to the left of the runway heading and 12° above the horizon.
Glare
Glare occurs when unwanted light enters the eye. Direct glare comes directly from a light source whereas veiling glare occurs when light is reflected from crazing[7] or dirt on the windscreen. The ATSB research report Limitations of the See-and-Avoid principle examined the effect of glare on pilots stating:
It has been claimed that glare which is half as intense as the general illumination can produce a 42 per cent reduction in visual effectiveness when it is 40 degrees from the line of sight.
When the glare source is 5 degrees from the line of sight, visual effectiveness is reduced by 84 per cent (Hawkins 1987). In general, older pilots will be more sensitive to glare.
Direct glare from the sun and veiling glare reflected from windscreens can effectively mask some areas of the view.
The pilot reported that the aircraft was equipped with a tinted sun visor. They had placed this between their eyes and the sun during the approach however this did not sufficiently reduce the direct glare. Consequently, they reported that for most of the final approach, when not required for power adjustments, they held their right hand in front of their face to block the sun.
They further reported that the windscreen was not crazed or dirty and that the aircraft had been recently washed. They were wearing reading correction glasses which did not provide glare protection and were not wearing any headwear that could be used to shield the sun.
Stabilised approach criteria
The operator’s procedures defined criteria for stabilised approaches. If an approach was not stable below 300 ft above aerodrome elevation, an immediate missed approach was required to be conducted. These criteria included that:
From 500 ft AGL on the descent, the aircraft shall be:
- on the correct flight path with only small changes in heading and pitch required to maintain the correct flight path
- the indicated airspeed is not more than Vref [landing reference speed] (-0/+ 10 kts)
- the aircraft is in an acceptable landing configuration
- sink rate is no greater than 600 fpm [feet per minute]; if an approach requires a sink rate greater than 1000 fpm, a special briefing should be conducted
- power setting is appropriate for the aircraft configuration and is not below the minimum power for approach as defined by the aircraft operating manual
- all briefings and checklists have been completed.
Safety analysis
The pilot conducted the final approach segment in clear conditions with the sun low in the sky and 10° to the left of runway heading. This exposed them to direct sun glare during the approach. To reduce the effect of the glare they used the aircraft’s visor and their right hand to block the sun. However, some glare remained, and their raised hand likely impacted their view of the runway and associated lighting. Consequently, the pilot misidentified the taxiway as the runway and aligned the aircraft with the taxiway centreline.
During the subsequent segment of the approach, the aircraft’s navigation instruments were likely indicating that the aircraft was to the left of the intended flight path. However, the pilot was looking outside during this time and therefore did not detect the deviation. Furthermore, they did not observe the C152 positioned on the taxiway, likely due to the continued reduced visibility throughout the approach.
The instructor on board the C152 broadcast over the radio after identifying that the approaching aircraft was aligned with the taxiway. Shortly after this broadcast, the aircraft commenced a turn towards the runway. While continuation to landing on the taxiway would likely have resulted in the aircraft passing over the C152, it would probably have resulted in a collision with obstacles associated with the airport’s construction works. As the aircraft commenced its turn toward the runway after the broadcast was made, it is likely that the broadcast contributed to the pilot’s recognition of the situation. However, they advised that they remained unaware that there was an aircraft on the taxiway.
During the manoeuvre, the aircraft passed behind and in close proximity to the C152. Conducting such a manoeuvre carried a risk of collision with both the C152 and other objects on the ground. Moreover, this manoeuvre was not in accordance with the operator’s stabilised approach criteria where only small heading changes were permitted below 500 ft above ground level (AGL). Upon recognising that the aircraft was not on the intended flight path, an immediate missed approach was required to be conducted. The broadcast from the C152 instructor also alerted air traffic control (ATC) to the situation, prompting them to instruct the pilot to discontinue the landing.
Consideration was given to whether the designation of the landing runway at Launceston Airport as the left runway may have led the pilot to misidentify the taxiway as the left of 2 parallel runways. However, this was not reported by the pilot. Furthermore, they had prior experience operating at the airport and were therefore familiar with the runway layout.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the passing in close proximity to an aircraft on a taxiway during approach involving a Pilatus PC‑12, VH‑NWI, Launceston Airport, Tasmania, on 13 June 2025.
Contributing factors
The final approach was conducted in clear conditions almost directly into the sun, exposing the pilot to glare. Subsequently, the pilot misidentified the taxiway as the runway and aligned the aircraft with the taxiway's extended centreline.
The pilot corrected the aircraft's flight path at a low level rather than immediately conducting a missed approach. During the manoeuvre, the aircraft passed in close proximity to an aircraft on the taxiway.
Other findings
After identifying that the approaching aircraft was aligned with the taxiway, the instructor on board the aircraft on the taxiway made a radio broadcast, likely alerting both the pilot and air traffic control to the situation.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future.
Safety action by Armada Aviation
Armada Aviation circulated a notice to its aircrew advising them of hazards associated with a visual approach, such as sun glare. Additionally, it made the following changes to its operating procedures:
Updated the final decision to proceed to landing to include a requirement that the runway was confirmed and clear by 400 ft above ground level, or the approach minima.
Added a top of descent safety briefing to ensure pilots brief other risks associated with the visual approach segment following an instrument approach, including lighting configuration and sun position.
Updated the checklist of the final phase of flight to include checking that the runway was confirmed and clear.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and operator
the pilot and operator of the aircraft on the taxiway
Bureau of Meteorology
Launceston Airport
Airservices Australia
recorded data from the electronic flight bag (EFB) on the aircraft.
References
Australian Transport Safety Bureau (ATSB) (2004). Limitations of the see-and-avoid principle, /sites/default/files/media/4050593/see_and_avoid_report_print.pdf, ATSB, accessed 13 June 2025
Hawkins, F.H. (1987). Human Factors in Flight, Gower, Aldershot.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and operator
the pilot and operator of the aircraft on the taxiway
Launceston Airport
Airservices Australia
Civil Aviation safety Authority.
Submissions were received from:
the operator.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, or R as required for left or right when there are parallel runways.
[2]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered.
[3]Missed approach / go-around: a standard aircraft manoeuvre that discontinues an approach to landing.
[4]Precision Approach Path Indicator (PAPI): a ground-based system that uses a system of coloured lights to visually identify the correct glide path to the runway when conducting an approach.
[5]Notice to Airmen (NOTAM): a notice containing information or instructions concerning the establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of which is essential to persons concerned with flight operations.
[6]Automatic terminal information service (ATIS): the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is updated either routinely or when there is a significant change to weather and/or operations.
[7]Crazing: Small, thin cracks or lines that can develop on the surface of an aircraft window.
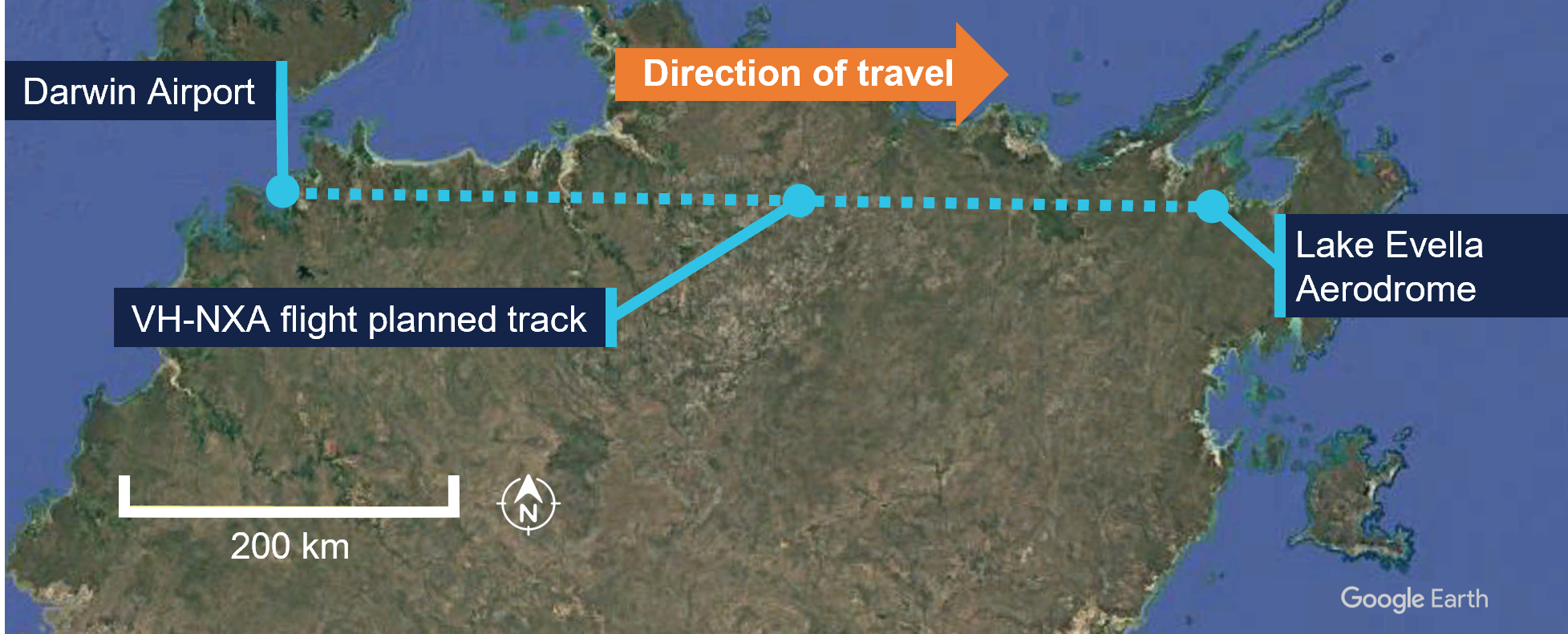
On 29 May 2025, a Cessna 310R, registered VH-NXA and operated by Marthakal Yolngu Airline, was conducting a non-scheduled passenger air transport flight from Darwin to Lake Evella, Northern Territory. On board were the pilot and 4 passengers.
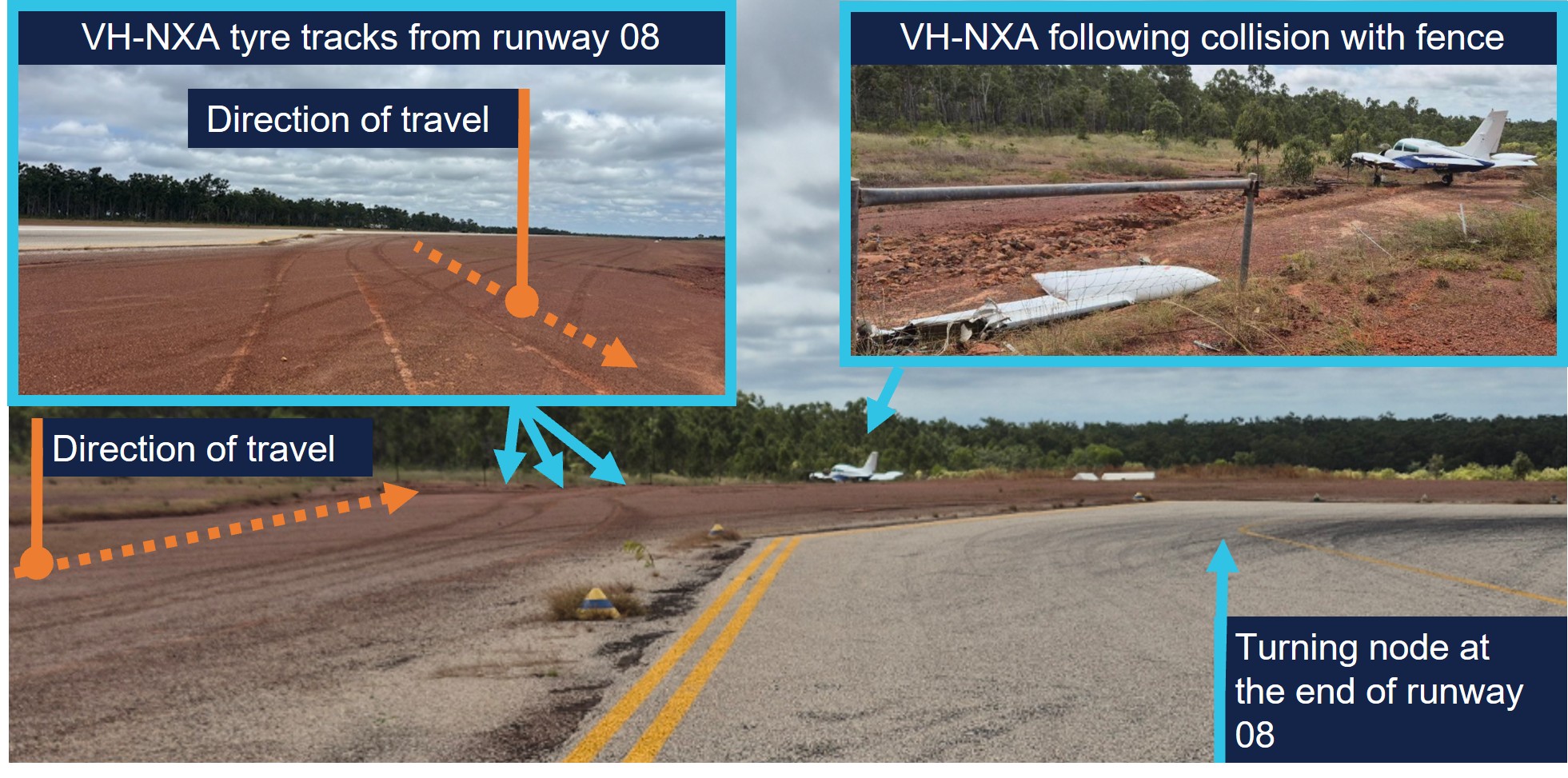
During the approach at Lake Evella Aerodrome, recorded data indicated that the aircraft touched down just prior to halfway along the runway. The pilot subsequently applied braking, but the aircraft did not decelerate as expected. This resulted in a runway excursion and the aircraft subsequently collided with a perimeter fence which substantially damaged the left wing. The pilot and 4 passengers were uninjured.
What the ATSB found
The ATSB found that the pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in the aircraft floating during the landing flare for a prolonged period in ground effect, and a landing beyond the planned touchdown point. After the aircraft touched down, the pilot subsequently commenced braking about halfway along the runway. The long landing reduced the available distance to decelerate on the runway.
At the aircraft’s landing weight, the remaining runway length should have provided sufficient stopping distance, but degraded braking capacity meant the aircraft could not be stopped before the runway end and it subsequently departed the runway.
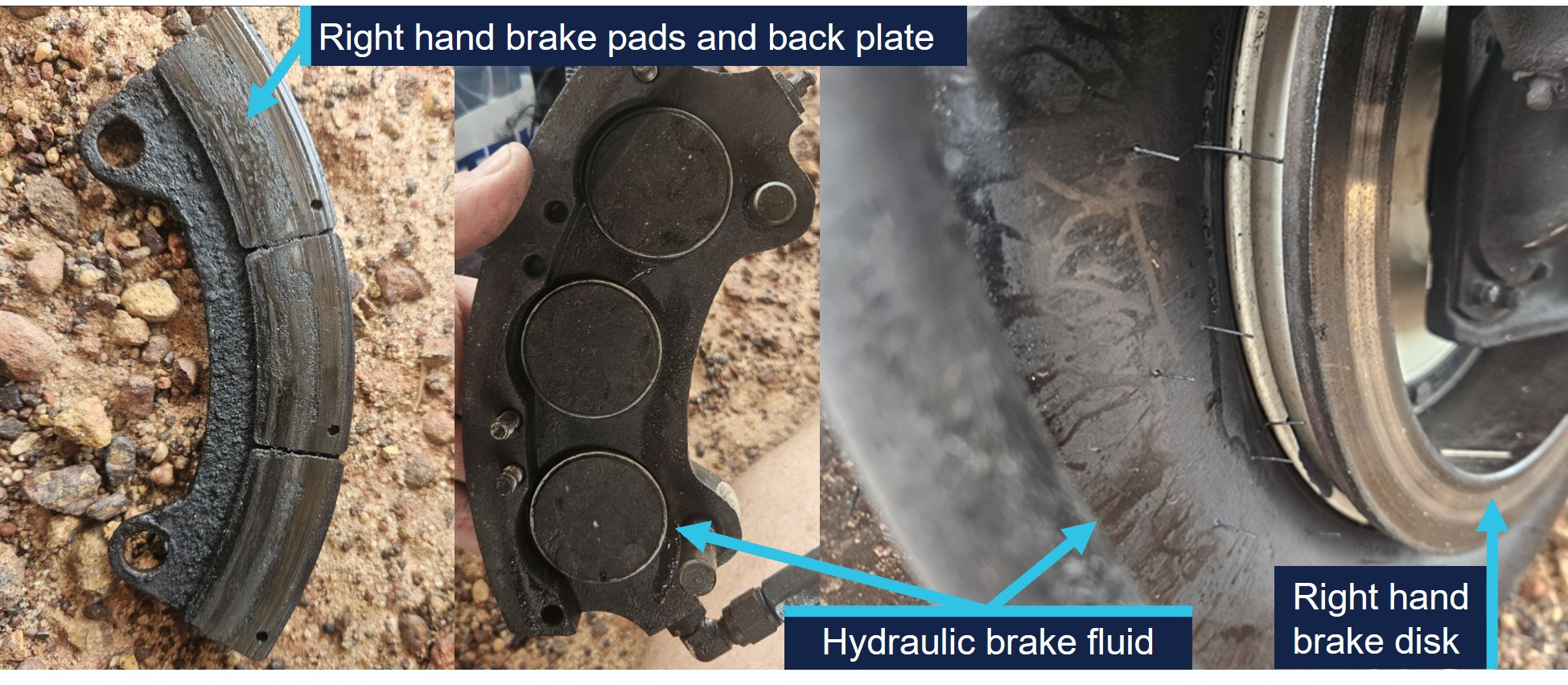
During a scheduled maintenance event prior to the occurrence, a licensed aircraft maintenance engineer believed an apprentice had replaced the main-wheel brake pads. An inspection after the occurrence found that the right brake reservoir was empty and that the right pads were worn beyond limits, which reduced braking capacity on that side.
The ATSB also identified that the operator’s procedures allowed the use of self-reported passenger weights without additional allowances, and that the electronic weight and balance system had been configured with higher maximum weights applicable to a modification not fitted to this aircraft. In combination with calculation errors on the day, this resulted in the aircraft being operated above the maximum permitted ramp and take‑off weights.
What has been done as result
Marthakal Yolngu Airline advised that all references to the use of self-reported passenger weights for the purposes of weight and balance calculations will be removed in the next amendment of the operations manual.
The operator also advised that the electronic weight and balance system will be amended to reflect the correct maximum weights for VH-NXA prior to its return to service.
The safety manager briefed company personnel about the proposed changes and advised existing pilots that actual weights for passengers must be used for all flights.
The ATSB will monitor these safety actions until the proposed changes to the operations manual and weight and balance system have been formally implemented.
D & T Aircraft Engineering advised that, following the occurrence, a debrief with maintenance personnel highlighted the importance of increased vigilance during inspections conducted after maintenance tasks, and that the organisation also identified opportunities to improve internal processes following similar occurrences.
Safety message
Factors such as additional airspeed over the threshold can result in a landing beyond the intended touchdown point, increasing the risk of a runway overrun excursion. While adherence to a pre-determined stabilised approach criteria can effectively mitigate such risks, pilots should always exercise vigilance and ensure the aircraft is flown within the assumed conditions used to calculate landing performance.
Pilots are therefore encouraged to continue to actively monitor the flight path using cockpit instrumentation and external visual cues until a safe landing is assured. This should include identifying and nominating an appropriate touchdown point on the runway to ensure a go‑around can be executed if a touchdown beyond this point is likely to occur.
Additionally, maintenance organisations should ensure that effective systems are in place to disseminate important information to all maintenance personnel, so that emerging defects are identified and rectified before they affect flight operations.
The occurrence
Pre-flight preparation
On the morning of 29 May 2025, a Cessna C310R, registered VH-NXA and operated by Marthakal Yolngu Airline, was being prepared for a non-scheduled passenger air transport flight from Darwin to Lake Evella, Northern Territory.
When the pilot arrived at the airport, they observed a licensed aircraft maintenance engineer (LAME) and their apprentice performing maintenance on the aircraft braking system. During this period the pilot prepared their flight plan and when they returned to the aircraft, the LAME and the apprentice had completed the maintenance.
The pilot, who was operating their first flight as pilot in command of a multi-engine aircraft, commenced their pre-flight checks. Due to the recent work on the braking system, they taxied to an aircraft bay to conduct a static engine run-up.[1]
With both engines at 1,700 RPM, they recalled that the aircraft moved forward slightly with the brakes applied. They physically increased their braking pressure, after which, the aircraft remained stationary. After completing the run-ups, the pilot taxied back to the terminal where the passengers were waiting. At this time, they also discussed the brakes with another C310 pilot who advised them that quite a lot of brake pressure was required during run-ups.
The pilot reported feeling rushed, and elected to use the self-reported passenger and baggage weights prior to boarding for weight and balance calculations, which were recorded on the manifest. These weights were entered into an electronic weight and balance system, which indicated that the planned load complied with the aircraft weight and balance limitations. The passengers were then taken to the aircraft where the pilot conducted a safety briefing before they boarded.
Occurrence flight
At 0857 local time, VH-NXA departed from Darwin Airport with the pilot and 4 passengers on board for Lake Evella (Figure 1). When approaching the Lake Evella Aerodrome, the pilot reported becoming visual with runway 08 at about 15 NM (28 km) and tracked for a straight in approach. At 1051, the aircraft was established on final approach for runway 08.
Figure 1: VH-NXA flight planned track
Source: Google Earth, annotated by the ATSB
The pilot recalled that there was a south-easterly wind between 8–10 kt for the approach, with a right crosswind component. Another pilot, who arrived at Lake Evella about 3 minutes after VH-NXA, recalled the wind was from an easterly direction at about 10 kt.
The pilot of VH-NXA recalled that the approach ‘seemed stable,’ (see Stabilised approach criteria) and stated that they generally used the runway threshold as their aiming point. They estimated crossing the threshold at their calculated approach speed of 90 kt or ‘just above.’
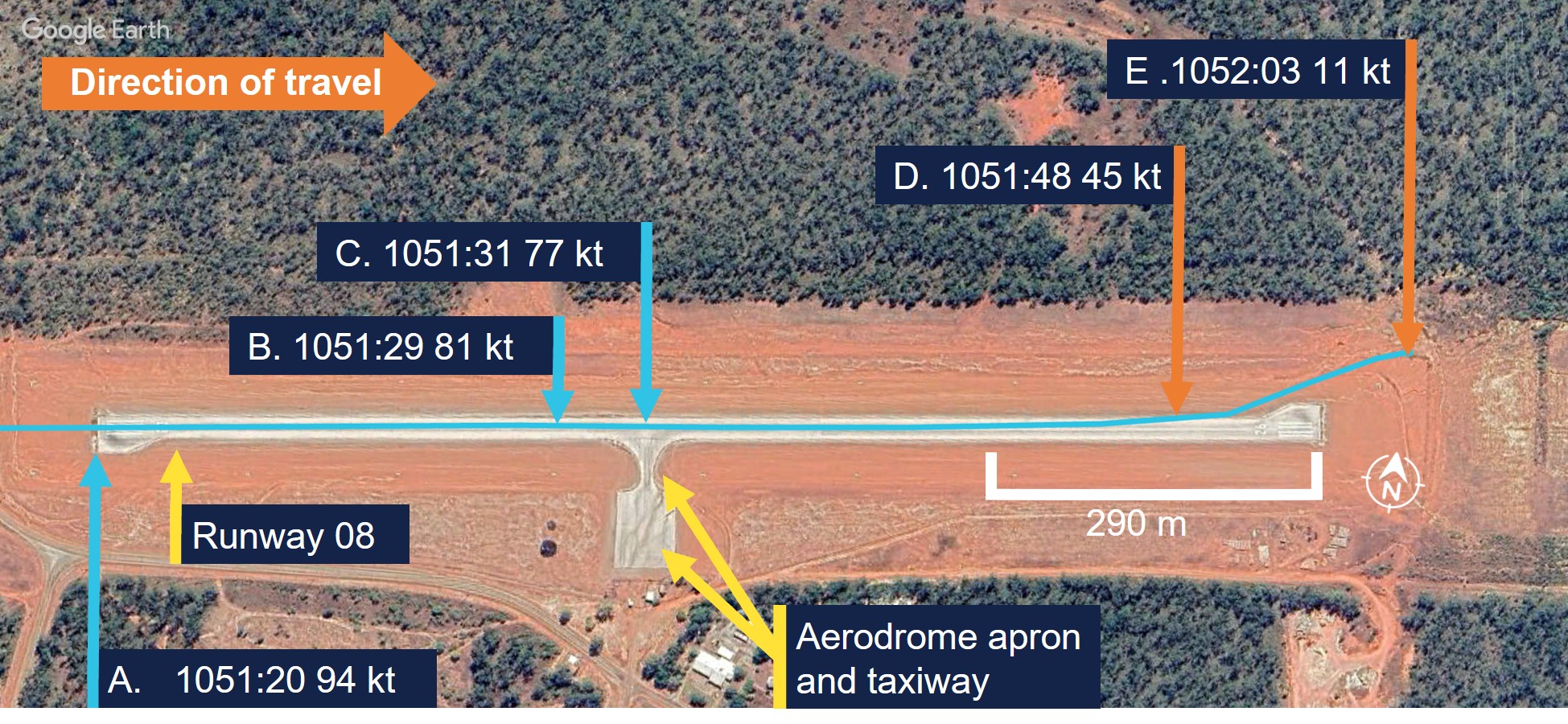
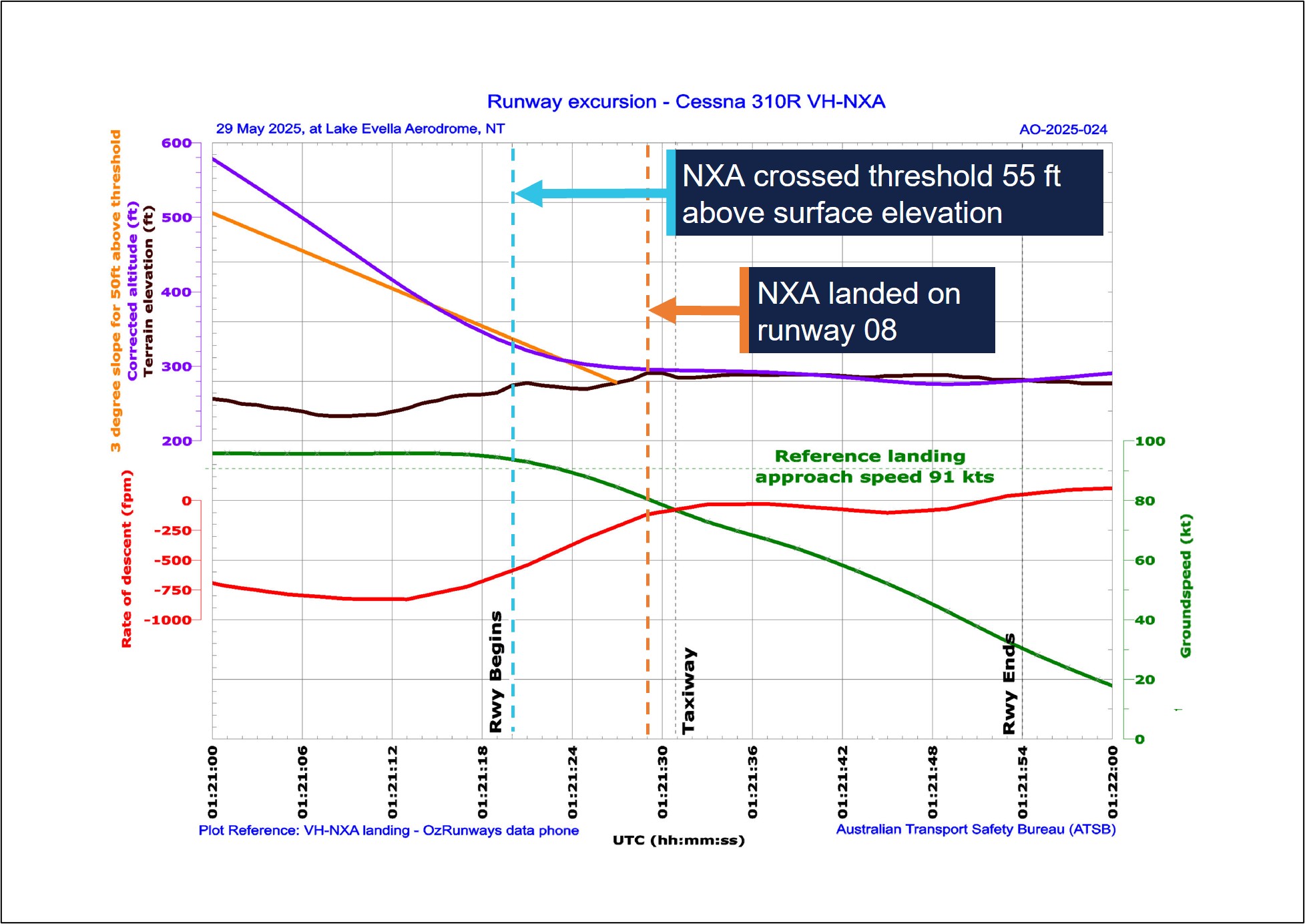
A navigational application (OzRunways) [2] was installed on a tablet computer and an Android phone on board the aircraft and broadcast flight data (see Recorded information). The OzRunways data taken from the Android phone, overlaid on a Google Earth image (Figure 2), showed the aircraft crossing the runway threshold at a height of 55 ft with a ground speed of 94 kt (Figure 2, A). The runway in Lake Evella was not equipped with visual slope guidance and the pilot relied on their visual assessment of ‘how the runway should look at certain height.’
Figure 2: VH-NXA ground speed at key points in landing sequence
Source: Google Earth, annotated by the ATSB
The pilot and the passenger seated directly behind them estimated that the aircraft touched down approximately 200 m past the threshold. ATSB analysis of recorded data indicated touchdown at 1051:29 (the corrected altitude of the aircraft matched the terrain elevation of runway 08), which was 402 m past the threshold (Figure 2, B). The passenger seated in the front row beside the pilot recalled passing the taxiway immediately after touchdown (Figure 2, C).
Another pilot on the ground standing at the apron who witnessed the landing reported observing VH-NXA a few feet above the ground in the ‘flaring attitude’ about a third of the distance along the runway. They also recalled that the aircraft was travelling faster than what they thought was normal and landed just beyond the taxiway (Figure 2, C).
The pilot reported that after touchdown, they applied the brakes passing the apron area about halfway along the runway (Figure 2, C). At that point, they reported that the aircraft did not appear to be slowing as expected and the passenger in the last row recalled the aircraft passing the apron ‘very fast’.
The pilot recalled increasing their braking pressure and when they saw the end of the runway approaching, they shut both engines down by selecting the mixture controls to idle cut-off. The pilot then elected to steer the aircraft to the left of the runway centreline to increase the runway distance for the deceleration required.
The aircraft departed the left side of the runway, 118 m from the runway end (Figure 2, D) (Figure 3, inset left), while the passenger seated beside the pilot verbally prompted the passengers to ‘brace.’ Recorded data indicated the aircraft was travelling at 45 kt at this point. The left wing subsequently collided with a fencepost (Figure 2, E) (Figure 3, inset right) located 193 m from the point the aircraft departed the runway.
Figure 3: VH-NXA ground roll following runway excursion
Source: Marthakal Yolngu Airline, annotated by the ATSB
Following the collision, the aircraft came to a stop and the pilot and passengers disembarked through the right cabin door. There were no injuries to the pilot or passengers, however the aircraft sustained substantial damage (see Post-accident inspection).
Context
Pilot information
The pilot held a Commercial Pilot Licence (Aeroplane) issued in 2021 and a class 1 aviation medical certificate. They also held a multi-engine aircraft class rating, which was issued in 2022 and renewed with a flight training organisation on 24 May 2025.
The pilot had accumulated 1,066 hours of total aeronautical experience, which included 71 hours of multi-engine time accumulated under the supervision of an instructor.
They reported they had flown about 70 hours in the last 90 days, including a total of 11.7 hours on the Cessna C310R, which was conducted during the course of their training.
The pilot’s training was conducted by a flight training organisation (FTO) in Darwin, on behalf of Marthakal Yolngu Airline. FTO training records detailed that the pilot commenced line training for the C310R on 15 May 2025.
This line training took place over 9.8 flight hours, after which they were assessed as proficient by a flight examiner during a combined line check and operator proficiency check for the C310R on 24 May.
The pilot had not operated the C310R to Lake Evella Aerodrome during the course of their training and had not operated there in any aircraft type prior to the occurrence. They reported sleeping about 8 hours the night before the occurrence and had been awake for about 7 hours at the time of the occurrence and feeling ‘fully alert.’
Aircraft information
The Cessna 310R is a twin-engine, low-wing (with a wingspan of 11.3 m), 6-seat, unpressurised aircraft equipped with retractable landing gear and powered by 2 Continental IO-520 piston engines. VH-NXA was manufactured in the United States in 1978 and first registered in Australia in 1989. A maintenance organisation located in Darwin became the registration holder on 4 March 2020.
Braking system
Section 7 of the Cessna 310R Pilots operating handbook (POH) contained the following description of the braking system:
The airplane is provided with an independent hydraulically actuated brake system for each main wheel. A hydraulic master cylinder is attached to each pilot’s rudder pedal. Hydraulic lines and hoses are routed from each master cylinder to the wheel cylinder on each brake assembly. No manual adjustment is necessary on these brakes. The brakes can be operated from either pilot’s or co-pilot’s pedals.
Meteorological information
The graphical area forecast and the applicable grid point wind and temperature forecast for the flight indicated:
prevailing visibility greater than 10 km
scattered cloud[3] with bases 1,500 ft above mean sea level (AMSL)
isolated areas of smoke reducing visibility to 5,000 m
isolated rain showers and thunderstorms reducing visibility to 2,000 m and 1,000 m respectively, and broken cloud with bases 800 ft above AMSL
moderate turbulence below 4,000 ft in thermals and dust/sand whirls (dust devils)
wind 130° at 21 kt and temperature of 24°C at 1,000 ft above AMSL.
Aerodrome information
Lake Evella Aerodrome (YLEV) is situated at an elevation of 278 ft AMSL and comprised of a single sealed runway, 08/26, measuring 1,065 m in length and 18 m in width and was sloped 0.5% up toward the east. The aerodrome is uncontrolled and operated on a dedicated CTAF,[4] and is subject to animal hazards.
Maintenance information
Aircraft maintenance manual
The Cessna 310R Aircraft maintenance manual (AMM) contained a troubleshooting guide to assist maintenance personnel to rectify defects relating to systems fitted to the aircraft. The section that covered the wheels and brakes included the following information (Table 1):
Check for brake linings worn beyond limits. Replace linings as required
Air in brake system
Check for air trapped in brake system. Bleed the brakes
Brakes spongy
Air in brake system
Check for air trapped in brake system. Bleed the brakes
The AMM also described the brake wear limits on the C310R, which included:
Check back plate and pressure plate linings for wear. If worn to a thickness of 0.125 to 0.100 inch, the linings should be replaced.
Scheduled maintenance
The aircraft was flown to Darwin on 15 February 2025, where the authorising licensed aircraft maintenance engineer (LAME) planned to conduct a corrosion inspection at their maintenance facility. The LAME also performed a ‘check 1’ inspection, which they stated was the equivalent of a 100-hour inspection.
During the inspections, additional maintenance was conducted due to leaking brake callipers, which was common to the brakes on the C310 according to the LAME. This involved the removal, bleeding, resealing and refitting of both callipers and was performed by an apprentice. It was also the LAME’s expectation that the brake pads would be replaced during this maintenance task because this was routine practice, although not in the procedure.
As part of the 100-hour inspection, the LAME performed an engine run-up and observed the aircraft did not hold under brakes at this time. Believing that they had been replaced, they believed that the new brake pads needed to be bedded or burnt in. The AMM stated ‘brake burn in is required to minimize glazing of the friction surfaces’ when new brakes are installed. They subsequently completed the engine run up on one engine at a time, which allowed the aircraft to remain stationary.
Following the completion of the inspections and associated maintenance tasks, including the additional work carried out on the brakes, the LAME certified the aircraft maintenance logbook on 26 May 2025.
The authorising LAME later stated that new brake pads should have been installed before the callipers were refitted to the landing gear, however they did not verify that this had occurred. They reported that the brake pads were last changed on 15 December 2023 and had 494 landings prior to the occurrence.
Pre-departure maintenance
The aircraft underwent a post‑maintenance verification flight the day prior to the accident flight, with a flight instructor and the occurrence pilot as an observer. After the flight, the instructor advised the LAME by text message that the brakes felt ‘spongy.’
On the morning of 29 May, prior to the accident flight, the LAME checked the aircraft brakes, reporting that they were acceptable, even though the brake pedal travel felt more than usual. The decision was made to bleed the brakes to remove any air or water in the brake lines and top up the brake fluid. With assistance from an apprentice during this process, the LAME reported that hydraulic fluid spilled onto the right tyre and was subsequently wiped down. The aircraft was then released back to service.
Post-accident inspection
Following the occurrence, the LAME inspected the aircraft at Lake Evella Aerodrome on 18 June 2025 and documented the aircraft damage. The aircraft had sustained significant damage to the left wing (Figure 4), which separated from the fuselage outboard of the left engine nacelle. The pitot tube, right tip tank, propeller and nose gear door were also damaged following the runway excursion.
Figure 4: VH-NXA damaged left wing
Source: Aircraft maintainer, annotated by the ATSB
The LAME found that the right brake reservoir was empty, with evidence of hydraulic fluid leakage on the right tyre, however stated that the right brake disc was serviceable.
They identified that the right brake pads were ‘heavily worn.’ Images supplied by the LAME also indicated the presence of hydraulic brake fluid, originating from the brake piston adjacent to the brake line (Figure 5). They also indicated that the hydraulic fluid on the tyre may have been from fluid spilling when the brakes were topped up on the morning of the occurrence flight.
Figure 5: VH-NXA right hand brake components and hydraulic brake fluid
Source: Aircraft maintainer, annotated by the ATSB
No defects were identified on the left brake system and the right brake calliper was removed and tested in Darwin by the LAME. The right brake calliper was bolted onto a brake disc with sufficient pressure applied to prevent calliper movement. After 13 days, sufficient hydraulic fluid had leaked, which allowed the calliper to be moved in relation to the brake disc. The LAME subsequently disassembled the right brake calliper and identified a ‘very small’ hydraulic fluid leak, which they did not consider was the cause of the fluid loss during the occurrence.
Operational information
Weight and balance
The operator’s standard operating procedures(SOP) stated that during the conduct of air transport operations, prior to each sector, the pilot in command must complete an aircraft load and trim sheet.
An operator‑approved electronic load sheet was available to pilots for the purpose of completing weight and balance calculations in accordance with the POH weight and balance limitations.
The operator’s Cessna 310R Flight crew operating manual (FCOM) included the following statement regarding the possible modification of company operated aircraft:
The Company operates C310R aircraft in several possible modification states, which may affect limiting weight.
The only modification listed in the FCOM that affected the weight limitations for VH-NXA was the fitment of a vortex generator (VG)[6] kit. The FCOM also contained information relating to the fitment of the VG kit including increased weight limitations, changes to various airspeeds and stated:
If less than 84 vortex generators are in place or undamaged, the aircraft must be operated in accordance with the original AFM performance data (ie nil VGs).
Electronic weight and balance system
The electronic weight and balance system was developed by a third party to calculate the weight and balance for each flight. In the system, each aircraft was configured with a weight and moment arm[7] when empty.
The pilot would enter the pilot and passengers’ weights, their seating positions and fuel to calculate both the weight and centre of gravity of the aircraft at take-off and landing. The system was designed to alert the user if any weight and balance limitations were exceeded.
For VH-NXA, the electronic weight and balance system incorporated an increase in weight in accordance with a supplemental type certificate number for a C310R VG modification. However, the maintenance organisation that owned and maintained the aircraft stated that VH-NXA had not been fitted with the VG modification, and they were not aware of any modifications that increased the standard maximum permitted weights as prescribed in the POH.
As a result, the weight and balance system contained the following increases to the standard POH weight limitations which were not applicable to the aircraft (Table 2):
Table 2: Cessna 310R maximum weights
POH limitation
Standard weight (kg) applicable for VH-NXA
C310R with VG kit (kg) as listed for VH-NXA
Maximum zero fuel weight
2,222
2,386
Maximum ramp weight
2,510
2,586
Maximum take-off weight
2,494
2,563
Maximum landing weight
2,449
2,449
Passenger-declared weights
The operator’s SOP stated that for the purposes of calculating the aircraft’s weight and balance, ‘passenger weights must be actual, or self-reported.’ Following the occurrence, a passenger reported that their body and baggage weights were requested without the use of a calibrated scale. The pilot did not indicate that any adjustments of additional amounts were applied to the passenger reported weights.
The CASA multi-part AC 121-05, AC 133-04 and AC 135-08 – Passenger crew and baggage weights, described acceptable weight calculation methods that could be defined in operating procedures. The circular stated that:
The use of actual weights is the most accurate method of maximising payload capacity. Appropriately calibrated weighing scales should be used. Actual weighing is more commonly used by Part 133 [helicopter passenger transport] and 135 [smaller aeroplane passenger transport] operators. This is, in part, due to the smaller number of passengers being carried, which makes this option less disruptive than it is for Part 121 [larger aeroplane passenger operations] operators.
Operators should have procedures to identify when passenger-declared weights are not appropriate, such as when operating close to limitations. Under these circumstances, the use of actual weights may be required to ensure limitations are not exceeded.
Passenger-declared weights have inherent inaccuracies as passengers may not know their actual weight, especially when fully dressed. An adjustment allowance should be added to any passenger-declared weight, as a factor or a fixed additional amount.
Weight and balance calculations
Following a review of documentation provided by the operator and pilot, the ATSB identified several discrepancies contained in the operational documentation from the day of the occurrence.
The passenger and baggage weights recorded in the manifest by the pilot indicated a combined weight of 387 kg. However, the corresponding load sheet indicated a combined passenger and baggage weight of 337 kg (excluding the pilot).
Additionally, the fuel plan prepared by the pilot indicated a total fuel figure of 441 kg. By comparison, the fuel figure on the load sheet was recorded as 432 kg.
Due to the identification of the combined discrepancy of 59 kg, the ATSB recalculated the aircraft’s weight and balance for the flight. This identified the following updated weights and exceedances (Table 3) prescribed in the POH for aircraft not fitted with a VG kit.
Table 3: VH-NXA calculated weights and exceedances
Item
POH weight limitation (kg)
Pilot-calculated weight (kg)
ATSB-calculated weight (kg)
ATSB-calculated exceedance (kg)
Zero fuel weight
2,222
2,087
2,137
Nil
Ramp weight
2,510
2,519
2,578
68
Take-off weight
2,494
2,510
2,569
75
Landing weight
2,449
2,339
2,367 [1]
Nil
[1] The re-calculated landing weight was based on pilot reported fuel remaining added to the ATSB calculated zero fuel weight.
Landing performance calculations
The operator’s SOPs stated that company aircraft are subject to the requirements of Civil Aviation Safety Regulations Part 135 Manual of Standards (MOS) with respect to take-off and landing performance requirements. Chapter 10 of the Part 135 MOS stipulated ‘that the aeroplane crosses the runway threshold at a height of 50 ft’ unless an approved short landing operation was being conducted. Additionally for landing, the FCOM stated that the reference landing approach speed (Vref)[8] should be achieved at 50 ft above the landing surface.
For aeroplanes, take-off and landing distance calculations to determine maximum take‑off weight or the maximum landing weight are achieved through a manual calculation using the limitations given in the POH for the specific aircraft type, taking into account:
environmental conditions
runway length.
The FCOM also required pilots to apply landing distance factoring of 1.20 for all calculations. The pilot stated they had calculated their landing performance based on the aircraft’s maximum landing weight and calculated a factored landing distance of 680 m on the flight plan with a Vref of 90 kt for their landing at Lake Evella.
Calculations using the ATSB recalculated landing weight and the estimated ambient conditions at the time of the occurrence determined that the required landing distance (with the 1.20 factoring) with a 50ft threshold crossing height was 659 m. This figure included a landing ground roll distance of 195 m and a corresponding Vref of 91 kt.
Stabilised approach criteria
The SOPs stated that, ‘unless the aircraft meets stabilised approach criteria at the specified altitude, a missed approach must be executed.’
A stabilised approach was described in the SOPs as an approach to land that met a number of criteria by 300 ft above the runway during a visual approach. These included the following:
• the aircraft is on the correct flight path
• only small changes in heading & pitch are required to maintain the correct flight path
• the aircraft speed is Vref to Vref +20 kt
• sink rate is not greater than 1,000 fpm or pre-briefed limits.
Recorded information
The pilot used a flight planning application (OzRunways) on an iPad and an Android phone for en route flight planning and navigation. The flight planning software provider was an approved source of electronic aeronautical charts, however the application could not be used as a primary means of GPS-based navigation as the iPad and Android phone GPS did not meet certification for aviation use. The pilot reported that the iPad was placed on the floor for the approach while the Android phone was in their chest pocket. By examining the combination of groundspeed and derived deceleration data, in addition to the best direct line of sight to satellites, it was assessed that the Android data had the highest positional accuracy.
The recorded data had limitations due to an altitude resolution of 100 ft, while filtering and adjustments were also applied to smooth the data and are known to affect the accuracy of small sections. Additionally, the altitude data of VH-NXA was corrected to match the terrain elevation during the landing ground roll (Figure 6).
Based upon the operator’s stabilised approach criteria, the decision to continue the approach, or conduct a go-around, became applicable by the time the aircraft reached 300 ft above the runway.
The following recorded parameters were observed from below 300 ft to the threshold:
the aircraft crossed the threshold of runway 08 at a height of 55 ft
aircraft speed remained within Vref to Vref +20 kt
sink rate (vertical speed) less than 1,000 fpm.
The recorded data indicated (purple line in Figure 6) that at the 300 ft (578 ft corrected altitude) stabilised approach gate, the aircraft was about 42 ft above the normal 3 degree slope (orange line), and remained above it until reaching 104 ft above the aerodrome elevation. During this period, the sink rate exceeded 800 fpm for 8 consecutive seconds between 1051:06 and 1051:14 local time.
At 1051:20, the aircraft crossed the threshold with a groundspeed of 94 kt. The pilot reported the wind component during the approach was a south-easterly wind between 8–10 kt, which would have resulted in a 3–4 kt headwind component. Accordingly, the aircraft’s airspeed was likely around 97–98 kt as it crossed the runway threshold, which was 6–7 kt above the Vref of 91 kt.
At 1051:29, the corrected altitude of the aircraft matched the terrain elevation, which indicated that the aircraft landed 402 m along the runway with a groundspeed of 81 kt. The pilot reported applying brakes as the aircraft passed the apron area, which occurred about 2 seconds after touchdown. Following a ground roll distance of about 540 m, the aircraft decelerated to a groundspeed of 45 kt when it vacated the left side of the runway at 1051:48.
Figure 6: VH-NXA approach and landing
All times are coordinated universal time (UTC). Local time was Central Standard Time (CST), which was UTC +9 hours and 30 minutes. The aerodrome elevation is 278 ft. Source: ATSB, data provided by OzRunways and Google Earth
On 2 November 2024, a GippsAero GA8-TC Airvan, was being used to conduct a scenic flight from Whitsunday Airport (Shute Harbour), Queensland. During the landing the aircraft departed the upwind end of the runway before entering marshy ground and coming to a stop in a ditch.
The ATSB investigation identified that the aircraft's approach was above profile with a high airspeed and the pilot had an incorrect understanding of the required approach speed. Subsequently, the pilot did not initiate a go-around, resulting in a landing beyond the planned touchdown point. The ATSB also identified that the operator’s weight and balance system used an incorrect empty weight moment arm to calculate the aircraft's centre of gravity, and passengers were not weighed in accordance with its procedures.
Safety analysis
On the morning of 29 May 2025, a Cessna 310R, registered VH-NXA, was being operated by Marthakal Yolngu Airline on a non-scheduled air transport flight from Darwin to Lake Evella, Northern Territory, with a pilot and 4 passengers on board.
During a straight-in visual approach, without visual slope guidance to runway 08 at Lake Evella, the pilot assessed that the approach was stable and continued with the landing. After the aircraft crossed the runway threshold, it floated for a prolonged period and subsequently landed before reaching a taxiway located about halfway along the runway.
When the pilot applied braking passing the airport’s apron area, the aircraft did not decelerate as expected. The aircraft subsequently overran the runway and collided with a fence. The pilot and passengers were uninjured, however, the aircraft sustained substantial damage.
This analysis examines how the condition of the aircraft braking system, and the conduct of the approach and landing, contributed to the runway excursion. It also explores the operator’s self-reported passenger weight procedures and electronic weight and balance system, and how the latter, in combination with incorrect pre-flight weight calculations, led to the aircraft being operated above the weight limits specified in the pilot’s operating handbook.
Pre-flight maintenance
Maintenance which was completed on the aircraft 3 days before the occurrence involved numerous concurrent tasks. These were conducted by a licensed aircraft maintenance engineer (LAME) with the assistance of an apprentice. One of the tasks involved the apprentice conducting maintenance on the braking system due to leaking brake callipers. It was the LAME’s expectation that the apprentice had replaced the main wheel brake pads during this maintenance task.
This expectation influenced their assessment that the aircraft rolled forward during post‑maintenance engine run-ups, due to the new brakes requiring ‘burning in.’ In this case, a physical verification of the brake pads was not conducted as a result.
On the morning of the occurrence, the LAME carried out corrective maintenance in response to the flight instructor text message report of ‘spongy brakes’ the day prior. While the occurrence pilot was aware of this report, they were not aware of the LAME’s experience with the aircraft rolling forward during the engine run-up.
When the pilot commenced the pre-flight engine run-up for the occurrence flight, the brakes failed to keep the aircraft stationary. The pilot physically increased the brake pressure and successfully kept the aircraft stationary, but did not advise maintenance personnel. The pilot’s limited experience on multi-engine aircraft led them to consider that this might be normal, which was reinforced during a brief discussion with another Cessna 310 pilot.
Gaps in communication and incorrect assumptions allowed a latent defect to persist into operation, contributing to the runway overrun in this occurrence.
Contributing factor
The certifying licensed aircraft maintenance engineer did not verify that the brake pads had been replaced by an apprentice during scheduled maintenance, which resulted in the aircraft being returned to service with worn brake pads on the right brake system.
Approach
Lake Evella Aerodrome was not equipped with visual slope guidance, and as a result, the pilot relied on their assessment of visual cues of the runway itself to assess whether they were on the correct approach path while they typically used the runway threshold as their aiming point.
Recorded data from the pilot’s Android phone indicated that the aircraft was higher than the usual 3 degree ‘correct flight path’. The rate of descent exceeded 800 fpm for a period of 8 consecutive seconds until the aircraft descended below 140 ft relative to the runway. At the time, the pilot recalled the approach ‘seemed stable,’ while the operator’s stable approach criteria permitted rates of descent up to 1,000 fpm.
The aircraft subsequently crossed the threshold of runway 08 at a height of 55 ft with a ground speed of 94 kt. ATSB analysis concluded that the aircraft’s airspeed was likely 6–7 kt above the Vref for the recalculated landing weight 91 kt.
When the aircraft neared the point of touchdown, it was subjected to ground effect, which meant that excess airspeed at the point of flare would result in a considerable float distance due to the reduction in drag and lack of power-off deceleration in ground effect (Federal Aviation Administration, 2023).
Additionally, landing distances provided in the aircraft flight manual are based on the aircraft achieving Vref (plus wind and gust additives) at 50 ft above the runway surface. As a result, any additional airspeed will result in a later touchdown and reduce the remaining landing distance available (Federal Aviation Administration, 2023).
In this case, the additional airspeed crossing the threshold likely resulted in a prolonged float in ground effect. This resulted in the aircraft touching down 402 m beyond the runway threshold which was the pilot’s usual aiming point. Subsequently, the pilot applied braking about 2 seconds after the touchdown, at which point, there was about 585 m of remaining distance available to decelerate on the runway.
Contributing factor
The pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in a landing beyond the planned touchdown point, and the pilot applied braking about halfway along the runway, which reduced the available distance to decelerate on the runway.
Excursion
The pilot first became aware of an issue with the braking system when they applied brake pressure during the landing roll with about 585 m of runway remaining. Witness accounts recalled the aircraft was travelling at high speed as it passed the taxiway and apron area without any significant deceleration. Additionally, recorded data showed the aircraft only slowed from 81 kt at touchdown to 45 kt when it vacated the left side of the runway following a ground roll distance of about 540 m.
At the aircraft’s landing weight, the ATSB calculated ground roll distance required was 195 m, which was sufficient to bring the aircraft to a stop within the remaining length of the runway had the brakes been functioning correctly. However, the loss of hydraulic brake fluid and the worn brake pads on the right-hand brake reduced the available braking capacity. As a result, the braking capacity was insufficient to arrest the aircraft’s forward momentum before the end of the runway. The pilot attempted to increase the available stopping distance by steering left and departing the runway, however it was insufficient, and the aircraft subsequently collided with the perimeter fence.
Contributing factor
Due to the worn right brake pad and the lack of hydraulic fluid in the right brake system, there was insufficient braking capacity available to prevent a runway overrun following the landing and the application of brakes about halfway along the runway.
Passenger weights
The operator’s exposition permitted the use of self-reported passenger weights for weight and balance calculations, without requiring the application of additional allowances or validation. This practice introduced errors into the weight and balance data used for pre-flight planning.
Research has found that people tend to underestimate the weights of themselves and others. Further, people are less accurate at estimating the weight of others than they are of themselves.[9] To cater for the variation in weight, it is recommended that operators weigh passengers or apply adjustment factors to self-reported values (Civil Aviation Safety Authority, 2025). In contrast, the operator’s reliance on unadjusted self-reported passenger and carry-on baggage weights provided no systematic mitigation for potential inaccuracies, which increased the likelihood that the aircraft would be operated overweight or at centre of gravity limits outside the manufacturer’s requirements.
Other factor that increased risk
Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations. (Safety issue)
Electronic weight and balance
The operator used an electronic weight and balance system to calculate aircraft loading data for each aircraft in operation. In that electronic system, VH-NXA had been configured with the higher maximum weight limits applicable to aircraft fitted with a vortex generator (VG) modification. However, the aircraft did not have the specified modification installed. Consequently, the programmed maximum zero-fuel, ramp and take-off and weights in the system exceeded those authorised in the aircraft’s POH.
This configuration error meant the electronic weight and balance system allowed VH‑NXA to be loaded in excess of the certified weight limitations, while still indicating that the loading complied with those limitations. This created an ongoing risk that the aircraft could be operated above the approved maximum weights.
Other factor that increased risk
Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations. (Safety issue)
Weight exceedances
During the occurrence flight, the aircraft was operated above the certified maximum ramp and take-off weights due to cumulative errors in the pilot’s weight and balance calculations. As a result of the configuration errors in the electronic weight and balance system, no alert to the overweight condition was made.
The pilot, who was conducting their first multi-engine command flight, reported feeling rushed during pre-flight preparation, which likely reduced the opportunity for careful verification of passenger weights, totals and data entry. Review of the weight and balance documentation from the occurrence identified multiple inaccuracies, indicating that the overweight condition arose from a breakdown in the usual cross-checking processes rather than a single isolated error.
Although the overweight condition did not result in the aircraft exceeding its maximum landing weight, operating above certified weight limits is known to increase take-off and landing distances and degrade braking performance. Additionally, excessive weight reduces the available safety margin if an in-flight emergency condition should arise (Federal Aviation Administration, 2016).
Other factor that increased risk
The aircraft was operated overweight due to incorrect weight and balance calculations, as well as errors in the electronic weight and balance system.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway excursion involving Cessna 310, VH-NXA, at Lake Evella Aerodrome, Northern Territory, on 29 May 2025.
Contributing factors
The certifying licensed aircraft maintenance engineer did not verify that the brake pads had been replaced by an apprentice during scheduled maintenance, which resulted in the aircraft being returned to service with worn brake pads on the right brake system.
The pilot conducted the approach above the standard profile and crossed the threshold above the normal approach speed. This resulted in a landing beyond the planned touchdown point, and the pilot applied braking about halfway along the runway, which reduced the available distance to decelerate on the runway.
Due to the worn right brake pad and the lack of hydraulic fluid in the right brake system, there was insufficient braking capacity available to prevent a runway overrun following the landing and the application of brakes about halfway along the runway.
Other factors that increased risk
Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations. (Safey issue)
Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations. (Safey issue)
The aircraft was operated overweight due to incorrect weight and balance calculations, as well as errors in the electronic weight and balance system.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Marthakal Yolngu Airline’s procedures did not require that additional allowances were applied when using self-reported passenger weights for weight and balance calculations.
Safety issue description: Marthakal Yolngu Airline’s electronic weight and balance system used incorrect maximum weights for the aircraft, which increased the risk of flight crew operating the aircraft above the certified weight limitations.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by D & T Aircraft Engineering
D & T Aircraft Engineering advised that, following this occurrence, a debriefing was conducted with maintenance personnel to discuss key learnings. It was acknowledged that increased vigilance would be exercised in the future to ensure that aircraft components are carefully inspected and confirmed to be in a serviceable condition following the completion of maintenance tasks. Additionally, the organisation stated that it would prioritise accessing the aircraft at the earliest opportunity in the future to assist in identifying potential causes of component failure, particularly in cases where perishable evidence plays a critical role in determining the cause.
Glossary
AFM
Aircraft flight manual
AMM
Aircraft maintenance manual
AMSL
Above mean sea level
CASA
Civil Aviation Safety Authority
FCOM
Flight crew operating manual
FTO
Flight training organisation
LAME
Licensed aircraft maintenance engineer
MOS
Manual of Standards
POH
Pilots operating handbook
RPM
Revolutions per minute
SOP
Standard operating procedures
VG
Vortex generator
VMC
Visual meteorological conditions
VREF
Reference landing approach speed
Sources and submissions
Sources of information
The sources of information during the investigation included:
Ramos , E., Lopes, C., & Barros , H. (2009). Unawareness of weight and height – the effect on self-reported prevalence of overweight in a population-based study. The Journal of Nutrition, vol. 13, pp.310–314.
Reed, D., & Price , R. (1998). Estimates of the heights and weights of family members: accuracy of informant reports. International Journal of Obesity, vol. 22, pp.827–835.
Shapiro , J. R., & Anderson, D. A. (2003). The effects of restraint, gender, and body mass index on the accuracy of self-reported weight. International Journal of Eating Disorders, vol. 34, pp.177–180.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot of the accident flight
the operator
maintenance organisation
Civil Aviation Safety Authority
Bureau of Meteorology.
Submissions were received from:
pilot of the accident flight
the operator maintenance organisation
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Run-up: a high power run-up check is carried out in a piston-engine aircraft to check the aircraft’s ignition and other systems before commencing an initial take off.
[2]OzRunways is an approved data provider for Australian pilots for flight planning and in-flight navigation.
[3]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered
[4]Common traffic advisory frequency (CTAF): A designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled aerodrome or within a broadcast area.
[5]Brake linings: brake linings, often referred to as brake pads, are the friction material that, when pressed against the brake discs, slows and stops the aircraft. Over time and with use, these linings wear down and require replacement.
[6]A vortex generator installation typically offers the advantages of reduced stall speeds, reduced minimum single engine control speed (Vmc), improved take-off and landing performance and increased maximum take-off weight.
[7]Moment arm: the horizontal distance from a reference datum to the centre of gravity of an item.
[8]Reference Landing Approach Speed: The airspeed used on approach down to 50 ft above the runway when determining landing distances which is normally 1.3 times the stall speed.
[9]For example, see Ramos and others (2009), Reed and Price (1998), Sahyoun and others (2008) and Shapiro and Anderson (2003).
The pilot of a fire surveillance aircraft that collided with terrain near Cloncurry, north‑west Queensland, was almost certainly hypoxic due to a known defect with the aircraft’s pressurisation system, the ATSB has found.
The AGAIR‑operated twin turboprop Gulfstream 695A (a variant of the Aero Commander aircraft series) had taken off from Toowoomba to map fire zones near Mount Isa on 4 November 2023, with a pilot and two camera operators on board.
“Over a period of many months, the accident aircraft’s pressurisation system was not reliably maintaining the required cabin altitude. This led some company pilots to employ a variety of actions in the aircraft to manage the potential and deadly effects of hypoxia, including at times briefly descending to lower altitudes, and improperly using emergency oxygen systems,” ATSB Chief Commissioner Angus Mitchell said.
Early in the accident flight, the pilot had descended from 28,000 ft to 15,000 ft for about 6 minutes, before climbing back to 28,000 ft.
Later, while the aircraft was nearing Cloncurry at 28,000 ft, both power levers were probably reduced, possibly with the intention of undertaking a similar descent profile. This caused the aircraft’s speed to decay, before it ultimately entered a steep, descending, anticlockwise turn.
At around 10,500 ft the aircraft transitioned from the steep descent into an unrecoverable aerodynamic spin, until it impacted terrain, fatally injuring all on board.
The transition from steep descent to unrecoverable spin was almost certainly due to pilot control inputs made in an unsuccessful attempt to regain controlled flight.
“The ATSB found the onset of hypoxia during the flight significantly degraded the pilot’s ability to safely operate the aircraft, and it is possible that at stages the pilot also experienced some loss of consciousness,” Mr Mitchell said.
Air traffic control recordings of the pilot’s speech during the accident flight demonstrated significant and progressive impairment, including slowed, stuttering and flat speech, operational mistakes and signs of confusion.
“Hypoxia can occur when an individual is exposed to high altitudes, typically above 10,000 ft, when not enough oxygen is supplied to the blood, tissues and cells for the body and brain to properly function,” Mr Mitchell said.
ATSB examination of maintenance documentation and relevant internal correspondence confirmed the aircraft had a long‑term intermittent defect with the pressurisation system. At times this manifested as a reduced maximum attainable cabin differential pressure, exposing the cabin occupants to a relative altitude known to induce hypoxia.
“The intermittent defect was known about by AGAIR senior management, who attempted to have it rectified,” Mr Mitchell said.
“However, they did not formally record the defect, communicate it to the safety manager, undertake a formal risk assessment of it, or provide explicit procedures to pilots for managing it.
“Instead, AGAIR management personnel participated in and encouraged the practice of continuing operations in the aircraft at a cabin altitude of 19,000 ft, and as such required the use of oxygen, without access to a suitable oxygen supply.”
Correspondence and flight data showed the accident pilot had normalised the practice of managing the intermittent pressurisation issue by undertaking short descents to lower altitudes, and by using the aircraft’s emergency oxygen system.
“This represented a practice of using a critical safety system designed for emergency use only, in order to continue a commercial activity,” Mr Mitchell said.
The ATSB’s investigation report details that about 1 hour and 50 minutes into the flight, while the aircraft was in the cruise at 28,000 ft, air traffic control (ATC) lost radio contact with the pilot.
Over the following 30 minutes, ATC made multiple attempts to re‑establish contact with the pilot, including using alternate frequencies and relaying messages via a military aircraft in the vicinity.
ATC eventually contacted the pilot on their mobile phone, and during that brief conversation, the controller noted the pilot’s speech was slow and flat. As a result, the aircraft’s status was upgraded to ‘alert phase’ and procedures for a hypoxic pilot emergency were initiated. Contact was again lost with the aircraft, and over the next 13 minutes multiple emergency radio broadcasts were made by ATC and the military aircraft in the vicinity.
During this ‘alert phase’, ATC phoned AGAIR management to raise concerns about the pilot experiencing hypoxia.
“In this conversation critical safety information about the known intermittent pressurisation defect in the aircraft was not relayed to ATC, had it been done so at that time, the aircraft could have been directed to a lower, safer, altitude when contact was re‑established with the pilot shortly afterwards.”
Soon after that call, when contact was made, the pilot confirmed that their oxygen system was operating normally.
Based on this advice from the pilot, and with no knowledge of the aircraft’s known pressurisation defect, the possibility of hypoxia was not re‑established a short time later when the pilot mispronounced words and repeated a clearance four times.
The investigation subsequently found there was no guidance in the ‘hypoxic pilot emergency checklist’ used by Airservices on ceasing an emergency response. This increased the risk during a potential hypoxia scenario of inappropriately downgrading the emergency response.
Since the accident, Airservices Australia has advised that it is in the process of conducting a review of the hypoxia in‑flight emergency response checklist.
Meanwhile, the ATSB has issued a formal safety recommendation to AGAIR to initiate an independent review of its organisational structure and oversight of operational activities to implement ongoing effective operational control by management.
Concluded Mr Mitchell, “This was a tragic and entirely unnecessary accident that underscores the dangers of operational practices which circumvent critical safety defences, and the insidious and deadly potential of altitude hypoxia.”
A Queensland Rail network control officer was not alerted by a SPAD alarm when a Brisbane suburban passenger train passed a stop signal after its driver was briefly impaired, an ATSB final report details.
During the morning peak on 24 May 2023, a suburban passenger train passed a stop signal between Brisbane’s Fortitude Valley and Bowen Hills stations when its driver (who later tested positive for COVID) was impaired by a sudden sneezing fit.
The driver identified the signal as they went past it and applied the emergency brake, with the train stopping 64 m beyond the signal. The driver then made an emergency radio call to network control.
The next signal was also at stop, providing protection to the rear of the next train, which was about 300 m in front.
An ATSB investigation found the driver had acknowledged an automatic warning system (AWS) alert as the train approached the stop signal, but did not then recognise the signal at stop, or later recall acknowledging the AWS alert.
“This was likely influenced by the habitual nature of AWS alerts, which were the same for all types of restricted indications and frequently presented during traffic congestion, as well as the driver’s brief impairment,” ATSB Chief Commissioner Angus Mitchell explained.
“This and other incidents investigated by the ATSB have demonstrated the potential limitations of AWS alerts to prevent signal passed at danger (SPAD) events such as this one.”
The ATSB’s investigation also found that due to inherent constraints in operator Queensland Rail’s signalling system, the network control officer was not alerted to the SPAD by a SPAD alarm, and would therefore not have been able to intervene.
In these situations, the final report notes, the emergency response is reliant on the driver self-reporting the SPAD to the network control officer, a control which is ineffective in scenarios where the driver misses the limit of authority.
“In most train-to-train collision scenarios, the accident is preceded by at least one train travelling through a stop signal,” Mr Mitchell said.
“Eliminating these SPAD events is therefore a key focus for rail industry participants, in particular operators, towards reducing the risk of accidents.”
The ATSB’s investigation found Queensland Rail’s risk register for SPADs did not assess the inherent constraints in the signalling system demonstrated by this incident.
“The ATSB considers a scenario where a SPAD alarm is not presented to the network control officer, and the driver is not aware of the SPAD, has not been considered in Queensland Rail’s risk assessments,” Mr Mitchell said.
The ATSB is subsequently recommending Queensland Rail reviews the risk associated with a SPAD in these circumstances and consider any risk controls that may be appropriate.
Queensland Rail continues to maintain the current risk control arrangements, in conjunction with the AWS functionality, to manage the risk of SPADs while the preferred engineering control of European Train Control System (ETCS) technology is being implemented. Until this occurs, the ATSB’s recommendation says, the established risk will remain.
“These types of limitations should be eliminated where possible,” Mr Mitchell said.
“Where that is not possible, the hazards they create should be considered in risk assessments related to SPAD and collision prevention.”
Incomplete change management processes contributed to a Batik Air 737 descending below minimum safe altitude during the airline’s inaugural Denpasar to Canberra service last year, an ATSB investigation has found.
Early on 14 June 2024, the Batik Air Boeing 737‑800 was descending for what would be the operator’s first scheduled landing in Canberra, an ATSB final report details.
Strong tailwinds during a flight from Denpasar put the aircraft significantly ahead of schedule, set to land before 0600 local time when Canberra Tower and Approach air traffic control services were not yet being provided.
The flight crew opted to proceed without delay, and to land using common traffic advisory frequency (CTAF) procedures, where pilots make positional radio broadcasts and coordinate self‑separation with other traffic.
While still in airspace being controlled by Melbourne Centre air traffic control, the aircraft approached the AVBEG waypoint north-west of Canberra and the flight crew planned to use the AVBEG 5A standard arrival route (STAR).
STARs use satellite-based positioning waypoints to transition aircraft from en route flight to, in this case, an initial approach fix waypoint for Canberra Airport’s instrument landing system approach, to land on runway 35.
“The crew did not request, nor were they provided clearance to use this route by Melbourne Centre,” ATSB Chief Commissioner Angus Mitchell said.
“Air traffic control in Melbourne expected them to follow their cleared track direct to Canberra, which would have descended the aircraft out of controlled airspace as it approached Canberra.
“Instead, the crew deviated from the clearance and flew the AVBEG 5A STAR.”
As the aircraft deviated from the cleared track, a shift change occurred in Melbourne Centre.
The oncoming controller observed the 737 deviating from the cleared track while still in controlled airspace, and noted the aircraft was approaching an area of restricted airspace over the Canberra Deep Space Communication Complex at Tidbinbilla, west of Canberra.
After the controller queried their intentions, the flight crew told them they were following the AVBEG 5A STAR.
Acknowledging this, the controller advised the flight crew to maintain at least 10,000 ft to stay above the restricted airspace. Once the aircraft had cleared the airspace, the controller then cleared them to descend.
“The STAR the flight crew was following takes aircraft over the Tidbinbilla restricted airspace at 10,000 ft by design,” Mr Mitchell said.
“This intervention by the controller resulted in the aircraft becoming higher than the desired descent profile, as well as the crew becoming confused regarding the airspace classification for the arrival and approach.”
Aiming to get the aircraft back onto the desired flightpath, the captain decided to conduct a holding pattern at the approach waypoint of MOMBI.
“This holding pattern was not correctly flown, and the aircraft was manoeuvred significantly below the minimum safe altitude and terrain clearance reduced to a minimum of 924 ft above ground level in darkness,” Mr Mitchell said.
Prior to landing in Canberra, and while in uncontrolled airspace, the CTAF was not selected by the flight crew, and the appropriate radio broadcasts were not made.
This meant safety alerts, being issued over the CTAF by an oncoming Canberra tower air traffic controller about to begin their shift, were not heard.
The ATSB’s investigation considered factors which contributed to the occurrence, including the preparatory work done by the airline prior to the inaugural flight into a new aerodrome.
“Batik Air’s change management processes were not effective at fully identifying and mitigating the risks associated with the commencement of the Denpasar to Canberra route,” Mr Mitchell concluded.
“This included the airline not ensuring flight crew completed all CTAF training prior to operating flights into Australia, where use of these procedures could be required – as in this instance.”
Batik has taken a range of measures to address the identified safety issues.
These include internal notices to flight crew highlighting the importance of a comprehensive approach briefing, and completing practical and theoretical CTAF training for all flight crew assigned to Australian operations.
“This incident underlines the need for operators to ensure that they have comprehensive and effective change management processes in place to identify all foreseeable risks relevant to a new route, and to implement appropriate mitigations to ensure the safe operation of these routes,” Mr Mitchell said.
“In this case, the unfamiliar operating environment included the potential for operations using a CTAF, an uncommon operating procedure for non-Australian operators and crews.”
On the morning of 5 June 2025, the pilot of a Piper Chieftain PA-31, registered VH-PGO and operated by Shine Aviation, was conducting a multi-leg return passenger transport operation from Geraldton Airport via Carnarvon Airport and Meekatharra Airport, Western Australia. After refuelling in Carnarvon, VH-PGO departed for Meekatharra with the pilot and 2 passengers on board.
The flight was being conducted under instrument flight rules. During the instrument approach to Meekatharra, the right low fuel flow warning light illuminated. Shortly after, the right boost pump inoperative warning illuminated, and the right engine commenced surging with associated aircraft yaw. The pilot performed the engine failure checks, feathered the propeller, and continued the approach. The aircraft landed without further incident.
What the ATSB found
The ATSB found that the pilot did not check that the fuel caps were secured after refuelling, as required by the pilot’s operating handbook and company procedures. This resulted in the aircraft departing with the right inboard fuel cap incorrectly secured. The incorrectly secured fuel cap led to fuel siphoning overboard in flight. Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in the fuel tank quantity gauge overreading its contents.
The ATSB also found that the pilot was unaware of the actions to be taken on illumination of the right low fuel flow warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach.
Additionally, the ATSB found that Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light.
What has been done as a result
Following the occurrence, Shine Aviation reminded company pilots of the significance of the PA-31 low fuel flow warning and associated procedures. The operator also revised its training programs to strengthen coverage of abnormal and emergency scenarios, with particular emphasis on fuel system management. This included increasing the number of questions in the PA-31 theory examination. In addition, the general competency training syllabus was updated to expand instruction on fuel loading and verification processes, in‑flight fuel management practices, and aircraft type-specific emergency procedures, including detailed guidance on PA-31 annunciator panel warning lights and their operational significance.
Following a repeat incorrect cap fitment in October 2025, Shine Aviation elected to replace the fuel cap as a precaution, with no further incidents reported.
Safety message
An unsecured or incorrectly installed fuel cap can result in significant fuel loss in-flight, potentially leading to an abnormal or emergency situation. Checks of fuel system security including fuel caps should be conducted by the pilot during pre-flight, turnarounds and after refuelling to ensure correct fitment. Fuel cells will collapse if tanks are not sufficiently vented when in use; a collapsed fuel cell can result in a fuel quantity gauge overreading and providing a false indication to the pilot.
Civil Aviation Safety Regulations require pilots to be competent to the standards specified for the aircraft they are operating. This includes being able to conduct all normal, abnormal and emergency flight procedures. An awareness and understanding of cautions, warnings, and limitations contained in the pilot’s operating handbook enables pilots to identify and respond to any problems that may arise, prior to them escalating further. In this case, had the pilot taken the documented action in response to the warning, it would have prevented an emergency situation arising. However, when the engine stopped during approach while in cloud, the pilot took immediate action to feather the propeller and ensure a safe landing.
Operators also play an important role in pilots achieving the competency requirements. This includes ensuring pilots receive comprehensive training that develops and reinforces aircraft specific system knowledge, particularly regarding manufacturer warnings and cautions, and decision-making skills.
CASA Advisory Circular 91-25 Fuel and oil safety provides advice and guidance on procedures and practices to ensure the safety of fuelling operations. Included in this guidance are recommendations associated with fuel caps and vents to prevent in‑flight fuel loss and starvation.
Summary video
The occurrence
On 5 June 2025, the pilot of a Piper Chieftain PA-31-350, registered VH-PGO and operated by Shine Aviation, was conducting a multi-leg passenger transport operation under the instrument flight rules.1 At 0650 local time, the aircraft departed Geraldton Airport, Western Australia (WA), with the pilot and 3 passengers on board, and all 4 fuel tanks full – left and right, inboard and outboard. Stops were planned at Carnarvon and Meekatharra, WA, where the pilot planned to refuel, before a return flight to Geraldton (Figure 1).
Figure 1: Flight path of VH-PGO
Source: Google Earth, annotated by the ATSB
At 0817, the aircraft landed at Carnarvon Airport. The pilot then escorted the 3 passengers to the terminal building, where one passenger left the airport. The pilot returned to the aircraft to supervise refuelling and conduct a post-flight, external visual inspection of the aircraft. The local fuel supplier, on the pilot’s request, filled VH-PGO to full and then replaced the fuel caps on all 4 tanks. The refueller informed the pilot that a total of 240 L had been added to the aircraft. The pilot calculated, from the previous flight’s fuel usage, that the total fuel on board was now 688 L, which was consistent with full fuel tanks. The pilot recalled that they visually inspected but did not physically check the fuel caps for security after refuelling, and that all fuel cap latches appeared ‘down’ and in the ‘locked’ position.
The pilot assisted the 2 remaining passengers to board the aircraft, removed the chocks and then boarded the aircraft. As the pilot climbed onto the left wing to enter the aircraft, they reported giving the fuel caps ‘one last look’ and noted that they appeared correctly installed.
At 0851, VH-PGO departed Carnarvon Airport. The pilot selected the inboard fuel tanks for departure as per company and the pilot’s operating handbook (POH)2 procedures. The aircraft climbed to 9,000 ft above mean sea level (AMSL), where the pilot selected the outboard fuel tanks for the cruise to Meekatharra. At that time, the pilot calculated a fuel total of 636 L, using the onboard digital fuel flow indicator (see the section titled Fuel flow indicators). The fuel consisted of a combined 348 L in the inboard tanks and 288 L in the outboard fuel tanks. The pilot recalled that the fuel quantity gauges were indicating expected fuel quantities and fuel flow to both engines was stable throughout the take-off, climb, and into the cruise phase of flight.
During the cruise, the pilot obtained the weather at Meekatharra Airport via the aerodrome weather information service3 over VHF radio. The pilot noted that the wind was from 210° at 10 kt, cloud was overcast with a base of 800 ft above ground level (AGL), and visibility was 25 km, with no significant weather present. Based on this information, the pilot planned to conduct a landing on runway 27.4
The pilot selected the inboard tanks prior to the top of descent, in accordance with procedures. The pilot noted that the fuel quantity indication for the right inboard fuel tank was reading slightly lower than the left gauge but reported that they considered it ‘within an acceptable discrepancy for the PA-31’. The pilot calculated that 348 L remained in the inboard tanks and 118 L of fuel remained in the outboard tanks, totalling 466 L of fuel remaining on board.
The pilot descended the aircraft to 1,700 ft AGL and levelled off in accordance with the instrument approach procedure, before commencing the final approach to runway 09 with the intention of conducting a circling approach to runway 27. During this segment the R LOW FUEL FLOW warning light illuminated on the annunciator panel (see Figure 2 and the section titled Fuel system).
Figure 2: Right low fuel flow annunciator illumination during approach to Meekatharra
Source: Pilot, annotated by the ATSB
The pilot scanned the engine indications and noted they were normal, with no discrepancies between the engines. The pilot reported observing that the left and right fuel flow gauges were stable and indicating similar values, the fuel pumps were selected on, the engine mixtures were set to full rich, and the fuel boost pump circuit breakers were in and not tripped. The pilot also checked the fuel quantity gauges and stated that, while they did not recall the exact readings, nothing appeared abnormal or suggested that a tank was empty. The pilot continued the approach to Meekatharra. On the final approach segment, the aircraft entered instrument meteorological conditions (IMC).5 After entering IMC, the R FUEL BOOST INOP warning light (see the section titled Fuel system) illuminated, followed by the right engine surging and associated aircraft yaw.
The pilot conducted their memory item initial engine failure checks and feathered the right propeller. At this time, the aircraft exited IMC and was about 800 ft AGL. The pilot elected to abandon the planned circling approach to land on runway 27 and instead accepted a 5 kt tail wind to conduct a straight-in approach to runway 09, landing without further incident.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Aeroplane) and an instrument rating. The pilot also held a class 1 aviation medical certificate, valid until February 2026. At the time of the occurrence, the pilot had a total flying time of 1,381 hours, with 104 hours on the PA‑31 aircraft type. The pilot had flown 47.8 hours in the last 90 days which included 45.4 hours on PA‑31 aircraft.
The pilot commenced work with the operator in January 2025 and since then, had flown approximately 250 hours, including 220 hours in multi-engine aeroplanes, prior to the occurrence.
Aircraft information
General information
VH-PGO was a Piper Aircraft Corporation PA‑313‑50, twin‑engine, 10‑seat aircraft manufactured in the United States in 1978 and first registered in June 1979. The aircraft was powered by 2 Textron Lycoming engines: a TIO‑540‑J2BD on the left and an LTIO‑540‑J2BD on the right, each driving a Hartzell 3‑bladed constant speed propeller.
Fuel system
In PA-31 aircraft, fuel is stored in 4 flexible fuel cells, 2 in each wing. The fuel cell is attached to the upper inside of the wing by a cord running around the top section of the cell (Figure 3). The inboard cells hold 212 L each and the outboard cells hold 151 L each, totalling 726 L, of which 689 L are usable fuel.6
Figure 3: Right inboard fuel cell
Source: Operator, annotated by the ATSB
A fuel vent is located on each cell and is designed to maintain each tank at atmospheric pressure by allowing air to enter the tanks as fuel is consumed and as fuel volume changes with temperature and altitude. This is designed to prevent the development of a vacuum in the tanks and ensures a continuous and reliable supply of fuel to the engines. The vent also provides for slight positive pressure in flight. A restriction or blockage of the vent system can result in reduced fuel flow and fuel starvation despite usable fuel remaining in the tanks.
The fuel control panel is located at the base of the central control pedestal and contains the fuel tank selectors, fuel shutoffs and crossfeed controls. During normal operation each engine is supplied with fuel from its own respective fuel system. The fuel controls on the right control the fuel from the right cells to the right engine and the controls on the left control the fuel from the left fuel cells to the left engine. In emergencies, fuel from one system can supply the opposite engine through a crossfeed system.
Fuel is routed from the fuel cells to the selector valves where, dependent on valve position, fuel from either the inboard or outboard tank is routed to the engine. Fuel leaving the selector travels through a fuel filter, a fuel boost pump, the emergency fuel pump, a firewall shutoff valve, and then to the engine-driven fuel pump and engine fuel system.
The emergency fuel pumps are installed for emergency use in case of an engine-driven fuel pump failure. They are also used for take-off and landing and, when necessary, to prime the engines. Control switches for the emergency fuel pumps are located on the overhead switch panel to the right of the fuel gauges.
Two electric fuel quantity gauges are also mounted on the overhead switch panel (Figure 5). These indicate the fuel tank level from float-style sender units in each tank. The gauges indicate left inboard or outboard tank, and right inboard or outboard fuel tank quantities dependent on selector valve position. The inboard tanks contain 2 sender units each, one near the wing root and one near the filler cap (Figure 3).
The fuel boost pumps are operated continuously and are provided to maintain fuel under pressure to the engine‑driven fuel pump. There are no fuel boost pump control switches or pressure gauges.
Each tank has a separate Shaw-style fuel cap for servicing (Figure 4). The inboard tank caps are located on the upper centre section of each wing and the outboard tank caps are on the upper outboard section of each wing. The right inboard fuel cap is not visible from the pilot’s seated position. The fuel caps are installed on the filler neck of each tank and utilise a twist‑to‑lock cam mechanism. As the latch is rotated, the upper and lower sections are drawn together, compressing the O‑ring seal against the filler neck to form a secure, fuel- and water-tight closure. The lower cap lugs engage under the filler neck flange to hold the cap in place against vibration, pressure changes, and airflow that is encountered in flight. The caps are also attached to the wing by a lanyard.
Figure 4: Shaw-style fuel cap
Source: Toby Dorn, annotated by the ATSB
Fuel flow indicators
Analogue fuel flow gauges located on the instrument panel indicate fuel flow to the engines in US gallons per hour. An FS-450 fuel flow indicator is also located on the instrument panel and digitally displays real-time fuel flow in litres per hour, fuel used, fuel remaining, and time-to empty. It is used to assist pilots in fuel management, however, it records fuel flowing through the fuel flow indicator transducer into the engine fuel system and would not detect a leak upstream such as a fuel tank leak.
Fuel system warning lights
Right and left fuel flow warning lights are mounted on the annunciator panel and illuminate to warn the pilot of an impending fuel flow interruption from the inboard tanks. The lights are activated by a probe that is mounted near each inboard fuel tank outlet (Figure 3). In the event of the fuel level near the tank outlet dropping to a point where a fuel flow interruption could occur, the LOW FUEL FLOW warning light will illuminate.
The pilot’s operating handbook contains the following warning:
WARNING
If either the right or left fuel flow warning light illuminates and the fuel gauge indicates fuel remaining in the corresponding inboard tank, this will indicate a malfunction of the flapper door in the inboard tank. Immediately select the outboard tank or select crossfeed to avoid fuel flow interruption.
This warning indicates a possible flapper door malfunction within the inboard fuel tank.7 In this condition, the fuel flow warning light may illuminate despite sufficient fuel remaining in the affected tank, as the malfunction may restrict fuel flow to the tank outlet. The procedure directs the pilot to immediately select the outboard tank or crossfeed to maintain fuel supply and prevent fuel flow interruption.
Left and right FUEL BOOST PUMP INOP warning lights are also mounted on the annunciator panel, and they illuminate when the fuel boost pressure to the associated engine fuel pump is less than 3 PSI. An illumination of a fuel boost pump inoperative warning light will occur immediately prior to that engine being starved of fuel.
Post‑occurrence
Pilot actions
After landing and shutting down the left engine, the pilot escorted the passengers to the terminal, reported the occurrence to Shine Aviation, and then returned to the aircraft. The pilot then applied battery power and noted that the right inboard tank fuel quantity gauge was indicating just above a quarter full, and the left inboard tank fuel quantity gauge was indicating half a tank (Figure 5). The pilot recalled that this was unusual and was more significant than the minor discrepancy observed at the top of descent.
Figure 5: Inboard tank quantity discrepancy after landing
Source: Pilot, annotated by the ATSB
The pilot then conducted a visual inspection of the right wing area and noted blue fuel streaks behind the right inboard fuel cap (Figure 6). After attempting to drain fuel out of the right inboard fuel tank without success, the pilot then removed the right fuel cap to see if any fuel was present. The pilot noted that the fuel cap latch was ‘extremely’ difficult to unlatch and required the use of both hands. Upon looking in the tank, the pilot observed that it was empty, and the bottom of the fuel cell had been sucked up towards the fuel filler area. The pilot then reinstalled the cap, commenting that the cap latched normally and without difficulty.
Figure 6: Fuel staining aft of right inboard fuel cap
Source: Pilot, annotated by the ATSB
At hourly intervals, the pilot reapplied battery power noting that it took 2.5 hours after landing for the right inboard tank fuel gauge to read zero.
Engineering inspection
The company’s chief engineer arrived about 3.5 hours after the occurrence to commence troubleshooting. They reported that there was no evidence of a leak source around the right inboard fuel tank aside from the fuel staining aft of the fuel cap. Although the pilot had already removed and refitted the fuel cap, an inspection of the fuel cap was conducted with no defects noted including the O‑ring being found serviceable. The chief engineer replaced the cap O‑ring seal and re-tensioned the cap’s latch mechanism as a precaution. They also commented that there was a possibility of the fuel cap lanyard interfering with the cap’s fitment however no damage to the cap or the lanyard was identified.
The chief engineer observed that the bottom of the fuel cell had been drawn up towards the fuel cap and required manual reseating. They filled the inboard tanks to maximum capacity; 67 L was required to fill the left inboard tank, and 204 L was required to fill the right inboard tank. The chief engineer stated that they were satisfied that the fuel cell had reseated correctly within the fuel tank cavity.
The engines had been operated alike up to the right engine starvation. The ATSB estimated that the left engine consumed 6 L of fuel after the right engine stopped. Therefore, about 131 L had been siphoned and lost overboard from the right tank through the fuel cap during flight.
During the draft report review process, the ATSB was informed of a repeat incorrect fitment of VH-PGO’s right inboard fuel cap that resulted in fuel leaking during flight. The operator advised that this occurred on 6 October 2025, 4 months and an estimated 60–70 refuels after the initial occurrence. However, the chief engineer was able to observe the cap in its incorrectly fitted state where they determined that the cap had not been seated correctly prior to being latched. This resulted in the upper and lower portions of the cap clamping on the filler neck of the wing (Figure 7). Following the second occurrence, the chief engineer elected to replace the fuel cap as a precaution.
Upon receipt of the new fuel cap the chief engineer noted that a skirt had been incorporated into the design of the replacement cap therefore limiting the ability of the upper and lower portions of the cap to clamp on the filler neck of the wing (Figure 7). The ATSB contacted the manufacturer for further information on the apparent design change. However, at the time of publication no response had been received.
Figure 7: Incorrect fitment on 6 October 2025
Source: Operator, annotated by the operator and the ATSB
Flight testing
Followingthe inspection, the aircraft was ferried back to Geraldton (without passengers) by the head of flying operations, with the chief engineer seated in a position that allowed full view of the right inboard fuel tank cap.
During climb out of Meekatharra Airport, they observed that the FS-450 fuel flow indicator for the right engine was displaying a significantly lower fuel flow than expected for the selected power and mixture setting, and it was lower than the corresponding analogue fuel flow gauge. The FS-450 indicated approximately 70 L/h, compared to the expected value of about 120‑L/h. However, the right engine exhaust gas temperatures, oil temperature, manifold pressure and cylinder head temperature were within normal limits for that power setting and comparable to the left engine. On that basis, they assessed that the FS‑450 indication was erroneous and not representative of the actual fuel flow to the engine, with the chief engineer stating that the engine would not be able to run with that fuel flow for that power setting. The engineer advised the head of flying operations to use the analogue fuel flow gauges for engine management for the remainder of the flight.
The occurrence pilot reported that they had not observed any irregularities with any of the engine indications prior to the occurrence. This was supported by a review, conducted by the operator’s head of safety and quality assurance, of VH‑PGO’s previous 8 flight logs, which found that fuel usage data was normal and within acceptable parameters for the PA‑31‑350.8 In addition, a review of the flight logs for flights conducted after the occurrence identified no abnormalities.
The chief engineer later commented that the FS‑450 unit’s calibration may have been inadvertently altered by the occurrence pilot after the event during their initial troubleshooting.
During the return flight to Geraldton, the chief engineer did not observe any fuel leaking from the right inboard fuel tank cap, and a post‑flight inspection confirmed that no fuel leakage was present. The aircraft was subsequently flown that evening and the following morning, with no further leaks or related issues identified.
Refueller
The refueller who uplifted fuel to the aircraft at Carnarvon and secured the fuel caps before the occurrence flight later recalled that the right inboard fuel cap was slightly difficult to close. However, based on their familiarity with the aircraft, they believed the cap was properly secured. They also stated that if they had any concerns about the aircraft, they would have informed the pilot.
Pre-flight and refuelling
The pre-flight inspection detailed in the POH stated that the fuel supply should be checked visually, and a check was required to ensure the fuel caps are securely in place. To visually check the fuel supply, the cap would have to be removed and therefore a physical check of security is performed when the caps are installed.
Shine Aviation’s Policy and Procedures manual provided instructions regarding refuelling and fuel caps, additional to the POH procedures. The instructions included:
When fuelling is complete, sufficient airspace must remain in each fuel tank to allow for anticipated fuel expansion, and the PIC must ensure that all fuel and oil tank caps have been securely refitted.
PA-31 training
Regulatory requirements
Shine Aviation operated as a Civil Aviation Safety Regulation (CASR) Part 135 operation (Australian Air Transport Operations - Smaller Aeroplanes) and held a Part 135 Air Operator’s Certificate (AOC). Section 12.05 of the Part 135 Manual of Standards stated the following:
• The flight crew member must have successfully completed the operator’s conversion training, and flight crew member proficiency check, for the aeroplane.
• The training must deal with the following:
- training in the duties and responsibilities for the flight crew member’s position;
- training in the standard operating procedures for the type or class of aeroplane used for the flight;
- training in the normal, non-normal and emergency procedures for an aeroplane of that type or class;
- training in any flight procedures or manoeuvres, conducted in an aeroplane of that type or class, for which the operator holds an approval under regulation 91.045, or 135.020, of CASR;
Note: Examples of approvals issued under regulation 91.045, or 135.020, of CASR include approvals to conduct low visibility operations and flights using certain PBN navigation specifications.
- training in the procedures for any other operations conducted by the operator in an aeroplane of that type or class that the flight crew member has not previously experienced, for example, precision runway monitor operations or land and hold short operations.
Under CASR Part 61.385 Limitations on exercise of privileges of pilot licences – general competency requirement, a pilot may only exercise the privileges of their licence if they are competent to the standards specified for the relevant aircraft they are operating. This includes being able to conduct all normal, abnormal and emergency flight procedures for that aircraft.
Company flight training
Shine Aviation was approved by CASA as a CASR Part 141 training organisation, enabling it to conduct in-house pilot training and competency assessments in support of pilot qualification for operations under the organisation’s Part 135 Air Operator’s Certificate.
Pilots underwent conversion training onto company aircraft in 2 parts: a ground-based theory component, followed by a flying component. The ground-based theory component consisted of self-paced study of the POH prior to undergoing a multiple-choice theory exam. The theory examination consisted of 25 PA-31 specific questions, automatically generated from a question bank of 82, including topics relating to weight and balance, aircraft performance, and systems knowledge.9
The flying component involved the pilot conducting 2 non-revenue (no passengers) training flights with a company flight instructor. Shine Aviation’s General Competency Training syllabus included the following competencies for the pilots to demonstrate:
departure and arrival (including appropriate engine management for turbocharged aircraft)
stalling
steep turning
different cruise configurations
upper air asymmetric where applicable
normal circuit
flapless circuit
crosswind circuit
engine failure on take-off
engine failure elsewhere in circuit
single engine go‑around
discussion on differences in standard practice between engine models (oil uplift, engine monitoring etc)
any other multi engine or single engine class rating competencies as deemed necessary by instructor.
Although this syllabus contained specific competencies for other types of aircraft Shine Aviation operated, it did not contain any specific PA-31 competencies. However, it did contain an ‘underpinning knowledge’ section in which ‘Instrument failure and warning systems fitted to the aeroplane’ was listed.
Following satisfactory demonstration of the required flying competencies, the pilot was required to act as a copilot for approximately 30 hours of normal company operations prior to conducting single pilot operations.
The pilot in this occurrence completed their ground component and 2 non-revenue training flights, involving 3 hours of flight and 4 hours of briefing time, in January 2025. The pilot then conducted approximately 30 hours of flying as a copilot in the PA-31, including 13.5 hours in VH-PGO, prior to being assessed and approved for single pilot operations. The pilot completed an instrument proficiency check in January 2025 in the PA-31 with a company examiner.10
In May 2025, the pilot successfully completed 2 recurrent flight training exercises in the company’s approved synthetic training device.11 These exercises involved various emergency and abnormal scenarios consisting of adverse weather, engine failures, single engine approaches, instrument failures and flight planning exercises.
Training regarding low fuel flow warning light
The theory examination contained the following question related to the LOW FUEL FLOW warning light:
Illumination of a LOW FUEL FLOW annunciator:
a) Indicates that outboard fuel quantity has decreased to a point where engine power loss could occur
b) Indicates low fuel quantity in the inboard tanks
c) Indicates that a fuel boost pump has failed
d) a and c
The correct answer is (b), however this question pertains to the function of the warning light but does not cover the published warning or the actions to be taken by the pilot upon its illumination (see the section titled Fuel system warning lights). Regardless, the theory examination that was generated for the occurrence pilot did not include this question.
Shine Aviation’s head of training for the PA-31 stated that the LOW FUEL FLOW warning light was likely discussed during the flight training component when the annunciator panel was covered. However, they also stated that not every annunciator panel indication was examined in detail.
The incident pilot advised that the LOW FUEL FLOW warning light was not specifically addressed during initial or copilot training and that, although they understood that it related to a fuel flow issue to the affected engine, they were not aware of, or could not recall, the required immediate actions that are directed by the warning in the POH.
Related occurrences
Excluding the incident flight, the ATSB occurrence database contained 49 reported occurrences of fuel leaking or venting from a fuel cap on non-jet aircraft between 2014 and 2025. Of those occurrences, 8 resulted in fuel starvation or fuel exhaustion. Those numbers likely under‑represent the total number of incidents of this type, as the ATSB only required instances of fuel leaking/venting or missing/insecure fuel caps to be reported for commercial passenger transport operations.
ATSB occurrence brief AB-2021-009 was published following a fuel starvation event involving a PA-31-350 in 2021:
On 21 March 2021 a Piper PA-31-350 aircraft was operating a scheduled freight flight from Moorabbin, Victoria to Devonport, Tasmania. During approach, the low fuel flow and low boost pump warning lights illuminated. The right engine stopped shortly after. The pilot in command confirmed the fuel selector was in the correct position and observed that the fuel gauges indicated three-quarters full, which was as expected. The pilot then attempted to cross-feed fuel from the left engine, which was unsuccessful. By this time, the aircraft was on mid-final and, once assured of making the runway, the pilot stopped troubleshooting and concentrated on landing the aircraft.
After landing, the pilot inspected the fuel cap, which appeared to be secured correctly. However, blue stains were evident on top of the wing consistent with fuel venting out of the fuel cap. The fuel system was subsequently inspected by maintenance personnel with nil defects found with the fuel cap and no blockages in the fuel tank vents.
The pilot later advised that the rubber bladder containing the fuel within the tank was sucked up against the top of the wing as the tank emptied, providing a false indication of the fuel remaining in the tank.
ATSB occurrence investigation AO-2024-008 was published following a fuel exhaustion event in 2024:
On 8 March 2024, the pilot of an Aero Commander 500-S, registered VH-MEH and operated by GAM Air, was conducting a return cargo transport operation from Bankstown Airport to Parkes Regional Airport, New South Wales with one intermediate stop outbound, and 2 intermediate stops on return.
After landing on the first sector, the pilot found the fuel cap was off and secured only by a retention chain. The pilot re-secured the cap but after landing at Parkes on the second sector, they again found the fuel cap off. They arranged an inspection by a maintenance engineer, where a fault was found that prevented the fuel cap from locking and rectified it.
Later that day, the pilot commenced the return sectors to Bankstown. Shortly after departing Bathurst for the final sector, both engines lost power, and the pilot conducted a forced landing in a field. The aircraft was undamaged and the pilot was uninjured.
The ATSB found that the fuel cap retention chain had lodged within the fuel tanks anti siphon valve. This allowed fuel to be siphoned overboard during flight.
CASA Advisory Circular 91-25 Fuel and oil safety, section 6, highlighted recommendations associated with fuel caps and vents. In particular, the circular advised of the possibility of fuel siphoning overboard due to a cap attachment chain or lanyard becoming trapped across a fuel cap seal. The advisory circular also identified that an insufficiently vented tank may collapse the fuel bladder and exaggerate indications of fuel within the tank.
Safety analysis
Introduction
On 5 June 2025, the pilot of a Piper Chieftain PA-31, registered VH-PGO, and operated by Shine Aviation, was conducting a passenger transport operation from Carnarvon to Meekatharra, Western Australia. During the approach to Meekatharra Airport, the R LOW FUEL FLOW warning light illuminated, followed shortly by the R FUEL BOOST INOP warning light and surging of the right engine. The pilot conducted their memory item initial engine failure checks and feathered the right propeller. The pilot continued the approach and landed without further incident.
Fuel siphoned overboard
Photographs taken by the pilot after landing at Meekatharra Airport show fuel staining immediately aft of the right inboard fuel cap, consistent with fuel leaking from the cap in flight. This staining, in conjunction with the pilot’s observation that the right inboard tank was emptied earlier than expected based on calculated consumption, and that the tank cell collapsed upwards towards the cap, all indicate that fuel had likely been siphoned through the cap in flight. The pilot also reported that the fuel cap latch was difficult to lift, suggesting the cap may not have been correctly seated.
During the post-occurrence inspection, the chief engineer found no evidence of any other fuel leaks around the right inboard tank. The pilot had removed and reinstalled the cap prior to this inspection, therefore the chief engineer could not determine exactly how the cap was incorrectly fitted. The chief engineer was also unable to reproduce an incorrect installation. However, the chief engineer considered it likely that the fuel cap had been incorrectly secured, including the possibility of the attaching lanyard interfering with the cap and seal. No damage was observed to the cap, seal, or lanyard and the chief engineer replaced the O-ring on the cap as a precaution, although they considered the removed O‑ring serviceable. Subsequent flights, including the immediate post‑occurrence flight with the chief engineer observing the cap, did not reproduce the leak. As the leak did not recur, it was almost certain the fuel cap was incorrectly secured in Carnarvon.
As part of the troubleshooting, the chief engineer refuelled the right inboard tank with 204 L, while the left tank required only 67 L to fill. Given that both tanks had been selected for use at similar times during the flight, and accounting for fuel used by the left engine after the right had stopped, the discrepancy indicated that approximately 131 L of fuel had been lost through the fuel cap from the right inboard tank.
Contributing factor
The fuel cap on the right inboard fuel tank was almost certainly incorrectly secured which led to fuel being siphoned overboard in flight.
Fuel cap installation
Shine Aviation’s Policy and Procedures manual required the pilot in command to ensure that fuel caps were securely fitted. While this did not explicitly require the pilot to remove and reinstall the caps, the pilot’s operating handbook specified that the pilot in command must visually check the fuel supply and confirm that the fuel caps are secure. Checking the fuel quantity required the pilot removing the caps and physically handling the fuel caps to verify correct fitment.
Although the pilot stated that they visually inspected the fuel cap, a closer inspection or physical check of the cap would likely have aided the pilot in identifying the incorrect installation. Consequently, the pilot did not detect that the right inboard fuel tank cap was incorrectly secured.
Contributing factor
The pilot did not check that the fuel caps were secured as required by the pilot’s operating handbook and company procedures, resulting in the aircraft departing with the right inboard fuel cap almost certainly incorrectly secured.
False gauge reading
During flight, the rate of fuel being siphoned through the fuel cap was likely sufficient to overcome the vent’s ability to equalise pressure in the fuel tank. This resulted in negative pressure collapsing the fuel cell as observed by both the pilot and the chief engineer during their post-occurrence inspections. As the fuel cell was secured by a single cord around the upper perimeter, the collapse of the fuel cell resulted in the base of the cell lifting towards the filler port.
As one of the right inboard fuel tank float-style sender units was located near the fuel filler port, it is likely that the upwards lifting of the fuel cell floor toward the filler port, raised the outboard sender unit’s float. This resulted in an overreading of the cockpit fuel quantity gauge. ATSB occurrence brief AB-2021-009 identified a similar failure mechanism where the fuel cell collapsed resulting in the fuel gauge overreading its contents. The Civil Aviation Safety Authority’s advisory circular (AC) 91-25 Fuel and oil safety, section 6, also contained information about collapsing fuel cells interfering with the accuracy of fuel gauge readings.
During the subsequent flight, the onboard fuel flow indicator was incorrectly and significantly underreading the right engine fuel flow. However, the pilot reported it was functioning normally during the flight to Meekatharra. Engineers assessed the instrument had probably been inadvertently recalibrated during post-incident fault finding.
When the pilot changed from the outboard tanks to the inboard tanks at the top of descent, they noticed that the right inboard tank quantity gauge was reading a slightly lower quantity than the left inboard, however they assessed that this was an acceptable discrepancy related to VH-PGO. It is likely that the right inboard tank was almost empty at that stage of flight as the R LOW FUEL FLOW warning light illuminated shortly after.
Contributing factor
Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in that fuel tank quantity gauge overreading its contents.
Response to warning
The warning in the pilot’s operating handbook (POH) stated that if the right or left LOW FUEL FLOW warning light illuminated, and the fuel gauge indicated fuel remaining in the corresponding inboard tank, this indicated a malfunction of the flapper door in the inboard tank. The prescribed action was to immediately select the outboard tank or select crossfeed to avoid fuel flow interruption. While a flapper door malfunction did not occur in this instance, compliance with the warning actions would likely have restored fuel supply.
The pilot was unaware of the required immediate actions and therefore did not respond to the R LOW FUEL FLOW warning light as directed by the POH. The pilot was also unaware that a fuel starvation event was developing, until the subsequent illumination of the right FUEL BOOST INOP warning light and associated engine surging.
The sequential activation of the R LOW FUEL FLOW warning followed by the right FUEL BOOST INOP warning was a progressive indication that fuel flow to the right engine would be interrupted. As the pilot did not restore fuel flow following either warning, the right engine became starved of fuel, resulting in the engine surging and a corresponding yaw of the aircraft.
Contributing factor
The pilot was unaware of the actions to be taken on illumination of the LOW FUEL FLOW warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach.
Training regarding low fuel flow warning light
As part of the Civil Aviation Safety Regulations (CASR) limitations on the privileges of a pilot licence, pilots were required to be competent in conducting all normal, abnormal and emergency flight procedures for the aircraft. This required the pilot to be aware of the POH warnings and associated instructions included in emergency procedures. Additionally, under CASR Part 135, operators were also required to ensure that flight crew were trained in the normal, non-normal and emergency procedures for the aircraft they were operating.
Shine Aviation PA-31 pilots independently studied the POH and subsequently undertook a theory examination. This examination consisted of 25 PA-31 specific questions that were automatically generated from a question bank of 82. Although there was one question regarding the illumination of the LOW FUEL FLOW warning light, this question did not evaluate the immediate response required. Furthermore, this question was not included in the occurrence pilot’s automatically generated examination.
Shine Aviation’s head of PA-31 training advised that the LOW FUEL FLOW annunciator and associated warning were likely addressed to some extent during practical line training. However, the occurrence pilot did not recall this topic being covered. Shine Aviation’s General Competency syllabus required a general knowledge of the warning systems, however, it did not specifically require demonstration of the appropriate response to a LOW FUEL FLOW warning. In this case, the training was ineffective at ensuring the incident pilot was competent in responding to the warning.
Contributing factor
Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light. (Safety issue)
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation involving Piper PA-31, VH-PGO, 28 km west of Meekatharra Airport, Western Australia, on 5 June 2025.
Contributing factors
The fuel cap on the right inboard fuel tank was almost certainly incorrectly secured which led to fuel being siphoned overboard in flight.
The pilot did not check that the fuel caps were secured as required by the pilot’s operating handbook and the company procedures, resulting in the aircraft departing with the right inboard fuel cap almost certainly incorrectly secured.
Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in that fuel tank quantity gauge overreading its contents.
The pilot was unaware of the actions to be taken on illumination of the LOW FUEL FLOW warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach.
Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Low fuel flow warning light and subsequent actions not highlighted in training
Safety issue description: Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow annunciator light.
Glossary
AMSL
Above mean sea level
AGL
Above ground level
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
IFR
Instrument flight rules
IMC
Instrument meteorological conditions
POH
Pilot’s Operating Handbook
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
the operator of VH-PGO
Civil Aviation Safety Authority
Airservices Australia.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
the operator of VH-PGO
Civil Aviation Safety Authority.
Submissions were received from:
the pilot
the operator of VH-PGO.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
^Pilot’s operating handbook: a manufacturer-produced manual that provides pilots with all the essential information needed to safely operate the aircraft.
^Aerodrome weather information service (AWIS): actual weather conditions, provided via telephone or radio broadcast, from Bureau of Meteorology (BoM) automatic weather stations, or weather stations approved for that purpose by the BoM. Winds are in degrees magnetic.
^Runway number: the number represents the magnetic heading of the runway to the nearest 10 degrees.
^Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
^Usable fuel: the amount of fuel in a fuel tank that can reliably be supplied to the engine in all operating conditions. This excludes fuel that cannot be used due to aspects such as tank geometry and fuel pickup locations.
^A flapper door is installed in each inboard tank to keep fuel around the tankoutlet by preventing it from flowing away during manoeuvring, climb, descent, turbulence, or uncoordinated flight.
^The pilot records fuel quantity prior to start, fuel quantity used via the FS-450, and fuel quantity after shutdown for each sector in a flight log. This allows the operator to monitor fuel usage for individual aircraft.
^Following the occurrence, Shine Aviation increased the number of questions in the PA-31 theory examination to 30.
^Instrument proficiency check (IPC): A required annual flight test to ensure that a pilot maintains the necessary skills and knowledge to safely operate an aircraft under instrument flight rules (IFR). It involves demonstrating competency in tasks such as navigation, communication, and handling the aircraft in various conditions, all while relying on instruments rather than visual references.
^Recurrent training: Shine Aviation conducts recurrent training for all its instrument rated pilots every 6 months. Training is delivered in a synthetic flight training device and consists of simulated IFR flights that include operational and decision-making scenarios tailored to the individual pilot. This recurrent training is in addition to regular instrument proficiency checks as required every 12 months under CASR Part 61.
Occurrence summary
Investigation number
AO-2025-026
Occurrence date
05/06/2025
Occurrence time and timezone
1031 Australian Western Standard Time
Location
28 km west of Meekatharra Airport
State
Western Australia
Report release date
04/06/2026
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Fuel starvation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-31-350
Registration
VH-PGO
Serial number
31-7852109
Aircraft operator
Shine Aviation
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Passenger transport charters
On 29 April 2025, the flight crew of an Alliance Airlines Fokker 100 aircraft, VH-FKF, were conducting scheduled passenger flight QQ 3811, from West Musgrave Airport to Perth Airport, Western Australia. The captain was the pilot flying and the first officer was the pilot monitoring.
The flight crew received an air traffic control clearance to conduct a visual approach following a standard instrument arrival to Perth Airport’s runway 03. The approach required a 90° turn onto final that resulted in the aircraft being aligned with the runway and on the correct approach profile about 4 NM from the runway threshold.
Passing about 1,000 ft radio altitude, the aircraft was above the operator’s permitted airspeed‑related stabilised approach criteria. However, a go‑around was not initiated and the aircraft landed uneventfully at 1539 local time.
What the ATSB found
The ATSB found that the pilot flying incorrectly assessed that the applicable stabilisation height was 500 ft. As a result, they did not manage the aircraft's energy state to ensure the stabilised approach speed requirement was met by 1,000 ft.
The pilot monitoring did not announce that the approach was unstable when the airspeed requirement was not met at 1,000 ft. This may have been influenced by their workload, the required check being completed slightly late, and an assessment that the airspeed was reducing.
Finally, although not contributory to the occurrence, during descent the captain inadvertently omitted to change the altimeter setting from standard pressure to QNH. This resulted in the left altimeter indicating 300 ft lower than the right altimeter. Neither flight crewmember detected the incorrect setting during 2 subsequent checks prior to landing.
Safety message
This incident highlights the importance of flight crew having a common understanding of the approach requirements. The International Air Transport Association provided guidance for flight crew to avoid an unstable approach. This included to:
be aware of the stable approach criteria
comply with the stable approach criteria published in the standard operating procedures (SOP)
advise air traffic control when unable to comply with a clearance that would result in the aircraft being too high and/or too fast
prepare for visual approaches by briefing speed/altitude/configuration gates, equivalent to those of an instrument approach, and follow the published visual approach pattern in the manufacturer’s or operator’s SOP
configure the aircraft for landing at some predetermined distance from the airport or altitude, after which only small corrections to pitch heading and power setting should be made.
This incident also illustrates the need for effective flight crew monitoring. The Flight Safety Foundation identified that monitoring can be improved by standard operating procedures, increased emphasis and practice, and stated:
One of the most important aspects of a safe flight operation is the requirement for crewmembers to carefully monitor the aircraft’s flight path and systems, as well as actively cross-check each other’s actions.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 29 April 2025, the flight crew of an Alliance Airlines (Alliance) Fokker 100 aircraft, VH‑FKF, were conducting scheduled passenger flight, callsign ‘Unity’ (QQ) 3811, from West Musgrave Airport to Perth Airport, Western Australia. The captain was the pilot flying (PF), and the first officer was the pilot monitoring (PM).[1]
At about 1449 local time, while in the cruise at flight level (FL) 340,[2] the flight crew received an air traffic control (ATC) clearance to conduct the KABLI One Victor standard instrument arrival (STAR) to Perth Airport’s runway 03 (Figure 1).
Before commencing descent, the flight crew reviewed the Perth Airport automatic terminal information service (ATIS), which included QNH[3] of 1,024 hPa and wind from 080° at 10 kt. The flight crew calculated the landing reference speed (VREF) for the aircraft’s weight using landing flap 25 to be 122 kt and the approach speed (VAPP) as 132 kt.
Note: Airservices advised that the VOR depicted on the chart is historical, does not serve a navigational purpose for the depicted procedure and can be removed. Source: Jeppesen, annotated by the ATSB
At about 1512, the flight crew were cleared to descend to FL 190 ‘when ready’ and instructed to switch to another Melbourne Centre ATC frequency. The PM reported having commenced descent from FL 340 at 1517, and 3 minutes later, the controller instructed them to maintain 250 kt (airspeed) from KABLI until advised and cleared them to descend via the STAR to 9,000 ft.
The aircraft passed waypoint KABLI at about 1527, descending through about FL 166 and then turned to track 50 NM via the STAR to fly-by waypoint[4] OBGOS, 5 NM from the runway 03 threshold.
During descent, approaching the transition level (FL 110),[5] the required transition check involved:
each flight crewmember setting the current local QNH (in this instance 1,024 hPa), on the altimeter set panel
changing the subscale for the captain’s (no 1) and first officer’s (no 2) primary flight displays (PFD), from standard (STD) to QNH by pressing the QNH/STD button on the electronic flight instrument system panel (Figure 2).
When set to QNH, the PFD displays the value selected on the altimeter set panel in hPa. When set to STD, the PFD displays ‘STD’.
Figure 2: Altimeter set panel and electronic flight instrument system (EFIS) panel (not collocated)
Source: Fokker, annotated by the ATSB
Recorded flight data showed that the first officer’s PFD altimeter reference pressure changed from STD to QNH passing about FL 114, but the captain’s PFD remained on STD. The standby altimeter pressure setting was not recorded, but the captain reported having set the standby altimeter to QNH.
After each setting their own PFD, the standard operating procedures required each flight crewmember to crosscheck all 3 altimeters were set correctly. The PF was required to call out ‘Transition [1,024] set. Passing [x] ft now. Speed [x] knots’. The PM was to respond, ‘[x] ft checked’. The crew reported completing the checks, but did not identify that the no 1 PFD was incorrectly set to STD and therefore indicating about 300 ft lower than the no 2 PFD (and the standby altimeter).
At about 1527, the PM contacted the Perth Approach controller, and at 1528:44, passing FL 136, was instructed to increase speed to 270 kt then cancel further speed restrictions, and descend to 7,000 ft (see the section titled Air traffic control speed instructions). About 4 minutes later, they were cleared to descend to 3,000 ft and report when visual.[6] The PM read back ‘descend 3,000’ and advised they were visual. The controller then cleared the flight crew to conduct a visual approach, which the PM read back.
At 1533, ATC broadcast that a new ATIS was current and the QNH had changed to 1,023 hPa. At that time, the aircraft was descending through about 5,000 ft. Passing 5,000 ft, the standard procedures required the PM to call out ‘5,000 ft on QNH [1,023]’ and the PF’s required response was ‘QNH [1,023] checked’. Both flight crewmembers recalled having set and then confirmed all 3 QNH displays were set to 1,023. However, they did not identify the altitude discrepancy between altimeters, or the no 1 PFD subscale setting of STD.
As ATC had cancelled the STAR speed restrictions, the flight crew did not have to adhere to the airspeeds on the approach chart. Therefore, as the aircraft descended through 5,000 ft, it passed waypoint VAVGA at an indicated airspeed of about 270 kt – 40 kt faster than the published speed restriction. The aircraft subsequently passed waypoint KARGO, descending through about 3,300 ft at 230 kt airspeed – 45 kt faster than the published speed restriction.
Approaching 2,500 ft and at about 200 kt airspeed, the PM selected flap 8. As the aircraft descended through 2,500 ft, the flight crew were required to crosscheck the radio altitude[7] indicating on both PFDs. The flight crew confirmed the radio altitudes matched, but again did not identify the no 1 altimeter subscale incorrectly set to STD. At the same time, the approach controller instructed the PM to change to the Perth Tower ATC frequency. The PM contacted the aerodrome controller at 1536:15.
A review of recorded flight data identified that, at 1536:46, the aircraft commenced the right turn past waypoint OBGOS (Figure 3), at about 2,000 ft above mean sea level (AMSL) and 180 kt airspeed. During the turn, landing gear was extended, followed by flap 25. Just before the aircraft was levelled, the captain deployed the speed brake.
Figure 3: Recorded flight data showing VH‑FKF turn past fly‑by waypoint OBGOS
Source: Recorded flight data overlaid on Google Earth, annotated by the ATSB
The captain reported identifying a discrepancy between the altimeter and the radio altitude during the turn, passing about 1,500 ft, and assessed it as an instrument error. As they were visual, the captain was primarily focused outside, ensuring the aircraft aligned with the runway and on the correct profile by following the precision approach path indicator (PAPI) guidance.
About 1 minute after commencing the turn, the aircraft was aligned with the runway centreline, about 4 NM from the threshold, at 1,250 ft radio altitude and 172 kt airspeed. The captain later reported that the airspeed was faster than normal due to their focused attention on the observed altimeter discrepancy. As the aircraft descended through about 1,000 ft radio altitude (also about 1,000 ft above aerodrome elevation), the PM assessed that all stabilised approach criteria were met and called ‘stable’, and the flight crew continued the approach.
The aerodrome controller cleared the flight crew to land as the aircraft passed about 600 ft radio altitude. At 1539, the aircraft landed normally within the touchdown zone. After landing, the captain realised that the no 1 PFD was set to STD and changed the setting to QNH.
Context
Flight crew information
The captain held an air transport pilot licence (aeroplane), class 1 aviation medical certificate, and had accrued 24,797 hours total flying time, 1,497 of which were in the Fokker 70 and 100 aircraft types.
The first officer held a commercial pilot licence (aeroplane), class 1 aviation medical certificate, and had 4,600 hours total flying time, 520 of which were on the Fokker aircraft types.
The captain reported their fatigue as 3/7 and the FO as 1/7.[8] There was no evidence fatigue was a factor in this occurrence.
Key speeds
The flight crew used the onboard performance tool to calculate the landing reference speed (VREF) of 122 kt. The Alliance Airlines Fokker 70–100 Aircraft Operating Manual (AOM) Supplement (SUP) defined the approach speed as VREF + 5 kt with the following wind correction:
The approach speed (VREF + 5) should be corrected for wind, including gusts, as follows:
Wind 0 up to 10 knots inclusive: no correction
Wind (+gust) more than 10 up to 20kts inclusive: add 5kts
Wind (+gust) more than 20kts: add 10 kts
Based on the ATIS specified wind speed of 10 kt and the Alliance AOM SUP, there was no wind correction required and the VAPP was 127 kt. However, the crew added 5 kt for wind correction and used VAPP of 132 kt. The flight crew could not recall their decision‑making around the wind correction, but reported it may have included consideration of the wind the aircraft was experiencing at the time of the calculation, and the aerodrome forecast wind speed of 12 kt.
The Fokker Aircraft Operating Manual specified maximum flap extended speeds of:
flap 8° – 250 kt
flap 15° and 25° – 220 kt
flap 42° – 180 kt
and the maximum landing gear extended and operating speed was 200 kt.
Air traffic control speed instructions
Airservices Australia’s Aeronautical Information Publication (AIP) included the following content related to airspeed requirements:
ENR 1.5 – 47:
10.1.5 When a clearance for the termination procedure is authorised e.g. visual approach, the published STAR speed restrictions still apply unless specifically cancelled.
10.2.5 Cancellation of ‘published speed restrictions’ cancels all speeds published on the STAR chart. Cancellation of ‘ATC-issued speed control instruction’ cancels any speed control instructions issued by ATC. Airspace speed limitation must be complied with unless specifically cancelled.
ENR 1.4 – 13:
4.1 Airspace speed limitations stated ‘N/A’ for IFR aircraft in Class C (and Class A) airspace.
GEN 3.4 – 56 included the phraseology [DESCEND VIA STAR TO (level)], CANCEL SPEED RESTRICTION(S), for the circumstances:
During a STAR descent:
a. comply with published level restrictions b. follow the lateral profile of the STAR c. published speed restriction and ATC-issued speed control instructions are cancelled
ENR 1.6 – 5:
5.2 The pilot must request an alternative when at ATC-issued speed control instruction is unacceptable on operational grounds.
5.5 A pilot will be advised when a specific ATC-issued speed control instruction is no longer necessary. Unless otherwise stated, an ATC-issued speed control instruction applies until the aircraft reaches the point in the descent profile where the speed would normally be reduced below that assigned by ATC. Except for a STAR, a DME arrival, or unless otherwise specified, a clearance for final approach or a clearance for a visual approach terminates speed control.
On this flight, after being cleared for the STAR, the flight crew were instructed to ‘increase speed to 270 knots and then cancel further speed restrictions’. About 3 minutes later, they were cleared to conduct a visual approach.
Airservices Australia advised that in this case, the aircraft was expected to maintain 270 kt until the point of normal profile speed reduction. The flight crew could then resume their desired profile speed.
The aircraft maintained 270 kt until it passed waypoint VAVGA, less than 2 minutes after being cleared for a visual approach. The captain reported that the cancellation of speed restrictions created a ‘subtle pressure’ to maintain a higher airspeed, and contributed to the faster approach speed.
Recorded flight data
At 1528:44 the aircraft was 40 NM from OBGOS at 13,915 ft (corrected barometric altitude for comparison) and 250 kt when ATC instructed the flight crew to increase speed to 270 kt then cancel further speed restrictions.
At 1531:42, the aircraft was 24.6 NM from OBGOS at 7,698 ft barometric altitude and 272 kt when cleared for a visual approach. The aircraft then continued at about 270kt to waypoint VAVGA, 16 NM from OBGOS. From there, about 140 kt deceleration to VAPP (132 kt) was required by 1,000 ft.
At VAVGA the aircraft was at 5,000 ft, 1,600 ft higher than the minimum permitted altitude. To that point, the average descent rate since the crew were instructed to increase to 270 kt (40 NM from OBGOS), had been 1,938 fpm. A descent rate of 2,286 fpm was required for the aircraft to have passed VAVGA at 3,400 ft and subsequently achieve the required deceleration.
Figure 4 depicts key parameters of the recorded flight data during the approach from 3,000 ft. At 1,000 ft radio altitude, the recorded airspeed was 158 kt, which reduced to the stabilised criterion of VAPP + 10 (142 kt) by 800 ft, 9 seconds later. The vertical speed was not recorded but was calculated from the change in recorded altitudes.
Table 1 shows the derived vertical speed, with exceedances of the stabilised criterion of 1,000 fpm between about 1,000 ft and 450 ft radio altitude. These included an expected increase in vertical speed associated with the retraction of the speed brake, passing about 800 ft radio altitude. The recorded data also showed that the aircraft was within one dot of the 3° glideslope from 1,000 ft and therefore on the correct approach profile.
Figure 4: Recorded flight data of approach to runway 03 from 3,000 ft
Source: ATSB analysis of recorded flight data
Table 1: Descent rates from about 1,000–400 ft radio altitude
Radio altitude (ft)
Descent rate (fpm)
1,015
-1,217
977
-1,127
965
-1,123
915
-1,087
913
-1,030
873
-890
868
-843
843
-870
843
-983
797
-990
798
-1,013
805
-1,103
773
-1,203
720
-1,200
719
-1,050
708
-1,013
683
-1,123
668
-1,170
609
-1,097
611
-1,067
606
-1,110
587
-1,197
541
-1,023
550
-940
561
-953
492
-1,140
491
-1,207
455
-1,163
437
-1,027
391
-820
Alliance Airlines documented procedures
Descent rates
The OPPM stated:
The following values for the rate of descent below the transition altitude shall not normally be exceeded:
• 3000 fpm down to an altitude of 3000 ft above aerodrome level (AAL).
• 2000 fpm down to an altitude of 2000 ft AAL transitioning to 1000 ft AAL
• 1000 fpm below 1000 feet AAL.
Visual approach
The OPPM stated that in visual meteorological conditions (VMC)[9] on a visual approach, the aircraft must join the circuit on the upwind, crosswind or downwind leg, or make a straight-in approach after establishing on final approach by 5 NM.
The Alliance Airlines F70–100 AOM SUP (versions 2.5 published in March 2024 and 2.6 published 10 June 2025) included section 7.12 Visual approach with subheadings 7.12.1 Procedure and 7.12.2 Straight-in visual approach. Both subsections included:
If not in the correct landing configuration at 1000ft AAL [above aerodrome level], a go around must be initiated.
If not stabilised on speed and glide path at 500ft AAL, a go around must be initiated.
The following are the requirements for configuring a straight in approach.
• The aircraft must be configured landing gear down and flap 25 prior to 1500ft AAL and a 5nm final.
• Select flap 42 (if required) at 1300ft AAL.
Vertical speed should not exceed 1000ft/min inside 5nm to touchdown.
Stabilised approach criteria
The Alliance Airlines OPPM defined a stabilised approach as one that met the following criteria:
a) the correct flight path;
b) only small changes in heading/pitch are required to maintain the correct flight path;
c) the aircraft speed is not more than VAPP + 10 knots indicated airspeed and not less than VREF;
d) the aircraft is in the correct landing configuration;
e) sink rate is no greater than 1,000 feet per minute
f) thrust or power setting is appropriate for the aircraft configuration;
g) all briefings and checklists have been completed;
h) specific types of approaches are stabilized if they also fulfil the following
i. instrument landing system (ILS) approaches must be flown within one dot of the glideslope and localizer
ii. a Category II or Category III ILS approach must be flown within the expanded localizer band
i) unique approach procedures or abnormal conditions requiring a deviation from the above elements of a stabilized approach require a special briefing to have been completed prior to beginning the approach.
• Note 1: A momentary excursion is permitted for points (c) & (e). A momentary excursion is defined as a deviation lasting only a few seconds and where every indication is that it will return to the stabilised criteria as listed in points (c) & (e).
• Note 2: Where the nominal descent path for a particular approach requires a descent rate greater than 1000 fpm. This is only permitted when expected rates of descent have been briefed prior to the approach being commenced.
Stabilized Heights
All flights shall meet all of the above stabilized approach criteria by 1,000 feet above aerodrome level except under the following circumstances:
Visual approach:
• Speed may be higher than VAPP + 10, provided it is within limits and expected to reduce to VAPP+10 or below by no later than 500ft AAL.
• Note 3: Visual conditions as defined by Jeppesen AUS or AIP - the pilot has established and can continue flight to the airport with continuous visual reference to the ground or water; and visibility along the flight path is not less than 5000m.
Visual circuit:
• Manoeuvring shall be completed no later than 500 AAL.
Circling approach
• Final Flap shall be selected no later than leaving the Circling Altitude.
• By 500ft AAL for the following shall be achieved.
◦ Approach Speed must be achieved
◦ Checklists must be completed
◦ Manoeuvring must be completed.
…[RNP-AR approach]
An approach that does not meet, or subsequently exhibits sustained deviations outside of these criteria requires an immediate go-around.
On 3 April 2025, Alliance issued Operations notice 25-038:
The Alliance Airlines Fokker AOM SUP (v2.5 released March 2024 and v2.6 released 10 June 2025) included the following visual approach standard calls:
Hierarchy of manuals
The Alliance Airlines hierarchy of manuals stated that the Operations Policy and Procedures Manual (OPPM) was the primary manual, and the aircraft operating manuals and supplements were supporting manuals. The OPPM section 7 – Standard operating procedures stated:
All Pilots must be fully aware and observant of the procedures and calls outlined in this chapter. Operate Alliance Airlines aircraft in accordance with the appropriate Aircraft Operating Manual and the Alliance Airlines Operations Policy and Procedures Manual. If information in either of these manuals conflict, the information in the most recent revision of the Aircraft Operating Manual or Operations Notice ‘date’ can be assumed to be valid.
Based on the hierarchy, the operations notice replaced the stabilised approach criteria documented in the OPPM. At the time of the incident, the operations notice had a more recent publication date than the AOM SUP and therefore took precedence where the information conflicted. However, an amendment to the AOM SUP was published after the incident (and subsequent to the operations notice), which did not amend the information that conflicted with the operations notice.
Alliance Airlines advised that it intended the flight crew to comply with the operations notice, which at the time of writing was to be incorporated into an amended OPPM. Additionally, a further amendment would be made to the AOM SUP to remove conflicting information.
Applicable stabilisation height
Alliance assessed that for the visual STAR via OBGOS the applicable stabilisation height was 1,000 ft, ‘because the STAR has FMS [flight management system] guidance and is not a visual circuit or circling manoeuvre’. However, Alliance’s stabilisation heights depended on whether a visual straight-in approach, instrument approach or visual circling/circuit approach was being conducted. The procedure did not describe the height based on whether an arrival was coded in the FMS. Alliance advised that initially the flight did not flag an exceedance in Alliance’s flight data analysis program and would therefore not have been further reviewed had the flight crew not reported setting the incorrect QNH. Having reviewed the recorded flight data, Alliance initially determined that there were no speed exceedances, and although the descent rate exceeded 1,000 fpm between 1,000 and 500 ft, this was considered transitory in nature and therefore was permitted in accordance with the stabilised approach criteria. However, Alliance subsequently assessed that the duration of the speed exceedance was not momentary.
The captain and first officer were familiar with the content of the operations notice. The first officer identified the approach as a straight‑in visual approach and therefore made the appropriate callout of ‘1,000 ft’, assessed that the stabilised approach criteria were met, then called ‘stable’. The first officer reported that due to the ‘busyness of [turning] the corner’, this check may have occurred slightly below 1,000 ft. Additionally, they reported assessing that the airspeed was reducing as required and subsequent vertical speed exceedances were momentary and therefore acceptable within the criteria.
Prior to Alliance Airlines issuing operations notice 25‑038, 26 days prior to the occurrence, the stabilisation height for a visual approach in VMC was 500 ft. However, the captain assessed that the visual approach via the STAR and waypoint OBGOS was not specifically defined in the operations notice, either by a visual approach with a 5 NM final, or a visual circuit, which did not permit joining the circuit on a base leg. Further, that for the intent of a stabilised approach, the approach was more aptly comparable to a visual circuit, albeit that the aircraft entered the circuit on base leg before turning onto final. The captain therefore interpreted the applicable stabilisation height to be 500 ft. As pilot flying, the captain reported having flown the approach with the intent to be stable by 500 ft, and had observed that otherwise the airspeed was too high at 1,000 ft.
The ATSB assessed that the approach was a straight‑in visual approach, though by design had a final leg somewhat less than 5 NM, and therefore based on the operations notice, the applicable stabilisation height was 1,000 ft.
Safety analysis
The flight crew reported performing the transition checks, which required each flight crewmember setting and then crosschecking that all 3 altimeters were set to the correct pressure subscale. However, neither flight crewmember identified that the captain’s primary flight display (PFD) had not been switched from standard (STD) to barometric pressure (QNH). This was again missed at the required 5,000 ft check, which coincided with air traffic control (ATC) advising of a change in the QNH.
The flight crew also did not identify the error when they later crosschecked that the radio altitudes matched on both PFDs, when passing about 2,500 ft. It could not be determined why this was missed, but it resulted in the captain’s PFD indicating about 300 ft lower than the aircraft’s actual height.
Having the altimeter set correctly is important to ensure the aircraft is operating at the same height basis as other aircraft in the same airspace, and to ensure adequate separation from terrain. In this case, indicating 300 ft lower than actual did not increase the risk of a collision with terrain. Additionally, had the captain, as pilot flying, based the approach profile on the indicating lower altitude, it should have resulted in the aircraft being stabilised 300 ft higher than the stabilisation height. However, by that stage, the flight crew were referencing radio altitude rather than barometric altitude.
The captain reported identifying the discrepancy between the altimeter and the radio altitude at about 1,500 ft, during the turn onto final. Their focus on the discrepancy may have contributed to the delay in achieving the required stabilised speed. However, having assessed the required stabilisation height as 500 ft, the captain was unconcerned (although aware) that the airspeed was fast at 1,000 ft. The airspeed reduced below the stabilisation criterion by 800 ft.
The first officer’s assessment that the 1,000 ft stabilised height applied, and all requirements were met, was consistent with Alliance Airlines’ assessment that the vertical speed deviations were transient and acceptable within the stabilisation criteria. However, at 1,000 ft, the airspeed was 26 kt above the approach speed, with only a 10 kt exceedance permitted. The pilot monitoring did not call ‘unstable’ as required by the stabilised approach policy. This may have been influenced by the pilot monitoring experiencing the turn onto final as a ‘busy corner’, the required checks being completed slightly below 1,000 ft and an assessment that the airspeed was reducing.
The ATC speed instructions resulted in the aircraft being significantly faster than the published speeds during the standard instrument arrival (STAR). Additionally, the captain reported some pressure to keep the speed up during the approach. However, according to the Airservices Australia Aeronautical Information Publication (AIP), an ATC‑issued speed instruction only applied to the point where the flight crew would reduce the speed on the normal profile for the approach. Furthermore, if flight crew assessed a speed control instruction was unacceptable, they were to request an alternative.
The aircraft’s average descent rate was less than 2,000 fpm between about 14,000 ft to 5,000 ft, during which 270 kt airspeed was maintained. As Alliance permitted up to 3,000 fpm above 3,000 ft, there was opportunity to descend faster earlier in the approach, which would have facilitated more effective speed reduction later in the approach. The airspeed was below the 200 kt landing gear extension speed for about 1 minute before the landing gear fully extended during the turn onto final. As the airspeed was only above the required stabilised approach speed at 1,000 ft for 9 seconds, extending the landing gear, flap, and/or speed brake slightly earlier, would likely have ensured the stabilised criteria could be met.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the unstable approach involving Fokker 100, VH-FKF, near Perth Airport, Western Australia on 29 April 2025.
Contributing factors
The pilot flying incorrectly assessed that the applicable stabilisation height was 500 ft. As a result, they did not manage the aircraft's energy state to ensure the stabilised approach speed requirement was met by 1,000 ft.
The pilot monitoring did not announce that the approach was unstable when the speed‑related stabilised approach criteria was not met at 1,000 ft. This may have been influenced by workload, the required check being completed slightly late, and an assessment that the airspeed was reducing.
Other factors that increased risk
Passing the transition level, the captain inadvertently omitted to change the altimeter setting from standard pressure to QNH, resulting in the left altimeter indicating 300 ft lower than the right altimeter. Neither flight crewmember detected the incorrect setting during 2 subsequent checks prior to landing.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
Alliance Airlines
Honeywell
Airservices Australia
the Bureau of Meteorology
recorded flight data from the aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew
Alliance Airlines
Airservices Australia
the Civil Aviation Safety Authority
Fokker
the Dutch Safety Board.
Submissions were received from:
Alliance Airlines
Airservices Australia
Fokker
the Dutch Safety Board.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot flying (PF) and Pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 340 equates to 34,000 ft.
[3]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[4]Fly-by waypoint: a waypoint that requires turn anticipation to allow tangential interception of the next segment of a route or procedure.
[5]At and above transition level, the altimeter subscale is set to standard pressure 1,013.2 hPa. At and below transition altitude, the altimeter subscale is set to local or area QNH.
[6]Visual conditions: The pilot has established and can continue flight to the airport with continuous visual reference to the ground or water and visibility along the flight path is not less than 5,000 m.
[7]Radio altitude is the height of the aircraft above terrain immediately below the aircraft measured by a radio altimeter.
[9]Visual meteorological conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
Occurrence summary
Investigation number
AO-2025-025
Occurrence date
29/04/2025
Location
Near Perth Airport
State
Western Australia
Report release date
12/08/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Aircraft preparation, Unstable approach
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Fokker B.V.
Model
F28 MK 0100
Registration
VH-FKF
Serial number
11365
Aircraft operator
Alliance Airlines Pty Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Departure point
West Musgrave Airport (Mantamaru), Western Australia