The derailment of a freight train after it entered track that had been overtopped by floodwaters at Traveston in Queensland highlights the importance of serviceable environmental monitoring station equipment, an ATSB investigation final report highlights.
In the early hours of 23 February 2022, an Aurizon containerised freight service was travelling north on Queensland Rail’s North Coast line when the train entered a washed-out section of track near Traveston, the investigation report details.
The train derailed and its two locomotives rolled over, while three wagons derailed but remained upright. The single driver sustained minor injuries but was able to exit the lead locomotive.
The accident occurred after a period of heavy rainfall and significant floodwater run-off in the region.
“Prior to the accident, floodwaters had risen above the track and scoured areas of the ballast and formation supporting it,” ATSB Chief Commissioner Angus Mitchell said.
“Due to the weather conditions and it being night, the driver's visibility of the track ahead was impeded. The driver sighted the scoured track area at a distance that was insufficient to stop the train before it entered the affected area and subsequently derailed.”
The investigation found that an environmental monitoring station at Traveston had generated a critical flood alarm prior to the accident.
However, the required warning was not directly displayed at the relevant workstation at the Rail Management Centre, and email and text message alerts had not been correctly configured, with key personnel details left empty.
The investigation found the Queensland Rail alarm response procedure and automated messaging system used at the Rail Management Centre were ineffective in providing network operations staff timely notification of alarms from the environmental monitoring stations in the Glass House Mountains to Gympie North control area.
In addition, personnel located at the Fault Coordination Centre did not follow up with network control when the critical flood alarm was not acknowledged, because roles were not clearly defined, and the Fault Coordination personnel often dealt with multiple alarms at a time.
The investigation identified the operator’s training program did not ensure personnel at the Rail Management Centre proactively monitored an adverse weather event or responded to reports and other information of a condition that could present a hazard to train movements. Subsequently, the network operations personnel relied on the clearance of a signal to determine the integrity of the track through a known flood-prone area.
Further, the investigation determined that the environmental monitoring station rainfall sensor and closed-circuit television camera were unserviceable at the time of the derailment.
Queensland Rail has subsequently implemented comprehensive systemic improvements addressing identified deficiencies in the investigation.
“In response to this accident and the ATSB investigation, the network operator has taken action aimed to improve alarm notification systems, training programs, equipment serviceability protocols, and operational procedures to manage adverse weather events,” Mr Mitchell said.
The investigation also found that both the emergency exit pathway used by the driver to exit the overturned locomotive, and the emergency equipment available in the enclosed Aurizon 2800 class locomotives, were inadequate to enable a prompt escape by crew, and potentially limited access by emergency services in the event of a locomotive overturning.
In response, Aurizon has developed an access and egress compliance strategy to align its locomotive fleet to the relevant national rail standard, and is taking part in a development group reviewing the standard.
“This accident highlights the importance of having serviceable environmental monitoring station equipment, and for network operations personnel to be promptly and reliably alerted to any hazardous condition detected by the system,” Mr Mitchell concluded.
“It also highlights the importance of equipping locomotive rollingstock with systems to mitigate evacuation hazards that rail traffic crew may encounter following the derailment and rollover of a locomotive.
“This is particularly so when operating driver only and in remote locations where assistance may not be readily available.”
At 1851 local time on 24 July 2025, the crew of an Alliance Airlines Embraer ERJ 190, registered VH‑A2T, departed Cairns, Queensland, for a passenger transport flight to Brisbane. For the departure, the crew took off from runway 15 with a clearance to follow the AKROM 1 standard instrument departure (SID).
As the aircraft became airborne in darkness, the captain, acting as pilot monitoring, announced ‘pitch rate’ to alert the first officer, who was pilot flying, that the aircraft’s rotation had slowed. Both crewmembers then focused on the aircraft flight path, and the retraction of the landing gear was inadvertently omitted.
As the aircraft continued climbing and turning left to follow the SID, the flight crew received 2 radio altimeter annunciations and observed the flight director unexpectedly command a right turn. After completing the left turn to follow the SID, the first officer engaged the autopilot, and the aircraft started a right turn toward terrain. The captain identified the turn and instructed the first officer to turn left back to the required track.
As the aircraft then continued along the SID, the captain recognised that the landing gear was still extended and quickly retracted it. The landing gear completed retracting when the aircraft had reached a speed of 252 kt, 17 kt above the maximum landing gear retraction speed.
The flight continued and the aircraft landed at Brisbane without further incident at 2044. Following the flight, the aircraft was inspected and found to be undamaged.
What the ATSB found
The ATSB found that the 'pitch rate' announcement was made at a time when a ‘positive rate’ announcement would normally be expected. This resulted in both flight crewmembers focusing on the pitch angle and the first officer was not prompted to call for landing gear retraction.
As the aircraft turned left to follow the SID, the crew were presented with radio altimeter alerts and unexpected flight director indications. These distractions increased the flight crew's workload and delayed their identification of the extended landing gear. Upon recognising the still extended landing gear, the captain reflexively retracted it without first checking the aircraft speed.
What has been done as a result
Alliance Airlines accelerated its program to upgrade E190 aircraft from load 25 avionics to load 27 and at the time of the release of this report, all E190s in the Alliance Airlines fleet have been upgraded. This should prevent recurrence of the unexpected flight management system indications presented to the crew during this incident.
In addition, the load 27 avionics upgrade incorporated electronic checklists that require associated actions to be undertaken before the electronic checklist is completed.
Safety message
This incident highlights the impact a combination of omitted actions and distractions can have on aircraft operations, during what is often a high workload period. Such situations can create challenges in responding to the unexpected with potential for a reduction in safety when pilots act rapidly and reflexively. In these situations, pilots may not be able to effectively process information or consider all relevant factors, which reduces the ability to make good decisions.
Crews of Embraer ERJ 190 aircraft equipped with load 25 avionics should also be aware that, on occasion, these systems may provide unexpected indications. This has been observed on multiple occasions on the Cairns AKROM 1 SID. When faced with unexpected indications, crews should use primary instruments to ensure that flight path requirements are adhered to.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the evening of 24 July 2025, the crew of an Alliance Airlines Embraer ERJ 190, registered VH‑A2T, prepared to operate a passenger transport flight from Cairns to Brisbane, Queensland. For the flight, the captain acted as pilot monitoring (PM), and the first officer as pilot flying (PF).[1] For the departure, the crew were provided with clearance to follow the AKROM 1 standard instrument departure (SID) (see the section titled Cairns runway 15 AKROM 1 standard instrument departure). While preparing for the flight, the captain advised the first officer that on previous flights, the first officer’s rotation[2] rate was slower than required and, as adherence to the SID climb requirements was essential for terrain avoidance, the rotation rate would be a point of focus for the departure.
In darkness at 1851 local time, the aircraft commenced a take-off from runway 15 with the lateral navigation flight guidance mode selected. After passing the rotation speed of 143 kt, the first officer commenced the rotation to the target pitch attitude of about 15° nose up. The aircraft became airborne, and the captain assessed that as the aircraft passed 10° pitch angle, the rotation rate slowed. To alert the first officer, the captain announced, ‘pitch rate’.
This announcement came at about the same time that the PM would normally announce ‘positive rate’ after checking that a positive rate of climb was indicated on the aircraft instrumentation. This ‘positive rate’ announcement would then trigger the PF to request the retraction of landing gear. On this occasion, the lateral navigation mode activated and, after the captain announced ‘pitch rate’, both crewmembers then focused on the aircraft flight path and the retraction of the landing gear was inadvertently omitted.
The aircraft continued climbing and turning left to follow the SID. As the aircraft climbed through about 840 ft above mean sea level (AMSL), the primary flight displays presented 2 radio altimeter alerts in quick succession and the engine indicating and crew alerting system (EICAS) presented ‘RADALT MISCOMPARE’ and ‘APPR 2 NOT AVAIL’ messages (see the section titled Radio altimeter). The crew noted these indications and determined that they were not relevant to that phase of flight and therefore took no action.
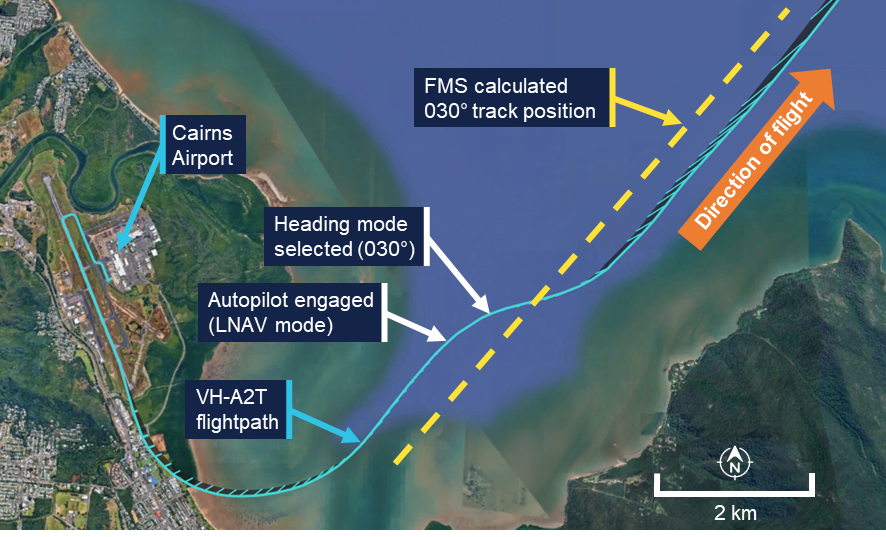
As the first officer manually turned the aircraft left to follow the SID, the aircraft followed a turn radius smaller than the flight management system’s (FMS) precalculated turn (see the section titled Flight instrumentation) and turned onto the SID 030° track[3] to the left of the FMS calculated track position (Figure 1). As the turn continued, the FMS targeted the wider track and the crew observed the flight director indications on the primary flight display unexpectedly command a right turn. The first officer briefly followed the right turn command by reducing the angle of bank from 24° left to 10° left before then increasing the angle back to 20° left to complete the turn.
Once the first officer established the aircraft on a 030° track, the autopilot was engaged while the flight director continued to indicate a right turn. The autopilot then started a right turn to intercept the FMS calculated 030° track position. At about the same time, air traffic control instructed the crew to change radio frequency. As the aircraft commenced the right turn, the captain identified the turn away from the SID track toward the high terrain and instructed the first officer to turn left to follow the 030° track. The first officer then engaged the autopilot heading mode and selected 030° and the aircraft turned left to a heading of 030° and continued climbing.
Figure 1: Departure flight path (initial)
Source: Recorded data from VH-A2T and Google Earth, annotated by the ATSB
The aircraft then continued along the SID and after climbing above 4,000 ft AMSL, turned right toward the waypoint AKROM. As the aircraft continued climbing toward AKROM, the captain, whose headset was not noise-cancelling, noted that the ambient noise was louder than expected and recognised that the landing gear was still extended. At about the same time, the first officer noted the landing gear extended indication on the EICAS. In response, while the aircraft was accelerating through 243 kt – 8 kt above the maximum landing gear retraction speed of 235 kt – the captain retracted the landing gear without first checking the indicated airspeed. The landing gear completed retracting when the aircraft had reached a speed of 252 kt, 17 kt above the maximum retraction speed (Figure 2).
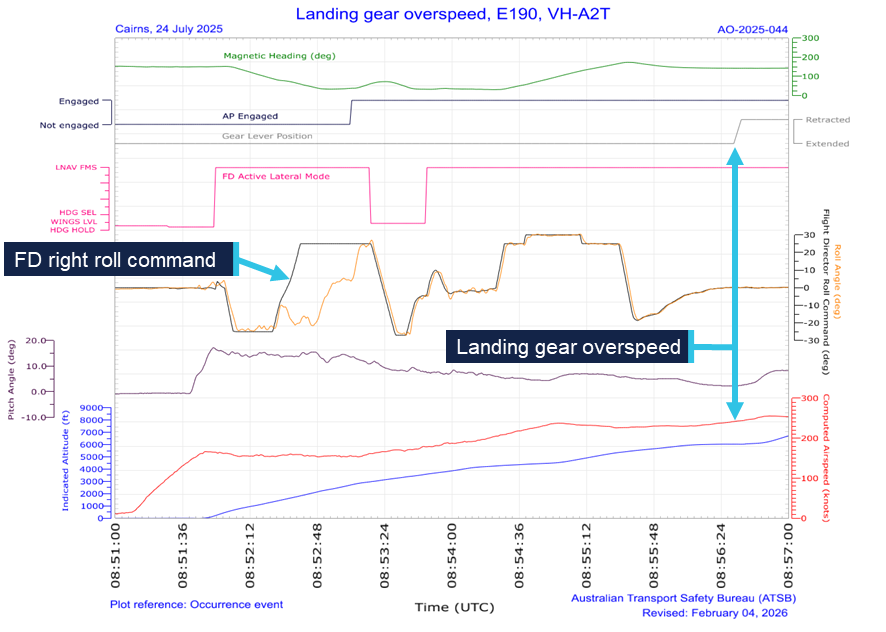
Figure 2: Departure flight path
Source: Recorded data from VH-A2T and Google Earth, annotated by the ATSB
The flight continued and, at 2044, the aircraft landed at Brisbane without further incident. Following the flight, the aircraft was inspected and found to be undamaged.
Context
Flight crew details
The captain held an Air Transport Pilot Licence (Aeroplane) and a class 1 aviation medical certificate. The captain had 15,192 hours of flying experience, of which 1,680 hours were on the Embraer 190 aircraft type, with 137 hours accrued in the previous 90 days.
The first officer held an Air Transport Pilot Licence (Aeroplane) and a class 1 aviation medical certificate. The first officer had 6,131 hours of flying experience, of which about 1,353 hours were on the Embraer 190 aircraft type, with 213 hours accrued in the previous 90 days.
The ATSB found no indicators that the flight crew were experiencing a level of fatigue known to adversely affect performance.
Operational information
Cairns Airport runway 15 AKROM 1 standard instrument departure
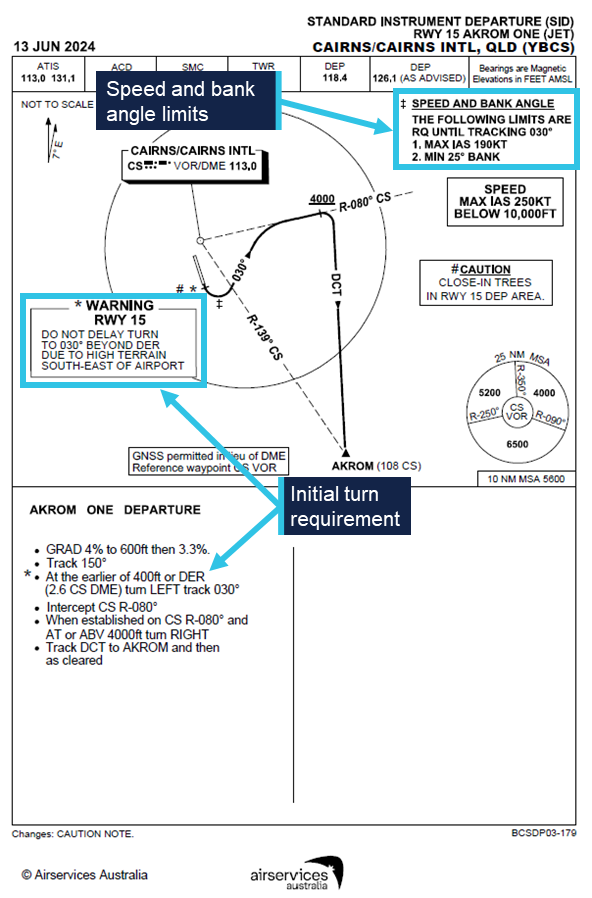
High terrain partly encircles Cairns Airport from the north-west through south-west and to the south-east. To avoid the high terrain, the AKROM 1 standard instrument departure (SID) required aircraft departing runway 15 to make a left turn at the earlier of either reaching 400 ft AMSL or passing the departure end of the runway (DER) (Figure 3). During the turn, flight crew needed to maintain a bank angle of at least 25° and a speed of no more than 190 kt until the aircraft was established on a track of 030°. The location of the 030° track was dependent upon both the position that the left turn was commenced and the radius of the turn. The departure required maintenance of the 030° track until intercepting the 080° radial of the Cairns very high frequency omni range navigation aid (VOR) and then followed that track until the aircraft climbed above 4,000 ft AMSL. The departure then turned to the waypoint AKROM.
Figure 3: Runway 15 AKROM 1 standard instrument departure
Source: Airservices Australia, annotated by the ATSB
Take-off standard operating procedures
The operator’s standard operating procedures manual (SOPM) required the pilot monitoring (PM) to verify a positive rate of climb immediately after take-off and then announce ‘positive rate’. After that announcement, the pilot flying (PF) confirmed the positive rate of climb and called for the landing gear to be retracted, and the PM then selected the landing gear ‘up’.
The SOPM also specified a normal rotation rate of 3° of pitch angle per second.
Aircraft information
The aircraft was an Embraer ERJ 190‑100 IGW, manufactured in Brazil in 2008 and issued serial number 19000179. It was registered in Australia as VH-A2T on 19 July 2024. The aircraft was fitted with 2 General Electric Company CF34-10E5 turbofan engines.
The maximum indicated airspeed at which the landing gear could be retracted or extended was 235 kt and the maximum airspeed with the landing gear in the extended position was 265 kt.
Flight instrumentation
The ERJ 190 was equipped with an integrated avionics system. VH-A2T was equipped with a ‘load 25’ version of the avionics. At the time of the incident, Alliance Airlines operated ERJ 190 aircraft equipped with both ‘load 25’ and upgraded ‘load 27’ avionics.
The flight management system (FMS) in ‘load 25’ equipped aircraft was designed to dynamically calculate the location of down path tracks, but only when these paths were inactive. Once the path became active, their location was fixed. The system should have predicted the 030° track leg of the AKROM 1 SID relative to where the system sequenced the 400 ft altitude crossing or departure end of the runway point. The avionics manufacturer, Honeywell, advised that in this case, the FMS sequenced the termination of the 400 ft altitude leg early and appeared to fix the location of the 030° track leg before it could be updated based on the position of the commencement of the left turn.
Subsequently, and as intended by design, the FMS did not recalculate the location of the 030° track during the turn. As a result, when the crew turned to the 030° track to the left of the FMS precalculated track, the FMS, still targeting the wider track, commanded a right turn to intercept that track (Figure 4).
Figure 4: Representation of primary flight and navigation displays during the left turn
Note: The figure is based on an animation of the incident. The flight director representation is different to actual aircraft, and indications are included that are not presented in the actual aircraft. Negative roll values indicated a left turn, positive a right turn. Source: Embraer, annotated by the ATSB
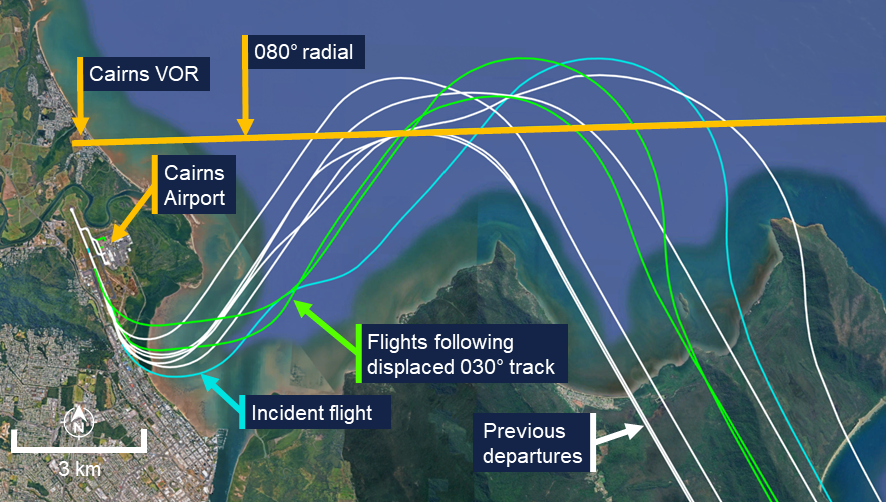
Recorded automatic dependent surveillance broadcast (ADS-B) data from previous AKROM 1 departures flown by VH-A2T identified 2 additional flights where the FMS had precalculated the 030° track at a wider location. On those occasions, the ADS-B data indicated that the flight crews followed the flight director commands and intercepted the wider track (Figure 5).
Figure 5: Departures of VH-A2T equipped with ‘load 25’ avionics
Source: Recorded data from VH-A2T and Google Earth, annotated by the ATSB
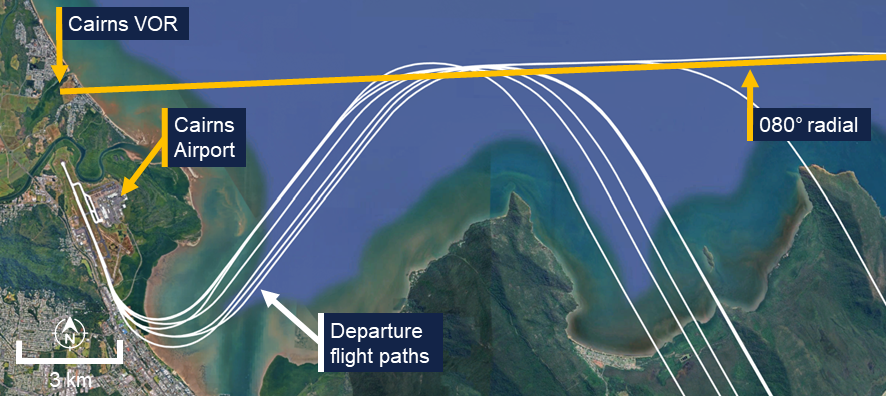
For ‘load 27’ equipped aircraft, the flight path was continuously updated as FMS track legs were flown and while in transition between them. This resulted in more accurate tracking of departure paths (Figure 6).
Figure 6: Departure paths of an E190 equipped with ‘load 27’ avionics
Source: Recorded data from VH-UYY and Google Earth, annotated by the ATSB
Radio altimeter
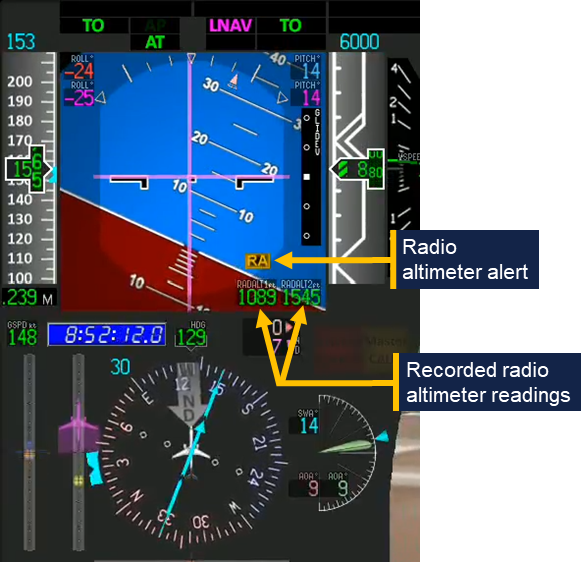
The Embraer ERJ 190 was fitted with 2 radio altimeters. These provided each crewmember with an indication of the height of the aircraft above underlying terrain measured using radio waves. When a difference in the height measured by the 2 radio altimeters exceeded a dynamic threshold, an ‘RA’ alert was presented on the primary flight display (Figure 7) and the RADALT MISCOMPARE alert was presented on the EICAS. Whenever this condition was detected, the associated EICAS message APPR 2 NOT AVAIL was also displayed.
Figure 7: Radio altimeter alert
Note: The figure is based on an animation of the incident and indications (such as the radio altimeter readings) are included that are not presented in the actual aircraft. Source: Embraer, annotated by the ATSB
United States Federal Aviation Administration Advisory Circular AC 25-7D Flight Test Guide for Certification of Transport Category Airplanes stated the following guidance and measurement conditions for radio altimeter certification:
32.1.5.5 Radio Altimeter System.
32.1.5.5.1 The radio altimeter system should display to the flightcrew, clearly and positively, the altitude information that indicates the airplane main landing gear wheel height above terrain.
32.1.5.5.2 Verify that the altimeters display altitude without loss of signal indications or excessive fluctuations, under the following measurement conditions:
• Pitch angle ±5° about the mean approach attitude.
• Roll angle zero to ±20°.
On departure from Cairns, the alerts were generated while the aircraft was operating over relatively flat terrain and when the aircraft’s pitch angle was about 14° nose up and the roll angle about 23° left. While the investigation did not determine the reason for the different radio altimeter readings that led to the radio altimeter alerts, the aircraft’s pitch and roll values at the time exceeded the guidance and measurement conditions specified in the FAA circular.
Light and meteorology
The departure was conducted in night visual meteorological conditions. The sun had set at 1802, 49 minutes before the departure, and the moon was below the horizon.
At the time of the departure, the Bureau of Meteorology automatic weather station at Cairns Airport recorded the temperature as 23°C and the wind as 9 kt from 161° magnetic. There was no recorded cloud, and visibility was recorded as 58 km.
Recorded data
Analysis of flight data from the flight data recorder fitted to VH‑A2T showed that the rotation rate during the take‑off was 1.49 degrees per second until the aircraft was pitched 9.7° nose up and then 1.73 degrees per second until 14.9° nose up. The pitch attitude stabilised at about 16° nose up during the turn.
As the aircraft turned left through a heading of 080°, the flight director began commanding a right turn (Figure 8). At 1853:08, the autopilot was engaged in the lateral navigation mode and while the flight director continued to command a right turn. The aircraft then rolled right, following that command. At 1853:20, while flying a heading of 058° the autopilot mode changed from lateral navigation mode to heading mode with 030° selected. The aircraft then began rolling left to turn to that heading.
At 1856:35, the landing gear was selected up at a speed of 243 kt. The landing gear completed the retraction sequence at 1856:47 as the aircraft accelerated to 252 kt.
Cockpit voice recorder data capturing the incident was not available as it had been overwritten.
Figure 8: Recorded flight data
Source: ATSB
Safety analysis
Non-retraction of landing gear
During the take-off, the first officer rotated the aircraft slower than required, prompting the captain to call for an increase in pitch rate. The captain’s attention then remained focused on monitoring the pitch attitude of the aircraft throughout the rotation manoeuvre to ensure the required pitch attitude targets were being achieved. Because of this, the captain likely did not have sufficient opportunity to move onto the next task, verifying the aircraft’s positive rate of climb, before it passed through 400 ft – the point at which the terrain avoidance turn was to be initiated. Consequently, the task step of verifying and announcing positive climb performance was not fully completed and the captain did not make the ‘positive rate’ announcement.
In the absence of the captain’s announcement, the first officer was not prompted to request landing gear retraction, and the landing gear remained extended. The captain’s announcement of ‘pitch rate’ at about the same time that the acoustically and semantically similar ‘positive rate’ announcement would normally be made, potentially caused interference in working memory (Lentoor 2023) and possibly gave both flight crew a false sense that the latter action had been successfully performed.
Delayed identification and overspeed
During the initial climb, which was a high workload phase of the flight, abnormal radio altimeter alerts and unexpected flight director indications further increased the flight crew’s workload. In particular, when the autopilot was engaged, it commenced a right turn toward high terrain in response to an unexpected flight director indication. This prompted the captain’s intervention and the crew’s attention then narrowed to focus on parameters which would enable them to verify the aircraft’s lateral tracking performance. Wickens (2009, 2021) notes that attentional tunnelling occurs under conditions of elevated stress and deliberate task focus and can cause other task-relevant stimuli to be ignored.
Consequently, increasing flight deck wind noise and abnormal engine indicating and crew alerting system (EICAS) indications, both of which provided an indication of the landing gear’s extended state, were not initially detected. Furthermore, the turn and speed restrictions of the departure also likely masked the performance degradation due to the extended landing gear, further reducing the likelihood of identifying that it was still extended.
As the flight crew’s workload decreased in the latter portion of the departure, the effects of attentional tunnelling reduced, and the noise from the landing gear increased as the aircraft accelerated. The captain (whose headset was not noise-cancelling) then detected the increased cockpit wind noise and was alerted to the misconfiguration of the landing gear. At about the same time, the first officer identified the landing gear extended indication on the EICAS.
As the aircraft had travelled well beyond the normal gear retraction point and was accelerating, the captain likely perceived some urgency to act upon noticing that the landing gear was still extended and experienced associated increased stress. Under such conditions research has shown that people often do not make optimal decisions and may act more reflexively (Dismukes and others, 2007).
Under time pressure and stress, experts may revert to a recognition primed decision mode (Klein, 2014), making rapid and intuitive interpretations of a situation and selecting actions based on their most familiar experiences.
The landing gear was normally retracted well below the retraction limiting speed, and this speed was not normally checked by the other crew member. Therefore, the captain reverted to their most familiar experience and initiated gear retraction without first confirming the action with the first officer and did not check the gear retraction limiting speed. Consequently, the landing gear retraction was initiated 8 kt above the 235 kt retraction limit speed and the retraction completed 17 kt above that speed.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the landing gear overspeed involving Embraer E190, VH-A2T on 24 July 2025.
Contributing factors
After take-off, the pilot monitoring made a 'pitch rate' announcement at a time when a 'positive rate' announcement would normally be expected. This resulted in both flight crewmembers focusing on the pitch angle and the pilot flying was not prompted to call for gear retraction. Subsequently the crew's attention was focused on following the departure flight path and the landing gear was not retracted.
As the aircraft turned left to follow the standard instrument departure, abnormal radio altimeter indications were presented, and the flight management system unexpectedly commanded a right turn. When the autopilot was engaged, the aircraft briefly followed the commanded turn before the captain intervened. These distractions increased the flight crew's workload and delayed their identification of the extended landing gear.
After recognising that the landing gear was still extended, the captain reflexively retracted the landing gear at a speed above the maximum landing gear retraction speed.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Alliance Airlines
Alliance Airlines has accelerated its program to upgrade E190 aircraft from load 25 avionics to load 27 and at the time of the release of this report, all E190s in the Alliance Airlines fleet have been upgraded. This should prevent recurrence of the unexpected flight management system indications presented to the crew during this incident.
In addition, the load 27 avionics upgrade incorporated electronic checklists that require associated actions to be undertaken before the electronic checklist is completed.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
Alliance Airlines
the aircraft and avionics manufacturers
Bureau of Meteorology
recorded data from VH-A2T.
References
Dismukes, R., Goldsmith, T. E., & Kochan, J. A. (2015). Effects of acute stress on aircrew performance: literature review and analysis of operational aspects. National Aeronautics and Space Administration Technical Memorandum, NASA/TM-2015-218930.
Klein, G. (2014). The recognition-primed decision (RPD) model: Looking back, looking forward. In Naturalistic decision making (pp. 285-292). Psychology Press.
Lentoor, A. G. (2023). Cognitive and neural mechanisms underlying false memories: misinformation, distortion or erroneous configuration? AIMS neuroscience, 10(3), 255.
Wickens, C. D., & Alexander, A. L. (2009). Attentional tunnelling and task management in synthetic vision displays. The international journal of aviation psychology, 19(2), 182-199.
Wickens, C. D., & Carswell, C. M. (2021). Information processing. In Handbook of human factors and ergonomics (pp. 114-158). John Wiley & Sons.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the flight crew
Alliance Airlines
the aircraft manufacturer
the avionics manufacturer
Civil Aviation Safety Authority
the United States National Transportation Safety Board.
Submissions were received from:
the flight crew
Alliance Airlines
the aircraft manufacturer
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Rotation: the positive, nose-up, movement of an aircraft about the lateral (pitch) axis immediately before becoming airborne.
[3]All tracks and headings mentioned in the report are magnetic.
On 13 September 2024, a BRM Aero Bristell Classic, registered 23-2136, collided with terrain about 32 km south of Bendigo aerodrome, Victoria. The pilot was fatally injured and the aircraft was destroyed by post-impact fire.
As part of an investigation by the Coroners Court of Victoria, Victoria Police requested assistance from the ATSB in the examination of components from the aircraft. The ATSB commenced an investigation under the Australian Transport Safety Investigation Act 2003.
The ATSB has completed its work recovering the recorded flight path data from the supplied avionics. A copy of the data and a report detailing the work undertaken by the ATSB was provided to Victoria Police on 17 March 2026.
Any enquiries relating to the investigation should be directed to Victoria Police.
Last updated:
Occurrence summary
Investigation number
AE-2024-007
Occurrence date
13/09/2024
Location
32 km south of Bendigo Airport
State
Victoria
Investigation type
External Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
BRM Aero S.R.O.
Model
Bristell Classic
Registration
23-2136
Sector
Piston
Operation type
Part 103 Sport and recreational aircraft
Activity
General aviation / Recreational-Sport and pleasure flying-Pleasure and personal transport
On the morning of 16 June 2025, a Cessna 182T departed a private aircraft landing area south of Emerald, Queensland, with a pilot and a passenger on board for a private flight to Atherton, Queensland.
Prior to their departure the pilot had obtained the weather conditions for Mareeba Airport, about 22 km to the north of their intended destination of Atherton, and assessed the conditions as acceptable for visual flight.
When the aircraft was about 95 km north of Charters Towers, the pilot assessed they would be unable to continue their direct track towards Atherton due to the cloud height over the terrain ahead. The pilot diverted west to avoid higher terrain and planned to divert to Mareeba due to its lower elevation by approaching from the west.
About 35 minutes after the diversion, the pilot descended the aircraft to about 500 ft above ground level, following a road. As they tracked towards rising terrain, their height reduced to about 200 ft above ground level. The pilot recalled that suddenly conditions ahead became a ‘white-out’ and they commenced a left turn and reduced the aircraft’s power in an attempt to avoid flying into the cloud.
During the turn the aircraft entered cloud and the pilot lost visual reference with the ground. Recorded data indicated the aircraft conducted a 360° left turn with several changes in altitude and coming in close proximity to terrain before the pilot could engage the autopilot to attempt to stabilise the aircraft.
The pilot then commanded a 180° left turn using the autopilot, intending to return to visual meteorological conditions. However, as the aircraft climbed, the air speed reduced and the aircraft likely stalled, leading to a rapid descent.
The pilot received a terrain warning and immediately applied recovery actions; as they eased out of the dive, the pilot momentarily became visual with terrain before the aircraft contacted tree-tops but continued to remain airborne.
The pilot was able to maintain control and became visual again on top of the cloud layer and, with the aircraft significantly damaged, diverted to Charters Towers Airport.
What the ATSB found
The pilot’s pre-flight planning was inadequate for the intended flight. The pilot had planned the second leg of the flight at a height that would not have allowed sufficient safe margin from terrain. While they obtained the forecast weather for a location close to their destination, which identified local conditions were suitable for visual flight, the pilot did not obtain the required graphical area forecast which indicated cloud height below terrain level on the flight planned track. Had the pilot obtained the area forecast this likely would have influenced their decision to commence the flight or plan an alternate route.
After encountering low cloud, the pilot continued flight towards the destination and into rising terrain, this forced them to descend below safe terrain clearance altitudes to a height of about 200 ft above ground level, rather than divert or return.
In an attempt to turn around, the aircraft entered cloud. The pilot was not rated for instrument flight, became spatially disorientated, resulting in a near collision with terrain.
While still in instrument meteorological conditions and disorientated, the pilot initiated a climbing turn and engaged the autopilot at reduced power. This resulted in the aircraft being unable to maintain airspeed and it likely entered a stall and rapidly lost height. During the recovery, the aircraft then impacted trees however continued to fly.
The pilot used the aircraft instruments to navigate out of cloud, regain visual reference to the ground and track south. Although the pilot was aware of the potential for damage sustained to the aircraft during the impact with the tree, they continued flight in the damaged aircraft for about 1.5 hours to Charters Towers (a familiar airport with a longer runway) rather than seek the nearest suitable landing area.
Safety message
Thorough information gathering is an essential part of a pilot’s pre-flight preparation. This is especially important in a single-engine aircraft and includes studying maps and routes to establish appropriate flight heights over terrain where forced landing areas may be limited. Weather conditions often vary over large distances and this is more likely over areas of elevated terrain. Although individual locations may indicate favourable conditions, other more widespread weather conditions, unsuitable for visual flight, may exist outside of the forecast location. Use of all available resources to ensure accurate knowledge of the expected conditions will assist pilots with informed decision‑making, both before and during flight.
It should be accepted that flying under visual flight rules will not always enable you to reach your planned destination. Making an early decision to land or divert and to resist the urge to ‘press on’ may prevent flight into marginal weather conditions and ultimately disaster.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
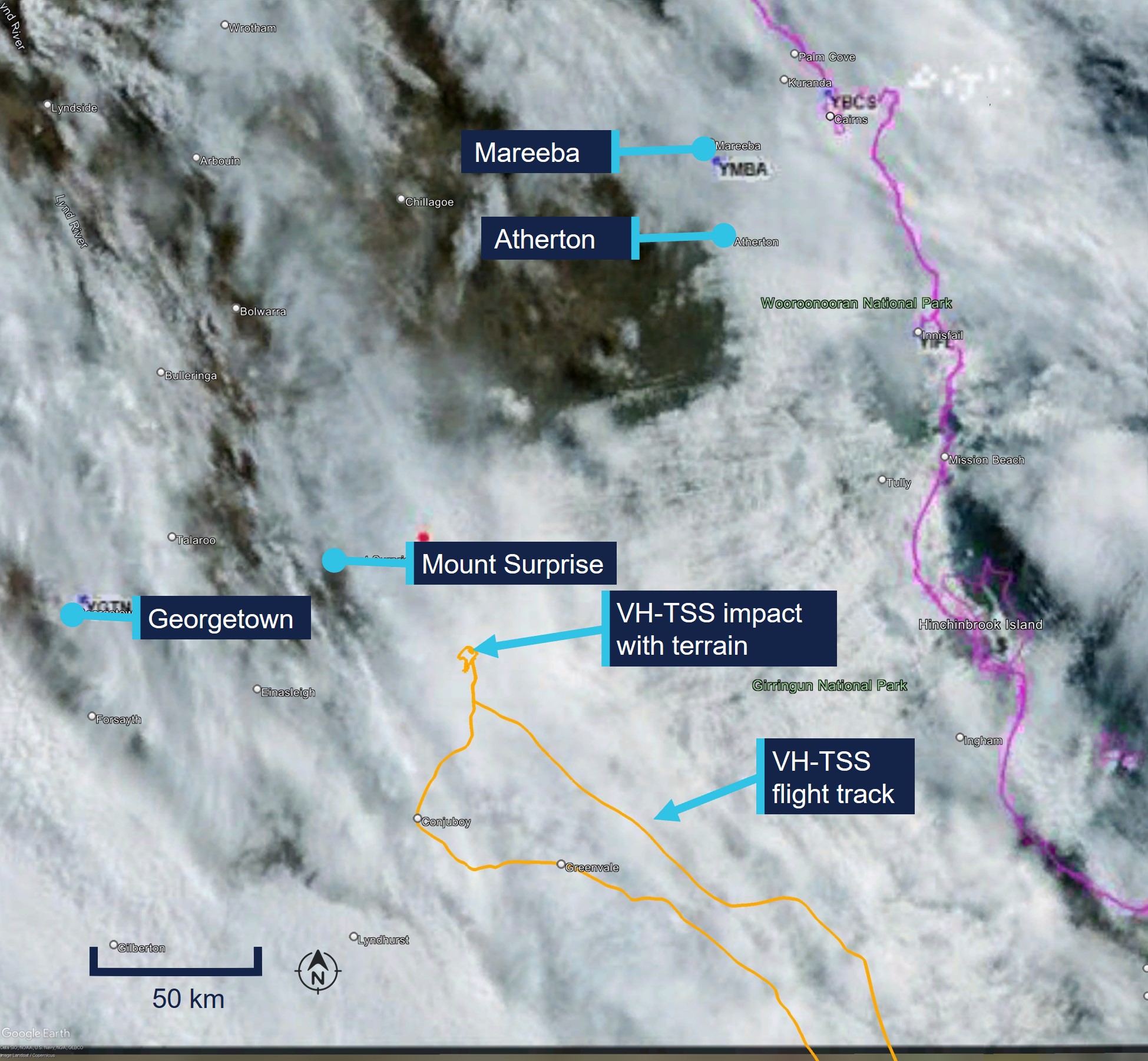
On 16 June 2025, at 0634 local time, a Cessna 182T, registered VH-TSS, departed a private aircraft landing area (ALA) about 16 NM south‑south-east of Emerald, Queensland, for a private flight to Atherton, Queensland. On board the aircraft were the pilot and one passenger.
Electronic flight data showed the aircraft departed and climbed to 4,500 ft above mean sea level (AMSL) where it initially held a steady track towards Atherton (Figure 1).
Figure 1: VH-TSS flight track between 0828 and 1115
Source: Google Earth, overlaid electronic flight data, annotated by the ATSB
At 0848, the aircraft descended to 3,000 ft AMSL, about 35 NM north of Charters Towers. The pilot then assessed that cloud and reduced visibility would affect continued visual flight direct to Atherton. The pilot stated they elected to continue, however diverted around weather to Mareeba Airport which they had planned as an alternative destination due to the lower elevation. They stated that they were familiar with the area, having flown a similar route 7 or 8 times previously and reported that they assessed the weather for Mareeba several times during the flight. At 0855 the aircraft was about 50 NM north of Charters Towers at an altitude of about 2,900 ft AMSL, about 1,650 ft above ground level (AGL).
The pilot recalled altering their heading to avoid weather and flying over higher terrain. The aircraft tracked generally in a north-west direction with numerous adjustments to the heading and altitude for about 35 minutes.
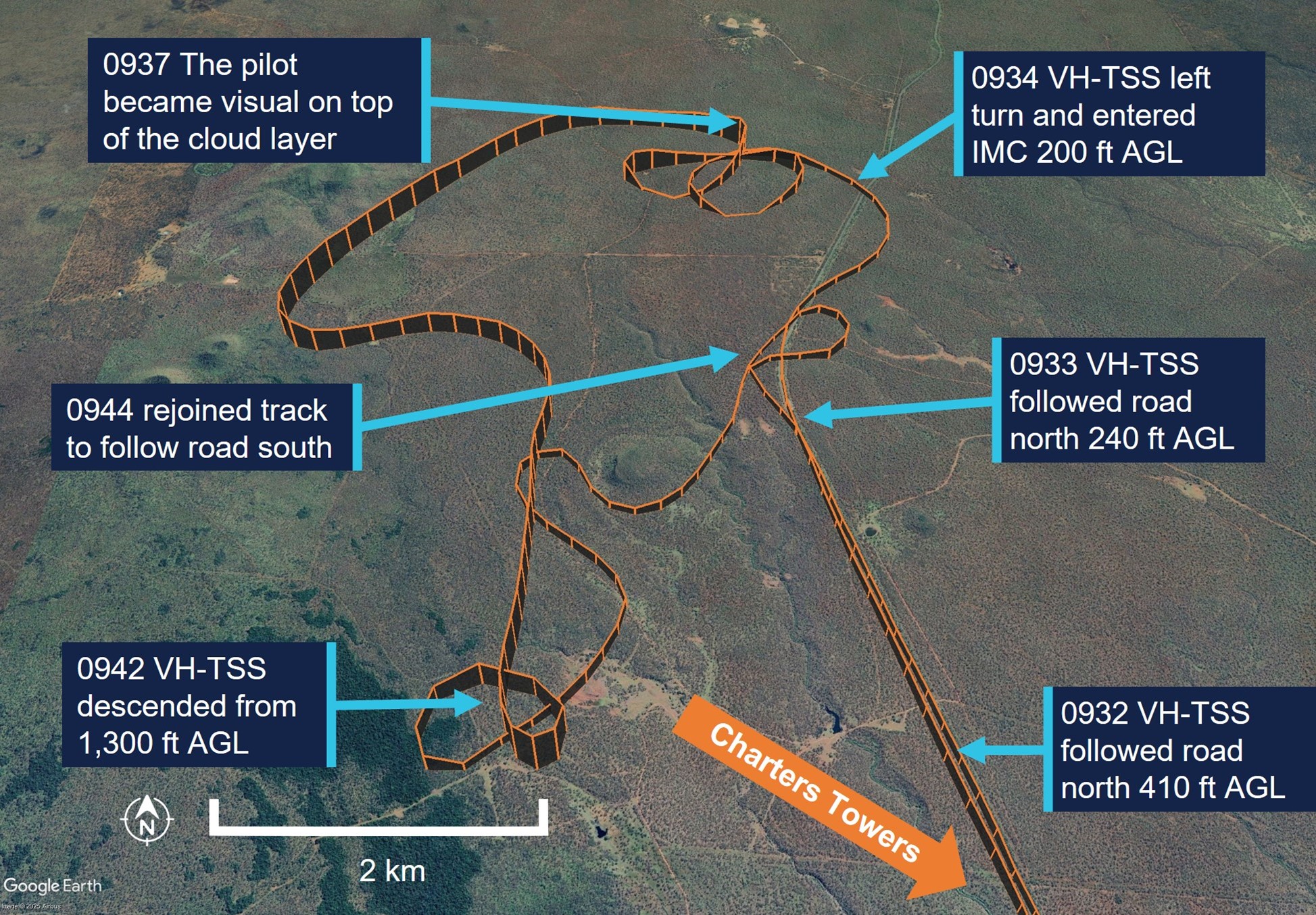
At 0930 the aircraft was recorded at about 530 ft AGL. The pilot recalled following Kennedy Developmental Road to the north. They reported this decision was due to the low cloud ceiling and advised that, in their experience, the road usually avoided the areas of highest terrain.
At 0932, the aircraft was recorded at about 410 ft AGL and the pilot made several heading adjustments to maintain visual reference with the road due to reducing visibility under heavy cloud cover.
At 0933 and about 90 NM south-west of Mareeba, the aircraft was recorded at about 240 ft AGL, with the pilot continuing to track following the road in a northerly direction.
About a minute later at about 200 ft AGL and 140 kt airspeed (Figure 2), the pilot recalled commencing a left turn and reduced the aircraft’s engine power to try to avoid flying into ‘white-out’ conditions ahead. However, during the turn, the pilot recalled that they entered cloud.
Figure 2: VH-TSS flight track between 0932 and 0946
Source: Google Earth, annotated by the ATSB
In the following minute, the aircraft continued a left turn and completed an orbit with several significant altitude changes, descending and climbing twice then descending again. The recorded altitude, which may not be an accurate representation of the aircraft’s actual altitude during manoeuvres, varied between 0 ft AGL on the second descent (the pilot did not report any impact occurring at this point) and 700 ft about 20 seconds later.
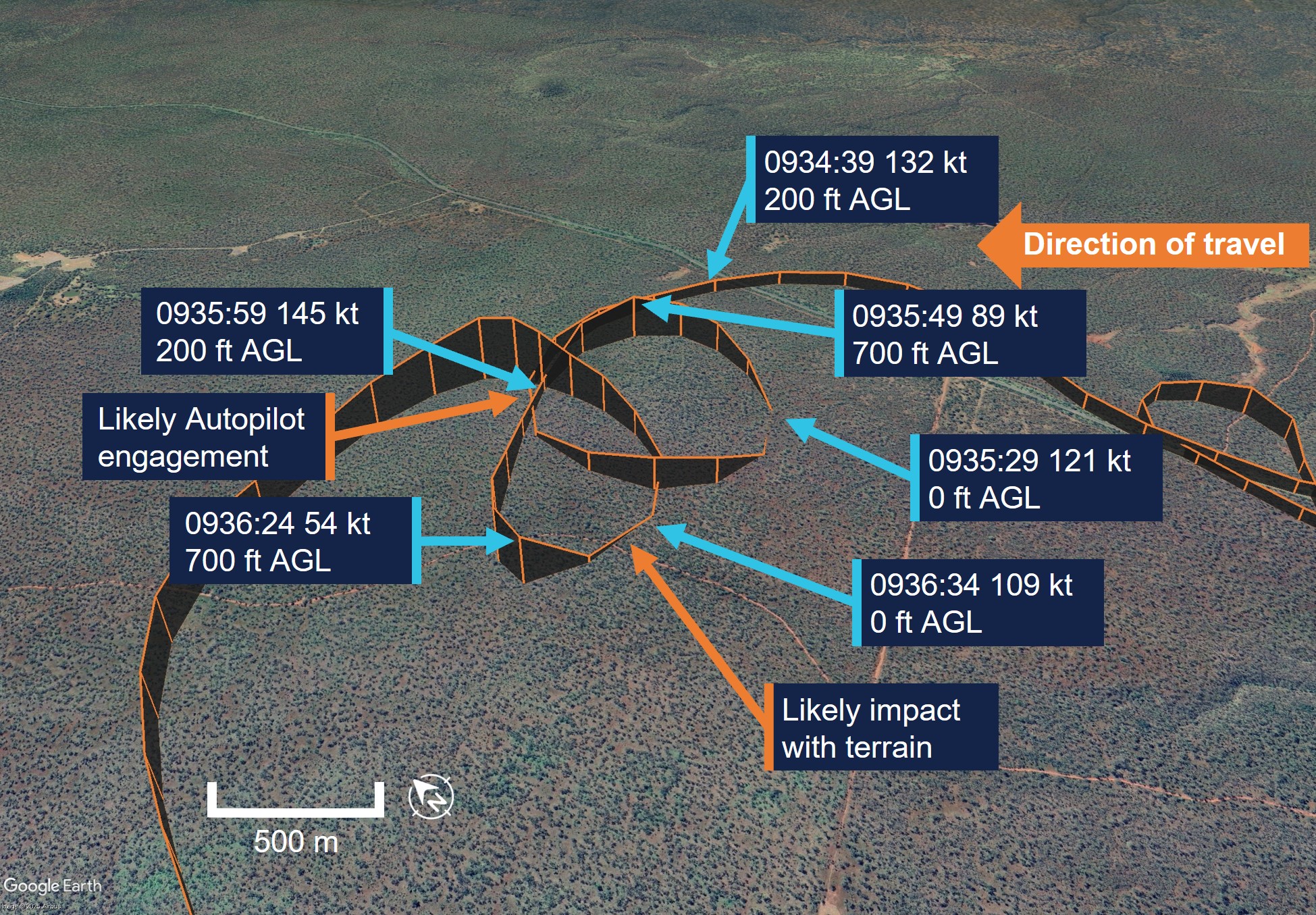
At 0936, having descended a third time to about 200 ft, the aircraft began to maintain a constant heading for about 20 seconds during which time it had a high rate of climb consistent with the engagement of the autopilot (see Autopilot). The aircraft climbed from about 200 ft to 700 ft AGL and reduced groundspeed to 54 kt. The pilot recalled they engaged the autopilot after entering cloud (this was likely after about 1–2 minutes after entering cloud) and then commanded a 180° left turn, in an attempt to reverse their track and navigate out of the instrument meteorological conditions (IMC) (Figure 3). During the next 10 seconds, the aircraft turned sharply left and descended rapidly. The pilot recalled the aircraft instrument panel went red and displayed a terrain warning and immediately applied right rudder and attempted to level the aircraft during the recovery, as it descended almost to ground level.
Figure 3: VH-TSS flight track between 0934 and 0938
Source: Google Earth, annotated by the ATSB
The pilot reported that they momentarily became visual and heard the aircraft impact trees. They pulled back on the control column and commenced a climb, entering IMC again. The pilot climbed to an altitude of about 1,000 ft AGL and was able to stabilise the aircraft and navigate out of IMC using the instruments. They became visual again once on top of the layer of cloud.
At 0942 the pilot descended from 1,000 ft to about 300 ft AGL. They then navigated back to Kennedy Developmental Road at a height of 200–350 ft AGL.
The pilot reported that they were unable to see the leading edge of the wing and unaware of the extent of the damage to the aircraft after the collision, however recalled the aircraft required more right rudder application than usual and that this prevented autopilot engagement. As a precaution, the pilot chose to follow major roads so that they could land if required and navigated the aircraft back to Charters Towers due to the runway length and their familiarity with the airport. The aircraft landed safely at 1114 local time.
As a result of the impact with the tree, the aircraft sustained substantial damage to the left wing (Figure 4), with minor damage to the left wing strut and both landing gear struts. No injuries were reported by either occupant.
Figure 4: Left wing damage
Source: Pilot
Context
Pilot information
The pilot held a valid Private Pilot Licence (Aeroplane) with a single engine aircraft rating since 1992. Their last flight review was conducted on 30 June 2023 and was valid to 31 July 2025. At the time of the occurrence, the pilot had about 3,580 hours total aeronautical experience of which 3,340 hours were reported to be on the Cessna 182. The pilot also reported that they had flown 48.5 hours during the last 90 days.
The pilot did not hold an instrument rating and was only rated to fly in visual meteorological conditions (VMC).[1]
The pilot held a valid class 2 medical certificate that was issued on 3 November 2023 and was valid until 12 November 2025. The class 2 was issued with a restriction requiring that reading correction must be available in flight and that the pilot must not fly within 24 hours of medical therapy.
Fatigue
The pilot reported that at the time of the occurrence they felt fully alert and wide awake. They indicated that they had slept 8 hours in the last 24 hours and 17 hours in the last 48 hours prior to the occurrence.
The ATSB considered that fatigue was unlikely to have affected the pilot’s performance at the time of the occurrence.
Instrument flight
As part of the pilot’s initial flight training for their licence, they recalled conducting 2–3 hours instrument flying with no visual references. However, since that time, they reported that they had not conducted any further instrument flight since their initial training.
Aircraft information
The Cessna 182T is a 4-seat, single engine, high-winged aircraft and is powered by a 6‑cylinder fuel-injected 235 hp (175 kW) Lycoming TIO-540-AK1A piston engine.
VH-TSS was manufactured in the United States in 2005 and was first registered in Australia to the pilot in April 2010. The aircraft was certified to be flown by day and night under visual flight rules (VFR)[2] and was only operated for private operations.
The pilot recorded the total time in service of the aircraft as 2,761.8 hours after arriving at Charters Towers.
Cessna 182 stall speeds
The Cessna 182T pilot operating handbook (POH) indicated the following stall speeds for the aircraft.
- flaps up, power idle 54 knots calibrated airspeed[3] (KCAS)
- flaps full, power idle 49 KCAS
The POH indicated that 54 KCAS would show as 50 kt indicated airspeed (IAS) to the pilot with no flap selected.
The POH also stated the stall speeds at known angles of bank at the aircraft’s maximum all up weight of 1,406 kg. The POH indicated that the stall speeds increased as the aircraft’s angle of bank increased.
Garmin G1000 terrain proximity
The aircraft instrument panel contained the Garmin G1000 display unit, which consisted of a primary flight display and multifunction display.
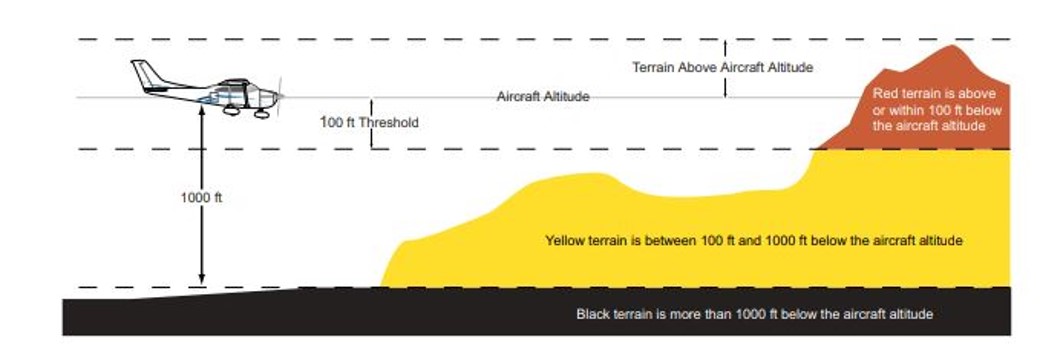
Colours are used to represent obstacles and aircraft altitude when the terrain proximity page is selected for display. Terrain proximity uses black, yellow, and red to represent terrain information relative to aircraft altitude. The colour of each obstacle is associated with the altitude of the aircraft (Figure 5):
black indicates terrain more than 1,000 ft below aircraft altitude
yellow indicates terrain between 100 ft and 1,000 ft below the aircraft altitude
red indicates terrain is above or within 100 ft below the aircraft altitude.
Figure 5: Garmin terrain proximity caution and warning
Source: Garmin G1000 pilot’s guide Cessna NAV III
Autopilot
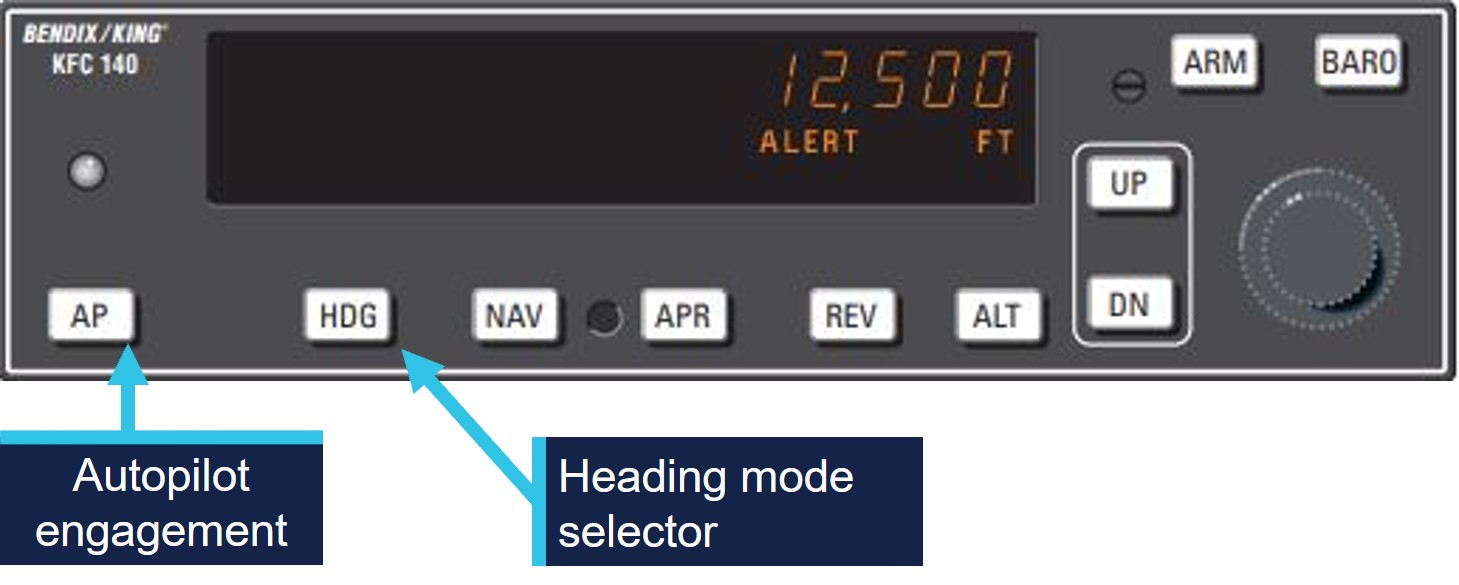
VH-TSS was fitted with a KAP 140 2-axis autopilot system, which provided both lateral and vertical modes and allowed the pilot to preselect an altitude.
The KAP 140 manual stated that when the autopilot was initially engaged, it activated the basic roll mode which levelled the aircraft wings and also engaged the vertical speed hold mode. This would capture the aircraft’s current vertical speed at the time of the autopilot engagement.
The manual provided a warning on the use of vertical speed mode stating:
When operating at or near the best rate of climb airspeed, at climb power settings, and using vertical speed hold, it is easy to decelerate to an airspeed where continued decreases in airspeed will result in a reduced rate of climb. Continued operation in vertical speed mode can result in a stall.
The engagement of the heading button would arm the heading mode, which would command the aircraft to turn to and maintain the heading selected on either the horizontal situation indicator[4] (HSI) or the directional gyroscope.
Figure 6: KAP 140 autopilot control panel
Source: KAP 140 manual, annotated by the ATSB
The pilot identified a key safety message from CASA seminars on ‘VFR into IMC’ that they had attended was to use the autopilot if available in case of inadvertent entry to IMC.
Meteorological information
The pilot had obtained the TAF[5] for Mareeba Airport, about 22 km north of Atherton Airport and elevation of 1,564 ft above mean sea level (AMSL). The TAF was issued at 0328 on 16 June and valid between 0500 and 1800 local time. The forecast indicated the wind at 150° at 10 kt, with visibility greater than 10 km and broken[6] cloud cover at 2,000 ft above airport elevation. From 1000, the wind was forecast to increase to 12 kt, with visibility greater than 10 km and scattered[7] cloud cover at about 2,500 ft.
The Bureau of Meteorology does not provide an aviation forecast or recordings for Atherton Airport.
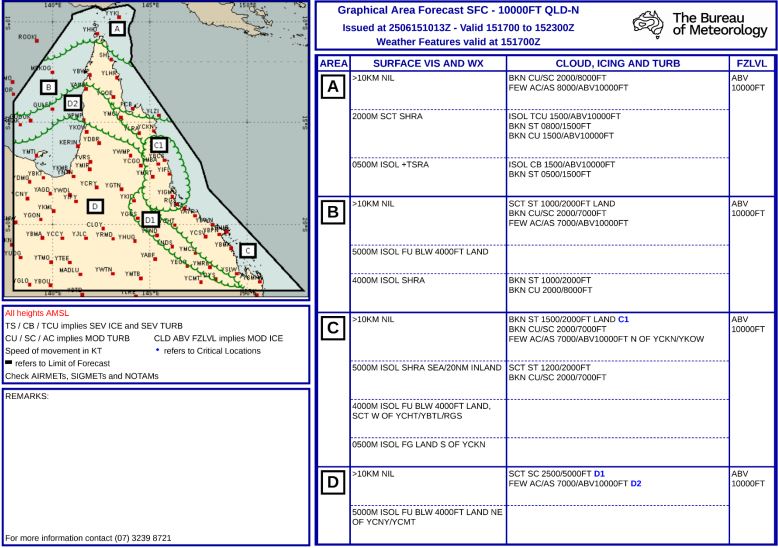
The pilot did not obtain a graphical area forecast (GAF) for the flight planned route (Appendix – Graphical Area Forecasts). The GAF for surface to 10,000 ft for the area in North Queensland was issued at 2013 on 15 June and was valid between 0300 and 0900 on 16 June. Cloud heights were forecast down to 1,500 ft AMSL with isolated fog reducing visibility to 500 m in areas along the pilot’s flight planned track.
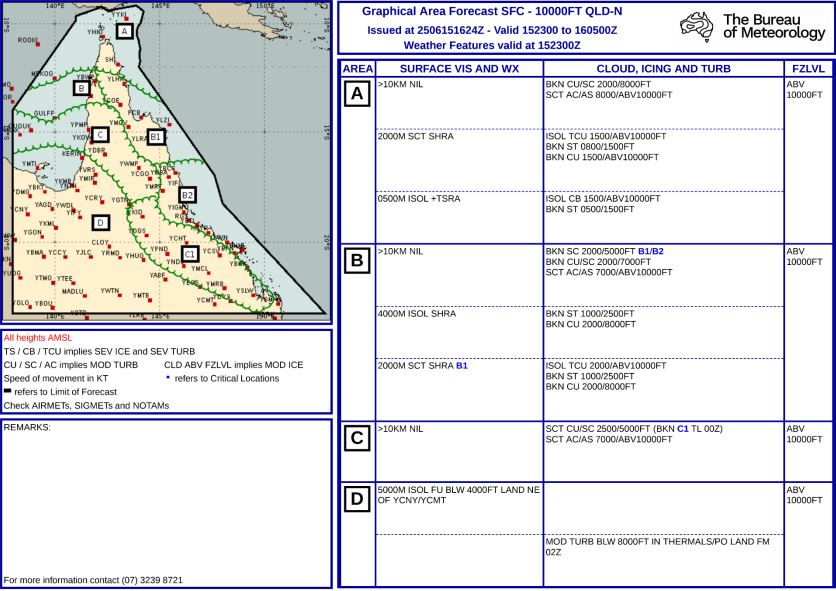
A further GAF for the same area was issued at 0224 on 16 June, it wasvalid between 0900–1500 the same day and indicated broken cloud down to 2,000 ft AMSL and to 1,000 ft AMSL with isolated rain showers reducing visibility to 4,000 m. It also indicated broken cloud cover down to 2,500 ft, becoming scattered after 1000. The GAF covered both the flight planned track and the aircraft’s diversion track (See Appendix – Graphical Area Forecasts).
Satellite image taken at 0930 provided by the Bureau of Meteorology indicated cloud cover in the flight planned area and the area the pilot intended to use as a diversion (Figure 7).
Figure 7: Satellite image 0930 local time
Source: Bureau of Meteorology, annotated by the ATSB
The pilot recalled that when they reached Kennedy Developmental Road, the cloud ceiling height had reduced. The pilot estimated they had more than 10 km visibility and a ‘good horizon’ with a crosswind from the east of about 15–18 kt.
After following the road north for about 3.5 minutes the pilot recalled that a ‘white-out’ appeared ahead and, shortly after, they entered instrument meteorological conditions (IMC).
Recorded data
The pilot used a flight planning application on an iPad for en route flight planning, navigation and to obtain weather information.
The software provider was an approved source of electronic aeronautical charts, however the application could not be used as a primary means of GPS‑based navigation as the iPad GPS did not meet certification for aviation use. Additionally, there were limitations to the recorded data as altitude information had a resolution of 100 ft, and filtering applied to smooth the data can affect the accuracy of small sections of data.
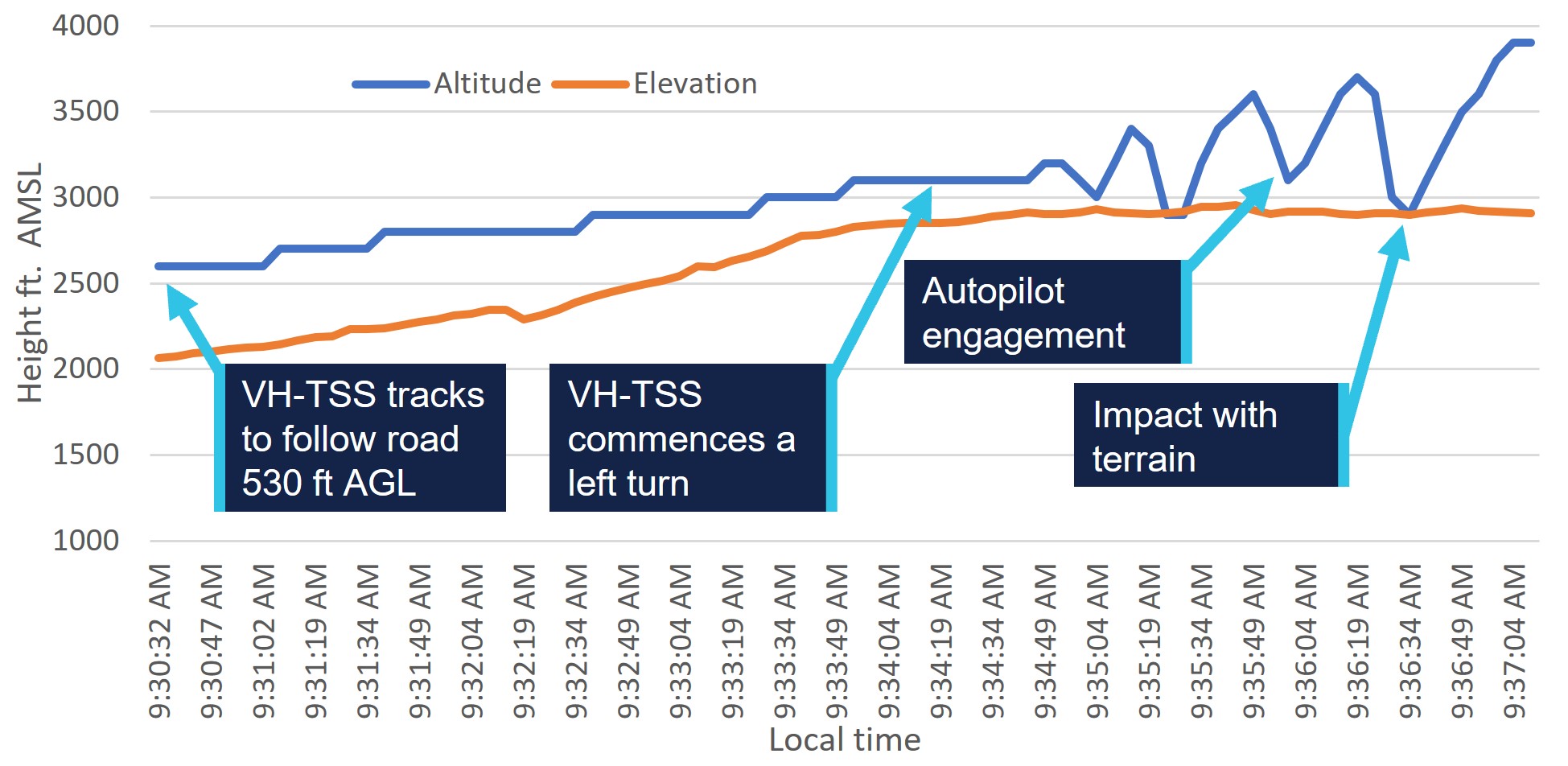
The aircraft height was about 560 ft AGL when the aircraft began to track north along Kennedy Developmental Road which the pilot followed for about 3.5 minutes. At 0934 the aircraft began to deviate away from the road after an increase in altitude of about 500 ft, however due to the rising terrain was about 250 ft AGL (Figure 8).
Figure 8: VH-TSS height above terrain
Source: ATSB, data provided by OzRunways and Google Earth
After tracking away from Kennedy Developmental Road, the aircraft turned to the west about 100° in 30 seconds. The turn radius then tightened conducting a 360° left orbit in 65 seconds, during this time the aircraft recorded altitude fluctuated between about 0 ft and 700 ft AGL.
The aircraft then maintained a westerly heading while commencing a climb from about 200 ft AGL with a reducing ground speed to 54 kt over a 20 second period.
The data then recorded the aircraft conducting a left turn through about 70° with a reduction in altitude to the terrain height, in about 5 seconds. The aircraft then commenced a further climb to 1,000 ft AGL before stabilising its altitude over the following 4 minutes in a southerly direction.
At 0941 the aircraft commenced about one and a half descending left turns through about 470° and descended from 1,300 ft AGL to about 300 ft AGL. The flight track then followed a dirt track before tracking east to again intercept Kennedy Developmental Road.
The flight track remained in close proximity to Kennedy Developmental Road, tracking south, passing within 0.7 NM of Greenvale ALA at 1017. The pilot continued to track at about 1,000 ft AGL and followed main roads until it landed at Charters Towers Airport at 1114.
Operational information
Visual meteorological conditions
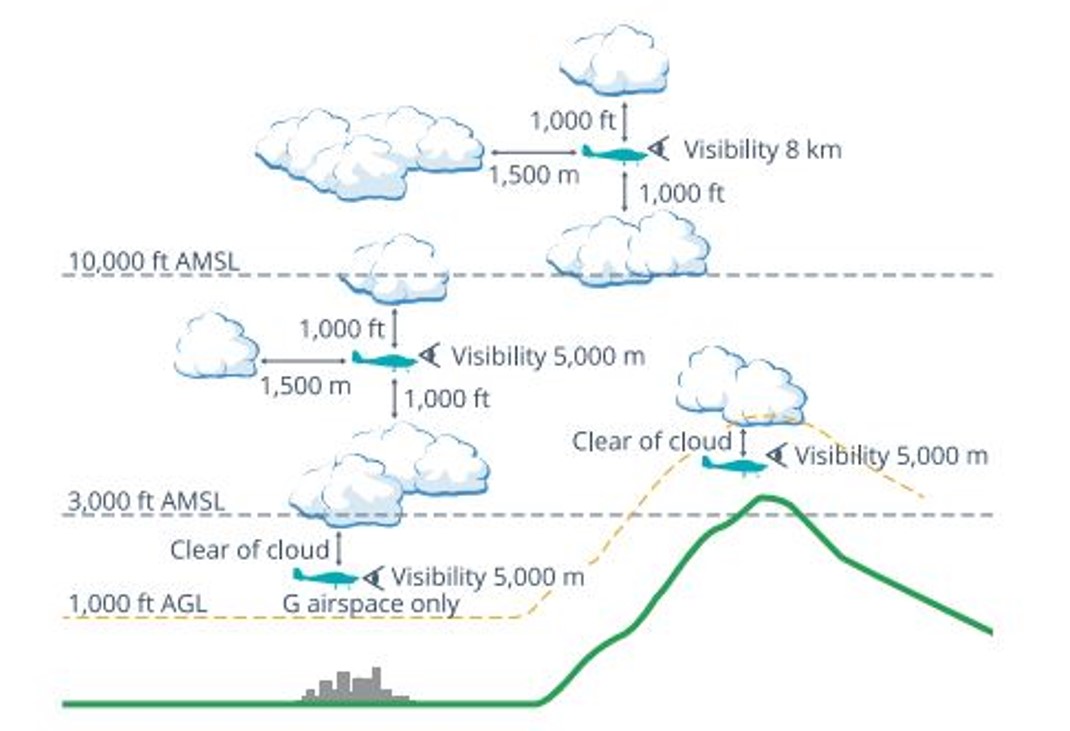
Visual meteorological conditions (VMC) are expressed in terms of in-flight visibility and distance from cloud (horizontal and vertical) and are prescribed in the Civil Aviation Safety Regulations (CASR) Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 2.07 VMC criteria. For aircraft in class G[8] airspace (Figure 9) the following requirements apply at a height below whichever is the higher of 3,000 ft AMSL or 1,000 ft AGL:
- a minimum of 5,000 m visibility
- maintain flight clear of cloud
- aircraft must be operated in sight of ground or water
Figure 9: Visual meteorological conditions criteria below 10,000 ft as illustrated in the CASA Visual Flight Rules Guide
Source: Civil Aviation Safety Authority
Minimum height rules
CASR Part 91.267 (2) stated that for flight over non-populous areas:
The pilot in command of an aircraft for a flight contravenes this subregulation if, during the flight:
- the aircraft is flown below 500 ft above the highest feature or obstacle within a horizontal radius of 300 m of the point on the ground or water immediately below the aircraft
- is not taking off or landing or conducting a missed approach
- is not carrying passengers and conducting practice forced landings with permission from the landowner.
The Civil Aviation Act,1998 section 30 also stated:
(1) In any proceedings for an offence against this Act or the regulations, it is a defence if the act or omission charged is established to have been due to extreme weather conditions or other unavoidable cause.
(2) Any defence established under subsection (1) need only be established on the balance of probabilities.
Flight planning
The pilot submitted an online flight plan at 0544 that morning to Airservices Australia via the NAIPS[9] application and received notification that the plan had been accepted.
The flight was planned to depart from a private ALA at 0630, climb to 4,500 ft AMSL and to track direct to Charters Towers, before descending and tracking direct for Atherton at 2,500 ft AMSL. Flight plan distance was about 425 NM.
Terrain heights on a direct track between Charters Towers and Atherton indicated terrain elevation consistently over 2,500 ft AMSL with areas above 4,000 ft AMSL.
The pilot reported that they had originally planned to fly on 17 June, however after reviewing the encroaching forecast weather conditions, planned the flight a day earlier.
CASR Part 91 (General Operating and Flight Rules) Manual of Standards 2020: 7.02 Forecasts for flight planning, described that a pilot in command must before commencing flight below 10,000 ft, study:
the authorised weather forecasts and authorised weather reports for the route being flown, departure aerodrome, planned destination, planned alternate aerodrome and any other reasonably available weather information that is relevant to the intended operation
the authorised weather forecast must include a wind and temperature forecast as well as either, a GAF, GAMET area forecast or a flight forecast
should the forecasts and reports be studied more than 1 hour before commencing the flight, the pilot in command must obtain, and review, an update to that information before the flight begins.
The pilot reported that they obtained the weather forecast for Mareeba the evening prior to their flight and again on the morning of their departure. They stated that they were aware of a frontal system that was due in the area later that day or evening. However, they had not obtained a GAF before their departure.
Alternative aircraft landing area
On regaining visual reference with the ground after the collision with terrain, the pilot continued the flight for about 155 NM, and about 1.5 hours flying time. During the flight, the aircraft passed within a nautical mile of another suitable ALA as it returned to Charters Towers.
The pilot stated they were aware of other aerodromes in the vicinity as they tracked towards Charters Towers and that although they were aware that the aircraft had sustained damaged during the collision, they were unaware of the extent and assessed that the aircraft was flying to an acceptable standard to continue the flight to Charters Towers Airport.
Other suitable airports or ALA in the area of the incident site included:
Greenvale ALA 38 NM south (within 1 NM of return track)
Einasleigh Airport 36 NM west
Valley of Lagoons ALA 50 NM south-east
Georgetown Airport 68 NM west.
Human factors
Spatial disorientation
The ATSB publication Avoidable Accidents No. 4: Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions(AR-2011-050) discusses the physiological limitations of the human body when trying to sense its orientation in space.
In conditions where visual cues are poor or absent, such as in poor weather, up to 80 per cent of the normal orientation information is missing. Humans are then forced to rely on the remaining 20 per cent, which is split equally between the vestibular system and the somatic system. Both of these senses are prone to powerful illusions and misinterpretation in the absence of visual references, which can quickly become overpowering.
Pilots can rapidly become spatially disoriented when they cannot see the horizon. The brain receives conflicting or ambiguous information from the sensory systems, resulting in a state of confusion that can rapidly lead to incorrect control inputs and resultant loss of aircraft control.
As described in ATSB report AR-2011-050 statistics show non-instrument rated pilots may not be able to recover at all. Research has shown the pilots not proficient in maintaining control of an aircraft with sole reference to the flight instruments will typically become spatially disoriented and lose control of the aircraft within 1 to 3 minutes after visual cues are lost.
ATSB report AR-2011-050 was updated in 2019 and identified that in the 10 years prior, there were 101 visual flight rules (VFR) into IMC occurrences in Australian airspace reported to the ATSB. Of these, 9 were accidents resulting in 21 fatalities. This details an almost 10% chance of a VFR into IMC encounter ending in a fatal accident.
The ATSB Aviation Occurrence Database indicated that in the 10 years since 2015, there have been 108 VFR into IMC occurrences reported to the ATSB. Of these, 14 resulted in accidents with 23 fatalities. The dangers of spatial disorientation following a loss of visual cues remains one of the most significant causes of concern in aviation safety.
Decision‑making
The pilot explained they had not previously flown in poor conditions and had previously turned back when conditions were not suitable on many occasions.
Flight under the VFR requires minimum conditions of visibility and distance from cloud (see Visual meteorological conditions). Variation from the expected weather conditions en route may prevent a pilot from reaching their destination under visual conditions.
Flight into IMC can occur in any phase of flight. However, a 2005 ATSB research publication – General Aviation Pilot Behaviours in the Face of AdverseWeather (B2005/0127)– concluded that the chances of a VFR into IMC encounter increased as the flight progressed, with the maximum chance occurring during the final 20 per cent of the planned flight. It stated:
This pattern suggests an increasing tendency on the part of pilots to ‘press on’ as they near their goal. To turn back or divert when the destination seemed ever closer became progressively more difficult.
Ambiguous cues and organisational and social factors may not in themselves be sufficient to cause decision errors. However, when the decision maker's cognitive limits are stressed, these factors may induce errors in certain contexts. Errors may be mediated by underestimation of the risk inherent in a situation, overconfidence in one's ability to cope with the situation, or failure to evaluate the consequences of planned actions.
VFR into IMC, loss of control and collision with terrain involving SOCATA-GroupeAerospatiale TB-20, VH-JTY
On the morning of 28 October 2023, a SOCATA-Groupe Aerospatiale TB-20, registered, VH‑JTY, departed Montpelier aircraft landing area, Queensland, for a visual flight rules private flight to Palmyra aircraft landing area, Queensland. The flight was to be just over one hour duration and the pilot and their passenger were familiar with the route.
Around 30 NM from the destination, shortly after commencing descent for the intended landing, the aircraft began a steep descending turn to the left towards mountainous terrain. During this descent, the aircraft exceeded the airframe’s designed maximum airspeed before pitching up and passing over the top of Bull Mountain. The aircraft then entered a second steep descending turn, this time to the right, before the recorded flight path data ceased. The aircraft collided with terrain, the aircraft was destroyed and both occupants received fatal injuries.
The ATSB found that, after encountering cloud en route, the pilot elected to continue along the intended flight path through cloud instead of diverting around or remaining on top of it. Shortly after, it is very likely the pilot entered weather conditions not suitable for visual navigation, leading to spatial disorientation and a descent into mountainous terrain.
VFR into IMC and in-flight break-up involving Van's Aircraft RV-7A, VH-XWI 90 km south of Charters Towers, Queensland, on 23 April 2021
On 23 April 2021, a Van’s Aircraft RV-7A, registered VH-XWI, was being operated on a private flight under the visual flight rules (VFR) from Winton to Bowen, Queensland. During the flight, the pilot most likely entered IMC and lost control of the aircraft several times. This led to the airspeed limitations for the aircraft being exceeded and the aircraft sustained an in-flight break-up. The pilot was fatally injured, and the aircraft was destroyed.
VFR into IMC resources
The 2011 ATSB publication, Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions(AR-2011-050), updated in 2019, includes a selection of weather‑related general aviation accidents and incidents that show weather alone is never the only factor affecting pilot decisions that result in inadvertent IMC encounters. The documented investigations consistently highlight that conducting thorough pre-flight planning is the best defence against flying into deteriorating weather.
CASA also released a collection of resources related to this type of occurrence on its website titled Weather and forecasting.
For more information on VFR into IMC occurrences, recognising inadvertent entry into IMC, and what to do to recover, refer to the following publications:
United Kingdom Civil Aviation Authority: Safety sense booklet VFR flight into IMC
United States Aircraft Owners and Pilots Association: Encountering IMC.
Safety analysis
Pre-flight planning
The flight was planned to track from the departure aircraft landing area (ALA) direct to Charters Towers and then Atherton, a distance of about 425 NM. The flight north of Charters Towers was flight planned at 2,500 ft above mean sea level (AMSL), however terrain elevations on the planned route north of Charters Towers were consistently higher than 2,500 ft AMSL.
The pilot had obtained a weather forecast for Mareeba Airport (close to their intended destination), which indicated a cloud height of 2,000 ft above the airport elevation (1,564 ft), conditions that the pilot considered suitable for visual flight rules (VFR) flight.
An updated available graphical area forecast (GAF), issued about 4 hours prior to departure, indicated cloud heights were forecast to be about 2,000 ft AMSL at the time the aircraft had planned to be flying over areas of high terrain.
While the pilot was aware of encroaching weather and accelerated their planned flight to a day earlier to avoid the weather, the pilot’s pre-flight planning in respect to planned altitude north of Charters Towers and the weather conditions at the time of the flight was inadequate. Without the required aviation forecast, or appreciation of weather conditions en route, the pilot departed for their destination without the knowledge of expected cloud en route that was lower than terrain elevation and would likely have prevented visual flight.
Continued flight at low level
After assessing in flight that conditions were unsuitable for continued flight direct to Atherton due to the low cloud height, the pilot planned for an alternate airport of Mareeba, visually tracking west to avoid higher terrain.
About 35 minutes after the diversion, the pilot intercepted and began to track north following Kennedy Developmental Road towards rising terrain.
The pilot described having visibility of greater than 10 km and a good horizon while tracking north following the road. As the terrain elevation increased about 900 ft during the few minutes of northerly flight along the road, the pilot was unable to maintain the minimum terrain clearance of 500 ft above ground level or the minimum 5 km visibility before entering instrument meteorological conditions (IMC).
The pilot stated that they had turned back several times on previous flights due to marginal weather conditions. The pilot and passenger were travelling on a private flight, it was unlikely that there was time pressure to arrive at the intended destination.
Consistent with other occurrences of visual flight rules (VFR) into IMC, the aircraft entered IMC conditions within the last 20% of the flight after continuing flight below the minimum required altitude. Although the pilot recalled initially having good visibility, they continued flight towards the destination below a safe altitude, this indicated a desire to ‘press on’ to the destination and increased the risk of unintended entry into IMC and collision with terrain.
Spatial disorientation
The pilot described being surprised how quickly they entered a ‘white-out’ that appeared in front of the aircraft. Likely as a result of attempting to avoid entering the cloud and losing visual reference, they instinctively reduced power and commenced a left turn. During the turn the aircraft entered cloud and the pilot described becoming ‘totally disorientated’ shortly thereafter.
Data showed that the aircraft altitude began to fluctuate with several changes of up to 500 ft vertically in about a 60-second period. While in cloud the aircraft came close to impacting terrain on more than one occasion.
The instability of the flight path with numerous rates of climb and descent are commonly observed in spatial disorientation occurrences where pilots perceive a departure from stable flight and attempt to correct the unusual flight sensations without visual reference.
Unable to reference the aircraft’s visual position or orientation to terrain after entering cloud, the pilot conducted a steep left turn and then engaged the autopilot with the intent to stabilise the aircraft.
Autopilot engagement and aircraft stall
The engagement of the autopilot levelled the aircraft’s wings and held a constant heading. However, the aircraft became established in a climb due to the aircraft attitude when the autopilot was engaged, capturing a high rate of climb.
The pilot used the heading bug on the horizontal situation indicator to reverse their track 180° to try to fly out of cloud.
The aircraft airspeed was likely less than the recorded ground speed of 54 kt due to a tailwind and therefore most likely below the aircraft’s published stall speed.
The pilot’s decision to engage the autopilot stabilised the aircraft’s heading, however without adequate power, the autopilot maintained the captured rate of climb while the airspeed reduced. As the aircraft commenced the pilot‑commanded left turn, the increased angle of bank and slow speed likely resulted in the aircraft stalling and entering a rapid descent at low level. The pilot’s immediate reaction to the red terrain display instigated them applying stall recovery techniques that very likely prevented a more serious collision with terrain.
Flight past a suitable landing area with a damaged aircraft
The pilot was aware the aircraft had sustained damage during the collision with terrain, reporting that the aircraft required additional right rudder trim to maintain balanced flight due to the damage.
Once the pilot became visual with the ground and tracked to the south, rather than conduct a precautionary landing or divert to a nearby aerodrome, they maintained a track following major roads towards Charters Towers for an additional 1.5 hours.
Following the collision with terrain the pilot likely became focused on the recovery of the damaged aircraft from the remote area. During the return flight south to Charters Towers, the pilot flew within 1 NM of the Greenvale aircraft landing area (ALA) about 41 minutes after the tree collision, and there were 3 other potential landing areas that were closer than Charters Towers. Instead, the pilot continued flight in the damaged aircraft to Charters Towers, a familiar airport with a longer runway.
With known damage and the performance characteristics of the aircraft adversely affected, the pilot’s decision to continue the flight to Charters Towers (past a suitable ALA) rather than seek the nearest suitable landing area that provided an opportunity to properly assess the damage, placed additional risk on the occupants’ safety.
Use of aircraft instruments for navigation
Following the impact with the tree, the pilot flew the damaged aircraft using basic flight instruments until they became visual again above the cloud layer.
Although the pilot had not recently practised instrument flight, their knowledge gained during their initial flight training, their familiarity with the aircraft systems and their use of the navigation instruments assisted to stabilise and manoeuvre the aircraft out of IMC conditions to regain visual reference and were then able to determine a track south away from cloud.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the VFR into IMC and collision with trees involving Cessna 182T, VH‑TSS, 57 km south-east of Mount Surprise, Queensland, on 16 June 2025.
Contributing factors
During pre-flight planning, the pilot obtained weather for the destination, however, did not obtain weather for the flight planned track.
Although the pilot could not maintain 500 ft terrain clearance due to the low cloud base, they continued flight towards the destination rather than divert to a known area of higher terrain clearance.
The visual flight rules pilot entered instrument meteorological conditions at low level and reduced power when they became disorientated. This resulted in an unintentional turn and near collision with terrain.
While disorientated in IMC, the pilot initiated a climbing turn and engaged the autopilot at reduced power, resulting in the aircraft being unable to maintain airspeed and likely entering a stall and rapidly lost height. During the recovery, the aircraft impacted with trees but continued to fly.
Other factors that increased risk
While aware of damage and controllability issues, the pilot did not land at the closest suitable aerodrome and continued for 1.5 hours to a larger airport.
Other findings
The pilot was able to use the aircraft’s instruments to stabilise the damaged aircraft and navigate out of instrument meteorological conditions
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
Civil Aviation Safety Authority
Bureau of Meteorology
Ozrunways.
References
Australian Transport Safety Bureau. (2005). General Aviation Pilot Behaviours in the Face of Adverse Weather. Aviation Research Investigation Report B2005/0127.
Australian Transport Safety Bureau. (2011). Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions.
Orasanu, J. L.-A. (1998). Errors in Aviation Decision Making: Bad Decision or Bad Luck.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
Civil Aviation Safety Authority
the manufacturer
Bureau of Meteorology.
Submissions were received from the:
pilot
Civil Aviation Safety Authority
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix – Graphical area forecasts
Graphical area forecast issued 2013, 15 June
Source: Bureau of Meteorology
Graphical area forecast issued 0224, 16 June
Source: Bureau of Meteorology
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual meteorological conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
[2]Visual flight rules (VFR): a set of flight regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[3]Calibrated airspeed: indicated airspeed corrected for position and instrument error and expressed in knots.
[4]HSI: a flight navigation instrument that combines the heading indicator with a CDI (course deviation indicator), in order to provide the pilot with better situational awareness of location with respect to the courseline.
[5]TAF- Aerodrome Forecast (TAF): a statement of meteorological conditions expected in the airspace within a radius of 8 km of the aerodrome reference point.
[6]Broken cloud indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[7]Scattered cloud indicates that cloud is covering between a quarter and a half of the sky.
[8]Class G airspace is uncontrolled airspace. Both IFR and VFR aircraft are permitted and neither require ATC clearance.
[9]NAIPS: National Aeronautical Information Processing System
Occurrence summary
Investigation number
AO-2025-028
Occurrence date
16/06/2025
Location
57 km south-east of Mount Surprise
State
Queensland
Report release date
28/10/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Diversion/return, VFR into IMC
On 16 July 2025, a Defence ARH Tiger helicopter experienced a hard landing at Timber Creek, Northern Territory.
The Australian Transport Safety Bureau (ATSB) is providing technical assistance to the ongoing Defence Flight Safety Bureau (DFSB) investigation.
To facilitate this support and to provide the appropriate protections for the information, the ATSB commenced an investigation under the Transport Safety Investigation Act 2003.
A shipboard helicopter accident likely due to ground resonance emphasises the importance of proper pilot coordination in responding to abnormal situations.
An ATSB investigation report outlines that on 25 February 2025, the Agusta A109E helicopter with two pilots on board – a pilot flying in‑command‑under‑supervision (ICUS) and a pilot supervising – was taking off from a bulk carrier about 200 km north‑east of Mackay, Queensland, after dropping off a marine pilot.
As it was lifting off from the ship’s helideck, the helicopter developed severe vibrations. The take‑off was discontinued but control of the helicopter was lost.
The helicopter came to rest upright on the helideck, more than 90° counterclockwise from its original position, having sustained substantial damage. No injuries were reported.
The ATSB found that the vibration was likely the result of the helicopter entering ground resonance, a phenomenon that dissipates when airborne, while it was in the process of departing from the ship. “When the vibrations started, the pilot supervising perceived the pilot flying to be holding the cyclic in an abnormally aft position, and believed the main rotor may have struck the tail boom,” ATSB Director Transport Safety Stuart Macleod said.
In response, the pilot supervising, unannounced, took hold of the cyclic and collective in order to discontinue the take‑off, while the pilot flying was still attempting to lift off.
“In isolation, the immediate responses taken by each pilot following the sudden onset of vibration were understandable,” Mr Macleod said.
“But discontinuing the take‑off after the onset of the vibration, with the rotor speed in the flight range, probably resulted in the loss of control and substantial damage to the helicopter.”
Mr Macleod noted the accident was a good example of the potentially catastrophic nature of ground resonance.
“Typically, the onset of ground resonance is sudden and if the pilot does not take immediate corrective action, loss of control can occur rapidly.”
After the accident, the helicopter operator added new guidelines on ground resonance to its procedures.
It has also developed an updated procedure for training and checking flight briefings that will include confirming the roles of each pilot, procedures for transferring aircraft control between pilots, and actions to be followed in the event of an actual emergency.
“Proper coordination between pilots is critical, particularly when responding to abnormal or emergency situations,” Mr Macleod said.
“Pilot roles and responsibilities for emergency response and flying duties should be well established prior to each flight.”
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 31 May 2025 at around 12:50 EST, the pilot of an amateur‑built Van’s RV-8 aircraft was carrying out a documented flight test program to qualify the aircraft for a Special Certificate of Airworthiness in the Experimental category. The flight was being operated in the vicinity of the Jervis Bay Aerodrome, Jervis Bay Territory, when the pilot reported that during a level turn, preparing for an accelerated stall test at approximately 3,500 ft AMSL, the engine lost all power and failed. After attempts at restarting the engine were unsuccessful, the pilot was able to configure the aircraft for a glide approach and safe landing on runway 15 at Jervis Bay.
The RV‑8 aircraft was fitted with a Textron Lycoming IO‑360‑M1B four‑cylinder fuel‑injected aeronautical engine. Inspections carried out on the engine and systems after the failure identified a loose and leaking fuel connection between the fuel/air control unit (fuel servo) and the fuel manifold valve (Figure 1). A loss of integrity of the fuel line at this point would result in the engine being starved of fuel and the power loss as sustained.
The pilot reported that since the engine’s assembly in 2023 there had been no maintenance or other activity around the fuel supply connection – leading to the conclusion that the leaking fitting may have been inadequately fastened at that time.
Figure 1: IO-360 fuel system - diagrammatical illustration
An ATSB research report Amateur-built aircraft Part 2: Analysis of accidents involving VH-registered non-factory-built aeroplanes 1988-2010found that across this period, amateur‑built aircraft had an accident rate that was 3 times higher than comparable factory‑built certified aircraft conducting similar flight operations. Further, over half of the accidents were precipitated by partial or complete engine failures – these being significantly more common when compared with factory‑built aircraft.
Considering these findings, this well‑managed safety occurrence provides a direct reminder, to all pilots and crew of sports and general aviation aircraft, of the importance of being prepared for an unexpected partial or complete loss of power during any phase of flight. In this instance, the pilot’s operation at an altitude and position in respect of the Jervis Bay Airport provided some assurance of the ability to conduct a safe unpowered descent and landing after the engine failure occurred.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-024
Occurrence date
31/05/2025
Location
Near Jervis Bay Airport
State
Australian Capital Territory
Occurrence class
Serious Incident
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing, Fuel starvation, Fuel systems
On the morning of 21 July 2025, a Virgin Australia Airlines Boeing 737-800, registered VH-YFY, was being operated on a scheduled air transport passenger flight from Sydney, New South Wales, to Hobart, Tasmania. About 10 minutes prior to landing in Hobart, one cabin crew member was checking the cabin was secure for landing when they identified smoke and flames coming from the top of an overhead locker. When the overhead locker was opened, a passenger’s backpack was found to be on fire. The cabin crew doused the flames with a fire extinguisher, and with the assistance of some passengers, poured water on the bag until no smoke was emitted. The aircraft landed without further incident.
After landing, aviation rescue firefighters retrieved a burnt power bank from inside the backpack.
What the ATSB found
The ATSB found that the lithium-ion battery in a power bank experienced a thermal runaway, resulting in a fire in the overhead locker inside a passenger’s bag. Due to the timing of the fire, when the aircraft was already close to landing, the cabin crew had limited time to complete the lithium battery firefighting procedure.
It was also identified that, while the cabin crew attempted to use the protective breathing equipment provided by the operator, difficulties during its fitment meant that they did not find it effective in this incident.
What has been done as a result
Following this incident, Virgin Australia Airlines reviewed its policy regarding the carriage of power banks and spare batteries. As of 1 December 2025, guidance provided to passengers stated:
Power banks, spare and loose batteries must be carried as carry-on baggage only and must be protected against damage.
Each battery and power bank must be individually protected to prevent short circuiting by placing it in the original retail packaging, in a separate plastic bag, a separate protective pouch or insulating the terminals by applying tape over the exposed terminals.
Only bring batteries and power banks that are clearly labelled and made by reputable manufacturers. Unlabelled, damaged, leaking, subject to product recall, and counterfeit batteries or power banks must not be brought on board the aircraft.
Batteries and power banks must be stowed in the seat pocket, under the seat in front, or be kept on you/in your hands. Do not store them in the overhead lockers.
Power banks must not be used to charge other devices on board the aircraft. Even when not in use, remove all cables/USB cables connected to power banks and batteries.
Power banks and batteries must not be recharged using the aircraft’s power supply.
Virgin Australia Airlines also stated that batteries that were damaged, swollen, leaking, recalled, showing signs of defects, or had been repaired or modified, could not be carried in either checked or carry-on baggage.
Safety message
Passengers often travel with multiple devices that contain lithium batteries, including laptop computers, mobile phones, headphones, and power banks. To reduce the risk associated with lithium battery fires, passengers should ensure their devices are packed safely, easily accessible in the cabin and are not carried on board an aircraft if they show signs of damage or deterioration.
The thermal runaway of a lithium battery can be difficult to manage, particularly when the aircraft is airborne. In-flight fires pose a significant risk to the safety of an aircraft if not managed quickly and appropriately. An operator’s procedure to manage battery fires is designed to limit the risk and reduce the likelihood of re-ignition of the battery until the aircraft can land. However, it requires the batteries to be out of a bag and accessible to be easily completed.
Passengers are encouraged to review their airline’s website, and check the Civil Aviation Safety Authority ‘Pack Right’ website to confirm that equipment they are planning to take on board an aircraft is permitted and packed safely.
Summary video
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 21 July 2025, a Virgin Australia Airlines Boeing 737-800 aircraft, registered VH-YFY, was being operated on a scheduled air transport passenger flight from Sydney, New South Wales, to Hobart, Tasmania. There were 2 flight crew, 4 cabin crew (comprised of a cabin manager under training (‘1L’), a cabin crew trainer (‘1R’), and 2 cabin crew (‘2L’ and ‘2R’) and 149 passengers on board. The first officer was pilot flying and the captain was the pilot monitoring.[1]
At about 0901 local time, as the aircraft descended through 10,000 ft with the seatbelt sign illuminated, the cabin crew began their final checks on the cabin prior to landing at Hobart. While near the front of the cabin, the 1R heard a sound that they described in their interview with the ATSB as a popping and hissing sound. On looking, they saw white smoke, then flames, emanating from the overhead locker above row 7DEF (Figure 1). They immediately instructed the passengers seated in both sides of rows 6,7 and 8 to move away from the area and into other seating in the aircraft. The 1R then retrieved a fire extinguisher, the portable breathing equipment (PBE), and water from the forward galley.
The 1L made a call from the front galley to the other cabin crew for assistance. The 2 rear cabin crew brought more water and another fire extinguisher forward. The 1R and 2R attempted to don the PBE around the same time, however, one was unable to stretch the neck ring sufficiently to don the PBE, and the other, after donning the PBE felt it restricted their ability to see and communicate effectively so decided to remove it.
Figure 1: Aircraft seat plan showing the location of the overhead locker where flames and smoke were observed
Source: Virgin Australia Airlines, modified by the ATSB
When the overhead locker was opened, flames and smoke were observed emanating from a backpack. Although they could not see what was causing the fire, from their training, the cabin crew suspected it was from a portable electronic device overheating. The 1L discharged a fire extinguisher into the locker until the flames were extinguished. The 1L and 1R then poured water over the bag, with the assistance of the 2R and passengers. To reduce the risk of re‑ignition, a second fire extinguisher was discharged into the locker. The cabin crew instructed passengers to keep their heads down and cover their nose and mouth to avoid inhaling smoke. They also asked the passengers who was the owner of the bag but did not receive a response at the time.
While the other cabin crew managed the fire, the 2L called the flight deck. The captain recalled in interview that, prior to the call, they detected a smoky odour in the flight deck, which they thought was ozone. The 2L advised the captain there was a fire in an overhead locker, which was extinguished, but there was still smoke, and the 1L was dousing the bag with water. They also stated that there were still passengers standing. On ending the call, the captain asked the 2L to ensure everyone was seated for landing.
Following receipt of this information, at 0905:17, just prior to descending through 5,100 ft, the captain made a ‘PAN PAN’[2] call to the Hobart approach air traffic control to advise of a possible fire in the cabin, and that they would require assistance on landing. The captain also asked to speak to the tower controller earlier to request clearances. The approach controller coordinated to get the tower controller on frequency.
The captain decided to take control of the aircraft for landing due to the emergency. At 0906:00, the aircraft was cleared to land on runway 30 by the tower controller. At this time, the first officer also asked to cancel the approach they had been previously cleared for and to instead conduct a visual approach. This change was permitted. At 0906:28, air traffic control contacted the aviation rescue and firefighting service at Hobart Airport, which deployed in preparation for the aircraft landing.
The 2L then retrieved gloves and the portable electronic device fire containment bag and took it to the other cabin crew, intending for the burnt device to be placed in the bag, and the bag stored in the rear lavatory, as per procedure. The backpack was too large to fit in the fire containment bag and there was difficulty in locating the device inside the backpack. Given the short amount of time remaining before landing, the decision was made by the 1R to keep the device inside the backpack in the overhead locker above row 7. It was identified by the cabin crew that the rounded shape of the overhead locker retained the water that had been poured on the backpack, which kept the bag soaked, and would help reduce the risk of re‑ignition during landing. The cabin crew planned to keep the overhead locker open, with the 1R seated in seat 7C adjacent to the locker to monitor the device during landing, with water to use if necessary. The cabin crew also directed the passengers standing to be seated immediately, even if it required 4 passengers to be in a row.
As recalled by the captain in interview with the ATSB, the first officer contacted the 1L just prior to the aircraft turning onto the final approach. This was likely just prior to 0909, with the aircraft between 1,500 ft and 1,000 ft. The 1L confirmed the fire was out, and the passengers were seated, but that the cabin crew were still standing. They assured the first officer the cabin crew would be seated for landing.
The 1L, 2L and 2R secured the final items for landing and seated themselves in their designated seats, except for 1L who sat in 1R’s seat to maintain better visibility of the cabin. On their way to their seat at the front, the 1L checked the overhead lockers around row 7 for heat or any developing hot spots. Once all the cabin crew were seated, the 1L signalled to the flight crew the cabin was secure. The 1L made a final announcement to passengers to ensure their seatbelts were fastened, to remain seated for landing and follow instructions of crew following the landing.
Flight data provided by Virgin Australia showed that the aircraft touched down at Hobart at 0910:29 (Figure 2).
Figure 2: Flight path with key events
Source: Google Earth, annotated by the ATSB
The captain stopped the aircraft on the taxiway and exited the flight deck to speak to 1L and observed the cabin to determine whether an evacuation was required. As the fire appeared to be contained, the captain taxied the aircraft to the parking bay. At 0919, the aviation rescue and firefighting personnel boarded the aircraft and removed the backpack from the overhead locker. They confirmed the origin of the fire was a lithium power bank, stored in one of the backpack’s front pockets (Figure 3).
Figure 3: Backpack containing the power bank
Source: Airservices Australia
The passengers were cleared to disembark normally at 0927. After disembarkation, one cabin crew member (2L) was treated by paramedics. It was unknown if this was due to the effects of smoke as they had been unwell throughout the flight prior to the fire commencing. No other crew or passengers reported to the operator about seeking medical attention from the effects of the smoke. The fire caused minor damage to the overhead locker above row 7/8 DEF (see section Aircraft damage).
Context
Cabin crew information
The flight comprised of 4 cabin crew, 2 located at the front set of aircraft doors (called ‘1L’ and ‘1R’) and 2 at the rear of the aircraft (called ‘2L’ and ‘2R’). Each cabin crew member had designated roles on the flight, based on which door they were operating. On this flight, the 1L position was filled by a trainee cabin manager who had previous experience in this role working for other airlines, but was completing their first flight as a cabin manager under training for this operator. The 1L was supervised by a cabin crew trainer in the 1R position.
Each of the cabin crew had between 1 and 17 years of experience as cabin crew. They had all completed their annual emergency procedures training between November 2024 and June 2025. This training included both theoretical information and a practical review of the lithium battery firefighting procedure. All cabin crew reported having completed simulated scenarios where the fire occurred either during cruise or on the ground, where there was plenty of time to complete the firefighting procedure, and store the damaged battery appropriately. None of the cabin crew had completed a simulated scenario involving a time‑pressured situation.
Aircraft cabin information
VH-YFY was a Boeing 737-800 aircraft, with a single aisle in the cabin and seating for 182 passengers. In economy, where this fire occurred, there were 3 seats on either side of the aisle.
The cabin on this aircraft was fitted with the Boeing 737 sky interior design. In this design, the overhead lockers lowered from the ceiling, creating a contained basket for the bags to sit in. In comparison, the doors in other locker designs would open upwards.
Lithium batteries
Overview
There are 2 primary types of lithium batteries – lithium metal and lithium-ion. Lithium metal batteries cannot be recharged and are designed to be disposed of once their initial charge has been used, whereas lithium-ion batteries are rechargeable. Compared to lithium metal, lithium-ion batteries store a high amount of energy and are commonly found in many portable electronic devices (PEDs) such as smartphones, tablets, cameras, laptops, and power banks.
Guidance on the safe carriage of lithium-ion batteries on board aircraft
Lithium batteries are classified by the United Nations as dangerous goods. As such, the International Civil Aviation Organization’s Technical Instructions for the Safe Transport of Dangerous Goods by Air (2025-2026 Edition) stated that lithium batteries, including power banks must be carried as carry-on baggage only.
The Civil Aviation Safety Authority stated that spare batteries and power banks should be packed in carry-on baggage only, so that trained aircrew can manage any issues quickly and safely. Their Pack right website provided safety tips when travelling with lithium batteries:
These simple steps help keep you and your fellow passengers safe:
• choose reputable suppliers when buying devices and spare batteries
• follow airline and manufacturer rules for carrying and charging lithium batteries
• keep spare batteries with you in the cabin and protect them from damage
• stop using or charging batteries that show signs of damage, overheating, or swelling
To prevent short circuits, protect spare battery terminals by:
• keeping them in original packaging
• covering terminals with tape
• placing each battery in a separate plastic bag or case.
At the time of the incident, the operator’s policy permitted power banks to be carried in the cabin only, but they could be stored inside a bag and there were no restrictions on their use on board. Advice on the carriage of power banks and other electronic devices was provided to passengers on the operator’s website and during check-in.
Thermal runaway
Thermal runaway is a rapid and uncontrolled increase in temperature and occurs when the internal cell(s) of a lithium battery become damaged for reasons including:
internal short circuits
breakage from dropping or crushing
exposure to excessive heat
failure of the battery cell due to manufacturing defects.
The operator’s Aircrew Emergency Manual stated that crew should be alert not just for signs of smoke or fire in the cabin but also to the smell of overheating electronic devices.
The smell of overheating may be the first sign of an impending lithium battery/PED fire. PEDs approaching a thermal runaway start initially displaying hissing, crackling sounds, as well as bubbling or blistering casings.
Once a lithium battery cell thermal runaway starts, it quickly leads to the failure of adjacent cells in a chain reaction that can produce fire, which is especially difficult to extinguish. A fire caused by lithium batteries can produce a fire burning with a temperature as high as 1,000°C, explosions releasing toxic gases and flammable electrolytes as well as shrapnel from damaged PED casings. The manual also stated that in some cases, the explosive force of the venting gasses could be significant enough to cause spikes in cabin pressure.
Managing lithium battery fires
The operator’s Aircrew Emergency Manual stated a general risk about onboard fires was that:
Any fire, no matter how small, may rapidly become out of control if not combatted quickly. Research has shown that if left uncontained, a smoke-filled cabin can be consumed by fire in as little as 6-10 minutes. The first priority shall always be to put the fire out.
In order to manage the risk, the manual outlined 3 important principles of firefighting:
Immediately locate the source of fire, smoke or fumes. Specific to lithium battery fires, all smoke or fire events occurring in baggage within an overhead locker should be assumed to be a PED/lithium battery fire until the source is positively confirmed.
Aggressively attack and extinguish the fire using all available resources, which can include able bodied persons.
Communicate to other crew and the flight crew, as soon as possible, specifying the location and source of fire.
Furthermore, the manual also guided crew that:
It is important to protect yourself from the effects of smoke and fumes while attempting to flight a fire. In some circumstances it may be safe and thus more important to attack a fire first than fitting of PBE [portable breathing equipment]. PBE should be worn by at least one person when a team is formed to flight a fire and anytime by the primary firefighter when they are in smoke, a confined space of affected by fumes.
In regard to managing a lithium battery fire, the manual stated:
The primary method for stopping a lithium battery from thermal runaway or overheating is to cool it down by pouring water or other non-flammable liquid on the battery or device. This should be done once any flames have been extinguished and continued until the device is cooled and there is no evidence of smoke, heat, crackling or hissing sounds usually associated with an overheating lithium battery. This could take as long as 10–15 minutes.
Another recommendation in the emergency procedures manual was a suggestion not to open any baggage if there was smoke or flames emanating from it, unless it was required to get a fire extinguisher and liquid onto an identified battery. Once the device was cooled, it could then be placed in a fire containment bag or other suitable container.
Aircraft firefighting equipment
Overview
The operator fitted the Boeing 737 aircraft with firefighting equipment. In addition to this designated equipment, the cabin crew were taught to use other equipment available on board as required, such as drinks used in the cabin service as well as wet blankets and pillows to smother a fire.
Fire extinguishers
The aircraft had 4 bromochlorodifluoromethane (BCF)/halon fire extinguishers. These fire extinguishers are designed to be used on all types of fires by discharging a colourless, odourless, non-corrosive, liquified gas. This gas is not cooling, meaning that further steps are required in fighting a lithium battery fire.
Fire protection gloves
Fire protection gloves were designed to protect the wearer’s hands when fighting fires, including lithium battery incidents. The emergency procedures also suggested that crew should use gloves whenever fighting fires, including using oven gloves if the fire protection gloves were not available.
The L2 retrieved the fire protection gloves from the galley with the intention to move the power bank once the fire was suppressed, but the gloves were not used during the firefighting process.
Portable breathing equipment
Portable breathing equipment (PBE), commonly referred to as a smoke hood, was provided for each cabin crew member on board. The PBE supplied was designed to protect the wearer from fumes and smoke by forming a secure seal using an elastic neoprene neck ring (Figure 4). An oxygen generator on the nape provided oxygen to the wearer.
Figure 4: Exemplar PBE, showing how to open the neck ring (left) and when donned (right)
Source: Virgin Australia Airlines, modified by the ATSB
Operator procedures recommend PBE should be used by at least one person involved in firefighting, or when one person was fighting a fire in an enclosed environment. Although, consideration was given that the first person to a fire might need to immediately attend to the fire while others gathered and donned the PBE.
The 2 cabin crew who attempted to use the PBE stated that the equipment provided in training was much easier to don as the neck ring was stretched from repeated usage.
In October 2025, the Airbus Safety First magazine contained an article about PBE, reviewing a case study where 7 cabin crew had difficulties using the PBE provided. The analysis indicated that, similar to this incident, despite having regular training in the use of PBE, the cabin crew found it difficult to use the PBE in a real emergency. The article recommended that ‘dummy’ PBE used in training may not represent the equipment found on board.
Fire containment bags
There were 2 sizes of fire containment bags carried on the operator’s Boeing 737 aircraft. The smaller sized bag, designed to fit an iPad, was carried in the flight deck in the event of a thermal runaway involving one of the flight crew’s electronic flight bags.
A larger bag, designed to fit a device the size of a laptop, was carried in the aircraft cabin (Figure 5). The purpose of this bag was to place the device in after it was cooled post‑fire, so that it could be stored in a water filled container in a secure place.
Figure 5: Fire containment bag
Source: Virgin Australia Airlines
Damage to the power bank
The power bank was inspected by the aviation rescue firefighters after being removed from the aircraft.
The power bank had a rated output of 37 watt hours and had both USB‑A and USB‑C charging ports. It was not charging a device when the fire started, but there was a cable plugged into the USB‑A charging port. When orientated with the manufacturer’s label facing up, most of the damage was observed along the top and right side of the power bank. The damaged right end contained the USB-C charging port. External observations suggest that the power bank contained 2 internal cells, of which only 1 was affected by the thermal runaway by the time the fire was extinguished (Figure 6). The power bank was not protected from short circuits as it did not appear to have the terminals covered and was not separated from other items in the bag by being placed in a protective pouch or the original packaging. The backpack was reported by the operator to be substantially damaged by the fire.
The owner of the power bank advised the operator that it was purchased in 2024 and:
it had no pre-existing damage
was fully charged the day prior to the incident, and there were no previous issues during charging or use
it was not dropped, exposed to moisture or heat prior to the incident.
Figure 6: Power bank showing damage from the back (left) and side view (right)
Source: Airservices Australia (left) and Virgin Australia Airlines (right)
Aircraft damage
An inspection of the aircraft found fire damage in the panels above and behind the overhead locker above row 7 and 8 DEF. The passenger service unit containing the reading lights, call bell and information signals under this locker also sustained fire and water damage. The overhead locker needed to be replaced post-fire (Figure 7).
Figure 7: Overhead locker above row 7DEF where the smoke and flames were observed (left) and area behind the overhead locker showing fire damage (right)
Source: Airservices Australia (left) and Virgin Australia Airlines (right)
Related occurrences
Australian data
This incident was the first reported power bank-related in-flight fire either in Australia or on an Australian‑registered aircraft. A review of the ATSB’s occurrence database identified 3 previous incidents where smoke was reported emanating from a power bank in the aircraft’s cabin, but no fire occurred:
OA2025-01608: On 20 January 2025, a Boeing 737 aircraft was being operated on a flight from Brisbane, Queensland, to Melbourne, Victoria. During cruise, a power bank overheated in the cabin, and smoke was observed emanating from the attached charging cable. The power bank and cable were placed in a container and stowed in the rear lavatory for the remainder of the flight.
OA2019-04325: On 28 May 2019, an Airbus A330 aircraft was being operated on a flight from Melbourne, Victoria, to Hong Kong. During cruise, smoke was detected emanating from a passenger's power bank.
OA2019-02629: On 15 April 2019, an Airbus A330 aircraft was being operated on a flight from Hong Kong to Melbourne, Victoria. During passenger disembarkation, smoke was observed emanating from a passenger's power bank. The crew doused the power bank in water.
ATSB records showed that, in the past 10 years, there were 4 in-flight fires resulting from mobile phones, 3 of which occurred after the mobile phone was crushed in the seat mechanism, damaging the lithium battery contained inside. The reason for the fourth fire was unknown.
International incidents
While this was the first reported incident in Australia, there have been a number of significant fires resulting from power banks, including:
In January 2025, an Air Busan A321 aircraft was preparing for flight at Busan, South Korea. Prior to taxi, a power bank fire started in an overhead locker. The fire spread, resulting in an evacuation. The aircraft was destroyed.
In March 2025, a Hong Kong Airlines A320 aircraft diverted after a power bank experienced a thermal runaway. The fire was extinguished.
In October 2025, an Air China A321 aircraft had to divert after a battery caught fire in an overhead locker.
The United States Federal Aviation Administration recorded 8 in‑flight fire incidents involving power banks occurring in the past 10 years.
Safety analysis
Power bank thermal runaway
For unknown reasons, one of the cells in a lithium-ion power bank stored in an overhead locker failed during the descent into Hobart. In this case, there was no reported pre‑existing damage, or any other identified problems with this power bank prior to flight. However, the power bank was stored with a cable in it and the ports uncovered, both factors which can increase the risk of a fault.
Inspection of the power bank post-flight, combined with the cabin crew reports of sounds they were trained to expect in the event of a lithium battery fire, suggested that the fire was characteristic of a thermal runaway. As the temperature of the power bank continued to increase, smoke, followed by flames resulted.
Completion of firefighting procedures
As described in the operator’s procedures, fires on board aircraft can spread quickly. As the aircraft was already on descent when the smoke was initially observed, there was limited time for the cabin crew to manage the power bank fire by completing all the procedures they were trained to do in response to an in-flight fire. In addition, they had the responsibility to ensure the cabin was secure for landing.
In less than 8 minutes, the cabin crew worked together to identify a fire, gather the required equipment, and aggressively fight the fire to a point where the fire appeared suppressed. In addition, they communicated the problem with the flight crew and managed moving passengers to alternative seating.
While the cabin crew had received emergency procedures training, they had never trained for a lithium battery fire in a compressed time. They completed as many of the procedures as they were able to in the available time, but by the time the fire was considered controlled, there was only around 90 seconds for the cabin crew to clear up the cabin and be seated for landing. Besides the logistics and risk that would result from handling the power bank to remove it from the backpack and place it in a fire containment bag, there was no time available.
The cabin crew identified an alternate solution to moving the burnt power bank. While the overhead locker held the water poured on the backpack, there was no assurance that the power bank was going to remain fully submerged for landing, in accordance with the operator’s procedures, or isolated from other lithium battery devices. Although there was no consequence as a result of the power bank remaining in the overhead locker, there was an increased risk of cabin occupant injury and aircraft damage if the power bank re‑ignited due to further exposure to fire and smoke.
Protective breathing equipment
Protective breathing equipment (PBE) was available for cabin crew to use if deemed necessary in preparation to fight a fire, and all crew were trained in their use. Two of the cabin crew attempted to use the PBE, but did not find it effective due to fitment and communication/visibility issues. As the cabin crew were unable to use the PBE, they had no protection from the smoke and were placed at an increased risk of smoke inhalation. While these cabin crew did not experience any residual effects from the smoke, any protective equipment provided should be efficient to don and wear continuously while managing an emergency situation.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the in-flight fire involving Boeing 737, VH-YFY, 56 km north‑north‑east of Hobart Airport, Tasmania, on 21 July 2025.
Contributing factors
During the descent, a passenger's lithium-ion power bank, located in the overhead locker, overheated due to thermal runaway and began to emit flames and smoke.
Other factors that increased risk
Due to the timing of the fire starting on descent, the cabin crew had limited time to complete the procedure for managing a lithium battery fire.
The cabin crew attempted to use the protective breathing equipment provided by the operator but did not find it effective when managing the lithium battery fire.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Virgin Australia Airlines
Virgin Australia Airlines advised it has reviewed its policy regarding the carriage of power banks in the cabin. As of 1 December 2025, guidance provided to passengers stated:
Power banks, spare and loose batteries must be carried as carry-on baggage only and must be protected against damage.
Each battery and power bank must be individually protected to prevent short circuiting by placing it in the original retail packaging, in a separate plastic bag, a separate protective pouch or insulating the terminals by applying tape over the exposed terminals.
Only bring batteries and power banks that are clearly labelled and made by reputable manufacturers. Unlabelled, damaged, leaking, subject to product recall, and counterfeit batteries or power banks must not be brought on board the aircraft.
Batteries and power banks must be stowed in the seat pocket, under the seat in front, or be kept on you/in your hands. Do not store them in the overhead lockers.
Power banks must not be used to charge other devices on board the aircraft. Even when not in use, remove all cables/USB cables connected to power banks and batteries.
Power banks and batteries must not be recharged using the aircraft’s power supply.
Virgin Australia Airlines also stated that batteries that are damaged, swollen, leaking, recalled, showing signs of defects, or have been repaired or modified, cannot be carried in either checked or carry-on baggage.
It has updated the cabin crew’s pre-flight announcement and website to inform passengers of the revised policy.
Virgin Australian Airlines has also acknowledged that, while it made changes to its policy, there are challenges in monitoring passengers’ compliance with these measures. It also stated that greater awareness about the risks of travelling with lithium batteries should be delivered by all airlines and airports.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the cabin crew
the flight crew
Virgin Australia Airlines
Airservices Australia
Civil Aviation Safety Authority.
Submissions were received from:
Virgin Australia Airlines
2 cabin crew members
Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
Occurrence summary
Investigation number
AO-2025-043
Occurrence date
21/07/2025
Location
56 km north-north-east of Hobart Airport
State
Tasmania
Report release date
18/12/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Fire, Smoke
Occurrence class
Serious Incident
Highest injury level
Unknown
Aircraft details
Manufacturer
The Boeing Company
Model
737-800
Registration
VH-YFY
Serial number
41016
Aircraft operator
Virgin Australia Airlines
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On the morning of 14 July 2025, a Bell 206L-3 helicopter, registered VH-JMM, was being operated on multiple passenger charter flights around the Arnhem region in the Northern Territory. On board was a pilot and one passenger.
During the fourth leg of the day at approximately 1338, while looking down and to the left out of the helicopter, the pilot heard a loud bang. The pilot saw a large bird laying between the 2 occupants, and what appeared to be serious injuries to the passenger’s upper body. The pilot reached over to the passenger to check for a pulse but was unable to feel one. Noting the passenger required immediate attention, they decided it would be better for the passenger to receive medical attention at Lake Evella Aerodrome where a police station was next to the airport.
Police, a local nurse and doctor attended to the passenger, however the passenger had succumbed to injuries. The helicopter sustained minor damage.
What the ATSB found
While cruising at about 900 ft AMSL, the helicopter struck a white bellied sea eagle which passed through the windshield and impacted the passenger.
The pilot had limited opportunity to detect the bird as they were looking down and to the left of the helicopter’s trajectory, reducing the pilot’s ability to see the bird and change the helicopter’s flight path in time, and likely rendering the collision unavoidable under the circumstances.
The passenger was not wearing a helmet at the time, nor was there an aviation regulatory requirement for them to do so. In this case, the location of the bird strike on the passenger was such that wearing a helmet probably would not have reduced the level of injury.
Safety message
Birdstrike is an almost unavoidable and relatively common hazard for all aviation operations. While these strikes typically result in minor or no damage to an aircraft and no injuries to occupants, this is the third fatal birdstrike accident in Australia in recent years.
Pilots are reminded that maintaining effective lookout will assist in maintaining better situational awareness in flight, and also assist in providing better outcomes to see‑and‑avoid not only birds, but other airspace users.
Additionally, pilots should maintain situational awareness, especially when flying over waterways or wetlands. It is relatively common for large birds, such as eagles, hawks, and gulls, to attack helicopters and drones, often perceiving them as threats or territorial intruders. These birds may display aggressive behaviour during nesting or breeding seasons, diving at or striking the aircraft in an attempt to drive it away. Helicopter operators should consider whether available occupant protections, such as the wearing of flight helmets and the fitment of impact-resistant aircraft windshields, are appropriate for their operations.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 14 July 2025, a Bell 206L-3 helicopter, registered VH‑JMM, was being operated by Nautilus Aviation on multiple air transport (passenger charter) flights around the Arnhem region in the Northern Territory. On board was a pilot and a passenger.
At approximately 0928 local time the helicopter departed Gove Airport for Donydji. The pilot reported that from Donydjii, they flew to ‘Nyquist tower’[1] and then on to Mirrnatja before departing for Burrum, which would be the last stop of the day before returning to Gove (Figure 1).
Figure 1: Flight path overview
Source: Google Earth, annotated by the ATSB
The flight departed for Burrum at 1313 (Figure 2) and the pilot established a cruise altitude of about 900 ft above ground level. The pilot recalled having a conversation with the passenger about a waterway which they were flying near, and was familiar to the passenger. The pilot recalled slightly deviating off track to view the waterway. At approximately 1338, while looking down to the left out of the aircraft, the pilot recalled hearing a loud bang.
The pilot saw a large bird laying between the 2 occupants, and what appeared to be serious injuries to the passenger’s upper body. The pilot reached over to the passenger to check for a pulse, but was unable to feel one. Noting the passenger required immediate attention, the pilot deliberated whether to land nearby and attempt resuscitation, and initially began to descend. However, considering the logistical issues with getting medical attention in a remote location, they decided it would be better for the passenger to receive medical attention at Lake Evella Aerodrome where a police station was next to the airport.
Figure 2: Accident flight overview
Source: Google Earth, annotated by the ATSB
The pilot landed the helicopter at Lake Evella Aerodrome at approximately 1346. They stated they attempted to call emergency services on 000, however the call did not connect. They decided not to attempt the call a second time and ran to the police station for assistance instead.
Police, a local nurse and doctor attended to the passenger, however the passenger had succumbed to injuries. The aircraft sustained minor damage (see Helicopter damage).
Context
Pilot information
The pilot held a valid Class 1 Aviation Medical Certificate and a Commercial Pilot Licence (Helicopter). The pilot had accumulated 2,553 hours of aeronautical experience, of which 1,319 hours was on the Bell 206L.
The pilot had been with the operator since September 2024 and had regularly flown these routes to remote communities as part of their employment.
Passenger information
The passenger was a frequent passenger on the routes operated on the day and had travelled by helicopter regularly to remote communities as part of their employment since 1995.
The pilot reported to having flown this passenger to remote communities on multiple occasions. Familiar with the aviation environment, the pilot reported the passenger would assist with monitoring for birds during flights, as they were aware they presented a hazard in flight.
The post-mortem examination report indicated the passenger was hit between the lower jaw and the upper chest, sustaining fatal injuries to the neck, chin, lower jaw and the right side of the chest.
Helicopter information
General
VH-JMM was a Bell Helicopter Company B206L‑3 Long Ranger, S/N 51400, manufactured in Canada in 1990. It was first registered in Australia in June 2017. The aircraft was registered to the operator in January 2024.
VH-JMM was a helicopter with two‑bladed main rotor and tail rotor systems, powered by a single Rolls-Royce 250‑C30P gas turbine engine.
At the time of the accident, the helicopter had completed 13,250 hours in service and had a current maintenance release.
Helicopter damage
The helicopter sustained damage to the passenger side windshield. There was no other reported damage to the aircraft (Figure 3).
Figure 3: Helicopter damage
Source: Northern Territory Police Force, annotated by the ATSB
Helicopter windshields
VH-JMM was fitted with standard acrylic windshields, which were not rated for impact resistance.
In 2016 Bell Helicopter Company introduced polycarbonate windshields, through a supplemental type certificate (STC) for the Bell 206 series, including the 206L. These were available as an additional option for current owners, offering higher impact resistance compared to traditional acrylic, reducing the risk of breaches from birdstrikes or other impacts. These were rated to United States regulatory requirements of a 2.2 lb (1 kg) bird traveling at VNE (the helicopter’s never-exceed speed).[2]
Despite having a higher impact resistance than acrylic, polycarbonate windshields are more sensitive to scratches, and reportedly susceptible to clouding or hazing due to ultraviolet light exposure, resulting in loss of optical clarity and necessitating more frequent replacements.
Weather information
The terminal aerodrome forecast for the accident region forecasted clear conditions for the flight with scattered cloud above 3,500 ft and visibility greater than 10 km.
At 1530, the weather station at Elcho Island Airport, 48 km north of the accident location, recorded the wind as 4 kt from 110° magnetic. There was scattered cloud at 1,000 ft, visibility was greater than 10 km and the temperature was 23°C.
The pilot reported that the weather varied depending on where they were flying, however it was mostly clear with some areas of cloud. They reported the clouds were above their cruise height.
Recorded data
The aircraft was fitted with a Spidertracks flight tracking unit and the pilot used OzRunways electronic flight bag software; both recorded flight data. Flight data indicated that the aircraft was cruising at 900 ft above ground level at a groundspeed of 94 kt at the approximate time the bird was struck. The data showed an initial deceleration to 86 kt groundspeed and a decrease in altitude of 50 ft, followed by a secondary decrease in altitude of approximately 150 ft (likely associated with the pilot’s consideration of whether to land). The track showed that the helicopter then climbed to 800 ft and increased groundspeed to about 70 kt (Figure 4).
Figure 4: Recorded flight track
Source: Google Earth, annotated by the ATSB
Bird information
Recovered biological specimens of the bird, including wing feathers and residue from the carcass, were found both inside the helicopter and on the passenger. Through images of the bird, the ATSB determined the species to be a white‑bellied sea eagle.
The white-bellied sea eagle (Haliaeetus leucogaster) (Figure 5) is a large raptor commonly found in coastal regions of Australia, recognised for its distinctive white head, belly, and tail contrasted by dark greyish‑brown wings and back. Adults measure approximately 66–85 cm in length, with a wingspan of 1.8–2.2 m (Debus, 2017). Adult males typically weigh between 1.8–3 kg, while females average 2.5–4.5 kg (Marchant & Higgins, 1993). The weight and sex of the bird in this accident was unknown.
Figure 5: Some of the bird remains retrieved from the helicopter
Source: Northern Territory Police Force
These eagles are often observed soaring over coastlines, estuaries, or inland waterways, preying on fish, seabirds, or carrion, and can reach heights of up to 1,000 m (about 3,300 ft) (Ferguson‑Lees & Christie, 2001). Their activity increases during the June to January period in Australia, which is their breeding season (Debus, 2017).
It is relatively common for large birds, such as eagles, hawks, and gulls, to attack helicopters and drones, often perceiving them as threats or territorial intruders. These birds may display aggressive behaviour during nesting or breeding seasons, diving at or striking the aircraft in an attempt to drive it away (Washburn & others, 2015).
Limitations of see-and-avoid
The human visual system is inherently limited in detecting small objects such as birds at distances. Hobbs (1991) notes that effective visual scanning requires systematic eye movements across the visual field, yet pilots often employ unsystematic techniques, resulting in unsearched areas. Furthermore, the cognitive process of identifying a threat, assessing its collision risk, deciding on evasive action, and executing control inputs requires time that is often unavailable in low‑altitude, high‑speed scenarios.
Birds present unique challenges to the see‑and‑avoid principle due to their relatively small size, unpredictable flight paths, and speed difference compared with aircraft.Unlike aircraft, birds cannot be tracked electronically, meaning pilots must rely solely on visual identification.
Survivability
Restraints
The helicopter was fitted with 4‑point harnesses in the front seats. The pilot reported both they and the passenger had been fastened into the seats by the aircraft’s 4‑point harnesses.
Helmets
The pilot reported wearing a flight helmet[3] and reported wearing a helmet whenever possible, noting that helmets had saved lives in the past. The pilot recalled previously having a discussion with the passenger about helmets and the benefits of them.
The passenger was not wearing a helmet at the time, nor was there an aviation regulatory requirement for them to do so. Nautilus Aviation stated that there was no requirement for passengers to wear a helmet and the decision on their use rested with the passengers themselves or their employers.
Telstra helicopter charters
The passenger was on board the aircraft as part of their work for Telstra, a telecommunications company. Telstra reported that its employees took about 630 helicopter charters on average per year, a mix of passenger charter (transit) and aerial work.
The employer had an operational framework for chartering aircraft that addressed many risks typically associated with helicopter flights, outlining expectations for the aircraft operator. These included the requirement for the aircraft operator to perform a risk assessment ‘prior to the first flight of any new operation by the Charter operator.’
Telstra did not have prescribed or recommended personal protective equipment for employees travelling or working on helicopters. Telstra advised that it relied on the licenced and accredited aviation providers that it engages to advise on safety of flight aspects including the use of personal protective equipment (PPE).
Related occurrences
Global data
Birdstrikes are a recognised hazard in aviation and there are mitigators in place at certified airports, however, there are challenges when operating outside of these areas.
A review of Australian and internation data was conducted using the Avisure serious accident database. Between 1912 and 2024, birdstrikes have resulted in 763[4] reported aviation occurrences worldwide that involved serious or fatal injuries, of which 204 were fatal. Among these fatal cases, 18 involved rotary‑wing aircraft such as helicopters. These 18 accidents comprised 13 civil and 5 military rotary‑wing aircraft (Figure 6).
Figure 6: Global birdstrike data resulting in fatalities
Data does not include this occurrence (AO-2025-039). Source: Avisure
United States data
In the United States, a total of 13,667 bird strike occurrences were reported to the Federal Aviation Administration (FAA) in operations involving aircraft (fixed-wing and rotary-wing) under 5,700 kg maximum take‑off weight from 2014 to 2024. Of these, 60 occurrences resulted in non-fatal injuries, and 11 were fatal.
A subset of 334 occurrences involved birds striking and damaging the aircraft windshield, with 48 of these occurrences (14.4%) resulting in serious injuries and 6 (1.8%) leading to fatal injuries.
Of the total, 3,001 occurrences involved rotary-wing aircraft, which equated to a birdstrike every 285,390 flight hours (Table 1). These included 201 recorded windshield strikes, that resulted in 28 (13.9%) serious injuries and 2 (1.0%) fatalities.
Flight hours per birdstrike to windshield resulting in damage
Australia
412
39,690
8,819
United States
3,001
285,390
19,026
In comparison to the most frequently struck aircraft component, the wings, with 1,171 occurrences, only 6 (0.5%) resulted in injuries including 1 with fatal injuries (0.09%), indicating that the proportion of serious and fatal outcomes from windshield strikes is unexpectedly high relative to other aircraft parts.
Australian data
Birdstrikes in Australia
Between 2014–2024 the ATSB aviation wildlife dashboard indicated there were 17,060 reported birdstrikes reported to the ATSB across all aircraft types (including fixed‑ and rotary-wing). There were 412 reported birdstrikes during helicopter operations (Table 2), which equated to a birdstrike every 39,690 flight hours. The data did not include what component was struck unless the component was damaged, so it was not possible to determine the proportion of windshields struck that were penetrated or damaged. Of the 412 reported birdstrikes to helicopters, 17 had damage to the windshield.
Table 2: Reported helicopter birdstrikes within Australia 2014–2024
Total reported incidents
Injury level
Aircraft damage
Nil
Minor
Fatal
Nil
Minor
Substantial
Destroyed
Unknown
412
411
0
1[1]
352
37
2
2
19
This figure does not include this occurrence
ATSB records indicate there were 2 fatal accidents in civil aircraft in Australia due to birdstrike. Additionally, there was 1 serious accident involving a bird entering through the windshield. These investigations are described in the following subsections.
Birdstrike involving Glasair Sportsman GS‑2, N666GM, near Bathurst, New South Wales, on 24 December 2015 (
During take-off the aircraft collided with a wedge‑tailed eagle (Aquila audax), penetrating the windscreen and causing significant damage to the propeller and engine, while also striking the pilot, who sustained serious facial injuries and was temporarily unable to see. The pilot, who was wearing a headset and spectacles (both dislodged and damaged during the impact), managed to land safely.
Birdstrike and in-flight break-up involving a Bell 206L‑1, VH‑ZMF, near Maroota, New South Wales, on 9 July 2022 (AO‑2022‑034)
Shortly after departing from a private helipad, the helicopter was struck by a wedge‑tailed eagle (Aquila audax) just below the front left windscreen. The pilot, likely startled by the birdstrike and distracted by sun glare and a required radio frequency change, made abrupt control inputs that caused the main rotor to sever the tail boom, resulting in an in‑flight breakup and collision with terrain. The pilot, who was the sole occupant, was fatally injured.
Birdstrike and collision with terrain involving Air Tractor AT‑502B, VH‑KDR, 32 km east‑north‑east of Chinchilla Airport, Queensland, on 19 September 2022 (AO‑2022‑043)
During low-level aerial spraying at about 8 feet above ground, the aircraft was struck by a large Australian bustard (Ardeotis australis), which shattered the right windshield. The bird entered the cockpit, likely impairing the pilot’s ability to control the aircraft. The aircraft continued for approximately 310 m before colliding with terrain, resulting in the pilot being fatally injured and destruction of the aircraft.
Safety analysis
Birdstrike
Images from the accident site showed that the aircraft collided with a white‑bellied sea eagle (Haliaeetus leucogaster). The pilot had limited opportunity to detect the bird as they were looking down and to the left of the helicopter’s trajectory, so it was probably in their peripheral vision where detection of small objects is very limited. Even if they had been looking ahead at the time, they may not have been able to see the bird in time to avoid it due to the inherent limitations of the see-and-avoid principle. The closure rate to the soaring bird would have been around 94 kt and the difference in speed between them would have also made the relative trajectory almost direct. These factors further reduced the pilot’s ability to see the bird and change the helicopter’s flight path in time, likely rendering the collision unavoidable under the circumstances.
Considerations for aircraft operators and employers
Windshield impact resistance
The analysis of bird strike data highlights the significant safety risks posed to windshields. In windshield impacts in the United States, 14.4% caused serious injuries and 1.8% caused fatalities. Australia’s occurrences included 3 fatal and 3 serious injuries. Comparison of the United States and Australian data indicated that there was a higher chance of both birdstrike and the strike resulting in windshield damage per flight hour in Australia.
There is an elevated risk for helicopter operations due to low‑altitude operations and often less robust windshield designs. This is because if a bird penetrates the windshield, it can directly impact occupants, causing injury or incapacitation of flight crew, which may lead to loss of aircraft control or further operational hazards. While advancements in windshield design, such as laminated materials and reinforced structures, have mitigated many impacts, the data highlights vulnerabilities in extreme cases.
Manufacturers like Robinson and Bell have both released birdstrike‑rated windshields that provide higher impact resistance and significantly decrease the likelihood of objects breaching the windshield upon impact. However, these windshields have been rated to withstand a 1 kg bird strike at the aircraft’s never‑exceed speed, and the occurrence scenario involving a 3 kg bird colliding with the helicopter would likely exceed the windshield’s design limits. Nevertheless, and noting there are some disadvantages of impact‑resistant windshields, operators are encouraged to consider installing impact‑resistant windshields if operating in areas with a high probability of birdstrike.
Helmets
Helicopter pilots often wear helmets as a safety measure due to their frequent exposure to the dynamic conditions of rotary‑wing flight, where turbulence, rapid manoeuvres, and potential accidents pose risks of head injury. In contrast, passengers often do not wear helmets, as the risk is lower for occasional travellers, particularly considering the other safety measures associated with commercial passenger transport operations.
Passengers who travel frequently in helicopters fall between these 2 extremes. They are naturally exposed to a higher risk (over the occasional passenger) simply due to the increased number of flights. While the pilot reported being a helmet advocate and had previously discussed the potential benefits with the passenger, the decision whether to wear a helmet was ultimately left to the passenger’s discretion.
Helmets provide an additional layer of protection against birdstrikes, particularly in aviation scenarios like the Glasair Sportsman GS‑2 incident (AO‑2016‑001). A helmet, often equipped with a sturdy visor, can shield the face and head from small‑object impacts, reducing the risk of injury from a shattered windshield. Additionally, a helmet, especially one designed for aviation, is engineered to absorb and disperse kinetic energy from impacts with larger objects such as a bird potentially mitigating the severity of injuries like those sustained by the pilot of the Glasair, who was not wearing a helmet and suffered serious facial injuries. The helmet’s hard outer shell and padded inner liner work together to reduce the force transmitted to the skull, significantly lowering the risk of traumatic brain injuries, concussions, or skull fractures.
A helmet would not have prevented the passenger’s injuries in this case due to the impact location. Nevertheless, wearing a helmet as standard practice would provide some protection against a range of other potential hazards.
Pilot response
The pilot maintained control of the aircraft despite the sudden disruption and potential aerodynamic effects of the compromised windscreen. They promptly identified the nearest suitable landing site with access to medical facilities and executed a controlled descent and landing.
The pilot’s effective response and adherence to emergency procedures ensured the injured passenger was positioned for immediate medical response, highlighting sound decision‑making under extreme circumstances.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the birdstrike involving Bell 206L‑3, VH‑JMM, 16 km west-north-west of Lake Evella Aerodrome, Northern Territory, on 14 July 2025.
Contributing factors
While cruising at about 900 ft above mean sea level, the helicopter struck a white‑bellied sea eagle, which passed through the windscreen and impacted the passenger.
Other factors
Despite the injuries to the passenger and the damage to the aircraft, the pilot demonstrated composure and maintained control of the aircraft, enabling a calm and controlled return to a location where medical assistance could be provided.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot
Nautilus Aviation
Northern Territory Police Service
recorded data from the Spidertracks unit on the helicopter
OzRunways.
References
Australian Transport Safety Bureau (2002). The Hazard Posed to Aircraft by Birds. Canberra: ATSB.
Debus, S. J. S. (2017). Australasian Eagles and Eagle-like Birds. CSIRO Publishing.
Ferguson-Lees, J., & Christie, D. A. (2001). Raptors of the World. Christopher Helm.
Hobbs, A. (1991). Limitations of the See-and-Avoid Principle. Canberra: ATSB.
Marchant, S., & Higgins, P. J. (Eds.). (1993). Handbook of Australian, New Zealand and Antarctic Birds: Volume 2 - Raptors to Lapwings. Oxford University Press.
Washburn, B. E., Begier, M. J., & Wright, S. E. (2015). Wildlife strikes to civil helicopters in the United States, 1990–2011. Wildlife Society Bulletin, 39(1), 115‑120.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
Nautilus Aviation
Telstra
Civil Aviation Safety Authority
Northern Territory Police Force
TSB Canada.
Submissions were received from:
Nautilus Aviation
Telstra
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Antenna tower with designation NYQUIST NT 0822.
On 12 June 2025, a student pilot conducting a solo navigation flight in a Piper PA-44 was returning to Jandakot Airport, Western Australia, at the same time a Cessna 172 was approaching the airport from the training area. Air traffic control (ATC) directed the pilot of the faster PA-44 to overtake the C172 as they approached the circuit area. However, the PA-44 did not pass the C172 prior to joining the circuit and, consequently, ATC amended their instruction to the pilot of the PA-44, instructing them to ‘follow the Cessna’ and instructed the C172 pilot to join downwind and land first.
Despite that instruction, the pilot of the PA-44 continued to overtake the C172 as per the previous instruction, by accelerating, descending and turning inside the C172.
What the ATSB found
The ATSB found that the PA-44 pilot did not identify the final part of the amended instruction to ‘follow the Cessna’, likely due to receiving an unexpected cockpit traffic alert at the time the approach clearance was issued. Consequently, the PA-44 pilot passed the C172 as per the original clearance, resulting in reduced separation between the 2 aircraft.
The ATSB also found that, although a key element of the revised approach clearance, the pilot’s incomplete readback was not corrected by the controller as the Manual of Air Traffic Services did not explicitly require sequencing instructions to be read back. This was a missed opportunity to resolve the situation and, more generally, provided no assurance that this safety-critical aspect had been correctly understood.
What has been done as a result
Following the incident, the operator of both aircraft completed a presentation to students regarding compliance with ATC instructions and conducted a flight with the incident pilot to assure circuit rejoin procedures and to regain their confidence. Similar flights were also conducted with other student pilots at the company. Additionally, the operator and Airservices have engaged to better understand the challenges with student training at Jandakot.
In addition, Airservices Australia advised that the Air Traffic Management Standards and Senior Air Traffic Services Specialists conducted a review, and will investigate a change to Manual of Air Traffic Services 9.2.2.13.2 and the respective Aeronautical Information Publication reference (GEN 3.4 – 37) to include the instruction ‘follow’ in the list of items requiring readback.
Safety message
This incident highlights the importance of ensuring that all parties have an accurate situational understanding, especially when plans change. Sequencing of aircraft is a safety critical component of assuring separation and needs to be unambiguous for all. For flight crew, they should seek confirmation from controllers if they are unsure of what is required of them or if the picture doesn’t look right. Similarly, if there is any doubt, ATC should confirm that pilots have a correct understanding of sequencing requirements.
The occurrence
At 1124 local time on 12 June 2025, a pilot conducting a navigation flight in a Piper Aircraft Inc. PA-44-180 (PA-44) aircraft, registered VH-KZJ, was inbound to the circuit area at Jandakot Airport, Western Australia. The flight was the third solo flight for the pilot in a twin-engine aircraft, and their first time operating VH-KZJ. At the same time, a Cessna 172 (C172) aircraft, registered VH-ZER, was also inbound to Jandakot Airport, with an instructor and student on board after conducting a training flight.
The runway in use at Jandakot was 06L[1] and local procedures required aircraft to contact air traffic control (ATC) at specified approach points (in this instance Oakford and Russell) then track to Forrestdale Lake. From there, aircraft were to fly overhead the airport at 1,500 ft above mean seal level (AMSL) towards the north and join the circuit as directed by Jandakot Tower (Figure 1).
As the PA-44 was passing the inbound reporting point Russell, ATC passed traffic information on the C172 inbound to the circuit area via the Forrestdale Lake inbound reporting point (Figure 1). With the PA-44 being the faster aircraft, ATC instructed the PA-44 pilot to overtake the C172 on the right which was acknowledged by the PA-44 pilot by a callsign response. The pilot then reported at Forrestdale Lake with the C172 in sight. Both aircraft were at 1,500 ft.
Figure 1: Aircraft inbound tracks
Source: Google Earth with fight radar tracking, annotated by the ATSB
Despite the ATC instruction to overtake the C172, the pilot in the PA-44 reduced the engine power to circuit power, which resulted in the aircraft slowing down. As such, the PA-44 did not overtake the C172 prior to joining the downwind leg of the circuit.[2]
Observing that the PA-44 had not overtaken the C172 as they had anticipated, the controller changed their sequencing plan to have the C172 land first. The table below details the exchange between the pilots and controller and Figure 2 shows where these calls were in relation to the flight paths.
Table 1: Communication
Time
From
To
Transcript
A
1127:55
Controller
C172
ZER make a left turn, join late downwind RWY 06L maintain 1,500
C172
Controller
Take a left turn join late downwind 06L and maintain 1,500 ZER
B
1128:13
Controller
PA-44
KZJ join downwind from that heading, cleared visual approach and follow the Cessna out to your left joining late downwind, high mid downwind
ZER that twin has cut you off they’re low in your 12 o’clock
C172
Controller
Yeah we’ve got the company twin, we’ll make number two to them ZER
Controller
C172
ZER thanks
Figure 2: Aircraft track with ATC clearances
Source: Google Earth with fight radar tracking, annotated by the ATSB
The pilot in the PA-44 reported that, as ATC was issuing its approach clearance, the traffic advisory system (TAS) in the aircraft began audibly alerting. The pilot later advised they were not familiar with the TAS and had never heard the audible alert before. They reported that as their attention was focused on the alert, they did not hear the sequencing part of the instruction to ‘follow the Cessna’. As such, they did not repeat this part of the instruction during the readback of their clearance and believed they were still cleared to pass the C172.
They further advised they had always previously been required to read back the complete sequencing instruction and as they were not prompted for any further readback on this occasion, did not consider that they had not heard the instruction correctly.
The PA-44 continued to overtake the C172 on downwind by descending and accelerating, and then turning inside the C172. The pilot recalled that they thought the sight picture of the close overtake ‘did look a bit odd’, but did not consider questioning the controller.
The instructor in the C172 was also an instructor of the pilot in the PA-44. When hearing their student’s interactions with ATC, they were concerned that the pilot may not have understood the intention of ATC. As such the instructor ensured they maintained visual contact with the PA-44 throughout the sequence.
Both pilots reported that they could see the other aircraft for the duration of the incident.
Context
Pilot details
The pilot of the Piper Aircraft PA-44 held a private pilot licence (aeroplane) and had a class 1 aviation medical certificate. They were undergoing training to obtain their commercial pilot licence (aeroplane) and had a total of 128 hours of flying experience, of which 22 were on the PA-44. They had flown 37 hours in the previous 90 days.
The instructor of the Cessna Aircraft Company 172 (C172) held a commercial pilot licence (aeroplane) with a class 1 aviation medical certificate. They held an instructor and instrument flight rating. They had a total of 1,200 hours of flying experience, of which 390 were on the C172. They had flown 155 hours in the previous 90 days.
Aircraft details
The Piper Aircraft Inc PA-44-180 is 4-seat, low-wing, retractable-undercarriage aircraft with 2 piston engines. VH-KZJ was equipped with the Garmin G1000 avionics suite and optional traffic advisory system (TAS).
The Cessna Aircraft Company 172S is a 4-seat, high-wing, fixed-undercarriage aircraft with one piston engine.
Training
The operator advised that VH-KZJ was the only aircraft in its fleet fitted with the optional traffic advisory system (TAS) with the avionics suite (G1000) and it does not provide formal syllabus training on the TAS. A general awareness was provided during a dual flight, where the TAS system test was conducted as part of the PA-44 (G1000) Normal Checklist – After Start Checklist.
Provision of separation in Class D airspace
In accordance with Aeronautical Information Publication Enroute 1.4-13 as both aircraft were operating under Visual Flight Rules (VFR) in Class D airspace there was no requirement for Air Traffic Control (ATC) to provide separation.
Readback requirements
Airservices Safety net – operating in Class D airspace highlighted the importance of correct readbacks from pilots to prevent frequency congestion. As part of this guidance, it referred pilots to Aeronautical Information Publication (AIP) General (GEN) 3.4.
AIP GEN 3.4 6.6 General Phrases provided the following phraseology when a pilot was assigned and required to maintain separation with a sighted aircraft:
when a pilot is assigned and required to maintain separation with a sighted aircraft ATC are to use the phrase FOLLOW (or MAINTAIN OWN SEPARATION WITH [AND PASS BEHIND]) (aircraft type or identification) [instructions or restrictions].
Manual of Air Traffic Services (MATS) pilot readback requirements stated:
Obtain a readback in sufficient detail that clearly indicates a pilot’s understanding of and compliance with all ATC clearances, including conditional clearances, instructions and information which are transmitted by voice.
MATS further stated that readback discrepancies must be immediately corrected by the controller.
The controller later advised that the ‘follow the’ instruction was not required to be read back as part of the [key elements] readback requirements in MATS (Figure 3), and therefore there was no reason to correct the incomplete readback. Airservices Australia later confirmed it does not require ‘follow the’ type instructions to be read back.
Figure 3: Manual of air traffic services
Safety analysis
When the air traffic controller identified that the PA-44 had not overtaken the C172 as expected, they amended the PA-44 pilot’s approach clearance to require them to follow it as the second aircraft in the landing sequence. However, when the amended clearance was issued, the pilot’s attention was focused on the aural alert from the traffic advisory system and they did not identify the final part of the instruction to ‘follow the Cessna’. Consequently, and despite recognising that the sight picture was ‘looking a bit odd’, the PA-44 pilot passed the C172 as per the original clearance, resulting in reduced separation between the 2 aircraft.
Contributing factor
The PA-44 pilot did not identify the final part of the amended instruction to ‘follow the Cessna’. Consequently, the PA-44 pilot passed the C172 as per the original clearance, resulting in reduced separation between the 2 aircraft.
Having missed the requirement in the amended clearance to follow the C172, the PA-44 pilot did not include the sequencing information in their readback. Although this was a key element of the revised approach clearance, the pilot’s incomplete readback was not corrected by the controller as they considered that the pilot was not required to read back that instruction. This was a missed opportunity to resolve the situation.
Contributing factor
Although a key element of the revised approach clearance, the pilot’s incomplete readback was not corrected by the controller as they considered that the pilot was not required to read back the ‘follow the Cessna’ instruction.
Safe circuit pattern operation relies on all the involved pilots having a common understanding of the aircraft sequence. Additionally, overarching guidance in the Manual of Air Traffic Services (MATS) required controllers to ‘obtain a readback of sufficient detail that clearly indicates pilots’ understanding of and compliance with all ATC clearances.’ Despite that, MATS did not explicitly require sequencing instructions to be read back as a ‘Key element’ of the approach clearance, providing no assurance that this safety-critical aspect had been correctly understood.
Contributing factor
The Manual of Air Traffic Services did not explicitly state that sequencing instructions were required to be read back by a pilot, providing no assurance that this safety-critical aspect had been correctly understood. (Safety issue)
Finally, the situation awareness maintained by the instructor in the C172 ensured that adequate separation was maintained between the 2 aircraft as the situation developed, possibly preventing a more serious outcome.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the separation occurrence involving Piper PA-44, VH-KZJ, and Cessna 172, VH-ZER, near Jandakot Airport, Western Australia, on 12 June 2025.
Contributing factors
The PA-44 pilot did not identify the final part of the amended instruction to ‘follow the Cessna’. Consequently, the PA-44 pilot passed the C172 as per the original clearance, resulting in reduced separation between the 2 aircraft.
Although a key element of the revised approach clearance, the pilot’s incomplete readback was not corrected by the controller as they considered that the pilot was not required to read back the ‘follow the Cessna’ instruction.
The Manual of Air Traffic Services did not explicitly state that sequencing instructions were required to be read back by a pilot, providing no assurance that this safety-critical aspect had been correctly understood. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: The Manual of Air Traffic Services did not explicitly state that sequencing instructions were required to be read back by a pilot, providing no assurance that this safety-critical aspect had been correctly understood.
Glossary
AIP
Aeronautical information publication
AMSL
Above mean sea level
ATC
Air traffic control
MATS
Manual of Air Traffic Services
TAS
Traffic Advisory System
VFR
Visual Flight Rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilots of both aircraft
the air traffic controller
Airservices Australia
ADS-B data for both aircraft
the operator of both aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilots of both aircraft
the air traffic controller
Airservices Australia
the operator
Civil Aviation Safety Authority.
Submissions were received from:
the air traffic controller
Airservices Australia
the operator.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
[2]The leg of the circuit pattern where the aircraft is flying parallel to the runway but opposite to the direction of landing.
Occurrence summary
Investigation number
AO-2025-033
Occurrence date
12/06/2025
Location
Near Jandakot Airport
State
Western Australia
Report release date
04/12/2025
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Operational non-compliance, Separation issue
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-44-180
Registration
VH-KZJ
Serial number
4496462
Aircraft operator
Airflite Pty Ltd
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
Departure point
Jandakot Airport, Western Australia
Destination
Jandakot Airport, Western Australia
Damage
Nil
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172S
Registration
VH-ZER
Serial number
172S10855
Aircraft operator
Airflite Pty Ltd
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training