Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 25 March 2025, the pilot of a Piper PA-44 was conducting solo circuit training operations on runway 07 at Bunbury Airport, Western Australia, operating under visual flight rules (VFR). While established on a left base circuit leg for runway 07, the pilot heard an inbound radio call on the common traffic advisory frequency (CTAF) from a Van's RV-10, 10 NM to the north-east tracking for the field. As the PA‑44 was already established in the circuit, the pilot reported that they believed they had priority.
The pilot of the RV-10 was conducting an instrument familiarisation flight, with a flight plan lodged under instrument flight rules (IFR). Tracking from the north‑east to Bunbury, the RV-10 was conducting a straight in required navigation performance (RNP) instrument approach for runway 25. Shortly after making the 10 NM call, the pilot of the RV-10 began to align with runway 25 and configure for the approach, descending not below 2,800 ft.
At the time of the RV-10’s arrival into the aerodrome, the PA‑44 was already established on runway 07 circuit operations. Neither pilot reported hearing or arranging arrival or departure sequencing at the time.
The pilot of the PA‑44 was unaware of any imminent conflict and initiated a touch‑and‑go on runway 07. The RV-10 was approximately 5 NM from the runway 25 threshold on a reciprocal heading to the departing PA‑44.
At approximately 3 NM from the threshold of runway 25, the PA‑44 (upwind for runway 07) made a radio call asking if the RV-10 was aware of a potential conflict. The RV-10 pilot advised that they had the PA‑44 in sight and intentionally descended below the reciprocal track in an attempt to increase separation. The pilot of the PA‑44 commenced an early left turn onto crosswind to avoid any further conflict. Separation between the 2 aircraft was reduced to 50 m horizontally at the same level.
Figure 1: Near collision between 2 aircraft on reciprocal headings
Source: Flight Radar24, annotated by the ATSB
Safety message
This occurrence highlights the requirement for pilots to always maintain a strong sense of situational awareness especially when operating at a non‑controlled aerodrome. When conducting an instrument approach in uncontrolled airspace, it is best practice to sequence your aircraft’s arrival with other established traffic (both VFR and IFR) operating in the area.
Alerted see and avoid communication is encouraged, particularly between VFR and IFR operated flights, as instrument approach procedures may interfere with VFR operations in visual conditions.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing the collision risk around non-towered airports.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-018
Occurrence date
25/03/2025
Location
Bunbury
State
Western Australia
Occurrence class
Serious Incident
Aviation occurrence category
Near collision
Highest injury level
None
Brief release date
14/07/2025
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-44-180
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
Date of access(date decision released to applicant)
FOI reference number
Description of documents
Documents released
Access
12 June 2026
FOI 25-26(21)
...any surviving documentation relating to a historical aviation occurrence recorded in July 1969 concerning unusual ground marks on golf courses in Sydney, NSW.
The entry appears in Australian government aviation occurrence listings with the following description:
Date: 2 July 1969 Location: Sydney, NSW Description: “Burn marks reported on two golf courses. Possible UFO landing. RAAF notified.”
I would like to know whether any of the following records still exist:
• the original Department of Civil Aviation occurrence report • any correspondence with the Royal Australian Air Force regarding the event • incident logs from Bankstown Airport air traffic control for that date • any investigation notes or reports concerning the ground marks
1.Copies of any Air Traffic Incident Package or Aviation Incident Files for ATSB’s Investigation OA2026-00097 for a serious incident flight on 22 January 2026 involving VH-DOJ and VH-XC5;
2.Copies of any ADS-B data with regard to the VH-DOJ and VH-XC5 serious incident flight on 22 January 2026 reference ATSB OA2026-00097;
3.Copies of any radar and/or automation data (replays) associated with the VH-DOJ/VH-XC5 serious incident flight on 22 January 2026 reference ATSB OA2026-00097; and
4.Copies of any audio communication from or to VH-DOJ or VH-XC5 and Air Traffic Control for the serious incident flight on 22 January 2026 reference ATSB OA2026-00097.
…copies of finalised ATSB aviation occurrences (including AO-series occurrence briefs, RO-series reports, and any internally generated narrative or summary fields) that meet all of the following criteria:
1. The occurrence involves an observation, report, near encounter, or pilot/controller communication regarding an aerial object, activity, or phenomenon that:
• was unidentified at the time of observation, • was unusual or unexpected, • was assessed by crew, ATS, or bystanders as anomalous, or • could not be readily classified as a known aircraft, drone, balloon, meteorological event, or other conventional source at the time of reporting.
2. ATSB occurrence data or narrative fields contain any of the following terms (including fragments and variations):
• “unidentified object” • “UAP” • “UFO” • “unidentified aerial” • “unknown object” • “unusual sighting” • “unexplained aerial” • “anomalous” • “object not identified” • or any equivalent qualifier indicating the object was not immediately identifiable.
3. The occurrence took place during the date range:
...a search of any aviation occurrences involving a Cessna 182L, registration VH-EHB operated in the Northern Territory, between 1 January 1995 and 31 December 1996.
The event of interest reportedly involved a low-level flight near the Stuart Highway close to Mataranka, enroute to Newcastle Waters Station.
The following data related to the recruitment process for the job titled "TRANSPORT SAFETY INVESTIGATOR - RESEARCH - Reference No: 2025/05" that ended on Wednesday the 25th of June, at 11:59 PM:
1) Total number of applications received, total number of applicants shortlisted for an interview and total number of applicants that were offered a job as a result of this recruitment process.
2) Without identifying individual applicants, a table with metadata for each applicant shortlisted for interview for this job. The table should have the following fields:
a. Applicant number (from 1 to total number of applicants)
b. Highest qualification achieved (Diploma, Bachelor, Master, PhD, etc from applicant's coversheet)
c. Diversity details (from applicant's coversheet)
d. Years of work experience (estimated from applicant's CV)
e. Current APS employment status (agency name if they are currently employed by the APS, from applicant's coversheet)
f. Whether they were shortlisted for an interview
g. Whether they were offered a position or a place in the merit list/pool
Complete copy of the ATSB’s investigation file, including, but not limited to, any communication, reports, records, handwritten notes, witness statements, electronic documents, photographs/video, improvement notices and prosecution notices relating in relation to an aircraft accident involving a McDonnell Douglas 369D, VH-PLU, in the vicinity of Townsville Airport (Queensland) on 09 April 2008. (AO-2008-025) [non-restricted information only].
Complete copy of the ATSB’s investigation file, including, but not limited to, any communication, reports, records, handwritten notes, witness statements, electronic documents, photographs/video, improvement notices and prosecution notices relating in relation to an aircraft accident involving an Airbus Helicopters AS350B3e, VH-SZS, in the vicinity of Woomera (South Australia) on 20 March 2019. (AO-2019-015) [non-restricted information only].
Complete copy of the ATSB’s investigation file, including, but not limited to, any communication, reports, records, handwritten notes, witness statements, electronic documents, photographs/video, improvement notices and prosecution notices in relation to an aircraft accident involving a McDonnell Douglas 369D, VH-PLY, in the vicinity of Hawker (South Australia) on 17 July 2016. (AO-2016-078) [non-restricted information only].
Complete copy of the ATSB’s investigation file, including, but not limited to, any communication, reports, records, handwritten notes, witness statements, electronic documents, photographs/video, improvement notices and prosecution notices in relation to an aircraft accident involving a McDonnell Douglas 369D, VH-PLJ, in the vicinity of Murray Bridge (South Australia) on 19 November 2008. (AO-2008-078) [non-restricted information only].
Regarding an accident on 7 January 2025 at Rottnest Island (investigation number AO‑2025‑001):
a complete copy of ATSB’s investigation file, comprising of, but not limited to: any investigation reports, file notes, photographs, witness statements, improvement notices and prosecution notices relating to the accident [non-restricted information only].
...a copy of all incident reports, investigation reports, recommendations, photographs, videos, statements held by the Australian Transport and Safety Bureau in respect of the freight train derailment incident on 15 April 2021 near Bomen NSW.
...copies for all RPAS "Routinely Reportable Matters" that have been submitted to the ATSB by:
FIRE RESCUE VICTORIA ARN 814048 CASA.ReOC.0762 Revision No: 7
If a specific type of RPA is required, I would request data pertaining to Type 2 RPA, otherwise all submissions that have been lodged with ATSB are fine.
On the evening of 2 July 2025, a Virgin Australia Airlines Boeing 737‑800 aircraft, registered VH-YFZ, operated a scheduled passenger flight from Sydney, New South Wales, to Melbourne, Victoria.
During the arrival into Melbourne, the aircraft exceeded 2 speed limitations on the standard terminal arrival route, and air traffic control issued 2 speed reduction instructions, likely to maintain separation from traffic.
Perceiving the ATC instructions to be urgent, the crew hastened the conduct of the approach actions and missed arming the speedbrake and performing the landing checks. As the aircraft descended below 1,000 ft above airfield elevation the crew assessed the approach to be stable and continued, resulting in the aircraft landing with the speedbrake not armed, which resulted in it not automatically deploying. Noticing this, the captain moved their hand to the lever to raise it manually. However, the speedbrake simultaneously automatically deployed as the first officer selected reverse thrust. Thereafter the aircraft’s deceleration was sufficient, and the flight concluded without further incident.
What the ATSB found
The ATSB found that the flight crew allowed the aircraft to exceed speed limitations on the arrival, resulting in air traffic control requiring them to reduce speed. The crew were slow to take positive steps to reduce speed requiring ATC to instruct them to slow further. The crew’s attention became focused on achieving the requested speed reductions, which likely resulted in them omitting to arm the speedbrake and conduct the landing checks.
As the aircraft passed 1,000 ft above airfield elevation, neither flight crew recognised that the speedbrake was not armed and the landing checklist had not been completed, resulting in the approach continuing despite the stabilised approach criteria not being met.
Safety message
Threat and error management (TEM) principles state that flight crews' proactive management of workload throughout the flight is a key defence against capacity and attention-related errors.
Checklists are a vital defence against human error and are integral to maintaining flight safety. This occurrence highlights the importance of adhering to standard operating procedures and ensuring checklists are conducted at the appropriate times.
Many of the speed limitations built into approach procedures are designed to facilitate predictable traffic flows and manage both controller and flight crew workloads. Exceeding the published approach speeds without clearance compromises this risk control and introduces the threat of additional workload and demands on attentional resources.
Many transport jets, such as the 737-800, have a limited capacity to simultaneously descend and decelerate when in a clean configuration. In some modes and flight conditions the aircraft’s autopilot system will be unable to meet altitude and airspeed constraints contained in arrival and approach procedures. The flight crew must therefore be vigilant in monitoring and managing the aircraft’s descent profile and energy condition and be ready to intervene as necessary.
Correct management of the aircraft’s profile and energy during the descent is an effective countermeasure against approach and landing accidents. The Flight Safety Foundation (2000) provides guidance to flight crew on this matter (FSF ALAR Briefing Note 4.1 – Descent-and-approach Profile Management) as part of its broader approach and landing accident reduction (ALAR) toolkit.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 2 July 2025, a Virgin Australia Airlines Boeing 737-800 aircraft, registered VH-YFZ, was operating a scheduled passenger flight,[1] VA882, from Sydney, New South Wales, to Melbourne, Victoria. On board were the captain as pilot monitoring (PM),[2] first officer as pilot flying (PF), 4 cabin crew and 170 passengers.
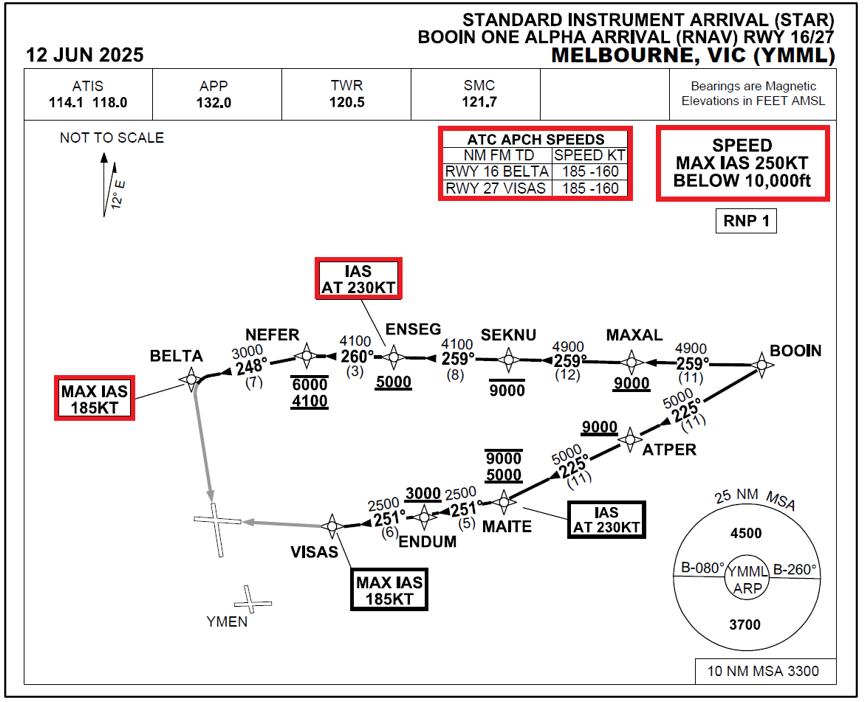
At 2040 local time the aircraft commenced an initial descent from its cruising altitude with a clearance from the Melbourne centre air traffic controller (ATC) to track via the BOOIN ONE ALPHA standard terminal arrival route (STAR) (Figure 1). ATC did not remove any of the speed restrictions associated with the arrival.
Seven minutes later, descending through flight level 140,[3] the aircraft was transferred to the Melbourne approach ATC, who cleared the flight for further descent via the STAR, initially to 5,000 ft, and soon after to 3,000 ft. ATC also issued a clearance for the ground based augmentation system (GBAS) landing system (GLS)[4] approach to runway 16, but again did not remove any speed restrictions.
With the autopilot engaged in VNAV PTH pitch mode (see the section titled Automatic flight modes), the aircraft’s descent was momentarily arrested at 10,000 ft, to decelerate to less than the maximum speed constraint of 250 kt below that altitude. However, as the airspeed decreased to about 260 kt, the autopilot recommenced the descent, and the aircraft’s deceleration ceased. Subsequently, the aircraft crossed the ENSEG waypoint,[5] located approximately 21 track miles from the runway threshold at 263 kt, 33 kt above the speed required at that waypoint by the arrival procedure.
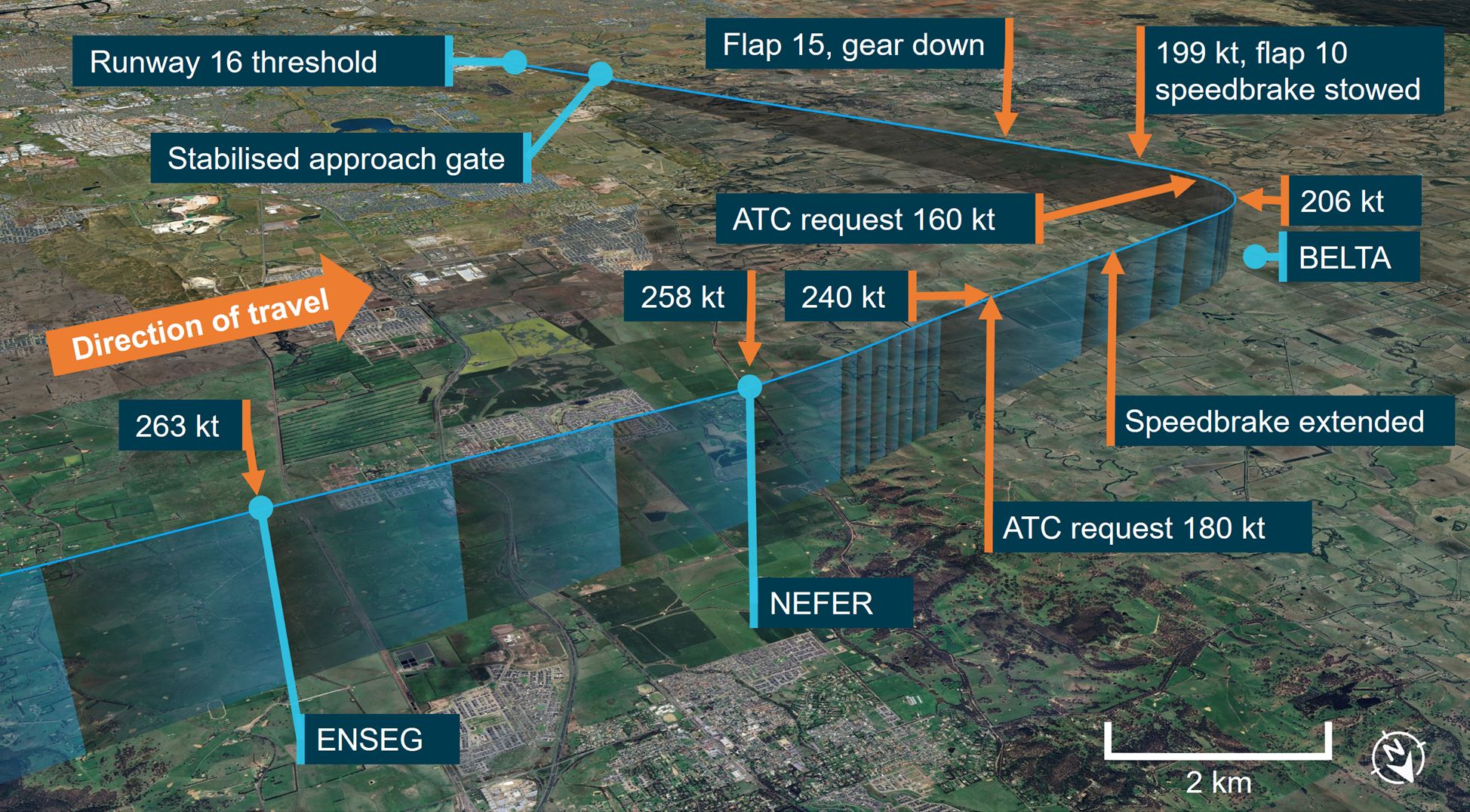
When the aircraft was approximately 15 track miles from the runway threshold, around 4 NM from initial approach fix BELTA and descending through 5,250 ft above mean sea level (AMSL), ATC instructed the flight crew to reduce their speed to 180 kt. At this stage, the aircraft was in a clean configuration[6] and slowly decelerating through 240 kt. Shortly thereafter the flight crew began to extend the initial stages of flap and deployed the speedbrake.
Figure 1: BOOIN ONE ALFA standard instrument arrival procedure chart
The chart shows graphical section of the STAR with the applicable speed restrictions highlighted in red by the ATSB. Source: Airservices Australia
Just over one minute later, as the aircraft was abeam BELTA and midway through the turn to the final approach course, ATC requested a further reduction in speed to 160 kt, likely for traffic separation. The crew perceived the ATC request to be urgent and began selecting flaps earlier than normal to arrest the aircraft’s speed. The aircraft passed abeam BELTA, with the speedbrakes still deployed, decelerating through 206 kt and descending through an altitude of 4,000 ft AMSL.
Shortly after passing BELTA at 199 kt, flap 10 was selected, and then the speedbrake was stowed. Twenty seconds later, at approximately 9.5 NM from the runway threshold and descending through 3,650 ft AMSL, flap 15 was selected and the landing gear was extended. While the operator’s standard procedures call for the speedbrake lever to be placed into the armed position after the selection of flap 15, it remained in the stowed position for the remainder of the approach.
The flight crew selected the landing flap configuration of 30, approximately 8.5 NM from the runway threshold at 3,330 ft AMSL, but did not action the landing checks, as called for in the operator’s standard procedures.
Figure 2: Aircraft flight path and key events during the transition from the arrival to the approach procedure
Source: Google Earth and Flightradar24, annotated by the ATSB
The aircraft descended through the 1,000 ft above airfield elevation stabilised approach gate (see the section titled Stabilised approach requirements) on the GLS course and glideslope, with the airspeed stable at 150 kt, but with the speedbrake lever still in the stowed position and the landing checks incomplete. The crew advised the ATSB that the stabilised approach criteria were assessed, but neither crewmember recognised that they had not been met. As a result, they continued the approach.
Upon touchdown, the captain sighted the speedbrake lever and noted that it had not automatically moved to the deployed position. As they moved their hand to the lever with the intention of manually extending the speedbrakes, the lever began to automatically deploy, coincident with the first officer selecting reverse thrust.
The aircraft decelerated normally and exited the runway. As the flight crew began their post‑landing actions, the captain noted that the line pointers on both yoke‑mounted checklists had not been moved below the bottom of the approach checks, signalling that the landing checks had not been completed. After manoeuvring the aircraft onto the stand and shutting down the engines, the flight crew discussed what they thought had probably happened. The first officer was unaware that the speedbrake had not been armed prior to landing, nor that the landing checks had not been performed.
Context
Flight crew background
The captain and first officer both held an air transport pilot licence (aeroplane) and a class 1 aviation medical certificate. The captain had around 13,600 total flight hours (5,500 on the 737), and the first officer had just over a total of 3,000 hours at the time of the incident. The flight was the captain’s first in almost a month, having been away from work on annual leave. They advised that although they were comfortable with the flight, they felt slightly below their normal performance capability.
Aircraft information
VH-YFZ was a Boeing 737-800, serial number 41005, manufactured in the United States in 2017. The 176-seat aircraft was fitted with 2 CFM International CFM56-7B24E turbofan engines.
Speedbrake system
The Boeing 737-800 speedbrake system is comprised of 6 hydraulically-actuated spoiler panels on the upper surface of each wing, 4 flight spoilers and 2 ground spoilers. In flight, only the flight spoilers may be extended, and are used symmetrically across the wings to increase drag. On the ground, both flight and ground spoilers may be extended to assist with deceleration.
The 737 NG Flight crew training manual stated that:
The use of speedbrakes with flaps extended should be avoided, if possible. With flaps 15 or greater, the speedbrakes should be retracted. If circumstances dictate the use of speedbrakes with flaps extended, high sink rates during the approach should be avoided. Speedbrakes should be retracted before reaching 1,000 feet AGL [above ground level].
Operation of the speedbrakes is achieved via the speedbrake lever. This lever can also be set in the ARMED position. In flight this will not result in speedbrake extension, however after landing, when the conditions are met, all spoiler panels will automatically raise to their maximum extent.
Normally, for the speedbrake system to operate automatically during landing, the following set of conditions must be met:
speedbrake lever in the armed position and the light illuminated
radio altitude less than 10 ft
landing gear strut compressed
both thrust levers retarded to idle
main landing gear wheels spun up (more than 60 kt).
However, if the speedbrake lever is not in the armed position during landing, the speedbrake system will also automatically operate when the following conditions are met:
main landing gear wheels spun up (more than 60 kt)
both thrust levers retarded to idle
reverse thrust levers positioned for reverse thrust.
Automatic flight modes
The aircraft’s automatic flight system consisted of the autopilot flight director system (AFDS) and autothrottle (A/T). They could be used together in a number of distinct modes to achieve lateral and vertical navigation, and speed management. For descents, a vertical navigation mode could be selected via the VNAV switch on the mode control panel (MCP). The aircraft’s flight management computer (FMC) would command the AFDS pitch and A/T to fly a pre‑programmed vertical profile, attempting to accommodate waypoint altitude and airspeed constraints.
In most scenarios, selecting VNAV engaged the VNAV PTH mode, where maintenance of vertical flightpath was prioritised over airspeed. In certain situations, such as steep descent profiles in clean configuration, the aircraft may be unable to decelerate or maintain airspeed limits, even with idle thrust. In these situations, VNAV PTH mode would seek to achieve the programmed descent path, including altitude constraints, and may allow the airspeed to increase within broad limits, before reverting to a speed prioritised mode (VNAV SPD).
Standard operating procedures
Approach configuration sequence
The operator’s 737 NG Flight Crew Operations Manual (FCOM) specified a normal sequence of flight crew actions for a GLS approach, as well as the areas of the flight deck for which each flight crew member was responsible.
When the first officer was operating as the pilot flying, it was their responsibility to move the speedbrake lever to the ARM position and verify the status of the corresponding annunciator, prior to landing. At around 2,000 ft above airfield elevation, the normal procedure specified that the speedbrake arming action should occur, immediately after the pilot flying called for ‘Gear Down’ and ‘Flaps 15’.
The normal procedure also specified that it was the pilot flying’s responsibility to call for the landing checklist to be completed at around 1,500 ft above airfield elevation. This should normally occur as part of a second block of configuration actions, immediately after the pilot flying called for the landing flap to be set and the threshold target speed to be bugged.
The Quick Reference Handbook (QRH) section of the FCOM specified the normal landing checklist, and contained the following items, all to be confirmed by the pilot flying:
Engine start switches………………………..CONT
Speedbrake………………………………......ARMED
Landing gear………………………………….Down
Flaps……………………………………..……Green light
A checklist and movable position marker were mounted to each of the aircraft’s control yokes. The occurrence happened at night in a darkened cockpit and the checklists did not have backlighting.
Stabilised approach requirements
The operator’s normal procedures for a GLS approach called for the flight crew to assess the approach against stabilisation criteria at 1,000 ft above airfield elevation and initiate a missed approach if the conditions were not met. The criteria were specified under the operator’s stabilised approach policy, contained within their general operating policies and procedures manual. They were as follows:
briefings and normal checklists completed
aircraft in the correct landing configuration
aircraft on the correct lateral and vertical flight path
sink rate, no greater than 1,000 fpm
thrust setting appropriate for the aircraft configuration and trajectory
speed within -5 kt to +10 kt of the speed target.
Instrument arrival procedure speed restrictions
The STAR contained several speed limitations (Figure 1). Airservices Australia’s Aeronautical Information Publication (AIP) Enroute 1.5 - 47 included the following requirements:
10.2.1 Unless explicitly cancelled or amended by ATC, the pilot must follow the vertical and lateral profile of the STAR and comply with any published speed restrictions.
On this occasion ATC did not cancel the speed restrictions when clearing the flight to conduct the STAR.
Safety analysis
The flight crew used the autopilot’s vertical navigation path (VNAV PTH) mode and auto throttle to manage the aircraft’s descent profile and airspeed for the arrival.
On this occasion, and as per expected system performance, in a clean configuration, the autopilot was unable to sufficiently reduce speed such that it could simultaneously meet the descent profile and airspeed requirements of the arrival procedure. With no additional drag added by the flight crew, the aircraft continued to maintain an airspeed around 30 kt higher than the speed restrictions in the STAR, until the air traffic controller issued a speed reduction instruction and the flight crew modified the aircraft’s configuration.
The crew perceived the ATC instruction to be urgent and advised that this increased their workload. It is likely the crew focused their attention on monitoring the airspeed and ensuring the flaps were extended promptly, but within their operational limits. Wickens (2021) describes attentional narrowing as a focus on a limited set of information at the expense of other sources. This focus can cause steps in the linear sequence of a procedure to be skipped.
As the aircraft was decelerated to final approach speed and configured for landing earlier than normal, it is probable that the crew omitted to arm the speedbrake and call for the landing checks because their attention was focused on achieving the ATC‑requested airspeed reduction. Compounding this, the captain perceived that their monitoring performance was modestly degraded due to a lack of recent flying experience.
During the final segment of the approach, while the aircraft was on the approach path and the speed had reduced to the required approach speed, the aircraft did not meet all the stabilised approach criteria since the landing checklist had not been completed, and the speedbrake was not in the armed position.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the incorrect landing configuration involving Boeing 737, VH-YFZ, near Melbourne Airport, Victoria, on 2 July 2025.
Contributing factors
The aircraft exceeded speed restrictions during the arrival and the crew did not take appropriate action to slow the aircraft in a timely manner. This resulted in the air traffic controller issuing instructions to reduce speed further and the crew subsequently not arming the speedbrake and performing the landing checks.
As the aircraft passed 1,000 ft above airfield elevation, neither flight crew recognised that the speedbrake was not armed and the landing checklist had not been completed, resulting in the approach continuing despite the stabilised approach criteria not being met.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilots of the incident flight
operational documentation from Virgin Australia Airlines
Airservices Australia
ADS-B data from Flightradar24
recorded data from the aircraft Quick Access Recorder.
Wickens, C. (2021). Attention: Theory, principles, models and applications. International Journal of Human–Computer Interaction, 37(5), 403-417.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilots of the incident flight
Virgin Australia Airlines
Civil Aviation Safety Authority.
Submissions were received from:
the pilots of the incident flight
Virgin Australia Airlines.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The flight departed Sydney at 1935 local time, 35 minutes later than the scheduled departure time, after weather conditions in the Sydney area had caused disruptions and delays to traffic movements.
[2]Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 140 equates to 14,000 ft.
[4]GLS: a GBAS Landing System (GLS) is an alternative to the Instrument Landing System and uses the Global Navigation Satellite System (GNSS), augmented by an airport ground station, to provided suitably equipped aircraft with precision approach guidance.
[5]Waypoint: a specific geographical location, defined by latitude and longitude coordinates, that is used to define an aircraft’s flight path
[6]Clean configuration: an aircraft is in a clean configuration when all external drag‑inducing equipment, such as landing gear, flaps and spoilers, are retracted.
An investigation is underway into a train separation, and the runaway of 64 wagons between Eastwood and Meadowbank, New South Wales, on 6 July 2025.
At 0433 hours on 6 July 2025, Qube Logistics freight service 1WB7 was travelling north on the Sydney Trains network, when the consist separated at the southern end of Eastwood station. 1WB7 consisted of 3 locomotives hauling 64 wagons loaded with steel products from Port Kembla, New South Wales, to Acacia Ridge in Brisbane, Queensland. The separation was a result of a broken knuckle between the hauling locomotives and the leading wagon.
At the time of separation, the train was travelling on a shared network with Sydney Trains passenger services, on a 1:40 uphill gradient. The separated wagons rolled backwards down the main line to Meadowbank station where they came to a standstill. There were no reported injuries.
The investigation scope includes risk controls for train separation and runaway, the condition of rollingstock and braking performance, train operations and emergency response, and gathering any other relevant information.
This investigation is being led by the Office of Transport Safety Investigations (OTSI). OTSI conducts rail investigations in NSW under the Transport Safety Investigation Act 2003 in accordance with a collaboration agreement with the ATSB.
The final report will be released at the conclusion of the investigation. However, should a critical safety issue be identified during the course of the investigation, OTSI and the ATSB will immediately notify relevant parties, so that appropriate and timely safety action can be taken.
On 1 July 2025, at about 1430, the pilot was the sole occupant of a Robinson R22 Beta II helicopter, being operated by North Australian Helicopters to conduct aerial mustering operations for a cattle station about 58 km north-west of Anthony Lagoon, Northern Territory.
Two R22’s provided by the operator were contracted by the cattle station owner and were assisted by stockmen on the ground.
While working an animal towards a holding yard, the animal baulked when about 4 m from the aircraft and turned away from the mustered direction. The pilot flared the helicopter as a reaction to the animal’s movement to prevent the animal from escaping, but at the time was about 6 ft above the ground with a quartering tailwind. The helicopter descended tail-low during the flare and the tail rotor struck the ground. Subsequently, the helicopter began to rotate, completing 2 or 3 rotations before the pilot conducted the emergency procedure for a tail rotor failure. As the helicopter descended, still rotating, during the recovery the right skid impacted the ground and caused the helicopter to roll to the right. The main rotor blades then impacted the ground, and the helicopter came to a stop on its right side.
The uninjured pilot freed themselves from the wreckage, however the helicopter was substantially damaged.
What the ATSB found
After a successful day mustering prior to the accident, the pilot’s attention became increasingly focused on moving the last remaining animal through to the holding paddock while flying in close proximity to the ground.
The last animal baulked before the gate and the pilot attempted to stop it changing direction. With limited time to react due to their close proximity to the animal, they did not anticipate the additional power required to flare the helicopter with a tailwind. The helicopter descended during the flare and the tail rotor impacted terrain, and the damaged helicopter began rotating uncontrollably.
The pilot had conducted a recent proficiency check with the operator that included simulated tail rotor failures. The recency of this training likely allowed the pilot to react quickly with the correct emergency technique, helping prevent a more serious accident and injury.
What has been done as a result
The operator advised that following the occurrence, a check flight was completed with all company pilots.
The operator also updated its collision with obstacles safe work method statement to include that pilots should prioritise flying the aircraft and if animals are unresponsive to the helicopter they should let the animal go.
Safety message
Mustering operations are a high-risk aviation activity, sometimes involving low flying in close proximity to terrain, obstacles, powerlines and stock. Any external distraction presents an increased risk of collision, especially when the aircraft is operated at low level, further reducing the margin of error. Operators are encouraged to identify and discuss the hazards involved in their low-level operations, including the risks of divided attention, with company pilots.
The accident highlights the benefit of recent training, with the pilot able to execute the correct emergency procedure, reducing the severity of the helicopter’s rotation and likely preventing a more serious accident and injury. Operators are encouraged to review the cycle of their recency training and the benefit it may have during an emergency situation.
Furthermore, the operator required pilots to wear helmets when conducting mustering operations. The use of flight helmets as well as seatbelts can prevent and reduce injuries.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 1 July 2025, the pilot and sole occupant of a Robinson R22 Beta II helicopter, registered VH-HGE and operated by North Australian Helicopters, was conducting contracted aerial cattle mustering operations about 58 km north-west of Anthony Lagoon, Northern Territory.
The muster commenced about 0730 local time to move stock to a cattle yarding area. North Australian Helicopters provided 2 Robinson R22 helicopters to assist the stockmen on the ground.
At about 1430, while being mustered into a holding paddock, a mob of 10–15 cattle broke away from the main group. The helicopters were sent to herd the stock back toward the holding paddock. Five animals[1] from the group again broke away and the helicopters successfully mustered 4 of the 5 back to the holding paddock.
At about 1510, the pilot of VH-HGE was working the one remaining animal along a fence line (Figure 1) towards the gate of the holding paddock at about 6 ft above the ground. The pilot described that the animal baulked when approaching the gate about 4 m from the helicopter and attempted to run behind the helicopter. The pilot reported that they were highly motivated to complete the mustering operation and became increasingly focused on moving the animal.
Figure 1: VH-HGE accident location and cattle yards
Source: Google Earth, annotated by the ATSB
Reacting to the animal’s movement, the pilot flared[2] the helicopter while travelling downwind in close proximity to the ground. During the flare, the pilot felt the helicopter sink more than expected and the tail rotor impacted the ground. This resulted in the tail rotor becoming ineffective. Without yaw[3] control, the helicopter rotated quickly to the right and the pilot assessed there was a tail rotor failure. The pilot reduced the throttle to decrease the torque and raised the collective to cushion the aircraft onto the ground. The pilot estimated that the helicopter had completed 2 or 3 full rotations, and still had some rotation when the right skid made contact with the ground, causing the helicopter to roll over to the right. The main rotor blades then impacted the ground and the helicopter came to a stop on its right side, resulting in substantial damage (Figure 2).
The pilot was restrained by their seatbelt and uninjured. They were able to free themselves from the wreckage, later stating that their use of a flight helmet had prevented a head impact during the accident sequence.
Figure 2: VH-HGE accident site
Source: North Australian Helicopters
Context
Personnel information
The pilot held a commercial pilot licence (helicopter) issued on 7 August 2023 and had held a private pilot licence (helicopter) since 3 June 2020, with a class rating for single‑engine helicopters. They had held an aerial mustering rating since 9 March 2022 and a low-level operations rating that was valid until 7 May 2027. The pilot had accumulated about 1,970 total hours flying time.
They also held a class 1 medical certificate, valid until 20 August 2025 with no restrictions.
Training
The pilot completed their last helicopter flight review and operator proficiency check flight on 7 May 2025. An operator’s proficiency check was required every 12 months and included low-level operations and simulated emergency procedures relevant to mustering operations, such as managing the loss of tail rotor control in forward flight and during hover. The pilot recalled that about 30 minutes of the check flight was focused on tail rotor failures and jammed flight controls.
Additionally, about 2 weeks earlier, the pilot conducted a check flight with the operator’s chief pilot. The flight included mustering procedures and general flying. The chief pilot recorded that the pilot showed above satisfactory techniques during the check flight.
Following the tail rotor impact with the ground, the pilot recalled there was limited time to assess what had happened before the helicopter began to rapidly rotate and indicated that the recent training allowed them to quickly apply the correct recovery technique.
Fatigue
The pilot reported starting work at 0700 on the day of the occurrence, having obtained about 8 hours of sleep and recalled feeling alert at the time of the occurrence.
Aircraft information
General information
The Robinson R22 is a single-engine, light utility and training helicopter with a semi-rigid, 2-bladed main rotor, a 2-bladed tail rotor and skid type landing gear. It has an enclosed cabin with 2 seats. The pilot sat on the right side, and extensive windows at the front of the helicopter generally afforded unrestricted visibility ahead. The accident helicopter was being flown without doors fitted, as is common in mustering operations.
The R22 Beta II is powered by a Lycoming O-360 4-cylinder piston engine that is derated to 131 hp (96 kW) for take-off and 124 hp (91 kW) for cruise at 2,652 RPM.
VH-HGE was manufactured in the United States in 1996 as serial number 2574. North Australian Helicopters held the registration since July 2009. Its maintenance release was current until June 2026 and did not record any outstanding maintenance or defects.
Helicopter performance
The pilot described a south-easterly wind at about 15 kt; at the time of the accident it was a quartering tailwind from the left.
The New Zealand Civil Aviation Authority Good Aviation Practice: Helicopter Performance publication (2025) stated that:
Only a few knots of wind on the tail can make a big difference to the power required to satisfactorily control the rate of descent during an approach.
In a helicopter, translational lift occurs when clear, undisturbed air flows through the rotor system, either from wind or directional flight improving rotor efficiency. As a helicopter’s airspeed increases the power required to maintain level flight decreases. (Wagtendonk, 2011).
To initiate a flare, the pilot is required to tilt the main rotor system of the helicopter rearwards, raising the nose so the downwash is angled in front of the helicopter, causing a reduction in forward airspeed. However, as the pilot tilts the rotor system, the thrust direction may no longer be vertical and therefore may require additional power to produce additional lift to maintain height.
Tail rotor failure
A helicopter’s tail rotor provides anti-torque control, which counteracts the torque of the main rotor system. A tail rotor failure at low airspeed will result in the helicopter rotating immediately in the opposite direction to the rotation of the main rotor system. The severity of the rotation is directly proportional to the power being applied.
A potentially damaging situation exists when total tail rotor loss occurs unexpectedly at lower than cruising speeds. The fuselage will begin to rotate immediately and it will be difficult to regain directional control. (Wagtendonk, 2011)
The Robinson R22 pilot operating handbook (POH) detailed the procedure for a loss of tail rotor thrust during a hover, stating:
Failure is usually indicated by nose right yaw which cannot be stopped by applying left pedal.
- Immediately roll throttle off into the overtravel spring and allow the aircraft to settle
- Raise collective just before touchdown to cushion landing.
Meteorological information
The graphical area forecast for the Northern Territory, valid between 0830 and 1430 local time, indicated expected visibility in the area greater than 10 km, isolated areas of fumes (smoke) below 5,000 ft, moderate turbulence from the surface to 10,000 ft expected from dust devils[4] and thermals; neither pilot reported any concerns with visibility or other localised weather phenomena. The grid point wind temperature forecast for the Northern Territory, valid from 1230, indicated expected winds at 1,000 ft were about 130° at 15 kt and a forecast temperature of 19°C.
The pilot recalled conditions on the day as fine and sunny and estimated the temperature between 18–20°C with a south-easterly wind of about 15 kt. They reported no issues with visibility while operating at low level. The pilot of the second helicopter also recalled similar conditions at the time of the occurrence.
Aerial mustering guidance
Civil Aviation Safety Authority (CASA) sector risk profile for agricultural flying, published in 2025, indicated for the 10‑year period between 2014 and 2023 a total of 90 accidents and incidents while conducting aerial mustering. Of these occurrences, 71 were categorised as accidents including 7 fatalities.
The sector risk profile also showed that collisions with terrain were the most common fatal and non-fatal accidents in the agricultural flying sector.
The mustering sector risk profile published in 2014 (now superseded by the current agricultural sector risk profile) advised:
The aerial mustering sector is hazard rich due to the inherent characteristics of the operation, such as very low flying, high workload, negative effects from weather, obstacles such as power lines, trees and terrain, pilot distraction, small power margins, and extended time operating within the height/velocity diagram (‘deadmans curve’)….. Pilot training, supervision and mentoring play an important role in developing pilot skills to manage aerial mustering manoeuvres.
North Australian Helicopters’ operations manual stated that the 4 main causes of accidents when conducting mustering operations are:
- turning downwind whilst reducing airspeed and then trying to arrest descent with more collective pitch rather than regaining airspeed
- tail rotor/main rotor strike
- poor recovery from partial power loss (e.g. stuck valve, magneto issues)
- lack of situational awareness due to focussing too much on the animals/job, and/or fatigue.
The operator’s safe work method statements highlighted inadvertent ground impact during low-level flying as a hazard during mustering operations. The assessment indicated a high risk level and the operator’s control for the hazard was instructing pilots that when tracking with a tailwind component to avoid bringing the aircraft into a hover (flaring).
Further resources and guidance material for both pilots and operators within the aerial mustering industry include.
Correctly fitted, secured and maintained flight helmets can save lives.
Divided attention
Humans attend selectively to information due to finite cognitive capacity, making it impossible to process all of the information in our environment at once. Conscious attention is also influenced by tasks that are prioritised (Wickens & McCarley, 2007). Attention directed to a primary task (flying), can quickly shift to a secondary task (mustering stock), at the expense of the primary task (Australian Transport Safety Bureau, 2005).
Task prioritisation is further influenced by motivation to complete a goal, such as an operational goal (Harris, Fein, & Machin, 2002), and pilots can be influenced to prioritise secondary goals (Bearman, Paletz, & Orasanu, 2009) intentionally or unintentionally.
Recency training
The Federal Aviation Authority (FAA) aviation instructor’s handbook details the benefit of recent training:
The principle of recency states that things most recently learned are best remembered. Conversely, the further a learner is removed in time from a new fact or understanding, the more difficult it is to remember. For example, it is easy for a learner to recall a torque value used a few minutes earlier, but it is more difficult or even impossible to remember a value last studied or used further back in time [.…..] In SBT (skills based training), the closer the training or learning time is to the time of the actual scenario, the more apt the learner is to perform successfully. This law is most effectively addressed by making the training experience as much like the scenario as possible.
Survivability
The helicopter was fitted with a lap and sash style seat belt which the pilot wore during the mustering operation.
The operator’s safe work method statements required pilots to wear helmets while conducting mustering operations. The pilot reported that they suspected their helmet probably prevented a head knock during the accident sequence.
The Civil Aviation Safety Regulations did not require pilots to wear flight helmets at the time of the accident. However, the wearing of flight helmets was often required by aircraft operators for pilots engaged in aerial work and mustering operations, and was necessary to meet federal and state legislated workplace, health and safety requirements.
Related occurrences
A search of the ATSB Aviation Occurrence Database showed that in the 5 years since 2020 there have been 7 occurrences that involved commercial mustering helicopters impacting the tail rotor with terrain or obstacles:
Collision with terrain involving a Robinson R22, 202 km south-west of Winton, Qld, June 2022 (AB-2022-003): During low‑level mustering operations, the helicopter struck a motorcyclist while in the hover. The pilot lost directional control and the helicopter subsequently collided with terrain and was destroyed. The motorcycle rider sustained serious injuries.
Collision with terrain involving Robinson R22, 13 km south‑south-east of Fitzroy Crossing, WA, June 2023: During low‑level mustering operations, the pilot applied excessive pitch to manoeuvre clear of trees resulting in the tail rotor striking the ground. The helicopter subsequently collided with terrain and sustained substantial damage.
Collision with terrain involving a Robinson R22, 76 km west‑south-west of Halls Creek, WA, September 2023: During aerial mustering operations, the helicopter’s tail rotor struck a tree and subsequently collided with terrain. The pilot received serious injuries and the helicopter was destroyed by post-impact fire.
Collision with terrain involving Robinson R22, 26 km east of Broome, WA, April 2024: During aerial mustering operations at 6 ft, the pilot detected a jolt through the tail rotor pedals followed by severe vibration. The helicopter collided with terrain and was substantially damaged. The pilot received minor injuries.
Collision with terrain involving Robinson R22, near Mount Valley, NT, May 2024: During aerial mustering operations at 6 ft, the tail rotor struck the ground and the helicopter collided with terrain resulting in substantial damage.
Collision with terrain involving Robinson R22, 139 km south of Kununurra, WA, June 2024: During approach, the tail struck the ground resulting in minor damage to the tail boom.
Collision with terrain involving Robinson R22, at Rockhampton Downs, NT, June 2025: During aerial mustering operations, the helicopter's tail struck the ground and the helicopter collided with terrain, resulting in substantial damage.
Safety analysis
Introduction
In the final stages of the muster, one remaining animal baulked when approaching a gate. To prevent the animal from escaping, the pilot flared the helicopter while low to the ground with a quartering tailwind. During the flare, the helicopter descended, resulting in the tail rotor impacting the ground. The pilot lost yaw control and the right skid contacted the ground, causing the helicopter to roll over.
Divided attention
Having returned 4 out of the 5 stock to the yard, the pilot was highly motivated to complete the mustering operation and their attention became increasingly focused on moving the last remaining animal through to the holding paddock while flying in close proximity to the ground. Associated with this divided attention, the pilot likely had reduced awareness of the helicopter’s proximity to the last animal, the ground and the potential effect of the prevailing wind on the performance of the helicopter.
The helicopter’s proximity to the animal and forward momentum reduced the pilot’s reaction time and options for recovery.
Pilot reaction to baulking animal
The pilot estimated the helicopter was moving forward about 4 m behind the animal at about 6 ft above ground level when it baulked. The pilot likely judged their airspeed by visual reference to ground features and the tailwind likely gave them a sensation of a higher airspeed. With limited time to respond, the pilot likely flared the aircraft as an automatic reaction to the animal’s movement while in close proximity to the ground.
This resulted in the pilot not anticipating the additional power required during the flare, leading to the helicopter descending. This, combined with the change in pitch attitude, lowered the tail rotor closer to the ground. With minimal clearance between the helicopter and the ground, there was likely insufficient opportunity for the pilot to apply additional power to climb or arrest the descent before the tail rotor impacted the ground.
Pilot response to ground impact
Following the tail rotor impacting terrain the helicopter began to rapidly rotate to the right. The pilot assessed there was a tail rotor failure and reduced the throttle to decrease the torque and then increased the collective prior to impact to manage the rate of descent. This likely helped prevent a more serious accident and possible injury.
The operator had conducted a proficiency check flight with the pilot less than 2 months prior to the accident and included tail rotor failure simulations which were recognised by the operator as a common accident during mustering operations.
The recent emergency training likely helped the pilot to react to the tail rotor failure with the correct technique before the helicopter became uncontrollable.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the tail rotor strike involving Robinson R22 Beta II, VH-HGE, 58 km north-west of Anthony Lagoon, Northern Territory on 1 July 2025.
Contributing factors
Focusing their attention on moving stock during mustering operations, the pilot flew the helicopter in close proximity to the ground and one of the animals.
The pilot flared the helicopter in response to the animal baulking at a gate. The combination of the tail wind component and flare at low level led to the helicopter descending and the tail rotor impacting the ground. This resulted in the helicopter uncontrollably yawing to the right.
Other findings
Recent tail rotor failure training during an operator proficiency check ensured the pilot reacted to the emergency with the correct technique, which likely helped prevent injury and minimised damage.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
North Australian Helicopters advised following the occurrence a check flight was conducted with each company pilot.
North Australian Helicopters also advised the safe work method statements had been updated for collision with obstacles adding that pilots were to prioritise flying the aircraft over the movement of stock and if an animal was unresponsive to the helicopter, pilots were advised to let the animal go.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the accident flight and another pilot who conducted flights for the operator
Bureau of Meteorology
operator’s manuals
pilot logbooks and training history
Civil Aviation Safety Authority
aircraft maintenance release.
References
Australian Transport Safety Bureau. (2005). Dangerous Distraction An examination of accidents and incidents involving pilot distraction in Australia between 1997 and 2004.
Bearman, C., Paletz, S. B., & Orasanu, J. (2009). Situational pressures on aviation decision making. Goal seduction and situation aversion. Aviation, Space, and Environmental Medicine, 80 (6), 556-560.
Harris, M. R., Fein, E. C., & Machin, M. A. (2002). A Systematic Review of Multilevel Influenced Risk-Taking in Helicopter and Small Airplane Normal Operations. Frontiers in Public Health.
New Zealand Civil Aviation Authority . (2025). Good aviation practise, Helicopter Performance.
Wagtendonk, W. J. (2011). Principles of Helicopter flight. Newcastle, Washington: Aviation Supplies and Academics, Inc.
Wickens, C. D., & McCarley, J. S. (2007). Executive Control: Attention Switching, Interruptions and Task Management. In Applied Attention Theory. Chapman and Hall.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilot
North Australian Helicopters
Civil Aviation Safety Authority
United States National Transport Safety Board.
A submission was received from:
Civil Aviation Safety Authority.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The animal was a weaner, which are often more erratic in behaviour during a muster.
[2]Flare: raising the nose of the helicopter to slow forward airspeed.
[3]Yaw: sideways rotation around the yaw (vertical) axis.
[4]Dust devils are dust-filled vortices, formed by strong surface heating, which are smaller and less intense than a tornado.
Occurrence summary
Investigation number
AO-2025-035
Occurrence date
01/07/2025
Location
Near Anthony Lagoon
State
Northern Territory
Report release date
21/11/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R22 Beta II
Registration
VH-HGE
Serial number
2574
Sector
Helicopter
Operation type
Part 138 Aerial work operations
Departure point
Anthony Lagoon Aircraft Landing Area, Northern Territory
Destination
Anthony Lagoon Aircraft Landing Area, Northern Territory
On 15 May 2025, a Eurocopter EC120B helicopter, registered VH-JDZ, was operated at Porepunkah aerodrome, with a pilot and one passenger on board. While lifting into a hover, left yaw was allowed to develop without correction. After turning 180° the pilot attempted to arrest the yaw with right pedal input. However, the yaw continued and the helicopter began to rotate, entering an uncontrolled turn. After about three quarters of a revolution the right skid contacted the ground while the helicopter continued to rotate. The helicopter then rolled over, resulting in substantial damage to the aircraft. Neither the pilot nor the passenger sustained injury and safely exited the aircraft.
What the ATSB found
Adequate control of the left yaw after hover was not achieved due to the insufficient application of opposing right pedal input to the tail rotor.
The pilot was highly experienced in rotary wing operations, though reported that they had not flown this type of helicopter (EC120B) for about 15 years. The EC120B is fitted with a Fenestron tail rotor which requires greater pedal response than conventional tail rotor helicopters to counter the torque effect. In this case the pilot had more recent experience flying helicopters with a conventional tail rotor system. Although they were a highly experienced helicopter pilot, the limited recent type-specific experience on the EC120B had degraded their ability to respond appropriately to the helicopter’s different pedal requirements.
Safety message
Maintaining recent type-specific flight experience is vital to prevent degraded performance when transitioning between aircraft with differing control characteristics.
Understanding the aircraft’s characteristics is important for helicopter pilots so that they can anticipate its response when becoming airborne and are not surprised by events. Controlling yaw in helicopters with a Fenestron tail rotor, as in this case, is an essential consideration. Airbus Helicopters and the European Union Aviation Safety Agency (EASA) provide specific guidance relating to this issue to assist pilots.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 15 May 2025, a Eurocopter[1] (Airbus Helicopters) EC120B helicopter, registered VH‑JDZ, was operated at Porepunkah aerodrome, Victoria, for planned private flight to Albury, about 38 NM to the north. On board were the pilot and a passenger, who was also licenced and qualified on the helicopter.
On arrival at the aerodrome, the pilot and passenger prepared the helicopter by moving it out of the hangar and conducting a visual inspection in preparation for flight. At about 1300, the pilot commenced engine start and a short time later began the take-off sequence and brought the helicopter into a hover. The pilot reported that the helicopter was initially slow to lift off but then rapidly rose and began an uncommanded 90° left yaw.[2] The pilot stated that although the yaw was not commanded, they intended to turn in that direction anyway so allowed the yaw to continue and planned to arrest it after it turned 180°.
The pilot then attempted to correct the left yaw with right pedal input while simultaneously pulling up the collective to gain more height. However, the yaw was not adequately countered and with additional torque, the left yaw increased. The helicopter then began to rotate and entered an uncontrolled turn.
The pilot was unable to regain control and the helicopter completed about three quarters of a revolution before the right aft skid contacted the ground, leading to a further rotation on the ground and a dynamic rollover.[3]
The helicopter came to a rest on its right side and the pilot immediatley checked on the welfare of the passenger and turned off the fuel. Noticing smoke and mindful of the potential fire risk, the pilot gave instructions to evacuate immediately.
With some difficulty, due to their wreckage position, both occupants removed their seat restraints, independently exited the helicopter and moved to an area a safe distance away from the wreckage.
As a result of the impact, the aircraft was substantially damaged (Figure 1).
Aerodrome staff and an ambulance arrived at the site shortly after the incident and conducted a medical assessment. It was determined that neither occupant had sustained serious injury.
Figure 1: VH-JDZ photographed after the dynamic rollover
Source: Owner
Context
Pilot information
The pilot held a commercial pilot licence (CPL-H) helicopter issued in September 1994. At the time of the occurrence the pilot’s total flying experience was 11,257 flight hours and they were endorsed to fly the EC120B and had previously owned and operated a commercial helicopter business.
In the 12 months before the accident, the pilot had logged about 100 flight hours, primarily in a Robinson R44. They stated they had not flown an EC120B for about 15 years.
The pilot held a Class 1 aviation medical certificate and reported having a regular sleep pattern of about 7.5–8 hours nightly and had no feeling of fatigue on the day of the incident.
To exercise the privileges of a flight crew licence, the regulations require the pilot to have a valid helicopter flight review (HFR). The pilot last completed this on 6 October 2024 in a Robinson R44 while obtaining a low-level endorsement on the same date.
Aircraft information
The EC120B is a 5-seat, light utility helicopter, powered by a single turboshaft engine. It has a 3-blade main rotor head and a Fenestron anti-torque tail rotor (see Fenestron tail rotor).
The EC120B is powered by a Safran Helicopter engines Arrius 2F single gas turbine engine. VH-JDZ was manufactured in France in 2003 and was first registered in Australia on 24 June 2003. The current owner purchased the helicopter on 14 September 2021.
The helicopter’s maintenance release showed the last daily inspection was completed on 2 May 2025 and showed the helicopter had accrued about 3,172 hours flight time.
Fuel, weight and balance
The pilot reported that the helicopter was carrying a full fuel load. The maximum take of weight (MTOW) is 1,715 kg, of which the fuel capacity is about 410 litres (326 kg) of aviation turbine fuel. With the pilot and passenger on board and full fuel tanks, the helicopter weighed about 1,560 kg which was below the MTOW and within balance.
Flight controls
The helicopter was fitted with standard primary flight controls: cyclic,[4] collective[5] and dual tail rotor anti-torque pedals. The pilot stated that the passenger (also a rated pilot) did not touch the controls. The aircraft was equipped with a single hydraulic system, which assisted main rotor control through 3 hydraulic servos. The tail rotor was not hydraulically assisted and dual controls were installed in the helicopter which are removable when not required. The pilot reported that they were not removed but had adjusted the pedals prior to flight on their side to suit their leg length.
Aircraft handling characteristics
Fenestron tail rotor
The EC120B is equipped with a Fenestron tail rotor or fan-in-fin system (Figure 2). The vertical fin or stabiliser was designed to provide aerodynamic directional stability in forward flight and is larger than those found on similar-sized helicopters with a conventional tail rotor (CTR). The fin was paired with a 0.75 m diameter, 8-bladed tail rotor. The tail rotor was mounted on stators[6] integrated into the vertical fin.
These features combined to change the aerodynamics of the tail rotor, and the relative effectiveness of the anti-torque pedals for a given range of movement, when compared with helicopters with a CTR. Because the tail rotor blades are located within a circular duct, the Fenestron design is considered a safety feature, reducing the risk of contact with people or objects.
Figure 2: Illustration of the design difference between the Fenestron tail rotor and a conventional tail rotor
Source: ATSB
Anti-torque pedals
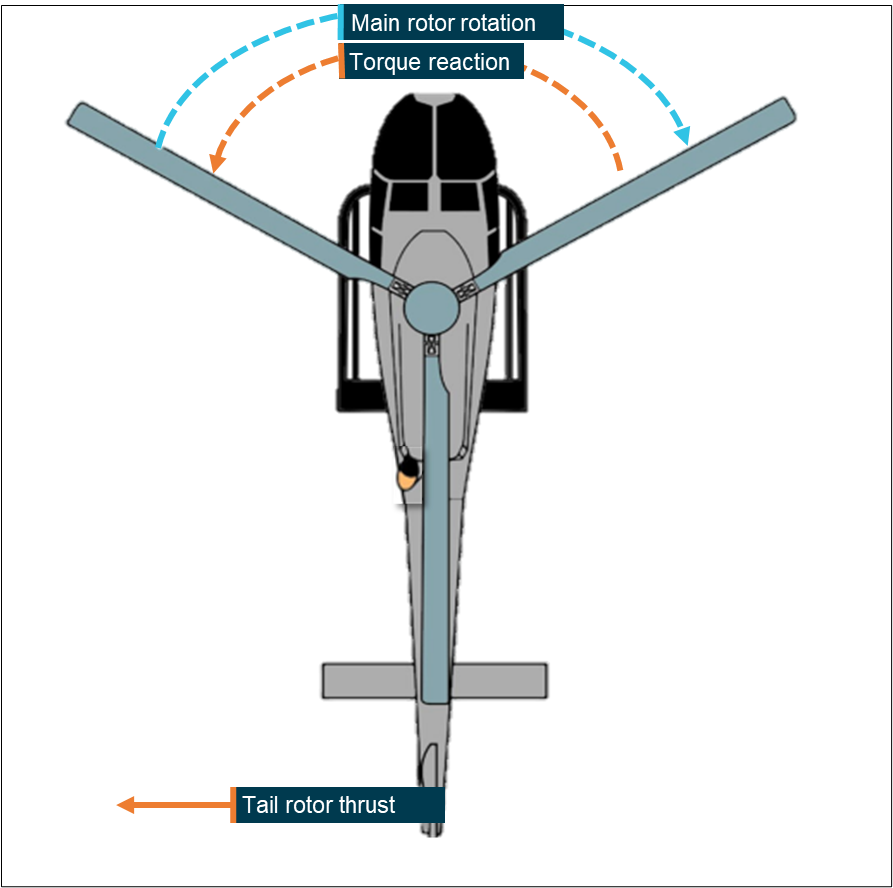
The main rotor on the EC120B rotated clockwise (as viewed from above). The main rotor is driven from a central point, resulting in a torque reaction which causes the fuselage of the helicopter to yaw in the opposite direction to the main rotor’s rotation (Figure 3). In the case of the EC120B, this torque reaction means the helicopter will yaw to the left when power is applied. The force to resist and balance the yaw is produced by the tail rotor and is controlled by the anti-torque pedals in the cockpit. Tail rotor thrust can be increased by pushing the right anti-torque pedal to force the nose to yaw to the right. When a pilot demands power from the engine to increase lift, or as a result of lifting the collective (increasing main rotor blade angle), the torque reaction and yaw to the left will increase.
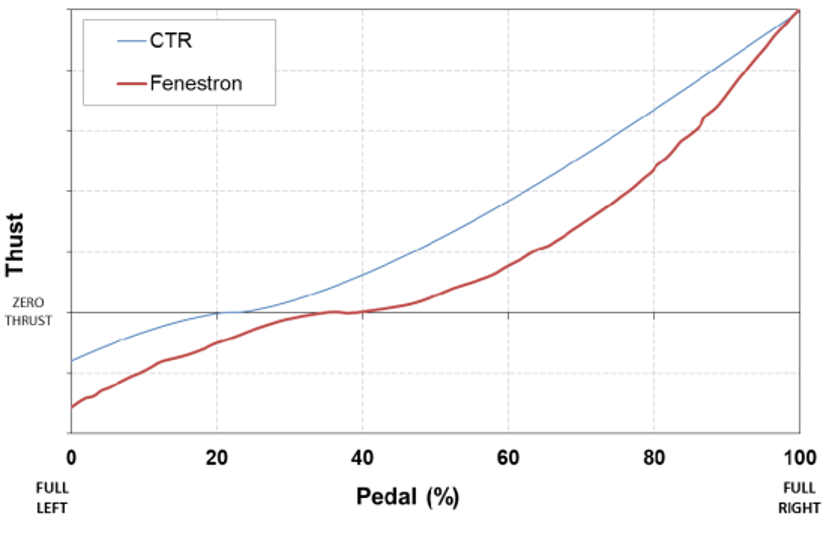
While both types of helicopters (Fenestron and CTR) may have the same methods of handling unanticipated yaw, the direction of rotation means that opposite pedal inputs are required and there are different requirements for the magnitude of pedal input and different expected performance (Airbus, 2020).
Figure 3: Direction of main rotor rotation for the EC120B showing corresponding torque reaction
Source: ATSB
Manufacturer’s guidance on unanticipated yaw
Unanticipated yaw at low speed has previously been the subject of Safety Information Notices (SIN) published by Airbus Helicopters. In 2005, Eurocopter (prior to becoming part of the Airbus group) released Service Letter 1673-67-04 (Reminder concerning the YAW axis control for all helicopters in some situations). The service letter reminded pilots that Fenestron tail rotors required significantly more pedal travel than conventional tail rotors when transitioning from forward flight to a hover.
Airbus Helicopters issued SIN 3297-S-00 Unanticipated left yaw (main rotor rotating clockwise), commonly referred to as LTE[7] in 2019.This notice outlined a detailed explanation of the phenomenon of unanticipated yaw due to insufficient pedal application. The full notice is provided in SIN 3297-S-00 and details of some related accidents are provided in Appendix A of ATSB report AO-2018-026.
The Airbus notice defined unanticipated yaw as an ‘uncommanded rapid yaw rate which does not subside of its own accord’. The notice also stated:
Unanticipated yaw is a flight characteristic to which all types of single rotor helicopter (regardless of anti-torque design) can be susceptible at low speed, often dependent on the direction and strength of the wind relative to the helicopter…
…Where this type of unanticipated yaw situation is encountered, it may be rapid and most often will be in the opposite direction of the rotation of the main rotor blades (i.e. left yaw where the blades rotate clockwise). Swift corrective action is needed in response otherwise loss of control and possible accident may result.
However, use of the rudder pedal in the first instance may not cause the yaw to immediately subside, thus causing the pilot to make inadequate use of the pedal to correct the situation because he suspects that it is ineffective when, in fact, thrust capability of the tail rotor available to him remains undiminished. "Loss of tail rotor effectiveness" is not, therefore, a most efficient description as it wrongly implies that tail rotor efficiency is reduced in certain conditions.
Related to SIN 3297-S-00 and superseding Service Letter 1673-67-04, Airbus issued SIN 3539-I-00 in 2020 (Fenestron versus Conventional Tail Rotor for helicopters equipped with a main rotor rotating clockwise when seen from above). This notice identified some specific characteristics of the Fenestron design, especially when transitioning from a helicopter equipped with a CTR. SIN 3529-I-00 showed graphically how the thrust varies with the pedal position on a Fenestron and on a CTR in hover conditions (Figure 4). The notice stated:
More negative thrust is required at 0% pedal position with a Fenestron to counterbalance the larger fin lateral lift in autorotation. The change of slope in the vicinity of zero thrust is more pronounced on the Fenestron curve than on the CTR curve. The CTR curve is more linear. The effect of a control input is almost constant in the whole pedal range, while it significantly varies for the Fenestron. The slope, and thus the perceived efficiency of the control, is much larger when coming close to full right pedal stop.
Figure 4: Comparison of Fenestron and conventional tail rotor in hover
Source: Airbus Helicopters
The pilot stated they were not aware of the information provided by Airbus, but were aware of the increased pedal input required to achieve tail rotor authority due to their previous flying experience on type.
Meteorological conditions
Meteorological conditions were not recorded at Porepunkah aerodrome, however during interview, the pilot and the passenger reported that no adverse weather conditions had been forecast or were observed. The pilot identified that there was very little wind directly before the incident as indicated by the windsock at the aerodrome. They estimated the wind to be very light as the pilot reported the windsock appeared to be wrapped around the flagpole.
General competency requirements
The Civil Aviation Safety Authority (CASA) recognises that skill decay occurs over time, and that checks are an ongoing measure and ensure that the licence competencies specified in the Civil Aviation Safety Regulation (CASR) Part 61 Manual of Standards continue to be met.
HFR is an opportunity for pilots to practise in-flight emergencies with an instructor and to demonstrate the required competence to safely operate a helicopter every 2 years. In discussing the aim of a flight review, CASA published Civil Aviation Advisory Publication (CAAP) 5.81-01 - Flight crew licensing flight reviews, which stated:
...With the passage of time and lack of practice some skills and knowledge can degrade. A flight review affords the opportunity to restore these degraded skills and gain new knowledge.
The flight review must be seen in the context of a broader aviation safety philosophy. The flight review, although important (and required by legislation), is one process that contributes to continuing pilot proficiency and consequently the safety of flight. A flight review every two years does not, in itself, ensure safety. Safety is achieved when each pilot takes responsibility for a continuing process of hazard identification and risk management for their own aviation activities.
CASR Part 61.385 Limitations on exercise of privileges of pilots licences – general competency requirement states:
- The holder of a pilot licence is authorised to exercise the privileges of the licence in an aircraft only if the holder is competent in operating the aircraft to the standards mentioned in the Part 61 Manual of Standards for the class or type to which the aircraft belongs…
CASA recommends that pilots should refresh their knowledge before commencing their next flight.
The guidance acknowledges that while a flight review can restore degraded skills it should be seen within the broader context of aviation safety. Regulations alone cannot guarantee safe outcomes and do not remove the need for pilots to monitor and maintain their own level of competency before flying.
Skill decay
Skill decay, sometimes termed as skill fade, is a recognised phenomenon in aviation particularly when pilots have not flown a specific aircraft type for some time. Arthur and others (1998) defined skill decay as ‘the loss or decay of trained or acquired skills (or knowledge) after periods of non-use’. Wang and others (2013) note several factors that influence skill decay such as retention interval, task type, conditions of retrieval, training methods, individual ability.
Skill decay is particularly salient in situations where individuals receive training on information and skills that they may not be required to use for extended periods of time. Previous research identified that there is a negative relation between skill retention and the length of non-use, starting from the day of training, with participants showing a 92 per cent reduction in performance when more than 365 days elapse between training and performing the skill again (Arthur and others 1998).
The pilot had logged nearly 12,000 hours on rotary aircraft but had not piloted an EC120B for over a decade.
Related occurrences
There have been a considerable number of accidents resulting from unanticipated yaw in helicopters at low height and low airspeed, both nationally and internationally. This is illustrated in the following cases drawn from other investigation reports.
Accident involving EC130 at Mansfield, Victoria, on 19 January 2019
The helicopter rolled on its side during take-off, resulting in substantial damage to the helicopter and minor injuries to the pilot. The ATSB report
On the morning of 19 January 2019, a Eurocopter EC130 helicopter, registered VH-YHS, conducted a private flight from Moorabbin Airport to an authorised landing area (ALA) near Mansfield, Victoria with the pilot and two passengers on board. A return flight to Moorabbin was planned for later that afternoon. At about 1500… the pilot and passengers boarded the helicopter at the ALA for the return flight. The pilot prepared for take-off and lifted off the helicopter more rapidly than he normally did. As the helicopter became airborne, it began to rotate counterclockwise (yaw to the left). The pilot tried to control the yaw but the helicopter quickly turned through 360° and, unable to control it, he made a decision to land the helicopter. The left skid of the descending helicopter subsequently contacted the ground, resulting in a rolling movement that led to the main rotor blades striking the ground… The investigation did not identify any airworthiness issues with the helicopter and it was considered that the loss of control was not attributable to a mechanical issue. It was also determined that the prevailing light winds did not contribute to the loss of control. The pilot reported that he did not lift the helicopter into a balanced hover and tried controlling its yaw mainly with the cyclic control instead of through the full application of opposing right, tail rotor pedal. Management of unanticipated yaw in helicopters with shrouded tail rotors (Fenestron) is the subject of the manufacturer’s guidance and learnings from similar accidents.
The pilot had 315 total flight hours, including 227 hours on the EC130.
Accident involving EC120B at Ballina, New South Wales, on 8 December 2013
The EC120B helicopter rolled onto its side during landing, resulting in substantial damage to the helicopter. The ATSB
On 8 December 2013, … [an EC120B] helicopter, registered VH-VMT, departed from a property 16 km north of the Ballina/Byron Gateway Airport, New South Wales for a local flight. On board the helicopter were the pilot and two passengers. At about 1555, the helicopter returned to the property from the north, overflew and approached to land on a heading of about 340º. The pilot reported that the wind was from the north, at about 20 kt. When about 3 ft above ground level, the pilot reported that he entered the hover with an airspeed of less than 10 kt and with full engine power selected. Immediately after, the helicopter began to yaw to the left. The pilot applied right anti-torque pedal to counteract the yaw and reduced the engine power to idle. The helicopter continued to yaw left and the pilot applied full right anti-torque pedal but was unable to arrest the rotation. The helicopter rotated left about 90° before the left skid lowered and contacted the ground. It continued to rotate and rolled onto its right side. The helicopter was substantially damaged and the pilot and passengers were able to evacuate uninjured…
The pilot had 550 total flight hours, including 280 hours on the EC120B. The pilot reported that they had recently been operating a Eurocopter AS350 helicopter, which required less anti-torque pedal input than the EC120B.
Accident involving EC130 at Deer Isle, United States, on 1 August 2009
The EC130 helicopter was substantially damaged during a forced landing. The NTSB report ERA09LA436 stated:
The helicopter departed a private yacht and was flying along an island shoreline at approximately 400 feet above mean sea level when the pilot entered an out-of-ground effect hover and initiated a left pedal turn. The helicopter started turning faster than commanded, and the pilot was unable to regain control. The helicopter subsequently lost altitude and impacted the water. Prior to impacting the water, the pilot deployed the emergency skid mounted floats to prevent sinking. According to the pilot, "the accident was totally pilot error with no mechanical malfunction." Examination of the wreckage confirmed no evidence of any mechanical malfunction or failure… The National Transportation Safety Board determines the probable cause(s) of this accident to be: The pilot's loss of directional control during an out-of-ground-effect hover.
The pilot had 680 total flight hours in rotorcraft, and 55 hours on the EC130.
Accident involving EC120B at Skogn Airport, Norway, on 25 May 2018
The EC120B helicopter rolled over during landing, resulting in substantial damage. The Accident Investigation Board Norway (AIBN) published an English summary, which stated:
The helicopter came out of control in connection with landing. It rotated uncontrolled before it ended up on the side, after the left skid had first hit the ground. There were two people on board. The commander was uninjured while the passenger suffered minor cuts. The helicopter was substantially damaged. Examinations of the helicopter have not revealed technical findings that can explain the loss of control. The Accident Investigation Board Norway finds it probable that the phenomenon of Loss of Tail rotor effectiveness (LTE) may have occurred after the commander failed to correct the helicopter using the right pedal. The AIBN believes that the commander's low experience level contributed to the situation, which was not interrupted in time.
Additional information from the full report (in Norwegian) included:
The pilot had 143 total flight hours and 8 flight hours on the EC120B (3 hours in command). The pilot’s other experience was on the Robinson R44.
The pilot reported applying full right pedal input to oppose the left yaw and then lifted the collective, which required additional power and increased the yaw to the left.
Safety analysis
On 15 May 2025, an Airbus EC120B helicopter was operated at Porepunkah aerodrome, Victoria, for planned private flight to Albury with the pilot and one passenger on board. During take-off into a hover the helicopter entered a left yaw. Attempts by the pilot to correct the yaw with the right pedal were ineffective and the helicopter entered an uncontrolled spin. The right skid struck the ground leading to a dynamic rollover. Both occupants evacuated without serious injury. The following analysis examines how a limited recency on type and skill decay contributed to the loss of control during take-off.
Skill decay
Aircraft type specific handling skills can deteriorate after periods of non-use (Childs and others, 1986; Wang and others, 2013). This effect has been shown in studies conducted during the COVID 19 pandemic which found that pilots underestimated skill decline after a period of extended absence (Mizzi and others, 2024). A similar underestimation is likely to have influenced the pilot’s expectation of yaw response in the EC120B.
In contrast to procedural skills for simple tasks, more complex tasks such as monitoring, detecting changes and predicting system behaviour typically take longer to acquire and may decay faster (Klostermann and others, 2022). The pilot reported completing a pre‑flight pedal check and was aware significant pedal input was required, however the pilot’s expectations of the aircraft yaw response were likely shaped by the handling characteristics of CTR aircraft, with lower anti-torque pedal demands.
In response to the yaw, the pilot attempted to gain height and reported increasing the collective. This action led to a corresponding rise in engine power. The increased power output and increased main rotor blade angle amplified the reaction torque and therefore the rotation in yaw to the left.
With more power to the main rotor, less was available to the tail rotor and therefore the effectiveness of the right pedal input was reduced, allowing the continued helicopter rotation that resulted in ground contact and dynamic rollover.
When the pilot increased the collective on the accident flight, it is almost certain that the range of pedal movement required to arrest the unanticipated yaw outpaced the pilot’s input.
Recency
Although the pilot had extensive helicopter flying experience and was licenced to operate the aircraft, the pilot had not flown an EC120B aircraft type for about 15 years. Having recency on the Robinson R44 helicopter, the yaw control characteristics of the EC120B were sufficiently different to produce effects in excess of the pilot’s expectations. The EC120B yawed to the left, rather than the right, on application of power and required a larger opposite pedal input to arrest the yaw. Being highly experienced in rotary wing operations, this likely increased the pilot’s perception of their ability to operate the helicopter type, even though they had not operated the aircraft type for several years.
It is likely that the lack of recency on the EC120B led to a degradation in the skill required to counter unanticipated yaw in an aircraft, where the pedal input required was much greater due to the Fenestron design.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Eurocopter EC120B, VH-JDZ, at Porepunkah aerodrome, Victoria, on 15 May 2025.
Contributing factors
The pilot did not anticipate the performance of the design difference of the EC120B. Almost immediately after lifting off, the pilot was unable to counter the helicopter’s left yaw resulting in ground contact and dynamic rollover.
Limited recent flying experience on this helicopter type degraded the pilot’s ability to manage the controls effectively. The pilot was unaware that this lack of currency had diminished their competence to safely operate the aircraft type.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the accident flight
passenger on board at time of accident
Civil Aviation Safety Authority
aircraft manufacturer
maintenance organisation for VH-JDZ
Bureau of Meteorology.
References
Airbus (2020). Fenestron versus Conventional Tail Rotor (CTR) for helicopters equipped with a main rotor rotating clockwise when seen from above. (Safety Information Notice 3539-I-00). Airbus S.A.S. Retrieved from Microsoft Word - 3539-I-00-Rev-0-EN.doc
Arthur Jr, W., Bennett, J. W., & Stanush, P. .. (1998). Factors that influence skill decay and retention: A Quantitative Review and Analysis. Human Performance, 11(1) 57-101.
Childs, J., & Spears, W. D. (1986). Flight-skill decay and recurrent training. Perceptual and motor skills, 62(1), 235-242.
Klostermann, M. C., Conein, S., Felkl, T., & Kluge, A. (2022). Factors influencing attenuating skill decay in high-risk industries: a scoping review. Safety, 8(2), 22.
Mizzi, A. L. Lohmann, G., & Carim Junior, G. (2024). The role of self-study in addressing competency decline among airline pilots during the COVID-19 pandemic. Human Factors, 66(3), 807-817.
Wang, X. D. (2013). Factors influencing knowledge and skill decay after training: A meta-analysis. In Individual and team skill decay. Individual and team skill decay , 68-116.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
the passenger
Bureau d'Enquêtes et d'Analyses pour la sécurité de l'aviation civile
Civil Aviation Safety Authority
Airbus.
Submissions were received from:
the pilot
the passenger
Bureau d'Enquêtes et d'Analyses pour la sécurité de l'aviation civile.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The EC120B Colibri was originally manufactured by Eurocopter in 1995. Eurocopter was purchased and became Airbus Helicopters in 2014. Airbus Helicopters ceased production of the EC120B in 2017.
[2]Yaw: the motion of an aircraft about its vertical or normal axis.
[3]Dynamic rollover: a helicopter is susceptible to a lateral rolling tendency. It begins when the helicopter starts to pivot laterally around its skid or wheel while in contact with the ground. Once the critical angle, typically around 5–8° is exceeded, the helicopter rolls over, often too quickly for any corrective pilot action.
[4]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[5]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[6]Stators are the ‘blades’ that you can see inside the Fenestron duct that never move and are designed to direct airflow.