
Grounding of Sea Pelican in Port Adelaide, South Australia, on 10 June 2025
Summary
The ATSB is investigating the grounding of the tug Sea Pelican in Port Adelaide, South Australia, on 10 June 2025.
On the morning of 10 June the 23.5 m tug Sea Pelican was pushing the 55 m barge Rocksea from its base of operations to a worksite further upriver in the port (berth 25).
The tug was hipped-up to the starboard quarter of the barge. On departing the base, the tug and barge combination was to transit the North Arm of the Port Adelaide River, before being manoeuvred through the hard port turn into the river. As the turn was being negotiated the tug and barge combination went wide in the turn and the tug touched bottom on a sandbank on the northern side of the channel. The tug came clear of the bottom and the transit continued to its destination.
While en route to the worksite, a bilge alarm sounded on the tug. Water ingress into the engine room was found. Operations were stopped while the engine room bilges were lowered and a temporary repair made to a hole in the hull.
The tug returned to base (the barge remained at the worksite) and plans for repairs were made. The tug was subsequently slipped and a permanent repair made to the hull.
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be published at the conclusion of the investigation. Should a critical safety issue be identified at any time during the investigation, the ATSB will immediately notify the operators of the ship and the port, and other relevant parties so that appropriate and timely safety action can be taken.
Last updated:
Occurrence summary
| Investigation number | MO-2025-005 |
|---|---|
| Occurrence date | 10/06/2025 |
| Occurrence time and timezone | 09:45 Australian Central Standard Time |
| Location | Port Adelaide |
| State | South Australia |
| Report status | Pending |
| Anticipated completion | Q3 2026 |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: External review |
| Investigation status | Active |
| Mode of transport | Marine |
| Marine occurrence category | Grounding |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Ship details
| Name | Sea Pelican |
|---|---|
| IMO number | 8950873; Official number 858366 |
| Ship type | Tug |
| Flag | Australia |
| Owner | MC Levitate Pty Ltd |
| Manager | Maritime Constructions |
| Destination | Berth 25, Port Adelaide, South Australia |
| Injuries | None |
| Damage | Substantial |
ATSB acknowledges ADS-B pioneer's induction into Aviation Hall of Fame

The ATSB congratulates the latest Australian aviation pioneers to be inducted into the Australian Aviation Hall of Fame, including ‘father of ADS-B in Australia’ Greg Dunstone.
Mr Dunstone will be one of four individuals inducted into the Hall of Fame(Opens in a new tab/window) at a gala dinner on 14 March 2026, as well as Bill Bristow, founder of Angel Flight Australia; pioneering pilot and holder of Australia’s first pilot certificate, William ‘Billy’ Hart; and Sir Ivan Holyman, founder and managing director of Australian National Airways. The dinner will also recognise the Regional Aviation Association of Australia through the bestowal of the Southern Cross Award.
Greg Dunstone’s induction is particularly noteworthy for the ATSB, given his pioneering work with the development and implementation of Automatic Dependent Surveillance Broadcast (ADS-B) technology. ADS-B is not only used by Airservices Australia for air traffic management of aircraft operating under instrument flight rules, but it can also provide pilots with enhanced situational awareness of other aircraft as an aid to self-separation in non-controlled airspace.
“Greg played a pivotal role in transforming the nation's air traffic management system through his leadership in radar and surveillance technologies during his 46-year career with Airservices Australia,” ATSB A/g Chief Commissioner Colin McNamara said.
“The work by Greg, and many others, on developing and introducing ADS-B technology has added additional levels of aviation safety, and we commend the Australian Aviation Hall of Fame for its recognition of him.”
All aircraft operating in Australia under instrument flight rules must be fitted with approved ADS-B OUT equipment to broadcast the precise location of the aircraft up to twice per second.
In addition, the Australian Government is currently incentivising the voluntary uptake of ADS-B installations in Australian-registered aircraft by providing a 50 per cent rebate on the purchase cost of eligible devices, and where applicable, the installation – capped to $5,000.
The rebate, covering Australian-registered aircraft operating under both visual and instrument flight rules, funds two classes of eligible ADS-B equipment: installed ADS-B equipment that air traffic controllers can use for aircraft separation purposes; and portable ADS-B equipment for local electronic traffic information purposes (ADS-B electronic conspicuity).
“The ATSB encourages the fitment of ADS-B in all general and recreational aircraft in Australia due to its proven abilities to enhance aviation safety and assisting in life-saving search and rescue operations undertaken by AMSA,” Mr McNamara said.
The rebate offer ends on 31 May 2027, but applications may close early if funding is fully allocated before the closing date.
More information, including on how to apply for the rebate, is available here(Opens in a new tab/window).
Engine failure and forced landing involving Robinson R44, VH-OOE, 13 km south of Tindal Airport, Northern Territory, on 11 June 2025
Final report
Report release date: 30/03/2026
Investigation summary
What happened
On 11 June 2025, a Robinson R44 Raven I helicopter, registered VH-OOE, was being operated on a personal transport flight from Daly Waters Aerodrome to Wally’s Airstrip, Northern Territory, with a pilot and one passenger on board. As the helicopter neared the destination, the pilot felt the onset of severe airframe vibration. The pilot elected to conduct a precautionary landing in an area of open farmland, resulting in a hard landing. The pilot and passenger were uninjured, and the helicopter sustained minor damage.
What the ATSB found
The helicopter’s engine was found to have suffered a mechanical failure due to in-service loosening of the nuts on the connecting rod bolts, leading to separation of one of the connecting rods from the crankshaft. The reason the nuts became loose was not determined.
While there was no indication of influence on this occurrence, independent inspection of the connecting rod attaching hardware performed during the overhaul of the engine did not involve a physical torque check of the connecting rod bolts. While the inspection was not a regulatory requirement, this was a missed opportunity to verify the installation torque.
During the most recent periodic inspection the helicopter maintenance provider did not refit the spark plugs using new gaskets, as required by the spark plug manufacturer. It was also found that the Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent in this respect.
What has been done as a result
The Civil Aviation Safety Authority acknowledged the inconsistent information contained within the 2 airworthiness bulletins. CASA advised that Airworthiness Bulletin AWB 20‑001 is scheduled for cancellation and Airworthiness Bulletin AWB 85-023 is to be amended to reflect current recommendations.
The helicopter maintenance provider advised the ATSB it now installs new gaskets when refitting spark plugs.
Safety message
This incident highlights the importance of managing inflight anomalies through a comprehensive understanding of aircraft systems and the application of emergency procedures. The pilot’s timely actions following the onset of the vibrations ensured a safe outcome for the occupants and resulted in minimal damage to the helicopter.
The incident also emphasises the importance of adhering to manufacturer requirements when installing aircraft components, as well as the additional assurance provided by a thorough independent inspection of completed work.
The investigation
The occurrence
On 11 June 2025, a Robinson R44 Raven I helicopter, registered VH-OOE, was being operated on a personal transport flight with a pilot and one passenger on board. The flight was conducted under the visual flight rules,[1] and the planned route was from Daly Waters Aerodrome to Wally’s Airstrip, Northern Territory (NT) (Figure 1).
On the morning of the flight, the pilot completed their pre-flight inspection and refuelled the helicopter. Shortly after starting the engine, the pilot recalled sensing an unusual sound and vibration through the helicopter, but it resolved when the engine speed was increased. The pilot completed their pre-take-off checks, and the helicopter departed Daly Waters Aerodrome at about 0900 local time. The pilot did not recount any issues with the helicopter’s performance during the take-off, climb or initial cruise.
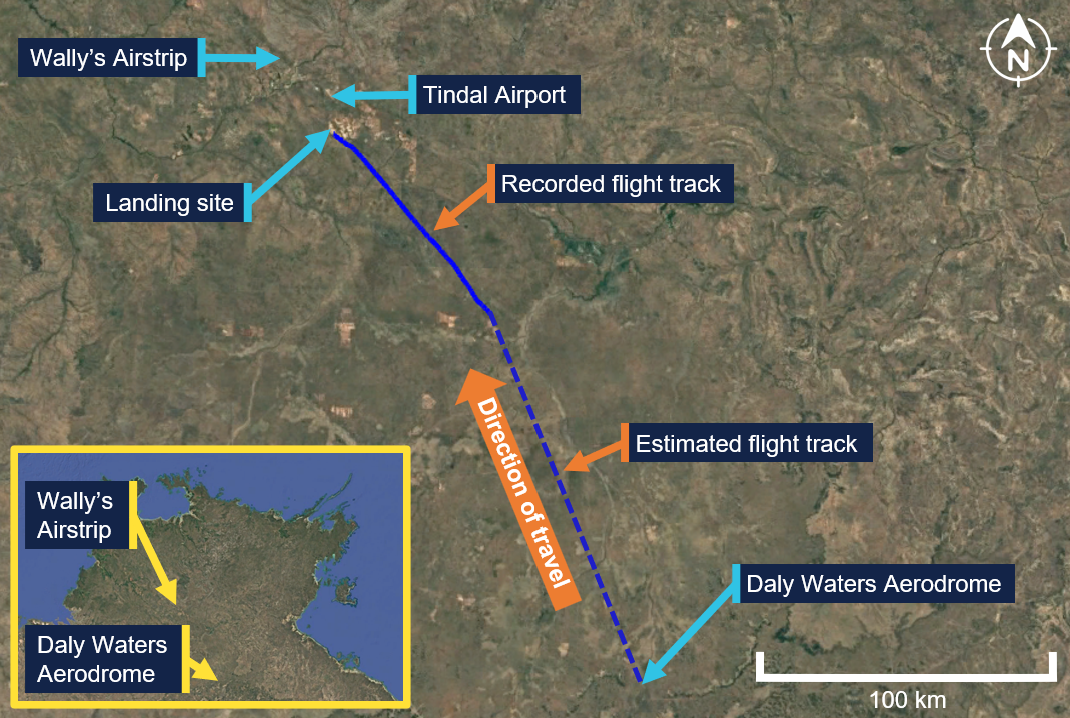
Source: Google Earth, annotated by the ATSB
At about 1015, when the helicopter was about 46 km to the south‑east of Wally’s Airstrip, the pilot contacted Tindal Airport air traffic control (ATC). Several exchanges with Tindal Airport ATC took place, during which the pilot was instructed to follow a railway line and maintain an altitude not above 1,500 ft above mean sea level. The pilot complied with these instructions and continued towards their destination. At about 1020, when the helicopter was at an altitude of about 1,100 ft, the pilot felt the onset of severe airframe vibration. They recalled initially thinking the helicopter tail may had been struck but later discounted that possibility when they identified they still had directional control. The pilot was unable to diagnose the cause of the vibration and decided to undertake a precautionary landing.
At 1020:42, and an altitude of about 1,100 ft, the pilot alerted Tindal Airport ATC that they had a ‘problem’ (Figure 2). The pilot selected a paddock for the landing that had recently been harvested of its crop and commenced a right turn towards the landing location at 1020:49. At 1020:52, they communicated that operations were not normal, and at 1021:00 they advised Tindal Airport ATC that they would be landing immediately. The pilot recalled noting the engine gauges and the rotor and engine speed indications at that time were normal.
Figure 2: VH-OOE flight path from the onset of vibrations until landing
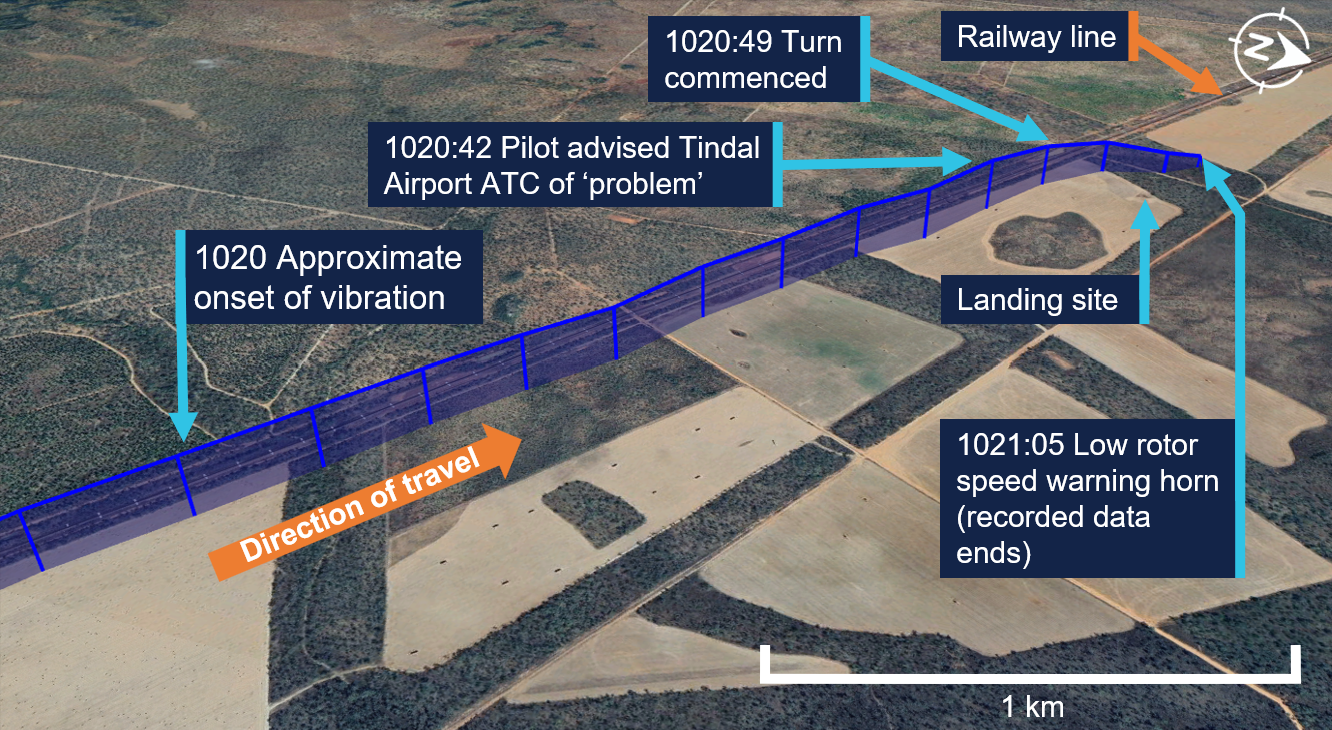
Source: Google Earth, annotated by the ATSB
At 1021:05, and an altitude of 700 ft, the pilot made a transmission to Tindal Airport ATC during which a low speed warning horn could be heard in the background (see Low rotor speed). The pilot did not recall hearing the horn. At about 150 ft above ground level, the pilot recalled noting a low oil pressure light on the helicopter’s caution warning panel (see Oil warning caution light). They continued the approach and, as the helicopter slowed for landing, they observed smoke blowing forward from the rear and recalled having concerns about a fire.
The helicopter landed heavily in the paddock. The pilot recalled that the landing was probably completed ‘quicker’ and with a lower tail position than normal, due to their concerns about a fire. Once the helicopter had landed, the pilot instructed the passenger to exit and run forward. They then shut down the helicopter’s engine, and at 1021:41 advised Tindal Airport ATC that they had landed and were safe. The pilot then exited the helicopter. Both occupants were uninjured, and the helicopter sustained minor damage.
Context
Pilot information
The pilot held a valid Commercial Pilot Licence (Helicopter) with single engine and low‑level ratings. The licence was issued on 6 June 2025 following the successful completion of a commercial pilot licence flight test in May 2025. The pilot had held a Private Pilot Licence (Helicopter) since October 2023. They also held a current class 1 aviation medical certificate valid to 6 August 2025. At the time of the incident, they had a total flying time of 194 hours of which 118 hours were on the Robinson R44.
Helicopter information
General information
The Robinson R44 Raven I is a 4-place helicopter with a 2-bladed main rotor system and a conventional 2-bladed tail rotor. VH-OOE was manufactured in the United States in 2008 and first registered in Australia in July 2008. At the time of the incident, the helicopter had accumulated 1,995 hours total time in service.
It was powered by a Lycoming O-540-F1B5, 6-cylinder, horizontally opposed piston engine that is naturally aspirated and rated at 235 horsepower. The overhauled engine was installed in September 2022 and had operated for 291 hours at the time of the incident, with a total time of about 1,614.6 hours. The last periodic inspection was undertaken on 6 May 2025, and the helicopter had flown about 25 hours since that inspection.
Airworthiness and maintenance history
Recent maintenance
The last periodic inspection was undertaken by Platinum Helicopters on 6 May 2025. During the inspection, the Champion REM38E spark plugs fitted to the engine were removed, inspected and then refitted by the maintenance engineer. The maintenance engineer recalled that it was not their practice to fit new spark plug washers (gaskets) when refitting the spark plugs, instead electing to use annealed[2] gaskets (see Spark plug maintenance).
Engine overhaul
In September 2022, VH-OOE underwent a 12 year/2,200 hour inspection. During the inspection, the engine was removed and an overhauled engine was fitted to the helicopter. This engine had been salvaged from a Robinson R44, and was overhauled by South West Aviation, a CASA‑approved maintenance organisation.
During the overhaul of the engine, additional components were used to replace some aspects, including:
- 6 new cylinder kits
- new connecting rod hardware (bolts and nuts) with parts manufacturer approval[3]
- a crankshaft that had been salvaged from a different Robinson R44.
Records show all salvaged components were inspected and tested to assess serviceability prior to fitment. Once the engine overhaul had been completed, it underwent ground runs and checks prior to being installed in VH-OOE.
Records show that independent inspections were undertaken during the engine overhaul of the engine fitted to VH-OEE. The purpose of an independent inspection is to verify that a maintenance task has been completed correctly. The inspection is undertaken by an appropriately authorised person who did not undertake the original activity. While there was no regulatory requirement for the independent inspection of maintenance work carried out on engine systems, South West Aviation had included these inspections as part of the organisation’s worksheets for engine overhaul.
The worksheets for the engine overhaul stated that an independent inspection of the engine sub-assembly was completed during the engine rebuild. Figure 3 shows the sub‑assembly of the crankshaft and the connecting rods, which were secured to the crankshaft by 2 connecting rod bolts and nuts. The crankshaft has 2 dynamic counterweight assemblies fitted, which assist in removing torsional vibration during engine operation.
Figure 3: O-540 crankshaft and connecting rod sub-assembly
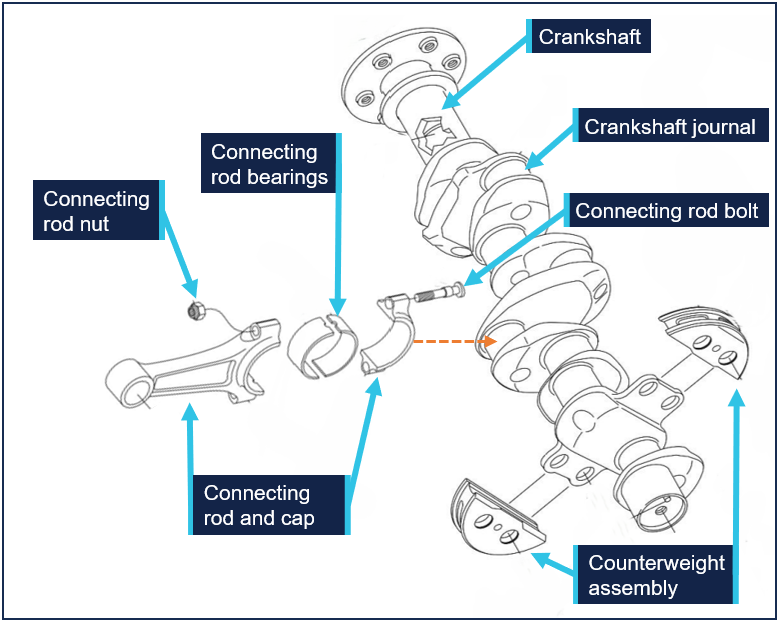
Source: Lycoming O-540-F1B5 Illustrated Parts Catalogue, annotated by the ATSB
During interview, when asked about a torque check of the connecting rod nuts, the engineer who conducted the independent inspection stated they would check the torque was set correctly on the tooling that had been used, but it was not their normal procedure to physically check the torque on each nut. South West Aviation did not have a documented procedure that detailed how the independent inspection of the connecting rod hardware should be conducted.
Helicopter systems and procedures
Vibration
The Robinson R44 pilot operating handbook (POH) contained advice for the management of vibration, and stated:
A change in the sound or vibration of the helicopter may indicate an impending failure of a critical component. If unusual sound or vibration begins in flight, make a safe landing and have the aircraft thoroughly inspected before flight is resumed.
Low rotor speed
The helicopter was fitted with a low rotor speed horn. The activation of the horn indicated that rotor speed may be below safe limits (97%). Power available from the engine is directly proportional to rotor speed. With less power the helicopter will start to sink. If the collective is raised to stop it from descending, the rotor speed will reduce even further causing the helicopter to sink faster. To restore rotor speed, the Robinson R44 POH stated that a pilot should lower the collective, roll throttle on and, in forward flight, apply aft cyclic.
Oil warning caution light
The helicopter was fitted with an oil warning caution light. The illumination of the light indicated a loss of engine power or oil pressure. The Robinson R44 POH stated the actions to take in response should be to check the engine tachometer for power loss and the oil pressure gauge. If oil pressure loss was confirmed, the POH stated the pilot should land immediately. Continued operation without oil pressure causes serious engine damage and engine failure can occur.
Spark plug maintenance
The Champion Aviation Service Manual,[4] which included recommended service, handling and reconditioning practices for Champion spark plugs stated:
Always install both new and reconditioned Champion aviation spark plugs with a new copper gasket.
Additionally, Champion Aviation Technical Bulletin 95-11[5] stated:
Gaskets that have become too hard with normal usage won’t “hold torque” correctly, and spark plugs can come loose with disastrous results. An annealed gasket will not meet new specifications.
The maintenance engineer stated they carried out the periodic inspection in accordance with the Lycoming O-540 Operator’s Manual.[6] However, this manual, which covered both the O-540 and IO-540 engines, contained no information regarding spark plug gasket fitment. The guidelines for the installation of spark plugs were contained in Lycoming service instruction 1042 Approved Spark Plugs, which stated:
Always install a spark plug with a new gasket.
The Civil Aviation Safety Authority (CASA) had produced 2 advisory airworthiness bulletins (AWBs) that included information on spark plug fitment. However, the advice within these 2 documents was not consistent.
AWB 20-001 Spark Plug Care, issued in September 2001, stated:
Most modern spark plugs have a solid copper gasket that requires annealing prior to spark plug installation to ensure a tight, gas sealed fit. The maintainer should check that the spark plug has only one washer, is of correct dimensions and is annealed. If the engine is equipped with a thermocouple probe in the form of a spark plug gasket, a normal gasket is not required.
Whereas AWB 85-023 Piston Engine Spark Plug Cracking, issued in June 2021, stated:
Always install a new spark plug gasket when servicing spark plugs or installing new spark plugs. Failure to install a new spark plug gasket may result in incomplete sealing of the combustion chamber, loss of heat transfer with spark plug overheating leading to possible pre-ignition.
Meteorological information
The weather at the time of the incident, recorded at Tindal Airport around 13 km to the north of the landing site, captured a wind of between 9–13 kt from the east, clear skies and a temperature of 23°C.
Recorded information
The helicopter was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to be. During the incident flight, data was being transmitted by the helicopter’s transponder. This data, recorded by ground-based receivers, captured the aircraft’s position, altitude, and groundspeed during the final 25 minutes of the flight. All radio communications made and received by Tindal Airport ATC throughout the flight were recorded.
Helicopter damage
The ATSB did not attend the landing site. A post-incident inspection of the helicopter was completed by a maintenance organisation located at Wally’s Airstrip, NT. This inspection identified:
- damage to the engine with scattered material within the cowling
- damaged and displaced drive belts
- impact damage to the engine oil cooler caused by engine material
- engine oil on external areas of the engine and airframe
- the skid landing gear was spread outwards (Figure 4).
The engine and a selection of components were removed for a detailed examination by the ATSB.
Figure 4: VH-OOE shortly after landing showing oil leak and smoke haze

Source: Supplied, annotated by the ATSB
Engine examination
The engine was disassembled and examined at a CASA‑approved engine overhaul facility under the supervision of the ATSB. The examination found that the number 4 connecting rod had separated from the crankshaft journal, resulting in mechanical damage to the internal engine components and fracture of the adjacent crankcase. Both connecting rod bolts had been fractured, with one connecting rod nut missing and the other unwound (see Component examination). There were also witness marks from impact between the number 4 piston crown and cylinder head.
Prior to removal of the remaining connecting rods, the nuts were checked for torque. The check found that the number 3 cylinder connecting rod nuts were at 20 ft/lb, while numbers 1, 2, 5 and 6 connecting rod nuts were at the correct torque of 40 ft/lb.
The number 4 cylinder spark plugs were found loosened, but the spark plug leads were attached tightly. Subsequent testing of the spark plugs found both were serviceable. Figure 5 depicts the engine prior to disassembly.
Figure 5: Engine assembly showing damage
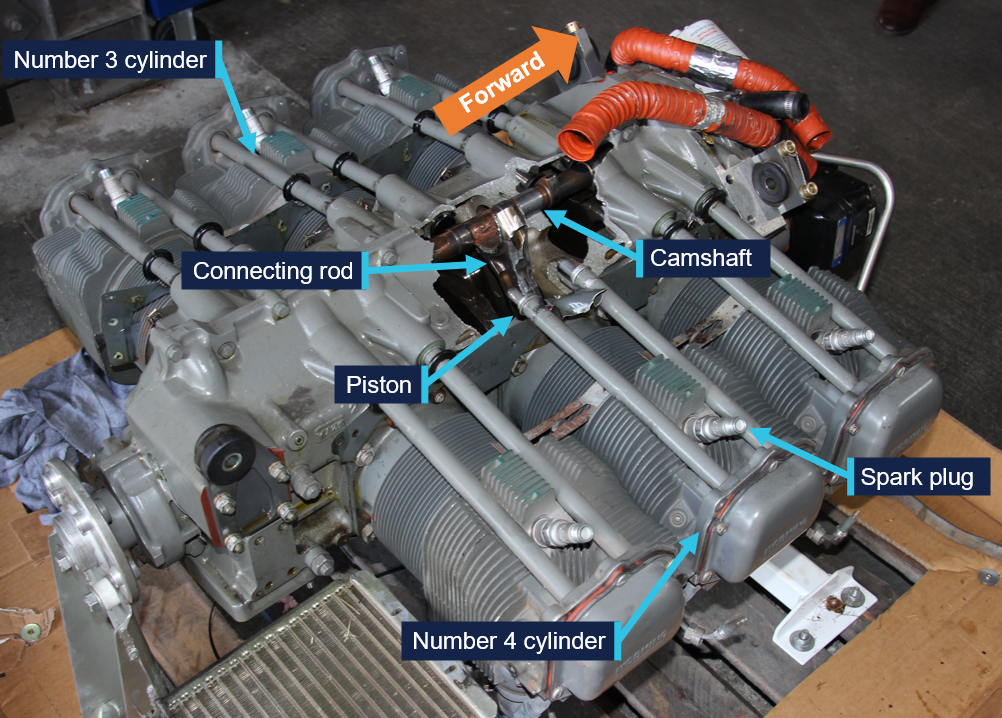
Source: ATSB
Component examination
Several components were retained from the engine disassembly and were examined at the ATSB’s technical facilities in Canberra, Australian Capital Territory.
Extensive deformation and fracture of the number 4 connecting rod (Figure 6) and deformation of the crankshaft journal, was consistent with initial separation of the connecting rod, followed by repeated impacts to the connecting rod by the still-rotating crankshaft.
Figure 6: Number 4 cylinder connecting rod and piston
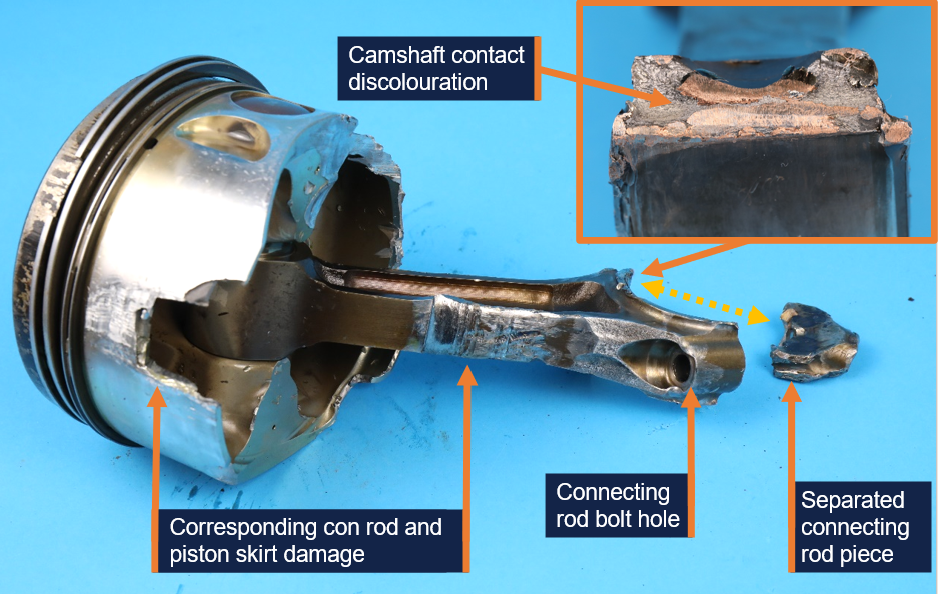
Source: ATSB
This resulted in significant damage to the adjacent cylinder wall, piston skirt, camshaft and the hole in the crankcase. The fractured connecting rod showed no evidence of fatigue cracking or other defect.
The number 4 connecting rod bearings were deformed due to contact with the moving internal engine components but were found to be the correct parts and did not exhibit any abnormal signs of wear. Bearings from some of the other connecting rods displayed minor surface wear, which was attributed to low engine oil volume during the final part of the flight.
There were visibly fewer combustion deposits on the number 4 piston crown, compared to the remaining pistons. However, a considerable amount of sand-like contamination was recovered from the number 4 cylinder during engine disassembly, which was found to be chemically similar to the piston deposits. There was no evidence of destructive combustion issues such as pre-ignition or significant detonation.
The connecting rod was secured to the crankshaft by 2 connecting rod bolts (Figure 3). Both number 4 cylinder connecting rod bolts were fractured in approximately the same location (Figure 7). The fracture surface features of both bolts and deformation of the adjacent shank were consistent with overstress failures.
Figure 7: Cylinder number 4 connecting rod bolts
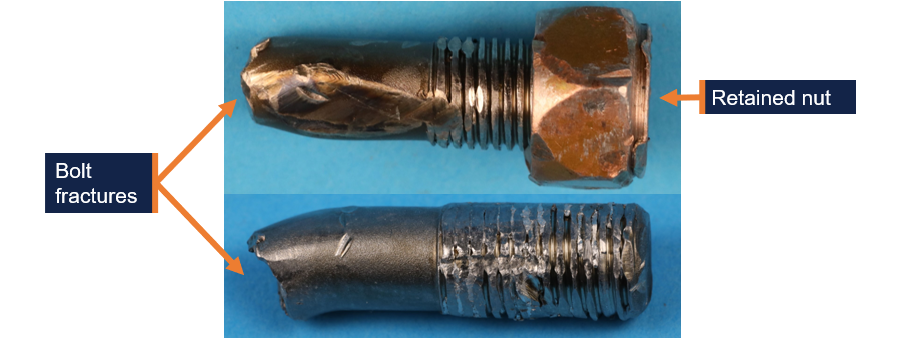
Source: ATSB
One of the cylinder 4 connecting rod bolts had no nut and heavily damaged threads. The nut was not located. The other connecting rod bolt had a partially unwound nut retained on the threads (Figure 8).[7] The exposed threads were damaged. The nut could not be further unwound by hand, likely due to impact damage. The bolts and nut material was in accordance with their specification. The extent of deformation precluded a detailed inspection of the threads; however, the threads were not stripped and the remnants of a compound consistent with thread lubricant was identified.
Figure 8: Number 4 cylinder connecting rod bolt showing position of retained nut
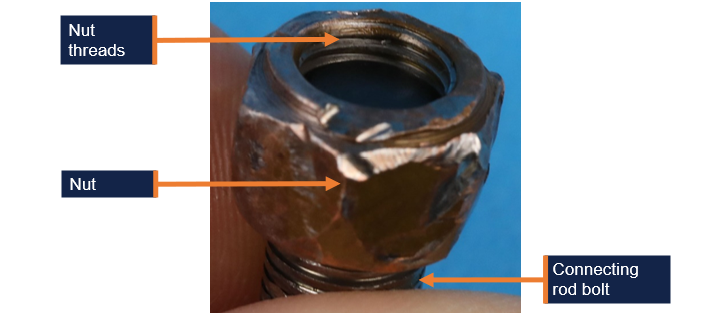
Source: ATSB
The examination also identified evidence of abnormal fretting[8] wear in the number 4 cylinder connecting rod bolt holes. A comparison between the number 4 cylinder and number 6 cylinder connecting rod bolt holes is depicted in Figure 9.
Figure 9: Number 4 cylinder connecting rod end cap bolt hole fretting wear and exemplar
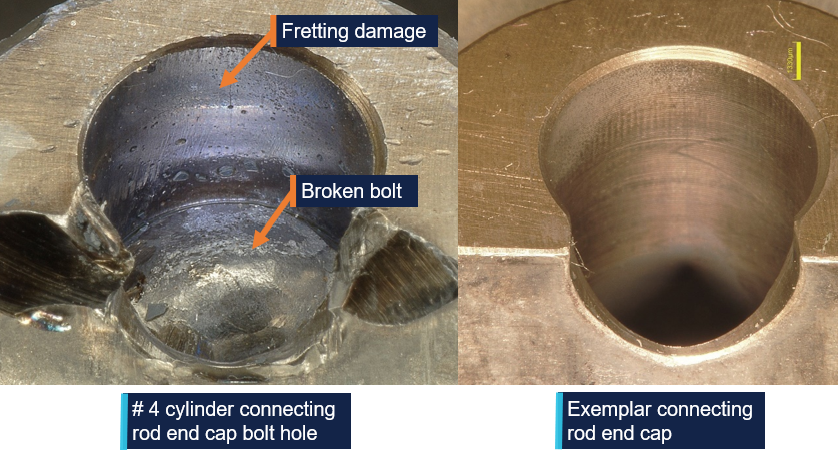
Source: ATSB
The abnormal fretting wear indicated relative movement (micro-slip) between the bolted surfaces during operation, which would occur if the bolt tension was insufficient to restrain movement under normal operational loads. The missing nut from one of the bolts, and the other nut retained in an improper position on the fractured bolt, was also an indicator that the nuts had loosened in-service.
Possible mechanisms that could result in the in-service loosening of the nuts included:
- Abnormal loading or vibration from engine overspeed or abnormal combustion that could lead to bolt stretch and nut loosening.
- Variations in thread condition or installing the threads dry versus lubricated could produce a lower bolt stress than desired.
- Unintended deformation due to improper or defective parts leading to reduced bolt stress over time.
- Microscopic surface deformation and fretting at contact interfaces could reduce clamping force by a small margin over time, which could then make the nut susceptible to further loosening during service.
- Inadequate torque applied to the nuts during installation that could lead to relative movement between the clamped surfaces and nut loosening during normal operation.
Related occurrences
In 2007, the ATSB published a research and analysis report (B20070191) into aircraft reciprocating (piston) engine failures. The report examined 20 high-power[9] piston engine structural failure occurrences in Australia, between 2000 and 2005. The report focused on failures of the combustion chamber, connecting rods and crankshaft assemblies. It included several engine failure investigations, including investigation 200105866 (below).
ATSB investigation 200105866
On 14 December 2001, a Piper PA31-350 aircraft, registered VH-JCH, was in cruise flight at 8,000 ft when the flight crew noticed that the propellers went out of synchronisation. Adjustments were made to correct the problem but were unsuccessful. Following right engine speed fluctuations, the crew shut the engine down, feathered the propeller and conducted a single‑engine landing.
During the subsequent disassembly of the engine, the crankshaft was noted to have fractured at the number 6 connecting rod journal, and the number 6 connecting rod big end had separated from the crankshaft and impacted the camshaft. The separation of the number 6 big end permitted the piston to strike the top of the combustion chamber with sufficient force to deform the top of the piston.
The number 6 connecting rod disconnection from the crankshaft was due to the loosening of the nuts on the connecting rod bolts, and eventual loss of one nut. Evidence of nut loosening, leading to fretting wear damage, was observed on the bolt threads and the connecting rod cap bolt hole locations. The reason for the loosening of the number 6 connecting rod nuts could not be determined.
The damage of these components was almost identical to the damage noted in the engine from VH-OOE.
Safety analysis
The ATSB examination of the engine components determined that the engine failure resulted from mechanical damage caused by the separation of the number 4 cylinder connecting rod from the crankshaft.
The initiating factor of the separation was almost certainly the in-service loosening of the connecting rod nuts of the number 4 cylinder. This was evidenced by the fretting wear in the connecting rod bolt holes, which was illustrative of engine operation after a loss of bolt tension, allowing relative movement between the bolts and holes. The absence of one of the associated nuts, and the opposite one mostly unwound was also evidence of the nuts loosening prior to the engine failure. There was also an absence of fatigue cracking of the number 4 bolts or connecting rod that might otherwise account for the component fractures and separation of the connecting rod.
Of the possible mechanisms identified that could have led to the connecting rod nuts loosening:
- Abnormal loading or vibration: there was no evidence of engine overspeed, or of piston melting or structural damage consistent with severe abnormal combustion. There was no evidence that the spark plugs, found loose during the disassembly, had any negative impact on the engine performance.
- Variation in thread condition and lubrication: this could not be fully assessed due to thread damage and the absence of one of the nuts.
- Improper or defective parts: the connecting rod bolts and nut material was correct; however, a full assessment of their original condition was not possible.
- Embedding (microscopic deformation): it is possible that the initial bolt tension reduced by a small margin due to microscopic deformation of the clamping or thread surfaces, which would then make the nut more susceptible to further loosening during service.
- Inadequate installation torque: like the above, it was possible that the nuts were slightly under-torqued during installation and progressively loosened during the subsequent 291 hours of operation. The number 3 connecting rod nuts being found at the incorrect torque value during the engine disassembly further supports this scenario.
Given most of the possibilities above could not be definitively ruled out, the reason for the nuts loosening was ultimately not determined.
Despite this, it was identified that during the overhaul of the engine fitted to VH-OOE, the independent inspection of the engine sub-assembly did not involve a torque check of the connecting rod nuts. While there was no evidence of influence on this occurrence and while the inspection was not a regulatory requirement, the ATSB considered it a missed opportunity to positively verify the installation torque.
Additionally, during the engine examination, both spark plugs in the number 4 cylinder were found to be loose. The reason for the loose spark plugs was not determined and, as above, there was no evidence identified to indicate influence on the engine failure. However, it was identified that during the most recent periodic inspection, the helicopter maintenance provider did not refit the spark plugs using new gaskets as required by the engine and spark plug manufacturer.
On the same subject, the Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent. Airworthiness Bulletin AWB 20-001 stated that annealed gaskets could be used, whereas Airworthiness Bulletin AWB 85-023 stated new gaskets must be used in all circumstances.
The unusual sound and vibration noted by the pilot during engine start was possibly a precursor to the eventual failure inflight, however the vibration disappeared when engine speed was increased. In response to the onset of severe vibration inflight, the pilot assessed the controllability of the helicopter and noted there were no abnormal engine indications at that time. In accordance with the Robinson R44 POH, the pilot conducted a precautionary landing in a suitable location. They also communicated the issue to Tindal Airport ATC, which increased the likelihood of a timely emergency response had one been necessary.
During the late stages of the approach, the low rotor speed warning horn and low oil pressure caution light activated. Both indicated a reduction in power, almost certainly due to the mechanical failure, resulting in less power than normal to arrest the rate of descent in the final stages of landing. This, in combination with the pilot’s concern about a possible fire and recollection of landing ‘quicker’ than normal, likely resulted in the helicopter landing heavily which spread the landing gear skids.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the engine failure and forced landing involving Robinson R44, VH-OOE, 13 km south of Tindal Airport, Northern Territory, on 11 June 2025.
Contributing factors
- In-service loosening of the connecting rod nuts resulted in the eventual separation of the connecting rod from the crankshaft and the mechanical failure of the engine. The reason for the nuts loosening was not determined.
- During the engine overhaul, the torque on the connecting rod nuts was not physically checked as part of the independent inspection of the engine assembly. This was a missed opportunity to verify that the installation of the connecting rod nuts had been completed correctly.
Other findings that increased risk
- During the most recent periodic inspection, the helicopter maintenance provider did not refit the spark plugs using new gaskets as required by the spark plug manufacturer. This increased the risk of loosened spark plugs, insufficient heat transfer and pre-ignition.
- The Civil Aviation Safety Authority guidance on spark plug gasket fitment was inconsistent. Airworthiness Bulletin AWB 20-001 stated that annealed gaskets could be used, whereas Airworthiness Bulletin AWB 85-023 stated new gaskets must be used in all circumstances. The inconsistency in this guidance could have led to incorrect procedures being performed which were not in accordance with spark plug maintenance requirements.
Safety actions
Safety action by Civil Aviation Safety Authority
The Civil Aviation Safety Authority acknowledged the inconsistency between Airworthiness Bulletin AWB 20-001 (that stated that annealed gaskets could be used) and Airworthiness Bulletin AWB 85-023 (that stated new gaskets must be used in all circumstances) and advised the ATSB that AWB 20-001 will be cancelled and AWB 85‑023 will be amended to reflect current recommendations.
Safety action by Platinum Helicopters
Platinum Helicopters advised the ATSB that new spark plug gaskets are now fitted each time spark plugs are reinstalled.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot of VH-OOE
- the engine overhaul organisation
- the maintenance provider for VH-OOE
- Civil Aviation Safety Authority
- the aircraft manufacturer
- the engine manufacturer
- the PMA parts manufacturer
- Airservices Australia
- the Bureau of Meteorology.
References
Australian Government (1988), Civil Aviation Regulations 1988 (Commonwealth), reg 42G. AustLII. https://classic.austlii.edu.au/au/legis/cth/consol_reg/car1988263/s42g.html
Australian Government (2021), Aircraft Reciprocating-Engine Failure: An Analysis of Failure in a Complex Engineered System, Australian Transport Safety Bureau, Canberra, ACT. /publications/2007/b20070191
Civil Aviation Safety Authority (2025). Airworthiness Bulletin 20-001. Retrieved from https://www.casa.gov.au/aircraft/airworthiness/airworthiness-bulletins/spark-plug-care
Civil Aviation Safety Authority (2025). Airworthiness Bulletin 85-023. Retrieved from https://www.casa.gov.au/aircraft/airworthiness/airworthiness-bulletins/piston-engine-spark-plug-insulator-cracking
Lycoming Engines Operator’s Manual 4th edition 2006, O-540, IO-540 Series
Lycoming Engines Overhaul Manual, Direct drive engines 1974
Lycoming Engines Parts Catalogue 2009, O-540-F1B5
Robinson Helicopter Company 2024, R44 Pilot’s Operating Handbook, section 10, p.10-2
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the pilot of VH-OOE
- Civil Aviation Safety Authority
- the maintenance provider
- the engine overhaul organisation
- Textron Lycoming
- Robinson Helicopters
- National Transportation Safety Board (NTSB).
Submissions were received from:
- the pilot of VH-OOE
- the maintenance provider
- the engine overhaul organisation
- Textron Lycoming
- Robinson Helicopters.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] Annealing: the process of heating a metal to a cherry red colour and them immersing into water to soften the material.
[3] A parts manufacturer approval (PMA) is a combined design and production approval for modification and replacement articles. It allows a manufacturer to produce and sell these articles for installation on type certificated products.
[4] Champion Service Manual AV6-R, revised August 2014.
[5] Champion Aviation Technical Bulletin 95-11, Aviation Spark Plugs – New and Reconditioned Should Always be Installed with a New Gasket, published November 1995.
[6] Lycoming Operator’s Manual O-540, IO-540 Series, 4th Edition, June 2006.
[7] When installed correctly, 2–3 bolt threads would protrude from the edge of the nut. In this case 2–3 nut threads were visible on the end of the bolt.
[8] Fretting refers to wear involving small amplitude relative movement or vibration between contact surfaces.
[9] The high-power engines analysed as part of the study were Lycoming TIO-540 and IO-540, and Continental TSIO-520 and GTSIO-520 engines.
Occurrence summary
| Investigation number | AO-2025-029 |
|---|---|
| Occurrence date | 11/06/2025 |
| Location | 13 km south of Tindal Airport |
| State | Northern Territory |
| Report release date | 30/03/2026 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Engine failure or malfunction, Forced/precautionary landing, Smoke |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Robinson Helicopter Co |
|---|---|
| Model | R44 Raven I |
| Registration | VH-OOE |
| Serial number | 1879 |
| Aircraft operator | BBH Southern Highlands Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Daly Waters Aerodrome, Northern Territory |
| Destination | Wally’s Airstrip, Northern Territory |
| Damage | Minor |
Cessna 206 cargo door emergency exit
Safety advisory notice
To operators of all Cessna 206 variants
The removal of a middle row seat or approved cargo door modifications can improve the survivability for occupants of the Cessna 206.
What happened
On the morning of 1 September 2024, the pilot of a Cessna U206F took off from a private aircraft landing area, 40 km south-east of Moora, Western Australia, to conduct a local scenic flight with 5 passengers on board. On return to the landing area, after bouncing twice on landing, the pilot then attempted to conduct a go-around. However, an incorrect flap setting resulted in the aircraft not climbing, impacting the right wing with terrain before coming to a stop in an adjacent field.

The rear seat passengers, an older person and a child, were unable to egress the aircraft via their closest emergency exit (the cargo doors). The pilot tried assisting them but found that the forward cargo door was blocked due to the flap extension and was unaware how to open the rear cargo door with the forward cargo door blocked by the flap. The pilot attempted to retract the flaps so the door could be opened, but they would not retract. The pilot then instructed the passengers in the rear seats to climb over the middle row of seats so they could exit through the left forward cabin door. This ultimately increased the time taken to evacuate the aircraft and further increased the risk of passenger injury and post-impact survivability, such as if fire or ditching had been a factor.
Why did it happen
The Cessna 206 is a 6‑seat, high wing aircraft with a forward cabin door on the pilot’s side and a double cargo ‘clam-shell’ style door on the rear right hand side of the aircraft. When the aircraft flaps are extended 10° or more, this prevents the forward, overlapping part of the cargo door from opening, requiring a multi-step process to open the rear part of the door to exit the aircraft.
In response to a fatal Canadian Cessna 206 accident in 2018, Transport Canada issued
Airworthiness Directive CF-2020-10
(190.97 KB)
requiring Canadian registered Cessna 206 aircraft to have one of the second row (middle row) seats removed if passengers were to be seated in the rear seats of the aircraft. The airworthiness directive was introduced due to aircraft occupants being unable to evacuate the aircraft during an emergency and allowed the rear seat passengers easier access to the forward cargo door. At the time, the Canadian airworthiness directive did provide for an alternative means of compliance to the removal of a middle row seat with a supplemental type certificate (STC) STC SA1470GL(Opens in a new tab/window), for the installation of a second forward cabin door located adjacent to the forward right seat.
In 2020, STC SA20-34(Opens in a new tab/window) was approved as an alternative means of compliance, which allowed the forward cargo door corner to be hinged so the door corner can fold and the door fully open with flap extended in any position and without any restriction to the rear cargo door.
In 2023, Transport Canada also approved STC SA23-21(Opens in a new tab/window) to provide an additional handle that is installed internally on the forward cargo door. The handle is accessible to the rear seat passengers, which, when activated, jettisons the front cargo door from the aircraft. The removal of the door provided enhanced egress to the middle row occupants when flaps remained extended. The release of the door from the aircraft also improved visibility of the rear cargo door handle and simplified opening the rear cargo door for occupants in the rear seats.
In 2021, CASA issued Airworthiness Bulletin 52‑006(Opens in a new tab/window) recommending operators consider incorporating the changes Transport Canada had enforced.
Safety advisory notice
AO-2024-049-SAN-002: The Australian Transport Safety Bureau strongly encourages operators and owners to review Transport Canada Airworthiness Directive(Opens in a new tab/window)
Airworthiness Directive CF-2020-10
(190.97 KB)
, and consider either the removal of a middle row seat to improve rear seat occupants’ access to the pilot’s forward left cabin door or the fitment of approved Cessna 206 emergency exit modifications to reduce the risk created by the extended flap preventing the immediate and unobstructed use of the rear cargo doors during an emergency exit.

Cessna 206 emergency egress modifications
The additional complexity involved with opening the rear cargo door of the Cessna 206 when the flaps remain extended requires a multi-step process that is not intuitive or simple.
Transport Canada made significant changes to the aircraft configuration mandating the removal of a middle row seat and therefore providing access for passengers in the rear seats and improved access to the pilot’s forward left door. As an alternative to the removal of a seat, Transport Canada also approved modifications that either provided an additional exit or modification to the cargo door, so as the extended flap does not block the forward cargo door exit.
Australian operators of Cessna 206 aircraft that feature the double cargo door are strongly encouraged to review the changes Transport Canada has mandated, or the approved modifications, and consider implementing the improvements for the survivability for passengers during emergency egress in the Cessna 206.
Read more about this ATSB investigation: Collision with terrain during go-around involving Cessna U206F, VH-TDQ, 39 km south-east of Moora, Western Australia, on 1 September 2024
Publication details
| Investigation number | AO-2024-049 |
|---|---|
| Publication type | Safety Advisory Notice |
| Publication mode | Aviation |
| Publication date | 30/06/2025 |
Cessna 206 cargo door passenger pre-flight briefing
Safety advisory notice
To operators of all Cessna 206 variants
Emergency egress from the rear cargo doors becomes more complex with flaps extended.
Ensure passengers have a thorough understanding of the use of emergency exits.
What happened
On the morning of 1 September 2024, the pilot of a Cessna U206F took off from a private aircraft landing area, 40 km south‑east of Moora, Western Australia, to conduct a local scenic flight with 5 passengers on board. On return to the landing area, after bouncing twice on landing, the pilot then attempted to conduct a go‑around. However, an incorrect flap setting resulted in the aircraft not climbing, impacting the right wing with terrain before coming to a stop in an adjacent field.

The rear seat passengers, an older person and a child, were unable to egress the aircraft via their closest emergency exit (the cargo doors). The pilot tried assisting them but found that the forward cargo door was blocked due to the flap extension and was unaware how to open the rear cargo door with the forward cargo door blocked by the flap. The pilot attempted to retract the flaps so the door could be opened, but they would not retract. The pilot then instructed the passengers in the rear seats to climb over the middle row of seats so they could exit through the left forward cabin door. This ultimately increased the time taken to evacuate the aircraft and further increased the risk of passenger injury and post-impact survivability, such as if fire or ditching had been a factor.
Why did it happen
The Cessna 206 is a 6‑seat, high wing aircraft with a forward cabin door on the pilot’s side and a double cargo ‘clam-shell’ style door on the rear right hand side of the aircraft. When the aircraft flaps are extended 10° or more, this prevented the forward, overlapping part of the cargo door from opening, requiring a multi-step process to open the rear part of the door to exit the aircraft.
The pilot reported they provided the passengers with a pre-flight briefing that included the operation of both the forward and rear cargo doors, however the briefing did not include a demonstration of the operation of the cargo door emergency exit with the flaps extended.
The emergency exit placard located on the forward cargo door states:
- Open forward cargo door as far as possible
- Rotate red lever in rear cargo door forward and unlatch/open door
- Restow red lever
- Force rear cargo door open

During landing and take-off, it is likely there will be flap extension and therefore also likely that the flaps would remain extended after a forced landing, ditching or accident, making the egress via the rear cargo doors more difficult for passengers.
The newer Cessna 206H model incorporates the improvements that were made with the 1991 Cessna service bulletin SEB 91-4 Cargo door latch improvement applicable to all models prior to the Cessna 206H. The service bulletin recommended modifying the rear door handle to include a spring to ensure that the handle would return to the stowed position after opening, this improved the ease of opening the rear cargo door when the flaps remained extended. The service bulletin was not a mandatory modifcation.
In 2021, the Civil Aviation Safety Authority (CASA) issued Airworthiness Bulletin 52‑006(Opens in a new tab/window) recommending that pilots demonstrate the operations of the cargo door emergency exit with the flaps in an extended position. This was further revised by CASA in January 2025 to detail advice on placarding or fitment of the ‘return spring’ on the emergency release handle.
Safety advisory notice
AO-2024-049-SAN-001: The Australian Transport Safety Bureau advises Cessna 206 pilots and operators that due to the difficulties occupants have encountered egressing the rear cargo door as identified in several transport safety investigations, to ensure they are familiar with CASA‑issued Airworthiness Bulletin 52‑006(Opens in a new tab/window), and ensure passengers are provided with a thorough safety briefing demonstrating the cargo door emergency egress when the wing flaps remain in the extended position.
Cargo door emergency egress briefing
The emergency egress via the cargo door is hampered by the extension of flaps and the process to evacuate when the flaps are extended is neither simple nor obvious. The ATSB has identified that this presents a high risk to passengers, particularly those seated in the rear of the aircraft.
Pilots and operators are encouraged to ensure passengers of Cessna 206 aircraft with the standard double cargo doors are provided a pre-flight safety briefing that demonstrates the emergency egress process required to use the cargo doors when the flaps are in the extended position. Operators are encouraged to develop safety briefing cards with imagery clearly depicting the process as well as incorporating into the passengers’ pre-flight briefing. The incident also highlights the responsibilities of pilots to ensure passengers have a thorough understanding of the use of emergency exits.
Read more about this ATSB investigation: Collision with terrain during go-around involving Cessna U206F, VH-TDQ, 39 km south-east of Moora, Western Australia, on 1 September 2024
Publication details
| Investigation number | AO-2024-049 |
|---|---|
| Publication type | Safety Advisory Notice |
| Publication mode | Aviation |
| Publication date | 30/06/2025 |
R66 in-flight break-up after turbulence-induced low-G
A Robinson R66 broke up in flight just 3.5 seconds after encountering a turbulence‑induced low‑G condition, with the helicopter rapidly rolling to the right and becoming inverted after the main rotor disc became unloaded, an ATSB investigation report details.
The helicopter, with a single pilot on board, had been flying from Cessnock to the New South Wales mid north coast on 26 October 2023 when it encountered the turbulence, likely in the form of rapidly rising air, while passing over the Yacaaba Headland, to the west of Mount Yacaaba, near Hawks Nest.
“The helicopter was flying on autopilot at an indicated airspeed of 115 kt, 45 kt above the manufacturer’s maximum recommended speed for flight in significant turbulence,” ATSB Director Transport Safety Stuart Macleod noted.
“This speed significantly increased the uncommanded right roll rate and reduced the time available for the pilot to respond by applying a gentle aft cyclic input to re‑load the main rotor disc.
“In addition, the pilot had been eating and had food in their right hand, and so they used their left hand to manipulate the cyclic, reducing their ability to slow the helicopter in a timely manner using coordinated flight control inputs.”
Footage from an on‑board video camera was instrumental in detailing the accident sequence, showing that after the helicopter began rolling to the right, the pilot did not apply aft cyclic to reload the main rotor, and the roll continued to develop.
“Instead, the pilot progressively applied increasing left cyclic during the right roll, increasing the risk of an extreme teetering event, where the spindles of the main rotor contact the main rotor shaft, precipitating a break‑up.”
The broken‑up helicopter subsequently impacted the waters of Providence Bay, near Hawks Nest, and the pilot was fatally injured.
“The investigation also found that the asymmetrical horizontal stabiliser fitted to Robinson series helicopters, comprising both the piston‑powered R22 and R44 as well as the turbine R66, significantly contributes to uncommanded right roll rates during low‑G conditions, adding to the risk of an in‑flight break‑up.”
The stabiliser is an inverted aerofoil that produces downward forces to counter the helicopter’s natural tendency to adopt a nose down attitude with increasing air speed. With the asymmetrical design on Robinson helicopters, it extends from the right side of the tail cone, and creates a right rolling moment, which is normally counteracted by a left tilt of the main rotor disc. However, in a low‑G condition where the main rotor disc is unloaded, it cannot counteract the right rolling moment.
“Pleasingly, Robinson Helicopter Company has developed a symmetrical horizontal stabiliser that is being fitted to all new Robinson helicopters, and is available as a modification for all existing Robinson helicopters,” Mr Macleod noted.
In addition, Robinson will replace the asymmetric stabiliser with the symmetrical design on all R66s and R44s returned to it for overhaul.
“Further, Robinson Helicopter is in the process of updating several safety notices to provide pilots with improved guidance specific to low‑G, turbulence, and pilot distraction.”
Mr Macleod said the ATSB strongly encourages fitment of the symmetrical stabiliser.
“The modification significantly reduces the right roll if a low‑G condition is encountered, allowing pilots more time to recognise and respond to the situation.”
Nonetheless, avoiding turbulent conditions where possible, and flying through turbulence at or below the maximum airspeed recommended by the manufacturer, remain critical safety defences for pilots of Robinson helicopters.
“In this case the pilot’s response to encountering the low‑G contributed to the development of the in‑flight break‑up, but we would caution all Robinson helicopter pilots that a low‑G condition can result from turbulence directly, and pilots must be ready to respond appropriately,” Mr Macleod explained.
“If the main rotor disc is not immediately reloaded, right roll can develop rapidly, particularly when an asymmetrical stabiliser is fitted.
“Therefore it is critical that pilots apply immediate gentle aft cyclic to reload the main rotor, before correcting the right roll.”
Read the final report: Loss of control and in-flight break-up involving Robinson R66, VH-KFT, near Hawks Nest, New South Wales on 26 October 2023
South Geelong level crossing accident

A truck that was struck by an empty passenger train at a Geelong level crossing had entered the crossing from an unsealed side road that had developed through usage over time but had not been identified as an emerging risk during regular inspections, a transport safety investigation report details.
The empty V/Line passenger train was approaching the Barwon Terrace level crossing in South Geelong on 3 April 2023 when the tip truck, having departed a nearby depot, drove onto the level crossing from the unsealed side road.
“The configuration of the side road meant vehicles could enter the level crossing even when the level crossing boom gates and flashing lights were operating,” explained Chief Investigator Mark Smallwood of the Office of the Chief Investigator, which conducts rail investigations in Victoria under a collaboration agreement with the ATSB.
“After likely becoming aware of the approaching train, the truck driver attempted to reverse their vehicle away from the track. However, the train collided with the truck before the truck was clear.”
The collision rotated the truck about 180° and the driver sustained fatal injuries. The train crew were uninjured.
CCTV footage showed that it was common practice for vehicles to turn right from the unsealed road onto Barwon Terrace between the level crossing protection and the track.
“Although the level crossing was inspected regularly by V/Line, the rail infrastructure manager, those inspections did not include a review of the emerging risks associated with the changing road usage and configuration at the level crossing,” Mr Smallwood said.
“Additionally, the safety interface agreement between rail operators and the City of Geelong, as the road manager, was also ineffective in triggering action to monitor the road to rail interface and changing usage.”
Since the accident, a V/Line maintenance alert was issued for track inspectors to identify roads or access tracks which bypass crossing controls.
In addition, changes to the Australian Level Crossing Assessment Model (ALCAM) survey program in Victoria now require contractors undertaking assessments to identify and report any road network configurations like the incident location.
“This tragic accident highlights that level crossing inspection regimes should always include checks on any changes that may introduce new hazards and associated risks,” Mr Smallwood concluded.
Read the final report: Collision between a truck and V/Line train 7727, Barwon Terrace level crossing, South Geelong, Victoria on 3 April 2023
Unstable approach involving Boeing 737, VH-YIL, near Sydney Airport, New South Wales, on 12 June 2025
Final report
Report release date: 30/09/2025
Investigation summary
What happened
On the morning of 12 June 2025, a Virgin Australia Airlines Boeing 737‑800, registered VH‑YIL, operated a passenger transport flight from Brisbane, Queensland, to Sydney, New South Wales.
As the aircraft descended towards Sydney, air traffic control provided clearance for the crew to conduct a visual approach to runway 34 left. During the approach, the speed brake was not armed, and the final flap selection was not completed until 875 ft above the airport elevation (AFE). The operator’s procedures required that both items be completed before the aircraft descend below 1,000 ft above the airport elevation.
As the aircraft later descended through about 500 ft AFE, the captain checked the aircraft configuration and identified that the speed brake was not armed. The captain then armed the speed brake as the aircraft descended below 405 ft AFE. The approach continued and the aircraft landed without further incident.
What the ATSB found
The ATSB found that after air traffic control provided clearance for the crew to conduct a visual approach, a required autopilot altitude selection was not completed. As a result, the aircraft later deviated above the desired approach path.
The crew immediately recognised the deviation and, in response, the captain disengaged the autopilot and auto thrust to manually re‑establish the approach descent profile, without informing the first officer. This led to an unexpected increase in flight crew workload. Then, in attempting to re‑establish the desired approach path, the crew did not fully complete the landing procedures and associated checklist before descending below the stabilisation criteria check altitude. Subsequently, the flight crew did not perform the required missed approach but instead continued the approach and landing.
Safety message
Unstable approaches continue to be a leading contributor to approach and landing accidents and runway excursions. This incident highlights how quickly a small oversight can disrupt an otherwise standard approach. If the disruption leads to a breach of the stabilised approach criteria, early recognition of the situation and prompt execution of a go‑around, rather than continuing the approach, will significantly reduce the risk of approach and landing accidents.
This incident also highlights that when crews are faced with the unexpected, effective crew resource management, with clear communication between the crewmembers, is essential. This ensures effective teamwork when responding to disruptions. Additionally, effective flight crew monitoring in a multi‑crew environment is paramount to aircraft safety. Bringing deviations to the attention of the pilot flying ensures that the aircraft remains on a safe flight path and is correctly configured for the relevant phase of flight.
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the morning of 12 June 2025, a Virgin Australia Airlines Boeing 737-800, registered VH‑YIL, operated a passenger transport flight from Brisbane, Queensland, to Sydney, New South Wales.
As the aircraft descended towards Sydney in day visual meteorological conditions and with the autopilot engaged, air traffic control provided clearance for the crew to conduct a visual approach to runway 34 left. At that time, an altitude of 2,000 ft was set in the altitude window of the autopilot mode control panel (MCP). After receiving clearance for a visual approach, operational procedures required that the pilot flying[1] select an altitude equivalent to 500 ft above the airfield elevation (in this case 500 ft, as the airport was close to sea level) in the MCP altitude window (see the section titled Approach procedures). However, the captain, acting as pilot flying, inadvertently did not make this selection and the first officer, acting as pilot monitoring, did not identify that this altitude selection had not been completed.
As the aircraft descended toward 2,000 ft above mean sea level (AMSL) (Figure 1), the aircraft intercepted the final approach track. The crew expected the descent to continue, but the aircraft began automatically levelling off to capture the 2,000 ft altitude set in the MCP altitude window, taking the aircraft above the desired approach descent profile.
The crew immediately recognised the deviation and identified that the incorrect altitude was entered into the MCP altitude window; to continue the descent, but without verbalising the action, the captain entered 500 ft in the altitude window. Shortly after, the captain recognised that this selection would not re‑establish the required approach path, so, without first alerting the first officer to their intentions, disengaged the autopilot and auto thrust to manually re‑establish the approach descent profile.
Figure 1: Overview of the approach
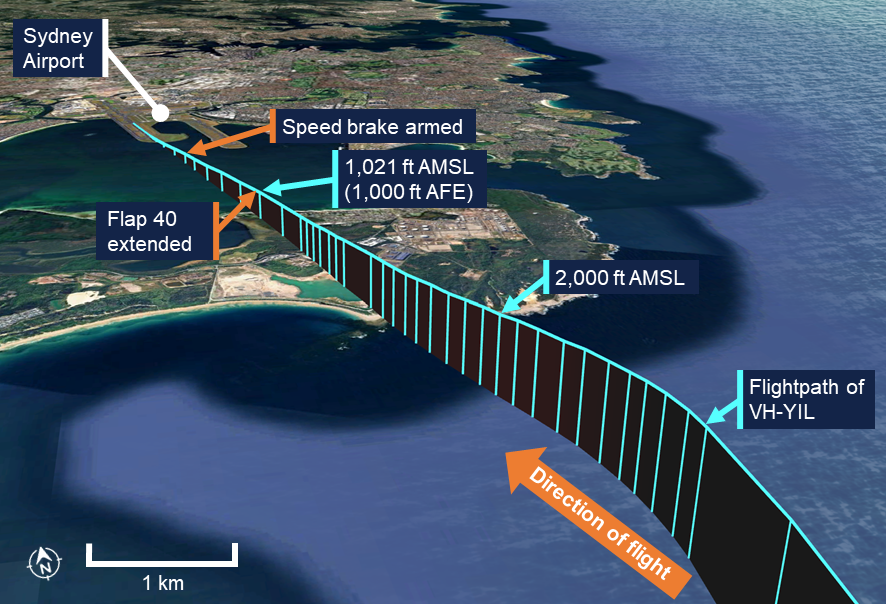
Source: Google Earth, recorded flight data and ATSB
As the crew worked to re-establish the desired approach path while completing the pre‑landing procedures, the speed brake was unintentionally not armed, and the final flap selection (flap 40) was not made until 939 ft above the airport elevation. These items, and the associated landing checklist, were required to be completed before the aircraft passed 1,000 ft as set out in the operator’s procedures (see the section titled Stabilised approach).
The captain did not recognise that the checklist was not complete and believed that the stabilised approach criteria had been met. The first officer, acting as pilot monitoring, did not identify that the speed brake was not armed, but did identify that the required final flap selection and the landing checklist had not been completed in time. However, the first officer noted that the approach path, speed and descent rate were within the criteria and announced that the approach was stable.
As the aircraft descended through about 500 ft AMSL, the captain checked the aircraft configuration and identified that the speed brake was not armed. The captain then armed the speed brake as the aircraft descended below 426 ft AMSL (405 ft above the airport elevation). The approach continued without further incident and the aircraft landed at 0905 local time.
After landing, the captain discussed the incident with the first officer and assessed that a missed approach should have been conducted.
Context
Pilot details
The captain held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The captain had 14,975 hours of flying experience, of which 10,081 hours were on the Boeing 737 aircraft type, with 127 hours accrued in the previous 90 days.
The captain held additional non‑flying duties in the organisation with 50% of their time spent in normal flying duties. The captain also stated that in their experience of regular flying operations, visual approach clearances were unusual.
The first officer held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer had about 28,000 hours of flying experience, of which about 14,000 hours were on the Boeing 737 aircraft type, with 117 hours accrued in the previous 90 days.
The ATSB found no indicators that the flight crew were experiencing a level of fatigue known to adversely affect performance.
Approach procedures
Visual approach
The operator’s flight crew operations manual (FCOM) for the Boeing 737‑800 aircraft included the following visual approach procedure:
When cleared for a visual approach, the MCP altitude should be selected to 500 ft above field elevation, however this does not preclude setting an intermediate level‑off altitude if desired.
Stabilised approach
The operator’s policy and procedure manual provided the following stabilised approach policy that included:
All approaches must be stabilised by 1000 ft above field elevation.
An approach is stabilised when the following criteria are met:
- Briefings and normal checklists are completed
- Aircraft is in the correct landing configuration
- Aircraft is on the correct lateral and vertical flight path
- Sink rate, no greater than 1,000 feet per minute.
The policy also noted that if the stabilisation criteria were exceeded for other than momentary periods at any time below the stabilisation height, the pilot monitoring must call "NOT STABLE”, and the pilot flying must initiate a missed approach.
The FCOM also stated that a missed approach shall be executed whenever required visual reference is not obtained or maintained or when an approach is not stabilised at 1000 ft above the airport elevation.
Meteorology
The approach was conducted in visual meteorological conditions.
At 0900, 3 minutes before the incident, the Bureau of Meteorology automatic weather station at Sydney Airport recorded the temperature as 12°C and the wind as 13 kt from 247° magnetic. Cloud cover was recorded as few[2] at 3,521 ft above mean sea level (AMSL). Visibility was recorded as greater than 10 km with no recorded precipitation.
Recorded data
Virgin Australia provided the ATSB with the aircraft’s quick access recorder data which captured the incident approach.
The recorded data (Figure 2) showed that the landing flap selection (flap 40) was completed 3 seconds after the aircraft descended below 1,000 ft above the airport elevation (AFE), at 939 ft AFE (960 ft AMSL). The flaps then completed moving to that extension as the aircraft descended below 875 ft AFE (896 ft AMSL). The speed brake lever was moved to the armed position as the aircraft descended below 405 ft AFE (426 ft AMSL).
Figure 2: Graphical representation of the recorded quick access data
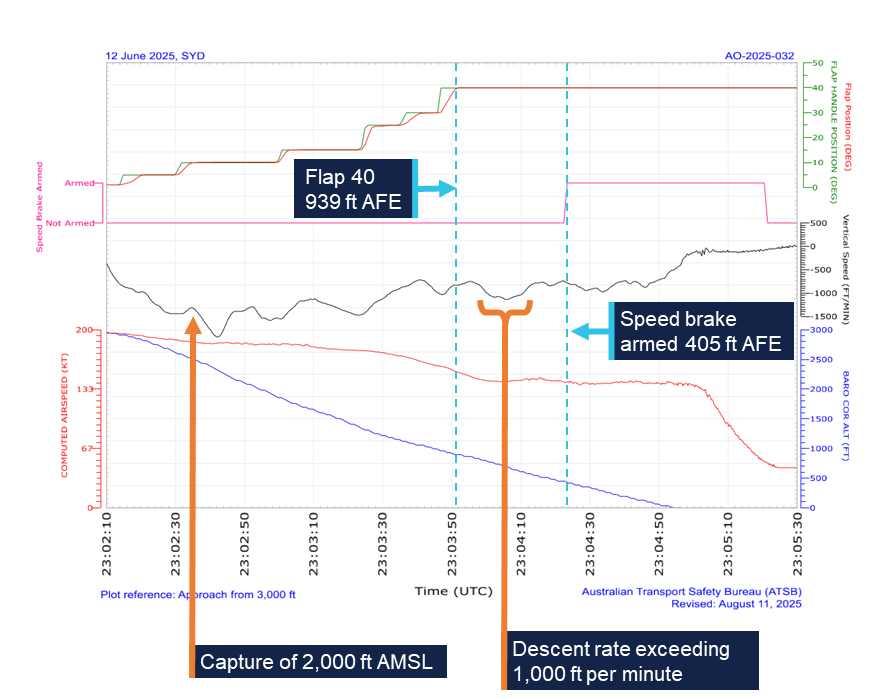
All times are coordinated universal time (UTC). Local time was Australian Eastern Standard Time (EST), which was UTC +10 hours. Source: Quick access recorder from VH-YIL, annotated by the ATSB
After descending below 1,000 ft, the aircraft maintained an appropriate speed and flightpath. The rate of descent exceeded the 1,000 ft per minute stabilised approach criteria limit for a 9 second period between 0904:02 and 0904:11. During this period, the aircraft descended from 747 ft AFE to 587 ft AFE, and the maximum recorded descent rate was 1,136 ft per minute at 0904:07.
Safety analysis
As the aircraft descended towards Sydney, the crew were provided with a visual approach clearance which the captain reported was unusual. After receiving the clearance, the captain unintentionally did not make the required 500 ft selection in the altitude window of the mode control panel. The first officer, as the pilot monitoring, did not identify that this omission had occurred. Consequently, as the aircraft descended to 2,000 ft the autopilot began to level off rather than continuing the descent to 500 ft, which took the aircraft above the desired descent profile. The captain responded with an unplanned manual intervention without alerting the first officer to their intention while the flight crew were also attempting to complete the final landing procedures. This led to an unexpected increase in flight crew workload and reduced the first officer’s situation awareness.
Workload has been defined as ‘reflecting the interaction between a specific individual and the demands imposed by a particular task. Workload represents the cost incurred by the human operator in achieving a particular level of performance’ (Orlady and Orlady, 1999). A discussion of the effect of workload on the completion of a task requires an understanding of an individual’s strategies for managing tasks.
An individual has a finite set of mental resources they can assign to a set of tasks (for example, performing an approach and landing). These resources can change given the individual’s experience and training and the level of stress being experienced at the time. An individual will seek to perform at an optimum workload by balancing the demands of their tasks. When workload is low, the individual will seek to take on tasks. When workload becomes excessive the individual must, as a result of their finite mental resources, shed tasks.
An individual can shed tasks in an efficient manner by eliminating performance on low priority tasks. Alternatively, they can shed tasks in an inefficient fashion by abandoning tasks that should be performed. Tasks make demands on an individual’s resources through the mental and physical requirements of the task, temporal demands and the wish to achieve performance goals (Hart and Staveland, 1988, and Lee and Liu, 2003).
In this case, likely in response to increased workload and the absence of crew coordination, they missed required checklist items (the final flap and speed brake selections). The stabilised approach criteria required that the aircraft be in the final landing configuration by 1,000 ft above the airport elevation. The landing flap selection was made 3 seconds after descending below this height, although the captain believed that the flap selection had been made in time to meet the stabilised approach criteria requirements. However, the flaps did not reach the required position until the aircraft descended through 875 ft above the airport elevation.
The first officer identified that the flap selection was made late and that, therefore, the stabilised approach criteria had not been met. However, as the descent rate, speed and profile were within the criteria, they announced that the approach was ‘stable’ instead of making the required ‘not stable’ announcement. Consequently, the required missed approach was not commenced, and the approach was continued. The first officer did not identify that the speed brake landing procedure action was not completed.
As the approach continued, the descent rate exceeded the stabilised approach criteria for a period of 9 seconds. This exceedance was momentary and not excessive and therefore it did not require the commencement of a missed approach.
When the unarmed speed brake was later identified by the captain, this should have acted as a further trigger for the commencement of a missed approach. Instead, this missed action was quickly rectified by the captain and the approach continued.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the unstable approach involving Boeing 737, VH-YIL, near Sydney Airport, New South Wales, on 12 June 2025.
Contributing factors
- After air traffic control provided clearance for the crew to conduct a visual approach, a required autopilot altitude selection was not completed. As a result, the aircraft later deviated above the desired approach path.
- While re-establishing the approach path, the crew did not complete required landing procedures until after the aircraft descended below the stabilisation criteria check altitude. Subsequently the flight crew did not perform the required missed approach, instead continuing the approach and landing.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Airservices Australia
- Bureau of Meteorology
- recorded data from the quick access recorder from VH-YIL
- the flight crew
- Virgin Australia Airlines.
References
Orlady, HW & Orlady, LM 1999, Human factors in multi-crew flight operations. Ashgate, Aldershot, p. 203.
Hart, SG & Staveland, LE 1988, ‘Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research’, In PA Hancock & N Meshkati (Eds.), Human Mental Workload. North Holland Press, Amsterdam.
Lee, YH & Liu, BS 2003, ‘Inflight workload assessment: Comparison of subjective and physiological measurements’, Aviation, Space, and Environmental Medicine, vol.74, pp. 1078- 1084.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Civil Aviation Safety Authority
- the flight crew
- Virgin Australia Airlines.
No submissions were received.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky was covered.
Occurrence summary
| Investigation number | AO-2025-032 |
|---|---|
| Occurrence date | 12/06/2025 |
| Location | Sydney Airport |
| State | New South Wales |
| Report release date | 30/09/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Aircraft preparation, Unstable approach |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-8FE |
| Registration | VH-YIL |
| Serial number | 38713 |
| Aircraft operator | Virgin Australia Airlines Pty Ltd |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Brisbane Airport, Queensland |
| Destination | Sydney Airport, New South Wales |
| Damage | Nil |