Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 22 May 2025, a commercially licenced (CPL) pilot was undergoing an examination for the initial issue of a multi-engine instrument rating. Around 1200 local time, upon completion of the examination ground components, the candidate boarded the aircraft (left front seat), alongside the certified examiner (right front seat) and an observing examiner (right rear seat). Take-off from Moorabbin Airport was routine, and the aircraft tracked for an instrument landing system (ILS) approach at Avalon Airport, Victoria, followed by a planned VHF omni-range (VOR) approach to runway 18.
Both examining officers reported that the pilot’s performance began to noticeably deteriorate following a simulated engine failure and the missed approach component of the flight test, with increasing inaccuracy in tracking and altitude holding and a loss of situational awareness described by both examiners. Subsequently, after the principal examiner discontinued the flight test, both officers became aware that the pilot was now sweating profusely and not responding verbally. Shortly thereafter, the pilot lost consciousness.
The principal examiner assumed control of the aircraft and advised Avalon Approach air traffic control (ATC) of the situation and the intent to return to Moorabbin. Moorabbin Tower ATC provided taxi guidance for the arrival to facilitate transfer of the candidate pilot to an ambulance. Both examiners worked to ensure the pilot’s arms and legs were away from the aircraft controls and their headset and instrument hood were removed. They both noted that in the DA 42, the aircraft’s seats were fixed and not able to be moved rearwards for better control clearance.
Landing at Moorabbin was uneventful, with the aircraft met by the Aerodrome Reporting Officer (ARO). Shortly thereafter, the candidate pilot regained consciousness and was able to climb unaided from the aircraft to meet the ambulance staff.
The candidate pilot reported that they had not eaten anything substantial on the day of the examination and had only 4 hours sleep in the preceding 24 hours, with a total of 10 hours in the past 2 days.
Figure 1: Flight path – flight test and return to Moorabbin
Both mentally and physically, flight examinations can be taxing for the candidate. Demanding concentration and focus – often for extended periods, these assessments require that pilots’ preparation also extends to their physiological readiness, if best performance and safety is to be assured.
The value and importance of Crew Resource Management (CRM) is most often discussed and considered in terms of larger passenger-carrying aircraft operations. This occurrence – specifically the cooperation displayed by the principal and observing examiners in ensuring the candidate pilot was safe and the aircraft controls uninhibited – illustrates that the principles of CRM extend to all multi-crew situations.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-020
Occurrence date
22/05/2025
Location
Overhead Avalon Airport
State
Victoria
Occurrence class
Incident
Aviation occurrence category
Diversion/return, Flight crew incapacitation
Highest injury level
None
Brief release date
28/07/2025
Aircraft details
Manufacturer
Diamond Aircraft Industries
Model
DA 42
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
The ATSB is investigating a collision with terrain accident involving a Reims Cessna F406 aircraft, registered VH‑EYQ, near Oakey, Queensland, on 20 July 2025.
The aircraft was being used for a pilot check flight and was conducting an instrument approach to land at Oakey Army Aviation Centre when it collided with terrain in a field approximately 2 km from the runway. The 2 occupants on board, a pilot and a flight examiner, were fatally injured.
The ATSB has commenced the examination and analysis of the initial evidence collected.
To date, the ATSB has:
examined the wreckage and accident site
examined meteorological information
interviewed relevant parties
collected radio communication, aircraft traffic surveillance data, and navigational application data
collected aircraft, pilot, crew and operator documentation.
The investigation is continuing and will include review and examination of:
pilots’ recent history
propellers
maintenance records
pilot and crew training and medical records
operational procedures and documentation
further interviews with relevant parties
flight data and air traffic surveillance data
the requirements of conducting simulated one engine inoperative exercises at low heights.
A preliminary report, which detailed factual information established during the evidence collection phase, was released on 10 December 2025 (see below).
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Preliminary report
Report release date: 10/12/2025
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Summary video
The occurrence
On 20 July 2025, a Reims Aviation F406 Caravan II, registered VH-EYQ, was being utilised for an instrument proficiency check (IPC)[1] with a pilot and a flight examiner on board. The flight was conducted under the instrument flight rules[2] and the planned route was from Warwick Airport to Oakey Airport, Queensland, later returning to Warwick Airport.
The IPC was the pilot’s third flight for the day. They had undertaken an aerial survey mission in VH-EYQ that morning for Aero Logistics, having departed Emerald Airport, Queensland, at 0747 and arrived at Archerfield Airport, Queensland, at 1208. The pilot refuelled the aircraft at Archerfield Airport and departed at 1308 for the flight to Warwick Airport for the purposes of undertaking the IPC.
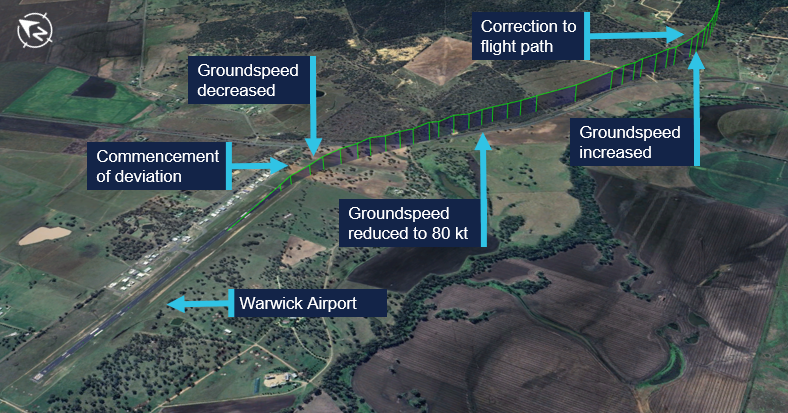
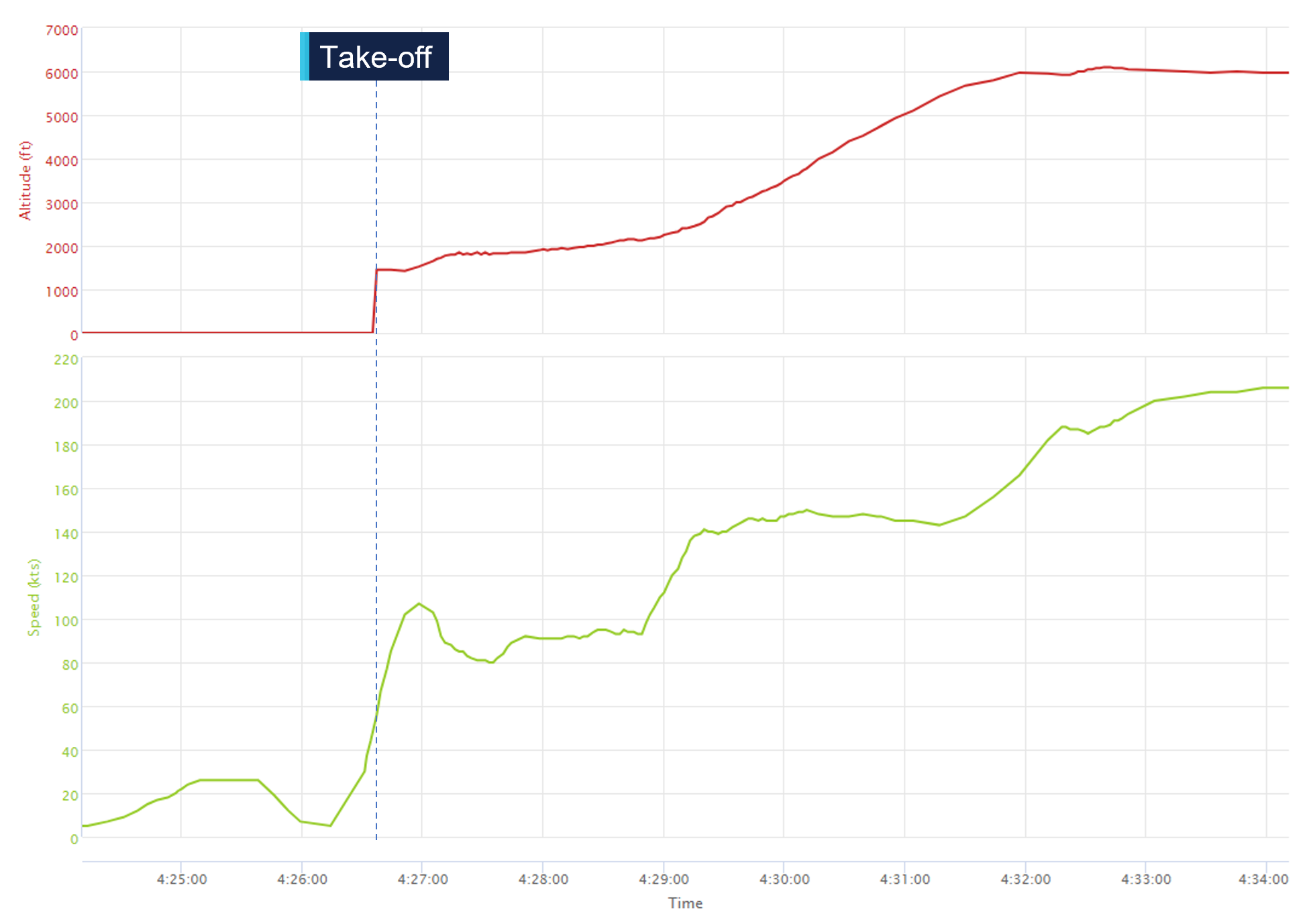
The pilot arrived at Warwick Airport at 1345 where they met the flight examiner. At 1426, the aircraft departed Warwick Airport. About 16 seconds after departure, the aircraft’s groundspeed began to decrease from 109 kt, and the aircraft stopped climbing and commenced a slow turn to the right (Figure 1). This turn was not consistent with the submitted flight plan. The aircraft’s groundspeed continued to reduce over a period of about one minute to 80 kt (see Recorded flight data). The aircraft then began to accelerate before turning left and commencing a climb to an altitude of 6,100 ft above mean sea level.
Figure 1: VH-EYQ departure from Warwick Airport
Source: Google Earth, annotated by the ATSB
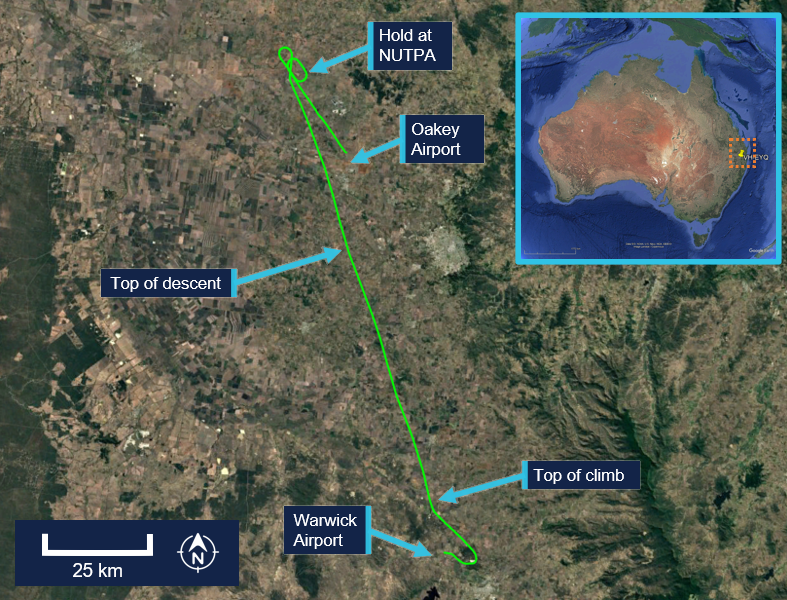
At 1433, Brisbane Centre air traffic control (ATC) issued the pilot with a clearance to track directly to reporting point[3] NUTPA, which was the commencement point for the Oakey Airport runway 14 instrument landing system (ILS)[4] approach (Figure 2).
Figure 2: VH-EYQ flight overview
Source: Google Earth, annotated by the ATSB
At 1439, the pilot advised ATC that they would be conducting airwork in the Oakey area, not above an altitude of 4,000 ft, and they would contact ATC again on completion or by 1530. At that time, the Oakey Airport ATC tower was inactive. After commencing the descent for NUTPA at 1441, the pilot changed frequency to the common traffic advisory frequency (CTAF) in the Oakey Airport area, and all subsequent air-to-air communications took place on the CTAF. Between 1443 and 1454 the pilot made 5 transmissions on this frequency for traffic sequencing purposes.
At 1450, the aircraft passed overhead NUTPA and conducted one holding pattern. At 1456, the aircraft commenced a descent from 3,800 ft and the pilot made a radio broadcast to advise that the aircraft was established on the ILS.
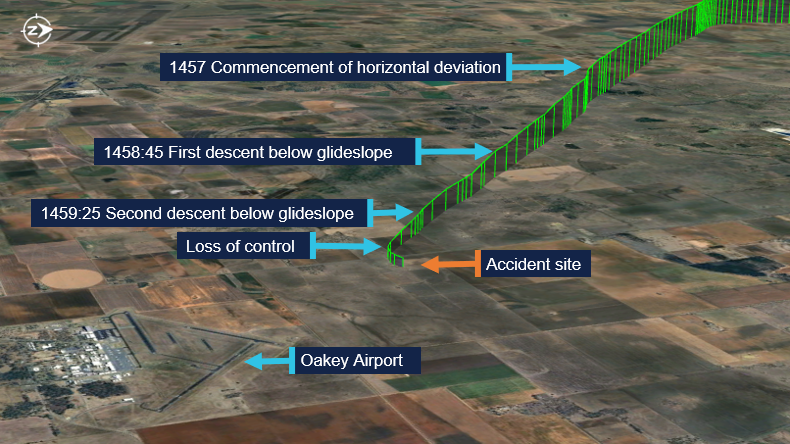
At 1457, the aircraft began to deviate from the horizontal profile for the approach. The aircraft initially deviated right of the extended centreline and then to the left (Figure 3). Fluctuations in vertical speed also occurred during this period. The aircraft continued the approach slightly left of the extended centreline, but the vertical profile of the approach remained on the glideslope.[5] The wind conditions recorded at Oakey Airport at the time were a light breeze of 6 kt, with a mean direction of 190°M (see Meteorological information).
Figure 3: Final approach track
Source: Google Earth, annotated by the ATSB
At about 1458:45, and an altitude of 2,500 ft, the aircraft began to descend below the glideslope. This was initially corrected, and the aircraft flew level at about 2,200 ft for 30 seconds. At 1459:25, the aircraft descended below the glideslope again, and the descent continued to an altitude of about 1,700 ft, which equated to a height of between 300–400 ft above ground level (AGL). During this period the aircraft’s groundspeed began to decay. At 1459:39, the aircraft’s groundspeed had reduced to 85 kt (see Recorded flight data). At about 1459:53,[6] a 2‑second radio broadcast was made from the aircraft with an alarm sounding in the background.
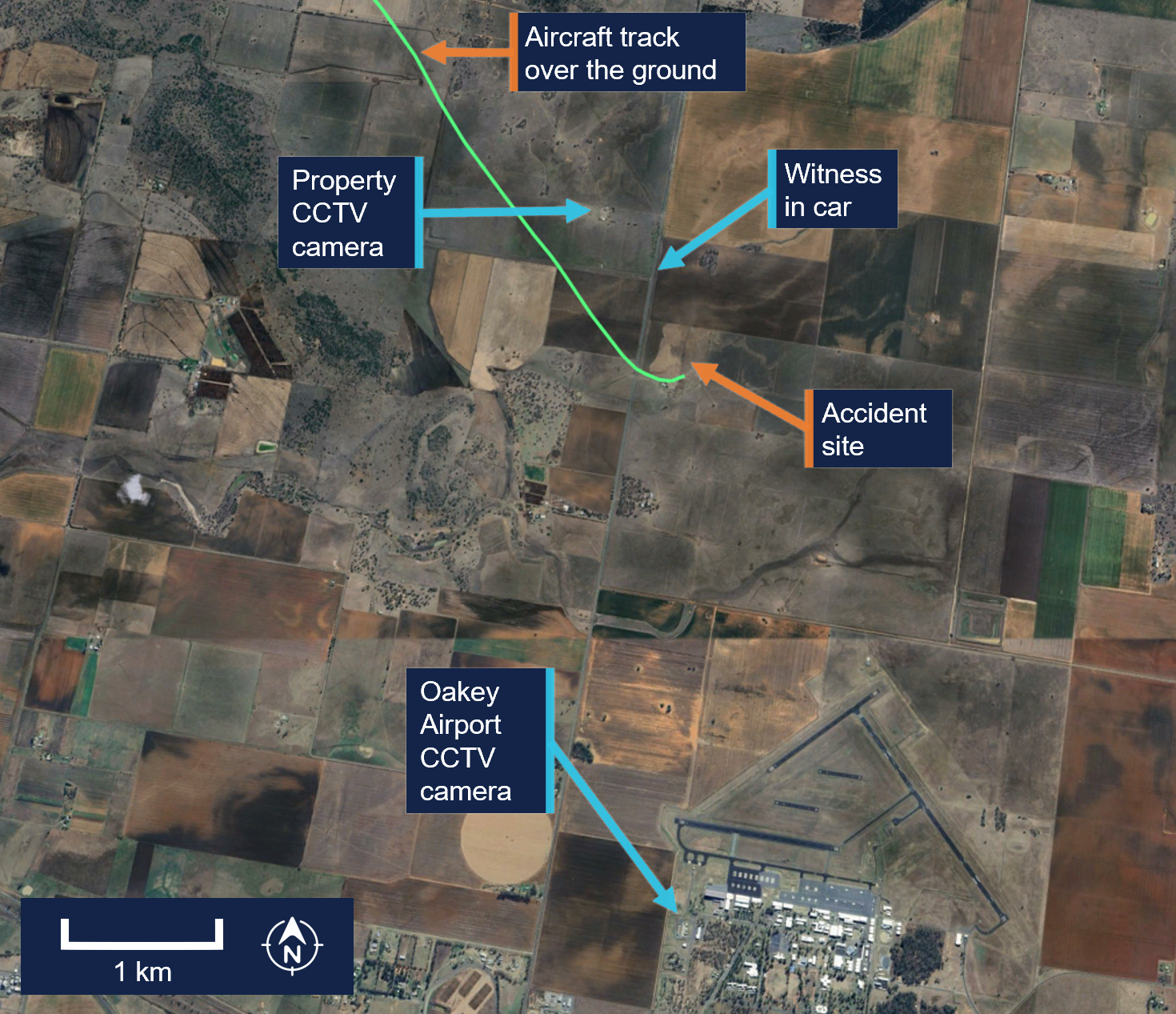
A motorist travelling south observed the aircraft on approach and maintained visual contact with it for about 3 km (Figure 4). They observed the aircraft commence a flat turn and yaw[7] to the left at a height of about 300 ft AGL and pass above the road ahead of them. They recalled seeing the aircraft then roll to the left, pitch down, and impact the terrain.
Figure 4: Witness and closed-circuit television camera locations
Source: Google Earth, annotated by the ATSB
Closed-circuit television (CCTV) cameras located at a nearby property and Oakey Airport captured the aircraft commence a steep descent before colliding with terrain (Figure 5).
The aircraft was destroyed in a post-impact fire, and both occupants were fatally injured.
Figure 5: Composite images of recorded CCTV camera footage
Source: CCTV camera recordings
Context
Pilot information
Pilot experience
The pilot held a valid class 1 aviation medical certificate and an air transport pilot licence (ATPL) (aeroplane). Additionally, they held a grade 3 flight instructor rating with multi‑engine aeroplane training approval and design feature endorsements to operate VH-EYQ. The pilot held a valid multi-engine instrument rating with the previous instrument proficiency check (IPC) completed in August 2024.
At the time of the accident, the pilot had accumulated 5,767 hours total aeronautical experience. This included 4,170 flight hours as pilot in command with 3,514 hours in multi-engine aeroplanes and about 1,200 hours in command of a Reims F406. In the preceding 90 days they had flown 95 hours, including 54 hours in the Reims F406. They had worked for the aircraft operator since March 2017.
Known recent activity
The pilot’s work roster for the week prior to the accident (from 14 to 20 July 2025) is shown in Table 1. During this week, the pilot was based away from home and conducted multiple survey flights. The pilot’s duties for 20 July included the survey flight in the morning with no additional rostered flying.
Table 1: Pilot rostered duties, 14 to 20 July 2025
Date
Shift start-finish time
Total flight hours
14 July
OFF
0
15 July
0630-1430
1.5
16 July
0630-1430
2.1
17 July
0630-1430
1.8
18 July
0630-1430
2.4
19 July
OFF
0
20 July
0730-1500
5:31
A text message sent from the pilot the evening of 19 July indicated that the pilot had intended to conduct the IPC the following day. Additionally, the message indicated they had sleep opportunity from about 2130.
Flight examiner information
Flight examiner experience
The flight examiner held a valid class 1 aviation medical certificate and an ATPL (aeroplane). They also held grade 1 flight instructor and flight examiner operational ratings, with multi-engine aeroplane and instrument rating (aeroplane) training approval. Their flight instructor rating also had a spin endorsement, and they held design feature endorsements to operate VH-EYQ. The examiner held a valid multi-engine instrument rating with the previous IPC completed in October 2024.
The flight examiner’s logbook records were destroyed in the post-impact fire. Based on records of the pilot’s hours from January 2025, the flight examiner’s total aeronautical experience was in excess of 20,000 hrs. Additionally, they had flown 3 similar proficiency check flights for the aircraft operator in the previous 12 months, totalling 3.6 hours in the Reims F406. The flight examiner was external to the aircraft operator and was regularly hired to complete the IPC for their pilots.
Known recent activity
Along with their logbook, the flight examiner's work records were destroyed in the post‑impact fire.
A family member recalled that the flight examiner had returned from a chartered flight to western Queensland on Tuesday 15 July. During the week, they had spent a day providing aviation theory instruction to students but had no other work engagements. On the day of the accident, the flight examiner woke at their normal time. They were reported to have slept well and, when leaving home for the IPC flight, they appeared their normal self with no signs of fatigue.
Aircraft information
General information
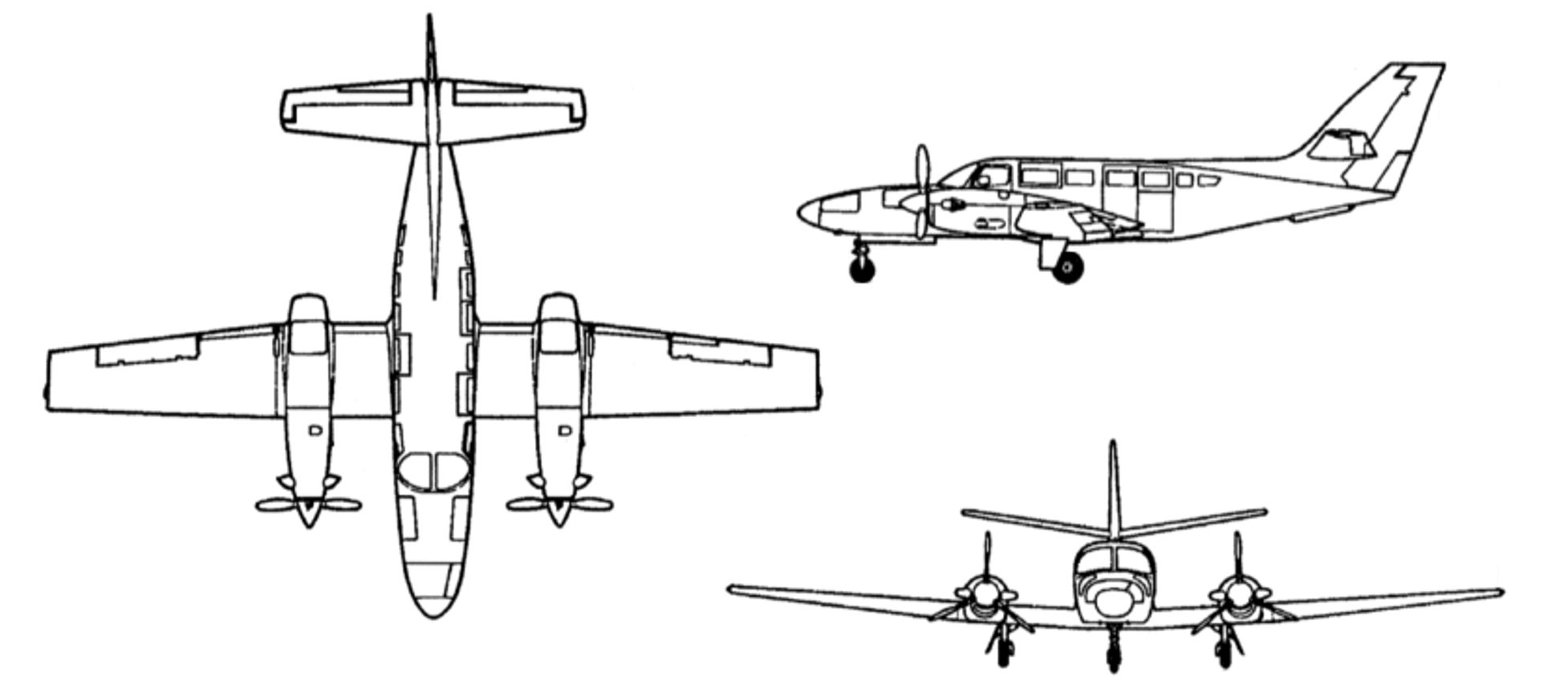
The Reims Aviation F406 is a low wing, twin‑engine aircraft powered by 2 Pratt & Whitney Canada PT6A-112 turbine engines, each driving a 3-bladed McCauley constant speed, full-feathering propeller (Figure 6). The accident aircraft, serial number F406‑0047, was manufactured in France in 1990 and first registered in Australia as VH‑EYQ in 2012.
Figure 6: Reims F406
Source: ASI Aviation
Recent maintenance activity
The aircraft was to be maintained in accordance with the aircraft operator’s Civil Aviation Safety Authority (CASA) approved system of maintenance. This required a periodic inspection every 100 hours or 12 months, whichever came first. The system of maintenance allowed for periodic inspection intervals to be extended up to a maximum of 10 hours. The most recent periodic inspection was completed on 11 June 2025, at 17,376 hours in service. At the time of the accident, the aircraft had accumulated 17,475.6 hours total time in service.
Configuration
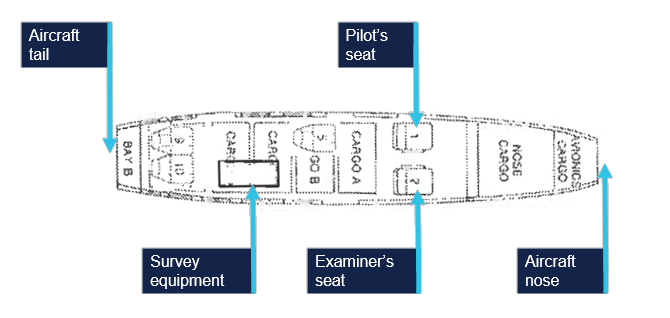
VH-EYQ was configured in a 5-seat survey layout. This comprised the pilot (left) and copilot (right) seats in the front row, followed by 1 passenger seat in row 3, and 2 passenger seats in row 5. The remaining passenger seats were removed from the cabin to accommodate the installation of aerial survey equipment (Figure 7). An electronic loading system had been generated for this configuration by an approved load controller, and records show that this was utilised by the pilot for previous flights.
Figure 7: VH-EYQ cabin configuration
Source: ASI Aviation, annotated by the ATSB
Weight and balance
Prior to its departure from Archerfield Airport, the aircraft was fuelled with 1,086 L of Jet A1 fuel. The aircraft operator advised that, based on this fuel uplift and the intended flying activity, it was very likely that the aircraft had full fuel on board for the flight to Warwick Airport. Fuel calculations based on flight times and expected consumption rates indicated that, at the time of the accident, the aircraft probably had about 1,280 L of fuel on board. This meant the aircraft weight at the time of the accident was about 600 kg below the aircraft’s maximum take-off weight. Based on the survey flying configuration and loading of the aircraft, the aircraft’s centre of gravity was calculated and assessed to be within prescribed limits.
Performance
The pilot operating handbook airplane flight manual (POH) provided applicable limitations which included:
a stall speed[8] of 75 KIAS[9] in the landing configuration (VSO), and 94 KIAS with flaps in the up position (VS)
an intentional one engine inoperative speed (VSSE)[10] of 98 KIAS
an air minimum control speed (VMCA)[11] of 90 KIAS
a one engine inoperative best rate-of-climb speed at sea level (VYSE) of 108 KIAS.
One engine inoperative procedures
The POH included recommended procedures in the event of an emergency. This included checklists for an engine failure in flight, and for the conduct of an approach and missed approach with one engine inoperative. The recommended approach speed with an engine inoperative was 110 KIAS reducing to 101 KIAS only once landing was assured.
Site and wreckage information
Accident site
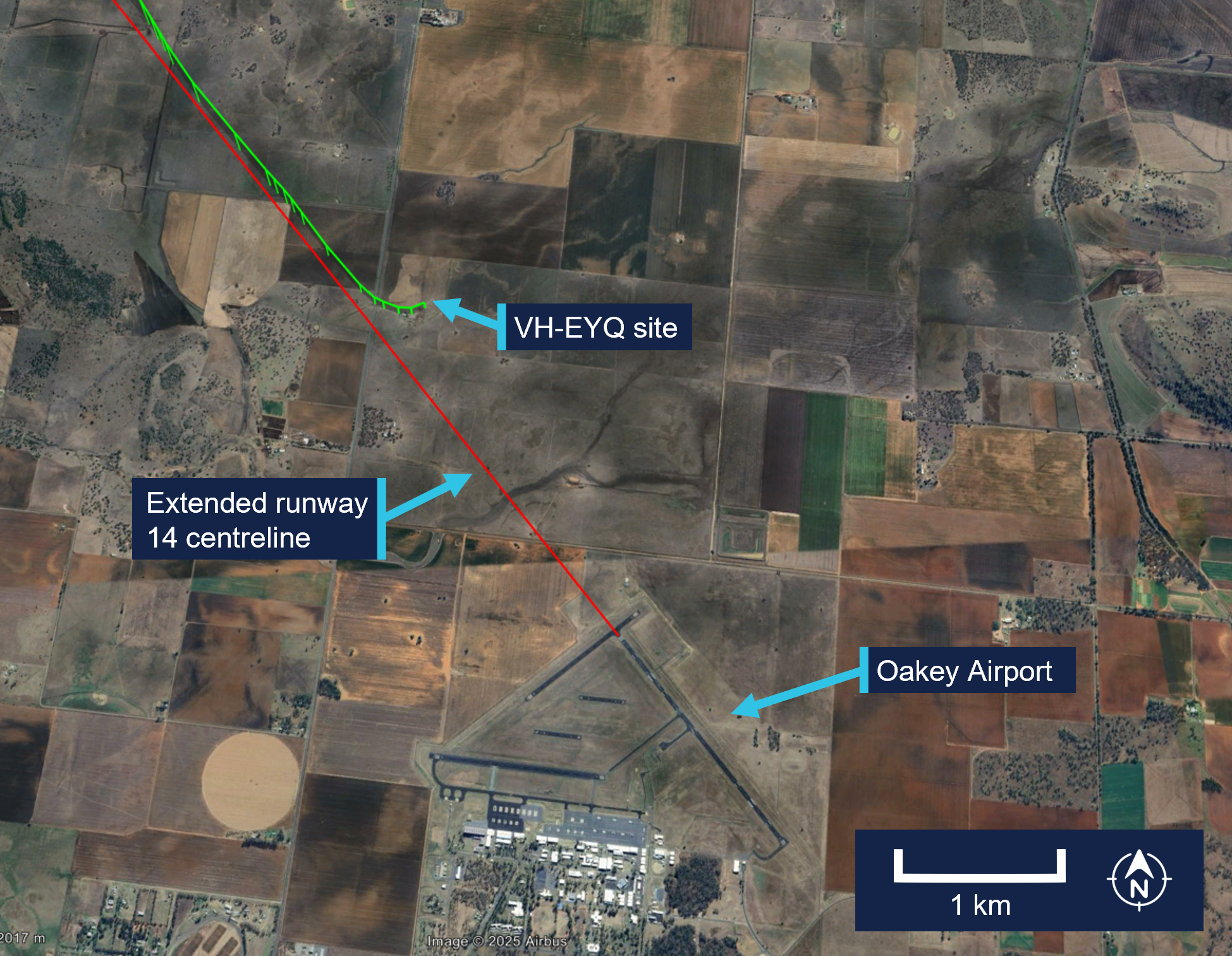
The ATSB conducted an onsite examination of the aircraft wreckage, which was located in an open paddock about 2.6 km from the threshold of runway 14 at Oakey Airport (Figure 8).
Figure 8: Location of accident
Source: Google Earth, annotated by the ATSB
The wreckage was confined to a 30 m radius of the accident site. The impact marks and wreckage position indicated the aircraft impacted terrain left wing low with little forward momentum. Ground scars indicated the aircraft moved about 6 m after the initial impact. All components were upright.
The tail and aft cabin section showed signs of vertical compression. There was no fore or aft compression damage to the nose or wings. The left wing had separated from the aircraft just outboard of the left engine, and the right wing had separated just inboard of the right engine. Both wings had swung forward to lay parallel to the fuselage (Figure 9).
Figure 9: VH-EYQ accident site
Source: ATSB
All major aircraft components were accounted for at the point of impact. A post‑impact fire consumed the forward section of the aircraft to the aft cabin door (Figure 10). This damage limited the extent to which pre-impact defects could be identified.
Figure 10: VH-EYQ wreckage
Source: ATSB
Engines
Both engines were retained for further examination. This was conducted by ATSB investigators who were assisted by investigators from Pratt & Whitney Canada.[12] The engine examination determined:
there were no indications of pre-impact mechanical anomalies to any of the engine components that would have precluded normal engine operation
the left engine displayed indications that it was rotating at the time of impact
the right engine displayed characteristics that it was developing power at the time of impact.
Propellers
Both propellers showed indications that the engines were running at impact. The right propeller was determined to be in a fine pitch position[13] and exhibited bending in multiple directions.
Both propellers were retained, and an independent inspection was carried out at a propeller overhaul facility under the direction of ATSB investigators. Further analysis is required to determine the position of the left propeller at the time of impact.
Meteorological information
The Bureau of Meteorology (BoM) graphical area forecast valid at the time of the accident included the following conditions en route:
scattered cloud bases of 3,000 ft to 5,000 ft, extending up to 8,000 ft
isolated showers of rain with broken cloud from 1,000 ft to 2,000 ft and scattered cloud from 2,000 ft to above 10,000 ft.
At 1500, at about the same time the aircraft impacted terrain, the BoM issued a meteorological aerodrome report for Oakey Airport which reported the conditions at that time were:
a wind of 6 kt, with a mean direction of 190°M, varying between 160°M–220°M
Satellite images and CCTV footage captured areas of scattered cloud in the vicinity of the aerodrome at the time of the approach.
Flight activity
General
For a pilot to operate an aircraft under the instrument flight rules, they are required to hold an instrument rating. Pilots are also required to pass an annual instrument proficiency check (IPC) flight to ensure that they maintain the necessary skills and competency to operate safely. The purpose of the accident flight was for the pilot to complete their annual IPC.
An IPC can be completed by a flight examiner with an instrument rating, MPL[15] or ATPL (aeroplane) flight test endorsement, or by a person approved by CASA. While the aircraft operator had a training and checking system,[16] they scheduled IPC flights with external examiners and permitted the pilots to arrange their IPC flights privately. The head of flying operations (HOFO) of the aircraft operator recalled that the accident pilot had advised them that their IPC expiry date was approaching and requested the use of VH‑EYQ to complete the flight. In response, provisions were made by the HOFO and head of aircraft airworthiness and maintenance control delegate to make the aircraft available to the pilot for the purpose of conducting the IPC flight.
The pilot arranged the IPC with the external flight examiner and records show that the IPC was booked into the CASA flight test management system[17] by the flight examiner during the afternoon of 18 July and scheduled to take place on the afternoon of 20 July.
Instrument proficiency check assessment
During an IPC flight, a pilot’s competency is assessed in actual or simulated instrument meteorological conditions. During the flight, a pilot is required to meet specified standards for:
departure
en route skills
arrival
approach
missed approach
approach to land manoeuvres.
If the IPC is for multi-engine operations, the assessment also requires the satisfactory completion of a simulated one engine inoperative (OEI) departure and a simulated OEI approach.
The HOFO of the aircraft operator recalled that the external flight examiner had, in the past, typically conducted the simulated OEI departure after take-off from Warwick Airport and the simulated OEI approach at Oakey Airport.
Recorded information
Recorded flight data
The aircraft was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to be. During the accident flight, data was being transmitted by the aircraft’s automatic dependent surveillance broadcast (ADS-B) equipment. This data, recorded at 2–5 second intervals by amateur ground-based receivers, captured the aircraft’s position, altitude and groundspeed during the flight. Flight data was also being transmitted from a Spidertracks[18]tracking device fitted to the aircraft. This data, recorded at 15-second intervals, captured the aircraft’s position, altitude, groundspeed and heading during the flight.
The ADS-B altitude and groundspeed data for the aircraft’s departure from Warwick Airport is depicted in Figure 11.
Figure 11: VH-EYQ altitude and groundspeed during the Warwick Airport departure
Source: ATSB
The ADS-B altitude and groundspeed data for the aircraft’s ILS approach at Oakey Airport is depicted in Figure 12.
Figure 12: VH-EYQ altitude and groundspeed during the Oakey Airport approach
Source: ATSB
A Garmin GTN-650 global positioning system was also recovered from the accident site and transported to the ATSB’s Canberra technical facility for further examination. The unit showed signs of significant heat damage with melting and evidence of charring on the internal circuitry. The remains of 2 SD[19] cards were found within the unit, however, the post-impact fire had damaged the SD card memory chips to the point that data could not be extracted using normal recovery methods.
Record radio communications
All radio communications made and received by Airservices Australia throughout the entirety of VH-EYQ’s flight from Warwick Airport were recorded.
Recorded CCTV footage
Two CCTV cameras captured footage of the aircraft immediately prior to the collision with terrain. One camera was located on a property 1.4 km to the north-west of the accident and the second camera was located on Oakey Airport about 3 km south of the accident site.
The property CCTV footage was timestamped. The aircraft entered frame at 1459:53 and remained in frame for the duration of the recording which captured the collision with terrain at 1500:00.
The Oakey Airport CCTV footage did not contain a timestamp. The aircraft entered frame 1 second into the recording and remained in frame until the collision with terrain that occurred 7 seconds later.
Further investigation
To date, the ATSB has:
examined the wreckage and accident site
examined meteorological information
interviewed relevant parties
collected radio communication, aircraft traffic surveillance data, and navigational application data
collected aircraft, pilot, crew and operator documentation.
The investigation is continuing and will include review and examination of:
pilots’ recent history
propellers
maintenance records
pilot and crew training and medical records
operational procedures and documentation
further interviews with relevant parties
flight data and air traffic surveillance data
the requirements of conducting simulated one engine inoperative exercises at low heights.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB would like to acknowledge the assistance provided by the Australian Defence Force personnel at the Oakey Army Aviation Centre during the initial evidence collection activities.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument proficiency check: an assessment of a pilot’s skills and operational knowledge required to exercise licence ratings and privileges when flying under the instrument flight rules.
[2]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
[3]Reporting point: a specified geographical location in relation to which the position of an aircraft can be reported.
[4]Instrument landing system (ILS): a precision instrument approach system which normally consists of a VHF localiser providing horizontal guidance and a UHF glideslope providing vertical guidance.
[5]Glideslope: a component of the instrument landing system providing vertical (up/down) guidance toward the runway touchdown point, usually at a 3° slope.
[6]The provided CTAF recording was found to have a discrepancy that could not be resolved.
[7]Yaw: the motion of an aircraft about its vertical or normal axis.
[8]Aerodynamic stall: or stall, occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16˚ to 18˚, and results in reduced lift.
[9]KIAS: indicated airspeed expressed in knots, used by pilots as a reference for all aircraft manoeuvres.
[10]The manufacturer’s minimum speed for rendering one engine inoperative in flight for pilot training.
[11]The minimum indicated airspeed at which the aircraft was laterally controllable with one engine inoperative and a 5° bank angle towards the operative engine.
[12]Pratt & Whitney Canada: engine manufacturer of the engines installed on VH-EYQ.
[13]Fine pitch: refers to a fine or low pitch angle which yields good low speed acceleration.
[14]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[16]Training and checking system: a training and checking system ensures that operational safety-critical personnel are proficient in the required competencies to support an operator's air operations.
[17]Flight test management system: online record system used to notify CASA of planned flight tests. Flight examiners also use the system to schedule and record the outcomes of flight tests and proficiency checks. The system is used by CASA to keep track of the flight testing process and analyse trends at industry level.
[18]Spidertracks: a satellite-based tracking system, combining satellite communication and GPS technology.
[19]Secure digital card (SD): a type of memory card typically used in portable devices.
Occurrence summary
Investigation number
AO-2025-042
Occurrence date
20/07/2025
Occurrence time and timezone
15:00 Australian Eastern Standard Time
Location
3.4 km north of Oakey Airport
State
Queensland
Report release date
10/12/2025
Report status
Preliminary
Anticipated completion
Q4 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Loss of control
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Reims Aviation S.A.
Model
F406
Registration
VH-EYQ
Serial number
F406-0047
Aircraft operator
Bayswater Road Pty Ltd (trading as Aero Logistics)
Sector
Turboprop
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Instructional flying-Instructional flying - dual
On 15 July 2025, a Beechcraft 35-C33 Debonair, registered VH-KZK, departed Wangaratta Airport, Victoria for a private flight under the visual flight rules (VFR) to Moruya Airport, New South Wales.
Soon after entering the Snowy Mountains area, the aircraft made a 150° right turn, shortly followed by another long left turn. The aircraft entered a spiralling descent to the right that continued until the aircraft collided with terrain. The pilot was fatally injured and the aircraft was destroyed.
What the ATSB found
It is very likely that the pilot, who did not hold an aircraft instrument rating, experienced spatial disorientation after flying into instrument meteorological conditions (IMC). This subsequently resulted in the collision with terrain.
Based on the forecast cloud between Wangaratta and Moruya, completing such a flight while maintaining VFR was likely not feasible. The pilot held a recreational pilot licence that did not include a navigation endorsement. While the pilot had completed some of the training required to attain a navigation endorsement, it is possible that the pilot’s limited training and experience in this respect affected their decision to conduct or continue the flight into challenging weather conditions.
Safety message
One of the key risk controls for a VFR pilot to avoid entering IMC is appropriate pre-flight preparation and planning. Not only should pilots obtain up-to-date weather information before and during flight, they should plan an alternate landing point and be prepared to make necessary deviations from the planned route should actual weather conditions necessitate it.
Licence restrictions and endorsements are a critical aspect of flight safety. They ensure that pilots have been trained to an acceptable standard and that the appropriate experience has been attained. Studies show that pilots with less weather experience are more likely to engage in high-risk activities when dealing with weather. This accident is an important reminder to respect these restrictions and endorsements when planning a flight.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 15 July 2025, the pilot and sole occupant of a Beechcraft 35-C33 Debonair, registered VH-KZK, was conducting a private flight under the visual flight rules (VFR)[1] from Wangaratta Airport, Victoria, to Moruya Airport, New South Wales. The pilot was returning to Moruya following the completion of routine maintenance on the aircraft.
It is not known what weather information was accessed by the pilot prior to departing Wangaratta, as no flight planning records were recovered. Text messages from the pilot at 0755 on the morning of the accident flight indicated that they were conducting flight planning and considering the weather on the morning of the accident flight, noting that ‘the sky outside is scattered clouds so we will see what the planning forecast is.’
A flight path recreated from automatic dependant surveillance broadcast (ADS-B) transmissions is shown in Figure 1. The pilot departed Wangaratta at 1302 and flew approximately east towards Moruya, 189 NM away, making occasional changes in heading. By 1315 the aircraft had climbed to an altitude of 4,500 ft above mean sea level (AMSL), where it remained until it approached the rising terrain of the Snowy Mountains, where the aircraft began climbing to 7,000 ft. The mountainous area along the aircraft’s flight path had varying terrain heights, with a maximum of approximately 6,000 ft AMSL.
Figure 1: Flight path of VH-KZK on 15 July 2025
Source: Google Earth, annotated by the ATSB
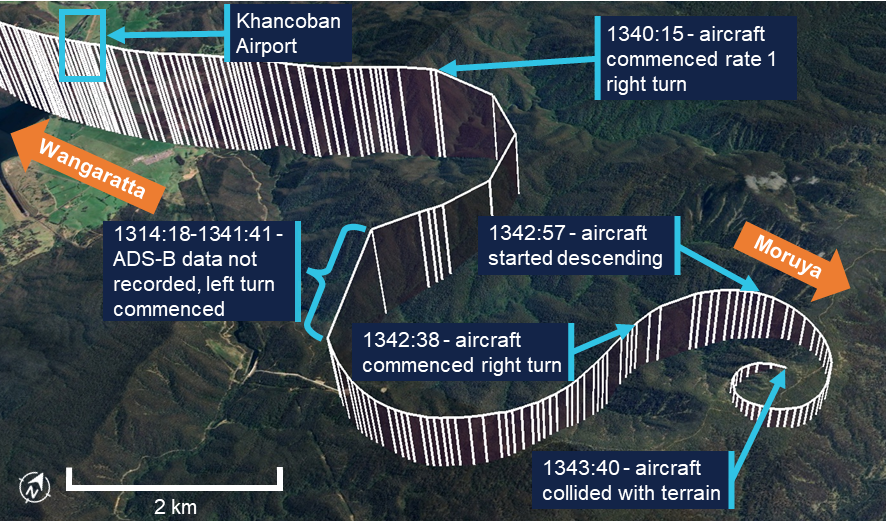
The aircraft flew past a small aerodrome, Khancoban Airport,[2] at about 1339 at an altitude of about 6,400 ft AMSL (Figure 2). At 1340:15, the pilot commenced a rate 1 turn[3] to the right with minimal change in altitude. At 1341:18, after turning through 150°, there was a 20-second period where ADS-B transmissions were not received. The aircraft was subsequently detected in a left turn through 206°, also approximately rate 1. An airspeed of approximately 150 kt was maintained through these turns.
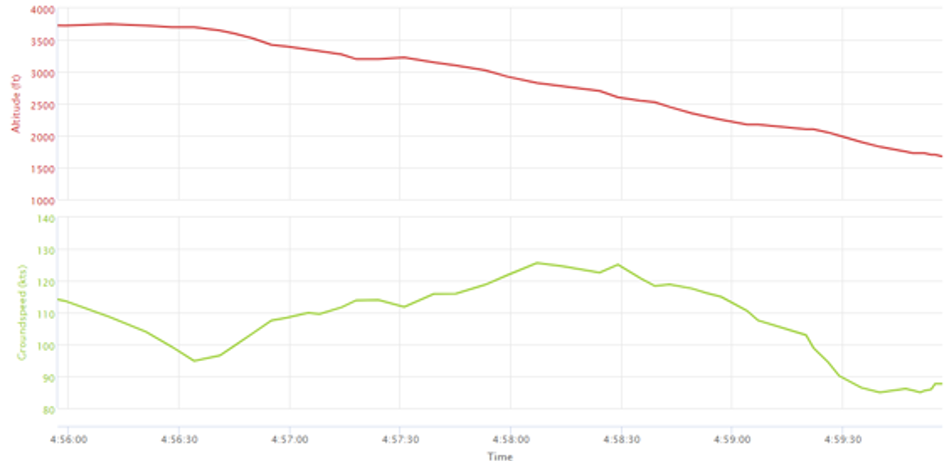
Figure 2: Flight path prior to colliding with terrain
Vertical lines are used to indicate the aircraft’s height above terrain. Each line represents a data point. Source: Google Earth, annotated by the ATSB
At approximately 1342:38, the aircraft entered another right turn and shortly after, began descending from 6,725 ft AMSL. From this point, the aircraft’s rate of turn, descent rate and groundspeed all steadily increased into a spiralling descent. The last ADS-B transmission was recorded 55 ft above ground level, with an estimated airspeed of 210 kt and a rate of descent above 4,000 ft/min. At 1343:40, the aircraft collided with terrain at an elevation of 4,830 ft AMSL. The pilot was fatally injured and the aircraft was destroyed.
The pilot had lodged a search and rescue time (SARTIME) with Airservices Australia, and when this time elapsed the Joint Rescue Coordination Centre (JRCC) was notified and commenced a search. The aircraft was not fitted with an emergency locator transmitter (ELT), and poor weather conditions limited JRCC search capabilities. Visibility was affected by cloud, and in the early stages of the search, helicopters had limited access to the area where the aircraft was last detected on ADS-B. After an extended search by air, the aircraft was located on 17 July in steep, forested terrain with snow cover.
Context
Pilot information
General information
The pilot held a Recreational Pilot (Aeroplane) Licence (RPL) with a single engine aeroplane class rating and a flight radio endorsement. The RPL permitted private or training flights by day under VFR. The pilot was issued with a basic class 2 aviation medical certificate that was valid until February 2026. The basic class 2 medical certificate was an alternative to a full class 2 certificate for RPL and Private Pilot Licence (PPL) holders. It imposed additional operational restrictions, including that the pilot was not permitted to fly above 10,000 ft.
The pilot’s next of kin reported no relevant medical conditions or medications. There was evidence that the pilot had up to about 9 hours sleep opportunity the night before the flight, but there was insufficient information available to assess fatigue.
Toxicology and pathology reports were not available at the time of publishing this report.
Training and experience
The ATSB estimated[4] the pilot had completed 142 hours total flight time, including 28 hours of solo flying. The pilot had an estimated 25 hours of flight experience in the Beechcraft 35-C33 Debonair, entirely in VH-KZK (which they owned), including 10 hours of solo flying.
The pilot did not have an RPL navigation endorsement, which meant they were restricted from flying beyond 25 NM of the departure aerodrome, unless it was to travel to a training area. Obtaining the navigation endorsement required completion of specific flying training and passing a written examination. The Civil Aviation Safety Authority (CASA) website stated that the examination covered a range of topics including:
• maps and charts properties
• forecast requirements and interpretation of forecasts, determination of alternate or holding requirements.
The pilot had received some navigation training, which included several navigation exercises, as well as a solo navigation flight. Including that flight, the pilot had completed 4 exercises within the standard PPL syllabus. Two additional dual exercises and 1 final long solo navigation exercise were required before an RPL navigation endorsement could be sought. During the training, with regard to flight planning, the pilot was assessed as having achieved ‘competency to the standard required for qualification issue’. Flight planning included the following elements:
• select a suitable route and altitude considering weather, terrain, airspace, NOTAMs[5] and alternate landing areas
• obtain and interpret meteorological forecasts, NOTAMs and operational information applicable to the planned flight
• determine whether the planned flight can be conducted under the applicable flight rules and taking account of the beginning and end of daylight times.
In total, the pilot had accrued 38.1 hours of navigation training, including 1.7 hours flying solo. The pilot had also received 1.0 hours of basic instrument flight training in 2021 on a different aircraft.
Recent flying
The pilot’s most recent formal navigation training was in March 2023. Between November 2023 and October 2024, the pilot undertook training in VH-KZK, having previously flown a Beechcraft C23 Sundowner. Following this training, ADS-B data showed VH-KZK flying (determined to be with this pilot in command) on 9 different occasions between November 2024 and May 2025. All of these flights took place along the New South Wales south coast between Moruya Airport, Merimbula Airport and Frog’s Hollow Airfield (Figure 3). Logbook entries for these flights were not found, but they were understood to be solo flights for pleasure and personal transport.
Figure 3: Aerodromes used by VH-KZK
Source: Google Earth, annotated by the ATSB
On the day before the accident, the pilot conducted a solo navigation flight from Frog’s Hollow to Wangaratta Airport where the aircraft was booked in for routine maintenance. Weather forecasts from the area predicted a cloud ceiling of 7,000 ft and scattered cloud. ADS-B data showed that the pilot conducted most of the flight at an altitude of 9,000 ft, above the forecast cloud tops. The flight appeared to be conducted without incident.
Aircraft information
The Beechcraft 35-C33 Debonair is a low-wing, 4-seat, all-metal aircraft with retractable tricycle landing gear. The Debonair, with a conventional vertical fin and tailplane, was a variant of the early Beechcraft Bonanza model, which had a distinctive V-tail. VH-KZK, serial number CD-985, was manufactured in 1967 in the United States and first registered in Australia in the same year. It was powered by a 6-cylinder Teledyne-Continental Motors IO-470-K engine driving a McCauley 2A36C23 constant-speed propeller. The aircraft was fitted with a pitot heat system.
The aircraft had been classified as capable of operating under the instrument flight rules (IFR) in September 2019. A review of the expired maintenance releases identified that the aircraft shifted between IFR and VFR categories, depending on IFR inspection status. The last IFR inspection recorded in the aircraft logbook was completed on 4 May 2023, with the maintenance release showing the IFR category selected. The current maintainer, who first inspected the aircraft in June 2024, reported that, due to uncertainty around the certification of the equipment, the IFR category was not indicated on the previous 2 maintenance releases.
The aircraft was being maintained in accordance with the standard CASA maintenance schedule (Schedule 5), which required a periodic inspection every 100 flight hours or 12 months, whichever came first. The most recent periodic inspection was completed on 15 July 2025, with the aircraft having accrued 17.5 hours in the previous 12 months. In addition to the periodic inspection requirements, the 2 main tyres were replaced. A new maintenance release was issued with the aircraft having accrued 3,279 hours total time in service.
Maintenance records indicated that an emergency locator transmitter (ELT) was removed from the aircraft in 2019. The maintainer confirmed that there was no ELT fitted to VH-KZK.
Wreckage and impact information
Access to the accident site was limited due to the terrain, snow and environmental conditions, and the ATSB did not attend the accident site. New South Wales Police Force personnel who winched to the site via helicopter to recover the pilot took photographs and collected physical evidence, including documentation and potential data recording devices, which were later examined by the ATSB.
The aircraft was significantly disrupted (Figure 4), consistent with the estimated final aircraft speed of 210 kt and a vertical rate of descent of over 4,000 ft/min. The impact was not survivable. Accident site photographs indicated that the wreckage was relatively contained, rather than spread over a long wreckage trail. This was consistent with the steep descent indicated by the flight data. The engine had separated from the aircraft wreckage and was located 10–15 m away. From the photographs, it was not possible to determine conditions such as aircraft configuration, control cable continuity or the state of control surfaces. It also could not be determined whether all components remained attached up to the point of impact.
Figure 4: Wreckage of VH-KZK
Source: New South Wales Police Force
Meteorological information
Aerodrome weather
The aerodromes closest to the accident site were Khancoban Airport and Corryong Airport (7 NM and 18 NM west of the accident site, respectively). Corryong did not provide meteorological observations and Khancoban had a non-aviation automatic weather station which did not report cloud or visibility. However, records for Albury Airport (Figure 3), which VH-KZK passed earlier in the flight, indicated that the following conditions existed at 1330:
visibility greater than 10 km
9 kt westerly wind
no precipitation
broken cloud at 4,600 ft AGL (5,100 ft AMSL).
Weather forecasts
The Bureau of Meteorology (BoM) issued a set of graphical area forecasts (GAFs) at 0820 on the morning of the accident flight. Based on the flight data, the aircraft’s flight path would have passed through 3 areas with varying forecast conditions.
For the initial part of the flight, beginning at Wangaratta and approaching the Victoria/New South Wales border, the terrain elevation along the flight path varied between about 500 and 3,800 ft AMSL. On this segment the following conditions were forecast (all altitudes are AMSL):
a broken[6] cloud layer from 1,000–2,000 ft that was forecast to clear by about the aircraft’s departure time
broken cloud from 3,000–8,000 ft
isolated showers of rain, during which visibility would reduce to 4,000 m and cloud would extend from 800 ft to above 10,000 ft
isolated showers of snow above 4,000 ft during which visibility would reduce to 500 m and cloud would extend to 8,000 ft
freezing level above 4,500 ft.
After crossing into New South Wales and over the Snowy Mountains, just beyond Khancoban, the flight overflew mountainous terrain where the elevation increased to between 600 and 6,000 ft. In this region the forecast was for:
scattered[7] cloud from 1,500–3,000 ft and broken cloud from 3,000 ft to above 10,000 ft
scattered areas of drizzle with visibility reducing to 3,000 m and overcast conditions from 3,000 ft to 9,000 ft
isolated showers of snow above 4,000 ft with broken cloud from 4,000 ft to above 10,000 ft
freezing level above 4,500 ft.
The accident occurred within this region of the GAF. East of the highest terrain in the Snowy Mountains, conditions were forecast to improve slightly:
scattered cloud from 2,500–8,000 ft
broken cloud from 6,000 ft to above 10,000 ft.
Satellite imagery
A satellite photograph taken at 1340, less than 4 minutes before the aircraft collided with terrain, showed cloud cover in the vicinity of the accident site (Figure 5). However, the image provided no information on cloud height or density.
Figure 5: Satellite image from 1340 on 15 July
Source: Bureau of Meteorology, annotated by the ATSB.
Witness report
A witness with an aviation background was located near Khancoban Airport around the time of the occurrence. They reported hearing an aircraft in the area that they later believed to be VH-KZK. The witness could not see the aircraft due to cloud, but noted that it sounded as if it was heading towards the mountains east of Khancoban. The witness said the aircraft sounded like it was much lower than aircraft travelling over the mountains at this point would typically be (9,000 ft AMSL); the witness estimated the aircraft to be travelling at about 4,000 ft AMSL.
The witness observed the weather to be completely overcast. The cloud was low enough to be sitting on nearby hilltops, the peaks of which the witness believed to be between 2,500-3,000 ft AMSL.
Icing conditions
BoM forecasts note that flying in any cloud above the freezing level implies moderate icing conditions. The BoM publication titled Airframe Icing advises pilots on the effects that icing can have on an aircraft. It states that icing can:
alter the smooth flow of air over the aircraft
reduce pilot visibility
produce errors in instrument readings of air speed, altitude and vertical speed
increase the stall speed by increasing its weight and changing the aerodynamics of the wing and tail
increase drag and decrease lift (tests have shown that icing no thicker or rougher than a piece of coarse sandpaper can reduce lift by 30% and increase drag by 40%)
make it almost impossible to operate control surfaces and landing gear
reduce thrust or cause engine failure.
Because VH-KZK was fitted with a pitot heat system, and a fuel-injected engine, the most likely adverse outcomes from icing involved ice forming on the exterior parts of the airframe. According to the BoM, this type of icing is caused by water droplets from cloud or precipitation striking the airframe at temperatures below the freezing level.
Operational information
Visual meteorological conditions
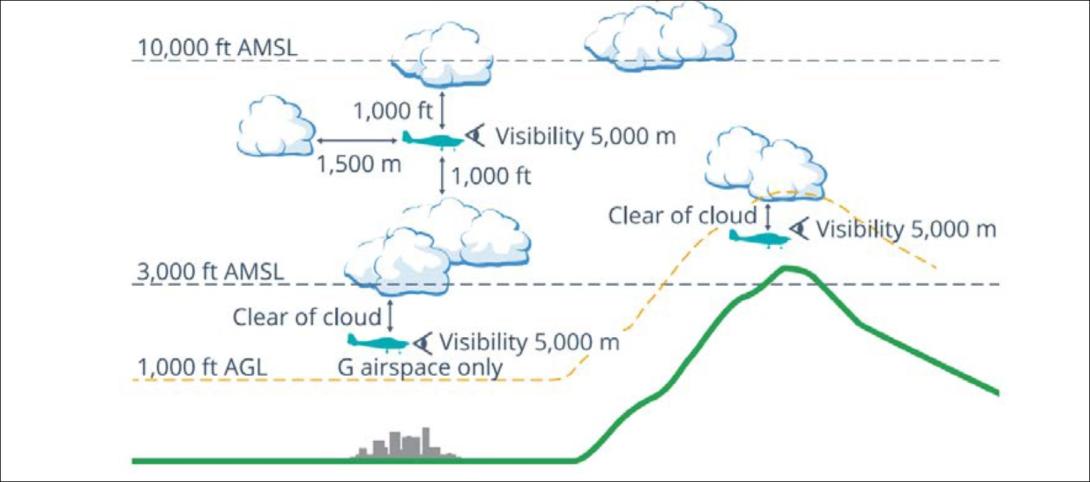
Visual meteorological conditions (VMC) are expressed in terms of in-flight visibility and distance from cloud (horizontal and vertical) as prescribed in the Civil Aviation Safety Regulations (CASR) Part 91 General Operating and Flight Rules. The accident flight was conducted entirely in uncontrolled (Class G) airspace. In order for the pilot to conduct such a flight under VFR while remaining below 10,000 ft (in accordance with licence requirements), the following VMC criteria needed to be maintained at all times:
5,000 m visibility with 1,000 ft vertical and 1,500 m horizontal distance from cloud
When below the higher of 3,000 ft AMSL or 1,000 ft AGL and in sight of ground or water, the aircraft may be just clear of cloud.
These criteria were illustrated in the CASA Visual Flight Rules Guide (Figure 6). Generally speaking, aircraft flying in conditions that do not meet these criteria are in instrument meteorological conditions (IMC).
Figure 6: Visual meteorological conditions (VMC) criteria below 10,000 ft
Source: Civil Aviation Safety Authority
Flight planning requirements
Flight rules required that pilots study the appropriate authorised weather forecasts and reports in accordance with the CASR Part 91 Manual of Standards. This included authorised weather forecasts and reports for:
the route to be flown
the departure aerodrome, the planned destination aerodrome and any planned alternate aerodrome.
Improving the odds
In 2010 the ATSB published Improving the odds: Trends in fatal and non-fatal accidents in private flying operations (AR-2008-045), which found that assessing and planning problems contributed to 46% of fatal accidents involving Australian private flights between 1999 and 2008. The report stated that:
Assessing and planning issues associated with collision with terrain and/or loss of control accidents mostly involved pilots failing to plan for the weather conditions, not properly assessing the weather during flight, or deciding to continue to fly in marginal weather.
The report provided extensive discussion (pages 16 through 21) on topics including ways of avoiding VFR into IMC accidents, such as through emphasising assessment of flight conditions (particularly weather conditions), evaluating effectiveness of plans, and setting personal minimums.
Spatial disorientation
The ATSB publication Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions (AR-2011-050) discusses the physiological limitations of the human body when trying to sense its orientation in space:
In conditions where visual cues are poor or absent, such as in poor weather, up to 80 per cent of the normal orientation information is missing. Humans are then forced to rely on the remaining 20 per cent, which is split equally between the vestibular system and the somatic system. Both of these senses are prone to powerful illusions and misinterpretation in the absence of visual references, which can quickly become overpowering.
Pilots can rapidly become spatially disoriented when they cannot see the horizon. The brain receives conflicting or ambiguous information from the sensory systems, resulting in a state of confusion that can rapidly lead to incorrect control inputs and resultant loss of aircraft control.
The somatogyral illusion is one possible consequence of spatial disorientation, described in the ATSB publication Visual flight at night accidents: What you can’t see can still hurt you (
This illusion relates to a pilot’s incorrect understanding of an aircraft’s angle of bank. When the angle of bank is changed, the pilot’s vestibular system will register any angular acceleration above a threshold level of activation. Once the aircraft is in a constant turn, the pilot’s vestibular system will stop registering any input because there is no angular acceleration. In the absence of any other sensory information or vestibular input a pilot may experience a sensation that the aircraft is no longer turning.
The CASA publication titled Spatial disorientation was published in 2024 as part of the AvSafety program. This detailed several commonly observed illusions that pilots can experience as a result of spatial disorientation. The ‘Graveyard spiral’ described in the publication can occur as a result of the somatogyral illusion:
This can happen when an aircraft begins to bank in cloud or dark night conditions. A constant rate of bank will be undetectable by the vestibular apparatus in a pilot’s head, and unless the pilot is scanning the attitude indicator continuously there will be no visual clue. Rushing slipstream will indicate the increasing airspeed of a dive in what otherwise appears to be straight-and-level flight. Attempts to pull out of the dive often only tighten the unrecognised turn and can cause overstressing and failure of the aircraft structure.
For non-instrument rated pilots, entering IMC can quickly become fatal. Research has shown that pilots not proficient in instrument-only flight will typically become spatially disoriented and lose control of the aircraft within 1–3 minutes after visual cues are lost.
Between 2015 and 2025 there were 116 VFR into IMC occurrences in Australian airspace reported to the ATSB. Of these, 13 were fatal accidents resulting in 24 fatalities. Based on these figures, approximately 1 in every 9 reported VFR into IMC occurrences results in a fatality.
Safety analysis
Spiral descent
The aircraft’s steadily increasing rate of descent and rate of turn in the period leading up to the impact with terrain were consistent with spatial disorientation, specifically, the somatogyral illusion and the ‘graveyard spiral’ described by CASA and others.
Broken cloud was forecast in the mountains east of Khancoban between 3,000 ft AMSL to above 10,000 ft AMSL. There were also areas of drizzle with overcast conditions between 3,000 ft and 9,000 ft AMSL. The report from the witness near Khancoban airport indicated local conditions consistent with this forecast. Given the terrain elevation in the area, it is therefore almost certain that the aircraft encountered weather conditions making visibility marginal or worse, possibly for extended periods.
The aircraft’s increasing rate of descent and maximum allowable airspeed exceedance just before the collision with terrain indicated that the pilot was either not aware of the aircraft’s speed and attitude, or was not able to correct it during the descent.
The pilot held a valid basic class 2 medical certificate and there was no available evidence to indicate any medical conditions likely to impact their flying ability, although an incapacitating medical event could not be entirely ruled out.
Prior to the spiral descent, the aircraft maintained a steady altitude and groundspeed, which did not indicate any engine or control issues to that point. An engine issue by itself should also not result in a high-speed, spiralling descent, unless there was also a control issue present. Control issues could not be entirely ruled out, since the wreckage was not examined, and photographs were insufficient to determine aspects such as control cable continuity or the presence of all control surfaces.
Aircraft icing was another possibility. It can affect a number of aspects relating to aircraft performance, handling or pilot visibility, and multiple control surfaces jammed by ice at the same time could result in an uncontrolled spiral flightpath. Structural icing would only be expected if the aircraft was in cloud or precipitation. In either case, based on the forecast, the aircraft would be in IMC where spatial disorientation would also be a concern.
In either case, the aircraft’s flight path, including what appear to be 2 controlled turns beyond Khancoban, indicates that the aircraft remained controllable until at least the commencement of the spiral. The manoeuvres also indicate that the pilot deliberately left the planned flight route, and were consistent with attempts to navigate around cloud or showers and possibly find a landing area. For example, the first turn might have been an attempt to return to Khancoban or another airport such as Corryong or Wangaratta, and the second turn the result of cloud closing in behind the aircraft, preventing such a return.
Considering the weather conditions on the day, the pilot’s limited training and experience, and the proven hazard of entering IMC as a VFR pilot, it is therefore very likely that the pilot experienced spatial disorientation in low-visibility conditions, leading to an undetected spiral descent.
VFR into IMC
Just beyond Khancoban, the weather forecast indicated that broken cloud was expected from ground level (above 3,000 ft AMSL) up to above 10,000 ft AMSL. The vertical extent of the cloud would have made this particularly challenging for the pilot because it was probably not possible to fly above the broken cloud and remain under 10,000 ft in accordance with licence restrictions.
Because there were no weather stations recording observations near the accident site, the actual weather conditions that the pilot encountered could not be determined beyond a single witness account (at ground level) and a satellite image that shows cloud in the area. While the conditions might have differed from the weather forecast, the forecast conditions indicated that a pilot would have no certainty of maintaining VFR. The pilot was not IFR rated and training records indicated that they had only flown 1 hour of instrument flight training.
While the pilot had completed some navigation training including a solo navigation flight, they were yet to complete the training syllabus necessary to obtain a navigation endorsement for their recreational pilot licence. As such, they were not authorised to fly the 189 NM distance between Wangaratta and Moruya. Additionally, while the pilot had received training and been assessed as competent at reading weather forecasts in an aviation context, they likely had limited experience in this respect and had not been assessed on some relevant elements required for the PPL such as the more advanced interpretation of forecasts, and determination of alternate or holding requirements. This increased the likelihood of misinterpreting the forecast or underestimating the difficulty of navigating the forecast conditions.
There is limited information available to establish the extent or specifics of the pilot’s pre-flight planning. The exact weather scene presented to the pilot upon entering the mountains was not known, nor was the pilot’s decision-making regarding initiation and continuation of the flight.
The number of reported VFR into IMC occurrences over the last 10 years indicates that many pilots, some likely with more experience, have found themselves in unsuitable weather situations yet continued the flight. However, studies have shown that pilots who do not accurately perceive the risks of adverse weather are more likely to engage in higher risk activities when dealing with weather (Cooper, 2003). The pilot’s limited training and experience with adverse weather conditions may therefore have contributed to their perception of risk and associated decision-making.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the VFR into IMC and collision with terrain involving Beechcraft 35-C33 Debonair VH-KZK, 12 km east of Khancoban, New South Wales on 15 July 2025.
Contributing factors
The pilot very likely encountered instrument meteorological conditions, resulting in spatial disorientation and collision with terrain.
The pilot commenced a solo navigation flight, into areas with forecast instrument meteorological conditions, without having completed the required training and licensing for cross-country navigation.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Cooper D. (2003). Psychology, Risk and Safety: Understanding how personality & perception can influence risk taking. Professional Safety. Journal of the American Society of Safety Engineers, November 2003, 39-46.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
Australian Maritime Safety Authority
Bureau of Meteorology
the pilot’s flight instructor.
Submissions were received from:
Civil Aviation Safety Authority
Bureau of Meteorology
the pilot’s flight instructor.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): regulations that permit a pilot to operate an aircraft in conditions whereby navigation and orientation of the aircraft by visual reference is possible.
[2]Khancoban Airport did not have an entry in the Airservices aeronautical information publication (AIP) en route supplement Australia (ERSA).
[3]A rate 1 turn, also known as a standard rate turn, is turn rate of 3° per second.
[4]The pilot’s logbook was not located. However, a copy of the pilot’s logbook with entries up until February 2023 was obtained. The ATSB also collated training records and publicly available flight data of the accident aircraft to estimate the pilot’s hours and experience.
[5]Notice to airmen (NOTAM): A notice distributed by means of telecommunication containing information concerning the
establishment, condition or change in any aeronautical facility, service, procedure or hazard, the timely knowledge of
which is essential to personnel concerned with flight operations.
[6]Broken cloud refers to cloud that covers between 5 to 7 oktas (eighths) of the sky.
[7]Scattered cloud refers to cloud that covers between 3 to 4 oktas (eighths) of the sky.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
At about 0947 local time on 2 June 2025, a Piper PA-28 was returning to Bankstown Airport, New South Wales, from the west via the 2RN radio towers, the inbound reporting point to Bankstown Airport, at the conclusion of a training flight with an instructor and student on board.
Passing slightly to the south of the reporting point (Figure 1) and tracking south‑east at 1,300 ft, the pilot of the PA‑28 made a radio call to Bankstown Tower to request clearance to enter the Bankstown airspace. They were instructed to join the crosswind leg of the circuit for runway 29R, maintaining 1,500 ft. The tower controller also advised the flight crew of traffic behind and to the left of their aircraft, which would pass to their left shortly. Acknowledging these instructions, the pilot of the PA‑28 turned left to take up a north‑easterly track and climbed slightly to 1,500 ft.
At around the same time, a Piper PA‑46 with one pilot and 2 passengers on board was also approaching Bankstown from the west, via the 2RN waypoint. Both the pilot and the front seat passenger held commercial pilot licences. The PA‑46 was operating under the instrument flight rules and was required to leave controlled airspace, enter Class G airspace and contact Bankstown Tower, to get a clearance to enter Class D airspace. As they left controlled airspace, the PA‑46 was advised by the Sydney Centre air traffic controller of traffic to the south‑east of the 2RN waypoint. The pilot visually identified an aircraft but having not heard the inbound call, incorrectly assessed it to be heading away from Bankstown and therefore did not consider there was a threat of collision.
Passing the inbound point on an easterly heading and descending through 2,400 ft, the PA‑46 was about 30 seconds behind the PA‑28 but above it and travelling 60 kt faster.
On switching to the Bankstown Tower frequency, the pilot of the PA‑46 heard the controller passing traffic information on their aircraft to the PA‑28. Consequently, when they made their inbound call, they advised that they were ’keeping an eye out for the Piper’. The controller instructed the PA‑46 to join crosswind for runway 29R and reiterated that there was traffic almost directly below them.
The pilot of the PA‑46 advised that they had sighted the PA‑28, however, while making a left turn to establish the aircraft on a crosswind track, they lost sight of the PA‑28. At around the same time, they noted they were high on the approach and commenced a rapid descent to reach the required height of 1,500 ft. The front seat passenger later advised that they had maintained visual contact with the PA‑28. The ATSB could not determine why this information was not communicated to the pilot at the time of the event.
The PA‑46 overtook the PA‑28 with very little separation, passing just to the left of the slower aircraft and at approximately the same altitude. Recorded ADS‑B data showed that the 2 aircraft came within about 80 m horizontally and about 25–30 ft[1] vertically at their closest point of separation.
The pilot of the PA‑46 reported that as they rolled out of the turn onto the crosswind leg of the circuit, they sighted the PA‑28 in their 2 o’clock[2] position and made an evasive turn to the left. The pilot of the PA‑28 reported that they had insufficient time to take any avoiding action.
Figure 1: Google Earth image of the flight paths
The PA-28 flight path is in red and the PA-46 flight path is in blue. Source: Google Earth with Flightradar24 data, annotated by the ATSB
Both aircraft continued their approaches and landed without further event. At the time of the near collision both aircraft were flying in non‑controlled airspace, and were about to enter the Bankstown Class D airspace.
Safety action
The operator of the PA‑46 reported that they often carry a commercially licenced pilot in the front passenger seat to act as a safety observer. Following the event, the operator has formalised a process for how the observer should communicate their observations and concerns to the pilot during flight.
Safety message
Operating into busy Class D airports such as Bankstown, requires pilots to maintain high levels of situational awareness, especially with respect to other traffic. A mixture of aircraft types of varying performance, converging around inbound reporting points, can create complex and challenging traffic scenarios. As such, these risks should be considered ahead of time.
While ATC will often provide information on other traffic, it is unable to provide positive separation. It remains the responsibility of the pilot to always maintain visual separation from other aircraft. If a pilot is unable to visually sight, or loses sight of, an aircraft they should immediately act to avoid a conflict.
In addition, descending rapidly in close proximity to an inbound reporting point, while not maintaining visual contact with traffic, significantly increases the risk of collision. It may be more appropriate to delay arrival at the reporting point, perhaps by flying an orbit, and descend to a more suitable height, to get a clear understanding of the traffic in the area, prior to approaching the inbound reporting point.
These issues were highlighted in an investigation conducted by the ATSB into a midair collision of 2 aircraft near the 2RN reporting point in 2008 (Midair collision Cessna Aircraft 152, VH‑FMG and Liberty Aerospace XL‑2, VH‑XLY, Casula, New South Wales, 18 December 2008 AO‑2008‑081).
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Position and altitude data from Flightradar24 includes some uncertainty.
[2]O’clock: the clock code is used to denote the direction of an aircraft or surface feature relative to the current heading of the observer’s aircraft, expressed in terms of position on an analogue clock face. Twelve o’clock is ahead while an aircraft observed abeam to the left would be said to be at 9 o’clock.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-021
Occurrence date
02/06/2025
Location
About 7 km west-south-west of Bankstown Airport
State
New South Wales
Occurrence class
Serious Incident
Aviation occurrence category
Near collision
Highest injury level
None
Brief release date
23/07/2025
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-46-500TP
Sector
Turboprop
Operation type
Part 91 General operating and flight rules
Departure point
Sunnyside Aircraft Landing Area, New South Wales
Destination
Bankstown Airport, New South Wales
Damage
Nil
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28-161
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
At about 1730 local time on 3 July 2025, after a repositioning ferry flight to Welcome Station, Queensland, for mustering operations the following day, the pilot and sole occupant of a Robinson R22 Beta helicopter made an approach to land next to a wooden pallet loaded with two 200 L drums of Avgas.[1] The pilot was likely unable to see the position of the left skid in relation to the pallet as they were seated on the right side of the helicopter. They reported that the left skid made contact with the pallet and caused the helicopter to bounce upwards. With no forward movement, the pilot reacted by quickly lowering the collective. They recalled hearing a bang and felt a ‘shimmy’ through the tail rotor pedal controls, which they suspected was the main rotor severing the tail boom.
Figure 1: Helicopter accident site
Source: Operator
The pilot recalled that the helicopter instantly began to rotate in a clockwise direction. The left skid impacted one of the fuel drums on the wooden pallet, and the helicopter rolled and impacted the ground, coming to a stop on its side about 15 m away from the pallet.
ATSB review of images provided by the operator and similar occurrences that involved main rotor blade contact with the tail boom identified that the condition of the tail boom, damage to the tail rotor and vertical stabiliser were consistent with contact with terrain or an object, likely resulting in the tail boom separating from the helicopter. Consistent with the pilot’s recollection, this would result in the helicopter rotating in a clockwise direction.
Figure 2: Occurrence aircraft tail boom
Source: Operator
The pilot extricated themselves from the wreckage and observed that fuel was leaking from the fuel cap. There were no reported injuries, and the pilot was assisted by 3 nearby colleagues to roll the substantially damaged helicopter upright to prevent further fuel spillage.
Safety action
The pilot had accumulated about 9,500 hours flying the R22 helicopter and was familiar with these types of operations.
They reported they would take this opportunity to educate other pilots on the risks posed by objects in close proximity to the helicopter and how quickly an accident can develop when contact is made with a fixed object.
Safety message
This accident highlights the importance of clear visual lookout in respect to obstacles as the helicopter is approaching the ground. This is particularly significant when a pilot is required to land close to refuelling stations where ignition or explosion risks exist.
Pilots should always conduct a thorough reconnaissance of a landing area and, where possible, use ground marshallers to determine any potential hazards, assess the terrain, and identify a safe location to land the helicopter.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Avgas is an aviation fuel used in aircraft with spark-ignited internal combustion engines.
At around 1830 on 10 February 2025, a Sharp Airlines Fairchild SA227, registered VH‑UZN, was being prepared for a freight operations flight from Townsville Airport to Brisbane Airport, Queensland, with 2 crew on board.
The captain conducted an undocumented abbreviated external inspection of the aircraft. Around the same time, the first officer removed engine bungs and static port covers, however, could not reach the pitot tube covers located on the nose of the aircraft. This was communicated to the captain, who advised they would remove them, however, the captain subsequently forgot.
During the take-off run, both crew members recognised that the airspeed indicators were rising slower than anticipated, however, by this time, the captain was uncertain if there was sufficient runway remaining to safely stop the aircraft and elected to continue the take-off. During the climb, the first officer identified that the pitot tube covers have been left installed on the pitot tubes, which they announced to the captain. The crew then returned the aircraft to Townsville for an uneventful landing.
What the ATSB found
The ATSB found that due to a combination of a memory lapse and incorrect assumption the pitot tube covers were not removed prior to departure. It was also identified that the operator’s expectation as to what external aircraft inspection was required prior to this flight was not clearly stated in the procedures. In addition, the operator’s expectation that crews would fit pitot tube covers when the aircraft was unattended on the ground for 60 minutes or longer was inconsistent with its written procedures.
Further, the external security check, required to be completed prior to every flight, did not include ensuring the pitot tube covers had been removed.
Finally, the flight crew did not recognise that slow rising airspeed indications was symptomatic of blocked pitot tubes and, as a result, did not reject the take-off.
What has been done as a result
Sharp Airlines advised that it was reviewing the company standard operating procedures to ensure clarity of process for pre-flight inspections.
Safety message
This occurrence highlights the importance of conducting an airspeed check early in the take-off run and recognising that if this is not as expected that the take-off should be rejected. Flight crews should be aware of the typical symptoms associated with a blocked pitot tube, and that the airspeed may slowly increase.
The occurrence also illustrates the importance of procedures clearly stating what inspections are required and when. Flight crew pre-flight inspections are an important risk control. If inspections are not done correctly, it increases the risk of defects not being identified and/or the aircraft not being correctly configured for flight.
The occurrence
Background
This incident occurred on 10 February 2025, however, due to a reported administrative error, the ATSB was not advised until 18 July 2025. The ATSB subsequently commenced an investigation on that day. As the interviews with the flight crew were conducted 5 months after the occurrence, their recollection of the occurrence was degraded.
Pre-flight
At around 1830 local time on 10 February 2025, a Sharp Airlines Fairchild SA227-DC Metro 23, registered VH-UZN, was being prepared for a freight flight from Townsville Airport to Brisbane Airport, Queensland with 2 crew on board.
The operator’s freight flights were usually conducted as a single-pilot operation, however, due to the aircraft’s autopilot being unserviceable, 2 flight crew were required to operate the aircraft. As such, the captain and first officer (FO), who normally conducted regular public transport operations, were relocated to Queensland for one week, to conduct freight operations.
Both crew members signed on for duty that morning at 0100 in Brisbane and signed off at 0818 in Townsville, where they spent the day resting in a hotel room. They re‑commenced the shift shortly after 1800 to operate the Townville to Brisbane sector. All of the flight planning had been completed during the first duty, so the crew reassessed the conditions to ensure nothing had changed. The preparation for the flight, including the inspection of the aircraft, was conducted just prior to last light with no visibility restriction.
It was the captain’s responsibility to conduct or allocate the pre-flight external inspection (see the section titled External inspections). They advised that, as they had flown the aircraft earlier that day, a daily inspection had already been completed, and a crew change inspection (see the section titled Crew change inspection) was not required.
Instead, the captain advised they conducted an abbreviated inspection, which they did not discuss with the FO. The FO advised that they had flown with the captain on a few occasions previously and the captain had always conducted the pre-flight inspection, and they expected this to occur on this day.
Regardless, to assist the captain, as they had done on previous days, the FO commenced some of the pre-flight tasks by removing the engine bungs and static port covers and preparing the aircraft for the aircraft loaders to arrive. They were unable to reach the pitot tube covers on the top of the nose cowl of the aircraft (Figure 1). The FO reported that they normally used a portable step, that was available in the passenger transport aircraft, to remove the pitot tube covers. However, the step was not available in the freight configuration aircraft.
In addition, they could not reach a ladder that was stowed in the rear locker as it had moved to the far side of the locker during flight. They placed the engine bungs and static port covers into a bag that they then placed on the ground beside the forward cargo hold, to remain until the pitot tube covers were removed and also placed in the bag.
Figure 1: Pitot tubes on Fairchild SA227
Source: EastWest Aviation, annotated by the ATSB
The captain was inside the aircraft completing pre-flight paperwork when the FO entered the aircraft and advised them that they could not reach the pitot tube covers. The captain acknowledged this and advised they would remove them.
There were delays of around 30 minutes while the crew waited for the aircraft loading to be completed. During this time, it had started raining heavily and became dark. The FO noticed that the bag containing the bungs and static covers was filling with water from the rain. In response, they retrieved the bag and placed it into the forward locker, observing ‘remove before flight’ tags in the bag.
Only aircraft operating at the Brisbane base had static port covers that also had ‘remove before flight’ tags attached, which the FO advised were identical to the tags attached to the pitot tube covers. As such, the FO, seeing the ‘remove before flight’ tags, presumed the captain had removed the pitot tube covers and placed them in the bag.
There were then further delays as the aircraft required reloading, and the captain was required to recalculate the manual trim configuration for the aircraft. The captain later stated feeling frustrated by the loading delays and that they likely felt some self-induced time pressure to depart, to avoid the worst of the incoming weather. They also later advised the operator that due to the heat and humidity, they did not wear the rain jacket provided, which may have influenced them not wanting to be outside the aircraft longer than necessary.
Once loading was complete and the aircraft was ready for departure, in accordance with company procedure, the FO commenced the final external security check (see the section titled External security check) which included a ‘4,3,2,1 check’ (see the section titled 4321 check). This check did not require that they inspect the pitot tubes to ensure the covers had been removed.
As the FO returned to the entry door, the captain stepped outside the aircraft. The FO incorrectly presumed that the captain was going to inspect the aircraft. However, neither crew discussed the external inspection, nor the final 4,3,2,1 check, prior to closing the aircraft’s main door.
Flight
The crew reported that as the aircraft commenced taxiing the heavy rain continued and it was very difficult to see out the front of the aircraft, and they did not detect the pitot tube covers. The crew reported that they completed all the required procedures prior to lining up on the runway including, as part of the ice protection and ignition step, selecting the pitot heat to ON.
During the initial stage of the take-off run, the captain set take-off power and then the FO took control of the aircraft (see the section titled Flight crew responsibilities during take‑off). At this time, the FO checked the airspeed, expecting to see it around 80 kt, but noted that it was fluctuating around 60–70 kt. The FO referenced the left side airspeed indicator, which also appeared to be fluctuating below 80 kts, quickly assessed how much runway was remaining, and called words to the effect of ‘Airspeed. Reject’.
Around the same time, the captain had also observed that their airspeed was indicating lower than they expected, and when the FO made the ‘reject’ call, they looked at the GPS unit which was indicating around 100–110 kt groundspeed. Noting there was minimal wind, the captain believed the GPS unit to be reasonably accurate and felt that the aircraft was ready to rotate.
Taking into consideration the wet runaway and not being sure how much runway was left due to the limited visibility, the captain made the decision to continue the take-off as they considered it was safer rather than risk running off the end of the runway. The captain called words to the effect of, ‘too fast, we’re going’.
During the initial climb, the FO heard a flapping noise coming from the front of the aircraft and identified that the pitot tube covers had been left installed on the pitot tubes, which they announced to the captain.
The FO referenced the GPS for speed to continue the climb and, shortly after, the FO’s airspeed indicator appeared to return to normal operation as it was indicating consistent with the GPS speed.
The crew discussed the situation and decided to return to Townsville Airport. The FO remained pilot flying due to having an operable airspeed indicator, while the captain contacted air traffic control (ATC) requesting a return to Townsville due to a technical problem. ATC provided radar vectors for the return, and the FO landed the aircraft uneventfully at 1958.
Following the post-flight inspection, the operator reported that the captain’s side pitot cover was mostly intact, and heat fused to the pitot tube. The FO’s side pitot cover had disintegrated, and the remnants of the cover had slid down to the rear of the pitot tube such that it did not obstruct normal operation.
Context
Flight crew details
The captain held a Commercial Pilot License (Aeroplane) and a class 1 aviation medical certificate. They had accumulated 3,642 flight hours, including 3,424 on the SA227‑DC.
The first officer (FO) held a Commercial Pilot License (Aeroplane) and a class 1 aviation medical certificate. They had accumulated around 5,000 flight hours, including 854 hours on the SA227-DC.
Analysis was undertaken to determine if fatigue was a factor which contributed to the captain forgetting to remove the pitot covers prior to departure. The time of day, crew work and rest patterns, and indicators of alertness were considered. The analysis concluded that the captain was unlikely to be experiencing fatigue at the time of the occurrence.
Due to the time that had passed between the incident and the crew being interviewed, the FO was unable to accurately recall their rest patterns in the days leading up to the occurrence. However, they advised that they felt rested and fit for duty.
Aircraft information
The Fairchild Swearingen SA227-DC is a low-wing, pressurised, twin-turboprop aircraft, manufactured in the United States in 1996 and issued serial number DC881B. It was registered in Australia as VH-UZN in 2005. The aircraft was fitted with 2 Garrett turbine TPE3311 engines.
The aircraft was fitted with a flight data recorder; however, the data was not downloaded by the operator at the time and had been overwritten when the ATSB was notified of the occurrence.
External inspections
The operator’s Flight crew operating manual (FCOM) stated there were 3 types of external inspections:
daily inspection (first flight of the day)
crew change inspection
post-flight inspection.
In addition, prior to closing the aircraft’s main door, both crew members were required to conduct a final security check, and the FO was required to do a ‘4321 check’.
Daily inspection
The operator’s Operations manual stated that:
A daily inspection is to be carried out as per the instructions in the Flight Crew Operating Manual for the aircraft type by the Pilot-in-Command or if he / she so delegates to, a person with the appropriate authority … on the first flight of the day for that aircraft.
The FCOM stated that the inspection consisted of an internal and external inspection. Further it stipulated (Figure 2) the path that flight crew should take when conducting the daily walk-around inspection. The numbers represent pause points to inspect a particular section of the aircraft, and each were associated with certain check items. One of the items to be checked was the condition of the pitot probes.
Figure 2: Schematic showing pre-flight walk-around path required prior to the first flight of the day
The crew change inspection was to be conducted whenever crew accepted an aircraft for duty and the aircraft had already flown that day.
The FCOM stated that:
It is not to be confused with a daily inspection. If an aircraft already operated by the crew has been taken offline for maintenance this inspection will be repeated. It consists of a Crew Change External Inspection and a Crew Change Internal Inspection. These inspections are similar to the Daily Inspection but omitting [first flight of the day] FFD items (unless that system had maintenance performed on it) and complete only hash (#) items on the internal component. Certification for the completion of this inspection was not required.
Among other items, the removal of bungs, pitot covers and wing tip flags was required as part of the crew change inspection.
External security check
In addition to the daily inspection (required for the first flight of the day), the FCOM required both crew members to conduct an external security check every flight, immediately prior to the cabin door being closed. This check comprised of the following:
• Check cargo and baggage is secure
• Tail stand (if fitted) is removed, stowed and pin retained
• All hatches, cowls and fuel caps closed
• Rotate the propellors to check for thermal distortion
• Check all ground equipment and the manoeuvring area is clear
4321 check
Prior to the cabin door being closed, the FO was also required to do an extra check, which the operator called a ‘4321 check’, and included:
Whilst standing at the front of the aircraft confirm with the “4,3,2,1 check” the following:
• 4 x doors latched and secure (excluding the main door at this stage)
• 3 x wheel chocks removed
• 2 x engine intakes and area underneath are clear, and 2 x fuel caps secure
• 1 x pogo stick (if fitted) removed.
Whilst this check is the RP [right pilot] responsibility, LP [left pilot] are not absolved from taking due care and diligence in this matter.
Post-flight inspection
The FCOM also set out the requirements for post-flight inspection. This was required to be conducted after each sector, and at the end of a duty period. The FCOM stated that after each sector the flight crew was required to, among other items:
• Ensure engine bungs, pitot covers and tail stand (if applicable) are in place.
An overview of the aircraft was to be conducted, checking the general condition and presence of any fluid (leaks or drips) on the aircraft or the adjacent ground.
Securing the aircraft
In addition to the post-flight inspection, the FCOM stated that on the last flight of the day, or if the aircraft was to be left unattended for greater than 60 minutes, the crew were required to secure the aircraft and conduct a terminating checklist (Figure 3). Securing the aircraft required the crew to:
• Ensure the A/C is parked correctly and in a safe secure area
• Ensure controls are locked (seat belt on last flight only)
• Chock all 3 landing gears.
• Tail stand in place (if fitted).
• Fit Engine Intake and Pitot covers (last flight only).
• Check cargo compartment lights (nose locker and rear) are off.
• Check for any fluid leaks under the A/C.
• Check tyres for wear and condition.
• Check all Beacons/Exterior Lights are serviceable.
• Complete and secure all Company Documentation (as appropriate).
• Complete a review of spare [Aircraft maintenance logs] AML, [Deferred defect list] DDL, [Flight deck log] FDL & ensure a spare book is available.
• Consult the TERMINATING Checklist when carrying out the above actions (Figure 3)
Despite the above list including the item ‘Fit engine intake and pitot covers (last flight only)’, Sharp Airlines later clarified that engine intake and pitot tube covers were expected to be fitted if the aircraft was left unattended for 60 minutes or more.
Sharp Airlines further advised that, although the first part of the duty was conducted on the same day, it expected that the flight crew should have conducted a full external (preflight) inspection, as a termination check had been completed at the end of the previous flight. However, the procedures did not state what checklist was required in this situation.
Flight crew responsibilities during take‑off
The captain (left pilot (LP)) was responsible for the take-off brief which included stating:
If prior to V1 you see anything that could adversely affect the safety of the flight clearly call “FAILURE” or clearly state “[the condition]”. I will decide whether to continue or reject the take-off by clearly stating either “CONTINUE” or “REJECT”
For a right pilot (FO) take-off the FCOM stated that:
• The LP advances the power levers to approx. 25–40% [torque] TQ whilst holding the aircraft on the brakes (paved surfaces only) and checks the BETA lights are off and calls [continuous alcohol water injection] “CAWI ON” (if CAWI required).
• The LP (Captain) observes the increase in TQ and the AWI pump lights are on (if CAWI required). Sets the power levers at 3% below required TQ calls “HANDING OVER” at approx. 60kts (ensure [nose wheel steering] NWS is released) and then calls “POWER SET” and leaves their hand on top of the power levers until V1.[1]
• RP responds, “TAKING OVER” and his/her hands remain clear of the power levers.
• LP Constantly scans the instruments for an impending failure or abnormality and calls “80kts”.
Sharp Airlines’ policy was that between 80 kt and V1 the take-off would only be rejected if there was an engine failure, a fire or the aircraft was otherwise unsafe or unable to fly.
Pitot static system
Pitot tubes
Pitot tubes are components of the aircraft’s pitot-static system. The Fairchild SA227-DC has 2 pitot tubes, which are attached to the upper cowl of the aircraft’s nose (Figure 1). The pitot tubes point directly into the airflow, measuring the total air pressure. This information and the static pressure, delivered by static ports on the fuselage, are used to compute the aircraft’s indicated airspeed. If the pitot tube is partially or completely blocked, airspeed indications will be inaccurate.
The pitot tubes have a heating system to prevent ice build-up. This is required to be selected ON prior to entering known icing conditions. The weather information from the Bureau of Meteorology for the time of the flight indicated that icing conditions were forecast above 10,000 ft. This required that the pitot heat was selected ON prior to take‑off.
Pitot tube covers
Pitot tube covers provide protection from foreign object obstruction when the aircraft is on the ground. They typically incorporate a ‘remove before flight’ warning tag/streamer (also known as a flag or ribbon) intended to alert relevant personnel of their presence.
Flight data
Take-off and landing data was not retained by the crew or the operator post-incident, however, the operator provided a recreated take-off and landing data (TOLD) card, with V1 calculated to be 114 kts.
The ADS-B flight data available to the ATSB had limited data points and parameters. During the take-off run, the recorded data periodicity was approximately 20 seconds, and this restricted an accurate estimation of the take-off location and groundspeed of the aircraft.
This data was compared to historical recorded flight data of 19 take-offs of another SA227-DC aircraft from Townsville Airport runway 01. Comparing the pitch attitude and indicated airspeed parameters in the historical data against the available ADS-B parameters for the flight, the ATSB was able to identify an approximate rotation location on runway 01 during the incident flight (Figure 4).
Figure 4: Estimated rotation location VH-UZN from historical flight analysis
Source: Google Earth using ADS-B exchange data, annotated by the ATSB
The ATSB estimated that the rotation speed (VR)[2] of VH-UZN, based on historical flights, was likely in the lower range of values between 112–130 kt.
Related occurrences
The ATSB has investigated several occurrences where ground use equipment has been left on aircraft due to inadequate flight crew inspections and/or inadequate operator guidance.
Airspeed indication failure on take-off involving Airbus A330 (AO-2018-053)
On 18 July 2018, a Malaysia Airlines Airbus A330, took off on a regular public transport flight from Brisbane, Queensland, to Kuala Lumpur, Malaysia. As the covers had been left on the aircraft’s 3 pitot probes, the instruments showed a red speed flag in place of the airspeed indication from early in the take-off, and unrealistically low airspeeds afterwards. The flight crew did not respond to the speed flags until the aircraft’s speed was too high for a safe rejection of the take-off, and the take-off was continued.
Aircraft preparation event involving Link Airways Saab 340 (AO-2022-055)
A propeller strap became embedded in a Link Airways Saab 340B regional airliner’s cabin on take-off from Canberra in November 2022. The ATSB’s investigation found that several factors contributed to the propeller strap not being noticed or removed by the first officer, captain, or dispatcher, prior to departure, including that the guidance provided by Link Airways for training of Swissport dispatchers did not explain the appearance, function and importance of the propeller strap.
Aircraft preparation event involving Saab 340B (AO-2022-058)
On 16 November 2022, a Regional Express (Rex) Saab 340B, was prepared for a scheduled air transport flight from Cairns Airport to Bamaga, Queensland. As the crew taxied the aircraft to the runway, an engineer on a nearby parking bay noticed something hanging from the aircraft and contacted the tower. The crew returned the aircraft to the bay. Aircraft parked overnight at Cairns were required to be fitted with an operator designed bung installed in the horizontal stabiliser trim actuator cove to prevent bird nesting. The inspection revealed the horizontal stabiliser bungs had not been removed and were still installed in the left trim actuator cove.
Aircraft preparation event involving a Hawker Beechcraft Corporation B200 (AB-2024-025)
On 8 May 2024, a Hawker Beechcraft B200 was being prepared for an air transport flight at Darwin Airport. Prior to departure, the pilot completed the preflight inspection, confirmed that both red flags were in their possession, and secured these items along with the propeller covers inside the aircraft. However, the pilot did not detect that the flag for the right-side cover had detached from the cover, nor that the cover was still attached to the pitot tube.
During the take-off, the pilot detected a speed discrepancy on their cockpit instrumentation. They continued the climb to 3,000 ft before returning via a visual approach to Darwin Airport.
During the post-flight inspection, the pilot identified that the right-side pitot cover was still in place, covering the pitot tube.
Aircraft preparation event involving Saab 340B (AO-2024-059)
On 19 November 2024, the aircraft was prepared for departure from Melbourne Airport. After the pilots started the engines, a passenger told the flight attendant they had seen a strap restraining the left propeller before it began to spin. The propeller strap was then found attached to the propeller, with the pins that connect it to the engine cowling broken on start‑up.
The report noted the final external walkaround check of the aircraft required the first officer to remove the propeller strap from the propeller, before rotating the propeller to a required position. However, the first officer inadvertently left the propeller strap attached, instead only disconnecting and removing the strap extension, which connected the propeller strap to the aircraft stairs to prevent them from being retracted while the strap is in place.
Once the first officer was in the flight deck, the ground handler assigned to the dispatch, who was a trainee, did not detect the propeller strap from their position at the nose of the aircraft, and provided the crew with a signal to start the engine.
Meanwhile, the pilots conducted the engine start checklist, which included a requirement for the captain to check that the left engine was clear. The captain also did not detect the propeller strap and proceeded to start the engine.
Safety analysis
A Sharp Airlines Fairchild SA227 departed Townsville Airport with pitot tube covers fitted. This analysis will discuss the pre-flight actions of the flight crew regarding the pitot tube covers and consider the operator’s procedures for pre-flight inspections. It will further examine the crew’s decision to take-off with unreliable airspeed.
Pre-flight inspection
The captain considered that the daily inspection had already been completed in the early hours of the morning on the previous sector, and therefore, it was not required to be completed prior to this flight. They also did not consider that a crew change external inspection was required. Consequently, they reportedly conducted an abbreviated walk‑around inspection prior to the incident flight but did not reference any aircraft or operator checklist.
The first officer (FO) assisted the captain by removing the engine bungs and static port covers. However, they were unable to reach the pitot covers on the nose of the aircraft and asked the captain to remove them. The captain advised that they would do so, but subsequently forgot. Additionally, the FO did not confirm with the captain that the pitot covers had been removed, likely due to seeing ‘remove before flight’ tags in the bag and incorrectly assuming those were attached to the pitot covers.
There was no further discussion between the captain and the FO regarding the external aircraft inspection, and the pitot covers were not removed prior to departure.
Contributing factor
Due to the combination of a memory lapse and incorrect assumption, the aircraft’s pitot covers were not removed prior to departure.
Operator’s guidance
The operator’s Flight crew operating manual (FCOM) required flight crews to secure the aircraft and conduct a terminating check if the aircraft was to be unattended for more than 60 minutes. While it was the operator’s expectation that a full daily inspection of the aircraft was required once a termination check had been completed; the procedures did not clearly state this, and it did not occur on this occasion.
The operator did have an abbreviated checklist, the crew change checklist, and it is possible some flight crew were conducting this checklist on returning to the aircraft after completing the terminating check, however, the procedures also did not specify that this was required.
In addition, the operator also expected that engine bungs and pitot covers would be fitted when the aircraft was on the ground for periods over 60 minutes; however, the procedure (securing the aircraft) specifically stated that they should be fitted only after the last flight. This created the potential for confusion among flight crew as to when they should be fitted.
Further, while the final ‘4321’ visual check was designed for quick turnarounds, it required that the engine intakes were checked, and although engine bungs were only required to be installed when the pitot tube covers were installed, it did not require that the pitot tube covers were checked.
a terminating check be completed if the aircraft was unattended for more than 60 minutes, but did not specify what checks were to be completed on return to the aircraft
pitot covers should be installed after the last flight of the day only, where the operator required that they be installed if the aircraft was unattended for longer than 60 minutes.
In addition, the final visual check, completed by the first officer prior to closing the doors, did not include checking that pitot covers had been removed. (Safety issue)
Poor visibility
It is likely that due to the night‑time conditions and heavy rain, neither flight crew detected the pitot covers in place, as they would have during the day, while taxiing the aircraft.
Similarly, there was no opportunity for air traffic control, other pilots or ground staff to visually observe the pitot tube covers in place. As such, the pitot tube covers remained in place undetected.
Contributing factor
Likely due to poor visibility, the flight crew did not detect the pitot tube covers were still in place prior to commencing the take-off.
Airspeed indications during take-off
The captain's decision to take off once the crew recognised that the airspeed was unreliable was understandable in the circumstances, and probably at, or close to V1. However, there was opportunity for the crew to have recognised earlier in the take-off run that the airspeed indicators were not functioning correctly, as the speeds were slowly increasing. Continuation of the take-off was likely due in part to neither crew realising that airspeed could still increase with pitot covers on.
Contributing factor
During the take-off run, the crew did not detect that the airspeed indicators were not indicating correctly, likely due to observing that they were slowly increasing, resulting in the crew not rejecting the take-off.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the unreliable airspeed indications on 10 February 2025:
Contributing factors
Due to the combination of a memory lapse and incorrect assumption, the aircraft’s pitot covers were not removed prior to departure.
- a terminating check be completed if the aircraft was unattended for more than 60 minutes, but did not specify what checks were to be completed on return to the aircraft
- pitot covers should be installed after the last flight of the day only, where the operator required that they be installed if the aircraft was unattended for longer than 60 minutes.
In addition, the final visual check, completed by the first officer prior to closing the doors, did not include checking that pitot covers had been removed. (Safety issue)
Likely due to poor visibility, the flight crew did not detect the pitot tube covers were still in place prior to commencing the take-off.
During the take-off run, the crew did not detect that the airspeed indicators were not indicating correctly, likely due to observing that they were slowly increasing, resulting in the crew not rejecting the take-off.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
a terminating check be completed if the aircraft was unattended for more than 60 minutes, but did not specify what checks were to be completed on return to the aircraft
pitot covers should be installed after the last flight of the day only, where the operator required that they be installed if the aircraft was unattended for longer than 60 minutes.
In addition, the final visual check, completed by the first officer prior to closing the doors, did not include checking that pitot covers had been removed.
Glossary
ATC
Air traffic control
FO
First officer
FCOM
Flight crew operating manual
GPS
Global positioning system
TOLD
Take off and landing data
V1
The critical engine failure speed or decision speed required for take-off. Engine failure below V1 should result in a rejected take off; above this speed the take-off should be continued. In this aircraft, V1 and VR are the same value.
VR
The speed at which the rotation of the aircraft is initiated to take-off attitude.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
flight crew of the incident flight and another pilot who conducted flights for the operator
Sharp Airlines
ADS-B data.
References
Sharp Airlines, Metro 3/23 Flight Crew Operating Manual, Issue 09, Revision 2, 24 June 2024
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
flight crew of incident flight
Sharp Airlines
Civil Aviation Safety Authority.
No submissions were received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]V1: the critical engine failure speed or decision speed required for take-off. Engine failure below V1 should result in a rejected take off; above this speed the take-off should be continued. In this aircraft, V1 and VR are the same value.
[2]VR: the speed at which the rotation of the aircraft is initiated to take-off attitude.
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into a collision with terrain accident involving a twin turboprop Reims Cessna F406 aircraft near Oakey, Queensland, on Sunday afternoon.
The ATSB is deploying a team of transport safety investigators from its Brisbane and Canberra offices, specialising in aircraft operations and maintenance.
Investigators will conduct a range of evidence-gathering activities, including site and wreckage examination, and recovery of any aircraft components for further examination at the ATSB’s technical facilities in Canberra.
Investigators will also seek to interview involved parties, and collect relevant recorded information including flight tracking data, as well as pilot and aircraft maintenance records, and weather information.
The ATSB asks anyone with video footage of the aircraft at any phase of the flight, or in the immediate aftermath of the accident, to make contact via the witness form on our website: atsb.gov.au/witness at their earliest opportunity.
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into a collision with terrain accident east of Khancoban, in the New South Wales Snowy Mountains, involving a Beechcraft Debonair light aircraft.
The aircraft was conducting a private flight from Wangaratta, Victoria to Moruya on the New South Wales south coast on Tuesday, and was reported missing when it failed to arrive at its destination.
The ATSB commenced its investigation into the accident after an extensive aerial search located the aircraft wreckage on Thursday afternoon, in snow-covered mountainous terrain in the Kosciuszko National Park, east of Khancoban.
Investigators are working closely with the NSW Police to gather available evidence, including imagery of the accident site and any aircraft components containing recorded data that can be retrieved and recovered to the ATSB’s technical facilities in Canberra for download and analysis.
Investigators are also collecting relevant recorded information including ADS-B flight tracking data, weather information, and pilot and aircraft maintenance records.
The ATSB will provide a substantive update on the progress of the investigation when it releases a preliminary report, which will detail factual information established in the investigation’s evidence gathering phase, in about two months.
The investigation’s findings will be contained in a final report to be released at the conclusion of the investigation. That report will also detail the ATSB’s analysis of the evidence to support those findings.
However, should a critical safety issue be identified during the investigation, the ATSB will immediately notify relevant parties so safety action can be taken.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 2 June 2025, at about 0830 local time, a student pilot operating a Piper PA‑28‑181 (PA‑28) aircraft, departed on a multi‑stop navigational exercise from Tamworth Airport, New South Wales, to Dubbo, then Mudgee and then returning to Tamworth. A supervising Grade 1 flight instructor was assigned to support the student and had provided them with a telephone number if assistance was needed. After refuelling at Dubbo Airport, the student departed for Mudgee for an intended return to Tamworth.
About 1 hour and 45 minutes after departing from Dubbo, the student noticed abnormalities with the throttle and was having difficulties reducing power smoothly due to friction through the throttle control. Unsure of what to do, the student orbited near Parkes before they contacted their flight instructor for advice by telephone. A licenced aircraft maintenance engineer was then consulted for possible airborne rectifications.
After discussing the aircraft fuel state, the student’s state of mind, the safest landing location and in consultation with senior staff, the flight instructor then advised the student that the best option was to track direct to Tamworth where an air traffic control (ATC) service, a long runway, and emergency services were available.
At 1351, the student advised the flight instructor that the throttle of the PA‑28 was stuck at almost full power. The flight instructor and other senior flying school management discussed the options with ATC and, as a precaution, a full emergency was declared due to the uncertainty of a safe landing.
With guidance, from the flight instructor and ATC, the student commenced the descent to Tamworth Airport with the engine still producing high power. The student was briefed that a mixture cut[1] would be required to stop the engine to allow them to land and where in the landing sequence to cut it. At about 1430, the student conducted a flapless landing at about 110 kt, moved the mixture to idle cut‑off over the threshold, and touched down bringing the aircraft safely to a stop on the runway.
Emergency services attended the aircraft after landing but were not required. The student did not sustain any injuries and there was no damage to the aircraft.
During debriefing, the flight instructor noted that the student:
‘…did so well through the whole event, remained calm and professional, and got the aircraft safely down on the runway’
A subsequent engineering inspection of the aircraft identified an inner section of the throttle control cable was worn and frayed which resulted in it becoming jammed in position.
Safety message
Regular inspection and maintenance of aircraft control systems is essential to detect early signs of mechanical wear to prevent in‑flight control issues.
The student pilot’s ability to manage the situation safely, supported remotely by their instructor and ATC, demonstrates the value of decision‑making support for abnormal operations and training environments. Having a clear emergency plan prior to the critical stages of a flight can assist in timely decision‑making and reduce workload during high stress situations.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]A mixture cut is the shutdown of a piston engine by cutting the fuel supply via the mixture control.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-026
Occurrence date
02/06/2025
Location
Near Parkes Airport
State
New South Wales
Occurrence class
Incident
Aviation occurrence category
Diversion/return, Powerplant/propulsion - Other
Highest injury level
None
Brief release date
21/07/2025
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28-181
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
A Robinson R44 scenic flight helicopter was likely affected by the rotor wake of a larger helicopter when its pilot encountered control difficulties necessitating a forced landing on the banks of Sydney’s Parramatta River.
On the morning of 7 April 2025, the Bankstown Helicopters-operated R44 took off from Bankstown Airport for a local scenic flight around Sydney Harbour with a pilot and two passengers on board, an ATSB investigation final report details.
About seven minutes into the flight, just as the R44 entered the Parramatta River helicopter lane, a larger EC120 helicopter suddenly appeared about 500–600 ft (150–180 m) in front of it and about 100 ft above them, according to the pilot’s estimate.
The R44 then experienced what the pilot described as very strong turbulence from a vertical motion in the atmosphere.
“In response, the pilot applied full collective to avoid the water, which caused the rotor speed to decay sufficiently for the low rotor speed warning horn to activate,” Acting Director Transport Safety Elaine Hargreaves said.
“The pilot then sighted a suitable forced landing area at Cabarita Park and, using the helicopter’s remaining airspeed and rotor speed, manoeuvred the helicopter to the shoreline for a safe landing.”
Air traffic control primary radar data and the pilot’s report indicated that the R44 had entered the Parramatta River helicopter lane and passed over the Ryde Bridge about 9 seconds behind and slightly below the larger, three-bladed EC120.
“Flight tests have demonstrated helicopter wake turbulence is comparatively larger and less predictable than that of fixed-wing aircraft of comparable weights,” Ms Hargreaves said.
“Helicopter rotor vortices can descend, remain level or climb, and the duration of their persistence can increase significantly in conducive weather conditions.”
Guidance, such as from the United States Helicopter Safety Team(Opens in a new tab/window), advises helicopter pilots to remain three rotor disks clear of a hovering or taxiing helicopter, and to allow 3 NM and/or 2 minutes for the rotor wake from a preceding helicopter to dissipate.