
Final report
Report release date: 12/06/2026
Investigation summary
What happened
On 7 February 2025, the fully laden bulk carrier FMG Nicola was departing Port Hedland under the conduct of 2 marine pilots with 3 tugs in attendance. At 1515 local time, about 5 miles into the pilotage, FMG Nicola’s main engine unexpectedly shut down. An emergency was declared, and the pilots immediately took action to control the ship’s movement while the port’s vessel traffic service mobilised additional port tugs and the ship’s engineers rectified the engine fault. The main engine was restarted at 1523, and the ship was brought back under control. Multiple tugs attended and the ship was brought clear of the channel side and taken safely to sea.
What the ATSB found
The ATSB investigation found that FMG Nicola lost propulsion because the main engine low lubricating oil pressure emergency shutdown switch erroneously activated with all system parameters otherwise normal.
Also, the investigation found that the emergency response was as per port guidance, procedures and training. The ship remained underway and kept moving and was safely navigated via the channel to sea. While the ship departed, and tracked along the edge of, the charted shipping channel, there was no evidence to show that the ship had contacted the seabed.
What has been done as a result
Pilbara Ports Authority advised that port operations have been reviewed in the areas of ship reliability and vetting, towage strategy and arrangements and pilotage and emergency response and relevant procedures have been updated. Actions taken included improved operational awareness of and training in escort towage arrangements and updating of pilotage and emergency response procedures.
The ship’s manager/operators responded to this incident by upgrading the management (testing and replacement) of main engine lubricating oil pressure switches on all ships in its fleet. This was supported by fleetwide implementation of a procedure for rapid response to main engine shutdown due to low lubricating oil pressure.
The Australian Maritime Safety Authority has updated its processes to better ensure prompt reporting of incidents to the ATSB.
Safety message
The safety of ports and ships that use them requires commitment to continued improvement and learning from incidents by port authorities, port users, facility owners and port services such as towage and pilotage. By working together, enhancing procedures and strategies, emergency situations can not only be safely managed, but lessons can be learned and used to further improve operational safety.
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
At 08321 on 7 February 2025, the 327 m bulk carrier FMG Nicola (cover image) completed loading 237,088 t of iron ore at its berth in Port Hedland, Western Australia. The fully laden ship had a draught of 17.51 m forward and 17.69 m aft and was due to depart its berth during the afternoon (a high water of 5.56 m was predicted for 1634).
At 1330, 2 harbour pilots, one of whom was under supervision, boarded the ship. The port authority’s marine services delivery manager (MSDM), who was also a harbour pilot, boarded to observe the departure. By 1348, the ship’s main engine and steering had been satisfactorily tested and the master-pilot information exchange was completed in readiness for departure. The pilot under supervision would conduct2 the pilotage and 4 tugs were secured to assist.
By 1412, all mooring lines had been cast off and the ship departed the berth (Figure 1). There was a 25-knot north‑north‑west wind with waves of up to 1.5 m on a 0.5 m swell in the area, including the port’s single shipping channel.
At 1442, with the ship progressing along the channel as planned, the MSDM disembarked via pilot launch. At 1446, one of the tugs was let go and returned to base.
At about 1500, FMG Nicola was turned to port to follow the channel at a speed of about 7 knots. Of the 3 tugs assisting, FMG Mako was fast at the ship’s port shoulder,3FMG Dusky at the starboard shoulder and FMG Spinner through the centre lead aft.
At 1514, as the ship approached beacons 32-33, the pilot ordered a heading4 of 334°. At about this time, FMG Mako’s master requested its towline be let go as conditions were uncomfortable due to choppy seas on the ship’s port side. The pilot concurred, and the towline was let go at 1515.
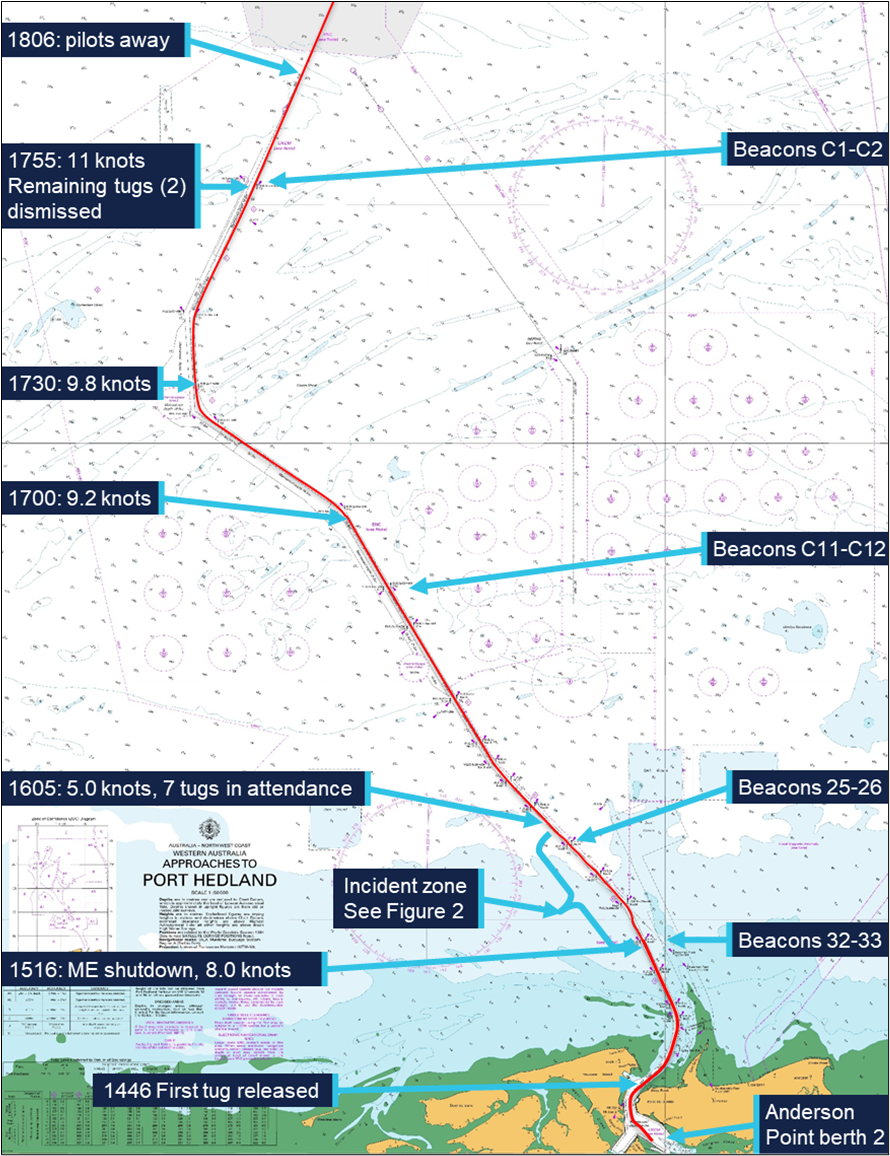
Figure 1: Overview of FMG Nicola's track through the Port Hedland shipping channel
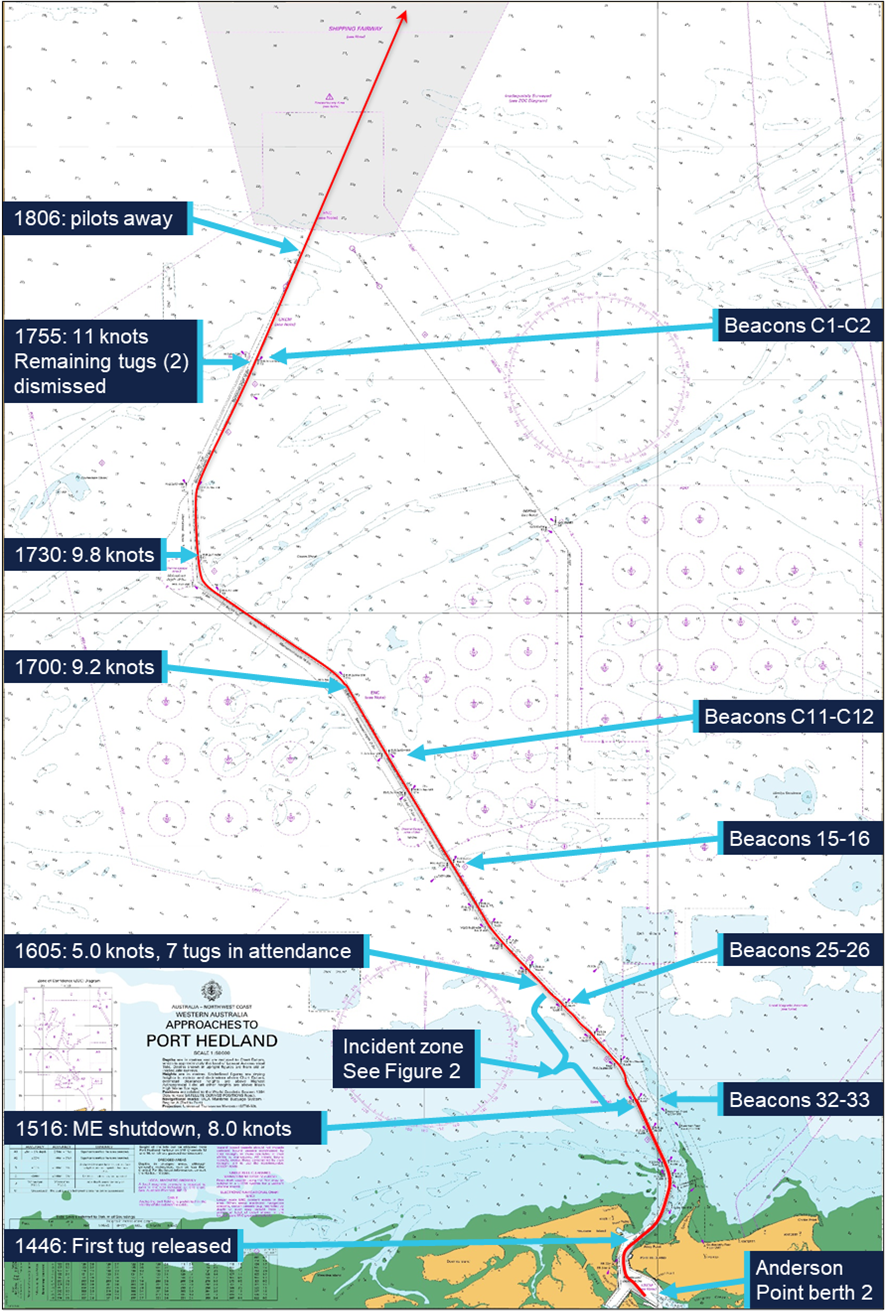
Source: Australian Hydrographic Office, data from Australian Maritime Safety Authority
Soon after, at about 1516, FMG Nicola’s main engine suddenly shut down as the ship was passing beacons 32-33 (Figure 2). The ship’s speed was 8.3 knots; the pilot ordered the rudder midships. The pilot informed the tug masters that the ship had lost propulsion and directed them to help keep it in the channel.
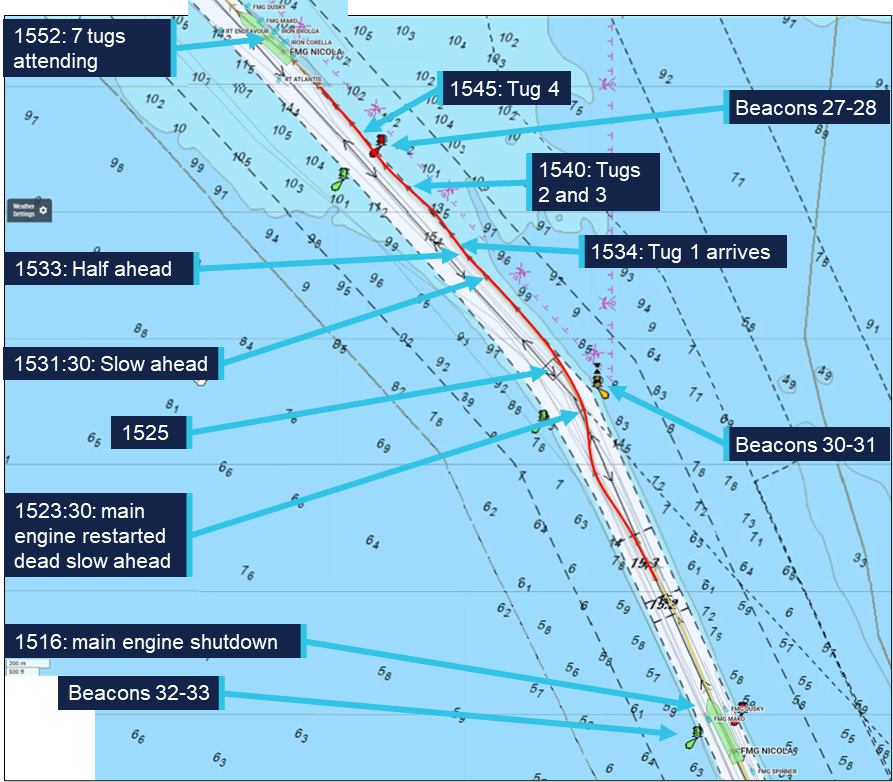
Figure 2: FMG Nicola track from about 1516 to 1552
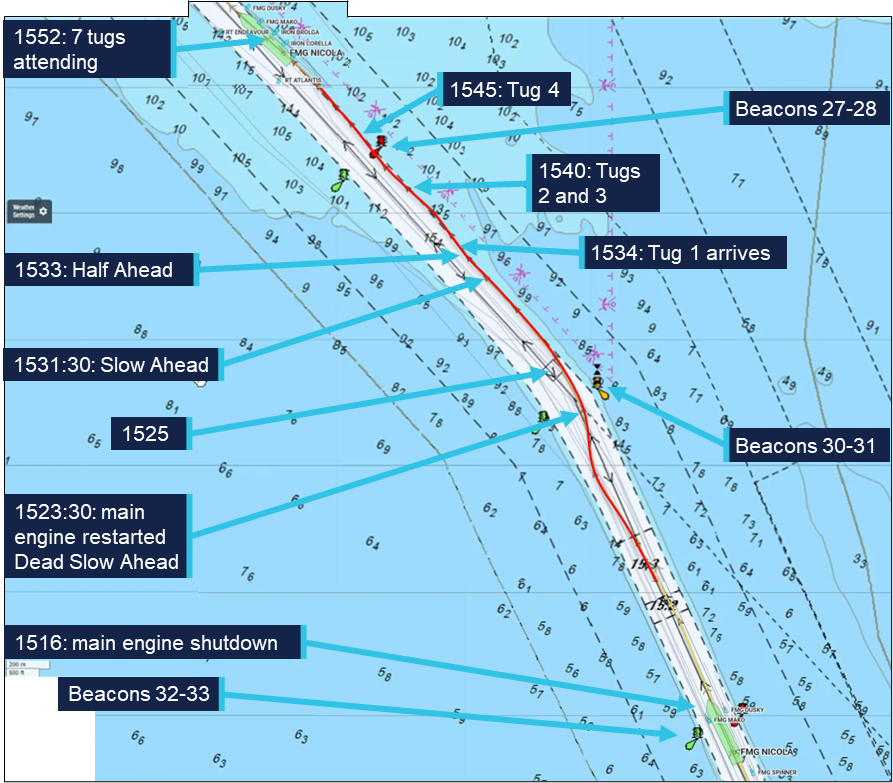
Source: Australian Maritime Safety Authority, Marine Traffic, annotated by the ATSB
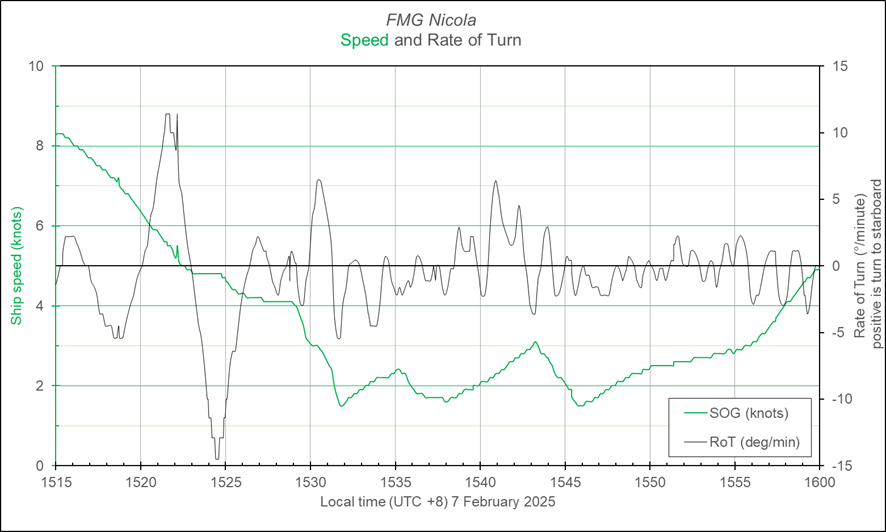
At 1518, the pilot notified Port Hedland vessel traffic service (VTS) of the emergency and requested additional tugs. The pilot gave helm orders and used the tugs to follow the channel. The ship’s speed decreased to 7.4 knots and it moved closer to the western side of the channel with a slow rate of turn of about 4° per minute to port (Figure 3).
Meanwhile, the ship’s engineers identified that the engine had shut down because the ‘main bearing and thrust bearing lubricating oil pressure low’ non‑cancellable trip had activated. The engineers determined that it had activated due to faulty operation of the pressure switch. After confirming all engine systems were operating normally, the engine trip lockout system5 was reset and, at 1523, the engine was restarted at dead slow ahead. By that time the ship had slowed to 4.8 knots.
Figure 3: FMG Nicola speed and rate of turn at the time of the incident
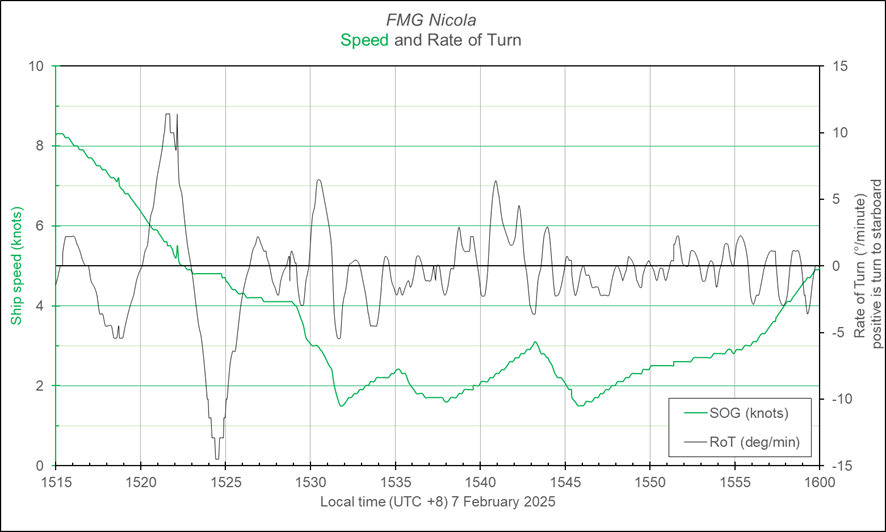
Graph derived from Automatic Identification System data and should not be used for further analysis. Source: Australian Maritime Safety Authority, analysis by the ATSB
By about 1525, FMG Nicola had passed beacons 30-31, and, with a rate of turn 7.5° per minute to port and speed of 4.3 knots, it closed on the eastern side of the channel. Soon after, the ship stopped turning and began moving along the side of the channel, which was aligned along a 318° (T) direction there. The choppy conditions hampered the use and effectiveness of the attending tugs. The pilots and master, with assistance from VTS, assessed the situation and awaited the arrival of additional towage assets to assist the ship.
The ship continued to move along the side of the channel (Figure 2), set to starboard by the conditions and influenced by the adjacent channel side and shallower water.6 With the main engine operating and the assistance of the tugs, headway was maintained.
At 1534, the first of the additional tugs arrived and was tasked to push up on the ship’s starboard side. In the following 10 minutes, 3 more tugs arrived and assisted as required by the pilot. At 1540, the ship passed close to beacon 28 while moving along the side of the channel at a speed of 2.5 knots. At 1545, with 7 tugs in attendance (4 on starboard side, 2 on port and 1 on centre lead aft) and clear of beacon 28, FMG Nicola had slowed to 1.5 knots (main engine on half ahead, 40 rpm). Multiple port rudder orders were used to counter the set to starboard and maintain the ship’s track while avoiding the stern swinging too far to starboard into the shallows. Using the main engine and the tugs, the pilots prepared to ease the ship clear of the channel side and avoid damage to the stern, rudder and propeller.
By 1550, the ship had been moved away from the channel side. The main engine was kept at half ahead and the ship’s speed increased as it came clear of the influence of the channel side and shallow water. The tugs continued escorting the ship out the channel towards open water.
At about 1635, 3 tugs were released and a further 2 were released about 10 minutes later as the ship approached beacons C11-C12. At 1648, with the ship speed at 8.3 knots, the main engine speed was increased to full ahead (46 rpm). The remaining 2 tugs were retained and escorted the ship until it passed beacons C1-C2 to sea.
By the time the ship passed beacons C1-C2, the ship’s crew had completed inspecting and testing the main engine systems. They had also conducted an inspection, including sounding tanks and compartments, to confirm there was no ingress of water.
Shortly after, at 1806, the pilots departed the ship by helicopter and the ship continued its passage to the next port, Dongjiakou, China. During the passage, the crew inspected all ballast tanks on the starboard side and found no physical damage to the ship’s side or structure.
Context
FMG Nicola
General details
FMG Nicola was a Singapore-registered, capesize7 bulk carrier built in 2016 by Jiangsu Yangzi Xinfu Shipbuilding, China. At the time of the incident, the ship was owned and operated by Fortescue Shipping Nicola, managed by Bernhard Schulte Shipmanagement (BSM), Hong Kong, and classed with Lloyd’s Register (LR).
At the time of the incident, FMG Nicola was crewed by 23 Sri Lankan and Indian nationals, including the master, all appropriately qualified for their positions on board.
The master had 26 years of seagoing experience, all on bulk carriers, with about 4 years in command. The master joined BSM in 2015 and had completed several assignments on FMG Nicola since 2021.
The chief engineer had about 18 years of seagoing experience, with about 9 years at that rank. The chief engineer joined BSM in September 2024 and was assigned to work on FMG Nicola.
Main engine
FMG Nicola’s propulsion was provided by a 6‑cylinder, MAN‑B&W 6G80ME‑C9.5 engine developing 18,240 kW. The main engine drove a single 4‑blade, fixed‑pitch propeller, providing a service speed of 14 knots.
Lubricating oil system
The main engine lubricating oil (LO) system was fitted with a hierarchy of oil pressure monitoring and alarm controls to limit inadvertent engine stoppage while preventing catastrophic engine damage. In addition to local, analogue indicators and pressure gauges, the LO pressure was monitored via a pressure transducer and pressure switches (Figure 4).
Signals from the sensors fed into the ship’s machinery alarm, monitoring and control system. This system provided real time, remote indication of the LO pressure. Software limits were incorporated to trigger alarms and other actions. Normal operating pressure for the system was about 250 kPa with software triggers set at:
- 210 kPa for standby pump start
- 200 kPa for low LO pressure alarm
- 180 kPa for main engine slow down alarm.
Figure 4: Main engine lubricating oil pressure sensing and switches
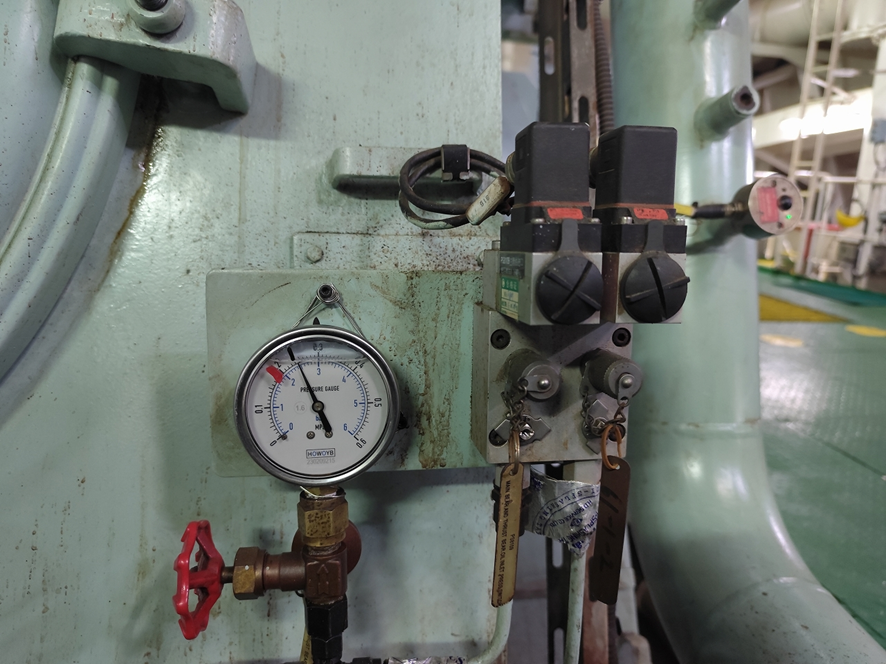
Source: Fortescue Metals Group
In addition to these triggers and alarms, the main engine LO system had a separate pressure switch set to activate at 160 kPa. This switch, independent of the oil pressure monitoring circuit, was for the main engine low LO pressure shutdown. This initiated rapid shutdown of the engine to prevent catastrophic damage due to complete loss of bearing lubricating oil.
The normal, expected, sequence of loss of LO pressure indications would follow persistently falling oil pressure: standby pump start, low pressure alarm and main engine automatic slow down prior to main engine shutdown.
The machinery monitoring system allowed for (adjustable) time delays on activation of each of these triggers. At the time of the incident, the engine LO pressure shutdown delay was set to 0.1 seconds. Following the incident, and after obtaining advice from the engine manufacturer that the delay could be increased up to 2 seconds, it was reset to 1.9 seconds.
Components of the main engine LO system were subject to regular maintenance through the ship’s planned maintenance system (PMS). The PMS records showed that the main engine pressure transmitter and pressure sensors had last been checked on 15 November 2024 (about 3 months before the incident).
Port Hedland
General information
Port Hedland, situated in the Pilbara region of Western Australia, is the world’s largest bulk export port by tonnage, handling over 500 million tonnes of cargo annually. More than 95% of this volume is iron ore, exported primarily by BHP,8 Fortescue Metals Group (FMG) and Roy Hill Infrastructure, with the port serving as the companies’ main export hub for all Pilbara output. In addition to iron ore, the port also handles exports of salt, manganese, copper concentrates, lithium minerals and livestock.
At the time of the incident, the port’s infrastructure included 19 operational berths. Eight of these berths were owned and operated by BHP, with the remaining berths owned and operated by FMG (5 berths), Roy Hill (2 berths) and Pilbara Ports Authority9 (4 berths). Shipping activity is significant, with more than 6,000 ship movements (inbound and outbound) each year.
Pilbara Ports Authority
The port was managed by the Pilbara Ports Authority (PPA), which had overarching responsibility for safety and efficiency of port operations and the environment under state legislation. The PPA’s jurisdictional responsibilities were exercised through the Port Hedland harbour master.
The harbour master’s responsibilities included the coordination of vessel traffic services, ship scheduling, pilotage and maintenance of shipping channels, navigational aids and port infrastructure. The PPA issued third‑party contracts or licences for stevedoring, towage, pilotage services and pilot transfers (helicopter and boat).
Shipping channel
Access to the port was provided by a single 22 mile10 dredged shipping channel, which allowed a single ship to traverse it at any given time. For most laden ships, particularly capesize ships, such as FMG Nicola, use of the channel was restricted by tidal conditions.
The Port Hedland navigation channel was divided into 6 zones11 based upon navigational or environmental characteristics that would impact the risk within that zone. These characteristics included location, channel alignment, bathymetry, channel slopes and sea conditions.
The incident took place within the 10-mile section of the channel closest to the port, an area prone to strong tidal flows and with particularly confined spaces, narrowing to a minimum width of 162 m. The channel depth in this section was maintained at about 15 m chart datum (Figure 5). The section of the channel from beacons 30-31 to 15-16 was described in the PPA documentation as:
…a relatively straight section of channel with one minor 13-degree alteration of course to starboard for outbound ships. The water adjacent to the channel is predominantly greater than 10 metres deep with scattered shoal patches…the channel batters are significantly flatter than [the channel out of the harbour].
Figure 5: Channel profile for beacons 30-31 to 25-26
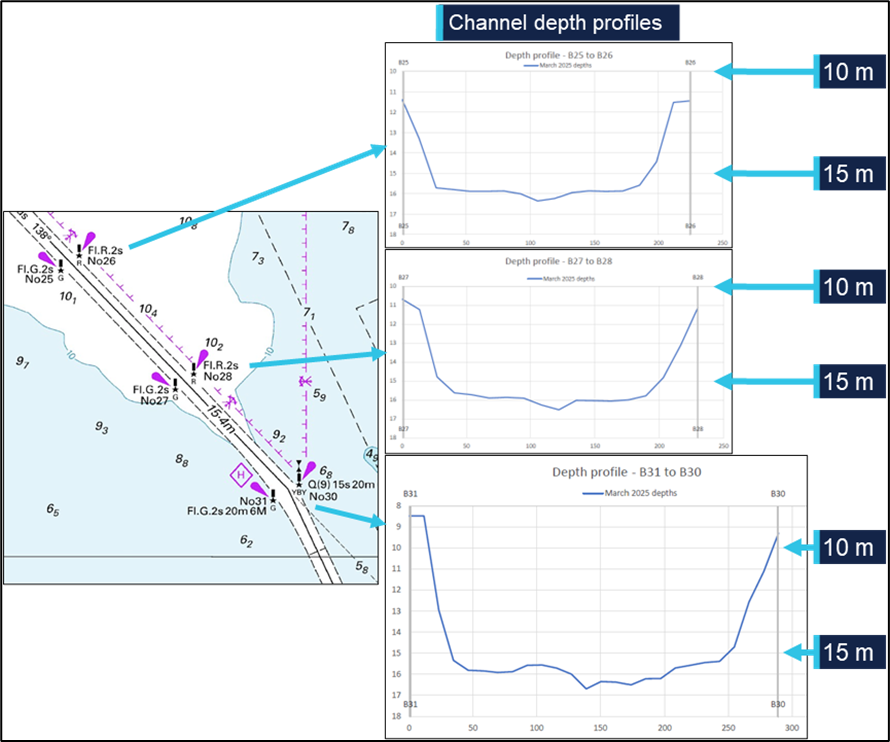
Source: Australian Hydrographic Office, Pilbara Ports Authority, annotated by the ATSB
The features of the channel make the risks associated with channel blockage high. A disabled ship can strand on a falling tide as well as blocking the passage of other ships. Depending on departure times, separation between ships and the location of an incident, up to 3 additional ships could be committed to, or within, the channel and exposed to this hazard at a given time.
Escort towage strategy
Since 2013, in support of the Port Hedland port user guidelines and procedures,12 the Port Hedland escort towage strategy (ETS) had been developed and updated. Escort towage was identified as a critical mitigative control to prevent a ship grounding or colliding with fixed objects if it experienced a loss of navigation control.
The resulting ETS was intended to assist Pilbara Ports, pilots, tug masters, towage operators and other stakeholders to understand the rationale for escort towage at Port Hedland and provide guidelines to support effective escort towage operations.
Primary objectives of the ETS included:
• to assist an escorted ship to maintain manoeuvrability and navigate within water of sufficient depth to prevent a ship grounding, and the potential consequential impact of channel blockage
• to document escort towage procedures that have been identified as effective at preventing a ship grounding and potential channel blockage through research, simulation and on-water trials.
In relation to the risks associated with a loss of navigation control event, the ETS stated that:
Steering-related incidents or main engine slowdowns or failures that result in loss of navigational control are the likely root causes for a grounding incident that may lead to channel blockage at Port Hedland. Both incident types occur at Port Hedland, with engine‑related incidents far more likely than steering incidents; however, steering incidents represent the greatest risk of a channel blockage…the time available to respond to a steering incident and prevent a ship grounding is typically 60 to 90 seconds.
Engine slowdowns or failures, which are ten times (10x) more likely to occur than steering incidents, may require escort tugs to assist with steering and maintaining headway of the ship. However, the response time required for an engine slowdown or failure is typically much longer than steering failures…[and]…allows for available towage assets, including passive assets, to be positioned appropriately to assist a ship transit to an emergency anchorage…or transit to the end of the channel…with tug assistance.
The principal guidance for immediate response to a vessel emergency in the channel was to maintain channel integrity (clearance). This manifested itself as making every effort to continue the transit, with tug assistance, through the channel to a place of safety, either to anchorage or out the channel and to sea.
Pilotage
Vessels 35 m or greater in length using the main shipping channel and navigating within port limits were required to use the services of a licensed harbour pilot. Pilotage services for the port were provided by PPA through directly employed pilots as well as by third party, contracted providers.
The pilots on board FMG Nicola at the time of the incident were employed by PPA. All PPA pilots had undertaken a competency‑based pilotage training program incorporating on‑water and simulator training and competency assessments.
The supervising pilot had worked for PPA since 2023. This pilot had over 25 years of experience in the maritime industry.
The pilot under supervision joined PPA in 2024 after more than 15 years piloting a wide variety of ship types and sizes, including capesize bulkers, and larger, in an overseas port. At the time of the incident, the pilot held a level 3 authority to pilot in Port Hedland and was undertaking supervised pilotages to upgrade this authority to level 4.
Towage
Tugs in Port Hedland were operated under towage licences granted by the PPA to Pilbara Marine (a subsidiary of FMG) and BHP Towage Services (BHPTS). KOTUG operated tugs under the Pilbara Marine towage licence while Rivtow was contracted to operate the tugs under the BHPTS licence.
The 4 tugs assigned to FMG Nicola on the day of the incident were ART85‑32W class advanced rotortugs, operated by KOTUG. Each tug had a bollard pull13 of 85 t and used a hybrid propulsion arrangement with 2 azimuth thrusters forward and a third azimuth thruster aft.
The tugs which came to render assistance after FMG Nicola lost propulsion were operated by Rivtow and comprised 2 ART80‑32 rotortugs and 2 RAstar85 azimuth stern drive (ASD) tugs.
Tug release point
The port user guidelines and procedures documented the tug allocation requirements based on specified criteria. Laden outbound capsize ships required 4 tugs secured to the ship from the berth to Hunt Point, near the harbour entrance. From Hunt Point to beacons 30-31, 3 tugs were to remain tethered to the ship – a tug on each shoulder and a dedicated, active escort tug made fast through the centre lead aft. The shoulder tugs could be let go, to remain in passive escort, should conditions require, and after risk assessment by the pilot.
From beacons 30-31 to beacons 15-16 the shoulder tugs would normally be let go and move to a passive escort position off the ship’s quarters. At beacons 15-16, the tugs could be dismissed. Ships were not generally escorted to the end of the channel, except in the case of an emergency or if the ship was deemed to require escort towage until clear of port limits.
In August of 2024, to increase time for immediate response to a steering failure, the speed of capesize ships was limited to a maximum of 8.4 knots from beacons 36-37 to the end of the channel.
On the day of the incident, conditions on the exposed port shoulder of FMG Nicola were such that the master of FMG Mako requested that the tug be let go just after passing beacons 32-33. The pilot agreed to the release and the tug was let go prior to passing beacons 30-31, and just before the ship lost propulsion.
Weather
There were multiple weather monitoring stations throughout PPA’s areas of responsibility, including at beacon 31. At 1515, when FMG Nicola’s main engine shut down, the conditions recorded at beacon 31 (Figure 6) were:
- Wind: 22 knots, gusting to 27 knots, from 280°
- Current: 0.5 knots, towards 90°
- Seas/Waves: 1.5 m, from 305°
- Swell: 0.52 m, from 315°
- Tide: 4.8 m rising.
Figure 6: Weather conditions (recorded at beacon 31) at 1515 hours
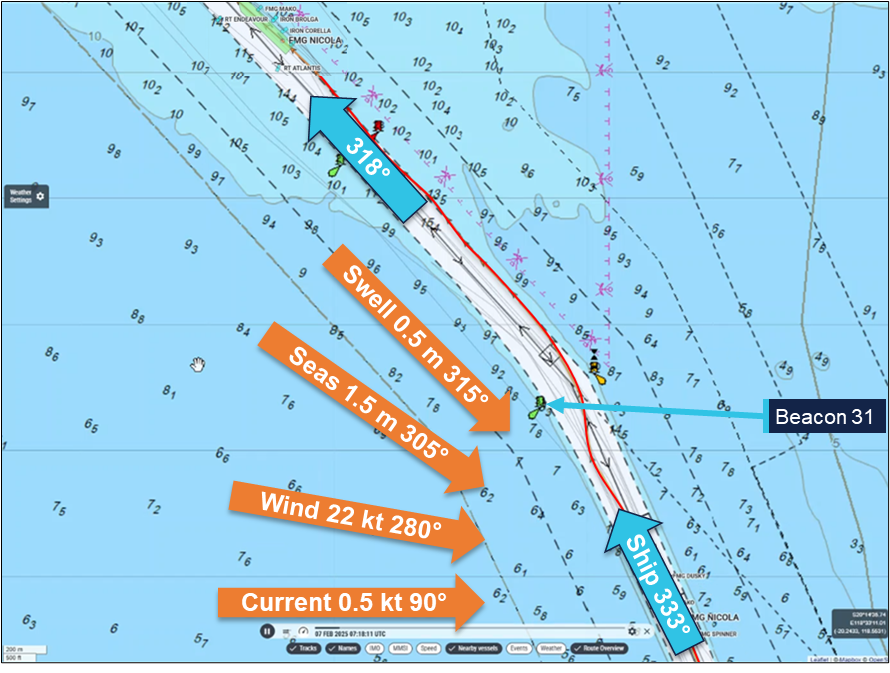
Source: Marine Traffic, Pilbara Ports Authority, annotated by the ATSB
Port Hedland port user guidelines and procedures stated that ‘average wind speeds ≥ 25 knots for 3 consecutive 10-minute intervals (were) considered to be the upper limit for handling vessels in the inner harbour and main shipping channel.’ Readings from beacon 31 showed the average wind speed to increase from 20 knots at 1400 to peak at 25 knots at about 1545, and remain at this level until after 1800. During this time, gusts to about 32 knots were recorded.
The 3 tugs assisting the ship out the channel all reported difficulties with the weather before and during the incident. FMG Mako was positioned at the port shoulder for the transit and exposed to the weather. While approaching beacons 30-31, the tug was let go and was directed to the port quarter to push up. In this location it was further hampered by the excessive movement of the tug in the prevailing conditions.
FMG Dusky’s master (starboard shoulder) reported that the weather was inclement which affected the effectiveness of the tug. During initial attempts to regain control of the ship, including applying braking force through FMG Dusky, one of the tug’s main engines shut down due to being overloaded. Power was quickly restored and the tug returned to full operation.
The master of FMG Spinner, at the centre lead aft position, reported the sea state as ‘poor, with a short, sharp, confused swell around 2 m’. During manoeuvring to take FMG Nicola’s stern to starboard, the tug shipped seas with sufficient force to shatter one of its bridge windows.
Post‑incident action
FMG Nicola
The ship’s managers (BSM) conducted an investigation, which focused on the cause of the main engine shutdown. Other interested parties also conducted independent investigations, which included inspections by the engine manufacturer and an underwater (dive) survey. All investigations concluded that the root cause of the main engine shutdown was an intermittent malfunction of the lubricating oil low pressure switch, which triggered an engine emergency stop despite all system parameters being normal.
The switch was replaced with a new spare on board and the operating point set to 160 kPa. In addition, the planned maintenance system routines were amended to require calibration of main engine LO pressure switches monthly and replacement of the shutdown switch reduced from 5 years to 2.5 years.
The ship’s hull inspections included an underwater survey. In summary, the survey report indicated that no evidence of hull or bilge keel damage was found and hull paintwork was intact. Similarly, no damage to the propeller and rudder was reported.
All inspections, testing and corrective actions were conducted to the satisfaction of the ship’s classification society.
Pilbara Ports Authority
Soon after being notified of the loss of propulsion, and before the ship exited the channel, PPA made a request to the master for reports into the incident and including root cause analysis and preventive measures. In addition, PPA conducted an investigation into the incident, which focused on the loss of propulsion, the effectiveness of pilotage and towage procedures, and the response.
The investigation made recommendations to various involved parties, including the ship’s operators and managers, and towage and pilotage organisations. Recommendations included updating pilotage emergency response procedures to consider loss of ship propulsion that affects steerage and optimal positioning and use of tugs. Additional training of pilots and tug masters, including on the hydrodynamic interaction between tugs and ships with low under keel clearance, was also advised.
Incident reporting
The Navigation Act 2012 required owners and masters of all vessels involved in a marine incident in Australian waters report it to the Australian Maritime Safety Authority (AMSA).14 The reporting involved a 2-step process by submitting an:
- incident alert form15 as soon as ‘reasonably practicable’ (within 4 hours) after the incident either online or by email to the AMSA email address identified on the form
- incident report form16 with further details within 72 hours.
Additionally, incidents were required to be reported to the ATSB in accordance with the governing legislation.17 Under this legislation, responsible persons (including the ship’s master, owner, operator or agent, the pilot, pilotage provider and VTS authority) were required to report an incident. Incident reports submitted to AMSA were forwarded to the ATSB, which allowed a responsible person to meet their Transport Safety Investigations Act reporting obligations.
Incident handling process
The AMSA Response Centre (ARC) was responsible for the receipt, assessment, triage and onward dissemination of all incident reports received by AMSA. A formal, documented procedure was followed in handling reports. All reports were assessed and classified into 4 categories:
- Red – an immediately reportable emergency such as imminent danger to the vessel, life or the environment.
- Orange – an immediately reportable incident that may require follow-up or prosecution, including fatalities, collision, breakaway, fire or explosion, grounding, serious pollution, damage which may affect safety of navigation, serious danger to the ship or persons, serious near miss.
- Yellow – a reportable incident that may require AMSA action or investigation. This category included any incident under pilotage, environmental incidents and hazards to navigation.
- Green – a reportable incident that did not meet the requirements of other categories.
Once categorised, the reports were processed as per the procedure with the levels of response and sharing of the details reducing with categories red through to green. All red and orange reports were forwarded to the ATSB. Yellow reports were forwarded to the relevant AMSA regional office and to other selected, incident-specific addresses (including the ATSB) for pollution or maritime labour convention related reports.
A process for the review of red and orange incident categorising was available for changing incident circumstances, such as severity, and for assurance and auditing purposes. Re-categorising required senior management assessment and approval.
Reporting of the incident
At 1642 on 7 February, a couple of hours after FMG Nicola’s propulsion loss, the ship’s local agent asked the master to submit the required incident reports, including the AMSA forms. Later that evening, the master emailed incident reports and supporting documents to the agent.
The following morning, 8 February, the agent forwarded the incident reports, including AMSA forms 18 and 19, and attachments, to relevant parties, including AMSA’s local office in Port Hedland. The reports were forwarded to AMSA’s incident reporting email address on 10 February.
The information in the reports indicated that the ship had not grounded and did not otherwise meet the guidelines to be categorised as red or orange. Consequently, as the incident had occurred ‘under pilotage’, it was categorised as ‘yellow’. As per procedures, the incident report documentation was not forwarded to the ATSB, but returned to the AMSA West regional office for information and review.
On 12 February, AMSA received an anonymous marine safety concern (AMSA form 355)18 of a ‘grounding event’ involving FMG Nicola that reportedly had occurred at 1412 on 8 February (the day after FMG Nicola’s departure). This report was forwarded to the AMSA West office and to AMSA’s Port Hedland office, and to the ATSB. The Port Hedland office responded that the ship’s agent and PPA had no record of a grounding event but noted there had been a stoppage of the ship’s main engine during departure (the incident reported on 10 February and categorised as ‘yellow’).
The ATSB followed up with AMSA for additional information about the anonymous report, but no further information was available. Over the following weeks, the ATSB followed up with AMSA again to check if further information, including AMSA incident report forms, was available. The ATSB was advised that no further information was available regarding a grounding, but that the ship had had a main engine failure, which did not involve grounding.
During July 2025, the ATSB became aware of media reports concerning the reported grounding of FMG Nicola while departing Port Hedland on 7 February. The ATSB followed up with AMSA and was advised that there was no information about a grounding event, other than the form 355 previously provided.
The ATSB then contacted PPA, which confirmed an incident involving a loss of the ship’s propulsion had occurred. The port authority provided copies of the incident reports and attachments that the master had submitted in February via the ship’s agent.
On 9 July 2025, after assessing the incident reports and other available information, the ATSB formally commenced this investigation.
Safety analysis
Loss of propulsion
Multiple investigations following the incident concluded that the root cause of the main engine shutdown was an intermittent malfunction of the lubricating oil (LO) low pressure switch, which triggered a main engine emergency stop, despite all system parameters being normal.
Separation between the LO shutdown system and the pressure monitoring system meant that when the shutdown switch activated, the monitoring system low LO pressure alarm was not triggered, and the pressure display did not show a fluctuation in pressure.
Inspection and testing of the shutdown pressure switch after the incident showed it to activate at 185 kPa and to operate erratically. No evidence was found to show that the failure was related to maintenance arrangements (inspection, calibration and replacement schedules); the switch had operated without any previous obvious fault.
Recovery
Following the main engine trip, the engine speed quickly dropped to zero. However, the ship’s speed fell away more slowly, due to the ship’s momentum, from 8.3 knots when the engine tripped, to 4.8 knots about 9 minutes later when the main engine was restarted.
The pilots immediately took action to control the ship’s movement and ensured steering was available. Port Hedland vessel traffic service (VTS) was notified and a ship emergency declared. In keeping with response guidelines, training and procedures, the ship was kept moving and additional assets were tasked to assist.
The ship was manoeuvred while being set to starboard and was passing between beacons 30-31 as operation of the main engine was restored. In unfavourable weather conditions, appropriate port rudder was used to manage the set to starboard and to avoid the stern swinging outside the channel and exposing the rudder and propeller to damage. Headway was maintained (minimum speed of 1.5 knots) with the main engine at half ahead (40 rpm) to keep the ship moving along the edge of the charted channel and avoid the adjacent shallow water. Beacon 28 was cleared successfully and at about 1550, 35 minutes after the initial loss of propulsion, with 7 tugs assisting, the ship was returned to the centre of the channel and safely navigated out the channel and to sea.
Inspections carried out as the ship continued to negotiate the channel and prior to departure of the pilots found no indication of water ingress or other damage. Further investigation including starboard side tank inspections, carried out at sea prior to arrival at the next port, also did not reveal any hull plating or ship structure damage. Following this, a class‑approved dive inspection found no hull or coating damage including that the bilge keels were in ‘normal’ condition.
In summary, the evidence showed that, while the ship moved along the edge of the charted channel, its hull did not contact the seabed.
Incident reporting
FMG Nicola’s loss of propulsion under pilotage met the requirements for reporting to AMSA as a marine incident. Shortly after the incident Pilbara Ports and the ship’s agent had requested incident reports from the ship’s crew, including those required by AMSA.
The morning after the incident, incident report forms were forwarded to the local Port Hedland office of AMSA. These were subsequently forwarded to the AMSA response centre. The information provided in and with the incident reports indicated that the ship lost propulsion, additional port towage assets were mobilised and the ship was safely taken to sea. The reports stated that the ship had not run aground or touched bottom. Consequently, as per AMSA procedures, the incident was assessed as being of lower severity than ‘red’ or ‘orange’ incidents and was triaged as ‘yellow’. The procedures did not require a ‘yellow’ level report to be forwarded to the ATSB.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the loss of propulsion of FMG Nicola, Port Hedland, Western Australia, on 7 February 2025.
Contributing factors
- FMG Nicola's main engine lubricating oil low pressure shutdown switch erroneously operated, causing the otherwise serviceable main engine to trip and stop.
Other factors that increased risk
- The risk of grounding increased as, while maintaining headway and avoiding damage to the stern while turning, FMG Nicola tracked along the edge of the charted channel.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action by Pilbara Ports Authority
Pilbara Ports Authority advised the ATSB that safety action had been taken, which continued the port’s focus on machinery reliability, towage effectiveness, and structured emergency response. The actions taken were applicable to 5 areas of port operations:
- Ship and machinery reliability – including increased ship vetting and inspection requirements for entry to Port Hedland.
- Towage and escort strategy – assessment of tug effectiveness and limitations, defined wind and sea state thresholds, simulations and operational trials.
- Tug management – guidance for pilot-tug communication protocols and tug release arrangements.
- Pilotage and emergency response – procedural updates to clarify roles and responsibilities during multiple pilot pilotages and emergency situations, and to improve understanding of tug use and limitations in response to an emergency.
- Training and operational awareness – to ensure that lessons learned from this incident were captured and implemented into port operations.
Safety action by FMG International
FMG International advised the ATSB that the following safety actions have been taken following this incident:
- Details of the incident and investigation outcomes were distributed to the crews of sister ships of FMG Nicola.
- Management of main engine lubricating oil pressure (MELOP) switches was updated:
- MELOP switches were renewed on sister ships of FMG Nicola
- the interval for renewal of MELOP switches was reduced from 5 years to 2.5 years on all ships in the FMG fleet
- the interval for MELOP switch testing and calibration was reduced from 3 months to 1 month on all fleet vessels
- after consulting with engine makers, the MELOP shutdown switch time delay was extended from 0.1 seconds to 1.9 seconds on all fleet vessels.
- A procedure for resetting the MELOP shut down alarm within 1 minute has been implemented fleetwide. The procedure has also been incorporated into vessel training (drills and simulations) tools and requirements.
Safety action by the Australian Maritime Safety Authority
The Australian Maritime Safety Authority has updated incident report handling and triage procedures to better ensure the ATSB is notified of reportable marine incidents under its legislative requirements. The amended procedure requires pilotage incidents be reported to the ATSB.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Australian Maritime Safety Authority
- Pilbara Ports Authority
- FMG Nicola’s master, managers and Port Hedland agent
- FMG International.
References
Rowe, R.W. (1996). The Shiphandler’s Guide. The Nautical Institute.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Australian Maritime Safety Authority
- Maritime and Port Authority (MPA) of Singapore
- Pilbara Ports Authority (PPA)
- the pilots on board during the incident
- FMG Nicola’s master
- FMG International
Submissions were received from:
- Maritime and Port Authority (MPA) of Singapore
- FMG International
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
- ^ All times referred to in this report are local time, Coordinated Universal Time (UTC) + 8 hours.
- ^ In conducting a pilotage, the pilot effectively has control of the ship’s navigation but legally only provides relevant advice to its master who remains responsible and always in command of the ship.
- ^ A shoulder is the area where a ship’s hull form changes from the bow shape to the parallel mid body.
- ^ The direction of the bow of a vessel expressed in degrees, either magnetic or true. All ship’s headings in this report are in degrees by gyro compass with negligible error.
- ^ With all engine systems verified to be operating normally, the main engine trip lockout reset required return of the engine telegraph to the stop position (on the bridge and in the machinery control room (MCR)) and operating a manual reset push-button in the MCR.
- ^ 'Bank effect' and 'shallow water effect or squat' are hydrodynamic phenomena resulting from the effects of a ship transiting close to a canal bank and in shallow water respectively. When making headway, a positive pressure is developed at the ship's bow and a stronger low pressure area at its stern. This causes the stern to be pulled towards the bank. These forces intensify significantly with increased speed or shallow water, where restricted flow further reduces buoyancy and control. Constant rudder correction is required to maintain heading control of the ship.
‘The Shiphandler’s Guide’ The Nautical Institute - ^ Capesize ships generally have dimensions larger than that allowable for transit of Panama and Suez Canals and therefore have to sail around Cape Horn and the Cape of Good Hope.
- ^ In 2001, BHP Limited merged with Billiton Plc to form BHP Billiton. In 2018, ‘Billiton’ was dropped from the organisation’s name, and it is now known as BHP.
- ^ The Pilbara Ports Authority (PPA) was established on 1 July 2014, as a result of the Ports Legislation Amendment Act 2014, which consolidated 7 of Western Australia’s 8 port authorities into 4 new regional port authorities. The PPA was formed by the amalgamation of the former port authorities of Dampier and Port Hedland and also encompassed the ports of Ashburton and Varanus Island.
- ^ A nautical mile of 1,852 m.
- ^ Port Hedland channel zones: Zone 1 – the inner harbour and berths; Zone 2 – the inner harbour and berths to the south-west of zone 1; Zone 3 – from the outer limit of the inner harbour at Hunt Point to beacons 36-37; Zone 4 – from beacons 36-37 to 30-31; Zone 5 – from beacons 30-31 to beacons 15-16; Zone 6 – from beacons 15-16 to the termination of the channel at beacons C1-C2.
- ^ Available at www.pilbaraports.com.au
- ^ The pulling power of a tug, expressed in tonnes.
- ^ Sections 185 and 186 of the Navigation Act 2012 (Cth), Incident reporting | AMSA.
- ^ Incident alert form 18, available at www.amsa.gov.au.
- ^ Incident report form 19, available at www.amsa.gov.au.
- ^ Transport Safety Investigation Act 2003 (TSI Act), refer to Marine accident or incident notification | ATSB.
- ^ Report of marine safety concern (form 355) | Australian Maritime Safety Authority
- ^ FMG International (subsidiary of Fortescue Ltd) acted primarily as owner’s representative for Fortescue owned ore carriers, managing vessels technical and crew ship management, performed through 3rd party vessel technical/crew managers.
Interim report
Report release date: 09/10/2025

| This interim report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Interim reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this interim report is released in accordance with section 25 of the Transport Safety Investigation Act 2003. |
The occurrence
At 0832 local time on 7 February 2025, the 327 m bulk carrier FMG Nicola (image above) completed loading 237,088 t of iron ore at its berth in Port Hedland, Western Australia. The fully laden ship had a draught of 17.51 m forward and 17.69 m aft and was due to depart its berth in the afternoon (a high water of 5.56 m was predicted for 1634).
At 1330, 2 harbour pilots, one of whom was under supervision, boarded the ship. The port authority’s marine services delivery manager (MSDM), who was also a harbour pilot, boarded to observe the departure. By 1348, the ship’s main engine and steering had been satisfactorily tested and the master-pilot information exchange was completed in readiness for departure. The pilot under supervision would conduct[1] the pilotage and 4 tugs were secured to assist (see the section titled Towage).
By 1412, all mooring lines had been cast off and the ship departed the berth (Figure 1). There was a 25-knot north‑north‑west wind with waves of up to 1.5 m on a 0.5 m swell in the area, including the port’s single shipping channel.
Figure 1: Overview of FMG Nicola's track through shipping channel
Source: Australian Hydrographic Office, data from Australian Maritime Safety Authority
At 1442, with the ship progressing along the channel as planned, the MSDM disembarked via pilot launch. At 1446, one of the tugs was let go and returned to base.
At about 1500, FMG Nicola was turned to port to follow the channel at a speed of about 7 knots. Of the 3 tugs assisting, FMG Mako was fast at the ship’s port shoulder,[2] FMG Dusky at the starboard shoulder and FMG Spinner through the centre lead aft.
At 1514, as the ship approached beacons 32-33 (Figure 1), the pilot ordered a heading[3] of 334°. At about this time, FMG Mako’s master requested the pilot for its towline to be let go as there were choppy seas on the ship’s port side. The pilot concurred, and the towline was let go at 1515.
Soon after, at about 1516, FMG Nicola’s main engine suddenly shut down as it was passing beacons 32-33 (Figure 2). The ship’s speed was 8.3 knots and the pilot ordered the rudder midships. The pilot informed the tug masters that the ship had lost propulsion and directed them to help keep it in the channel.
Figure 2: FMG Nicola track from about 1516 to 1552
Source: Australian Maritime Safety Authority, Marine Traffic, annotated by the ATSB
At 1518, the pilot notified Port Hedland vessel traffic service (VTS) of the emergency and requested additional tugs. The pilot gave helm orders and used the tugs to follow the channel. The ship’s speed had decreased to 7.4 knots and it was getting closer to the western side of the channel and with a slow rate of turn of about 4° per minute to port (Figure 3).
Figure 3: FMG Nicola speed and rate of turn at the time of the incident
Graph derived from Automatic Identification System data and should not be used for further analysis. Source: Australian Maritime Safety Authority, analysis by the ATSB
Meanwhile, the ship’s engineers identified that the engine had shut down as the ‘main bearing and thrust bearing lubricating oil pressure low’ non‑cancellable trip had activated. The engineers determined that it had activated due to faulty operation of the pressure switch. After confirming all engine systems were operating normally, the engine trip lockout system[4] was reset and, at 1523, the engine was restarted at dead slow ahead.
At about 1525, FMG Nicola had passed beacons 30-31, and, with a rate of turn 7.5° per minute to port and speed of 4.3 knots, it closed on the eastern side of the channel. Soon after, the ship stopped turning and began moving along the side of the channel, which was aligned along a 318° (T) direction there.
The ship continued to move along the side of the channel (Figure 2). At 1534, the first of the additional tugs arrived and was tasked to push up on the ship’s starboard side. In the following 10 minutes, 3 more tugs arrived and assisted as required by the pilot. At 1540, the ship passed close to beacon 28 while moving along the side of the channel at a speed of 2.5 knots.
By 1550, the ship had been moved away from the channel side and its speed was increasing as the main engine speed had progressively been increased to full ahead. The tugs continued escorting the ship out the channel towards open water.
At about 1635, 3 tugs were released and a further 2 were released about 10 minutes later as the ship approached beacons C11-C12. The remaining 2 tugs were retained and escorted the ship until it passed beacons C1-C2 and to sea.
By the time the ship passed beacons C1-C2, the ship’s crew had completed inspecting and testing the main engine systems and rectified the fault. They had also conducted an inspection, including sounding compartments, to confirm there was no ingress of water.
Shortly after, at 1806, the pilots departed the ship by helicopter and the ship continued its passage to the next port, Dongjiakou, China.
During the passage, the crew inspected all ballast tanks on the starboard side and found no physical damage to the ship’s side or structure.
Context
FMG Nicola
General details
FMG Nicola was a Singapore-registered, capesize[5] bulk carrier built in 2016 by Jiangsu Yangzi Xinfu Shipbuilding, China. At the time of the incident, the ship was owned and operated by Fortescue Shipping Nicola, managed by Bernhard Schulte Shipmanagement (BSM), Hong Kong, and classed with Lloyd’s Register (LR).
At the time of the incident, FMG Nicola was crewed by 23 Sri Lankan and Indian nationals, including the master, all appropriately qualified for their positions on board.
The master had 26 years of seagoing experience, all on bulk carriers, with about 4 years in command. The master joined Bernhard Schulte Shipmanagement in 2015 and had completed several assignments on FMG Nicola since 2021.
The chief engineer had about 18 years of seagoing experience, with about 9 years at that rank. The chief engineer joined Bernhard Schulte Shipmanagement in September 2024 and was assigned to work on FMG Nicola.
Main engine
FMG Nicola’s propulsion was provided by a 6‑cylinder, MAN‑B&W 6G80ME‑C9.5 engine developing 18,240 kW. The main engine drove a single 4‑blade, fixed‑pitch propeller, providing a service speed of 14 knots.
Lubricating oil system
The main engine lubricating oil (LO) system was fitted with a hierarchy of oil pressure monitoring and alarm controls to limit inadvertent engine stoppage while preventing catastrophic engine damage. In addition to local, analogue indicators and pressure gauges, the LO pressure was monitored via a pressure transducer and pressure switches (Figure 4).
Signals from the sensors fed into the ship’s machinery alarm, monitoring and control system. This system provided real time, remote indication of the LO pressure. Software limits were incorporated to trigger alarms and other actions. Normal operating pressure for the system was about 250 kPa with software triggers set at:
- 210 kPa for standby pump start
- 200 kPa for low LO pressure alarm
- 180 kPa for main engine slow down alarm.
In addition to these triggers and alarms, the main engine LO system had a separate pressure switch set to activate at 160 kPa. This switch, independent of the oil pressure monitoring circuit, was for the main engine low LO pressure shutdown. This initiated rapid shutdown of the engine to prevent catastrophic damage due to complete loss of bearing lubricating oil.
Figure 4: Main engine lubricating oil pressure sensing and switches

Source: Fortescue Metals Group
The normal, expected, sequence of loss of LO pressure indications would follow persistently falling oil pressure: standby pump start, low pressure alarm and main engine automatic slow down prior to main engine shutdown.
The machinery monitoring system allowed for (adjustable) time delays on activation of each of these triggers. At the time of the incident, the engine LO pressure shutdown delay was set to 0.1 s (following subsequent advice from the engine manufacturer that the delay could be increased up to 2 s, it was reset to 1.9 s).
Components of the main engine LO system were subject to regular maintenance through the ship’s planned maintenance system (PMS). The PMS records showed that the main engine pressure transmitter and pressure sensors had last been checked on 15 November 2024 (about 3 months before the incident).
Post‑incident action
The ship’s managers (BSM) conducted an investigation, which focused on the cause of the main engine shutdown. Other interested parties also conducted independent investigations, which included inspections by the engine manufacturer and an underwater (dive) survey. All investigations concluded that the root cause of the main engine shutdown was a faulty lubricating oil low pressure switch which triggered an engine emergency stop despite all system parameters being normal.
The separation between the LO shutdown system and the pressure monitoring system meant that when the shutdown switch activated, the monitoring system low LO pressure alarm was not triggered, and the pressure display did not show a fluctuation in pressure.
Inspection and testing of the shutdown pressure switch showed it to activate at 185 kPa and to operate erratically. The switch was replaced with a new spare on board and the operating point set to 160 kPa. In addition, the planned maintenance system routines were amended to require calibration of main engine LO pressure switches monthly and replacement of the shutdown switch reduced to 2.5 years (from 5 years).
The ship’s hull inspections included an underwater survey. In summary, the survey report indicated that no evidence of hull or bilge keel damage was found and the hull paint was intact. Similarly, no damage to the propeller and rudder was reported.
All inspections, testing and corrective actions were conducted to the satisfaction of Lloyds Register, the ship’s Classification Society.
Port Hedland
General information
Port Hedland, situated in the Pilbara region of Western Australia, is the world’s largest bulk export port by tonnage, handling over 500 million tonnes of cargo annually. More than 95 per cent of this volume is iron ore, exported primarily by BHP,[6] Fortescue Metals Group (FMG) and Roy Hill Infrastructure, with the port serving as the companies’ main export hub for all Pilbara output. In addition to iron ore, the port also handles exports of salt, manganese, copper concentrates, lithium minerals and livestock.
At the time of the incident, the port’s infrastructure comprised 19 operational berths. Eight of these berths were owned and operated by BHP, with the remaining berths owned and operated by FMG (5 berths), Roy Hill (2 berths) and Pilbara Ports Authority[7] (4 berths). Shipping activity is significant, with more than 6,000 ship movements (inbound and outbound) each year.
Shipping channel
Access to the port was provided by a single 22‑mile[8] dredged channel, which allowed only one large ship to pass at a time. For most laden ships, particularly capesize ships, such as FMG Nicola, use of the channel was restricted by tidal conditions. The incident took place within the 10‑mile section of the channel closest to the port, an area prone to strong tidal flows and with particularly confined spaces, narrowing to a minimum width of 162 m and featuring steep batter slopes. The channel depth in this section was maintained at about 15 m, while adjacent waters were generally about 6 m deep.
The features of the channel described above make the risks associated with channel blockage high. A disabled ship can strand on a receding tide as well as blocking the passage of other ships. Depending on departure times, separation between ships and the location of an incident, up to 3 additional ships could be committed to, or within, the channel and exposed to this hazard at a given time.
Pilbara Ports Authority
The port was managed by the Pilbara Ports Authority (PPA), which had overarching responsibility for safety and efficiency of port operations and the environment under state legislation. The PPA’s jurisdictional responsibilities were exercised through the Port Hedland harbour master.
The harbour master’s responsibilities included the coordination of vessel traffic services, ship scheduling, pilotage and maintenance of shipping channels, navigational aids and port infrastructure. The PPA issued third‑party contracts or licences for stevedoring, towage, some pilotage services and pilot transfers (helicopter and boat).
Pilotage
Vessels 35 m or greater in length using the main shipping channel and navigating within port limits were required to use the services of a licenced harbour pilot. Pilotage services for the port were provided by PPA through directly employed pilots as well as by third‑party, contracted providers.
The pilots on board FMG Nicola at the time of the incident were employed by PPA. All PPA pilots had undertaken a competency‑based pilotage training program incorporating on‑water and simulator training and competency assessments.
The supervising pilot had worked for PPA since 2023. They had over 25 years of experience in the maritime industry, including positions as a marine pilot in Brisbane, Queensland, as an LNG loading master and as Senior Advisor Seafarer Standards with AMSA.
The pilot under supervision joined PPA in 2024 after more than 15 years as a pilot in Ningbo‑Zhoushan, China. At the time of the incident, they held a level 3 authority to pilot in Port Hedland and were undertaking supervised pilotages to upgrade this licence to level 4.
Towage
The Port of Port Hedland - Port User Guidelines and Procedures documented the tug allocation requirements based on specified criteria. Laden outbound capsize ships required 4 tugs secured to the ship from the berth to Hunt Point, near the harbour entrance. The requirement for the transit from Hunt Point to beacons 31/30 was 3 tugs.
Tugs in Port Hedland were operated under towage licences granted by the PPA to Pilbara Marine (a subsidiary of FMG) and BHP Towage Services (BHPTS). KOTUG operated tugs under the Pilbara Marine towage licence while Rivtow was contracted to operate the tugs under the BHPTS licence.
The 4 tugs assigned to FMG Nicola on the day of the incident were ART85‑32W class advanced rotortugs, operated by KOTUG. Each tug had a bollard pull[9] of 85 tonnes and used a hybrid propulsion arrangement with 2 azimuth thrusters forward and a third azimuth thruster aft.
The tugs which came to render assistance after FMG Nicola lost propulsion were operated by Rivtow and comprised of 2 ART80‑32 rotortugs and 2 RAstar85 azimuth stern drive (ASD) tugs.
Investigation into incident
Pilbara Ports Authority conducted an investigation into this incident, which focused on the loss of propulsion, the effectiveness of pilotage and towage procedures, and the response. The investigation recommended updating pilotage emergency response procedures to consider loss of ship propulsion resulting in loss of steerage and optimal positioning and use of tugs. Another recommendation was the additional training of pilots and tug masters, including on the hydrodynamic interaction between tugs and ships with low under keel clearance.
Incident reporting
The Navigation Act 2012 required owners and masters of all vessels involved in a marine incident in Australian waters report it to the Australian Maritime Safety Authority (AMSA).[10] The reporting involved a 2-step process by submitting an:
- incident alert form[11] as soon as ‘reasonably practicable’ (within 4 hours) after the incident either online or by email to the AMSA email address identified on the form.
- incident report form[12] with further details within 72 hours.
Additionally, incidents were required to be reported to the ATSB in accordance with the governing legislation.[13] Under this legislation, responsible persons (that in summary, included the ship’s master, owner, operator, agent, the pilot, pilotage provider and VTS authority) were required to report an incident. Incident reports submitted to AMSA are forwarded to the ATSB, which allowed a responsible person to meet their TSI Act reporting obligations.
Reporting of the incident
At 1642 on 7 February, a couple of hours after FMG Nicola’s propulsion loss, the ship’s local agent asked the master to submit the required incident reports, including the AMSA forms. Later that evening, the master emailed incident reports and supporting documents to the agent.
The following morning, 8 February, the agent forwarded the incident reports, including AMSA forms 18 and 19, and attachments to relevant parties, including AMSA’s local office in Port Hedland. The reports were forwarded to AMSA’s incident reporting email address on 10 February. The notifications submitted by FMG Nicola’s master regarding the loss of propulsion incident did not, at that time, reach the ATSB.
On 12 February, AMSA received an anonymous marine safety concern (AMSA form 355) of a ‘grounding event’ involving the ship that reportedly had occurred at 1412 on 8 February (the day after FMG Nicola’s departure). This report was forwarded to the ATSB and AMSA’s offices in Fremantle and Port Hedland. The Port Hedland office reported back that the ship’s agent and PPA had no record of a grounding event, but noted there had been a stoppage of the ship’s main engine during departure.
The ATSB immediately followed up AMSA for information about the anonymous report but no further information was reportedly available. Over the following weeks, the ATSB followed up with AMSA to check if further information, including AMSA incident report forms, had become available. The ATSB was advised no further information was available.
In July of 2025, the ATSB became aware of media reports about the grounding of FMG Nicola while departing Port Hedland on 7 February. The ATSB again followed up with AMSA and was advised that there was no information about such an incident, other than the form 355 previously provided.
The ATSB then contacted PPA, which confirmed an incident involving a loss of the ship’s propulsion had occurred. The port authority also provided copies of the incident reports and attachments that the master had submitted in February via the ship’s agent.
On 9 July 2025, after assessing the incident reports and other available information, the ATSB formally commenced an investigation into this incident and its reporting.
Further investigation
To date, the ATSB has collected evidence from relevant parties including:
- AMSA
- PPA
- FMG Nicola’s master
- FMG Nicola’s managers
- FMG Nicola’s local agent
- FMG International.[14]
The investigation is continuing and will include examination and analysis of the evidence received, including:
- event sequence
- corroborating data
- ship track and position
- response to the incident
- reporting of the incident to authorities.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] In conducting a pilotage, the pilot effectively has control of the ship’s navigation but legally only provides relevant advice to its master who remains responsible and always in command of the ship.
[2] A shoulder is the area where a ship’s hull form changes from the bow shape to the parallel mid body.
[3] The direction of the bow of a vessel expressed in degrees, either magnetic or true. All ship’s headings in this report are in degrees by gyro compass with negligible error.
[4] With all engine systems verified to be operating normally, the main engine trip lockout reset required return of the engine telegraph to the stop position (on the bridge and in the machinery control room (MCR)) and operating a manual reset push-button in the MCR.
[5] Capesize ships generally have dimensions larger than that allowable for transit of Panama and Suez Canals and therefore have to sail around Cape Horn and the Cape of Good Hope.
[6] In 2001, BHP Limited merged with Billiton Plc to form BHP Billiton. In 2018, ‘Billiton’ was dropped from the organisation’s name, and it is now known as BHP.
[7] The Pilbara Ports Authority (PPA) was established on 1 July 2014, as a result of the Ports Legislation Amendment Act 2014 which consolidated 7 of Western Australia’s 8 port authorities into 4 new regional port authorities. The PPA was formed by the amalgamation of the former port authorities of Dampier and Port Hedland and also encompassed the ports of Ashburton and Varanus Island.
[8] A nautical mile of 1,852 m.
[9] The pulling power of a tug, expressed in tonnes.
[10] Sections 185 and 186 of the Navigation Act 2012 (Cth), Incident reporting | AMSA.
[11] Incident alert form 18, available at www.amsa.gov.au.
[12] Incident alert form 19, available at www.amsa.gov.au
[13] Transport Safety Investigation Act 2003 (TSI Act), refer to Marine accident or incident notification | ATSB
[14] FMG International (subsidiary of Fortescue Ltd) acted primarily as owner’s representative for Fortescue owned ore carriers, managing vessels technical and crew ship management, performed through 3rd party vessel technical/crew managers.
Occurrence summary
| Investigation number | MO-2025-007 |
|---|---|
| Occurrence date | 07/02/2025 |
| Occurrence time and timezone | 1516 Western Standard Time (UTC + 8 hours) |
| Location | 6.5 km due north of Port Hedland |
| State | Western Australia |
| Report release date | 12/06/2026 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Marine |
| Marine occurrence category | Machinery failure |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Ship details
| Name | FMG Nicola |
|---|---|
| IMO number | 9747778 |
| Ship type | Dry bulk (ore) carrier |
| Flag | Singapore |
| Classification society | Lloyd's Register |
| Owner | Fortescue Shipping Nicola, Singapore |
| Manager | Bernard Schulte Shipmanagement, Hong Kong |
| Departure point | Port Hedland, Western Australia |
| Destination | Dongjiakou, China |
| Injuries | None |
| Damage | Nil |