
Mona Vale light aircraft accident
The Australian Transport Safety Bureau (ATSB) is calling for witnesses who have video of Sunday’s aircraft accident at the Mona Vale Golf Course, on Sydney’s Northern Beaches, to make contact via our website.
The Piper PA-28-140 Cherokee had departed Camden Airport and was conducting a training flight with a pilot and instructor on board when it reportedly experienced engine power loss.
As part of the evidence-gathering phase of the investigation, ATSB transport safety investigators will interview the pilots, other involved parties and witnesses, and collect available recorded information, including footage and ADS-B flight tracking data, as well as weather information and pilot and aircraft maintenance records.
Investigators may also seek to recover any relevant aircraft componentry from the aircraft for further examination at the ATSB’s technical facilities in Canberra.
The ATSB calls for anyone who may have footage of the aircraft in any stage of its flight to submit it via atsb.gov.au/witness.
The ATSB will publish a final report at the conclusion of its investigation, detailing findings and the analysis to support those findings.
However, should a critical safety issue be identified at any stage during the investigation, the ATSB will immediately notify relevant parties so safety action can be taken.
Wheels up landing involving a Lancair 200 amateur-built aircraft, Aldinga Aerodrome, South Australia, on 31 July 2025
What happened
On 31 July 2025, at 12:10 local time, a Lancair 200 landed wheels up at Aldinga Aerodrome, South Australia after a short flight from Murray Bridge Aerodrome, South Australia. The pilot and passenger on board were uninjured.
After joining the circuit at Aldinga Aerodrome, the pilot identified that they were 100 ft below the normal circuit height while turning downwind. The pilot decided not to lower the landing gear at that time to allow a faster climb back to circuit height.
Once they regained circuit height, the pilot continued their landing sequence but forgot to extend the landing gear. During the final approach check, the pilot checked the mixture and propeller but did not detect that the ‘three green’ landing gear indication lights were not illuminated, which indicated the landing gear had not been extended. The aircraft was also fitted with a bright amber warning light that illuminates when the landing gear is up, the flaps are down, and the aircraft is below 800 ft above the ground as determined by GPS. The pilot reported that bright sun glare may have hindered their perception of the LED undercarriage lights and the warning light on the panel.
The aircraft touched down smoothly on the runway and gradually slid from the tarmac to the grass verge where it came to rest after travelling about 100 m after contact with the runway (Figure 1).
Figure 1: Aircraft skidding off the runway

Source: Darren Campbell Photography
The pilot radioed their position to a following aircraft; in response this aircraft went around. Once stopped, the pilot shut down the aircraft master, switches and fuel before ordering the evacuation.
Nil injuries and minimal damage were reported.
Safety action
The pilot reported that once the aircraft is repaired, they will add an audible warning alert to help reinforce the visual indication of the landing gear.
Safety message
Normal limitations of human memory make it difficult to ‘remember to remember’ to perform future tasks (such as extending the landing gear) if not prompted by a salient cue.
Pilots must ensure that all pre-landing checklists are carried out systematically as detailed in the flight manual. If interrupted, it is best practice to start again from the beginning to ensure that nothing is missed.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2025-035 |
| Occurrence date | 31/07/2025 |
| Location | Aldinga Aerodrome |
| State | South Australia |
| Occurrence class | Serious Incident |
| Aviation occurrence category | Wheels up landing |
| Highest injury level | None |
| Brief release date | 21/08/2025 |
Aircraft details
| Manufacturer | Amateur Built Aircraft |
|---|---|
| Model | Lancair 200 |
| Sector | Piston |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Murray Bridge Aerodrome, South Australia |
| Destination | Aldinga Aerodrome, South Australia |
| Damage | Minor |
Aerobridge collision with parked aircraft events, Brisbane Airport, Queensland, on 18 June and 26 July 2025
Final report
Report release date: 02/04/2026
Investigation summary
What happened
On 2 separate occasions in 2025, the Gate 82 aerobridge at the Brisbane International Airport Terminal collided with 2 narrow-body Boeing 737 aircraft, registrations VH-VZG (18 June) and DQ-FAE (26 July 2025).
The aerobridge operators, from 2 separate airlines, intended to drive the aerobridge parallel to the parked aircraft on the bay from the aerobridge home position prior to docking. However, the aerobridge moved diagonally towards the aircraft until the bottom right corner of the aerobridge impacted the aircraft and broke through the aircraft cockpit windshield. The collisions resulted in minor damage on both occasions with no recorded injuries.
What the ATSB found
Visibility of narrow-body aircraft was restricted from the aerobridge home position due to the required parking location of narrow-body aircraft, to the far right of the aerobridge home position. In addition, the design of the aerobridge cab walls, which lacked viewing windows installed in some other aerobridges at the airport, also limited direct visibility.
Both operators did not have visual reference of the aircraft prior to the collisions but expected to gain visibility following aerobridge extension. This expectation was reinforced by previous successful operations and was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft.
Both operators had moved the joystick to a 3 o’clock position and believed they were moving the aerobridge parallel to the aircraft. However, the aerobridge moved diagonally towards the aircraft. Both operators had rotated the cab left and were unaware that this orientation changed the direction of travel of the aerobridge. The operators were not alerted to the diagonal movement because they could not see the aircraft and perceived no other information to challenge their spatial orientation.
The ATSB identified that Brisbane Airport Corporation’s training material and in-cab instructions did not provide direction to operators to gain and maintain visibility of the aircraft from the home position, before moving the aerobridge.
Safety features designed to prevent collisions and damage to aircraft did not activate due to the approach angle of the aerobridge.
In the first occurrence an engineer on the ground activated the aerobridge emergency stop button to prevent further damage to the aircraft.
What has been done as a result
Following the occurrences in August 2025, Brisbane Airport Corporation (BAC) disseminated a safety notice to all operators that emphasised the requirement to rotate the cab towards the aircraft, always maintain positive line-of-sight with the aircraft, and cease operations if visual reference is lost.
BAC also reviewed the operator training material and identified gaps and an opportunity to be more specific in the process to safely attach aerobridges (similar to aerobridge 82) to aircraft. The training was updated in January 2026. Obsolete and inconsistent in‑cab instructions are in the process of being removed and will not be replaced in the aerobridge cabs.
BAC also created a new role focused on airside performance of assets and operators, including aerobridges, and all supporting infrastructure tools the operators use. Quality assurance activities have commenced with the role in place.
An aerobridge replacement program will renew 8 aerobridges at Brisbane Airport, including the aerobridge at Gate 82, commencing in 2026 at the International Terminal. BAC will review safety features and narrow-body visibility will be reviewed as part of this program. BAC is also planning to trial automated docking of aerobridges in the first half of 2026.
Fiji Airways has temporarily introduced a second operator as a ‘spotter’ at Gate 82 pending the release of this report.
Safety message
There are many risk controls in place at airports and within ground handling companies and airlines to help minimise the hazards associated with airport ground operations.
Visibility of aircraft is critical for safe aerobridge operations. Aerobridges should be designed to maximise visibility and aerobridge training should reinforce visibility as a critical step in safe operations.
Aerobridge training and operational documentation should also highlight the mental rotation required for operators when joystick movement is relative to the orientation of the cab and not fixed to the direction of the aerobridge tunnel, or other stationary visual references outside the aerobridge.
The occurrences
Aerobridge operation – both occurrences
On 2 separate occasions, during aircraft arrival at the bay at night, prior to passenger disembarkation, the aerobridge at Gate 82 of the international terminal at Brisbane Airport collided with 2 different aircraft, resulting in minor damage to the cockpit windshields.
The first aircraft was a B737-838 narrow-body operating as Qantas flight QF186 (VH‑VZG), from Queenstown, New Zealand, on 18 June 2025.
The second aircraft was a B737-8 MAX narrow-body operating as Fiji Airways flight FJ923 (DQ-FAE), from Nadi, Fiji, on 26 July 2025.
On both occasions, the aircraft were correctly parked in the designated marshaller’s position[1] for a Boeing 737 (Figure 1), in line with the visual docking guidance system (VDGS).
Figure 1: Overview of aerobridge operational area

Source: Brisbane Airport Corporation
On both occasions, the aerobridge was operated at night (Figure 2). Rain was present in the area prior to the second event on 26 July 2025, with water visible on the ground (Figure 2, right).
After receiving visual confirmation from ground staff to indicate the wheels were chocked and the park brake was released, both operators activated the aerobridge by swiping their security identity card at the operator console and then initiated movement from the default home position (Figure 2).
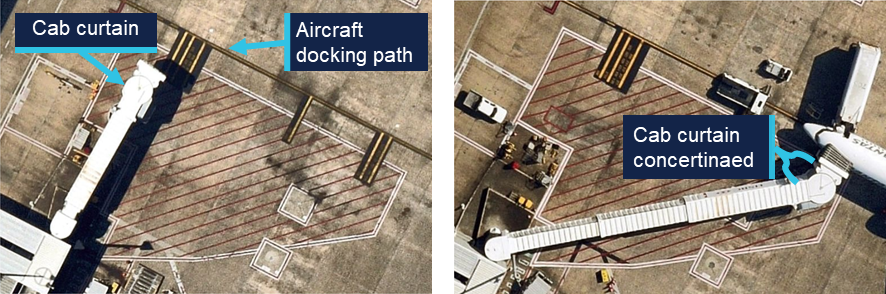
Figure 2: Home position of aerobridge with parked QF186 (left) and FJ923 (right)

Source: Brisbane Airport Corporation
Closed circuit television (CCTV) showed that at about 30 seconds into the aerobridge extension (halfway through), and while moving diagonally, the aerobridge cab was rotated to the left as identified by contraction of the concertinaed side curtain (Figure 3).
Figure 3: Left orientation of cab at 1845, 18 June 2025 (left) and 2304, 26 July 2025 (right)

Source: Brisbane Airport Corporation, annotated by the ATSB
During this time, the aerobridge continued to move diagonally towards the aircraft before the bottom right corner of the aerobridge impacted the aircraft windshield.
Both operators expected to gain visibility of the aircraft from the cab window during the aerobridge extension from the home position. They both reported previous successful operations where gaining visibility of the aircraft was delayed, but always occurred, and both stated that they were surprised by the unexpected collision.
While glass fragments entered the cockpit, and a jolt occurred, no injuries resulted to crew or passengers on either occasion. The aircraft windshields were subsequently replaced, and pressurisation was checked before both aircraft continued operations. The aerobridge was also assessed, however no faults were identified, and a return to service check was conducted before further operations on each occasion.
Occurrence 1 details
At 1845 on 18 June 2025, aerobridge 82 was being operated by a Qantas customer service agent (Operator 1) to disembark QF186 (VH-VZG), a B737-838 narrow-body aircraft after arrival from Queenstown, New Zealand.
At 1846 the right aircraft windshield was impacted by the front right aerobridge corner (Figure 4, left). A licensed aircraft maintenance engineer (LAME) was on the ground assessing the aircraft following a potential bird strike. They detected abnormal operation of the aerobridge and attempted to alert the aerobridge operator by hand gestures before activating the on-ground emergency stop at the same time as the impact.
From the cockpit, 2 flight crew members noticed the aerobridge approaching the aircraft from a high angle and further towards the nose of the aircraft than usual. The captain pressed the ground call switch on board to contact engineering or other ground staff to advise them of their urgent concern that the aerobridge was likely to impact the aircraft.
The crew were unable to make contact with engineering or ground staff before the aerobridge collided with the first officer’s windshield, shattering the glass (Figure 4, right). Although the glass fragments landed on the first officer, they were uninjured. The flight crew reported a jolt at impact, however, no passengers or cabin crew were injured.
Figure 4: Collision and damage to QF186

Occurrence 2 details
At 2304 on 26 July 2025, aerobridge 82 was being operated by a Fiji Airways customer service agent (Operator 2) to disembark FJ923 (DQ-FAE), a B737-8 MAX narrow-body aircraft after arriving from Nadi, Fiji.
At 2305 the left aircraft windshield was impacted by the front right aerobridge corner (Figure 5, left). From the cockpit, 2 flight crew members noticed the unusual movement of the aerobridge towards the aircraft, aligned with the windshield (rather than the side of the fuselage). They expected the movement to stop, but it continued until impact.
Although glass fragments and the corner of the aerobridge partially entered the cockpit (Figure 5, right), the captain was able to move out of their seat and they were uninjured. The flight crew reported a jolt at impact; however, no passengers or cabin crew were injured.
Figure 5: Collision and damage to FJ923

Source: Brisbane Airport Corporation
Context
Personnel information
Both aerobridge operators were airline customer service agents employed directly by airlines. Their normal tasking involved customer-facing pre-flight and post-flight services as well as ground operations support.
Operator 1 (Qantas) was certified in January 2024, and Operator 2 (Fiji Airways) was certified in June 2024, both were certified to operate international aerobridges, including aerobridge 82. At the time of the occurrences Operator 1 had 17 months experience and Operator 2 had 13 months experience in operating aerobridges.
Operator 1 had controlled aerobridge 82 within 3 months of the occurrence and Operator 2 had controlled aerobridge 82 within 2 months of the occurrence.
Both operators reported adequate prior sleep and recalled feeling fully alert at the time of the occurrences.
Aircraft information
Both aircraft were Boeing B737 narrow-body aircraft. VH-VZG (QF186) was a Boeing 737‑838 and DQ-FAE (FJ923) was a B737-8 MAX.
Meteorological information
Dark night conditions were present in both occurrences, and the operational area was illuminated with bright lights (Figure 2).
No significant weather was recorded prior to the first occurrence on 18 June 2025. In contrast, rain occurred at Brisbane Airport on 26 July 2025, and precipitation was present in the area prior to the second occurrence.
Aerobridge information
An aerobridge (or passenger boarding bridge) is an enclosed, elevated passageway which extends from an airport terminal gate to an aircraft.
Five types of aerobridges were in operation at Brisbane Airport across the international and domestic aprons, these ranged from fixed or pedestal aerobridges to moveable or apron drive aerobridges.
Aerobridge 82
The aerobridge at Gate 82 of the Brisbane international terminal was a Jetway Apron Drive Aerobridge. It was installed in 1995 and was in continued service for 30 years at the time of both occurrences.
As a telescopic bridge, aerobridge 82 was used for a wide range of aircraft and parking positions. The aerobridge could swing up to 180 degrees (clockwise and counterclockwise) across the bay and extend, raise or lower depending on the aircraft size. Fiji Airways used aerobridge 82 mostly for narrow-body aircraft, while Qantas used aerobridge 82 for mostly wide-body aircraft, and narrow-body aircraft on occasion.
- A prime factor determining the parking position of the aircraft and therefore the required orientation and extension length of the aerobridge was maintaining aerobridge slope as close to the design limit of 1:14. For example, if the aerobridge was to rise 1 m, then it also needs to extend by 14 m to maintain suitable slope.
Another factor determining the parking position of the aircraft was the aircraft length forward from the wings (Figure 6):
- Wide-body aircraft fuselage length from the wings forward is relatively long. The designated parking position provided sufficient clearance for the wings from the aerobridge passenger tunnel. When in the designated parking position, the left‑front door lined up with the aerobridge and the required aerobridge extension was minimal.
- Narrow-body aircraft fuselage length from the wings forward is relatively short and require parking further from the aerobridge home position to maintain clearance of the left wing and the aerobridge passenger tunnel. The aerobridge required further extension to the right to line up with the left-front door of the aircraft for aerobridge attachment.
Figure 6: Schematic drawing showing aerobridge movement in relation to a wide-body and narrow-body aircraft

Source: Brisbane Airport Corporation, modified by the ATSB
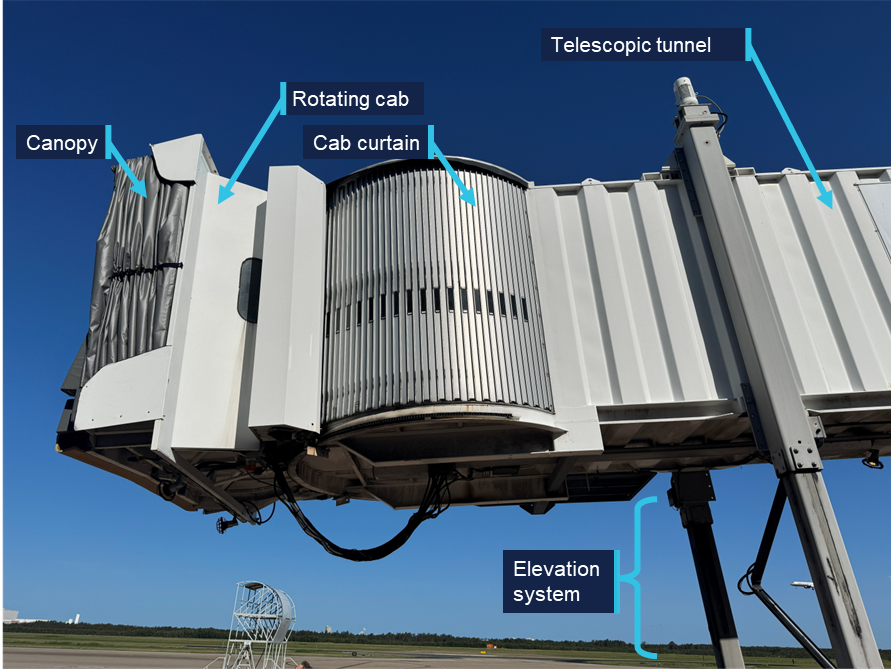
The aerobridge was formed by the following main elements (Figure 7 and Figure 8):
- rotunda with column
- canopy (which closes on to aircraft once the aerobridge is docked)
- bumper with bumper proximity switches
- slow down sensor located under the cab floor
- rotating cab and cab curtain
- telescopic tunnels (which extend and retract)
- elevation and traveling systems.
Figure 7: Front view of aerobridge 82 in the home position

Source: ATSB
An external/on ground emergency stop button was located above the aerobridge wheels (Figure 7).
Figure 8: Side view of aerobridge 82 in the home position
Source: ATSB
Home position
Before and after aerobridge operations, the aerobridge returned to a default home position (Figure 7) where the:
- wheels faced forward within a red home position box marked on the ground
- telescopic tunnel retracted and sat perpendicular to the passenger walkway
- rotating cab faced directly forward
- height was set to 3.57 m.
The home position ensured safe clearance for parking aircraft wing tips, engines and fuselage. Pre-positioning of aerobridge 82 prior to aircraft arrival was previously considered by BAC, however, was removed following safety concerns.
Operator console
The aerobridge was operated using controls mounted on a console on the left side of the cab (Figure 9). The console was positioned and orientated to provide the operator a clear view of aircraft in front during final aerobridge manoeuvring and docking. The operator stood on a slightly raised step below the console.
The step and the console moved together left or right as the cab was rotated, while the circular cab floor remained stationary,[2] and the cab side curtains concertinaed (folded in) or expanded (folded out).
Figure 9: Example operator standing at operator console
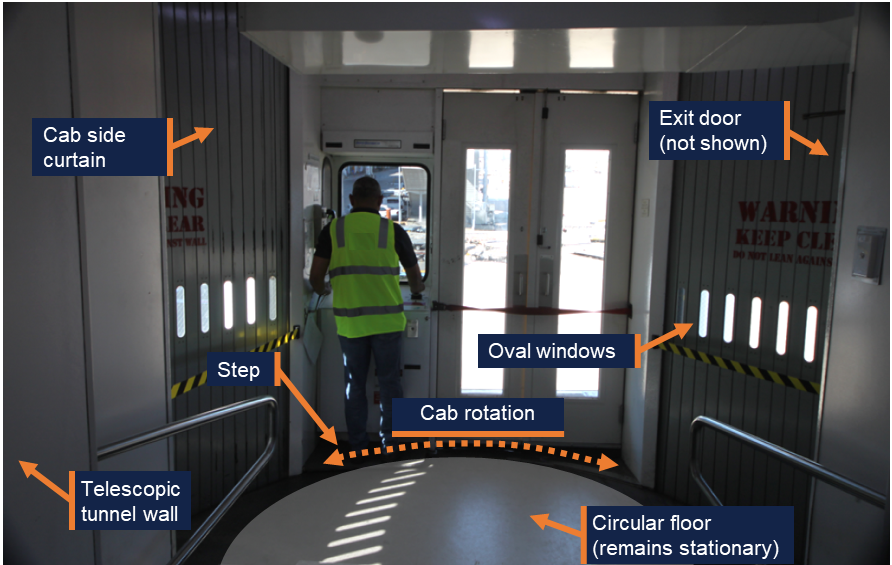
Note: The footprint of circular floor has been exaggerated by the ATSB to illustrate cab rotation around the stationary floor. Source: ATSB
Visibility of narrow-body aircraft
From the home position, wide-body aircraft were visible to aerobridge operators standing at the operator console (Figure 6). However, narrow-body aircraft fell outside the operator’s field of view at the console as the designated parking position was to the far right of the aerobridge. The operator’s view of narrow-body aircraft was blocked by protruding walls inside and outside the right side of the cab (Figure 7 and Figure 9).
For aerobridge 82, oval shaped windows interspersed on the right curtain below the operator’s eye height provided very limited visibility unless the operator left the operating console and bent down to establish visibility directly through the section of window. However, full visibility was not possible while operating the aerobridge and manoeuvring to narrow-bodied aircraft (Figure 9).
Similarly, the operator could exit the cab to view the aircraft via a service door on the far‑right of the cab. This was done on occasion to obtain visual confirmation from the ground crew prior to operation, but the operator could not operate the aerobridge unless they returned to the console.
Some other aerobridge types had been designed with large windows on the right side of the cab at eye level and below, such as the aerobridge at Gate 44 of the Brisbane Domestic terminal (Figure 10).
Figure 10: Right side windows on aerobridge at Gate 44 of the Brisbane Domestic terminal

Source: Brisbane Airport Corporation
Control panel
The control panel contained the required switches, buttons and control sticks to operate the aerobridge (Figure 11). By design, operators could rotate the cab, adjust the height, and move towards the aircraft with simultaneous actions to align with the aircraft door. Operators reported it was normal practice to do so.
Figure 11: Aerobridge control panel
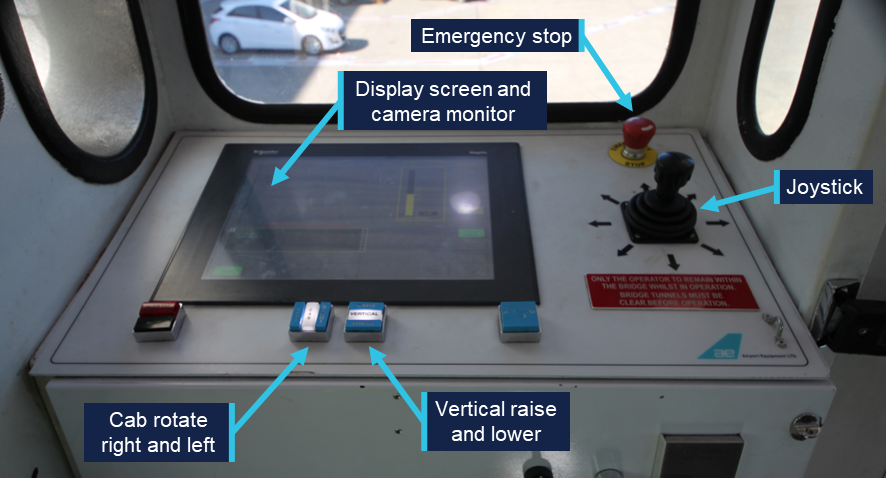
Source: Brisbane Airport Corporation, annotated by the ATSB
Vertical control
Aerobridge height could be adjusted via the vertical raise and lower buttons (Figure 11) to meet the height requirements of each aircraft type. The current height of the front bumper was displayed to the operator via a height gauge on the display screen (Figure 12). The gauge also showed 8 different aircraft types for reference.
Figure 12: Display screen and camera monitor
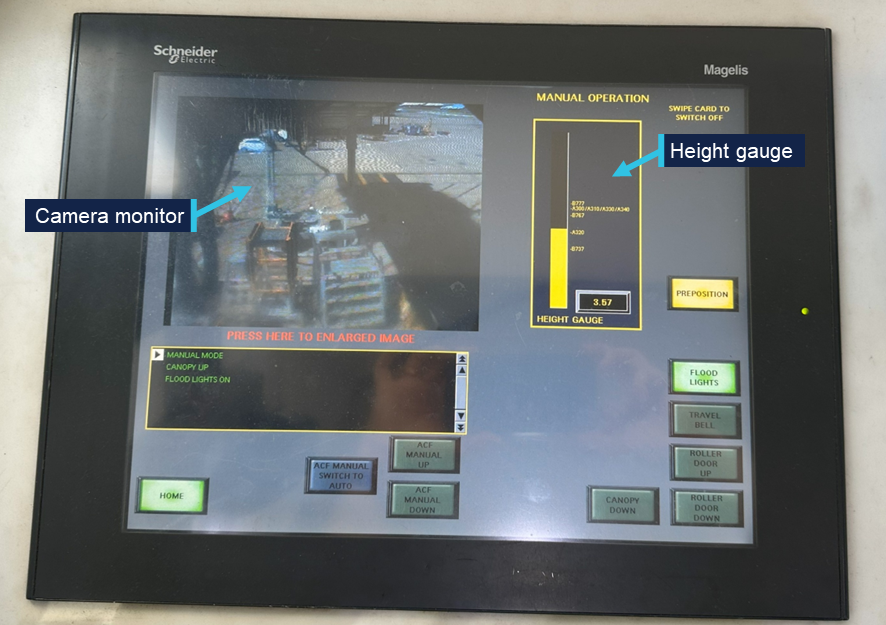
Source: ATSB
The default home height of 3.57 m was suitable for attaching aerobridge 82 to the door of an Airbus A320 aircraft, however the aerobridge needed to be lowered to meet the door height of a Boeing 737.
Cab rotate right and left
To attach the aerobridge to the aircraft door, operators were required to orient the rotating cab, using the left and right buttons (Figure 11) to ensure the cab was parallel to the fuselage (or the aircraft docking path). As the home position of the cab faced directly forward, the cab also needed to be rotated left to attach to a 737 (Figure 13), demonstrated by the concertinaed cab curtain.
Operators reported it was normal technique to pre-emptively rotate the cab to the left while moving the aerobridge horizontally or laterally.
Figure 13: Aerobridge in home position (left) and correctly attached to a 737 (right)
Source: Qantas
Joystick
The joystick controlled the aerobridge’s direction of travel and could be moved 360 degrees about its central point (Figure 11). The aerobridge drive wheels oriented to the desired direction of travel when the operator pushed the joystick in the required direction.
Speed of aerobridge movement and extension was controlled by the amount of pressure the operator applied to the joystick. The further control input, the faster the aerobridge would move. Movement stopped when the operator released the joystick (following a short delay which was perceived as a minor jolt to operators) and the joystick returned to the central neutral position.
The joystick was designed to move relative to the orientation of the cab. Specifically, relative to the forward-facing window (and therefore the direction the operator was normally facing) and not the direction of the tunnel. If the orientation or rotation of the cab changed, so did the direction of travel.
From the home position, the operator could move the joystick to a 3 o’clock direction, and the wheels would orient to travel right (Figure 14, left), and the aerobridge would travel to the right, parallel to the parked aircraft.[3]
If the operator rotated the cab slightly left from the home position (Figure 14, right), and pushed the joystick to a 3 o’clock position, as the movement of the aerobridge would be relative to the direction the cab was orientated, the aerobridge would travel diagonally towards the parked aircraft.
Figure 14: The operator’s 3 o’clock direction from home position (left) versus the operator’s 3 o’clock direction when the cab rotated slightly left (right)
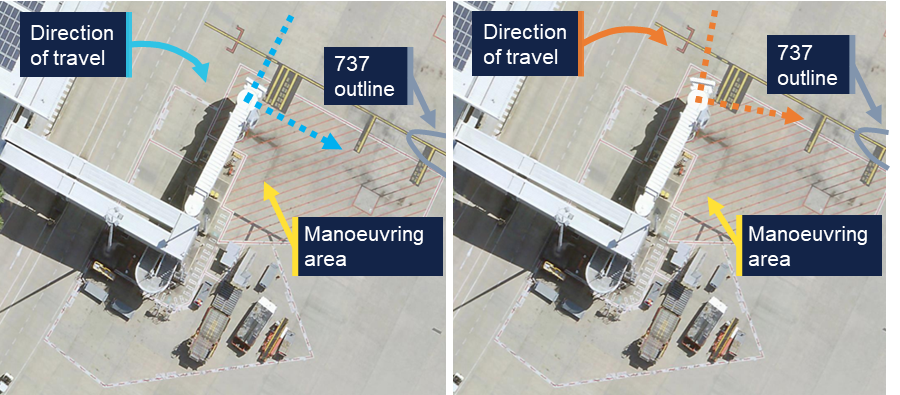
Note: Right image was edited to replicate left cab rotation. Source: Brisbane Airport Corporation, annotated by the ATSB
To anticipate the direction of travel, operators were therefore required to mentally rotate[4] the direction of travel relative to the orientation of the cab. Visible stationary references outside the cab would likely aid operators to orient the direction of travel during aerobridge movement (and correct any potential orientation errors).
Camera monitor
A front facing CCTV view of the area underneath the cab (around the wheels) was presented to the operator as a safety control to prevent contact between the elevation and travel systems (Figure 7) and any person or object inside the aerobridge manoeuvring area marked by red hatching (Figure 14).
Operators reported, and the ATSB observed, that perceptibility of the CCTV could be reduced by glare and shadows (Figure 12).
The aerobridge operator of the second occurrence reported additional blurriness on the monitor, potentially due to condensation following rain in the area prior to the event.
Safety features
The following safety features were installed on aerobridge 82 to prevent collisions with aircraft:
- A slow down sensor (or slow down beam) located under the cab floor was used to detect aerobridge proximity to the aircraft fuselage. When the ultrasonic sensor detected an obstruction directly in front of the cab, the horizontal speed slowed.
- Four bumper switches (or bumper proximity switches) located in the bumper of each aerobridge were designed to detect when the aerobridge bumper contacted an aircraft. Four spring loaded probes stopped bridge extension if activated by forward touch, while the outer 2 probes also prevented cab rotation if activated by forward touch.
Neither proximity nor bumper switches activated during the 2 occurrences.
More sophisticated anti-collision systems were installed on 7 multi-bridge[5] aerobridges at Brisbane Airport. These anti-collision systems were designed to avoid collision with other aerobridges or aircraft in front of, and either side of, the aerobridges. However, these were not equipped on single aerobridges like aerobridge 82.
Separate to the camera monitor which showed the wheel area, no other CCTV cameras were installed. Additional camera views had been discussed and considered by Brisbane Airport Corporation (BAC) for aerobridge 82, however were not installed. Further, these camera views were for inside the cab to view operator functions, not as additional visibility for the operator.
While alarms (and alerts via the display screen) were frequently presented to operators of aerobridge 82 to help operators troubleshoot common faults or issues, no alarms or alerts activated prior to the collisions.
Maintenance
Aerobridge 82 was maintained by a third party service provider, Alstef Group on behalf of BAC.
Onsite technicians responded to phone calls and callouts to address issues, faults and alarms that could not be addressed by aerobridge operators. Operator training highlighted the reporting process (and 24/7 phone number) for faults, error messages and persistent alarms. A phone was installed on the wall near the operator console for maintenance provider contact.
Preventative maintenance inspections were carried out at 3, 6, and 12 months in line with the Operating and maintenance manual[6] using standardised checklists. Weekly inspections were conducted as an additional control for aerobridge serviceability and operation. A weekly cab curtain serviceability check was also added following a fall from height occurrence at Sydney Airport in 2025.
Return to service inspections were conducted following both occurrences, with no significant damage and no faults identified.
Aerobridge operator training
BAC was responsible for the aerobridge operations at Brisbane Airport. BAC held the responsibility for operator training, operational procedures and instructions and governed user access. However, the day-to-day operation was performed by airline staff or contracted to third party service providers (e.g. ground handlers).
Certification
BAC required aerobridge operators to be trained and certified for the appropriate aerobridge type. Training involved e-learning modules, in-person demonstrations and assessment by certified aerobridge trainer/assessors for competency.
E-learning
Operators were required to successfully complete a general aerobridge e-learning module (updated in June 2022) and at least one other aerobridge specific e-learning module for each aerobridge type.
The specific module that was applicable to aerobridge 82 was the Jetway Apron Drive (International) module (updated in September 2023). The training content of this module was relevant to 3 different Jetway Apron Drive aerobridges in use at Brisbane Airport, with different control panels, but similar functionality. The training material broadly covered operations for both wide and narrow-body aircraft but did not specify individual instructions for different aircraft types.
Both the general and specific modules included online assessments that required a 100% pass mark. Ten questions were provided for the general module and 5 questions for the Jetway Apron Drive (International) module.
The training content was based on Airport Equipment (New Zealand) Limited Operation and Maintenance manuals, particularly the standard operating procedures for manual docking.
The training modules contained clear safety messages about the operation of aerobridges. Safety risks (and controls) were emphasised for:
- movement of aircraft once docked (use of auto lever and safety shoe)
- contact with the elevation and travel systems (visual check of the control area to ensure no person or obstruction is present)
- injury due to moving machine parts (one operator permitted in cab (unless training))
- risk of falls from height (use of safety straps and curtain gap checks)
- loss of control during operation (emergency stop button).
The general module also contained case studies of previous safety occurrences to communicate safety lessons.
The BAC docking procedure detailed in the training module (Figure 15) instructed operators to:
- first use the joystick to drive towards the aircraft door until approximately 500 mm (Step 4)
- then use the cab rotate buttons to ensure the bumper was parallel with the aircraft (Step 5)
- then use the joystick to extend further (Step 5)
- further adjust the cabin height and angle to align the with the aircraft door (Step 5).
Figure 15: Docking procedure from the Jetway Apron Drive (International) module
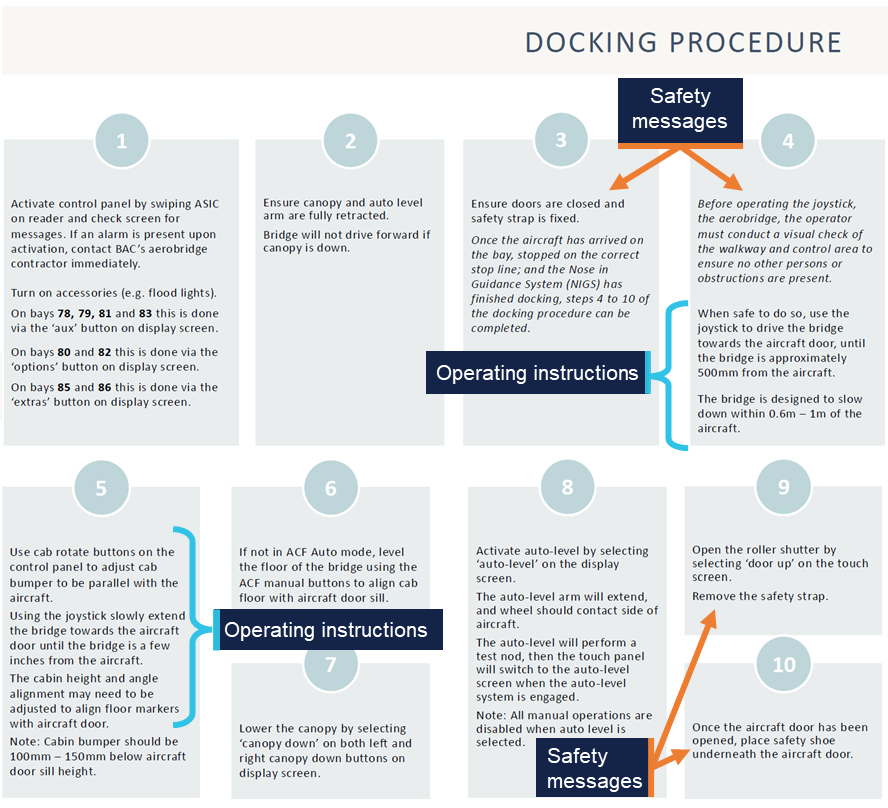
Source: Brisbane Airport Corporation
The docking procedure did not detail rotation of the cab to obtain visibility of the aircraft prior to movement, or to stop movement if visibility was lost. Also, visibility of aircraft was not explicitly mentioned elsewhere in the 2 modules or online assessments.
ATSB review of available training material from other airports showed that at least one other Australian international airport emphasises visibility in aerobridge operator training and assessment material.
Interviews with involved personnel (including Operator 1 and 2) did not highlight that joystick operation was relative to the operator’s front facing window. The operator training and instructions were also silent on this feature of the joystick.
Train-the-trainer
BAC provided train-the-trainer service to designated airline staff (such as experienced airline aerobridge operators), who would then internally train and assess airline aerobridge operators. The train-the-trainer service was provided by a third party contractor, Aviator Operator Solutions, which was contracted by Airport Equipment (New Zealand) Limited, which in turn was contracted by Alstef, on behalf of BAC.
Trainers completed a train-the-trainer session every 2 years to maintain approved trainer/assessor status.
The training involved 2 days of classroom theory and concluded with an in-person demonstration and assessment.
Both operator 1 and 2 received in-person practical training and assessment by trainer/assessors from their company airline.
Operator assessment
Assessment was conducted by an approved trainer/assessor using the BNE Operator Practical Assessment form (updated on 1 July 2022).
An operator was deemed competent once 14 steps were observed by the trainer/assessor. Each step contained several sub-steps, however full competency was recorded (yes or no) for the full step (Figure 16).
Figure 16: BNE Aerobridge Operator – Practical Assessment
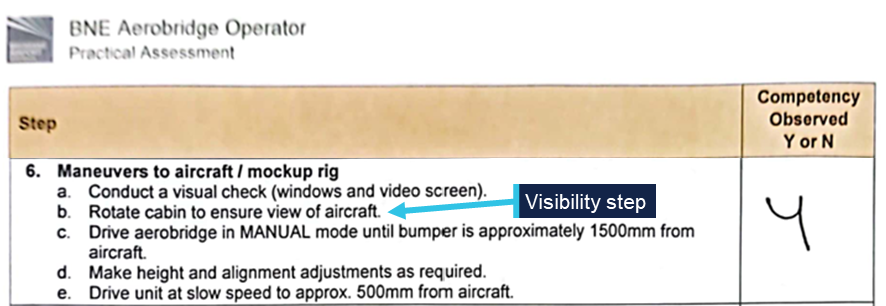
Source: Supplied
One item, step 6b, of the assessment form required operators to rotate the cab to ensure view of the aircraft (Figure 16).
Once assessed as competent under the BNE Operator Practical Assessment, competency was valid for a maximum of 2 years before the operator would need to be reassessed.
Operator recency
Where an operator had not operated an aerobridge for 6 months, e-learning refresher training was required. The BAC security card system would automatically revoke the operator’s access if operator recency was not up to date.
Aerobridge operating instructions
Laminated operating instructions were stuck to the cab wall next to the operator console (Figure 17). Step 6 of the instructions stated: ‘approach aircraft using joystick’ and steps 7–12 contained instruction to continue docking with control movements once the aerobridge was within 1.2 m of the aircraft.
These instructions did not require operators to obtain visibility of the aircraft, rotate the cab prior to movement or to stop movement if visibility was lost.
Figure 17: Laminated operating instructions
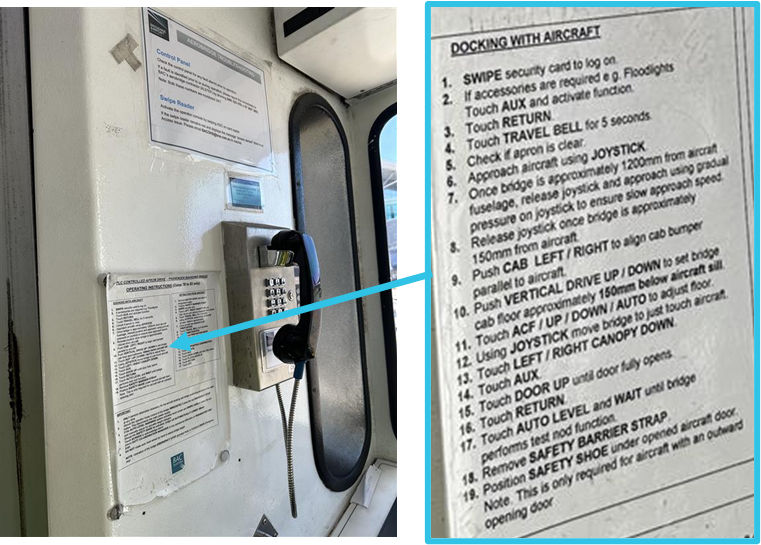
Source: ATSB
Visibility requirements for safe operation
Interviews with involved personnel (including Operator 1 and 2) revealed that rotating the cab to ensure visibility was not widely understood as a critical safety step prior to the occurrences.
Both operators reported multiple previous successful aerobridge dockings, including at aerobridge 82, where they did gain visibility of the aircraft prior to docking, but not prior to initial aerobridge movement.
Insufficient visibility from the driving or operating position is recognised as an ergonomic hazard in the European design standard used for Australian aerobridges (EN 12312‑4:2024).
External visual reference points
While not formally documented or trained, both operators reported using alternate visual reference points. Operator 1 reported using the CCTV camera monitor (Figure 12) briefly to view the nose of the aircraft prior to the collision. Operator 2 reported using the ‘red line’ aircraft docking path (Figure 13) to help orient their direction of travel on occasion during normal operations, but not on this occasion. The height of the cab during operation may restrict visibility of these ground reference points, depending on the position of the aerobridge and the height of the operator.
Recorded information
BAC automatically recorded each time an operator swiped their aviation security identity card (ASIC) to activate an aerobridge at Brisbane Airport.
BAC also recorded Gate 82 aerobridge operations from a CCTV camera mounted on the terminal building (view shown in Figure 2 and Figure 3).
No cameras were installed inside the aerobridge cab and the CCTV camera monitor showing the underneath wheel area of the aerobridge was not recorded. The aerobridge 82 control system did not log or record specific user actions or system output while the bridge was in operation.
Regulatory information
The Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (the Part 139 MOS) required aerodrome operators to ensure that the apron safety management procedures were followed by any organisation that conducts operational activities on the apron. Where operations on an apron are controlled by third parties, such as airline operators, ground handling agents or other parties, the responsibility of apron safety remains with the aerodrome operator. Further guidance is available at Advisory Circular 139.C-13 v1.0.
Related occurrences
Two similar occurrences have been recorded at Brisbane International Airport Gate 82, occurring on 3 March 2011 and 19 February 2012.[7]
On 3 March 2011, the lower, right-hand corner of the aerobridge contacted the nose cone of a Boeing 737-800 during aerobridge docking. An internal investigation by the aircraft operator identified several contributing factors, including:
- The aerobridge operator’s visual reference was impeded.
- The slowdown sensors fitted to the aerobridge did not detect/sense the aircraft due to the approach angle of the aerobridge.
On 19 February 2012, the lower, right-hand corner of the aerobridge contacted the forward upper fuselage of a Boeing 737-800 aircraft during docking, penetrating the skin forward of the windscreen. The internal investigation by Brisbane Airport Corporation identified an option of determining via a risk management process whether retrofitting the existing aerobridges with extra sensor equipment at the side will minimise future impacts with aircraft fuselage.
Safety analysis
Introduction
On 2 separate occasions in 2025, the Gate 82 aerobridge at the Brisbane International Airport Terminal collided with 2 narrow-body Boeing 737 aircraft, registrations VH-VZG (18 June) and DQ-FAE (26 July 2025).
The aerobridge operators, employed by 2 separate airlines, intended to dock with the parked aircraft on the bay. However, the aerobridge collided with the aircraft cockpit windshield resulting in minor damage on both occasions with no recorded injuries.
This analysis will explore the visibility of narrow-body aircraft, the training provided to operators, the design of the joystick operation, the required mental rotation for operators to orient movement, and aerobridge safety features.
Visibility of narrow-body aircraft
From the home position, with the default home cab orientation, operators standing at the operational console have clear visibility directly in front via the front-facing cab windows. As such, there was good visibility of wide-body aircraft parked to the right of the aerobridge. However, due to the parking location of narrow-body aircraft on the bay and the design of the aerobridge 82 walls and windows, there was limited visibility of narrow‑body aircraft for an aerobridge operator at the control console prior to aerobridge movement.
Aerobridge 82 also lacked viewing windows that were available on some other aerobridges at Brisbane Airport. Such windows may have given the operators visibility towards aircraft parked in the narrow-body parking position. Without such windows, the operator was effectively restricted to seeing only what was in front of the cab.
This created a hazard for the safe operation of the aerobridge and increased the risk of an aerobridge collision with narrow-body aircraft.
Contributing factor The aerobridge home position and cab orientation, and lack of side-viewing windows, provided limited outside visual reference to narrow‑body aircraft along the docking path, limiting the safe operation of the aerobridge. |
Normal operations
While not explicitly emphasised in their training, both aerobridge operators understood that visibility of the aircraft prior to docking was required for safe operation. They reported that gaining visibility was immediate for wide-body aircraft from the home position and normally delayed for narrow-body aircraft. Both operators expected to gain visibility of the narrow-body aircraft following aerobridge movement. Their normal steps included simultaneous actions of rotating the cab, lowering the bridge, and moving toward the aircraft.
Both operators did not expect their actions to result in a collision and they did not believe their technique was incorrect or that it differed from other aerobridge operators.
The operators understood they were required to rotate the cabin left to dock successfully and likely pre-emptively rotated the cab left while moving the aerobridge, further reducing visibility. They did not believe that rotating the cab (to the right) to gain and maintain visibility was a critical step before moving from the home position. While there was an opportunity for the operators to become aware of the critical step when they completed their practical assessment, the step was not explicitly trained or emphasised via in-cab instructions.
Contributing factor It was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft, and both operators operated without visual reference prior to the collisions. |
Object orientation and mental rotation
The aerobridge operators believed that they were extending the aerobridge parallel to the aircraft. However, it is certain that both operators rotated the cab left from the home position during aerobridge extension, and this changed the aerobridge travel direction from parallel to diagonal towards the aircraft.
Due to the design of the joystick, cab rotation required operators to mentally rotate, and account for, the expected aerobridge movement. Both operators were unaware that their 3 o’clock frame of reference had rotated (after rotating the cab left) and did not perceive other visual information to make them aware of the diagonal movement.
The operators reported that the movement did not feel different to normal, and that they expected to gain visibility of the aircraft imminently.
However, in the absence of any contradictory feedback, the operators proceeded with an incorrect awareness of the aerobridge directional movement. It was likely that the complexity of the mental rotation required, was not widely understood by the operators and that the task complexity likely increased prior to both collisions because the cab was simultaneously orientated to the left during aerobridge extension, further blocking the operator’s already limited view of the aircraft on the bay.
Contributing factor Both operators rotated the aerobridge cab left, the orientation of the cab changed the relative joystick direction creating a complex mental rotation task. |
Diagonal movement
Both operators reported pushing the joystick right (to a 3 o’clock position) to move the aerobridge parallel to the aircraft and did not perceive any conflicting information (in what they heard, saw, or felt).
Following the occurrences, one operator believed that the aerobridge system had performed an incorrect movement and was faulty (whereby the operator’s action of pushing the joystick right did not match the system behaviour). However, the system did not record user input (or system output) and no relevant pre-occurrence faults were recorded. Post-occurrence return to service inspections also found no faults.
CCTV footage of the occurrences shows that the aerobridge moved diagonally from the home position towards the aircraft at a 2 o’clock angle. The operators did not gain visibility of the aircraft because the cab had been rotated left (away from the aircraft), and because they did not perceive conflicting information, they were unaware of the parallel movement toward the aircraft.
Contributing factor The aerobridge extended diagonally towards the aircraft, in a direction that did not provide visual reference to the aircraft, and the operators were unaware of the diagonal movement, increasing the risk of aircraft collision. |
Operator training and instruction gaps
Operator training material and in-cab instructions contained clear safety messages regarding the operation of aerobridges. The operator training material also included case studies of previous safety occurrences to communicate safety lessons. However, the importance of initial visibility was not highlighted in the safety messages and the case studies did not mention limited visibility operations, particularly due to the parking position of narrow-body aircraft at Gate 82 and some other international gates at Brisbane Airport.
By design, operators could rotate the cab, adjust the height, and move towards the aircraft with simultaneous actions. The operator training material and in-cab instructions provided specific instructions for how to operate the aerobridge to successfully dock with aircraft, however omitted instructions to gain and maintain visibility of the aircraft as a critical first step.
While gaining and maintaining visibility of the aircraft may not be explicitly trained or emphasised via instructions, there was an opportunity for the step to be raised with operators at the time they were assessed. The practical operator competency assessment required operators to ensure aircraft visibility from the home position, before moving the aerobridge.
However, interviews with involved personnel (including Operator 1 and 2) revealed that rotating the cab to ensure visibility was not understood as a critical safety step prior to the occurrences and it was normal to rotate the cab left while moving the aerobridge horizontally and laterally.
Contributing factor The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge. (Safety issue) |
Safety features
The slow down and bumper contact sensors installed on the aerobridge were designed to aid docking and prevent damage to the aircraft when the aerobridge approached the aircraft from a forward direction (normal operations). The sensors would either slow or stop movement. There were no similar sensors installed on the side of aerobridge 82, therefore no sensors activated prior to the collisions when the side of the aerobridge and the corner of the cab approach the aircraft windshields.
Further, no alarms or alerts were presented to the users prior to the collisions, and no side cameras were installed to aid outside visibility of the aircraft blocked by the right side of the cab.
Contributing factor Available safety features did not activate as they were not designed to work when the aerobridge approached the aircraft from the side. |
Emergency stop
An engineer on the ground at the time of the first occurrence detected the abnormal operation of the aerobridge and immediately attempted to alert the aerobridge driver (via hand signals) before activating the ground emergency stop button. Activation of the emergency stop button was a positive action to prevent further damage to the aircraft.
Other finding In the first occurrence a licensed aircraft maintenance engineer activated the aerobridge emergency stop button to prevent further damage to the aircraft. |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the Ground handling events involving Boeing 737-838, VH-VZG, and Boeing 737-8 MAX, DQ-FAE, at Brisbane Airport, Queensland, on 18 June and 26 July 2025.
Contributing factors
- The aerobridge home position and cab orientation, and lack of side-viewing windows, provided limited outside visual reference to narrow‑body aircraft along the docking path, limiting the safe operation of the aerobridge.
- It was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft, and both operators operated without visual reference prior to the collisions.
- Both operators rotated the aerobridge cab left, the orientation of the cab changed the relative joystick direction creating a complex mental rotation task.
- The aerobridge extended diagonally towards the aircraft, in a direction that did not provide visual reference to the aircraft, and the operators were unaware of the diagonal movement, increasing the risk of aircraft collision.
- The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge. (Safety issue)
- Available safety features did not activate as they were not designed to work when the aerobridge approached the aircraft from the side.
Other findings
- In the first occurrence a licensed aircraft maintenance engineer activated the aerobridge emergency stop button to prevent further damage to the aircraft.
Safety issues and actions
Training gap
Safety issue number: AO-2025-047-SI-01
Safety issue description: The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Additional safety action taken by Fiji Airways
Fiji Airways temporarily introduced a second operator as a ‘spotter’ at Gate 82 pending the release of this report.
Glossary
| ASIC | Aviation security identify card |
| BAC | Brisbane Airport Corporation |
| BNE | Brisbane |
| CASA | Civil Aviation Safety Authority |
| CCTV | Closed-circuit television |
| LAME | Licensed Aircraft Maintenance Engineer |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Brisbane Airport Corporation
- the aerobridge operators and aerobridge trainer/assessors
- Qantas Airways
- Fiji Airways
- Civil Aviation Safety Authority
- Airport Equipment (New Zealand) Limited
- video footage of the occurrences and other photographs and videos taken on the day of the accident
- recorded data from the aerobridge access security card system.
References
CASA (Civil Aviation Safety Authority), (2023), Part 139 Apron safety management, Advisory Circular AC 139.C-13 v1.0, CASA
European Committee for Standardisation, (2024), Aircraft ground support equipment - Specific requirements - Part 4: Passenger boarding bridges (European standard EN 12312-4:2024). CEN.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Aerobridge operator 1
- Aerobridge operator 2
- Brisbane Airport Corporation
- Qantas Airways
- Fiji Airways
- Civil Aviation Safety Authority
- Airport Equipment (New Zealand) Limited
- National Transport Safety Board.
Submissions were received from:
- Brisbane Airport Corporation
- Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The marshaller’s stop line indicates the designated position where the aircraft’s nose wheel must stop.
[2] The circular cab floor remained stationary unless the bridge was moving horizontally or laterally at the same time (separate operations to cab rotation).
[3] If the operator continued with the cab in the home orientation, with no rotation, and continued to hold the joystick at 3 o’clock, the aerobridge would continue to arc around to the right.
[4] The cognitive ability to rotate 2-dimensional or 3-dimensional mental representations of objects in one’s mind.
[5] Feature multiple and independent walkways, tunnels or arms that connect to an aircraft at different doors simultaneously.
[6] Jetway Systems Apron Drive 2 & 3 tunnel computerized smart bridge manual, June 1994.
[7] Note that the incident described in this report as ‘Occurrence 1’ was originally published as an ATSB Occurrence Brief (AB-2025-025).
Occurrence summary
| Investigation number | AO-2025-047 |
|---|---|
| Occurrence date | 26/07/2025 |
| Location | Brisbane Airport |
| State | Queensland |
| Report release date | 02/04/2026 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Ground handling |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-838 |
| Registration | VH-VZG |
| Serial number | 34201 |
| Aircraft operator | Qantas Airways Limited |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Queenstown International Airport, New Zealand |
| Destination | Brisbane Airport, Queensland |
| Damage | Minor |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-8 MAX |
| Registration | DQ-FAE |
| Serial number | 64309 |
| Aircraft operator | Fiji Airways |
| Sector | Jet |
| Operation type | Part 129 Foreign air transport operators |
| Departure point | Nadi International Airport, Fiji |
| Destination | Brisbane Airport, Queensland |
| Damage | Minor |
Level crossing collision between passenger train DB09 and a B-double truck, near Runcorn, Queensland, on 14 August 2025
Final report
Report release date: 25/06/2026
Investigation summary
What happened
On 14 August 2025, Queensland Rail (QR) Citytrain passenger service to Doomben (DB09) was travelling on the Gold Coast/Beenleigh line. Train DB09 was running express towards Altandi Station with about 300 passengers on board. Ahead of DB09, a B‑double truck was immobilised on the Bonemill Road level crossing, obstructing the railway tracks. As DB09 approached, the level crossing flashing lights and boom barriers activated, and the train driver was unable to stop the train before it collided with the unloaded rear trailer of the truck.
There was substantial damage to the trailer, front of the train and level crossing equipment. The truck driver, train driver and train guard were physically uninjured. Paramedics attended to 6 passengers with minor injuries.
What the ATSB found
The ATSB found that the truck was immobilised due to a sudden air line failure between the A‑ and B‑trailers. The rear B‑trailer had obstructed the Third road and Down southern main lines for 4 minutes and 24 seconds before the level crossing warning equipment activated. The truck also obstructed road traffic.
The driver attempted multiple times to move the truck from the level crossing. Neither the truck driver or witnesses in the area telephoned the signposted QR incident reporting number or triple zero for emergency services. As such, the QR Rail Management Centre personnel were not alerted to the emergency, and they were not prompted to monitor the closed-circuit television (CCTV), which showed the truck was visible on the level crossing. Therefore, the network control officer was unaware of the track obstruction and could not warn the train crew and stop rail traffic.
The colour of the stationary truck meant it was difficult for the train driver to see it against the surroundings. However, on identifying the track obstruction, their actions in applying emergency braking in combination with the truck being empty and stationary at the time, likely reduced the severity of the collision.
What has been done as a result
QR has planned a program of works to update its level crossing strategy for financial year 2026–27. This included:
- an independent review of its current level crossing management methodology benchmarked against other rail operators.
- collaboration with the National Heavy Vehicle Regulator (NHVR) on heavy vehicle compliance activities and communication campaigns.
While not directly related to any findings from the investigation, QR advised that it has relocated the eastern rail approach whistle board from 265 m prior to the level crossing to meet the required specification in accordance with MD-23-67 Civil – Level Crossing Design.
Safety message
Accidental obstruction of railway tracks should be treated as an emergency. In the event of a vehicle becoming immobilised on a level crossing, the occupants should immediately move away from the vehicle and railway track. The next priority is to report the emergency, using either the signposted incident reporting number or triple zero. Once alerted to an obstruction, network control centre personnel can take immediate actions to stop rail traffic in the area.
Additionally, rail operators should consider the adoption of available technology for the timely identification of track obstructions that may also reduce the risk from collisions.
Summary video
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On 14 August 2025, a Wilton’s Transport standard B‑double1 truck loaded with cardboard departed Glass House Mountains towards a recycling facility at Bonemill Road, Runcorn, Queensland. At about 0538 local time, closed-circuit television (CCTV) located at the Bonemill Road level crossing recorded the truck turn right from Beenleigh Road onto Bonemill Road, traverse the 3 railway tracks2 and continue toward the recycling facility without issue.
At 0601, Queensland Rail (QR) Citytrain passenger service DB09 departed Varsity Lakes Station, Gold Coast for Doomben Station, Brisbane. At 0633, there was a train crew change at Beenleigh Station. Train DB09 then continued towards Doomben Station, travelling express between Loganlea and Altandi Stations on the Third road line. There were about 300 passengers on board.
After unloading, the B-double truck departed the recycling facility towards Rocklea. At about 0643, CCTV footage recorded the B‑double truck stop at the stop line, as the Bonemill Road level crossing was active and the traffic signal was at red. After the rail traffic passed at about 0646, the flashing aspects of the level crossing de‑activated and the traffic signal turned green.
While the truck was turning left onto Beenleigh Road, the CCTV recorded the second trailer (B‑trailer) wheels skidding. At about 0647, the truck came to a sudden stop.
The B‑trailer obstructed the Third road line and the Down southern main line.3 The prime mover and A‑trailer (first trailer) had cleared the rail corridor but were obstructing road traffic on Beenleigh Road heading east (Figure 1). The CCTV recorded the truck lurching, as the truck driver attempted to move the vehicle. The driver then exited the truck and went to inspect the area between the A‑ and B‑trailer (Figure 2). There were other motor vehicles overtaking the truck, and some pedestrians in the area at that time.
Around the same time, train DB09 was approaching the Oates Avenue level crossing near Trinder Park Station, 5.65 km from Bonemill Road.
Figure 1: Bonemill Road level crossing and vehicle directions of travel
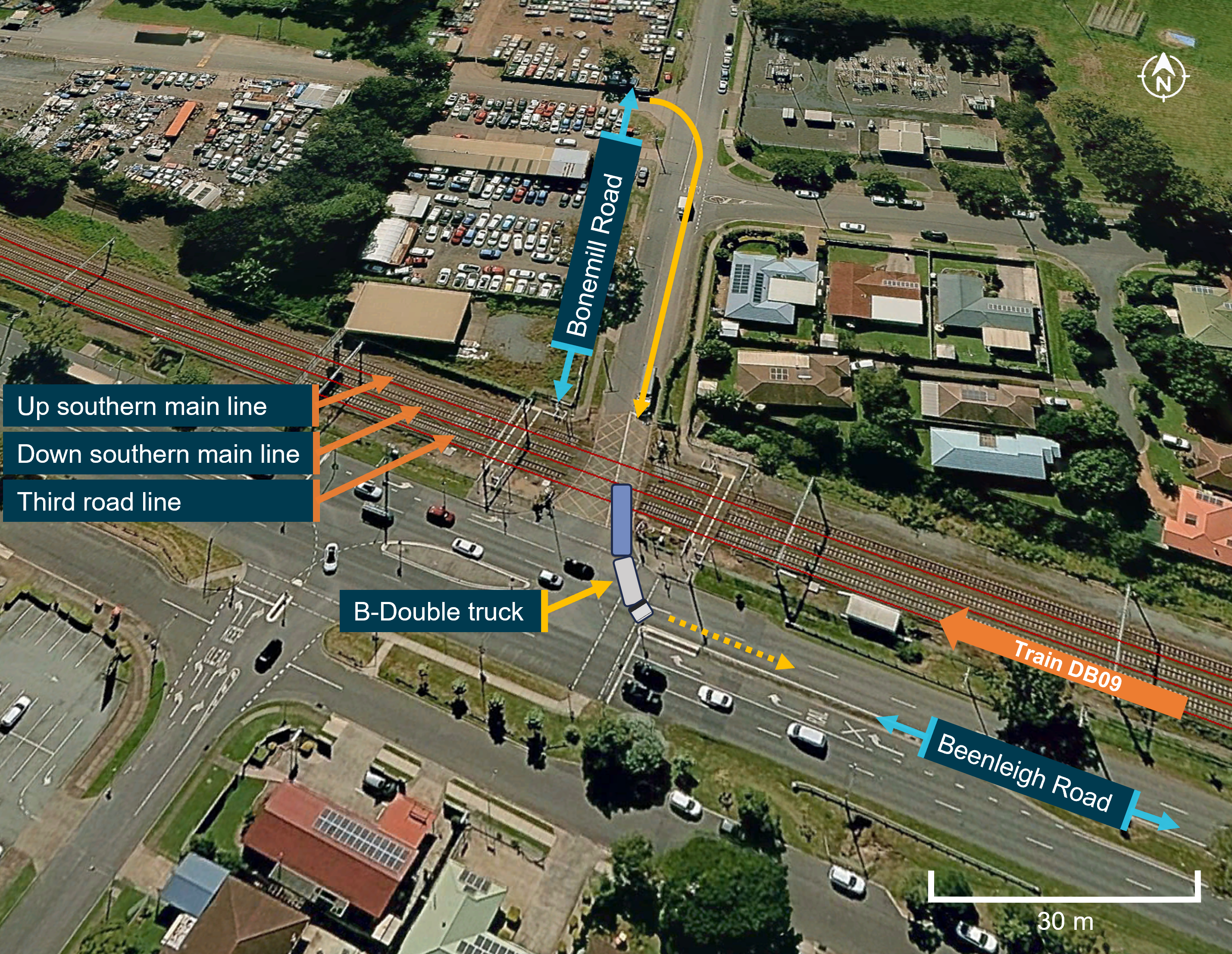
Source: Google Earth and Digital Atlas of Australia, annotated by the ATSB
Figure 2: Bonemill Road level crossing CCTV at 0650:53
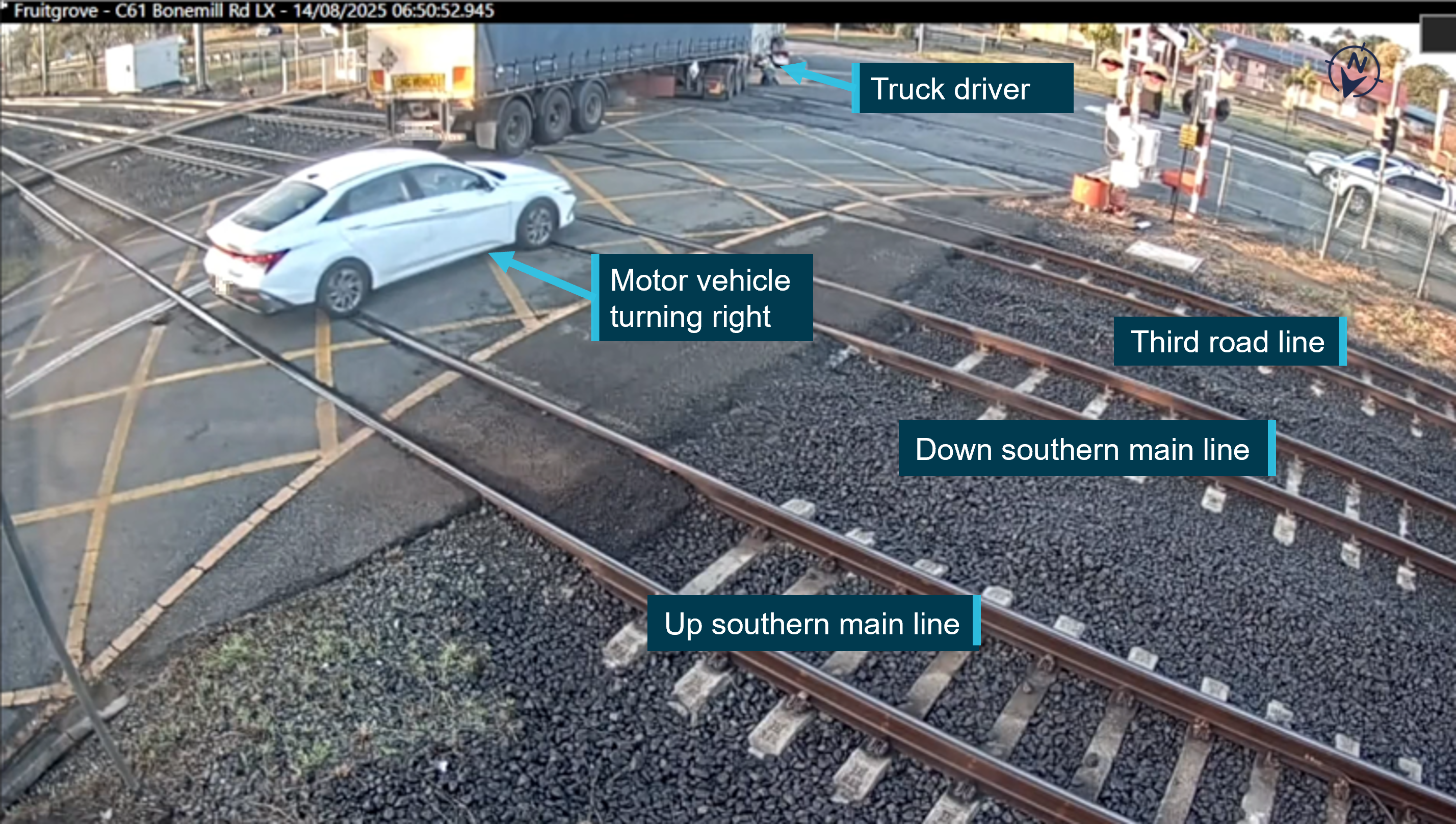
Source: Queensland Rail, annotated and pixelated by the ATSB
While the truck was immobilised, the truck driver said they were focused on moving the vehicle out of the way. As the truck driver continued to inspect the area between the trailers, the level crossing warning equipment activated. The half boom barrier on the southern side of the crossing lowered, and the tip pierced through the right side of the B‑trailer curtain, before stopping in the boom down position. At this time, train DB09 was travelling at about 96 km/h, approaching Warrigal Road level crossing, about 990 m away from Bonemill Road.
After passing Fruitgrove Station, the train driver recalled noticing a ‘large shadow’ on the tracks ahead and activated the country horn.4 The train was travelling at about 99 km/h and about 317 m from the level crossing when the driver realised the shadow was a vehicle. The train driver recalled they commenced braking and operated the main circuit breaker emergency trip to lower (disconnect) the pantographs,5 before bracing for impact.
At 0652, train DB09 collided with the side of the truck’s B‑trailer at 41 km/h, pushing it towards Beenleigh Road. The front of train DB09 came to a stop about 52 m past the point of collision. There was substantial damage to the truck, front of the train and level crossing equipment. Train DB09 did not derail, and the adjacent tracks were not fouled. There were other trains in the area at the time of the collision.
The train driver radioed the network control officer (NCO) declaring an emergency. They reported colliding with a truck hanging over the crossing. Additionally, the train guard radioed the NCO to notify them that they were moving from the rear driving compartment towards the train driver. The NCO then protected the site from other train movements by placing track blocks in the area and arranged for emergency services and the QR emergency response unit to attend the site. Queensland Police Service arrived at the accident site at 0702, and the QR incident commander arrived soon after at 0717 to take control of the site from emergency services.
Following their arrival, QR emergency response personnel inspected the train for damage, and the train crew were relieved from duty. Train DB09 had emergency power and passengers remained on the train. No emergency door releases were activated following the collision.
It was determined that the train was able to proceed to the next station for detrainment. At 0808, the QR incident commander confirmed with the NCO that train DB09 was moving towards Runcorn at walking speed. At 0813, the train stopped at Runcorn Station platform 3 and passenger detrainment was completed at 0820. The train driver, train guard and truck driver were physically uninjured. Paramedics attended to 6 passengers with minor injuries.
Context
Train crew information
Train driver
The train driver had about 14 years experience driving Citytrains and was route qualified for the Gold Coast/Beenleigh line. Their most recent Category 1 medical assessment was 3 days prior to the accident, which was approved subject to conditions. The driver’s medical assessment required them to wear glasses, and they were wearing prescription sunglasses at the time of the accident.
The train driver stated that they preferred to be rostered for early morning shifts. They were off work the previous day and reported obtaining a good night’s sleep before sign‑on at Beenleigh Station at 0608. After the collision, the train driver was tested for drugs and alcohol, which returned a negative result.
Train guard
The train guard had about 12 years experience in the position at QR. They were at the rear of the train when the collision occurred. After the collision, they were tested for drugs and alcohol, which returned a negative result.
Train information
Train DB09 was a Queensland new generation rollingstock 6‑car consist electrical multiple unit number 728. The train length was 146.7 m, and tare weight was about 438 t. The front motoring unit was DMB 728, which had substantial damage to the nose cone, coupler and air lines from the collision (Figure 3).
Figure 3: Impact damage to Queensland new generation rollingstock DMB 729

Source: Queensland Rail
The total carrying capacity was 1,206 passengers (420 seated, 786 standing with 6 people per 1 m2). The train crew estimated there were about 300 passengers on board train DB09 at the time of the collision.
The train had at least 120 minutes of emergency battery power available for ventilation, diminished lighting and full communication functions. There were 2 toilet modules installed for passenger comfort.
Road vehicle and driver information
Truck driver information
The truck driver was licenced for multi-combination vehicles and had over 40 years experience driving heavy vehicles. They had been employed by Wilton’s Transport for over 10 years. The driver had the previous day off work and only worked day shifts. Their most recent medical was about a year ago, which had no restrictions on their licence.
The driver was very familiar with Bonemill Road level crossing and worked trips in the Runcorn area about twice a week.
Heavy vehicle information
The truck was registered and operated by Wilton’s Transport. The prime mover was a white 2006 Kenworth K104, coupled to a white heavy trailer (A‑trailer – the first trailer) and blue freighter trailer (B‑trailer – the second trailer) in a 9‑axle standard B‑double configuration of 24.94 m long (Figure 4). The unloaded truck weighed about 23 t.
The truck driver stated that the truck was in good condition, and they had performed a daily check before departing Glass House Mountains. They did not identify any defects with the truck during this check. After becoming immobilised on the level crossing, the truck driver stated that they had found an air hose6 fractured between the trailers, locking the brakes on. They did not recall seeing an air pressure warning when the truck became immobilised. The operator reported that the sudden air line failure was not attributed to inadequate maintenance or inspection practices.
After the collision, a compliance inspector from the National Heavy Vehicle Regulator (NHVR) conducted an inspection of the B‑trailer and noted ‘severe’ impact damage (Figure 4).
Figure 4: B-double truck configuration and damage

Source: National Heavy Vehicle Regulator and Queensland Rail, annotated and pixelated by the ATSB
Heavy vehicle access permit
The NHVR National Network Map7 and Queensland Globe8 showed that Beenleigh Road and Bonemill Road were not included in the approved routes for B‑doubles up to 26 m long. Heavy vehicle access to these roads required a separate permit from the NHVR.
Wilton’s Transport was issued a permit by NHVR on 15 June 2021, which was renewed on 8 August 2025, 6 days prior to the accident. The permit allowed standard B‑double 9‑axle configurations up to 26 m long to carry general freight on the authorised routes. The permit listed the following route:
Start: Approved B-Double Network, Compton Rd, Runcorn QLD 4113
Persse Rd, Runcorn
Beenleigh Rd, Runcorn
Bonemill Rd, Runcorn
End: 20 Bonemill Rd, Runcorn QLD 4113
Other local council conditions were also listed in the permit, which included travel times. The Brisbane City Council listed the following condition:
Time of travel - Schedule
The heavy vehicle must not travel on Beenleigh Rd and Persse Rd between 06:00 am and 09:00 am and 03:00 pm and 06:00 pm.
Bonemill Road was not listed in the travel time conditions.
The truck driver stated they were aware of the truck access permit, but unaware of the condition that did not allow access to Beenleigh Road between 0600–0900.
Standard B-double trucks were not required to have an access permit issued by QR for railway crossings such as Bonemill Road, unless they met the requirements for over‑dimensional road loads9. The B‑double truck involved in the collision was not over‑dimensional or over-weight.
Level crossing information
Bonemill Road level crossing
QR was the accredited rail infrastructure manager for the Gold Coast/Beenleigh line, including the Bonemill Road level crossing. Bonemill Road level crossing was located between Fruitgrove and Runcorn stations, at the 19.8 km point on the Gold Coast/Beenleigh line. There were 3 narrow gauge (1,067 mm) bi‑directional railway tracks (Down southern main line, Up southern main line and Third road line). The level crossing was actively protected with flashing lights and half boom barriers (see Layout and active warning assemblies).
The track grade between Fruitgrove and Bonemill Road was slightly descending toward the road crossing, where the grade was level. The eastern rail approach whistle board10 was located about 265 m prior to the level crossing.11
The QR Characteristic Report for Bonemill Road noted the crossing was approved for B‑double trucks. The most recent ALCAM12 assessment of the level crossing was dated 6 August 2025, which also noted the level crossing was approved for B‑double trucks.
Bonemill Road level crossing was located off Beenleigh Road, and surrounded by residential areas, school zones and industrial areas. Rail traffic was busy, with about 204 train movements a day, and high boom down times during peak hour periods. The maximum speed for suburban and freight trains on the corridor was 100 km/h. There were no published speed restrictions that were in place for the Runcorn area.
Road and level crossing inspections and maintenance activities were managed under a safety interface agreement between QR and Brisbane City Council, dated 4 August 2021. The council was not required to notify QR of access permits issued by NHVR.
There were no recorded near misses or incidents involving heavy vehicles at Bonemill Road in the previous 5 years.
Layout and active warning assemblies
Road traffic controls at the interface comprised of level crossing mast assemblies, including flashing lights, audible bells and half boom barriers. Keep clear signage and yellow crosshatch pavement markings were also installed to prevent queuing across the level crossing. Additionally, there were 2 active pedestrian crossings on each side of the road. The level crossing was interfaced with the 3‑aspect traffic signals that controlled single lane traffic turning onto, and from, Beenleigh Road (Figure 5).
Figure 5: Bonemill Road level crossing overview and layout
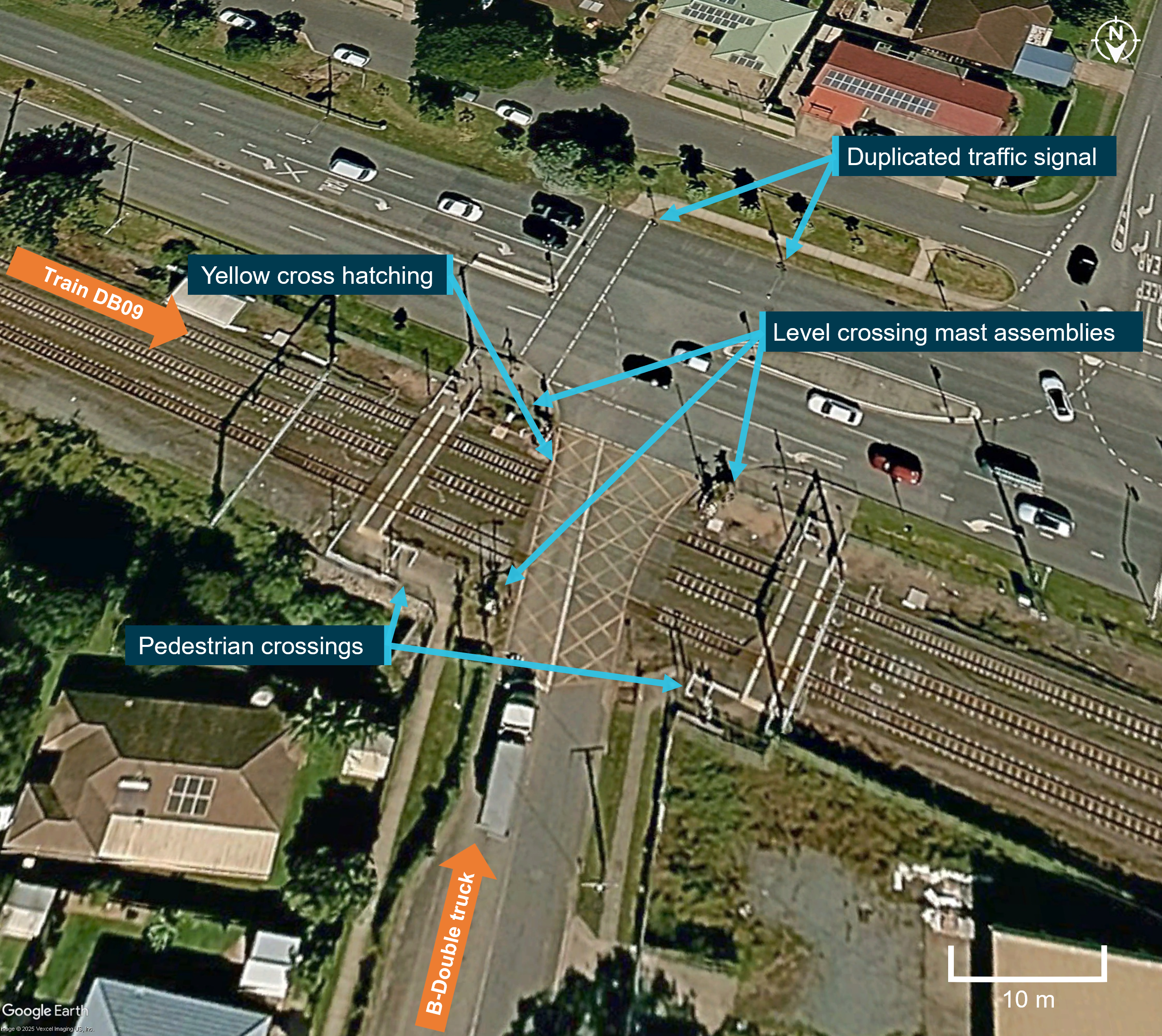
Source: Google Earth, annotated by the ATSB
On the north-east and south-west side of the level crossing, incident reporting signage was installed near the mast assembly, facing inwards to the yellow crosshatch pavement markings (Figure 6). The incident reporting signage included a 24-hour emergency phone number (1800 079 303) for anyone to report a safety incident, such as a track obstruction. This number connected directly to the QR Rail Management Centre. The truck driver recalled they had probably seen the incident reporting numbers before but had not taken any notice.
Figure 6: Bonemill Road level crossing incident reporting signage

Source: Queensland Rail, annotated by the ATSB
Recorded information
Event recorder
The train was fitted with a Hasler Rail Teloc 3000 event recorder and forward-facing CCTV camera (FFCCTV) at the A and B ends of the train. The timestamp on the event recorder and DMB 728 FFCTV were within 1 second of each other.
The ATSB compared the braking performance of train DB09 to the vehicle braking performance standard in QR MD-10-194 Interface Standard and track geometry of the area. The deceleration rate of the train was within the allowable rates in the standard. The train stopped within an acceptable distance, based on when the emergency brake was applied.
Figure 7 compares the event recorder train speeds and train driver actions to what was visible to the train driver leading up to the collision. The train driver recalled that, when they first noticed a shadow ahead, it was very difficult to distinguish from the surrounds.
At the point of the collision at 0652:07, train DB09 was travelling at 41.0 km/h.
Figure 7: Comparison of train speeds, train driver actions and DMB 728 FFCCTV

Source: Queensland Rail, annotated by the ATSB
Level crossing recorded events
The QR universal traffic control (UTC)13 system recorded the events related to the approach of train DB09 and operation of the level crossing equipment (Table 1). If the boom barriers did not fully deploy to the lowered position, this would present an alarm on the UTC network control panel. There were no relevant UTC alarm messages displayed on the control panel prior to the collision recorded at 0651:46.
Table 1: Recorded events for Bonemill Road level crossing
| Timestamp | Event |
| 0650:42 | Train DB09 was detected approaching the level crossing. |
| 0651:09 | Level crossing flashing lights begin to operate. |
| 0651:18 | Boom barriers begin to lower (9 seconds after the lights start flashing). |
| 0651:28 | Boom barriers detected down (10 seconds after the boom started to lower). |
| 0651:44 | Train DB09 detected on the Third road line. |
| 0651:46 | Boom barrier down detection lost. UTC alarm ‘Bone Mill Rd Level Crossing Failed at KURABY’. |
Closed-circuit television
There were 9 CCTV cameras installed at the crossing, with 4 positioned on the north‑west side and 5 on the south-east side. While the truck was immobilised, it was visible on 4 of the cameras.
Table 2 summarises the events recorded across the 4 cameras from the time the truck first used the Bonemill Road level crossing and then returned until the collision with train DB09.14 The truck came to a stop at 0647:07, and the level crossing active warning equipment started for train DB09 at 0651:31.
Table 2: Recorded closed-circuit television events at Bonemill Road level crossing
| Timestamps | Event |
| 0538:02 to 0538:18 | The B-double truck turned right from Beenleigh Road onto Bonemill Road, and exited the level crossing. |
| 0643:19 to 0646:21 | Level crossing activated for the passage of 3 trains. B‑double truck returned and stopped at the stop line. Level crossing boom barriers lower. |
| 0646:42 to 0647:07 | Level crossing cleared and B-double truck departed stop line on green traffic signal. The left-side wheel on the 6th axle locked, leaving a 17.4 m skid mark, then rotated again. Other wheels on the B‑trailer were not gaining traction. B‑double truck comes to a sudden stop. No smoke or sparks were evident. |
| 0647:12 to 0650:06 | The B-double truck lurched about 15 times. |
| 0647:22 to 0650:53 | 8 motor vehicles overtook the B-double truck to turn right onto Beenleigh Road. |
| 0648:26 to 0651:34 | 7 motor vehicles passed the B-double truck to turn left onto Bonemill Road. Other vehicles heading east down Beenleigh Road were blocked by the truck. |
| 0648:49 to 0650:51 | 3 pedestrians in the vicinity of the truck. |
| 0650:32 to 0651:00 | Truck driver walked around the prime mover to the right side and kneeled to inspect the area between the A and B trailer, then walked back. |
| 0651:18 to 0651:28 | The truck jolted, and the hazard lights were turned on. |
| 0651:31 to 0651:47 | Level crossing flashing lights started. The south-most level crossing boom barrier lowered and pierced the side canvas cover of the truck trailer. Boom barriers were in the down position. The truck driver jogged towards the back of the truck to look between the A and B trailer. |
| 0652:04 to 0652:07 | Truck driver walks away from the truck. Collision with train DB09. |
Environmental information
The weather at 0652 was fine and clear. The sun had risen and was low in the sky (azimuth 70.79°, elevation 6.19°) in a north-east direction. Therefore, sun glare had a negligible effect on the train driver as they approached the Bonemill Road level crossing.
Network control information
The QR Management Centre (RMC) was located in Mayne, Queensland. The NCO for the Runcorn to Varsity Lakes rail section, which included the area around the Bonemill Road level crossing, was located at workstation UTC 6. The train control leader (TCL) for the southern area of the south-east Queensland network was located behind them at workstation TCL 2. The security monitoring officers were located separately in the centre.
The 24-hour emergency phone number detailed on the incident reporting signage connected to the TCL 2 workstation, and information received would be disseminated to the relevant area within the control centre. Dependant on the length of a call, QR estimated that transfer of emergency information within the centre would typically occur within 30–90 seconds.
The security monitoring team at the RMC were responsible for monitoring more than 12,000 individual CCTV cameras across the south-east Queensland network. Active monitoring of specific locations by the team was dependent on daily priority areas, intelligence reports and reported incidents. In addition to CCTV monitoring, the team were responsible for:
- managing incidents in real time in partnership with Network Control
- deploying resources such as authorised officers and mobile security patrols
- coordinating with the Queensland Police Service, including the Railway Squad
- undertaking CCTV reviews to investigate and validate incidents
- responding to the station emergency help phones and various asset security system alarms
- receiving incident reports from operational staff in the field via telephone and radio including station operations, authorised officers and security officers
- providing remote access control to various facilities.
In the event of a reported incident that impacted train operations, the team would communicate directly with the relevant NCO. QR confirmed that on the day of the accident, there were no priorities in the Runcorn area that would have triggered CCTV monitoring. There were also no automated systems to detect immobilised vehicles or other obstructions on the level crossing.
The first notification to the RMC of the track obstruction was the train driver’s emergency radio call after the collision. The first notification to the Queensland Police Service of the emergency was from the RMC requesting police attend the scene. There were no records of triple zero (000) calls reporting the track obstruction.
Emergency procedures for track obstructions
QR procedure Rail Emergency Response Module EP1-01 covered emergency situations that could impact the QR network. Rail traffic crew were required to:
• Stop the rail traffic.
• Press “Emergency Pan Down” (Big Red) if the incident involves the OHLE [overhead line equipment], whether people are in contact with or within 3 metres of the OHLE and or if the OHLE is down and/or damaged or tangled.
• Warn all rail traffic, secure the rail traffic against movement, and protect adjacent track sections.
• Immediately contact the NCO stating “Emergency, Emergency, Emergency”…
In addition to the module EP1-01 requirements, other requirements for level crossing emergencies were outlined in Module MD-11-31 Level Crossing Emergency. Indicators of a level crossing emergency included:
• Obstruction of level crossing (vehicle stalled etc.)
• Collision damage (vehicle wreckage / train stopped across crossing etc.)
• Person struck inside level crossing
• Advice from workers or members of the public
• Remote Monitoring System (RMS) Alarms
• Alarms on UTC screen
• Public Safety Preservation Act 1986 (Qld) - Declaration of emergency situation.
The NCO was required to act in the event of a level crossing emergency, including:
- Obtain contact details for first worker on scene15 and maintain contact.
- Notify the electrical control officer if the OHLE (overhead line equipment) was impacted and state ‘Emergency, Emergency, Emergency’. Tell them all the information obtained by the first worker on scene.
- If adjacent tracks were fouled, warn rail traffic on adjacent tracks, and immediately protect any rail traffic in danger through emergency calls, placing signals at stop and placing blocks on affected signals and routes.
- Contact emergency services on triple zero if required and inform them of the name, position, contact details and details of emergency.
Related occurrences
The ATSB Review of level crossing collisions involving trains and heavy road vehicles in Australia (RS-2021-001) examined 49 collisions between trains and heavy vehicles at Australian level crossings between July 2014 and August 2022, in which 24 rail or road users were fatally or seriously injured. The safety study identified 3 collisions at boom barrier crossings where the truck stopped on the crossing, and the heavy vehicle driver had been unable to exit the level crossing due to unanticipated events. In one of these collisions, the heavy vehicle reportedly entered the crossing but encountered a mechanical problem and was unable to move.The ATSB investigation (RO-2021-012), into the collision between passenger train C012 and a motor vehicle near the West Dapto Road level crossing in Kembla Grange, New South Wales, on 20 October 2021, undertaken by the Office of Transport Safety Investigations16. At 0339 local time, the train departed Kiama Station en route to Sydney Central Station. At 0409:06, the train passed the track circuit that activated the West Dapto Road level crossing warning bells and lights. Twenty-six seconds later, the driver made an initial brake application. It was estimated the train was approximately 200 m from the motor vehicle at this time. Three seconds later, the driver applied full braking and within the second after, applied emergency braking when travelling at about 90 km/h. Over the next 4 seconds, the train collided with the vehicle. This resulted in the train derailing and the separation of train carriages, seriously injuring the train driver, train guard and 2 passengers, with 8 minor injuries to passengers.
In this accident, there was an abandoned motor vehicle on the crossing. A member of the public called triple zero, and this information was passed to the Rail Operations Centre. However, information was not communicated to the train driver of C012 in time to stop safely prior to the collision.
Safety analysis
Track obstruction
When traversing the Bonemill Road level crossing, the empty B‑trailer of a B‑double truck became immobilised across the Third road line and Down southern main line before the active warning equipment started. The truck obstructed 2 of the 3 railway tracks during morning peak hour, before the arrival of train DB09, which was travelling express at about 95 km/h on the Third road line. The train driver did not see the truck until around 317 m prior to the crossing. While the driver immediately applied the emergency braking, there was insufficient distance to stop the train before colliding with the truck at 41 km/h.
Incident reporting
The truck obstructed the tracks for 4 minutes and 24 seconds, which provided an opportunity for an alarm to be raised. Signage located at the level crossing provided an emergency phone number for incident reporting, which connected directly to the Rail Management Centre. While the truck driver reported that they had seen the incident reporting number before, they did not take notice of it. They did not telephone triple zero to raise the alarm. Instead, they were focused on moving the truck off the level crossing and allowing road traffic to pass. There were several bystanders in the vicinity who were aware of the track obstruction, and they also did not attempt to contact network control or emergency services.
There were no UTC alarms at the NCO’s workstation and the CCTV at the level crossing was not being actively monitored by the security monitoring team at the time. Therefore, the Rail Management Centre only became aware of the track obstruction when the train driver made an emergency call after the collision.
There were no automated systems to detect immobilised vehicles or other obstructions on the level crossing. This meant that avoidance of a collision was solely reliant on the train driver seeing the obstruction at a distance sufficient to stop the train. The Office of the National Rail Safety Regulator safety messaging on track obstructions have noted risk controls for rollingstock to detect obstacles on the track, such as mounted sensing and detection equipment (ONRSR, 2025). Additionally, the United Kingdom Rail Safety and Standards Board has documented academic studies of technology used to detect trespassing on the rail corridor, including vehicles on level crossings (RSSB, 2025). These studies identified technologies such as CCTV and video analytics, artificial intelligence approaches, fibre-optic acoustic sensing, lasers and drones, noting strengths and weaknesses with each approach. While rail transport operators must consider various factors, including the likelihood of the hazard and the degree of harm to determine what controls are reasonably practicable to implement, there are technologies available that do not rely on manual monitoring of CCTV or members of the public reporting a track obstruction to prevent a collision.
Truck visibility
The first opportunity for the train driver to sight the obstruction on the Bonemill Road level crossing was as the train approached Fruitgrove Station. However, the obstruction was not immediately identifiable as a stationary truck. The white prime mover and A‑trailer were situated outside of the rail corridor and would have been obscured from the driver’s view by trackside equipment. The plain blue curtain of the B‑trailer did not contrast well with the background environment and the shadows that were present at the time the truck was on the level crossing. As a result, the train driver identified the hazard around 317 m prior to the crossing and while they implemented the emergency procedures, there was insufficient distance to prevent the collision.
Train driver’s response
On sighting the track obstruction, the train driver’s response of applying emergency braking reduced the train’s speed from 98.8 km/h to 41 km/h when the collision occurred, resulting in minor physical injuries. In comparison, the level crossing accident at Kembla Grange occurred at a higher train speed, resulting in significant injuries. Additionally, the train driver operated the main circuit breaker emergency trip to lower the pantographs. This meant that, at the point of impact, the pantograph was disconnected from the overhead line equipment. Overall, the driver’s response, in combination with the truck being empty and stationary at the time, likely prevented more serious consequences from the collision.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the level crossing collision between passenger train DB09 and a B‑double truck at Runcorn, Queensland, on 14 August 2025.
Contributing factors
- A B-double truck became immobilised on the Bonemill Road level crossing before the warning equipment activated, resulting in the B‑trailer obstructing 2 of the 3 railway tracks. The driver of train DB09 was not aware of the obstruction in time to stop the train prior to colliding with the truck.
- While the truck was stopped on the crossing for about 4 and a half minutes, neither the driver nor bystanders rang the signposted incident reporting number or emergency services. As a result, the network control officer was not aware of the emergency and was unable to alert DB09 and other trains in the area of the need to stop.
Other factors that increased risk
- The B-trailer of the stationary B-double truck was equipped with a plain dark blue curtain, which had poor contrast with the background environment at the time of the accident. This reduced the conspicuity of the trailer and the train driver's early recognition of the obstruction.
Other findings
- On recognition of an obstruction ahead, the train driver applied emergency braking and the associated emergency procedures. This likely reduced the severity of the collision between the train and stationary truck.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence |
Safety action by Queensland Rail
Queensland Rail is currently updating its level crossing strategy for the 2026–27 financial year. This strategy included a set of initiatives, such as an independent review of its current level crossing management methodology benchmarked against other rail operators. It also included collaboration with the National Heavy Vehicle Regulator on heavy vehicle compliance activities and communication campaigns.
While not directly related to any findings from the investigation, Queensland Rail also advised that it has relocated the eastern rail approach whistle board from 265 m prior to the level crossing to meet the required specification in accordance with MD-23-67 Civil – Level Crossing Design.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the train driver of train service DB09
- the truck driver of Wilton’s Transport
- Queensland Rail
- Queensland Police Service
- Queensland Ambulance Service
- Queensland State Department of Transport and Main Roads
- National Heavy Vehicle Regulator.
References
Department of Transport and Main Roads. (2023). Heavy vehicle route maps and restrictions. Retrieved 27 August 2025, from https://www.tmr.qld.gov.au/business-industry/heavy-vehicles/heavy-vehicle-route-maps-and-restrictions#qld-globe
National Heavy Vehicle Regulator. (2016). Glossary of common terms. https://www.nhvr.gov.au/files/201612-0062-nhvr-glossary-of-common-terms.pdf
National Heavy Vehicle Regulator. (2024). NHVR National Network Factsheet. https://www.nhvr.gov.au/document/385/
Office of the National Rail Safety Regulator. (2025). Safety Message: Track Obstructions. Retrieved 28 January 2026, from https://www.onrsr.com.au/safety-essentials/safety-messages/safety-message-track-obstructions
Queensland Rail. (2022). Driving Over-dimensional road loads (ODRL) across Queensland Rail's railway crossings - Application for permits. Retrieved 19 August 2025, from https://www.queenslandrail.com.au/forbusiness/overdimensionalloads
Rail Safety and Standards Board. (2025). Technologies to tackle trespassing: an update (S389) New developments in technologies that can be used to detect and prevent trespass incidents. https://www.rssb.co.uk/research-catalogue/CatalogueItem/S389
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the train driver of service DB09
- the train guard of train service DB09
- the truck driver of Wilton’s Transport
- Queensland Rail
- Wilton’s Transport
- Queensland State Department of Transport and Main Roads
- National Heavy Vehicle Regulator
- Office of the National Rail Safety Regulator.
Submissions were received from:
- Queensland Rail
- Wilton’s Transport
- Office of the National Rail Safety Regulator.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
- ^ A combination consisting of a prime mover towing 2 semitrailers, with one semitrailer supported at the front by, and connected to, the other semitrailer.
- ^ The 3 tracks included the Up southern main line, the Down southern main line and the Third road line.
- ^ Up southern main line: the rail line that facilitated train movements towards Brisbane.
- ^ The Queensland new generation rollingstock was fitted with a town horn and a louder country horn. Operation of either horn automatically activated the front of train visibility lights alternatively for 20 seconds.
- ^ Pantograph: an apparatus fixed to the roof of electric trains to draw power from the overhead supply.
- ^ Heavy vehicles use an air brake system designed to fail-safe (that is, apply the brakes) if air pressure is lost. Air pressure is displayed to the truck driver, with an alarm if the pressure is too low.
- ^ National Network Map: https://www.nhvr.gov.au/road-access/route-planner/national-network-map
- ^ Queensland Globe: https://www.tmr.qld.gov.au/business-industry/heavy-vehicles/heavy-vehicle-route-maps-and-restrictions#qld-globe
- ^ Requirements to obtain written permission from QR to take over-dimensional road loads across QR’s railway crossings under the Transport Infrastructure (Rail) Regulation 2017: https://www.queenslandrail.com.au/forbusiness/overdimensionalloads
- ^ Whistle board: when a train passes a whistle board, the train driver must sound the horn to warn workers and/or members of the public that rail traffic is approaching.
- ^ QR Specification MD-23-67 Civil – Level Crossing Design required the whistle board to be placed 450 m from the level crossing at train speeds of 100 km/h to provide a minimum warning time of 16 seconds.
- ^ ALCAM: The Australian Level Crossing Assessment Model. This assessment was based on observed vehicles, including B‑double trucks with an access permit for Bonemill Road. Bonemill Road was not a NHVR gazetted B‑double route.
- ^ Universal traffic control: a system unique to QR that assists NCOs safely route and monitor the movement of trains.
- ^ There was a variance of about 22 seconds between the UTC and CCTV recorded events. The time clocks were not synchronised between these systems.
- ^ First worker at the scene: this could also be a member of the public.
- ^ Under a collaboration agreement, rail safety investigations are conducted and resourced in New South Wales by the Office of Transport Safety Investigations, on behalf of the ATSB, under the provisions of the Transport Safety Investigation Act 2003.
Occurrence summary
| Investigation number | RO-2025-006 |
|---|---|
| Occurrence date | 14/08/2025 |
| Occurrence time and timezone | 0652 Australian Eastern Standard Time |
| Location | Bonemill Road level crossing, Runcorn |
| State | Queensland |
| Report release date | 25/06/2026 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Rail |
| Rail occurrence category | Collision, Level Crossing |
| Occurrence class | Accident |
| Highest injury level | Minor |
Train details
| Train operator | Queensland Rail |
|---|---|
| Train number | DB09 |
| Track operator | Queensland Rail |
| Type of operation | Suburban passenger |
| Rail vehicle sector | Passenger - metropolitan |
| Consist | 6 car electrical multiple unit 728 |
| Departure point | Varsity Lakes Station, Queensland |
| Destination | Doomben Station, Queensland |
| Persons on board | Crew - 2, Passengers - about 300 |
| Injuries | Crew - 0, Passengers - 6 (minor) |
| Train damage | Substantial |
Propulsion failure of Basic Victory, near the coast, 33 km north of Newcastle, New South Wales, on 30 July 2025
Summary
The ATSB is investigating the incident which involved the propulsion failure of the bulk carrier, Basic Victory, close to the coast of New South Wales, north of Newcastle, on 30 July 2025.
At about 0800 local time on 30 July, Basic Victory was drifting about 20 miles off the Port of Newcastle while waiting to berth there, when its main engine failed. The ship drifted towards the coastline north of Newcastle and by about 1730 had closed to within 3 miles of the nearest land. At about this time, the ship’s master reported the propulsion failure to Newcastle vessel traffic service and requested permission to anchor. Shortly afterwards, however, the crew succeeded in restarting the main engine and the ship steamed clear of the coastline.
ATSB investigators attended the ship after it had berthed in Newcastle on 7 August to collect evidence and interview the master and relevant crewmembers.
The ATSB has commenced the examination and analysis of the initial evidence collected. To date, the ATSB investigation has included:
- interviewing the ship's crew and operators
- interviewing the Newcastle harbour master and vessel traffic services operators
- a preliminary review of the ship's track
- collecting documentary evidence including communication records from the concerned parties
- a preliminary review of the actions taken by the various parties during the incident.
The continuing investigation will include further examination and analysis of:
- procedural documentation from the various parties
- operational and maintenance documentation from the ship
- incident related communications
- emergency actions implemented by the concerned parties
- related occurrences.
A final report will be published at the conclusion of the investigation. Should a critical safety issue be identified at any time during the investigation, the ATSB will immediately notify the operators of the ship and the port, and other relevant parties so that appropriate and timely safety action can be taken.
Occurrence summary
| Investigation number | MO-2025-010 |
|---|---|
| Occurrence date | 30/07/2025 |
| Occurrence time and timezone | 18:20 Australian Eastern Standard Time |
| Location | 33 km north of Newcastle |
| State | New South Wales |
| Report status | Pending |
| Anticipated completion | Q3 2026 |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Examination and analysis |
| Investigation status | Active |
| Mode of transport | Marine |
| Marine occurrence category | Engine Failure |
| Occurrence class | Incident |
| Highest injury level | None |
Ship details
| Name | Basic Victory |
|---|---|
| IMO number | 9836787 |
| Ship type | Bulk Carrier |
| Flag | Marshall Islands |
| Owner | Four Land Panama SA |
| Destination | Port of Newcastle, New South Wales |
| Injuries | None |
Highway forced landing after SR22 engine failure and fire

The pilot of a Cirrus SR22 conducted a forced landing on the Mitchell Highway in central NSW after the light aircraft experienced an engine failure and in-flight fire, an ATSB investigation report details.
On 24 January 2025, a pilot and a passenger were flying from the Gold Coast to Mildura.
About three hours into the flight, while approximately 150 km north-west of Dubbo and cruising at about 8,000 ft, the aircraft’s engine oil pressure decreased below normal operating limits.
In response the pilot began to divert for a landing at Nyngan. But as they were making a PAN PAN radio call announcing their intentions, they heard the engine begin to ‘rev up’, followed by a ‘bang’.
The pilot then made a MAYDAY broadcast to ATC, advising that the engine had experienced a mechanical failure and they would be making an emergency landing on the Mitchell Highway, east of Nyngan.
As ATC acknowledged the broadcast, the pilot observed flames ‘pouring’ from the top of the cowl.
The report notes the pilot elected not to deploy the aircraft’s ballistic recovery parachute due to concerns that the fire was fuel related, and that a parachute-assisted landing may result in injuries to the passenger, who was pregnant.
Instead, the pilot began an emergency descent, putting the aircraft into a ‘dive’ in an attempt to put out the fire. The fire self-extinguished, but smoke began to enter the cockpit.
Despite the subsequent reduced visibility, the pilot proceeded to navigate the aircraft to land on the highway, while avoiding road traffic, for a successful forced landing with no injuries.
“The pilot’s timely and effective decision-making, likely supported by their experience on the aircraft type and knowledge of its performance capabilities, mitigated the risk of injury and further damage to the aircraft,” ATSB Director Transport Safety Dr Stuart Godley said.
Dr Godley noted in-flight engine failures in single-engine aircraft often result in the pilot experiencing high workload and time pressure, making preparedness critical.
“This incident demonstrates how the ‘aviate, navigate, communicate’ framework establishes a clear hierarchy of priorities, particularly during emergencies,” he continued.
“Acting in the appropriate order of priority improves situational awareness and supports coordinated responses in a dynamic environment.”
After the landing, the pilot inspected the engine and found the crankcase had ruptured adjacent to cylinder 6, below the induction duct assembly. A connecting rod had separated from the crankshaft and the air filter was visibly damaged by fire.
A disassembly and inspection of the engine had yet to be conducted at the time of publication of the ATSB’s investigation report. As a result, the ATSB was unable to determine the root cause for the loss of oil pressure or the mechanical failure of the engine.
“Although engine failures are relatively rare, they do happen,” Dr Godley concluded. “Given the potential severity of the consequences of an engine failure or power loss in a single‑engine aircraft, such occurrences therefore need to be planned for and managed appropriately.”
Read the final report: Engine failure involving Cirrus SR22, VH-DCB, 28 km east of Nyngan, New South Wales, on 24 January 2025
Fall overboard during pilot transfer, Moreton Bay, Queensland, on 2 July 2025
What happened
At 2306 local time on 1 July 2025, 2 pilots boarded a 316 m container ship at the Mooloolaba pilot boarding ground for its transit through Moreton Bay to the port of Brisbane. Wind speeds during the day had exceeded the limits for berthing this size and type of ship and the pilots expected that it would be required to anchor at the inner anchorage. They planned to stay on board until later the following morning when a pilot launch would be available.
At 0200, one of the pilots checked with Brisbane vessel traffic service (VTS) and was informed that the weather conditions remained unsuitable for the ship’s berthing and advised that it be anchored in the inner anchorage. At 0236, the ship was anchored in a position to the north‑east of the STS‑2 anchorage (Figure 1).
At the same time, the pilot launch was at the anchorage with the pilots of 2 ships that had anchored earlier. While the launch had been scheduled to return to base, a decision was made to delay its return to allow the pilots of the container ship to disembark.
At 0255, after confirming that the anchor was holding, the officer of the watch escorted the pilots from the bridge for disembarking via the pilot ladder. The pilot ladder was properly rigged through the access door on the ship’s starboard side and it appeared to be in good condition. Weather conditions at the time were a 25-knot[1] westerly wind gusting to 30 knots and short, choppy seas with an average wave height of about 2 m.
As the tide was close to slack water,[2] the ship was riding to the wind and its yawing[3] intermittently exposed both the port and starboard sides to the weather. This meant that its hull did not provide adequate shelter (a lee) to the pilot launch, and the launch master found conditions unacceptable for a transfer when attempting to come alongside.
Consequently, the launch master asked the ship’s master (via radio) to provide a better lee. The ship’s main engine, rudder and bow‑thruster were then used to bring the wind on its port bow. This created a partial lee on the starboard side (considered marginal, but acceptable, by the launch master).
At about 0310, one pilot descended the ladder with a careful eye on the launch’s motion in the waves and stepped onto its deck. At the same time, a large wave pushed the launch away from the ship’s side, putting the pilot in a precarious position. The launch deckhand was unable to hold onto the pilot, who then slipped off the deck and fell overboard.
The pilot’s personal floatation device (PFD) inflated immediately and the launch master quickly manoeuvred clear and activated the man overboard procedures. This included deploying lifebuoys from launch and ship, but these were beyond the pilot’s reach. The launch master then moved it close to the pilot, which allowed the deckhand and the other pilots on board to recover the pilot using the stern‑mounted rescue scoop.
The pilot transfer operation was suspended and, after recovering the lifebuoys from the water, the launch began its return to base. The other pilot remained on board the ship to wait for weather conditions suitable for disembarking.
The recovered pilot was not injured but was feeling cold and exhausted. With no blankets or towels on board, the launch crew improvised with available clothing to keep the pilot warm while the launch made its way ashore. Once landed, the pilot was transported to hospital for treatment and confirmed to have no injuries.
Figure 1: Brisbane inner anchorage
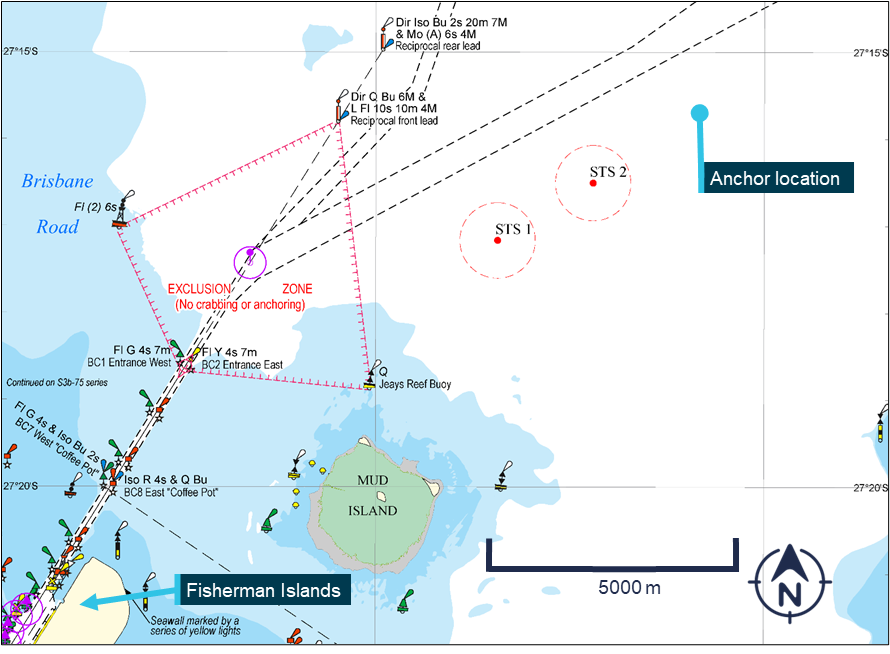
Source: Maritime Safety Queensland, annotated by the ATSB
Safety action
The pilotage provider’s internal investigation into the incident resulted in various proactive safety actions, including:
- promulgating lessons learned to its pilots and launch crews, with an emphasis on the need for greater care for pilot transfers at anchor and reiterating the need to stop the operation if anyone involved felt the conditions are unsuitable
- developing a formalised approach to assess transfer risk at the inner anchorage in consultation with the harbour master
- strengthening overboard rescue preparedness through refresher drills for launch crew and in-water survival training for pilots
- providing thermal care kits to launches and updating casualty care procedures.
Safety message
Pilot transfer via ladder continues to be a high‑risk operation, with associated incidents often resulting in serious or fatal injuries. Even when the equipment is in good condition and rigged correctly, environmental conditions must be carefully considered before starting the transfer. The responsibility for assessing suitability of the conditions rests with both the launch crew and the pilot(s), and both have the authority to stop the transfer in case of doubt.
Transfers from anchored ships involve additional risks, as they may not be able to provide a suitable lee and yawing may expose either side of the ship to the weather, making timing of the operation critical. In addition, pilot launches and their arrangements are designed for transfers while the ship is underway when the speed through the water allows the launch to be pushed up against the ship’s hull. This advantage is lost when the ship is at anchor when the launch is prone to being pushed away from the hull by waves, which also exacerbates unpredictable vertical motion.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Marine |
|---|---|
| Occurrence ID | MB-2025-005 |
| Occurrence date | 02/07/2025 |
| Location | Moreton Bay |
| State | Queensland |
| Occurrence class | Incident |
| Highest injury level | None |
| Brief release date | 19/08/2025 |
Ship details
| Departure point | Melbourne, Victoria |
|---|---|
| Destination | Brisbane, Queensland |
Runcorn level crossing collision
The ATSB has commenced a transport safety investigation into a collision between a B-double truck and a city-bound Queensland Rail suburban passenger train near Runcorn, Queensland on Thursday morning.
As reported to the ATSB, the truck was travelling south on Bonemill Road and entered the level crossing to turn left onto Beenleigh Road. While negotiating the turn, the truck became stuck, with its rear trailer obstructing the level crossing.
The driver of the passenger train, which was travelling from the Gold Coast towards Brisbane, applied emergency braking before the train collided with the rear of the truck a short time later.
The train and truck driver were uninjured, and there was one train passenger injury reported.
The ATSB requests anyone with footage of any part of the accident sequence to provide it via atsb.gov.au/witness.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.