Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
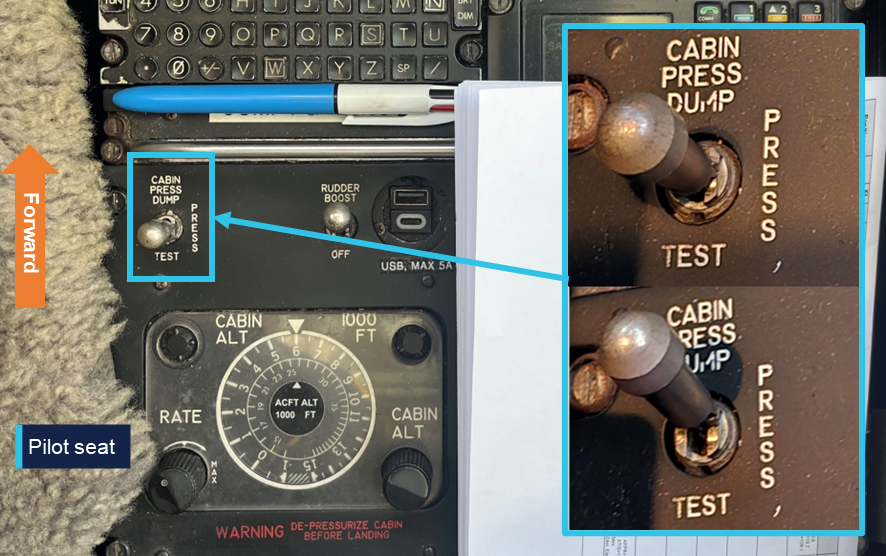
On 23 July 2025, a Raytheon B200 was being used to conduct a positioning flight from Darwin Airport to Gove Airport, Northern Territory with a single pilot on board. At 0217 local time, the aircraft was cruising at flight level 250[1] approximately 192 km from Darwin. The pilot reported that, at about this time, they momentarily placed their knee board on the centre console before picking it back up. While lifting it from the console, it caught on the cabin pressure switch, inadvertently moving it upwards from the centre PRESS position to the DUMP position (Figure 1).
Figure 1: Cabin pressure switch
Source: Supplied
Immediately the pilot felt a pressure change and a sudden drop in temperature consistent with a depressurisation. Additionally, the cockpit cabin altitude warning indicator illuminated, and the passenger oxygen masks deployed throughout the cabin. In response, the pilot donned their emergency oxygen mask. Suspecting the likely reason for the sudden depressurisation, they checked the cabin pressure switch and returned it to the PRESS position. Not sensing that cabin pressure was returning, the pilot conducted a descent to 10,000 ft. By the completion of the descent the cabin had repressurised.
Following the descent, the pilot determined that the passenger oxygen masks would need to be reset, and they elected to return to Darwin where engineering services were available. During the return flight at FL 240, the aircraft’s pressurisation system functioned normally, and the aircraft landed without further incident.
Safety action
The operator issued a safety notice to all flight crew outlining the event and highlighting the dangers of loose objects in the cockpit.
Safety message
Loose items in an aircraft can be a significant hazard, potentially interfering with flight controls, cabin switches or aircraft systems. Pilots should carefully consider the surrounding cockpit environment when moving or stowing loose objects in flight, particularly at night in a dark cockpit.
These items can also become dangerous projectiles causing serious injuries during an abrupt stop, turbulence or an accident sequence. Therefore, all loose items should be securely stowed for take-off and landing.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 250 equates to 25,000 ft.
The ATSB is advising operators of single-engine Pratt & Whitney Canada PT6A powered aircraft to train pilots for uncommanded engine acceleration malfunctions, after 10 people were injured in a charter flight accident involving a Cessna Caravan on Far North Queensland’s Lizard Island last year.
On 8 January 2024, the East Air-operated aircraft took off from Lizard Island for a planned flight to Cairns, with a pilot and nine passengers on board, an ATSB investigation report details.
During the climb, the pilot heard a change in the engine and noted that the aircraft was accelerating. The gauges showed engine torque and temperature above the redline, and no indications for gas generator speed or fuel flow. Propeller revolutions were high but within the normal operating range.
The pilot elected to return to land at Lizard Island. However, the uncontrollable excessive engine power led to a high‑speed approach, and the aircraft touching down long on the short runway.
The pilot applied maximum braking, but the aircraft overran the end of the runway at 92 kt and continued across undulating sandy soil, and low vegetation, until its left wingtip struck the ground.
The aircraft spun, flipped, and came to rest inverted, 127 m from the runway end. All ten occupants sustained minor injuries.
“The ATSB investigation concluded the uncommanded engine acceleration was likely due to a malfunction of the engine’s fuel control unit,” ATSB Director Transport Safety Kerri Hughes said.
Data provided by engine manufacturer Pratt & Whitney Canada indicated uncommanded engine acceleration events historically occurred more often than ‘roll back to idle’ malfunctions.
“Pilots of PT6A turbine single engine aircraft are trained for ‘roll back to idle’ malfunctions, but not trained for uncommanded engine acceleration malfunctions,” Ms Hughes said.
“Consequently, as demonstrated in this accident, there is limited awareness by pilots and operators of how to safely respond to an uncommanded engine acceleration event in aircraft powered by PT6A engines.”
Subsequently, the ATSB has issued a safety advisory notice to single-engine PT6A-powered aircraft operators, encouraging them to consider the potential responses to an uncommanded engine acceleration malfunction for different phases of flight, to document appropriate actions, and to train pilots for such scenarios.
“ATSB consultation with Cessna Caravan training organisations found that there was limited awareness of this type of event,” Ms Hughes said.
“While not as immediately dire as an engine failure or roll back to idle, an uncommanded engine acceleration is alarming and requires prompt action to control the aircraft and prevent overstress of the engine and airframe.”
Ms Hughes acknowledged changes made by the operator of the accident aircraft including publishing a temporary revision to its Quick Reference Handbook for the Cessna 208B to include an emergency item for unscheduled power increase during flight.
“When faced with non‑normal or emergency scenarios for which there are no procedures, pilots are required to exercise judgement based on their experience, skills and knowledge,” Ms Hughes noted.
“Operators should consider updating their procedures and providing appropriate training to ensure that their pilots are adequately prepared for such events.”
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the evening of 6 July 2025, a Saab 340 was being used to conduct a scheduled air transport flight to Sydney Airport, New South Wales. On board were 2 flight crew, 1 cabin crew and 27 passengers. The captain reported that the weather around Sydney at the time included developed thunderstorms and that holding and diversions had been in effect. They further reported that arrivals had recently been resumed as storms had passed and that, on final approach, weather radar indicated that the nearest storm cell was no closer than 19 km to the north.
When the aircraft was about 19 km west of Sydney, the automatic terminal information system (ATIS)[1] was revised to advise that the wind had increased from 20 kt from the west to include gusts of up to 40 kt. Consequently, air traffic control (ATC) changed the active runway to runway 25.[2] The aircraft was the second to be sequenced for an approach to the revised runway, following an Airbus A320. Passing about 14 km from the airport on final approach, the Saab crew heard a broadcast from the A320 crew that they were conducting a windshear escape[3] (Figure 1).
At the time, the A320 was approximately 9 km ahead. Hearing that the preceding aircraft had encountered windshear, the Saab crew discussed their windshear escape procedure and decided to continue the approach, waiting to hear more details about the nature of the windshear.
Figure 1: Aircraft flight path
Source: Flightradar24 overlaid on Google Earth, annotated by the ATSB
Approximately 2 minutes later, ATC advised the Saab crew that the A320 had encountered severe undershoot windshear.[4] The crew assessed that they were passing the position the A320 had first detected the windshear at this time. Shortly afterwards, when at approximately 700–800 ft, the captain reported that they observed a decrease in airspeed and an abnormal power indication consistent with windshear. The captain called for a windshear escape which the crew initiated. Throughout the subsequent climbing manoeuvre, they conducted a series of power, airspeed and configuration changes until confident they were no longer affected by windshear.
Two subsequent aircraft landed on runway 25 without any further reported windshear encounters, after which arriving aircraft were again sequenced for runways 34L/34R. Following the windshear escape, the aircraft was re-sequenced for runway 34L and landed without further incident.
Safety message
Low-level windshear is a serious threat to the safety of departing and landing aircraft. If windshear is encountered, rapid and large control inputs may be required and in severe cases, the effect of windshear may exceed the performance capabilities of the aircraft. Flight crew should use all available indicators to avoid areas of known windshear on the intended flight path. These include the presence of thunderstorm cells, and reports from pilots of other aircraft and air traffic control.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Automatic terminal information service: the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is updated either routinely or when there is a significant change to weather and/or operations.
[2]Runway number: the number represents the magnetic heading of the runway. The runway identification may include L or R as required for left or right when there are parallel runways.
[3]Windshear: a change in wind speed and/or direction over a short distance. A windshear escape is a pilot recovery technique used when an inadvertent windshear encounter is experienced.
[4]Undershoot windshear: a rapid decrease in the headwind component of the wind.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-029
Occurrence date
06/07/2025
Location
5 km east of Sydney Airport
State
New South Wales
Occurrence class
Incident
Aviation occurrence category
Missed approach, Turbulence/windshear/microburst
Highest injury level
None
Brief release date
25/08/2025
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340B
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
The ATSB is investigating a descent below minimum safe altitude and ground proximity alert involving a Cessna 560, registration VH-OHE, 23 km north-east of Perth Airport, Western Australia, on 13 August 2025.
Prior to commencing an instrument approach for runway 24 at Perth Airport, the aircraft descended below the minimum safe altitude. During this time flight crew reported that the autopilot disengaged and recalled observing an autopilot fail message on the primary flight displays.
The aircraft continued descending, and the flight crew subsequently received a terrain alert from the enhanced ground proximity warning system fitted to the aircraft. After responding to the alert, the flight crew continued the instrument approach and landed on runway 24.
The final report has been drafted and is undergoing internal review to ensure the report adequately and accurately reflects the evidence collected, analysis, and agreed findings.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
The ATSB has issued a safety advisory notice urging Cessna 206 operators to consider fitting an approved emergency exit modification or removing a middle row seat to allow better passenger emergency egress.
The notice stems from the investigation of a landing accident involving a Cessna U206F, where passengers were unable to exit from the rear cargo door after the accident due to the aircraft’s flaps being extended.
The ATSB’s final report into the 1 September 2024 accident notes the aircraft was being used for a short local area flight out of a private airstrip near the WA wheatbelt town of Moora, with a pilot and five passengers on board.
During the landing, which followed a non-standard approach, the aircraft bounced twice.
The pilot attempted a go-around, however the flap was set incorrectly and the aircraft was unable to gain height. The right wing struck the ground before the aircraft touched down on its landing gear, causing it to deviate from the runway and come to rest in an adjacent paddock.
After the aircraft came to a stop, the pilot and the passengers in the front and middle rows exited through the pilot’s forward, left cabin door.
However, the two passengers in the rear row were unable to operate the rear ‘clam shell’ cargo door as their emergency exit, with the forward half of the door blocked by the right wing’s flap, which was still extended.
The pilot was unable to retract the flaps, and the rear row passengers – a child and an older person – had to climb over the middle row of seats to exit the aircraft via the forward left cabin door.
“When the Cessna 206’s flaps are extended 10° or more, this prevents the cargo door from being opened, other than by following a multi-step process that is not intuitive or simple,” explained ATSB Chief Commissioner Angus Mitchell.
“Fortunately, in this case no injuries occurred, but this scenario has resulted in fatal injuries in the past due to the increased time taken to evacuate the aircraft, which impacts post-impact survivability, particularly if there is a fire or a water ditching.”
Mr Mitchell said Cessna 206 operators should consider either the removal of a middle row seat to improve rear seat occupants’ access to the pilot’s forward left cabin door, or the fitment of an approved Cessna 206 emergency exit modification that allows the immediate and unobstructed use of the rear cargo doors during an emergency exit.
“The removal of a middle row seat or fitment of an approved cargo door modification can improve the survivability for occupants of the Cessna 206,” he said.
Following a fatal accident in 2018, the Canadian aviation regulator, Transport Canada, now requires Canadian Cessna 206 operators to either remove a middle row seat, or to fit an STC‑approved modification that either provides an additional exit or modifies the cargo door such that extended flap does not block its opening.
“The ATSB strongly encourages Australian operators of Cessna 206 aircraft with the double cargo door, to review the Transport Canada mandated changes(Opens in a new tab/window), and consider implementing the improvements for the survivability for passengers during emergency egress in their Cessna 206s.”
Mr Mitchell said the ATSB investigation also highlighted the importance of passenger emergency briefings.
“The investigation found that the operator’s pre-flight passenger briefing did not include the demonstration of, and pilots were not trained how to operate, the emergency exit via the cargo door with the flaps extended,” he said.
“This highlights the importance of Cessna 206 pre-flight passenger briefings incorporating a demonstration of the limitations of the cargo door as an emergency exit with the flaps extended.”
"The ATSB advises Cessna 206 pilots and operators that due to the difficulties occupants have encountered egressing the rear cargo door to ensure they are familiar with CASA‑issued Airworthiness Bulletin 52‑006(Opens in a new tab/window), and ensure passengers are provided with a thorough safety briefing demonstrating the cargo door emergency egress when the wing flaps remain in the extended position," Mr Mitchell concluded.
On 17 August 2025, a Piper PA-28, registration VH-BUN, was undertaking a navigation training exercise under the visual flight rules from Wollongong (Shellharbour) Airport, New South Wales, with a student pilot and instructor on board.
While flying south along the coast north of Sydney, at around 1,600 ft above mean sea level, the crew heard unusual engine noises and observed a rapid drop in engine RPM. This was accompanied by a period of heavy engine vibration and a smell of oil. As they continued south, the engine RPM progressively reduced. Approximately 6 minutes after the first abnormal engine indications, the instructor determined that the safest option would be to conduct a landing on the Mona Vale golf course.
However, during the final stages of the approach to the golf course, the pilot slowed the aircraft to around 50 kt indicated airspeed before they realised they could not safely land straight ahead, and made a right turn to avoid the club house facilities. The aircraft subsequently landed heavily in a right-wing low attitude. All 3 undercarriage legs detached, and the aircraft slid approximately 45 m before coming to rest. The student pilot received minor injuries while the instructor was uninjured. The aircraft suffered substantial damage.
What the ATSB found
The ATSB found that the exhaust valve of the engine’s number 3 cylinder broke away from its stem and caused extensive damage to the internal surfaces of the cylinder, its piston, and spark plugs. This resulted in a rapid loss of power from the engine, such that the aircraft was unable to maintain level flight. The specific failure sequence of the exhaust valve could not be determined.
The instructor was proactive in maintaining an awareness of potential landing sites throughout the flight. Consequently, they were able to promptly identify a suitable area to conduct a precautionary landing and avoid a more adverse outcome.
What has been done as a result
Following the accident, the operator undertook several safety actions, including:
Revision of the emergency briefing content, and formal re-statement of the requirement for pre-impact and evacuation procedures to be briefed by the instructor, and confirmed by the student, before every flight.
Completion of a review of competency in conducting engine failure procedures for all flight instructors, and implementation of additional training and enhanced supervision where required.
Commencement of a process to check students’ post‑engine failure competencies, including glide path judgement, execution of post‑failure actions, and engine securing checks.
Safety message
This investigation highlights the importance of effective contingency management and decision-making skills in emergency situations.
In a single engine aircraft, a partial engine failure can present more options and decision‑making challenges than a total loss of power. Greater uncertainty of the aircraft’s performance over time makes it more difficult to choose the lowest risk course of action and potentially requires decisions to be revisited and revised. However, certain traits of human cognition, such as confirmation bias, may resist changing decisions which have already been made.
The instructor in this investigation reported they had an awareness of several contingency landing locations along their route prior to the engine malfunction occurring. This subsequently helped them to decide a suitable course of action when the malfunction did occur. Furthermore, as the situation evolved, they recognised the need to re‑evaluate their original choice of landing site. Their timely selection of a different landing site likely minimised the adverse consequences of the occurrence. A previous ATSB investigation (AO-2024-010) highlighted how a delayed decision to land following an engine malfunction in a single engine aircraft led to a more challenging forced landing.
In this case the cause of the exhaust valve failure could not be determined. However, in 1988 Textron Lycoming, the manufacturer of the aircraft’s engine, provided guidance on maintenance practices to reduce the possibility of valve sticking (Service Instruction No. 1425 ASuggested Maintenance Procedures to Reduce the Possibility of Valve Sticking). The guidance noted that engine oil contamination increases the possibility of valve sticking and advised preventative actions, including:
regular changing of oil and oil filters
cleaning of air filters
proper sealing of the air induction system.
The risk of valve sticking is increased for engines operating in hot ambient conditions, and where engines are regularly shut down before they have cooled sufficiently.
Summary video
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 17 August 2025, a Piper PA-28-140, registration VH-BUN, was undertaking a navigation training exercise under the visual flight rules (VFR)[1] from Wollongong (Shellharbour) Airport, New South Wales, with a student pilot and flight instructor on board.
The aircraft departed Wollongong at 1222 local time, initially flying north to Camden Airport. The student flew 3 circuits at Camden before landing and shutting down the aircraft for a brief stop. Departing Camden at 1331, the aircraft continued north to Wisemans Ferry, before turning south-east at Barrenjoey Head. From there the crew had planned to follow the coast south before returning to Wollongong (Figure 1).
At 1413, shortly after the aircraft passed overhead Barrenjoey Head at an altitude of 1,600 ft, the aircraft’s engine suddenly started to produce an unusual noise, accompanied by a brief period of heavy vibration and a smell of oil in the cockpit. The instructor observed the engine RPM indication drop rapidly from the cruise setting of 2,450 to around 2,100. Indications of oil temperature, oil pressure and fuel pressure all remained in the normal range.
The instructor assumed control of the aircraft from the student. The student then followed the instructor’s directive to turn on the fuel pump and switch the fuel selector valve from the right tank to the left tank. The instructor advised they did not select the carburettor heat to ON as they assessed it would further reduce the engine RPM by about 100 and, as they had been flying at cruise power for about an hour, it was unlikely they were experiencing carburettor icing.
The instructor communicated the nature of the engine problems to Sydney terminal air traffic control (ATC) and was informed that the nearest airport to them was Sydney, directly to the south. Shortly after, the instructor reported that they would continue tracking south, but that the engine RPM had fallen further to 1,900. ATC advised that Long Reef golf course was 4 NM (7 km) ahead of the aircraft. The instructor assessed that the engine’s performance was deteriorating, and the aircraft could not maintain level flight. They therefore decided to make a landing at Long Reef golf course, noting that although Mona Vale golf course was closer, its abundance of trees would make landing more challenging.
Shortly after, with the aircraft approximately 1 NM (1.9 km) south-east of the Mona Vale golf course the instructor detected that the engine RPM had reduced further to 1,500. They determined that the aircraft would no longer be able to reach Long Reef and decided that Mona Vale golf course was now the best available option for a landing. The instructor advised ATC of their intention to land at Mona Vale and turned the aircraft north towards it.
Once the instructor felt assured that the aircraft was able to reach the golf course, they began to progressively extend the aircraft’s flaps and reduce the airspeed from the best glide speed, which based on the aircraft’s weight they assessed to be 70 kt, aiming for approximately 55 kt, reducing to 50 kt on touchdown. However, as the aircraft neared the ground, travelling in a north-east direction, the instructor judged that there was insufficient clear area ahead of them to land safely. Consequently, they made a right turn of approximately 90 degrees to avoid the club house facilities and re-aligned the aircraft to land in a south-east, downslope direction. The instructor did not identify the extent of the downslope.
During the turn, the right wing dropped, and the aircraft impacted the golf course heavily. All 3 undercarriage legs detached on impact and the aircraft slid approximately 45 m before coming to rest upright on a section of fairway.
Figure 1: Flightpath of VH-BUN
The image shows the point at which abnormal engine indications were first noticed and the location of the precautionary landing on Mona Vale golf course. Source: Google Earth and Flightradar24, annotated by the ATSB
Fuel began leaking from the underside of the aircraft but there was no fire. Both occupants were able to exit the aircraft soon after, assisted by first responders from the golf club. The aircraft received substantial damage. The student suffered minor injuries during the impact, while the instructor was uninjured. Both were subsequently taken by ambulance to a local hospital for assessment, where the student remained overnight, but the instructor discharged themselves later in the evening.
Context
Flight crew background
The flight instructor held a Commercial Pilot Licence (Aeroplane) and a CASA class 1 aviation medical certificate. At the time of the occurrence, they had accumulated 1,392 flying hours, 305 of which were in the Piper PA-28. The instructor had flown 75 hours in the past 90 days, 31 of which were in the PA-28.
The instructor reported that they had flown the same navigational route many times prior to the occurrence flight. They had developed knowledge of various sites along the route, which could serve as contingency landing locations in the event of an emergency.
The student pilot was undertaking training towards their Private Pilot Licence (Aeroplane) and held a CASA class 2 aviation medical certificate. At the time of the occurrence, they had accumulated a total of 91 hours flying time, 3 of which were in the PA-28.
Aircraft information
General
The aircraft was a Piper PA-28-140 (serial number 28-23228) manufactured in the United States in 1967. The aircraft was fitted with a Textron Lycoming O-320-E2A piston engine and Sensenich fixed pitch propeller. The aircraft was being maintained under the Civil Aviation Safety Authority Schedule 5. The most recent periodic maintenance was a 100‑hour inspection completed on 26 May 2025. At that time the aircraft had accumulated 8,478 hours in service. The next periodic inspection was due on 26 May 2026, or 8,578 hours, whichever occurred first. The aircraft’s total time in service at the time of the occurrence was around 8,509 hours.
A review of the maintenance documentation indicated that the aircraft’s engine was last overhauled in November 1993 and was maintained under Civil Aviation Regulation 42B CASA maintenance schedule using Airworthiness Directive AD/ENG/4 during every periodic inspection. During the last periodic inspection in May 2025, there were no engine discrepancies identified. At the time of the occurrence, the engine had accrued approximately 1,680 hours since overhaul.
Fuel system
The aircraft was equipped with 2 fuel tanks, one in each wing, referred to as the left and right tanks. Each tank had a maximum capacity of 95 litres, providing a total capacity of 190 litres.[2] A fuel tank selector valve in the cockpit could be positioned to control which tank provided fuel to the engine. The selector valve could be positioned to feed fuel from either the left tank or the right tank, or to an off position, where neither tank would provide fuel. It was not possible to supply fuel to the engine from both tanks simultaneously. After the selector valve, fuel passed through a strainer, 2 fuel pumps, and a carburettor before reaching the engine.
Pre-flight inspection
On the morning of the flight, both the instructor and the student pilot conducted independent pre‑flight inspections. This included inspection of the engine compartment where there was no evidence of oil leaks. They checked the oil levels and observed that there was sufficient oil, and it was a normal colour.
Both of the aircraft’s fuel tanks were filled to their maximum capacity shortly before departing Wollongong. The crew started up and taxied out using fuel from the left tank, before switching to the right tank just before take-off. The first flight to Camden was 41 minutes in duration and was flown entirely using the right tank. After landing at Camden, the student pilot inspected the quantity of fuel in each tank using a dipstick. The amount of fuel consumed during the first flight was as expected and there was sufficient fuel on board to perform the second flight as planned, with significant reserves.
Approximately the first 30 minutes of the second flight were flown using the left tank, before the crew switched to using the right tank again, at around 1404, just after passing Wisemans Ferry. The right tank remained selected until the engine began to malfunction. The crew switched back to the left tank as part of their efforts to rectify the engine problems, and the fuel selector valve remained in this position for the rest of the flight.
Post-flight fuel inspection
A post-accident inspection of the aircraft’s fuel system determined that approximately 58 litres of fuel remained in the right tank, but only around 2.5 litres remained in the left tank. The fuel selector valve was positioned to feed fuel from the left tank.
However, the fuel strainer, located on the lower edge of the engine firewall, was ruptured during the impact and a significant quantity of fuel was observed draining from it after the accident. With the fuel selector valve positioned to the left tank, it is therefore likely that the low quantity of fuel observed in the left tank was a result of fuel draining away via the damaged fuel strainer post-accident. The ATSB determined that fuel starvation was not a contributing factor.
Post-flight engine inspection
The ATSB undertook a detailed engineering inspection of the aircraft’s engine following the occurrence. Each of the engine’s 4 cylinders was subject to a compression check, external visual inspection, and internal borescope inspection. Cylinders 1, 2 and 4 exhibited no major defects. However, cylinder 3 showed signs of significant damage.
The exhaust manifold of cylinder 3 was heavily soaked with oil and its valve train components showed signs of exposure to combustion gases. Cylinder 3 provided no compression, and an internal inspection showed its upper surface and piston face to be heavily damaged with multiple strike marks and 2 large holes (Figure 2). The exhaust valve had broken off at its stem and was missing, while the valve guide exhibited a small fracture line. Both of the cylinder’s spark plugs had sustained impact damage to their electrodes.
Figure 2: Borescope images of cylinder 3 showing the missing exhaust valve and damage to the piston face
Source: ATSB
Meteorological information
The Bureau of Meteorology reported the visibility at the time of the occurrence as greater than 10 km. The temperature was around 16°C, with a dew point of around 1°C, and an atmospheric pressure adjusted to mean sea level of 1,017 hectopascals.
Both the instructor and student pilot reported that the weather conditions were favourable for VFR flying, with extensive visibility, little turbulence, and only light southerly winds.
Safety analysis
The ATSB determined that the exhaust valve of cylinder 3 impacted the piston surface multiple times, causing damage to the piston, cylinder and spark plugs. This resulted in a sudden loss of compression and subsequent loss of engine power. It could not be determined if the valve had stuck open, resulting in the piston impact and valve fracture, or if the valve fractured prior to impacting the piston.
Following the loss of power, the instructor identified that an off-airport landing was required. The instructor’s prior knowledge of the area and proactive contingency planning helped them identify possible locations. Furthermore, as the engine’s performance continued to deteriorate, they re-evaluated their decision and changed the plan, including shortly before touchdown when it was assessed that there was insufficient clear area ahead.
While the turn away from obstacles prevented a potentially significant frontal impact, it also led to the aircraft contacting the ground with substantial vertical force due to the low remaining airspeed limiting the instructor’s ability to flare the aircraft. Fortunately, the aircraft absorbed the vertical impact, preventing significant injury to the occupants.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following finding is made with respect to the loss of power and forced landing involving Piper PA-28, VH-BUN, 32 km north-north-east of Sydney Airport, New South Wales, on 17 August 2025.
Contributing factor
An exhaust valve in the aircraft's engine failed, resulting in a significant reduction of power and aircraft performance. Subsequently, the pilot in command conducted a forced landing on a golf course.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety actions by operator
The operator undertook the following safety actions after this accident:
Revised the emergency briefing content and formally re-stated the requirement for pre‑impact and evacuation procedures to be briefed by the instructor and confirmed by the student before every flight.
Completed a review of competency in conducting engine failure procedures for all flight instructors and implemented remedial training and enhanced supervision where required.
Commenced a process to check students’ post‑engine failure competencies, including glide path judgement, execution of post‑failure actions, and engine securing checks.
Implemented Drugs and Alcohol Management Plan (DAMP) policy refresher training and increased the frequency of random Alcohol and Other Drugs (AOD) testing across all employees undertaking safety sensitive aviation activities.
Introduced carburettor icing probability assessment as part of the standard pre-flight preparation activities and provided education on the precautionary use of carburettor heat.
Reviewed the on-boarding process for cross-hired aircraft and is consulting with other industry participants to create internal guidance around the use of aircraft with older engines.
Sources and submissions
Sources of information
The sources of information during the investigation included:
pilots of the accident flight
the aircraft operator
the aircraft owner
the maintenance organisation
the aircraft insurer
Airservices Australia
Civil Aviation Safety Authority
New South Wales Fire and Rescue
the Bureau of Meteorology
video footage of the accident flight and other photographs and videos taken on the day of the accident
ADS-B data from Flightradar24.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
pilots of the accident flight
operator of the accident aircraft
owner of the accident aircraft
Civil Aviation Safety Authority.
Submissions were received from:
one of the accident flight pilots
the operator of the accident aircraft
the owner of the accident aircraft.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]The operator’s documentation noted that of the total 190 litre fuel capacity, only 187 litres were usable.
Occurrence summary
Investigation number
AO-2025-049
Occurrence date
17/08/2025
Occurrence time and timezone
14:00 Australian Eastern Standard Time
Location
32 km north-north-east of Sydney Airport
State
New South Wales
Report release date
22/01/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Engine failure or malfunction, Forced/precautionary landing
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28-140
Registration
VH-BUN
Serial number
28-23228
Aircraft operator
Airspeed Aviation
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Departure point
Wollongong (Shellharbour) Airport, New South Wales
Destination
Wollongong (Shellharbour) Airport, New South Wales