Runway incursion involving De Havilland Aircraft of Canada Limited DHC-8, VH-QOD, and Piper PA-28, VH-XDK, Wagga Wagga Airport, New South Wales, on 15 July 2024
Final report
Report release date: 13/11/2025
Investigation summary
What happened
On 15 July 2024, a QantasLink De Havilland Aircraft of Canada Limited DHC-8-402, (Dash 8), registered VH-QOD, was taxied to reposition to a different bay at Wagga Wagga Airport, New South Wales. This repositioning required the Dash 8 crew to taxi out onto the runway and then return to a different bay. As the Dash 8 entered runway 05, the crew were unaware that a Piper PA-28, registered VH-XDK, operating on a training flight by the Australian Airline Pilot Academy (AAPA), had already commenced its take-off roll from the opposite end of the runway.
The instructor of the PA-28 was aware of the Dash 8 taxiing and assumed that the Dash 8 had received and understood their previous positional broadcasts. However, the crew of the Dash 8 were not aware of the PA-28 preparing for take-off on runway 23.
Upon entering runway 05, the Dash 8 was notified by a preceding aircraft that had landed, that there was another aircraft taking off from runway 23. The captain of the Dash 8 immediately stopped the aircraft and engaged reverse thrust to clear the runway. Simultaneously, the PA-28 pilot rejected their take-off from runway 05.
What the ATSB found
The ATSB identified that during ground-based repositioning, the Dash 8 was unaware of the PA-28 that was taxiing for take-off on an opposing runway. This led to a situation where the crew of the Dash 8 had an incomplete comprehension of the ground-based traffic.
Without any prior alert or expectation of the presence of the PA-28, the Dash 8 crew did not visually detect the PA-28 on take-off from the reciprocal end of the runway, prior to the Dash 8 entering the runway to taxi to the terminal. The PA-28 presented a difficult visual target due to its size and orientation over the 1,700 m distance, making unalerted detection unlikely.
Once made aware of the potential conflict of collision, the captain of the Dash 8 immediately reversed the aircraft away from the preferred runway without confirming that no other aircraft or obstacle was behind the Dash 8.
While the pilot of the PA-28 gave all the required radio calls, they did not directly communicate with the Dash 8 crew to identify the possible conflict, then positively arrange separation. Additionally, the Dash 8 ground-based reception, on VHF communications panel radio 2, had reduced strength and clarity.
The QantasLink radio procedure required crew to use the number 2 VHF communications panel radio to broadcast and receive on local frequencies during operations at a non-controlled aerodrome. This likely reduced ground-based reception strength and the likelihood of the Dash 8 hearing other traffic in certain circumstances.
Reduced VHF ground-based communication was identified at the eastern end of runway 23 at Wagga Wagga Airport. Local operator reports and procedures indicate that reduced communication strength and clarity can be experienced on the eastern end of taxiway A to other areas of the airport.
During taxi for take-off, the PA-28 was not broadcasting transponder information, which also did not identify them to other traffic in the vicinity of the aerodrome. The AAPA procedure requiring the selection of the transponder to ‘ALT’ before entering the runway, rather than prior to taxi, became a missed opportunity to provide electronic enhancement of situational awareness to other airport operators.
What has been done as a result
ATSB issued a safety advisory notice (AO‑2024‑041‑SAN‑01) to advise pilots and operators to review their procedures to ensure that mode S transponders are on from first movement of the aircraft.
AAPA has advised the ATSB that changes have been made to its PA-28 Flight Crew Operating Manual, and Quick Reference Handbook, which reflects the transponder being selected to ALT mode after start in both the checklist as well as being incorporated as part of the scan action flow.
On 6 December 2024, De Havilland Aircraft of Canada Limited issued 2 flight operations service letters relating to radio communications, with one covering Dash 8 100-300 series aircraft and the other covering the Dash 8 400 series aircraft. The service letters remind operators that ground‑based VHF communications are affected by line of sight and can be impacted by buildings, terrain or aircraft structures and that use of VHF COM 1 is more effective for ground-based communications with other aircraft on the ground.
The airport operator had issued a notice to airmen (NOTAM) notifying aircraft of a potential radio black spot at Wagga Wagga Airport under some conditions.
QantasLink issued a safety alert notice encouraging crew to consider additional precautions when taxiing for departure or any other manoeuvring on-ground at Wagga Wagga Airport. This advice was issued due to on-ground VHF communications between aircraft possibly being affected by obstacles in the line of sight.
Safety message
Communication and self-separation in non-controlled airspace is one of the ATSB’s SafetyWatch priorities. Wherever you fly, into either non-controlled or controlled aerodromes, maintaining a vigilant lookout at all times is important. Situational awareness and alerted see-and-avoid is an effective defence against collision and good airmanship dictates that all pilots should be looking out and not be solely reliant on the radio for traffic separation. Being aware of other nearby aircraft and their operational intentions is important.
Effective use of all available sources of information is an effective risk control to achieve enhanced situational awareness and an accurate mental model of other traffic at a non‑controlled aerodrome.
Pilots are reminded that although accurate and timely radio calls play a critical role in ensuring collision avoidance in uncontrolled airspace, they cannot assume from an absence of other radio calls that there is no conflicting traffic. This is particularly important in an environment where there is high expectation of mixing with other aircraft of different sizes, flight rules and performance levels operating at the same time, in the same airspace.
Pilots can enhance their situational awareness and mutual traffic separation by:
- making the recommended broadcasts when in the vicinity of a non-controlled aerodrome
- actively monitoring the common traffic advisory frequency while maintaining a visual lookout and constructively organising separation through direct contact with other aircraft
- ensuring mode S transponders, where fitted, are selected to transmit altitude information before taxiing
- not hesitating to contact another aircraft if there is any uncertainty as to their position and/or intentions.

The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. This investigation report highlights the safety concerns around reducing the collision risk around non-towered airports.
The occurrence
On 15 July 2024, a Piper Aircraft Corporation PA-28, registered VH-XDK, operated by the Australian Airline Pilot Academy (AAPA), with an instructor and student on board, taxied from the apron at Wagga Wagga Airport, New South Wales (Figure 1) for a training flight. At 1609 local time, the crew broadcast they were taxiing for runway 23 (Figure 2, position A). About 20 seconds later, the crew of an inbound Saab 340 responded, asking for the call sign to be repeated. The Saab 340 was 30 NM away at this stage and could not understand the call sign, even when repeated twice more. About 5 minutes later at 1614:12, the crew of the Saab 340 broadcasted that they were now on a 10 NM straight in approach for runway 23 (see Appendix A – CTAF Recordings).
At about the same time, the 2 crew members of a QantasLink De Havilland Aircraft of Canada Limited DHC-8-402 (Dash 8), registered VH-QOD, were on board the aircraft at the Wagga Wagga Airport apron. The crew were making preparations to reposition the aircraft from the apron to another bay (on the apron) by taxiing the aircraft via the runway (Figure 1). The Dash 8 crew reported they spent about 5 minutes[1] preparing the aircraft on the flightdeck prior to taxiing. However, they did not recall hearing the initial taxi call and callsign repeats from the PA-28, but did recall hearing the 10 NM inbound call from the Saab 340.
Figure 1: Intended taxi routes for aircraft
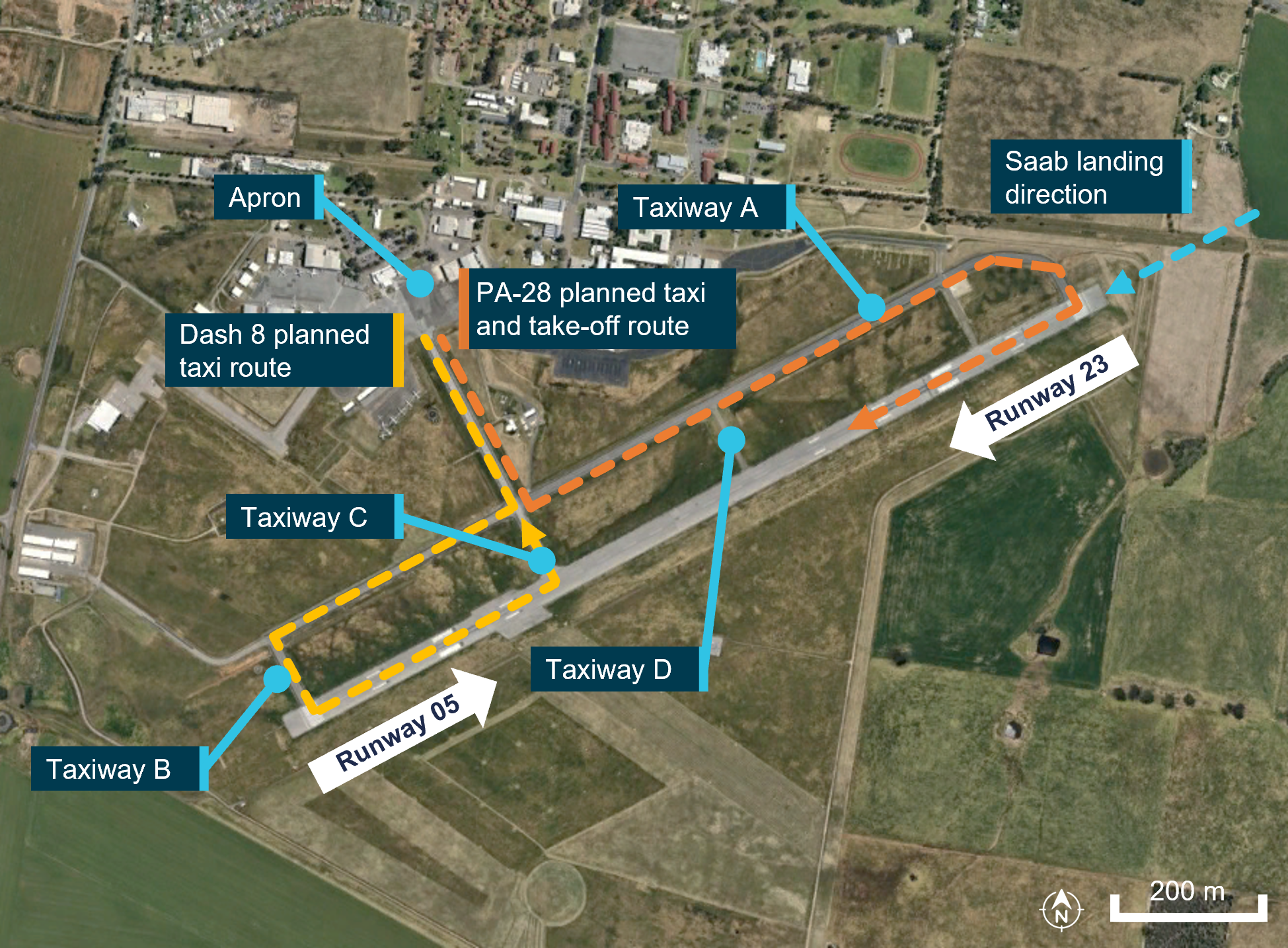
Source: Google Earth, annotated by the ATSB
At 1616:27 the Saab 340 crew broadcast that they had joined a 5 NM final for runway 23.
At 1617:31 (Figure 2, position B, Dash 8) the Dash 8 crew broadcast that they were taxiing for runway 05. At this time, the PA-28 was on taxiway A, approaching runway 23 (Figure 2, position B, PA-28).
Figure 2: Position of respective aircraft at given times
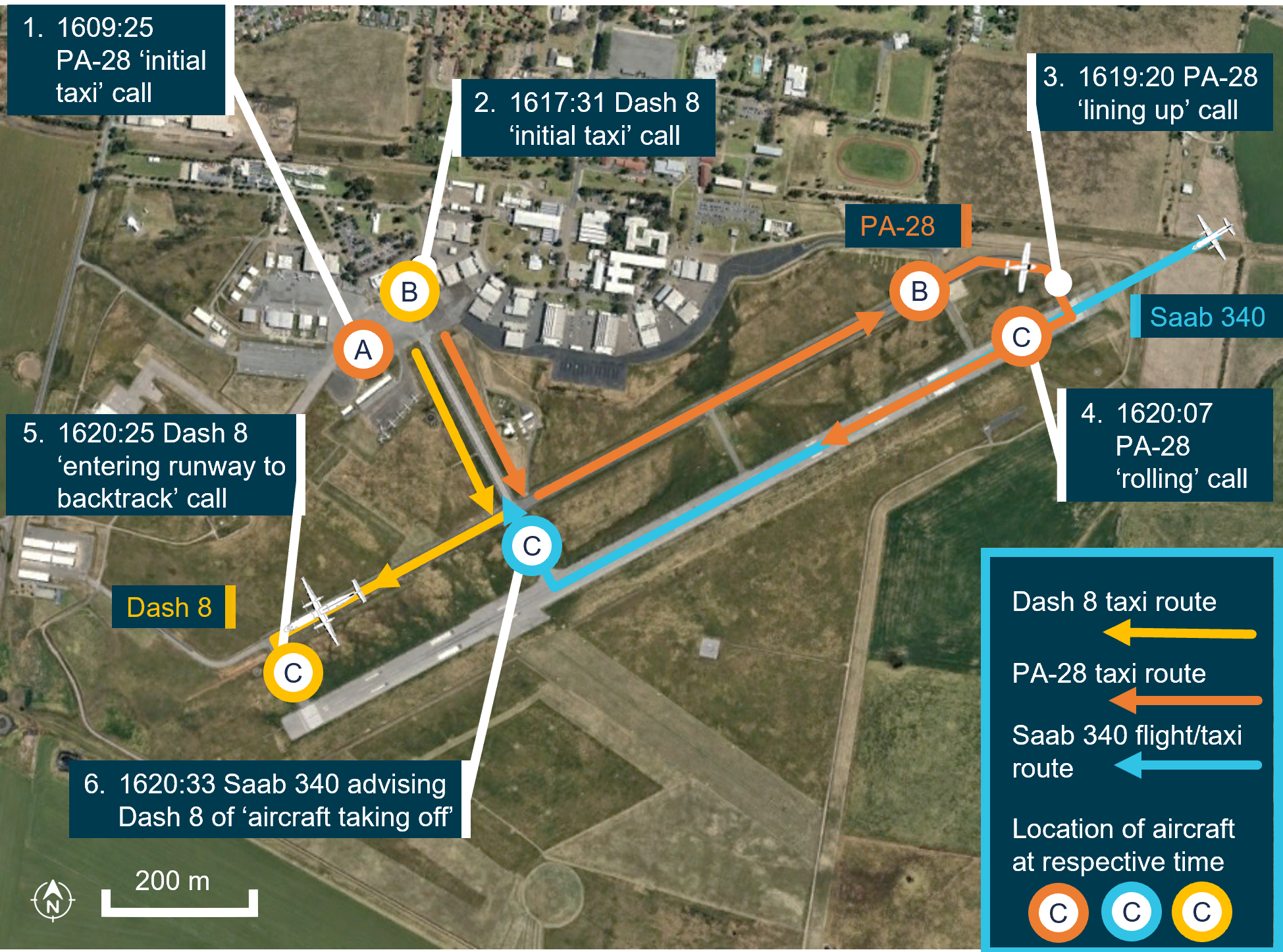
Source: Google Earth, annotated by the ATSB. Note: aircraft not to scale
Being aware only of the inbound Saab 340, the Dash 8 crew communicated directly with them. This was to gain an understanding of the Saab 340 crew’s intentions on landing and exiting the runway. While still taxiing towards the runway at 1618:32, the Dash 8 crew told the Saab 340 crew of their intent to enter and backtrack from the threshold of runway 05, keeping out of the way of the Saab 340’s landing.
The instructor of the PA-28 recalled hearing the radio calls from both aircraft during this time. The PA-28 was aware of the Dash 8 taxiing for runway 05 and assumed that the Dash 8 had also heard their earlier calls, and would hold short of the runway for their departure.
At 1619:20, the PA-28 was positioned on runway 23, with strobe lights on, behind the landed Saab 340 and the instructor made a ‘lining up and holding’ call (Figure 2, position B, PA-28). About 30 seconds later the Saab 340 crew made a broadcast that they were clear of the preferred runway (Figure 2, position C, Saab 340). The PA-28 instructor then broadcast their ‘rolling call’ (Figure 2, position C, PA-28) and commenced take-off at 1620:07.
At 1620:25, the Dash 8 crew gave an entering call for runway 05 with intentions to taxi to taxiway C (Figure 2, position C, Dash 8) and then entered the runway.
On hearing the Dash 8 crew’s broadcast, the Saab 340 crew notified the Dash 8 that ‘there is an aircraft taking off on runway 23’ at 1620:33. Simultaneously, the PA-28 student pilot also rejected their take-off.
The Dash 8 crew immediately stopped at their current position, with the aircraft still perpendicular with the runway and estimated by the captain to be about 5 m inside the runway gable markers.[2] The captain acknowledged the broadcast and then visually identified the PA-28 on the runway.
The captain of the Dash 8 subsequently engaged Beta plus power mode[3] (reverse thrust) to reverse the Dash 8 backwards along taxiway B to ensure clearance of the preferred runway. The PA-28 crew broadcast they would exit runway 23 on taxiway D.
The Dash 8 captain then established direct radio contact with the PA-28 crew, stating ‘nil radio transmission heard and they are still broken’.
The PA-28 vacated the runway and taxied again for a subsequent departure. The Dash 8 then re-entered runway 05 and backtracked runway 23 and vacated to the apron.
Context
Pilot information
Flight crew VH-QOD (Dash 8)
The captain held an Air Transport Pilot Licence (Aeroplane) and a valid class 1 aviation medical certificate. They reported a total flying time of 2,912 hours with 2,389 of those being on the Dash 8 aircraft type. The captain reported being familiar with Wagga Wagga Airport and had operated there regularly.
The first officer (FO) held a Commercial Pilot Licence (Aeroplane) (CPL-A) and a valid class 1 aviation medical certificate. They reported a total flying time of 1,312 hours with about 438 of those hours being on the Dash 8. The FO had been employed with the operator for approximately a year and had flown into Wagga Wagga Airport during their training and subsequent line operations.
Flight crew VH-XDK (Piper PA-28)
The instructor of the PA-28 held a CPL (Aeroplane) with a grade 2 instructor rating. They held a valid class 1 aviation medical certificate and reported a total flying time of 796 hours, with approximately 146 hours being on the PA-28. The instructor regularly operated out of Wagga Wagga Airport, as it was the company base of operation.
The student pilot of the PA-28 held a class 1 aviation medical certificate and reported about 17 hours of flying time.
Aircraft information
VH-QOD (Dash 8)
The De Havilland Aircraft of Canada Limited (DHC) DHC-8-402, was a high-wing, pressurised, commuter aircraft powered by 2 turboprop engines. VH-QOD was manufactured in Canada in 2006 and was first registered in Australia on 22 May 2006.
VHF radio antenna position and condition
The Dash 8 had 2 VHF radio systems, each using separate antennas installed on the upper and lower fuselage (Figure 3):
- Number 1 VHF COM antenna (VHF COM 1) mounted on the roof of the aircraft forward of the wings.
- Number 2 VHF COM antenna (VHF COM 2) mounted on the belly of the aircraft.
Figure 3: Dash 8 with annotations of VHF antenna locations on airframe

Source: Gyo Kamata Jetphotos.com, annotated by the ATSB
Transponder and ADS-B system on the Dash 8
The Dash 8 was equipped with an automatic dependent surveillance-broadcast ADS-B mode S transponder. ADS-B uses digital positional data provided by a GPS sensor on board the aircraft. This information is transmitted via the same channels used in conventional aircraft transponder transmissions. The Dash 8, ADS-B transponder units are fully integrated through the Dash 8 audio and radio control and display unit. Positional data for each ADS-B transponder is provided through the aircraft flight management system.
TCAS system on the Dash 8
A traffic collision avoidance system (TCAS) was fitted to the Dash 8. A TCAS interrogates the transponders of nearby aircraft and uses this information to calculate the relative range and direction of this traffic. The system displays this information to the flight crew, providing situational awareness of the location of other aircraft, and is available on the ground and when airborne.
TCAS is designed to be used as an airborne device, which performs surveillance of nearby aircraft and provides information on the relative direction and altitude of these aircraft so that the collision avoidance algorithms can perform their function (Federal Aviation Administration, 2011)
Limitations exist for the use of TCAS in lateral separation. Current generations of TCAS are primarily focused on vertical separation (climb or descent); TCAS I and II generations of TCAS do not provide horizontal separation.
In certain circumstances functions and alerts within the TCAS system are inhibited. An example is documented in FAA AC 90-120 (Federal Aviation Administration, 2024) that noted:
2.11.5 ACAS[4] does not display aircraft on the ground and may not display an aircraft when own-ship ACAS estimates that the other aircraft is below 380 feet Above Ground Level (AGL), unless the other aircraft is operating with a Mode S transponder that reports airborne status.
While the use of TCAS for monitoring other aircraft on the ground was not an operator procedure, the Dash 8 crew identified that they regularly used it as an aid for situational awareness. The captain and FO both recalled reviewing their TCAS with only one aircraft (the Saab 340) being seen.
Flightradar24 application
The crew of the Dash 8 utilised an electronic flight bag (EFB).[5] Additionally during taxi, they reviewed the Flightradar24 application as a tool to enhance their situational awareness of potential traffic in the area.
Flightradar24 is a global flight tracker that shows live air traffic from around the world and combines data from several sources including ADS-B.
QantasLink did not have a formal policy referring to the use of the Flightradar24 application. However, the flight crew advised that this application is often used by pilots as a resource to aid situational awareness. As with TCAS, only the Saab 340 aircraft was visible on the Flightradar24 app during the Dash 8 taxi period.
VH-XDK (Piper PA-28)
VH-XDK was a Piper Aircraft Corporation, PA-28-161 Cherokee Warrior III, manufactured in the US in 2008. VH-XDK was a single‑engine, 4‑seat, low‑wing design aircraft, operated by Australian Airline Pilot Academy Pty Ltd (AAPA).
VHF radio systems on PA-28
The aircraft was equipped with 2 Garmin G430[6] VHF navigation/communication systems, transmitting at a minimum of 10 watts through 2 independent antennas. The VHF COM 2 antenna is located on the top of the fuselage and the VHF COM 1 antenna is located on the underside of the fuselage.
Figure 4: Antenna location on PA-28
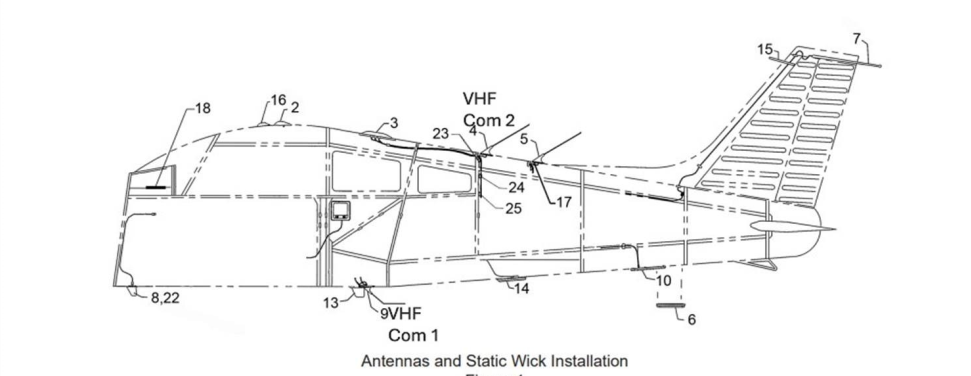
Source: PA-28 operator
Transponder and ADSB system PA-28
The PA-28 was fitted with a Garmin GTX 330ES MODE-S, providing a mode S digital transponder signal. The transponder likely would have made the PA-28 electronically conspicuous to the Dash 8 crew through the flight crew’s Flightradar24 application on their EFBs, when selected to ON/ALT.
Meteorological information
Weather conditions at Wagga Wagga Airport around the time of the occurrence were identified as a moderate north-westerly wind at about 13 kt, with greater than 10 km visibility. The cloud was reported as broken (between 5–7 oktas[7]) between 2,000 ft and 2,600 ft above ground level.
Airport information
Wagga Wagga Airport
Wagga Wagga Airport is a regional, certified aerodrome, located about 6 NM to the south‑east of Wagga Wagga township in New South Wales, Australia. The aerodrome had an elevation of 724 ft (221 m) above mean sea level (AMSL), and had 2 runways running north‑east, south-west and north-west, south-east. The primary sealed runway at Wagga Wagga is runway 05/23 and is 1,770 m long with the secondary, unsealed runway 12/30 being 851 m long (Figure 5).
Runway 05/23 exhibited a minor elevation differential between each runway threshold. The threshold of runway 05 was recorded at 216 m AMSL while the threshold of runway 23 was slightly lower at 214 m AMSL, resulting in a 2 m downward gradient from runway 05 to runway 23. Approximately 300 m from the runway 05 threshold, the elevation increased to 217.5 m AMSL, a rise of 1.5 m, before gradually declining towards the runway 23 threshold. This subtle elevation change created a minor undulation in the runway profile.
Figure 5: Wagga Wagga Airport layout
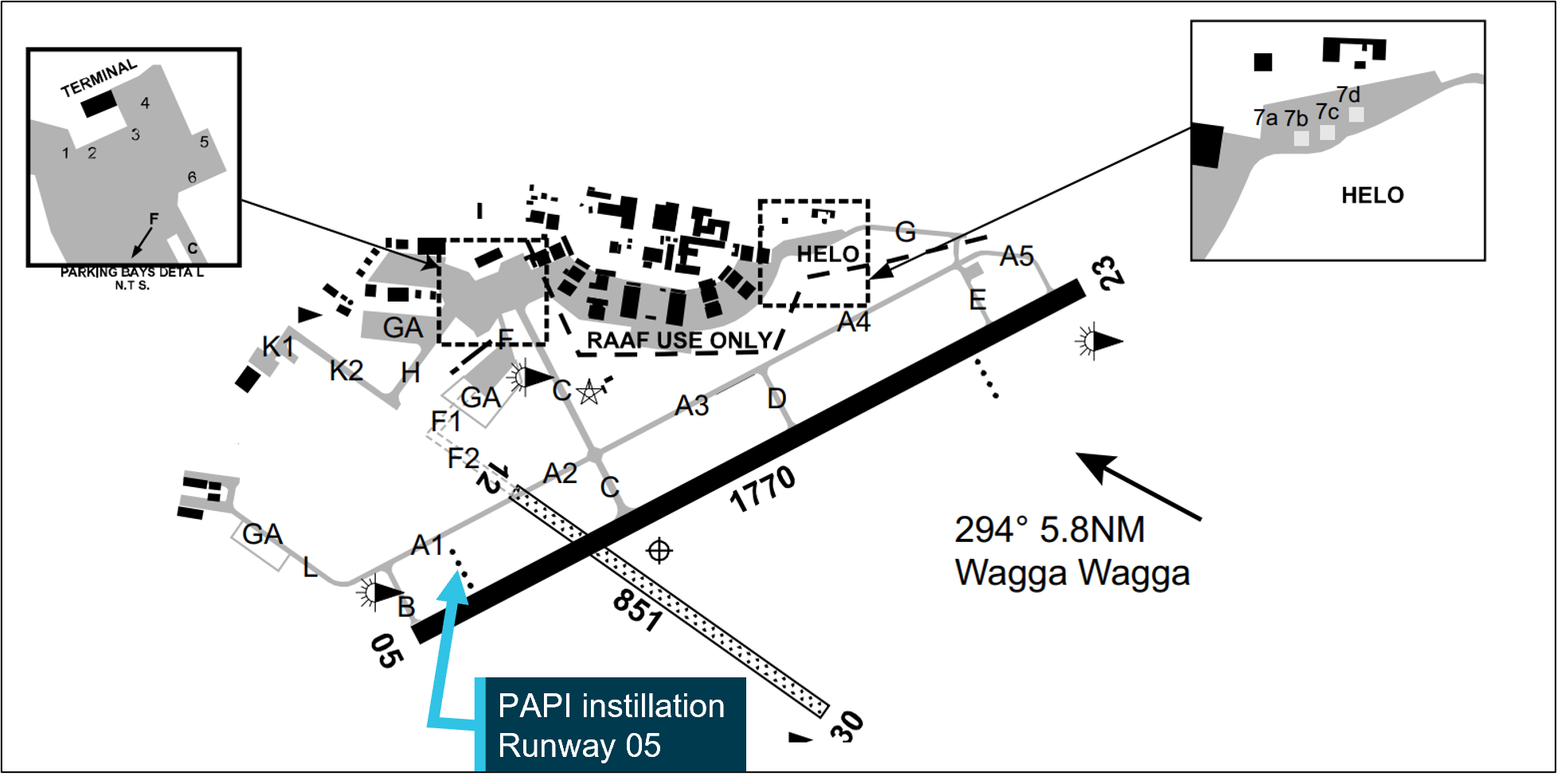
Source: En Route Supplement Australia (ERSA). Airservices Australia, annotated by the ATSB
Airspace
Wagga Wagga Airport was located within non-controlled Class G[8] airspace which was available for use by aircraft operating under visual flight rules (VFR) and instrument flight rules (IFR).
No air traffic control separation service was provided between aircraft operating in this airspace. Pilots are responsible for making themselves aware of nearby aircraft and maintaining mutual self‑separation. The primary method of traffic separation at Wagga Wagga Airport was by VHF communications coupled with visual reference, and relied on pilots using ‘alerted see-and-avoid’[9] practices (see See-and-avoid).
The Wagga Wagga CTAF operated on the VHF radio band and required pilots to monitor and make some positional broadcasts when operating within the vicinity of the aerodrome, or within 10 NM.
Reported radio dead spot
The Australian Airline Pilot Academy (AAPA) had issued an internal notice to all crew (NOTAC) on 23 August 2023, advising of a potential radio ‘deadspot’ on Wagga Wagga Airport. The NOTAC detailed:
NOTAC 032/17 CURRENT 23 08 1100 LST - Until Removed To: All Pilots
POTENTIAL RADIO DEADSPOT ON WAGGA AIRPORT
There is an identified radio dead spot on Taxiway Alpha between taxiway Charlie and the runway 23 holding point, prior to entering Runway 23, crew must visually check that no aircraft are entering the runway from taxiway Charlie.
Authority: Chief Pilot.
Prior to the occurrence, the aerodrome operator had identified that ground-based vehicle radio communications were observed to have reduced effectiveness in some circumstances, however no further testing was carried out.
Radio signal transmission reception
The ATSB conducted an analysis to determine whether the radio line of sight (LOS) between the 2 aircraft, positioned at opposite ends of the runway, was obstructed by the terrain elevation at approximately 300 m down runway 05.
Firstly, a geometric LOS analysis was conducted. The analysis utilised a strict geometric LOS model, assuming a direct, unobstructed path between the transmitter and receiver, as described in standard International Telecommunications Union (ITU-R) (2019) radio propagation principles (Parsons, 2000). The results determined that the terrain elevation created a physical obstruction, blocking the direct radio LOS between the aircraft.
To assess the potential for radio communication despite the LOS obstruction, diffraction[10] effects were evaluated. The inclusion of diffraction effects was used as radio waves, particularly in the very high frequency (VHF) band used in aviation, can propagate beyond geometric LOS by bending around obstacles such as terrain features (Rappaport, 2002). This phenomenon enables communication in scenarios where direct LOS is obstructed.
A knife-edge diffraction model was used to estimate the signal loss caused by the terrain. This model, a standard method in radio wave propagation analysis, approximates the terrain feature as a sharp, idealised edge obstructing the radio wave path (International Telecommunications Union (ITU-R), 2019). The knife-edge model was selected due to its applicability for analysing diffraction over a single, well-defined obstacle and its computational simplicity for VHF frequency analysis.
The calculations were completed using the Wagga Wagga CTAF frequency of 118.2 MHz and assumed values derived from generic radio and antenna specifications.
Results indicated that despite the geometric LOS obstruction caused by the terrain, communication between the 2 aircraft was feasible[11] due to diffraction effects.
A similar calculation was conducted between taxiway C and taxiway A5. It indicated that communication between 2 aircraft was also feasible. The calculated signal strength indicated that a radio transmission should have theoretically been received clearly.
All calculations regarding VHF line of sight communication were theoretical and assumed idealised conditions. Noting the advice by AAPA of a potential radio dead spot on the airport, it should be noted that this observed dead spot may result from real-world environmental factors such as localised interference or other unmodeled conditions like vegetation or temporary obstacles, which cannot be fully replicated in theoretical calculations.
Visibility between opposite runway thresholds
A clear line of visual (eye level) sight existed between the taxiway B holding point at the threshold of runway 05 and the threshold of runway 23 (Figure 6). The pilot of the PA-28 reported they could clearly see the Dash 8 at the threshold of runway 05, as the Saab 340 vacated the runway, prior to them commencing take-off. The crew of the Dash 8 reported being able to see the Saab 340 land and vacate the runway, but did not visually detect the PA-28 prior to entering the preferred runway. After they were notified by the Saab 340, the captain and first officer were able to visually identify the PA-28 on runway 23 which was at that stage moving towards the Dash 8 on its take-off roll.
Both the FO and the captain commented during interview of a possible obstruction to their line of sight from the PAPI[12] installation. The PAPI installation is positioned to the left of runway 05. The orientation was to the left of the Dash 8 when the aircraft was holding on taxiway B, prior to entering runway 05. PAPI units must be no more than 0.9 m above ground level.
Figure 6: View from ground level, threshold runway 05

Source: airport operator, annotated by the ATSB
It was noted that the visual range from holding point B to the threshold of runway 23 is greater than 1,700 m over undulating terrain, with the PA-28 presenting a small target for visual identification by the Dash 8 crew.
ATSB calculations indicate there was a clear line of sight between the eye height of the Dash 8 crew and the eye height of the PA-28 crew. The visual line of sight between both aircraft was about 1.7 m above the geographical terrain undulations between the thresholds of runways 05 and 23.
Human performance limitations
Object perception
There are limitations to the size of objects that are perceptible at a distance. The ATSB considered whether the crew of the Dash 8 could have been able to detect there was a small aircraft (PA-28) at the threshold of runway 23 when the Dash 8 was at taxiway B at the runway 05 end, based on the known limitations of distant object perception. It was reported by the PA-28 pilots that the Dash 8 was visible to them when they were lined up for take-off once the Saab 340 cleared the runway. However, the Dash 8 is a larger aircraft and was side-on to the PA-28 pilots at this point, and they were alerted to the Dash 8’s presence through broadcasts, however this does not mean that the Dash 8 crew could identify the PA‑28.
The 3 main factors that would affect the visual image size of the PA-28 aircraft in the Dash 8 pilot’s eye are:
- the dimensions of the aircraft
- its relative orientation
- distance from the viewer.
Past research (Hobbs, 2004) has shown distant objects can be seen when their visual angle is at least 24−36 minutes of arc (0.4−0.6°), and down to a minimum of 12 minutes of arc (0.2°) in ideal viewing conditions (ATSB, 2025).
Once the Saab 340 had cleared the runway and the visual path to the PA-28 was clear for the Dash 8 crew, the PA-28 was lined up for take-off. When lined up on the runway, the most prominent part of the PA-28 was the fuselage, which was 1.65 m high, with a wingspan of 10.79 m (noting that the wings would be edge-on). At the distance of 1,700 m, this would have presented a visual image that was about 3 minutes of arc (0.06°).[13] Additionally, as the PA-28 was moving down the runway, the gradual change in angular size would likely have been virtually imperceptible due to the eye’s limited sensitivity to small angular variations. Therefore, in the absence of confounding factors, it would have been very unlikely that the PA-28 would have been detectable by the Dash 8 pilots at that distance.
Other factors can also exist that can affect whether a pilot will be able to see another aircraft, including the background that an object is seen against. As can be seen in Figure 6, the background behind the runway 23 threshold was dark and would have provided good contrast to the white PA-28 aircraft, making detection easier.
Finally, the use of lights by the PA-28 would have enhanced detection. Strobe lights would have enhanced detection though flash and movement. However, landing lights are angled forward and downwards, and may not have been as detectable by the Dash 8 crew.
See-and-avoid
At and around non-controlled aerodromes, pilots are responsible for making themselves aware of nearby aircraft and maintaining separation. Safe operations at non-controlled aerodromes rely on all pilots maintaining an awareness of their surroundings and other aircraft, the principle of ‘see‑and‑avoid’.
A visual traffic search in the absence of specific traffic information is less likely to be successful than a search where traffic information has been provided. Knowing where to look can greatly increase the chance of sighting the traffic.
An ‘unalerted’ search is one where reliance is entirely on the pilot searching for, and sighting, another aircraft without prior knowledge of its presence. An ‘alerted’ search is one where the pilot is alerted to another aircraft’s presence, typically through radio communications or aircraft-based alerting systems. An alerted search supports a pilot’s situational awareness and enhances their visual lookout for traffic by developing an expectation of visually acquiring the traffic in a particular area.
Issues associated with unalerted see-and-avoid have been detailed in the ATSB research report, Limitations of the See-and-Avoid Principles(Hobbs, 2004). The report highlights that unalerted see-and-avoid relies entirely on the pilot’s ability to sight other aircraft.
Tools to enable ‘alerted see-and-avoid’ include:
- VHF radio
- transponders, used by traffic collision avoidance system (TCAS)
- automatic dependent surveillance broadcast (ADS-B)
- electronic flight bag (EFB) applications
Hobbs (2004) identified that an alerted search is likely to be 8 times more effective than an unalerted search, this highlighted that knowing where to look greatly increases the chances of sighting other traffic.
Alerted see-and-avoid relies on pilot or crew awareness of all traffic in their vicinity, especially those that may be considered a hazard to their operations. Enhanced situational awareness requires the pilot or crew mental model of the location and intentions of nearby traffic to be updated regularly to form an evolving understanding of the nearby traffic. Without this information, the likelihood of effective situational awareness is degraded, and the mental model and shared understanding of hazards is compromised.
Operational procedures
QantasLink Dash 8 procedures
Non-controlled aerodrome VHF radio procedure
The QantasLink Dash 8 standard operating procedure for departure from a non‑controlled aerodrome (such as Wagga Wagga Airport), at the time of the occurrence, required VHF COM 1 to be set to the area frequency and VHF COM 2 to be set to the CTAF, as passenger boarding commenced.
Prior to releasing the handbrake to taxi, a call was to be made to the relevant air traffic centre on VHF COM 1 and then followed by a taxi call to the CTAF on VHF COM 2. However, due to this being a repositioning flight, the crew only broadcast on VHF COM 2 on the CTAF frequency.
Controlled aerodrome VHF radio procedure
The QantasLink Dash 8 standard operating procedure for departure from a controlled aerodrome, at the time of the occurrence, required VHF COM 1 to be set to the primary air traffic control frequency for ground and air-based communications. The VHF COM 2 was set for other communications (such as ATIS,[14] AWIS,[15] PAL and CTAF).
Reverse thrust on the ground
QantasLink policy for engaging reverse thrust during ground operations required prior approval from the Head of Flight Operations. This approval requirement was due to the risks associated with not being able to confirm clearance from other traffic or obstacles that cannot be visually identified from the flight deck. The captain advised during interview that they were aware of this policy.
Procedures for transponder use
The QantasLink procedure was to set the transponder to ‘ON/ALT’ with the applicable transponder code[16] as part of the pre-flight process. This is achieved either after obtaining airways clearance or (at airports where airways clearance is not obtained until after take-off), as part of the pre‑flight process before engine start.
AAPA PA-28 operator procedures
VHF radio procedure
The AAPA procedures, contained within the ‘Piper Warrior III Crew Operating Manual’, normal procedures, required COM 1 to be selected to the local area frequency, tower, ground, clearance delivery, approach or departure frequency as required. COM 2 was required to be set to the CTAF, ATIS, AWIS, MULTICOM or guard frequency (121.5 MHz) as required.
The instructor confirmed during interview that, at the time of the occurrence, COM 1 was set to Melbourne Centre (area frequency) and COM 2 was set to the Wagga Wagga CTAF.
Procedures for transponder use
The PA-28 operator’s’ procedure for transponder operation was to set the applicable transponder code and select the STBY[17] function during taxi. Prior to entering the runway, ON/ALT mode[18] was to be selected.
The PA-28 operator’s training manual notes:
All pilots must ensure ALT is selected on the transponder during the LINE UP CHECKLIST. Other aircraft equipped with TCAS rely on transponder information for pilot alerting and collision avoidance functions.
PA-28 external light use
The PA-28 operator’s procedure for the selection of external lights is documented in its Piper Warrior III flight crew operating manual, normal procedures.
As required by the ‘pre line up scan action flow’, the pilot selects the landing lights ‘on’ (during daytime operations), immediately prior to commencing a take-off roll at a non‑controlled aerodrome.
The instructor recalled that normal behaviour would involve the pilot selecting the landing lights ‘on’, when the ‘rolling call was issued’.
Regulations regarding transponder use
The use of surveillance equipment such as ADS-B and transponder is outlined in the Civil Aviation Safety Regulations Part 91 Manual of Standards (MOS) and the Airservices Australia Aeronautical Information Publication (AIP).
Chapter 26 of the Part 91 MOS, operation of surveillance equipment – general requirements stated, among other things, that transponder equipment required to be fitted and carried on an aircraft must be continuously operated. It also identified that ‘continuous operation’ for a transponder means that the equipment must be operated in a mode that enables a secondary surveillance radar (SSR)[19] response to be transmitted and, where an altitude reporting capability is available, that this capability is also activated.
AIP Australia ENR 1.6 paragraph 7.1.9 stated:
A pilot operating a Mode S transponder must:
b. On receipt of ATC clearance, or requesting the earlier of Push Back or Taxi, select TA/RA/XPDR/ ON AUTO as applicable.
CASA advised that item ‘b’ only applies at controlled aerodromes. At non-controlled aerodromes, transponders must be turned on prior to becoming airborne.
Radio communication
VHF radio is the primary communication tool commonly used to provide ‘alerted see‑and‑avoid’ from sport and recreational private flying to air transport. Broadcasts on the CTAF to any other traffic in the vicinity of a non-controlled aerodrome are made to provide situational awareness, traffic separation and deconfliction to other traffic in the vicinity.
Positional broadcasts
Civil Aviation Safety Regulation 91.630 made certain radio calls mandatory for aircraft that are fitted with or carry a VHF radio. Chapter 21 of the Part 91 Manual of Standards (MOS) prescribed one type of mandatory broadcast that applies at all non-controlled aerodromes, namely:
When the pilot in command considers it reasonably necessary to broadcast to avoid the risk of a collision with another aircraft.
To aid in increasing situational awareness at non-controlled aerodromes, recommended broadcasts are published by the Civil Aviation Safety Authority (CASA). These broadcasts enable pilots to alert other traffic to their location and intentions before take‑off, inbound to land at, or if intending to overfly a non-controlled aerodrome.
Standardised radio transmissions and phraseology assist with effective and efficient radio communication. To achieve this, the application of recommended positional broadcasts (Table 1) for VFR traffic are published in CASA Advisory Circular (AC) 91-10, Operations in the vicinity of non-controlled aerodromes.
Table 1: Recommended positional broadcasts in the vicinity of a non-controlled aerodrome
| Item | Situation | Broadcast |
| Recommended calls in all circumstances | ||
| 1 | The pilot intends to take off. | Immediately before, or during taxi. |
| 2 | The pilot is inbound to the aerodrome. | 10 NM from the aerodrome, or earlier, commensurate with aeroplane performance and pilot workload, with an estimated time of arrival (ETA) for aerodrome. |
| 3 | The pilot intends to fly through the vicinity of, but not land at, a non-controlled aerodrome. | 10 NM from the aerodrome, or earlier, commensurate with aeroplane performance and pilot workload, and an estimated time of arrival. |
| Recommended calls dependent on traffic | ||
| 4 | The pilot intends to enter the runway. | Immediately before entering a runway. |
| 5 | The pilot is ready to join the circuit. | Immediately before joining the circuit. |
| 6 | The pilot intends to make a straight in approach. | On final approach at not less than 3 NM from threshold. |
| 7 | The pilot intends to join on base leg. | Prior to joining base leg. |
| 8 | During an instrument approach when: a. departing FAF or established on final approach segment inbound b. terminating the approach, commencing the missed approach. | Include the details of position and intentions that are clear to all pilots (both IFR and VFR). |
| 9 | The aircraft is clear of the runway(s). | Once established outside of the runway strip. |
Source: CASA AC 91-10 Operations in the vicinity of non-controlled aerodromes
Limitations of positional broadcasts
Positional broadcasts are a one-way communication and do not imply receipt of information by other parties unless direct radio contact is made between stations.
Positional broadcasts rely on the accuracy of the information being broadcast and the ability of other traffic receiving, comprehending and reacting to this information.
CASA AC 91-10 stated:
8.2.1 Pilots are reminded that although correct and informative radio calls play a critical role in ensuring collision avoidance in uncontrolled airspace, to ensure the safety of their aircraft they cannot assume that an absence of other radio calls means there are no nearby or conflicting aircraft.
8.2.2 Pilots must continually look out for other aircraft, even when their broadcasts have generated no response
8.2.3 Accidents and incidents have occurred where pilots incorrectly assessed the threat posed by another aircraft, either due to the pilot incorrectly assessing the relative aircraft flight paths, or inaccurate information being provided by other pilots.
Dash 8 radio reception and transmission
Two Dash 8 ground communication events has been previously identified by ATSB investigations (AO-2023-025 and AO-2023-050) at Mildura Airport (see Related occurrences).
These 2 events resulted in the second investigation testing the Dash 8’s VHF systems. The testing was conducted by the ATSB, the Australian Media and Communications Authority[20] and QantasLink. The testing measured the transmission power pattern of the Dash 8’s 2 communication systems (upper and lower antennae), when the aircraft was on the ground at Mildura Airport.
The testing identified that ground‑based Dash 8 signal strength reception could be adversely affected by the aircraft’s orientation relative to the other aircraft or antenna locations. Additionally, the average signal strength forward of the aircraft was 8.5 dBm[21] stronger than the average signal strength behind and to the side of the aircraft. A significant recorded signal strength and clarity reduction on both VHF COM 1 and VHF COM 2 radios was observed when the tail of the Dash 8 was pointed towards the receiver.
It was further identified that reception and transmission on VHF COM 2 on the ground (via the lower antenna, as used for QantasLink Dash 8 ground communications at non‑controlled aerodromes) had significantly reduced strength and clarity compared to VHF COM 1.
The Dash 8 manufacturer, De Havilland Aircraft of Canada Limited, advised that VHF COM 1 was expected to provide more reliable performance in ground-based communication with other ground stations.
Two flight operations service letters (Appendix B – Flight Operations Service Letters) were released on 6 December 2024 for the Dash 8-100/200/300 (DH8-SL-23-008A) and Dash 8‑400 (DH8-SL-23-020A). Details included a description of the limitations of VHF line of sight communications and the recommendation that VHF COM 1 may provide a better signal (receiving and transmitting) to other stations on the ground, or nearby in the air.
As a result of the first occurrence at Mildura on 6 June 2023 (see ATSB investigation report AO-2023-025), QantasLink issued a technical advisory bulletin, effective from 17 July 2024, which changed the VHF communications procedure for Mildura departures. The aim of the change was to improve ground-to-ground CTAF VHF communication during the taxi phase. However, this has only been adopted at Mildura Airport through a route manual amendment (now company port supplement) and does not provide any effective level of mitigation to this known risk for other non-controlled aerodromes.
Related occurrences
ATSB investigation (AO-2023-025)
On 6 June 2023, a Piper PA-28-161, taxied for runway 36 at Mildura Airport, Victoria. At about the same time, a QantasLink De Havilland Aircraft of Canada Limited DHC-8-315 (Dash 8) began to taxi for runway 09. Both aircraft broadcast their intentions on the local common traffic advisory frequency. The pilot of the PA-28 was aware of the Dash 8, but the crew of the Dash 8 were not aware of the PA-28. Both aircraft commenced their take‑off at about the same time and the Dash 8 crossed ahead of the PA-28 at the runway intersection of 09/36 by about 600 m.
The pilot of the PA-28 was unable to visually sight the location of the Dash 8 due to airport buildings and assumed that the Dash 8 was still backtracking on runway 09. They did not directly contact the Dash 8 to positively organise separation. They also incorrectly referred to the runway direction at Mildura Airport as ‘runway 35’ instead of ‘runway 36’.
The Dash 8 crew was focused on obtaining their pre-departure information from air traffic control and had the volume for the radio tuned to the common traffic advisory frequency turned down. An over transmission from air traffic control meant that the Dash 8 crew only received certain elements of the PA-28 pilot’s radio calls. This likely led to an incomplete comprehension of traffic by the Dash 8 crew who believed that the PA-28 was not at Mildura (due to the incorrect reference to runway 35). However, they did not seek further information of the source of the radio calls to positively identify the traffic location.
The investigation found that, due to the topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runways 09, 27 and 36. The Dash 8 crew did not give a rolling call on runway 09, nor were they required to. The lack of a requirement for mandatory rolling calls increased the risk of aircraft not being aware of each other immediately prior to take-off.
ATSB investigation (AO-2023-050)
On 29 September 2023, De Havilland Aircraft of Canada Limited DHC-8-315 (Dash 8), taxied for runway 09 at Mildura, Victoria. A short time later, an amateur‑built Lancair Super ES aircraft taxied for runway 36 at Mildura, for a private flight to Ballarat.
Both aircraft gave taxi, entering and backtracking calls on the local common traffic advisory frequency. Neither the pilot of the Lancair, nor the crew of the Dash 8, were aware of each other. The crew of the Dash 8 gave a rolling call and had commenced their take-off on runway 09 as the pilot of the Lancair gave a rolling call on runway 36, this was received by the Dash 8 crew with an immediate response given to the Lancair to hold on the runway. Another aircraft, taxiing behind the Lancair for runway 36, advised them to hold position while the Dash 8 departed.
The Dash 8 crossed the runway 09/36 intersection while the Lancair remained on the threshold of runway 36.
The investigation found that, due to the topography and buildings at Mildura Airport, aircraft are not directly visible to each other on the threshold of runways 09, 27 and 36. It was also identified that the crew of the Dash 8 were actively engaged in in organising separation with other airborne traffic and the Lancair’s entering and backtracking call was over transmitted.
It was also identified that the Dash 8 had reduced ground-based radio reception and transmission strength and clarity on VHF COM 2 (which used an antenna on the aircraft underbelly) and was required to be used by company procedures. The investigation also found that the Dash 8 had reduced radio reception and transmission strength to and from other airfield users located behind the Dash 8 which affected radio call readability.
This led to a situation where the crew of the Dash 8 had an incomplete comprehension of the ground-based traffic at Mildura, and had no knowledge of the Lancair until during the take-off. In addition, due to the position and distance of the Dash 8, the pilot of the Lancair had no awareness of the Dash 8 until another aircraft advised that the Dash 8 was rolling on runway 09.
ATSB investigation (AO-2024-009)
On 19 March 2024, a Fairchild SA226-TC (Metroliner), taxied at Geraldton, Western Australia, for runway 03. About one minute later, a Beechcraft A36 (Bonanza), taxied for runway 14. After reaching their respective runway thresholds, both pilots attempted to contact the other, however, they did not hear each other, nor could they see each other. A third aircraft assisted by relaying information. Based on the information received, the Bonanza and Metroliner pilots commenced their take-off within 3 seconds of each other. The Metroliner crossed runway 14 about 400 m in front of the Bonanza, with a vertical separation of about 250–300 ft.
The investigation found that, when aircraft were positioned at the thresholds of runway 03 and 14 (and 08), they will unlikely be visible to each other due to the position of the airport buildings. Further, they may not be contactable on VHF radio due to potential shielding effects. This resulted in the pilots being unable to verify each other’s position and intentions prior to commencing their take-off.
While the pilot of the third aircraft was attempting to assist, the details provided were inaccurate and incomplete. This inadvertently resulted in misinterpretation by the Bonanza and Metroliner pilots and influenced their decision to take off.
Safety analysis
Introduction
On 15 July 2024, a QantasLink De Havilland Aircraft of Canada Limited DHC-8-402, registered VH-QOD, entered runway 05 at Wagga Wagga Airport, unaware that a Piper PA-28, registered VH-XDK, was commencing its take-off roll from runway 23.
While the crew of the Dash 8 was entering the runway, the crew of a third aircraft (Saab 340), notified the Dash 8 crew of the PA-28’s presence.
Once the Dash 8 crew was aware of the PA-28, the captain stopped the aircraft about 5 m past the holding point, then engaged ‘reverse thrust’ to back the Dash 8 clear of the runway. Concurrently, the pilot of the PA-28 rejected their take-off from runway 23.
This analysis will explore operational considerations such as situational awareness, the breakdown of communication, shared mental model and alerted see‑and‑avoid, as well as the limitations identified within operational procedures and specific aircraft system limitations.
Situational awareness and communication
The PA-28 crew was aware of the Dash 8 intentions and location. The PA-28 instructor subsequently held the assumption that the Dash 8 crew had, likewise, received their radio broadcasts and were aware of the PA-28’s location and intentions for take-off.
The Dash 8 crew did not expect any other traffic, in addition to the Saab 340. The Dash 8 crew reported not identifying the PA-28 either visually or via electronic means, nor hearing the PA-28’s radio communications. During taxi to the opposite end of the runway, the Dash 8 was pointing in the opposite direction to the PA-28, and later the line of sight to the PA-28 would have been obscured by the landing Saab 340. As the PA-28 transponder was not turned on prior to entering the runway, it was not identifiable electronically either prior to this time. The remaining opportunity to increase situational awareness was the initial taxiing radio calls. The Dash 8 crew’s broadcast immediately after they were told about the conflicting traffic shows they were surprised to learn there was another aircraft operating from the airport, this suggests that the Dash 8 crew members did not hear these transmissions rather than forgot them.
Contributing factor During ground-based repositioning, the Dash 8 entered runway 05 while the PA-28 had commenced its take-off roll from runway 23. The Dash 8 crew were not aware of the PA-28 until notified by the crew of a third aircraft of the potential conflict. |
Communication
Succinct and timely radio communication is important to ensure high levels of situational awareness and aids in providing alerted see-and-avoid safety outcomes. As such, the accuracy of the information broadcast by pilots is critical in ensuring minimum misunderstanding.
Common traffic advisory frequency (CTAF) recordings indicated that the PA-28 pilot made the recommended positional broadcasts in preparation for their departure – a taxi call when leaving the apron area, entering the runway and then a rolling call on the runway. However, positional broadcasts are ‘one-way’ communications by nature and do not explicitly mean that other traffic in the vicinity interpret and understand the intended information.
The PA-28 instructor reported that they believed that the Dash 8 crew had received and understood their broadcasts. This misunderstanding was based on the presumption that because the PA-28 could hear the radio calls and see the Dash 8, that the Dash 8 crew also could hear the radio calls and see the PA-28.
The PA-28 crew could hear the communications between the Dash 8 and Saab 340, centring on the Dash 8 crew ensuring they did not impede the Saab 340’s landing. However, the PA-28 instructor expected that the Dash 8 would hold short of the runway to allow them to take-off without hearing any broadcasts to that effect. As a result, the PA-28 crew did not initiate any direct radio contact with the Dash 8 crew to clarify their intentions.
Had the PA-28 instructor attempted to make direct contact with the Dash 8, and not been successful, they would have subsequently realised there had been a communication breakdown.
Contributing factor The pilots of the PA-28 gave the recommended radio calls, however, did not directly communicate or engage with the Dash 8 crew to arrange separation. |
Visual identification
The topography at the aerodrome results in a runway height change between the thresholds of runway 05/23 at Wagga Wagga Airport. This change is up to 2 m in elevation between the thresholds, with a slight hump towards the runway 05 end. However, there was a clear visual line of sight from one threshold to the other.
When the Dash 8 was on taxiway B at the holding point of the runway, the crew’s vision of the PA-28 may have been blocked by the landing Saab 340. By the time that aircraft cleared the runway, the PA-28 was lined up on the runway and had started its take-off roll.
Based on the limitations of vision, it is very unlikely that the Dash 8 crew would have been able to detect the presence of the PA-28 about 1,700 m away, simply by looking in that direction, as the image of that aircraft would have been too small for detection. The use of landing and strobe lights would have assisted, but over that distance would have been limited. Consequently, the Dash 8 crew, who reported looking before entering the runway, did not detect its presence.
If the Dash 8 crew had previously been alerted to the presence of another aircraft, this would have increased the chance of detection. Alerted see‑and‑avoid means that the presence and approximate location of another aircraft is known or expected, allowing the crew to narrow their visual search. However, in this case, the absence of the Dash 8 crew detecting radio calls from the PA-28 and no other aircraft identified during taxi either visually or electronically, meant that the Dash 8 crew held an expectation that there were no other ground-based aircraft operating at the airport at that time. Not detecting the PA‑28 was consistent with that expectation.
Contributing factor Without any prior alert or expectation of the presence of the PA-28, the Dash 8 crew did not visually detect the PA-28 on take-off from the reciprocal end of the runway, prior to the Dash 8 entering the runway to taxi to the terminal. |
The ATSB identified that while the PA-28 crew conducted their taxi, engine run-ups and aircraft checks, their transponder was set to standby. Prior to entering the runway for take-off, the pilot of the PA-28 then switched the transponder from standby to ‘ON’.
The Dash 8 crew reported that electronic surveillance equipment was used as an aid to supplement the identification of potential conflicting traffic in the vicinity of a non‑controlled aerodrome prior to take-off. Both the captain and first officer of the Dash 8 recalled conducting a check of their onboard surveillance systems (electronic flight bag, traffic collision avoidance system (TCAS) aircraft display and Flightradar24 application) during taxi and did not identify any traffic other than the third-party landing aircraft.
Non-active mode S transponders do not provide electronic surveillance information to other aircraft. If the transponder is not selected ‘on’, a missed opportunity exists to provide situational awareness to other aircraft.
It is likely, had the PA-28 mode S transponder been activated at the first aircraft movement for taxi, the flight crew of the Dash 8 would have detected the presence of the PA-28 and developed an expectation of its location and potential confliction. This would have prompted the crew to coordinate both verbally and aided alerted see‑and‑avoid.
Contributing factor During taxi for take-off, the PA-28 was not broadcasting transponder information to identify them to other traffic in the vicinity of the aerodrome. |
Australian Airline Pilot Academy procedures for transponder
The AAPA’s manual had a procedure that prescribed the use of the transponder on standby during startup and taxi, with a requirement to only switch it to ‘ALT’ prior to entering the runway.
Widespread use of surveillance equipment, such as transponders with ADS-B installed, offer significant improvement to allow pilots to be more certain of the location of traffic, particularly outside controlled airspace environments.
Had the PA-28 crew been required to select their mode S transponder to ‘ON/ALT’ prior to initial taxi, this would have made them electronically visible to the Dash 8 crew who reported actively seeking this information.
Contributing factor The Australian Airline Pilot Academy flying school flight crew operating manual only required pilots to activate the transponder prior to entering the runway. The use of a transponder during taxi would normally provide an additional source of positional data to other pilots, aiding visual identification and alerted 'see‑and‑avoid' to other aircraft. (Safety issue) |
Topographic shielding
Local operators at Wagga Wagga Airport have observed and reported that a reduction in effectiveness of VHF communications had been experienced at certain locations on the airport. This observation of topographical radio shielding was identified by multiple parties.
Topographic changes exist in and around Wagga Wagga Airport and were suggested by stakeholders to result in varying levels of topographical radio shielding at the eastern end of taxiway A and the end of runway 23.
Prior to the occurrence, the PA-28 operator issued internal notifications of an ‘identified radio dead spot’, to its flight crews.
Operator advice and reported experience regarding topographical shielding at Wagga Wagga Airport was documented procedurally for AAPA, but was not available to Dash 8 crew operating into Wagga Wagga Airport. The ATSB did not independently confirm the existence of radio shielding. Operator experience and local procedure indicates this is likely an ongoing issue at Wagga Wagga Airport.
Contributing factor Reduced VHF ground-based communication was identified at the eastern end of runway 23 at Wagga Wagga Airport. Local operator reports and procedures indicate likely reduced communications on the eastern end of taxiway A to other areas on the aerodrome. |
Dash 8 radio reception and transmission
VHF radio transmissions facilitate exchanges between air traffic control, aircraft, and emergency services. These signals primarily rely on line of sight propagation, requiring an unobstructed path between the transmitting and receiving antennas. When line of sight is obstructed by terrain features, aircraft structure, or by man-made structures like buildings, VHF signals can be significantly attenuated, leading to reduced communication range, signal distortion, or complete loss of contact. However, under certain conditions, VHF signals may propagate beyond line of sight through mechanisms such as reflection and diffraction. While these phenomena can marginally extend communication range, their effectiveness is highly dependent on the environment.
Previous analysis of Dash 8 ground-based communications (AO-2023-050) identified a significant reduction in radio signal strength and readability when using the VHF COM 2 antenna for ground operations. The analysis determined that the aircraft structure and surrounding airport infrastructure at Mildura Airport impeded VHF COM 2 signal transmission and reception, limiting its effectiveness. In contrast, using the VHF COM 1 antenna provided a clearer line of sight to ground-based stations, resulting in more reliable communication.
ATSB analysis of the radio communications between the Dash 8, the Saab 340, and the PA-28 identified that the Dash 8 crew, while using VHF COM 2, could hear and respond to the Saab 340, likely due to its proximity to the aircraft. However, they could not hear the PA-28.
Their inability to hear the PA-28 was likely due to previously identified issues with the VHF COM 2 antenna and the addition of runway undulations which further obstructed the line of sight between the Dash 8’s VHF COM 2 antenna and the PA-28. This likely exacerbated the antenna’s limitations and hindered effective signal propagation.
Contributing factor Dash 8 ground-based transmissions on VHF COM 2 had reduced strength and clarity. This likely led to situations where other aircraft had difficulty in receiving and understanding radio transmissions, and the Dash 8 not receiving the PA-28 radio transmissions. |
Qantas procedures for VHF
QantasLink procedures required the use of VHF COM 2 for ground-based communication at non-controlled aerodromes. However, the use of VHF COM 2 for ground-based communications was not required for controlled airspace, where ground‑based communications were conducted by VHF COM 1.
In previous ground-based signal strength testing at Mildura Airport (see ATSB investigation report AO-2023-050), the ATSB identified a significant reduction in the Dash 8 VHF radio transmission strength and readability particularly when greater transmission and reception distances were involved. It was also found that the use of VHF COM 2 reduced ground-based transmission reception strength and clarity in comparison with VHF COM 1.
Following a near collision occurrence at Mildura on 6 June 2023, QantasLink changed the VHF communications procedure for Mildura Airport departures. The changed procedure required use of the VHF COM 1 system, noting that this was found to have an improvement in both transmission clarity and reception. However, this has only been adopted at Mildura Airport and so does not provide any effective level of mitigation to this known risk for other non-controlled aerodromes.
Given the reported radio dead spot at Wagga Wagga Airport, the use of VHF COM 2 with the bottom‑mounted antenna by QantasLink Dash 8s likely increased the likelihood of Dash 8 crews not receiving strong and readable radio calls from other ground-based aerodrome users.
Contributing factor QantasLink's radio procedure required crew to use communications panel radio 2 (COM 2) to broadcast and receive on local frequencies during operations at a non-controlled aerodrome. This reduced the likelihood of the Dash 8 receiving the calls from other aircraft at either end of runway 05/23 at Wagga Wagga Airport in certain circumstances. (Safety issue) |
Part of the shared mental model for all operations at non-controlled aerodromes is the situational awareness of all crew, in this instance the crew of the Saab 340 identified a potential threat to the safety of the other 2 aircraft and clearly broadcasted their concern.
Crew interviews as well as CTAF recordings clearly showed that the proactive initiative of the Saab 340 crew to alert the Dash 8 crew of the presence of the PA-28 was instrumental in preventing a potential on runway collision.
Other finding Third party intervention by the Saab 340 crew prevented the Dash 8 from lining up on runway 05 whilst the PA-28 was engaged in the take-off roll. |
After entering the preferred runway, the captain became aware of the hazard present due to the vacating third party aircraft report. The captain’s decision to apply brakes and then engage reverse thrust to clear the runway was almost certainly made to avoid the greatest perceived threat, that being, a possible collision on the runway.
Reversing the aircraft under its own power is a non-normal manoeuvre with additional risks. As such QantasLink policy would normally require Head of Flight Operations approval to conduct the manoeuvre.
The captain’s decision to reverse the aircraft could be attributed to the lower (perceived) risk involved with reversing the aircraft, versus the known risk of a possible collision.
The captain exercised their command authority, based on the information available, to make an assessment of the greatest threat, subsequently deciding to reverse the aircraft, without being able to positively confirm traffic and obstacle avoidance.
Risk management focuses on reducing the potential risks associated with a decision. Thus, considering that decision‑making, when elements of uncertainty exist, focuses on making the best decision given the available information.
The pilot in command of an aircraft has the final authority over the safety of the aircraft and its occupants. When operating in dynamic environments, the pilot in command will need to consider possible outcomes and alternative courses of action to ensure clear risk-based decisions are made. In this instance the captain elected to reduce the likelihood of a catastrophic event by reversing clear of the preferred runway after having a reasonable expectation that the taxiway was clear behind the Dash 8.
Other finding On assessing that a collision risk existed with the rolling PA-28, the captain held a reasonable expectation that it was clear and reversed the aircraft away from the preferred runway without being able to confirm that no other aircraft were behind the Dash 8. |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the runway incursion involving De Havilland Aircraft of Canada Limited DHC-8, VH-QOD, and Piper PA‑28, VH-XDK, at Wagga Wagga Airport, New South Wales, on 15 July 2024.
Contributing factors
- During ground-based repositioning, the Dash 8 entered runway 05 while the PA-28 had commenced its take-off roll from runway 23. The Dash 8 crew were not aware of the PA‑28 until notified by the crew of a third aircraft of the potential conflict.
- The pilots of the PA-28 gave the recommended radio calls, however, did not directly communicate or engage with Dash 8 crew to arrange separation.
- Without any prior alert or expectation of the presence of the PA-28, the Dash 8 crew did not visually detect the PA-28 on take-off from the reciprocal end of the runway, prior to the Dash 8 entering the runway to taxi to the terminal.
- During taxi for take-off, the PA-28 was not broadcasting transponder information to identify them to other traffic in the vicinity of the aerodrome.
- The Australian Airline Pilot Academy flying school flight crew operating manual only required pilots to activate the transponder prior to entering the runway. The use of a transponder during taxi would normally provide an additional source of positional data to other pilots, aiding visual identification and alerted 'see‑and‑avoid' to other aircraft. (Safety issue)
- Reduced VHF ground-based communication was identified at the eastern end of runway 23 at Wagga Wagga Airport. Local operator reports and procedures indicate likely reduced communications on the eastern end of taxiway A to other areas on the aerodrome.
- Dash 8 ground-based transmissions on VHF COM 2 had reduced strength and clarity. This likely led to situations where other aircraft had difficulty in receiving and understanding radio transmissions, and the Dash 8 not receiving the PA-28 radio transmissions.
- QantasLink's radio procedure required crew to use communications panel radio 2 (COM 2) to broadcast and receive on local frequencies during operations at a non-controlled aerodrome. This reduced the likelihood of the Dash 8 receiving the calls from other aircraft at either end of runway 05/23 at Wagga Wagga Airport in certain circumstances. (Safety issue)
Other (key) findings
- Third party intervention by the Saab 340 crew prevented the Dash 8 from lining up on runway 05 whilst the PA-28 was engaged in the take-off roll.
- On assessing that a collision risk existed with the rolling PA-28, the captain held a reasonable expectation that it was clear and reversed the aircraft away from the preferred runway without being able to confirm that no other aircraft were behind the Dash 8.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
AAPA procedures for transponder usage
Safety issue number: AO-2024-041-SI-01
Safety issue description: The Australian Airline Pilot Academy flying school flight crew operation manual only required pilots to select ALT on the transponder, as part of the Pre Line Up Scan Action Flow and associated Checklist prior to entering the runway. The use of a transponder during taxi would normally provide an additional source of positional data to other pilots, aiding visual identification and alerted 'see‑and‑avoid' to other aircraft.
Safety advisory notice to pilots and operators of mode S transponder equipped aircraft
SAN number: AO-2024-041-SAN-01
The effective use of the mode S transponder from first movement of the aircraft can serve as an effective tool in adding another layer of collision avoidance between aircraft on the ground. Utilising the mode S transponder with ADS-B OUT enabled is the most effective way of making an aircraft electronically conspicuous and delivering maximum interoperability with other aircraft as well as the ground ATM environment. The ATSB advises pilots and operators to review their procedures to ensure that mode S transponders are on from first movement of the aircraft, particularly at non-controlled aerodromes.
QantasLink radio procedure
Safety issue number: AO-2024-041-SI-02
Safety issue description: QantasLink's radio procedure required crew to use communications panel radio 2 (COM 2) to broadcast and receive on local frequencies during operations at a non‑controlled aerodrome. This reduced the likelihood of the Dash 8 receiving the calls from other aircraft at either end of runway 05/23 at Wagga Wagga in certain circumstances.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence. |
Safety action by Wagga Wagga Airport
After the occurrence, the aerodrome operator identified that it was possible that a radio black spot may be present based on observations of radio reception just beyond the threshold of runway 23.
Wagga Wagga city council has issued a precautionary NOTAM after the occurrence which provides advice to all operators of possible visibility issues with aircraft on the threshold of runway 23 and the possibility of radio black spots existing under some conditions. The NOTAM note reads:
LIGHT ACFT AT THR OF RWY 23 NOT VISIBLE TO OTHER ACFT USING RWY 05.
RADIO BLACK SPOTS MAY RESULT UNDER SOME CONDITIONS.
Safety action by QantasLink
On 2 August 2024 QantasLink safety issued a company safety alert notice advising crew of a suspected VHF radio blackspot on taxiway A4 and A5 towards the threshold of runway 23 and other areas of the Wagga Wagga aerodrome. They issued the following advice to crew:
Whilst we investigate the issue with the aerodrome operator and other aerodrome users, we encourage crew to consider the following precautions when taxiing for departure or any other manoeuvring on the ground:
- ensure any weak, garbled or carrier-wave only CTAF transmissions are clarified to ensure your separation plan remains valid; -
- stop at runway holding points and visually check for traffic prior to runway entry; -
- where possible all aircraft to use the into wind (duty) runway for departure so aircraft are not departing from opposite ends of the runway; and –
- ensure AFRU responses on the CTAF frequency are heard clearly.
Safety action by Civil Aviation Safety Authority
On 9 September 2025, CASA advised that new guidance and recommendations relating to the use of radios where the antenna is mounted on the underside of the aircraft fuselage to both Advisory Circular (AC) 91-10 and AC 91-14 had been updated.
This guidance advised:
Pilots operating aircraft with similar antenna placements are reminded that ground-based transmissions, when made using a radio with a fuselage underside antenna, are likely to have an increased risk of not being reliably received by other traffic. To enhance situational awareness and collision avoidance, especially at non-controlled aerodromes where radio-alerted see‑and‑avoid is critical, pilots are strongly recommended, wherever practicable, to use radios connected to antennas in unobstructed locations, such as an aircraft upper fuselage, for ground communications
Glossary
| AAPA | Australian Airline Pilot Academy |
| ADSB | Automatic Dependent Surveillance–Broadcast |
| AIP | Aeronautical information publication |
| AMSL | Above mean sea level |
| ATC | Air traffic control |
| CASA | Civil Aviation Safety Authority |
| CPL | Commercial pilot licence |
| CTAF | Common traffic advisory frequency |
| EFB | Electronic Flight Bag |
| ERSA | En route supplement Australia |
| FO | First officer |
| IFR | Instrument flight rules |
| LOS | Line of sight |
| MOS | Manual of Standards |
| NOTAC | Notice to all crew |
| NOTAM | Notice to airmen |
| TCAS | Traffic collision avoidance system |
| VFR | Visual flight rules |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the instructor of VH-XDK
- the crew of VH-QOD
- QantasLink
- Australian Airline Pilot Academy
- Civil Aviation Safety Authority
- Wagga Wagga Airport
- Aviation Bureau de la sécurité des transports du Canada
- De Havilland Aircraft of Canada.
References
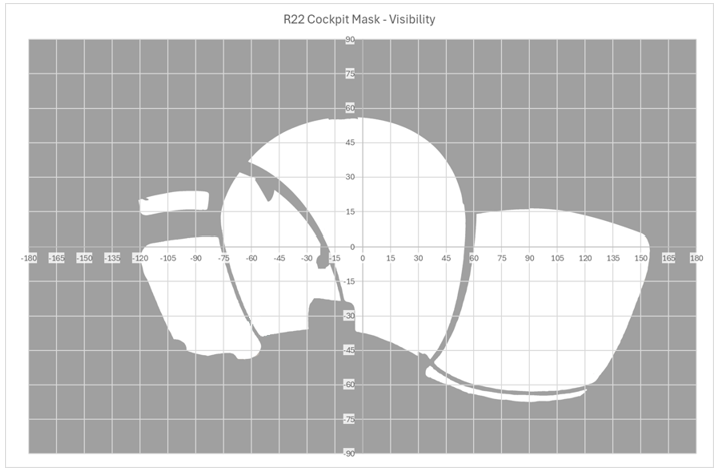
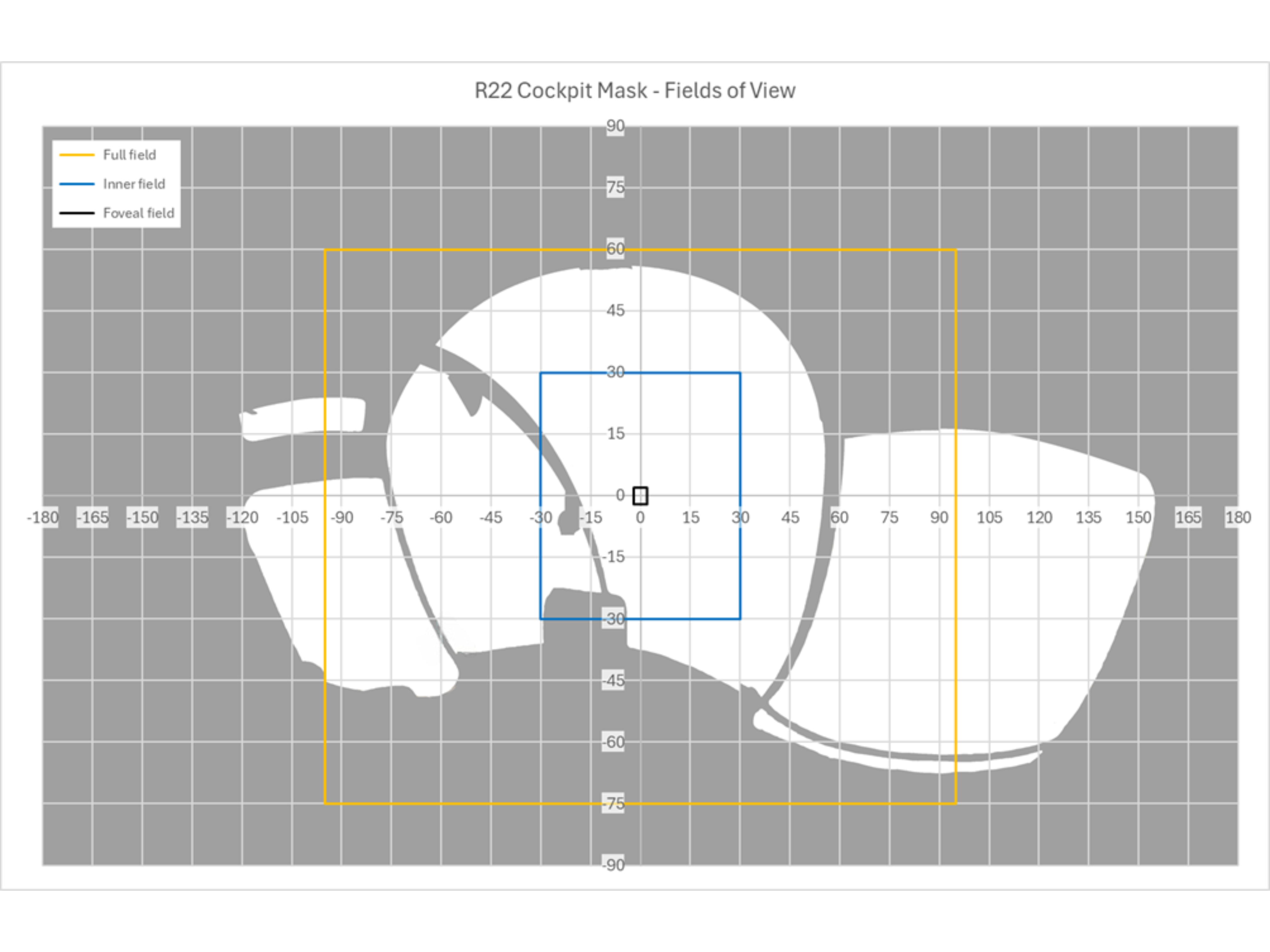
ATSB. (2025). Cockpit Visibility Study. Supporting AO-2023-001 – Midair collision involving Eurocopter EC130 B4, . Canberra: Australian Transport Safety Bureau.
Bailey, L. L., & Thompson , R. C. (2000). The effects of performance feedback on air traffic control team coordination: A simulation study. United States: Department of Tranportation. Federal Aviation Administration. Office of Aviation. Civil Aerospace Medical Institute.
Civil Aviation Safety Authority. (2013, December). PIlot's responsibility for collision avoidance in the vicinity of non-controlled aerodromes using 'see-and-avoid'. Canberra, ACT, Australia.
Civil Aviation Safety Authority. (2014). SMS 3: Safety Risk Management: SMS for Aviation, A Practical Guide. Canberra, ACT, Australia.
Federal Aviation Administration. (2011). Introduction to TCAS II Version 7.1. U.S. Department of Transportation.
Federal Aviation Administration. (2024). AC 91-120. Operational Use of Airborne Collision Avoidance Systems. U.S. Department of Transportation.
Hobbs, A. (2004). Limitations of the see-and-avoid principle. Canberra, Australia: Australian Transport Safety Bureau.
International Telecommunications Union (ITU-R). (2019). Recommendation ITU-R P.526-15: Propagation by diffraction. Geneva: ITU.
Nguyen, T., Lim, C., Nguyen, N., Gorden-Brown, L., & Nahavandi, S. (2019). A review of situation awareness assessment approaches in aviation environments. IEEE Systems Journal, 3590-3603.
Parsons, J. D. (2000). The mobile radio proagation channel (2nd ed.). Wiley.
Rappaport, T. S. (2002). Wireless Communications: Principles and Practice (2nd ed). Cambridge University Press.
Reynolds , R., & Blickensderfer, E. (2009). Crew Resource managment and shared mental models: A proposal. Journal of Aviation/Aerospace Education & Research, 15‑23.
Stanton , N., Salmon, P., Walker, G., Salas, E., & Hancock, P. (2017). State of science: situation awareness in individuals, teams and systems. . Ergonomics, 449-466.
Wickens , C., & McCarley, J. (2008). Applied attention theory. Boca Raton FL : CRC Press.
Wickens, C., Hollands , J., Banbury, S., & Parasuraman , R. (2013). Engineering psychology and human performance. Person Bostan, MA
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the Civil Aviation Safety Authority
- the Australian Airline Pilot Academy
- QantasLink
- Wagga Wagga Airport
- Aviation Bureau de la sécurité des transports du Canada
- De Havilland Aircraft of Canada Limited
- the pilot of PA-28
- the crew of Dash 8.
Submissions were received from:
- the Civil Aviation Safety Authority
- the Australian Airline Pilot Academy
- QantasLink.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – CTAF recordings
| Time stamp EST | Aircraft | Radio broadcast | ATSB assessment of readability at Wagga CTAF |
|---|---|---|---|
| 1609.25 | VH-XDK | "Wagga Traffic Warrior XDK Taxiing holding point A5 RWY 23 Wagga | 5 |
| 1609.43 | REX 6673 | “Wagga traffic, REX 6673, Saab 340, IFR, 29 DME from the north east, through 9200(ft), Turning right for Echo Echo for the RNP runway 23, for that position at 14 (time), short final 17 (time), last aircraft calling on the CTAF, just callsign? | 5 |
| 1610.05 | VH-XDK | "Yea, that was XDK" | 5 |
| 1610.10 | REX 6673 | "Ahaa, sorry one more time your readability is one at moment" | 5 |
| 1610.16 | VH-XDK | "ahhh XDK" | 5 |
| 1610.22 | REX 6673 | "Still can’t hear you will speak a little bit closer thanks" | 5 |
| 1614.12 | REX 6673 | "Wagga Traffic Rex 6673 now 10 NM final straight in runway 23 Wagga" | 5 |
| 1614.26 | Unknown | carrier wave only (3 transmissions of PTT,) followed by, AUTOMATED “Wagga Wagga Airport airfield lighting on” | 5 |
| 1616.27 | REX 6673 | "Wagga Traffic Rex 6673 now 5nm final runway 23 Wagga" | 5 |
| 1617.31 | VH-QOD | "Wagga Traffic, QOD, is a Dash 8, taxiing to the runway and then we will be coming back in for amended Bay 18 Wagga….." | 5 |
| 1617.47 | REX 6673 | "Wagga Traffic REX 6673 Saab 340 we are now Short final RWY 23 Wagga". | 5 |
| 1618.02 | VH-QOD | "Aaah REX 6673, QOD will you be exiting at Charlie, do you think?….." | 5 |
| 1618.10 | REX 6673 | "Ahh Hard to say at the moment but we will let you know in about 30sec…." | 5 |
| 1618.15 | VH-QOD | "Copy that we will just hold until you are sure thanks….." | 5 |
| 1618.32 | VH-QOD | "Rex 6673, QOD we will just start taxi enter and backtrack from the threshold of runway 05 but we will be out of your way…" | 5 |
| 1618.42 | REX.6673 | Aahh 6673 yep | 5 |
| 1619.20 | VH-XDK | "Wagga traffic, Warrior XDK lining up and holding RWY 23 wagga" | 4 |
| 1619.55 | REX 6673 | "Wagga traffic REX 6673 clear of all RWY'S Wagga" | 5 |
| 1620.07 | VH-XDK | "Wagga traffic, Warrior XDK rolling runway 23 Wagga…" | 3 |
| 1620.25 | VH-QOD | " Wagga traffic QOD is entering and taxiing for an exit on Charlie Wagga…" | 5 |
| 1620.33 | REX 6673 | "…. There is an aircraft taking off on runway 23…" | 5 |
| 1620.35 | VH-QOD | "…. Thanks…." | 5 |
| 1620.47 | VH-XDK | "Wagga traffic XDK will exit on delta and taxi for holding point A5 runway 23…." | 4 |
| 1621.01 | VH-QOD | "…. Aircraft on the 23 threshold… QOD…. nil radio transmission heard and they are still broken…." | 5 |
| 1621.11 | VH-XDK | "….QOD, XDK Yea we might have been in the radio deadspot" | 4 |
| 1621.48 | VH-QOD | " Aircraft on the RWY at Wagga, QOD, … we can see you guys exiting the RWY now, we are clear here at the 05 threshold, behind the gable markers, but we still can’t hear any of your transmission” | 5 |
| 1622.03 | VH-XDK | "…. QOD this is XDK… how do you read?" | 4 |
| 1622.03 | VH-QOD | "… XDX… yea we read you 5's now but we didn’t hear any transmission from you guys before…." | 5 |
| 1622.08 | VH-XDK | "…Might have been in the radio dead spot down at A5…" | 5 |
| 1622.18 | VH-QOD | "….Righto, no worries, we are not aware of any radio dead spot ummm,…we are clear of the gable markers here, are you taxiing back for RWY 23?" | 5 |
| 1622.28 | VH-XDK | "Affirm you can enter and continue as planned" | 4 |
| 1622.33 | VH-QOD | "Yea no worries, appreciate that guys,…. …and REXS if you are still on frequency …. Thanks for that we did not hear any radio calls" | 5 |
| 1623.51 | Other aircraft Flight Ops 249 | "And traffic Wagga,Flight Ops 249, IFR King Airis currently 30 NM north of Wagga inbound via Echo Delta for the RNP 29 estimating Echo Delta at time 28 and Wagga at time 32, Traffic Wagga …." | 5 |
| 1624.23 | VH-QOD | "Wagga Traffic QOD Clear RWY all done" | 5 |
| 1626.11 | VH-XDK | "Wagga trafficXDK Lining up and shortly rolling RWY 23 for a circuit, and will extend upwind and downwind for flight ops 249 | 4 |
| 1626.24 | Other aircraft – Flight Ops 249 | "Yea Flight Ops Thanks for that"… | 5 |
Appendix B – Flight Operations Service Letters
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The ground manoeuvre required a shorter than normal preparation timeframe than for normal operations (preparing for a revenue flight).
[2] Gable markers are used clearly define the runway strip. The runway strip means a defined area, including the runway and stopway. Aircraft required to hold short of a runway must hold at the appropriate runway holding position or the runway strip edge.
[3] Beta range plus power operations/reverse thrust, can be used for reversing the aircraft on the ground. This is achieved by adjusting the propeller pitch, to generate thrust in the opposite direction to normal operations.
[4] A traffic alert and collision avoidance system (TCAS) fulfills the International Civil Aviation Organization (ICAO) airborne collision avoidance system (ACAS) standard, and the terms are often used interchangeably.
[5] An electronic flight bag (EFB) is an electronic storage and display system. EFBs replace traditional paper products in the flight deck.
[6] The GNS 430 features a digitally‑tuned VHF COM radio. The GNS 430’s COM radio operates in the aviation voice band, from 118.000 to 136.975 MHz, in 25 kHz steps (default).
[7] Total cloud amount measured visually by the fraction (in eighths or oktas) of the sky covered by clouds.
[8] This airspace is uncontrolled. Both IFR and VFR aircraft are permitted and neither require air traffic control clearance.
[9] Improved visual acquisition by pilots alerted to traffic presence (by radio, electronic conspicuity, or other means).
[10] Diffraction, in the context of radio LOS refers to the bending of radio waves around obstacles or edges when they encounter an obstruction in their path, such as a building, hill, or other physical barrier.
[11] Real-world factors such as equipment degradation or interference could lead to deviations, potentially affecting the reliability of the predicted communication outcomes.
[12] A precision approach path indicator (PAPI) is a visual glide slope indicator that consists of 4 lights arranged perpendicular to the edge of the runway.
[13] This assumes the aircraft being observed was directly head on, which underestimates the visual surface, and the actual visible dimension may have been slightly larger.
[14] Automatic Terminal information Services (ATIS) is a continuous broadcast of recorded information, that providing pilots with current and routine data about an airport and its surrounding area, such as weather conditions and runway usage.
[15] Aerodrome Weather Information services (AWIS) broadcasts actual weather conditions using Bureau of Meteorology approved equipment.
[16] Transponder codes are 4-digit numbers transmitted by an aircraft transponder in response to a secondary surveillance radar interrogation signal to assist air traffic controllers with traffic separation.
[17] Selects the standby mode. When in standby mode, the transponder will not reply to any interrogations.
[18] In ALT mode, the transponder replies to identification and altitude interrogations.
[19] A surveillance radar system which uses transmitters/receivers (interrogators) and transponders.
[20] Australian Communications and Media Authority (ACMA) which regulates communications and media services in Australia.
[21] 1 mW = 0 dBm. The dBm scale is logarithmic (so a loss of −3 dBm is half of the signal strength (10-0.3) and −10 dBm is 10 times less than 0 dBm at 0.1 mW, similarly 0.01 mW = −20 dBm. The closer the value is to 0, the stronger the signal. e.g. −56 dBm is a better signal strength than −90 dBm.
Occurrence summary
| Investigation number | AO-2024-041 |
|---|---|
| Occurrence date | 15/07/2024 |
| Location | Wagga Wagga Airport |
| State | New South Wales |
| Report release date | 13/11/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Communications - Other, Rejected take-off, Runway incursion |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Bombardier Inc |
|---|---|
| Model | DHC-8-402 |
| Registration | VH-QOD |
| Serial number | 4123 |
| Aircraft operator | Sunstate Airlines (QLD) Pty. Limited |
| Sector | Turboprop |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Wagga Wagga Airport, New South Wales |
| Damage | Nil |
Aircraft details
| Manufacturer | Piper Aircraft Corp |
|---|---|
| Model | PA-28-161 |
| Registration | VH-XDK |
| Serial number | 2842304 |
| Aircraft operator | Australian Airline Pilot Academy Pty Ltd |
| Sector | Piston |
| Operation type | Part 141 Recreational, private and commercial pilot flight training |
| Departure point | Wagga Wagga Airport, New South Wales |
| Destination | Wagga Wagga Airport, New South Wales |
| Damage | Nil |