ATSB transport safety investigators are expected to complete their evidence collection activities in Cairns today (Wednesday).
To date they have examined the accident site and the helicopter wreckage; retrieved helicopter instrumentation for the download of recorded data at the ATSB’s Canberra facilities; interviewed the operator and witnesses; and collected CCTV footage and air traffic control surveillance information.
The ATSB conducts ‘no blame’ transport safety investigations to uncover and share safety concerns and lessons, and not for the purposes the purposes of taking administrative, regulatory or criminal action. As the flight was undertaken by a pilot who the operator has stated was not authorised to fly the helicopter, the ATSB may elect to discontinue the investigation should we determine there are unlikely to be broader safety lessons to be shared.
Based on the evidence gathered to date, the ATSB has assessed that other safety lessons may emerge from this accident.
As such, the ATSB currently plans to continue the investigation through to the publication of a preliminary report in 6-8 weeks’ time, at which point we will provide a further update on the course of the investigation. The preliminary report will detail the accident flight’s sequence of events and evidence gathered by the ATSB.
A Saab 340’s stall warning activation during the aircraft’s descent in turbulent conditions into Merimbula, NSW, highlights the importance of effectively monitoring aircraft systems and performance during the approach and landing, an ATSB final report notes.
Shortly after 1500 on 8 June 2023, the Rex Airlines-operated Saab 340 was on descent into Merimbula at the end of a scheduled passenger flight from Sydney, with 3 crewmembers and 22 passengers on board.
Icing conditions were expected during the descent, and so the first officer, who was pilot monitoring, selected the engine and wing anti-ice ON.
About 7 minutes later, the crew commenced a visual approach to Merimbula’s runway 21, and selected the flaps to 20 degrees for the landing.
During the approach, in turbulent conditions, the airspeed reduced and the aircraft’s stall warning activated, at a speed of 109 kt.
The captain then re-established the required approach flight path and speed, and continued the landing without further incident.
An ATSB investigation found prior to the stall warning activation, the captain, who was pilot flying, had reduced engine power to flight idle to avoid an inadvertent flap overspeed.
“However, when the flight crew had earlier turned on the anti-ice systems, this also activated the ice speed system, which reduced the angle of attack activation angle for a stall warning,” ATSB Director Transport Safety Stuart Macleod explained.
“Due to the autopilot mode active at the time, the reduced thrust resulted in a continuous reduction in airspeed that required pilot intervention to prevent a stall warning.”
Due possibly to distraction associated with a windscreen wiper setting, the airspeed continued to decrease undetected by the crew, until the stall warning activated, at a higher than normal margin above the stall speed due to the anti-ice systems being activated.
“The approach and landing phases can be a time of substantially increased flight crew workload,” Mr Macleod observed.
“As such, effectively monitoring aircraft and approach parameters, including performance associated with autopilot modes, and managing any distractions is essential to ensuring that an approach is safely completed.”
A Cessna 210 forced landing accident that followed a partial power loss due to the engine mixture probably not being set to full rich highlights the importance of pilots familiarising themselves with aircraft systems and the operational environment, and a well-structured take-off safety brief.
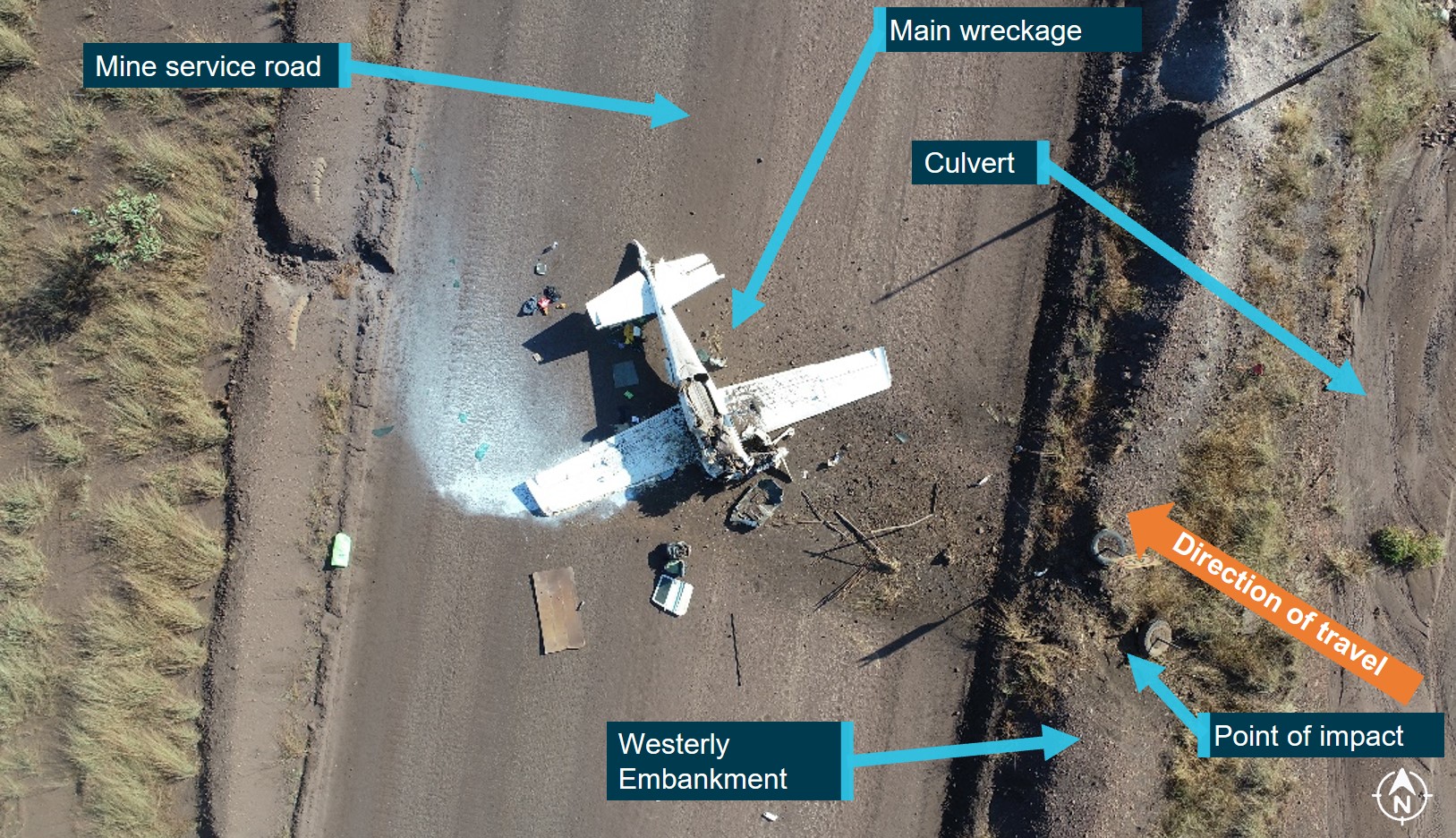
The single piston-engine Cessna 210L was being used for a charter flight from Groote Eylandt to Ngkurr, Northern Territory, on 16 June 2023 when, shortly after becoming airborne, the pilot reported the engine began to surge, and there were fuel flow fluctuations.
During the attempted turn back and landing, the aircraft passed diagonally over the runway then touched down beyond the airport boundary, in a clear grassed area.
The aircraft continued along the ground for about 120 m before hitting an embankment, flipping over, and coming to rest inverted on a mine service road.
Three passengers were seriously injured, while the other two passengers and pilot sustained minor injuries. The aircraft was substantially damaged.
An ATSB investigation concluded the reduced power and unanticipated engine behaviour was probably the result of the mixture control, which controls the ratio of fuel to air entering the engine cylinders, not being set to full rich prior to take-off. This meant that during the take-off roll when full throttle was applied, there was a disproportionately low fuel component of the air-fuel ratio, reducing engine power output, resulting in the partial power loss and unanticipated engine behaviour.
“The pilot was likely surprised by the partial power loss, which was compounded by their limited experience of flying the Cessna 210, and took no action to resolve the situation, and did not effectively manage the attempted landing,” Director Transport Safety Dr Stuart Godley said.
“Notably, the ATSB found the pilot’s take-off safety self-brief, and the aircraft operator’s documented example brief, did not detail actions to be taken in the event of a partial power loss.”
“Forward planning, such as a well-structured take-off safety brief, increases a pilot’s situation awareness, reduces mental workload under stress, and increases the prospect of a safe and well-managed outcome in the event of an emergency,” he said.
The investigation also noted that the risk of injuries to passengers in the aircraft was increased by the aircraft’s rear seats not being fitted with upper torso restraints.
“Although any effect this had on the occupants’ injuries in this accident could not be determined, the lack of upper torso restraints for rear passenger seats increases the likelihood of serious injury,” Dr Godley said.
Regulations did not require the aircraft to have upper torso restraints for the rear passenger seats, and their lack of fitment and usage in older light aircraft is highlighted by the ATSB’s SafetyWatch concern, reducing the severity of injuries in accidents involving small aircraft.
“Upper torso restraints can significantly reduce the risk of injury, compared to lap belts only, by minimising the flailing of the upper body and the potential of impacts involving the head and upper body,” Dr Godley concluded.
At about 0151 on 12 August 2024, a Robinson R44, registered VH‑ERH, collided with the top of a 7-storey hotel building in Cairns, Queensland after flying for several minutes below 500 ft around the city. The pilot was fatally injured, the helicopter was destroyed, and the building was damaged. None of the occupants of the hotel were injured. A post-impact fire developed which was contained on the roof of the hotel before being extinguished.
What the ATSB found
There were no airworthiness factors with the helicopter that likely contributed to the accident.
The flight was not authorised, and the pilot was not approved to fly the operator’s helicopters. The pilot had access to the operator’s premises at the airport as they were employed by the operator as a ground crew member.
The pilot was affected by a significant amount of alcohol before and during the flight, and further increased risk to themselves and those on the ground by conducting the unauthorised flight well below the 1,000 ft allowed for flight over a built-up area.
The ATSB concluded that, for reasons unknown, pilot actions resulted in a collision with a building while conducting an unauthorised and unnecessary flight, while affected by alcohol, late at night and at low heights over a built-up area, and without night flying endorsements.
Summary video
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At about 0151 on 12 August 2024, a Robinson R44, registered VH‑ERH, collided with the top of a 7-storey hotel building in Cairns, Queensland. The pilot was fatally injured, the helicopter was destroyed, and the building was damaged. None of the occupants of the hotel were injured. A post-impact fire developed which was contained on the roof of the hotel before being extinguished.
The operator, Nautilus Aviation, reported that the flight was not authorised, and that the pilot was not approved to fly the operator’s helicopters.
Prior to the accident, on the evening of 11 August, the pilot had been socialising with friends at various venues in Cairns. Witnesses reported and video recordings showed that the pilot had been consuming alcohol and that they returned to their apartment around 2300. Video recording from the apartment carpark showed the pilot making their way to a vehicle at 0109 on 12 August and driving away.
A video recording from a Nautilus Aviation hangar at Cairns Airport showed that at 0131 the pilot used ground wheels[1] to position one of the operator’s Robinson R44 Raven II helicopters, registered VH-ERH, onto a helipad. The pilot had access to the premises as they were employed by the operator as a ground crew member (see Pilot information).
After removing the ground wheels and storing them clear of the helipad, the pilot entered the helicopter at 0134:51 and closed the door. At 0135:47 lighting in the cockpit illuminated, and the helicopter’s strobe lights began to flash. This was likely the time that the pilot selected the helicopter’s battery switch.[2] The strobe lights continued to flash until 0137:23. At the same time the strobes stopped flashing, the lighting in the cockpit also darkened.
Lighting in the cockpit illuminated again at 0137:51, however on this occasion the strobe lights did not flash. The lighting in the cockpit darkened and illuminated 3 more times until 0144:06. The main rotor began to rotate 8 seconds later and at 0146:50 the helicopter lifted off the helipad, turned to the left and headed south towards the Cairns city centre.
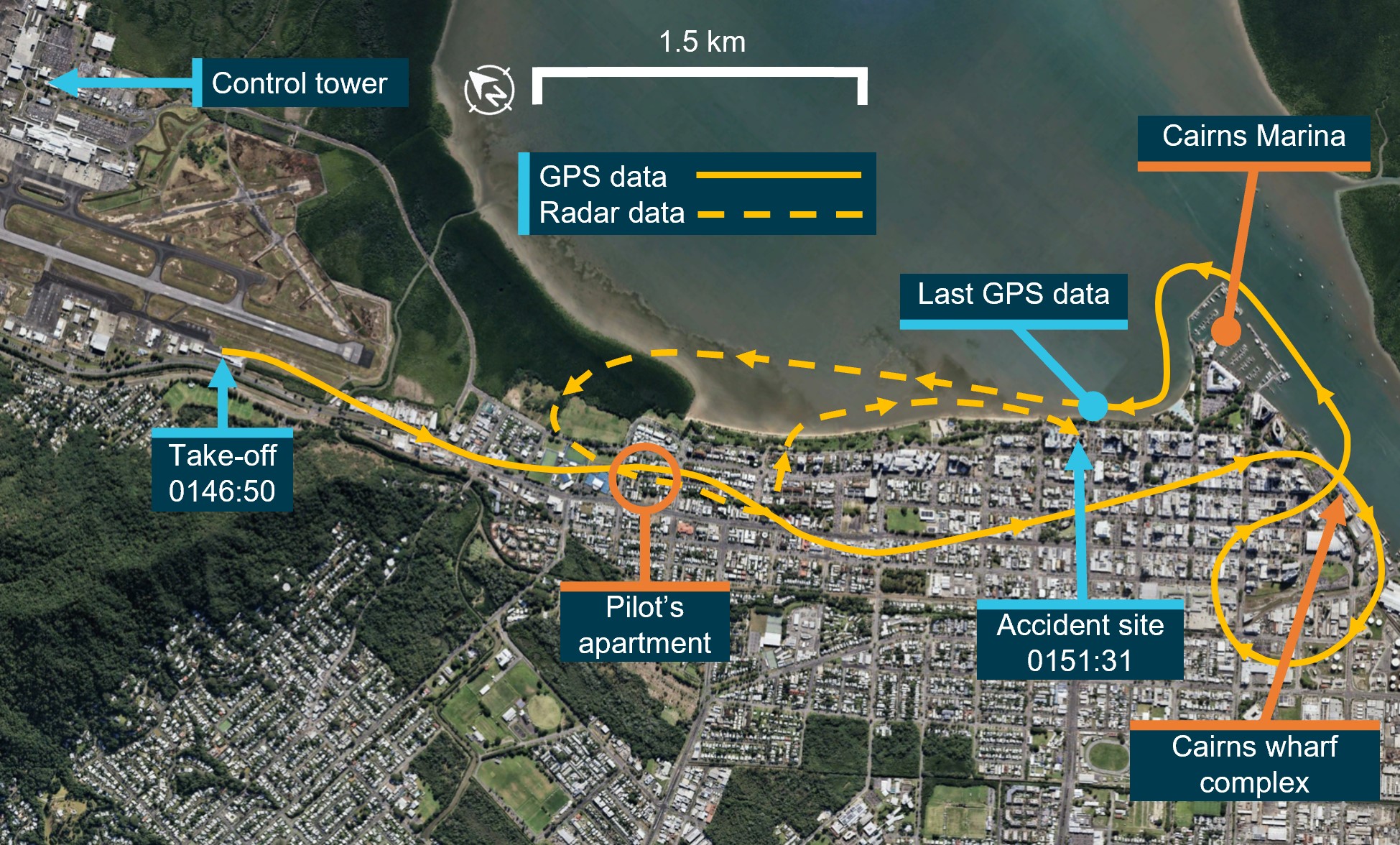
Position data (Figure 1) from an onboard global positioning system (GPS, see Recorded data) showed the helicopter tracking along a highway towards the city, before making a slight turn to a new track that corresponded with the location of the pilot’s shared apartment. The helicopter then turned to the right and tracked directly to the northern end of the Cairns wharf complex. The helicopter orbited the complex then headed north towards the Cairns marina and continued along the coastline. Recorded data from the GPS ended about 70 seconds prior to the collision.[3]
Figure 1: Flightpath of VH-ERH
Image source: Google Earth, annotated by the ATSB.
Ground-based radar data recorded by Airservices Australia (see Recorded data) showed the helicopter’s track crossing from the coastline and flying over the pilot’s apartment a second time. The helicopter circled back towards the coastline, following it for about 1 km before crossing the coastline again. The helicopter’s altitude did not exceed 500 ft throughout the flight.
Two security cameras recorded very brief portions of the final part of the flight (Figure 2). These show the helicopter pitching up, then almost immediately descending steeply before colliding into the roof of the hotel at about 0151:31.
Figure 2: VH-ERH final flightpath and collision with building
Image source: Google Earth, annotated by the ATSB.
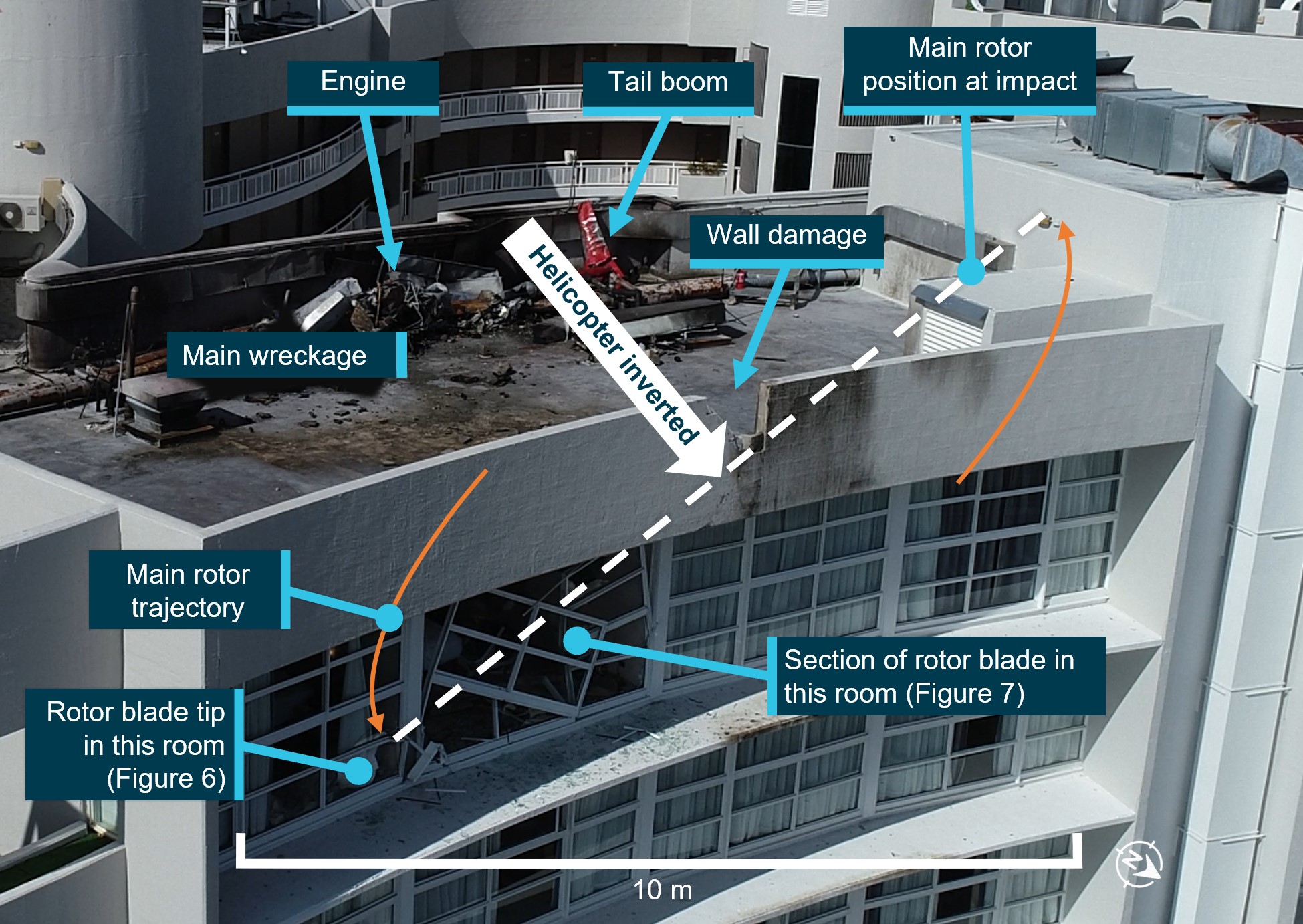
The distribution of the wreckage and impact marks (including the main rotor impact marks underneath the accident site) indicated that the helicopter was inverted at impact (Figure 3). Most of the helicopter, including its skids, came to rest on the hotel roof and was destroyed by impact forces and a fuel-fed post-impact fire.
Figure 3: Impact location and hotel room damage
Image source: Queensland Police, annotated by the ATSB.
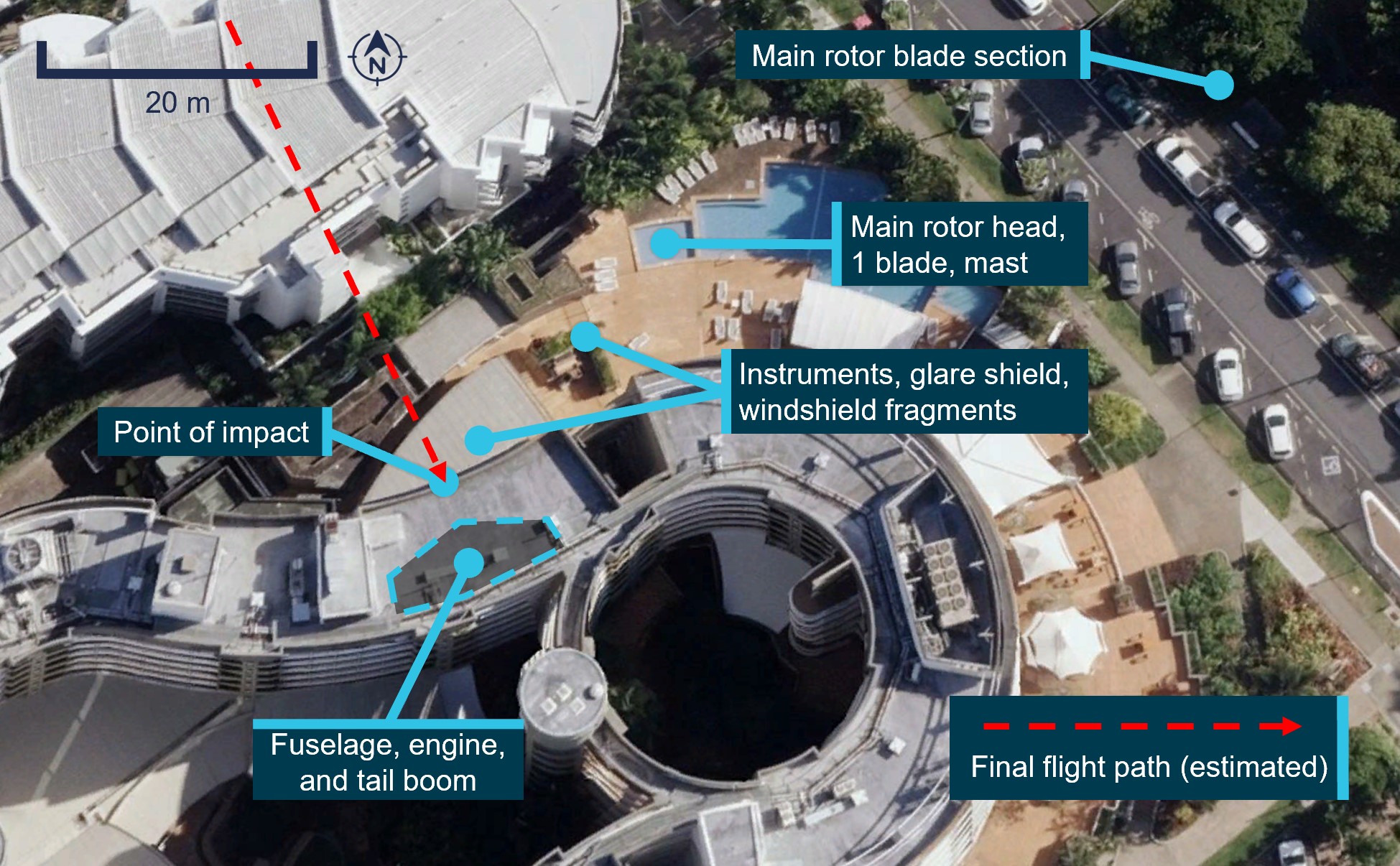
Parts of the main rotor were found in the rooms underneath the accident site. The helicopter instrument panel, glareshield-mounted GPS, mast, main rotor head and blades were separated from the helicopter’s fuselage during the accident sequence. They were located within the hotel grounds below the impact location. The remaining portion of the rotor blade that impacted the windows was found in parkland across the road from the hotel (Figure 4).
Figure 4: Accident site and wreckage distribution
Note: Image captured 2022. Image source: Google Earth, annotated by the ATSB.
Context
Pilot information
Experience and qualifications
The pilot was a New Zealand citizen and held a New Zealand Civil Aviation Authority (CAA) commercial pilot licence (helicopter). This licence carried a limitation for night flights to be conducted within 25 NM of a lit aerodrome. The pilot held New Zealand CAA type ratings for Cabri G2 and Robinson R44 helicopters, and a sling endorsement.
The pilot had accumulated 157.8 hours total aeronautical experience, 16.8 hours of which were flown in Robinson R44 helicopters, and 10.35 of which were flown at night in Cabri G2 helicopters. The last flight recorded in the pilot’s logbook was on 29 February 2024 in New Zealand.
In February 2023, the pilot registered for an equivalent Civil Aviation Safety Authority (CASA) flight crew licence in accordance with the Trans-Tasman Mutual Recognition Act 1997. They were granted a Civil Aviation Safety Regulation Part 61 commercial pilot licence (helicopter) in March 2023 with a class rating for single-engine helicopters. The pilot held a CASA helicopter low-level rating and a sling endorsement but did not hold a night VFR rating. There were no entries in the pilot’s logbook to indicate they had previously flown a helicopter in Australia.
Employment with the helicopter operator
The pilot was employed by the operator, Nautilus Aviation, as a ground crew member in April 2024. Their duties included taking fuel by road to the operator’s helipad near the Cairns marina, washing and re-fuelling helicopters, passenger transfer by vehicle, and other general ground duties. On the day of the accident, the pilot was due to travel to Horn Island to commence a new role within the organisation driving a fuel truck and re-fuelling aircraft.
Medical information
The pilot held a valid New Zealand CAA class 2 medical certificate and CASA class 1 and 2 civil aviation medical certificates with no restrictions. Prior to commencing work with the operator, the pilot was required to undertake drug screening and on 26 April 2024, was re-screened as a requirement for their new role within the organisation. The results on both occasions were negative.
A toxicology report indicated that the pilot had a significant blood alcohol content (BAC). A full drug screen was conducted and no drugs were detected. No significant carbon monoxide was detected (below 5%). A post-mortem examination report was not available at the time of publication.
Minimum height rule
Civil Aviation Safety Regulations 1998, Reg 91.265 (3) requires that, when over populous areas (including a city or a town), the pilot in command of a rotorcraft must fly at least 1,000 ft above the highest feature or obstacle within a 300 m horizontal radius immediately below the helicopter. Limited exceptions to the rule apply for medical transport operations and certain aerial work operations.
Air traffic control
Airservices Australia operates a control tower at Cairns Airport that is staffed 24 hours a day. On the night of the accident there was a single controller on a shift from 2145 to 0530.
Prior to the accident, the controller had handled a flight at around 0030, and they were expecting another flight at about 0500. While there were no scheduled flights between those times, the controller remained available for unscheduled flights such as search and rescue operations or for diverted flights. During this time, the controller completed internal computer-based training courses and clerical tasks.
The controller was able to take rest breaks but remained in the visual control room[4] where they were provided with a lounge chair, television, and basic amenities. While away from their normal workstation, the controller maintained a listening watch for unscheduled flights through speakers in the tower. The controller stated that they did not notice any airport activity outside of the tower.
As there were no scheduled flights, most of the controller’s attention was with equipment inside the control tower, such as the integrated tower automation suite (INTAS) console. At night, a controller would normally be alerted to an aircraft’s presence by:
monitoring the displays for the expected appearance of an aircraft based on submitted flight plan data
radio communications or radio interference sounds.
There were no other audible or attention-getting alerts to advise controllers to aircraft becoming active in the controller’s airspace; rather, an aircraft symbol would appear on the console display. In this case, the helicopter would have been visible on the console from 0144:28.
The controller recalled that they heard unexpected radio interference sounds on multiple occasions and checked the INTAS console for any new flight plans that may have appeared in the system. Recorded INTAS data shows the controller interacting with it at 0143:11 which was around the time the accident flight helicopter was being started.
Airside access and security
As an employee of the operator, the pilot had security code access to the building and was able to make their way to the hangar. In addition to VH-ERH, there were 2 larger helicopters in the hangar and their overall length prevented the hangar doors from being closed. The pilot was able to remove the helicopter from the hangar and position it on a helipad. To start the engine of a Robinson R44, a key is used to select both magnetos,[5] and the engine starter is engaged by pushing a button on the collective.[6] The operator stated that it was normal practice to leave keys in helicopters that were positioned in their hangars.
Operators such as Nautilus Aviation were required to be compliant with the North Queensland Airports (NQA)[7] transport security program. This required unattended aircraft positioned airside to be secured. This could be achieved by removing keys from keyed ignitions, not storing keys in the aircraft, locking doors, and other methods such as storing aircraft in locked or secured hangars.
There were Australian Federal Police officers and airport safety officers on duty at the time the pilot was preparing the helicopter, but they were not in the vicinity of the hangar. Additionally, by the pilot turning off the helicopter’s strobe lights, there would have been no visual cues to attract the attention of these officers.
Aircraft information
The helicopter was a Robinson R44 Raven II, serial number 12465, manufactured in the United States in 2008 and first registered in Australia on 29 October 2008. It was issued with a certificate of airworthiness in the normal category on 14 November 2008. The helicopter was registered with Nautilus Aviation on 13 August 2014.
A periodic inspection and other maintenance tasks were carried out on 7 August 2024. At the time of the accident, the helicopter had accumulated 4,142 flying hours.
The R44 is a single-engine, light utility and training helicopter with a semi-rigid, two-bladed main rotor, a two-bladed tail rotor and skid type landing gear. It has an enclosed cabin with two rows of side-by-side seating for a pilot and three passengers.
Meteorological information
Light drizzle with visibility to the Cairns airport terminal 1.5 km away could be seen on a video recording from the operator’s hangar when the pilot arrived at 0131. The drizzle had increased to a point where the terminal was less visible by time the pilot took-off at 0146:50.
While the flight was conducted at night, this would not have affected visibility for the pilot as there was an abundance of artificial lighting from city buildings and street lighting.
Recorded data
The helicopter was fitted with a Garmin aera 660 GPS, from which position and altitude data from the accident flight was successfully recovered at the ATSB’s technical facility in Canberra.
Airservices Australia provided ground-based radar data for the accident flight. This data combined primary surveillance radar (PSR) and secondary surveillance radar (SSR) data into a single, smoothed track.
The helicopter was not fitted with a cockpit voice recorder or flight data recorder, and due to the size of the aircraft, was not required to be.
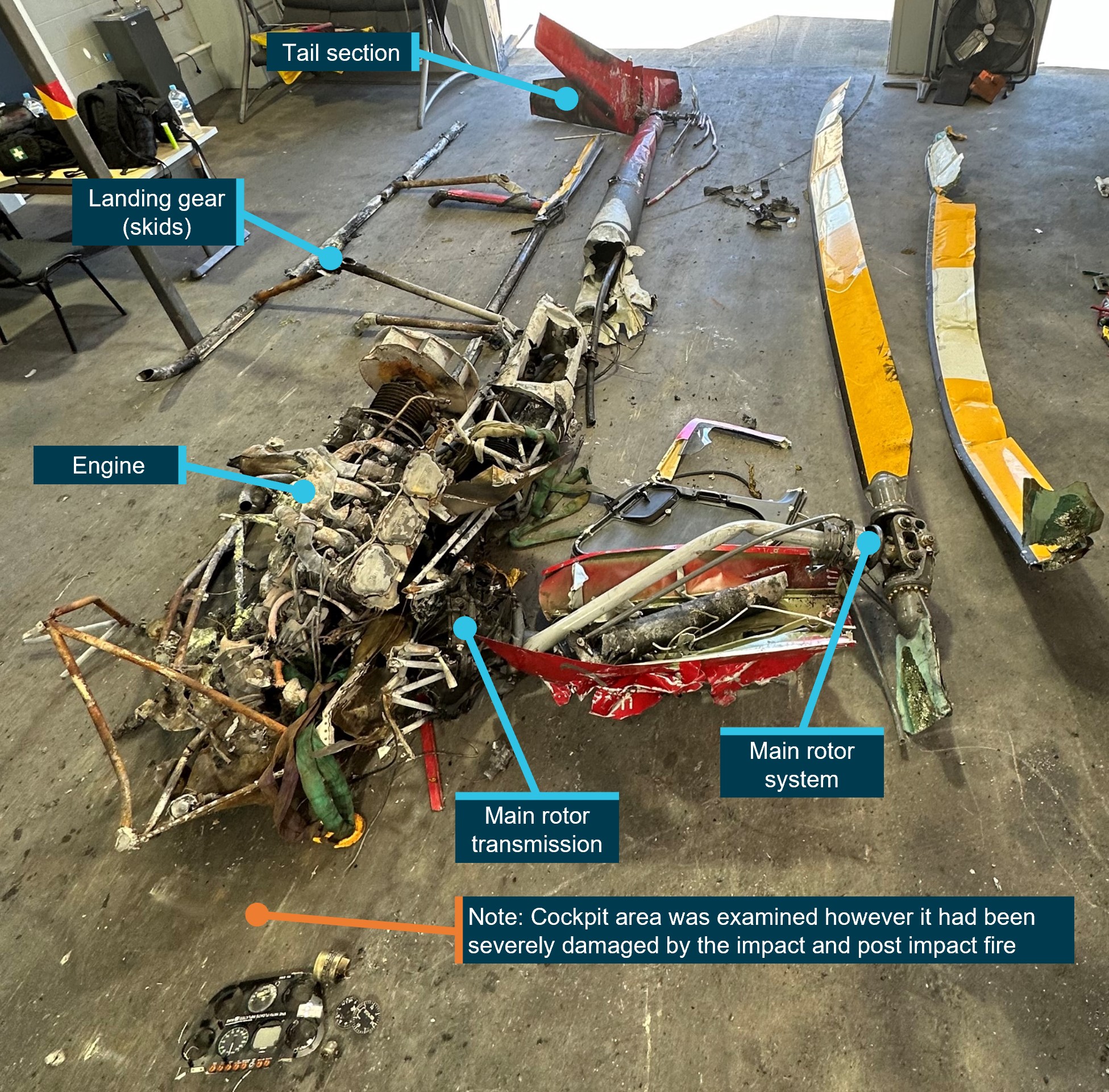
Wreckage information
The ATSB conducted a basic examination of the helicopter wreckage on the hotel roof and within the hotel grounds. The helicopter was subsequently transported to a secure facility where a detailed examination was carried out (Figure 5).
Figure 5: Examination of wreckage
Image source: ATSB.
The helicopter’s cockpit, systems and engine were severely damaged by the impact and post‑impact fire. Within the limitations of the available evidence, there were no indications of in‑flight fire or defects.
The absence of noteworthy damage to the helicopter’s skids indicated that the helicopter did not impact the hotel roof in an upright position.
There was no evidence of the main rotor contacting the tail boom, which remained intact.
Marks on one of the engine oil coolers indicated that the engine and ring gear were rotating at the time of impact.
Where possible, continuity was established with the main rotor, tail rotor drives and flight controls.
Main rotor blade damage was indicative of the engine driving the main rotors at a high-power setting.
The helicopter was fitted with bladder fuel tanks, which were breached during the accident sequence, but it was not possible to assess how the tanks were breached.
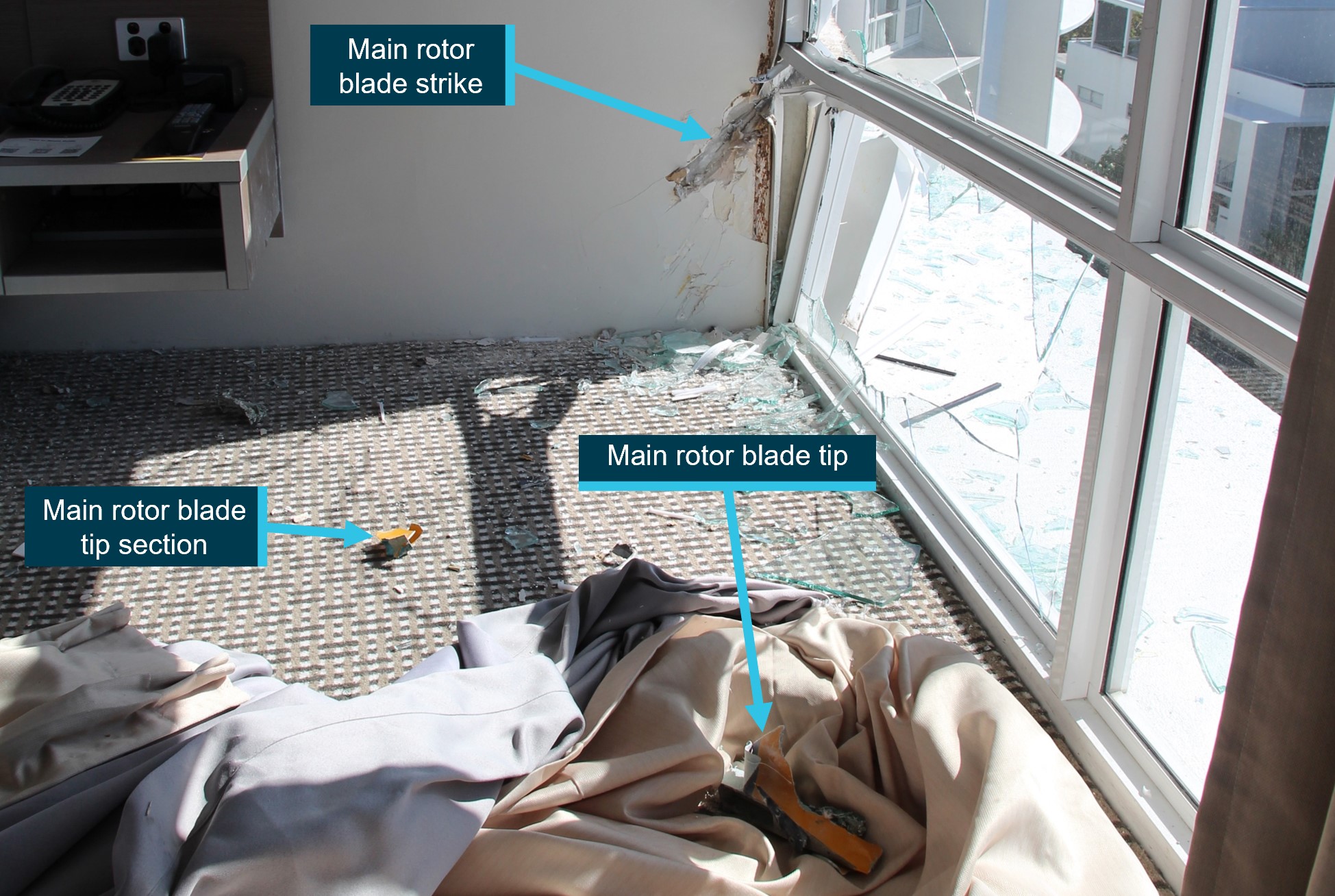
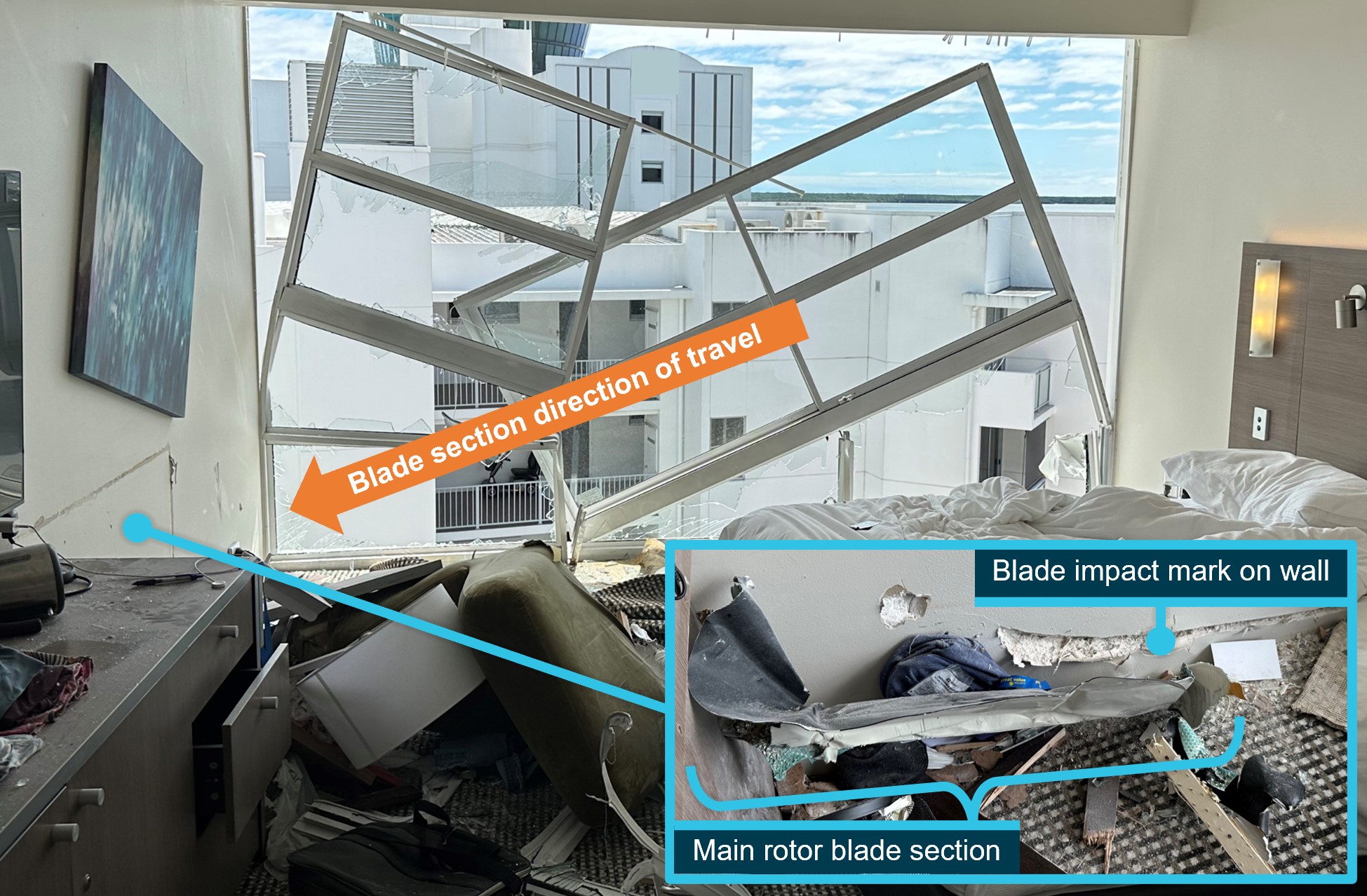
A rotor blade tip shattered the window of the room underneath the accident site (Figure 6), and a section from the same rotor blade destroyed the window of an adjacent room (Figure 7).
Figure 6: Hotel room damage
Image source: ATSB.
Figure 7: Hotel adjacent room damage
Image source: ATSB.
Safety analysis
The flight was an unauthorised but purposeful act, however the ATSB did not determine the reason the pilot elected to conduct the flight. The ATSB can conclude from the available evidence that there were no airworthiness factors with the helicopter that likely contributed to the accident.
The Civil Aviation Safety Authority has put in place regulations designed to ensure the safety of flight. The pilot was affected by a significant amount of alcohol before and during the flight. The pilot further increased risk to themselves and those on the ground by conducting the unauthorised flight well below the 1,000 ft allowed for flight over a built-up area.
While the pilot held a helicopter commercial pilot licence and had experience flying the Robinson R44, the pilot was not approved to fly the operator’s helicopters at any time. Additionally, the pilot did not hold the appropriate rating to fly helicopters at night and had never flown a Robinson R44 at night.
Aviation transport security regulations are in place to keep unauthorised persons out of airports. However, as a ground crew of the operator, the pilot was authorised to have access to the helicopter at Cairns Airport and took advantage of that access. Further, based on the strobe lights being turned off, it was apparent that the pilot was wanting to conceal the departure from the airport from air traffic control and airport staff.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following finding is made with respect to the collision with building involving Robinson R44 II, VH-ERH, Cairns, Queensland on 12 August 2024.
Contributing factors
For reasons unknown, pilot actions resulted in a collision with a building while conducting an unauthorised and unnecessary flight, while affected by alcohol, late at night and at low heights over a built-up area, and without night flying endorsements.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Robinson R44 helicopters can be manoeuvred (such as in and out of hangars) by detachable ‘ground wheels’ temporarily fitted to the helicopter’s skids.
[2]The operator reported that it was normal practice for the strobe lights to remain selected on at all times and not selected off post-flight. The strobe lights would flash immediately after the battery switch was selected on.
[3]This is consistent with Garmin aera 660 units previously recovered from accident sites.
[4]The top floor of the control tower from which the airport can be seen.
[5]A magneto is a device that provides a self-generated charge to the spark plugs of a piston engine.
[6]A collective is a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[7]North Queensland Airports is a group comprised of Cairns Airport, Mackay Airport and Mackay Airport Hotel.
UPDATED 1545: The ATSB has commenced a transport safety investigation into Monday morning’s helicopter accident in Cairns.
At about 0154, the Robinson R44 helicopter collided with a hotel building, and the sole occupant of the helicopter was fatally injured. The helicopter was destroyed by impact forces and fire.
A team of three transport safety investigators from the ATSB’s Brisbane office, with experience in aircraft operations and maintenance, arrived in Cairns on late Monday morning to commence the evidence collection phase of the investigation.
The ATSB asks anyone who may have witnessed or has photos or video footage of the aircraft during any phase of the flight (up to the impact), or heard the helicopter prior to the impact, to make contact via the witness form on our website at their earliest opportunity.
The ATSB notes the flight has been described as ‘unauthorised’. The ATSB conducts ‘no blame’ transport safety investigations, and does not investigate for the purposes of taking administrative, regulatory or criminal action.
Over the coming days we will seek to determine if this accident was a transport safety matter.
If the accident is determined not to be a transport safety matter the ATSB may elect to discontinue its investigation, on the basis that an ATSB investigation would be unlikely to determine new safety learnings and issues, and leave further investigation efforts to the police and other appropriate agencies.
If at any time during the course of the investigation we identify a critical safety issue, the ATSB will immediately notify relevant parties so that appropriate safety action can be taken.
The empennage and tail rotor gearbox of a Robinson R22 helicopter separated during a low hover after a tail rotor blade tip cap detached due to a moisture-induced adhesive bond failure, an ATSB final report notes.
The serious incident occurred on the morning of 26 February 2022 when a student pilot and instructor were conducting a low-level training exercise over Gold Coast Airport’s western grassed training area.
After around 30 seconds of stable hover, with the skids approximately 3–5 feet from the ground, there was a ‘bang’ through the airframe. The helicopter pitched nose up, developed a large vibration and then yawed to the right.
“The instructor immediately took control of the helicopter, lowered the collective and closed the throttle to control the yaw,” Director Transport Safety Dr Stuart Godley said.
The helicopter was landed safely and inspection found that both the tail rotor gearbox and empennage assembly had separated from the tailboom and were located within 10 metres of where the helicopter landed.
“The ATSB’s investigation found that the tail rotor tip cap detached due to a failure of the adhesive bond induced by moisture, with the resulting tail rotor imbalance leading to the fracture of the tailcone aft casting,” Dr Godley said.
Tap testing of the tail rotor blades during the most recent scheduled inspection, for the purpose of detecting adhesive failure, did not identify disbonds that were very likely present at the time.
Later in 2022 Robinson released updated service bulletins and service letters in response to seeing tail rotor blades that were allowed to corrode to an unserviceable condition, and after reports of tail rotor blade tips coming loose in service due to corrosion.
Notably, in June 2022 the manufacturer released a revised service letter for the R22, R44 and R66 helicopters requiring blades be replaced should there be any evidence of bond line corrosion.
“This service letter also included updated visual inspection and acceptance criteria which supplement the existing tap testing and increase the likelihood that degraded blades will be identified and removed from service,” Dr Godley noted.
Robinson has also identified certain part and serial number blades are susceptible to corrosion.
“These blades require additional visual inspection prior to the first flight of the day, until they are replaced with blades that are less susceptible to corrosion.”
The service bulletin details that newer blades have tip caps manufactured from an alternate alloy that reduces the likelihood of corrosion.
In addition, in April 2024 the US Federal Aviation Administration released an airworthiness directive(Opens in a new tab/window) requiring visually checking and inspecting certain part-numbered and serial-numbered R22, R44 and R66 tail rotor blade tip caps for corrosion.
All road users are reminded to ‘Expect the unexpected – watch out for trains’ when approaching level crossings, particularly when driving in regional areas where a large proportion of crossings are passively controlled without flashing lights or boom gates.
This Rail Safety Week (5-11 August), the Australian Transport Safety Bureau (ATSB) is again supporting the TrackSAFE Foundation’s annual rail safety initiative to positively influence driver behaviour by increasing their awareness of safe actions at and around level crossings.
“A moment of distraction while driving or riding can significantly impair safety and can lead to serious injuries or have fatal consequences,” ATSB Director, Rail Kerri Hughes said.
“Given the size and weight of most trains, the onus to take action to avoid a level crossing collision rests almost entirely on the road user.”
In March, the ATSB published a safety study into the risks associated with level crossing collisions, in particular involving heavy road vehicles. The study set out to compare the severity of level crossing collisions involving heavy road vehicles to those involving light road vehicles.
“Our study found that in a large majority of accidents at passively controlled crossings, the heavy vehicle driver did not detect the train, or detected the train too late to avoid a collision,” Ms Hughes said.
“Safety at passive level crossings relies on road users looking for and identifying trains, which can pass through a crossing at any time of the day or night, including when you are least expecting them. No matter where you are driving, riding or walking, if you are using a level crossing always expect the unexpected and watch out for trains.”