The ATSB is investigating a wirestrike and collision with terrain involving an Air Tractor AT-502, registration VH‑CJY, 19 km south-east of Lake Cargelligo Airport, New South Wales, on 18 July 2024.
During aerial agricultural spraying operations, the aircraft struck a wire and subsequently collided with terrain resulting in substantial damage. The pilot was fatally injured.
The ATSB deployed a team of transport safety investigators to the accident site with experience in aircraft operations, engineering, and human factors. As part of the onsite phase of the investigation, ATSB investigators examined the aircraft wreckage and other information from the accident site, interviewed witnesses and any involved parties, and examined maintenance records and any recorded data.
The ATSB has completed the evidence collection and analysis phases of the investigation and is drafting the final report.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2024-042
Occurrence date
18/07/2024
Occurrence time and timezone
12:56 Australian Eastern Standard Time
Location
19 km south-east of Lake Cargelligo Airport
State
New South Wales
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: Drafting
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Wirestrike
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Air Tractor Inc
Model
AT-502
Registration
VH-CJY
Serial number
502-0093
Aircraft operator
Thomson Airborne Pty Ltd
Sector
Turboprop
Operation type
Part 137 Aerial application operations
Activity
General aviation / Recreational-Aerial work-Agricultural spreading / spraying
The ATSB has released the final report from its investigation into an accident involving a Cessna 172 light aircraft near Camden Airport, south-west of Sydney, on 24 January 2024.
The aircraft was being used for flight instruction of a student pilot. After conducting a number of circuits, the instructor assessed that the student, who had previously flown solo in a Gazelle aircraft and held a recreational aviation pilot certificate, was competent to complete their first solo in the Cessna 172.
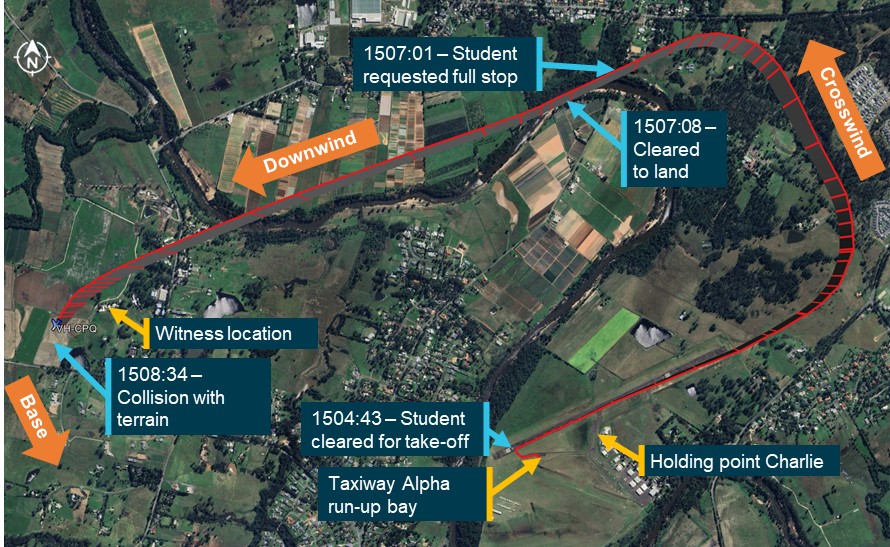
After receiving air traffic control clearance shortly after 3pm the student pilot commenced the flight, which was to be a standard circuit of the airport followed by a ‘full-stop’ landing.
Towards the end of the downwind leg of the circuit, the aircraft departed level flight, rapidly descended and impacted the ground in an open paddock. The pilot was fatally injured, and the aircraft was destroyed.
The ATSB’s investigation found there was no evidence of any in-flight failure of the airframe structure or flight control system and that the engine appeared to have been producing significant power at impact.
In the absence of an identified problem with the aircraft, and after consulting with the aircraft manufacturer to confirm performance characteristics, the investigation found that continual nose-down control input was almost certainly applied to the flight controls throughout the increasingly steep, accelerating descent.
The investigation considered potential reasons for the sustained forward pressure on the control yoke, which are discussed in the report’s Safety Analysis section.
However, based on the evidence available, the reason for the continued control input could not be determined.
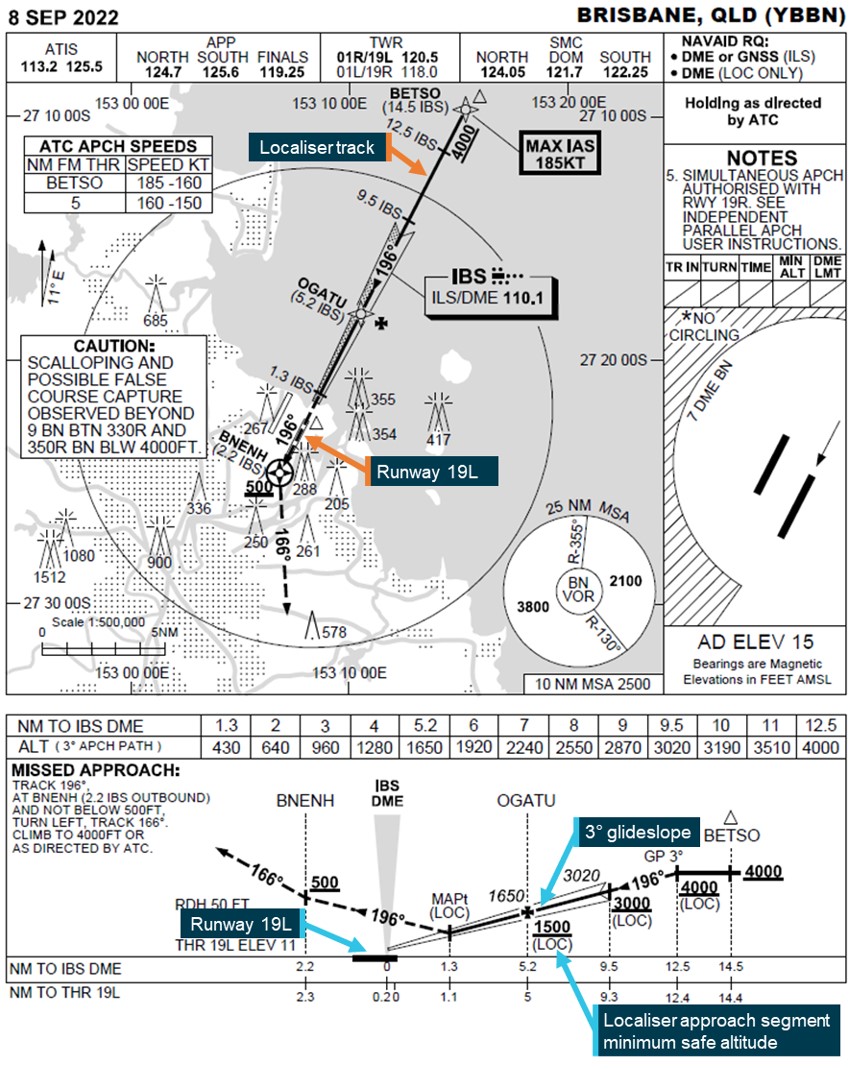
On 2 July 2024, a Fairchild Industries SA227-DC, registered VH-VEU and operated by Corporate Air, departed Cobar Regional Airport, New South Wales for a passenger charter air transport flight to Brisbane Airport, Queensland. During the instrument landing system (ILS) approach into Brisbane, the aircraft descended below the glideslope and approximately 8 NM (14.8 km) from the runway triggered an air traffic control (ATC) minimum safe altitude warning.
ATC advised the crew that they were observed below the glideslope, however the aircraft continued descent below the glideslope until 3 NM (5.6 km) when the descent rate was reduced. The aircraft then passed above the glideslope before the rate of descent increased again and subsequently the glideslope was re‑intercepted from above 1 NM (1.8 km) from the runway at 500 ft. The aircraft then followed a stabilised flight path to landing.
What the ATSB found
The ATSB found that the pilot flying descended the aircraft below the 3° glideslope after briefing and receiving a clearance for an instrument landing system approach. During the deviation, the aircraft’s descent rate and altitude triggered an air traffic control minimum safe altitude warning.
Additionally, the pilot monitoring was not monitoring the glideslope and did not challenge the pilot flying to correct the deviation and reduce the aircraft’s descent rate.
The ATSB also found that the operator's standard operating procedures (SOPs) contained areas of inconsistency when an aircraft entered visual conditions during an instrument approach, and that the Aeronautical Information Package (AIP) was unclear as to whether pilots were required to comply with precision approach flight tolerances.
What has been done as a result
Corporate Air made the following changes to its standard operating procedures after the incident:
the instrument approach procedure has been updated:
the approach brief now requires discussion of expectations if visual conditions arise
the statement that ‘during a visual approach using the ILS, the glideslope calls do not need to be given’ has been removed
a requirement to make callouts using reference to visual slope indications has been added.
a note has been added to the visual approach procedures stating that crew require a clearance to discontinue an instrument approach in controlled airspace
increased focus on pilot monitoring skills during:
proficiency checks, which will now include standard instrument departure and standard arrival routes
line training for new flight crew.
addition of a pilot monitoring sector to the annual line check.
Additionally, the Civil Aviation Safety Authority advised that it will be amending information regarding precision approach flight tolerances in the Aeronautical Information Package to include clearer links to existing legislative requirements and the use of defined terms.
Safety message
Effective monitoring in a multi-crew environment is paramount to aircraft safety. Bringing deviations to the attention of the pilot flying, whether in instrument or visual meteorological conditions, ensures the aircraft remains on a safe flight path and receiving confirmation from the pilot flying can assist in early detection of incapacitation.
When an approach has been briefed, flight crew share the same mental model of the expected flight path and deviations can be readily identified, advised and corrected. If the approach type changes without further briefing, both crew members are unlikely to have the same expectations, making it difficult for the pilot monitoring to identify and advise the pilot flying of deviations.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 2 July 2024, a Fairchild Industries SA227-DC, registered VH-VEU and operated by Corporate Air, departed Cobar Regional Airport, New South Wales, for a charter air transport flight to Brisbane Airport, Queensland with 2 flight crewmembers and 10 passengers on board. The flight crew consisted of a captain, undergoing training as pilot in command under supervision, performing the role of pilot monitoring (PM). A training captain, in the position of first officer, was the pilot flying (PF).[1] At 1511 local time, on approach to Brisbane Airport, air traffic control (ATC) advised the flight crew to expect an instrument landing system (ILS)[2] approach to runway 19L.[3] The crew reported that they conducted a brief of the expected ILS approach as per the operator’s standard operating procedures (SOPs).
At 1515, the flight crew commenced descent during which the aircraft entered instrument meteorological conditions.[4] At 1526, ATC cleared the flight crew to conduct the ILS approach to runway 19L, which the crew read back.
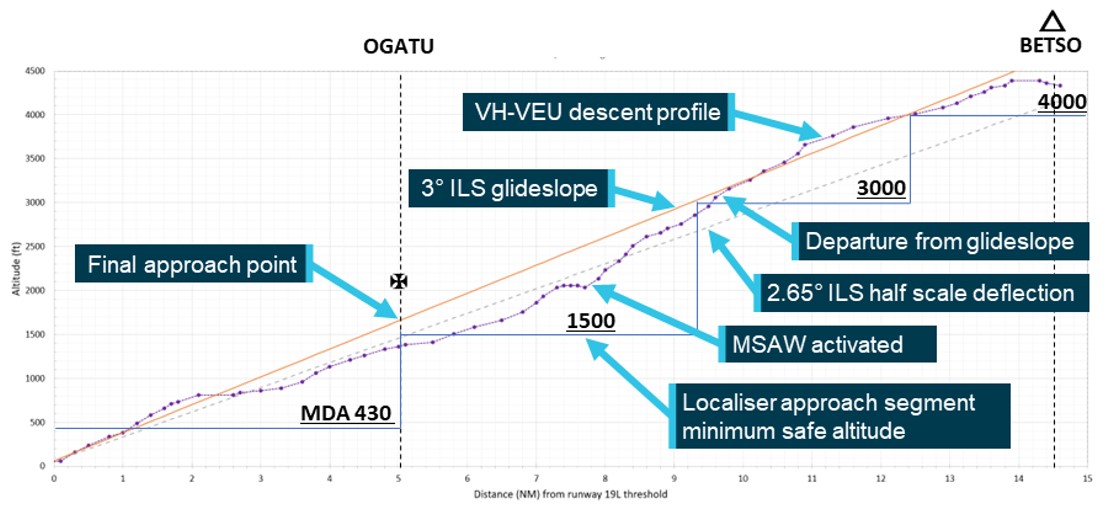
About 1 minute later the aircraft overflew the waypoint BETSO[5] (Figure 4), the initial approach fix for the ILS 19L approach, at approximately 4,400 ft above mean sea level (AMSL) (Figure 1) and commenced the ILS approach. The crew recalled that they became visual with the water and clear of cloud at about that time, but that was not reported to ATC and no request was made to discontinue the ILS approach and conduct a visual approach. The PM also recalled that upon becoming visual, they observed patches of lower cloud, but none that would affect their ability to proceed visually to the runway.
Figure 1: Descent profile of VH-VEU
Source: Flight data from ADSB Exchange, annotated by the ATSB
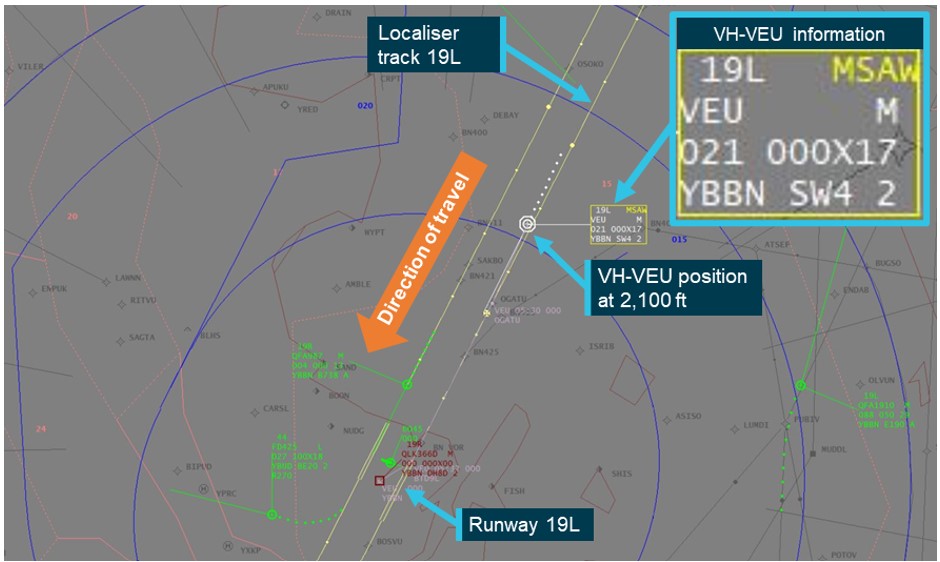
Passing 3,000 ft and 9.5 NM (17.6 km) from the runway threshold, the aircraft began to descend below the 3° glideslope. The PM recalled that the PF advised that they would stay below the lower patches of cloud to ensure that they remained visual. At 1529:36, ATC radar recorded the aircraft at an altitude of 2,100 ft with a descent rate of 2,068 ft/min, approximately 8 NM (14.8 km) from the runway threshold and 400 ft below the glideslope. This descent rate and low altitude triggered an ATC minimum safe altitude warning (MSAW),[6] which was visually displayed (Figure 2) and aurally alerted to the approach controller. Upon receipt of the MSAW the controller assessed that the aircraft was above the minimum altitude on the radar terrain clearance chart and not in unsafe proximity to terrain. Therefore, a safety alert was not issued.
Instead, as the flight crew had switched the radio to the aerodrome controller’s frequency, the approach controller alerted the aerodrome controller that the aircraft was below the glideslope, which the aerodrome controller then passed on to the crew. In response, the pilot monitoring asked the aerodrome controller if the glideslope was serviceable, to which they responded that it was. During the exchange, the aircraft entered the area surrounding the airport where MSAWs were inhibited, and the alert was no longer presented on the approach controller’s display.
Figure 2: Approach controller display at 1529:46
Source: Airservices Australia, annotated by the ATSB
The aircraft continued descent and at the final approach point remained more than half scale deflection below the glideslope. At approximately 3 NM (5.6 km) the rate of descent reduced, with the aircraft passing above the glideslope, before increasing again and the glideslope being re‑intercepted 1 NM (1.8 km) from the runway at 500 ft. The aircraft then followed a stabilised flight path to landing.
Context
Crew
The captain undergoing training held an Australian commercial pilot licence (aeroplane) and class 1 aviation medical certificate as well as an overseas air transport pilot licence that they were in the process of converting to the Australian equivalent. The captain had 5,350 hours of flying experience, of which 330 were obtained in the SA227-DC. They completed their initial line training with the operator in August 2023 before moving overseas in October 2023 to conduct training on a new aircraft type with a different operator. They returned to Australia and to flying duties with the operator in June 2024 and were conducting training due to the time spent away, with this flight being a check flight.
The training captain, operating as the first officer, held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. They had over 11,000 hours of flying experience, of which 851 were in the SA227-DC. They had previously conducted senior flying roles for the operator.
The ATSB found no indicators that the flight crewmembers were experiencing a level of fatigue known to affect performance.
Aircraft
VH-VEU was a Fairchild Industries SA227-DC fitted with two TPE331-12UA engines and capable of carrying up to 19 passengers and 2 flight crew.
Meteorology
Prior to commencing descent, the crew reported receipt of Brisbane Airport’s automatic terminal information service (ATIS)[7] information ‘Romeo’ to ATC. This information included:
few clouds at 600 ft and a layer of broken cloud at 1,200 ft[8]
visibility reducing to 4,000 m in passing showers
arriving aircraft were to expect an instrument approach procedure.
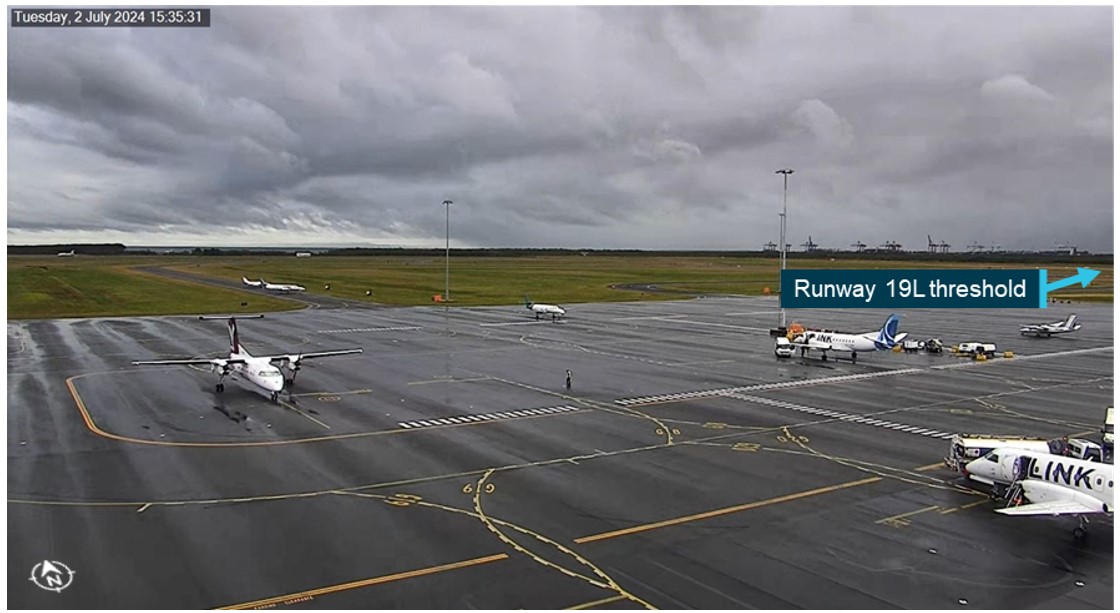
The ATSB obtained further information regarding the weather conditions that would likely have been encountered during the approach. The automatic METAR,[9] issued at 1530, reported few clouds at 600 ft, scattered cloud at 1,500 ft and broken cloud at 3,500 ft. Video footage from the airport (Figure 3) and satellite imagery showed cloud coverage consistent with the aerodrome meteorological reports.
Figure 3: CCTV image of weather conditions at Brisbane Airport at 1535
The image is taken from CCTV footage in the direction of the approach to runway 19L.
Source: Brisbane Airport, annotated by the ATSB
Crew actions
The PF reported having difficulty recalling details from the flight due to the time elapsed since the incident. However, they did recall that the aircraft had entered visual conditions. They also reported that they considered they were still complying with the ILS approach clearance. They advised that they were not required to maintain the glideslope, and they were permitted to descend to the localiser segment minimum safe altitudes.
The PM reported that the crew had briefed the expected ILS approach and had not included items relating to a possible transition to a visual approach. They also reported that due to the weather conditions, they transitioned to a visual approach and were looking outside the aircraft rather than monitoring the aircraft instruments.
The PM also reported that they questioned the serviceability of the glideslope as a learned response from flying in an overseas environment where navigation aids were sometimes unreliable and required verification.
Instrument approach
Aeronautical Information Publication instrument approach requirements
To conduct the 19L instrument landing system (ILS) approach (Figure 4) in controlled airspace, the crew required a clearance from ATC. The Aeronautical Information Publication (AIP) stated that:
Unless authorised to make a visual approach, an IFR flight must conform to the published instrument approach procedure nominated by ATC.
During an instrument approach, the crew was required to maintain the aircraft’s flight path within certain flight tolerances. For an ILS approach the AIP stated:
Pilots must conform to the following flight tolerances:
a) To ensure obstacle clearance, both [localiser/Ground based augmentation system (GBAS) landing system] LOC/GLS final approach course and glideslope should be maintained within half scale deflection (or equivalent on expanded scale).
b) If, at any time during the approach after the [final approach point] FAP, the LOC/GLS final approach or glideslope indicates full scale deflection, a missed approach should be commenced.
The AIP wording combined the terms ‘must’ and ‘should’, making it unclear as to whether this was a requirement or a recommendation. However, Airservices Australia confirmed that aircraft were required to comply with the vertical guidance of the glideslope when conducting an ILS approach, and that descent outside this vertical guidance could be safety critical.
For a 3° ILS approach, half scale deflection below the glideslope was the equivalent to an approach angle of approximately 2.65°. Airservices Australia also confirmed that a clearance to conduct the ILS approach was not a clearance to conduct the localiser approach, despite both approaches using the localiser for lateral guidance and sharing the same instrument approach chart.
Figure 4: Brisbane runway 19L instrument landing system approach
Source: Airservices Australia, annotated by the ATSB
Operator procedures
The operator’s standard operating procedures (SOPs) defined the expectations of both the PF and PM during an instrument approach and emphasised the importance of the roles of both crew members in monitoring the approach.
Both the PF and the PM shall monitor the progress of the approach using their own flight instruments, with the PM cross-referencing to the PF’s flight instruments.
It is an essential duty of the PM to automatically inform the PF of any deviation from the published approach procedure as briefed.
Prior to conducting an instrument approach, the operator required an instrument approach brief to be conducted. The operator’s SOPs stated:
Whenever changing from the intentions discussed in the briefing, the PF will re-brief accordingly.
The guidance around the instrument approach brief did not include a requirement to include the planned actions if there was an expectation of become visual during the approach. The approach guidance also advised:
During a visual approach using the ILS, the glideslope calls do not need to be given.
The SOPs for conducting an ILS approach required the pilot flying to establish the aircraft on the localiser, then intercept and track the glideslope. Several speed and configuration changes were then required while maintaining the aircraft’s flight path within the required tolerances of both the localiser and glideslope.
The pilot monitoring was required to monitor the aircraft’s flight path and manage communication with ATC. The SOPs listed the mandatory callouts and required responses during an ILS approach, including when the aircraft deviated half scale deflection or greater from glideslope (Table 1). It was also stated that making callouts:
… applies on all instrument approaches until 100 ft above the threshold height, even if visual flight conditions are established before reaching the minima.
Table 1: ILS approach callouts
Phase of Flight
Pilot Monitoring
Pilot Flying
Level flight, when outside ± 100 ft of the required altitude
Altitude
Checked
Speed + 10 KTS or – 5 KTS from target speed
Airspeed
Checked
Localiser or course bar moves from full scale deflection
Course bar active
Checked
Passing the outer marker/locator or its DME equivalent
Glideslope altitude checked
Checked
ILS or localiser approach, half scale deflection or greater
Localiser
Checked
Glideslope half scale deflection or greater
Glideslope
Checked
Speed outside approach speed profile
Airspeed
Checked
Below 1,000 ft AGL and VSI exceeds 1,000 fpm
Sink Rate
Checked
When reaching 200 ft to the applicable instrument approach minima
Approaching minima
Checked
At any time you get visual with the runway in sight
Runway visual in your … o’clock
Checked OR Nil sighting, continuing the approach
On reaching the minimum
Minima
Visual or Nil sighting, ground around
Source: Operator, emphasis added by the ATSB
The SOPs further required that:
if advisory calls are required on more than two occasions in any instrument approach before the final approach fix or more than once beyond the final approach fix, the crew should initiate a missed approach.
Visual approach
Aeronautical Information Publication visual approach requirements
The AIP listed meteorological conditions required for an IFR aircraft to conduct a visual approach. These conditions included the requirements for the aircraft to remain clear of cloud, and be in sight of ground or water with an in-flight visibility of not less than 5,000 m. If these conditions existed:
the pilot need not commence or may discontinue the approved instrument approach procedure to that aerodrome
The AIP also stated that when in controlled airspace, a clearance was required from ATC to conduct a visual approach. The crew was required to report ‘VISUAL’ to signify to ATC that the visual approach requirements could be met and maintained as part of any request for a visual approach.
Operator procedures
The operator’s SOPs contained advice consistent with the AIP, that if the meteorological conditions for a visual approach were met:
the pilot need not commence or may discontinue the approved instrument approach procedure to that aerodrome
The SOPs also required that:
Before starting a visual approach, the PF must brief any other flight crew on the following, (as appropriate):
• Expected manoeuvring to the final approach, including the runway, circuit direction, altitude and any restrictions
• Required navigation aids and/or approach slope guidance system
• Airport elevation
• Go-round procedures
The operator advised that these items would be included in the initial approach briefing for an instrument approach if there was an expectation of becoming visual and being issued with a visual approach clearance.
The SOPs contained requirements for conducting a visual approach and landing that stated:
Where possible approaches shall follow normal PAPI/T-VASI profile, i.e. 3 degrees. This angle will provide adequate height over threshold and the shortest landing distance. Level‑off segments should be avoided when conducting runway approaches. Aim to fly a constant descent profile as per the AIP/Jeppesen profile. Where available, approach guidance must be used.
Runway 19L was equipped with a Precision Approach Path Indicator (PAPI)[10] which would have been visible from about 5 NM (9.3 km) from the threshold in visual conditions. The SOPs required that:
When available, VASIS/PAPI must be used for approach slope guidance. Fly up indications must be responded to immediately unless the aeroplane is in level flight during daytime and in sight of ground or water.
The advisory callouts required from the PM when conducting a visual approach differed from those required when conducting an ILS approach (Table 2).
Table 2: Visual approach advisory callouts
Phase of Flight
Pilot Monitoring
Pilot Flying
At ‘500’ foot AGL If all Stabilised Approach Criteria are met: Or If not stable:
Stable Or Unstable
Continuing
Going-Around
Below 1,000 ft AGL and speed below or greater than +20 kt from target speed
Airspeed
Correcting
Below 1,000 ft AGL and VSI exceeds 1,000 fpm
Sink Rate
Correcting
When PAPI indicates aeroplane is more than one light above or below normal on slope profile
Glideslope
Correcting
Stabilised approach
A stabilised approach is one where an aircraft maintains a constant angle descent to the runway while other key flight parameters such as airspeed and aircraft configuration are controlled within specific ranges.
The operator’s SOPs stated that all flights must be stabilised by 1,000 ft above airport elevation in instrument meteorological conditions and by 500 ft in visual meteorological conditions (VMC). To be considered to have met these stabilised approach criteria in VMC the aircraft was required:
From 500 ft above ground level on the descent:
• aircraft on the correct flight path and only small changes in heading/pitch/power are required to maintain it, and
• speed is not less than VREF and not more than VREF + 20 knots indicated airspeed (KIAS), and
• aircraft is in the correct/final landing configuration, and
• sink rate is no greater than 1,000 ft per min, and
• power setting is appropriate for the aircraft configuration.
These requirements were in accordance with the minimum altitudes recommended in guidance material for Part 121.200 from the Civil Aviation Safety Regulations (CASR) Part 121 Acceptable means of compliance and guidance material (AMC/GM) - Australian air transport operations—larger aeroplanes and the International Air Transport Association (IATA) guidance document - Unstable Approaches: Risk Mitigation Policies, Procedures, and Best Practices (3rd Edition). The flight data showed that the aircraft was stabilised by 500 ft.
There are significant benefits in establishing and maintaining a stabilised approach with a constant angle descent prior to these minimums and the operator’s SOPs contained guidance that:
Flight crew(s) should aim to organise descent profiles such that their aeroplane can readily meet the speeds, heights and configurations, relevant to any Standard Arrival Route/Instrument Approach Procedure(s), and as set out in the respective FCOM and approach gradient table to ensure a constant descent profile and should aim to become stabilised as early as possible in the approach.
A stabilised approach has the effect of reducing pilot workload and allowing greater focus on flight path and airspeed. In a multi-crew environment, stabilised approach criteria enables the pilot flying and pilot monitoring to share the same mental model of the expected flight path and the parameters within which the aircraft is required to operate. This allows the pilot monitoring to effectively detect and advise of deviations which could then be corrected by the pilot flying. The operator’s SOPs highlighted the importance of effective monitoring and calling out of observed deviations:
The PM shall maintain a parallel line of thought to that of the PF, constantly questioning mentally the actions being planned and executed. If the perception of what is required closely matches the events occurring, no comment need be made. If however the events unfolding differ significantly from the ‘mental plot’, it is vital that the conflict be resolved as soon as possible.
It may be that the progress of the operation is being affected by factors not known to the PM, or it could be that the PF is not aware of an impending problem, which may affect the safety of the flight. In either case, the doubt shall be verbalised, and the conflict resolved in order that a smooth, efficient, and safe team effort can be resumed.
The IATA guidance document also highlighted the importance of callouts in achieving and maintaining a stable approach:
In order to achieve and maintain a stable approach, pilots must be constantly aware of each of the required parameters throughout the approach. A ‘callout’ is required if either pilot observes a deviation from the specified limits of the stabilization criteria or a deviation from the SOPs ...Each callout requires a corresponding acknowledgement from the other pilot, which canalso assist in the early detection of pilot incapacitation. The timely standard and the routine use of callouts inthis manner improves communication and enhances situational awareness throughout the approach. It also encourages effective flight management and rapid error correction.
Guidance material for Part 121.200 from CASR Part 121 AMC/GM - Australian air transport operations—larger aeroplanes discussed avoiding situations that may lead to an unstable approach, such as discontinuing an approach once visual:
Some situations that reduce the likelihood of a stabilised approach include:
• circling approaches
• discontinuing an approach before the minima/MAPT to continue in VMC
• instrument approaches flown with ‘step-down’ segments instead of a continuous descent
• low level circuits.
These circumstances should be avoided when they are not operationally necessary, or where other more suitable procedures exist.
Additionally, the IATA guidance document identified that to mitigate an unstable approach, it was important for flight crew:
To prepare for visual approaches by briefing speed/altitude/configuration gates, equivalent to those of an instrument approach and follow the published 'visual approach' pattern in the manufacturer’s or operator’s SOP
Safety analysis
Although the crew had briefed and were cleared to fly the instrument landing system (ILS) approach, the PF descended the aircraft significantly below the 3° glideslope and remained more than half scale deflection below the glideslope. This was contrary to the AIP requirements which required that the aircraft remain within a half scale deflection of the glideslope. Shortly after deviating beyond half scale deflection, the aircraft triggered a minimum safe altitude warning (MSAW), which led to the crew being advised by ATC that they were below glideslope. Despite this, the aircraft remained more than half scale deflection below the glideslope for a 5 NM (9.3 km) segment of the approach.
The PM reported that as the aircraft became visual, they transitioned to a visual approach and were not monitoring the glideslope. Consequently, when the aircraft's flight path deviated beyond half scale deflection, this was not detected or challenged. A change to a visual approach required a clearance from ATC which was not obtained. In addition, the operator required that the glideslope be used for approach guidance when conducting a visual approach. The operator further required that a brief be conducted prior to the commencement of a visual approach and neither crew member reported that this occurred. It is likely that as the PF reported they were complying with the ILS approach and the PM considered they were flying a visual approachthere was no shared mental model between the crew of the approach being flown.
The ATSB determined that there were areas of inconsistency within the operator’s SOPs relating to approach procedures in visual conditions. The procedures allowed the flight crew to discontinue an instrument approach if the aircraft became visual, and required that the crew brief whenever their intentions were changed. However, there was no specific requirement that an instrument approach could not be discontinued unless the change had been briefed, nor that discontinuing the approach should be briefed at the top of descent if there was a likelihood of the aircraft becoming visual. Discontinuing an instrument approach to continue visually was also contrary to Civil Aviation Safety Regulations (CASR) Part 121 guidance material advice that such circumstances should be avoided to reduce the likelihood of an unstable approach.
In addition, the instrument approach procedure required the crew to continue making glideslope deviation calls to 100 ft above the threshold, even if the aircraft entered visual conditions, whereas the visual approach procedure removed this requirement. Despite this, the operator required that approach guidance must be used where available during a visual approach. Not making glideslope deviation calls limited the effectiveness of the pilot monitoring in managing the stability of the approach and reduced the safety benefits offered by a multi-crew environment.
The ATSB also identified that the Airservices Aeronautical Information Publication (AIP) section regarding flight tolerances when conducting a precision approach was unclear as to whether the tolerances were a requirement or a recommendation.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the descent below glideslope involving Fairchild SA227-DC, VH-VEU about 17 km north-east of Brisbane Airport, Queensland on 2 July 2024.
Contributing factors
The pilot flying descended the aircraft significantly below the 3° glideslope after briefing and receiving a clearance for an instrument landing system approach. During the deviation, the aircraft's descent rate and altitude triggered an air traffic control minimum safe altitude warning.
The pilot monitoring was not monitoring the glideslope and did not challenge the pilot flying to correct the deviation and reduce the aircraft's descent rate.
Corporate Air’s standard operating procedures contained areas of inconsistency when an aircraft entered visual conditions during an instrument approach.
Other factor that increased risk
The Aeronautical Information Package (AIP) was unclear as to whether pilots were required to comply with precision approach flight tolerances.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Corporate Air
Corporate Air made the following changes to its standard operating procedures after the incident:
the instrument approach procedure has been updated:
the approach brief now requires discussion of expectations if visual conditions arise
the statement that ‘during a visual approach using the ILS, the glideslope calls do not need to be given’ has been removed
a requirement to make callouts using reference to visual slope indications has been added.
a note has been added to the visual approach procedures stating that crew require a clearance to discontinue an instrument approach in controlled airspace
increased focus on pilot monitoring skills during:
proficiency checks, which will now include standard instrument departure and standard arrival routes
line training for new flight crew.
addition of a pilot monitoring sector to the annual line check.
Safety action by the Civil Aviation Safety Authority
The Civil Aviation Safety Authority advised that it will be amending information regarding precision approach flight tolerances in the Aeronautical Information Package to include clearer links to existing legislative requirements and the use of defined terms.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew and operator
Bureau of Meteorology
Civil Aviation Safety Authority
Airservices Australia
Brisbane Airport.
References
Civil Aviation Safety Authority, 2023, Civil Aviation Safety Regulations (CASR) Part 121 Acceptable Means of Compliance and Guidance Material (AMC/GM) – Australian air transport operations—larger aeroplanes
International Air Transport Association, 2017, Unstable Approaches – Risk Mitigation Policies, Procedures and Best Practices (3rd Edition)
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
the flight crew
Civil Aviation Safety Authority
Airservices Australia.
Submissions were received from:
the operator
the flight crew
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Instrument Landing System (ILS): a precision instrument approach system which normally consists of a VHF localiser providing horizontal guidance and a UHF glideslope providing vertical guidance.
[3]Runway number: the number represents the magnetic heading of the runway. L specifies the left runway when there are parallel runways available.
[4]Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[5]Waypoint: a specified geographical location used to define an area navigation route or the flight path of an aircraft employing area navigation.
[6]Minimum Safe Altitude Warning (MSAW): an automated warning for air traffic controllers to draw attention to an aircraft that at its current descent rate is 60 seconds to terrain.
[7]Automatic terminal information service: the provision of current, routine information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations.
[8]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[9]METAR: a routine report of observations of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[10]Precision Approach Path Indicator (PAPI): a ground-based system that uses a system of coloured lights used by pilots to visually identify the correct glide path to the runway when conducting an approach.
Occurrence summary
Investigation number
AO-2024-040
Occurrence date
02/07/2024
Location
About 17 km north-east of Brisbane Airport
State
Queensland
Report release date
04/03/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Operational non-compliance
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Fairchild Industries Inc
Model
SA227-DC
Registration
VH-VEU
Serial number
DC-797B
Aircraft operator
Vee H Aviation Pty Ltd.
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
A twin-engine Piper PA-31 aircraft conducted a forced landing by a Brisbane railway line due to fuel starvation after the pilot, who was likely fatigued, misdiagnosed the loss of engine power, an ATSB investigation report has found.
The aircraft was returning to Brisbane’s Archerfield Airport, from where it had departed shortly after midnight, on the return leg of a freight charter flight to Sydney’s Bankstown Airport on the morning of 7 April 2023.
Approaching Archerfield, the pilot observed a loss of engine power from the right engine, then the left engine.
“Unable to reach Archerfield, the pilot conducted a gear-up forced landing alongside a railway line,” ATSB Director Transport Safety Dr Stuart Godley said.
The aircraft struck multiple trees and was substantially damaged, but fortunately, the pilot only received very minor injuries.
Post accident inspections found no indication of a mechanical failure that could have caused the engines to fail.
“Although the pilot reported changing from the auxiliary tanks to the main fuel tanks prior to descent, the quantity of fuel recovered from each tank after the accident, and fuel burn calculations, indicated that those selections had probably not been made and both engines lost power as a result of fuel starvation,” Dr Godley said.
The ATSB investigation report notes that the pilot misdiagnosed the loss of engine power as a partial power loss, and did not carry out the loss of engine procedure.
“Following the first power loss on the right engine, the right propeller was not feathered, resulting in excessive drag,” Dr Godley explained.
The pilot operated the return flight late at night after working in outside employment during the day. By the time of the accident, the pilot had been awake for almost 20 hours.
“A review of the pilot’s sleep history found that it is likely that the pilot was experiencing a level of fatigue shown to have an effect on performance,” Dr Godley added.
“In this case it is likely that fatigue impacted the pilot’s incorrect tank selection as well as their ability to troubleshoot the loss of power.”
Following the accident, the aircraft operator issued a notice to aircrew and conducted a review of pilot training to include the recognition and management of fuel starvation, and updated its fatigue management manual to include external employment and restrictions around hours of work and duty times.
Dr Godley said the occurrence highlights to pilots the importance of understanding their aircraft’s fuel system, and being familiar and proficient in its operation.
“During a power loss event, pilots should take the time to determine whether a total failure has transpired or if the engine is still delivering some power,” Dr Godley said.
“While this may not be clearly apparent in all configurations, the consequences of misdiagnosing a failed engine can be fatal.”
“The management of fatigue is a joint responsibility between the operator and the pilot,” Dr Godley said.
“This accident also reinforces the importance of obtaining some sleep during the day prior to commencing operations at night during normal periods of sleep.”
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into a collision with terrain accident involving an Air Tractor aerial application aircraft south-east of Lake Cargelligo, New South Wales.
While conducting aerial spraying on a property, the aircraft reportedly struck a wire, and collided with terrain.
The ATSB is deploying a transport safety investigation team from its Canberra office.
On site investigation work will include a range of evidence-gathering activities, including site mapping, wreckage examination, and recovery of any aircraft components for further examination at the ATSB’s technical facilities in Canberra.
The ATSB will also seek to interview any witnesses and involved parties, and collect relevant recorded information including flight tracking data, as well as pilot and aircraft maintenance records, and weather information.
The ATSB will release a final report at the conclusion of the investigation. However, if at any time should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so safety action can be taken.
The mid-air collision of two S-211 jets during aerial photography south of Melbourne highlights the importance of in-depth pre-flight planning of formation flying manoeuvres and strictly adhering to procedures and the agreed plan.
Two SIAI Marchetti S-211 ex-military jet trainer aircraft were conducting a formation flight over Port Phillip Bay on 19 November 2023, for aerial filming of both aircraft to promote a proposed television program.
The manoeuvre leading to the collision involved the formation lead aircraft, callsign ‘Viper 1’, rolling inverted before the second jet, ‘Viper 2’ passed directly beneath it. This manoeuvre had not been specifically briefed before the flight, and was conducted without the prior knowledge of the crew of Viper 1, the ATSB investigation of the accident found.
After the first attempt at the manoeuvre, the pilots of both aircraft discussed repeating the manoeuvre over the radio.
“This in-flight discussion did not allow the pilots to fully consider the risks associated with the manoeuvre before it was attempted for a second time,” Chief Commissioner Angus Mitchell said.
During the second attempt, the right wing of Viper 2 struck the right wing of the inverted Viper 1. Viper 2 sustained substantial damage, resulting in the failure of its front wing spar and deformation of the outboard wing section, and an immediate loss of control. Soon after the aircraft impacted the water, fatally injuring both occupants (the pilot and a camera operator).
Viper 1 was not significantly damaged, having been struck on a section of wing where the structure is relatively stiffer and stronger, and was able to return safely to Essendon Airport.
“Pre-briefing of in-flight manoeuvres is critical to safe formation flying to mitigate the risks of increased pilot workload and distraction,” Mr Mitchell said.
“Minimising the risk of these flights requires pilots to prioritise operational safety, in particular through in-depth briefings, pre-flight planning of manoeuvres, and strict adherence to procedures and the agreed plan.
“This ensures everyone has a similar understanding of the intended manoeuvres, and can fully consider the associated risks.”
Pre-briefing of a manoeuvre can also be conducted in-flight, as done by the crew before the second attempt. However, when compared to a face-to-face pre-flight briefing, an in-flight briefing, using radio and while also flying the aircraft, limits a pilot’s ability to articulate and understand intended manoeuvres and fully consider associated risks.
“In-flight briefings can also reduce the lead’s ability to assess that there is mutual understanding before approving a manoeuvre,” Mr Mitchell said.
The investigation also found the aircraft operator did not hold the required certificate to undertake the filming flight, which under CASA regulations is required to be conducted as an aerial work (task specialist) operation.
In addition, as ex-military aircraft operated in the Limited airworthiness category, the S-211s were not permitted to be used for that purpose.
Finally, the pilot of Viper 1 had medical restriction requirements which were not being fully followed during the flight (they were required to only operate aircraft with a side-by-side seating configuration and with a type-qualified safety pilot).
“While these factors did not directly contribute to the aircraft handling or decision-making that led to the collision, regulatory limitations exist to mitigate known risks associated with this type of operation,” Mr Mitchell explained.
“Operating outside of these limitations removes in-built safety defences and organisational structures designed to identify and mitigate these risks.”
The ATSB has released a preliminary report from its ongoing investigation into an accident involving an Air Tractor aircraft conducting aerial spraying on a property near Bourke, in north-western New South Wales, on the morning of 10 February 2024.
Recorded data showed the AT-502 aircraft took off in a southerly direction from an airstrip on the property with its first load of herbicide, and commenced spraying a field, which was expected to be conducted with the aircraft’s wheels about 2-3 m above the ground.
Twelve seconds after spraying commenced, the recorded data ended, with a final recorded ground speed of about 114 kt.
The aircraft wreckage was subsequently located in a cotton field adjacent to that being sprayed by another pilot spraying the same property, who had become concerned when they could not contact the accident pilot.
The pilot was found to be fatally injured, and the aircraft was destroyed.
“A site examination found the aircraft had impacted an irrigation levee adjacent to the southernmost field being sprayed,” acting Director Transport Safety Dr Nathalie Boston said.
“A ground scar about 27 m long from the aircraft’s left main wheel was found in the paddock just before the levee, and two more wheel marks were found where the main landing gear struck the levee.”
Examination of the wreckage itself indicated the aircraft collided with terrain nose down, then came to rest inverted.
“All of the aircraft’s major components were present at the accident site, and there was no evidence of an in-flight break-up,” Dr Boston said.
“Additionally, there were no pre-impact defects identified with the airframe or flight controls, and examination of the engine and propellor indicated that the aircraft was under power at impact.”
As it progresses the investigation will include review and examination of electronic components recovered from the aircraft, medical and pathological records, operational documentation, and aircraft maintenance records.
A final report, which will detail the ATSB’s findings and its analysis of the collected evidence, will be released at the investigation’s conclusion.
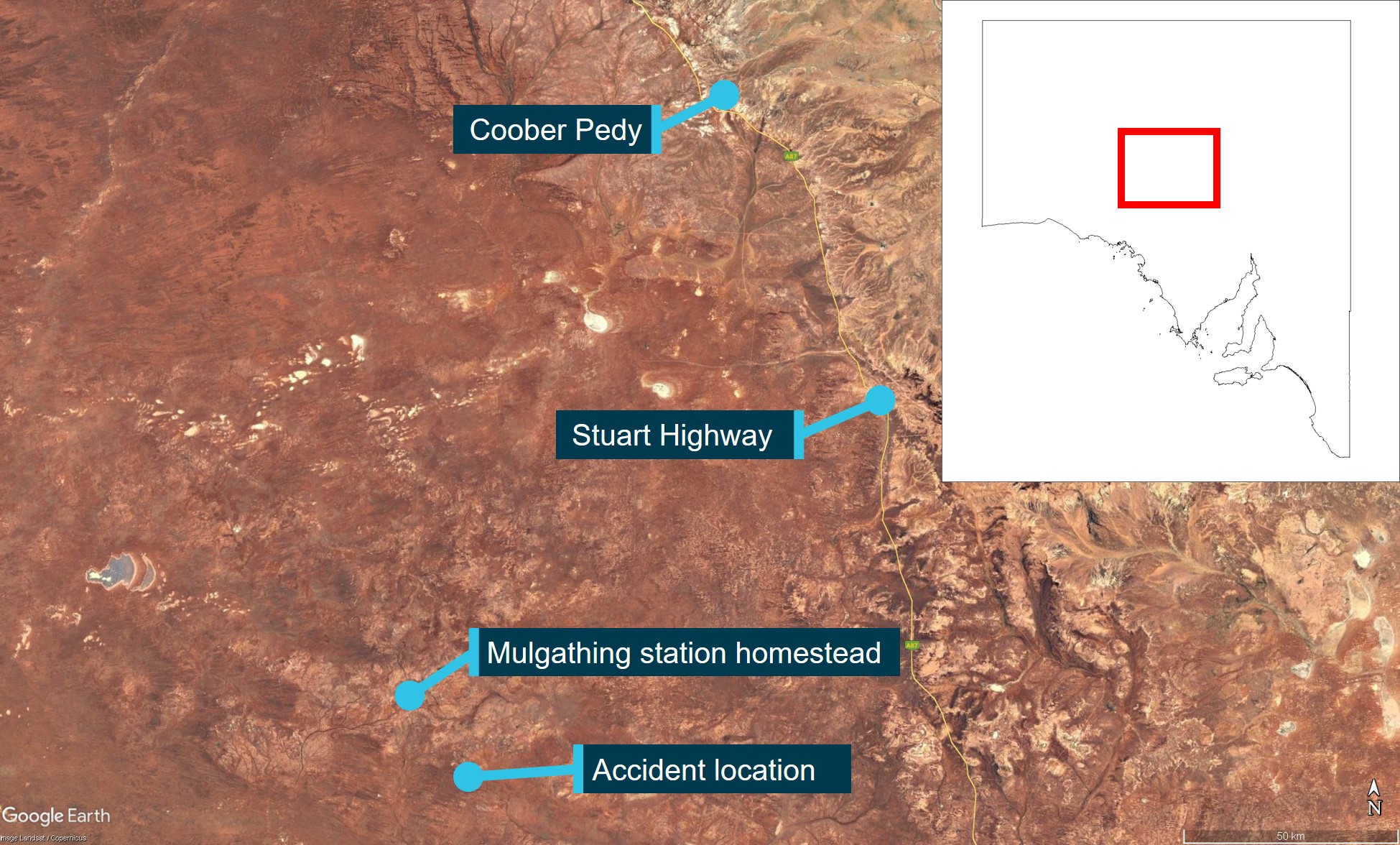
On the morning of 27 June 2024, the pilot of a Cessna Aircraft Company 172N, registered VH‑SQO, was assisting with mustering sheep at Mulgathing Station, South Australia. At about 0810 local time, a witness on a motorbike about 500 m away observed the aircraft dive down on what they presumed was a flock of sheep to an estimated height of about 50 ft above the ground before climbing rapidly, turning to the left and then descending towards the ground. The aircraft was destroyed, and the pilot who was the sole occupant was fatally injured.
What the ATSB found
The ATSB found that, while mustering sheep without the appropriate endorsement to do so, the pilot lost control of the aircraft leading to an aerodynamic stall and spin from an altitude that was not recoverable. Although not contributory, it was also found that the upper torso restraint part of the lap-sash seatbelt was not worn at the time of the accident. Further, the pilot was hired for a job advertised as aerial stock mustering but did not require an aerial mustering endorsement as the operator’s intention was that the role only involved aerial spotting.
What has been done as a result
The operator has advised that it is preparing a Safe Aerial Spotting & General Station Aviation Manual. It has also implemented a pilot mentoring program and initiated a third-party safety audit. It is also undertaking a review of its operations to ensure compliance with the Civil Aviation Safety Authority regulations as well as the safety and training standards for pilots.
Safety message
This accident highlights the importance of managing airspeed and bank angle to minimise the risk of an aerodynamic stall. This is particularly important when operating in close proximity to the ground, such as during take-off, landing and when conducing low-level air work, as recovery may not be possible. Low-level flying is a higher risk activity and mustering at low-level adds additional complexity and risk. It is important that pilots operate within the boundaries of their training and qualifications to ensure an adequate margin of safety is maintained.
The ATSB’s SafetyWatch initiative highlights broad safety concerns generated by its investigation findings, and fromoccurrence data reported by industry. One of the safety concerns is Reducing the severity of injuries in accidents involving small aircraft, which includes the appropriate fitment and use of seatbelts. This SafetyWatch notes that in several of its investigations, the ATSB has found injuries to aircraft occupants may have been avoided, or made less severe, through the appropriate use of multi-point harnesses.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
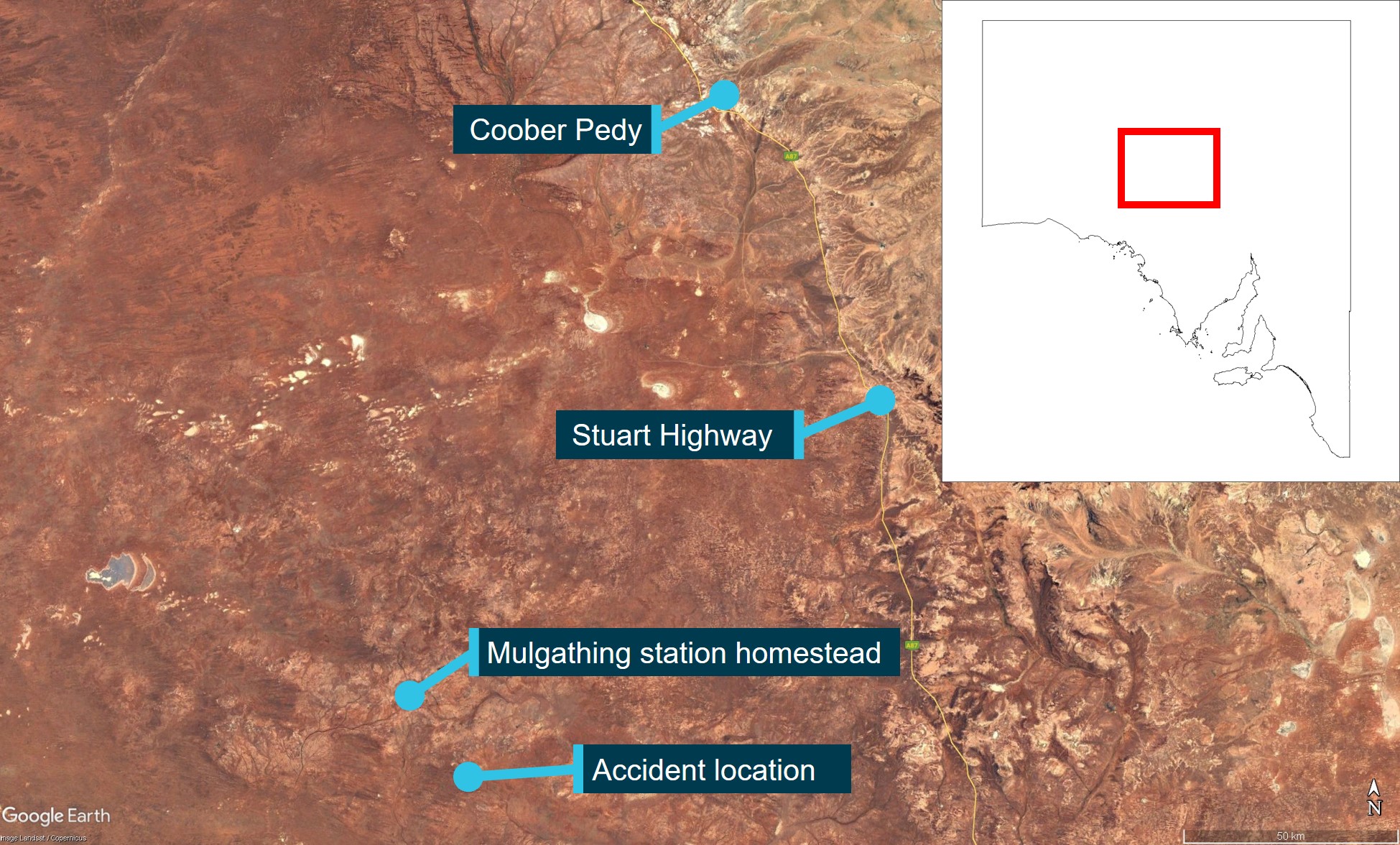
On the morning of 27 June 2024, the pilot of a Cessna Aircraft Company 172N, registered VH‑SQO, met co-workers for breakfast at about 0630 local time before a morning briefing on the task for the day, which involved mustering sheep at Mulgathing Station (owned by Jumbuck Pastoral (operator)), South Australia. At about 0700, the station manager, assistant manager and 4 station hands set off for a yard about 30 km south-east of the homestead (Figure 1). Meanwhile, the pilot drove to the airstrip about 5 minutes away, took off and flew towards the yard to rendezvous with the other workers.
The station manager and 4 station hands were marking[1] lambs in the yard while the pilot, in the aircraft, and the assistant manager (witness) on a motorbike, were rounding up stray sheep. At about 0810, the witness observed the aircraft flying overhead at about 300 ft above ground level looking for sheep when the pilot radioed to say they had found 2 flocks about 2 km away. The witness converged on one flock and observed the aircraft circling about 500 m away over what was presumed to be the second flock.
The witness radioed the pilot to ask if they needed help moving the sheep. The pilot responded that they thought they would be able to do it with the aircraft. The aircraft was then observed to continue circling to the left at a height the witness estimated to be 150–200 ft before diving at an angle of about 45° towards what was presumed to be the flock of sheep, to a height of about 50 ft. The witness estimated that the aircraft then climbed out at about a 60° nose‑up attitude to a height of about 250–300 ft, rolled to the left and descended nose-down towards the ground and impacted terrain. No bird activity was noted by the witness and they reported not hearing any changes in the engine noise during the accident sequence. While they were not certain of the actual angle of climb, they noted that it was steeper than the descent. The aircraft was destroyed, and the pilot who was the sole occupant was fatally injured.
Figure 1: Accident location with reference to Coober Pedy and the Stuart Highway
Source: Google Earth, annotated by the ATSB
Context
Pilot information
The pilot, a New Zealand citizen, held a Civil Aviation Safety Authority Part 61 Commercial Pilot Licence (Aeroplane) with a single and multi-engine class rating with endorsements for retractable undercarriage, manual propeller pitch control, and low‑level and instrument ratings. They did not hold an aeroplane aerial mustering endorsement. The pilot’s commercial licence was issued on 17 August 2023 in accordance with the Trans‑Tasman Mutual Recognition Act 1997. They had recorded 441.5 total flying hours in their logbook, dated 16 June 2024.
The pilot’s low‑level training was conducted on 1–3 December 2023 and their low‑level rating was issued on 3 December 2023, which was also their last flight review. The flight test was conducted in a Cessna 172 aircraft, with all elements of the low‑level rating with a single‑engine aeroplane endorsement assessed as satisfactory, including the approach and recovery from a stall in level flight and turning.[2] The instructor who conducted the pilot’s low‑level training noted that the role was for aerial spotting rather than mustering, therefore, the elements for the aerial mustering endorsement were not tested.
The pilot was employed by Jumbuck Pastoral to work at Mulgathing Station in December 2023. The pilot’s logbook showed 70 flights were conducted by the pilot at Mulgathing between January 2024 and the last logbook entry on 16 June 2024. These flights totalled 198.3 hours, all of which were conducted in VH‑SQO.
The pilot held a Class 1 Aviation Medical Certificate with no restrictions, valid to 29 November 2024. The pilot’s aviation medical examination indicated no reported medical conditions nor prescribed medications. Co‑workers reported the pilot was fit, healthy, did not drink alcohol excessively and did not smoke. On the morning of the accident, witnesses stated that the pilot demonstrated no abnormal behaviour.
Aircraft information
VH‑SQO was a Cessna Aircraft Company 172N 4‑seat, single‑engine, high (strut‑braced) wing, all metal, unpressurised, fixed (tricycle) undercarriage aircraft. The aircraft was manufactured in the United States in 1978 and assigned serial number 17270255. It was first registered in Australia on 29 August 1978. The operator had been the registered owner of the aircraft since the date of registry.
The current maintenance release was issued on 8 March 2024 and was valid until 8 March 2025 or 14,620.8 hours total time‑in‑service, whichever came first. At the time of take‑off for the accident flight, the aircraft had accumulated 14,602.7 hours. The maintenance release showed that required maintenance had been completed and no defects were recorded.
Meteorological information
There was no airport forecast for Mulgathing Station, however, the Bureau of Meteorology graphical area forecast issued at 0137 local time and current for the time of the accident forecast no cloud or weather below 5,000 ft and visibility greater than 10 km. This was consistent with witness accounts, which reported that, on the morning of the accident, the weather was fine, clear and the temperature was cool, not cold. No wind or cloud cover was observed, and the conditions were described by a witness as being ‘almost perfect for paddock work’.
Wreckage and impact information
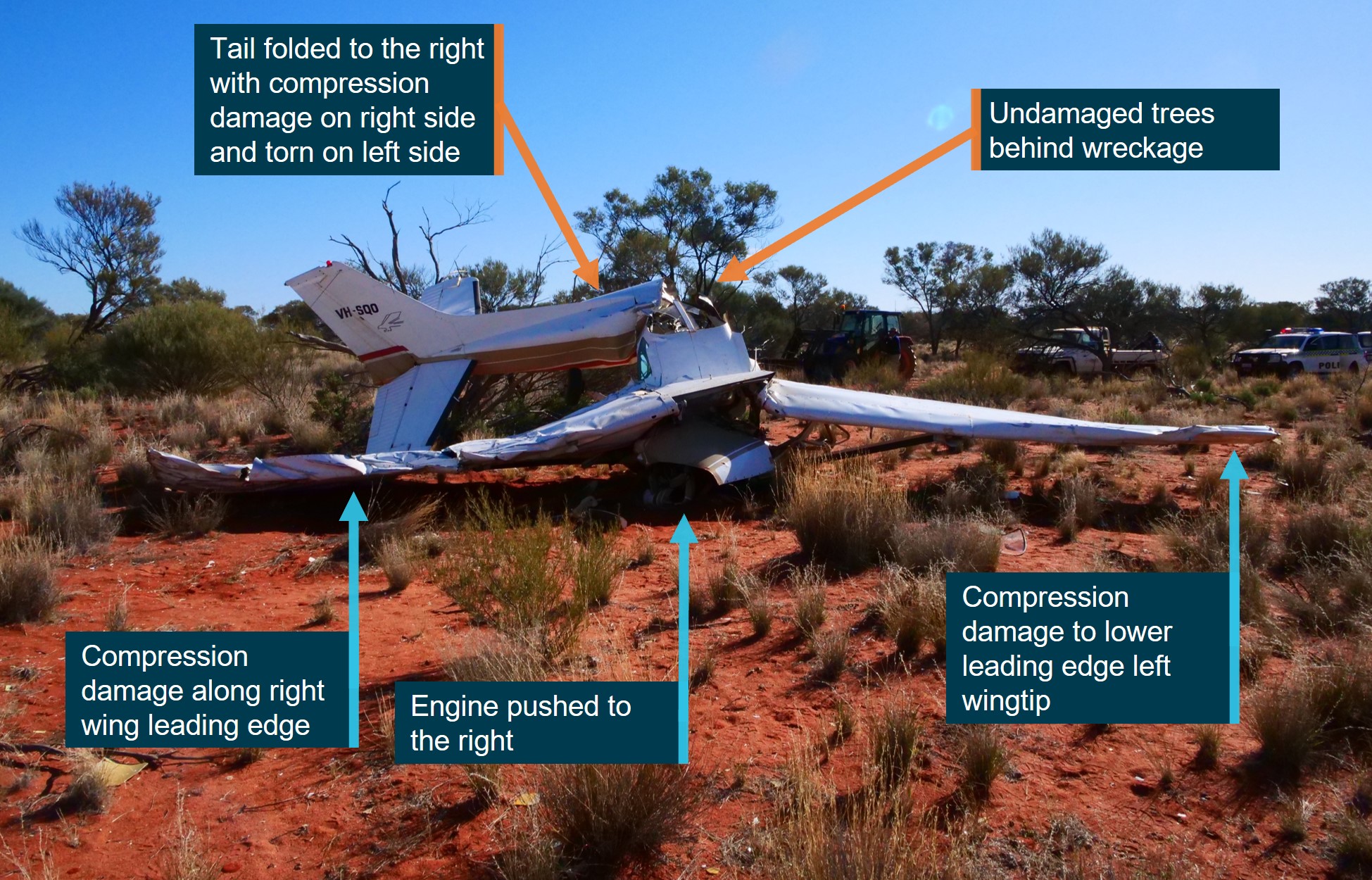
The ATSB’s onsite examination found that the aircraft impacted with terrain at about a 70° pitch down attitude with undamaged trees behind the wreckage. Ground impact marks were directly under the wreckage indicating no forward momentum.
The engine was deflected to the right of the longitudinal axis by about 25° (Figure 2). The crank case had fractured in overload, which separated the propeller from the engine. The underside of the left wingtip leading edge exhibited compression damage, which was also evident along the span of the right wing leading edge. The aft fuselage had folded towards the right with compression damage evident on the right side. The flaps were in the full retracted position.
Figure 2: VH-SQO accident site
Source: ATSB
The aircraft’s flight controls and structure did not identify any pre‑existing faults or pre‑impact defects or failures, and no evidence of a birdstrike was observed. Additionally, one of the propeller blades showed significant rotational abrasion damage and chord-wise twisting indicating that the engine was driving the propeller under significant power at the time of impact.
Examination of the fuel drum used to refuel the aircraft showed it had a water drain and filter in a clear bowl with uncontaminated fuel evident in the filter bowl. Although the fuel selector was found to be in an undetermined position due to the accident damage, there was a significant amount of fuel remaining in both tanks, a strong smell of fuel around the aircraft, and the fuel tank caps were observed to be locked in place.
Aerodynamic stall and spin
A wing generates lift as a result of the pressure differential created by airflow over the wing’s surface. The angle between the incoming or relative air flow and wing chord is known as the angle of attack (AoA). As the AoA increases, lift increases up to a certain angle, known as the critical AoA. At this point, the airflow over the upper surface of the wing becomes separated. This condition is referred to as an aerodynamic stall (or simply a stall) and results in a significant loss of lift and an increase in drag. Due to the sudden reduction in lift from the wing and rearward movement of the centre of lift, typically an uncommanded aircraft nose-down pitch results. Most general aviation aircraft typically have a critical AoA of around 16°. This critical AoA can be exceeded at any airspeed, any (pitch) attitude and any power setting. However, a high AoA combined with a low airspeed most commonly results in a stall condition.
A spin can result when an aircraft simultaneously stalls and yaws.[3] The yaw can be initiated by rudder application (through manipulation of the rudder pedals) or by yaw effects from a range of factors that include aileron deflection, torque and engine/propeller effects. A spin is characterised by the aircraft following a downward, corkscrew path and requires significantly more altitude for recovery compared to a wings level stall (Federal Aviation Administration, 2021).
The Cessna Aircraft Company Pilot’s Operating Handbook stated that the stall recovery height for the Cessna 172N is 180 ft. The handbook also stated that the recovery height for a one‑turn spin is 1,000 ft.
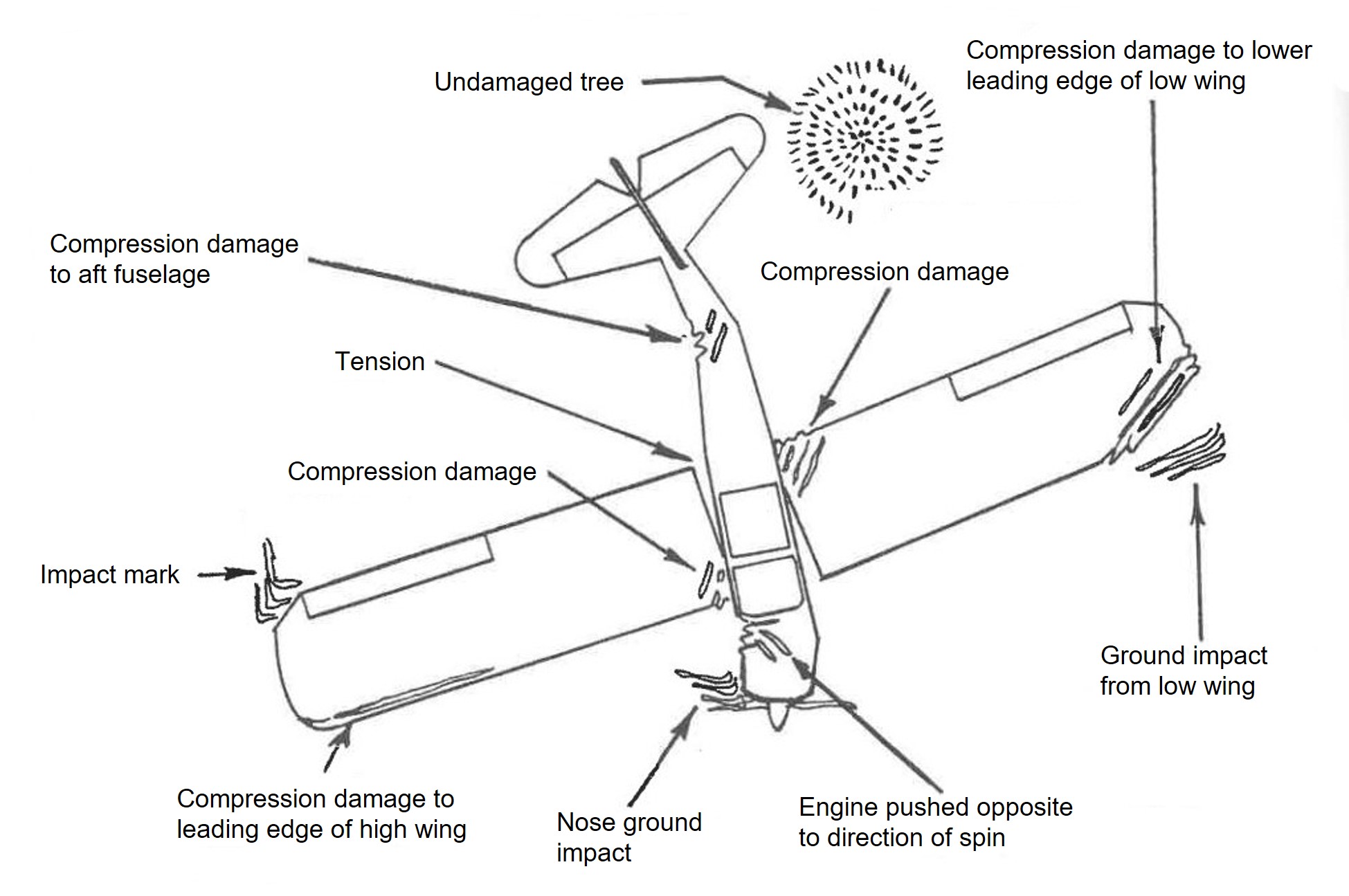
Wood and Sweginnis (2006), Aircraft Accident Investigation – 2nd edition, provides the following description of the wreckage from an aircraft that had spun into the ground, with reference to Figure 3:
There is little or no evidence of forward motion. Although the fuselage probably impacted at a steep nose down attitude, it is likely that there is evidence of a wing tip striking the ground before the nose. The down-going wing will normally strike the ground before the up-going wing, providing one clue as to the direction of the spin. Both the fuselage and the wings will probably have damage which reflects both a high sink rate and yaw. Tall thin objects on the ground, like trees and fence posts, are likely to penetrate the airplane almost from bottom to top, reflecting the almost vertical trajectory of the airplane. Undamaged objects may be found immediately behind the trailing edges, again indicating the vertical path of the airplane.
Figure 3: Example wreckage pattern from a spin
Source: Wood and Sweginnis (2006)
Aerial mustering operations and observations
General information
Aerial mustering is defined as the use of an aircraft to locate, direct and concentrate livestock. By definition, it is a hazard‑rich activity due to the inherent characteristics of the operation. Such hazards include manoeuvring at low-level, high workload, negative effects from weather, proximity to obstacles and the division of attention between flying and livestock management (Civil Aviation Safety Authority, 2015).
In addition to the aviation-specific definition for aerial mustering described above, in general terms, mustering livestock is usually a collaborative activity involving a ground-based team, typically using vehicles such as motorbikes, as well as personnel in the air, in either aeroplanes or rotorcraft. The role of the pilot in the overall mustering team could either be aerial spotting, or aerial mustering. The spotting role would involve the pilot searching for livestock and communicating their location to the ground team for them to round up. This is generally performed at a higher position and does not require the need to perform dynamic aircraft movements. This is somewhat different to aerial mustering, which, as defined by the Civil Aviation Safety Authority, would involve the intentional use of the aircraft to direct or concentrate the livestock. The ratings and endorsements a pilot had would limit which of these activities they could undertake.
Regulatory requirements
Since the introduction of Civil Aviation Safety Authority Civil Aviation Safety Regulations 1998 Part 61 in September 2014, an aeroplane aerial mustering endorsement was required to muster livestock with an aeroplane in Australia. Furthermore, an applicant for the aeroplane aerial mustering endorsement was required to hold a low-level rating with an aeroplane low-level endorsement. The mustering endorsement had additional elements and performance criteria to the low-level rating, which included demonstrating:
handling of the aeroplane up to the limits of the flight-manoeuvring envelope
coordinating and conducting an aerial mustering operation
an underpinning knowledge of critical operational conditions including aerodynamic stall and the safety hazards and risks of low‑level operations and methods of control.
To conduct aerial spotting a low‑level endorsement was required.
All aerial work operations in aeroplanes and rotorcraft are covered by Part 138 of the regulations. This includes operations that require an aerial work certificate as well as those that do not. However, if the aerial work is conducted over land owned or occupied by the person who is the registered operator of the aircraft or otherwise the owner of the aircraft, an aerial work certificate is not required. This is known as limited aerial work operations.
VH-SQO was owned by Jumbuck Pastoral and flying operations were conducted over their land.
Mustering observations
For the duration of the pilot’s time at Mulgathing Station, the pilot was observed by several staff members to have used a ‘dive‑bombing’ technique to muster sheep on multiple occasions. However, all staff members stated that they thought the procedure was normal operations for mustering and that the pilot was qualified to perform the activity. Following the accident, these staff became aware that the pilot was not qualified to conduct these aerial mustering manoeuvres.
Job application and role description
The pilot originally applied for a job with Jumbuck Pastoral at Bulgunnia Station, about 90 km east of Mulgathing. Although that application was not successful, Jumbuck Pastoral subsequently offered the pilot a similar job at Mulgathing Station. The job advertisement described the position as a pilot/station hand, stating that:
Your main duties while flying will be aerial stock mustering and supporting the crew on the ground during musters along with periodical property and stock inspections.
The qualifications required for the role were described as:
• Australian Commercial Pilots License (essential)
• Minimum 200 hours of total flying time (essential)
• Experience flying a Cessna 172 (essential)
• Low-Level Flying Endorsement (can be obtained if successful)
On 13 February 2025, in response to the draft report, the operator advised that the job description for the role involved aerial spotting only, to assist on‑ground mustering teams. It indicated that it had never required its aeroplane pilots to control or manoeuvre livestock directly. Instead, it relied on helicopter pilots for controlling stock movement when motorbikes could not be safely used on the ground for mustering cattle.
The operator also stated that the intention of the role was communicated to the pilot during their engagement with the company and the pilot was provided a copy of the Mulgathing Station Guide, which stated that:
Our mustering activities are supported by a Cessna 172 plane, with the pilot coordinating the muster below by relaying the location of stock in the paddocks. For those on 2-wheel motorbikes, stock visibility can be limited for a number of reasons, so having a pilot in the air assisting is an enormous help to ensure we muster paddocks cleanly and don’t leave any sheep behind. The terrain around the station can be tricky with a lot of rock, scrub and rough paddocks, so this is an added benefit.
Survival aspects
The aircraft impacted terrain with a 70° nose down attitude, which significantly compressed the liveable space within the cockpit. Injuries observed by first responders were consistent with those typically sustained from an aircraft accident. At the time of publication, the post‑mortem report was pending, however, the toxicology report indicated no presence of alcohol or drugs, and carbon monoxide[4] levels were also indicated to be within the normal range.
The pilot was not wearing a helmet at the time of the accident, nor were they required to. The pilot seat remained attached to the seat rails and was locked in a mid‑forward position. The pilot’s seat was fitted with a 3‑point lap‑sash belt and shoulder harness (upper torso restraint (UTR)). The pilot’s lap belt was reported to have been removed by the first responder to facilitate the pilot’s removal. The lap belt and clasp remained anchored to the floor and appeared to be in good condition. Inspection of the cockpit revealed that the UTR was stowed in the roof line.
When correctly worn, UTRs form an important part of the occupant protection system in aircraft, and the benefits in reducing the likelihood and severity of injuries is well established. A significant benefit of correctly fitted UTRs is the minimisation of body movement to prevent the body striking the aircraft structure in lateral and longitudinal impacts (Young, 1967). These findings are supported by research conducted by the United States National Transportation Safety Board (NTSB, 2011), which found that pilots who used lap belts only were nearly 50% more likely to be seriously or fatally injured compared with those who wore lap belts with UTRs.
With regards to the requirement for seatbelt usage in Australia, Civil Aviation Safety Authority Civil Aviation Safety Regulations 1998 Part 91.550 stated the following requirements:
• At all times during the flight, such a pilot must occupy a pilot seat, with the seatbelt [lap-sash belt] securely fastened.
• During take-off, landing or any other period that the pilot in command directs, each flight crew member required for the flight must occupy the flight crew member’s crew station with the seatbelt and shoulder harness securely fastened.
Safety analysis
Introduction
While mustering sheep on Mulgathing Station, South Australia, a Cessna Aircraft Corporation 172N, registered VH-SQO, was observed to dive towards a group of sheep before pulling out of the dive, rolling to the left, descending towards the ground and impacting terrain.
The wreckage examination found there were no defects or anomalies with the recovered components of the aircraft that might have contributed to the accident and the damage to the propeller indicated a power‑on impact. Additionally, there was no evidence indicating an adverse weather event or fuel issue. Pilot incapacitation was also unlikely given the pilot’s age, medical history, reported health prior to the flight and toxicological results.
This analysis will focus on the examination of the factors that led to the pilot losing control of the aircraft at low-level while attempting to muster sheep. It will also consider the job advertisement for the pilot position and the use of upper torso restraints.
Loss of control
The aircraft was observed diving from about 150–200 ft to approximately 50 ft above the ground then pitching up at about a 60° nose-up attitude to about 250–300 ft with no observed change in the engine power setting, before banking to the left and descending to the ground. While there can be limitations to witness recollections, the key points made by the witness were that the angle of climb was steeper than the angle of descent, and that the exit height was greater than the entry. These aspects were consistent with a loss of control during the exit of the dive. The steep climb‑out from the dive likely resulted in a rapid decay of airspeed and increase in the angle of attack that made the aircraft susceptible to a power‑on stall/spin situation. Furthermore, the onsite examination showed that the aircraft impacted terrain in about a 70° nose-down attitude with no forward momentum with both the engine and tail sections deflected to the right.
Both the observations made by the witness and the condition of the wreckage were consistent with the aircraft stalling and entering a left spin. The Pilot’s Operating Handbook indicated that this occurred at a height from which the stall and spin was not recoverable, resulting in the impact with terrain.
Pilot qualifications
In order to undertake the activity of aerial mustering with an aeroplane, both a low-level rating and aerial mustering endorsement were required, however, the pilot did not possess the latter. During their time at Mulgathing Station, the pilot was observed on several occasions to dive towards sheep in an attempt to move them. This manoeuvre is considered to be aerial mustering. On the day of the accident, the pilot declined assistance from a colleague on a motorbike, stating their intention to move the sheep with the aircraft and they were subsequently observed conducting this manoeuvre.
Low-level flying is a higher risk activity and aerial mustering adds further complexity and risk as the pilot must divide their attention between flying the aircraft, monitoring the livestock on the ground and the effects of their flying on the livestock. Not having the additional training and experience that would have come with the aerial mustering endorsement likely left the pilot ill‑equipped to manage the challenges associated with mustering sheep. As they were not instructed in the appropriate techniques for mustering, this placed the pilot at an increased risk of experiencing a loss of control at low-level.
Job application and role
The pilot applied for, and was awarded, the job described as being a pilot/station hand. The job advertisement stated that the main flying duties would be ‘aerial stock mustering’. As mentioned above, from an aviation perspective this meant that the pilot was required to have an aeroplane aerial mustering endorsement. However, the qualifications specified for the role did not include such an endorsement, nor did the pilot have one. Instead, the qualifications listed were consistent with the operator’s intention for the role of aerial spotting requiring only a low-level rating, which the pilot had. It was unclear to what extent, if any, the description of ‘aerial stock mustering’ influenced the pilot’s actions.
Despite this, from the time they started the role, up until the day of the accident, they were observed mustering sheep using manoeuvres that were outside the scope of their qualifications and the operator’s intentions. Furthermore, although these actions were witnessed by several staff at the station, including the station manager, none of the staff reported being aware that the pilot was not qualified to perform aerial mustering.
Seatbelts
The onsite inspection found that the upper torso restraint was stowed in the roof line indicating that it was not used by the pilot. Although the pilot was only required to use the lap belt at the time of the accident, the aircraft was fitted with an over the shoulder sash belt and the benefits of using them are well documented. However, in this case, given the extent of damage to the aircraft, it was unlikely the upper torso restraint would have contributed to the survivability of the accident.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving a Cessna 172N, registered VH‑SQO, near Mulgathing, South Australia, on 27 June 2024.
Contributing factors
While in a steep climb-out after diving towards sheep, control of the aircraft was lost leading to an aerodynamic stall and spin from a height that was not recoverable.
Although the pilot held a low-level rating, they were conducting aerial mustering operations without the related qualification. Consequently, the pilot was not appropriately experienced to manage the challenges likely encountered during aerial mustering.
Other factors that increased risk
The operator had advertised for a pilot to conduct ‘aerial stock mustering’ operations, but did not require the qualifications to perform that activity as their expectation was that the role would only involve aerial spotting.
The upper torso restraint part of the lap-sash seatbelt was not worn on the accident flight.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Jumbuck Pastoral
On 13 February 2025, Jumbuck Pastoral advised the ATSB that it has undertaken the following safety action:
A Safe Aerial Spotting & General Station Aviation Manual is in the process of being prepared.
Implemented a mentoring program for pilots, particularly at Mulgathing Station.
A safety audit has been conducted by an external third party. This is currently before the Board.
It is undertaking a full review of its operations to ensure compliance with the Civil Aviation Regulations 1988 and Civil Aviation Safety Regulations 1998, as well as the safety and training standards for pilots.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
Jumbuck Pastoral
South Australian Police Service
maintenance organisation for VH-SQO
accident witnesses.
Submissions were received from:
Civil Aviation Safety Authority
Jumbuck Pastoral
South Australian Police Service.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Lamb marking refers to husbandry procedures including tail docking, castration of males, ear tagging, mulesing, and vaccination.
[2]For training purposes, these manoeuvres were performed above 3,000 ft.
[3]Yaw: the motion of an aircraft about its vertical or normal axis.
[4]Carbon monoxide is a colourless, odourless, tasteless, and poisonous gas that is produced as a by-product of burnt fuel. Exposure to a leak from the exhaust of an aircraft engine into the cabin can lead to elevated levels of carbon monoxide, which can impair cognitive function.
Preliminary report
Report release date: 18/09/2024
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On the morning of 27 June 2024, the pilot of a Cessna Aircraft Company 172N, registered VH‑SQO, commenced sheep spotting operations at Mulgathing Station, South Australia (Figure 1). At about 0810 local time, a witness on a motorbike about 500 m away observed the aircraft dive down on what they presumed was a mob of sheep to an altitude of about 50 ft above the ground before climbing rapidly, turning to the left and then nosediving towards the ground. The aircraft was destroyed, and the pilot who was the sole occupant was fatally injured.
Figure 1: Accident location with reference to Coober Pedy and the Stuart Highway
Source: Google Earth, annotated by the ATSB
Context
Pilot information
The pilot, a New Zealand citizen, held a Civil Aviation Safety Authority Part 61 Commercial Pilot Licence (Aeroplane) with a single and multi-engine class rating with endorsements for retractable undercarriage, manual propeller pitch control, and low-level and instrument ratings. The pilot’s commercial licence was issued on 17 August 2023 in accordance with the Trans-Tasman Mutual Recognition Act 1997. The pilot held a Class 1 Aviation Medical Certificate with no restrictions, valid to 29 November 2024.
At the pilot’s last medical examination on 6 November 2023, the pilot reported having 251 hours of total aeronautical experience.
Aircraft information
VH-SQO was a Cessna Aircraft Company 172N 4-seat, single-engine, high (strut-braced) wing, all metal, unpressurised, fixed (tricycle) undercarriage aircraft. The aircraft was manufactured in the United States in 1978 and first registered in Australia on 29 August 1978. The operator had been the registered owner of the aircraft since the date of registry.
The current maintenance release was issued on 8 March 2024 and was valid until 8 March 2025 or 14,620.8 hours total time-in-service, whichever came first. At the time of take-off for the accident flight, the aircraft had accumulated 14,602.7 hours.
Meteorological information
Witnesses reported that on the morning of the accident, the weather was fine, clear and the temperature was cool, not cold. No wind or cloud cover was observed, and the conditions were described by a witness as being ‘almost perfect for paddock work’.
Wreckage examination
The ATSB’s onsite examination found that the aircraft impacted with terrain at about a 70° pitch down attitude, with ground impact marks directly under the nose showing no forward momentum (Figure 2). The aircraft’s flight controls and structure did not identify any pre‑existing faults or pre‑impact defects or failures. Additionally, one of the propeller blades showed significant rotational abrasion damage and chord-wise twisting indicating that the engine was driving the propeller under significant power at the time of impact.
Figure 2: VH-SQO accident site
Source: ATSB
Further investigation
To date, the ATSB has examined the aircraft wreckage, interviewed witnesses, and gathered electronic devices from the accident site. The investigation is continuing and will include consideration of the following:
evaluation of witness information
examination of the:
GPS device recovered from site
aircraft maintenance history
aircraft weight and balance, and performance
meteorological conditions
impact sequence and survivability
the conduct of similar flight operations
pilot qualifications, experience and medical information
regulatory requirements for fixed-wing aerial mustering.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Occurrence summary
Investigation number
AO-2024-037
Occurrence date
27/06/2024
Occurrence time and timezone
09:10 Australian Central Standard Time
Location
Near Mulgathing Station
State
South Australia
Report release date
01/05/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172N
Registration
VH-SQO
Serial number
17270255
Aircraft operator
Mulgathing Proprietary Limited
Sector
Piston
Operation type
Private
Activity
General aviation / Recreational-Aerial work-Agricultural mustering