
Final report
Report release date: 03/12/2025
Investigation summary
What happened
On the morning of 25 July 2024, 4 Robinson R22 helicopters were involved in a mustering operation at Mount Anderson Station, located about 51 km south-south-east of Curtin Airport, Western Australia.
The group planned to depart and travel together to the proposed muster location, about a 10-minute flight away. The lead pilot and another experienced mustering pilot departed first. Shortly after take-off, at about 150 ft, the helicopters departed controlled flight, collided with terrain and were destroyed. Both pilots were fatally injured.
What the ATSB found
The ATSB found that during the initial climb, while flying in close proximity, the lead helicopter manoeuvred to the right, and neither pilot detected their converging flight paths, which resulted in the midair collision. The ATSB found that the tools used by the operator to consider and manage operational risk were not tailored to their business. In the context of their primary flying activity of aerial mustering involving multiple helicopters, the risk of collision had not been identified in operational risk assessments, and the operator’s manuals did not provide documented procedures to ensure pilots establish and maintain adequate separation between helicopters.
The investigation also identified that company pilots were permitted to arrange their own separation based on personal preference. Pilots routinely flew with reduced vertical and lateral separation, and over time this became an accepted operating practice. Consistent with this practice, the pilots flew in proximity on the day of the accident.
While it did not contribute to the accident, the topics discussed in the morning brief were operational in nature and did not include elements of aviation safety risk such as separation. This represented a missed opportunity to establish a shared understanding of how the helicopters would be coordinated, which may have provided the pilots with a better understanding of what to expect, and how other pilots would be operating their helicopters.
What has been done as a result
Following the accident, the operator conducted a review of the operations manual and defined procedures for operations involving multiple aircraft and the conduct of operations in the vicinity of other aircraft. These changes were contained in a company notice to air crew (NOTAC) and all pilots were briefed on the changes prior to resuming flying operations. Additionally, a specific risk assessment for mustering operations was generated that included multi‑helicopter operations and considered the risk of collision.
Safety message
The regulations that govern CASR Part 138 aerial work activities are intended to provide operators with flexibility through scalable risk management practices.
For risk management to be effective, it must identify, assess and mitigate actual threats to a flying activity. Without consideration of the actual work being conducted, including commonplace activities, it is more likely that operational risks will not be uncovered, and risk management opportunities will be missed.
The ATSB encourages operators to review available guidance to assist with identification and management of hazards. For mustering operators, CASA provides a sample manual that includes sample acceptable procedures. Other resources such as the Flight Safety Foundation’s Basic Aviation Risk Standard for Aerial Mustering are a valuable resource to assist operator’s in coordinating aviation activities to manage and understand the aviation risk to their operation.
This occurrence also reinforces the fallibility of the see‑and‑avoid principle as the primary tool for identifying and managing the threat of collision. Defined separation minimums and pre-planned safe exits designed to provide opportunity to identify and respond to emerging collision threats would enhance the pilot’s ability to detect a conflict and recover from an unsafe condition. Additionally, airframe obstructions that limit the application of the see‑and‑avoid principle, in even the most open aircraft cabins, should be a consideration when establishing how aircraft should be positioned when flying in close proximity.
The occurrence
On the morning of 25 July 2024, 4 Robinson Helicopter Company R22 Beta II helicopters were being operated at Mount Anderson Station, located about 51 km south-south-east of Curtin Airport, Western Australia (Figure 1). The helicopters were operated by Pearl Coast Helicopters and were being used as part of a cattle mustering operation, which also included multiple land vehicles.
Figure 1: Accident location

Source: Google Earth, annotated by the ATSB
At about 0515 local time, a briefing was held by the lead pilot to cover the planned muster along a section of the Fitzroy River, a 10-minute flight to the west-north-west of the station homestead (Figure 2). This briefing was attended by the helicopter pilots and the head stockman, who provided input on where the ground crew would be located. The stated plan was for the helicopters to take-off one after the other and travel together to the muster location. Once there, the lead pilot would show the other pilots various locations before each pilot would peel off and work their section.
Figure 2: Planned muster location
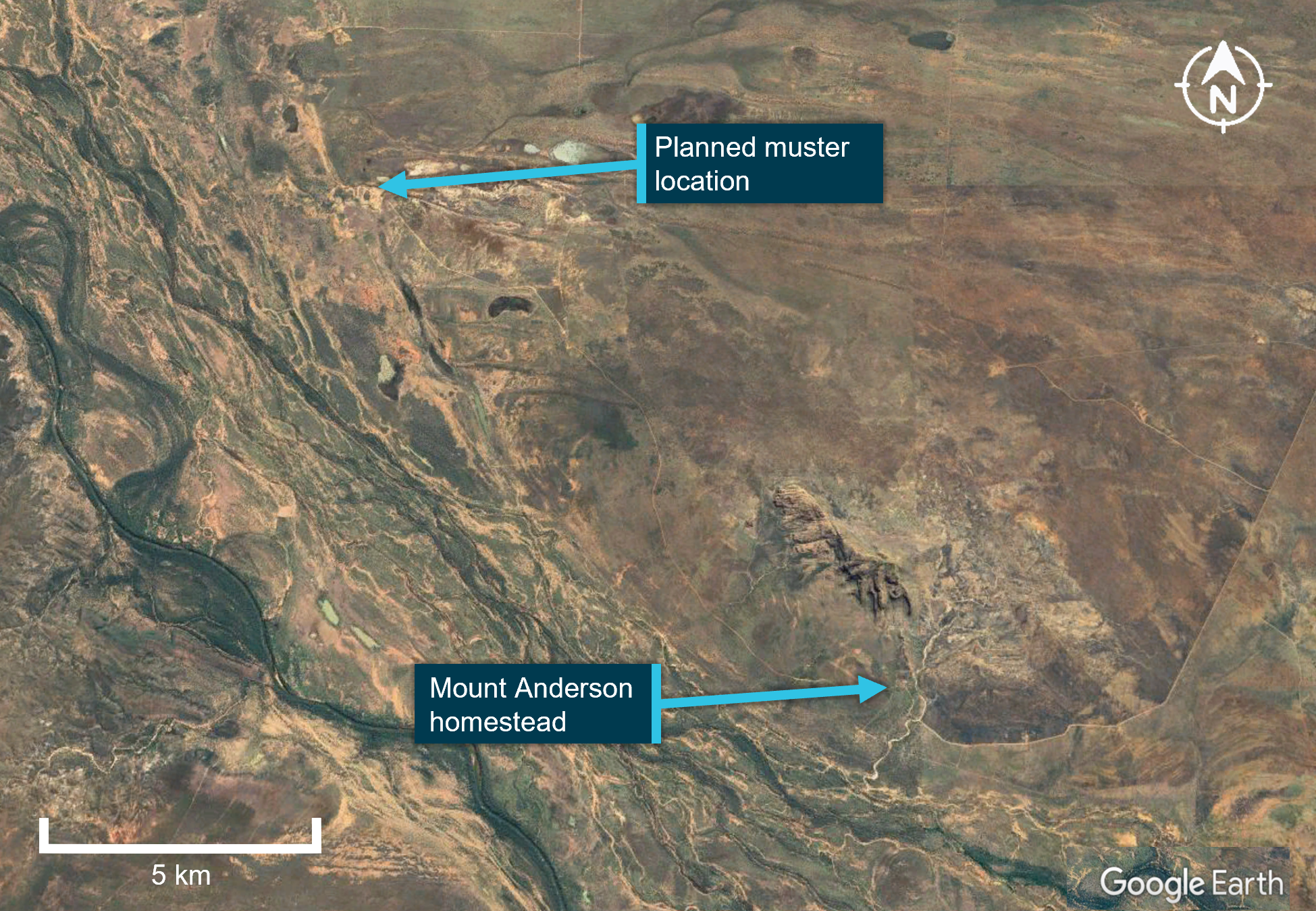
Source: Google Earth, annotated by the ATSB
At about 0540, the pilots commenced their pre-flight preparations. VH-HQH (Heli 1) and VH-HYQ (Heli 2) were parked in a grassed clearing behind the homestead (Figure 3). The other 2 helicopters, VH‑HMR (Heli 3) and VH-YKC (Heli 4), were parked about 400 m to the west. Heli 3 was parked on a small mound about 3 m high, and Heli 4 was parked about 20 m to the north-east at the base of the mound. Both aircraft were parked facing east towards the homestead.
The pilots started the helicopters just before 0600, and established communication with each other on a discreet company VHF radio frequency. The lead pilot in Heli 1 radioed they were ready to depart and would lead the group out. This radio broadcast was acknowledged by the pilots of Heli 2 and Heli 3. The pilot of Heli 2 replied that they were also ready and would follow the lead pilot. The pilot of Heli 4 did not have their flight helmet on at this time and did not hear these radio calls.
At 0603, Heli 1 (lead helicopter) and Heli 2 (following helicopter) departed the overnight parking area and flew west. The track to the planned muster took them past the location where the other helicopters were parked (Figure 3). The intention was for the remaining helicopters to join them as they flew past and the group would fly together to the muster.
A witness (witness 3) located near the stockyards about 200 m to the south of the homestead watched the 2 helicopters depart, climbing above the buildings with the following helicopter slightly lower and off to one side. They recalled that the helicopters were already established on the departure track, travelling about the same speed, and appeared to be close to one another when they first saw them.
Figure 3: Witness locations

Source: Google Earth, annotated by the ATSB
The pilot of Heli 3 observed Heli 1 and Heli 2 flying together off the right of their helicopter’s nose. They recalled that the helicopters were above the tree line to the east, slightly north of the camp kitchen at about 100 ft, moving from left to right in their windscreen and would have passed about 80 m south of where Heli 3 was parked. One helicopter appeared higher than the other, with the following helicopter slightly behind and off to one side. The pilot of Heli 3 recalled that they were probably closer than 100 m apart at this point, but it was difficult to be sure because the helicopters were silhouetted against the bright sky.
The pilot of Heli 4 was a few minutes behind in their own pre-flight preparations. The pilot recalled seeing the 2 helicopters approach from the east, but did not see a risk of collision at that point. The pilot of Heli 4 put on their helmet and established radio contact with the group. The pilot in nearby Heli 3 acknowledged the radio check and broadcast that they would lift into a low hover.
Both pilots were still on the ground and heard the pilot of Heli 1, the lead helicopter, acknowledge this radio transmission with the reply “Yep, I see you there”. The pilot in Heli 3 lifted into a low hover, focusing on the manoeuvre, and the pilot of Heli 4 turned their attention to their own helicopter before they heard Heli 1 and Heli 2 collide.
Witness 3 recalled that when the helicopters collided, they were partially obscured behind a tree but recalled that neither helicopter appeared to manoeuvre prior to colliding. After hearing the collision, the pilot of Heli 3 looked up and saw that Heli 1 was descending toward their location. Already established in the hover, the pilot manoeuvred the helicopter away to avoid being struck. The pilots of Heli 3 and Heli 4 advised that after the collision, Heli 1 maintained a generally straight track over the ground as it descended. Witnesses were unable to recall any details regarding the movement of Heli 2 following the accident. Several witnesses including the other helicopter pilots reported seeing smoke or flames as the helicopters descended.
As a result of the midair collision, both helicopters were rendered uncontrollable, collided with terrain and were destroyed. Both pilots were fatally injured.
Context
Pilot information
Both pilots involved in the collision were qualified and authorised to conduct aerial mustering operations.
Pilot of VH-HQH
The pilot of VH-HQH (Heli 1) held a commercial pilot licence (helicopter) with a low‑level endorsement and an aerial mustering endorsement. They had 6 years of aerial mustering operation experience and had been with the operator for 4 years. Their total flight time was 4,750 hours, with about 3,600 flight hours mustering, and about 4,250 flight hours in R22 helicopters. Their most recent flight review was a low-level single engine helicopter flight review on 1 April 2024.
The pilot held a class 1 aviation medical certificate that was valid until 20 March 2025. There were no medical conditions listed on their licence. A post-mortem examination identified no significant pre-existing medical conditions.
Pilot of VH-HYQ
The pilot of VH-HYQ (Heli 2) held a commercial pilot licence (helicopter), with a low-level endorsement and an aerial mustering endorsement. They had 4 years of aerial mustering operation experience and had been with the operator for 2 years. Their total flight time was 2,100 hours, with about 1,350 flight hours mustering, and about 2,000 flight hours in R22 helicopters. They had conducted a low-level single engine helicopter flight review on 30 March 2024.
The pilot held a class 1 aviation medical certificate that was valid until 21 February 2025. There were no medical conditions listed on their licence and a post-mortem examination identified no significant pre-existing medical conditions.
Aircraft information
The Robinson Helicopter Company R22 Beta II helicopter is powered by a 4‑cylinder carburetted piston engine. The R22 has 2 seats, with the pilot flying from the right seat, and each seat was fitted with a 3-point seatbelt and inertia reel shoulder strap, similar to those used in motor vehicles. The 2-blade main rotor assembly rotates counterclockwise when viewed from above.
Fitment of doors is optional (Figure 4) and it is normal for mustering operations to operate without doors. On the day of the accident both helicopters were operated without doors.
Figure 4: Exemplar R22 without doors

Source: ATSB
Both helicopters had a high visibility paint scheme on the upper surface of the main rotor blades (Figure 5).
Figure 5: High visibility main rotor blades

Source: ATSB
VH-HQH (Heli 1)
VH-HQH, serial number 3936 (Figure 6), was manufactured in the United States in 2005 and first registered in Australia in September 2005. The helicopter had undergone a periodic inspection along with a 2,200 hr / 12-year inspection and overhaul that was completed on 8 July 2024 at 6,087 hours total time in service. The maintenance release current at the time of the accident was not located, however, the operator reported the helicopter had accrued about 60 hours since the rebuild.
Figure 6: VH-HQH (left) and VH-HYQ (right)

Source: Helico
During this recent overhaul, HQH was fitted with several optional items including a carbon fibre console cover, carbon fibre battery box, and a smoker unit to aid in aerial mustering operations (Figure 7).[1] The smoker consisted of a small tank (about 5 L capacity), that was filled with either diesel or paraffin oil and mounted on the right-side lower frame.
Figure 7: VH-HQH smoker unit installation
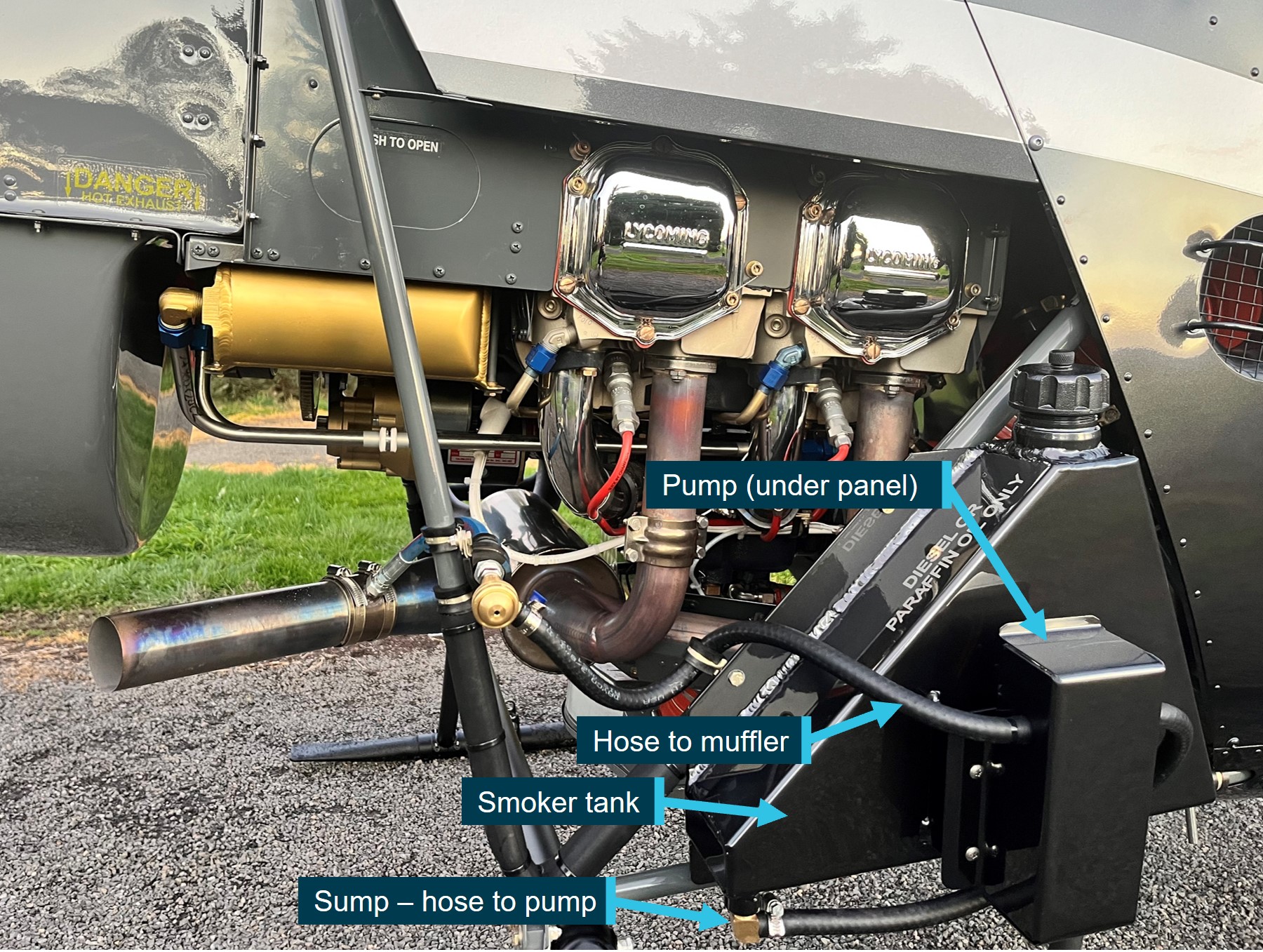
Source: Helico, annotated by the ATSB
VH-HYQ (Heli 2)
VH-HYQ (HYQ), serial number 3835 (Figure 6), was manufactured in the US in 2005 and first registered in Australia in May 2005. A 2,200 hr / 12-year inspection/overhaul was completed in April 2023. The most recent periodic inspection, at 4,946 hours, was conducted on 19 July 2024. The current maintenance release was not located, however, the operator reported the helicopter had accrued about 40 hours since the last periodic inspection.
HYQ was not fitted with a smoker unit.
Accident site information
Overview
The accident site was located about 400 m west-north-west of the Mount Anderson homestead at an elevation of about 42 m above mean sea level (AMSL). The small hill beyond the site had an elevation of about 80 m. Power to the property was produced via generator. There were some low powerlines immediately above the buildings, but the powerlines did not extend along or across the flight path (Figure 8).
Figure 8: View from departure point towards the accident site

Source: ATSB
The local vegetation was dry, low, open woodland and a flock of Cacatua sanguinea (Little Corella) were observed by the ATSB around the homestead during the onsite phase of the investigation. There was no evidence of any tree or wildlife strike in the vicinity of the start of the debris trail or among the wreckage.
Wreckage information
The first items in the debris field, about 300 m west-north-west of the take-off location, were consistent with a rotor blade strike to the right side of VH-HQH/Heli 1 (Figure 9), and consisted of:
- smoker unit pump cover panel
- smoker tank sump (separated horizontally from most of the upper portion of the tank)
- smoker unit lower mount
- fuselage skin from just forward of right position light
- right seat ‘pocket’ material section (located on forward panel of the pilot seat structure)
- trim from around the forward and right edges of pilot seat.
Figure 9: VH-HQH (pre-accident) showing approximate location of rotor strike and first items in debris field

Source: Helico and ATSB, annotated by the ATSB
The main debris trail was arranged in 2 key areas (Figure 10), in a north-westerly direction ending with the wreckage of Heli 1, and in a west-north-westerly direction, ending with the wreckage of Heli 2. The heaviest items of wreckage were found to have followed these general directions.
Kepert (1976) looked at wreckage trajectories to assist with fixed wing aircraft accident investigations. The research found that heavy items possess a high weight/surface area ratio and are little effected by wind drift with their trajectories depending primarily on the velocity of the aircraft at the time of break-up. With regard to heavy items including engines and batteries, the research identified the following:
Such items are generally recovered from points lying close to the line of the extended flight path of the aircraft. A mean line drawn through the ground impact points of heavy items will define the extended flight path of the aircraft with sufficient accuracy.
Kepert’s research must be considered in the context of a helicopter midair collision. While helicopters and their components can be subject to changes of trajectory when damage occurs while airborne, when considering heavier items of wreckage, the research provides a likely scenario for establishing flight path information. The flight path estimates for the accident are depicted as white dotted lines in Figure 10.
Figure 10: Debris field showing main areas of wreckage for each helicopter
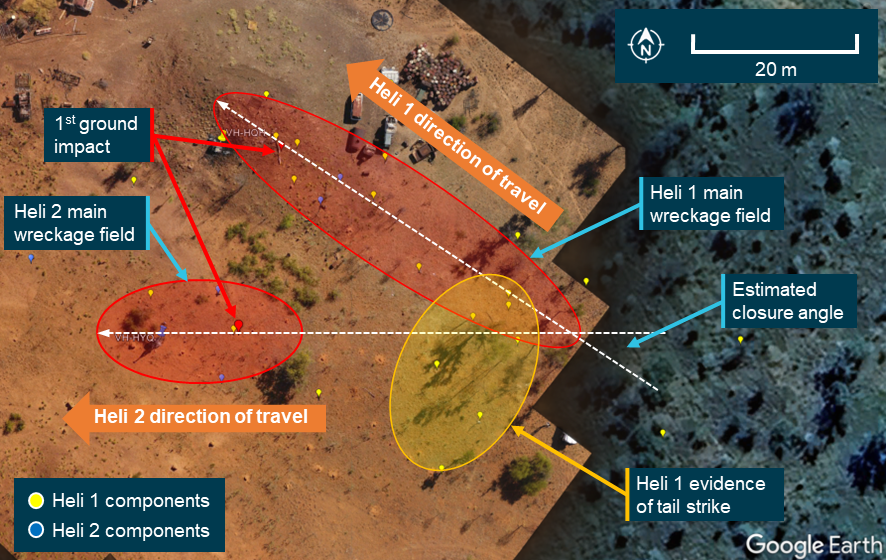
Note: The image does not show all items of wreckage identified in the debris field. Source: Google Earth, annotated by the ATSB
Wreckage examination of both helicopters identified all the major components were present at the accident site with no evidence of an in‑flight break-up prior to the midair collision. Heli 1 impacted the ground about 50 m to the west of the start of the debris trail, with Heli 2 a further 5 m west, and about 30 m to the south of Heli 1. Various components separated from the helicopters during the accident sequence, with fracture surfaces consistent with overstress.
Heli 1 was consumed by fire, contained within an approximate 6 m diameter. The fire damage to Heli 1 limited examination of the flight controls. However, though flight control tubes had been destroyed, security was established through observation that control tube rod ends were secured to identified controls and bellcranks.
Heli 2’s main fuel tank bladder was destroyed by impact forces, however there was no fire. The auxiliary fuel tank assembly was ejected, likely at the second impact with the ground. Its outer structure was impact damaged, however, the bladder remained intact. Flight control continuity of Heli 2 was established.
Samples of fuel taken from Heli 2’s auxiliary tank and gascolator were visually examined and noted to be clean and clear of visible debris. The samples were also tested for the presence of water, with nil indication. Further, all 4 helicopters had been using the same bulk fuel with no quality issues reported.
Loss of control following the midair collision
VH-HQH (Heli 1)
Distribution of tailcone and tail rotor driveshaft and control tube segments, along with yellow paint transfer, was consistent with multiple strikes from the helicopter’s own main rotor blades early in the accident sequence. Both teeter stops exhibited impact damage, from main rotor spindle contact with the mast,[2] coincident with extreme teetering of the main rotor assembly that resulted in the tailcone strike. Such excessive movement of the main rotor and loss of tail cone and tail rotor components would render the helicopter uncontrollable.
Heli 1 collided with terrain left side low and almost inverted about 50 m to the west of the start of the debris trail and came to rest a further 9 m west. The main rotor assembly and mast separated after colliding with terrain and were located adjacent to the ground scar.
VH-HYQ (Heli 2)
Examination of the wreckage identified signatures indicative of the engine providing power to a rapidly slowing main rotor assembly, including torsional distortion at mast fracture location, as would occur with Heli 2’s rotor contacting Heli 1. One main rotor pitch link was secured. The other main rotor pitch link had failed in overstress at the lower rod end. The pitch horn had also fractured due to overstress. Loss of continuity in either pitch link will lead to loss of control of the helicopter. The mast fractured, about mid length, with the main rotor assembly and mast fairing separating and coming to rest about 10 m southwest of the other helicopter’s main rotor. This was indicative of the mast separation occurring during or immediately following the contact with the other helicopter.
Heli 2 impacted terrain on its left side and slightly nose down, about 50 m to the west of the start of the debris trail, and about 30 m to the south of Heli 1. Heli 2 then came to rest about 10 m further west.
Survival aspects
Onsite examination identified the storage compartment under both seats in VH-HYQ were filled to volumetric capacity.[3] Once items were removed from under the right seat, distortion to the seat structure was evident. While this reduction in energy absorption may have contributed to some of the pilot’s injuries, the extent to which it influenced those injuries could not be determined.
Accident site inspection showed that both pilots were correctly restrained and wearing flight helmets at the time of the collision. However, the accident was determined to be unsurvivable.
Recorded information
Neither helicopter was equipped with a flight data recorder, tracking device or onboard camera, nor were they required to be.
Onboard recording devices
Two damaged Garmin aera 660 portable aviation GPS units recovered from the accident helicopters were transported to the ATSB facilities for further examination.
The GPS unit from Heli 1 was largely intact but showed signs of moderate fire damage. The memory board was installed in a donor chassis and a successful board-level data recovery was conducted.
The ‘current.gpx’[4] file had data from the day of the accident with 3 track points recorded, however, these were found to have been recorded while Heli 1 was on the ground. Timing data indicated that this was likely within one minute of the accident occurring.
Damage to the unit recovered from Heli 2 was consistent with something penetrating the device. As a result of that damage the memory chip was knocked from the board. The memory chip was not found, and no data could be recovered from the device.
Witness video
Video of livestock in a nearby yard was captured on a handheld device at the time of the accident. The video was 14.37 seconds in length and while it did not contain any footage of the helicopters, it did capture audio of the departure and the collision.
Spectral analysis of the audio determined the following:
- The ratios of the main rotor, tail rotor and piston firing frequencies throughout the recording are consistent with the helicopters operating at normal engine and rotor speeds prior to the collision.
- There are notable frequency changes from key helicopter components between 7 and 11.5 seconds in the audio recording, likely due to one of the helicopters starting to move away from the recording source.
- On the balance of this evidence, it is considered likely that prior to the collision, Heli 1 conducted a right turn while both helicopters were travelling at about 40 knots in a similar direction. After 3 seconds, Heli 1 likely stopped turning and continued on this path for another 1.5 seconds.
- Following the change in flightpath, the helicopters maintained this general orientation for about 1.5 seconds before high amplitude sounds and noises consistent with midair collision between the 2 aircraft were recorded.
- Following the collision, a higher pitched whirring sound was recorded, indicative of engine and/or drive components running in an overspeed condition.
Weather and environmental information
Weather
The site was remote and there were no official weather observations available. The nearest official data was obtained from Curtin Aerodrome located 51 km to the north‑west of Mount Anderson Station.
The aerodrome forecast (TAF)[5] issued at 0321 local for Curtin Aerodrome indicated CAVOK[6] conditions with a south‑east breeze (150°) around 8 kt (Figure 11). The TAF included a low chance of fog, however, this was removed in an updated forecast issued 15 minutes prior to the occurrence.
Figure 11: Terminal Area Forecast for nearby Curtin
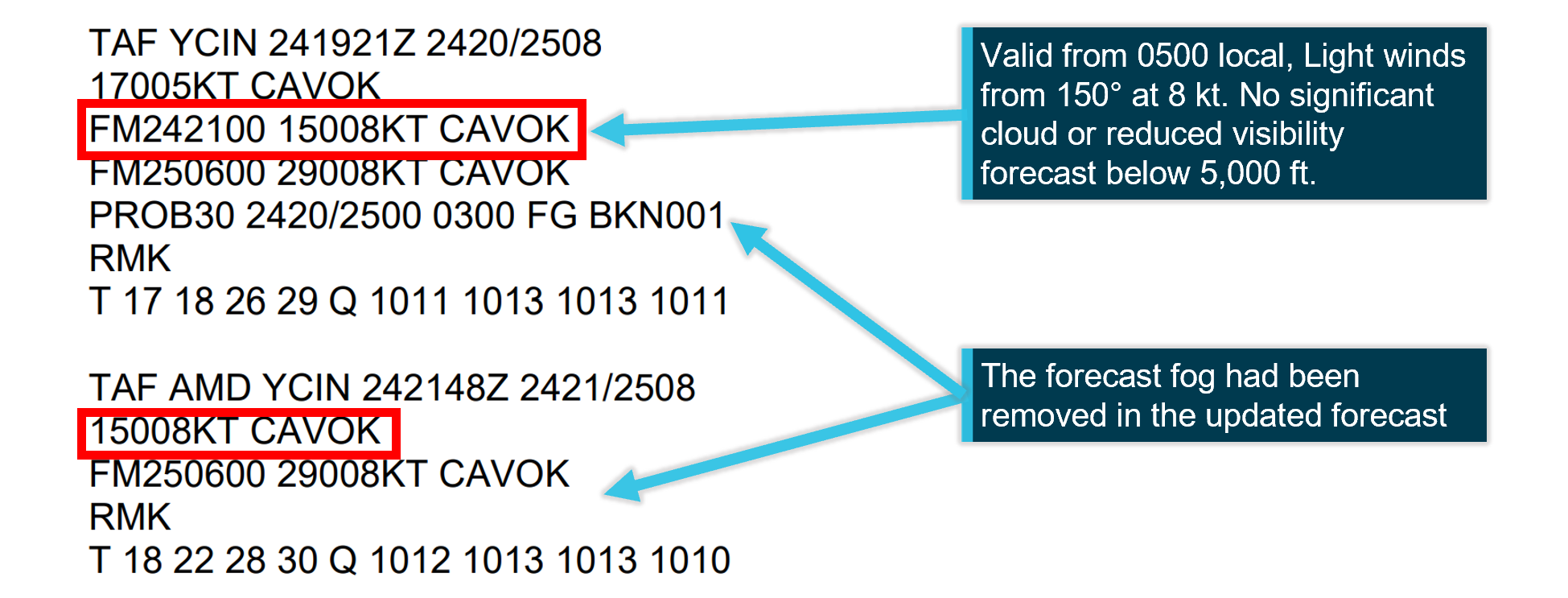
Source: Airservices, annotated by the ATSB
The meteorological aerodrome report (METAR)[7] for Curtin Aerodrome reported wind from the south‑east (130°) at 7 kt, visibility greater than 10 km and no cloud detected. There was no rainfall recorded in the previous 24 hours (Figure 12).
Figure 12: Meteorological aerodrome report for nearby Curtin

Source: Airservices
While the graphical area forecast (GAF)[8] that covered Mount Anderson Station and was valid at the time of the accident included isolated fog, witnesses and video recorded on the morning indicated there was no fog at the station.
Ambient lighting conditions
The Civil Aviation Safety Authority[9] defines daytime as the period between the beginning of morning civil twilight to the end of evening civil twilight. Geoscience Australia[10] states that in morning civil twilight, large objects may be seen but no detail is discernible.
Geoscience Australia recorded the first light at Mount Anderson Homestead at 0551 and sunrise at 0614. At the time of the accident (0603), it was civil twilight with the sun approximately 3° below the horizon. Witnesses to the accident recalled being able to see, however when looking east, objects were silhouetted against the light background and depth perception was diminished (Figure 13).
Figure 13: Witness video showing ambient lighting conditions

The image on the left is the view looking to the east in the direction of the rising sun. The image on the right is facing towards the south and shows the increased detail visible when not looking directly towards the east. Source: Witness video provided by Western Australia Police Force
It is likely that during twilight conditions, the greatest degradations will be in the ability to perceive detail and colour. This reflects physiological changes within the eye, where cone photoreceptors become more effective as light levels increase (Purves and others, 2001). Performance on visual tasks such as motion perception and the ability to detect larger environmental features such as the horizon are less affected. Liebowitz and Owens (1991) suggest:
During civil twilight visual guidance and spatial orientation functions may be carried out normally, but tasks for which contrast sensitivity, resolution, or reaction time are critical may be degraded or no longer possible.
Organisational information
General information
Pearl Coast Helicopters Pty Ltd (PCH) commenced operations in 2004 to provide aerial mustering services across the Kimberley region of Western Australia. At the time of the occurrence, it employed 6 pilots and operated a fleet of 8 Robinson R22 helicopters and 1 Robinson R44 helicopter.
PCH operated under a Civil Aviation Safety Regulations (CASR) Part 138 (Aerial work operations) aerial work certificate that authorised it to conduct dispensing, external load and task specialist activities, including aerial mustering. The PCH chief executive officer (CEO), who was also the head of flight operations (HOFO), reported that aerial mustering was the company’s primary business and accounted for about 95% of the flying conducted by the company. They added that approximately 70% of musters were flown with multiple helicopters and advised that the utilisation of multiple aircraft on a muster was consistent with industry practice.
Mustering operations
Aerial Mustering incorporates the use of aircraft, primarily helicopters,[11] to locate, direct and concentrate animals. It is conducted at low level (below 500 feet above ground level) and used to complement traditional animal management techniques using vehicles, horses and motorcycles. The operator reported that where large areas need to be covered, it is common practice to utilise multiple helicopters on a single muster.
Data published by the Bureau of Infrastructure and Transport Research Economics available in the CASA agricultural flying sector safety risk profile[12] showed that aerial mustering operators conducted 145,500 hours of flying in 2023. The data showed that for the period between 2014 and 2023, the average number of aerial mustering hours flown per year was 149,700 hours.
Transit to a muster
The accident occurred shortly after take-off during the transit to the planned muster. With respect to the transit to the area that the mustering activity will take place, there are 2 CASR rule sets that could apply. Certain Part 138 provisions disapply general operating and flight rules when aerial work is being conducted. The relevant CASA definition of flight is outlined in section 3 Interpretation of the Civil Aviation Act 1988 (CA Act) as follows:
flight means:
(a) in the case of a heavier than air aircraft, the operation of the aircraft from the moment at which the aircraft first moves under its own power for the purpose of taking off until the moment at which it comes to rest after being airborne
If the entirety of the flight was just to position the aircraft and no aerial work took place, that would be covered by Part 91 - General operating and flight rules. If a helicopter travels to site and begins aerial work activity such as mustering without coming to rest, the Part 138 rule set will apply.
Part 138 scalable risk management
The interactions of the general Part 91 rules and Part 138 are covered in CASA AC 138-01 v3.1 Part 138 core concepts. It contained the following explanation of how risk is considered when Part 138 alleviations are applied:
Recognising that the absence of certain Part 91 rules could result in a lower level of aviation safety assurance, Part 138 compensates by setting out a series of safety risk management processes that require an aerial work operator to manage the risks of their aerial work operations. The requirement to manage risk is fundamental to Part 138 and is achieved both directly within the legislation, for example, by specifying particular performance requirements for carriage of aerial work passengers at night, and by requiring an operator to conduct a risk assessment specific to their operations together with implementing procedures to mitigate the identified risks. These steps are designed to ensure that the operation is within the operator's capabilities and that it can be carried out safely.
This guidance outlines how the provisions of the regulations are designed to recognise the differences in organisational elements (structure, processes, flight activity) without reducing the safety margin of the operational risk assessments required. Operators that did not conduct ‘complex operations’ (defined in regulation 138.140) were not required to have a safety management system (SMS). CASA advised that mustering by day in VFR single piston engine helicopters would not be considered a complex operation and confirmed that the operator was not required to have a safety management system (SMS) as part of its manual suite. However, the operator was still required to consider its operational risk.
In lieu of this SMS requirement, Part 138 Manual of Standards Chapter 13 required operators wanting to conduct aerial mustering to consider hazards associated with the operation. PCH did this using safe work method statements (SWMS) to consider and manage their operational hazards (see Safe Work Method Statements).
In the context of an operator conducting mustering operations using multiple helicopters, the operator had to provide instructions in its operations manual for how additional risk associated with the use of more than one helicopter would be mitigated. This was not discussed in the operator’s SWMS.
Operations manual
Following CASA’s regulatory reform in 2021, there was a significant change in the regulations that applied to aerial work operators not conducting charter or air transport operations. While still required to comply with the requirements of Part 91 – General Operating and Flight Rules, under the new Part 138, aerial work certificate holders were able to scale risk management practices to meet the complexity of their aerial work activities. These changes necessitated significant changes to many operators’ existing manuals.
An operations manual for a Part 138 operator does not need to include the Part 91 general operating flight rules that are intrinsic to the operation of an aircraft. If the operator wishes to place additional obligations on its flight crew that exceeds the Part 91 requirements, the operations manual must contain these instructions. For example, regulation 91.265 prescribes the pilot in command responsibilities for minimum height rules over populous areas.[13] If the aerial work activity requires the pilots to fly lower or closer than the Part 91 regulations specify, then additional instructions must be provided to flight crew.
Management of the manual
The CEO advised that a third party was contracted by PCH to produce an operations manual (OM) that was compliant with the new regulations. The author of the manual advised the ATSB that there was no ongoing contractual obligation for management, update or oversight. The expectation was that the ongoing oversight and updating of the documents would be the responsibility of the operator which would tailor the basic elements to its operation.
Following the initial issue of the new OM in July 2022, the manual update history showed updates in March 2023 to capture a change of CEO; and June 2024 in response to a CASA surveillance audit.
Management of risk
Safe Work Method Statements
To comply with the risk-based approach of the Part 138 regulations, a collection of Safe Work Method Statements (SWMS) was generated as part of the new manual. The use of SWMS to manage risk was adapted from other industries based on information available from CASA at the time. These were in essence, standalone risk assessments for the operator’s flying activities that were not part of an integrated SMS. The author advised that SWMS were also used by other operators conducting similar flying activities in Western Australia.
The HOFO and company pilots recalled during interview that the SWMS were the company’s primary risk assessment tool and they referred to these documents to identify hazards and manage threats for all flying activities.
Update history
A review of the operator’s master forms register showed that version 1 of the SWMS published in July 2022 were current at the time of the accident. The register contained the following SWMS:
- General operations
- Stock and feral animal control
- Powerline inspection
- Incendiary
- Underslung load.
Notably, there was not a specific SWMS available for mustering. The HOFO advised that they had been developing a mustering SWMS, but it had not yet been incorporated into the operations manual at the time of the accident.
Operational risk assessments
The HOFO advised that they referred to the general flying SWMS for their mustering risk assessments but did not produce risk assessments for each muster location. The HOFO would then provide a brief to the lead pilot including a general overview of the property and the areas to be mustered. Following the initial brief, the lead pilot would then assume control of the muster and brief the other pilots and ground crew on the plan for the muster.
The HOFO maintained oversight of the muster by remaining in contact with the lead pilot throughout the day. If the lead pilot had any questions for the HOFO, or the nature of the muster changed, the HOFO was contactable via satellite phone and daily check-in calls at the end of the day.
Mount Anderson HLS
The operator held a helicopter landing site (HLS) register,[14] but because Mount Anderson Station was not visited often, there was not a dedicated plate in the register. However, the lead pilot had previously operated out of Mount Anderson. The HOFO considered the lead pilot to be very experienced and familiar with the area.
Operational information
Operator’s procedures
General flying separation and minimum heights
Section 2 of the OM outlined each pilot's responsibilities around separation and avoiding a collision. The manual required the pilots to 'maintain a constant look-out at all times' and 'refer to SWMS' for further risk mitigation practices. Elsewhere, the manual required pilots to make use of the radio and helicopter lighting to increase visibility.
The company procedures for aerial work activities were contained in part 6 of the OM. The operator’s procedures noted an exception to the standard 500 ft vertical and 300 m lateral separation standard for helicopters operating over unpopulous areas in CASR 91.267. The relevant set of conditions that were required to disapply the normal minima were as follows:
All of the following apply:
a. The pilot in command of the aircraft is authorised under Part 61,[15] or holds an approval under regulation 91.045, to fly the aircraft below the height mentioned in paragraph (2)(a);
b. The pilot in command of the aircraft conducts a risk assessment of the area to be flown over;
c. The point on the ground or water vertically below the aircraft is not within 150 m of a person, vessel, vehicle or structure or of livestock.
Unless all of these conditions were met, the OM required pilots to adhere to the standard Part 91 rules.
Mustering brief
The task specialist activity of aerial stock mustering was covered in part 6 of the OM. The procedures identified threats to be managed including obstacles on the ground, weather and fatigue. Based on the content of the OM, the manual did not contain procedures relating to the use of multiple helicopters and there was no requirement to conduct a separation briefing.
A Flight Safety Foundation article on effective briefings[16] outlined that an effective briefing should seek to establish a common mental model between participants with an agreed understanding of key aspects of the proposed flight. These should include:
- defining how the flight will be conducted
- objectives
- route
- spacing between aircraft and responsibilities for its continued application
- how unplanned changes will be managed
- what communication will be provided and when
- unexpected events and criteria indicating the flight is not proceeding as planned
- a corrective action plan to either restore or abandon the proposed flight
- other aspects identified during the activity risk assessment.
Standard practice
Pilots advised that morning briefings were led by the lead pilot and covered operational aspects with the lead pilot often referring to topographical maps or OzRunways to point out significant locations and landmarks.
Elements typically covered in the morning brief included:
- where the stock were located
- how many head of stock there were likely to be
- in which direction the muster should go
- the location of fences, yards, windmills and any specific reference points such as hills, and powerlines etc
- any hazards or obstacles in the area to be operated in
- location of fuel and that the refuelling point is suitable for landing and taking off.
Company pilots and the HOFO stated that separation was not usually discussed in the briefing.
While the OM did include a dedicated section on collision avoidance, the OM did not include instructions on what the operator considered acceptable separation. Besides requiring pilots to ‘maintain a constant look-out at all times’, there were no instructions on how separation should be maintained. The expectation was that pilots would arrange their own separation once airborne.
Pilots reported that the improvised application of reduced vertical and lateral separation became a common and widely accepted practice, and limits varied between pilots. In the absence of formal separation minimums, the accepted practices employed by the pilots became standard operating practice. The HOFO and company pilots stated that this was typical of how mustering operations were conducted.
Flight conduct on the day of the accident
The HOFO advised that it was normal for company helicopters to arrange a departure sequence prior to take-off and then depart together and travel to the muster as a group. Pilots advised that the sequencing was arranged over the radio on the morning of the accident, and there was nothing unusual about how the group were preparing to depart.
The use of airframe strobe lights and anti-collision lighting were intended to support see‑and‑avoid by attracting the attention of a pilot looking for other aircraft. While the pilots did not recall seeing the strobe lights on the accident helicopters, they recalled having their own lights on, and believed that the other pilots would also have their lights on, having routinely observed the other pilots fly with the strobes on.
Undocumented risk controls
The operator had identified certain risks associated with mustering activities and had developed practices to mitigate the risks. However, some of these were not published in the OM or SWMS.
The operator had implemented a practice that utilised GPS lines between locations as demarcation of operational boundaries. This was used when more than one helicopter was operating in the same location to alert pilots to the potential for conflict with a helicopter in the adjoining area.
In support of the use of these virtual boundaries, radio calls were required when operating near the perimeter of an area to increase awareness among pilots. Company pilots reported use of this practice and the HOFO stated that this method of separation had been effective for many years on musters involving up to 5 helicopters.
Visibility
The limitations of the see‑and‑avoid principle as the primary means of conflict detection are well understood and covered in numerous ATSB investigations and the ATSB research report
. While the rate of midair collision during mustering is very low, with the ATSB Aviation Occurrence Database showing about one mustering midair collision every 10 years for the past 20 years, the risk of a collision increases with the introduction of additional aircraft and collision pairs.[17]
R22 cockpit visibility
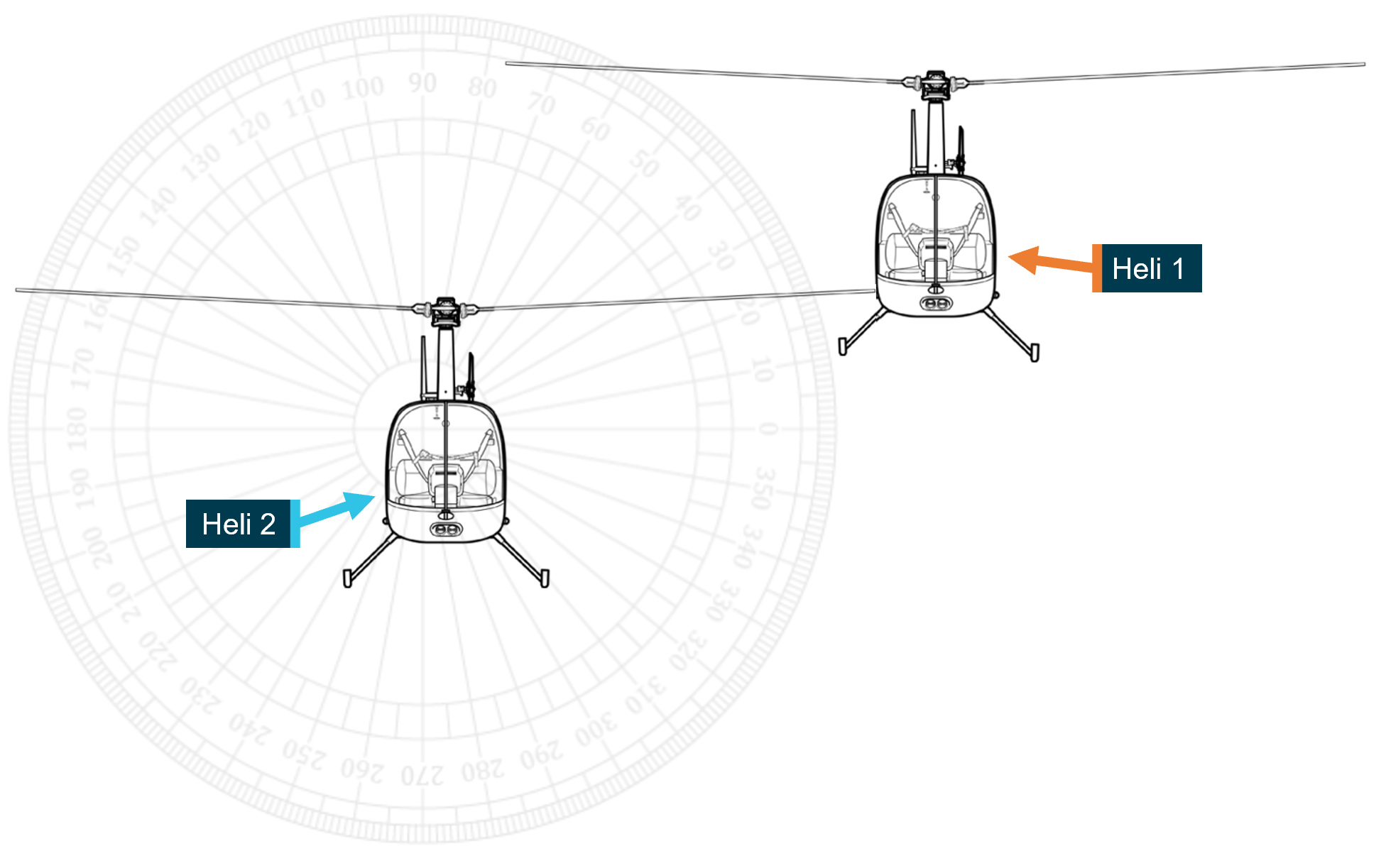
Based on the wreckage examination and the location of the Heli 2 main rotor strike to Heli 1, the approximate relative lateral position of each helicopter was calculated (Figure 14).
Figure 14: Approximate relative positions of Heli 1 and Heli 2 at the point of collision
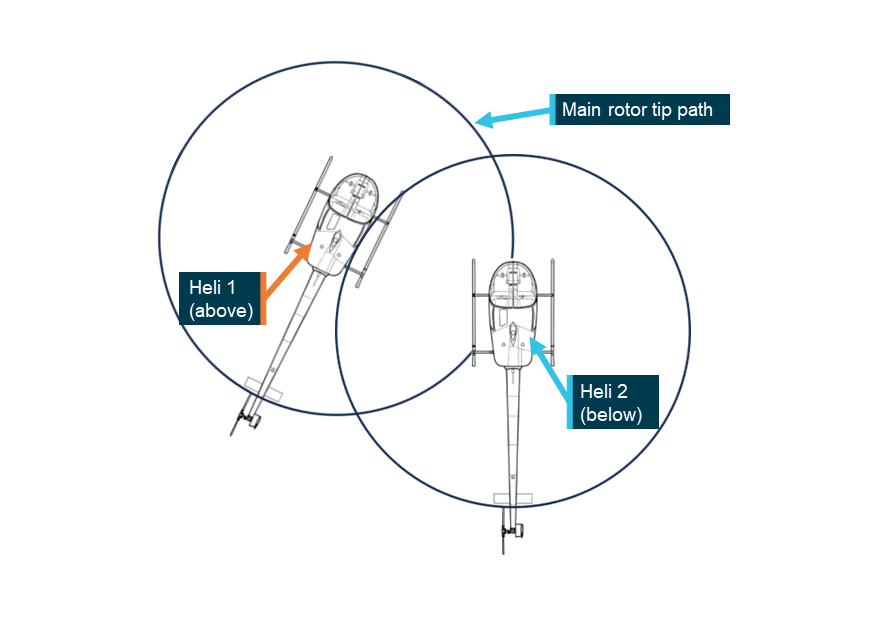
Source: ATSB
Similarly, based on the main rotor strike location on Heli 1, the vertical orientation of the aircraft was estimated in Figure 15.
Figure 15: Approximate vertical orientation of Heli 1 and Heli 2 at the point of collision
Source: ATSB
Due to the lack of available flight path and aircraft body angle information it was not possible to complete a full visibility analysis from both aircraft. However, it was possible to demonstrate the limitations to visibility presented by the R22’s cockpit by using a cockpit mask from the pilot’s perspective (Figure 16). Refer to Appendix A – Visibility and R22 exemplar cockpit mask for more detail.
Figure 16: Equirectangular cockpit image of exemplar R22

Source: ATSB
The image was overlaid with a grid to indicate the viewer’s eye position as azimuth and elevation angles from the centre of the view. As the eyes were moved upwards and to the left, so too would these boxes (Figure 17). The cockpit mask shows that although visibility is generally very good out the front of the cockpit, obstructions to line of sight exist above and to the left of the helicopter.
Figure 17: R22 generic cockpit mask
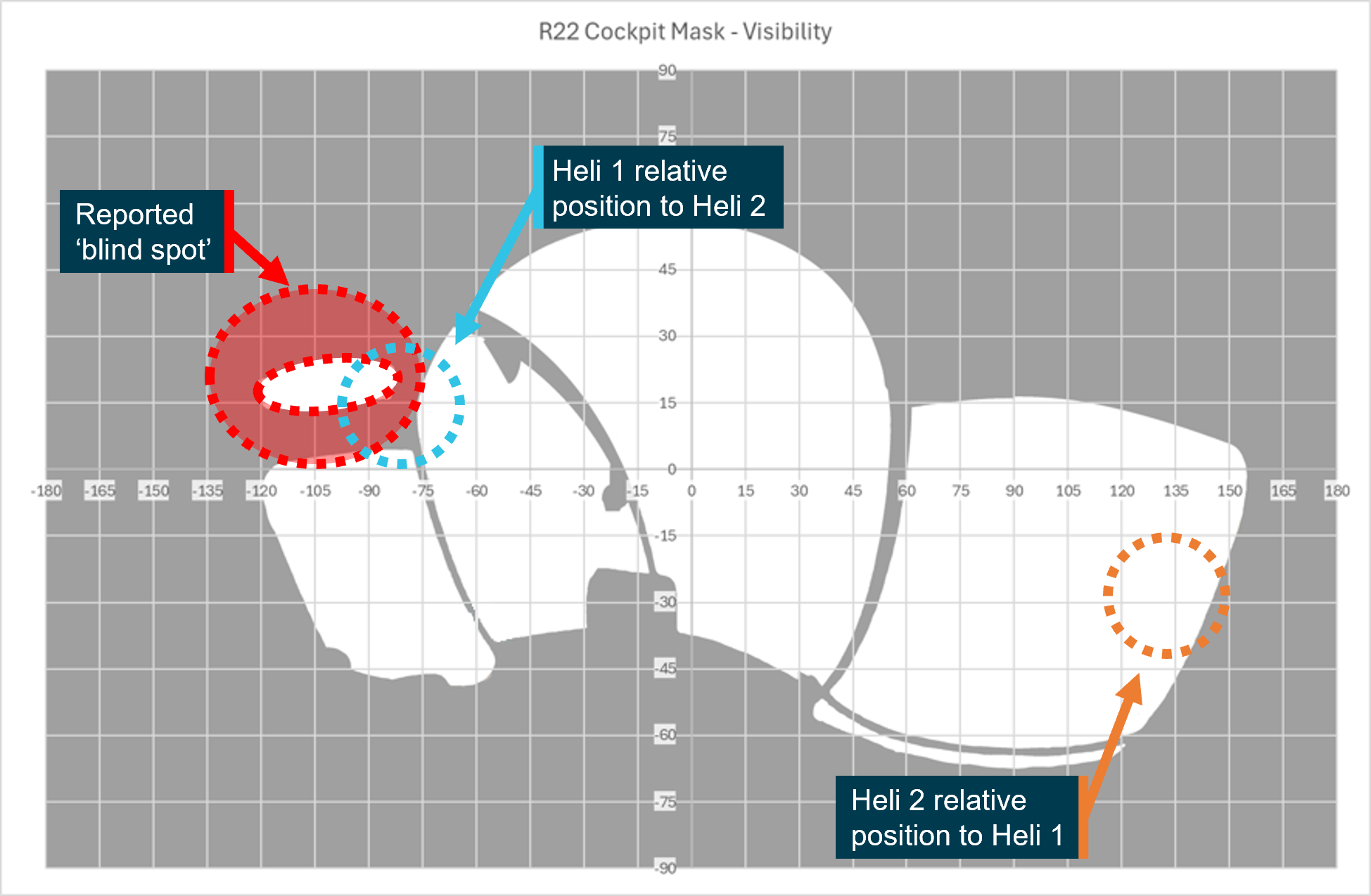
The blue and orange circles represent the approximate location of the other helicopter at the time of collision. Source: ATSB
For visual detection to be effective, a target must be visible. That is to say it must be, large enough, unshielded, conspicuous, in a location where it is likely to be seen and, detectable against the background.
The operator and other pilots referred to the presence of a ‘blind spot’ above and to the left of the R22 from the pilot’s seat (Figure 17). This is relevant when considering the opportunity available to the pilot of Heli 2 to detect a conflict in this direction.
For the pilot of Heli 1, although the relative position to Heli 2 is unshielded, that position, at about 135° from centre, is behind the pilot.
Regulatory oversight
CASA employs a surveillance schedule to ensure a consistent level of oversight of industry to address compliance issues. Operators, or authorisation holders,[18] are assigned to a surveillance group based on their risk profile which considers the risk to safety posed by their flying activity.
PCH was assigned to a group with aerial work certificate holders that did not have a training and checking manual or SMS. The surveillance schedule required one surveillance event focusing on core scope items every 5 years.
Previous ATSB investigations have noted that regulatory oversight processes will always have constraints in their ability to detect problems. There is restricted time and limited resources available for these activities. Regulatory surveillance by CASA is therefore a sampling exercise and cannot examine every aspect of an operator’s activities. The CASA audit schedule seeks to address this limitation by scheduling different types or levels of surveillance over the approval period of an aerial work certificate.
Surveillance
Recent activity
In April 2023, a change of PCH’s CEO triggered a formal review of the organisation’s operations manual finalising the transition to Part 138. A systems level, or level 1 audit was conducted in January 2024. Systems audits are based on a defined scope that references mandatory planning and scoping development documentation. They consider the specific activities conducted by an operator, ensuring their compliance with regulations and the suitability of operators’ systems to manage their flying activities. Additional items can be added by the lead auditor. None were added to the scope of the audit conducted in January.
Findings
Incomplete procedures and plans to safely conduct operations were identified by CASA during the January surveillance event. The operator made the required changes to its manual, and all findings were acquitted in May 2024.
While the surveillance activity identified areas where improvements could be made, it did not identify that separation procedures for operations involving multiple helicopters had not been specified. Considering the low likelihood of this type of accident in the mustering sector, the attention of the surveillance team was probably focused on other areas of the operator's activities.
Post‑accident review
Following the accident, CASA conducted a review of the operator’s procedures manual and issued a safety alert to PCH after it was identified that the OM and SWMS did not provide adequate assessment of the risk, nor sufficient guidance, regarding lateral or vertical separation to pilots when conducting multi‑helicopter operations. The operator reviewed and updated its operations manual (see Safety issues and actions section). This finding was acquitted August 2025.
Related occurrences
The ATSB reviewed 7 investigation reports which involved 2 or more aircraft colliding midair while working together (Table 1). Most of the accidents were fatal. All took place in visual meteorological conditions, and almost all involved a breakdown of see‑and‑avoid as a control for preventing midair collision. Across the investigation reports there are common findings around briefings, planning and procedures.
Table 1: Investigation reports concerning midair collision between aircraft working together
| Agency | Number | Table header |
| NTSB (US) | AAR-09/02 | Midair Collision of Electronic News Gathering Helicopters KTVK-TV, Eurocopter AS350B2, N613TV, and U.S. Helicopters, Inc., Eurocopter AS350B2, N215TV Phoenix, Arizona July 27, 2007 |
| ATSB | AO-2008-010 | Mid-air collision 53 km NNW of Gascoyne Junction, WA 13 February 2008 VH-OUS Piper Aircraft Corporation PA-18 Super Cub VH-ZDP Robinson Helicopter Company R44 Raven |
| ATSB | AO-2009-018 | Mid-air collision - 15 km SE Springvale Station, WA, 5 May 2009, VH-PHT, Robinson Helicopter Company R22 Beta II, VH-HCB, Robinson Helicopter Company R22 Beta II |
| JIAAC (Argentina) | 088/15 | Mid-air collision LQ-CGK / LQ-FJQ Villa Castelli, Province of La Rioja 9 March 2015. |
| AAIB (UK) | EW/C2017/09/05 | North American P-51D, Mustang, G-SHWN and North American P-51D-20 (Modified), Mustang, G-BIXL 23 September 2017 |
| ATSB | AO-2023-001 | Midair collision involving Eurocopter EC130 B4, VH-XH9, and Eurocopter EC130 B4, VH-XKQ Main Beach, Gold Coast, Queensland, on 2 January 2023 |
| ATSB | AO-2023-057 | Mid-air collision involving SIAI Marchetti S-211s, VH-DZJ and VH-DQJ 25 km west of Tyabb Airport, Victoria, on 19 November 2023 |
Risk management and planning was highlighted in JIAAC report 088/15. It reported that there was no formal assessment of the risks of operating in close proximity, and no plans for loss of visual contact were in place, such as performance of an evasive manoeuvre. It stated that 2 of the contributing factors were:
Lack of a formal assessment of the safety risks for an unusual operation (filming and flight in proximity), which prevented the identification and analysis of the dangers inherent to that operation.
and
Deficiencies in the operation planning that led to the accident, including the failure of observing the “see and be seen” concept or an evasive maneuver if visual contact is lost between both aircrafts.
Four of the reports (JIAAC 088/15, ATSB AO-2008-010, AO-2023-001, NTSB AAR‑09/02) found that a lack of procedures to support operations with multiple aircraft contributed to the midair collisions. They note that providing procedures specific to the operation would support maintenance of separation and assist pilots to maintain awareness of each other. ATSB investigation report AO-2008-010 found that:
There were no formalised operating procedures detailing the conduct of multiple aircraft culling operations, including the assurance of aircraft separation, that would have assisted the pilots to maintain separation from each other.
ATSB report AO-2023-001 stated:
…documented procedures for communication between inbound and outbound helicopters were not specific to their usual operation and location, and permitted a reactive model of separation, increasing the likelihood that an outbound pilot would not form awareness of relevant traffic.
Pre-flight briefings between pilots were also raised in 2 of the reports. ATSB AO‑2023‑057 found that a manoeuvre conducted had not been briefed on the ground prior to departure and an in-flight discussion did not allow for full consideration of the risks associated with it. AAIB EW/C2017/09/05 stated that while a brief was conducted it did not focus on the whole operation and contributed to an incorrect recall and subsequent incorrect joining manoeuvre when operating in formation.
Together, the investigation reports highlight the risk of midair collision between aircraft, often from the same company, operating in close proximity. The findings highlight the importance of managing the risks of operating multiple aircraft in close proximity to each other and show that pre-prepared proactive methods of separation and deconfliction should be briefed and available to pilots prior to commencing flight. They show that sound operating procedures can support pilots and help ensure that multi-aircraft operations are managed to safe outcomes.
Guidance material
In addition to the acceptable means of compliance and guidance documents produced by CASA, there are a number of other resources available to assist mustering operators to develop the procedures contained in their manuals.
CASA Sample Part 138 OM
CASA published a Part 138 sample operations manual (Mustering). This sample manual contains guidance on content and examples of acceptable procedures for operations using multiple helicopters and separation.
Basic Aviation Risk Standard
The Flight Safety Foundation’s Basic Aviation Risk Standard (BARS) is a suite of risk‑based aviation industry standards with supporting implementation guidelines. The standards are developed by the industry and contracting companies and based around the specific risk these operations face in their day-to-day aviation activities.
The Aerial Mustering Standard is presented in a risk-based format to emphasise the relationship between threats to aerial mustering operations, associated controls and recovery measures. It has been designed to be used as a primary reference tool for aerial mustering operators and contracting companies to manage and understand the aviation safety risk in their operation.
Safety analysis
Introduction
On 25 July 2024, 4 helicopters were involved in a multi‑helicopter mustering operation along the Fitzroy River, about 13 km north-west of the Mount Anderson Station near Curtin, Western Australia. The pilots of 2 Robinson R22 helicopters, VH-HQH (Heli 1) and VH‑HYQ (Heli 2), departed from a clearing behind the homestead to track initially to the west where they would be joined by the 2 other helicopters before following the river to the muster. Shortly after take-off, at a height of about 150 ft, the 2 helicopters collided resulting in an immediate loss of control. Both aircraft collided with terrain and the pilots were fatally injured.
No evidence of pre-existing mechanical defects were found with the helicopters. Additionally, there was no evidence that either helicopter had struck flora, fauna or a wire prior to the collision. The smoke that was observed from the lead helicopter immediately following the collision was likely due to the damaged smoker tank spilling diesel onto the hot engine and exhaust after it was struck by the main rotor of the following helicopter.
This analysis will discuss the:
- pilots’ awareness of the other helicopter prior to collision
- briefing that was conducted prior to the flight
- typical separation employed by company pilots
- operator’s standard operating procedures and management of operational risk.
Collision detection
Estimated flight path prior to collision
A witness reported that the helicopters were travelling in a similar direction and at a similar speed to one another prior to the collision. Wreckage examination revealed that when the helicopters collided, they were almost alongside each other in an attitude consistent with level flight, with Heli 2 being about 2 m behind and about 2.5 m lower. This was not consistent with the agreed sequencing that Heli 2 would follow Heli 1 out.
The pilot of Heli 3 reported the last sighted track of Heli 1 and Heli 2 was of them passing about 80 m south of where Heli 3 was parked, closer than 100 m apart. This meant that prior to the collision, they were probably established on a parallel west-north-west track (about 285° magnetic) from the overnight parking area.
Environmental considerations
The twilight conditions should not have impacted the pilot of Heli 2, given Heli 1 was higher and set against the sky. The conditions would have an uncertain effect on the pilot of Heli 1 who would need to observe Heli 2 against the background consisting of terrain and vegetation. There was no reason to suspect the helicopters were not utilising standard position indication (conspicuity) lighting, which would also mitigate that effect. Additionally, while both helicopters were fitted with high-visibility paint schemes on the main rotor blades to increase conspicuity, the contrast against the background in the morning light could not be determined.
Audio analysis
Audio analysis of video recorded at the time of the collision (that did not include footage of the helicopters) showed that prior to the collision, a notable reduction in frequency was observed from one source. As the helicopters were established to be operating normally, this frequency change was consistent with one of the helicopters manoeuvring away from the microphone of the recorder at a greater speed. As the helicopters were moving from right to left relative to the microphone, likely at similar speeds, this was most likely due to one of the helicopters turning right.
Based on the relative position of Heli 1 being in front of Heli 2, the turning helicopter was almost certainly Heli 1. On the balance of evidence, this change established the helicopters on converging flightpaths. About 2 seconds after the completion of the turn, audio analysis showed sounds consistent with the collision between Heli 1 and Heli 2.
Wreckage trajectory
Following the midair collision, witnesses observed the helicopters descend on different trajectories. The main debris trail was arranged in 2 key areas. Each consisted of the heaviest components for each helicopter (except the main rotor of Heli 2 which detached at the point of collision or immediately thereafter). Based on the wreckage trajectories from the estimated point of collision, the helicopters were likely maintaining different tracks at the point of collision.
Conflicting traffic undetected
Shortly prior to the midair collision, the pilot of Heli 1 was communicating with Heli 3 and Heli 4 on the ground. It is plausible that the pilot of Heli 1 was looking towards the helicopters at this time, focused ahead and to the right of the helicopter with the expectation that Heli 2 would have been behind.
Additionally, the pilot of Heli 2, operating slightly lower than Heli 1, may also have looked towards Heli 3 and Heli 4 on the ground. Heli 3 and Heli 4 were preparing to lift, and the pilot of Heli 2 may have needed to assess a potential risk of collision. For the pilot of Heli 2, the helicopters on the ground would have been located to the right of the nose and any attempt to sight them would have drawn their attention away from Heli 1 located above and to their left. This relative position is known to include a potential ‘blind spot’ caused by cabin structure. While limited data prevented a full visibility study, the wreckage examination indicated that the orientation of the helicopters at the point of collision may have placed Heli 1 in this area which could have resulted in an obscured line of sight for the pilot of Heli 2, limiting their opportunity to detect the conflict.
The evidence shows that the pilots involved in the accident were aware of the other helicopter’s existence but did not detect the converging flight paths either at all, or with sufficient time to take evasive action. The strongest indication of this was the lack of any radio transmission or evasive manoeuvring from either pilot.
Contributing factor During initial climb while flying in close proximity towards the muster location, the pilots of VH-HQH and VH-HYQ did not detect their converging flight paths, which resulted in the midair collision. |
Established separation practice
Normalisation of deviance
Repeated exposure to risk without consequence is known to affect pilots' decision‑making (Hollenbeck and others, 1994). The concept of ‘normalisation of deviance’ describes the desensitisation to risk experienced by individuals or groups who repeatedly deviate from safe operating practices, without encountering negative consequences. A prominent feature of the normalisation of deviance is the desensitisation process, where frequent deviations result in the practice’s normalisation and perceived standardisation within everyday operations. This sets a precedent for what is considered tolerable and establishes a new normal from which further deviations may occur. In the absence of intervention, this cycle of deviance is disrupted only when the behaviour results in an undesirable outcome such as an accident (Sedlar and others, 2022).
Standard practice
The other pilots involved in the muster confirmed that although sequencing was arranged between the accident pilots on the day, the collision occurred before the pilots had arranged their own separation. While sequencing was one means of establishing initial separation, it would not ensure separation was maintained.
An established plan or standard procedure to manage the risk of collision after take-off would have provided the pilots with a tool to support effective decision‑making around in‑flight separation. By not defining procedures for operations that carried inherent risk, the operator did not have control of how the risk was managed. With pilots permitted to set their own separation, this produced varying results based on personal preference and over time, the practice of flying in proximity became the accepted norm.
In this system, there was a reliance on the pilots maintaining a lookout for other helicopters and taking avoiding action as necessary. See-and-avoid, though a well‑established defence against midair collision in uncontrolled airspace, is known to be fallible (CASA, 2021) and its limitations as a primary means of collision avoidance are well documented.
Repeated exposure to the established separation practice probably affected the mustering pilots’ perception of the associated risk. Flying in proximity to other aircraft reduced the opportunity to detect a conflict and manage the situation by decreasing the time available to respond to a threat. Further, this practice increased the risk of collision in the event of an unexpected or unanticipated manoeuvre.
Contributing factor Consistent with the operator's accepted and routine practice, the pilots flew in close proximity without an established plan for separation, increasing the risk of collision. |
Briefing
Based on the information obtained during interview, the morning brief was attended by all pilots and included the content specified in the operations manual. It focused solely on the operational aspects of the planned muster and did not include safety elements such as how the aircraft would be flown with regard to sequencing and separation.
The concept of a shared mental model has been found to be an essential component of how teams process information and perform (Salas & Fiore, 2004). Shared mental models affect team coordination by providing mutual expectations from which team members can know what their teammates are doing and predict future actions (Cannon‑Bowers and others, 1993). Through situation awareness, a team has a better understanding of the current and future state of the system and is more likely to be successful (Endsley, 2015). Mechanisms to support team members in monitoring each other and adapting to each other’s performance to modify their own task performance accordingly, result in better outcomes (Marks & Panzer, 2004).
The morning briefing was an opportunity for the pilots to establish a mutual understanding of how the day’s flying would be conducted and their responsibilities when changing the plan or recovering from a deviation from the plan. Guidance on effective briefings by the Flight Safety Foundation[19] suggests that including these elements in the pre-muster brief with some prescriptive minimums would have allowed the pilots to form a better understanding of how the flight would be conducted and, importantly, what the other pilots were trying to achieve and how the other helicopter would be flown. It could have prompted the pilots to consider where other aircraft would be during departure and may have helped the pilots detect a potential conflict. While not including these safety elements in the morning brief did not contribute to the accident, it represented a missed opportunity to manage the risk of collision shortly after departure.
Other factor that increased risk The morning briefing was solely operational and did not include elements of safety. Critically, separation between helicopters was not discussed. |
Operator’s procedures
Awareness of operational risk
The majority of the work conducted by the operator was aerial mustering utilising multiple helicopters. A review of the operations manual and evidence obtained during interview confirmed that the operator documented its expectation that pilots would maintain a good lookout and use visual aids such as aircraft lights to avoid a collision. In addition, the operator had implemented undocumented procedures for managing separation during mustering. This indicated an awareness that the risk of collision existed when operating with more than one helicopter.
The operator permitted pilots to establish their own separation relying on the pilot’s ability to identify and manage the risks of collision in multi-helicopter operations. Operating with unofficial guidelines can be one way to allow for autonomy and flexibility, however, an inherent problem with this approach is that even though guidelines have no official status, in practice, they can take on the character of formal policy in the absence of an alternative, however well-reasoned, without being sanctioned (Brandsen and others, 2006).
Importance of separation procedures
The importance of procedures to manage separation were identified in a previous ATSB report into a midair collision involving a Robinson Helicopters R44 and Piper Super Cub.[20] The report identified the following:
A procedural framework comprising, for example, lateral separation minima, radio communication requirements, the designation of a ‘coordinating pilot’, and specified responses to abnormal situations, could have assisted the pilots to maintain adequate separation, and to respond appropriately once they knew separation had broken down.
It was found that the operator did not provide a procedural framework for establishing and maintaining separation during aerial work activities.
Like the benefits of an effective briefing, defined separation procedures would provide participants with a shared understanding of how elements of the flight would be conducted in proximity to other machines. Further, practices enabling sighting of the helicopter ahead would assist with detection, and appropriate separation practices would assist the pilots by providing additional time to identify and respond to emerging threats.
The accepted separation practice increased the risk that 2 helicopters would be flown close enough to cause a collision hazard and the operator’s existing procedures did not manage this operational risk.
Contributing factor Pearl Coast Helicopters did not establish appropriate separation standards for its helicopters or provide documented procedures to ensure pilots established and maintained appropriate separation. (Safety issue) |
Operator’s management of risk
Historically, there has been a preference for using multiple helicopters on a single muster. The risk of collision was known to the operator, demonstrated by the undocumented strategies and practices implemented to avoid collisions during mustering operations. However, the risks associated with operating more than one aircraft in proximity had not been captured in the operator’s Safe Work Method Statements (SWMS) which were the primary tool for identifying and considering operational risks.
Records showed that the contents of the SWMS had not been updated since their introduction 2 years prior and did not include a mustering‑specific SWMS even though SWMS were available for other task specialist activities. Critically, the existing SWMS did not identify the hazard of midair collision or provide controls to manage aircraft separation. In the context of its primary business, this represented an under-utilisation of the operator’s available risk management tools. Not considering the nature of the flying activities increased the likelihood that operational risk would not be identified or managed appropriately.
Contributing factor Pearl Coast Helicopters did not formally manage risk in the context of its primary business which was multiple helicopter mustering operations. (Safety issue) |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the midair collision involving Robinson R22 Beta II, VH-HQH, and Robinson R22 Beta II, VH‑HYQ, 51 km south-south-east of Curtin Airport, Western Australia, on 25 July 2024.
Contributing factors
- During initial climb while flying in close proximity towards the muster location, the pilots of VH-HQH and VH-HYQ did not detect their converging flight paths, which resulted in the midair collision.
- Consistent with the operator's accepted and routine practice, the pilots flew in close proximity without an established plan for separation, increasing the risk of collision.
- Pearl Coast Helicopters did not establish appropriate separation standards for its helicopters or provide documented procedures to ensure pilots established and maintained appropriate separation. (Safety Issue)
- Pearl Coast Helicopters did not formally manage risk in the context of its primary business which was multiple helicopter mustering operations. (Safety Issue)
Other factors that increased risk
- The morning briefing was solely operational and did not include elements of safety. Critically, separation between helicopters was not discussed.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Absent procedures
Safety issue number: AO-2024-044-SI-01
Safety issue description: Pearl Coast Helicopters did not establish appropriate separation standards for its helicopters or provide documented procedures to ensure pilots established and maintained appropriate separation.
Identification of risk not tailored to flying operations
Safety issue number: AO-2024-044-SI-02
Safety issue description: Pearl Coast Helicopters did not formally manage risk in the context of its primary business which was multiple helicopter mustering operations.
Glossary
| AAIB | Air Accident Investigation Branch |
| AC | Advisory Circular |
| AMSL | Above mean sea level |
| AOC | Air Operator Certificate |
| BARS | Basic Aviation Risk Standard |
| CA Act | Civil Aviation Act |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| CAVOK | Ceiling and visibility okay |
| CEO | Chief Executive Officer |
| GAF | Graphical Area Forecast |
| GPS | Global Positioning System |
| HLS | Helicopter landing site |
| HOFO | Head of Flying Operations |
| JIAAC | Junta de Investigación de Accidentes de Aviación Civil |
| METAR | Meteorological aerodrome report |
| NTSB | National Transportation Safety Board |
| OM | Operations manual |
| PCH | Pearl Coast Helicopters Pty Ltd |
| SMS | Safety management system |
| SWMS | Safe Work Method Statements |
| VFR | Visual flight rules |
| VHF | Very high frequency |
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- Pearl Coast Helicopters Pty Ltd
- other pilots employed by the operator involved in the muster
- Civil Aviation Safety Authority
- Western Australia Police Force
- Robinson Helicopter Company
- Helico Australia
- Bureau of Meteorology
- accident witnesses
- video footage of the accident flight and other photographs and videos taken on the day of the accident
- recorded data from the GPS unit on the aircraft.
References
Brandsen, T., Boogers, M., & Tops, P. (2006). Soft Governance, Hard Consequences: The Ambiguous Status of Unofficial Guidelines. Public Administration Review, 66(4), 546–553. http://www.jstor.org/stable/3843940)
Cannon-Bowers, J. A., Salas, E., & Converse, S. (1993). Shared mental models in expert team decision making. In N. J. Castellan, Jr. (Ed.), Individual and group decision making: Current issues (pp. 221–246). Lawrence Erlbaum Associates, Inc.
CASA. (2014). Sector safety risk profile – Aerial mustering.
CASA. (2021). AC 91-14 v1.0 Pilots’ responsibility for collision avoidance. Canberra: Civil Aviation Safety Authority
CASA. (2024). AC 138-01 v3.1 Part 138 core concepts. Canberra: Civil Aviation Safety Authority
CASA. (2025). Agricultural flying sector safety risk profile. https://www.casa.gov.au/operations-safety-and-travel/safety-management-systems/sector-safety-risk-profiles/agricultural-flying-sector-safety-risk-profile/
CASA. (2025). Part 138 guide to sample operations manual (Mustering). Canberra: Civil Aviation Safety Authority
CASA. (2025). Visual flight rules guide v8.2 Canberra: Civil Aviation Safety Authority
CASR Part 91 (General flying and operating flight rules), (1998) Cth.
CASR Part 138 (Aerial work operations) Manual of Standards, (2020) Cth.
Civil Aviation Act (1988) Cth.
Civil Aviation Safety Regulation (1988) Cth.
Endsley, M. R. (2015). Situation Awareness Misconceptions and Misunderstandings. Journal of Cognitive Engineering and Decision Making, 9(1), 4-32. https://doi.org/10.1177/1555343415572631
Flight Safety Foundation. (2025). Basic Aviation Risk Standard for Aerial Mustering v4.0. Flight Safety Foundation. https://flightsafety.org/
Hobbs, A. (1991). Limitations of the see-and-avoid principle. Canberra: Australian Transport Safety Bureau.
Hollenbeck, J. Ilgen, D. Phillips, J. Hedlund J. (1994) Decision risk in dynamic two-stage contexts: beyond the status quo. Journal of Applied Psychology, Vol. 79, Issue 4, pp. 592–598.
Kepert, J.L. (1976). The use of wreckage trajectories in aircraft accident investigation. Department of Defence. Defence science and technology organization aeronautical research laboratories.
Leibowitz, H. W., & Owens, D. A. (1991). Can normal outdoor activities be carried out during civil twilight? Applied Optics 30 (24), 3501-3503.
Marks, M. A., & Panzer, F. J. (2004). The influence of team monitoring on team processes and performance. Human Performance, 17(1), 25-41.
Purves D, Augustine GJ, Fitzpatrick D, et al., 2001.Functional Specialization of the Rod and Cone Systems. Neuroscience. 2nd edition. Editors. Sunderland (MA): Sinauer Associates.
Salas, E. E., & Fiore, S. M. (2004). Team cognition: Understanding the factors that drive process and performance. American Psychological Association.
Sedlar, N. Irwin, A. Martin, D. & Roberts, R. (2022). A qualitative systematic review on the application of the normalization of deviance phenomenon within high-risk industries. Journal of Safety Research. School of Psychology, William Guild Building, University of Aberdeen, Aberdeen, UK. & Aberdeen Business School, Robert Gordon University (RGU), Aberdeen, UK.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Pearl Coast Helicopters Pty Ltd
- other pilots employed by the operator involved in the muster
- Civil Aviation Safety Authority
- Western Australia Police Service
- Robinson Helicopter Company
- Helico Australia.
Submissions were received from:
- Pearl Coast Helicopters Pty Ltd
- Civil Aviation Safety Authority
- Robinson Helicopter Company.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Visibility and R22 exemplar cockpit mask
Capture of the base image
The cockpit mask in Figure 16 was developed from a 360° equirectangular image taken from a location approximating the eye position of a person seated in the pilot’s seat. This position was determined from medical records and an exemplar pilot of similar height.
While there are limitations to this method of image capture, these limitations do not invalidate the use of the mask.
Limitations include:
- mask developed from a single position
- image based on an aircraft on level ground and not in flight attitude
- use of wide‑angle lenses can introduce image distortion at the edges of an image
- flight controls captured in a static position.
Visual detection of a target aircraft is impacted by 3 different but related factors: visibility, detectability and conspicuity. Visibility considers whether an aircraft is visible to the person looking for it. Detectability considers how easily a target can be detected from the eye position of the person looking for it. Conspicuity is whether a target stands out from its background sufficiently to be identified.
Creating the mask
The relative position of a target from the viewer’s eye position is represented as azimuth and elevation angles from the centre of the view. As the equirectangular image and subsequently the mask represents a full 360° of azimuth and 180° of elevation, a grid can be overlayed on the image to assist the viewer to understand how far from the centre of the view objects will appear or the relative angle between 2 things in their view.
Figure 18 shows the mask overlain with a 15° marked grid in both azimuth and elevation angles.
Figure 18: R22 generic mask with grid overlay
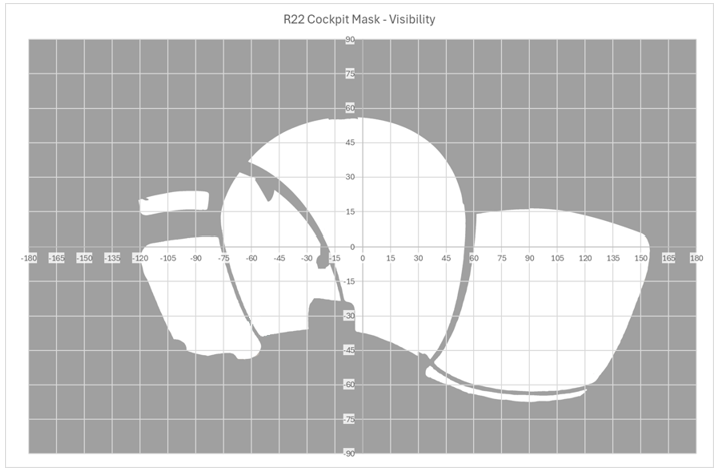
Source: ATSB
Field of view
The cockpit mask is a spherical representation of the aircraft structure around the estimated pilot’s eye position. While the 360° camera can capture this whole area, the human eye has a limitation to how much of this area that it can detect. This is referred to as the field of view (FOV), it consists of approximately 200° of azimuth and 135° of elevation. The opportunity for target detection is not constant across this area, it varies depending on where the target is located. For the purposes of ATSB visibility analysis, the FOV is broken down into 3 areas consisting of the foveal, inner and full visual fields, progressing from the centre of the visual field outwards. Further detail of the size and differences between these areas can be found in
.
Figure 19 shows approximate areas of the visual field overlain on the R22 generic cockpit mask as developed earlier. In this case the field of view has been positioned as if the eyes are directed straight ahead to demonstrate the size of the field. Rotation of the eyes will change where in the FOV parts of the structure appear, which may impact visual acquisition of the target. It is important to note that movement of the head may also impact FOV but it will impact the relative location of the structure so modelling rotation of the head would require a different cockpit mask.
Figure 19: R22 generic cockpit mask showing fields of view
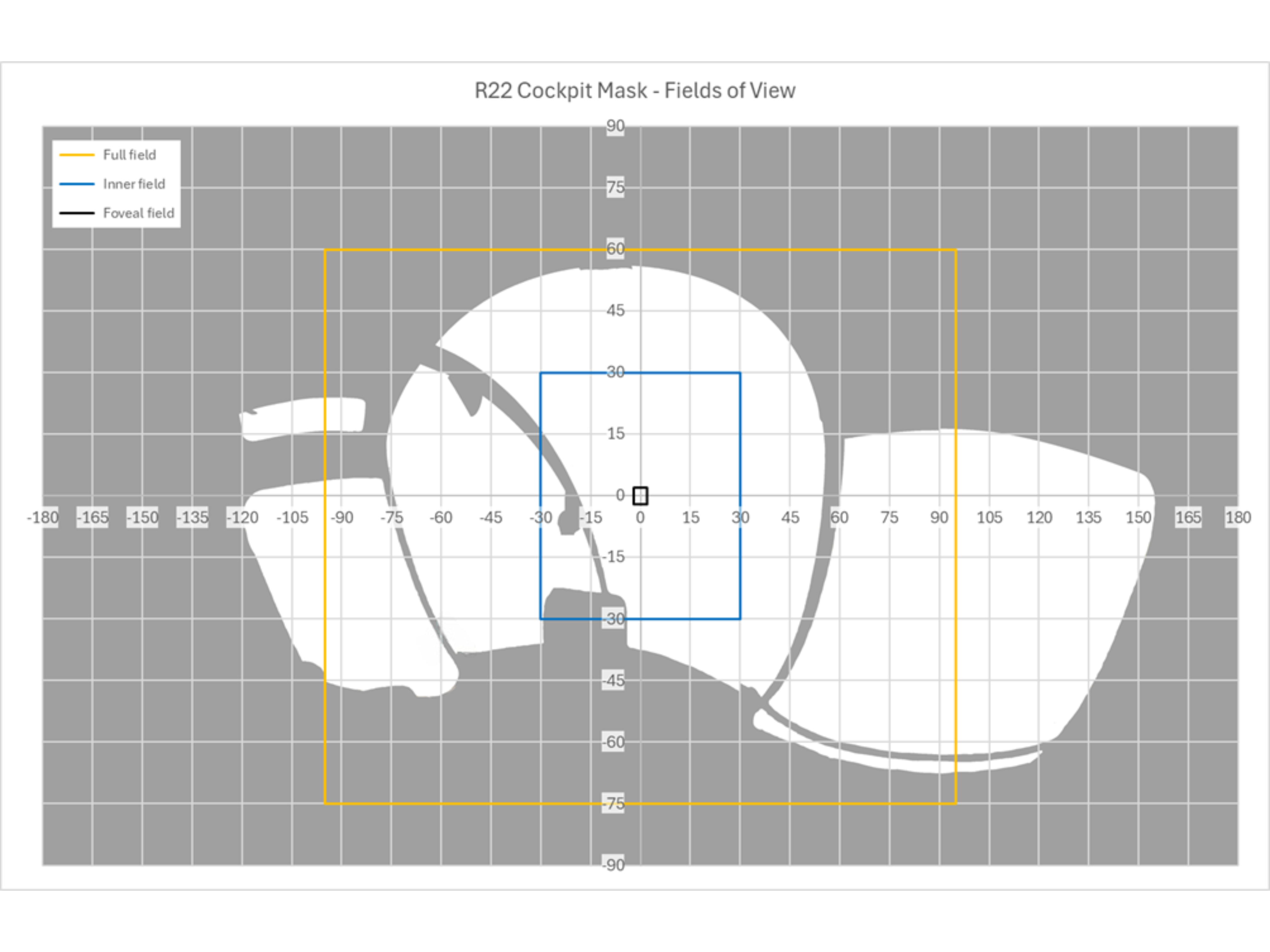
Source: ATSB
Conclusions
The mask shows that when looking ahead there is minimal obstruction to the pilot’s view and with the doors removed there are large areas on both sides that are unobstructed. However, there are areas where a target will be shielded such as behind the instrument cluster and the cabin roof. For a pilot seated in the right seat, this shielding is greater in the left side of the pilot’s field of view. This means that a potential conflict is more likely to be obstructed when the threat originates from the left of the helicopter.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Smoker units, when activated by the pilot, create a veil of smoke below the helicopter by squirting diesel fuel onto the hot exhaust. The smoke is used to direct the movement of cattle.
[2] The teeter stops were crushed and the teeter mounts exhibited some distortion, yet this damage did not extend through to the mast.
[3] The pilot operating handbook advised ‘avoid placing objects in compartments which could injure occupant if seat collapses during a hard landing’.
[4] GPX file: a GPX file, also known as a GPS Exchange Format, is a common GPS data format for software applications. Files contain data such as routes, tracks, waypoints, and geocaches.
[5] TAF (Aerodrome Forecast): a statement of meteorological conditions expected for the specified period of time in the airspace within 5 NM (9 km) of the aerodrome reference point.
[6] Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[7] METAR (Meteorological Aerodrome Report) is a routine aerodrome weather report issued at half‑hourly time intervals. The report ordinarily covers an area of 8 km radius from the aerodrome reference point.
[8] GAF (Graphical Area Forecast): provides information on weather, cloud, visibility, icing, turbulence and freezing level in a graphical layout with supporting text.
[9] See CASA Day VFR guide.
[11] Over 90 per cent of aerial mustering is conducted by rotary wing aircraft. CASA Sector risk profile – aerial mustering (2014).
[13] This regulation also specifies the lateral distance an aircraft must maintain from an obstacle based on a point on the ground directly beneath the aircraft.
[14] Helicopter landing site (HLS) register: a reference document used to record critical information about frequently visited landing sites. This information is used by a pilot to determine the suitability of a site for the intended operations.
[15] CASR Part 61 – Flight crew licensing.
[17] The number of possible collision pairs is given by the formula: P = N x (N-l)/2 where N is the number of aircraft operating in a given airspace.
.
[18] Authorisation holder: the term used by CASA to refer to the holder of a Civil Aviation Authorisation to undertake a particular activity (whether the authorisation is called an AOC, permission, authority, licence, certificate, rating or endorsement or is known by some other name).”
Preliminary report
Report release date: 27/09/2024
| This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003. |
The occurrence
On the morning of 25 July 2024, 4 Robinson Helicopter Company R22 Beta II aircraft were being operated at Mount Anderson Station, located about 51 km south-south-east of Curtin Airport, Western Australia. The helicopters were being used as part of a cattle mustering operation, which also included multiple land vehicles.
At about 0515 local time, a briefing was held by the lead pilot to cover the planned muster along a section of the Fitzroy River, a 10-minute flight to the west-north-west of the station homestead. This brief lasted around 15 minutes and was attended by the helicopter pilots and the head stockman, who provided input on where the ground crew would be located.
At about 0540, the pilots commenced their pre-flight preparations. VH-HQH (HQH) and VH-HYQ (HYQ) were parked in a grassed clearing behind the homestead and the other 2 helicopters, VH‑HMR (HMR) and VH-YKC (YKC), were parked about 400 m to the west. The helicopters were started just before 0600, and the pilots established communication with each other on a discreet company VHF radio frequency. The lead pilot in HQH radioed they were ready to depart and would lead the group out. This radio broadcast was acknowledged by the pilot of HYQ who replied that they would follow HQH.
At 0603, HQH and HYQ departed the overnight parking area and flew west, to where the other 2 helicopters would join them (Figure 1). A witness (witness 3) located near the stockyards about 200 m to the south of the homestead watched the 2 helicopters accelerate away, climbing above the buildings and depart with HQH in front and HYQ following slightly lower and behind off to one side.
Figure 1: Witness locations
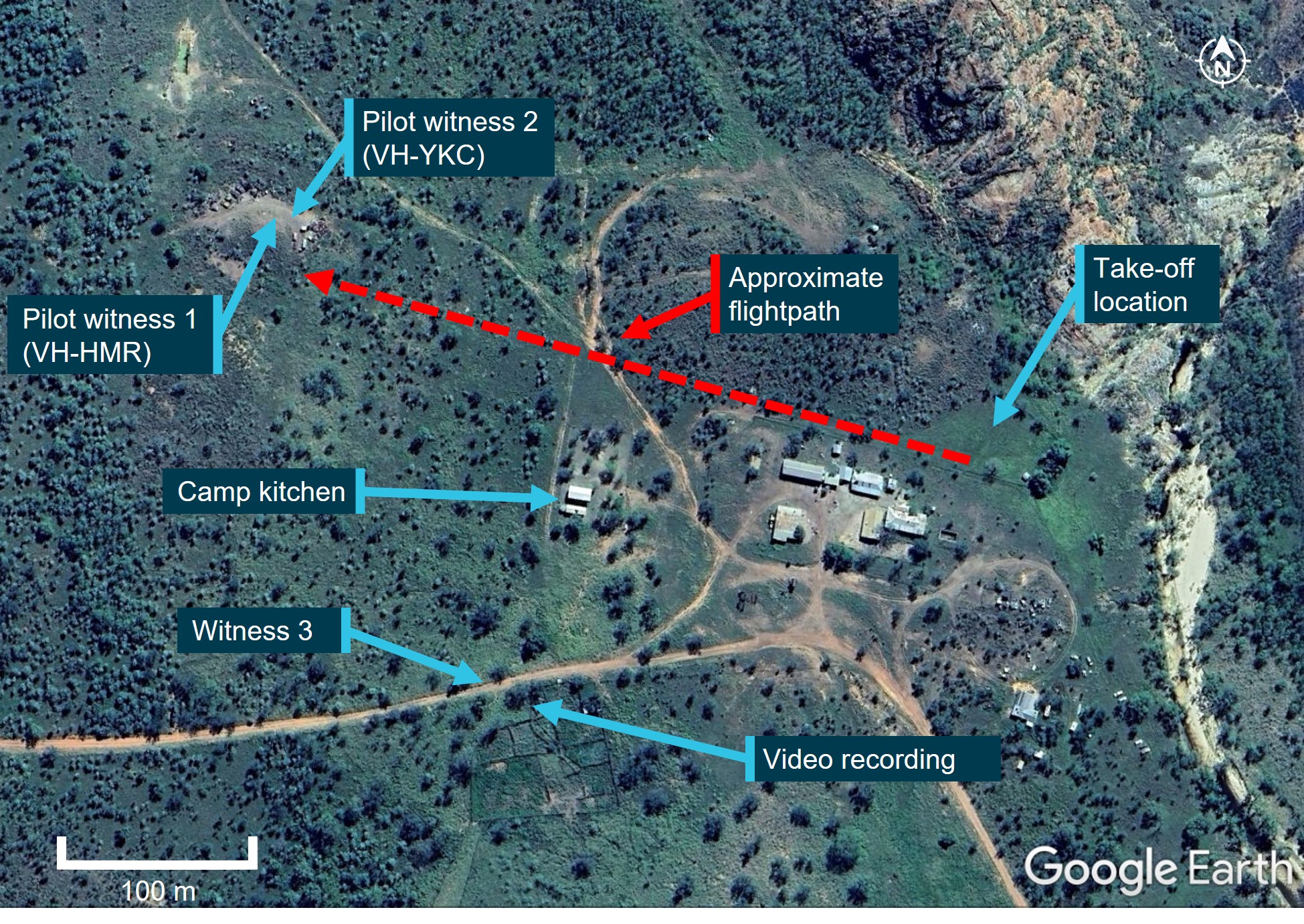
Source: Google Earth annotated by ATSB
The pilots in HMR and YKC saw both helicopters approach from above the tree line to the east at about 100 ft. The pilot of YKC, who was a few minutes behind in their own pre-flight preparations, recalled seeing the 2 helicopters flying together but did not detect a risk of collision at that point. They put on their helmet and checked their radio. The pilot in nearby HMR acknowledged the radio check and advised that they would lift into the hover. The pilots in HMR and YKC remembered hearing the lead pilot in HQH acknowledge this radio call with the reply “Yep, I see you there”. The pilot in HMR lifted into a low hover and the pilot of YKC turned their attention to their own machine when they heard the 2 aircraft collide.
Upon hearing the collision, the pilot of HMR looked up and saw that HQH was descending toward their location. Already established in the hover, the pilot manoeuvred the helicopter away to avoid being struck.
Following the mid-air collision, the pilots of HQH and HYQ were unable to maintain control and both helicopters collided with terrain and were destroyed. Both pilots sustained fatal injuries.
Context
Pilot information
Both pilots involved in the collision were authorised to conduct aerial mustering operations, and both held valid Class 1 aviation medical certificates with no restrictions.
The pilot of VH-HQH held a Commercial Pilot Licence (Helicopter) and low-level helicopter operational rating with an aerial mustering endorsement, 6 years of aerial mustering operation experience and had been with the operator for 4 years. They had about 4,750 total flight hours, with about 3,600 flight hours mustering, and about 4,250 flight hours in R22 helicopters. Their most recent flight review was a low-level single engine helicopter flight review on 1 April 2024.
The pilot of VH-HYQ held a Commercial Pilot Licence (Helicopter), low-level helicopter operational ratings with an aerial mustering endorsement, 4 years of aerial mustering operation experience and had been with the operator for 2 years. They had about 2,100 total flight hours, with about 1,350 flight hours mustering, and about 2,000 flight hours in R22 helicopters. They had conducted a low-level single engine helicopter flight review on 30 March 2024.
Aircraft information
The Robinson Helicopter Company R22 Beta II helicopter is powered by a 4‑cylinder carburetted piston engine. The R22 has 2 seats, with the pilot flying from the right seat, and each seat was fitted with a seatbelt and inertia reel shoulder strap, similar to those used in motor vehicles. The 2-blade main rotor assembly rotating counterclockwise when viewed from above.
Typical for mustering activities, the helicopters were being operated with both doors removed.
Figure 2: VH-HQH (left) and VH-HYQ (right)

Source: Helico
VH-HQH
VH-HQH, serial number 3936, was manufactured in the US in 2005 and first registered in Australia in September 2005 (Figure 2). The helicopter had undergone a periodic inspection along with a 2,200 hr / 12-year inspection/overhaul that was completed on 8 July 2024 at 6,087 hours total time-in-service. The current maintenance release was not located, however, the operator reported the helicopter had accrued about 60 hours since the rebuild.
HQH was fitted with a smoker unit to aid in aerial mustering operations (Figure 3).[1] It consisted of a small tank (about 5 L capacity), that was filled with either diesel or paraffin oil and mounted on the right-side lower frame. A small integrated electrical pump activated by a trigger on the pilot’s controls would transfer the diesel from the tank into the exhaust outlet where it was vaporised by the exhaust heat creating a veil of smoke that was blown downward by the main rotor downwash.
Figure 3: VH-HQH smoker unit installation
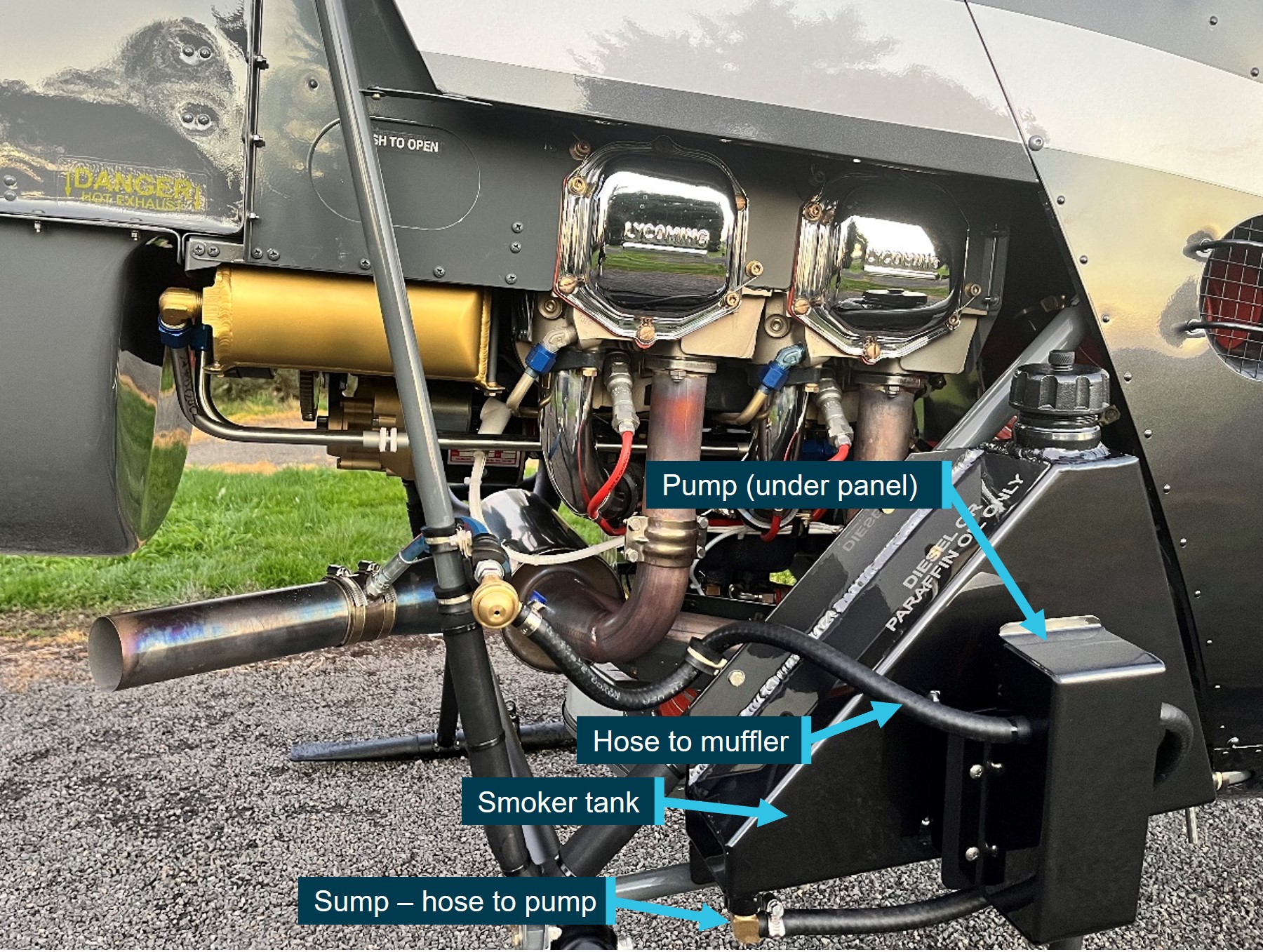
Source: Helico, annotated by ATSB
VH-HYQ
VH-HYQ (HYQ), serial number 3835, was manufactured in the US in 2005 and first registered in Australia in May 2005 (Figure 2). A 2,200 hr / 12-year inspection/overhaul was completed in April 2023. The most recent periodic inspection, at 4,946 hours, was conducted on 19 July 2024. The current maintenance release was not located, however, the operator reported the helicopter had accrued about 40 hours since the last periodic inspection.
HYQ was not fitted with a smoker unit.
Meteorological information
Daylight
Geoscience Australia recorded the first light at Mount Anderson Homestead at 0551 and sunrise at 0614. This was consistent with witness reports and a video recording which confirmed that the collision (0603 local) occurred after first light but before sunrise.
Weather
Due to the remote location of the site, there were no official weather observations available. The nearest official data was obtained from Curtin Airport located 51 km to the north-west of Mount Anderson Station.
While the Graphical Area Forecast (GAF)[2] that covered Mount Anderson Station and was valid at the time of the accident included isolated fog, witnesses and the video indicated there was no fog at the station. The Terminal Forecast (TAF)[3] obtained for nearby Curtin Aerodrome indicated CAVOK[4] conditions with a southeast breeze (150°) around 8 kt.
Site and wreckage
The accident site was located about 300 m west-north-west of the historic Mt Anderson homestead (Figure 1). Power to the homestead buildings was produced via generator. There were some low power lines immediately above, and close to, the roof line but there were no power lines situated on the flight path. The local vegetation was dry, low open woodland. There was no evidence of any wildlife or tree strike in the vicinity of the start of the debris trail.
The first items in the debris field, about 300 m west-north-west of the take-off location, were consistent with a rotor blade strike to the right side of HQH (Figure 4), and consisted of:
- smoker unit pump cover panel
- smoker tank sump (separated horizontally from most of the upper portion of the tank)
- smoker unit lower (horizontal) mount
- fuselage skin from just forward of right position light
- right seat ‘pocket’ material section (located on forward panel of the pilot seat structure)
- trim from around the forward and right edges of pilot seat.
Figure 4: VH-HQH (pre-accident) showing approximate location of rotor strike location and locations of first items in debris field

Source: Helico and ATSB, annotated by ATSB
The debris trail then consisted of HQH components including tailcone, tail rotor driveshaft and tail rotor control tube sections, tail rotor gearbox and blades and stabiliser assembly. HYQ liberated components included the stabiliser assembly and section of one tail rotor blade.
Both helicopters’ masts fractured mid-length, and both main rotor head assemblies, with blades attached, were located about 10 m apart and about 70 m from the start of the debris trail. The fuselage of HQH was located 9 m west of its rotor head, lying on its right side on an approximate north-north-east orientation. The fuselage was destroyed by fire.
HYQ impacted terrain on its left side and slightly nose down. The impact site contained multiple pieces of windshield and other cabin components. The next ground scar, about 10 m further in a westerly direction, was consistent with the right skid. The helicopter came to rest upright, with the belly resting on top of a termite mound. The nose of the fuselage was about 1 m south of the skid ground scar and facing a north‑easterly orientation. The main fuel tank bladder was destroyed by impact forces. The auxiliary fuel tank assembly was ejected, likely at the second impact. Its outer structure was impact damaged, however, the bladder remained intact.
Wreckage examination of both helicopters identified all the major components were present at the accident site with no evidence of an in‑flight break-up prior to the mid-air collision. Flight control continuity of HYQ was established. The fire damage to HQH limited the extent to which the flight controls could be examined, however, where flight control tubes had been destroyed, security was established through control tube rod ends being secured to identified controls and bellcranks.
Samples of fuel taken from HYQ’s auxiliary tank and gascolator were visually examined and noted to be clean and clear of visible debris. The samples were also tested for the presence of water, with nil indication. Further, all 4 helicopters had been using the same bulk fuel with no quality issues reported.
Recorded data
Neither helicopter was equipped with a flight data recorder, tracking device or on board camera, nor were they required to be. Both aircraft were equipped with portable GPS units which were located onsite and taken to the ATSB’s technical facility in Canberra for further examination.
Video of livestock in a nearby yard was recorded at the time of the accident. While it did not contain any footage of the helicopters, it did capture audio of the departure and the collision.
A smart watch, which may contain additional information or data, was retained for further examination.
Safety action
Following the accident, the operator conducted a review of the operations manual and revised procedures for operations involving multiple aircraft and the operation in the vicinity of other aircraft. These changes were contained in a company notice to air crew (NOTAC) and all pilots were briefed on the changes prior to resuming flying operations.
Further investigation
To date, the ATSB has examined the accident site and wreckage, collected meteorological data from the Bureau of Meteorology, collected operator, pilot and aircraft related records, conducted interviews, and liaised with the Western Australia Police Force.
The investigation is continuing and will include further examination and analysis of:
- weather conditions at the time of the accident
- components retained from both helicopters
- witness information
- analysis of recorded audio
- download and analysis of the electronic items retrieved from the accident site
- pilot qualifications, experience and medical histories
- aircraft maintenance and operational records
- operational documentation and procedures
- visibility from both helicopters.
Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The smoker unit is used to direct cattle or to deter them from running back on the helicopter by creating a veil of smoke that is blown down below the helicopter.
[2] GAF (Graphical Area Forecast): provides information on weather, cloud, visibility, icing, turbulence and freezing level in a graphical layout with supporting text.
[3] TAF (Aerodrome Forecast): a statement of meteorological conditions expected for the specified period of time in the airspace within 5 NM (9 km) of the aerodrome reference point.
[4] Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
Occurrence summary
| Investigation number | AO-2024-044 |
|---|---|
| Occurrence date | 25/07/2024 |
| Location | 51 km south-south-east of Curtin Airport |
| State | Western Australia |
| Report release date | 03/12/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Airborne collision |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | Robinson Helicopter Co |
|---|---|
| Model | R22 Beta II |
| Registration | VH-HQH |
| Serial number | 3936 |
| Aircraft operator | Helico Australia Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 138 Aerial work operations |
| Damage | Destroyed |
Aircraft details
| Manufacturer | Robinson Helicopter Co |
|---|---|
| Model | R22 Beta II |
| Registration | VH-HYQ |
| Serial number | 3835 |
| Aircraft operator | Pearl Coast Helicopters Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 138 Aerial work operations |
| Damage | Destroyed |