
Ineffective bridge resource management before Bunbury grounding
Ineffective bridge resource management contributed to the grounding of a bulk carrier in the Port of Bunbury, Western Australia, an ATSB investigation has found.
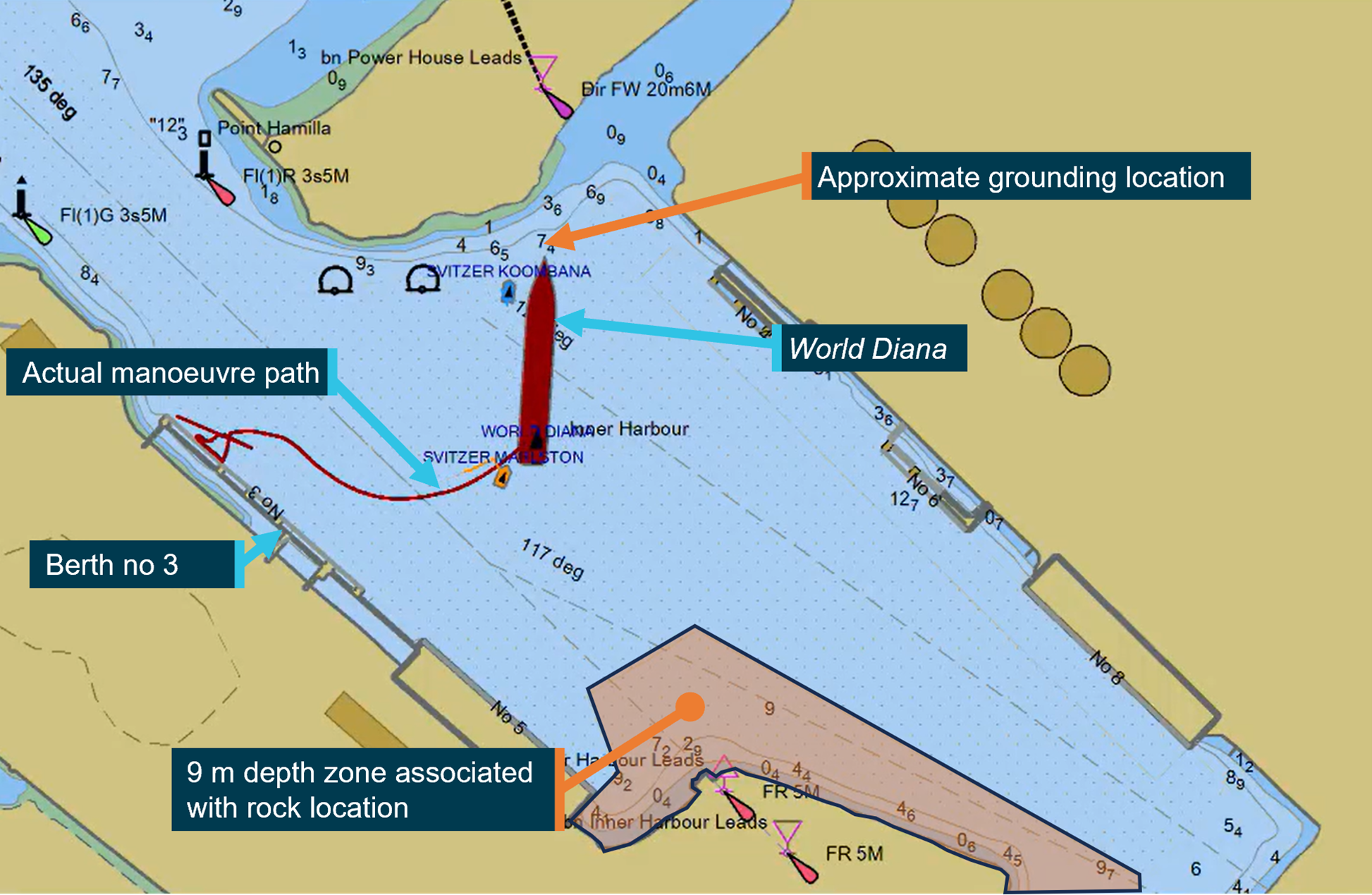
The grounding occurred on 22 April 2023 as the 229 m long, Isle of Man-registered bulk carrier World Diana was departing Bunbury under the conduct of a harbour pilot, with two tugs assisting.
After being moved off its berth, the ship had to be turned in the swing basin before exiting the harbour.
“This turn was started earlier than planned, reducing the amount of room available,” Chief Commissioner Angus Mitchell said.
“The ship’s speed was then allowed to increase until there was no room to safely turn, and the bow of the ship grounded on a shallow bank to the east of the harbour entrance.”
The ship sustained minor hull damage, but was able to be manoeuvred off the bank. Fortunately, there was no pollution reported.
The ATSB’s investigation found bridge resource management during the pilotage was ineffective.
“Bridge resource management is an important part of safe pilotage,” Mr Mitchell said.
“Effective use of available resources reduces the chance of single-person errors and minimises their impact.”
In this case, the report notes, proper use of the available portable pilot unit, effective communication, and active involvement of the World Diana’s bridge team and the tug masters, would have allowed the deviation from the plan to be detected in time to prevent the grounding.
“Specific information and limits for the departure plan were only known to the pilot, which made it difficult for the bridge team to raise concerns during the event,” Mr Mitchell said.
“Nevertheless, had the ship’s master – an experienced ship-handler familiar with the ship’s movement characteristics – been actively monitoring the pilotage, the early turn and ship’s increasing headway should have become evident.”
While not found to have contributed to the grounding, in the course of the investigation the ATSB also found the Port of Bunbury had not developed adequate procedures for arrival and departure plans for larger ships berthed on their starboard side alongside berth no. 3.
“This reduced the information available to pilots for these ship movements, and to share with bridge teams and tug masters to ensure a common understanding of how manoeuvring would be conducted,” Mr Mitchell concluded.
Read the final report: Grounding of World Diana, Port of Bunbury, Western Australia, on 22 April 2023
Flight below minimum sector altitude involving Cessna 310R, VH-ZMB, 14 km west-north-west of Alice Springs Airport, Northern Territory, on 1 July 2024
Final report
Report release date: 20/03/2025
Investigation summary
What happened
On 1 July 2024, a Cessna 310R, registered VH-ZMB, was returning to Alice Springs from Willowra aircraft landing area, Northern Territory (NT), with only the pilot on board.
During an instrument approach in instrument meteorological conditions, the pilot reported receiving false indications from the attitude indicator and directional gyroscope. The aircraft deviated from the published approach path and tracked perpendicular to the approach track, below minimum sector altitude (MSA).
The pilot notified air traffic control at Alice Springs tower of the situation, before obtaining a clearance to track from their present position back to the initial instrument landing system approach point, for a subsequent attempt at landing.
A second approach was then flown, followed by a successful landing at Alice Springs Airport.
What the ATSB found
The ATSB found that the pilot, whilst established on the ILS approach to Alice Springs, likely experienced spatial disorientation that led to an undesired flight path, below the MSA.
In their state of distress, the pilot did not broadcast a PAN PAN call notifying air traffic control of their situation. Further, air traffic control did not issue a safety alert, which would have alerted the pilot that they were in unsafe proximity to terrain and needed to climb immediately. This was also influenced by the pilot not broadcasting a PAN PAN, but could have been made independently.
Once the pilot was outside of the required tolerances for the instrument approach and below the MSA, the pilot did not conduct a missed approach, remaining below minimum sector altitude for an extended period.
Other factors that increased the risks identified in this investigation include post‑occurrence fault finding that found the artificial horizon exhibited deviations outside the manufacturer’s required tolerances. Additionally, the pilot’s choice to not make use of the autopilot for the approach may have increased their workload and the subsequent risk of spatial disorientation during the instrument approach procedure.
What has been done as a result
The operator has since introduced an automation policy for the use of autopilot in instrument meteorological conditions and in high workload single-pilot operations.
Safety message
Pilots should not hesitate to report an urgent condition when encountering situations that may not be immediately perilous but significantly increase risk. Broadcasting a PAN PAN call when there is uncertainty about the safety status of the aircraft will alert ATC to the need for immediate assistance.
Air traffic control has a duty of care to provide safety alerts to pilots on becoming aware that an unsafe situation such as proximity to terrain has, or may, occur.
Once an aircraft is no longer on an established approach path and doubt exists as to its lateral position and location, a missed approach should be conducted, including an immediate climb to achieve a safe altitude, clear of terrain.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the morning of 1 July 2024, a Cessna 310R, registered VH-ZMB, conducted a passenger transport flight[1] to Willowra aircraft landing area, NT, and was repositioning[2] to Alice Springs, NT, with only the pilot onboard.
At approximately 1020 local time, the pilot commenced an instrument landing system (ILS) approach[3] for runway 12 at Alice Springs Airport. This approach was manually flown (not utilising the autopilot system), in instrument meteorological conditions.[4]
At 1022:05, the aircraft was established at 4,250 ft above mean sea level (AMSL) on the approach into Alice Springs Airport on the published ILS approach profile. About 25 seconds later, the pilot recalled receiving erroneous instrument indications from the artificial horizon (AH). At 1022:30, flight data showed the aircraft departing the ILS to the left, and tracking at a perpindicular direction from the approach path with unusual aircraft bank angles (AOB) (Figure 1).
Figure 1: VH-ZMB flight path
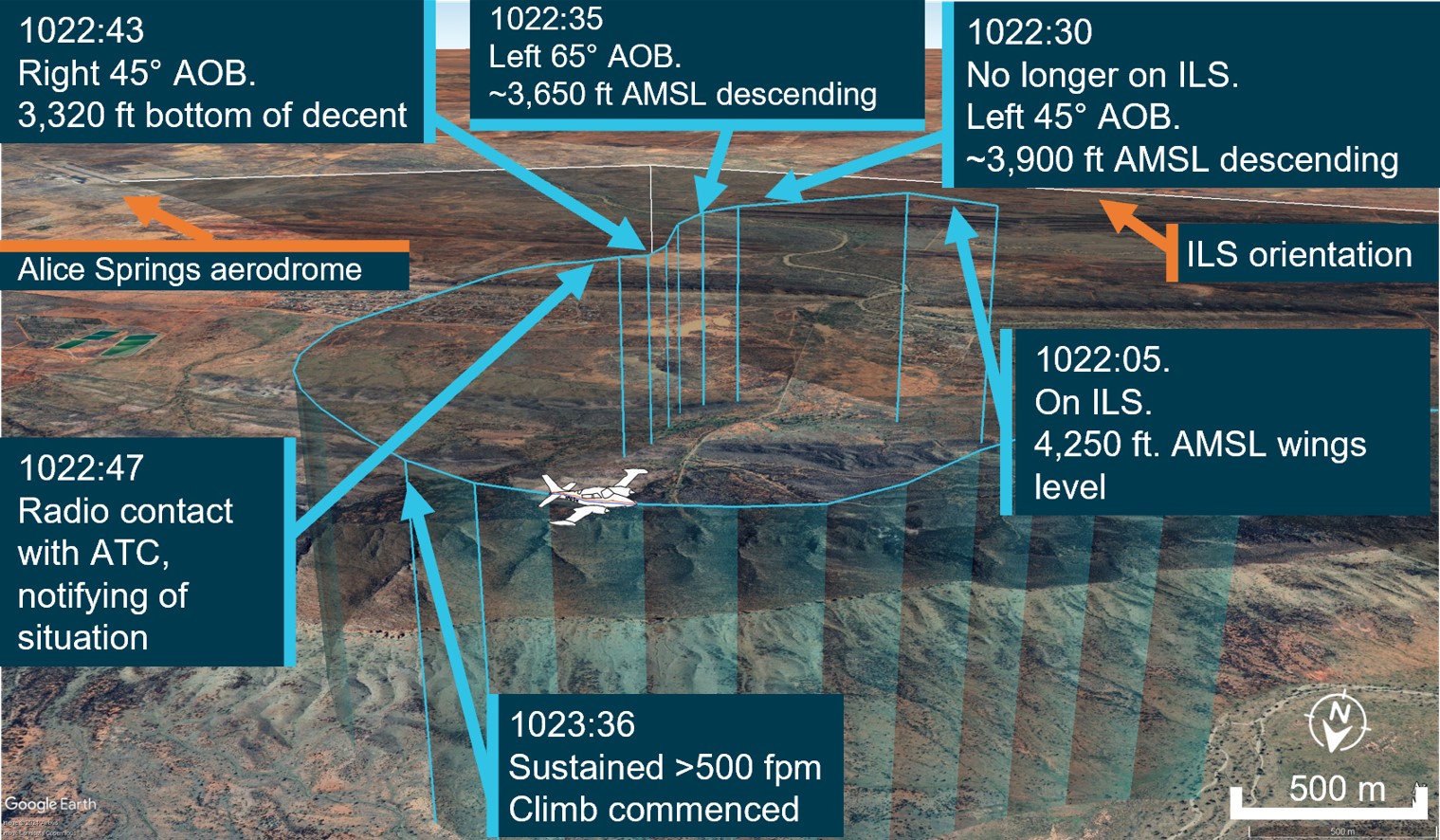
Source: ATC recordings and recorded flight data, overlaid on Google Earth and annotated by the ATSB
At 1022:47, the pilot contacted air traffic control (ATC), using their callsign twice. The pilot reported an issue with the instruments and requested clearance to commence a second approach. The ATC controller observed, and ATC recordings indicate, a level of stress in the voice of the pilot at this time.
ATC subsequetly cleared the pilot to climb to 5,500 ft and to track directly to the initial approach fix for the ILS (position LISZT).
At 1023:36, nearly a minute after obtaining a clearance from air traffic control and over a minute from leaving the ILS profile, the pilot commenced a sustained climb.
Recorded flight data indicated that during this time, the aircraft was below the minimum sector altitude of 4,300 ft and tracking towards rising terrain. The aircraft came within its closest proximity to terrain as it passed the ridgeline at about 810 ft above ground level.
At 1024:30 the pilot acheived an altitude of 4,300 ft enroute to position for a second approach.
A subsequent ILS approach was then flown into Alice Springs, followed by a successful landing.
Table 1: Sequence of events
| Time: local | Description of event |
| 1022:05 | On ILS, wings level, 4,250 ft. Standard rate of descent (ROD) |
| 1022:30 | No longer on localiser (LOC), AOB 45° left, ~3,900 ft, descending |
| 1022:35 | Tracking greater the 90° off LOC, AOB 65° left, ~3,650 ft descending |
| 1022:43 | Tracking greater than 90°of LOC, AOB 45° right, bottom of descent ~3,320 ft |
1022:47 ZMB – Tower broadcast | VH-ZMB: ‘ZMB, ZMB we’ve got incorrect AH [artificial horizon] information we have lost glidepath request tracking direct to LISZT…Currently at 3,700…’ ATC: ‘Climb to 5,500 track direct to LISZT’ |
| 1023:16 | Closest point of approach to the terrain was approximately 810 ft recorded |
| 1023:36-38 | Sustained climb begun with >500 fpm climb. Sustained 15° AOB left (controlled), ~3,800 ft |
| 1024:30 | 10 NM minimum sector altitude (MSA) achieved 4,300 ft |
Source: ATC recordings and recorded positional data tabulated by the ATSB
Context
Pilot qualifications and experience
The pilot held a commercial pilot licence (aeroplane) and a valid class 1 aviation medical certificate. The pilot reported a total flying time of 386 hours with about 66 of those being on the Cessna 310. The pilot obtained a multi-engine aeroplane instrument rating in February 2024. The pilot reported accruing 27.3 total hours of instrument flight time with 5.7 hours being accrued in the last 90 days. The pilot had been employed with the operator since April 2024 and had completed their Operator Proficiency Check – IFR [5], on 17 May 2024.
Aircraft
The Cessna 310R is a twin-engine, low-wing, 6-seat, unpressurised aircraft equipped with retractable landing gear. The aircraft was manufactured in 1976 and had greater than 16,600 hours recorded on the maintenance release. VH-ZMB was fitted with Garmin 430W avionics, coupled with a traditional avionics suite (Figure 2).
Figure 2: Photo of cockpit instruments from perspective of left (pilot) seat

Source: Operator annotated by the ATSB
The pilot reported that placement of the standby artificial horizon on the far right‑hand side of the instrument panel (Figure 2) precludes the pilot from observing angles of bank (especially to the left). However, the pilot also reported utilising the standby AH as the primary means of spatial orientation, both during the occurrence and post‑occurrence to fly the second approach and identified that recovery to a safe altitude was ultimately slowed by the significant workload of stabilising the aircraft on a limited instrument panel.
Weather conditions
Weather conditions in the Alice Springs terminal area at the time of the occurrence were identified as a moderate south-easterly wind of 10 kt, with greater than 10 km of visibility. The cloud was reported as scattered (between 3–4 oktas[6]) at 900 ft, broken (between 5–7 oktas) at 1,300 ft and overcast (8 oktas) at 2,400 ft above ground level. The pilot reported the approach was conducted in instrument meteorological conditions and recalled being in stratiform cloud [7] from 7,000 ft to 2,500 ft AMSL.
Instrument landing system approach
The Alice Springs ILS runway 12 initial approach fix is a waypoint designated as LISZT which is about 15 NM (27.8 km) from the end of runway 12. The approach descent commences at 11.5 NM (21.2 km) from the runway 12 threshold, on a standard 3° descent profile. The missed approach procedure is to track 116° magnetic and climb to 5,500 ft AMSL.
Minimum sector altitude
Minimum sector altitude (MSA) is the lowest altitude which will provide a minimum clearance of 1,000 ft above all objects located within a specified area. This specified area is contained within a circle, or a sector of a circle of 25 NM (46.3 km) or 10 NM (18.5 km) radius centred on a significant point.
In the case for Alice Springs, the significant point being used as the datum reference point is the Alice Springs VHF Omni Directional Range (VOR) station[8].
The 10 NM MSA in the area around Alice Springs Airport is 4,300 ft AMSL.
Missed approach procedures
The missed approach procedure plays a pivotal role in instrument approach safety. It provides a standardised procedure for managing an aborted approach and landing attempt, ensuring appropriate terrain clearance to safely conduct flight operations in diverse environmental conditions.
Section 15.11 of the Part 91[9] Manual of Standards contains specific circumstances where a missed approach must be conducted.
A summary of these circumstances is as follows:
- during the final segment of an instrument approach, where the aircraft is not maintained within the applicable navigation tolerance for the aid in use
- when the required visual reference is not established at or before reaching the missed approach point from which the missed approach procedure commences
- when a landing cannot be made from a runway approach, unless a circling approach can be conducted in weather conditions equal to or better than those specified for circling
- when visual reference is lost while circling to land from an instrument approach.
Procedures outlined in the Aeronautical Information Publication (AIP) state that a missed approach must be conducted under certain conditions if the aircraft is below MSA. These conditions include, but are not limited to:
• issues arising with the radio aid,
• visual reference not being established, and
• a landing cannot be effected from the runway approach.
Operational procedures require that during a missed approach manoeuvre, an immediate climb is carried out to achieve an altitude that will remove the aircraft’s exposure to the risks of collision with terrain.
Instrument approach procedures
An instrument approach or instrument approach procedure (IAP) is a series of predetermined manoeuvres for the orderly transfer of an aircraft operating under instrument flight rules from the beginning of the initial approach fix to a landing, or to a point from which a landing may be made visually.
An IAP enables a descent below the MSA, positioning the aircraft to safely approach and land.
Operations below MSA increase the risk of collision with terrain or obstacles which are an immediate threat. Maintaining the published instrument approach path assures the pilot of obstacle clearance below the MSA. Outside of these areas, while below the MSA and in instrument meteorological conditions (IMC), separation from terrain and obstacles cannot be guaranteed and the pilot must conduct a missed approach procedure.
Recorded data
Automatic dependant surveillance broadcast (ADS-B) Exchange and Flightradar24 data was collected by the ATSB and was supplemented with OzRunways data provided by the pilot.
ATSB analysis combined the ADS-B flight data and the OzRunways aircraft track data to ascertain the track position and orientation of the aircraft during the occurrence.
At 1022:30 the aircraft deviated significantly to the left of the approach path resulting in the aircraft no longer being established on the ILS approach. The aircraft was below the MSA at 3,900 ft and continued to descend to the lowest point of 3,320 ft.
About 35 seconds later the aircraft crossed a ridgeline, further reducing the vertical separation with terrain to 810 ft above ground level.
Recorded data indicated (Figure 3) that 30–40 seconds after speaking to ATC and approximately 70 seconds after leaving the ILS approach profile, the pilot commenced a sustained climb and began tracking to the initial approach fix of LISZT. During this time the aircraft was operated below the MSA.
Figure 3: Aircraft vertical profile
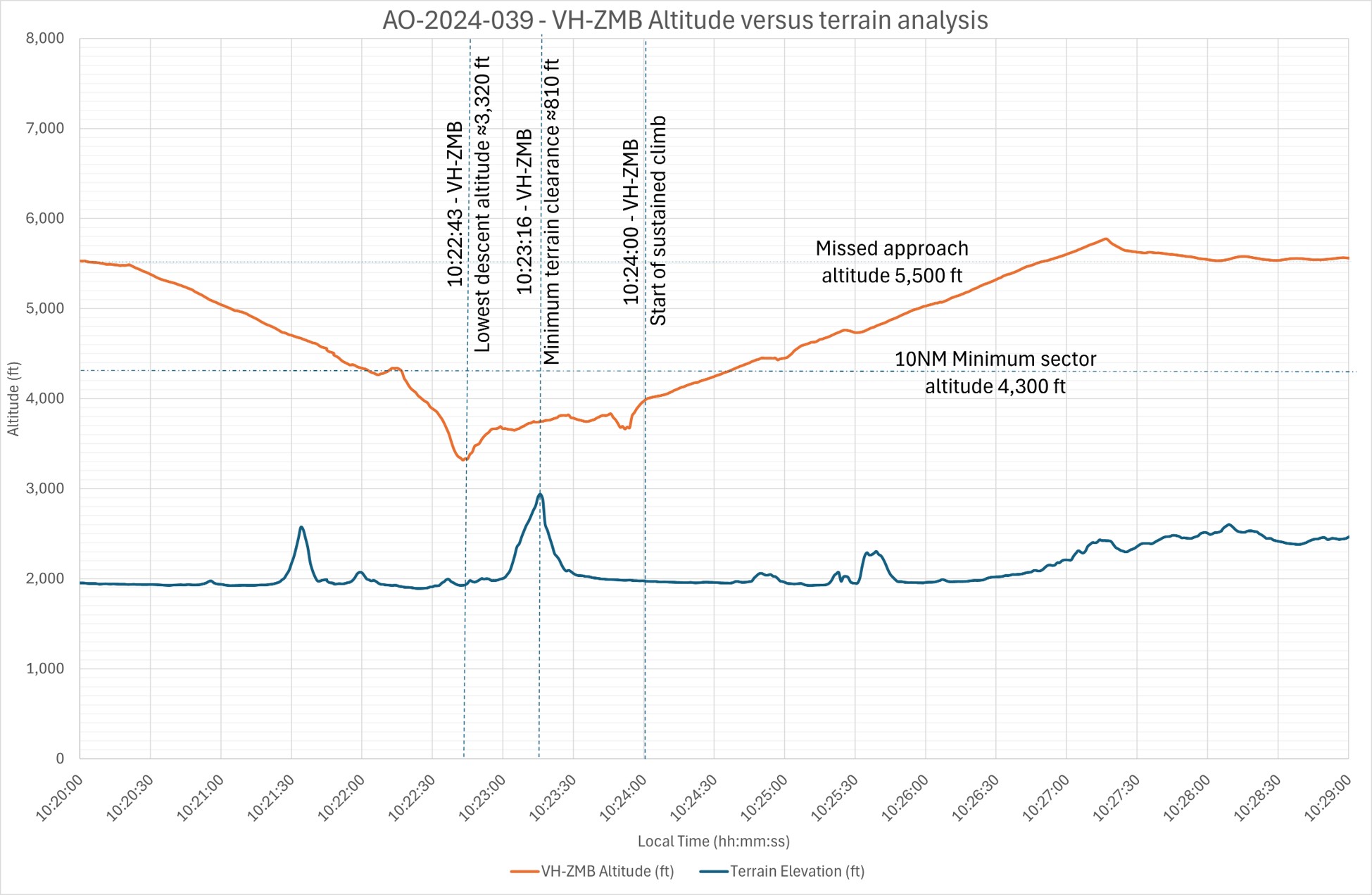
Source: ADS-B Exchange, Flightradar24 and OzRunways data analysed and annotated by the ATSB
Recorded data identified a significant left turn, greater than 60° AOB, with a subsequent bank to the right of greater than 40° AOB and a further left correction (Figure 4). These occurred while the aircraft was still descending. The descent was arrested, at an altitude of about 3,320 ft. With minimal climb observed for about 30 seconds before approaching rising terrain, the aircraft then passed over the ridgeline at a height of approximately 810 ft (Figure 3). (Note: Graphical figures contain smoothed data profiles that may not precisely reflect the exact data point at an exact period).
Figure 4: VH-ZMB bank angles
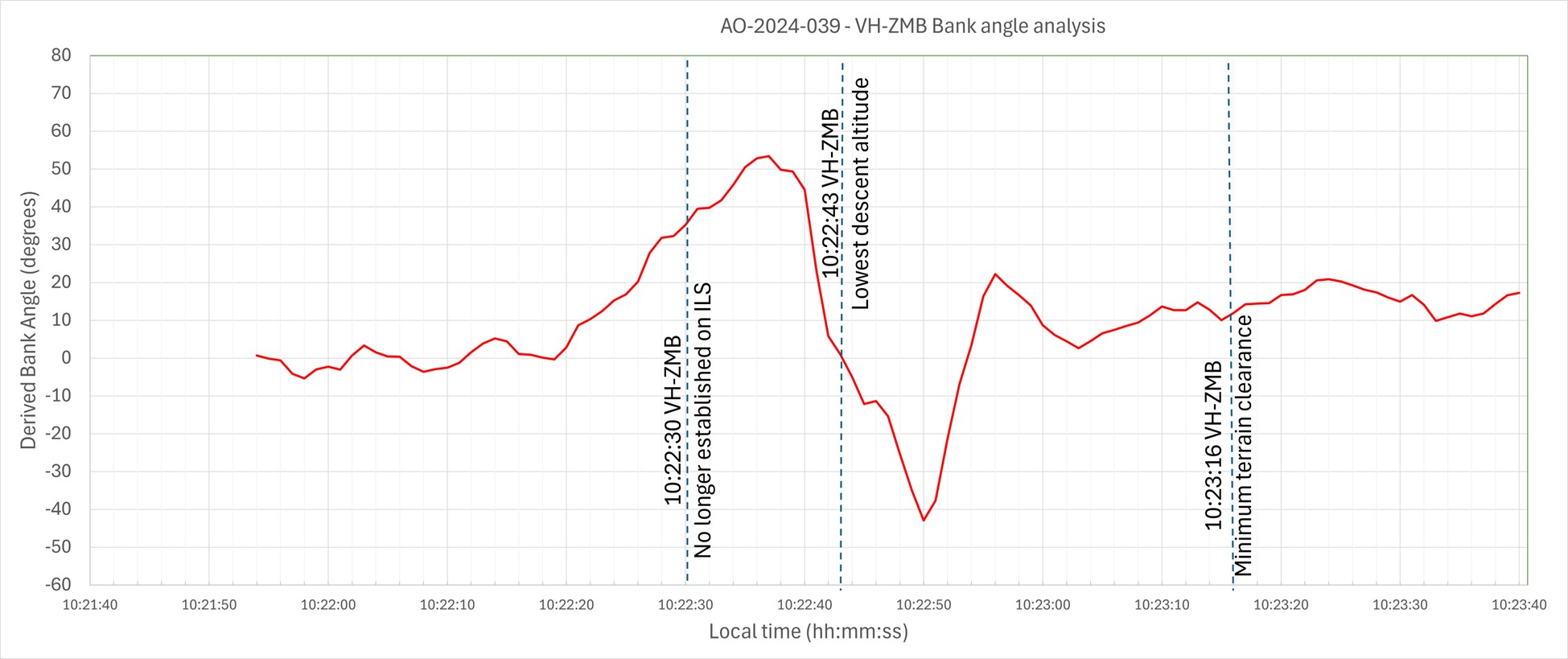
Source: ADS-B Exchange, Flight Radar 24 and OzRunways data analysed and annotated by ATSB
Vacuum‑powered gyroscopic instrumentation (artificial horizon)
The Cessna 310R is fitted with gyroscopic instruments[10] including an artificial horizon (AH), heading indicators and turn coordinators (turn and bank).
The vacuum system instruments on the Cessna 310R consist of 2 directional gyros, 2 AH gyros and the suction gauge.
The artificial horizon is the main instrument pilots use to fly through IMC. This instrument is considered a master instrument because it presents pitch and bank attitude information directly against an artificial horizon. It is a critical instrument to allow pilots to fly through non-visual and low-visibility conditions. It indicates the aircraft's orientation relative to the earth, expressed in pitch, roll, and yaw.[11]
Figure 5: Generic example of an artificial horizon

Source: Wikipedia
The gyroscopic instruments are powered by the vacuum system, consisting of a vacuum pump on each engine, pressure relief valve for each pump, a common vacuum manifold, vacuum air filter and suction gauge. Air pressure is used to rotate vanes to spin the instrument gyroscopes thus utilising gyroscopic forces as a mechanism that keeps the instrument level with respect to the direction of gravity. The AH gyro is mounted in a double gimbal, which allows the aircraft to pitch and roll as the gyro stays vertically upright.
The pilot reported that during the approach they noticed that the suction gauge was indicating ‘low pressure’. A partial blockage or issue in the pilot suction line, immediately after the air filter, could affect the pilot (left-side) AH and the suction gauge, with nil effect on the copilot (right-side) gauges.
However, post‑occurrence maintenance inspections and ground runs could not identify any abnormalities in the vacuum system.
Figure 6: Example of the suction gauge
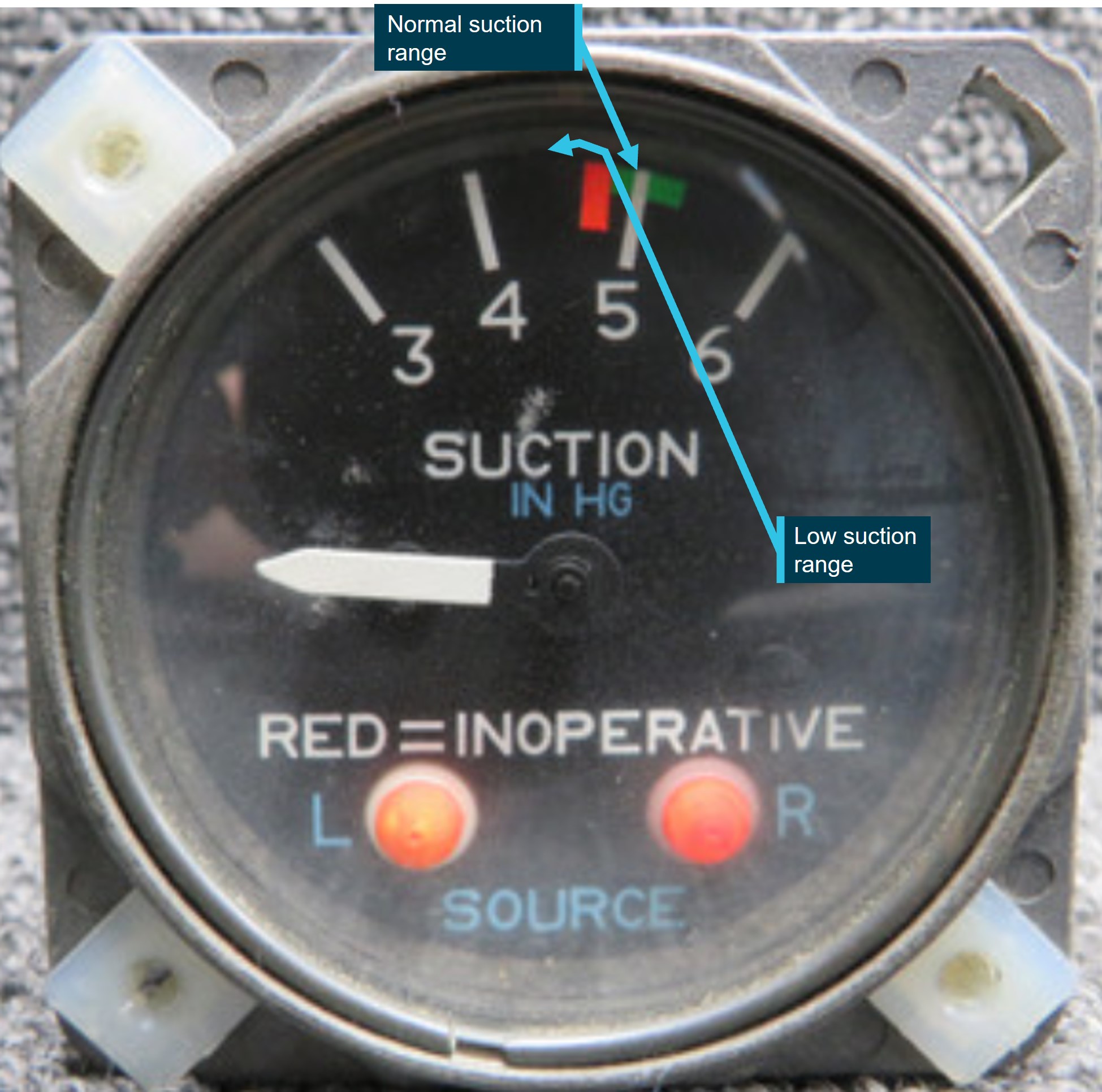
Source: ATSB
Post occurrence maintenance testing of the artificial horizon identified a gradual drift in pitch, up to 7°, and up to 4° drift in the roll axis over a period of 20 minutes. The AH deviations were gradual, inconsistent and outside the manufacturer’s required tolerances.
Flight automation and operator policy
Flight automation, such as an approved autopilot, utilises different control systems and technologies that reduce the requirements of human interaction.
An autopilot system can reduce the pilot’s workload. This is achieved by the automation taking over routine tasks such as maintaining altitude, heading, and airspeed. Subsequently allowing the pilot mental capacity to focus on other critical aspects of the flight, such as monitoring systems, flight path, weather conditions and communicating with air traffic control. This is particularly useful in times of a high workload environment.
The operator’s policy did not detail requirements on when it was appropriate or required to use the autopilot.
PAN PAN call
A ‘PAN PAN’ transmission is used to describe an urgent situation, but one that does not require immediate assistance. Examples of such situations include instrument malfunctions, deviation from route or entering controlled airspace without a clearance.
When an air traffic controller receives a PAN PAN call from an aircraft, the controller will declare an alert phase.[12] The Safety bulletin What happens when I declare an emergency, released by Airservices Australia, stated that ATC may provide a range of support services including:
• passing information appropriate to the situation, but not overloading the pilot
• allocating a priority status
• allocating a discrete frequency (where available) to reduce distractions
• notifying the Joint Rescue Coordination Centre (JRCC), appropriate aerodrome or other agency
• asking other aircraft in the vicinity to provide assistance.
An aircraft is in an urgency condition the moment that the pilot becomes doubtful about position, fuel endurance, weather, or any other condition that could adversely affect flight safety. The time for a pilot to request assistance is when an urgent situation may or has just occurred.
No ‘PAN PAN call was made by the pilot during the occurrence.
Air traffic control safety alert
A safety alert issued by air traffic control is instructions prefixed by the phrase 'SAFETY ALERT'. The AIP outlines a safety alert as:
ATC will issue a Safety Alert to aircraft, in all classes of airspace, when they become aware that an aircraft is in a situation that is considered to place it in an unsafe proximity to:
1. terrain;
2. obstruction;
3. active restricted areas; or
4. other aircraft.
A safety alert should trigger an appropriate response from the pilot to address and resolve the undesirable state.
When the pilot made contact with ATC, the controller reported observing a level of stress in the pilot’s voice and noticed the pilot tracking perpendicular to the approach path for the runway 12 ILS, below the MSA, towards rising terrain.
No safety alert was made by air traffic control during the occurrence.
Spatial disorientation
Spatial disorientation (SD) occurs when a pilot has a false perception of the motion or orientation of the aircraft with respect to the Earth (Ledegang & Groen, 2018), subsequently incorrectly interpreting the aircraft attitude, altitude or airspeed.
The ATSB publication Accidents involving Visual Flight Rules pilots in Instrument Meteorological Conditions (AR-2011-050) explains the basis of SD.
In order to correctly sense the orientation of the body relative to its environment, a pilot relies on a number of sensory systems in order to establish or maintain orientation:
» the visual system
» the vestibular system, which obtains its information from the balance organs in the inner ear
» the somatic sensory system which uses the nerves in the skin and proprioceptive senses in our muscles and joints to sense gravity and other pressures on the body.
The visual system is by far the most important of the three systems, providing some 80 per cent of the raw orientation information. In conditions where visual cues are poor or absent, such as in poor weather, up to 80 per cent of the normal orientation information is missing. Humans are then forced to rely on the remaining 20 per cent, which is split equally between the vestibular system and the somatic system. Both of these senses are prone to powerful illusions and misinterpretation in the absence of visual references, which can quickly become overpowering.
Pilots can rapidly become spatially disoriented when they cannot see the horizon. The brain receives conflicting or ambiguous information from the sensory systems, resulting in a state of confusion that can rapidly lead to incorrect control inputs and resultant loss of aircraft control.
The ATSB research report, An overview of spatial disorientation as a factor in aviation accidents and incidents (B2007/0063)identified that spatial disorientation is a very common problem and estimates that the chance of a pilot experiencing SD during their career is in the order of 90 to 100%. This report also detailed several international studies showing that SD accounts for some 6 to 32% of major accidents, and some 15 to 26% of fatal accidents. The report also identified that the true prevalence of SD events is almost certainly underestimated.
The FAA Advisory Circular, Pilot’s spatial disorientation (FAA AC60-4A) discussed the challenges associated with recovering from spatial disorientation. The results of a test conducted with qualified instrument pilots found that it took as much as 35 seconds to establish full control by instruments after a loss of an applicable visual reference.
Safety analysis
This analysis will explore the factors that involved aircraft directional changes, resulting in the aircraft deviating from the published ILS approach. The deviations occurred whilst the pilot was manually flying, in instrument meteorological conditions. The consequence of this deviation led to extended flight below the minimum sector altitude with increased pilot workload prior to recovering to a safe altitude.
The pilot reported being concerned with the aircraft’s location in relation to terrain, however, believed the aircraft was under control, attributing the unusual attitudes indicated on the artificial horizon to an instrument error rather than the aircrafts attitude.
The pilot reported that, at the time, false indications by the vacuum instruments were incorrectly indicating a turn to the right, which the pilot believed to be a consequence of erroneous instrument indications. The pilot recalled that their initial response to correct this was a turn to the left and believed that the vacuum instruments were still incorrectly indicating a level of bank even though the aircraft was level.
ATSB analysis of the recorded data reviewed the aircraft pitch and bank angles, descent and climb profiles, and aircraft tracks and timings confirmed that the instrument indications (at this time) correlated with high levels of bank and the aircrafts track.
Furthermore, although the pilot remembered observing a low vacuum pressure indication, a post‑incident system inspection indicated no identified problems with vacuum pumps or the check valves.
As such, it is almost certain that there was no instrument malfunction to the extent believed by the pilot. Rather, with no visual cues due to the IMC, the pilot likely became spatially disorientated and interpreted the real instrument indications as false as they mismatched the pilot’s sensed orientation.
As is common in spatial disorientation, the pilot likely followed their sense of direction rather than the (perceived faulty) instruments, leading to directional changes of up to 90° from the approach track as well as left and right angles of bank up to 65°, whilst continuing to descend.
However, post‑occurrence maintenance fault‑finding of the artificial horizon did identify a gradual drift in pitch, (up to 7°) and roll, (up to 4°) over a period of 20 minutes. While this may have indicated a degree of unserviceability of the instrument, this was not consistent with the reported sudden and absolute failure reported by the pilot.
Prior to the deviations on approach in IMC, the pilot descended below the minimum sector altitude. However, after deviating from the approach and no longer meeting approach tolerances, the pilot did not conduct a missed approach as quickly as practicable to achieve an altitude that would remove the aircraft’s exposure to the risks of collision with terrain.
Subsequently, the pilot was below MSA and no longer offered the protection of being on the approach. This situation was further exacerbated by the aircraft being in unusual attitudes and tracking perpendicular to the approach path, without intent. If this high-risk situation had been identified either by ATC issuing a safety alert or the pilot issuing a PAN PAN call, (a PAN PAN call should have triggered a safety alert to climb), a climb could have been expedited and the risk of proximity to terrain removed sooner than was the case.
Pilots should not hesitate to report an urgent condition when encountering situations that may not be immediately perilous but significantly increase risk.
ATC recordings indicated that the pilot notified ATC that they had incorrect artificial horizon information and had lost glidepath guidance. The pilot used their callsign twice, (which can often precede a distress call), and other verbal cues were also identified by the controller to indicate the pilot was under a level of stress. Being below the MSA and off the ILS, with indications of stress, was an opportunity for the controller to issue a safety alert to the pilot to climb immediately.
In an urgent situation such as this where the safety of the aircraft was uncertain, the broadcast of a PAN PAN call would have been appropriate. Had a PAN PAN call been broadcast, ATC would have almost certainly issued a safety alert. This would have required the pilot to conduct an immediate climb, removing their subsequent risk exposure to collision with terrain.
Flight data and recordings indicated that the aircraft was below MSA, from leaving the approach profile to commencing a sustained climb to a safe altitude, for greater than one minute. Additionally, the time elapsed from notifying ATC (below MSA), to commencing a sustained climb to a safe altitude, was greater than 30 seconds. During this time, in IMC, the aircraft came within 810 ft of terrain.
Instrument flight can be considered one of the more challenging operational environments to which a pilot can be exposed. Single-pilot operations have the potential to increase pilot workload (ALPA 2019).
Manually flying a single pilot approach in IMC increases the workload of any pilot. In this occurrence, the suspected loss of a primary instrument during an instrument flight rules approach, departing the ILS approach, experiencing unusual aircraft attitudes in IMC, and subsequently conducting a second approach all increased the workload of the pilot. Use of the autopilot system has the potential to significantly reduce the workload on pilots during this approach. This is achieved by the autopilot taking over routine tasks such as maintaining altitude, heading and airspeed. Thus, allowing the pilot to focus on other critical aspects of the flight. Whilst compliant with operator procedures at the time, use of the autopilot may have reduced the risk of spatial disorientation of the pilot on approach. The pilot reported that the autopilot could not be engaged post the occurrence, when positioning for the second approach.
Use of automation can afford the pilot spare mental capacity to recognise and address navigational deviations and tolerances. Thus, aiding the pilot to respond to the operational demands of the flight in a correct and timely manner.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the flight below minimum sector altitude involving Cessna 310R, VH-ZMB, 14 km west-north-west of Alice Springs Airport, Northern Territory, on 1 July 2024.
Contributing factors
- At about 8 NM from Alice Springs whilst established on the ILS approach in instrument meteorological conditions, the pilot likely experienced spatial disorientation that led to directional changes of up to 90° from the approach track as well as left and right angles of bank up to 65°, whilst continuing to descend.
- The pilot did not maintain track or glidepath and deviated from instrument landing system below the minimum sector altitude. Once outside of the required tolerances, the pilot did not conduct a missed approach, which increased the risk of collision with terrain.
- Air traffic control did not issue a safety alert. This would have alerted the pilot that they were in unsafe proximity to terrain and needed to climb immediately.
- The pilot did not broadcast a PAN PAN call notifying air traffic control and other traffic of their situation, leading to the pilot remaining below minimum sector altitude for an extended period without air traffic control instruction to climb.
Other factors that increased risk
- Post occurrence fault‑finding of the artificial horizon, identified gradual and inconsistent deviations outside the manufacturer’s required tolerances.
- The pilot did not utilise the autopilot for the approach even though they were in a high workload environment. The appropriate use of autopilot can reduce workload and subsequent risk of spatial disorientation such as during an instrument approach.
Safety actions
Safety action by Avcharter
The operator has since introduced an automation policy for the use of autopilot in conditions applicable to instrument meteorological conditions (IMC) and in high workload single-pilot environments.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot of the flight
- the head of flight operations for the operator
- Civil Aviation Safety Authority
- the aircraft manufacturer
- the maintenance organisation for VH-ZMB
- independent avionics specialists
- Airservices Australia
- recorded data from the GPS unit on the aircraft.
References
Airservices Australia. (2024) Aeronautical Information Publication Australia.
Airline Pilots Association International (ALPA) (2019) The dangers of single pilot operations Retrieved from
white-paper-single-pilot-operations.pdf
(1.31 MB)
Australian Transport Safety Bureau. (2007). An overview of spatial disorientation as a factor in aviation accidents and incidents. ATSB Aviation Research and Analysis Report B2007/0063.
Bailey, R. E., Kramer, L. J., Kennedy, K. D., Stephens, C. L., & Etherington, T. J. (2017, September). An assessment of reduced crew and single pilot operations in commercial transport aircraft operations. InN2017 IEEE/AIAA 36th Digital Avionics Systems Conference (DASC) (pp. 1‑15). IEEE.
Barnum, F., & Bonner, R. (1971). Epidemiology of USAF spatial disorientation aircraft accidents, 1 Jan 1958-31 Dec 1968. Aerospace Med, 42, 896-898.
Braithwaite, M., Durnford, S., & Crowley, J. (1998b). Spatial disorientation in US Army rotary-wing operations. Aviation Space Environ Med, 69, 1031-1037.
Cessna 1976, Pilot’s Operating Handbook, Cessna 310 Skyhawk, model C310R
Cheung, B., Money, K., Wright, H., & Bateman, W. (1995). Spatial disorientation implicated accidents in the Canadian forces, 1982-92. Aviation Space Environ Med, 66, 579-585.
Civil Aviation Safety Authority. (2020) Part 91 (General Operating and Flight Rules) Manual of Standards.
Federal Aviation Authority. (1983). Advisory Circular AC60-4A: Pilot’s spatial disorientation
Gillingham, K., & Previc, F. (1996). Spatial orientation in flight. In R. DeHart (Ed.), Fundamentals of aerospace medicine (2nd ed., pp. 309-397.). Baltimore: Williams & Wilkins
Hixson, W., Niven, J., & Spezia, E. (1972). Major orientation error accidents in regular Army UH-1 aircraft during FY 1969. Accident factors report namrl1169. Pensacola, FL: Naval Aerospace Medical Research Laboratory.
Knapp, C., & Johnson, R. (1996). F-16 class a mishaps in the U.S. Air Force, 1975- 93. Aviat Space Environ Med, 67, 777-783
Ledegang, W. D., & Groen, E. L. (2018). Spatial disorientation influences on pilots’ visual scanning and flight performance. Aerospace medicine and human performance, 89(10), 873-882.
Lyons, T., Ercoline, W., O’Toole, K., & Grayson, K. (2006). Aircraft and related factors in crashes involving spatial disorientation: 15 years of U.S. Air Force data. Aviat Space Environ Med, 77, 720-723.
Moser, R., Jr. (1969). Spatial disorientation as a factor in accidents in an operational command. Aerospace Med, 40, 174-176.
Singh, B., & Navathe, P. (1994). Indian Air Force and world spatial disorientation accidents: A comparison. Aviation Space Environ Med, 65, 254-256.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a peon receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- The pilot of the flight
- The operator
- Air traffic controller
- Airservices Australia
- Civil Aviation Safety Authority
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Flight operated under Part 135 of the Civil Aviation Safety Regulations. Part 135 of the Civil Aviation Safety Regulations (CASR) covers the air transport rules for smaller aeroplanes.
[2] Flight was operated under Part 91 of Civil Aviation Safety Regulations. Part 91 of the Civil Aviation Safety Regulations (CASR) – General operating and flight rules, sets out the general operating rules for all pilots and operators. It consolidates all of the general operating and flight rules for Australian aircraft.
[3] Instrument Landing System (ILS) approach is defined as a precision runway approach aid based on two radio beams which together provide pilots with both vertical and horizontal guidance during an approach to land.
[4] Instrument meteorological conditions (IMC) means meteorological conditions other than visual meteorological conditions.
[5] Instrument proficiency check means an assessment, against the standards mentioned in the Part 61 Manual of Standards, of a pilot’s competency to pilot an aircraft under the IFR
[6] Total cloud amount measured visually by the fraction (in eighths or oktas) of the sky covered by clouds.
[7] Stratus clouds tend to be featureless, low altitude clouds that cover the sky in a blanket of white or grey.
[8] VHF Omni Directional Range (VOR) navigation consists of a ground-based component, called VOR stations, (as well as receivers installed in the aircraft). VOR stations are infrastructure, often located at terminal areas, to aid in navigation and approaches.
[9] Part 91 of Civil Aviation Safety Regulations, General operating and flight rules.
[10] Gyroscopic flight instruments are instruments which have a mechanical gyroscope incorporated into their design.
[11] Rotation around the front-to-back axis is called roll. Rotation around the side-to-side axis is called pitch. Rotation around the vertical axis is called yaw.
[12] Alert phase: a situation where apprehension exists as to the safety of an aircraft and its occupants (this generally equates to a PAN PAN).
Occurrence summary
| Investigation number | AO-2024-039 |
|---|---|
| Occurrence date | 01/07/2024 |
| Location | 14 km WNW of Alice Springs Airport |
| State | Northern Territory |
| Report release date | 20/03/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Avionics/flight instruments, Flight below minimum altitude, Warning devices |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 310R |
| Registration | VH-ZMB |
| Serial number | 310R0815 |
| Aircraft operator | AvLease Pty Ltd |
| Sector | Piston |
| Operation type | Part 135 Air transport operations - smaller aeroplanes |
| Departure point | Willowra |
| Destination | Alice Springs |
| Damage | Nil |
Jandakot Chipmunk aircraft accident preliminary report
A preliminary report details evidence gathered to date by the ATSB from its ongoing investigation into an accident involving a Chipmunk aircraft at Perth’s Jandakot Airport on 26 April 2024.
ATSB investigators deployed to Jandakot after the DHC-1 Chipmunk, a former military pilot training aircraft, collided with the ground within the airport boundary shortly after take-off.
The pilot, who was the sole occupant, sustained fatal injuries in the accident.
Prior to the accident, the aircraft had been taxied by the pilot from Jandakot’s southern apron to the end of runway 24L, the report details.
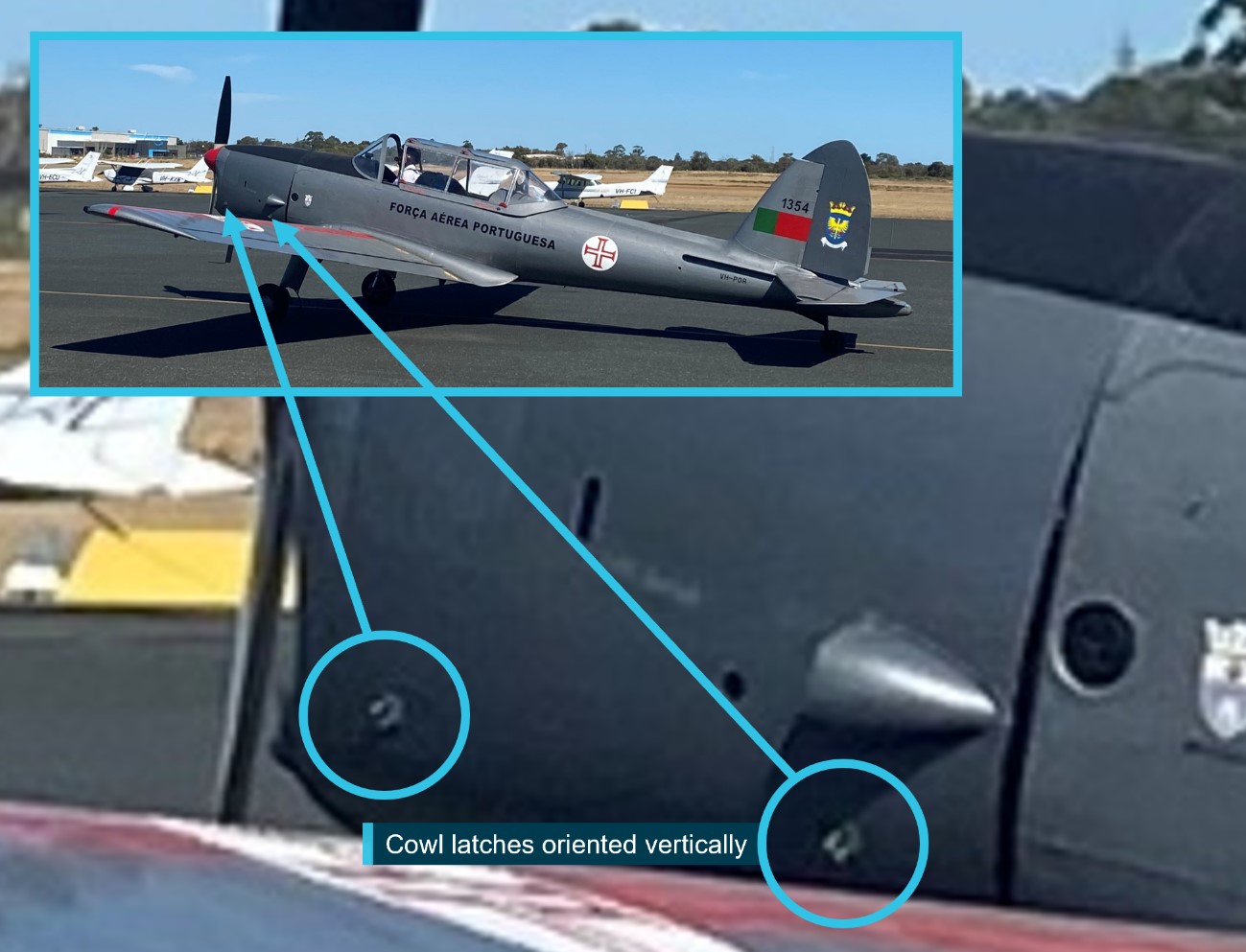
“A witness on the southern apron took photographs of the aircraft taxiing past, and these show the latches on the left side engine cowl were oriented vertically,” Chief Commissioner Angus Mitchell said.
The Chipmunk’s left and right engine cowling doors are each secured by two latches. The latches fasten the doors when they are in the horizontal position, and the doors are unfastened when the latches are vertical.
After the pilot was given clearance, they began the take-off roll, and the aircraft became airborne about halfway along the runway.
“One witness recalled seeing something ‘flapping’ on the aircraft during the take-off,” Mr Mitchell explained.
That witness, and others in a nearby building, observed the aircraft roll to the left at low height near the end of runway 24L.
“Camera footage showed the aircraft’s angle of bank increasing and the aircraft descending into terrain. A camera about 180 m to the south-east of the accident site recorded the engine cowling on the left side opening and closing in the seconds prior to the accident.”
ATSB investigators’ wreckage examination noted damage to the engine cowl latches indicative of their being correctly fastened on the right side and unfastened on the left.
“All major aircraft components were accounted for, witnesses had not reported any change in engine sound prior to the accident, and the propeller showed evidence that the engine was running at impact,” Mr Mitchell said.
ATSB examination established continuity of the aircraft’s flight controls, and the flaps were assessed to have likely been in the retracted position at time of impact.
As the investigation progresses, the ATSB will conduct further examination of the aircraft components, review aircraft and pilot documentation, and analyse the aircraft’s flight path, and impact forces.
A final report, which will detail analysis and the ATSB’s findings, will be released at the conclusion of the investigation.
“Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken,” Mr Mitchell concluded.
Read the preliminary report: Collision with terrain involving a Oficinas Gerais de Material Aeronautico DHC-1 MK 22 Chipmunk, VH-POR, at Jandakot Airport, Western Australia, on 26 April 2024
Smoke and fumes event involving a Cessna 208, near Horn Island, Queensland, on 18 March 2024
What happened
On 18 March 2024, a Cessna 208 (Caravan) aircraft was being operated with a pilot and one passenger on a service from Horn Island to Murray/Mer Island, Queensland.
Shortly after take-off, the pilot became aware of very hot air entering the cockpit from beneath the instrument panel. The temperature of the air was such that the pilot chose to return the aircraft to Horn Island, and while doing so, pulled the cabin heat control in an endeavour to diagnose the issue. Shortly after, smoke began entering the cockpit area – described as ‘initially quite thick’, but beginning to clear with only ‘a little bit wafting up’.
After advising Brisbane Centre air traffic control of the decision to return and the flight particulars, the aircraft returned to Horn Island, where the pilot made an uneventful approach and landing. There were no reported injuries or adverse effects to the pilot or passenger.
Engineering inspections
The operator’s engineering inspections of the aircraft while grounded at Horn Island identified an engine bleed air control valve that had stuck and not fully closed, allowing a continuous flow of hot bleed air into the cockpit while the engine was operating. Heating of oil residues within the bleed air diverter box (part of the bleed air management system) created the smoke and fumes reported by the pilot.
Further investigations by engineering staff found that the bleed air control valve as-fitted to the occurrence aircraft was of a poppet-valve type (part number 1H101-3 or -4), whereas other C208 aircraft in the operator’s fleet employed a butterfly-valve type (part number 1422-6 or -7).
The aircraft maintenance documentation noted that the P/N 1H101-3/4 poppet valves were fitted to earlier C208 aircraft with serial numbers less than 20804999, whereas the P/N 1422-6/7 butterfly valves were specified for later aircraft with serial numbers 20805000 and above.
The aircraft operator also noted that the maintenance documentation for the valve removal, installation and servicing was not inclusive of aircraft within their fleet. Advice from the aircraft manufacturer, Textron Aviation, acknowledged the omissions and noted that the instruction scope would be expanded with the next manual revision.
Safety message
Operators and maintainers of Cessna Aircraft Company model 208 and 208B aircraft are advised to ensure the engine bleed air flow control valve/s fitted to their aircraft are inspected and maintained in accordance with the manufacturer’s instructions. In instances where aircraft serial numbers (or number ranges) are not covered by those instructions, operators and maintainers are encouraged to contact the aircraft manufacturer or representative to ascertain the specific maintenance activities that apply to those aircraft.
About this report
Decisions regarding whether to investigate, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2024-007 |
| Occurrence date | 18/03/2024 |
| Location | Near Horn Island Aerodrome |
| State | Queensland |
| Occurrence class | Incident |
| Aviation occurrence category | Air/pressurisation |
| Highest injury level | None |
| Brief release date | 02/07/2024 |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 208 |
| Sector | Turboprop |
| Operation type | Part 135 Air transport operations - smaller aeroplanes |
| Departure point | Horn Island Airport, Qld |
| Destination | Murray/Mer Island ALA, Qld |
| Damage | Nil |
Interactive wildlife strike database published
The ATSB has launched a new interactive tool allowing pilots, aerodrome and aircraft operators and members of the public to review figures on wildlife strikes with aircraft across Australia.
The National Aviation Wildlife Strike Dashboard, published today, details all wildlife strikes reported to the ATSB over the last ten years.
“Wildlife strikes – particularly birdstrikes – represent around a third of the 5,500 aviation occurrences reported to the ATSB each year,” Chief Commissioner Angus Mitchell noted.
“While the vast majority of these do not result in any injury to flight crew or passengers, they are a potential safety risk, and present a significant economic cost for aerodrome and aircraft operators.
“This dashboard aims to provide information back to pilots, aerodrome and aircraft operators, regulators, and other industry participants, to assist with understanding and managing the hazards associated with wildlife strikes.”
In the past, the ATSB has published periodical data reports detailing wildlife strike data. The new dashboard will instead make the data available for analysis on a more regular basis.
The dashboard includes a number of different filtering methods, for stakeholders to better understand the data relevant to their operation.
Mr Mitchell noted a pair of recent birdstrikes involving Australian-registered passenger aircraft – one which returned to Sydney shortly after a birdstrike on take-off, and another which diverted to Invercargill after a birdstrike on take-off from Queenstown.
Mr Mitchell also noted another incident earlier this month, where a Royal Flying Doctor Service PC-12 collided with a cow during landing at a remote airstrip in WA’s Pilbara region.
“While these incidents were safely managed by crews, and fortunately did not result in any injuries to those on board the aircraft, they serve as recent demonstrations of the hazards wildlife strikes pose to the aviation industry.”
The ATSB investigated a pair of fatal wildlife strikes in 2022 – a Bell 206 LongRanger which collided with terrain after being impacted by a wedgetail eagle during flight in the NSW Hunter Region, and an agricultural spraying aircraft which collided with terrain after striking an Australian bustard near Chinchilla, Queensland.
“These two accidents demonstrate the risk wildlife strikes can pose to light aircraft during private and commercial operations,” Mr Mitchell concluded.
Find out more about the dashboard, and try it out, here.
National Aviation Wildlife Strike Dashboard
The National Aviation Wildlife Strike Dashboard allows users to search for wildlife (bird or animal) strike incidents and accidents reported to the ATSB. Users can refine the data using several parameters including occurrence time, location, aircraft type and activity group.
Why the ATSB produced this dashboard
Occurrences involving aircraft striking wildlife, particularly birds, continue to be the most common aviation occurrence reported to the ATSB. Wildlife strikes are a potential safety risk and present a significant economic risk for aerodrome and aircraft operators. The aim of this dashboard is to provide information back to pilots, aerodrome and aircraft operators, regulators, and other aviation industry participants to assist them with understanding and managing the risks associated with bird and animal strikes. The data in the dashboard does not include any identifying information about the aircraft (no aircraft registration or operator names) or pilots.
How the data is collected?
ATSB data is collected through the mandatory occurrence reporting requirements of the Transport Safety Investigation Act 2003 and associated Regulations from the aviation industry. It is provided publicly as a result of the cooperative efforts between the ATSB and the aviation industry as a whole.
An explanation of the reporting requirements (what to report and who is responsible for reporting) is explained on the ATSB Aviation reporting requirements page. For wildlife strikes, apart from accidents and serious incidents which are immediately reportable to the ATSB, other strikes are routine reportable (within 72 hours) via the ATSB aviation incident reporting form. Routine reportable wildlife strikes includes birdstrikes and animal strikes (including when the pilot suspects a birdstrike/animal strike) where the aircraft is in flight, or taking off or landing anywhere. It also includes birdstrike and animal strikes based on evidence from where a carcass is found on a runway. Reporting does not include near strikes.
Data refresh cycle
To align with reporting, data processing and data quality review timelines, this dashboard is updated on the 3rd Friday of each month containing data from the previous 10 years and the current year up to 2 months prior to the refresh date.
Due to processing delays, not all reported occurrences from airlines after July 2021 are included in the dataset at this stage. This has been related to technical difficulties that are now resolved and the ATSB is working through the backlog and will update this page as processing is progressed.
Can I download the whole database?
No. The ATSB limits exporting of data from the National Aviation Occurrence Database (including reported wildlife strike occurrences), which has been made available for general statistical purposes only. This is due in part to the need for the ATSB to preserve confidentiality, continuously update and improve data on receipt of additional information and ongoing data cleaning efforts. The National Aviation Occurrence Database is the only authoritative and controlled dataset that is updated regularly. Some data may be missing, incomplete or yet to be reported and/or processed.
The ATSB does not endorse, and disclaims any responsibility for, use of the data beyond general statistical purposes. The ATSB also does not endorse the use of its aviation occurrence data for any commercial purposes.
Taxonomy and terminology
The ATSB uses several taxonomies (including activity group, occurrence category and classification) to efficiently and consistently categorise and code transport safety occurrences. Read more here.
Wildlife descriptors and groupings
Bird and animal species types are grouped by similar species. These groupings were defined by grouping birds and animals of similar species, size, and/or appearance. These groupings were applied because similar birds are often reported to the ATSB as an incorrect species. In addition to these groupings, the complete list of bird and animal species is also included in the dashboard. For the purpose of this dashboard, the birdstrike data includes all flying animals (including bats and flying foxes). Animal strikes were considered to involve all non-flying animals (including flightless birds: for example Emus and Cassowaries). The bird ingestion (into an engine) requirements outlined in the United States Federal Aviation Regulations (FAR) 33.76(Opens in a new tab/window) were used as a guide to develop bird size categories. The bird size categories used are outlined below:
- small bird: up to and including 0.085 kg
- medium bird: greater than 0.085 kg, and up to and including 1.15 kg
- large bird: greater than 1.15 kg, and up to and including 3.65 kg
- very large bird: greater than 3.65 kg.
Location data
Wildlife strikes are sometimes identified during a pre-, or post-flight aircraft inspection, where the previous flight crew had no knowledge of striking an animal/bird. In these cases, the location of the wildlife strike has been set to ‘unknown’, rather than at the aerodrome where the inspection was carried out. The proximity of the aerodrome to a wildlife strike has been coded as either:
- on aerodrome (within the aerodrome’s border)
- off aerodrome < 10 km (from the aerodrome’s border to 10 km from the aerodrome)
- off aerodrome > 10 km (outside 10 km from the aerodrome)
- unknown.
In the dashboard, generally at aerodrome locations within the map, multiple occurrences are located at the same latitude and longitude. This typically occurs when the reported location is ‘on aerodrome’ with the latitude/longitude for the aerodrome being used instead of a more accurate position within the aerodrome.
Activity types
The activity group for aircraft involved in a wildlife strike presented in this dashboard. These are defined as:
- Commercial air transport: includes scheduled and non-scheduled commercial passenger carrying and freight operations
- General aviation/recreational: includes aerial work, instruction flying, sport and pleasure flying and other general aviation activities
- Military: all flights where a military aircraft is involved
- Unknown activity group: flying where the activity group is unknown.
Limitations of the dataset
The data quality and consistency is largely dependent on the details reported to the ATSB. The information in the majority of non-investigated occurrence reports is not subject to thorough verification. Species are often recorded as unknown as this is what is reported to the ATSB. When reporting bird and animal strikes to the ATSB, please include as much detail as possible to ensure the highest level of information can be provided back to you through this dashboard, including (when known) species or common bird/animal name and size.
The dataset is subject to change. The ATSB may need to update and improve these data as it receives additional information and validates the data already received.
The ATSB data includes information obtained from all reports that meet the reporting requirements of the Transport Safety Investigation Regulations 2021. Not all notifications reported to the ATSB are classified as occurrences (incidents, serious incidents or accidents). Those that are deemed to not be a transport safety matter are classified as ‘events’, including suspected strikes or near misses. Events are not included in this dashboard.
Using the dashboard
There are 6 wildlife dashboards available through the page button at the bottom of the dashboard:
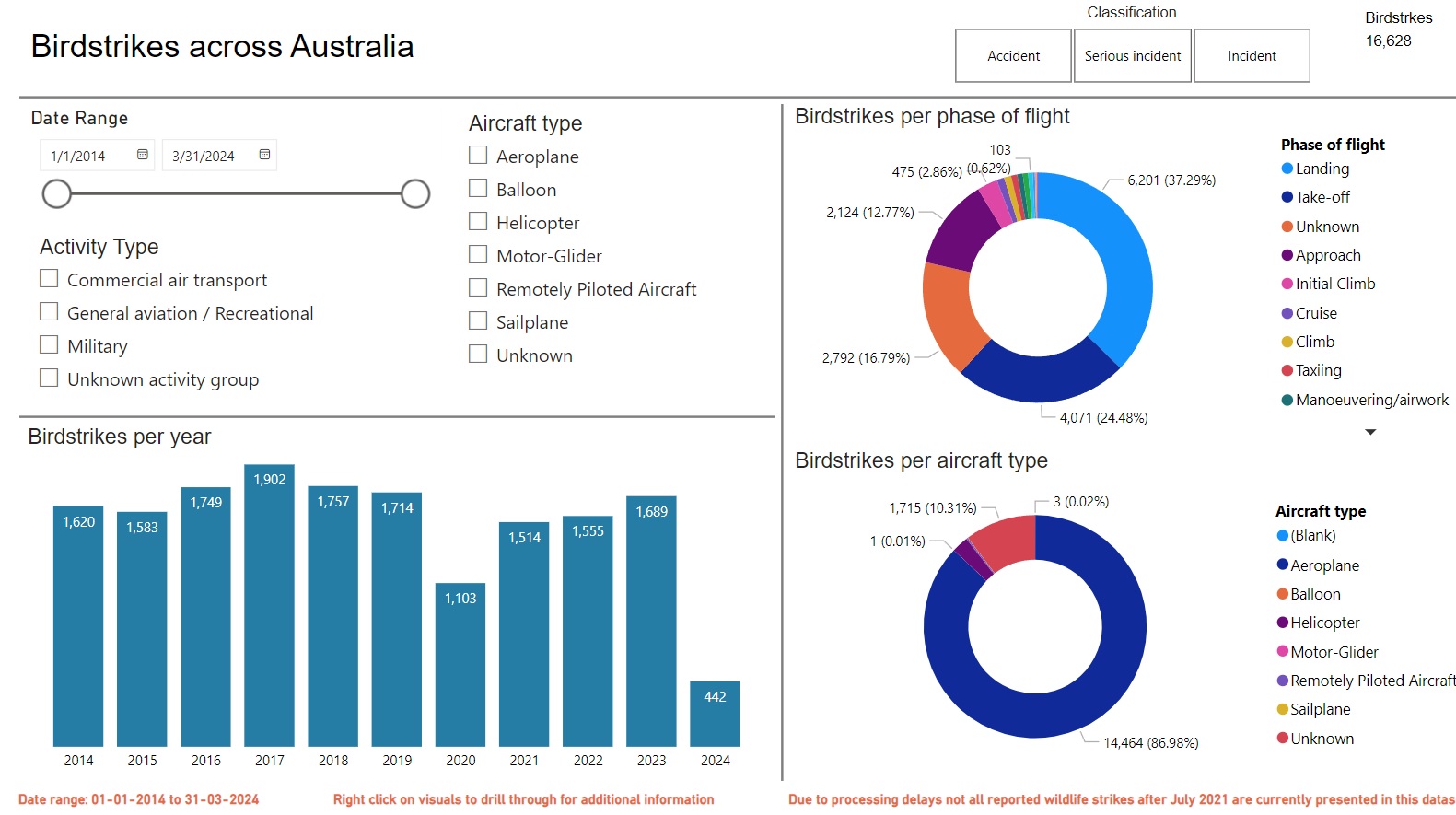
- Birdstrikes across Australia
- Birdstrikes by year and location
- Birdstrikes by species and location
- Significant birdstrikes
- Animal strikes across Australia
- Animal strikes by species and location
Further information regarding wildlife strikes can be obtained by ‘drilling through’ (right clicking) on visuals in the dashboard to display a data table containing all relevant details of the occurrence.
Disclaimer on data use
The ATSB collects aviation safety data and investigates air safety occurrences for the sole purpose of enhancing aviation safety. Consequently, the ATSB material is confined to matters of safety significance and may be misleading if used for any other purpose.
The ATSB aims to publish occurrence data as soon as reasonably practicable after receiving reports from industry. However, depending on workload and the volume of reports received, it may take time to input and process the reported data from when we received the report. If you are seeking data or information on a specific recent occurrence that does not appear in search results, you should contact the ATSB via email: atsbinfo@atsb.gov.au.
When using this data, it is important to remember that occurrence data is provided to the ATSB by responsible persons as defined in the Transport Safety Investigation Regulations 2021.
The ATSB accepts no liability for any loss or damage suffered by any person or organisation resulting from the use of these data. The ATSB does not warrant the completeness, accuracy or suitability of these data and the database for your intended purpose.
Incorrect configuration involving Bombardier DHC-8-402, VH-QOI, Horn Island Airport, Queensland, on 26 June 2024
Final report
Report release date: 21/01/2025
Executive summary
What happened
On 26 June 2024, a De Havilland Canada DHC-8-402 (Dash 8), was preparing to operate a QantasLink passenger flight from Horn Island to Cairns, Queensland. The flight crew identified that the take-off would be performance-limited due to the runway length at Horn Island and the high passenger and cargo weights. The crew determined that a flap setting of 15° and the bleed air system switched off was required for take-off.
During pre-flight preparation, the first officer (FO) was the pilot flying and inadvertently selected a flap setting of 5° instead of the required flap setting of 15°. The crew completed the after start checks and after start checklists in accordance with the standard operating procedures, however neither the first officer, nor the captain as pilot monitoring, detected the incorrect flap setting.
During the initial take-off run, the Dash 8 accelerated normally, however the crew noted that the aircraft’s rotation was slow and that the aircraft performance differed from their usual experience during take-off. The first officer’s application of continued back pressure to the controls during the take-off run resulted in the aircraft successfully becoming airborne slightly after the expected rotation speed. The first officer identified that the flaps were configured at a setting of 5° and immediately advised the captain. The captain instructed the first officer to continue to fly the aircraft. The first officer slightly lowered the nose of the aircraft to increase airspeed. The aircraft accelerated in response to this action and a positive rate of climb was maintained. The flight continued to Cairns without further incident.
What the ATSB found
During preparation for take-off from Horn Island, the FO inadvertently selected the flap lever to 5° instead of the required setting of 15°. This was likely due to habitual behaviour as the flap setting of 5° was the most common take-off flap setting for other sectors in the network and was the flap setting required on the 2 sectors flown prior to the incident. Standard pre‑flight checks and crosschecks were conducted, however the flight crew failed to identify the incorrect flap setting before take-off at Horn Island. This was likely due to automatic behaviour by the crew registering flap 5° to be the usual setting at take-off.
What has been done as a result
Following the occurrence, the operator implemented the following organisational and operational, changes:
- Review of standard operations procedures as necessary to reduce the likelihood of erroneous flap selection and misidentification.
- Review of relevant checklists to strengthen crosschecking in accordance with the computed take-off performance data.
- Training for crew focusing on standard operating procedures and compliance.
Safety message
The preparation, taxi and take-off phases of flight involve high workload and demand heightened attention to ensure correct settings are selected as unintentional slips can easily occur without. To minimise the risk of slips going unnoticed, flight crews must carefully verify and methodically complete checks and checklists. Maintaining focus and staying mindful of potential deviations to usual settings is essential during periods of high workload for safe operations.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On 26 June 2024, a De Havilland Canada DHC-8 402 (Dash 8) registered VH-QOI was being prepared to operate a QantasLink passenger flight from Horn Island, Queensland, following an arrival from Cairns. The aircraft arrived at Horn Island airport about 1015 local time and was scheduled to return to Cairns at 1055 with the same flight crew. The crew consisted of the first officer (FO), assigned as the pilot flying, the captain in the role of pilot monitoring and 2 cabin crew.
The flight crew followed standard pre-departure procedures in preparation for the flight. The FO loaded the flight plan into the flight management system (FMS)[1] and the captain confirmed the FMS was programmed in accordance with the flight plan. During the confirmation, the captain had to adjust performance data calculations that had previously been entered. This was prompted by a revised forecast for adverse weather conditions for arrival at Cairns and a full passenger load. The captain reported repeatedly checking the automatic weather information service due to changes in the prevailing wind and efforts to avoid offloading any passengers due to weight restrictions. The captain stated that they made several calls to load control and frequently checked the automated weather information service to calculate the headwind component for the final performance data which allowed for the uplift of all the passengers and their baggage.
The main runway length for runway 08 at Horn Island is considered performance limiting for Dash 8 operations at a length of 1,389 m, with higher terrain near the departure end presenting a potential obstacle. The captain was cognisant of the aircraft performance limitations as the aircraft was carrying a full load. The calculation of thrust requirements, and the corresponding FMS entries, were made prior to the engine start. The FO reported that each flight crew programmed their own Aerodata apps[2] on their iPads to calculate the airspeeds required for take-off, based on the weather information and the aircraft weight. The final weight of the aircraft was 27,800 kg and was close to the maximum regulated take‑off weight (RTOW). The Aerodata results produced a requirement to turn off the bleed air system to provide the increased thrust necessary for take-off with a flap[3] setting of 15°. The FO recorded this information on the take-off and landing distance card (TOLD)[4] card.
After the passengers were boarded, the flight crew conducted the before start procedure and then commenced taxiing to runway 08. The crew then conducted the after start checks and checklist, during which time the FO inadvertently selected flap 5° instead of 15°. The checklist is completed as a ‘challenge and response’ format. The FO calls the check which requires a verbal confirmation from the captain. One of the items on the list specifically called for is the flap setting. The FO called for ‘flaps’ and recalled that they checked that flap 5 was indicating for the flap lever and the digital indications. However, the captain did not recall the response given for this challenge during interview.
For the take-off run, the crew reported no issues with acceleration as the aircraft increased speed along the runway until the captain called for ‘V1’[5] and ‘rotate’. The FO described the rotation as slow but reported rationalising the heavy weight of the aircraft as the reason and continued to apply more pressure to the control column until the aircraft rotated about 5 kt after the planned rotation speed.
The flight crew noticed that aircraft performance was not what they would normally expect at the start of the climb. The captain checked the speeds and trim which were identified as being set correctly. At about the same time, the FO checked the flap setting and noticed that the flaps were configured to 5° and alerted the captain immediately.
By this time, the main landing gear was up and the captain instructed the FO to continue to fly the aircraft. The FO momentarily lowered the nose of the aircraft by a small amount to assist with increasing the airspeed. The aircraft accelerated and continued to Cairns without further incident.
Context
Aircraft information
VH-QOI was manufactured in Canada in 2008 and was powered by 2 Pratt & Whitney Canada PW150A (turboprop) engines.
Flight crew information
The captain held an air transport pilot licence (aeroplane) and had been flying for about 30 years with a total aeronautical time of about 8,450 hours, of which 5,800 hours were on the Dash 8.
The FO had been flying for 12 years and held a commercial pilot licence (aeroplane) with about 3,870 hours, of which 346 were on the Dash 8.
Both pilots had valid class one medical certificates.
Meteorological conditions
The meteorological aerodrome report provided the weather observations for Horn Island as warm and humid, with moderate south-east winds to 13 kt, good visibility and broken to overcast clouds. The valid terminal forecast for Cairns airport was issued at 0902 local time and identified a temporary forecast for showers of moderate rain and scattered cloud at 3,000 ft with periods of 30–60 minutes where showers of rain were forecast, potentially reducing visibility to 7,000 m.
Airport information
Horn Island airport is located at the northern end of Cape York Peninsula and is one of the primary airports for local transportation. The main runway orientation is 08/26 and is 1,389 m in length and has an elevation of approximately 13 m above mean sea level. Some higher terrain and trees are located at the of end of runway 08 and are a potential obstacle.
Recorded information
Flight data from the aircraft’s quick access recorder (QAR) was provided to the ATSB and contained about 70 seconds of data, recorded at one-second resolution, commencing at the beginning of the take-off on runway 08 at Horn Island (Figure 1). The data indicated that the Dash 8 had the flaps set to 5° prior to taxi and were retracted as the aircraft was flying through 1,406 ft above mean sea level.
Figure 1: QAR derived flight data depicting aircraft position and flap setting
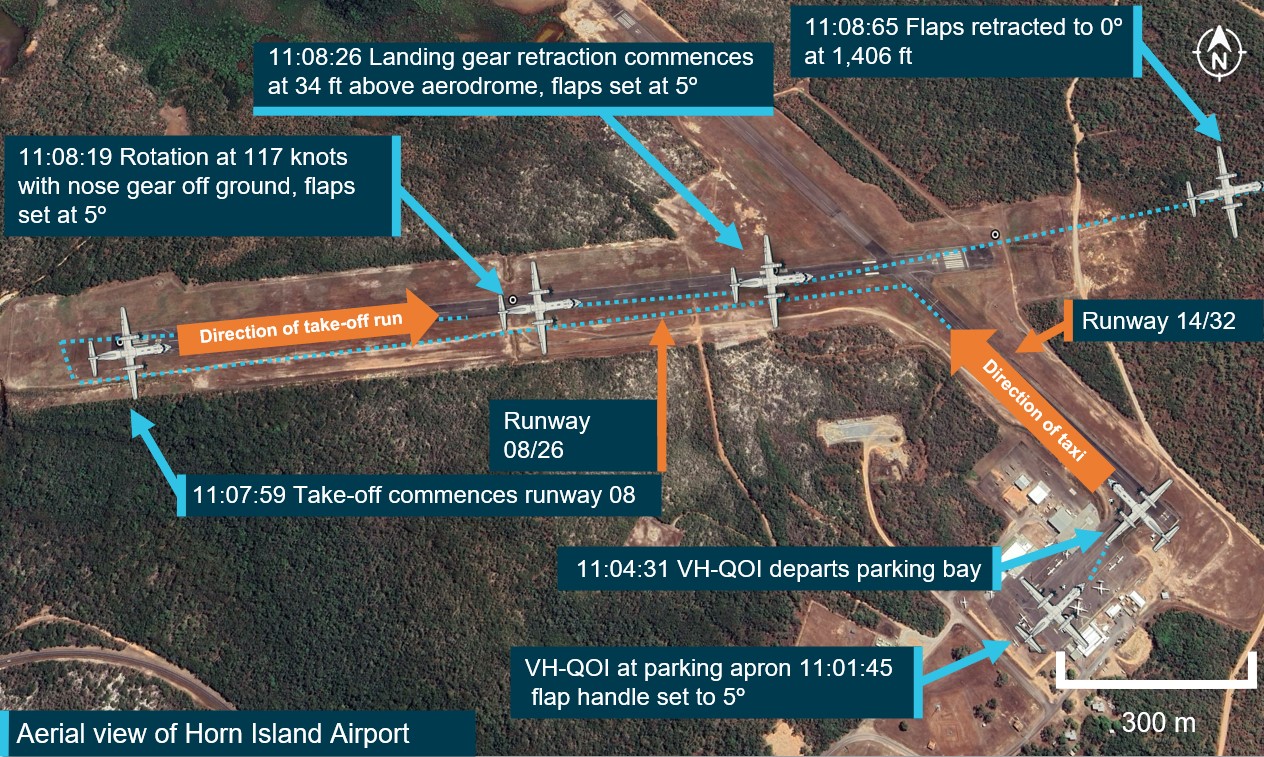
Source: QAR data and Google Earth, annotated by the ATSB (all heights indicated as above mean sea level). Note: Dash 8 figures not to scale
Take-off distance
In the event of an engine failure during take-off, pilots must actively monitor several key speed parameters in order to ensure the aircraft can either continue or reject the take-off and stop on the runway if necessary. These are collectively referred to as ‘V speeds’.
- Should an engine failure occur before V1 the aircraft should be able to stop within the distance of the remaining runway.
- V2 is the speed that ensures that the aircraft can continue climbing safely with one inoperative engine in an emergency.
- Vr is the speed at which the rotation of the aircraft is initiated to take-off attitude. This speed cannot be less than V1
The QAR data determined that the mismatch in actual versus intended take-off flap configuration meant that the calculated take-off reference speeds and aircraft performance differed. The Dash 8 aircraft scheduled speeds for flap settings are stipulated in the operator’s aircraft performance manual (APM) (Figure 2).
Flap settings for take‑off
Pilots use different flap settings to increase or decrease performance during take-off and landings. The flap setting deployed for the take-off phase contributes to the performance of the aircraft on the take-off roll and the initial airborne segment. The Dash 8 flap setting requirements for take-off are stated in the APM and are based on the performance data, such as the prevailing weather conditions and aircraft take-off weight.
The crew advised that the performance calculations for the Dash 8 at Horn Island on the day required a flap setting of 15° for take-off to account for the lift required due to the limiting factor of the short runway. This setting was unusual for the crew as they stated that the last two sectors flown, the flap setting of 5° had been used and that, in their experience, flaps of 5° was the normal setting for take-off at most of the airports in the airlines network.
Figure 2: APM specified take-off performance for flap settings 5 and 15 degrees
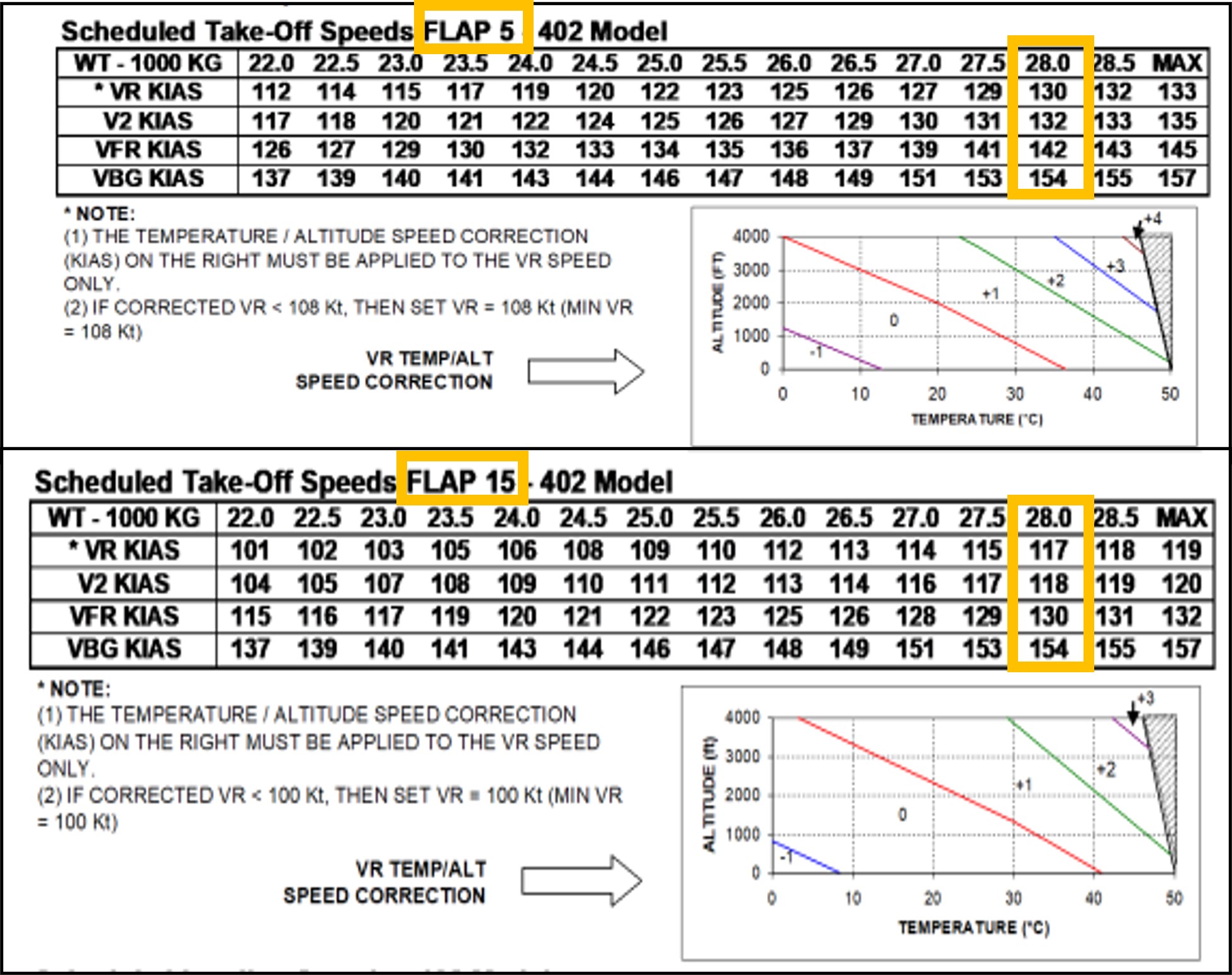
Source: APM provided by operator, annotated by the ATSB
Bleed air system
The bleed air system plays a role in multiple aircraft functions and operates through a network of ducts, valves, and regulators using high pressure air bled from the compressor section of the engine and auxiliary power unit. Turning off the bleed air system provides extra engine performance and maximises take-off power, which is beneficial for optimal performance on short runways with a high payload. The requirement to turn off the bleed air was not a routine occurrence, the FO reported they were very conscious of remembering ‘bleeds off’ for the take-off and so had written themselves a reminder note.
Procedures for pre-departure checks
At each critical phase of aircraft operation, pilots refer to checklists to guide them through specific items to configure the aircraft for the next planned phase of the flight. These enhance safety by providing an opportunity to confirm that the safety‑critical aspects of the aircraft configuration are correctly set. Consequently, any omissions or mistakes are more likely to be identified and rectified by the flight crew. Checklist deviations occur relatively frequently, compared to other forms of procedural deviation. A common form of checklist deviation includes responding without checking (Dismukes and others, 2010).
The company flight crew operating manual[6] (FCOM) states that many checklists are preceded by ‘checks’ which are memory items completed prior to actioning the checklist. For example, in the case of the after start checks, the captain will ask for the after start checks and the crew conduct their check flows, then the FO reads the after start checklist and the captain responds to the checklist. The standard operating procedures (SOPs) are outlined in the FCOM which documents 4 procedures that could potentially identify an incorrect flap setting:
- departure briefing
- take-off data crosscheck
- after start checks
- after start checklist.
Departure briefing
Crew departure briefings are intended to bring awareness of operational information and conditions that are not covered in the SOPs. The flap setting of 15° is an uncommon flap setting on the network and although there was no mandatory requirement to brief the take‑off flap setting, it did provide an opportunity to acknowledge the flap setting of 15° as an operational consideration or as a threat. Neither the FO nor the captain recalled if the flap setting was included as a threat in the content of the briefing. Calling out the flap setting as a threat would have provided a prompt to the crew which may have made the incorrect flap setting easier to detect. The crew stated that as they had previously flown out of Horn Island, the take-off flap setting of 15° was not considered abnormal unless a pilot had not previously flown from the aerodrome. The crew recalled that the ‘bleeds off’ procedure was briefed.
Take-off data crosscheck
The take-off data crosscheck required the captain to verify the take-off weight, runway distance intersection, and the flap setting from their Aerodata app while the FO was required to confirm the aircraft weight using the load sheet. The captain then ensured the correct take-off speeds were displayed on their primary flight display (PFD), which the FO cross referenced with their own PFD. The captain and the FO reported completing this step. Following this, the captain read the take-off speeds from the Aerodata and their PFD and the FO was required to verbally reiterate the speeds read from their own PFD.
After start checks
Among other items, the after start checks required the FO to set the flaps for take-off and that to complete this task, the Aerodata or TOLD card should be referenced to set and confirm the flap setting. The FO reported setting the flaps to 5° but could not remember referring to the Aerodata or the TOLD card to do this and recalled they may have had the load sheet or something else displayed on their iPad.
After start checklists
Directly following the after start checks, the after start checklist was a ‘challenge and response’ format which prompted for verification of the take-off data and flap settings among several other items. The captain and the FO reported they had no recollection of the response provided for the flap-setting challenge. On completion of this checklist, the captain and the FO had not detected that the flap setting was 5° which contrasted with the Aerodata display that showed a required flap setting of 15°.
Operator’s report
The findings from the operator’s internal safety investigation report stated that the flap setting of 5° increased the risk for tailstrike and reduced the margin for obstacle clearance. The aircraft would have been 2,112 kg overweight for take-off configured with a flap setting of 5° (Figure 3). The report determined that the required take-off distance with flap setting of 5° was 1,680 m which was greater than the available runway distance. However, the report concluded that as the aircraft was configured with flap 15° speeds set for take-off, the decision to reject the take-off would have been made with reference to the bugged[7] V1 speed of 116 kt and the accelerated stop distance required (ASDR)[8] would have been adequate. Therefore, the operator calculated that in the event of a rejected take-off, at or below the V1 that was set, the aircraft would have had sufficient deceleration to come to a stop before the runway threshold.
Figure 3: Aerodata performance calculations for VH-QOI for a flap settings of 15° and 5°
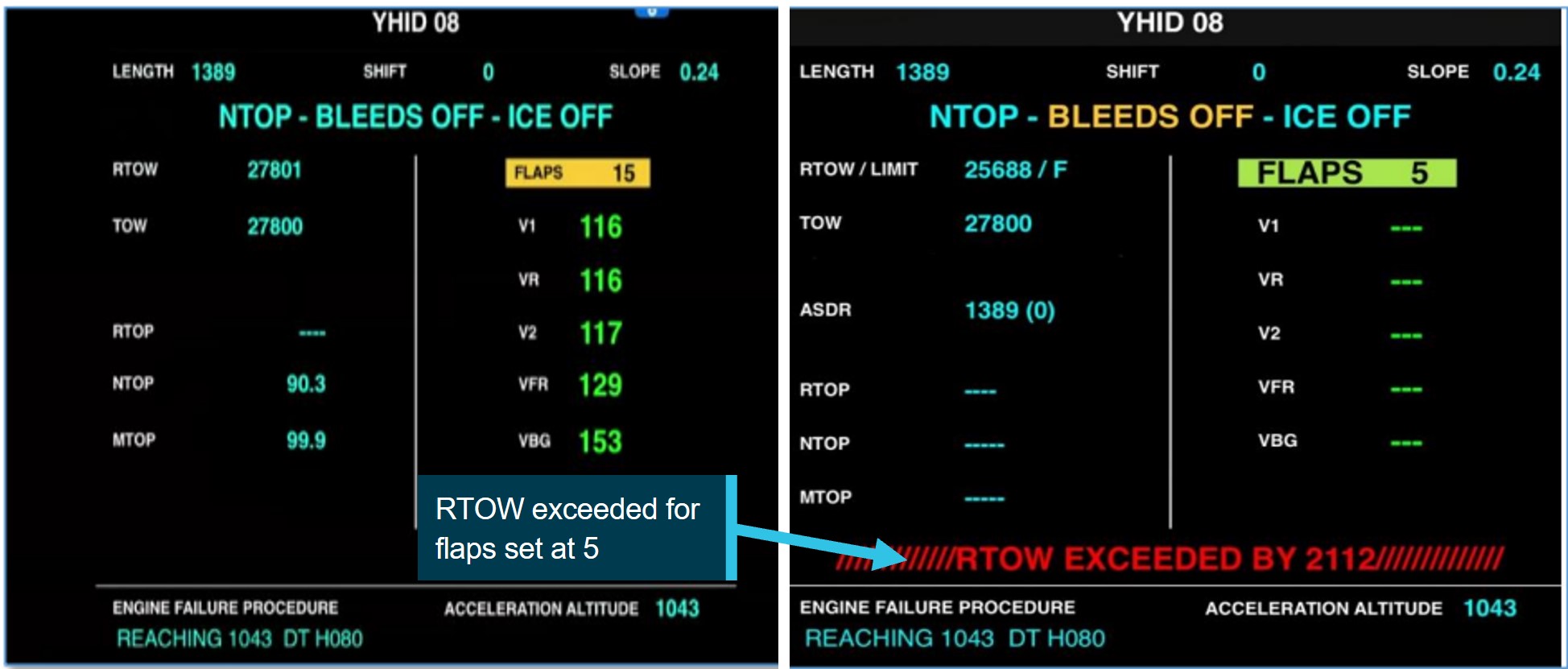
Source: Reproduction provided by operator, annotated by the ATSB
Fatigue
Fatigue is defined as a decrease in performance as a function of time on task (Salas and others, 2010). Fatigue can have a range of adverse influences on human performance and can lead to slips or lapses associated with attention, problem-solving, memory, vigilance and decision‑making. ATSB has identified that people experiencing fatigue are not able to accurately evaluate their own fatigue level or their ability to perform tasks, rather they tend to overestimate their abilities (ATSB, 2019). As such, fatigue is considered an important safety concern and an ATSB SafetyWatch priority.
The flight crew’s previous 72-hour roster allowed for regulated sleep opportunities. The flight crew commenced duty from Townsville at 0600 where they had stayed overnight. Their duty roster included three sectors for the day:
- Townville–Cairns
- Cairns–Horn Island
- Horn Island–Cairns.
Both flight crew members had presented for duty that morning stating they were fit to fly, although both reported to the ATSB that the environmental conditions at their accommodation in Townsville were not conducive for sleep. The captain noted that their sleep was broken due to noise and air‑conditioning issues and self-reported being a little tired at the commencement of duty as their previous night’s sleep prior to the incident was poor. The FO described their alertness at the beginning of duty as very lively and their sleep quality as good but also reported sleep disruption due to unreliable air-conditioning in the room. The ATSB concluded that it was very unlikely that either crew were experiencing fatigue to a level that could influence performance.
Safety analysis
Introduction
During a scheduled sector from Horn Island to Cairns, a reduced aircraft performance during take‑off and the initial climb did not align with the flight crew’s expectations. The first officer (FO), as the pilot flying, discovered that the flap setting was incorrectly configured at 5° instead of 15° and advised the captain. The aircraft was established in a positive climb and continued the flight without further incident.
This analysis will discuss factors that contributed to the incorrect aircraft configuration and lack of detection during the pre-flight crosschecks.
Crew actions
The inadvertent selection of the flaps to 5° instead of 15° by the FO was likely influenced by habitual behaviour driven by prior experience. A flap setting of 5° had been used for the previous two sectors flown by the flight crew and was, in their experience, the most common setting for take-off at most of the airports in the operator’s network. It is likely therefore, that the FO developed an unconscious habit for a flap setting of 5°, and the setting of 5° was a result of a slip. A slip is a form of human error defined to be the performance of an action that was not intended (Reason, 1990). Slips often occur during the largely automatic performance of routine tasks, usually in familiar surroundings, and characteristically involve an incorrect implementation of an intention (Mylopoulos, 2022). If other factors are also present, such as distraction, then the chance of such errors occurring increases. This type of slip cannot be eliminated by training alone, however, improvements in system design can reduce the likelihood of occurrence and provide a more error tolerant environment, which is why checks of the flap setting are built into the pre-flight processes (the after start checklist).
The flight crew reported adhering to the procedures for the pre-departure checks which provided 4 occasions to potentially identify or rectify the incorrect flap setting. Flight crews are particularly vulnerable to checklist errors during the pre-flight sequence in the time‑compressed phase of pre‑departure (Loukopoulos, and others, 2001). Under normal pre‑flight procedures workload is usually at a high level and for this flight the extra calculations for weight, weather and performance limitations elevated the crew workload. When workload is high, automaticity can be amplified as the mind seeks to conserve energy by relying on well learned routines (Bermúdez and others, 2021). This can be detrimental when a situation requires mindful engagement. The flight crew likely conducted the after start checklist with a high degree of automaticity, rather than consciously verifying the flap setting against the Aerodata or TOLD card. In this case there was a breakdown of this normal layer of defence, which emphasises how safety measures can be degraded if crews are not consciously focused on the task. It was possible that the crew had diminished sensitivity for error detection due to completing the checklist without carefully ensuring the confirmation of each of the steps.
As a result, the crew performed the take‑off with the flaps inadvertently at 5° instead of 15°. The incorrect configuration reduced the intended performance envelope of the aircraft. The FO’s continued back pressure to the controls during the take-off run resulted in the aircraft successfully becoming airborne slightly after the expected rotation speed. The FO’s actions to reduce pitch during the take‑off increased the airspeed and the aircraft maintained a positive climb.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the incorrect configuration involving Bombardier DHC-8, VH-QOI, at Horn Island Airport, Queensland on 26 June 2024.
Contributing factors
- The FO mistakenly set flaps to 5° for take-off at Horn Island when pre-flight planning identified flaps 15° should have been set.
- Standard pre-flight checks and crosschecks were conducted, however the flight crew failed to identify the incorrect flap setting before take-off at Horn Island. This was likely due to automatic behaviour by the crew registering flap 5° to be the usual setting at take-off.
- The incorrect configuration of the aircraft reduced the climb performance and potential obstacle clearance on departure from Horn Island.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence. |
Safety action by QantasLink
In response to this occurrence the ATSB was advised by QantasLink that the following actions had been undertaken:
- Review of standard operating procedures to strengthen procedures as necessary to reduce the likelihood of erroneous flap selection and misidentification.
- Review of relevant checklists to strengthen crosschecking in accordance with the computed take-off performance data.
- Training for crew focusing on standard operating procedures and compliance.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- interviews with the captain and first officer
- QantasLink internal safety report
- recorded data from the aircraft QAR.
References
ATSB (2019) Fatigue experiences and culture in Australian commercial air transport
Bermúdez, J. P., & Felletti, F. (2021). Introduction: Habitual Action, Automaticity, and Control. Topoi, 40(3), 587-595.
Dismukes, R., & Berman, B. (2010). Checklists and monitoring in the cockpit: Why crucial defenses sometimes fail (No. ARC-E-DAA-TN1902).
Loukopoulos, L. D., Dismukes, R. K., & Barshi, I. (2001). Cockpit interruptions and distractions: A line observation study. In Proceedings of the 11th international symposium on aviation psychology (p.1-6). Columbus: Ohio State University Press.
Mylopoulos, M. (2022). Oops! I did it again: the psychology of everyday action slips. Topics in Cognitive Science, 14(2), 282-294.
Reason, J. (1990). Human error. Cambridge University Press.
Salas, E., & Maurino, D. (Eds.). (2010). Human factors in aviation. Academic Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- flight crew consisting of captain and first officer
- QantasLink
- CASA
Submissions were received from:
- QantasLink
- flight crew – captain and first officer
- CASA
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] FMS is an avionics system. It supports navigation, flight plans, positioning, guidance and other flight-related tasks.
[2] Aerodata software is QantasLink’s primary method for calculating take-off data.
[3] Flaps are hinged inboard trailing edge surfaces on an aircraft’s wings that can be extended down or retracted upwards.
[4] Take-off and Landing Distance card – a quick reference guide for data fields pertaining to take-off and landing.
[5] V1 is the maximum speed at which a rejected take-off can be initiated in the event of an emergency. V1 is also the minimum speed at which a pilot can continue take-off following an engine failure.
[6] The Flight Crew Operating Manual (FCOM 4.42, March 2024) is issued by the manufacturer as a guideline for operators to develop their own standard operating procedures (SOPs) in accordance with applicable requirements.
[7] Speed bugs are small pointers on the airspeed indicator, usually referred to as bugs. Pilots use the bugs as references for important take-off speeds.
[8] ASDR is the distance required to accelerate from brake release to V1, experience an engine failure at V1 and decelerate to a stop.
Occurrence summary
| Investigation number | AO-2024-038 |
|---|---|
| Occurrence date | 26/06/2024 |
| Location | Horn Island Airport |
| State | Queensland |
| Report release date | 21/01/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Aircraft preparation, Incorrect configuration |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Bombardier Inc |
|---|---|
| Model | DHC-8-402 |
| Registration | VH-QOI |
| Serial number | 4189 |
| Aircraft operator | Sunstate Airlines (QLD) Pty. Limited |
| Sector | Turboprop |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Horn Island Airport |
| Destination | Cairns Airport |
| Damage | Nil |
Ground strike involving British Aerospace BAe 146-300, VH-SAJ, at Brisbane Airport, Queensland, on 25 June 2024
Final report
Report release date: 09/09/2025
Investigation summary
What happened
On 25 June 2024, a British Aerospace BAe 146‑300, registered VH‑SAJ, was being operated by ASL Airlines Australia on a freight flight from Sydney, New South Wales, to Brisbane, Queensland. On board the aircraft were the captain and first officer.
While on descent into Brisbane, the meteorological conditions worsened with visibility reducing to about 1,000 m in fog. The crew conducted an instrument approach for runway 19L, using the autopilot, and visually identified the high intensity approach lighting at about 220 ft. The first officer disconnected the autopilot at about 110 ft and made control inputs that resulted in an increasing aircraft pitch attitude with decreasing airspeed. The aircraft touched down with a high pitch angle and a vertical acceleration of about 2.4 g. The tail of the aircraft struck the runway, resulting in damage to the tail strike indicator and surrounding panels.
What the ATSB found
The ATSB’s investigation identified that the first officer likely became disoriented after disconnecting the autopilot and lost situation awareness. Consequently, they did not identify the increasing aircraft pitch attitude, decreasing airspeed, or low power setting and did not correct the resulting sink rate prior to touchdown. The captain prevented further rearward input by the first officer during the flare by placing their hand on the control column, likely reducing the severity of the tail strike.
It was also found that during the approach the captain became preoccupied with the remaining fuel on board and this likely limited their capacity to monitor other factors such as the first officer’s ability to undertake the approach and the undesired state of the aircraft during the flare. The ATSB also identified that the captain’s actions and communications during the approach likely increased the pressure on the first officer to commit to the landing.
Prior to joining the operator, the captain had predominantly flown single pilot operations in non‑jet aircraft. They had been promoted to the position of captain early, which resulted in a missed opportunity to gain valuable experience within a multi‑crew environment prior to commencing in the role. This limited multi‑crew experience likely reduced the captain’s capacity to include the first officer in the decision-making process during the approach or make an authoritative decision to assume the pilot flying role.
The ATSB identified that both the captain and first officer had been appointed to their respective positions despite not meeting the ASL Airlines Australia minimum experience requirements. This occurred without additional controls in place to manage the risk of lower experienced pilots and resulted in a reduction in the intended experience level on the flight deck for the incident flight.
What has been done as a result
Following an internal investigation by ASL Airlines Australia the following safety actions have been taken:
- The upgrade or fleet transfer requirement of a minimum of 500 hours on a company type, or as deemed appropriate by the Director of Flight Operations contained in the operations manual was amended to a minimum of 500 hours on a company type, or similar type in terms of maximum take‑off weight as deemed appropriate by the Director of Flight Operations, Head of Training and Checking and Director of Safety.
- Inexperienced flight crew that have been checked to line will not have their inexperienced status removed without a review of the candidate’s progress by the Director of Flying Operations or Head of Training and Checking.
- The Planned Supervised Line Flying sectors for Captains – No Jet Experience listed in the OM‑D – Training and Checking Manual have been increased from 30 to 36 sectors.
- Supervised Line Flying sectors for First Officers without previous jet experience has been increased from 30 to 36 sectors.
- The Fleet Training Manager will review a candidate’s experience at the planning stage, and may elect to plan less, or more sectors, dependent upon the candidate’s progress.
- Additional systems to track pilots with inexperienced status to avoid inadvertent rostering of inexperienced crew together.
- The operator’s internal review identified an inconsistency between the operator’s standard operating procedures and the manufacturer’s recommendation with regard to which pilot (the pilot flying or the pilot monitoring) was to make an ‘attitude’ call when the aircraft pitch angle approaching landing increased above 5°.
- The BAe 146 standard operating procedures manual has been updated and aligns with the manufacturer’s recommendation.
- The operator’s internal review identified there was no policy stipulating that the captain must perform the landing when the weather conditions are below certain weather criteria.
- A policy has been developed and incorporated into the operations manual that states the captain must conduct the approach and landing with visibility within 1,000 m and cloud within 100 ft of the minima unless the pilot in command is a company approved training or check pilot.
Safety message
Current shortages of aviation professionals, including pilots, have resulted in the need for operators to employ crew with less experience than has previously been expected. Operators are encouraged to review the employment and promotion processes for inexperienced crew, ensuring that additional training programs, or limitations on inexperienced crew and the pairing of less experienced crew during rostering are considered.
The occurrence
Overview
On 25 June 2024, a British Aerospace BAe 146‑300, registered VH‑SAJ, was being operated by ASL Airlines Australia on a freight flight[1] from Sydney, New South Wales, to Brisbane, Queensland. There were 2 flight crew on board. The captain was pilot monitoring, and the first officer (FO) was pilot flying. [2]
The aircraft departed Sydney at about 0415 with first light occurring at Brisbane at 0613. The forecast visibility for arrival at Brisbane was 10 km. While on descent to Brisbane, the meteorological conditions worsened with visibility reducing to about 1,000 m in fog. The crew conducted an instrument landing system (ILS) approach for runway 19L,[3] using the autopilot, and visually identified the high intensity approach lighting at about 220 ft.
The FO disconnected the autopilot at about 110 ft and made control inputs that resulted in an increasing aircraft pitch attitude with decreasing airspeed. The aircraft touched down with a high pitch angle and a vertical acceleration of about 2.4 g. The tail of the aircraft struck the runway, resulting in damage to the tail strike indicator and surrounding panels.
Cruise and descent
At about 0457, while the aircraft was in cruise at flight level[4] (FL) 270 and approximately 350 km to the south of Brisbane, air traffic control (ATC) advised the crew to expect runway 19L for their arrival.
At about 0505, cockpit voice recorder (CVR) data indicated that the captain obtained the automatic terminal information service (ATIS)[5] for Brisbane Airport. The meteorological conditions at that time were reported as a wind from 190° at 8 kt, visibility greater than 10 km with showers in the area, cloud few[6] at 500 ft, scattered[7] at 3,000 ft, and a temperature of 14°C (see Meteorological information). The captain then completed the take‑off and landing data (TOLD) card. This included calculated figures for fuel overhead the destination (Brisbane) of 2,400 kg and a minimum divert fuel of 1,700 kg.
The crew then conducted a briefing for the arrival into Brisbane and the ILS approach for runway 19L (see Airport information).
During the briefing, the FO noted the minima for the approach including a decision altitude (DA)[8] of 220 ft and visibility of 800 m, stating that conditions in Brisbane at the time were ‘showers and wet’.
At 0513, ATC advised the crew that the ATIS had been updated, and the cloud was now few at 200 ft, scattered at 3,000 ft and the temperature was 13°C. At 0519, when the aircraft was about 125 km south of Brisbane, ATC issued the crew with a clearance to descend to FL 130. A short time later, the captain commented on the cloud at 200 ft to the FO. The FO stated that they had 20 minutes of fuel, which was enough for a second approach if needed. The captain replied with ‘yeah, then we’re landing anyway’. The crew then completed the approach checklist.
The captain later advised that they believed their comment was a standard operational comment based on fuel limits.
Figure 1: VH-SAJ flight track for arrival to Brisbane Airport
Source: Google Earth, annotated by the ATSB. *Flight was conducted in darkness
At 0521, the crew commenced the descent to FL 130. At 0525, ATC issued the crew with a further clearance to descend to 9,000 ft. A short time later, the crew were advised by ATC to expect the ILS approach for runway 19L.
At 0526, when the aircraft was about 67 km south-east of Brisbane, ATC advised the crew of low cloud south of the airport that was moving north and that they may be required to delay their arrival. On receipt of the meteorological information from ATC, the captain commented to the FO that they had ‘no fuel’. The FO proposed that they had sufficient fuel to complete 2 approaches, declare minimum fuel, and complete a third approach. The captain commented that they would just land from the second approach as they would ‘rather be on the ground’, expressing concerns about the paperwork involved.
Over the following 2 minutes, the captain and the FO continued to discuss the options for the approach with the captain stating that, given the fuel state, conducting a go‑around may result in a worse scenario as they expected the meteorological conditions at Brisbane to worsen. The crew did not discuss options for a diversion if they were required to undertake a go‑around due to the meteorological conditions. The closest suitable airport was the Gold Coast (see Gold Coast Airport meteorological conditions during flight).
At 0529, ATC advised that the visibility had reduced to 1,000 m in fog, with a cloud base of 200 ft and that low visibility procedures were in force with the high-intensity approach and runway lighting operating.
At 0530 the crew discussed the changing meteorological conditions. During this discussion, the captain stated that the conditions would only get worse and if they could see the high‑intensity approach lighting, then they were going to land. The FO agreed and stated that the captain should ‘call it when you see it’.
At about 0531, the aircraft passed through 11,000 ft and, a short time later, the crew initiated the additional approach checks. At 0533, the crew were cleared to continue the descent to 4,000 ft.
There were 3 aircraft ahead of VH-SAJ on approach to land on runway 19L at Brisbane Airport. At about 0532, the first of the 3 preceding aircraft landed and reported becoming visual with the runway at the minima.
Final approach
At 0534, ATC provided a clearance for the crew to undertake the ILS approach for runway 19L.
At 0536, the second aircraft in the sequence ahead of VH‑SAJ conducted a go‑around, later reporting to the ATSB that the combination of reduced visibility and low cloud prevented them from landing. At 0537, the captain of the third aircraft in the sequence declared to ATC, ‘should we, we will require an immediate diversion to the Gold Coast’. However, the third aircraft landed successfully.
The CVR indicated on hearing the transmission from the aircraft advising a go‑around, the captain stated ‘we haven't got the fuel for this’. The captain later stated that their comment was over concern should multiple go‑arounds be required.
At about 0539, VH-SAJ became established on the ILS for runway 19L. At about 0540, approximately 4 minutes prior to landing, the captain stated to the FO that they did not have enough fuel to divert to the Gold Coast. The FO queried if it was possible to recalculate if there was sufficient fuel to conduct the diversion to the Gold Coast, to which the captain responded ‘not now on final, but let's try and get in’.
The captain later stated that they believed that it was not appropriate on final approach to calculate fuel for a diversion.
At 0541:28, the crew completed the landing checklist.
Landing
At 0541:45, the crew were provided with a landing clearance from ATC (Figure 2) and were advised that the runway visual range[9] was 1,200 m at the touchdown zone, 1,200 m at the runway mid‑point and 1,800 m at the end point of the runway.
Figure 2: VH-SAJ final approach to Brisbane Airport
Source: Google Earth, annotated by the ATSB. *Flight was conducted in darkness
At 0542:05, the captain instructed the FO to leave the autopilot connected until the aircraft reached 220 ft (the BAe 146‑300 minimum autopilot disconnect height is 60 ft). The captain later recalled to the ATSB that they did so to keep the aircraft on an accurate approach to the runway. The FO confirmed they would leave the autopilot engaged but also stated they would disconnect it should they require a go-around. In response, the captain stated ‘we don't want to go around. It’s gonna be a world of hurt’. The FO responded ‘but if we can't see, then we're gonna have to’.
The captain later responded after reviewing the draft report that their comment was over concern that a go‑around may lead to a more dangerous fuel critical situation and recalled at the time they considered similar occurrences that had occurred to other operators.
At 0542:40, the aircraft descended through 1,000 ft and was about 7 km from the runway threshold. At the same time, the captain advised the FO that the aircraft was stable, with the missed approach altitude set and armed.
At 0543:05 and about 600 ft, the captain announced they were visual with the high intensity approach lighting, the FO responded that they could also see the lighting, however ‘not super clearly’. At 0543:31 and about 350 ft, the captain instructed the FO to increase engine power.
At 0543:45, the aircraft reached the DA and the FO announced they could see the high intensity approach lighting. Four seconds later, the captain announced ‘there’s the runway’. The captain later recalled to the ATSB that they had more visibility than they had expected.
At 0543:57 the captain instructed the FO to disconnect the autopilot, which occurred at about 110 ft and an airspeed of about 128 kt. The airbrake[10] was extended and fully deployed as the aircraft passed 80 ft. Several pitch adjustments were made by the FO after the autopilot was disconnected. The FO later described that from the DA until landing, their workload increased ‘to a 9 or 10 out of 10’, they became ‘overwhelmed’ and that their scan pattern had broken down. The CVR indicated that neither the FO nor the captain commented on workload during the approach.
At 0544:01, both the captain and the FO announced becoming visual with the PAPI lights.[11] The FO later recalled they could make out the runway edge lighting, however could not see the touchdown point.
Just prior to touchdown, the captain instructed the FO ‘don’t come back too far’. The captain later recalled to the ATSB that the FO had levelled the aircraft shortly after disconnecting the autopilot and began to flare[12] too early. They recalled that the aircraft became high, slowed and then developed a high sink rate. From previous experiences they anticipated that the FO would attempt to pitch the aircraft up to arrest the sink rate. As a result, the captain placed their hand on the control column to prevent the FO from pulling back too far without verbalising their intention (see Operational policy and procedures). The FO also later recalled feeling the captain’s pressure on the control to prevent further rearward input.
The captain recalled to the ATSB that it was a common reaction for less experienced pilots to pull back and increase the pitch when the aircraft experienced a drop, and that this is discussed during their command training.
At 0544:11 the aircraft main wheels contacted the runway. The onboard flight data recorder captured a vertical acceleration of 2.4 g at initial touchdown, an aircraft pitch attitude of about 5.3°, and an airspeed of 105 kt (see Recorded information).
The crew were unaware of the tail strike until the damage was discovered on the post‑flight aircraft inspection. The tail contact with the runway damaged the tail strike indicator and surrounding fuselage skin panels (Figure 3).
Figure 3: VH-SAJ damage to tail strike indicator and surrounding panels

Source: ATSB
Context
Personnel information
Captain
Experience
The captain held an air transport pilot licence (aeroplane), issued in October 2017, and a valid class 1 aviation medical certificate. At the time of the incident, the captain had about 7,500 hours total aeronautical experience, of which about 5,400 hours was multi‑engine command. They had a total of 411 hours on the BAe 146, which included 198 hours as captain. The BAe 146 was the captain’s first jet aircraft rating, having previously flown smaller twin turboprop aircraft mostly in single pilot operations before commencing employment with the operator.
Operator training
The captain joined ASL Airlines Australia in November 2022 as a first officer. They completed their type rating on the BAe 146 aircraft in early 2023 and they were checked to line as a first officer in July 2023. In October 2023, they were assessed and recommended to undertake command training. At that time, their total BAe 146 time was 155 hours.
Their command training commenced in November 2023 and involved simulator training and command checks. During this training, the captain’s initial operator proficiency check (OPC) was assessed as unsatisfactory due to a breakdown in situation awareness during an instrument approach. Additional simulator training was provided, and the captain passed their OPC on 23 November 2023. The captain’s subsequent command simulator training was also assessed as unsatisfactory and was required to be retaken.
On 4 December 2023, the captain commenced supervised line flying sectors. The captain completed 19 sectors before being recommended to undertake their check to line on 19 December 2023. The captain’s check to line was assessed as unsatisfactory after the first sector. The captain was provided with additional simulator and ground school training support. The captain completed a further 8 supervised line flying sectors before being recommended to retake their line check. The captain successfully completed their line check on 15 February 2024.
The captain’s command training consisted of 31 sectors and 58 hours of flying.
First officer
Experience
The first officer (FO) held a commercial pilot licence (aeroplane), issued in March 2020, and a valid class 1 aviation medical certificate. The FO’s total aeronautical experience was about 1,090 hours, including about 113 hours as an FO on the BAe 146. Prior to their employment with the operator, the FO had flown for a general aviation operator, flying mostly smaller, single-engine aircraft and operating under visual flight rules.
Operator training
The FO joined ASL Airlines Australia in January 2024. They completed their type rating on the BAe 146 aircraft on 4 March 2024. They undertook 2 simulator sessions before successfully completing their OPC on 28 March 2024.
The FO commenced supervised line flying sectors in April 2024. The FO was assessed as achieving below the required standard in several areas including situation awareness, approach and landing. The FO undertook a simulator session on 8 May 2024 and an additional 16 supervised line flying sectors. The FO recalled that their simulator training included low visibility operations, but they had not previously landed an aircraft in foggy conditions.
On 28 May 2024 they were assessed as not proficient during their check to line. The FO was reassessed on 29 May 2024, 28 days prior to the incident and successfully completed their check to line.
The FO’s training consisted of 51 sectors and 90 hours of flying.
Fatigue
The ATSB considered the role of crew performance due to fatigue and found that, from the available evidence, fatigue was unlikely to have contributed to the incident (see Fatigue).
Aircraft information
General information
The BAe 146 (Figure 4) is a high‑wing cantilever monoplane with a T‑tail. It is powered by 4 Avco Lycoming ALF 502 turbofan engines mounted on pylons underneath the wings and had retractable tricycle landing gear.
The aircraft, serial number E3150, was a BAe 146‑300 series aircraft manufactured in 1989 and configured for air freight operations. It was first registered in Australia as VH‑SAJ on 24 October 2019. The last periodic inspection was completed on 12 June 2024 and on the day of the occurrence, the aircraft had accumulated 34,746 hours total time in service.
Figure 4: VH-SAJ BAe 146-300

Source: Jet photos, Cameron Roberts
Aircraft operator
At the time of the incident, ASL Airlines Australia (previously Pionair) held an air operator’s certificate issued by the Civil Aviation Safety Authority (CASA) on 14 May 2020 and valid until 1 December 2027, that authorised air transport in larger aeroplanes (CASR Part 121). ASL Airlines Australia operated a mixed fleet of aircraft that comprised 6 BAe 146s and 1 Boeing 737 aircraft, conducting mostly domestic air freight operations.
Airport information
Brisbane Airport
Brisbane Airport has 2 runways oriented 10°/190° magnetic (01L/19R and 01R/19L). At the time of the incident, aircraft departures and arrivals were taking place using runway 19L. The airport has a category 1 instrument landing system (ILS) on both runways. This landing system, combined with a 100% LED[13] category 1 lighting system,[14] including stop bar lighting, enables operations during low visibility events like fog.
Instrument approach
The crew of VH-SAJ were flying an ILS approach for runway 19L. The minima for the approach included a decision altitude8 of 220 ft, visibility of 800 m, and a runway visual range of 550 m (Figure 5).
Figure 5: Brisbane ILS runway 19L approach chart with landing minimums (blue box)
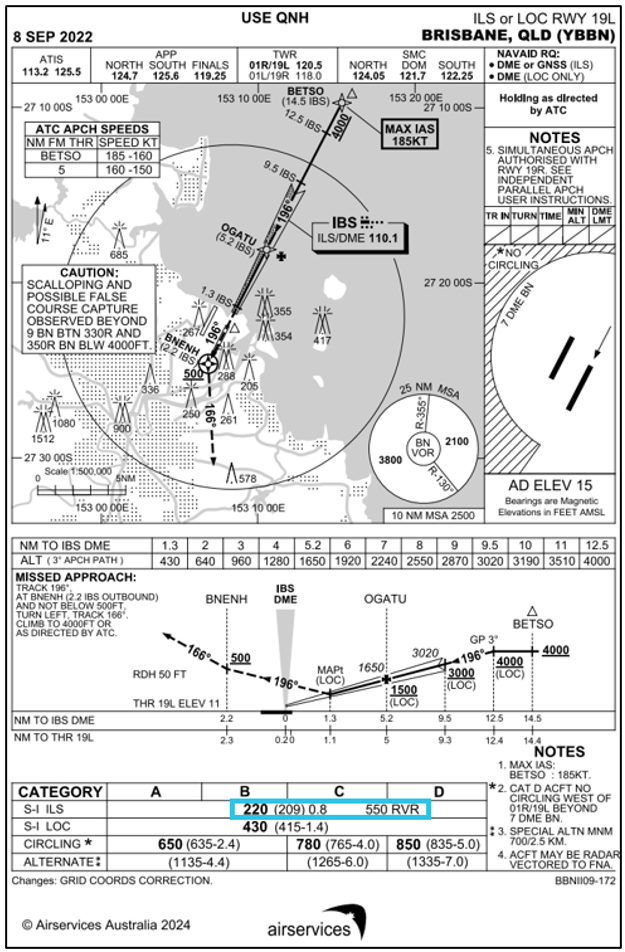
Source: Airservices Australia, annotated by the ATSB
Meteorological information
Predeparture briefing
The captain and FO were issued with a flight briefing package at 0057 that morning, which included the current terminal aerodrome forecast (TAF)[15] that was valid between 0000 on 25 June and 0400 on 26 June for Brisbane Airport.
At the time the flight briefing was issued, the TAF for Brisbane indicated:
- wind 210° at about 4 kt
- visibility greater than 10 km
- cloud few at 2,000 ft and broken[16] at 4,000 ft
- active INTER[17] from 0000 through till 0400 for visibility of 3,000 m in showers of moderate rain and broken cloud at 1,500 ft.
Prior to their departure from Sydney, the crew checked the latest weather information for their arrival into Brisbane. The latest TAF had not extended the INTER period for showers beyond 0400.
Brisbane Airport meteorological conditions during flight
The aircraft departed Sydney Airport at 0415, one hour and 15 minutes after the scheduled departure time and had an estimated time of arrival in Brisbane at 0555. Over the period 0500 to 0525 the visibility at Brisbane Airport remained greater than 10 km. From 0525 to 0550 the visibility reduced from greater than 10 km to 660 m due to the formation of advected fog.[18] The recorded visibility at the time VH‑SAJ landed was 912 m (Figure 6).
Figure 6: Brisbane Airport visibility 0445 to 0615 on 25 June 2024
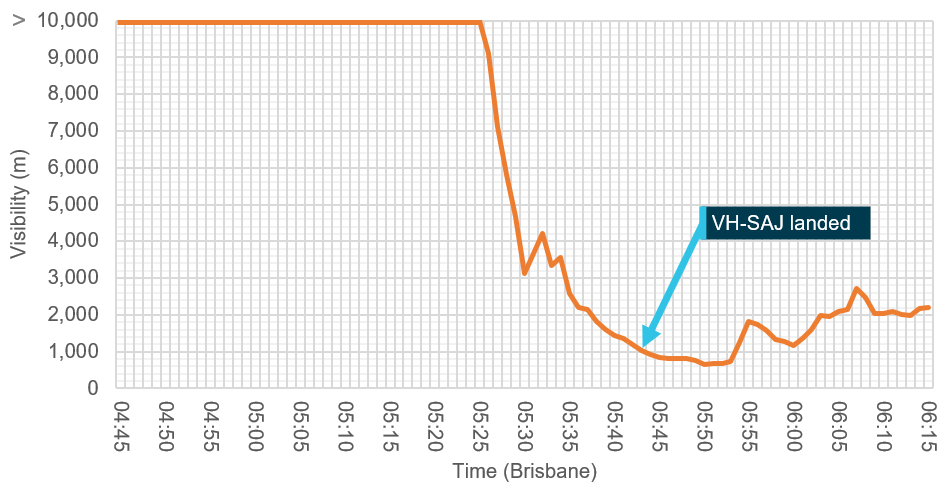
Source: Bureau of Meteorology, annotated by the ATSB
Closed circuit television (CCTV) recorded from the Brisbane air traffic control tower captured a progressive reduction in visibility that was consistent with the recorded meteorological information (Figure 7).
Figure 7: CCTV images from Brisbane Airport tower facing south
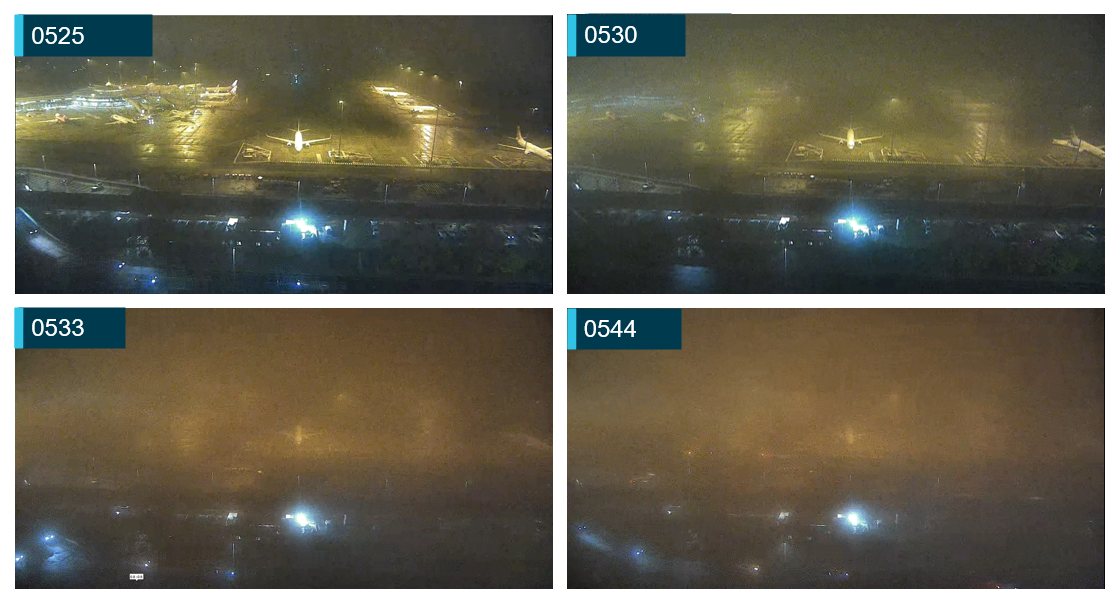
Source: Brisbane Airport Corporation, annotated by the ATSB
Gold Coast Airport meteorological conditions during flight
The closest alternate to Brisbane Airport was Gold Coast Airport which had a TAF issued at 0306 that contained an active TEMPO[19] for visibility of 4,000 m in showers of rain, with cloud scattered at 1,000 ft and broken at 2,000 ft.
At 0530, the Gold Coast meteorological aerodrome report (METAR) indicated visibility greater than 10 km and lowest cloud base of few at 6,100 ft. The subsequent METAR, issued at 0600, indicated visibility was still greater than 10 km with the lowest cloud base being scattered at 3,600 ft.
The Gold Coast Airport forecast was not issued to the crew as part of their flight briefing package and the crew did not obtain the Gold Coast Airport ATIS during the flight.
Recorded information
The aircraft was fitted with an L3[20] F1000 flight data recorder and L3 FA2100 cockpit voice recorder. Both units were transferred to the ATSB technical facilities in Canberra, Australian Capital Territory, for download.
Recorded flight data during the approach phase indicated the aircraft was flown within the ASL Airlines Australia stabilised approach criteria. At a height of about 110 ft, approximately 13.5 seconds before the main gear touchdown, the data indicated the autopilot was disconnected. Immediately following the disconnection of the autopilot, over a period of 5 seconds, the aircraft pitch attitude increased from about −4.3° to about 0° (Figure 8). At the same time the aircraft speed reduced from about 128 kt to about 120 kt. The crew had calculated the aircraft landing reference speed (Vref)[21] to be 115 kt and the aircraft approach speed (Vapp)[22] to be 120 kt (Vref + 5 kt).
The airbrake was deployed at a height of 100 ft and was fully extended when the aircraft reached 80 ft. ASL Airlines Australia standard operating procedures manual for the BAe 146 advised that the airbrake should be deployed on final approach once the landing was assured.
Figure 8: Recorded flight data
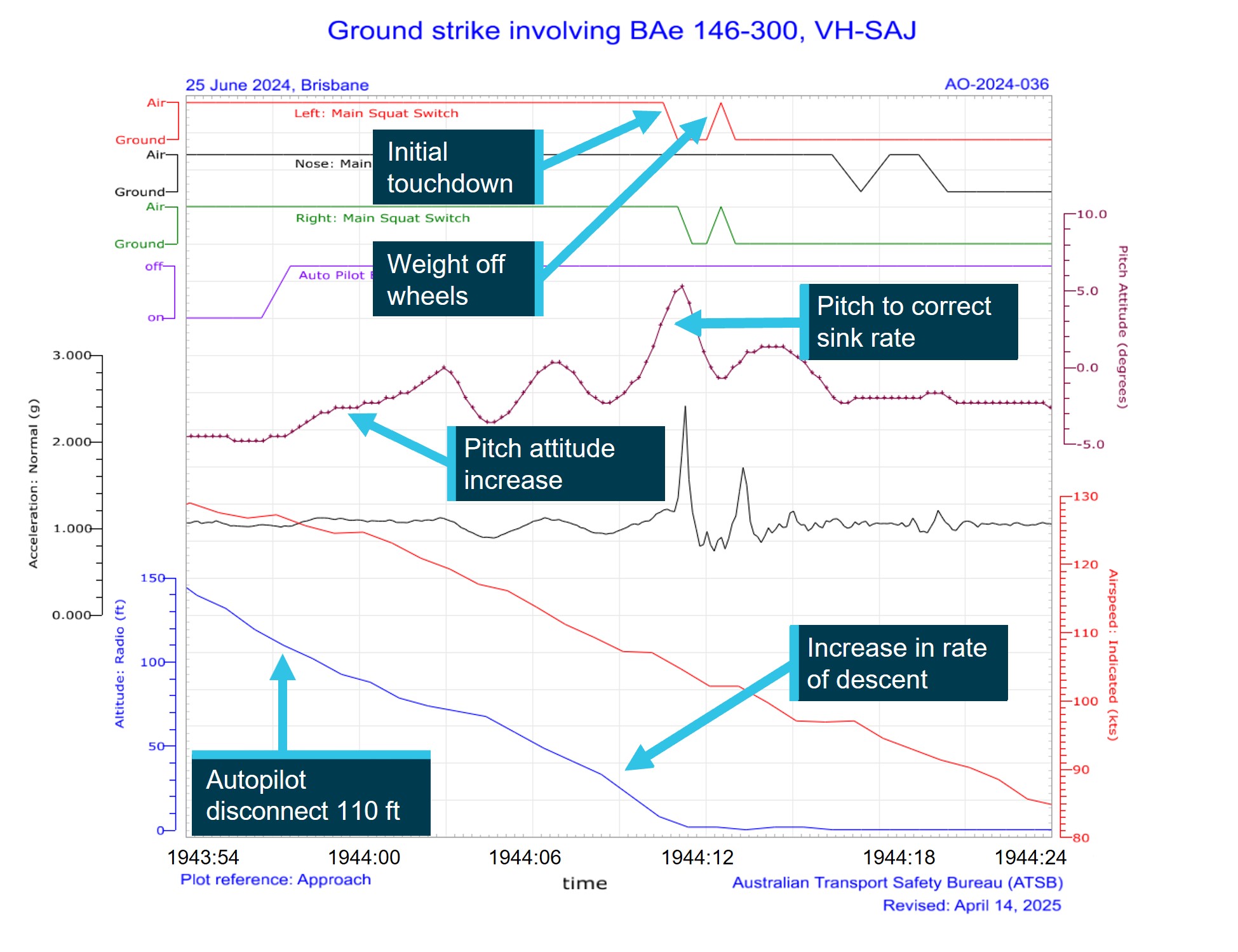
Source: ATSB
At a height of about 65 ft, the aircraft decelerated through 117 kt with a pitch attitude of about −3.6° and an increasing rate of descent. Several further pitch attitude adjustments were recorded as the aircraft continued to descend.
At a height of about 30 ft, the pitch attitude decreased to about −2.3°, airspeed reduced to about 109 kt and the rate of descent increased. Shortly after, the pitch attitude increased to a maximum of about 5.3° coincident with main gear touchdown. The vertical acceleration at main gear touchdown was 2.4 g and the airspeed was 105 kt. The aircraft engine power throughout the landing sequence was about 37% N1[23] and there was no recorded increase in power prior to contact with the runway. About 4 seconds after the initial touchdown the main gear momentarily recorded a weight off wheels followed by a vertical acceleration of 1.7 g, indicating a possible bounce.
The aircraft manufacturer advised that a tail strike in a BAe 146‑300 would occur on a hard landing, when the main gear oleos[24] had fully compressed, at a pitch attitude of 6.9° or higher. The difference between the values provided by the manufacturer and the recorded data were likely due to a combination of the flight data recorder sampling rate for the pitch attitude parameter (4 times a second) and the overall system accuracy (+/− 1.34°).
Operational information
Flight plan
ASL Airlines Australia operations provided the flight plan as part of the flight briefing package. The flight would depart Sydney and climb to FL 270. The track would take the flight overhead Newcastle, Grafton, Lismore and the Gold Coast, before landing at Brisbane. The flight was scheduled to continue from Brisbane with a planned landing in Townsville before the crew would end their duty period in Cairns.
Fuel planning
On departure from Sydney, the onboard fuel load was recorded as 5,800 kg with a planned trip fuel of 3,332 kg, including taxi fuel. ASL Airlines Australia operations had planned the flight with an additional 30 minutes of holding fuel due to the forecast INTER, planned between midnight and 0400 in Brisbane, which was later cancelled. A delay due to an engine vibration warning light resulted in an additional fuel burn, however the crew determined that as the INTER had been removed, that they had sufficient fuel for the sector. After discussion with the engineering team, the warning light was deemed to be a faulty indicator and the aircraft cleared to depart.
The operator’s fuel policy required a fixed final reserve fuel of 30 minutes as well as an additional 15 minutes of holding fuel when no alternate was required. This was a provision for weather, GPS RAIM[25] outage, traffic, or beginning of daylight. A contingency fuel margin of 5% of the trip fuel was also required to compensate for unforeseen factors.
VH-SAJ landed in Brisbane with about 2,300 kg of fuel remaining, which equated to about 72 minutes of flight time that included the use of reserve fuel. The ATSB was advised that ASL Airlines Australia had undertaken an internal review of the flight and that this review determined that the aircraft had sufficient fuel to conduct a missed approach at Brisbane and then divert to the Gold Coast before having to utilise the final reserve fuel margin.
Weight and balance
The operator’s load and trim sheet records indicated the aircraft was within the weight and balance limitations for the intended flight.
Preflight briefing
At the beginning of the duty period, the operator’s policy was for flight crew to conduct a ‘big picture briefing’. This was an opportunity to discuss any significant factors that may affect the planned operation and to focus on underlying threats or unusual factors and to discuss any means of mitigating those threats.
During the big picture briefing conducted prior to flight, the captain and FO recalled that they discussed that they had not previously flown together, and the captain communicated that they were open to receiving any criticisms or concerns regarding their operating practices. The captain recalled assuming that the FO was new to the position, but they were unaware of the FO’s previous flying experience and were also unaware they had not previously landed in low visibility conditions.
Operational policy and procedures
Flight crew experience requirements
Legislative requirements to be qualified as pilot in command
Civil Aviation Safety Regulation (CASR) part 121.495 required the following pilot in command experience:
(1) A pilot is qualified as pilot in command for a flight of an aeroplane if:
(a) the pilot meets the minimum flying experience requirements specified, in accordance with subregulation (2), in the aeroplane operator’s exposition for the aeroplane; and
(b) the pilot has successfully completed command training that complies with regulation 121.565 for the aeroplane operator and an aeroplane; and
(c) the pilot is:
(i) if the aeroplane is an Australian aircraft—authorised to pilot the aeroplane during the flight as pilot in command under Part 61; or
(ii) if the aeroplane is a foreign registered aircraft—authorised to pilot the aeroplane during the flight as pilot in command by the aeroplane’s State of registry.
(2) For the purposes of paragraph (1)(a), the aeroplane operator’s exposition must include minimum flying experience requirements for all aeroplanes operated by the operator for Part 121 operations.
Operator’s documented requirements
The ASL Airlines Australia operations manual (OM-A) version 5.5, which was current when the flight crew were checked to their positions, contained the minimum experience requirements to be met before an FO could be considered for promotion to the position of captain (pilot in command). The stated experience requirements were:
• meet all regulatory requirements
• minimum of 3000 hours aeroplane
• minimum of 500 hours on a company type, or as deemed appropriate by the GMFO [General manager of flying operations]
• minimum of 500 hours multi-engine PIC [pilot in command] or ICUS [in command under supervision]
• Australian ATPL [air transport pilot licence] or CPL [commercial pilot licence] with exam credit in all required examination subjects may be acceptable if the company is able to arrange/conduct an ATPL flight test as part of the upgrade training program.
The OM-A also contained the minimum experience required for the employment of a first officer. The stated experience requirements were:
• minimum total time of 1000 hours
• minimum of 500 hours in multi-engine aircraft
• a current Australian CPL [commercial pilot licence] or ATPL [air transport pilot licence].
The OM-A permitted the employment or promotion of crew below the prescribed minimum hours in ‘exceptional circumstances’, with the specific approval of the director of flight operations (DFO). It stated:
All crew seeking positions as pilots with Pionair are to comply with the Australian CASR Part 61 requirements with respect to licencing. Flight crew experience criteria for the various categories are as detailed below. These criteria may be varied, with the specific approval of the Director of Flight Operations to cater for exceptional circumstances.
There was no definition of what would be considered ‘exceptional circumstances’ within the OM-A.
Incident flight crew engagement
Neither the captain nor the FO met the documented minimum requirements to hold their assigned positions at the time of the occurrence.
The FO had about 106 hours of multi-engine experience at the time of their engagement with ASL Airlines Australia and about 219 hours of multi‑engine experience at the time of the incident. The OM-A minimum multi-engine experience requirement for the position was 500 hours.
The captain completed their command check to line in February 2024. At that time, they had accumulated about 213 hours on the BAe 146, of which 155 hours were as FO and an additional 58.7 hours in command under supervision as part of their command training course. At the time of the incident, they had accumulated about 411 hours total flying in the BAe 146 as FO and captain. The minimum company type experience requirement for the position was 500 hours.
The DFO was interviewed by the ATSB and described the captain as having ‘significant operational experience in night freight operations and the ability to manage fatigue with appropriate rest which was a very important but often overlooked skill for a new captain.
The DFO also recalled that the FO had previously been an airline cadet (for a major carrier) and had performed well in their interview.
No evidence of the ‘exceptional circumstances’ that led to the promotion of the captain or the employment of the FO was provided or identified by ATSB. There was also no evidence that ASL Airlines Australia had considered and managed the risks associated with the engagement of flight crew that did not meet the stated minimum requirements.
The DFO explained that during the period after COVID‑19, other airlines were recruiting significant numbers of flight crew and that ASL Airlines Australia had less opportunity to recruit for experienced crew during that time.
The Australian Government’s Aviation White Paper released in 2024 cited that a shortage of aviation professionals, including flight crew, was worsening, with job vacancies having more than tripled since 2019. The report also identified the effect a pilot shortage has on regional airlines and smaller operators, as crew leave these organisations to progress their careers with larger airlines, resulting in a higher turnover and a pool of less experienced applicants during recruitment.
Rostering of ‘inexperienced’ flight crew
The ASL Aviation Australia OM-A contained a policy to prevent ‘inexperienced’ flight crew being rostered together for a flight. It stated:
A flight crew member is deemed to be 'inexperienced' following completion of a type rating or command course until achieving the following additional experience on the type in their respective flight crew role after a successful check-to-line:
a. 100 flying hours and 10 operational sectors, within a consolidation period of 60 days; or
b. 150 flying hours and 20 operational sectors (with no time limit).
The policy further stated:
The OCC [Operations Control Centre] must ensure that inexperienced flight crew are not rostered together. In exceptional circumstances on Day of Operations the Director of Flight Operations may approve a crew complement that does not meet the above minimum experience requirements. To ensure compliance with current Regulations the Director of Flight Operations must ensure that, at an absolute minimum, the above minimum hours and sectors have been met when considering a crew member’s total type experience (including line training).
The captain had accumulated 198 hours since their successful check to line in February 2024 and was not considered inexperienced.
The FO had accumulated a total of 113 hours total time on the BAe 146 including their line training. Since their successful check to line on 29 May 2024, they had flown about 25 hours and completed 15 sectors as FO and was still considered ‘inexperienced’ according to the operator’s policy.
The policy did not have a provision for crew members that had been promoted to their position below the operator’s minimum prescribed hours.
Operational restrictions for 'inexperienced' flight crew
CASA acceptable means of compliance guidance material regarding pilot experience, stated:
The operator should consider any operational restrictions to be placed on an 'inexperienced' crew member after the completion of the conversion training or post command line check. These considerations may include cross wind limits, aerodrome limits and weather minima limits if the operator assesses these limits as suitable for their operation.
ASL Airlines Australia reported that it did not have a policy that restricted ‘inexperienced’ FOs landing in adverse weather and raised concern that this would reduce the exposure of FOs to less than desirable weather conditions.
The ATSB interviewed the captains of 2 of the 3 aircraft that were on approach to Brisbane ahead of VH‑SAJ. These aircraft were being operated by the same CASR Part 121 operator. Both captains advised that the FO on board was originally the pilot flying for that sector. However, if the visibility was less than 2,000 m or if the cloud was within 200 ft of the minima,[26] their operator’s policy was that the captain was required to conduct the approach and landing. Both captains reported that as the visibility on the ATIS was reported as 1,000 m and the cloud height at 200 ft, both had assumed the pilot flying roles of their respective aircraft prior to landing in accordance with their operator’s captains only approach procedure.
The ATSB reviewed expositions from 6 CASR Part 121 operators and found that 5 out of 6 operators had restrictions on FO’s conducting take‑offs and landings in adverse weather conditions, including reduced visibility, low cloud and strong winds.
Responsibility for control of the aircraft
The ASL Airlines Australia OM-A stated:
The authority and responsibilities of the captain are crucial for the safe operation of an aircraft. The captain holds ultimate authority over the aircraft, maintains discipline, and is responsible for ensuring the safety of individuals and cargo onboard, as well as the overall safe operation of the aircraft.
During interview with the ATSB, the FO recalled that as the approach continued, they became uncomfortable with the reduced visibility and described feeling overwhelmed by the conditions. However, the cockpit voice recording indicated the FO did not advise the captain of this, and they continued the approach as pilot flying. The FO recalled that, in hindsight, they should have requested control handover to the captain when they started feeling uncomfortable. Additionally, the captain also reported that in hindsight they should have assumed control and landed the aircraft.
The ASL Airlines Australia OM-A required:
Handover of control from one pilot to another must always be conducted in a positive manner. To minimise confusion or operational risk, the PF must not relinquish control until the PM has advised that they have taken control of the aircraft. NOTE: The standard phraseology to be used for handover/takeover procedures is: "You have control" and "I have control".
• In non-normal situations or when required, the Captain must initiate the takeover procedure.
• If corrected responses are not achieved from control inputs, control should be handed over to another flight crew member.
• In critical phases of flight, Captains must be in a position to enable rapid takeover of controls.
Standard calls
ASL Airlines Australia operations manual B (OM-B) for the BAe 146 detailed the required standard calls for flight crew during an approach. Cockpit voice recorder information indicated that the crew missed several required calls (Table 1).
Table 1: Standard calls on descent BAe 146
| Event | Standard call | Call event description |
| Gear extension | PF : Gear Down PM : Speeds Checked … Selected … Gear Down, 3 Greens | Speed checked not called |
| ILS glideslope Alt/distance check | PM : (Position) ___ (Altitude) PM : ___ DME ___ (Altitude) | Not called |
| 100 ft above minima | PM : Approaching Minimum PF: Check | Not called |
| Minima | PM : Minimum PF : Continue; or Go-Around | Continue or go-around not called |
In addition to the standard calls, the ASL Airlines Australia OM-B for the BAe 146 stated that during landing the:
PF/PM must monitor the attitude – if the nose up attitude becomes excessive on the ADI the PF should stop the increase in pitch attitude and consider a go-around if necessary. Recommended attitudes at which an “attitude” call should be made by the PF are:
…
• BAe146-300: 5°
The cockpit voice recording indicated that no attitude call was made by the crew when the aircraft pitch attitude increased above 5° just prior to main gear touchdown.
Fatigue
General
Fatigue affects everyone regardless of skill, knowledge and training and its effects can be particularly dangerous in the transportation sector, including the aviation industry.
The International Civil Aviation Organization (ICAO, 2015) defined fatigue as a physiological state of reduced mental or physical performance capability resulting from sleep loss, extended wakefulness, circadian phase, and/or workload (mental and/or physical activity) that can impair a person’s alertness and ability to perform safety related operational duties. Fatigue can have a range of adverse influences on human performance. These include:
- slowed reaction time
- decreased work efficiency
- increased variability in work performance
- lapses or errors of omission (Battelle Memorial Institue, 1998).
Duty period and sleep obtained
ASL Airlines Australia exposition stated that when flight crew are rostered to begin a duty period between 0000 and 0459 and scheduled to fly 4 sectors, the maximum duty period is 9.5 hours. If both flight crew agree, the duty may be extended by 1 hour during the duty period.
The captain recalled not being rostered on for the previous 72 hours before they signed on for their duty period in Melbourne at about 0015. They reported that, on the Samn‑Perelli scale of alertness,[27] they felt fully alert, however at the time of the occurrence, reported they felt ‘okay, somewhat fresh’. The captain reported having about 5 hours sleep in the 24 hours prior to their duty period and about 12 hours of sleep in the past 48 hours.
The FO recalled not being rostered on for the previous 72 hours before starting their duty. They reported having about 9 hours sleep in the past 24 hours prior to their duty period and about 17 hours in the past 48 hours and that they felt ‘a little tired, less than fresh’ at the time of the occurrence.
The ATSB assessed that both crew had sufficient sleep opportunity prior to commencing their duty.
Adequate sleep is an obvious prerequisite for alertness during duty. The concept of adequate sleep however is subject to individual variability with inconsistencies in amount and quality.
Window of circadian low
The duty period required working through the time in the circadian body clock cycle when self‐rated fatigue and mood are worst (Salas & Maurino, 2010). According to ICAO (2015) there are 2 times of peak sleepiness within a 24‑hour cycle. The main peak is in the early morning between 0300‑0500 known as the window of circadian low (WOCL), another smaller peak is around 1500‑1700 known as the afternoon nap window (International Civil Aviation Organisation, 2015). For each individual this time can vary. The incident occurred at 0544 which was close to the WOCL, which would have had some impact on their alertness levels as seen in their subjective alertness ratings above.
However, the FO’s alertness was possibly heightened (Causse and others, 2024) due to their unfamiliarity with the unforecast conditions and as a result this would likely have counteracted any effect of fatigue.
Operator's biomathematical model of fatigue
The operator provided the ATSB with a summary of the June 2024 report from their fatigue management software which uses biomathematical modelling to predict fatigue risk from the roster times and duty periods. The results did not identify fatigue risk had occurred with either crew member. However, the model does not account for individual susceptibility or resilience to fatigue.
Fatigue summary
The ATSB considered the role of crew performance due to fatigue and found that the available evidence indicated that fatigue was unlikely to have contributed to the incident. However, the captain’s self-reported amount of sleep in the 24 hours prior to their duty period is below the guidelines for recommended hours (Hirshkowitz and others, 2015).
Related occurrences
Tail strike – Brisbane Airport, Queensland, 23 October 2008 (AO‑2008‑74)
On 23 October 2008 at 2357 Eastern Standard Time, a BAe 146‑300 aircraft, registered VH‑NJM, operating a freighter flight, had a tail strike on landing at Brisbane Airport, Queensland. The aircraft and crew had commenced duty earlier that evening at Adelaide, South Australia, and had flown via Sydney, New South Wales, to Brisbane. The aircraft and crew then did the reverse sectors back to Adelaide. It was only after landing at Adelaide that the crew became aware of the tail strike. Damage to the aircraft consisted of abrasion to the tail strike indicator through to the fuselage skin and abrasion to the fuselage skin. There was also damage to the aircraft’s structural frame under the tail strike indicator. The aircraft manufacturer had identified an increase in the number of BAe 146‑300 tail strikes and has recommended a number of procedural changes for flight crew. The aircraft operator has implemented those changes and issued notices to flight crew highlighting the risks and conditions for tail strike.
Tail strikes during landing involving Bombardier DHC-8 402, VH‑QOT and VH‑QOS, Brisbane Airport, Queensland, on 5 November 2013 and Roma Airport, Queensland, on 11 December 2013 (AO-2013-201)
On 5 November 2013 and 11 December 2013, 2 Dash 8‑400 aircraft, registered VH‑QOT and VH‑QOS, were being operated by QantasLink on scheduled passenger flights from Roma to Brisbane and Brisbane to Roma, Queensland, respectively. Both flights were crewed by a training captain, operating as pilot monitoring, and a trainee first officer, operating as pilot flying.
Although the 2 approaches utilised different flap settings, both were conducted using a propeller setting of 1,020 RPM. The early, initial and final stages of the approaches were unremarkable. Both training captains reported that as the aircraft approached the flare, they thought that the respective trainees had handled the approach well.
During landing, both trainees arrested the descent rate by raising the nose of the aircraft. In both cases the maximum pitch attitude was exceeded and the aircraft’s tail contacted the runway. Each aircraft sustained impact and abrasion damage to the fuselage skin and buckling of internal structures in the area of the tail strike sensor.
Safety analysis
Introduction
On 25 June 2024, a British Aerospace BAe 146‑300, registered VH‑SAJ, was being operated by ASL Airlines Australia on a freight flight from Sydney, New South Wales to Brisbane, Queensland. There were 2 flight crew on board. The captain was pilot monitoring (PM), and the first officer (FO) was pilot flying (PF).
While on descent to Brisbane, the meteorological conditions worsened with visibility reducing to about 1,000 m in fog. The crew conducted an instrument landing system (ILS) approach for runway 19L, using the autopilot, and visually identified the high intensity approach lighting at about 220 ft. The FO disconnected the autopilot at about 110 ft and made control inputs that resulted in an increasing aircraft pitch attitude followed by several corrections and continued decreasing airspeed. The aircraft touched down with a high pitch angle and a vertical acceleration of about 2.4 g. The tail of the aircraft struck the runway, resulting in damage to the tail strike indicator and surrounding panels.
This analysis will explore the operational considerations pertaining to flight crew experience and training, situation awareness, command decision‑making and crew communication.
Loss of situation awareness
The FO was new to their position with ASL Airlines Australia, having been checked to line 28 days prior to the incident. During their line training, the FO required additional simulator and supervised line flying sectors to achieve the required standard associated with situation awareness, approach and landing. At the time of the incident, the FO had accumulated a total of 113 hours of flying on the BAe 146.
The meteorological conditions at Brisbane at the time of the approach included reduced visibility due to the formation of advected fog. At the time the crew reached the ILS decision altitude (DA) for runway 19L, the visibility was recorded as 912 m. Although this exceeded the minimum required for the approach, the FO had only experienced flying in reduced visibility during their BAe 146 simulated training, and they had not previously landed an aircraft in foggy conditions. (The FO’s experience prior to employment with the operator had predominately been flying smaller single engine aircraft in visual meteorological conditions).
The presence of low cloud or fog can create a false visual reference which can result in a pilot orientating the aircraft to the fog layer, rather than the ground references (Federal Aviation Administration). The FO recalled that the low cloud and fog created a sight picture that they had not previously experienced in the aircraft and that following the transition to visual flying, their instrument scan pattern broke down as their attention shifted to outside the aircraft as they attempted to make sense of the landing environment.
Research by Garland et al, (1999) identified that high mental workload can negatively impact situation awareness, as only a subset of the available information can be processed and acted upon. Situation awareness can be defined as ‘the perception of the elements in the environment within a volume of time and space, the comprehension of their meaning and the projection of their status in the near future’ (Endsley, 1988) . The maintenance of a high level of situation awareness is a critical feature of a pilot’s role (Garland et al, 1999).
The combination of degraded visibility, potential visual illusion, high workload, and inexperience operating in similar meteorological conditions likely resulted in the FO losing situation awareness of the aircraft state. Consequently, the FO did not effectively manage the aircraft following the disconnection of the autopilot resulting in the aircraft initially becoming high on the approach.
A short time later, the FO likely became aware of the high profile and attempted to correct the height with several pitch attitude changes. However, the FO’s attention was outside the aircraft at this time and their instrument scan had broken down.
Consequently, they were likely not monitoring aircraft airspeed and did not command any change to the engine power settings. As a result, the airspeed reduced and the aircraft’s rate of descent increased. The FO likely identified the increased rate of descent as the aircraft neared the runway, as a large pitch attitude increase was recorded just prior to touchdown. However, these actions were not sufficient to arrest the high rate of descent and this, in combination with the high pitch attitude, resulted in the tail of the aircraft striking the runway surface.
Contributing factor The first officer became disoriented after disconnecting the autopilot on short final and likely lost situation awareness. Consequently, they did not identify the increasing aircraft pitch attitude, decreasing airspeed, or low power setting and did not correct the resulting sink rate prior to touchdown. |
Captain’s focus on remaining fuel
As a consequence of the unforecast reduction in visibility, with no original requirement to plan an alternative airport, the captain became increasingly concerned about the fuel state as the aircraft continued on the approach.
It was also an expectation of the captain that the visibility would deteriorate further, commenting to the FO that if they were to conduct a go-around this could potentially leave them in a worse situation. During the approach, the captain also made several remarks about committing to a landing including that if they could see the high-intensity approach lighting, then they were going to land. About 2 minutes prior to landing, the FO expressed concern regarding the autopilot usage stating that they would disconnect it should a go‑around be required. In response, the captain stated ‘we don't want to go around. It’s gonna be a world of hurt’.
Prior to their descent into Brisbane, the crew had calculated the minimum fuel to divert to the Gold Coast was about 1,700 kg. The aircraft landed at Brisbane with about 2,300 kg of fuel on board, indicating there was sufficient fuel to conduct a go-around at Brisbane and safely divert the aircraft to the Gold Coast.
The captain’s preoccupation with the aircraft fuel state, combined with the expectation of worsening conditions, led to an increased desire to land the aircraft on the first approach and avoid conducting a go‑around which they perceived would have resulted in an approach in conditions that would likely deteriorate further.
Contributing factor The captain became preoccupied with remaining fuel. This combined with an expectation of worsening visibility resulted in a sense of urgency to land off the first approach. |
Continued communication regarding fuel
Brisbane air traffic control (ATC) had alerted the crew to the approaching low cloud bank about 18 minutes prior to landing. From the time of the alert until the landing, the CVR recorded continued concern from the captain.
This concern included that they had ‘no fuel’ and ‘we haven't got the fuel for this’ as well as concern with the conditions stating, ‘the weather will only get worse’ and ‘if we can see the HIAL’s,[28] we’re going to land’.
About 4 minutes prior to landing, the FO asked if it was possible to calculate the fuel needed to divert to the Gold Coast, to which the captain responded ‘not now, on final, but let's try and get in’. Shortly after the FO discussed the go‑around procedure in preparation for the DA, to which the captain reinforced their intention to land.
Although there was continued communication regarding the fuel state and visibility, no discussion was recorded regarding diversion plans to an alternative airport until established on the final approach. Additionally, the crew did not proactively obtain the weather conditions for alternate aerodromes, in the event that they were required to conduct a go-around without a planned diversion, limiting the crew’s options to return to conduct a second approach in Brisbane, further exacerbating the expectation of landing off the approach.
In contrast, the crew of the preceding aircraft on the approach prior to VH‑SAJ, advised that there was sufficient time during descent to plan for a diversion on receipt of the weather changes. Subsequent ATC recordings indicated that this crew also advised ATC of their intention to divert to the Gold Coast, if a go-around was required.
The FO had no previous experience in a multi‑crew environment and had only recently been checked to line. According to Fabre (2022), when a newly appointed FO is paired with a captain that they consider as experienced, the captain’s opinion strongly influences the FO’s decision‑making and significantly increases the likelihood of the crew attempting a moderate to high-risk landing scenario. The FO’s limited experience in the position and in a multi‑crew environment likely meant they were more susceptible to the captain’s pressure to land and less likely to voice any concerns.
The continued verbal concern over landing off the approach compounded pressure on the FO, which likely compelled them to commit to a landing on reaching the DA.
Contributing factor Repeated communications from the captain regarding the need to land off the first approach likely increased pressure on the first officer to commit to a landing. |
Crew appointments
The ASL Airlines Australia operations manual outlined the minimum experience requirements for the appointment of captains and first officers. However, neither the captain nor the FO met these requirements at the time of their engagement, nor at the time of the incident.
In ‘exceptional circumstances’, the ASL Airlines Australia operations manual permitted the variance of the experience requirements with the specific approval of the director of flight operations.
There was no evidence that ASL Airlines Australia had considered the hazards associated with the appointment of pilots that did not hold the required level of experience, nor was any control put in place to manage the risks. Such controls could have included, but were not limited to, operational limitations for low experience crew. The ATSB reviewed expositions from 6 CASR Part 121 operators and found that 5 had restrictions on FOs conducting landings in marginal meteorological conditions, including reduced visibility and low cloud.
ASL Airlines Australia did not have such a policy, and it reported that having similar limitations could lead to FOs being promoted to captain without having acted as pilot flying in adverse weather conditions. However, the FO’s limited experience in marginal meteorological conditions likely contributed to the tail strike incident. Had a similar limitation been in place, it would likely have resulted in the captain assuming control when the crew were alerted to the low visibility at Brisbane Airport.
ASL Airlines Australia had a rostering policy that prevented crew who had not accumulated 100 hours in their positions from being rostered together. However, there was no consideration made for crew who had been provided early promotion to their positions. As a result, the captain, promoted early to their position and at the time of the occurrence had not yet attained the minimum experience requirements to hold the position, was paired with an inexperienced FO. Without administrative controls in the rostering policy to prevent unsuitable pairing of crew without requisite experience, the result was a reduction in the intended experience level on the flight deck for the incident flight.
Contributing factor ASL Airlines Australia employed and promoted pilots earlier than the prescribed minimum experience hours without additional controls in place to manage the risk of lower experienced pilots on the flight deck. (Safety issue) |
Captain’s multi-crew experience
The captain commenced with ASL Airlines Australia in November 2022, initially as a FO, before undertaking command upgrade training after 155 hours. They had held the position since February 2024 and had accrued 198 hours as a captain at the time of the incident. Prior to joining ASL Airlines Australia, the captain had not flown a jet aircraft and had mostly flown in single pilot operations. As discussed above in Crew appointments, the captain had been nominated for command upgrade training below the required 500 hours, and this reduced their opportunity:
- to gain valuable exposure operating in a multi-crew environment
- to model behaviour on experienced captains’ decision making
prior to commencing in the captain role themselves.
The missed opportunity to gain valuable multi-crew experience likely impacted the captain’s capacity to include the FO in the decision‑making process and limited the effectiveness of the crew during the approach. Although the captain was not the PF during the approach, the ultimate responsibility for the safety of the aircraft lay with them. The cockpit voice recording indicated that, although it was reasonable for the captain to assume the FO was competent in flying the ILS, they did not ask the FO if they were comfortable to continue the approach after being alerted to the low cloud, fog and changing weather conditions. Likewise, while the FO did not advise the captain that they were experiencing difficulties during the approach, the captain did not recognise other cues, such as the FO’s response when requested to disconnect the autopilot at the DA, their ability to clearly see the approach lighting on short final, or their obvious discomfort with the approach.
It is likely that the captain’s limited command multi-crew experience may also have reduced their ability to establish an appropriate ‘cockpit gradient’ following advice that the meteorological conditions at Brisbane Airport were deteriorating. The term ‘cockpit gradient’ describes the level of authority that exists between the crew members, and the way this authority influences communication and decision‑making. Although the pilot in command has ultimate responsibility in terms of decision‑making, depending on the cockpit gradient, other crew members can be either encouraged or discouraged from influencing these decisions through their own inputs.
A ‘steep’ cockpit gradient exists when the pilot in command has an overwhelming influence in decision‑making, with little input sought from other crew members. A steep gradient can ‘inhibit communication, coordination and the cross-checking of errors’ (Harris, 2011). The cockpit voice recording indicated a steep cockpit gradient existed during the approach phase, with the captain dismissing the FO’s request to recalculate diversion fuel or plans in the event of a go-around, thereby reducing the effectiveness of the decision‑making process.
The captain provided control input instructions to the FO during the final stages of the approach. Likely due to their limited experience in the captain role, they did not recognise that the approach would have been better handled by a more experienced crew member who had previously encountered comparable conditions. Consequently, no authoritative decision was made by the captain to assume the PF role or to command a go‑around when the aircraft entered an undesired state after autopilot disconnection.
Contributing factor The captain’s limited command experience in a multi-crew environment likely reduced their capacity to include the first officer in the decision‑making process, consider the need to assume the pilot flying role or command a go-around when the aircraft entered an undesired state during landing. |
Captain’s control input
The captain reported that as the high sink rate developed, they anticipated the FO’s reaction and placed their hand on the control column to prevent any further increase in the aircraft’s pitch during the landing. This likely reduced the severity of airframe damage caused by the tail strike.
ASL Airlines Australia procedures stated that any control handover must be conducted in a positive manner to minimise confusion and operational risk. The FO recalled feeling the captain’s pressure on the control column preventing further rearward input, but the captain did not verbalise their actions at the time. While the control column input from the captain may have prevented further damage to the aircraft, it also risked confusion about who was in control of the aircraft during a critical stage of flight.
Other finding The captain prevented further rearward input by the first officer during the flare by placing their hand on the control column. While this action is not usually completed without the required takeover procedure it likely reduced the severity of the tail strike. |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the ground strike involving British Aerospace BAe 146‑300, registered VH‑SAJ on 25 June 2024.
Contributing factors
- The first officer became disoriented after disconnecting the autopilot on short final and likely lost situation awareness. Consequently, they did not identify the increasing aircraft pitch attitude, decreasing airspeed, or low power setting and did not correct the resulting sink rate prior to touchdown.
- The captain became preoccupied with remaining fuel. This combined with an expectation of worsening visibility resulted in a sense of urgency to land off the first approach.
- Repeated communications from the captain regarding the need to land off the first approach likely increased pressure on the first officer to commit to a landing.
- ASL Airlines Australia employed and promoted pilots earlier than the prescribed minimum experience hours without additional controls in place to manage the risk of lower experienced pilots on the flight deck. (Safety issue)
- The captain’s limited command experience in a multi-crew environment likely reduced their capacity to include the first officer in the decision‑making process, consider the need to assume the pilot flying role or command a go-around when the aircraft entered an undesired state during landing
Other findings
- The captain prevented further rearward input by the first officer during the flare by placing their hand on the control column. While this action is not usually completed without the required takeover procedure it likely reduced the severity of the tail strike.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Employment and promotion of pilots earlier than company minimum hours
Safety issue number: AO-2024-036-SI-01
Safety issue description: ASL Airlines Australia employed and promoted pilots earlier than the prescribed minimum experience hours without additional controls in place to manage the risk of lower experienced pilots on the flight deck.
Additional safety action by ASL Airlines Australia
The operator’s internal review identified an inconsistency between the operator’s standard operating procedures and the manufacturer’s recommendation with regard to which pilot (the pilot flying or the pilot monitoring) was to make an ‘attitude’ call when the aircraft pitch angle approaching landing increased above 5°.
ASL Airlines Australia’s internal investigation of the occurrence will be incorporated into the relevant sections of the ASL Airlines Australia HF/NTS training.
A summary of the internal investigation will also be included in the operator’s internal safety publication.
Glossary
| ATC | Air traffic control |
| ATIS | Automatic terminal information service |
| CAA | Civil Aviation Authority (UK) |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| CCTV | Closed circuit television |
| CVR | Cockpit voice recorder |
| DFO | Director of flight operations |
| DA | Decision altitude |
| FO | First officer |
| ILS | Instrument landing system |
| LED | Light-emitting diode |
| METAR | Meteorological aerodrome report |
| OPC | Operator proficiency check |
| PAPI | Precision approach path indicator |
| PF | Pilot flying |
| PM | Pilot monitoring |
| TAF | Terminal area forecast |
| TEMPO | Temporary significant variation to prevailing conditions |
| WOCL | Window of circadian low |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- ASL Airline Australia flight records from the occurrence aircraft
- ASL Airlines Australia Operations Manuals and Standard Operating Procedures for the BAe 146
- the captain and first officer of the occurrence aircraft
- the director of flying operations, ASL Airlines Australia
- Civil Aviation Safety Authority
- BAE Systems
- Airservices Australia
- cockpit voice recorder and flight data recorder
- Brisbane Airport Corporation CCTV images
- the captains from the 2 preceding aircraft to VH-SAJ
- Bureau of Meteorology
- Flight Radar24
- Google Earth
References
Australian Transport Safety Bureau. (2009). Tail Strike, Brisbane Airport, Queensland, on 23 October 2008, VH-NJM, British Aerospace BAe 146-300. Retrieved from /publications/investigation_reports/2008/aair/ao-2008-074
Australian Transport Safety Bureau. (2016). Tail strikes during landing involving Bombardier DHC-8 402, VH-QOT and VH-QOS, Brisbane Airport, Queensland, on 5 November 2013 and Roma Airport, Queensland, on 11 December 2013. AO-2013-201.
Causse. (2024). How a pilot's brain copes with a stress and mental load.
Civil Aviation Safety Aurthority. (2024). Civil Aviation Safety Regulations 1998. Retrieved from CASR 121.495: https://www.legislation.gov.au/F1998B00220/latest/text/3
Endsley, M. (1988). Design and evaluation for situation awareness enhancement. Proceedings of the Human Factors Society 32nd Annual Meeting , 97-101.
Fabre, D. E. (2022, June). AXA. Retrieved from Hierarchy in the cockpit: understanding decision making at the time of landing: https://www.axa.com/en/insights/hierarchy-in-the-cockpit-understanding-…
Federal Aviation Administration. (n.d.). Spatial Disorientation Visual Illusion.
Garland, D. W. (1999). Handbook of Aviation Human Factors. Mahwah, NJ.
Harris, D. (2011). Human Performance on the Flight Deck. Ashgate Surrey, England.
Hirshkowitz, M. W.-4. (2015). National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep health.
Institute, Battelle Memorial. (1998). An Overview of the scientific literature concerning fatigue, sleep and the circadian cycle.
International Civil Aviation Organisation. (2015). ICAO, Fatigue Management Guide for Airline Operators. Retrieved from ICAO:
Roach, G. D. (2004). A model to predict work-related fatigue based on hours of work. Aviation, Space and Environmental Medicine,.
Salas, & Maurino. (2010). Human Factors in Aviation, Second edition.
United Kingdom Civil Aviation Authority. (2023). Flight-crew human factors handbook. Retrieved from https://www.caa.co.uk/publication/download/14984
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Director of Safety, ASL Airlines Australia
- the captain
- the first officer
- Civil Aviation Safety Authority
- Air Accidents Investigation Branch, United Kingdom
- Part 121 aircraft operator (party with involvement)
- Bureau of Meteorology
- Airservices Australia.
Submissions were received from:
- the captain
- ASL Airlines Australia
- Civil Aviation Safety Authority
- Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The flight was operated under Civil Aviation Safety Regulations Part 121 (Air transport operations – larger aeroplanes).
[2] Pilot flying and pilot monitoring: procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[3] Runways are named by a number representing the magnetic heading of the runway. Parallel runways are represented by an L for left and R for right.
[4] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL).
[5] ATIS: an automatic service which broadcasts airport specific information on the aviation VHF radio frequencies.
[6] Few: 1–2 okta of cloud cover. An Okta is a unit of measurement used to describe the extent of cloud cover (1–8).
[7] Scattered: 3–4 okta of cloud cover. An Okta is a unit of measurement used to describe the extent of cloud cover (1–8).
[8] Decision altitude is a specified altitude in the precision approach at which a missed approach must be initiated if the required visual reference to continue the approach has not been established.
[9] Runway Visual Range: measured using an electronic instrument RVR is the maximum distance at which the runway, or lights or markers delineating it, can be seen from a position above a specified point on its centreline.
[10] BAe 146 airbrake forms part of the aircraft’s tail cone when in the closed position, two petals extend from the tail cone to provide aerodynamic resistance and slow the aircraft.
[11] Precision Approach Path Indicator (PAPI): a ground-based system that uses a system of coloured lights used by pilots to identify the correct glide path to the runway when conducting a visual approach. Four white PAPI lights on approach indicate the aircraft is too high.
[12] Flare: the final nose-up pitch of a landing aeroplane used to reduce the rate of descent to about zero at touchdown.
[13] Light-emitting Diode: a semiconductor diode which glows when a voltage is applied.
[14] Category 1 (CAT I) lighting system: a CAT I lighting system normally consists of a row of lights on the extended centre line of the runway extending over a distance of 900 m from the runway threshold.
[15] TAF: a statement of meteorological conditions expected for a specific period of time in the airspace within a radius of 5 NM (9 km) of the aerodrome reference point.
[16] Broken: 5–7 okta of cloud cover. An okta is a unit of measurement used to describe the extent of cloud cover (1–8).
[17] INTER: an intermittent deterioration in the forecast weather conditions, during which a significant variation in prevailing conditions is expected to last for periods of less than 30 minutes duration.
[18] Advection fog develops when warm moist air moves (advects) over a cooler surface resulting in the cooling of the air to below its dew-point temperature, and subsequent saturation and condensation.
[19] Tempo: used to indicate significant temporary variations from the prevailing conditions of 30 minutes or more but less than 60 minutes.
[20] L3: now L3 Harris Technologies, Inc. Melbourne, Florida, USA.
[21] Vref: reference landing speed calculated on the aircrafts gross weight for landing.
[22] Vapp: reference approach speed when the flaps are in landing configuration and the landing gear extended.
[23] N1: presents the rotational speed of the low pressure (low speed) engine spool.
[24] Oleo: an oleo strut is a pneumatic air–oil hydraulic shock absorber used on the landing gear of most large aircraft
[25] RAIM: receiver autonomous integrity monitoring – used to assess the integrity of individual signals collected by a GPS receiver.
[26] Minima: landing minima consist of both visibility and/or RVR, and cloud base elements.
[27] The self-report instrument utilised the Samn-Perelli Fatigue Checklist, which utilises a 7‑point scale ranging from “1 – Fully Alert, Wide Awake” to “7 – Completely Exhausted, Unable to Function Effectively” (Samn & Perelli, 1982).
[28] HIAL’s: high intensity approach lighting.
Occurrence summary
| Investigation number | AO-2024-036 |
|---|---|
| Occurrence date | 25/06/2024 |
| Location | Brisbane Airport |
| State | Queensland |
| Report release date | 09/09/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Ground strike, Unstable approach |
| Occurrence class | Serious Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | British Aerospace |
|---|---|
| Model | BAe 146 Series 300 |
| Registration | VH-SAJ |
| Serial number | E3150 |
| Aircraft operator | ASL Airlines Australia |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Sydney Airport, New South Wales |
| Destination | Brisbane Airport, Queensland |
| Damage | Minor |