A Baron that yawed and rolled before impacting the ground next to the runway after the mixture instead of the throttle had been used to simulate an engine failure highlights the importance of procedures aligning with manufacturer guidance.
On 11 April 2024, an instructor and student pilot were operating the twin-engine Beechcraft E55 Baron to conduct a navigation exercise under the instrument flight rules from Cowra, New South Wales, an ATSB investigation report details
After conducting instrument approaches to Goulburn and Canberra, the aircraft returned to Cowra to fly an instrument approach with one engine inoperative.
Arriving over the airport, the instructor simulated a single engine failure by moving the left engine mixture control lever to the idle cut-off position.
“This was in accordance with the operator’s relevant procedure at the time, but differed from Beechcraft’s aircraft flight manual,” Director Transport Safety Stuart Macleod said.
The manufacturer’s procedure prescribes setting zero thrust by retarding the propeller lever to the feather detent, and the throttle lever to 12 inches of manifold pressure.
“The Beechcraft flight manual states using the throttle to simulate engine failure is to ‘avoid difficulties of restarting an engine and preserve the availability of engine power’,” Mr Macleod noted.
Civil Aviation Safety Authority guidance also recommends using the throttle, and not mixture, for one engine inoperative training.
With the aircraft operating on just the right engine, and the left engine’s propeller windmilling, the student conducted an instrument approach before visually establishing the aircraft on final approach to the runway.
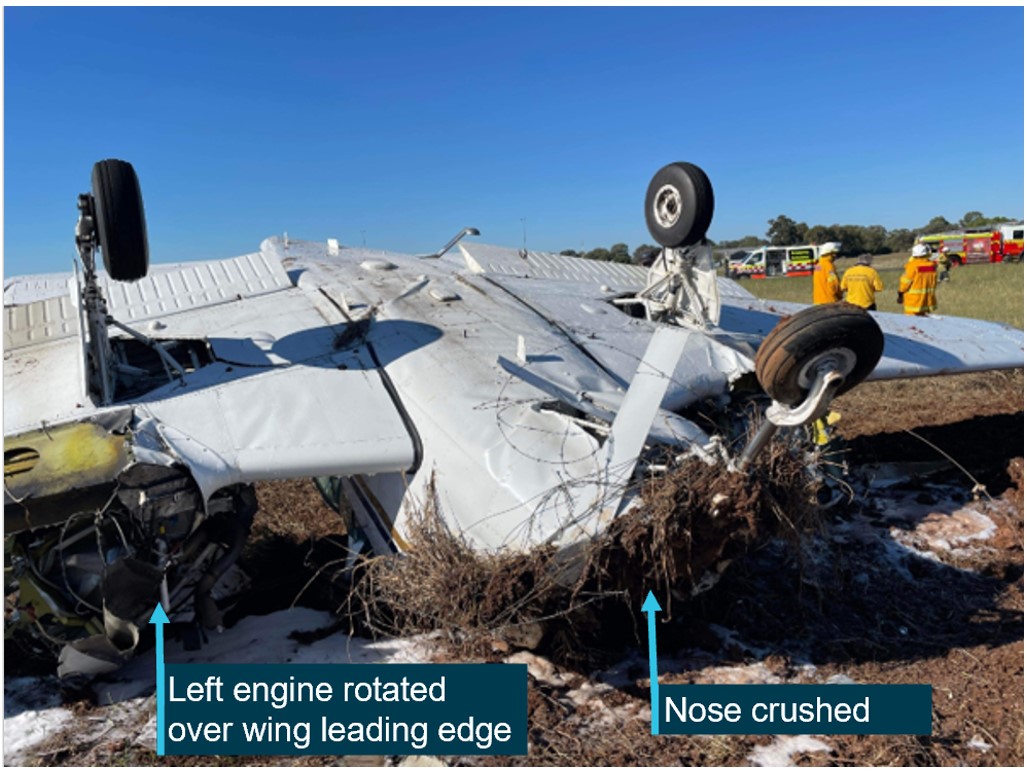
During the landing flare, the instructor initiated a go-around, and the aircraft rapidly yawed and rolled to the left, impacting the ground in an almost vertical nose-down attitude, before coming to rest inverted.
Fortunately, the pilots survived with minor injuries, even though ATSB analysis found the impact deceleration likely exceeded 30 G, principally in a forward direction, with the stable collapse of the airframe structure forward of the cabin and crash-resistant fuel cells aiding their survivability.
“When attempting to set zero thrust during the downwind leg of the final circuit, it was likely the instructor unintentionally did not move the left engine’s mixture lever back to rich, to ensure it was available for instant use if needed,” Mr Macleod explained.
“As a result, the go-around was initiated below the minimum control speed, with the left engine inoperative, resulting in an asymmetric loss of control.”
Since the accident the training operator, Fly Oz, has amended its multi-engine training procedures to only simulate engine failures using throttle at any height.
“Accidents as a result of engine malfunctions in twin-engine aeroplanes are rare, but often fatal. As such, training to manage one engine inoperative flight is important but should not introduce unnecessary risks,” Mr Macleod remarked.
“In this case, the manufacturer required the throttle be used to simulate an engine failure, and CASA guidance also recommends using the throttle rather than the mixture. This ensures power can quickly be restored if needed.”
On the morning of 12 August 2024, a Fairchild SA227-DC was being operated by Skippers Aviation on a non-scheduled air transport passenger flight from Forrestania to Perth, Western Australia. Close to the top of descent into Perth, the crew experienced a complete loss of pressure in the aircraft’s hydraulic system. The crew coordinated with air traffic control for a holding pattern to allow for time to troubleshoot the failure and prepare for an appropriate approach and flapless landing. Ground inspection vehicles were requested to ascertain post-landing if fluid was visibly leaking onto the runway and a tow vehicle was requested to recover the aircraft after landing.
After successfully landing and stopping on the taxiway, the captain was unable to establish contact with the tow vehicle and then decided to continue to taxi to the operator’s apron. As the aircraft approached the operator’s apron, a slight downhill slope caused an increase in speed. However, when the crew applied the brakes, they were ineffective. In an effort to avoid collision with a hangar, the captain applied reverse thrust. However the aircraft continued to roll forward, the captain shut down the engines and feathered the propellors before impacting the hangar. The aircraft sustained damage to the right-side wingtip and propellor, there were no injuries to crew or passengers.
What the ATSB found
During the flight, the captain was supervising the cadet-entry first officer’s flying when a crack in a hydraulic line led to a hydraulic fluid leak and in-flight failure of the hydraulic system.
Consistent with the first officer’s minimal experience, their ability to contribute to the in-flight emergency management was limited, requiring the captain to manage the emergency. The captain was required to take on both the pilot flying and pilot monitoring roles, which reduced their ability to effectively manage the emergency.
The first officer's inexperience limited their ability to contribute to managing the hydraulic system failure. This negatively impacted crew resource management and increased the captain's workload.
After stopping on the taxiway, the captain mistakenly assumed the brakes were functioning. Unable to locate or contact the tow tug, and influenced by self-imposed pressure, they continued the taxi to the apron.
On arrival at the operator’s apron, the aircraft had minimal braking capacity and the crew was not able to stop the aircraft. Due to the proximity of the hangar, the captain had limited opportunity to take corrective action and a collision occurred.
What has been done as a result
The operator has advised it is reviewing maintenance practices for tube repairs and replacements for the fleet. In addition, the following actions have been advised to the ATSB by the operator:
The flight crew received refresher training in human factors, standard operating procedures, workload management and decision‑making. Additionally, the captain has completed remedial training on decision‑making.
The captain has completed a series of simulator exercises to confirm all procedures are followed in accordance with the aircraft quick reference handbook (QRH) and company standards.
During their fleet meeting, all fleet pilots were made aware of the incident and the lessons learnt to prevent reoccurrence.
All fleet pilots have completed theory training and examination on the hydraulic system.
Safety message
This occurrence highlights the necessity for accurate assessment of system functionality following an in-flight system failure and the need to follow standard operating procedures. Vigilance when assessing aircraft performance and an objective assessment of system status are vital to minimise opportunities for error and avoid relying on potentially misleading indicators.
Flight crews are advised to prioritise procedural compliance in uncertain circumstances, especially when perceived pressure is heightened to continue to operate an aircraft in non‑normal situations.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At about 0900 local time on 12 August 2024, a Fairchild SA227-DC Metroliner (Metro) aircraft, registered VH-WAJ and operated by Skippers Aviation, was conducting a non‑scheduled air transport flight with 2 crew and 4 passengers on board from Forrestania to Perth, Western Australia. The first officer (FO), who was completing supervised line flying, was the pilot flying and the captain was in the pilot monitoring role.
At about 1000, the aircraft was close to the top of descent into Perth (Figure 1), when the right hydraulic system low-pressure annunciator light flickered and then subsequently remained solid, which indicated a system failure.
Figure 1: Flightpath and location of VH-WAJ at the time of hydraulic failure
Source: Google Earth and QAR data, annotated by the ATSB
The flight crew consulted the aircraft quick reference handbook (QRH) and followed the standard checklist procedures to manage the indicated hydraulic system failure. The crew identified that the hydraulic pressure remained between 1,700 and 2,100 psi and as per the QRH instruction, the flight should be continued as originally planned. The crew reported following the planned route until, a short time later, the left hydraulic low-pressure annunciator light illuminated. The captain checked the main pressure gauge which displayed 0 psi and identified that there was a total failure of the hydraulic system.[1] The captain requested vectors[2] from air traffic control (ATC) for a holding pattern to allow time to determine the appropriate speed and extra distance required to conduct a flapless landing. This also provided time for the captain to instruct the FO on how to conduct a manual extension of the landing gear using the hand pump, as this was the first time the FO had undertaken this task.
ATC provided vectors for holding, while the captain recalled trying to contact the company maintenance watch directly, however, was unable to find the correct frequency and instead was able to advise other company representatives of the situation.
The captain considered but elected not to broadcast a PAN PAN[3] call to ATC, instead advising them that a tow vehicle (tug) would be required to tow them from the runway to the apron. The captain also requested ATC to provide a vehicle to follow the aircraft after landing for an inspection of any fluid visibly leaking onto the runway.
After finalising details for landing, the captain and first officer swapped ‘pilot flying’ roles due to the limited experience of the FO. The captain then took control of the aircraft and conducted the flapless landing on runway 24 at Perth Airport.
After a successful landing, they exited the runway and stopped on taxiway ‘A’. The captain reported looking for the tow vehicle but could not visually locate it and was unable to establish direct communication with the tug. The captain recalled that at this time the hydraulic system pressure gauge showed a positive pressure and so they elected to test the brakes and found that some braking pressure was evident.
An airport vehicle following the aircraft reported to ATC that no fluid was observed on the runway. ATC requested the crew’s intentions, and the captain informed them that they would continue the taxi back to the operator’s apron without the assistance of a tug.
As the aircraft approached the operator’s apron and turned toward the hangar, the aircraft’s speed increased due to a slight downhill gradient. The captain and FO applied full braking, but neither of their systems responded.
Figure 2: VH-WAJ shown stationary after collision with operator’s hangar
Source: Operator
In an attempt to avoid collision with the hangar, the captain momentarily used reverse thrust, then shut down the engines and feathered[4] the propellers. However, the aircraft’s right wingtip collided with the hangar at low speed, before the right propeller made contact. The impact resulted in minor damage to the right propeller and wingtip (Figure 2). All of the occupants disembarked safely, with no injuries to the crew or passengers.
Context
Aircraft information
VH-WAJ, a Fairchild Industries SA227-DC Metroliner was manufactured in the United States in 1995. The 19-seat aircraft was fitted with 2 Garrett TPE331-12 turboprop engines.
The flight log for the morning of the incident showed that the aircraft was considered serviceable. Maintenance documentation identified the successful repair of a hydraulic leak in April 2024, with no known hydraulic deficiencies prior to the incident flight.
Flight crew
The crew was composed of a training captain and FO. Each pilot held a commercial pilot licence (aeroplane) and a class 1 medical certificate.
The captain had about 3,620 hours total flying experience of which about 1,120 hours were on the Metro.
The FO had 325 hours total flying experience and was a cadet in training, with about 34 hours experience on the Metro.
Cadet training
Skippers Aviation partnered with a training organisation, accepting cadets with little prior aviation experience and providing a training captain for them while conducting Part 121 operations.[5] For this scheme, the operator had identified that new cadet FOs may have little prior aeronautical experience and so may be near capacity in normal operations of the aircraft and possibly unable to effectively handle emergency situations or support other crew during such an event.
The operator confirmed that significant training is conducted with training captains to ensure that pilots’ skills are developed in live operational environments while ensuring safety through operational oversight. Supervised line flying, line training and line checks were used to expose cadets to the operator’s procedures and to enable them to gain real time experience conducting authorised activities on the aircraft over the operator's network. Additional training requirements for cadet FOs included increased simulator training sessions and expanded line oriented flight training to 100 hours from 50 hours to improve preparedness for both routine and emergency scenarios.
Civil Aviation Safety Regulation 119 (Australian air transport operators, certification and management) Subpart 119.E (Training and checking for operational safety‑critical personnel) details how an approved company exposition assesses the competence of a flight crew member and the training and checking system.
Airport information
Perth Airport is the major international aerodrome in Western Australia. The main runway 03/21 is 3,444 m in length and the secondary runway 06/24 is 2,163 m in length; both runways are 45 m wide (Figure 3).
A system of interconnected taxiways connects runways with terminals, aircraft aprons and hangars. The captain reported using asymmetric power to taxi (as nose wheel steering was not functional due to the hydraulics failure) at walking pace via taxiways D and H to the operator’s apron.
Figure 3: Aerial view of Perth Airport showing the route used by VH-WAJ after landing
Source: Google Earth and QAR data annotated by the ATSB. Metro model not to scale.
Meteorological conditions
The terminal forecast for Perth Airport on the day of the occurrence was for intermittent rain showers and scattered low cloud. The wind was mainly from the west at 15–25 kt and visibility was reduced to 5,000 m at times with low cloud down to 1,500 ft.
Recorded information
The aircraft was fitted with a Fairchild model A200S cockpit voice recorder (CVR) which was transported to the ATSB technical facilities in Canberra for download. The recovered audio data contained 5 channels of high-quality audio with about 32 minutes recorded which included the descent, landing and taxi.
The recorded audio is consistent with the crew’s recollection at interview of the event and their discussions with ATC for the descent, landing and taxi.
Hydraulic system
The main hydraulic system on the Metro provides hydraulic pressure for actuation of the landing gear, flaps and nose wheel steering. Without the hydraulic system, the flaps, nose wheel steering and landing gear were inoperable and aircraft braking had limited functionality.
The nose wheel steering system provides directional control while taxiing, however the nose wheel casters move freely when the system is not engaged. Additionally, there is a self‑contained hydraulic power system for brake operation.
The main hydraulic system is pressurised by two engine‐driven hydraulic pumps (EDPs) and there is one manually‑operated hand pump. The hand pump draws reserve hydraulic fluid from the same reservoir as the EDPs and provides pressure for the emergency landing gear extension.
Normal system pressure is 2,000 psi. Two warning lights on the annunciator panel warn of low pump pressure or pump failure and a pressure gauge on the instrument panel is used to monitor the hydraulic system.
The brake hydraulic system is completely independent of the main hydraulic system used for landing gear and wing flap actuation. The power brake system includes master cylinders, brake accumulators and a pressure gauge. The brake accumulators, pre-charged with nitrogen (to 650 psi) and hydraulic fluid (from the aircraft main landing gear extension lines to 2,000 psi), provide back-up to the main hydraulic system in case of hydraulic pressure loss. The brake accumulators allow multiple brake applications without anti-skid protection until the pressure depletes to a minimum level. A pressure gauge monitors the hydraulic pressure in the accumulators showing normal levels during operation and residual pressure in the case of hydraulic fluid loss. When the accumulators bleed down to their minimum pressure, the brakes become unavailable.
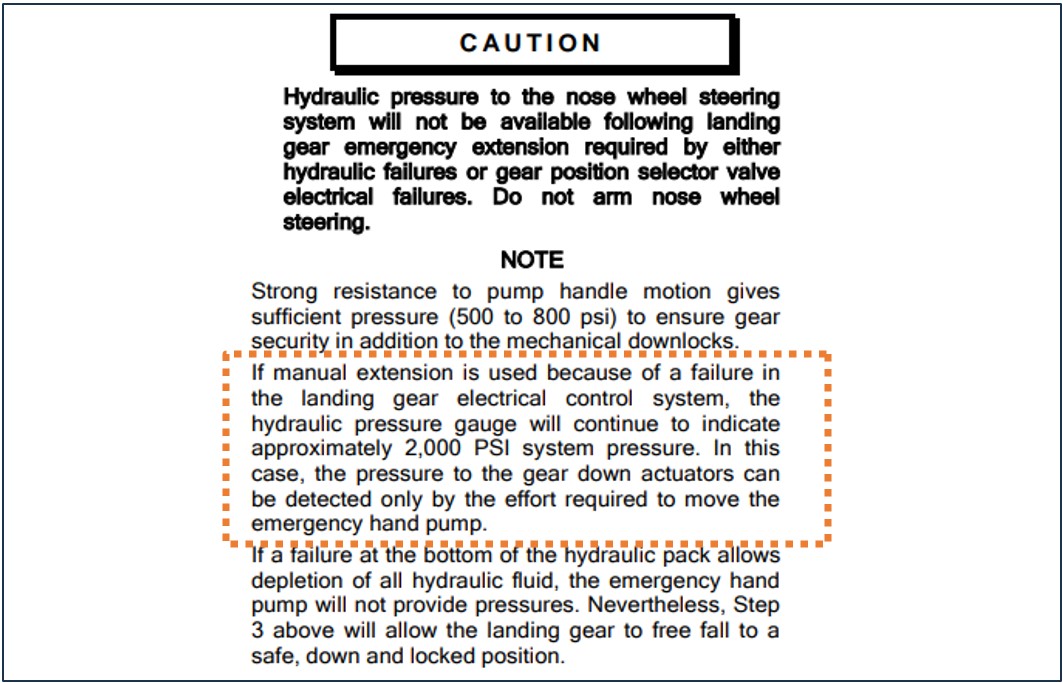
If an emergency manual extension of landing gear is needed, the main hydraulic pressure gauge will continue to indicate approximately 2,000 psi system pressure (Figure4). The captain recalled identifying that the hydraulic pressure read about 2,100 psi after landing.
Figure 4: Extract from operator’s QRH describing the pressure reading after landing gear emergency extension
Source: Operator’s Quick Reference Handbook, annotated by the ATSB
QRH procedure for hydraulic pressure loss
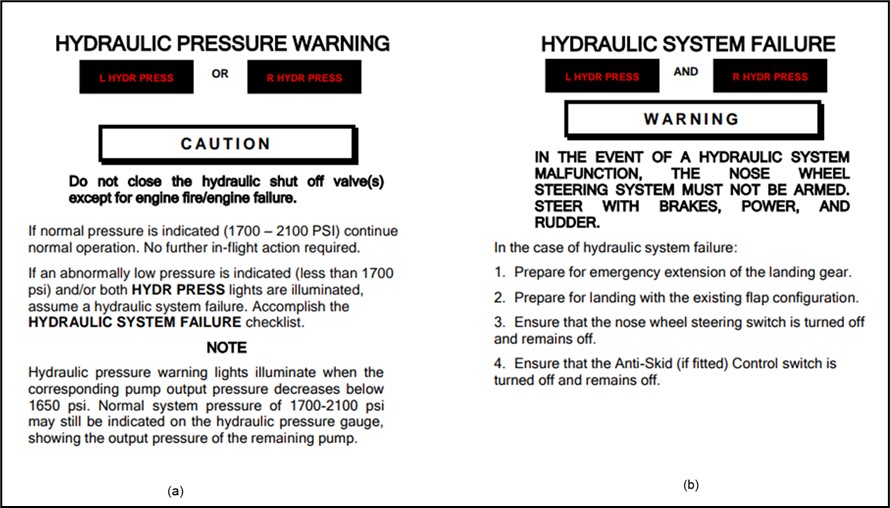
The crew reported that they followed the checklist procedures from the operator’s QRH to manage the hydraulic system failure. Figure 5 shows extracts from the QRH detailing the procedure for management of a hydraulic system failure.
Figure 5: Partial extracts from the operator’s QRH for hydraulic failure management
Source: Operator’s Quick Reference Handbook
The QRH also indicated that after landing with hydraulic system failure, the aircraft should have sufficient accumulator pressure to taxi clear of the runway.
Post‑event maintenance inspection
A post‑event maintenance inspection, conducted by the operator, indicated that the hydraulic system failure was due to a stress crack in the hydraulic pipe's union flare (located in the left landing gear wheel well). This crack allowed fluid loss, which then depleted the remaining hydraulic fluid and caused the warning lights to illuminate.
Flight crew workload
Descent, approach and landing phases are periods of high workload during normal operations due to the increase in task demand. In non-normal operations, such as equipment malfunction, workload levels escalate significantly for the crew who must assess and manage the abnormal conditions, complete additional tasks and make timely decisions under pressure.
At interview, the crew reported that the captain’s workload was very high at the time.
Research that has examined unexpected changes in workload during flight indicate that pilots who face abnormal or emergency situations experience a higher workload and increased number of errors, compared to pilots who do not encounter the same scenarios (Johannsen and Rouse, 1983).
During this time the captain was trying to involve the FO in the handling of the emergency situation by instructing them on the manual release of the landing gear.
Crew resource management
Crew resource management (CRM)[6] plays an important role in workload management and communication in the cockpit, particularly during non-normal situations. For the captain, who had to monitor the FO’s actions and provide instruction, this dual role led to task saturation and increased the likelihood of errors. The normal benefits of CRM to load-shed and delegate tasks can be unrealised when supporting flight crew have minimal experience in the aircraft type and low aeronautical experience.
Confirmation bias
Cognitive biases are mental shortcuts used to aid decision-making. Research points to most incidents of cognitive bias in flight operations happening during landing and at the end of their journey, with over 55% of incidents occurring in this phase (Nadri and others, 2024). A common bias is confirmation bias which describes a tendency for people to seek information and cues that confirm a tentatively held belief and not seek (or avoid) information that supports an opposite conclusion (Wickens & Hollands, 2000). Under high cognitive load this is amplified and individuals tend to focus on familiar or expected information reducing their openness to consider all relevant information (Liden, 2023).
Self-imposed pressure
Pilots may experience self-imposed pressure, for a range of reasons, that can form a desire to meet operational expectations. This pressure can manifest as a feeling to expedite tasks to avoid impacting schedules or inconveniencing other operators. The captain described that, after landing and bringing the aircraft to a stop on taxiway A, there was self-imposed pressure to clear the taxiway for incoming and outgoing aircraft.
Safety analysis
During a non-scheduled air transport flight from Forrestania to Perth, the crew of VH-WAJ experienced a complete loss of pressure in the hydraulic system. Without the hydraulic system, the flaps, nose wheel steering, and landing gear were not functional, however limited braking was available from a reserve pressure accumulator. The captain conducted a flapless landing and after stopping on the taxiway for a short moment, opted to continue the taxi to the operator’s hangar, mistakenly believing the hydraulic pressure had returned and that the brakes were functioning. In close proximity to the operator’s hangar, the crew applied the brakes to stop the aircraft while on a slight slope, but they were ineffective and the aircraft collided with the hangar, damaging the right wingtip and right propellor.
The complete loss of hydraulic pressure was identified post-flight as a result of a fluid leak from a hydraulic pipe crack in the union flare in the left main landing gear wheel well.
The training captain ordinarily had an increased physical and cognitive workload due to oversight of the aircraft and providing guidance for the novice FO. However, their workload surged considerably when the illumination of both hydraulic system warning lights required immediate management of the in-flight emergency. In addition to conducting the checklist procedures, the captain had the added responsibilities of all the radio communications and guiding the FO through the emergency task of the manual extension of the landing gear. Additionally, the captain assumed the role of pilot flying from the FO for the approach and landing at Perth. This contributed to the captain’s decision to continue taxiing to the apron after exiting the runway, as the demands of the emergency likely disrupted the typical task prioritisation for post-landing procedures after this event, which would have been to have the aircraft towed.
The FO’s inexperience and low number of hours on the Metro, while completing supervised line‑flying, reduced their capacity to contribute to decision-making, workload and task‑sharing in the same manner as a more experienced FO during the emergency. The FO’s unfamiliarity with non-normal procedures outside of the simulator meant that they were unable to anticipate the needs of the captain to help distribute the workload after the hydraulic system had failed. As a result, this limited their ability to fully support the captain, which negatively impacted CRM and further increased the captain’s workload.
The captain reported that they did not check the brake accumulator gauge after landing. It was likely that after using the brakes during landing, the reserve accumulator pressure became depleted, although this was not obvious based on the feel of the brakes when tested after stopping.
Both the in-flight positive pressure indication observed on the main hydraulic pressure gauge (due to the manual extension of the landing gear) and the report of no fluid on the runway mistakenly supported the captain‘s understanding that the pressure had returned to the aircraft and that the brakes were functional. The absence of establishing contact with a tow vehicle and being aware of other traffic requiring access to the taxiway, it is likely that the captain felt self-imposed pressure to continue to move the aircraft. This likely influenced the captain’s decision to continue to taxi to the hangar.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the hydraulics system failure involving Fairchild SA227-DC, registered VH-WAJ, at Perth Airport, Western Australia, on 12 August 2024.
Contributing factors
A crack in a hydraulic line in flight resulted in a loss of hydraulic pressure and required the crew to manage the emergency.
Following the hydraulic system failure, the captain was required to take-on both the pilot flying and pilot monitoring roles. This reduced the ability to effectively manage the emergency.
The first officer's inexperience limited their ability to contribute to managing the hydraulic system failure. This negatively impacted crew resource management and increased the captain's workload
After stopping on the taxiway, the captain mistakenly assumed the brakes were functioning. Unable to locate or contact the tow tug and influenced by self-imposed pressure, continued the taxi to the apron. Approaching a hangar, the crew applied the brakes, but they were ineffective and resulted in the right wingtip and propellor colliding with the hangar.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence
Safety action by the operator
The flight crew received refresher training in human factors, standard operating procedures, workload management and decision‑making. Additionally, the captain has completed remedial training on decision‑making.
The captain has completed a series of simulator exercises to confirm all procedures are followed in accordance with the QRH and company standards.
During their fleet meeting, all fleet pilots were made aware of the incident and the lessons learnt to prevent reoccurrence.
All fleet pilots have completed theory training and examination of the hydraulic system.
Skippers Aviation is carrying out a review of maintenance practices for tube repairs and replacements for the fleet.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the captain and first officer
Skippers Aviation safety manager
video footage of the accident flight and other photographs taken on the day of the accident
cockpit voice recorder.
References
Johannsen, G & Rouse, WB, (1983). Studies of planning behaviour of aircraft pilots in normal, abnormal, and emergency situations. Systems, Man and Cybernetics, IEEE Transactions on, (3), pp.267-278.
Nadri, C., Regalado, J., Ferris, T., & Zahabi, M. (2024). Cognitive Biases in Commercial Aviation: Empirical Review of Accident Reports. Proceedings of the Human Factors and Ergonomics Society Annual Meeting.
Wickens, C. D., & Hollands, J. (2000). Engineering psychology and human performance
(3rd ed.). Upper Saddle River, NJ: Prentice Hall.
Liden, M. (2023). Confirmation bias in criminal cases. Oxford University Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
captain and first officer
Skippers Aviation (the operator)
the Civil Aviation Safety Authority
Airservices Australia
There were no submissions received.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The hydraulic system controls movement of external components including flaps and landing gear.
[2]Specific directions to sequence an aircraft for the safe and efficient movement of aircraft in controlled airspace.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition, which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[4]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[5]Part 121 of Civil Aviation Safety Authority (CASA) regulations cover air transport rules for larger aeroplanes.
[6]Crew resource management (CRM) refers to the effective use of all available resources: human resources, hardware, and information to achieve safe and efficient operation.
A Robinson R44 helicopter was operating at a high-density altitude, and likely above its maximum gross weight, when it impacted rocky terrain shortly after take-off in Western Australia’s Pilbara region, an ATSB investigation has found.
On 3 November 2022, the R44 was departing a cultural heritage site in the Collier Ranges, with a pilot and three passengers, who were members of a survey team, on board.
During the take-off, travelling about 27 kt and just above treetop height, the pilot experienced a severe drop in the helicopter’s performance, and the low rotor RPM warning sounded.
“The pilot conducted the low rotor RPM recovery actions, but was unable to arrest the descent,” ATSB Director Transport Safety Dr Stuart Godley said.
The helicopter impacted rocky terrain about 150–200 m from its take-off location, and rolled onto its left side, resulting in substantial damage, serious injuries to one passenger, and minor injuries to the pilot and other two passengers.
The ATSB’s final report notes the take-off occurred at an elevation of 2,170 ft above mean sea level, with a calculated density altitude of 4,210 ft.
Compounding this, the pilot used estimated weights for the passengers, based on figures provided by one of the passengers. This resulted in the calculated helicopter gross weight below the maximum take-off weight, although the helicopter was likely being about 30 kg over the maximum take-off weight.
“More power than the engine could provide was needed to safely conduct the take-off, given the overweight helicopter condition, confined take-off area and high-density altitude,” Dr Godley said.
“This highlights the importance of using accurate figures when calculating weight and balance, and expected performance, especially when operating at full capacity and near the maximum gross weight.”
The investigation report notes the drop in performance observed by the pilot coincided with the helicopter transitioning out-of-ground effect. (In ground effect, air drawn down through the rotor collects under the helicopter and provides a ‘cushion’ of air, meaning slightly less power is required than would otherwise be needed.)
“Regularly reviewing and being prepared to amend flight plans, such as by reducing passenger numbers to increase performance margins, is central to safe operations,” Dr Godley added.
While not found to have contributed to the accident, the ATSB investigation also found the flight was operated under CASA’s Part 138 regulations, which are for aerial work operations.
The flight should have been operated under Part 133, for air transport operations, as it was a passenger carrying flight. Further, the operator was only approved for aerial work operations.
Rail transport operators and registered training organisations are urged to review and validate their rail safety worker competency assessments, in response to an investigation into a grain train collision near Tamworth, New South Wales.
On 6 January 2022, three banking locomotives were added to the rear of a loaded grain train at Werris Creek, to assist it up a steep uphill gradient later in its journey.
During transit, the banking locomotives separated from the train. Shortly afterwards, the train stopped, and the locomotives collided with the rear of the train, resulting in significant damage to the rear wagon and the front banking locomotive.
A transport safety investigation was conducted by the Office of Transport Safety Investigations (OTSI), which investigates rail accidents in New South Wales on behalf of the Australian Transport Safety Bureau.
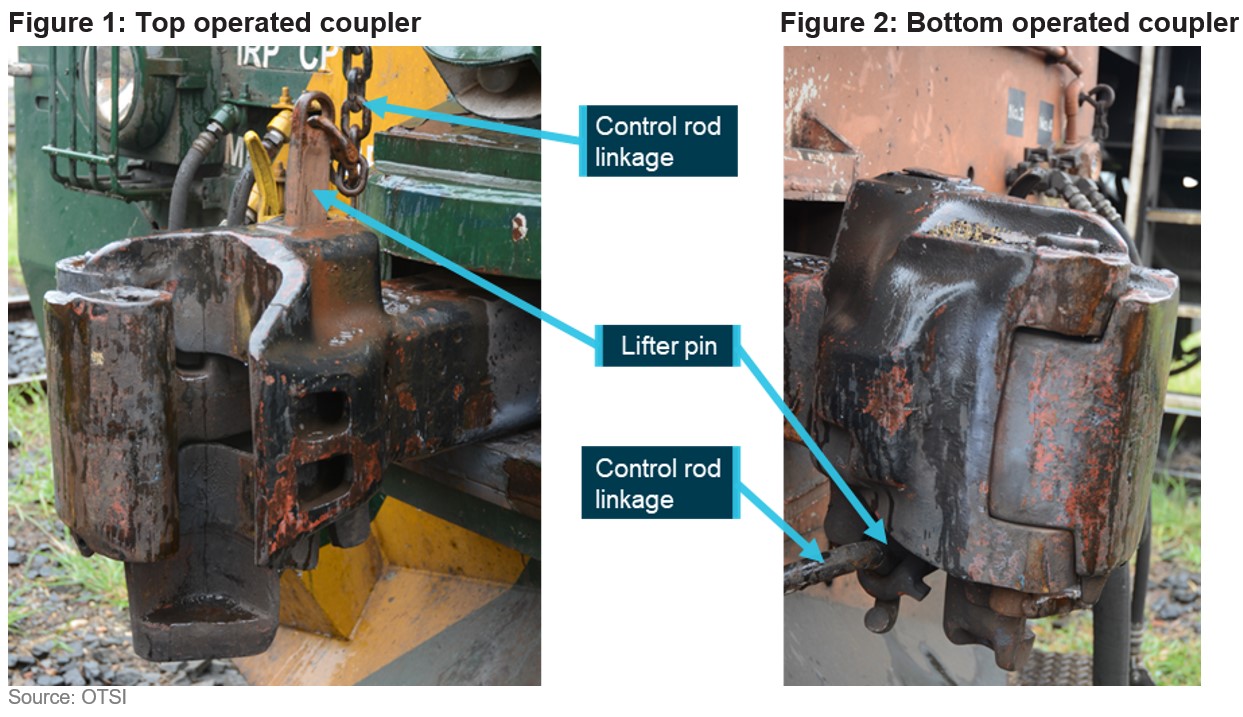
The investigation found the train separation was highly likely due to the knuckle on the bottom operated coupler of the lead banking locomotive remaining unlocked after coupling.
Notably, it was found the train crew had not performed a ‘stretch test’ after attaching the banking locomotives.
“A stretch test would have identified that the knuckle on the bottom operated coupler of the lead banking locomotive had remained unlocked after coupling,” OTSI’s Acting Chief Investigator Jim Modrouvanos said.
“It was also found that while the train crew had been assessed as competent in shunting during both vocational education and training (VET) and enterprise-based assessments on several occasions, the supporting evidence collected was usually limited to a single check box that the task had been ‘performed correctly’.”
As a result of these findings, a Safety Advisory Notice has been issued to rail transport operators, and registered training organisations acting on their behalf, to review and validate their rail safety worker competency assessments.
“The competence of rail safety workers is critical to safe railway operations,” Mr Modrouvanos asserted.
“Relevant industry members should validate their competency assessments to ensure their assessment tools, processes and judgements are reliably meeting the principles and requirements of competency-based training and assessment.”
Additionally, OTSI’s investigation found after the separation event, the response taken by the banking locomotive’s driver in relation to the sudden loss of brake pipe pressure was consistent with their training and the operator, Southern Shorthaul Railroad’s emergency response procedures, despite being inappropriate for the situation.
“It was also found the operator’s risk assessments for this operation were mostly performed by members of the management team,” Mr Modrouvanos added.
“While the team had varying levels of operational experience, consultation with operational staff directly affected by the operation did not occur.
“During assessment of risk, consultation consisting of effective and meaningful engagement becomes critical in identifying novel risks which may not be immediately apparent,” he continued.
“Particular attention should be given to procedures utilised in past operational environments, to ensure their ongoing appropriateness in these unique operational circumstances.”
Southern Shorthaul Railroad has taken a range of safety actions since the accident, including providing train crew with reference materials related to coupler functionality, defining the process for a ‘stretch test’ after coupling, and contextualising emergency response procedures for banking operations.
As part of the final report release, a second Safety Advisory Notice focuses on the operation and design features of automatic couplers.
A recent ATSB / OTSI investigation has found issues with the assessment of rail safety worker competence. These issues have involved both vocational education and training (VET) and enterprise‑based qualifications.
What happened
The Office of Transport Safety Investigations (OTSI) has completed an investigation into an accident, on behalf of the ATSB, where 3 locomotives located at the rear of a loaded grain train separated from the lead portion of the train in transit. Shortly afterwards, the lead portion of the train stopped and the 3 now detached locomotives at the rear collided with the stationary lead portion. This resulted in significant damage to the rear wagon and a locomotive.
What increased risk
The investigation found that the train crew had not performed a ‘stretch test’ after completing shunting duties at Werris Creek, which contributed to the incident. It also found that while the train crew had been assessed as competent in shunting during both VET and enterprise-based assessments on several occasions, the supporting evidence collected was usually limited to a single check box that the task had been ‘performed correctly’.
Safety advisory notice
RO-2022-001-SAN-02: The Australian Transport Safety Bureau strongly encourages rail transport operators, and registered training organisations acting on their behalf, to review and validate their rail safety worker competency assessments. This is to ensure these assessment tools, processes and judgements are reliably meeting the principles and requirements of competency-based training and assessment.
Assessment of competence
The competence of rail safety workers is critical to safe railway operations. Where competency assessments are aligned to the Australian Qualifications Framework (AQF), i.e. VET, certain standards must be met. These include, in part, that sufficient assessment evidence is collected to ensure a sound, reliable and consistent competency decision is made, irrespective of the assessor. For example, for practical assessments well-described skills, observable behaviours and underpinning knowledge of the task being performed should be assessed and recorded.
Where complying with the AQF is not reasonably practical, for example, a suitable unit of competency or qualification is not available, enterprise-based assessments should still follow these same principles of competence-based training and assessment.
Practical guidance to assist rail transport operators in meeting their obligations include those from the Australian Skills Quality Authority (Users’ guide to the standards for registered training organisations 2015) and the Office of the National Rail Safety Regulator (Application of the AQF to rail safety worker competence assessment).
On 15 August 2024, a Fairchild SA227-DC Metroliner 23, operated by Skippers Aviation, departed Perth Airport, Western Australia (WA) for a flight to Bronzewing Airport, WA, with 12 passengers and 2 flight crew on board. As the aircraft climbed, the crew noted high-temperature air and light smoke emanating from flight deck air vents.
As the smoke quickly increased, the crew commenced actioning the ‘smoke in aircraft’ checklist but required items of the checklist were not completed – the first officer did not don an oxygen mask due to difficulty with its usage, and the left bleed air system was not selected ‘off’. Instead, the crew commenced preparations for a return to Perth and subsequently, the left wing overheat light illuminated. The crew then actioned the ‘wheel well and wing overheat’ checklist and selected the left bleed air system ‘off’, which stopped the smoke ingress into the cabin, but elected not to complete the required action of extending the landing gear.
During the return to Perth, the aircraft deviated both above and below the altitude assigned by air traffic control including a descent to 639 ft below the lowest safe altitude. The crew then completed the ILS approach and landed without further incident. The aircraft was not damaged, and there were no crew or passenger injuries.
What the ATSB found
The ATSB found that a failure within the left air cycle machine prior to departure resulted in hot engine bleed air and smoke entering the cabin and that items on the ‘smoke in aircraft’ checklist were not completed. Consequently, the smoke ingress into the cabin continued and during the return, the left air conditioning duct overheated, and the wing overheat light illuminated. Furthermore, the first officer’s decision not to don an oxygen mask increased their risk of impairment or incapacitation. A later decision not to extend the landing gear, as required by the response checklist, had the potential to increase risk if the wing overheat indication had been associated with a brake fire or wheel well overheat.
The ATSB determined that the workload associated with the in-flight response to the smoke in the cockpit and wing overheat indication adversely affected the flight crew's performance, leading to errors in flight path adherence, checklist completion and decision making.
During the return to Perth, the first officer readback an air traffic control altitude instruction as 2,000 ft AMSL instead of 2,800 ft AMSL. The controller did not identify or correct the error however, following a query from the crew, this was later corrected. Finally, after the assigned altitude had been confirmed by the crew, the aircraft descended below the lowest safe altitude. While the crew were advised of the deviation by air traffic control, the required ‘safety alert’ wording was not used.
What has been done as a result
Following the occurrence, the operator conducted a refresher training course for flight crew on emergency response briefings and a theory examination for flight crew on bleed air, pneumatics, pressurisation and fire warning systems. Practical training sessions were also held for flight crew on revised emergency procedures and the use of the crew oxygen system.
The operator also changed the Metroliner 23 flight crew training program to include a revised Line Oriented Flight Training (LOFT) program including more comprehensive oxygen system training and a presentation on the Metroliner 23 oxygen system.
Safety message
This occurrence highlights the importance of careful and methodical checklist completion. In this case, not completing a checklist resulted in increased risk to the flight and an avoidable increase to an already high workload. This in turn led to later decision-making and flight path management errors.
Additionally, the incident also emphasises the importance of flight crew familiarising themselves with the operation and use of the onboard emergency equipment. When exposed to an environment of smoke and fumes, flight crew must ensure that emergency breathing equipment is correctly utilised.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 15 August 2024, the crew of a Fairchild SA227-DC Metroliner 23 aircraft operated by Skippers Aviation, registered VH-WBQ and callsign ‘Skippy 5003’, taxied the aircraft to runway 24 at Perth Airport, Western Australia (WA) for a flight to Bronzewing Airport, WA. There were 12 passengers on board and the flight crew comprised the captain acting as pilot flying,[1] and the first officer acting as pilot monitoring.
As the aircraft taxied to the runway, the first officer noted that the cabin temperature was unusually warm and selected ‘full cold’ on the temperature selector.
At 0746, the aircraft departed runway 24 and turned left turn following the REPOK 1 standard instrument departure. As the aircraft climbed above about 1,500 ft above mean sea level (AMSL), the captain noted that the cabin temperature was warm and asked the first officer to select full cold on the temperature selector. The first officer responded by advising that full cold was already selected.
As the aircraft climbed above about 3,000 ft AMSL, the first officer attempted to reduce the high cabin temperature by selecting ‘auto’ on the temperature controller before then reselecting ‘full cold’. At about this time, the crew noted that vents on the captain’s (left) side of the flight deck (Figure 1) were blowing very hot air while the vents on the first officer’s (right) side blew the expected cool air.
Figure 1: Exemplar Metroliner 23 flight deck
Source: Matt Hayes, annotated by the ATSB
In response, the captain attempted to close the vent but found it too hot to touch. At the same time, they observed light smoke emanating from the vent. The smoke quickly increased, and the crew commenced the quick reference handbook (QRH) ‘smoke in aircraft’ checklist memory items.[2]
These memory items required the crew to don oxygen masks, establish communications (see the section titled Crew oxygen system) and consider donning smoke goggles. As the smoke was not impacting their vision, both flight crew members elected not to don smoke goggles. The captain donned an oxygen mask and made the required audio selections to establish communications using the mask.
The first officer encountered difficulties in adjusting the mask straps and could not get the mask to fit. They also did not make the required selections to establish communications using the mask, which resulted in the first officer hearing breathing noses through the headset and not being able to communicate using the oxygen mask microphone. As a result of these difficulties, the first officer elected not to wear the mask at that time.
The first officer retrieved the QRH ‘smoke in aircraft’ checklist to confirm the required memory actions had been completed and complete the remaining items of the checklist. For smoke emanating from a bleed air source, such as the air-conditioning system, the checklist required selecting the appropriate bleed air system ‘off’ (see the section titled Quick reference handbook). Before completing those checklist actions, the crew made a PAN PAN[3] broadcast advising air traffic control that there was smoke in the cockpit and that a return to Perth was required. The crew then began preparing for the return to Perth and did not complete the remaining items of the checklist at that time.
At 0751, the Perth Departures air traffic controller acknowledged the PAN transmission and instructed the crew to turn to a heading[4] of 360° and descend to 3,000 ft AMSL to commence the return. At this time, air traffic control also activated the Perth Airport emergency services.
Shortly after, the controller handed the crew over to the Perth Approach controller. One minute later, the approach controller instructed the crew to turn to a heading of 240° and descend to the lowest safe altitude of 2,800 ft AMSL. The first officer incorrectly read back the descent altitude as 2,000 ft AMSL, however the controller did not identify the error (Figure 2). The crew subsequently began descending the aircraft.
Figure 2: Flight path of VH-WBQ
Source: Airservices Australia and Google Earth, annotated by the ATSB
As the aircraft descended, the captain assisted the first officer with donning the oxygen mask and making the required audio selections to establish communications. From this time on, the use of the oxygen mask significantly reduced the intelligibility of the first officer’s radio broadcasts.
At 0756, the crew levelled the aircraft at 2,800 ft AMSL and contacted the controller to confirm the assigned altitude. The controller confirmed the altitude was 2,800 ft AMSL and the assigned heading as 180°. The first officer readback the altitude and heading instructions correctly.
At 0756, as the aircraft turned to the assigned heading, a descent commenced from 2,800 ft AMSL (Figure 3). About 50 seconds later, having observed the descent, the air traffic controller advised the crew to maintain 2,800 ft AMSL and that 2,800 ft AMSL was the lowest safe altitude. The crew immediately commenced climbing the aircraft, having descended to 2,338 ft AMSL (about 1,600 ft above ground level (AGL)).
Figure 3: Flightpath of VH-WBQ after the incorrect readback
Source: Airservices Australia and Google Earth, annotated by the ATSB
In response to the air traffic control instruction, the first officer replied stating ‘unable, Skippy 5003’ intending to convey that the crew were ‘unable’ to clearly hear the instructions. The controller interpreted the statement to mean that the crew were unable to maintain 2,800 ft AMSL and queried if the crew were in visual conditions. The first officer replied that the aircraft was not visual. At the same time, the air traffic control system generated a cleared level adherence monitoring (CLAM) alert for the aircraft. The controller, believing that the aircraft could not maintain altitude and aware that the Perth runway 24 instrument landing system (ILS) provided the lowest available minimum safe altitude, provided the crew with heading instructions directly to the ILS localiser.
While tracking toward the localiser, the aircraft continued climbing until 0757:57 when it reached 2,717 ft AMSL, before it once again commenced descending. At about this time, the crew returned to the ‘smoke in aircraft’ QRH checklist to complete the remaining items, but before these could be completed, the left wing overheat light illuminated continuously (see the section titled Quick reference handbook). The crew then actioned the relevant memory items of the ‘wheel well and wing overheat’ QRH checklist, including switching off the left bleed air system. Soon after switching off the bleed air, the crew noted that the smoke ceased. The checklist also required the crew to extend the main landing gear. As the aircraft was descending at a speed of over 220 kt (in excess of the 175 kt maximum landing gear extension speed), and wanting to expedite the return, the crew decided not to extend the landing gear at that time.
The aircraft continued descending and at 0758:23 reached 2,161 ft AMSL (about 1,200 ft AGL) before recommencing a climb. The air traffic controller observed the aircraft descend below the minimum safe altitude and, shortly after, a second CLAM alert was generated. The controller did not advise the crew of the low altitude as they believed the crew were unable to maintain altitude and that contacting them would only increase their workload.
At the same time, the crew commenced a right turn to intercept the ILS localiser and 12 seconds later, while still wearing the oxygen masks, the crew contacted the controller to request airport emergency services. The controller did not comprehend the broadcast and asked the crew to repeat the request. The crew repeated the request, but the controller again could not understand it. The controller did not query the crew further and commenced coordinating the handover of the aircraft to the Perth Tower controller. During this period, the left wing overheat light extinguished.
At 0758:41, the aircraft crossed the ILS localiser while climbing above about 2,800 ft AMSL. The climb and right turn continued until the aircraft levelled at about 3,000 ft AMSL for 7 seconds before recommencing a descent. The aircraft descended to 2,751 ft AMSL, before again climbing. The right turn continued for a further short period, followed by the aircraft commencing an intercept of the localiser from the left side. The aircraft climbed for a final time to 2,947 ft AMSL before again commencing a descent and levelling at 2,800 ft AMSL about 10 seconds later. The aircraft then maintained 2,800 ft AMSL until intercepting the localiser at 0800.
The crew completed the ILS approach and landed without further incident. The aircraft was not damaged, and there were no crew or passenger injuries.
Context
Crew details
The captain held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The captain commenced flying with Skippers Aviation as a first officer in May 2022 before progressing to captain in April 2024 and had 1,484 hours of flying experience, of which 1,270 hours were accrued in the Metroliner.
The first officer held a commercial pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer commenced flying with Skippers Aviation in April 2024 and had 509 hours of flying experience, of which 247 hours were obtained in the Metroliner.
The ATSB found no indicators that the flight crewmembers were experiencing a level of fatigue known to affect performance.
Aircraft details
The Fairchild SA227-DC Metroliner 23 is a twin-engine turboprop regional airliner and an enhanced version of the Metroliner series that initially entered service in 1972. The aircraft was fitted with an analogue cockpit and was not equipped with an autopilot or flight director. VH-WBQ (Figure 4) was configured with 2 crew seats and 19 passenger seats.
Figure 4: VH-WBQ
Source: Lloyd Cartwright
Crew oxygen system
The aircraft was fitted with oxygen masks for use by the flight crew during a smoke event. After donning the masks, the following steps were to be followed to establish communications between the crew members and when using the aircraft radios:
select the microphone switch at the rear of the cockpit side panel from ‘boom’ to ‘mask’
deselect the cockpit button on the audio panel
to communicate with the other flight crew member, use the intercom push-to-talk button on the front side of the control column
to transmit using the radio use the push-to-talk button on the reverse side of the control column as normal.
If these steps were not fully followed, breathing noises would be heard through the crew’s headsets that could distract from, and disrupt, normal communications.
Air conditioning system
The aircraft was fitted with 2 identical air conditioning systems, one associated with each engine, and feeding conditioned air to the associated side of the flight deck and cabin. Each air conditioning system was supplied with hot, high pressure bleed air from the engine compressor through a shut‑off valve to the air cycle machine. The air cycle machine used ambient air to cool the bleed air and incorporated a mixing valve (for cabin temperature control).
An engineering evaluation of the left engine air cycle machine, conducted after the flight, found that it had overheated and that the cooling turbine was expelling oil. The hot air mixing valve was also found to be operating intermittently and sticking in various positions.
Quick reference handbook
The operator’s Metroliner 23 Flight Operations Manual included quick reference handbook (QRH) checklists with memory items specified within red brackets. This manual provided the following guidance for usage:
In a situation where the PM has had to reference the QRH to cross check correct memory item completion they will then announce to the PF that he/she is “Standing by with the ……..checklist”…Both pilots will then silently carry out the circuit breaker check at this point after which the PF then commands “Continue” when he/she is ready, and the checklist is read from the beginning.
The checklist must be announced by title and checklist notes must be read before proceeding with the checklist. A checklist is not completed until stating, “…. checklist complete”.
QRH items shall be read and actioned (any memory items will just be checked for completion) by the PM (where practical). A self-challenge and response technique is required.
Most of the PF attention should be directed at flying the aircraft; however, he must also be kept informed with the management process of accomplishing the appropriate procedures/checklist.
It would be appropriate for the PM to delay reading of the checklist procedure until the PF is in a position to monitor and assist if required. Confusion is often a problem area when conducting QRH procedures. Checklist procedures must not be rushed. It is important crews conduct checklists in a careful and controlled manner.
To stop smoke ingress into the aircraft from a bleed air source such as the air conditioning system, the ‘smoke in aircraft’ checklist required the crew to select the affected bleed air system ‘off’ (Figure 5).
Figure 5: Smoke in aircraft QRH checklist
Source: Operator, annotated by the ATSB
The wing overheat annunciator illuminated with either a steady or flashing indication. A steady light indicated a brake fire, wheel well or air conditioning duct overheat condition. A flashing light indicated a wing leading edge bleed air line failure or an overheated generator wire. The QRH checklist for a steady indication (Figure 6) required the crew to extend the landing gear to reduce the risk of a brake or tyre fire, overheat condition or a tyre explosion.
Figure 6: Wheel well and wing overheat, steady light QRH checklist
Source: Operator
Smoke and fumes exposure
The United States Federal Aviation Administration pilot safety brochure Smoke toxicity highlighted that smoke inhalation should be recognised as a very real danger. It also stated that ‘smoke gas levels do not need to be lethal to seriously impair a pilot’s performance’.
ATSB research report AR-2013-213 Analysis of fumes and smoke events in Australian aviation from 2008 to 2012: A joint initiative of Australian aviation safety agencies found that over 1,000 fumes/smoke events were reported to the ATSB and the Civil Aviation Safety Authority in the period from 2008–2012. The report highlighted that fumes associated with these events may have the potential to pose a health risk through eye/skin irritation, difficulty in breathing, incapacitation or illness. This was especially the case if the fumes were associated with particulates (smoke) or fire. However, while occurrences involving smoke were more likely to result in an outcome than a fumes‑only event, the research also found that ‘very few led to a serious consequential event (such as a forced landing) or outcome such as fire or crew incapacitation’.
Air traffic control safety alert
The air traffic control manual of air traffic services provided the following guidance for issuing a safety alert:
Unless the pilot has advised that action is being taken to resolve the situation or that the other aircraft is in sight, issue a safety alert prefixed by the phrase 'SAFETY ALERT' when you become aware that an aircraft is in a situation that places it in unsafe proximity to:
a) terrain;
b) obstruction;
c) active Prohibited/Restricted/Military Operating Areas; or
d) other aircraft.
As the crew prepared the aircraft for the return to Perth, it descended below the 2,800 ft altitude assigned by the air traffic controller. The controller identified the aircraft descending below the assigned altitude and contacted the crew stating, ‘maintain 2,800, 2,800 lowest safe’, but the broadcast was not prefixed by the required statement ‘safety alert’.
Meteorology
From soon after take-off until after the aircraft was established on the ILS approach, the flight was conducted in instrument meteorological conditions.[5]
At 0800, the Bureau of Meteorology (BoM) automatic weather station at Perth Airport recorded the wind as 5 kt from 222° magnetic. Cloud cover was recorded as few[6] at 1,267 ft above mean sea level (AMSL), scattered at 1,867 ft AMSL and broken at 3,067 ft AMSL. Visibility was recorded as 9,000 m in light rain showers.
Recorded data
Airservices Australia provided recorded air traffic control audio and surveillance data.
During maintenance actions following the occurrence, the aircraft electrical system was powered‑up and the cockpit voice recording of the incident flight was overwritten.
Flight data recorded by the aircraft’s flight data recorder, combined with recorded surveillance and audio data is presented in Figure 7.
Figure 7: Recorded flight data from 0756 to 0800
Source: ATSB
Safety analysis
Air conditioning pack failure and checklist error
The unusually high temperature noted by the first officer during the taxi to the runway, combined with the findings of the post‑event engineering examination, indicated that the left air cycle machine (ACM) failed prior to departure. This failure resulted in oil being expelled from the ACM cooling turbine and unconditioned hot bleed air entering the air conditioning system. This in turn resulted in the temperature control difficulties faced by the crew and, after take-off, smoke being emitted from the left side flight deck and cabin vents.
In response to the smoke, the crew actioned the memory items of the ‘smoke in aircraft’ checklist. This included donning oxygen masks however the first officer had difficulty in fitting the mask and establishing communications with the mask in use. As a result, the first officer elected not to wear the mask. This exposed the first officer to potentially harmful smoke and fumes. While the first officer reported no adverse effects from this exposure, it did increase the risk of impairment and incapacitation.
After completing the checklist memory items, the crew were required to action the complete ‘smoke in aircraft’ quick reference handbook (QRH) checklist to ensure all required actions had been completed. However, before completing the checklist, the crew commenced the actions required to return to Perth as they assessed that task was of higher priority. Had the QRH checklist been subsequently fully completed, the left bleed air would have been selected ‘off’ and this would have stopped the smoke ingress into the cabin. This action would also have likely prevented the later overheating of the air conditioning duct that triggered the ‘wheel well and wing overheat’ annunciation.
Workload and unsafe descents
The aircraft was equipped with analogue instrumentation with no flight automation to reduce flight crew workload and the smoke was detected immediately after take-off while the aircraft was operating in instrument flight conditions. These factors combined to create a high workload period for the relatively inexperienced crew.
Workload has been defined as ‘reflecting the interaction between a specific individual and the demands imposed by a particular task. Workload represents the cost incurred by the human operator in achieving a particular level of performance’ (Orlady and Orlady, 1999). A discussion of the effect of workload on the completion of a task requires an understanding of an individual’s strategies for managing tasks.
An individual has a finite set of mental resources they can assign to a set of tasks (for example, performing a take-off). These resources can change given the individual’s experience and training and the level of stress and fatigue being experienced at the time. An individual will seek to perform at an optimum workload by balancing the demands of their tasks. When workload is low, the individual will seek to take on tasks. When workload becomes excessive the individual must, as a result of their finite mental resources, shed tasks.
An individual can shed tasks in an efficient manner by eliminating performance on low priority tasks. Alternately, they can shed tasks in an inefficient fashion by abandoning tasks that should be performed. Tasks make demands on an individual’s resources through the mental and physical requirements of the task, temporal demands and the wish to achieve performance goals (Hart and Staveland, 1988, and Lee and Liu, 2003).
Examples of errors associated with excessive workload include:[7]
Flight crew may mishear, misunderstand or miss setting an air traffic control clearance provided during a period of high workload, leading to:
A deviation from assigned altitude (level bust)
controlled flight into terrain (CFIT)
loss of separation from other aircraft, or
an unstabilised approach.
The pilot becoming distracted from primary tasks resulting in an error in handling or managing the aircraft.
In response to the smoke and due to the high workload, the crew initially omitted or missed required checklist items (donning the oxygen mask and completing the ‘smoke in aircraft’ checklist). Had the checklist been completed with the left bleed air selected ‘off’ and the oxygen mask fitted, with communications correctly established, the additional workload associated with returning the aircraft to Perth would have been reduced. Furthermore, the increased distraction and workload associated with the response to the subsequent wing overheat annunciation would have been avoided.
Later, when the crew returned to complete the ‘smoke in aircraft’ checklist, they were interrupted by the wing overheat annunciator illuminating. The required response actions further compounded their workload and this likely influenced the decision error to leave the landing gear retracted. While the crew elected not to extend the gear due to their desire to expedite the return, the decision was not fully considered and would have exposed the aircraft to increased risk if the overheat condition had been associated with the landing gear.
The significant workload that the crew were subject to also adversely affected the crew’s management of the aircraft’s flight path. Without automation to reduce workload and support flightpath management, the aircraft deviated above and critically, twice considerably below the assigned and lowest safe altitude. The aircraft also passed through, and then deviated significantly left of, the localiser before the crew recovered and completed the approach.
Air traffic control factors
The clearance to descend to 2,800 ft was incorrectly readback as 2,000 ft by the first officer (who was not wearing the oxygen mask at that time), but this error was not identified by the air traffic controller. The purpose of a clearance readback is to ensure that the clearance has been correctly received and provides the controller an opportunity to correct any errors. As this error was not identified, there was increased risk of the crew descending the aircraft below the minimum safe altitude while still operating in instrument meteorological conditions. However, despite reading back the clearance incorrectly, the crew initially levelled the aircraft at 2,800 ft before querying and confirming the assigned altitude as 2,800 ft. Therefore, the non-identification of the readback error did not contribute to the aircraft descending below the lowest safe altitude.
Despite obtaining confirmation of the assigned altitude, very soon after, the aircraft began descending. The controller identified the aircraft descending below the assigned altitude and contacted the crew, advising them to maintain 2,800 ft as that was the lowest safe altitude. However, this broadcast was not prefixed by the required statement ‘safety alert’. Commencing such a broadcast with the phraseology ‘safety alert’ is designed to alert crews to safety critical information to ensure a response is prioritised and is particularly important during times of high crew workload. Despite the correct phraseology not being used, the broadcast achieved the desired crew response. The recorded data showed that immediately after the controller contacted the crew, the descent was stopped, and the aircraft commenced climbing. As such, the absence of a safety alert did not contribute to the occurrence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the smoke in the aircraft and descent below lowest safe altitude involving Fairchild Industries SA227-DC, VH-WBQ, 25 km north-east of Perth Airport, Western Australia on 15 August 2024.
Contributing factors
A failure within the left air cycle machine resulted in hot engine bleed air and smoke entering the cabin soon after take-off. In response, the crew elected to return to Perth.
After commencing the ‘smoke in aircraft’ checklist memory items, the quick reference handbook checklist was not completed, and the left engine bleed air system was not selected off. As a result, during the return, the left air conditioning duct overheated, and the wing overheat light illuminated.
The workload associated with the in-flight response to the smoke in the aircraft and wing overheat indication adversely affected the flight crew's performance, leading to errors in flight path adherence, checklist completion and decision‑making.
On several occasions during the return to Perth Airport, the aircraft deviated above and below the assigned and lowest safe altitude. These deviations included a descent to 639 ft below the lowest safe altitude.
Other factors that increased risk
Following the smoke entering the cabin, the first officer initially elected not to wear the oxygen mask due to difficulties in donning the mask and then establishing communications. This increased their risk of impairment or incapacitation.
An incorrect altitude readback from the flight crew was not identified or corrected by air traffic control. Later, after the assigned altitude had been communicated, when the aircraft first descended below the lowest safe altitude, the crew were advised of the deviation by air traffic control, but the required ‘safety alert’ was not issued.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action taken by Skippers Aviation
Line oriented flight training
Action number:
AO-2024-048-PSA-01
Action organisation:
Skippers Aviation
In response to this incident, Skippers Aviation:
revised the Line Oriented Flight Training (LOFT) program to include more comprehensive oxygen system training
conducted the following refresher training for Metroliner 23 flight crew:
emergency response briefings
theory examination for the Metroliner 23 bleed air, pneumatics, pressurisation and fire warning systems.
practical training of the crew oxygen system
revised emergency procedures
updated the aircrew initial and recurrent training to include a presentation on the Metroliner 23 oxygen system.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the flight crew
the aircraft operator
Civil Aviation Safety Authority
Airservices Australia
recorded data from VH-WBQ.
References
Orlady, HW & Orlady, LM 1999, Human factors in multi-crew flight operations. Ashgate, Aldershot, p. 203.
Hart, SG & Staveland, LE 1988, ‘Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research’, In PA Hancock & N Meshkati (Eds.), Human Mental Workload. North Holland Press, Amsterdam.
Lee, YH & Liu, BS 2003, ‘Inflight workload assessment: Comparison of subjective and physiological measurements’, Aviation, Space, and Environmental Medicine, vol.74, pp. 1078-1084
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
the flight crew
the air traffic controller
Airservices Australia
Civil Aviation Safety Authority.
A submission was received from Airservices Australia. The submission was reviewed and did not result in any amendment to the report.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2]Memory items are checklist items required to be committed to memory to allow an immediate response to high priority abnormal events.
[3]PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[5]Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under Instrument Flight Rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
[6]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, and ‘broken’ indicates that more than half to almost all the sky is covered.
A recent ATSB / OTSI investigation highlights risks associated with misunderstood functionality of automatic couplers. The correct operation and verification of the locking mechanism after coupling is essential in avoiding train separation events.
What happened
The Office of Transport Safety Investigations (OTSI) has completed an investigation into an accident, on behalf of the ATSB, where 3 locomotives located at the rear of a loaded grain train separated from the lead portion of the train in transit. Shortly afterwards, the lead portion of the train stopped and the 3 now detached locomotives at the rear collided with the stationary lead portion. This resulted in significant damage to the rear wagon and a locomotive.
What increased risk
Three locomotives were coupled to the rear of the loaded grain train for the purposes of banking[1] the train later in the journey. The couplers did not lock correctly and the train separated during transit when it changed from a compressive (bunched) to a stretched state. The investigation found that a positive stretch test was not performed prior to departure. Commonly, a stretch test is performed with a low traction power setting to ensure sufficient tensile pressure is placed on the coupler knuckles to confirm they have locked after coupling.
Safety advisory notice
RO-2022-001-SAN-01: Knowledge of the design features of automatic couplers, their differences and limitations, particularly with regards to locking mechanisms, is key to understanding the importance of conducting a positive stretch test at the conclusion of a coupling manoeuvre. The ATSB advises that rolling stock operators should ensure their operational staff are advised and assessed on coupler locking design features which assist in maintaining a knuckle in an unlocked state and methods required to ensure the knuckle has again locked after coupling has occurred.
Ensure understanding of coupler operation
Understanding the purpose of a procedure is important in assisting recall of critical steps.
In automatic couplers, after being lifted by the control (uncoupling) rod the locking block rests on a set shelf.[2] This allows the knuckle to unlock and remain unlocked during coupling / uncoupling operations, enabling operational staff to release the control rod and move clear of the rolling stock profile during shunting.
To allow the knuckle to re-lock it must first be opened to dislodge the locking block from the set shelf, effectively arming the locking block to automatically drop into place and lock the knuckle again once closed.
While top operated couplers provide a clear visual cue when the knuckle is unlocked, specifically, the lifter pin is significantly raised above the coupler assembly (Figure 1), the range of movement and vision of a lifter pin on a bottom operated coupler is markedly reduced (Figure 2).
Due to significant limitations in visual cues, a positive stretch test, particularly of bottom operated couplers, is essential for verifying that the knuckle is locked at the conclusion of a coupling manoeuvre.
The ATSB continues to acknowledge and support World Helicopter Day to help raise awareness of the valuable contributions helicopters make to society, and as an opportunity to share information to influence safety.
On this World Helicopter Day – as a pilot or an operator – have you the required knowledge and skills in place to manage the risk of an inadvertent entry into IMC?
Since the release of our final report into the fatal VFR into IMC, loss of control and collision with terrain accident involving an EC130 T2 near Mount Disappointment, Victoria in March 2022 we have been advocating for all VFR-rated helicopter pilots, particularly those undertaking Part 133 passenger carrying operations, to develop the knowledge and skills required to manage the risk of inadvertent entry into IMC.
While avoidance of IMC is important, it is not always assured. And to help mitigate against inadvertent entry into IMC, there are several available risk controls for VFR pilots to strongly consider.
Before flight, decision-making in marginal weather conditions can be supported with the use of a pre-flight risk assessment tool. And to increase the chances of safely recovering from an inadvertent entry, we highly encourage VFR pilots undertake recovery training and basic instrument flying competency checks during their operator proficiency checks or during other training.
At an organisational level, the risk of helicopter inadvertent IMC should be considered within the context of a company’s operations. The effective management of this risk relies on multiple layers of controls to reduce the risk of single point-of-failure accidents. This includes training and procedures for both avoidance and recovery, which can be enhanced with equipment, such as autopilots to reduce the risk of loss of control, and terrain awareness and warning systems to reduce the risk of controlled flight into terrain.
The ATSB continues to monitor the intended safety action by CASA in response to our safety recommendation to further address the risk of inadvertent IMC events in Part 133 helicopter passenger operations.
On 2 August 2024, a Leonardo Helicopters AW139, registered VH‑EXK, departed Longford Heliport, Victoria, for a hoist training exercise conducted under visual flight rules near Golden Beach, Victoria. During the training, the crew faced difficulties retrieving a waterborne training aid, but due to encroaching fog the instructor (Pilot Flying) elected to depart for Longford. They initiated a climb with the aid of the radar height hold function before ensuring the helicopter was correctly configured for departure. The helicopter then inadvertently entered instrument meteorological conditions (IMC) and the altitude and airspeed began to fluctuate. The enhanced ground proximity warning system then triggered as a result of increased airspeed and the helicopter’s flight path descending below 150 ft above sea level. The captain (Pilot Monitoring) took control and initiated a climb, allowing for a safe return to Longford Heliport without further incident.
What the ATSB found
Due to encountering fog the instructor conducted a hastened departure from the training area before securing the hoist, the cabin door and occupants. At the time, the captain, who was acting as pilot monitoring, was still occupied with recording the training aid position. During the initial climb, the helicopter inadvertently entered the encroaching fog, and the instructor, who was the pilot flying, lost visual references and became spatially disoriented.
The disoriented instructor attempted to exit instrument meteorological conditions but applied control inputs that resulted in the helicopter entering an unstable state. This triggered a terrain alert, and airspeed exceedances with the main rotor RPM at 102% and operations with the door open and the hoist extended.
Following the terrain warning, the captain took control of the helicopter prior to gaining situational awareness or conducting an appropriate control handover, increasing the risk of control conflict between the 2 crew members. Additionally, the operator had no defined procedures for inadvertent instrument meteorological conditions recovery during hoist operations or for responding to enhanced ground proximity warning system alerts and advisories.
Despite not gaining situational awareness and bypassing handover protocols, the captain’s control inputs immediately arrested vertical descent and initiated a climb, reducing the risk of collision with terrain.
What has been done as a result
Following this incident, Esso Australia conducted an internal investigation and has identified several actions to be taken.
A standardised procedure has been developed to ensure a controlled entry into instrument meteorological conditions from a low hover, including scenarios where aircrew may be connected to the hoist beneath the aircraft.
Flight crews will undergo further training during low-level operations in the helicopter and simulator to reinforce techniques for handling degraded visual environments.
Briefings for search and rescue and hoisting training operations will emphasise the importance of maintaining a safe distance from visibility-reducing conditions.
Crew resource management courses will also be updated to focus on upset training scenarios and flight crew responses.
Safety message
The ATSB encourages pilots to take proactive measures to manage the risks associated with inadvertent entry into instrument meteorological conditions. Loss of visual references can lead to spatial disorientation, reduced situational awareness and loss of control, particularly for pilots operating under visual flight rules. Pilots rated for instrument flight rules should prioritise the use of rehearsed recovery procedures, referencing flight instruments to safely regain visual meteorological conditions.
This incident shows the importance of establishing and monitoring operational safety margins, adherence to documented procedures, maintaining situational awareness and fostering effective crew resource management during high-workload scenarios like hoisting and search and rescue operations. The challenges presented by degraded visual environments, such as inadvertent entry to instrument meteorological conditions, increase the likelihood of spatial disorientation and loss of control in flight.
These proactive steps can significantly enhance safety and improve outcomes during low‑level operations in demanding conditions.
The occurrence
On 2 August 2024, a Leonardo Helicopters AW139, registered VH-EXK and operated by Esso Australia, departed Longford Heliport, Victoria at 0816 local time for a hoisting training exercise. The crew consisted of the captain, a flight instructor, a check aircrewman, and a hoist operator. The captain was initially the pilot flying (PF)[1] and was under the supervision of the instructor who was acting as pilot monitoring (PM).[2] The hoisting exercise took place near Golden Beach, Victoria (Figure 1) and was conducted under visual flight rules (VFR).[3] The crew crossed the coastline at 0821 and selected a training area approximately 2 km offshore. The exercise involved retrieving a training aid amidst large swells, sea spray and encroaching fog from the north-west. The training aid was deployed, and the exercise commenced at about 0825.
Figure 1: EXK track and key locations
Source: Google Earth, annotated by the ATSB
As the training progressed, the helicopter's proximity to the fog on the left side, where the instructor was seated, was observed to be decreasing. The flight crew noted that the skies were clear to the north and northeast of their position on the instructor’s side of the helicopter.
After conducting training for approximately 40 minutes, the instructor assumed control as PF and the check aircrewman assumed the role of hoist operator to retrieve the training aid. This involved hovering in a stationary position approximately 40 ft above the water's surface to retrieve a training aid, which was a wooden cross with ropes attached, designed to simulate a search and rescue scenario.
However, the attempt was unsuccessful, and due to the encroaching fog, the instructor immediately elected to depart and announced they would climb to avoid fog.
At 0908, the instructor manoeuvred the helicopter onto a north-westerly heading (Figure 2) and engaged the radar height hold (RHT) system while climbing using a combination of the collective[4] beep trim and force trim release (FTR).[5] At this time, the captain, acting as the PM, was focused on marking the GPS position of the training aid. This facilitated its retrieval in a subsequent training exercise later that day, as the large swells and fog disrupted the current exercise. During the departure climb, the right cabin door was open and approximately 40 ft of the hoist cable was extended.
Figure 2: EXK flight track and enhanced ground proximity warning system alert
Source: Google Earth, annotated by the ATSB
At about this time, the helicopter inadvertently entered instrument meteorological conditions (IMC),[6] and the instructor announced their intention to move forward to depart. The check aircrewman objected via the intercom to departing with the hoist still extended, as the post‑hoist procedures requiring the aircrew to secure the hoist cable and cabin had not yet been completed. Despite their objection, the instructor proceeded with the departure to regain visual meteorological conditions (VMC).
The instructor accelerated and continued to climb, reaching an altitude of 185 ft and an airspeed of 72 kt before beginning a shallow descent. The instructor who was PF noticed the increasing airspeed but took no actions to arrest this trend. As the helicopter continued accelerating, the captain observed on the primary flight display (PFD) a nose-down attitude and airspeed increasing through 80 kt, which exceeded the operational speed for the hoist operation. The captain announced ‘80 kt’ to draw the attention of the instructor to the increasing airspeed. The airspeed continued to increase above 90 kt, which resulted in an airspeed exceedance with the RPM (NR) at 102%, despite the captain’s attempt to set the RPM switch[7] to 100% to avoid this exceedance. As the helicopter accelerated through 100 kt it exceeded the maximum airspeed for the right main cabin door in the open and locked position.
At 0909, the helicopter had descended to 147 ft above sea level with an airspeed of 101 kt, triggering caution and warning alerts from the enhanced ground proximity warning system (EGPWS). In the 10-second period preceding the EGPWS warning, the collective FTR was active for 5 seconds while it was engaged and disengaged 3 times. The instructor recalled climbing and using the collective beep trim and collective FTR. However, they did not recall engaging the collective FTR after the negative vertical speed developed. The captain later noted that the collective FTR could be activated instinctively while manipulating the collective due to the switch's position, requiring discipline to avoid unintentional activation.
Responding to the increasing speed and ground proximity alert on the PFD, the captain reactively assumed control, reduced the helicopter’s speed, and initiated a climb by pulling back on the cyclic.[8] The check aircrewman suggested cutting the hoist cable for safety and indicated that the cable was trailing behind the aircraft. This was not actioned after consultation with the instructor, who stated they were satisfied that the cable did not pose a danger, and they lacked visual reference to the ground. The instructor decided not to cut the cable because they were unsure of what was underneath the helicopter at the time.
During the recovery, the captain climbed on a north‑westerly heading and reduced the helicopter’s airspeed and the instructor resumed control after a brief exchange with the captain. The flight crew regained VMC shortly after the recovery was initiated, recovered the cable and the helicopter was flown in an easterly direction away from the shoreline. The crew configured the helicopter for departure from the training area and returned to Longford Heliport. The helicopter landed without further incident at 0936 local time.
Context
Pilot information
Instructor
The instructor held an Airline Transport Pilot Licence (helicopter) with an instrument rating and a Class 1 aviation medical certificate. They had 11,129 flight hours, including 3,695 hours on the AW139, they had also logged 114 hours on the AW139 in the last 90 days. They were approved for training and checking duties with the operator, Esso Australia, including hoisting operational proficiency checks.
The instructor reported sleeping 7 hours the night before the occurrence. They were awake for 4 hours and were on duty for 2 and a half hours at the time of the occurrence, they stated they felt ‘alert but not at peak performance’.
Captain
The captain held an Airline Transport Pilot Licence (helicopter) with an instrument rating and a Class 1 aviation medical certificate. They had 15,402 flight hours, including 2,603 hours on the AW139 and had logged 81.9 hours on the AW139 in the last 90 days. They were approved as a line supervisory pilot with the operator.
The captain reported sleeping 7 and a half hours the night before the occurrence. They were awake for 4 hours and were on duty for 2 and a half hours at the time of the occurrence. They reported feeling ‘somewhat fresh’.
Helicopter information
The Leonardo Helicopters AW139, serial number 31886, was registered as VH-EXK in Australia to the operator, Esso Australia, on 8 January 2020. The helicopter was certified for day and night VFR, IFR,[9] offshore/elevated helideck[10] operations, and external load[11] operations.
Powerplant
The AW139 is equipped with two Pratt & Whitney PT6C‑67C engines. The main rotor power can be set to 100% or 102% using the RPM selector switch (Figure 3) on the pilot’s (right seat) collective grip.
For Category A[12] operations below 80 kt, rotor RPM (NR) is set to 102%, enabling optimal performance in the event of an engine failure, allowing for either continued safe flight or a controlled landing. Real‑time rotor RPM is monitored on the multi‑function display with the maximum airspeed set to 90 kt at 102% NR to protect the rotor system from excessive stress.
Crew alerting system (CAS) messages are not triggered during RPM adjustments, allowing for changes without distracting alerts.
Figure 3: Pilot RPM selector switch
Source: Leonardo Helicopter file photo, annotated by the ATSB
Autopilot and radar height hold
The AW139 is fitted with a 4‑axis autopilot system coupled with a 3‑cue flight director (FD), which controls the helicopter’s pitch, roll, yaw, and vertical axis. The radar height hold (RHT) mode maintains the helicopter at the radar height at the time of engagement. The RHT reference height is presented on a magenta bug (Figure 4) on the radar altimeter tape with a digital readout.
The helicopter flight manual stated that during hoist operations, that pilots should consider the effect of the use of the RHT function in flight and to monitor the helicopter performance closely when used.
Figure 4: RHT reference height
Source: Operator, annotated by the ATSB
The RHT reference height is adjustable using the following methods:
Collective force trim release (FTR): the ‘push and hold’ collective lever trim release button (Figure 5 left insert) is depressed to disengage the spring feel mechanism which enables the collective to be moved freely. When the button is released, the spring feel[13] is reset to zero force and the reference height is reset.
Collective beep trim switch: crews make incremental height adjustments using the collective beep trim switch, moving it aft to increase height and forward to decrease it (Figure 5 right insert). Adjustments occur at a rate of ±50 ft/second down or up, with audio tones (beep) signalling changes.
While RHT is designed to assist in stable altitude hold, crews are required to actively monitor and control the flight path.
Source: Leonardo Helicopters file photos, annotated by the ATSB
Cabin doors and hoist system
The sliding cabin doors fitted to VH‑EXK allowed for in‑flight hoisting operations, with speed limitations in place to prevent damage from slipstream pressure. The door could be locked open during hoist use. The operator required that the airspeed not exceed 80 kt when opening or closing the cabin sliding door and 100 kt when the door was locked open. The helicopter’s hoist system, located on the right side of the cabin, was equipped with an electric hoist motor, winch, and safety features including the primary quick release system, accessible to both flight crew and the hoist operator.
Enhanced ground proximity warning system
The helicopter was equipped with a Honeywell MK XXII‑30 enhanced ground proximity warning system (EGPWS), which displays terrain and obstacles. It is designed to provide alerts about nearby terrain or obstacles approximately 30 seconds ahead of the aircraft, giving warning of potential conflicts.
The functionality of the terrain awareness display and the ‘look ahead’ alerting and warning function was detailed in the AW139 rotor flight manual as:
This function uses information from the GPS and other sources on the aircraft to calculate horizontal position and vertical altitude. This data provides a three-dimensional position for the aircraft. This position is then compared to the terrain database and if a conflict with terrain or a known obstacle is imminent the system provides an alert.
Offshore mode
The EGPWS system fitted to the operator’s AW139 fleet included a dedicated offshore mode, which could be activated by the flight crew. Offshore mode is recommended for operations over water, as it adjusts terrain awareness boundaries to minimise nuisance alerts. This mode inhibits certain alerts and warnings in specific flight conditions. However, offshore mode is unsuitable for conventional IFR procedures, as it modifies terrain alerting parameters essential for standard instrument approaches and departures.
Operator information
Esso Australia operated from its headquarters in Longford, Victoria, supporting gas platform operations in Bass Strait. On 11 June 2024, the operator was issued with an air operator’s certificate (AOC), authorising Australian air transport operations and a Part 138 aerial work certificate, authorising aerial work operations.
Esso Australia operated a single helicopter type, the Leonardo AW139 helicopter, primarily for passenger transport, cargo transport and specialist aerial work operations, including external load and dispensing tasks. Its personnel were authorised to conduct both VFR and IFR flights.
Meteorological information
On the morning of 2 August 2024, the flight crew stated they conducted a weather briefing at the Esso Australia heliport base in Longford, Victoria. They recalled the presence of fog which delayed the departure by about an hour. While the crew prepared for departure, they received a report from another Esso Australia helicopter crew that the fog had sufficiently dissipated in the aera. Following a routine job safety analysis (JSA)[14] and final weather review, the crew assessed that the remaining fog posed no significant concern and proceeded with the flight.
Graphical area forecast
The flight to the training area and back was within the graphical area forecast for Victoria (GAF VIC), covering subdivisions A and A1. For the duration of the flight, the forecast conditions indicated:
visibility greater than 10 km, with broken stratus clouds between 100 and 1,000 ft above mean sea level (AMSL) in A1.
isolated freezing fog over land, with scattered fog south‑east of Mangalore and Wangaratta airports, reducing visibility to as low as 300 m.
Terminal forecast and special weather report East Sale (YMES)
The terminal forecast for East Sale predicted calm winds from 320° at 3 kt, with visibility reduced to 200 m in freezing fog, early in the morning.
By 0930 local time, conditions were expected to improve to greater than 10 km visibility with light winds. A 30% chance of mist, reducing visibility to 1,000 m was also forecast between 0900 and 1000. A special report (SPECI) at 0800 recorded calm conditions, with freezing fog reducing visibility to 200 m with scattered clouds at 100 ft.
Figure 6: Weather reporting locations
Source: Google Earth, annotated by the ATSB
Inflight weather observations
After a routine departure, the crew recalled observing a bank of fog along the coastline as the helicopter approached the training area. The instructor estimated that the fog bank was less than one kilometre from shore at the time. As the exercise began the flight crew reported that the fog began to obscure the shoreline near Golden Beach. However, clear skies were visible to the north and north‑east, while a large easterly swell created rough sea conditions below.
During the exercise, the flight crew reported that the helicopter was manoeuvred closer to the fog, which was situated on the left side of the helicopter, where the instructor was seated.
Operator procedures
Hoisting
Hoisting operations require coordination between all crew members and adherence to procedures and safety protocols. The hoist system, equipped with a cable and hook, facilitates the controlled retrieval of individuals or equipment, sometimes in challenging environments, such as water or rugged terrain.
Esso Australia hoisting crew compliment
Esso Australia hoist operations required a minimum crew of two flight crew, a hoist operator, and a wireman, each with defined roles (Table 1).
Table 1: Crew member location and roles
Crew member
Location
Role
Captain
Right side pilot seat
Oversees all aspects of the flight, especially during rescue operations, and briefs all crew members prior to departure.
Copilot
Left side pilot seat
Manages flight planning, navigates, monitors radios and helicopter systems, and assists with hoist operations as necessary.
Hoist operator (HO)
Cabin
Prepares rescue equipment, conducts pre-hoist checks, ensures cabin security, operates the hoist, and guides the pilot during hoisting.
Wireman
Cabin
Assists the HO, manages personal safety, and is prepared to descend on the hoist cable if needed.
The flight crew reported that the instructor and check aircrewman acted as copilot and wireman during the occurrence.
Hoist patterns and limitations
When conducting hoist exercises, helicopters typically follow a structured racetrack pattern approach, initially at 60 kt about 200–500 ft above obstacles. After approaching the site, the crew hover at a height below 100 ft over the target area to facilitate a stable hoisting environment.
The AW139 rotorcraft flight manual outlined the following operational limitations for hoist operations:
maximum 80 kt maximum forward flight speed during hoist operations
maximum 80 kt for opening/closing cabin door or 100 kt when door is locked open
fly manually or attentively when RHT mode is engaged.
The flight data from the occurrence revealed that the helicopter exceeded airspeed limitations for hoisting and the main door in the locked open position (See section titled Recorded information).
Post hoist procedures
Following a hoisting task, the hoist operator (HO) would secure the cabin and equipment, complete a post‑hoist checklist with the pilot monitoring (PM) using the challenge and response methodology,[15] and confirm the completion of the checklist items. The PM then completes the post‑hoist checks with the HO using the same checklist methodology (Table 2).
Table 2: Post hoist procedure and checks
Procedure
Actions
Post-hoist procedure
HO stows the equipment and closes the right main cabin door
HO announces, ‘cabin secure, post-hoist checks’
at this point the PF can climb.
Post-hoist check
PF safely establishes helicopter in the climb out
PM powers off the hoist and confirms circuit breakers are out
HO announces, ‘post hoist checks complete, clear to rotate’
PM initiates after take-off check.
After take-off check
PM checks NR set to 100% >80 kt
PM checks landing gear up >200 ft.
The crew recalled that before they departed the exercise site, the post‑hoist procedures and checks had not been performed.
Automation use
The use of automation for day VFR offshore flights, was detailed in the operator’s exposition stated as follows:
The advanced avionics suite in the AW139 promotes a high level of safety and crew situational awareness when used correctly. When not used correctly or understood, the opposite can occur allowing dangerous deviations and loss of situational awareness to quickly manifest.
ESSO Australia policy is for the flight management systems, multi-function control display units and avionics to be operated at a level that provides optimum navigation, communication and traffic awareness to the crews without drawing too much attention ‘inside the cockpit’. At all times, it is the responsibility of the PF to maintain effective control of the helicopter and its flight path/situation.
Handover and takeover procedures
Handover procedures in the operator exposition detailed the protocols flight crews must follow when transferring control to another pilot. The relinquishing pilot is required to state, ‘handing over,’ and the receiving pilot confirm by stating ‘taking over’ while placing their hands and feet on the controls. The first pilot then removes their inputs, ensuring clear role delineation. Handover drills must incorporate an active flight director, with no alternative transfer methods allowed.
The flight crew recalled that there was no verbalisation of the transfer of control during the recovery following the EGPWS alert.
The handover procedure was intended to ensure clear communication and role clarity by requiring the relinquishing pilot to state, 'handing over,' with the flying pilot to respond 'taking over' while actively taking control. These structured procedures are critical for maintaining operational safety and minimising risks during complex or dynamic situations. Neither pilot recalled referencing any rehearsed procedures in response to the inadvertent entry to IMC during the recovery. Additionally, they did not recall specific training in the helicopter or the simulator for EGPWS recovery.
Enhanced ground proximity warning procedures
As part of the pre‑flight checks, flight crews were required to test the EGPWS to confirm the serviceability of the system. The operator exposition also required that flight crews must respond to EGPWS cautions and warnings in marginal weather.
Neither pilot recalled any prescribed operator procedures that were referenced during the recovery following the EGPWS warnings during the occurrence.
Offshore operations
Standard procedures required crew to activate offshore mode once established beyond the coastline and to deactivate once established onshore. This selection of the offshore mode is verified by the PM and PF using the ‘coast check’ contained in the AW139 normal checklist.
Both flight crew recalled that offshore mode was activated on the EGPWS for the duration of the hoisting exercise.
Operator training
The operator’s exposition described the training and checking policies and procedures, and the regulatory requirements of the applicable Civil Aviation Safety Regulations (CASR). The operator maintained a training and checking organisation authorised by an instrument issued by the Civil Aviation Safety Authority (CASA). This training was conducted by nominated personnel put forward by the operator.
Upon completion of induction training, crews were required to complete recurrent training which included an operational proficiency check (OPC) for each type of operation.
Crew hoisting training
Crew hoisting training was provided by the operator as part of the combined search and rescue (SAR)/hoisting OPC. Additionally, a standalone hoisting OPC was conducted at 6‑monthly intervals. While the check events alternated every 6 months, they remained valid for 12 months from the date of completion.
The hoisting OPC assessed theoretical and practical aspects of hoisting, encompassing all phases of flight, with technical and non‑technical skills being assessed by approved personnel.
The instructor and captain conducted their hoisting OPC on 4 December 2023 and 23 October 2023 respectively. The instructor also conducted the captain’s combined SAR/hoist OPC on 16 May 2024, which included the same hoisting elements of the training that took place during the occurrence.
Scenarios involving a recovery from the hover with a prescribed low‑level inadvertent instrument meteorological conditions (IIMC) operating procedure were not included in the biannual SAR/hoist syllabus at the time of the occurrence.
Recurrent simulator training
Esso Australia conducted emergency OPC check every 6 months, in accordance with CASR 61 requirements in an AW139 full flight simulator. The emergency OPC satisfies the requirements for the type rating and low-level flight reviews.
All sequences flown were in a reduced visual cueing environment to mimic weather conditions that are regularly encountered when conducting flight operations in the Bass Strait.
Flight crews would encounter a simulated technical failure in reducing visibility at ‘low‑level’ below 500 ft leading to IIMC. This scenario would lead to either a ditching, or recovery in IIMC. In the case of the latter, this scenario required the flight crew to recover to a safe altitude, which the instructor and captain completed as a crew pairing on 18 September 2023.
Flight crew also received briefings on the 4 ‘Cs’ (Control, Climb, Course and Communicate) IIMC recovery technique (International Helicopter Safety Team).
Scenarios involving a recovery from the hover in IIMC conditions with a prescribed operating low‑level IIMC procedure were not included in the biannual simulator training syllabus at the time of the occurrence.
Esso Australia crew resource management training
Esso Australia conducted annual crew resource management (CRM) training every 12 months, in accordance with CASR 119 and CASR 133 requirements. The training modules covered:
human performance and limitations
situational awareness
decision-making
teamwork and communication
threat and error management
workload management and automation.
EGPWS training
The operator training requirements required that crew completed training specific to the Honeywell MK XXII‑30 EGPWS system installed on its AW139 fleet. The EGPWS training was incorporated into the AW139 differences training, which all flight crew had to complete during their initial entry into the Esso Australia check and training system. This included both theoretical knowledge and practical exercises to ensure proficiency in managing system operations. The training covered:
general overview of the system
normal procedures including setup for flight operations, functionality, general actions during an alert, and a demonstration of the self-test
limitations of the system
emergency and malfunction procedures.
The operator stated that EGPWS training events in the simulator had ceased in 2021 due to inaccuracies of the simulator‑generated warnings and alerts. As a result, Esso Australia flight crew underwent technical refresher ground training, which included a module dedicated to EGPWS. The instructor and captain conducted their EGPWS refresher training on 19 September 2023.
Recorded information
The AW139 helicopter is equipped with a multipurpose flight data recorder (MPFDR). The MPFDR combines both a flight data recorder (FDR) and a cockpit voice recorder (CVR), capturing helicopter data and audio.
Personnel from Esso Australia secured a copy of the FDR data for analysis and provided a copy of that data to the ATSB. The files were downloaded and confirmed to have contained flight data recorded during the EGPWS occurrence on 19 August 2024 from the MPFDR fitted to AW139 VH‑EXK. Although FDR data was available, no CVR data was retrieved for this occurrence due to the helicopter operating multiple flights in the days following the occurrence.
The recorded flight data captured parameters such as altitude, airspeed, control inputs and the activation of systems such as the RHT, FTR and EGPWS alerts. This data enabled a detailed reconstruction of the flight, providing insights into the helicopter’s performance and crew actions leading up to the event.
Recorded data
Just prior to the EGPWS event, an airspeed exceedance was identified, with the NR at 102% when the airspeed was above 90 kt. This persisted for a period of 3 seconds and occurred 2 seconds prior to the activation of the EGPWS system.
The EGPWS event trigger was identified as a combination of the radar altitude reducing below 150 ft as the airspeed exceeded 100 kt. The minimum radar altitude reached was 140 ft.
The MPFDR data revealed multiple key events during the event (Table 3).
Key events
Table 3: VH-EXK flight data
Local time
Event
Radio Height feet AGL
Pitch
+/- °
Groundspeed
knots
Computed airspeed
knots
Vertical speed
+/- fpm
0908:08
Collective beep AFT active; collective FTR active
72
5.976
0
0
-32
0908:18
Groundspeed begins increasing collective beep AFT active collective FTR active
85
5.625
2
0
128
0908:38
Computed airspeed above 0, helicopter climbing
Collective FTR active; over the next ten second period, the collective FTR is active for 8 seconds
154
0.176
28
38.5
192
0908:50
Rad alt peak 185, airspeed increasing through 75 kt collective FTR active
185
-5.976
66
75.5
-64
0908:51
Collective trim engaged
negative vertical speed begins developing
183
-6.855
70
79.5
-128
0908:55
Collective trim disengaged NR exceedance - >90 kt at 102% for 3 second duration
173
-2.109
82
93.75
-224
0908:59
Collective trim engaged; negative vertical speed is reducing
153
-1.406
90
99.5
-224
0909:00
Collective FTR active; EGPWS alert is activated for one second, followed by the EGPWS warning for 5 seconds
147
-0.879
90
101.5
-64
0909:03
Collective FTR active; minimum altitude reached
140
10.019
88
99.5
832
0909:07
Collective FTR active; following this, the collective FTR is active for 41 seconds of the following 54 seconds, as the helicopter climbs through 680 ft.
215
13.007
76
89.75
2048
Source: Operator supplied flight data recorder, tabulated by the ATSB
The recorded pitch changes during 60 seconds of flight data, showing a pitch range of up to 19°, coupled with fluctuating airspeed above limitations and unstable vertical speed, demonstrate an unstable aircraft profile during departure.
Operator internal investigation
Following the occurrence, Esso Australia conducted an internal investigation, concluding that inadequate procedures and work standards were the primary factors contributing to the incident. The internal investigation identified the root cause as:
Deficiencies in procedures regarding Search and Rescue (SAR) Training in the vicinity of fog.
Related occurrences
The following 2 ATSB investigations highlight the risks of inadvertent IMC encounters at close proximity to the ground and demonstrate the importance of rehearsed recovery drills in these situations. In both instances, the flight crew were IFR rated, and the helicopters were also IFR equipped.
These occurrences emphasise the effects of spatial disorientation[16] due to powerful and misleading orientation sensations during times of reduced visual cues, which can affect any pilot, no matter what their level of experience.
On 21 October 2016, the crew of a BK 117‑C2 were returning to their home base from Crookwell, New South Wales, after carrying out an emergency medical service mission. The flight was conducted under night visual flight rules with the aid of a night vision imaging system.
Conditions were marginal and, on departure, the helicopter entered low cloud. The aircrew officer declared loss of visibility on take‑off. The pilot had poor visibility ahead yet could see well to the right. The pilot thought visibility would improve as they passed ground lighting that was reflecting in raindrops on the canopy.
The visibility did not improve, and the pilot slowed the aircraft to maintain visual meteorological conditions. The low‑speed manoeuvre resulted in an undesired aircraft state and an EGPWS warning activated. The pilot conducted an inadvertent IMC drill, restabilised control, and continued the flight before landing safely.
On 13 May 2018, the crew of a Leonardo Helicopters AW139 departed Darwin, Northern Territory, to search for an active emergency position‑indicating radio beacon. The crew flew under night visual flight rules with support of a night vision imaging system.
During an approach to a potential target, smoke from nearby bushfires affected visibility and the helicopter developed an uncommanded high rate of descent. The aircrew officer, in the rear of the helicopter, called ‘Climb! Climb! Climb!’, and the pilot regained control with a rehearsed recovery drill.
During the recovery procedure, the power demand exceeded airframe limitations. This exceedance went undetected, and the helicopter was flown on a second sortie that same evening.
Safety analysis
Introduction and background
After concluding hoist training exercises near Golden Beach, Victoria, a Leonardo Helicopters AW139, registered VH‑EXK and operated by Esso Australia, inadvertently entered instrument meteorological conditions (IMC), which resulted in an enhanced ground proximity warning system (EGPWS) alert.
This analysis will examine factors contributing to the occurrence, including:
crew decision‑making
the transition from visual meteorological conditions (VMC) to IMC
the effects of spatial disorientation
control inputs during the event
operator procedures
crew response to the EGPWS alert.
Departure
During the hoisting exercise, both flight crews observed clear skies on the captain’s side of the helicopter to the north and north‑east of their position. Meanwhile fog approached from the north‑west on the instructor’s side and the instructor elected to depart and announced their intention to climb. Climbing immediately in the vicinity of fog may not have been necessary, as manoeuvring to the north or north‑east would have increased the distance from the fog. However, as the helicopter climbed, it encountered fog and the instructor immediately elected to depart, attempting to climb above the fog while tracking north‑west toward the shoreline.
As the instructor departed the training area for Longford at the conclusion of the exercise, the helicopter remained in a hoisting configuration. This meant the hoist was extended approximately 40 ft below the helicopter, the main cabin door was locked open and the helicopter’s main rotor RPM was set to 102%.
After hoisting exercises, the post‑hoist procedure required the hoist operator (HO) to stow the hoist, secure the cabin and advise the pilot monitoring (PM) prior to climbing. The PM would assist the HO in completing the post‑hoist check, confirming the crew actioned the appropriate items. However, due to the encroaching fog, the instructor elected to climb, lost visual references and reactively began to accelerate and climb the helicopter before completing the post‑hoist check.
These procedures ensure the helicopter is properly configured for departure, including securing the cabin, stowing the hoist and adjusting the main rotor RPM to 100%, once the helicopter accelerates through 80 kt.
As the helicopter accelerated the check aircrewman voiced their concern about departing, likely due to the present configuration not being suitable for forward flight.
Completing the post‑hoist procedure before departing would have removed the risk associated with potential interference from the extended hoist cable and exceeding the flight envelope limitations with the helicopter in the hoisting configuration. Additionally, by completing these procedures in a stationary position, the captain could have more effectively monitored the flight path during departure.
At the time of departure, the captain, who was the PM, was focused on marking the GPS position of the training aid in the flight management system (FMS) to facilitate retrieval during the next exercise. While this task had operational value, it distracted the captain from monitoring the helicopter’s dynamic state and assisting the instructor with flight path management, navigation and maintaining situational awareness. However, the captain was unaware of the instructor’s intention to depart, likely due to the expectation that the completion of the post‑hoist procedure had not been completed as a prerequisite to climb away.
Contributing factor
The instructor hastily departed the training area, due to encountering fog, before the hoist was secured with the door open, and while the captain as pilot monitoring was still occupied recording the training aid position.
Spatial disorientation
The instructor departed the training area on a north‑westerly heading, toward the shoreline and the previously observed fog. The instructor achieved a relatively stable climb, albeit with a steadily increasing forward airspeed. The helicopter's altitude peaked at 185 ft at 72 kt; however, as the climb progressed, the helicopter inadvertently entered IMC, depriving the crew of external visual references.
Both flight crew recall being in VMC when the climb commenced with the instructor verbalising their intention to climb above the fog toward an area of VMC. According to the instructor the helicopter entered fog as the helicopter began to climb while the captain was looking down and didn’t observe the transition to IMC.
The flight data recorder (FDR) captured altitude and airspeed fluctuations, consistent with flight control inputs from the pilot flying being uncertain of the flight path, including a nose‑down attitude and airspeed increasing through 80 kt. Therefore, without visual cues, the instructor likely became subject to the effects of spatial disorientation. This condition significantly impairs a pilot's ability to accurately interpret attitude, altitude and airspeed.
Contributing factor
After inadvertently entering instrument meteorological conditions, the instructor (pilot flying) became spatially disorientated.
Operating in degrading visibility creates ambiguity, stalling decision‑making as flight crew face conflicting situational cues (Orasanu, Martin, & Davidson, 2001). Continued reliance on visual cues in these scenarios can draw attention away from critical instrument readings (Summerfield & Enger, 2009). Coupled with the inherent instability of medium‑sized helicopters, these cognitive tendencies further increase the risks associated with spatial disorientation in degraded visibility environments.
Unstable flight
Frequent engagement and disengagement of the collective force trim release (FTR) when the radar height hold (RHT) was active further destabilised the helicopter, causing altitude and airspeed fluctuations. The operator exposition highlighted the potential risks by stating that the incorrect use of the AW139's automation systems can lead to dangerous deviations and loss of situational awareness. Additionally, the AW139's rotorcraft flight manual (RFM) stated that the helicopter must be attentively flown during hoisting operations using the RHT function. The FTR switch demands disciplined use, as its unintentional instinctual engagement can lead to unintended control inputs. As a result, crews must carefully monitor their inputs and selections when using the RHT and FTR functions. Pilots tend to overestimate their ability to continue to control the aircraft when visual references are lost (Wiggins, Hunter, O'Hare, & Martinussen, 2012). During the periods of high crew workload, the interactions of these systems added to the difficulties in sustaining stability in the degraded visual environment.
The combination of spatial disorientation, intermittent collective FTR use, flight control inputs and an overall impaired situational awareness of the crew, culminated in the helicopter being still in the hoisting configuration, whilst descending below 150 ft above sea level and exceeding 100 kt.
This resulted in flight envelope exceedances of:
operation with the hoist cable extended
the right cabin door in the open position
operation with the main rotor RPM at 102%.
This posed additional risks, including potential aircraft damage as a result of the hoist cable interfering with the tail rotor, damage to the aircraft due to slipstream pressure on the door. The situation reached a critical point when the EGPWS issued a terrain alert, signalling the imminent risk of collision with terrain.
Contributing factor
The instructor's attempt to leave IMC, while being spatially disorientated, resulted in control inputs that led to the helicopter entering an unstable state while still in IMC, triggering a terrain alert below 150 ft, and airspeed exceedances for operations with the main rotor RPM at 102%, the door open and hoist extended.
Recovery
Immediately following the EGPWS alert, the captain took control of the helicopter without a formal handover from the instructor by reactively pulling back on the cyclic. Prior to assuming control, the captain was occupied with entering GPS coordinates into the flight management system (FMS), which diverted their attention from monitoring the helicopter's flight path. This meant they were not able to actively observe changes to the dynamic state of the helicopter and missed the early indications of loss of spatial orientation by the PF due to the degrading visibility.
Due to a lack of visual cues, the captain was unsure of their altitude and reactively pulled back on the cyclic to arrest the helicopter's forward momentum and gain altitude. After the helicopter was established in a climb and following a brief exchange, control of the helicopter was transferred back to the instructor.
The captain bypassed handover protocols, likely due to the receipt of the EGPWS warning and perceived rapidly escalating events. Operator procedures also mandate that flight crews respond promptly to EGPWS warnings.
Reactive assumption of control by the non‑flying pilot had the potential to introduce further distractions, conflicting control inputs or further inappropriate control inputs in an already dynamic and demanding environment. Although the captain bypassed standard handover procedures, the absence of a structured handover also highlights the difficulties of managing dynamic situations under pressure and balancing conflicting demands.
Other factor that increased risk
Prior to gaining situational awareness and without an appropriate control handover, the captain reactively assumed control of the helicopter after the terrain warning, increasing the risk of control conflict between the 2 crew.
Operator procedures
Esso Australia did not provide crew with structured procedures for managing inadvertent entry into IMC and EGPWS alerts during hoist operations. Although the Esso Australia exposition required a pilot response to EGPWS alerts, this did not include specific guidance for managing such alerts. While training covered general EGPWS functionality, it did not include scenario‑based drills for complex situations involving degraded visibility or low-level operations.
Consequently, responses to alerts were reactive, with the crew relying on instinct rather than following a predefined recovery procedure. The absence of predefined inadvertent IMC‑specific recovery actions also exposed the crew to the cognitive effects and demands of operating in degraded visual environments.
The related occurrences further demonstrate the effectiveness of structured recovery protocols and crew resource management (CRM) in stabilising helicopters during degraded visual conditions. The absence of similar predefined procedures that the crew could have utilised, underscores the need for enhanced training and clear protocols to manage scenarios involving inadvertent IMC and EGPWS alerts.
Other factor that increased risk
Esso Australia did not have a procedure for a helicopter recovery from inadvertent IMC during hoist operations or recovery procedures for EGPWS alerts or advisories. (Safety issue)
Captain’s decision‑making
In a matter of seconds following the initial EGPWS caution, the captain arrested the rate of descent and transitioned into a climb while reducing the forward airspeed of the helicopter. The captain’s intervention immediately reduced the risk of a collision with terrain.
Before assuming control, the captain was able to identify and vocalise the increasing airspeed in an attempt to illicit corrective action from the instructor. A progressive intervention strategy is initiated by communicating a flightpath deviation (alert), then suggesting a course of action (advocacy and assertion) and then directly intervening, if necessary (Civil Aviation Safety Authority 2020). Despite bypassing Esso Australia handover protocols, the captain effectively recognised and responded to the EGPWS alerts and the reduced proximity to terrain.
Although the captain’s initial degraded situational awareness and lack of visual cues limited their initial understanding of the situation, their decision to establish control of the aircraft during a critical situation was sound.
Their decision to prioritise scanning the instruments to regain situational awareness during the event contributed to a successful recovery. The decisive nature of their intervention further underscores the importance of training and rehearsed recovery actions to mitigate the risks of spatial disorientation in degraded visual environments.
Other finding
The captain's control inputs stopped the vertical descent and established the helicopter in a climb, which reduced the risk of collision with terrain.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the loss of control in flight involving Leonardo Helicopters AW139, VH‑EXK, 19 km east of Longford Heliport, Victoria, on 2 August 2024.
Contributing factors
The instructor hastily departed the training area, due to encountering fog, before the hoist was secured with the door open, and while the captain as pilot monitoring was still occupied recording the training aid position.
After inadvertently entering instrument meteorological conditions, the instructor (pilot flying) became spatially disorientated.
The instructor's attempt to leave IMC, while being spatially disorientated, resulted in control inputs that led to the helicopter entering an unstable state while still in IMC, triggering a terrain alert below 150 ft, and maximum airspeed exceedances for operations with the main rotor RPM at 102%, the door open and hoist extended.
Other factors that increased risk
Prior to gaining situational awareness, and without an appropriate control handover, the captain reactively assumed control of the helicopter after the terrain warning, increasing the risk of control conflict between the 2 crew.
Esso Australia did not have a procedure for a helicopter recovery from inadvertent IMC during hoist operations or recovery procedures for EGPWS alerts or advisories. (Safety issue)
Other findings
The captain's control inputs stopped the vertical descent and established the helicopter in a climb, which reduced the risk of collision with terrain.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Esso Australia did not have a procedure for a helicopter recovery from inadvertent IMC during hoist operations or recovery procedures for EGPWS alerts or advisories.
Safety action not associated with an identified safety issue
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Additional safety action by Esso Australia
In addition to developing training and procedures for inadvertent IMC recovery from a search and rescue and hoisting scenario, the operator identified several actions to be taken which included:
discussing the weather phenomena and the possibility for sudden loss of visibility with crews
updating pre-flight training brief to highlight the need to maintain a safe distance to fog or cloud
developing training focusing on the radar height hold function of the AW139
including upset recovery training in CRM.
Glossary
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CRM
Crew resource management
CVR
Cockpit voice recorder
EGPWS
Enhanced ground proximity system
FDR
Flight data recorder
FTR
Force trim release
FMS
Flight management system
HO
Hoist operator
IIMC
Inadvertent IMC
IMC
Instrument meteorological conditions
JSA
Job safety analysis
MPFDR
Multi-purpose flight data recorder
NR
Rotor speed
OPC
Operational proficiency check
PF
Pilot flying
PFD
Primary flight display
PM
Pilot monitoring
RFM
Rotor flight manual
RHT
Radar height hold
SAR
Search and rescue
SPECI
A special report of meteorological conditions, issued when one or more elements meet specified criteria significant to aviation
VMC
Visual meteorological conditions
VFR
Visual flight rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
Airservices Australia
Bureau of Meteorology
captain and instructor of VH-EXK
Civil Aviation Safety Authority
flight data from VH-EXK.
References
Australian Transport Safety Bureau. (2007). An overview of spatial disorientation as a factor in aviation accidents and incidents. ATSB Aviation Research and Analysis Report B2007/0063. Retrieved from/publications/2007/b20070063
Hoh, R. (1990). The effects of degraded visual cueing and divided attention on obstruction avoidance in rotorcraft, Report prepared for the United States Federal Aviation Administration (DOT/FAA/RD-90/40). Retrieved fromhttps://apps.dtic.mil/sti/citations/ADA380260
International Helicopter Safety Team. (n.d.). Training Fact Sheet – Inadvertent Entry Into Instrument Meteorological Conditions (IIMC). Retrieved from https://ushst.org/IIMC/Bulletin%20IIMC.doc
L, O. J. (1998). Errors in aviation decision making: A factor in accidents and incidents. In Proceedings of the Workshop on Human Error, Safety, and Systems Development. 100-107.
Orasanu J., Martin, L., & Davidson, J., (2001). Cognitive and contextual factors in aviation accidents, Linking expertise and naturalistic decision making, 209–226.
Summerfield C & Enger T. (2009). Expectation (and attention) in visual cognition, Trends in Trends in Cognitive Sciences. 13(9). 403-409.
United Kingdom Civil Aviation Authority. (2007). Helicopter flight in degraded visual conditions (Paper 2007/03). Retrieved fromwww.caa.co.uk.
Wiggins, M. W., Hunter, D. R., O’Hare, D., & Martinussen, M. (2012). Characteristics of pilots who report deliberate versus inadvertent visual flight into instrument meteorological conditions’, Safety Science. 50(3). 472-477.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
captain and instructor of VH-EXK
Esso Australia
Bureau of Meteorology
Civil Aviation Safety Authority
Submissions were received from:
Esso Australia
Bureau of Meteorology
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pilot flying (PF): focuses on handling the helicopter during hoisting operations.
[2]Pilot monitoring (PM): manages non-hoist communications, logs positions, monitors performance, and completes in‑flight checks, especially for height and potential obstructions.
[3]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[4]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[5]See Helicopter information, Autopilot and radar height hold
[6]Instrument meteorological conditions (IMC): weather conditions that require crews to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference.
[8]Cyclic: helicopter control mechanism for periodically varying the blade angle of each rotor blade, producing a tilt in the tip-path plane and effecting motion in a desired direction
[9]Instrument flight rules (IFR): rules which allow properly equipped aircraft to be flown under instrument meteorological conditions (IMC)
[10]Helideck: A heliport located on a fixed or floating offshore facility such as an exploration and/or production unit used for the exploitation of oil or gas.
[11]External load: carrying or towing a load outside an aircraft in flight and includes training for such an operation.
[12]Category A: In relation to rotorcraft, means a multi-engine rotorcraft that is capable of operation using take-off and landing data scheduled under a critical engine failure concept, which assures adequate designated ground or water area and adequate performance capability for continued safe flight, or safe rejected take-off in the event of engine failure, as mentioned in the rotorcraft’s flight manual.
[13]A dual action spring permits force‑feel hands on flying while the force trim is engaged. A pilot moving the flight controls without releasing the force trim results in full hands‑on controllability with control force feedback to the pilot. As the pilot releases the control to resume hands‑off flying, the spring returns the collective to its neutral position against the force trim.
[14]JSA: job safety analysis – crew briefing review of operational data, tech log details and rotor flight manual aircraft performance.
[15]Challenge and response procedures apply to multi‑crew operations, where checklist items are called by one crew member and either checked or completed by another.
A range of safety actions have been taken, or are underway, to address issues highlighted in the investigation of boom gates failing to operate at a pair of level crossings in an incident at Werribee, south-west of Melbourne.
On 4 December 2020, a train hauling containerised freight passed over the Werribee Street and Cherry Street level crossings, without either crossing’s boom gates activating.
At one crossing, cars passed less than two seconds in front of the train as it approached.
An investigation by Victoria’s Office of the Chief Investigator, conducted on behalf of the Australian Transport Safety Bureau, has yielded a number of safety issues relating to the management and communication of changes during complex infrastructure projects.
The investigation’s final report explains that the incident was associated with electrical circuit isolation arrangements for level crossing removal signalling works.
“The design for the isolation of these circuits was changed two days before work began, and this was not effectively reflected in program documentation, nor effectively disseminated to all those potentially affected,” Chief Investigator Mark Smallwood said.
As part of the isolation, two fuses which were supposed to be ‘removed and secured’ were instead disconnected, but folded out, with one end remaining in the fuse holder.
“A few days later, a different set of workers – who were not familiar with the isolation arrangement – rotated the two fuses back into place for the purpose of testing,” Mr Smallwood explained.
“This reconnection, combined with temporary jumper wires installed as part of the isolation, prevented the level crossing protection equipment from operating when the train approached.”
It was found that there was probably no independent check of the isolation arrangements as originally installed. An earlier internal audit of the project also identified instances of testers in charge checking their own work.
“This occurrence highlights the importance of considering the implications of late design changes, updating plans and programs, and ensuring all affected parties have a clear understanding of the implications of their work activities,” Mr Smallwood said.
“This is particularly the case in complex projects that involve consortia, contractors, sub‑contractors, and the responsible rail infrastructure manager.”
After the incident, the project alliance in charge of the level crossing removal – which includes operator Metro Trains Melbourne – took several safety actions, including updating of assurance frameworks and associated procedures, and awareness initiatives.
“These actions should address identified safety issues in testing and commissioning practices and assurances,” Mr Smallwood remarked.
The final report also notes Metro Trains Melbourne is contributing to the development of consistent signalling practices and enhanced competency frameworks across all of its major projects.
“The work of Victoria’s Signalling Strategy Taskforce, in which Metro Trains Melbourne is an active participant, has the potential to provide an industry-wide framework to address safety issues like those identified in this investigation,” Mr Smallwood concluded.