During maintenance of a Bell UH-1B, several cracks were found in a tension-torsion strap from one of the helicopter's main rotor blades. Following the provision of a defect report from the helicopter maintainer, the Civil Aviation Safety Authority has requested the ATSB to complete a technical examination of the defective tension-torsion strap.
To facilitate this work, the ATSB has initiated an external investigation under the provisions of the Transport Safety Investigation Act 2003.
The Civil Aviation Safety Authority is responsible for and will administer the release of any information from the technical examination. Any enquires relating to the matter should be directed to CASA at www.casa.gov.au.
On 29 January 2026, a Saab 340 aircraft, registered VH‑VEZ, was operating a scheduled passenger service from Canberra Airport, Australian Capital Territory, to Newcastle Airport, New South Wales, with 3 crew members and 19 passengers on board. During take-off, the left inboard main landing gear wheel separated from the aircraft.
After coordinating with air traffic control (ATC) the crew returned the aircraft to Canberra where it landed without incident. The crew shut down both engines on the runway, and the aircraft was towed to the apron, where passengers later disembarked. The main wheel was subsequently located against an internal airport fence.
What the ATSB found
Examination of the components found that the left inboard wheel separated due to failure of the wheel bearings. Due to the degree of damage sustained by the bearing components, it was not possible to determine the cause of the bearing failure.
What has been done as a result
As a result of this occurrence, the aircraft operator conducted a fleet‑wide inspection of main wheel assemblies and nose wheel assemblies for any defects. No faults were found on any aircraft at the time of inspection.
In addition, the operator implemented a proactive change to its wheel bearing maintenance schedule.
Safety message
This occurrence highlights the importance of effective communication and decision‑making in managing unexpected aircraft malfunctions. After being advised by ATC that a wheel had separated from the aircraft, the crew initially focused on climbing the aircraft to the minimum safe altitude, before taking time to apply standard operating procedures to plan a return to Canberra Airport.
Communication and coordination with ATC enabled confirmation of the specific missing wheel and emergency services preparation. In combination, these actions maintained safety margins and resulted in a safe landing.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 29 January 2026, a Saab 340 aircraft, registered VH‑VEZ, was operating a scheduled passenger service from Canberra Airport, Australian Capital Territory, to Newcastle Airport, New South Wales, as flight FC201, with 3 crewmembers and 19 passengers on board. At 1548 local time, the aircraft taxied from the apron and conducted a take-off from runway 35.1
During the initial climb, air traffic control (ATC) advised the flight crew that a wheel had separated from the aircraft. In response, the crew requested and received clearance to maintain runway heading and climbed to the minimum safe altitude. They reviewed the quick reference handbook (QRH) for checklist items applicable to the event, however none were identified.
As the aircraft approached the limit of the Canberra Airport control area, the crew made the decision to return to the airport. They advised the cabin manager and ground staff of the decision. In coordination with ATC, the crew conducted a fly‑by of the control tower to allow for a visual inspection of the landing gear. Tower personnel confirmed that the left inboard main landing gear wheel was missing. The crew then commenced orbits on the eastern side of the airport to allow time for landing preparation, ensuring the landing performance calculations and briefing tasks were completed. They assessed that a normal landing configuration was most appropriate for the situation, and advised the cabin manager and passengers accordingly.
The crew notified ATC of their intention to return to land and emergency services were placed on standby. The captain declared a PAN2 while the first officer coordinated with company operations staff. The aircraft was subsequently positioned on an extended final approach to runway 35.
At 1611, the aircraft landed safely and was brought to a stop at the end of the runway (Figure 1). Airport emergency services reported no fire, smoke, or fluid leaks from the landing gear. The crew shut down both engines on the runway, and the aircraft was towed to the apron, where passengers were disembarked. Canberra Airport safety personnel located the main wheel against an internal airport fence on the eastern side of runway 35.
Figure 1: VH-VEZ left main landing gear with separated inboard wheel
Source: Aircraft operator
Context
Aircraft information
VH-VEZ was a Saab 340B, serial number 340B‑450. It was manufactured in Sweden in 1998 and was first registered in Australia on 18 November 2022. The aircraft was powered by 2 General Electric CT7‑9B turboprop engines, equipped with Dowty Aerospace R390/4‑123‑F propellers.
Main wheel assembly information
The Saab 340B main landing gear has an inboard and outboard main wheel, both with a brake assembly, attached to the main landing gear leg axle.
Main wheel assembly
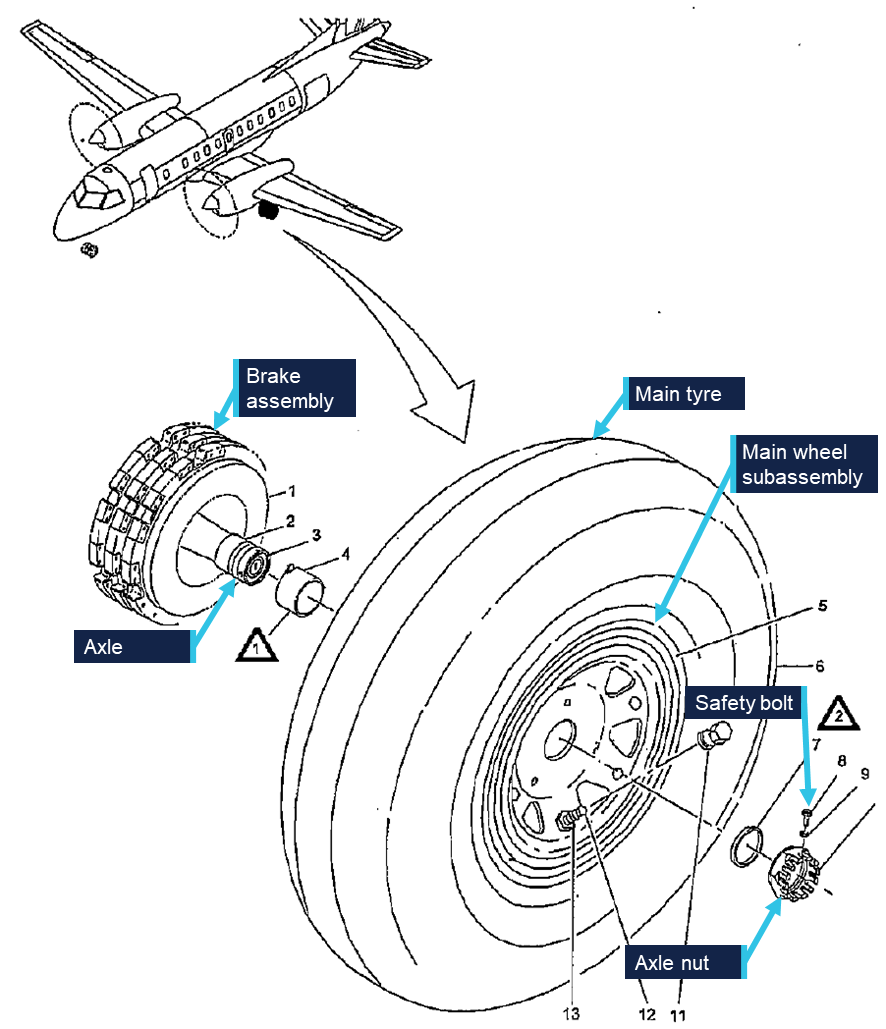
An overview of a main wheel is shown in Figure 2. The main wheel assembly consists primarily of the tyre and the wheel subassembly; also referred to as the wheel hub. The main wheel assembly connects to the axle via an inboard and outboard tapered roller bearing, installed in the wheel subassembly as shown in Figure 2. The main wheel assembly is held onto the axle via a single axle nut and safety bolt.
Figure 2: Saab 340 main wheel assembly
Source: Saab Aircraft Maintenance Manual, annotated by the ATSB
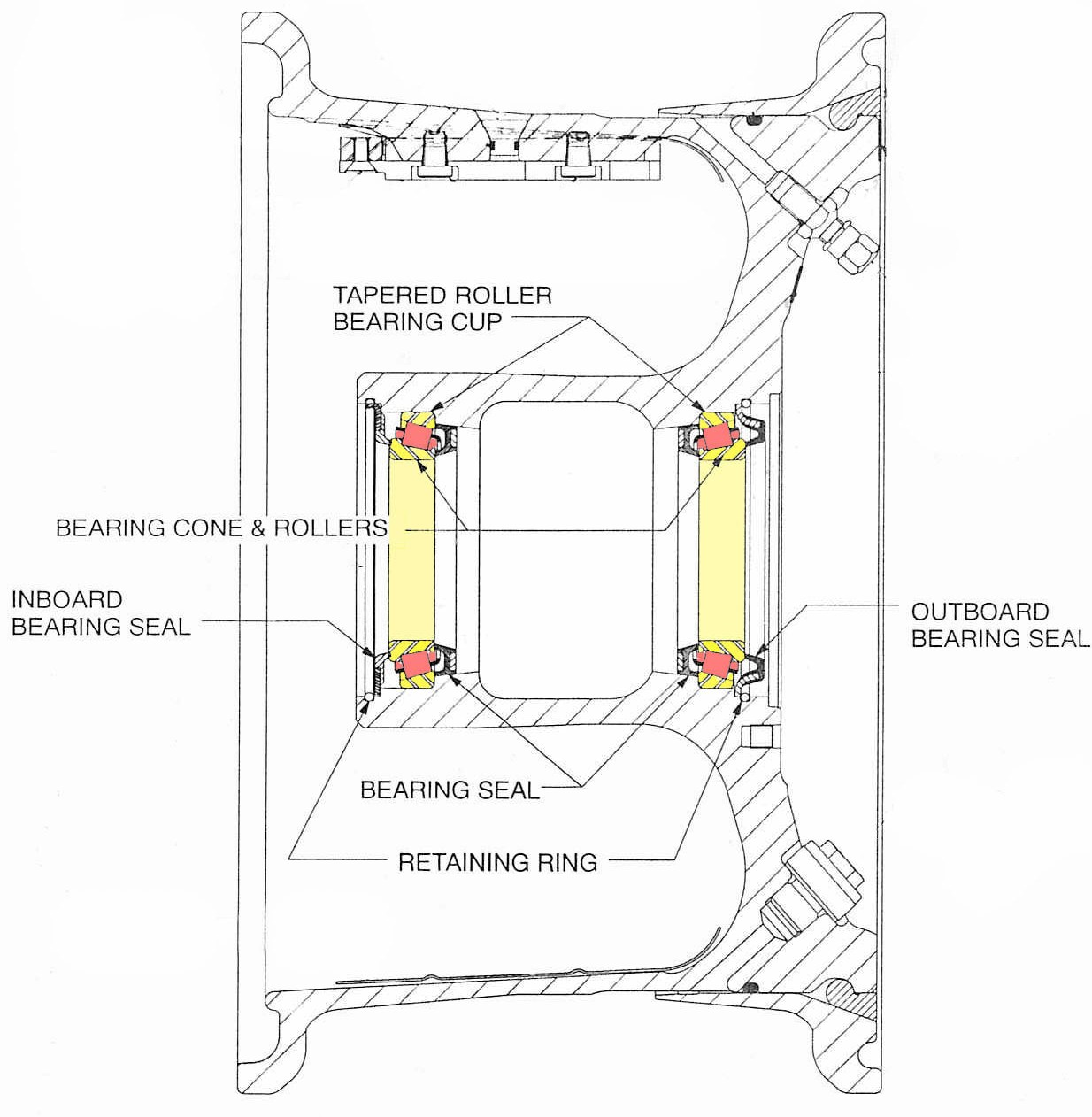
Figure 3: Wheel subassembly cross section with inner and outer bearings highlighted
Source: Meggitt Aircraft Braking Systems Component Maintenance Manual, amended by the ATSB
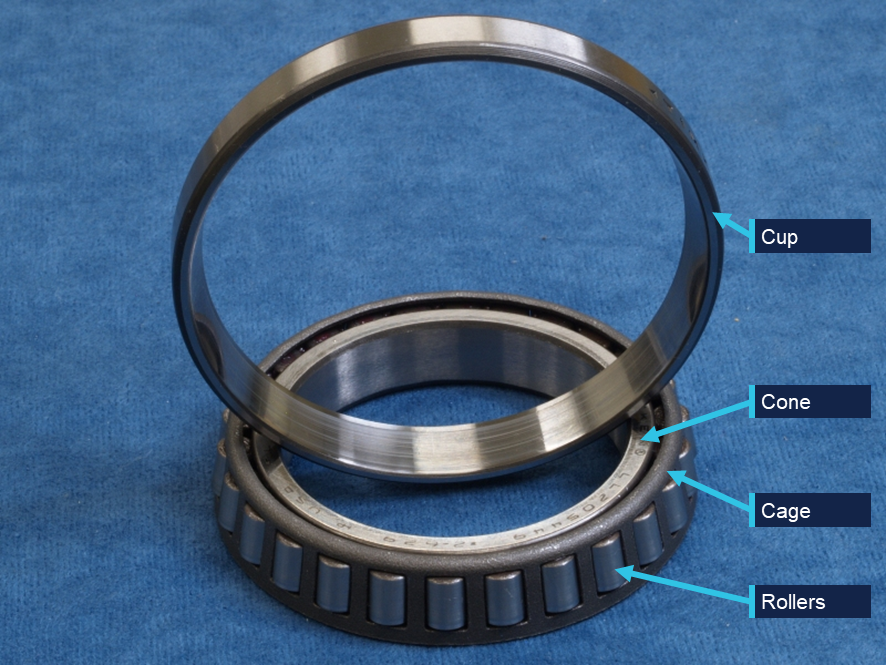
Each wheel subassembly bearing is comprised of a cup (outer race), cone (inner race), cage, and rolling elements (rollers) (Figure 4), held in place with a retaining ring. The bearing cups are shrink fitted into the wheel subassembly. Each bearing then has an inner and outer seal to protect it from contamination while preserving the grease lubrication. The cup or the cone-and-rollers can be replaced independently without changing the entire bearing.
Figure 4: Example bearing
Source: ATSB
Main wheel assembly examination
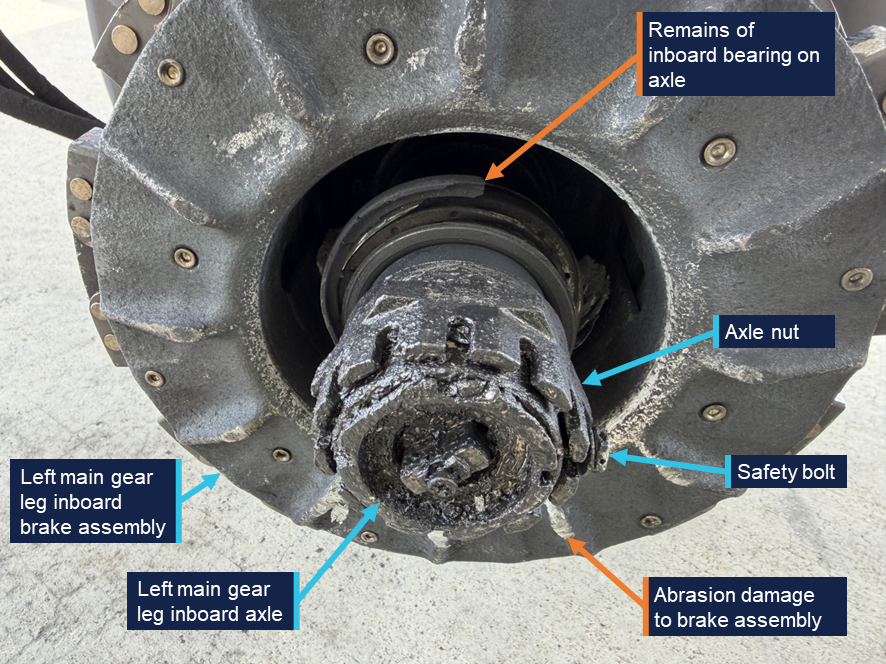
A post-incident inspection of the left main landing gear wheel and the main landing gear axle identified significant damage to both components. The axle nut and safety bolt remained in place on the axle (Figure 5). Remains of the inboard bearing were also identified on the axle, and there was visible abrasion to the brake assembly.
Figure 5: Left main gear leg inboard axle
Source: Aircraft operator, annotated by the ATSB
The tyre on the main wheel remained inflated and the fusible plug3 had not activated. The wheel face had sustained minor damage and the hub cap remained installed and was secured with safety wire. Grease residue was observed around the hub cap.
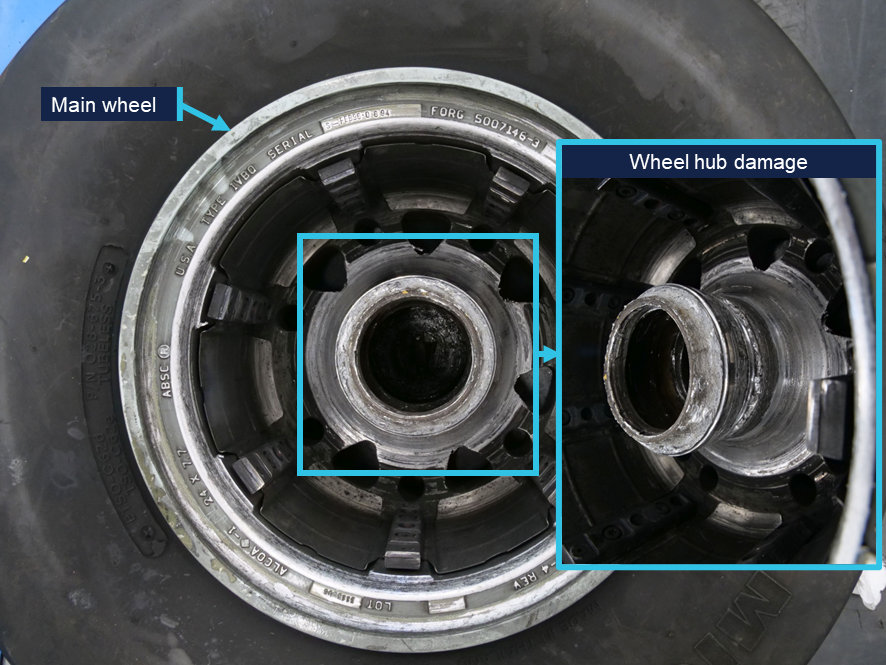
The inboard side of the wheel sustained significant damage (Figure 6). A circumferential fracture surface was visible on the inboard region of the hub encompassing the inboard bearing cone seat. The hub surfaces in proximity to the brake assembly when the wheel is installed exhibited deep rotational gouging and scoring.
Figure 6: Main wheel hub damage
Source: ATSB
Pieces of bearing material were found with the wheel, including 13 roller elements, fragments of the roller cages and bearing seals. The outboard cup remained installed in the wheel. All of the bearing races exhibited significant damage and smearing,4 including deformation from impact with loose rollers. Both cones had heat colouration as evidence of exposure to high temperatures.
The fractured sections of wheel hub also had evidence of heat damage. To the extent that could be established,5 the ATSB did not identify any evidence of progressive cracking or pre-existing defect that might have contributed to the fracture.
Main wheel assembly history
The main wheel assembly part number 5010488-2 and serial number APR93‑1167, was manufactured by the Aircraft Braking Systems Corporation (ABSC), now Meggitt Aircraft Braking Systems (MABS), in April 1993. The wheel was installed on VH‑VEZ on 11 December 2025 following an overhaul on 26 November 2025. Maintenance records documented the history of work on the wheel assembly in accordance with maintenance instructions. During those workshop visits, bearing cups and/or cone‑and‑rollers were replaced, however, the records did not specify whether the replaced components were installed in the inboard or outboard positions.
Component maintenance procedures
Service letter (SL) SL-GS-366 and component maintenance manual (CMM) 32-41-167 outlined the wheel inspection and overhaul schedules, and maintenance procedures for this type of wheel. The CMM stated that wheels are an ‘on condition’ part, meaning there was no defined service life and that inspections, tests and checks were used to determine the condition of the wheel and subcomponents with regard to continued serviceability.
Two key procedures given in the CMM include tyre change and overhaul.
Tyre change
The tyre change procedure was carried out when a tyre was worn to its tread limit. This involved removing the worn tyre, conducting a detailed visual inspection of the whole wheel assembly and non-destructive (eddy current or ultrasonic) inspection of specific areas. At each tyre change, the bearing cones, cups and rollers were cleaned, inspected and regreased prior to install. Parts were replaced when they failed to meet the inspection criteria within the CMM.
Overhaul
At an overhaul, wheels had to undergo a full tyre change inspection plus eddy current, ultrasonic or fluorescent penetrant inspection of the whole wheel. The SL stated that overhauls for fixed wing commercial aircraft wheels should be performed at maximum intervals of 5 tyre changes, or 1,500 cycles,8 whichever occurred first.
Operator’s maintenance process
The operator contracted an external maintenance organisation to conduct wheel tyre changes and overhauls for its Saab fleet. The operator advised the ATSB that the average cycles between tyre changes is 260, meaning that the wheel and bearings are inspected approximately every 260 cycles.
Previous occurrences
The aircraft manufacturer provided the ATSB with data on similar reported occurrences from global Saab 340B operators. Since 1997 there have been 14 reported occurrences relating to a main landing gear wheel departing the aircraft, one of which (AO-2008-046) was investigated by the ATSB, and 2 occurrences of bearing failures where the wheel did not depart the aircraft.
The aircraft manufacturer advised the ATSB that it had not identified any trends or variations related to loss of wheel or main wheel bearing failure occurrences. In 2008, the aircraft manufacturer released a service newsletter highlighting the importance of rotating the wheel while torquing the wheel axle nut to prevent axial play, which can result in bearing failures.
On 6 July 2008, a Saab 340B aircraft departed Orange for a scheduled flight to Sydney, New South Wales.
During take-off, the right outboard main wheel detached from the aircraft. The crew continued to Sydney where the aircraft landed without further incident.
Examination of the components identified that the wheel detachment occurred due to a failed wheel bearing. It was possible that the failure was related to a lubrication or setting (installation) issue, however the degree of damage sustained by the bearing components prevented a determination of the specific failure mechanism.
As a result of that occurrence, the aircraft operator implemented a range of safety actions, including a review of wheel bearing maintenance procedures, and an audit of main wheel axle nut torques across the fleet.
Safety analysis
As the aircraft rotated, the left inboard main landing gear wheel separated from the aircraft. Post-flight inspection of the aircraft identified that the axle nut remained secured on the end of the axle. As such, the potential mechanisms for wheel detachment were limited to a fracture of the wheel or bearing failure.
The level of damage to both bearings, and the absence of any identified pre-existing cracking or defect on the fractured hub pieces supported failure of the bearings as the initiating event. The hub fracture was assessed as secondary, the result of abnormal loading during continued wheel rotation with collapsed bearings.
The bearing failure allowed the wheel to move axially outward, pass over the axle nut, and separate once it was no longer restrained on the landing gear axle.
A bearing failure may have resulted from various initiating factors including:
material or manufacturing defect
improper installation
insufficient lubrication
corrosion
material fatigue
contamination by foreign material.
The condition of the bearing races and the other retained bearing fragments did not provide clear evidence as to an initiating event for the failure. Maintenance records indicated that the wheel was installed and maintained in accordance with the relevant maintenance instructions, and there was a history of replacement of the bearing components.
Additionally, all components were inspected during the overhaul on 26 November 2025 prior to being installed on VH-VEZ, and the wheel had subsequently completed 271 cycles on VH-VEZ. Taken together, they opposed failure being the result of an installation or maintenance error.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following finding is made with respect to the main landing gear wheel separation involving Saab 340, VH-VEZ, Canberra Airport, Australian Capital Territory, on 29 January 2026.
Contributing factors
During take-off, the left main landing gear inboard wheel bearings failed, resulting in the wheel separating from the aircraft. The cause of the bearing failure could not be determined.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Aircraft operator
In response to the occurrence, the operator conducted a fleet‑wide inspection of main wheel assemblies and nose wheel assemblies for any defects. No faults were found on any aircraft at the time of inspection.
In addition, the operator has elected to replace wheel bearings on-condition or at every second wheel overhaul, whichever occurs first.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
first officer
operator
aircraft manufacturer
aircraft component manufacturer.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
flight crew
operator
aircraft manufacturer
aircraft component manufacturer
Civil Aviation Safety Authority
Airservices Australia.
A submission was received from the operator.
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^Runway number: the number represents the magnetic heading of the runway. The runway identification may include L, R or C as required for left, right or centre.
^PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
^The fusible plug is a safety device to prevent tyre explosion by deflating the tyre when a specific temperature is reached.
^Deformation of metal associated with shear loading.
^Not all of the separated wheel hub sections were recovered and there was limited deformation of the fracture surface.
^SL-GS-36 was first issued in July 1993. The most recent revision, version 7, was issued in January 2006.
^CMM 32-41-16 was first issued in April 1992. The most recent revision, revision 6, was issued in April 2014.
^A cycle is a completed take-off and landing sequence.
Occurrence summary
Investigation number
AO-2026-008
Occurrence date
29/01/2026
Occurrence time and timezone
1609 Eastern Daylight-saving Time
Location
Canberra Airport
State
Australian Capital Territory
Report release date
28/05/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Diversion/return, Landing gear/indication, Objects falling from aircraft
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340B
Registration
VH-VEZ
Serial number
340B-450
Aircraft operator
Vee H Aviation Pty Ltd
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
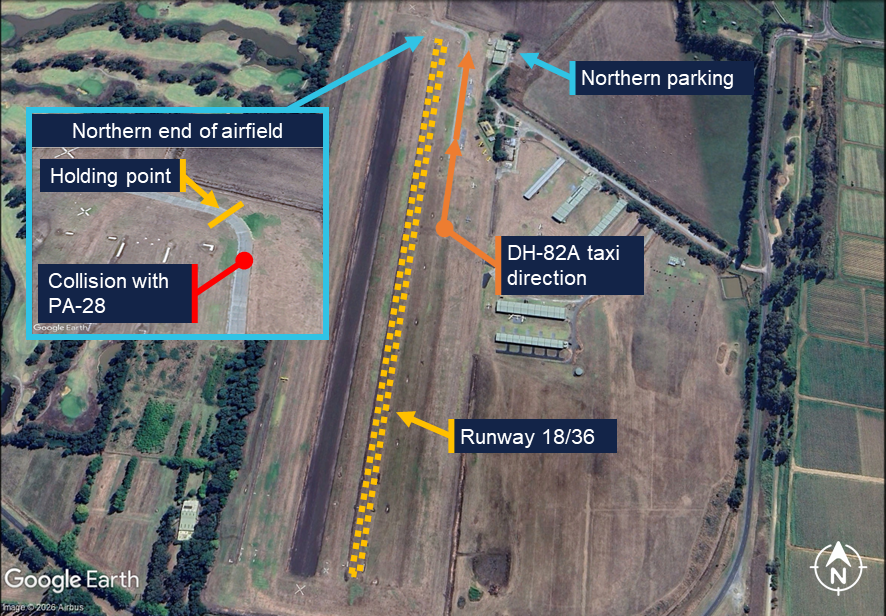
On 27 December 2025 at approximately 1015 local time, an instructor and student operating a Piper PA-28 were preparing to depart Lilydale Aircraft Landing Area (ALA), Victoria, for circuit training. After completing the pre-take-off and run-up[1] checks, the crew taxied to the holding point of runway 18 behind another aircraft. The instructor reported sighting a de Havilland DH-82A Tiger Moth taxiing from the southern end of the airfield.
The DH-82A, having returned from a joy flight with a pilot and passenger on board, exited runway 18 at approximately midfield and began to taxi back to parking at the northern end of the airfield (Figure 1).
Figure 1: Lilydale ALA
Source: Google Earth, annotated by the ATSB with information from operator
The pilot of the DH-82A reported that they did not observe the PA-28 during the taxi, with the nose-high characteristic of tailwheel aircraft likely limiting forward visibility. As the preceding aircraft entered the runway and began its take-off roll, the PA-28 crew were preparing to move forward to the holding point when the DH-82A’s left wing section collided with the rear of the PA-28. The impact resulted in damage to the PA-28’s right elevator trim tab, tail cone and beacon light (Figure 2).
Figure 2: Piper PA-28 damage
Source: Operator, annotated by the ATSB
The damage to the DH-82A was limited to the upper and lower wings (Figure 3). No injuries were sustained by the occupants of either aircraft.
Figure 3: de Havilland DH-82A damage
Source: Operator, annotated by the ATSB
Safety message
Maintaining situational awareness is crucial to ensure safe separation while operating in the vicinity of other aircraft and obstacles. When manoeuvring on the ground it is important that pilots maintain an effective lookout and communicate with other traffic when necessary. These risk controls help mitigate the risk of a taxi collision if a pilot is unsure of the surrounding hazards at any point. This is particularly applicable to pilots operating tailwheel aircraft due to their inherent nose-high attitude which limits forward visibility.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Run-up: a high‑power run-up check is carried out in a piston-engine aircraft to check the aircraft’s ignition and other systems before commencing an initial take‑off.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-003
Occurrence date
27/12/2025
Location
Lilydale Aircraft Landing Area
State
Victoria
Occurrence class
Serious Incident
Aviation occurrence category
Taxiing collision/near collision
Highest injury level
None
Brief release date
10/02/2026
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28-151
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Damage
Minor
Aircraft details
Manufacturer
de Havilland Aircraft
Model
DH-82A
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
The ATSB is investigating a collision with terrain involving a Van's RV-8A, registered VH-MKX, near Heck Field aircraft landing area, Queensland, on 27 January 2026.
The pilot had planned to conduct a private flight from Heck Field to Barraba, New South Wales, with one passenger on board. Shortly after becoming airborne off runway 28, the aircraft collided with terrain. The pilot and passenger were fatally injured, and the aircraft was destroyed.
To date, the ATSB investigation has:
evaluated the accident site and aircraft wreckage
interviewed witnesses and other parties
collected closed circuit television footage
analysed aircraft weight and balance
recovered of the engine from the accident site for more detailed examination
collected of maintenance and pilot records.
The continuing investigation will include:
detailed inspection of components recovered from the accident site
analysis of video and audio recordings
examination of pilot and maintenance records
assessment of related occurrences.
The ATSB released a preliminary report, which details factual information established in the investigation’s early evidence collection phase, on 31 March 2026. See below.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Preliminary report
Report release date: 31/03/2026
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
Accident flight details
Early on the morning of 27 January 2026, the pilot of a Van’s Aircraft RV-8A, registered VH‑MKX, commenced preparation for a private flight from the Heck Field aeroplane landing area, Queensland, to Barraba, New South Wales. At 0328 local time, the pilot submitted a location briefing request to the National Aeronautical Information Processing System[1] through OzRunways.[2] At 0450, the pilot and their passenger were observed arriving at Heck Field by security. The pilot later lodged a flight plan with Airservices Australia at 0528 to depart at 0600 and land at Barraba at 0900. At 0538, closed circuit television (CCTV) footage recorded the pilot and passenger boarding the aircraft, with the pilot sitting in the front seat and the passenger in the rear seat.
The pilot taxied the aircraft to the start of runway 28[3] and commenced the take-off roll. At 0550:14, the aircraft entered the view of the CCTV around 100 m from the runway threshold and was observed accelerating (Figure 1). Fifteen seconds later, the aircraft had travelled around 350 m whereupon it lifted off, flying just above and along the runway surface. At 0550:32, the aircraft began to sink, after which it pitched up and began to climb with wings level. The climb ceased at 0550:41, then the aircraft started to descend. The footage showed that the right wing dropped and the aircraft subsequently collided with terrain at 0550:43. Both occupants sustained fatal injuries and the aircraft was destroyed.
Figure 1: Montage of frames from CCTV showing the accident flight path
The image has been cropped to show the later portion of the flight. The yellow line shows the indicative path of travel for the aircraft. Source: Heck Field airfield CCTV, annotated by the ATSB
Witness observation
An earwitness located at Heck Field reported that their attention was drawn to the sound of the aircraft due to what they described as abnormal engine noises that developed during the take‑off.
Context
Pilot information
The pilot held a Private Pilot Licence (Aeroplane), issued in 1975, and a Private Pilot Licence (Helicopter), issued in 1993. Their total aeronautical experience was reported to be about 5,500 hours. The available flight records indicated they had flown about 60 hours in the last 6 months. The pilot held a valid class 5 aviation medical certificate[4] through self‑declaration of fitness to fly on 15 December 2025.
Aircraft information
General
The Van’s Aircraft RV-8A is a low-wing, all-metal, amateur-built aircraft. It is supplied in kit form and is designed to be constructed for the education and recreation of the owner. The RV-8A has 2 seats in tandem configuration, has a fixed, tricycle landing gear, and is suitable for cross-country flying or for flying aerobatic manoeuvres.
Construction of VH-MKX, serial number 82025, was completed in 2015.[5] It was fitted with a 4-cylinder, horizontally opposed Subaru EJ25 engine modified for aircraft use driving a MT Propellor 3-blade electric constant speed propeller.
A special certificate of airworthiness in the experimental category[6] was issued in 2024. The aircraft was sold to the pilot of the accident flight in January 2025. The most recent maintenance record available to the investigation, dated 8 January 2025, indicated that the aircraft had accrued 614.5 hours time since new.
Meteorological information
There was no Bureau of Meteorology weather monitoring station for Heck Field, however, the graphical area forecast valid for the time and area did not indicate any significant weather phenomena. The airfield CCTV recorded the windsock movements during the take‑off and indicated a south-easterly wind (between 100º to 160º) at around 5 to 10 kt. Geoscience Australia recorded sunrise at the airfield to be 0515.
Recorded information
The aircraft was not fitted with, nor was it required to have, a flight data recorder or cockpit voice recorder. The aircraft was fitted with an electronic flight instrument system that had the capacity to record flight and engine parameters. This device was damaged beyond the ability to recover data.
Automatic dependent surveillance broadcast (ADS-B)[7] flight tracking data was obtained from ADS-B Exchange, which identified 3 data points for the accident flight (Figure 2). The final data point identified an aircraft ground speed of 68 kt.
CCTV (no audio available) of the take-off was recorded by the Gold Coast Sport Flying Club. Another camera at a nearby industrial property recorded audio of the accident flight in which the sounds of the aircraft engine were apparent. The engine was audible for around 40 seconds and the engine revolutions per minute fluctuated periodically for that time.
Figure 2: Flight tracking data and location of closed-circuit television cameras
Source: Google Earth and ADS-B Exchange flight tracking data, annotated by the ATSB
Wreckage and impact information
The accident site was about 360 m from the end of runway 28, on the same heading, in an area of lightly timbered bushland with some felled trees. The distribution of the wreckage indicated that the aircraft collided with terrain right-wing low, at a high angle of entry, and at a relatively slow speed. The aircraft came to rest inverted and facing in the opposite direction to its flightpath. An immediate fuel-fed, post‑impact fire developed into a bushfire in the surrounding area that required a firefighting helicopter to contain.
The fire destroyed the aircraft, limiting the extent to which it could be examined (Figure 3). However, all major aircraft components were accounted for at the accident site. Examination of the flap actuator indicated that the flaps were at or near the fully extended position. Damage to the propeller blades showed that the engine was operating at impact. The engine was recovered from the accident site and taken to a facility for detailed inspection by Queensland Police Service vehicle inspection officers under the supervision of the ATSB. The engine was extensively damaged by the fire, which limited the examination. However, based on the available evidence, no obvious malfunction was identified.
Figure 3: Aircraft at the accident site destroyed by the post-impact fire
Source: Queensland Police Service, annotated by the ATSB
Further investigation
To date, the ATSB has:
examined the wreckage and accident site
recovered and examined the engine
recovered and examined avionics components
interviewed involved parties with knowledge of the pilot, passenger, and the aircraft
collected aircraft and pilot documentation.
The investigation is continuing and will include:
review of aircraft maintenance and pilot documentation
further analysis of the take-off sequence using the CCTV recordings and other recorded data
review of the post-mortem information and survivability factors.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB acknowledges the assistance provided by the Queensland Police Service, the Queensland State Emergency Services, and the Gold Coast Sport Flying Club during the onsite phase of the investigation and additional examination of the engine.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]The National Aeronautical Information Processing System is a multi-function, computerised, aeronautical information system that allows users, such as pilots, to obtain weather information and submit flight plans into the air traffic system.
[2]OzRunways is an electronic flight bag application that provides navigation, weather, area briefings and other flight information. It provides the option for live flight tracking by transmitting the device’s position and altitude.
[3]Runway number: the number represents the magnetic heading closest to the runway orientation. In this case 280º.
[4]The class 5 medical self-declaration allows recreational and private pilots to self-assess and self-declare without requiring a medical assessment. Eligibility and operational limitations apply.
[5]This registration and serial number had been previously used for a Van’s RV-8A that was involved in an accident on 1 October 2010. Some components, such as the avionics and electrical system, from the original aircraft were fitted to the accident aircraft.
[6]Experimental category: the Civil Aviation Safety Authority can issue experimental certificates to allow specific operations of aircraft, which are not by their nature type certificated or have modifications incorporated that are not yet approved. Pilots and passengers of experimental aircraft in Australia accept the risk that the aircraft may not meet the same airworthiness safety standards as certified aircraft and, therefore, operate on the basis of informed participation. Informed participation relies on the premise that before the participant takes part, or pays for an activity, they are fully aware of the potential risks and consequences.
[7]Automatic dependent surveillance-broadcast is a surveillance technology in which an aircraft determines its position via satellite navigation and periodically broadcasts it, enabling it to be tracked.
Occurrence summary
Investigation number
AO-2026-005
Occurrence date
27/01/2026
Occurrence time and timezone
0551 Australian Eastern Standard Time
Location
Near Heck Field aeroplane landing area
State
Queensland
Report release date
31/03/2026
Report status
Preliminary
Anticipated completion
Q1 2027
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Amateur Built Aircraft
Model
RV-8A
Registration
VH-MKX
Serial number
82025
Sector
Piston
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Sport and pleasure flying-Pleasure and personal transport
In 2025 the ATSB adopted a new purpose statement, to “influence transport safety improvements for the greatest public benefit through independent no-blame investigations and fostering safety awareness”.
The updated statement highlights that our role is not just the independent investigation of transport accidents and incidents, it is also to use the reports and their safety messaging to influence safety changes across the aviation, rail and marine sectors.
But it also reflects the broader responsibilities of the ATSB in improving transport safety, such as by helping Australia’s neighbours develop their own best practice safety investigation bodies, providing investigator training for other safety agencies and organisations, administering the REPCON confidential reporting scheme, and publishing and maintaining a national aviation safety occurrence database.
In 2025, in line with our purpose, the ATSB published no fewer than 304 safety products, up from 202 in 2024 and almost double the 153 published in 2023.
Illustrating the breadth of the ATSB’s outputs, these comprised:
91 investigation final reports
34 other investigation reports, including preliminary and interim reports, safety studies and safety advisory notices
74 occurrence briefs
26 safety promotion videos, and
79 REPCON reports.
Significant among those 91 investigation final reports included, in the aviation sector, the systemic investigation of the midair collision of two sightseeing helicopters over the Gold Coast, which made 27 findings and identified 12 safety issues.
Also concluded in 2025 was a systemic investigation into two international widebody airliners taking off over a closed section of runway at Melbourne Airport, which led to safety improvements being implemented or planned by Australia’s aviation regulator and air traffic management provider, the International Civil Aviation Organization and both airlines involved.
In the marine sector we released the final report from our investigation into the collision of a container ship with the Leeuwin sail training ship in Fremantle, with important lessons for marine pilots, and safety action taken by the port and marine pilot operator.
And in rail, our final report from the investigation of a washaway and derailment of a freight train at Traveston, near Gympie in Queensland, emphasised the importance of serviceable environmental monitoring equipment.
All of these significant investigations were supported by ATSB‑produced digital content in the form of educational videos that used graphics, animations and interviews with ATSB investigators to explain the nature of the occurrences, our findings, and broader safety lessons for industry. On social media platforms our videos can generate 10s, and even 100s of thousands of views. (The screenshot above is from an animation created to explain the Melbourne Airport runway investigation.)
In recent years we have invested heavily in producing digital content, as using footage, animations and graphics has proven to be very effective in sharing safety information in a time‑poor, information-rich world.
Occurrence briefs are another platform where the ATSB has increased investment to highlight safety messaging. Briefs are short reports into occurrences that may not justify investigation under the Transport Safety investigation Act, but still offer important safety lessons. Shared on our social media accounts, the 74 briefs published in 2025 (up from 27 in 2024 and 9 in 2023) generated a high level of engagement, increased awareness and discussion.
Also driving the year’s increased publication output was the ATSB’s renewed focus on preliminary and interim reports. For significant accidents and incidents the ATSB aims to publish a preliminary report within 8 weeks of the occurrence, while all investigations that extend beyond a year in length will now have an comprehensive investigation update, typically in the form of an interim report, published every 12 months.
That way industry and key stakeholders are kept updated and informed, and safety information is shared even before an investigation is completed and the ATSB’s findings are fully developed.
The critical role the ATSB plays in receiving and processing confidential reports, through our REPCON system, provides another platform to influence transport safety. REPCON is a voluntary and confidential reporting scheme where industry participants can raise transport safety concerns. After assessing those concerns and approaching involved parties for input and facilitating safety action, a summary REPCON report is published on our website for broader industry awareness.
Other ATSB publications in 2025 included 7 safety advisory notices, a safety study into passenger-carrying hot air ballooning, and 3 reports providing assistance to other Australian agencies conducting their own safety investigations. In addition, 7,636 aviation safety occurrences reported to the ATSB in 2025 were processed and added to our searchable online database.
Beyond Australia, the ATSB continues to engage with and support our equivalent transport safety agencies in the Asia Pacific. For example, long standing partnerships with our counterparts in Indonesia and Papua New Guinea in 2025 continued to see investigators from these nations undertake tertiary level investigator training under the ATSB’s partnership agreement with RMIT University (training that is also available to industry participants).
In addition, in 2025 the ATSB also delivered transport safety investigation training and specific investigation assistance to our colleagues in Tonga and Vanuatu – important capacity-building activities that were supported by funding from the Department of Foreign Affairs and Trade (DFAT).
More broadly our international responsibilities continued to extend to our participation in key United Nations transport agencies, the International Civil Aviation Organization (ICAO) and the International Maritime Organisation (IMO), where we play leading roles in shaping best practice transport safety investigation globally.
But that ability to influence transport safety investigation internationally is only because the ATSB has built and sustained a reputation for high quality, timely investigation reports and safety information products – a reputation that is critical to our ability to effectively influence safety action and foster safety awareness.
The ATSB Annual Report 2024–25 outlines performance against the outcome and program structure in the Department of Infrastructure, Transport, Regional Development, Communications, Sport and the Arts' Portfolio Budget Statements 2024–25(Opens in a new tab/window).
Chief Commissioner's Review
On behalf of the Australian Transport Safety Bureau (ATSB), I am pleased to present the ATSB Annual Report 2024–25. This was a significant year as we celebrated the 25th anniversary of our establishment on 1 July 1999. As we have for each of those 25 years, in 2024–25 we continued delivering on our purpose of improving transport safety for all Australians.
During the year, we focused on the direction contained in the Minister’s Statement of Expectations 2023 to 2025, and the priorities as detailed in the ATSB Strategic Plan. Through our strategic plan we aim to:
» influence positive transport safety outcomes through independently identifying and sharing safety concerns and fostering safety awareness, knowledge and action
» further position the ATSB as Australia’s national transport safety investigator, maximising safety outcomes across transport sectors through growth and innovation
» be an enduring and adaptable organisation that delivers on its mission across changing environments by investing in its people, systems and partnerships.
Some of the actions taken during the year demonstrating our progress in line with these goals included:
» increasing engagement and awareness through investment in stakeholder relationships and the promotion of safety messages through videos and animations
» prioritising the release of timely information from our investigations through prioritising the publication of preliminary and interim reports
» continuing to strengthen our partnership with RMIT University to provide a centre‑of‑excellence for transport safety investigation with the roll-out of the Graduate Diploma in Transport Safety Investigation postgraduate qualification
» strengthening our relationships with our counterparts internationally to improve accident investigation capability and compliance with international protocols and obligations.
In 2024–25, the ATSB published 142 safety-related products, including 67 final investigation reports, 10 preliminary and interim reports, 46 occurrence briefs, 14 safety promotion videos, and 5 safety advisory notices covering the aviation, marine and rail modes of transport.
Significant investigations completed during the year included:
» Gold Coast – Aviation tourism. In April 2025, we released the final report into the midair collision between 2 Eurocopter EC130 helicopters conducting scenic flights on the Gold Coast in early January 2023 (AO-2023-001). The investigation made 28 findings, identified 12 safety issues, and resulted in the release of 2 safety advisory notices. The investigation stressed a number of key safety messages including the potential for unintended consequences when managing changes in aviation operations, and the correct fitment and wearing of seatbelts in helicopter tourism operations.
» Cloncurry – Aviation fire spotting. In June 2025, the final report was released into the pilot incapacitation, loss of control and collision with terrain of a Gulfstream fire surveillance aircraft, south-east of Cloncurry, Queensland, on 4 November 2023 (AO‑2023‑053). The report, supported by a safety promotion video, underscored the dangers of operational practices which circumvent critical safety defences, and the insidious and deadly potential of altitude hypoxia.
» Sydney – Marine SOLAS. Our investigation of a near grounding of the bulk carrier Portland Bay off Royal National Park, south of Sydney in July 2022 (MO-2022-006), resulted in the ATSB issuing formal recommendations to one federal and 2 state government agencies and a salvage operator. The investigation, released in May 2025, identified 9 safety issues, and found a key factor in the prolonged exposure of the ship and its crew to stranding was the extensive delay in tasking the state’s nominated ocean-going emergency towage vessel.
» Brisbane – Rail passenger. In June 2025, we released a final report (RO-2023-004) into a signal passed at danger (SPAD) involving a Brisbane suburban passenger train that passed a stop signal after its driver was briefly impaired. The investigation highlighted the potential limitations of automatic warning system (AWS) alerts to prevent SPAD events. The investigation resulted in one safety recommendation being issued to the operator.
Our investigations over the year uncovered a total of 90 safety issues – factors that if unaddressed have the potential to adversely affect the safety of future operations. Of those safety issues identified, 57% were addressed through appropriate safety action, and a further 10% were partially addressed. Where identified safety issues were not effectively mitigated, the ATSB had cause to make 19 formal safety recommendations to the owners of those safety issues. We will continue to monitor the responses of the risk owners, with the objective of influencing them to take further effective safety action.
Central to our ability to achieve significant outcomes from our investigations are our dedicated staff. During the year we continued working to ensure everyone at the ATSB is supported and valued for their important roles in improving transport safety through implementing several development and wellbeing initiatives. These initiatives have also led to significant improvements in our Australian Public Service (APS) employee census results across all areas of employee engagement, communication and wellbeing.
Our staff are also supported by my fellow Commission members Mr Gary Prosser, Mr Peter Wilson and Ms Julie Bullas. I thank them for their expertise and advice in shaping ATSB investigation reports, which is central to delivering on our role as Australia’s national transport safety investigator.
As we transition into the 2025–26 period, we will continue to focus on the implementation of our strategic plan with a particular focus on improving the efficiency and effectiveness of our operations. We will continue to build our relationships with key stakeholders, including regulators, state governments, industry, and international counterparts. Similarly, we will focus on maintaining our positive APS employee census results by investing further in leadership development, data and innovation to ensure our staff have the appropriate tools and resources to do their jobs.
I look forward to continuing to work with government and all our stakeholders to ensure we are best positioned to effect safety improvements well into the future.
A hot air balloon was operated on a passenger flight after its pilot conducted a field repair without fully understanding the manufacturer’s limits or requirements, an ATSB final report explains.
On 18 October 2025, a Kubíček BB142P hot air balloon was being cold inflated before an early morning sightseeing flight near Beaudesert, Queensland, when a change in wind direction pushed its partially inflated envelope across a field, striking two light posts.
After the crew recovered the balloon, the pilot identified a tear in one of the upper envelope panels above the balloon equator.
The pilot, who was also the maintainer of the aircraft, estimated the tear to be about 45 cm, and conducted a field repair using specialised adhesive tape.
During the subsequent flight with the pilot and 24 passengers on board, the repair degraded and a hole opened in the envelope, allowing air to escape from the balloon. The pilot was able to continue the flight and land at the planned destination without further incident.
“The initial damage occurred after an inflation and launch position was selected which did not provide sufficient clearance from nearby obstacles,” ATSB Director of Transport Safety Dr Stuart Godley explained.
“The resulting tear, which the pilot estimated as 45 cm, was far in exceedance of the 2.5 cm limit without overstitching defined by the manufacturer for this type of field repair. However the pilot did not fully understand the manufacturer’s guidance.”
Dr Godley said the pilot was likely also influenced by their perception of passengers’ expectations.
“After hot inflating the balloon and observing no immediate degradation of the repair, the pilot likely perceived the expectations of the 24 passengers, who had already arrived for the flight, as a strong motivator to continue,” he said.
“The weight of the perceived passenger expectation would likely have the pilot searching for solutions to allow the flight to proceed, rather than cancelling and rescheduling the flight to conduct required repairs.”
The pilot reported seeing the tape repair degrading during the flight, but assessed they did not need to land earlier than planned.
“When the repair degraded in flight, the pilot continued for the remaining 5-10 minutes of the planned flight, rather than landing immediately, despite the manufacturer’s flight manual instructions to land as soon as possible following in-flight envelope damage,” Dr Godley said.
A recent ATSB safety study provided balloon operators with guidance to reduce the risk of passenger injuries in commercial operations, with recommended risk controls including thorough passenger safety briefings, clear go/no-go decision criteria, and implementing a Safety Management System.
“This incident demonstrates how pilots and maintainers should be aware of external and internal commercial pressures to continue a flight without fully researching and conducting an appropriate repair, in the event of a damaged envelope,” Dr Godley added.
“These repairs must be conducted in accordance with the manufacturer’s instructions, as non-approved repairs can normalise unsafe practices over time, and represent a significant risk to those on board.”
Limited night-time hours on type and workload contributed to an autopilot mode selection error that resulted inan S-92 helicopter inadvertently descending below 200 ft above the water at night, triggering an EGPWS terrain warning, an ATSB investigation has found.
The investigation’s final report details that threepilots were onboard the PHI International Australia operated Sikorsky S-92A when it took off from Exmouth, WA just prior to last light on 1 February 2025.
The helicopter tracked towards the drilling rig Transocean Endurance, about 71 km to the north‑north-west, where each of the pilots was to conduct three take-offs and landings to maintain recency in case of an emergency night evacuation from an offshore rig.
The captain was the pilot flying for the outbound flight to the rig, with the copilot as pilot monitoring. The third pilot was seated in a passenger seat in the helicopter’s main cabin.
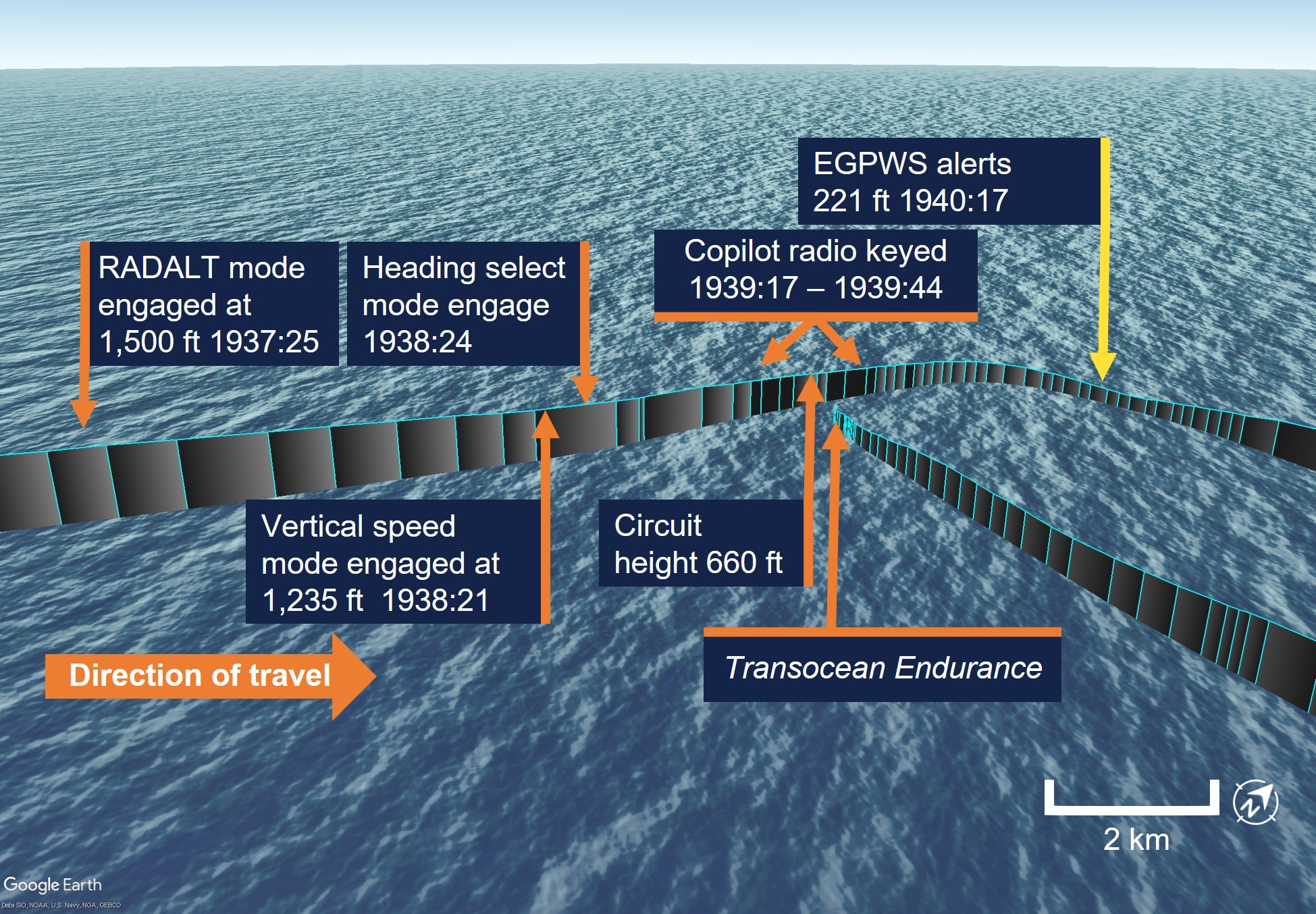
A short time after arriving in the vicinity of the Transocean Endurance, the helicopter continued descent below the intended pre-set circuit height, which was not recognised by the flight crew.
As it descended to 220 ft above the ocean, the helicopter’s enhanced ground proximity warning system (EGPWS) indicated a terrain caution alert, which was followed by a terrain warning about 4 seconds later, as the S-92 descended through 181 ft.
The crew responded and initiated a climb,stabilised, and debriefed the incident before continuing with the planned exercise.
The lowest recorded altitude of the helicopter during the incident was 152 ft.
The ATSB investigation final report notes that, when the helicopter arrived near the rig, the captain had set the radar altitude hold mode to the circuit height of 660 ft.
“The intent of this setting was for the helicopter to descend from its 1,500 ft cruise altitude to the circuit height, and then for it to automatically hold there,” ATSB Director of Transport Safety Dr Stuart Godley said.
“However, during the descent the captain inadvertently mis-selected the vertical speed mode while attempting to select the helicopter’s autopilot heading hold mode.
“This selection error, which was not recognised by either flight crew member, cancelled the original radar altitude hold order, and instead inadvertently commanded the helicopter to descend at a continuous 500 ft per minute.”
The ATSB found both the pilot flying and pilot monitoring at the time of the incident had limited experience on the S-92A at night, and were experiencing a higher than normal workload.
“The vast majority of the flight crew’s experience in the S-92A was from daytime passenger transfer flights, which involved flying first from Exmouth to Learmonth, to collect passengers before flying out to an offshore rig,” Dr Godley explained.
“The recency flight, which departed from Exmouth directly to the rig, was therefore shorter than usual, reducing the copilot’s time to complete the required cockpit administration and plan the approach, and resulting in the flight crew experiencing a higher than normal workload, at night.”
In the shorter flight time available, the pilots had been unable to accurately determine the take-off safety speed prior to their descent for landing. While in the circuit area the captain requested the copilot calculate it, increasing their workload and focusing them away from their monitoring duties.
At about the same time, the captain elected to activate the helicopter’s moveable searchlight, shifting their focus outside to adjust its position.
“This meant both flight crew members were preoccupied with additional tasks and therefore not monitoring the helicopter’s altitude as it descended towards the water,” Dr Godley said.
“In this case, the EGPWS performed its role, and alerted the flight crew to the undesired low altitude.”
In response to this occurrence, PHI International Australia made several procedural improvements, and adjusted its operational risk assessment for pilots with less than 500 hours on type, or for night flights where both pilots have less than 500 hours at night on type.
“This incident highlights the importance of disciplined and effective multi-crew cooperation, and is a reminder of the risks associated with divided attention in the cockpit.”
Dr Godley said the incident also highlights to S-92A operators of a potential hazard that exists with differing display versions of the automatic flight control system mode select panel.
“Due to the lighting of the panel, distinguishing between hard and soft keys is more difficult at night,” he explained.
“More recent versions of the mode select panel include a tactile white finger barrier installed between the rows of hard and soft keys, reducing – but not eliminating – the risk of a mode selection error.”