GNR = General notification roster – available for after hours phone duty
On rare occasions and to meet operational requirements such as a major accident, the need for a particular skill or specialist knowledge, or concurrent accidents, non-rostered transport safety investigators may be contacted in- or out-of-hours and asked if they are able to deploy at short notice.
All investigators on the deployment roster are provided with a Go-kit for deployment purposes. The Go-kit typically contains a uniform and Personal Protective Equipment (PPE) used during deployments.
The ATSB is investigating a runway incursion and near collision involving a Cessna 402C, registered VH-HMG, and a safety vehicle, at Jandakot Airport, Western Australia, on 3 March 2026.
During take-off for an air transport operation flight with 4 passengers on board, the sole pilot of the Cessna 402 observed a safety vehicle enter the runway in front of the aircraft. The aircraft was above the maximum speed for a rejected take-off and took off above the vehicle in close proximity.
The ATSB has completed the evidence collection and analysis phases of the investigation and is drafting the final report.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-064
Occurrence date
03/03/2026
Occurrence time and timezone
07:07 Western Australia Standard Time
Location
Jandakot Airport
State
Western Australia
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Drafting
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Near collision, Runway incursion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
402C
Registration
VH-HMG
Serial number
402C1002
Aircraft operator
Paul Lyons Aviation Pty Ltd
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Passenger transport charters
Despite continued concerted efforts to prevent collisions at level crossings by local, state and federal governments in conjunction with the rail industry, the ATSB continues to investigate similar occurrences.
The following investigations highlight some key learnings for both road users and rail infrastructure managers to help reduce collisions at level crossings.
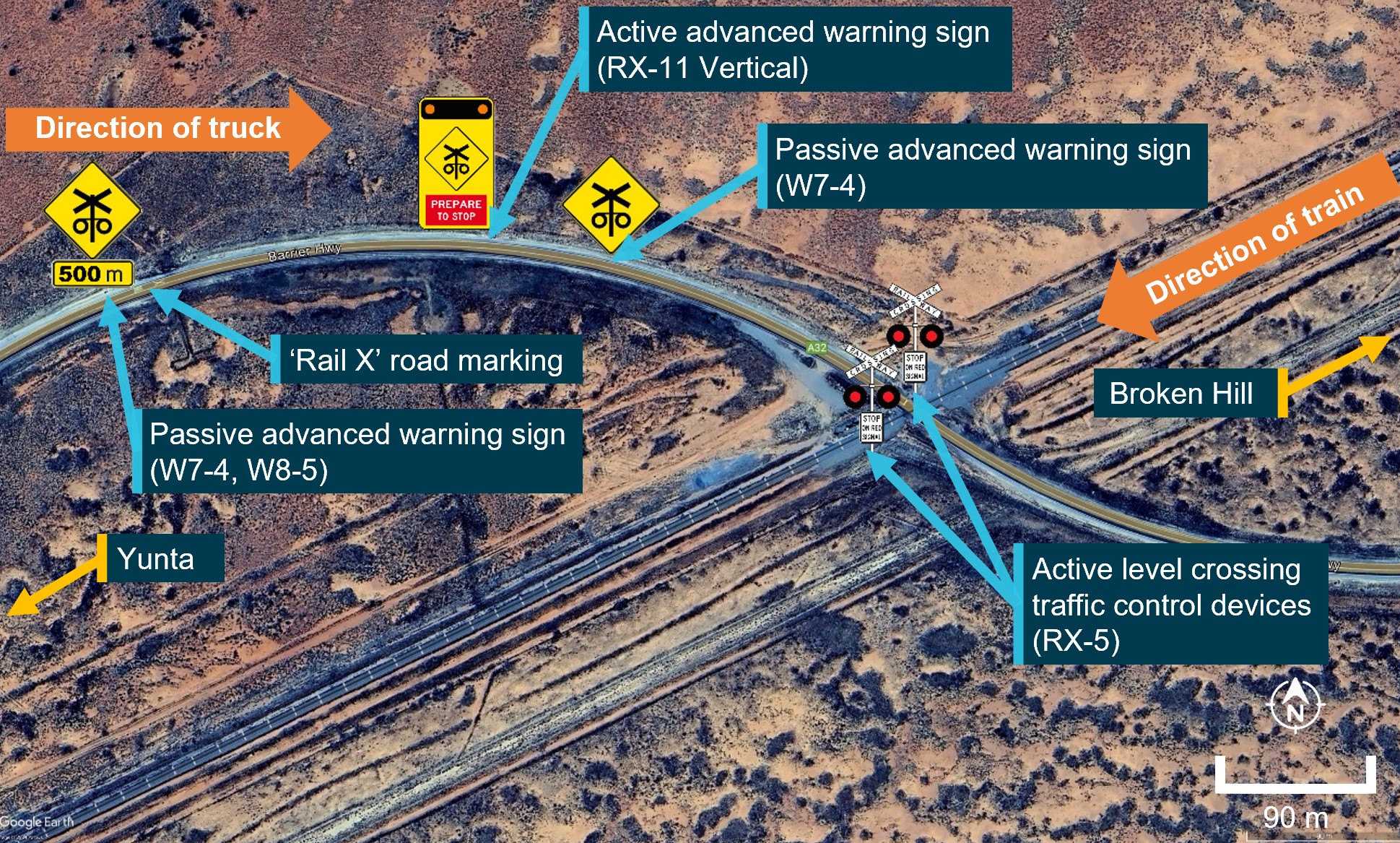
A truck driver who failed to stop before a passive level crossing collision in southern Queensland was probably influenced by expectation bias, having likely never seen a train at the crossing in the past.
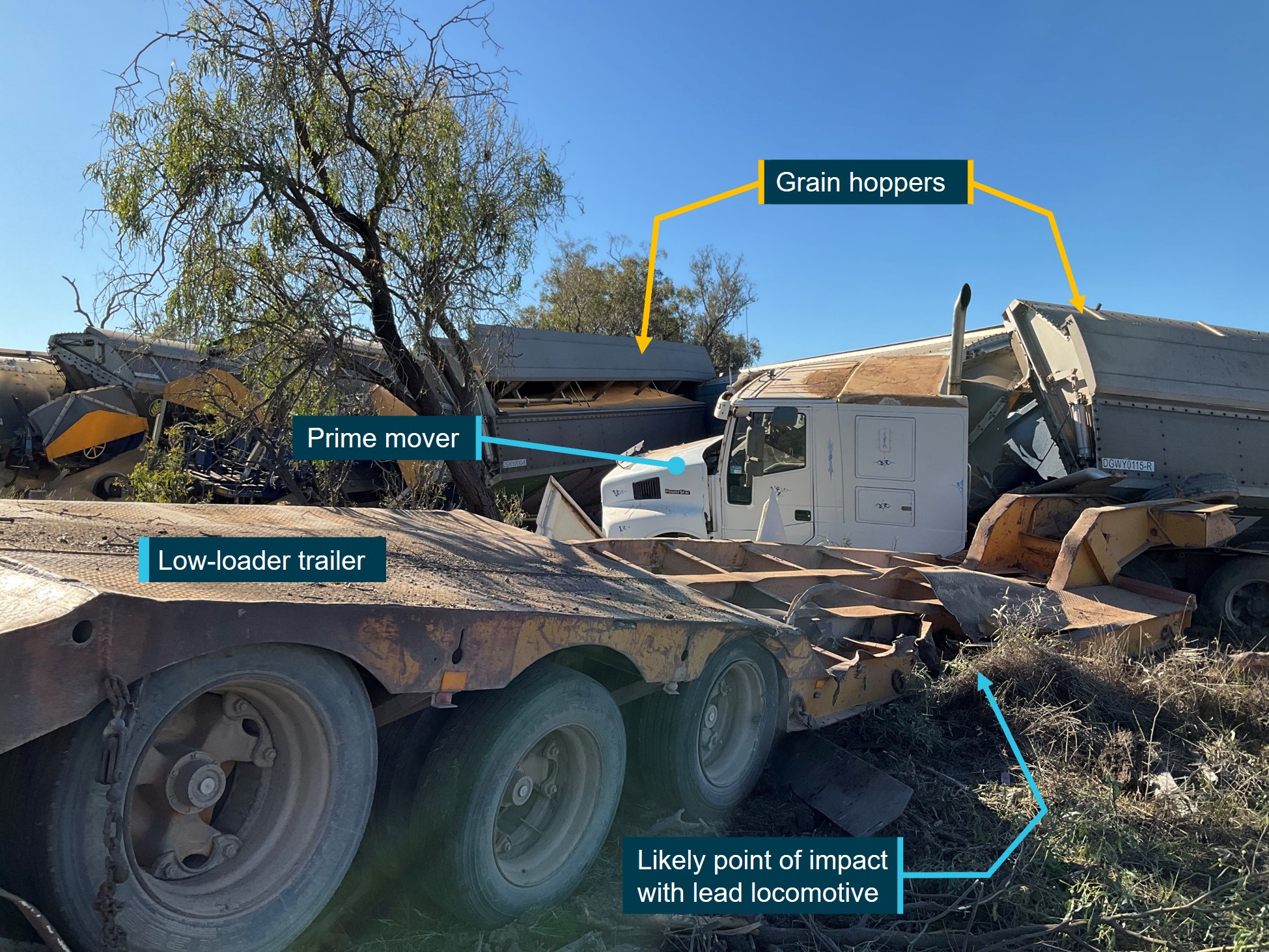
On 23 May 2024, a prime mover hauling a skid steer was about 50 metres north of Gooray Road level crossing, near Goondiwindi, when the truck driver saw a train approaching from the west. Assessing they could not stop in time, the truck driver accelerated, but the truck was unable to clear the crossing before the train collided with the truck’s trailer.
The truck driver and two train drivers were seriously injured in the collision, which also destroyed the train’s two locomotives and 12 grain hoppers, and the truck’s prime mover and low-load trailer.
Due to the infrequency of trains on that corridor, it is likely the truck driver had not seen a train at that crossing in the past. This created an expectation bias which probably reduced the effectiveness of the truck driver’s scan while approaching the crossing. Nonetheless, the signage instructed the driver to stop at the crossing, and the driver did not comply with this requirement.
This accident demonstrates the limitations of passive controls at level crossings, where the onus is on road users to follow these controls – making them particularly vulnerable to unintentional driver error, or intentional driver decisions.
Passive controls are common at level crossings where road and rail traffic volumes are low, and it is unlikely most road users will encounter a train at such a crossing. As road users become familiar with a level crossing where they have not previously encountered trains, they can unconsciously form an expectation that no trains will be present every time they approach that crossing.
It is therefore crucial that road users remain cognisant of the potential presence of trains at every level crossing, and are mindful of the consequences of a collision such as this one.
Lessons learnt
Passive controls cannot physically prevent vehicles from entering a crossing, and the onus is on road users to follow these controls. This makes passive level crossings particularly vulnerable to driver error (unintentional) or driver decisions (intentional), which can place road users at imminent risk of collision with rail traffic.
This incident also highlights, for truck drivers, the importance of completing preparatory checks and rectifying any problems which may be observed prior to moving their vehicle, as there is a significant risk of harm and damage when driving vehicles with mechanical issues.
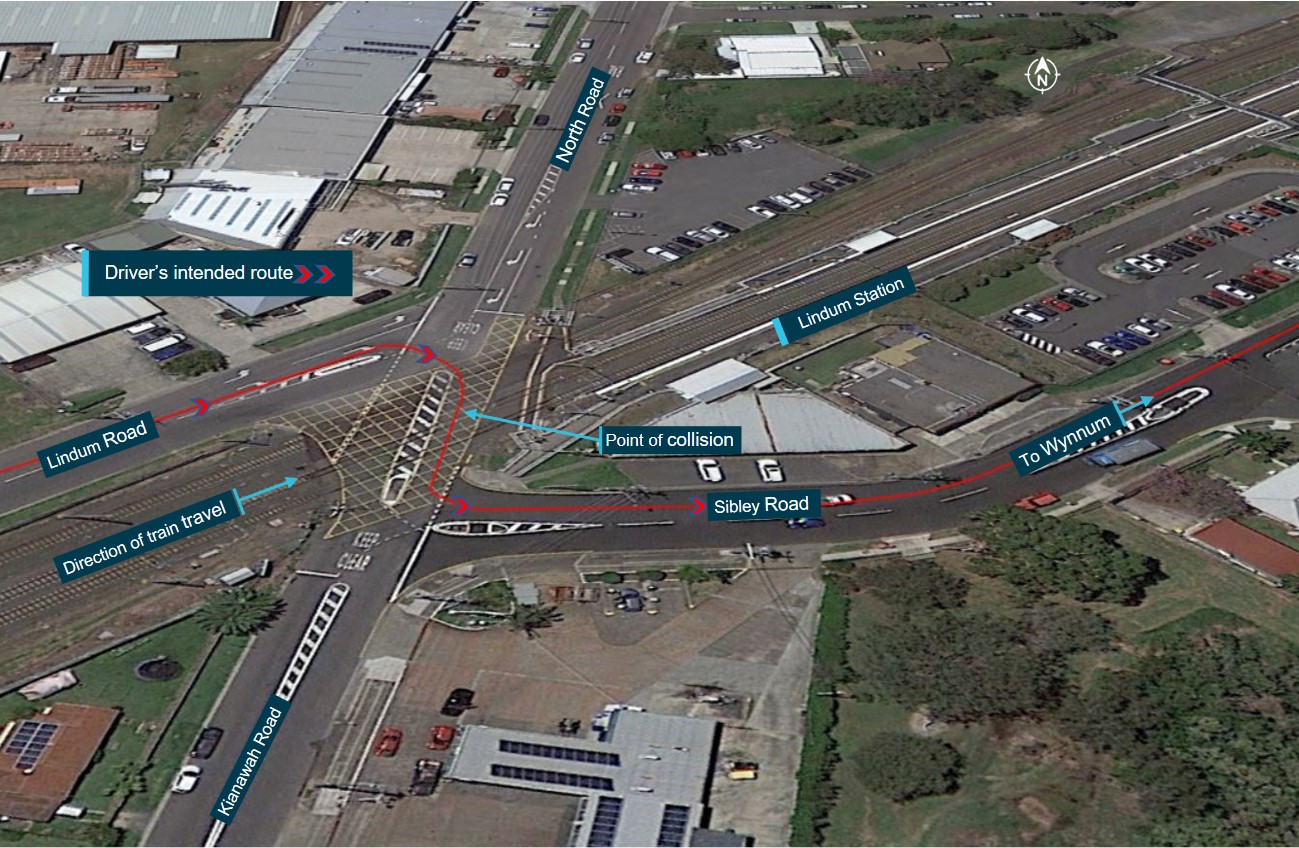
A motorist was fatally injured in a collision with a passenger train at the Kianawah Road level crossing, near Lindum Station in Wynnum West, Queensland after they passed through a gap between the end of the lowered boom barrier and a median island.
On the afternoon of 26 February 2021, a Queensland Rail suburban express passenger train was approaching the Kianawah Road level crossing in the Brisbane suburb of Wynnum West, Queensland. The boom barriers were in the lowered position and other protection devices (flashing lights) were active at the level crossing.
At the same time, after stopping to give way to opposing road traffic at the intersection, immediately adjacent to the level crossing, a motor vehicle turned towards the crossing. It then continued through the level crossing, bypassing the lowered boom barrier, colliding with the train. The motor vehicle was destroyed, and the sole occupant was fatally injured. The only 2 occupants of the train, the driver and guard, were not injured.
Our investigation found that there was a 3.1 m gap between the end of the boom barrier and the median island, which meant that the barrier only partially blocked road traffic that approached the level crossing from Lindum Road. In this instance, it was very likely that the driver of the motor vehicle followed the turn line markings on the road surface, which directed them past the end of the lowered boom barrier onto the level crossing and into the path of the approaching train. Safety concerns raised by local road users and work undertaken by the Government also indicated that the road-rail interface at the Kianawah Road level crossing was complex and visually noisy from a road user’s perspective.
Queensland Rail had not been managing risk at level crossings in accordance with the requirements of its level crossing safety standard. In particular, the standard stated that public and pedestrian level crossings were to be assessed every 5 years or sooner. However, the Kianawah Road level crossing had not been assessed for 19 years. Some other level crossings with high instances of incidents and accidents had also not been assessed for 20 years.
It was also identified that, between 2016 and 2021, Queensland Rail had just one person qualified to assess all their public, pedestrian, private, maintenance, and construction level crossings, which numbered in the thousands. Of the 1,138 public level crossings that required assessment within the 5-year timeframe, just 52 were completed.
Further, Queensland Rail and the Brisbane City Council did not have a formal road-rail interface agreement in place at the time of the accident, although negotiations were ongoing. This was a missed opportunity to collectively identify any unique risks associated with the level crossing and manage and maintain those risks through an agreed process.
Following the accident at the Kianawah Road level crossing, Queensland Rail and the Brisbane City Council have formalised an interface agreement encompassing all level crossings where they have a shared responsibility. In addition, Queensland Rail:
Has installed a new boom barrier at the level crossing, compliant with the Australian Standard (1742.7), that fully protects road users when approaching the active crossing from Lindum Road. In addition, rectified a safety issue where the boom barrier did not fully comply with the requirements of the Australian Standard at 29 other level crossings within its jurisdiction.
Assessed the Kianawah Road level crossing in accordance with the Australian Level Crossing Assessment Model (ALCAM) to establish a current assessment risk score rating.
Has trained 4 internal staff to undertake ALCAM assessments and introduced a procurement process to engage a contract firm to update outstanding regional ALCAM assessments over the next 5 years.
Lessons learnt
Level crossings are a complex environment and are well known for their high-risk consequences. While the ultimate preference is to avoid or remove level crossings, this is often very costly and not a practical solution. Therefore, it is important that road authorities and rail infrastructure managers collectively manage these risks. To achieve this, they should enter into an interface agreement as soon as possible to identify and manage hazards and risks at the road and rail interface, so far as is reasonably practicable.
Sighting from road vehicles can be severely restricted at passively protected level crossings with an acute angle road-to-track interface.
On 13 July 2016, a Warrnambool-bound V/Line passenger train collided with a semi-trailer at the Phalps Road passive level crossing at Larpent, near Colac, Victoria.
When the truck initially stopped at the crossing, the train was more than 300 metres away. The truck commenced moving towards the track when the train was between 220 and 260 m from the crossing. Unaware of the train approaching beyond their line of sight, the truck driver entered the level crossing and heard the train’s horn shortly before the locomotive struck the truck’s semi-trailer.
After impact, the train’s locomotive and all passenger cars derailed. The locomotive driver, train conductor, 18 passengers and the truck driver were injured. There were no fatalities.
The investigation, conducted by Victoria's Chief Investigator, Transport Safety, on behalf of the ATSB, found the driver was unable to detect the approaching train on the left due to the restricted view from the level crossing’s acute road-to-rail angle and the composition of the truck’s passenger-side window.
The ability of a truck driver to see along a railway track to their left can be affected by in-cab obstructions. The Australian Design Standard for passively controlled level crossings accounts for this possibility by requiring a viewing angle of no more 110 degrees for a driver looking to their left from the straight-ahead direction. If this viewing angel is exceeded, passive level crossing controls should not be used.
The investigation found that for a vehicle stopped at the northern side of the Phalps Road level crossing, the viewing angle to achieve the required sighting distance was 116 degrees. The Phalps Road level crossing was subsequently upgraded to active protection controls in August 2016.
Lessons learnt
Rail infrastructure and road managers should ensure that risk assessment processes take account available risk controls for hazards stemming from poor sighting at acute-angle level crossings and actively pursue their implementation.
Road users should be particularly cautious at passively-controlled acute-angle level crossings where their vision to the left may be affected by the road vehicle cabin design.
Conclusion
Each year, people continue to lose their lives or are injured at Australia's level crossings causing significant social and economic impacts on individuals, communities and businesses.
Record investment in rail and road infrastructure, combined with growing passenger traffic and freight demand, is continuing to increase interactions at level crossings.
Our investigations have identified there is a higher rate of collisions at passive level crossing, with a large proportion of these collisions involving heavy vehicles.
Passive controls cannot physically prevent vehicles from entering a crossing, and the onus is on road users to follow these controls. This makes passive level crossings particularly vulnerable to driver error (unintentional) or driver decisions (intentional), which can place road users at imminent risk of collision with rail traffic.
Ensuring the safety of rail travel is integral to growth in patronage, economic contribution, innovation, and sustained investment. There is a significant public benefit in avoiding rail accidents and incidents (occurrences). The ATSB aims to prevent future occurrences by ensuring lessons are learned and safety improvements are made through independent, evidence-based, no-blame investigations, providing assurance that systems are operating safely through growth and change.
What are no-blame investigations?
We do not investigate for the purpose of taking administrative, regulatory, or criminal action.
The Transport Safety Investigation Act 2003 (TSI Act) guards against the inappropriate use of evidence gathered in ATSB investigations in legal proceedings. This gives those directly involved in an occurrence greater confidence that they can provide open disclosure in the interests of safety.
Depending on the circumstances, ONRSR, the police, work health and safety regulators, and coroners may also investigate. The investigation remit of the ATSB, OTSI and OCI is distinct from these organisations. For example, ONRSR undertakes compliance investigations and may employ enforcement mechanisms. In contrast, we investigate and report on systemic safety issues involving risk controls in the rail transport operator, standards, and regulatory frameworks. Safety action taken in response reduces the risk of future occurrences.
Resourcing
ATSB rail safety investigations rely on a combination of funding and resourcing from the Commonwealth and State governments. In addition to the collaboration arrangement we have in New South Wales and Victoria, the Queensland Government provides funding for ATSB investigations in their State. Other States and Territories have not opted into similar arrangements. We are working with governments to provide future certainty around resourcing for a national capability.
Deciding to investigate
The ATSB receives approximately 160 notifications of investigable occurrences each year. Investigation resources are prioritised to investigate occurrences likely to have the greatest public safety benefit through lessons learned.
The ATSB considers:
the availability, including extant tasking, of ATSB rail resources
whether the track is part of the interstate network
if the track is off the interstate network, whether the relevant State or Territory provides funding
whether OTSI or OCI will commit existing resources under the Commonwealth TSI Act
the prioritisation given to mainline passenger operations and then freight and other commercial operations
the severity of the occurrence and anticipated safety outcomes of the investigation.
The severity of the outcome, such as deaths, injuries and damage, does not necessarily indicate the extent of the anticipated safety outcomes. It is important that the ATSB considers near miss occurrences for investigation. The factors that led to the near miss might reveal safety issues that, left unaddressed, could lead to a catastrophic accident in the future.
The criteria above is important for decision-making as the ATSB is currently only able to commence a limited number of investigations annually with its available resourcing.
Rail investigations in Australia
Download the Rail investigations in Australia placemat
The Australian Transport Safety Bureau has published a preliminary report from its ongoing investigation of last month’s accident involving a Cessna 210 off Murray Mouth, South Australia.
The preliminary report, which presents evidence gathered so far in the ATSB’s investigation but does not include analysis or findings, notes the accident occurred on the afternoon of 6 February 2026, approximately 13 minutes after take-off from Goolwa Airport.
“The purpose of the flight was for a commercial licensed pilot, seated in the front left seat, to accumulate Cessna 210 flying experience, under the supervision of a flight instructor,” said ATSB Chief Commissioner Angus Mitchell.
The instructor, who was head of training and checking for the aircraft operator, was seated in the front right seat.
Seated behind them in the second row left seat was a third occupant, a passenger who held a recreational pilot licence.
“A witness on the west side of Murray Mouth saw the aircraft in a steep descent and filmed the aircraft for a few seconds before it collided with water,” ATSB Chief Commissioner Angus Mitchell said.
“The footage shows the aircraft in a left turn spin in a steep nose down and left-wing low attitude, with the landing gear retracted.
“Several witnesses reported the engine sounded like it was running until the collision.”
The 3 occupants were fatally injured and the aircraft was destroyed.
The preliminary report details that to date, investigation activities have included analysis of the video footage, as well as a review of air traffic control radar data, which showed the aircraft’s altitude had reached 3,375 ft and its groundspeed had reduced to 74 kt, before the descent started.
As the investigation progresses, an onboard GPS unit will be examined and data from electronic flight bag apps will be analysed, while an elevator control cable turnbuckle was recovered from the aircraft wreckage for further examination in the ATSB’s Canberra facilities.
A final report will be released at the conclusion of the investigation once the available evidence has been analysed and findings are developed and established.
“However, should a critical safety issue be identified at any time during the course of the investigation, the ATSB will immediately notify affected parties so they can take safety action,” Mr Mitchell concluded.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 9 December 2025, an Ayres Thrush S2R-T34was being used to conduct agricultural spraying, which involved multiple circuits and landings to pick up and disperse approximately 40 loads.
During landing, before picking up the final load for the day, the pilot observed a vehicle approaching the landing strip towards the loading area. The pilot applied additional braking to avoid a possible collision with the vehicle and the aircraft subsequently veered towards a drainage channel adjacent to the landing strip.
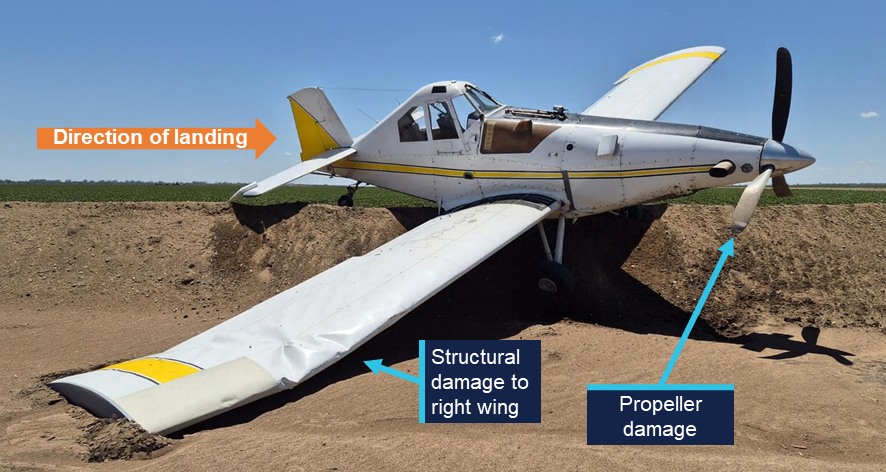
While the pilot monitored the approaching vehicle, the aircraft continued towards the end of the landing strip and the drainage channel. The pilot subsequently attempted to correct the aircraft to remain on the strip however there was insufficient distance and time, and the aircraft entered the channel. There were no injuries to the pilot, and the aircraft was substantially damaged.
Figure 1: Aircraft damage
Source: operator, edited by the ATSB
Safety message
In this occurrence the distraction of the vehicle approaching the landing strip diverted the pilot’s attention from monitoring the landing roll, resulting in a loss of situational awareness.
This type of distraction is more likely to impact performance due to the cognitive demands of one spatial visual scanning task (i.e. monitoring landing roll) being interrupted by another spatial task (i.e. a vehicle moving towards the aircraft’s projected path), particularly during a critical phase of flight where there is very little time to assess the situation.
Concurrent task management depends on the pilot’s ability to effectively prioritise tasks and appropriately time share tasks by rapid switching, whereby attention quickly shifts between tasks. This is essential when the pilot is dealing with multiple tasks, which are all critical to flight safety.
The ability to appropriately prioritise and use rapid switching may be affected by workload and fatigue, which can be a factor during operations involving large numbers of short, similar flights in quick succession. Effective use of rapid switching can also be improved through experience as well as specific task management training.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
The ATSB is investigating a tail rotor failure and subsequent collision with terrain involving a Robinson R22 Beta, registered VH-UBY, about 56 km west of Coonamble Airport, New South Wales, on 6 February 2026.
During aerial mustering operations approximately 100 ft above the ground, the pilot and sole occupant of the helicopter experienced an RPM spike followed by a yaw and a loss in rudder effectiveness. Unable to counteract the yaw, the pilot attempted to land the helicopter, which spun several times during the descent.
Upon contact with the ground, the helicopter rolled onto its side, resulting in substantial damage. The pilot experienced serious injuries, but was able to exit the helicopter without assistance. There was no fire.
The evidence collection phase of the investigation will involve examining tail rotor components, interviewing the pilot and any witnesses, examination of maintenance records, retrieving and reviewing recorded data, and the collection of other relevant information.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Occurrence summary
Investigation number
AO-2026-063
Occurrence date
06/02/2026
Occurrence time and timezone
10:15 Australian Eastern Daylight Time
Location
About 56 km west of Coonamble Airport
State
New South Wales
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Evidence collection
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Abnormal engine indications, Collision with terrain, Propeller/rotor malfunction
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R22 Beta
Registration
VH-UBY
Serial number
4733
Aircraft operator
Dustdevil Helicopters Pty Ltd
Sector
Helicopter
Operation type
Part 138 Aerial work operations
Activity
General aviation / Recreational-Aerial work-Agricultural mustering
Just after midnight, at 0003 on 24 February 2026, a Royal Flying Doctor Service, Queensland Section, Beechcraft King Air B200, registered VH-FDI, with one pilot, a doctor and a nurse on board, taxied at Wellcamp Airport, Queensland, for a flight to Bundaberg. While taxiing for take-off, the aircraft conducted a 180° turn on the turn pad at the end of runway 12 and shortly after, commenced take-off. The aircraft was incorrectly aligned with the right runway edge lights and struck a turn pad edge light during the take-off roll. Parts of the damaged light impacted both propellers and dented the fuselage.
After recognising a ground strike had occurred, the pilot rejected the take-off, cancelled their flight plan with air traffic control, returned to the parking apron and grounded the aircraft.
What the ATSB found
The ATSB found that the incident took place in dark ambient conditions, limiting the visibility of the taxi guidance line markings which were not followed during the turn to line up. Instead, the aircraft was turned tighter, which aligned it with the right edge of the runway.
The pilot perceived the aircraft to be aligned with the runway centreline after they misidentified the right runway edge lights as centreline lights and did not recognise the misalignment by other contradictory cues available at the time.
What has been done as a result
The Royal Flying Doctor Service, Queensland Section, reviewed internal procedures for checklist management, entering and backtracking runways, conducting 180° turns, and requirements around identifying and lining up on runways.
The next version of the flight operations manual will be amended to:
require the ‘before take-off checklist’ be fully completed prior to entering the runway
include clear guidance on checklist interruption management, requiring that, when resuming a checklist, the pilot returns to the previously completed item before continuing.
Further, a notification will be issued to all pilots highlighting the importance of ensuring positive runway centreline environment is established before applying take-off power.
Safety message
A number of factors known to influence misaligned take-off occurrences were identified in this investigation, including dark ambient conditions and taxiway guidance markings. Dark ambient conditions have been consistently identified in similar occurrences and can reduce available visual cues, limiting the ability of pilots to identify their position during line‑up.
Operators should consider the regular use of turn pad guidance line markings which will orientate aircraft with the centre of the runway if followed completely, particularly where the area of the turn pad extends wider than the runway width.
Pilots should crosscheck all available cues to confirm their position prior to take-off at night.
Summary video
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 24 February 2026, a Beechcraft B200C King Air aircraft, registered VH-FDI, was being operated from Wellcamp Airport, Queensland, by the Royal Flying Doctor Service (RFDS), Queensland Section, on an aeromedical flight to Bundaberg Airport.
On board were the pilot and 2 medical crew. The conditions during the midnight departure were dark with little moonlight, low cloud, but otherwise good visibility.
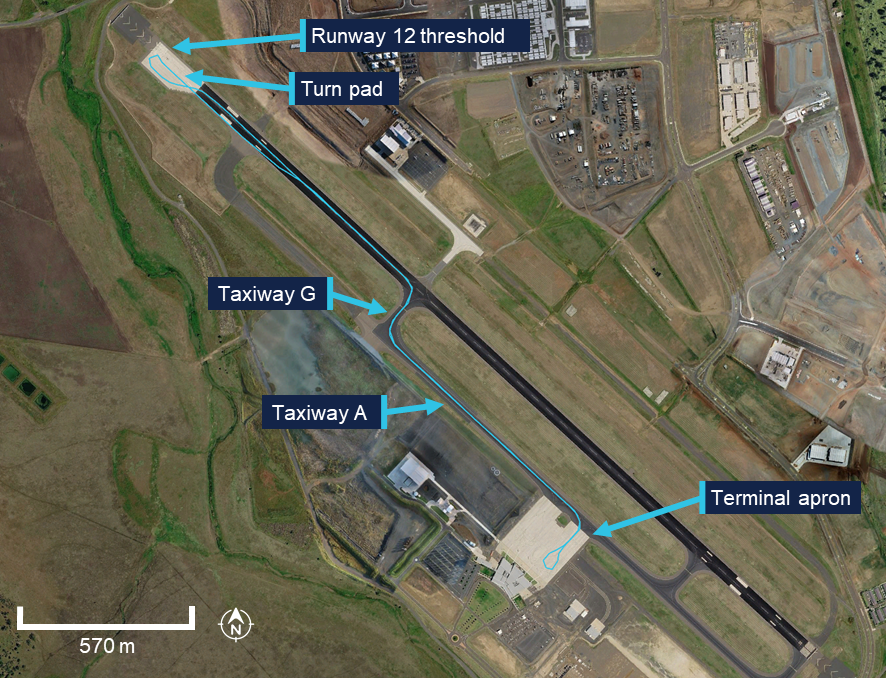
The aircraft taxied from the terminal apron at 2355 (23 February) on taxiway A, before entering and backtracking1 runway 12 at taxiway G. The pilot then taxied along the runway centreline towards the runway 12 threshold (Figure 1).
The flight was planned via instrument flight rules,2 the pilot notified Brisbane Centre of their intended departure from Wellcamp Airport and made appropriate radio broadcasts via the common traffic advisory frequency (CTAF), in preparation for their departure.
Figure 1: Aircraft movement overview
Source: Google Earth, annotated by the ATSB
The pilot recalled completing all the required take-off and line‑up checks while backtracking on the runway.
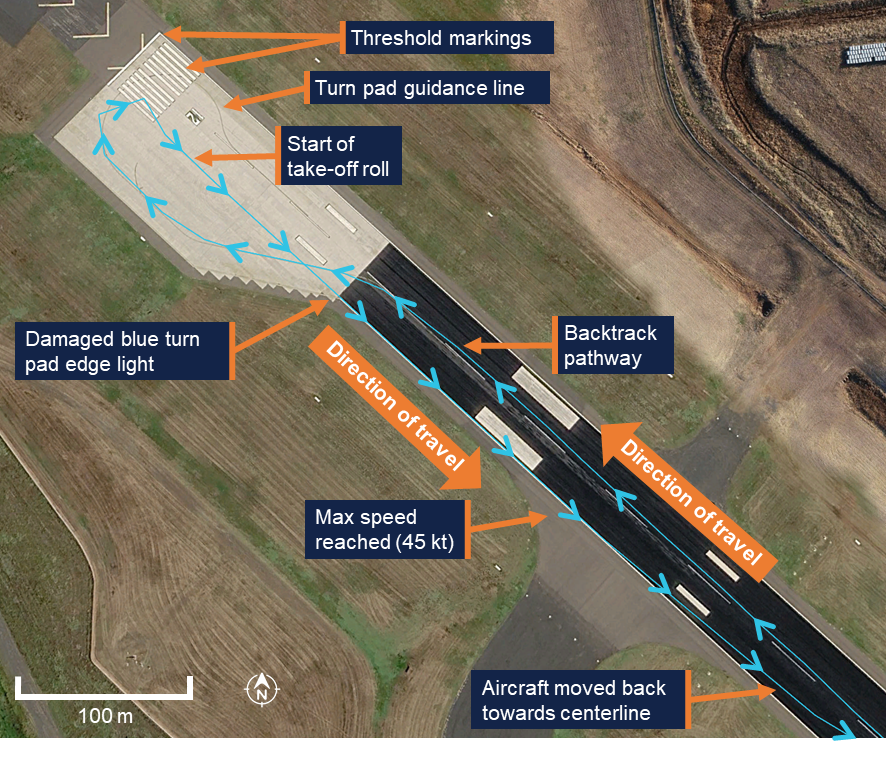
At the end of the runway, the pilot conducted a 180⁰ right turn. When entering the turn pad, the pilot initially turned left to allow room for the right turn, then part-way through the turn identified the right runway edge lights and anchored their alignment with these lights. Although recorded data indicated the aircraft initially followed the turn pad guidance line, the pilot reported that they did not recall seeing the turn pad guidance line or the threshold markings,3 and did not use the markings to orient the aircraft during the turn (Figure 2).
Figure 2: Aircraft movement details
Source: Google Earth, annotated by the ATSB
The aircraft was now in the centre of the concrete turn pad but misaligned with the white lights of the right runway edge for take-off. The pilot reported mistaking the right runway edge lights for centreline lights, however, no centreline lights were present at Wellcamp Airport.
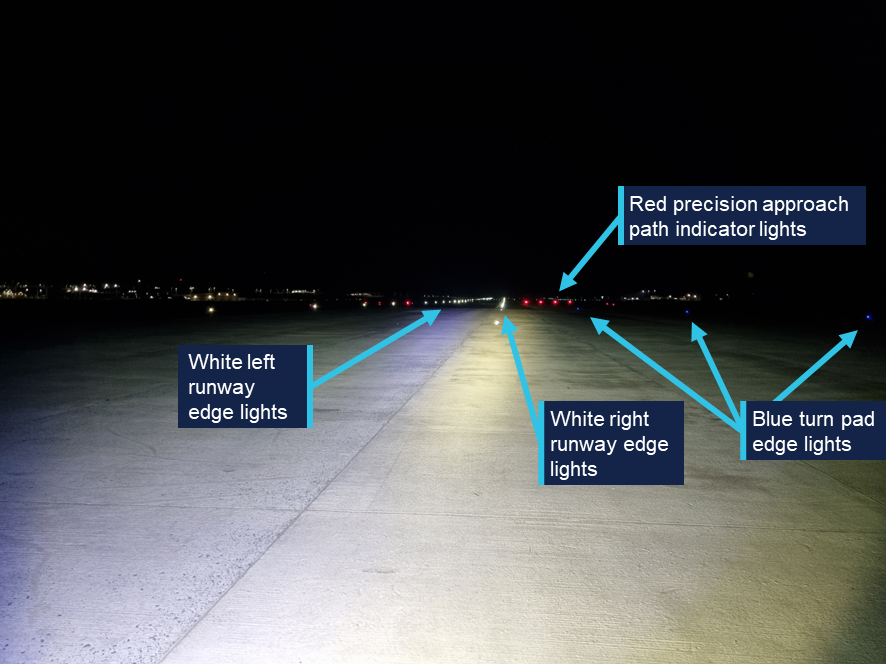
The pilot did not recall seeing the left runway edge lights which were about 45 m to the left of their lined-up position, nor did they recall seeing the blue turn pad node lights spaced in a diagonal direction along the start of the right turn node edge. They also did not identify the red precision approach path indicator (PAPI) lights close to the right runway edge lights (Figure 3).
Figure 3: Reconstructed view of the runway 12 lighting when lined up with the right edge
Source: Wellcamp Airport, annotated by the ATSB
The pilot commenced the take-off roll and at 0003 (24 February), the aircraft’s front wheel struck an elevated blue turn node light, leaving blue marks on the wheel tyre (Figure 4, right).
The pilot heard a bang during the take-off roll, detected the misaligned position, rejected the take-off and steered left towards the runway centreline. They then cancelled their flight plan, returned to the terminal apron and notified the aerodrome reporting officer (ARO), who subsequently conducted a runway inspection and identified the runway light damage (Figure 4, left).
Figure 4: Damaged blue turn node light (left) and blue marks on the aircraft front wheel (right)
Source: Wellcamp Airport (left) and RFDS (right)
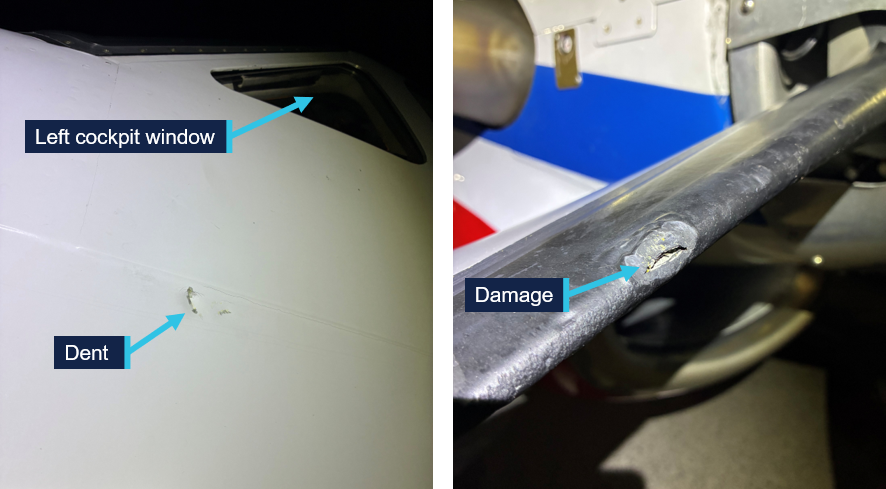
On impact with the front wheel, debris from the frangible4 blue turning node light caused minor damage to both aircraft propellers, and a dent to the aircraft fuselage below the left cockpit window (Figure 5).
Figure 5: Dent on aircraft fuselage (left) and damage to one of the left propeller blades (right)
Source: RFDS
The aircraft sustained minor damage which prevented further flight until repaired.
Context
Pilot information
The pilot held a Commercial Pilot (Aeroplane) Licence and a valid class 1 and 2 aviation medical certificate. Having joined the RFDS in 2016, the pilot reported a total flying time of 9,794 hours, with 5,691 of those being on the King Air B200. They reported operating at a range of aerodromes, most without centreline lights or turn pads. In contrast, their home base at Brisbane Airport had centreline lighting. The pilot’s logbook showed that they had conducted at least 1,790 night take-offs previously.
The ATSB assessed the pilot’s rostered sleep opportunity, reported sleep obtained, quality of sleep leading up to the flight, time on duty, as well as the time of the occurrence and concluded it was unlikely that the pilot had experienced a level of fatigue known to have an adverse effect on performance.
Aircraft information
VH-FDI was a Hawker Beechcraft Corporation B200C King Air (Figure 6) manufactured in the United States in 2010 and issued with serial number BL-162. The aircraft was a pressurised, low-wing, twin turbine-engine aircraft with retractable landing gear. The aircraft had a certified maximum take-off weight of 5,670 kg and could be operated by a single pilot.
Figure 6: VH-FDI, a Hawker Beechcraft Corporation B200C King Air
Source: RFDS
Meteorological information
Between 2230 and 0030, the Bureau of Meteorology meteorological reports for Wellcamp Airport identified an easterly wind at 10–11 kt, nil to few5 oktas of cloud with a base of 2,100 ft to 2,300 ft above the aerodrome, and visibility in excess of 10 km.
The pilot recalled that the lighting conditions during the taxi were dark, and there was no ambient airport lighting around the turn pad and runway 12 threshold areas to enhance visibility.
Airport information
Wellcamp Airport was a certified, non-controlled aerodrome, capable of supporting operations for aircraft as large as Boeing 747-800. Runway 12/30 was 2,870 m long and 45 m wide and featured a large runway turn pad6 near the threshold of runway 12. The turn pad included a paved area that was about 90 m wide and was offset on the right side of the runway. The runway threshold markings were situated on the turn pad pavement extending only to the width of the runway (Figure 2).
Line markings and lights on the runway and turn pad assisted pilots in turning and lining up their aircraft for departure. The white runway edge lights on the turn pad were flush with the surface of the runway and did not protrude. In contrast, the blue turn node lights were elevated. The markings and design were consistent with the requirements of the Civil Aviation Safety Authority Part 139 Manual of Standards.
The pilot reported that the painted lines and markings appeared less prominent in the dark ambient conditions at the time, while the right runway edge lights were highly noticeable.
Wellcamp Airport did not have, nor was it required to have, runway centreline lighting.
Operational information
The RFDS Flight Operations manual FCOM2 – B200 section 3.5.2 Line up procedure stated that:
The entry onto a runway is a critical phase of aircraft operation where observation of other aircraft and animals is a safety of flight issue, particularly at night.
Minimise the time spent with head and eyes inside the cockpit by completing as many of the ground checklists as practicable before entering and/or backtracking the runway.
There is no line up allowance promulgated in the AFM [Aircraft Flight Manual]. The aircraft should be lined up as close as practicable to the runway end.
The RFDS B200 Normal Procedures Checklist contained sections for ‘before take-off checks’ and ‘line up checks’.
However, neither of the above documents contained information about 180° turns, turns via turns pads, or specified centreline alignment checks prior to take-off. The pilot reported that specific turning techniques were not used in RFDS aircraft operations.
RFDS operations involving remote area medical emergency transport by their very nature, occur at unprepared, non-certified, and often narrow runways in addition to operations at larger all-weather, major airports.
Previous research
The ATSB research report Factors influencing misaligned take-off occurrences at night (AR-2009-033) was published in 2010 following the review of 24 misaligned take‑offs that occurred at night in Australia and overseas. The report identified 8 common and recurring factors that contributed to misaligned take-offs at night, including:
confusing lights/markings
extra runway pavement, and
no centreline lighting.
Related occurrences
Runway lighting events at Wellcamp
A review of the ATSB occurrence database found 2 runway lighting occurrences were reported on 15 March and 11 August 2024 at Wellcamp Airport whereby routine runway inspections identified tire marks and damaged edge lights on runway 12. The timing of the events and the aircraft involved could not be determined, however no damaged aircraft were reported at the time, and the occurrences were not investigated further by the ATSB.
Misaligned take-off
A review of the ATSB occurrence database found 5 reported incidents of similar misaligned take-offs in the 3 years prior to February 2026.
Between June 2023 and April 2024, 3 misaligned take-offs occurred at Perth Airport, Western Australia. Each occurred before first light and in all 3 incidents, when entering runway 06 from taxiway V, the pilots taxied past the turn onto the centreline and lined the aircraft up along the runway edge lighting on the far side of the runway to where they entered. The investigation found that in each incident, the pilots believed they had correctly aligned the aircraft with the runway centreline, prior to taking off. Several factors known to increase the risk of a misaligned take-off in the dark were identified from the investigation:
• In terms of the runway environment, there was an unlit and unmarked extended pavement area on each side of runway 06, which made the runway appear wider.
• In relation to the available airport lighting, the lead-on lights from the taxiway continued across the taxiway to the other side, meaning there was limited guidance when taxiing to the runway’s centreline.
• Recessed edge lights at the start of runway 06 could be mistaken for centreline lighting.
• There was limited ambient airport lighting around taxiway V and runway 06 to enhance visibility.
• The taxi lighting on one of the aircraft was reported by the pilots as being of limited benefit.
• The required runway markings were reported by 2 of the incident pilots to be difficult to see at night.
On 13 May 2024, at 0537 local time, the pilot of an Aero Commander 500-S aircraft conducted a take-off from Brisbane Airport runway 01 from the intersection of taxiway A7. While turning onto the runway, the pilot inadvertently lined up along the left side runway edge lighting instead of the runway centreline. During the take-off roll, the pilot recognised the aircraft was left of the centreline and took corrective action to reposition the aircraft on the runway. The underside of the aircraft had minor damage and several runway lights were also damaged.
The brief highlighted the complexity of the intersection with multiple lead-off lines into the runway as well the runway touchdown zone markings near the runway centreline markings that were both broken white lines.
At 1807 local time on the evening of 1 July 2025, a Beechcraft King Air B200, with 2 pilots on board was taxiing for take-off at Hobart Airport. During a 180° turn using the runway 30 turn pad, the aircraft struck a taxi light with the right propeller. The aircraft incurred damage to the propeller and a turn pad edge taxi light was also damaged.
The ATSB found that the pilot flying subconsciously mistook the blue taxiway edge lights and double yellow line on the edge of the turning pad as taxi centreline guidance. This resulted in the pilot deviating from the marked taxiway centreline towards the runway edge light, resulting in the propeller strike.
Safety analysis
Turn pad alignment
While taxiing on the turn pad at the end of runway 12, the pilot initiated a tighter right turn than the guidance line to line up for take-off. The pilot reported that this tight turn was an accepted operational practice as no specified operational procedure was provided for turn pads. The pilot also reported that they could not recall seeing the threshold markings, or the guidance line in the dark conditions, and stated that they were not intentionally using these features to guide the turn. As they progressed through the turn, they noticed the right runway edge lights and aligned the aircraft with these.
Following the turn, the aircraft was positioned in the centre of the 90 m wide turn pad with concrete visible to the right of the aircraft within the limits of the aircraft’s forward lights, which likely reinforced the pilot’s perception that they were lined up in the centre of the runway. While turn pads are both useful and necessary, they can increase the risk of misalignment at night where a wider paved area leads onto a narrower runway, as demonstrated via previous occurrences.
Centreline misidentification
When pilots taxi and take off during daylight conditions, they are normally presented with a wide range of visual cues by which they can navigate and verify their location. At night, however, the amount of visual information available is markedly reduced. Pilots rely more on the taxiway and runway lighting patterns presented to them and what can be seen in the field of the aircraft’s taxi and landing lights. For instance, the painted lines and markings were reportedly less prominent to the pilot, while the right edge lights were highly noticeable and the pilot anchored their orientation towards these lights, mistakenly identifying them as the runway centreline.
The pilot then missed several conflicting cues to alert them of the aircraft’s misalignment. Before completing the turn, the threshold markings were not identified by the pilot. Furthermore, the pilot did not identify the left runway edge lights 45 m away from the aircraft position on the turn pad. This would have contradicted their perception that the right edge lights were centreline lights, because only 2, rather than 3, parallel lines of lights were present.
Other available cues included the blue turn pad node lights spaced in a diagonal direction along the start of the right diagonal turn node edge. If perceived, the angle of the lights had the potential to alert the pilot to their alignment with the turn pad edge. Lastly, the pilot was unaware of the red precision approach path indicator (PAPI) lights visible to the right of the runway edge lights which indicated the area to the right of the aircraft was outside the runway surface.
None of the above cues sufficiently alerted the pilot to their misalignment with the right runway edge, and the pilot misperceived the right runway edge lights as the centreline lighting. The pilot then started the take-off roll from the turn pad, resulting in the aircraft accelerating faster than taxi speed by the time the edge of the runway was reached.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the misaligned take-off involving Beechcraft B200C King Air, VH-FDI, at Brisbane West Wellcamp Airport, Queensland, on 24 February 2026.
Contributing factors
The pilot diverged from the turn pad taxi centreline guidance which positioned the aircraft in the centre of the large turn pad which aligned with the right runway edge.
While lining up on the runway at night, the pilot misidentified the runway edge lighting as the centreline and collided with an edge light during take-off.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action by Royal Flying Doctor Service, Queensland Section to review operational procedures
The Royal Flying Doctor Service, Queensland Section, reviewed internal procedures for checklist management, entering and backtracking runways, conducting 180° turns, and requirements around identifying and lining up on runways.
The next version of the flight operations manual will be amended to:
require the ‘before take-off checklist’ be fully completed prior to entering the runway
include clear guidance on checklist interruption management, requiring that, when resuming a checklist, the pilot returns to the previously completed item before continuing.
Further, a notification will be issued to all pilots highlighting the importance of ensuring positive runway centreline environment is established before applying take-off power.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot flying
Royal Flying Doctor Service, Queensland Section
Wellcamp Airport
Civil Aviation Safety Authority
Airservices Australia
Bureau of Meteorology
Flightradar24.
References
Australian Transport Safety Bureau. (2010). Factors influencing misaligned take-off occurrences at night, Australian Transport Safety Bureau, Australian Government.
Civil Aviation Safety Authority. (2019). Part 139 Manual of Standards for Aerodromes, Civil Aviation Safety Authority, Australian Government.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot flying
Royal Flying Doctor Service, Queensland Section
Wellcamp Airport
Civil Aviation Safety Authority
Bureau of Meteorology
National Transportation Safety Board
Transportation Safety Board of Canada (TSB).
Submissions were received from:
Royal Flying Doctor Service, Queensland Section
Bureau of Meteorology
Transportation Safety Board of Canada (TSB).
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^Backtracking: to taxi on a runway-in-use, in the opposite direction to the aircraft’s take-off or landing direction.
^Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR).
^Threshold markings identify the beginning of the runway that is available and suitable for landing and take-off. They consist of a white line across the width of the runway and a series of white longitudinal stripes of uniform dimensions (often referred to as ‘piano keys’).
^Frangible: easily broken, shattered, or fragmented upon impact.
^Few: an amount of cloud covering the sky of between 1–2 oktas (eighths)
^A specially designed paved area at the end of a runway that allows aircraft to safely make a 180° turn, especially when the runway is too narrow for larger aircraft to turn around on their own.
Occurrence summary
Investigation number
AO-2026-062
Occurrence date
24/02/2026
Occurrence time and timezone
0003 Australia Eastern Standard Time
Location
Brisbane West Wellcamp Airport
State
Queensland
Report release date
15/07/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Ground strike, Rejected take-off
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Hawker Beechcraft Corporation
Model
B200C
Registration
VH-FDI
Serial number
BL-162
Aircraft operator
Royal Flying Doctor Service of Australia (Queensland Section) Limited
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Medical transport
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 21 November 2025 at approximately 1135 Central Standard Time, the pilot of a Piper PA‑32R was conducting a private flight from Numbulwar Aerodrome to Tindal Aerodrome, Northern Territory. During cruise the aircraft engine experienced a sudden loss of performance and subsequently failed at 2,500 ft above mean sea level.
The pilot undertook immediate engine failure actions and attempted multiple restarts but was unable to restore power. The pilot conducted a forced power-off landing in a clear area north of Bamyili, Northern Territory.
During the landing the aircraft impacted trees and uneven ground surfaces, resulting in substantial structural damage including a detached left wing tip and landing gear, a hole in the right wing and bent propellor blades. The pilot was able to self-evacuate and did not sustain any injuries.
Figure 1: Aircraft accident site
Source: Operator
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.