When required to stop at a level crossing, drivers must stop their vehicle, sight, and remain clear of trains, a final report from the ATSB’s investigation of a collision between a truck and The Ghan passenger train highlights.
A truck driver sustained serious injuries in the accident on 15 September 2024, which fortunately did not result in a derailment or injuries to any of the 260 people aboard The Ghan.
The passenger train was travelling towards Alice Springs, about 48 km south, when a road train (an A-triple comprising a prime mover towing two trailers full of cattle, and a third empty trailer) turned from the Stuart Highway onto The Garden Road, driving towards where the road and railway intersected at a level crossing.
Advance road warnings and passive controls, including a stop sign, were installed from the highway turn‑off and along The Garden Road to alert road users of the upcoming crossing.
About 270 m from the level crossing the locomotive driver sounded the horn for 2 seconds. Then, when The Ghan was approximately 120 m from the crossing, the crew observed the truck come into full view from behind roadside vegetation and progress toward the crossing.
“A video camera fitted to the front of The Ghan’s leading locomotive recorded that about 5 seconds before the collision the truck appears from behind the vegetation,” ATSB Director of Transport Safety Kerri Hughes said.
The train driver then sounded the horn but the truck did not stop and the front end of the prime mover impacted the right rear bogie of The Ghan’s trailing locomotive, resulting in substantial damage to the truck, and extensive damage to the locomotive’s air pipes, side ladder and front cowling.
“Fortunately, through the collision sequence, The Ghan remained upright and neither the locomotives nor carriages derailed. By the time the train had come to a stop, the lead locomotive was 1,380 m beyond the level crossing.”
The prime mover of the truck, meanwhile, came to rest on the field side of the track with engine bay components scattered along the rail corridor.
ATSB analysis of the video concluded the truck was still travelling between 22 and 28 km/h when it was 23 m from the level crossing.
“The truck driver had no recollection of The Ghan’s horn, which was sounded as the truck approached the stop sign. On seeing the leading locomotive, the truck driver rapidly applied brakes, but there was not enough distance to bring the truck to a stop before the collision,” Ms Hughes said.
Attending police concluded the truck driver was not wearing their seatbelt properly at the time of the collision, but it was unknown to what extent this contributed to their serious injuries.
“This accident demonstrates the importance of drivers obeying road rules around level crossings,” Ms Hughes said.
“The truck driver in this case reported they had not seen a train at this crossing before. They also reported that they would sometimes roll through level crossings, as it required significantly more time and effort to stop a loaded truck and then accelerate, than it did to roll through a crossing at low speed.”
ATSB calculations found that, given the rail line speed limit of 115 km/h, a road vehicle driver stopped at the stop line would have been able to see a southbound train about 49 seconds before it reached the crossing.
While the ATSB’s investigation found no issues with geometry or sightlines at the crossing, it did note some aspects of the level crossing’s passive controls were not to standard, or were faded.
“Nonetheless, there was sufficient signage and markings for road users to be aware of the crossing, and to bring their vehicles to a controlled stop before entering the crossing,” Ms Hughes said.
“Passive level crossings use controls that cannot physically prevent road users from entering the rail corridor. It is therefore paramount that road users obey all signs, particularly as a train cannot be stopped promptly when a road vehicle enters the crossing ahead of them.”
After the accident, the Northern Territory’s Department of Logistics and Infrastructure undertook a series of safety actions at the level crossing, including upgrading the approach signage, and refreshing the faded road line markings.
The interface agreement for the level crossing was also revised and renegotiated with the rail infrastructure manager, who committed to install updated signage to meet current standards.
On 24 April 2025, an MX Aircraft MXS single-engine light aircraft, registered N530RH, collided with terrain near the runway while on approach for landing at Langley Air Force Base near Hampton, Virginia, United States. The pilot sustained fatal injuries, and the aircraft was substantially damaged.
The United States National Transportation Safety Board (NTSB) commenced an investigation into the accident and requested assistance and the appointment of an accredited representative from the ATSB.
To facilitate this support and to provide the appropriate protections for the information, the ATSB appointed an accredited representative in accordance with paragraph 5.23 of Annex 13 to the Convention on International Civil Aviation and commenced an investigation under the Australian Transport Safety Investigation Act 2003.
On 2 July 2026, the NTSB released the final investigation report into this accident. Accordingly, the ATSB has concluded its involvement in the investigation. Any enquiries relating to the investigation should be directed to the NTSB.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the morning of 3 December 2025, the pilot of a Cessna Aircraft Company 340, with 4 passengers on board, departed Gnowangerup Airport for a private business flight to Jandakot Airport, Western Australia, under instrument flight rules (IFR).
After departure, as the aircraft was climbing through flight level 110 (11,000 ft above mean sea level), the left side cockpit window failed (Figure 1) and was ejected from the aircraft, which rapidly depressurised. The pilot assessed the situation, and after ensuring continued aircraft controllability, requested clearance to descend and traffic information from air traffic control. A descent to 8,000 ft followed and the aircraft was subsequently cleared for a direct track to Jandakot. With the aircraft stable, the pilot and passengers examined the exterior, and with no airframe or control surface damage evident, continued the flight to Jandakot, where the approach and landing were uneventful.
Figure 1: Failed left cockpit window
Source: Aircraft operator
Engineering information
The Cessna 340 is a 6-seat pressurised twin-engined aircraft with a maximum take-off weight of 2,717 kg. It was introduced in 1972, with production continuing until 1984, with 1,351 aircraft built. The 340 cockpit is framed with 4 acrylic (plexiglass) windows – 2 forward windscreens, each with adjacent side panel windows that have smaller, inward opening quarter vent panels. The initial design of the side windows with the vent panels has been found to be susceptible to cracking and in-flight failure, and in April/May 1982 Cessna introduced Service Kits SK340-26-1/2 and issued Service Information Letter ME82-18 for earlier build 340/340A aircraft. The letter and service kits provide instructions and equipment for the reinforcement of both pilot and copilot’s side windows by adding a diagonal brace (Figure 2) behind the quarter panel vent. This supports the larger window panel and reduces the pressurisation stresses that could lead to cracking or in-flight failure such as sustained in this incident. The service letter recommended compliance within the next maintenance period but not exceeding the next 200 flight hours.
Information from the aircraft owner advised that following the incident aircraft’s importation into Australia in mid-2021, the left and right window service kits had been procured, however due to pandemic-related delays, the kits had not yet been installed at the time of the occurrence.
Figure 2: Example of reinforced cockpit side window
Owners and operators of Cessna Aircraft Company 340 and 340A aircraft are advised to check their aircraft for the installation of cockpit side window reinforcing in accordance with Service Letter ME82-18. Where such reinforcing has not been installed, regular inspection of the windows and surrounds for evidence of cracking and degradation is recommended – particularly in areas around the quarter vent panel. Installation of Cessna Service Kit SK340-26-1/2 (or approved equivalent) is recommended.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2026-006
Occurrence date
03/12/2025
Location
5 km north-west of Katanning Airport
State
Western Australia
Occurrence class
Incident
Aviation occurrence category
Emergency/precautionary descent, Objects falling from aircraft, Windows
On 25 January 2026, at 0917 local time, the pilot and only occupant of a Robinson R44 Raven I helicopter, registered VH-8HR and operated by Whitsunday Air Services, departed Whitsunday Airport (Shute Harbour), Queensland, for nearby Daydream Island.
After departing, the helicopter climbed to an altitude of about 1,000 ft above sea level and shortly after crossing the coast, the pilot reported that the low rotor RPM horn sounded. The pilot recalled that they immediately reacted by increasing the throttle and lowering the collective lever which returned the engine and rotor RPM to within the normal operating range.
About 10 seconds later, the engine RPM briefly reduced a second time before a rapid increase of engine and rotor RPM which activated the high rotor RPM alert. The pilot recalled then switching off the engine governor to manually control the throttle inputs and maintain a constant engine RPM. They were able to stabilise the engine and rotor RPM for about 10 seconds, during this time they observed the engine was running rough with a significant increase in manifold pressure and the helicopter had begun an uncommanded descent.
The pilot reported that they began to slow the helicopter to the best rate of climb speed of 55 kt. While over water and beyond gliding distance from land they observed another engine RPM reduction, and elected to enter an autorotation, activated the emergency pop-out floats and ditched the helicopter onto the ocean. After ditching, the helicopter remained upright and the pilot reported they were uninjured. They were subsequently rescued by water police about 20 minutes later.
What the ATSB found
The right magneto distributor gear jammed when an internal rotating electrode became loose. This led to a mechanical failure of the gear teeth that affected the engine timing and subsequently reduced the helicopter power output.
The altered engine timing likely resulted in the number one cylinder exhaust valve being damaged. This resulted in a loss of compression in the cylinder and a further loss of power.
As a result of the power loss, the pilot was unable to maintain altitude, entered autorotation, and activated the emergency pop-out floats before conducting a successful forced landing onto the water.
The damaged magneto likely caused erroneous engine governor inputs which caused an engine and rotor RPM overspeed.
Safety message
The occurrence highlights the importance of pilot training and understanding of governor‑off throttle control and engine RPM management. The pilot’s decision to switch the engine governor off, and manually control the throttle, likely eliminated erroneous throttle inputs from the governor that caused the fluctuations in engine RPM.
Pilots are required to demonstrate competency in governor-off control during their biennial single engine helicopter flight reviews. Operators of Robinson R44 and R22 helicopters with engine governors should ensure that pilots have good understanding of the situations that could require manual throttle control and the techniques and precautions to manage those abnormal situations.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 25 January 2026, at 0917 local time, the pilot of a Robinson R44 Raven I helicopter, registered VH-8HR and operated by Whitsunday Air Services, departed Whitsunday Airport (Shute Harbour), Queensland, for nearby Daydream Island, where the pilot was to board 2 passengers for a scheduled scenic flight at 0930.
On departure from Shute Harbour, the helicopter climbed to an altitude of about 1,000 ft above sea level. However, shortly after crossing the coast, the pilot reported that the low rotor RPM horn sounded. The pilot recalled that they immediately reacted by increasing the throttle and lowering the collective1 which returned the engine and rotor RPM to within the normal operating range.
About 10 seconds later the engine RPM briefly reduced a second time before a rapid engine RPM increase, reaching 115.9% engine RPM and 114.2% rotor RPM, activating the high rotor RPM alert. The pilot recalled then switching the engine governor off to manually control the throttle inputs which maintained a constant engine RPM for about 10 seconds. The pilot observed the engine was running rough with a significant increase in manifold pressure and that the helicopter had begun an uncommanded descent the pilot was unable to arrest.
The pilot attempted to slow the helicopter to the best rate of climb speed of 55 kt. As the helicopter airspeed slowed to about 60 kt it was still descending and they were still unable to maintain altitude. The pilot reported that the engine RPM again reduced while over water and they elected to enter an autorotation. The helicopter was beyond gliding distance from land, and the pilot activated the emergency pop-out floats and conducted a ditching onto the ocean (Figure 1).
Figure 1: VH-8HR shortly after pilot was met by local water police
Source: Queensland Police
The helicopter landed and remained upright on the water without further damage. The pilot then transmitted a MAYDAY call which was received by a nearby fixed-wing aircraft that relayed the distress call to Brisbane Centre air traffic control. The pilot observed a knocking sound which they suspected was coming from the engine and shut the helicopter down.
The pilot remained in the helicopter and recalled that, about 20 minutes after the ditching, they were met by the local water police and transferred from the helicopter onto the police vessel.
The pilot was uninjured during the ditching and the helicopter was towed back to land upright on its floats before being transported to the operator’s maintenance provider.
Context
Personnel information
The pilot held a Commercial Pilot Licence (Helicopter) issued on 6 April 2023 having previously completed their initial flight training and a commercial licence in New Zealand. They had also successfully completed a gas turbine engine endorsement on 29 January 2024 and a low-level rating on 12 May 2025. They also held a class one medical certificate that was valid until 4 October 2026 with no restrictions.
The pilot had accumulated about 1,600 total hours flying helicopters including 835 hours flying the Robinson R44.
They had last completed a proficiency check flight with the operator on 12 June 2025 that included autorotation landings and governor malfunctions and was found competent by the operator.
The pilot had last completed helicopter underwater escape training on 4 June 2025, which was valid for 3 years.
Fatigue
The pilot reported they felt fully alert at the time of the occurrence having slept 9 hours in the previous 24 hours and 17 hours in the past 48 hours.
The ATSB considered that it was very unlikely that fatigue affected the pilot’s performance on the day of the occurrence.
Aircraft information
The Robinson Helicopter Company (RHC) R44, Raven I is a 4‑place, light helicopter, powered by a Lycoming O-540-F1B5, 6-cylinder, horizontally-opposed piston engine. It has a 2‑bladed main rotor system and a conventional 2‑bladed tail rotor. The R44 pilot operating handbook (POH) stated that at maximum continuous power, the engine operated at 2,718 RPM, which indicated as 102% on the engine tachometer display in the cockpit and also advised a transient limit of 105% RPM with a warning:
Intentional operation above maximum continuous speed (engine RPM) prohibited.
Engine power is displayed to the pilot via the manifold pressure gauge in inches of mercury. A placard on the pilot’s cyclic2 control displayed the maximum continuous power limit adjusted for pressure altitude3 and outside air temperature. It also included a transient 5-minute limit of an additional 1.6 inches of manifold pressure above the continuous power limit for maximum take-off power. Conditions on the day indicated a maximum continuous power limit of about 24.1 inches and a 5-minute maximum take-off limit of 25.7 inches.
The POH also stated the safe operational rotor RPM range is between 90 and 108%, which is marked with a green arc on the rotor RPM tachometer.
The R44 helicopter is equipped with a low rotor RPM horn and caution light which both activated when the rotor RPM dropped below 97%. VH-8HR was also equipped with a high rotor RPM alert that sounded through the pilot’s headset and activated when the rotor RPM was approaching 108%.
VH-8HR was manufactured in the United States as serial number 2751 in 2023 and had flown a total of 1,116.8 hours prior to the occurrence flight. The operator had been the registration holder since July 2023.
VH-8HR was equipped with emergency pop-out floats manufactured by DART Aerospace. A helium‑filled cylinder was located under the front left seat that provided the means for float inflation. The pop-out floats are activated when the inflation lever on the pilot’s collective control is squeezed (9 kg of force required).
Engine
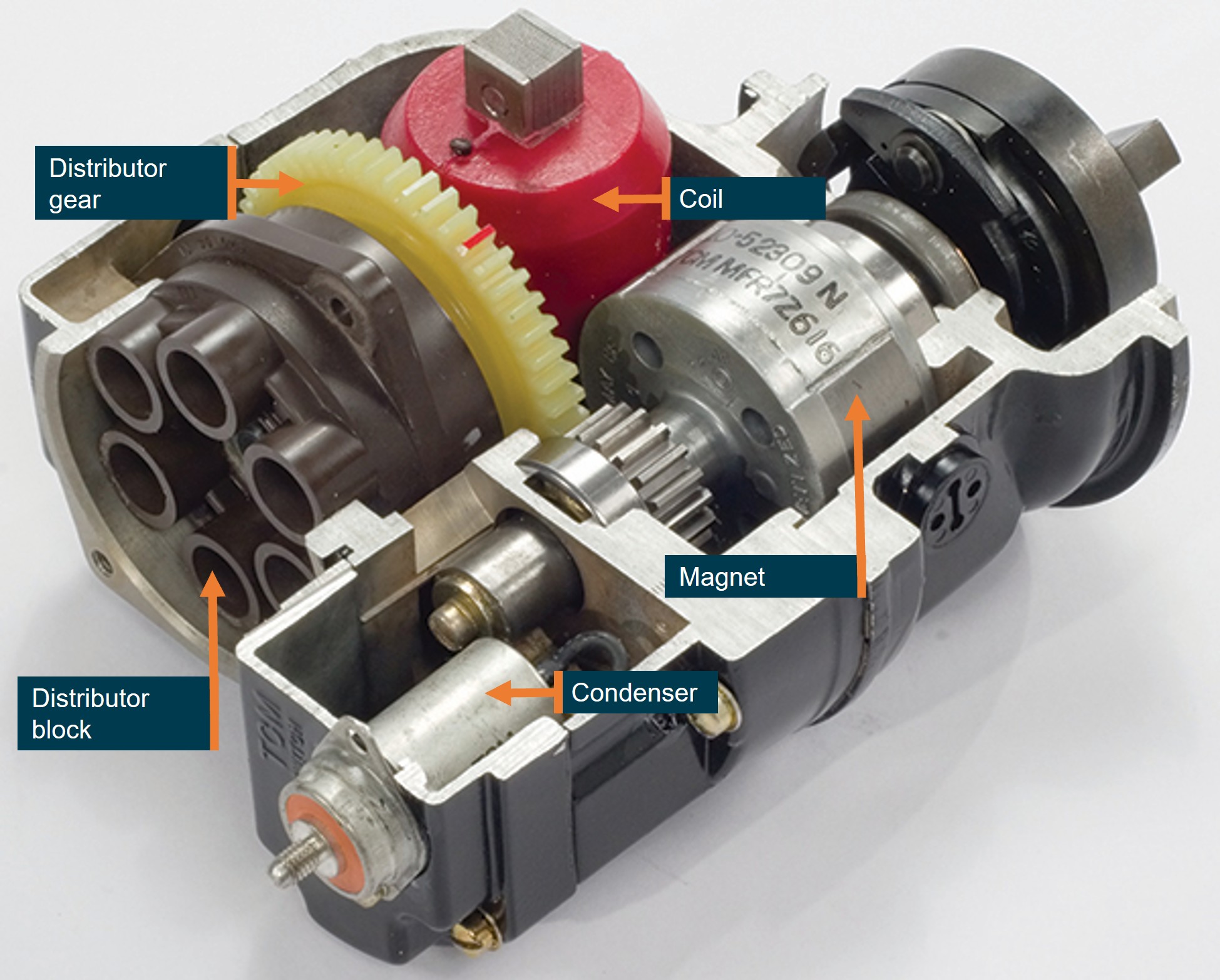
At the time of the occurrence, the Lycoming engine was fitted with 2 magnetos (part number 10-6006-46-201), manufactured by Continental Aerospace Technologies (CAT), that produced high voltage for the 12 spark plugs. Fitted to the distributor gear of each magneto (Figure 2) was a rotating electrode that provided the timing of the electrical energy to the distributor block4 and then to the relevant spark plug via a high-tension lead.
Figure 2: Sectioned view of an exemplar magneto
This magneto is similar to the one that was fitted to VH-8HR. Source: Aviation Safety Magazine, annotated by the ATSB
The R44 helicopter is equipped with an automatic throttle governor designed to assist pilots in controlling RPM under normal flight conditions.
The POH provided a description of the governor operation.
The governor maintains engine RPM by sensing changes and applying corrective throttle inputs through a friction clutch which can be easily overridden by the pilot. The governor is active only above 80% engine RPM and can be switched on or off using the toggle switch on the end of the right seat collective.
The R44 throttle governor takes its signal source from the tachometer breaker contact (points) assembly within the engine-right5 magneto and provides throttle inputs to maintain the engine RPM at 102%. Above 112% RPM, the governor is inactive.
R44 magneto changes
Prior to January 2021 all piston-engined RHC helicopters were fitted with dual magnetos. In 2020 RHC received United States Federal Aviation Administration (FAA) approval to replace the engine-left magneto with an electronic ignition system (EIS) manufactured by Lycoming. The July 2020 Robinson newsletter described the new EIS:
The EIS installation replaces the left starting magneto. The remaining right magneto provides redundant ignition and eliminates the need for a backup power supply. EIS has very high spark-energy for easy engine starts and eliminates internal moving parts for increased reliability.
On 13 February 2024, Lycoming issued mandatory service bulletin 656 (revised to 656A in April 2025) that stated:
Lycoming has identified an internal wear issue with some EIS units used on 6-cylinder engines in rotary wing applications. This internal wear progresses over time and can lead to engine power fluctuations. This bulletin requires the replacement of EIS units in 6-cylinder helicopter applications. Affected 6-cylinder EIS part numbers are 66K6D3SN-03, 66K6D3SN-02, and 66K6D3SN-01.
The service bulletin required the replacement of the EIS every 50 flight hours in helicopters with 6-cylinder engines due to the wear issues.
On 24 February 2024 RHC released kit instructions KI-272-5 for the installation of Bendix Style magnetos that replaced the EIS and avoided the required 50‑hour EIS replacement.
Maintenance history
On 31 May 2024, the operator’s maintenance provider replaced the EIS (engine-left) on VH-8HR using the RHC KI 272-5 magneto conversion kit. At that time the helicopter had flown 389.7 hours flight time.
On 8 November 2024, and 585.4 hours flight time, the maintenance records showed the engine-left magneto was unable to be timed to the engine and was replaced.
On 7 April 2025, the helicopter had accumulated 781.2 hours and underwent scheduled maintenance that included a 500-hour inspection of the distributor gear within the magnetos. The maintenance organisation reported nil defects with the distributor gear during this inspection.
On 17 December 2025, the helicopter had accumulated 1,066.5 hours, and maintenance records showed a pilot had reported that the engine ran rough on the engine-left magneto. One high-tension lead was found to be unserviceable and the lead was repaired and a subsequent engine run found the engine operated normally.
The magnetos had been inspected every 100 hours as per CAT service bulletin SB 643C part 1 and magneto timing had also been completed as per Lycoming service bulletin SB 183A during the last five 100‑hourly inspections.
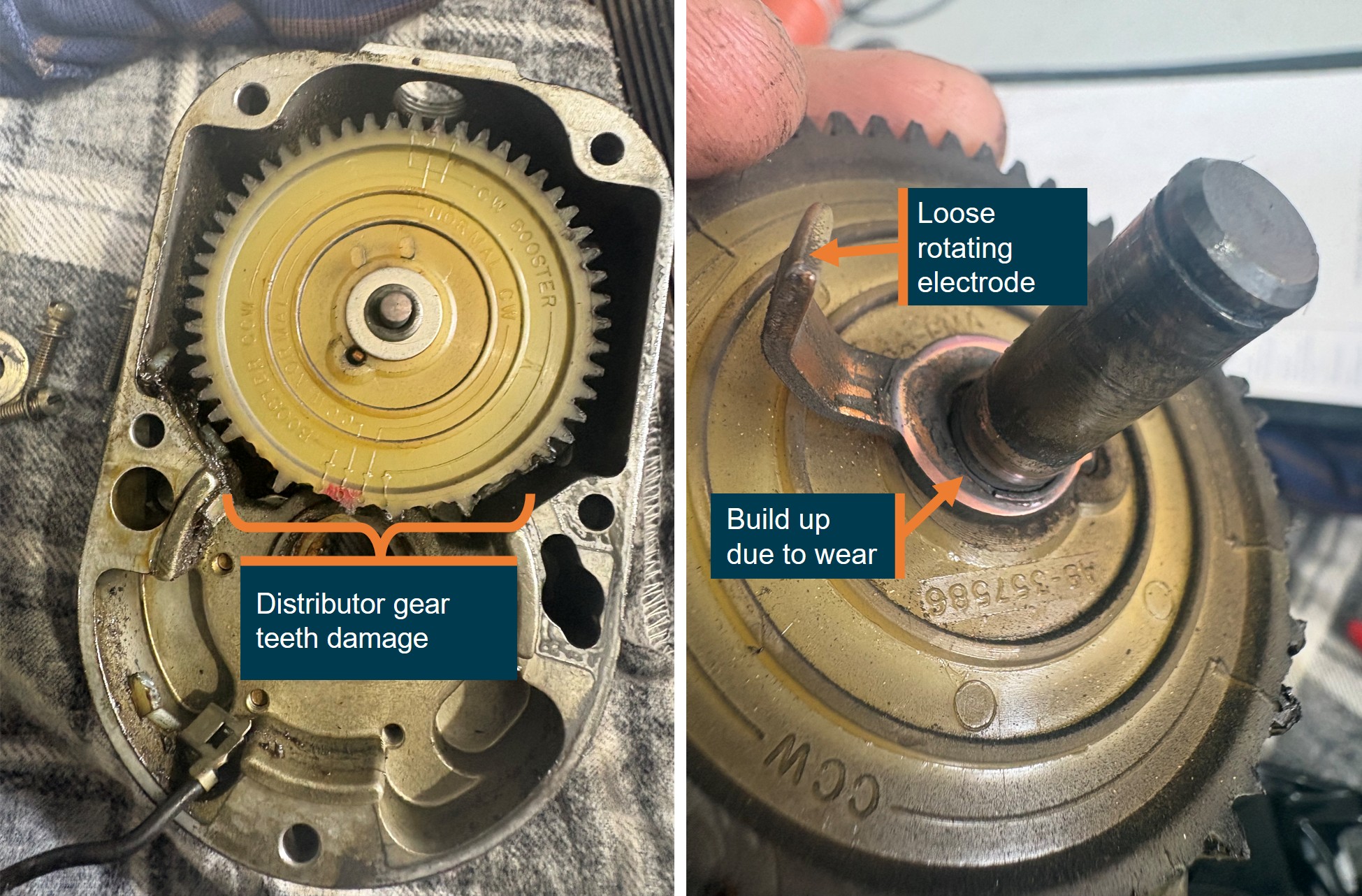
Following the occurrence, the operator’s maintenance provider inspected the engine‑right magneto and identified that the rotating electrode on the distributor gear had come loose and subsequently contacted the distributor block, jamming the gear which resulted in numerous gear teeth being stripped (Figure 3).
Source: Whitsunday Air Services, annotated by the ATSB
The engine-right magneto had been fitted to the helicopter for about 18 months and 727 flying hours. The magneto distributor gear was last inspected on 7 April 2025. After that inspection, the helicopter operated a further 335.6 hours before the magneto failed. At the time of the occurrence, the 500-hour magneto distributor gear inspection was due in 164.4 hours flying time.
Maintenance records also indicated that individual cylinder compression checks had been completed at 100-hourly service intervals with nil defects reported.
The post‑occurrence engine inspection also identified damage to the exhaust valve on the number one engine cylinder, with a compression test indicating nil compression. The maintenance organisation reported the erosion damage was likely from environmental conditions, fuel and exhaust deposits. The maintenance organisation identified that the combination of a magneto failure and lack of compression in the cylinder would have resulted in a substantial power loss.
CAT reviewed the supplied images and a summary of the occurrence and advised that the distributor gear rotating electrode could detach due to:
• Mechanical fatigue or vibration: High cyclic loading and torsional vibration in the O‑540 engine can weaken the electrode attachment over time.
• Improper staking or attachment during a prior overhaul: If the rotor assembly was not correctly staked, riveted, or assembled during the last 500‑hour inspection, the electrode can loosen prematurely.
• Internal contamination or sudden rotor binding: Foreign material or gear debris can momentarily jam the rotor, placing abnormal shear loads on the electrode.
• Heat distortion: Excessive magneto temperature (due to lean running, under‑cowl heat, or advanced timing) can warp the rotor plate or insulator, stressing the electrode until it separates.
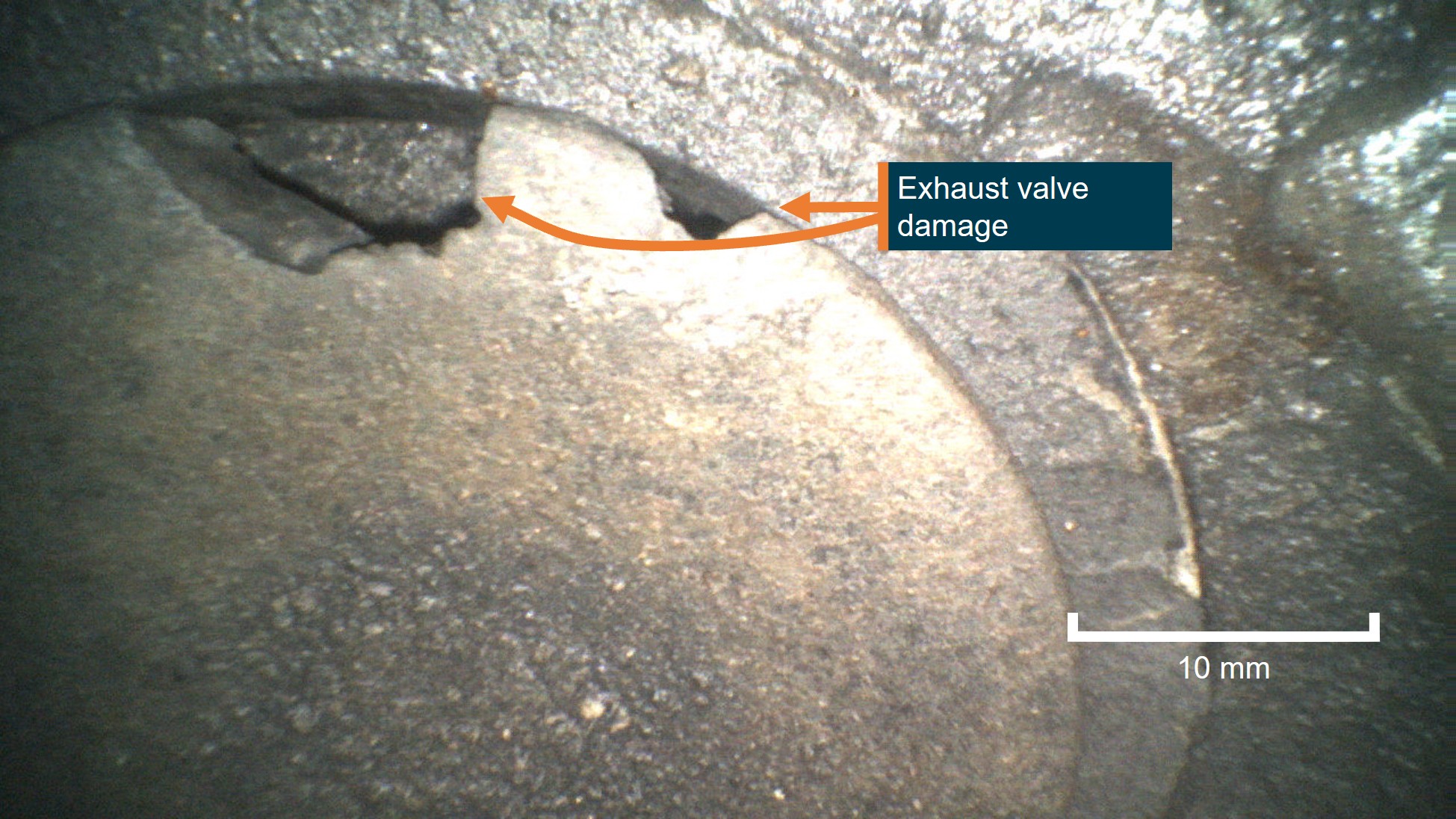
CAT also provided an assessment of the exhaust valve damage (Figure 4) stating that it was entirely consistent with late, weak or erratic ignition timing and provided the following explanation:
A jammed magneto or slipping distributor gear causes late or erratic ignition timing. When ignition occurs too late:
• Combustion continues as the exhaust valve opens, exposing the valve face to extremely hot combustion gases.
•This leads to localized overheating, erosion, and burning of the valve edge, matching the borescope damage observed on No. 1 cylinder.
• Intermittent or weak ignition can also cause backfiring or detonation, further overstressing the exhaust valve and increasing temperature spikes.
Late timing = combustion into exhaust stroke → valve overheating → valve burning.
Figure 4: VH-8HR cylinder one exhaust valve
Source: Whitsunday Air Services, annotated by the ATSB
Meteorological information
Meteorological information recorded at 0900 local time at Hamilton Island Airport, 19 km south-east of the ditching location showed:
wind from 110° at 20 kt
visibility greater than 10 km
cloud broken6 at 2,200 ft and overcast at 2,700 ft
temperature was 27° C and dew point 24° C
QNH7 of 1,010 hectopascals.
The pilot estimated that the wind strength on the day was 10–15 kt from the south-east and recalled the sea state was about 0.5 m of swell when they landed on the water.
Recorded data
The helicopter was equipped with an RHC installed engine monitoring unit (EMU). The user guide for the EMU stated:
The EMU monitors engine speed, rotor speed, engine oil temperature, cylinder head temperature, manifold pressure, ambient pressure, and outside air temperature. Data is stored once per second. If the EMU detects an engine or rotor parameter outside of operating limits, an exceedance record is created and data is stored at a higher rate of 15 times per second during the exceedance event.
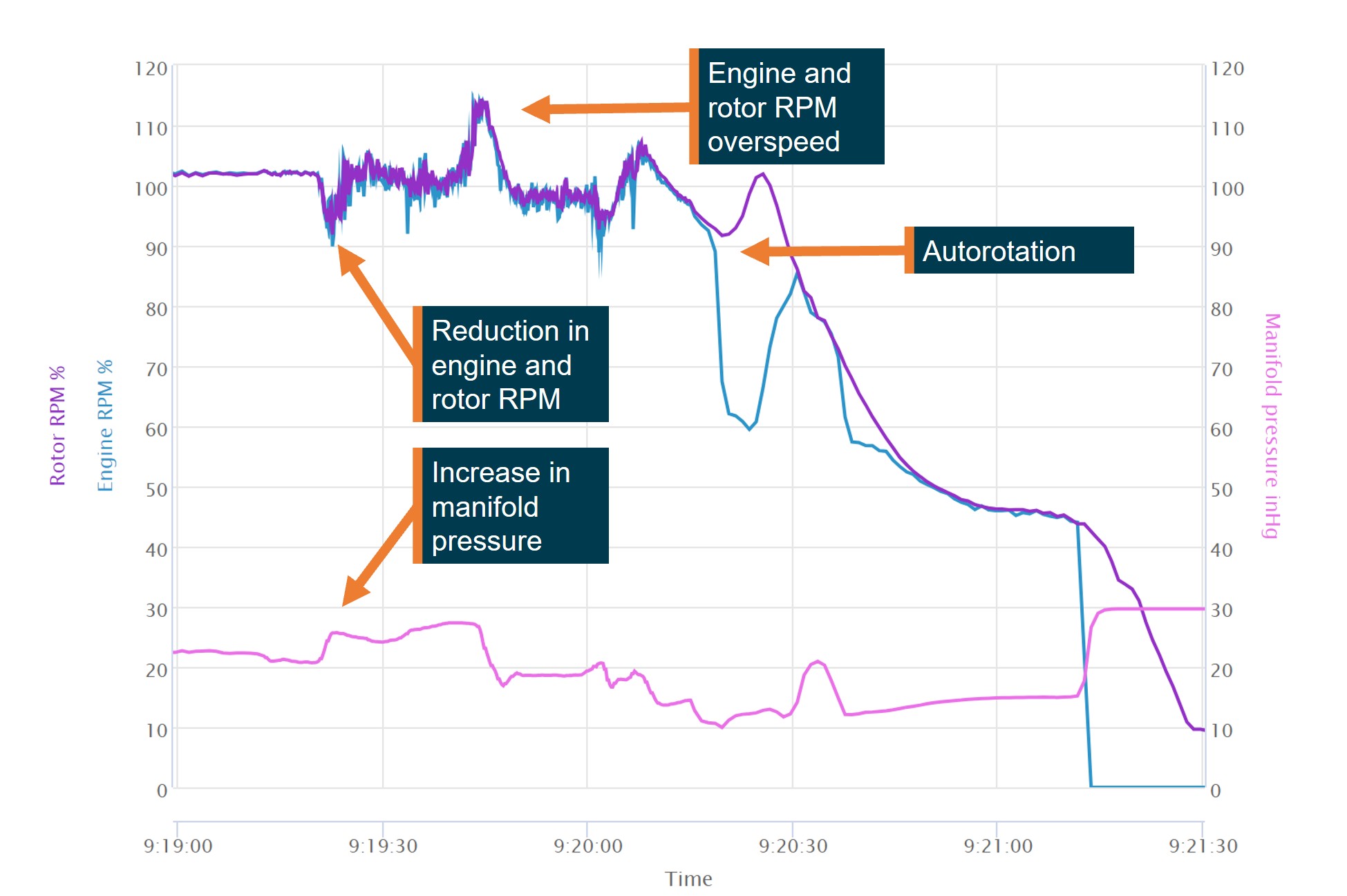
The EMU data (Figure 5) recorded at 0919:208 showed an engine RPM reduction from the normal 101–102% RPM operating range reducing to about 94% RPM before increasing again. A further momentary reduction in engine RPM was recorded about 10 seconds later and then returned to within the normal operating range before then rapidly increasing, peaking at 115.9% engine RPM. The increase in engine RPM also resulted in a rotor RPM overspeed, peaking at 114.2%. The pilot reported after the overspeed that they switched the governor off and manually controlled the throttle.
The engine RPM then reduced and stabilised at about 98% for about 10 seconds. At about 0920 the engine RPM again dropped below 90% and then increased to about 104%.
At about 0920:20 the engine RPM reduced to about 62%, while the rotor RPM remained above 90% and increased to 100%, consistent with the pilot closing the throttle and conducting an autorotation before flaring to land on the water.
Engine manifold pressure recorded by the EMU on departure indicated pressure within normal operating range. At about 0919:20, at a similar time to the first engine RPM reduction, the manifold pressure increased above 25 inches before it momentarily reduced to about 24 inches, then increased and peaked at about 27.5 inches.
Figure 5: VH-8HR engine monitoring unit data
Source: ATSB
The helicopter was also equipped with a cockpit video recording camera, as optional equipment from the RHC factory. The camera featured both internal and external storage, however no external storage was fitted for the occurrence flight. The internal storage recorded continuously and was sufficient for 3 hours of recordings before being overwritten. During the subsequent post‑occurrence inspection it was identified that the internal camera battery had failed and the last recorded data stored was from June 2025. It was reported that previous internal battery failures had been identified by RHC, and a requirement for battery replacement to be carried out yearly had been added to the maintenance schedule in August 2025. The battery on this device had not reached the required replacement date.
It was also identified during the inspection that the internal camera mountings had failed, with the potential to impact the data quality and footage available.
Survivability
MAYDAY transmission
Following the successful forced landing, the pilot reported that they broadcast a MAYDAY transmission on the local area common traffic advisory frequency (CTAF). A nearby fixed‑wing aircraft heard the transmission and relayed the details of the MAYDAY to Brisbane Centre air traffic control. The pilot recalled that their workload during the management of the event prevented an earlier MAYDAY call being made.
Lifejackets and emergency locator transmitters
The pilot wore a constant-wear vest style lifejacket and felt no need to inflate the lifejacket at any point. The lifejacket was equipped with pockets and was where the pilot kept a personal survival emergency locator transmitter (ELT) that was an operator requirement to be carried. The onboard automatic ELT fitted to the helicopter was not activated during the occurrence.
Communication
The pilot reported they were able to communicate with the operator’s base on Hamilton Island via VHF radio while awaiting rescue and made several phone calls to assist with the coordination of the retrieval of the helicopter.
Rescue
The pilot reported about 20 minutes after the ditching, local police arrived by boat and they transferred to the police boat. They remained on station to monitor the helicopter until a larger vessel arrived that towed the helicopter to shore.
Similar occurrences
Partial engine power loss and ditching involving Robinson R44, VH-WRR (AO‑2017‑110)
On 8 November 2017, the pilot of a Robinson R44 ditched about 49 km north of Hamilton Island Airport, Queensland. In addition to the pilot, there were 3 passengers on board.
When about 40 minutes into the flight, on return to Hamilton Island, the pilot heard the engine sound decrease and noted that the helicopter was unable to maintain the cruise altitude of 1,000 ft. The pilot reported that the indicated main rotor revolutions per minute (RPM) decreased and the low rotor RPM horn activated. The engine RPM indication was also oscillating throughout the range. In response to the low RPM horn, the pilot increased throttle and again raised the collective. The rotor RPM initially spiked and then decreased with associated re-activation of the low rotor RPM horn. The engine RPM gauge continued to oscillate and the helicopter could not maintain altitude. The pilot noticed the engine noise was changing with the fluctuations in the indications. While there appeared to be no observable damage sustained to the helicopter, it later sank and was unable to be recovered.
A maintenance logbook entry around 2 weeks prior to the accident noted that the helicopter had intermittent tachometer/governor fluctuations. The right magneto points were found to be out-of-tolerance and adjusted. A ground run to test the adjusted magneto was completed satisfactorily.
Post-accident discussions between the manufacturer, operator and maintenance provider resulted in a consensus of opinion that the power reduction was associated with either a governor control failure and/or a compromised engine RPM signal from poor tachometer points.
On 15 June 2018, at 1050 local time, a Robinson R44 conducting a charter flight experienced an engine RPM governor failure.
The pilot was not certain of the cause of the drop in RPM. Rather than turning off the governor as the flight manual instructs for governor failure, the pilot elected to manually control engine RPM by overriding the clutch in the governor.
The aircraft’s magnetos had undergone a 500-hour service immediately prior to the scenic charter flight. An engineering inspection following the incident flight found that a problem with the tachometer points of the magneto caused the governor to read a higher RPM than existed and wind down the throttle, subsequently slowing the rotor system.
Safety analysis
Magneto damage
Since the magneto distributor gear was last inspected, VH-8HR had flown 335.6 hours and it was due to be re-inspected in 164.4 hours flying time.
The reason for the loose electrode on the distributor gear was not able to be determined, however the magneto manufacturer indicated that the rotating electrode could become loose due to fatigue, vibration, incorrect installation, or heat damage.
The loose electrode likely caused the distributor gear to jam, damaging the gear. Either due to this damage or a result of the jamming, the timing of the electrical supply to the spark plugs was affected and caused the engine to misfire.
Exhaust valve damage
The helicopter had accumulated 1,116.8 total flying hours and had mostly been operated throughout the Whitsunday Islands and Great Barrier Reef, exposing the helicopter to a corrosive salt air environment. The helicopter’s maintainer reported erosion damage to the valve sealing face following the occurrence, likely due to the corrosive operational environment, fuel or exhaust deposits.
The magneto manufacturer, Continental Aerospace Technologies (CAT), stated the damage to the valves was consistent with late ignition timing due to the damaged magneto. The late timing of the ignition resulted in combustion during the exhaust stroke and therefore overheated the exhaust valve resulting in burning, increasing the likelihood of premature failure.
The damage to the exhaust valve prevented adequate compression during the combustion cycle in the cylinder, leading to a reduction of power.
Forced landing
As a result of the damaged magneto and damaged exhaust valve, the power available was insufficient for the pilot to maintain altitude.
Without sufficient power to maintain altitude, the pilot’s decision to close the throttle and enter autorotation removed the threat of further engine RPM fluctuations during the landing. During the autorotation the rotor RPM increased from about 92% to more than 100% RPM, therefore, the increased inertia in the rotor system likely assisted the pilot to conduct a controlled ditching without further damage to the helicopter or emergency pop‑out floats.
The pilot activated the emergency pop-out floats during the autorotation which allowed the aircraft to remain upright on landing and remain buoyant. They were then able to take refuge in the helicopter until first responders arrived.
Erratic governor control
The Robinson R44 engine-right magneto provided electrical signal to the engine tachometer in the cockpit. The engine governor applied throttle inputs to maintain a constant engine RPM.
The damaged right magneto likely caused the engine tachometer to incorrectly read the engine RPM and therefore throttle inputs made by the governor were not accurate and resulted in engine RPM fluctuations. The fluctuations resulted in several reductions in engine RPM and one significant engine RPM increase which increased both the engine and rotor RPM over the manufacturer’s limits, increasing the likelihood of damage to the helicopter.
The pilot reported that following the overspeed, they elected to switch the governor control off and fly the aircraft using manual throttle control. The engine monitoring unit (EMU) data showed a 10‑second period where the engine and rotor remained at about 98% RPM, consistent with the pilot manually controlling the throttle. The data then showed a further, momentary engine RPM reduction. The governor switch position was not a parameter recorded by the onboard EMU and therefore the ATSB was unable to determine if the cause of the further reduction was caused by inputs from the governor.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the power loss and ditching involving Robinson R44, VH-8HR, 19 km north-west of Hamilton Island, Queensland, on 25 January 2026.
Contributing factors
The right magneto distributor gear was jammed by a loose electrode. This led to a mechanical failure of the gear teeth affecting the engine timing and subsequently the helicopter lost power.
The altered engine timing likely resulted in the number one cylinder exhaust valve being damaged. This resulted in a loss of compression and a further loss of power.
The pilot was unable to maintain altitude and entered autorotation, activated the emergency pop-out floats and conducted a successful forced landing onto the water.
Other factors that increased risk
The damaged magneto likely caused erroneous governor inputs and therefore an engine and rotor RPM overspeed.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot of the accident flight
operator
Civil Aviation Safety Authority
Queensland Police Service
aircraft manufacturer
magneto manufacturer
recorded data from the engine monitoring unit on the aircraft.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of the accident flight
Whitsunday Air Services
Heli Biz
United States National Transportation Safety Board
Robinson Helicopter Company
Continental Aerospace Technologies
Bureau of Meteorology
Civil Aviation Safety Authority.
Submissions were received from:
Whitsunday Air Services
Heli Biz.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Footnotes
1
^ A primary flight control that collectively adjusts the pitch on the main rotor blades.
2
^ Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
3
^ Pressure altitude is the altitude corrected for atmospheric pressure.
4
^ A distribution block is a device used to consolidate and distribute electrical power from a single source.
5
^ This term is derived from the way the engine is fitted in fixed-wing aircraft with a front‑mounted propeller. The engine is fitted facing aft in the R44, therefore engine-right is on the left side of the helicopter.
6
^ Broken: 5–7 okta of cloud cover. An okta is a unit of measurement used to describe the extent of cloud cover (1–8).
7
^ QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
8
^ A timing correction was made to align with ADS-B data. Timing is initially set by a technician and is not linked to GPS or other sources. Additionally, while there is an internal clock, this can drift over time.
Occurrence summary
Investigation number
AO-2026-009
Occurrence date
25/01/2026
Occurrence time and timezone
09:22 Australian Eastern Standard Time
Location
19 km north-west of Hamilton Island
State
Queensland
Report release date
14/05/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Abnormal engine indications, Ditching, Engine failure or malfunction
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R44
Registration
VH-8HR
Serial number
2751
Aircraft operator
Whitsunday Air Services Pty Ltd
Sector
Helicopter
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Other general aviation flying-Ferry flights
Departure point
Whitsunday Airport (Shute Harbour), Queensland
Destination
Daydream Island Helicopter Landing Site, Queensland
The ATSB is investigating a collision with terrain involving a Cessna 210N, registered VH-RDH, 15 km south-east of Goolwa Airport, South Australia, on 6 February 2026.
During a flight, the aircraft collided with water and was destroyed, fatally injuring the 3 occupants.
The ATSB has commenced the examination and analysis of the initial evidence collected.
A preliminary report, which detailed the factual information established during the evidence collection phase, was released on 4 March 2026 (see the adjacent tab).
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Preliminary report
Report release date: 04/03/2026
This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 6 February 2026, at about 1608 local time, a Cessna 210N, registered VH-RDH, departed from Goolwa Airport, South Australia, with 3 persons on board for a private local area flight. The persons on board comprised a flight instructor in the front right seat, a commercial pilot licence holder in the front left seat and a passenger, who held a recreational pilot licence, in the second row left seat. The purpose of the flight was for the commercial pilot licence holder to accumulate Cessna 210 flying experience. This was conducted under the supervision of the aircraft operator’s head of training and checking, who was the onboard flight instructor.
Air Traffic Control (ATC) radar detected the aircraft at 1609:45 and the ATC system started generating a track for the aircraft at 1609:50 at an uncorrected altitude[1] of 1,100 ft and groundspeed of 93 kt. Calculated barometric altitude[2] started at 1609:58 and recorded the aircraft at 1,275 ft and a groundspeed of 93 kt.[3] Goolwa Airport CTAF[4] recordings captured a runway 19 upwind departure call from the instructor, that they were climbing through 1,000 ft to 1,500 ft and tracking coastal to the east. The departure call was followed by an amendment that the aircraft was climbing to 2,500 ft for smoother air.
ATC radar tracked the aircraft as it followed the coast to the east at about 2,350 ft for about 5 minutes at about 130 kt. The aircraft then commenced a right turn through south to track west along the coast back towards the mouth of the Murray River (Murray Mouth) at about 136 kt. As the aircraft approached Murray Mouth, the altitude increased and reached 3,375 ft at 1620:52. As the aircraft climbed above 3,000 ft the tracking data shifted slightly south (at 1620:17) and the speed reduced to 74 kt while maintaining a westerly track.
At 1620:57 the aircraft was recorded at an uncorrected altitude of 2,700 ft, still on a westerly track, and the speed had reduced to 66 kt. The ATC system then ceased tracking the aircraft, but it was captured a final time on radar at 1621:05, at an uncorrected altitude of 1,200 ft. Figure 1 depicts the accident flight with 4 data points annotated.
Figure 1: Air traffic control generated track with data points annotated
Airservices Australia generated tracking data for the accident flight with ATSB numbered data points – at data point 2 the aircraft has climbed above 3,000 ft and the track has shifted to the south. Source: Airservices Australia, annotated by the ATSB
A witness located on the west side of Murray Mouth observed the aircraft in a steep descent and used their phone to record the final seconds of the descent. The footage indicated the aircraft was in a left turn spin just prior to colliding with the water in a steep nose down and left-wing low attitude, intact with the landing gear retracted. Several witnesses reported to the ATSB that the engine sounded like it was running until the collision. The 3 occupants were fatally injured and the aircraft was destroyed.
Wreckage inspection
The wreckage was retrieved from the water by South Australia Police prior to the ATSB’s arrival at the site on the afternoon of 7 February 2026. The wreckage was heavily fragmented and missing the engine, propeller, wings, vertical fin and rudder. The main gear was found down and locked and the nose gear retracted. Several seat belts had been cut by emergency services personnel to remove the occupants.
The left front seat was attached to the seat rails and fitted with an inertial reel strap to prevent inadvertent movement in flight. The strap was cut to remove the seat from the aircraft. The front right seat had separated from the seat rails, but the seat lock pins were in the down (locked) position and appeared undamaged. The second row left seat had separated from the floor of the aircraft but was contained within the wreckage. The second row right seat was not fitted. The rear seats (third row) were attached to the airframe.
The elevator control cables were identified, and the elevator trim surface was present and attached to the elevator. The elevator was free to move in the correct sense. Measurements of the elevator trim position were made, and an elevator control cable turnbuckle was removed and, in addition to the aircraft global positioning system unit, retained for further examination.
Further investigation
To date, the ATSB has:
inspected the wreckage and the departure airport’s fuel supply
recovered and retained equipment for further examination
collected records from the aircraft operator and Civil Aviation Safety Authority
collected air traffic control and airport data
collected electronic flight bag data
interviewed witnesses and other Cessna 210 pilots.
The investigation is continuing and will include:
further interviews
a review of aircraft operator and Civil Aviation Safety Authority records
analysis of witness videos, photographs, airport data and interviews
analysis of data from air traffic control, electronic flight bags and from equipment recovered from the aircraft.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB acknowledges the assistance provided by South Australia Police and State Emergency Service personnel.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Uncorrected altitude data was based on the standard atmosphere altimeter pressure setting of 1013 hPa, rounded to the nearest hundred feet.
[2]The calculated barometric altitude was based on the Adelaide altimeter pressure setting of 1015 hPa.
[3]All speeds in the report are ATC-recorded groundspeeds.
[4]CTAF: common traffic advisory frequency is the radio frequency used by pilots when operating in the vicinity of non‑towered airports.
Occurrence summary
Investigation number
AO-2026-010
Occurrence date
06/02/2026
Occurrence time and timezone
16:21 Central Australia Daylight Time
Location
14 km south-east of Goolwa Airport
State
South Australia
Report release date
04/03/2026
Report status
Preliminary
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
210N
Registration
VH-RDH
Serial number
21064374
Aircraft operator
Goolwa Air Pty Ltd
Sector
Piston
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Other general aviation flying-Other flights
The ATSB is investigating a collision with terrain involving Beechcraft B200C, registration VH‑PUY, near Normanton Airport, Queensland, on 6 February 2026.
After 4 passengers disembarked the aircraft, the pilot planned to conduct a flight from Normanton to Cairns, Queensland. Shortly after take-off from Normanton Airport's runway 32, the aircraft collided with terrain and a post-impact fire ensued. The pilot, who was the sole occupant of the aircraft, sustained fatal injuries, and the aircraft was destroyed.
The ATSB has commenced the examination and analysis of the initial evidence collected.
To date, the ATSB has:
inspected the wreckage
recovered and retained equipment, including the cockpit voice recorder, for further examination
collected operational and aircraft records from the aircraft operator and Civil Aviation Safety Authority
collected air traffic control and airport data
collected electronic flight bag data
interviewed witnesses and company pilots
collected weather data.
The investigation is continuing and will include:
further interviews
analysis of witness videos, photographs, airport data and interviews
review of operational information
analysis of data from air traffic control, the Bureau of Meteorology and equipment recovered from the aircraft.
A preliminary report, which detailed factual information established during the evidence collection phase, was released on 2 April 2026. See below.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Preliminary report
Report release date: 02/04/2026
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On the afternoon of 6 February 2026, the pilot of a Beechcraft B200C, registered VH‑PUY and operated by Machjet International, planned to conduct a ferry flight[1] from Cairns to Normanton, followed by a return passenger transport flight[2] from Normanton to Doomadgee, then ferry the aircraft back to Cairns (all locations in Queensland). The flights were conducted under the instrument flight rules (IFR),[3] using callsign Machflight 313.
The aircraft took off from Cairns Airport at about 1318 local time and arrived at Normanton Airport at 1431. At 1455, the aircraft took off from runway 32 at Normanton Airport, with the pilot and 4 passengers on board, arriving at Doomadgee Airport at 1532. The aircraft then departed Doomadgee at 1853, and landed on runway 14 at Normanton Airport at 1932, where the pilot shut down the aircraft and the passengers disembarked.
At 1945:47, the pilot radioed Brisbane Centre air traffic control[4] and advised they were taxiing at Normanton for Cairns on runway 32. The controller responded that there was no reported IFR traffic and issued the pilot a transponder code. The controller then confirmed that the pilot was aware of the significant weather advisory (SIGMET)[5] ‘V03’, which was for frequent thunderstorms in an area that included Normanton Airport (see the section titled Meteorological conditions).
As the pilot had activated the airport lighting during approach, at 1947, a recorded message on the aerodrome frequency response unit was broadcast on the common traffic advisory frequency (CTAF)[6]: ‘Normanton airport airfield lighting 10 minutes remaining’.
At 1948, the pilot broadcast on the CTAF that they were ‘entering and backtracking runway 14’. There were no further recorded transmissions from the pilot. The aircraft then entered and backtracked runway 32.
Based on recorded ADS-B[7] data, the aircraft commenced take-off from runway 32 at 1950. The aircraft accelerated and climbed to a maximum height of about 150 ft above ground level prior to entering a descent (Figure 1).
Figure 1: ADS-B data path of VH-PUY
Source: Google Earth, annotated by the ATSB
The aircraft impacted a small tree, 360 m from the end of the runway, prior to impacting the ground in a wings-level attitude. Following the ground impact, the aircraft slid beneath powerlines and while there was no indication that the aircraft struck the wires, it triggered a local power outage. While sliding along the ground, the aircraft commenced a gradual right yaw,[8] impacting trees and breaking up in the process before coming to rest in flood water 580 m beyond the end of the runway.
At 1951:28, the final ADS-B position transmitted from the aircraft indicated that it:
was 370 m beyond the end of runway 32 (after the initial impact with the tree)
had a ground speed of 162 kt
had descended from the previous transmitted position to that point at 1,100 fpm.
The pilot was fatally injured. A post-impact fire ensued and the aircraft was destroyed.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Aeroplane), a class 1 aviation medical certificate, a command instrument rating and the appropriate endorsements and ratings for the aircraft. The pilot had accrued 1,721 hours total flight time, 381 of which were on the B200 aircraft type. The pilot had completed 191 hours on the aircraft type in the last 90 days, with 116 of those hours as pilot in command.
Aircraft information
VH-PUY was a Beechcraft B200C twin-engine turboprop aircraft, manufactured in the United States in 1981 as serial number BL 41, and first registered in Australia in 1987. The aircraft had retractable landing gear, a pressurised cabin and a T-tail horizontal stabiliser. It was powered by 2 Pratt & Whitney Canada PT6A-42 engines and Hartzell HC-D4N-3A propellers. The aircraft avionics suite included Garmin G600 electronic flight instruments. According to the maintenance release, at the start of the day’s flying on 6 February 2026, the aircraft had accumulated a total time of 23,708.4 hours in service. There were no outstanding defects documented on the maintenance release.
Meteorological conditions
Area forecast
The Bureau of Meteorology grid point wind and temperature forecast, issued at 1604 and valid from 1900 on 6 February at 1,000 ft above mean sea level (AMSL) in the area including Normanton, was wind from 050° at 8 kt and temperature of 27°C.
The graphical area forecast (cloud heights AMSL) issued at 1421 and valid from 1500 to 2100 included the following information:
broken stratocumulus with bases at 1,500 ft and tops at 3,000 ft over land from 1900
broken cumulus/stratocumulus with bases at 3,000 ft and tops above 10,000 ft.
visibility reducing to 2,000 m in isolated to scattered showers of rain associated with:
isolated[10] towering cumulus with bases at 3,000 ft and tops above 10,000 ft
broken stratus with bases 800 ft and tops 3,000 ft
broken cumulus/stratocumulus with bases at 3,000 ft and tops above 10,000 ft.
visibility reducing to 1,000 m in isolated to occasional[11] thunderstorms with rain associated with:
isolated cumulonimbus with bases at 3,000 ft and tops above 10,000 ft
broken stratus with bases at 600 ft and tops at 3,000 ft.
The forecast also included SIGMET V02 valid from 1730–1930, for frequent[12] thunderstorms with tops at flight level 550 moving south-west at 15 kt in a region that included Normanton.
That SIGMET was reissued at 1852 as SIGMET V03, valid from 1930–2130 with no change in detail from V02.
Aerodrome forecast
The aerodrome forecast[13] (all cloud heights above the aerodrome elevation of 73 ft) for Normanton issued at 1630 and valid from 1800 to 0600 (on 7 February) included the following information relevant to the accident flight:
Wind from 350° at 8 kt, visibility greater than 10 km, light showers of rain and scattered cloud at 3,000 ft.
A probability for periods up to 60 minutes between 1800 and 0300 (on 7 February) of:
variable winds at 20 kt gusting to 30 kt
visibility 1,000 m in thunderstorms and rain
broken cloud at 800 ft and scattered cumulonimbus clouds with bases at 3,000 ft.
From 1800–2100, temperature 30°C and QNH[14] 1,008 hPa.
Aerodrome weather observations
Weather observations (all cloud heights above aerodrome elevation) at Normanton Airport between 1900 and 1956 included the following routine weather reports (METAR)[15] and special reports (SPECI)[16].
METAR at 1900: wind from 360° at 4 kt, visibility greater than 10 km, light showers of rain. Cloud broken at 6,200 ft, broken cloud at 7,400 ft, overcast at 8,200 ft. Temperature 31°C, dewpoint 26°C, QNH 1,010 hPa. No rain in the last 10 minutes, 0.2 mm since 0900 local time. Distant lightning detected to the north.
METAR at 1930: wind from 360° at 5 kt, visibility greater than 10 km, scattered cloud at 6,700 ft, broken cloud at 7,900 ft, overcast at 9,300 ft. Temperature 31°C, dewpoint 26°C, QNH 1,011 hPa. No rain in the last 10 minutes, 0.2 mm since 0900 local time. Distant lightning detected to the north-east, east, south-east and north-west.
SPECI at 1940: wind from 350° at 19 kt, visibility greater than 10 km, few cloud at 1,800 ft, scattered cloud at 4,700 ft, broken cloud at 6,700 ft. Temperature 27°C, dewpoint 22°C, QNH 1,011 hPa. No rain in the last 10 minutes, 0.2 mm since 0900 local time. Distant lightning detected in the north, north-east, east, south-east and north-west.
SPECI at 1952: wind from 020° at 16 kt gusting to 26 kt, visibility 7,000 m, thunderstorms in the vicinity, light showers of rain with scattered cloud at 800 ft, broken at 2,000 ft, broken at 4,800 ft. Temperature 25°C, dewpoint 24°C, QNH 1,012 hPa. 0.4 mm of rain in the last 10 minutes, 0.6 mm total rainfall since 0900 local time. Thunderstorms to the north and north-east.
SPECI at 1956: wind from 030° at 15 kt gusting to 25 kt, visibility 5,000 m and thunderstorms in the vicinity. Temperature 25°C, dewpoint 24°C, QNH 1,013 hPa. 0.4 mm of rain in the last 10 minutes, 0.6 mm total rainfall since 0900 local time. Thunderstorms to the north and north-east.
Figure 2 shows the Bureau of Meteorology weather radar, 2 minutes prior to the accident, with light to moderate rain rate detected to the north-west of Normanton.
Figure 2: Radar imagery 2 minutes prior to the accident
Source: Bureau of Meteorology, annotated by the ATSB
Table 1 shows the one-minute weather data from the automatic weather station at Normanton Airport from when the aircraft landed at 1932 to 2010. The data shows that when the aircraft landed at Normanton, the wind was northerly at 5 kt, gusting to 6 kt. As the pilot prepared the aircraft and taxied out, the wind veered to the east-north-east and increased in average and gust speed. The maximum wind speed and gust occurred at 1941. By 2009, the wind average and gust speeds had reduced below 10 kt.
The pilot’s briefing package included the forecast weather, aerodrome weather reports for Normanton and Cairns at 1730 local time and the relevant SIGMETs, consistent with that detailed above.
Sunset times
On 6 February 2026 at Normanton, daylight was from 0625–1913 and civil twilight[17] was 1913–1936. The moon rose at 2205.
Site and wreckage examination
The wreckage trail commenced at an impact mark at the top of a small tree to the left of an extended runway centreline, 360 m from the end of the runway (Figure 3). Propeller slash marks were evident on another tree approximately 20 m after the initial tree impact, followed by evidence of the aircraft fuselage’s impact with the ground.
The left and right wing tips were located embedded in trees on either side of the wreckage trail, 60 m from the initial tree impact. Browning of vegetation commenced from this point onwards in the direction of travel, indicating rupturing of the wing fuel tanks. From there, the aircraft slid, underneath a set of powerlines, with a gradual right yaw that continued until its final resting place. There was no evidence of landing gear marks anywhere in the wreckage trail, indicating that all landing gear was in the ‘up and locked’ position.
The main fuselage was located in an upright position with the empennage fractured at the base of the vertical stabiliser (T-tail), which was lying on its right side. The cockpit had separated from the aircraft at the rear of the pilot’s seat and was resting on its left side, partially submerged in water. The left wing and both engines had separated from the aircraft during the accident sequence. The fuselage, cockpit and right wing were heavily damaged from a post‑impact fire.
Impact damage to the engine propellers indicated they were being driven by the engine during the impact sequence. All flight controls were located with the aircraft and measurements were taken of the flap, rudder trim and elevator trim actuators for further analysis.
Figure 3: Wreckage trail of VH-PUY
Source: ATSB
Further investigation
To date, the ATSB has:
inspected the wreckage
recovered and retained equipment, including the cockpit voice recorder, for further examination
collected operational and aircraft records from the aircraft operator and Civil Aviation Safety Authority
collected air traffic control and airport data
collected electronic flight bag data
interviewed witnesses and company pilots
collected weather data.
The investigation is continuing and will include:
further interviews
analysis of witness videos, photographs, airport data and interviews
review of operational information
analysis of data from air traffic control, the Bureau of Meteorology and equipment recovered from the aircraft.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB acknowledges the assistance provided by the Queensland Police Service and Carpentaria Shire Council.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Ferry flights were conducted under Part 91 of the Civil Aviation Safety Regulations (CASR).
[2]Passenger transport flights were conducted under Part 135 of the CASR.
[3]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[4]Brisbane centre: Brisbane Centre air traffic control is one of 2 major air traffic control centres – the other being in Melbourne. From Brisbane Centre, Airservices manages the airspace over the northern half of Australia, representing around 5% of the world’s total airspace. Brisbane Centre’s flight information region (FIR) neighbours include Indonesia, East Timor, Papua New Guinea, Fiji, New Zealand, and the USA.
[5]Significant meteorological information (SIGMET): a weather advisory service that provides the location, extent, expected movement and change in intensity of potentially hazardous (significant) or extreme meteorological conditions that are dangerous to most aircraft, such as thunderstorms or severe turbulence.
[6]Common Traffic Advisory Frequency (CTAF): a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled airport or within a broadcast area.
[7]Automatic dependent surveillance–broadcast (ADS-B): a surveillance technology in which an aircraft determines its position via satellite navigation and periodically broadcasts it, enabling it to be tracked.
[8]Yawing: the motion of an aircraft about its vertical or normal axis.
[9]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[10]Isolated thunderstorms and/or cloud: individual features are affecting, or forecast to affect, up to 50% of an area.
[11]Occasional: well-separated features affecting, or are forecast to affect, greater than 50% but not more than 75% of an area.
[12]Frequent thunderstorms: an area of thunderstorms with little or no separation between adjacent storms and covering more than 75% of the affected area.
[13]Aerodrome forecast (TAF): a statement of meteorological conditions expected for a specific period of time in the airspace within a radius of 5 NM (9 km) of the aerodrome reference point.
[14]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
[15]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[16]A SPECI is a special report of meteorological conditions, issued when one or more elements meet specified criteria significant to aviation. SPECI is also used to identify reports of observations recorded 10 minutes following an improvement (in visibility, weather or cloud) to above SPECI conditions.
[17]During civil twilight, the sun is between 0–6° below the horizon. There is enough natural sunlight during this period that artificial light may not be required to carry out outdoor activities. Only the brightest celestial objects can be observed by the naked eye during this time.
Occurrence summary
Investigation number
AO-2026-060
Occurrence date
06/02/2026
Occurrence time and timezone
19:51 Eastern Australia Standard Time
Location
Near Normanton Airport
State
Queensland
Report release date
02/04/2026
Report status
Preliminary
Anticipated completion
Q4 2026
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Beech Aircraft Corp
Model
B200C
Registration
VH-PUY
Serial number
BL 41
Aircraft operator
Machjet International Pty. Ltd.
Sector
Turboprop
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Other general aviation flying-Ferry flights
The ATSB has commenced evidence collection as part of its transport safety investigation into an accident involving a Beechcraft B200C King Air, registration VH-PUY, near Normanton, Queensland, on Friday evening.
As reported to the ATSB, the pilot planned to conduct a return flight to Cairns after 4 passengers had disembarked the aircraft at Normanton.
Shortly after take-off from Normanton Airport's runway 32 at around 8.16pm local time, the aircraft collided with terrain and a post-impact fire ensued. The pilot, who was the sole occupant of the aircraft, sustained fatal injuries, and the aircraft, which came to rest in floodwaters about 1,000m beyond the runway threshold, was destroyed.
Transport safety investigators from the ATSB’s Canberra and Sydney offices, with expertise in aircraft maintenance and engineering, are due to arrive in Normanton on Monday.
Once at the accident site, weather and access restrictions permitting, they plan to conduct a range of evidence‑gathering activities including site mapping with a drone, wreckage examination, retrieval of the cockpit voice recorder, and recovery of other relevant aircraft components for further examination and analysis at the ATSB’s Canberra technical facilities.
Investigators will also interview witnesses, and the ATSB asks anyone who witnessed the accident, including ear witness, or anyone with footage of the aircraft at any stage of its flight, to make contact via the witness form on our website - atsb.gov.au/witness - at their earliest opportunity.
As well as on-site activities, ATSB investigators will obtain pilot and aircraft maintenance records, and collect weather information and any available recorded flight tracking data.
The ATSB anticipates publishing a preliminary report, detailing factual information about the circumstances of the accident, in about 8 weeks.
A final report detailing findings and the analysis to support those findings will be released at the conclusion of the investigation. However, if the investigation identifies a critical safety issue at any time the ATSB will immediately inform relevant stakeholders.
The ATSB acknowledges the significant assistance being provided by the Queensland Police Service during the onsite phase of the investigation.
The ATSB has commenced an investigation into an accident involving a Beechcraft King Air aircraft near Normanton, Queensland on Friday evening.
ATSB transport safety investigators are preparing to deploy to the accident site, where they will conduct a range of evidence gathering activities including site survey, wreckage examination, witness interviews, and retrieval of the cockpit voice recorder and other relevant components for further examination and analysis at the ATSB’s Canberra technical facilities.
As well as on-site activities, investigators will also obtain pilot and aircraft maintenance records, and collect weather information and any available recorded flight tracking data.
The ATSB asks anyone who witnessed the accident, including ear witness, or anyone with video footage of the aircraft at any stage of its flight, to make contact via the witness form on our website - atsb.gov.au/witness - at their earliest opportunity.
Statement can be attributed to ATSB acting Chief Commissioner Colin McNamara:
The Australian Transport Safety Bureau has commenced an investigation into Friday’s accident near Goolwa involving a Cessna 210 aircraft with three people on board.
This was a tragic day for three families, and the wider aviation community, and on behalf of the ATSB I express our deepest condolences to the families and friends who have lost loved ones.
Upon being notified of the accident the ATSB immediately began pulling together a team of investigators. This morning, we deployed 4 investigators from our Canberra office, who have specialist expertise as pilots, aircraft maintenance engineers and in human factors, to the scene.
They are expected in Goolwa later today, where they will begin examining the recovered aircraft wreckage.
Over coming days investigators will also interview witnesses and involved parties, and obtain any available flight track data and aircraft and maintenance records.
Any aircraft components of interest will also be recovered to our Canberra technical facilities for further examination.
Crucially, we are aware there are a number of video recordings of the accident sequence, some of which have been shown in media.That footage captured the aircraft rolling to the left in a very steep nose down trajectory a couple of hundred metres offshore.
Analysis of those video recordings will be instrumental to the investigation, and we do ask that anyone with video footage of the aircraft at any stage of its flight, and of the accident sequence, to make contact with the ATSB via the witness form on our website at their earliest opportunity.
Following the on-site phase, the ATSB expects to publish a preliminary report, which will detailing factual information about the circumstances of the accident, in about 8 weeks.
A final report detailing findings and the analysis to support those findings will then be released at the conclusion of the investigation. However, if the investigation identifies a critical safety issue at any time the ATSB will immediately inform relevant stakeholders.
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into an accident involving a single-engine Cessna aircraft which collided with water near Goolwa, South Australia, on Friday afternoon.
ATSB transport safety investigators are expected on scene on Saturday, where they will examine the wreckage once it has been recovered from the water.
Investigators will also interview witnesses and involved parties, collect available video footage and any recorded flight tracking data, and obtain pilot and aircraft maintenance records.
The ATSB asks anyone with video footage of the aircraft in-flight, the accident sequence or the immediate aftermath of the accident, to make contact via the witness form on our website - atsb.gov.au/witness - at their earliest opportunity.
The ATSB expects to issue a more substantive investigation update on Saturday.