Separation issue involving Bell 212, VH-KHO, and PZL M18B, VH-VWF, 58 km west of Mount Hotham Airport, Victoria, on 18 January 2026
Final report
Report release date: 05/05/2026
Investigation summary
What happened
On 18 January 2026, firefighting aircraft, ground personnel and assets were conducting firefighting operations at Wabonga – The Razor fireground, 58 km west of Mount Hotham, Victoria.
There were 2 helicopters and 3 fixed wing aircraft conducting firebombing and 1 helicopter conducting rappelling operations, being coordinated by an air attack supervisor (AAS) in a Eurocopter AS350 helicopter, callsign Firebird 303. There were also 2 large air tankers (LATs) operating on the Razor ridge south of the fireground, being coordinated by a LAT AAS in a fixed wing aircraft, callsign Birddog 376.
At about 1421, the pilot of a Bell 212 helicopter, callsign Helitak 368, reported broadcasting on the fire common traffic advisory frequency when about 5 NM (9 km) south of the fireground and inbound for rappelling operations. The pilot recalled being cleared to enter the fireground by the AAS. While the AAS could not recall issuing the clearance, they recalled checking there was no conflict with the large air tankers. As all the other aircraft were entering the fireground from the north, the AAS expected Helitak 368 to track east and remain clear of the fireground before holding and entering from the north, but did not communicate that to the pilot of Helitak 368.
About 90 seconds before Helitak 368 crossed the Razor ridge, a PZL M18B aircraft, callsign Bomber 359, left its holding position north of the fireground to conduct a drop at the southern end of the fireground, having been cleared by the AAS.
Shortly after crossing the Razor ridge, the crew of Helitak 368 sighted Bomber 359 ahead on a conflicting track. The Helitak pilot conducted a left descending turn to increase separation between the aircraft. At about the same time, Bomber 359 commenced a drop, then climbed and departed the area.
The pilot of Bomber 359 was unaware of the incident. The pilot of Helitak 368 elected to continue tracking northwards through the fireground and did not report the incident to the AAS.
What the ATSB found
The ATSB found that the air attack supervisor did not provide tracking instructions to the Helitak 368 pilot when approaching the fireground. Additionally, the Helitak pilot believed that they had separation assurance and were clear to conduct rappelling operations, resulting in a separation issue with an aircraft conducting firebombing operations.
The ATSB also found that, despite communications on the fire common traffic advisory frequency, the pilots of both Helitak 368 and Bomber 359 were unaware they were on a conflicting track. However, upon sighting the aeroplane, the pilot of Helitak 368 took action to maintain safe separation.
Additionally, the ATSB found that the pilot of Helitak 368 did not advise the air attack supervisor of the separation issue and continued to track north through the fireground, with no assurance of positive separation with other aircraft in the fireground.
What has been done as a result
The Victorian Department of Energy, Environment and Climate Action (DEECA) advised that the findings and contributing factors in this report would be further analysed, and lessons learned through this investigation reinforced through future Victorian aviation pre‑season briefings and incorporated into Victorian training and case study material. Lessons learned would also be shared with the Victorian aviation sector and with national counterparts via the National Aviation Firefighting Centre (NAFC) Aviation Safety Group to enhance collective safety awareness with the broader sector.
DEECA also advised that it would focus learnings on mandatory escalation of separation issues and supervisory control recovery following airspace conflicts to inform doctrine enhancements to interagency aviation operating procedures. Specifically, accident and incident response procedures and the management of aircraft at incidents.
Safety message
Aerial firefighting is a critical capability for the management and suppression of bushfires in Australia. To effectively achieve this, multiple aircraft are flown at low heights above the ground and varying airspeeds, often in challenging environmental conditions. The low operating heights, conditions, and high traffic density increase the complexity of flight crew tasks.
Maintenance of situational awareness of other aircraft operating in the vicinity is significantly enhanced by radio communications, aided by the presence of an air attack supervisor issuing directed communications and tactically separating aircraft. However, the effectiveness of radio communications can be affected by factors such as the number of aircraft operating on a fire common traffic advisory frequency and by terrain shielding.
The last line of defence to avoid midair collisions under visual flight rules is for pilots to see‑and-avoid other aircraft, noting that the limitations of see-and-avoid are well‑documented, particularly where visibility may be reduced by smoke. It is therefore vital that pilots involved in firefighting operations understand where other aircraft are operating and immediately communicate any issues so that all have a common mental model of the fireground.
The investigation
The occurrence
Background
On 18 January 2026, firefighting aircraft as well as ground personnel and assets were conducting firefighting operations at Wabonga – The Razor (Razor) fireground, 58 km west of Mount Hotham, Victoria. This was the third day of operations at the fireground, and as the wind and turbulence had eased, it was the first day large air tankers (LATs) had been deployed to the area. It was also the first day conditions were suitable for helicopters to be used to rappel[1] ground crews into the fireground.
During the morning, the following aerial assets were operating at the fireground:
- 2 Sikorsky (heavy) helicopters (Helitak 369 and Helitak 290) conducting long line waterbombing
- 2 Eurocopter AS350 B3 (light) helicopters (Firebird 303 and Firebird 312) with a pilot and air attack supervisor (AAS), alternating with only 1 helicopter at the fireground at a time
- 1 Bell 412 (medium) helicopter (Helitak 332) conducting rappelling operations
- 2 Bombardier DHC-8-400 LATs, Bomber 390 and Bomber 391, with a SOCATA TBM700 aircraft operating as a LAT Birddog[2] (Birddog 376)
- 3 fixed wing single engine air tankers (SEATs), Bomber 358, Bomber 359, and Bomber 363
- Firescan (fire intelligence gathering) aircraft (usually twin-engine turbo-propeller aircraft) were also present at times.
All aircraft were operating on a discrete fire common traffic advisory frequency (Fire‑CTAF)[3] 128.90, identified for radio communications as the ‘Razor spur fire’. Communications on the Fire-CTAF were not recorded (normally and on the incident day), nor were they required to be.
The AAS was responsible for the safe and efficient tactical coordination of aircraft operations and with directing the firebombing aircraft to ensure there was separation between aircraft. However, the aircraft were operating under visual flight rules,[4] with the pilots ultimately responsible for separation with other aircraft, using ‘see-and-avoid’ principles.
The firebombing helicopters (Helitaks) were filling up from a water source referred to as the ‘dip’, north-west of the fireground. The SEATs were refuelling and filling with retardant at Mansfield aircraft landing area (ALA) 50 km to the west of the fireground. The dip was then being used as the inbound entry point to the fireground. After reporting when passing the dip, the aircraft were joining a holding pattern or ‘stack’, north of the fireground. To ensure separation, the Helitaks were joining the stack below 3,000 ft above mean sea level (AMSL) and the SEATs were joining above 3,500 ft, with all aircraft conducting left circuits. The AAS was then clearing the aircraft into the fireground, with the SEATs primarily dropping retardant on the western side of the fire (in an easterly direction) and the Helitaks dropping water on the northern and eastern side, with aircraft making left circuits to enter, drop, and exit the fireground. The AAS reported that they sighted each aircraft prior to clearing them into the fireground.
The LATs and LAT Birddog were dispatched from Avalon Airport, Victoria, dropping retardant on the Razor ridge south of the fireground, and then proceeded to Albury Airport, New South Wales, to refuel and reload retardant. The LATs were operating at altitudes not below 3,500 ft and were separated from the SEATs and Helitaks by a ‘virtual fence’ about 500 m north of the ridge (Figure 1).
Figure 1: Wabonga – The Razor fireground map showing firebombing drops, the holding area and virtual fence
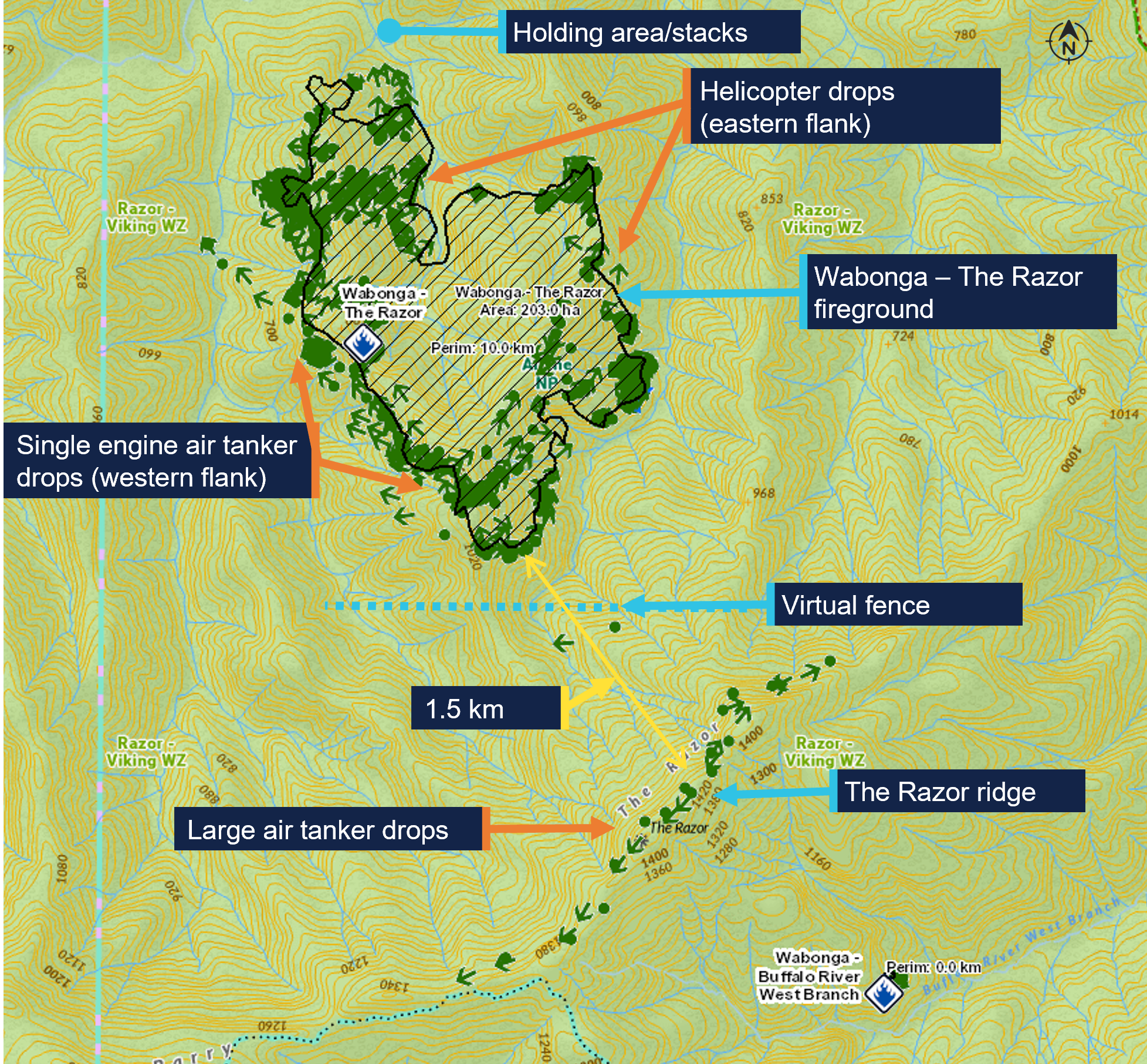
The green dots are the drops over the 5-day duration of the fire 16–20 January 2026. Source: DEECA, annotated by the ATSB
What happened
On 18 January 2026, at 0948 local time, a PZL M18B aircraft, VH-VWF, operating as a SEAT with callsign Bomber 359, departed from the pilot’s base at Benambra Airport, 93 km east of the fireground. Between 1014 and 1359, the pilot conducted 5 drops at the Razor fireground, returning to Mansfield ALA after each drop to refill.
Meanwhile, a Bell 412 helicopter, callsign Helitak 333, which had been tasked for rappel operations, left 5 rappelers and a rappel dispatcher at Snowy Range Mountain Airport, 28 km south of the Razor ridge, while the helicopter departed to get maintenance on a radio issue. A Bell 212 helicopter, VH-KHO, callsign Helitak 368, was then tasked to collect the rappelling crew and conduct the rappelling operation. The pilot of Helitak 368 had not previously operated at the Razor fireground and was not expecting to operate there that day. Helitak 368 departed Latrobe Valley Airport at 1331 and arrived at Snowy Range Mountain Airport at 1404, departing for the fireground with the rappelling crew 11 minutes later.
Also at 1404, Bomber 359 left Mansfield for the fireground with its sixth load. When 5 NM (9 km) from the fireground, at about 1419 based on tracking data, the pilot reported broadcasting on the Fire-CTAF that they were inbound and tracking for the dip. Bomber 359 then entered the stack at 1421:30 and held there, awaiting clearance from the AAS (in Firebird 303) to enter the fireground and conduct a drop.
The pilot of Helitak 368 also reported broadcasting on the Fire-CTAF when inbound about 5 NM south of the fireground, at about 1421 based on tracking data. The pilot reported handing over ‘flight following’[5] to the AAS and requesting a clearance from them to enter the fireground. The Helitak pilot reported that they would have included in the request to enter the fireground that they were also seeking clearance to enter for reconnaissance and insertion of the rappelling crew. The helicopter then commenced descent from about 5,000 ft AMSL.
The rappel dispatcher in Helitak 368 recalled that the pilot made a 10-NM call and then a 5‑NM call, saying words to the effect of ‘We are 5 miles out. Are we ok to approach?’ and confirming what aircraft were in the area. The dispatcher reported writing the aircraft callsigns on the helicopter window and recalled the AAS saying they could enter the area. The dispatcher also recalled being aware from the communications that a bomber was in the vicinity, but did not know where the reporting points being referred to were.
The AAS recalled Helitak 368 reporting being inbound from the south and reported that this was the first time an aircraft had entered the fireground from that direction. They recalled checking that the LATs were clear of the Razor ridge and would not conflict with Helitak 368 but could not specifically recall clearing Helitak 368 into the fireground.
The AAS advised that it was likely they had instructed Helitak 368 to hold to the north of the fireground while the SEATs were conducting drops on the western side of the fire. They reported that they had expected Helitak 368 to follow lower terrain east of the fireground before holding to the north with the other aircraft but did not specifically instruct the pilot of Helitak 368 to do so. The AAS was typically operating north-east of the fire, away from the SEAT and helicopter water/retardant dropping circuits, and did not see Helitak 368 entering the fireground from the south. The first time the AAS recalled sighting Helitak 368 was after the incident, when it was holding to the north. The pilot of Firebird 303 could not recall Helitak 368 being cleared into the fireground from the south.
At 1422:30, recorded track data showed that Bomber 359 left the stack and tracked south‑west towards the drop target, near the virtual fence at the southern edge of the fire. The Bomber 359 pilot, AAS and Firebird 303 pilot expressed confidence that Bomber 359 would not have left the stack to commence a drop without first receiving AAS clearance, which the AAS would not give until they had sighted the aircraft and ensured the area was clear of ground personnel. However, they could not recall the clearance being given.
At 1423:55, Helitak 368 crossed the Razor ridge at about 4,700 ft AMSL, tracking approximately north-north-east and immediately commenced descending and tracking north into the fireground to conduct reconnaissance for the rappel crew insertion. The elevation of the ridge was about 4,600 ft, with most of the fireground about 2,000–3,000 ft AMSL. The pilot of Helitak 368 reported that they did not expect to encounter any other aircraft, as they believed they had been cleared into the fireground. At the time Helitak 368 crossed the ridge, Bomber 359 was about 4 km to the north-west, from where it commenced a left turn before lining up for a drop at an altitude of about 4,000 ft, tracking approximately east (Figure 2).
Figure 2: Relative positions of Bomber 359 and Helitak 368 at 1423:55

Source: DEECA, overlaid on Google Earth, annotated by the ATSB
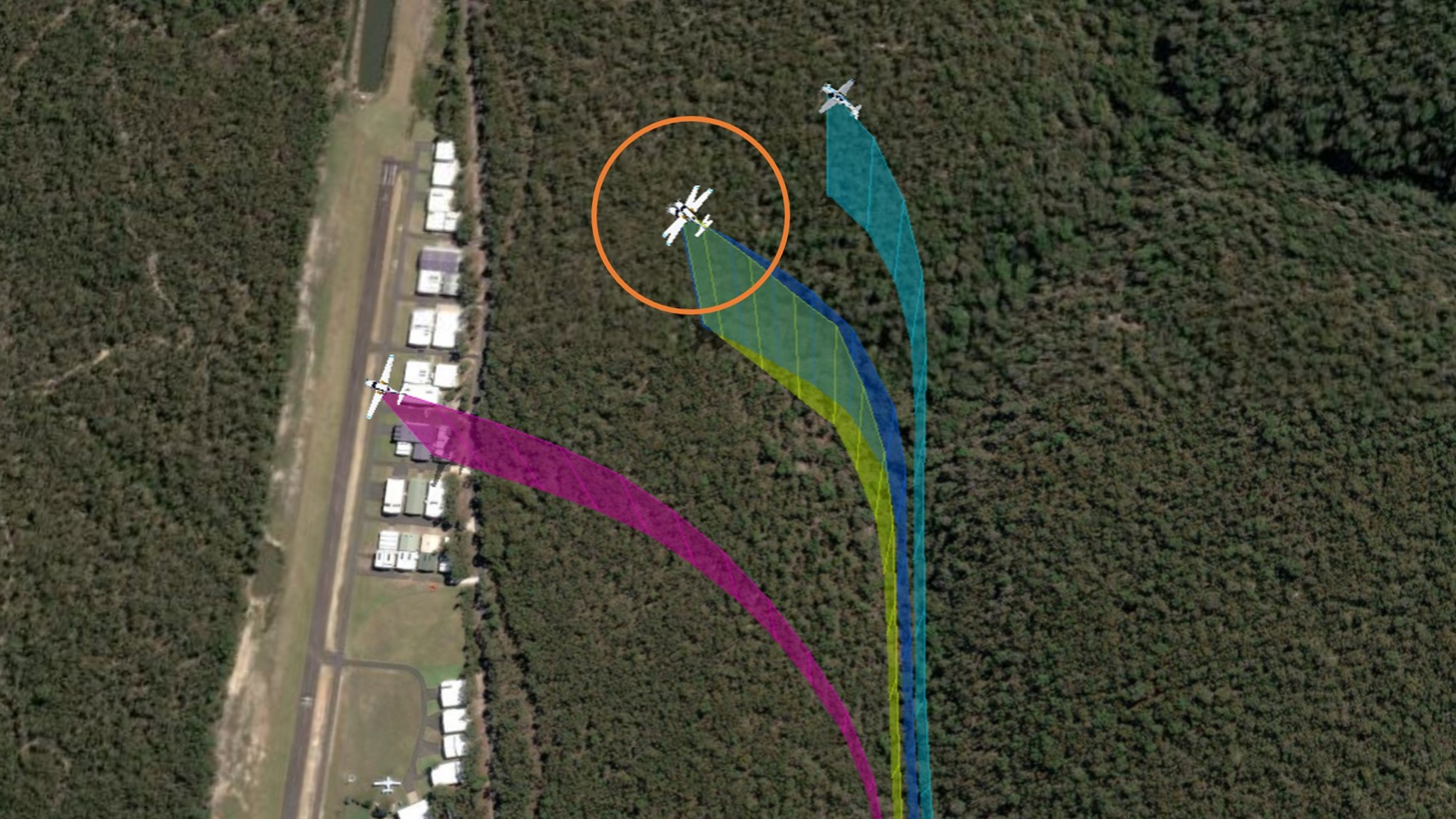
The rappel dispatcher reported sighting a bomber pointed out by the rappel crew leader and directing the Helitak 368 pilot to go left to increase separation. The Helitak pilot reported that they then observed a ‘yellow’ bomber in their 10 o’clock position slightly below their altitude on a reciprocal track. On sighting the aeroplane, they immediately conducted a descending left turn (Figure 3).
Figure 3: Relative positions when Helitak 368 turned left at 1424:25

Source: DEECA, overlaid on Google Earth, annotated by the ATSB
Based on the recorded data for Helitak 368, the helicopter turned left to track west about 30 seconds after crossing the ridge, and Bomber 359 commenced the drop in an easterly direction about 5 seconds later. The pilot of Bomber 359 reported that they would have broadcast both ‘on the drop’ and ‘off the drop’ on the Fire-CTAF. After the drop, Bomber 359 climbed and conducted a left climbing turn before returning to Mansfield. The closest proximity between the 2 aircraft occurred at 1424:45, with Helitak 368 about 400 ft below and 500 m horizontally from Bomber 359 (Figure 4).
Figure 4: Closest proximity of Bomber 359 to Helitak 368 at 1424:45

Source: DEECA, overlaid on Google Earth, annotated by the ATSB
The pilot of Helitak 368 reported checking with and receiving confirmation from the onboard rappel dispatcher that they had received a clearance to enter the fireground and conduct reconnaissance operations. The pilot also reported attempting to say something like ‘that was close’ on the Fire-CTAF but thought they may not have successfully transmitted that communication while focused on returning the aircraft to normal operations.
At 1425:10, Helitak 368 conducted a left orbit then tracked northwards through the fireground. The pilot reported that they did not conduct rappel operations and instead exited the fireground to the north, to ensure they remained clear of other aircraft. At about 1429, Helitak 368 joined the stack at the northern end of the fireground, conducted 2 left orbits over the next 7 minutes, then departed the fireground to refuel at a refuelling site, about 11 km to the north-east.
The Bomber 359 pilot had not seen or heard Helitak 368 and was unaware of any separation issue. The first time the Bomber 359 pilot recalled hearing the Helitak 368 pilot on the Fire-CTAF was when Helitak 368 was holding north of the fireground and the pilot advised they were ‘fuel critical’ and needed to depart the fireground to refuel.
The AAS and Firebird 303 pilot were also unaware of the incident as the Helitak 368 pilot did not communicate it to them. Shortly after Helitak 368 left the fireground to refuel, the AAS in Firebird 303 handed over to the AAS in Firebird 312 and Firebird 303 departed the fireground to refuel.
Helitak 368 subsequently re-entered the fireground from the north and conducted rappelling operations. At 1939, Helitak 368 returned the rappelling crew to Heyfield and arrived at Latrobe Valley Airport at 2001.
The pilot of Bomber 359 completed 9 loads that day before ferrying the aircraft to Benambra. Figure 5 shows the tracks for Helitak 368 and Bomber 359 at the Razor fireground on 18 January 2026.
Figure 5: Helitak 368 and Bomber 359 tracks for 18 January 2026 showing key locations
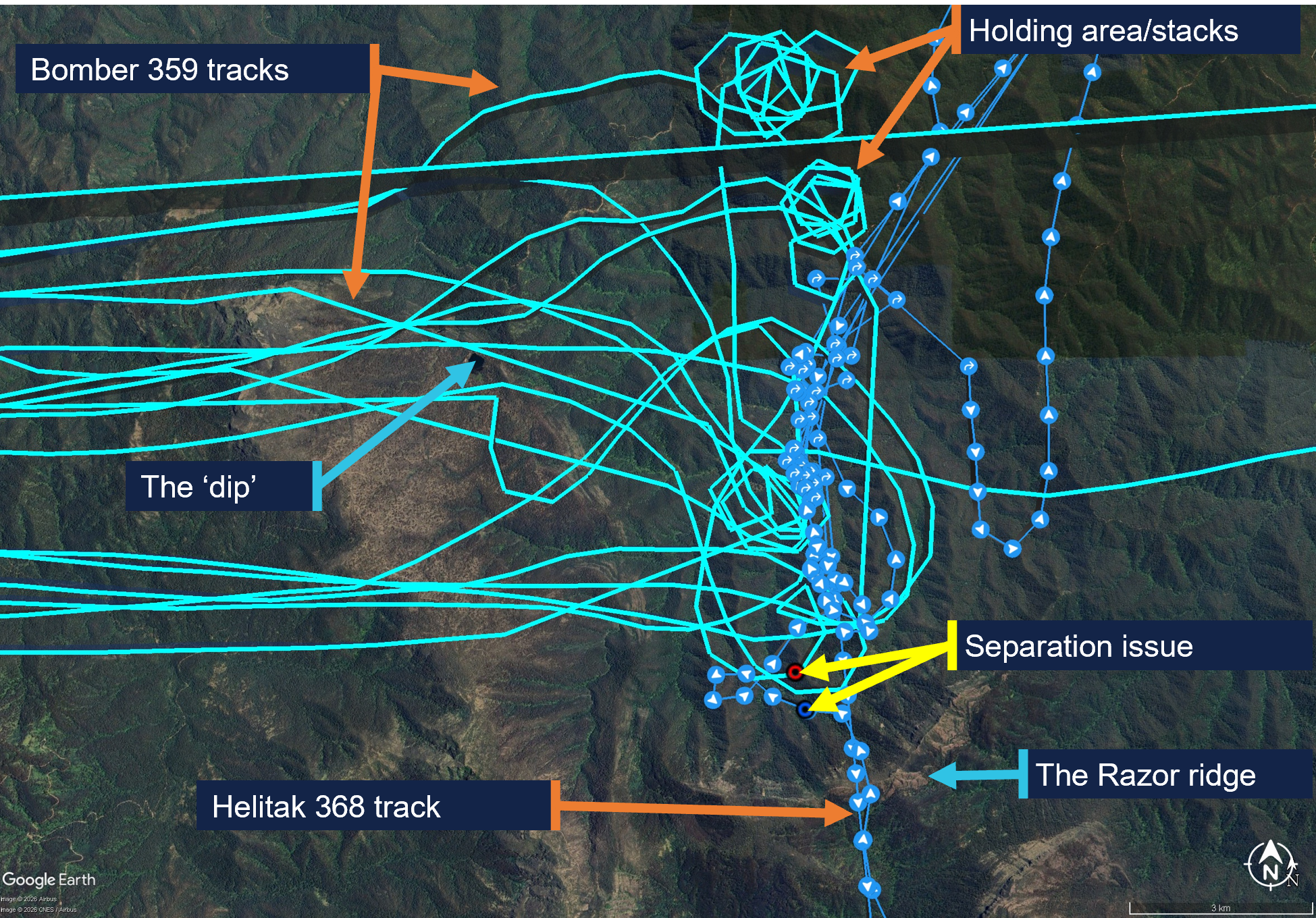
Source: DEECA, overlaid on Google Earth, annotated by the ATSB
Reporting of the occurrence
On 19 January 2026, the operator of Helitak 368 reported the incident as a ‘near miss’ to the Department of Energy, Environment and Climate Action of Victoria (DEECA). Unsure whether the operator had reported the incident to the ATSB as required, on 20 January, DEECA reported the incident to the ATSB as a ‘near miss’ between Helitak 368 and an unknown aircraft.[6] The Helitak 368 pilot reported having a seen a yellow aircraft and having later spoken to the pilot of Bomber 360 (a yellow Air Tractor 802 aircraft),[7] however Bomber 360 was not operating at the Razor fireground on 18 January. DEECA reviewed the available data and identified Bomber 359 (red and white livery) as the most likely aircraft involved in the reported occurrence. The ATSB investigation commenced on 2 February. The AAS was notified of the event on 29 January. The operator of Bomber 359 was made aware of the occurrence on 23 January and subsequently advised DEECA on 27 January that their pilots had no knowledge of the event. This limited the ability of those involved to recall the events.
Context
Personnel and aircraft information
Bomber 359
The pilot of PZL M18B, VH-VWF, callsign Bomber 359, held a Commercial Pilot Licence (Aeroplane), a class 2 aviation medical certificate, and had been conducting aerial firefighting operations since 1997. The pilot had accrued 13,501 hours total flight time, 103 of which were in the last 90 days. Of the total flight time, 3,987 hours were on the PZL M18 aircraft type, 75 of which were in the last 90 days.
The incident occurred on the pilot’s third day operating at the Razor fireground, which they described as ‘very technical’ with ‘cliffs, steep escarpments, tumbling air and severe turbulence’, and a complex mix of aerial assets.
The pilot reported that the AAS was ‘doing really well’ and the pilot of Firebird 303 was very experienced and was helping manage the AAS’s workload by assisting with communications.
The Bomber 359 pilot also reported that pilots of inbound aircraft could hear communications from the AAS, but generally not from other aircraft until they were within the fireground, due to terrain shielding. Further, pilots entering from north of the fireground would have been unable to see aircraft in the south due to smoke.
The pilot rated their fatigue as 1/7[8] and fatigue was not considered to be a factor in the occurrence.
Helitak 368
Pilot
The pilot of Bell 212, VH-KHO, callsign Helitak 368, held a Commercial Pilot Licence (Helicopter), a class 1 aviation medical certificate, and had about 2,500 hours total flight time, 600 of which were conducting aerial firefighting operations. The pilot had accrued 190 flight hours on the Bell 212 aircraft, 80 of which had been in the previous 90 days.
The pilot’s self-assessed fatigue score was 1/7 and fatigue was not considered to be a factor in the occurrence.
Rappel dispatcher
The rappel dispatcher was serving their fifth year as a flightcrew member, with 2 years as a rappeler followed by 3 years as a rappel dispatcher in firefighting operations. The rappel dispatcher was seated in the rear section of the helicopter cabin facing rearwards, attached to a ‘wander lead’ mounted to the cabin roof and connected to a harness.
The DEECA Helicopter Rappel Operations Manual stated that the rappel dispatcher was responsible for:
- the pre-flight preparation of the helicopter for a rappel operation
- the conduct of aerial reconnaissance of the fire area and selection of a suitable deployment location in consultation with the pilot and rappel crew leader
- the safe dispatch of rappelers and rappel equipment from the helicopter to the ground.
The pilot advised that in the aircraft, the dispatcher assisted in reducing the pilot’s workload by managing firefighting agency radios. Additionally, the dispatcher monitored the external environment while maintaining constant communication with the pilot.
Rappel crew leader
The rappel crew leader was seated in the rear of Helitak 368 at the right-side door, facing forwards. The rappel crew leader, as the ‘mission commander’, was responsible for conducting a mission briefing with the pilot, air operations manager and other relevant personnel.
The rappel crew leader was dispatched to the Razor fire by the district duty officer at 1205. The details they received included a ground contact, command and fireground radio communication channels and a grid reference for the fireground. Before Helitak 333 departed Heyfield, the state air desk provided the Fire-CTAF and AAS callsign (Firebird 303).
The rappel crew were picked up during a ‘hot change’ at Snowy Range Mountain airport, in which the helicopter was not shut down. Once airborne, the rappel crew leader relayed the communications channels, fire location, Fire-CTAF, AAS and other aircraft details to the pilot of Helitak 368.
Rappel operation
The pilot reported that they were tasked to conduct reconnaissance of the fireground for a suitable insertion point for the rappel crew. They expected that if there were aircraft that could conflict with the rappel operation, the AAS would have told them to remain south of the area until the bombers finished their drops.
The pilot reported that the task was to get crew into the proposed site and they wanted to ‘get in and get that job done’, and that the reconnaissance would take about 5 to 10 minutes.
The dispatcher reported that their assigned task was to liaise with another rappel crew already on the ground and either assist where they were or go elsewhere on the fireground. They reported that rappel aircraft were ‘awkward to deal with’, as rather than joining the firebombing circuit, ‘we just appear and want to go straight through and do our thing straight away’. Additionally, when they first arrive at a fireground, although they would hear bomber pilots broadcasting (for example, ‘off the dip’, or ‘on the drop’), they would not necessarily know where the dip site or drop targets were.
Firebird 303
Air attack supervisor
The air attack supervisor was in an Airbus AS350 B3 helicopter, VH-PXX, callsign Firebird 303. The AAS had substantial firefighting experience in other roles, and this was their second season as an AAS. The incident day was the AAS’s fifth consecutive day as AAS and third day at the Razor fireground, with a similar traffic mix to the previous days, although the conditions had been unsuitable for LATs or rappel crews on the previous days.
The AAS assessed their workload as 7–8 out of 10 due to the number (up to 12 aircraft) and different types of aircraft operating in the fireground during the day. They self‑assessed their fatigue at the time as about 3–4 out of 7.
The DEECA Air Attack Supervisor Manual described the AAS role as being:
primarily responsible for the safe and efficient tactical coordination of aircraft operations when fixed and/or rotary wing firebombing aircraft are operating on a fire.
The AAS duties included ensuring safety standards were maintained at all times. The AAS was also required to establish and maintain communications with the fire aircraft.
The AAS described their role as primarily being a safety role ensuring safety between aircraft and other aircraft, and between aircraft and people on the ground and secondly, coordinating the effective use of the aircraft to suppress bushfires.
The AAS responsibilities also included reporting accidents and incidents. The AAS manual specified notification procedures, which included the requirement to notify the incident controller and State Air Desk in the event of an aircraft occurrence. The Interagency Aviation Operating Procedure – Victoria, Management of aircraft at incidents, included a standdown matrix with the requirements for standing down resources in accordance with interagency procedure and that a standdown may be required as a result of an incident or near miss.
The AAS training included strategies to tactically separate firebombing aircraft from each other, segregating fixed and rotary wing aircraft, and scaling requirements for large and heavy aircraft. While this did not include separate strategies for helicopters conducting rappel operations, the same principles of situation awareness and clear communications for the tactical separation of aircraft applied.
Pilot
The Firebird 303 pilot had accrued over 3,000 hours in the AS350 aircraft type and more than 8,000 hours total flight time, about 40% of which was in firefighting operations.
Air operations manager
The air operations manager’s responsibilities involved coordinating all operational components of the air operation, including the conduct of required briefings.
The air operations manager did not recall communicating with the pilot of Helitak 368 or the AAS, but ensured the rappel crew leader made the pilot aware that there were 2 Fire‑CTAFs in use (at different firegrounds). As Helitak 368 was dispatched by the state air desk, and transported the same rappelling crew that had been in Helitak 333, essential details were provided to the pilot by the rappel crew leader.
Meteorological information
The Bureau of Meteorology forecast for the area at 5,000 ft AMSL included north to north-easterly winds up to 14 kt, visibility greater than 10 km and, for the time of the incident, broken[9] cumulus/stratocumulus clouds with bases at 5,000 ft and tops at 9,000 ft (all AMSL).
The AAS reported that the visibility was ‘really good’ and the flying conditions were good, with no cloud that day. Weather over the previous 2 days included turbulence and south‑easterly winds that had prevented insertion of ground crew. On the day of the incident, the winds remained easterly but had abated and one rappelling crew had already deployed on the ground.
Safety analysis
The pilot of Helitak 368 had not previously been to the fireground and was unaware of the operational tactics in place where aircraft were holding and entering the fireground from the north. The air attack supervisor (AAS) was aware Helitak 368 intended to conduct rappelling operations, and expected Helitak 368 would track east of the fireground and enter from the stack in the north, however, they did not specifically instruct the pilot of Helitak 368 to do so. While the AAS could not recall clearing Helitak 368 to enter the fireground, the pilot believed they had been cleared to do so. Additionally, they also assumed that the AAS had assured they would not conflict with other aircraft and could commence their reconnaissance and rappelling task from the south.
As a result of the misunderstanding, Helitak 368 tracked north through the fireground, without the AAS’s awareness, and unexpectedly sighted and came into proximity with Bomber 359 on a drop run.
Any clearances issued by the AAS for Helitak 368 to enter the fireground and for Bomber 359 to conduct a drop would have occurred within a 3-minute period and been broadcast on the fire common traffic advisory frequency (Fire-CTAF) that both aircraft were monitoring. Additionally, Bomber 359’s pilot also broadcast twice (on and off the drop) during the run for their retardant drop. However, neither of the pilots were aware of the presence or of the increasing proximity of the other aircraft. While the reason for this could not be conclusively determined, there are several potential factors which may have limited the crew’s ability to identify the presence of the other. There were a number of other aircraft operating in the fireground with the associated additional communications on the Fire-CTAF in that period. The ability of the pilots of both aircraft to hear all Fire‑CTAF communications may also have been affected by terrain shielding. Further, as the pilot of Helitak 368 was unaware of the operational tactics to be used, it is likely that they would not have been aware of the locations of the reporting points and geographical references in the communications and may not have understood that Bomber 359 was operating in their vicinity.
Although the external communication was ineffective at alerting the Helitak 368 pilot to a potential conflict, the rappel dispatcher sighted Bomber 359, and instructed the Helitak 368 pilot to go left. When the pilot sighted the aeroplane, they manoeuvred the helicopter to increase separation. The 2 aircraft passed within about 500 m horizontally and 400 ft vertically of each other.
The pilot of Helitak 368 did not alert the AAS to the incident but continued to track through the fireground. This increased the risk of a subsequent separation issue, as the AAS still had an expectation that Helitak 368 was flying to the east of the firebombing area. However, no subsequent separation issues were reported.
As the AAS was unaware of the incident at the time, the required post‑incident actions, which would have included advising the incident controller and may have involved a standdown of personnel, were not conducted.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the separation issue involving Bell 212, VH-KHO, and PZL M18B, VH-VWF, 58 km west of Mount Hotham Airport, Victoria, on 18 January 2026.
Contributing factors
- The air attack supervisor did not provide tracking instructions to the Helitak 368 pilot when approaching the fireground. Additionally, the Helitak pilot believed they had separation assurance and were clear to conduct rappelling operations, resulting in a separation issue with an aircraft conducting firebombing operations.
- Despite communications on the fire common traffic advisory frequency, the pilots of both Helitak 368 and Bomber 359 were unaware they were on a conflicting track. However, upon sighting the aeroplane, the pilot of Helitak 368 took action to maintain safe separation.
Other factors that increased risk
- The pilot of Helitak 368 did not advise the air attack supervisor of the separation issue and continued to track north through the fireground, with no assurance of positive separation with other aircraft in the fireground.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action by Department of Energy, Environment and Climate Action
The Victorian Department of Energy, Environment and Climate Action (DEECA) advised that the findings and contributing factors in this report would be further analysed, and lessons learned through this investigation reinforced through future Victorian aviation pre‑season briefings and incorporated into Victorian training and case study material. Lessons learned would also be shared with the Victorian aviation sector and with national counterparts via the National Aviation Firefighting Centre (NAFC) Aviation Safety Group to enhance collective safety awareness with the broader sector.
DEECA also advised that it would focus learnings on mandatory escalation of separation issues and supervisory control recovery following airspace conflicts to inform doctrine enhancements to interagency aviation operating procedures. Specifically, accident and incident response procedures and the management of aircraft at incidents.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- pilots and operators of the involved aircraft
- air attack supervisor
- rappel dispatcher
- rappel crew leader
- air operations manager
- recorded tracking data
- Department of Energy, Environment and Climate Action
- Civil Aviation Safety Authority.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- pilots and operators of the involved aircraft
- air attack supervisor
- air operations manager
- rappel dispatcher and rappel crew leader
- Department of Energy, Environment and Climate Action
- Civil Aviation Safety Authority.
Submissions were received from:
- air attack supervisor
- rappel crew leader
- the operator of VH-KHO
- Department of Energy, Environment and Climate Action.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Civil Aviation Safety Regulations Part 138 MOS defined rappelling as an aerial work Class D external load operation that involves a person exiting or entering an aircraft in flight using a rope or ladder attached to the helicopter.
[2] Birddog is used to assess the fireground and determine the most appropriate flight path to facilitate LAT integration with other aircraft.
[3] Discrete radio frequencies are allocated for Victorian firefighting operations, which the state air desk assigns to respective firegrounds.
[4] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[5] Flight following during flight: requirement to communicate position and intentions every 30 mins to nominated person and to advise of any changes, diversions and pick-ups. Failure to communicate activates search and rescue action.
[6] ATSB occurrence type is ‘near collision'.
[7] DEECA stated that there are psychological factors in witness recall, whereby individuals can rely on stereotypical associations when reconstructing events. Such associations are a normal aspect of human memory and can result in familiar or expected characteristics being recalled in place of the observed features (e.g. yellow for a bomber aircraft).
[8] Samn-Perelli fatigue scale: A self-assessed 7-point fatigue scale where 1 is ‘fully alert and wide awake’ and 7 is ‘completely exhausted, not able to function’.
[9] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘broken’ indicates that more than half to almost all the sky is covered.
Occurrence summary
| Investigation number | AO-2026-006 |
|---|---|
| Occurrence date | 18/01/2026 |
| Occurrence time and timezone | 1424 Eastern Daylight-Saving Time |
| Location | 58 km west of Mount Hotham Airport |
| State | Victoria |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Separation issue |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | PZL Mielec |
|---|---|
| Model | M18B |
| Registration | VH-VWF |
| Serial number | 1Z027 26 |
| Aircraft operator | Alpine Airwork |
| Sector | Piston |
| Operation type | Part 138 Aerial work operations |
| Activity | General aviation / Recreational-Aerial work-Firefighting |
| Departure point | Benambra aircraft landing area, Victoria |
| Destination | Benambra aircraft landing area, Victoria |
| Injuries | None |
| Damage | Nil |
Aircraft details
| Manufacturer | Bell Helicopter Co |
|---|---|
| Model | 212 |
| Registration | VH-KHO |
| Serial number | 31181 |
| Aircraft operator | Kestrel Aviation Pty Ltd |
| Sector | Helicopter |
| Operation type | Part 138 Aerial work operations |
| Activity | General aviation / Recreational-Aerial work-Firefighting |
| Departure point | Latrobe Valley Aerodrome, Victoria |
| Destination | Albury Airport, New South Wales |
| Injuries | None |
| Damage | Nil |