The ATSB is investigating a runway excursion and collision with tree involving a GippsAero GA8 Airvan, VH-WSU, at Lindeman Island, Queensland, on 8 March 2026.
During landing on soft and wet ground, the wheels slid and the pilot applied full power to conduct a go-around. The aircraft became airborne after the end of the runway and the landing gear contacted a tree, resulting in substantial damage. The aircraft was flown with reduced performance to Shute Harbour due to the runway condition at Lindeman Island being deemed unsuitable.
The ATSB has completed the evidence collection and analysis phases of the investigation and is drafting the final report.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2026-065
Occurrence date
08/03/2026
Occurrence time and timezone
14:35 Eastern Australia Standard Time
Location
Lindeman Island
State
Queensland
Report status
Pending
Anticipated completion
Q4 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Drafting
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Control issues, Diversion/return, Missed approach, Stall warning
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Gippsland Aeronautics Pty Ltd
Model
GA8
Registration
VH-WSU
Serial number
GA8-17-244
Aircraft operator
Wave Air
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Activity
Commercial air transport-Non-scheduled-Joyflights / sightseeing charters
An ATSB preliminary investigation report details the circumstances leading up to the brief grounding of the Australian research vessel Nuyina off Heard Island, 4,000 km south-west of Perth, last October.
The report details evidence gathered so far in the ongoing transport safety investigation into the 13 October 2025 serious incident, but does not contain analysis or findings, which will be published in a final report at the conclusion of the investigation.
“The grounding occurred while Nuyina, the Australian Antarctic Division’s research and supply vessel, was conducting drone survey operations over the shore of Heard Island, close to an area of uncharted seafloor,” ATSB Chief Commissioner Angus Mitchell said.
On board the vessel were 37 marine crew and 85 expeditioners.
“Nuyina had several scientific instruments installed on a retractable drop keel, which at the time of the incident was extended 75 cm below the vessel’s nominal 9 m draft,” Mr Mitchell explained.
“One of the drop keel devices was a high-resolution multi-beam echo sounder system, which was still collecting data, after having been used for overnight bathymetric surveys in deeper water.”
To avoid acoustic interference, the ship’s navigational echo sounders were switched off.
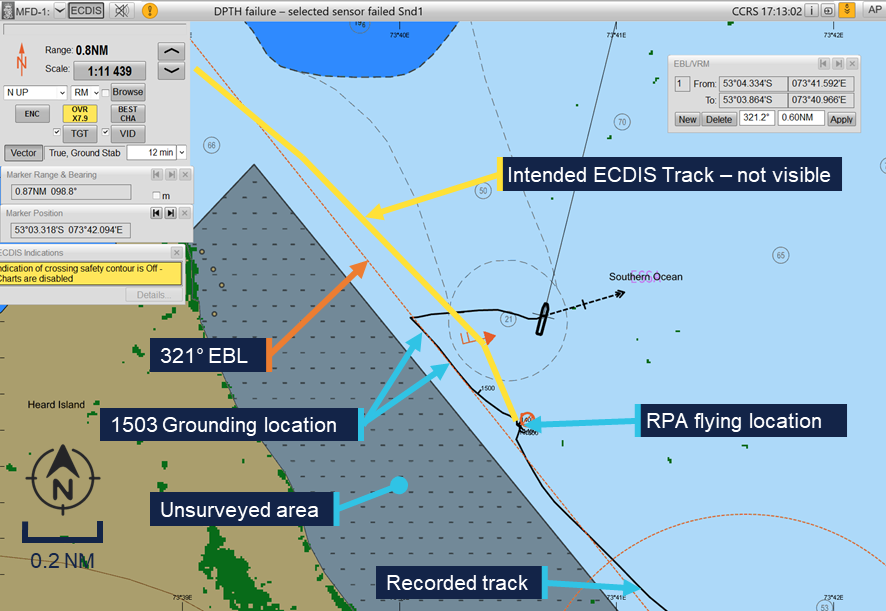
“Depth information from the multi-beam system was shown on a dedicated display on the bridge but was not fed into the ship’s integrated bridge system. This meant the depth information was not displayed on the electronic chart display and information system (ECDIS), and could not be used to generate navigational alarms,” Mr Mitchell said.
Nuyina had been conducting the drone aerial survey work while holding position using its dynamic positioning system off Fur Seal beach before the voyage leader requested the master reposition the ship to a new location around 5 miles to the north-west, the preliminary report details.
After discussion with the second officer the master then planned a route to the new location on the ECDIS planning station in the aft area of the bridge, conducted a route check and loaded it in the system.
The second officer then began turning the ship towards the intended course, which increased the load on the on thrusters as it turned abeam to the wind. On the master’s request the second officer then took the ship on manual control and began the transit.
However, at this point they noted that the new route was not visible on the forward ECDIS.
While the master tried to correct this issue with the ECDIS, the second officer followed an electronic bearing line which had been loaded earlier to guide the ship along the coast while it was conducting the drone flights.
“This bearing line was in a similar direction to the planned route, taking the ship between an unsurveyed area to the west and a charted bank to the east,” Mr Mitchell explained.
A short time later, the acoustics operator contacted the bridge by phone to advise that the multibeam was showing a depth of 15 m. Shortly after, the master ordered ‘stop engines’ followed a short time later by ‘dead slow astern’.
At about the same time the acoustics operator contacted the bridge again, to warn of shallow water.
However, Nuyina then briefly grounded, with its retractable drop keel initially impacting the seabed, followed by the ship’s hull.
The vessel then cleared the shallow water and drifted away from the coast, before the crew stopped its movement and held position.
The drop keel was retracted for inspection, revealing substantial damage with mounted instruments damaged or missing.
The hull of the ship itself only sustained scratches and paint damage.
After consultation with the relevant authorities and experts ashore, Nuyina continued its operations at Heard Island as well as a scheduled resupply operation at Davis station in Antarctica before returning to Hobart.
Mr Mitchell said the ATSB’s investigation had so far included interviews with key personnel, examination of recorded data and CCTV footage, and the gathering of operational documentation and historic and recorded bathymetric data.
“As the investigation proceeds, the ATSB will examine operator procedures, as well as recorded data from the vessel and the bathymetric data, before determining the safety factors which contributed to this occurrence,” he said.
A final report will be released at the conclusion of the investigation.
A firefighting helicopter sustained substantial damage when it unexpectedly lost height when filling its underslung bucket from the Murchison River on Tasmania’s West Coast, an ATSB investigation interim report details.
The twin-engine Bell 412 helicopter, operated by Coulson Aviation, was performing waterbombing activities for the Tasmanian Fire Service in the Cradle Mountain-Lake St Clair National Park in the state’s west on 10 March 2025.
While hovering at about 150 ft over the Murchison River refilling its bucket, which was attached via a longline, the helicopter sank unexpectedly about 50 ft.
While applying recovery control inputs, the pilot, the sole occupant, unsuccessfully attempted to jettison the longline, and it subsequently became taut.
“The helicopter then came to an abrupt stop and the pilot heard a ‘loud clunking noise’,” said ATSB Director Transport Safety Dr Stuart Godley.
“The pilot then recovered the helicopter to a stable hover approximately 30 ft above the water and initiated rearward flight to release the water and retrieve the bucket from the river.”
The pilot then observed an engine torque split – when the proportion of main rotor torque is spread unevenly between the helicopter’s two engines.
“After regaining control and recovering the longline and bucket, the pilot found the tail rotor pedals to be stiff, but said they were still able to control the helicopter.”
The pilot subsequently flew the helicopter back to the air base at Zeehan, about 33 km away.
“During this flight, the air attack supervisor – in a different aircraft – observed the helicopter’s flight as abnormal: slower and lower than usual, and yawing from side to side,” Dr Godley said.
After landing at Zeehan, the pilot was unable to roll the engine throttles back to idle, and had to cut fuel supply to shut the engines down.
A post-flight inspection found substantial damage to the helicopter’s fuselage structure aft of the external hook, and damage to the water bucket.
A technical inspection by the operator the following morning found the #1 (left) engine control tube had sheared, resulting in a complete loss of pilot input to that engine, and the #2 (right) engine control tube bell crank attachment bracket had detached, restricting pilot control of that engine.
Dr Godley noted the investigation had so far included interviews with involved parties, and the review of recorded aircraft information, weather conditions, maintenance documentation and pilot training.
“As the investigation progresses towards a final report, it will also review Coulson’s risk controls for bucketing operations in the Bell 412, and operational and reporting procedures for both Coulson and the Tasmanian Fire Service,” Dr Godley explained.
“A final report will be released at the conclusion of the investigation once the available evidence has been analysed and findings are developed and established.”
The ATSB is investigating a collision with terrain involving a Robinson R44 II, VH-TCF, 46 km north‑east of Tenterfield Airport, New South Wales.
During a private flight from the Gold Coast, Queensland, to Mudgee, New South Wales, the helicopter collided with terrain and a post-impact fire ensued. The pilot, who was the sole occupant, sustained fatal injuries. An ATSB investigation team was deployed to the accident site.
A preliminary report, which detailed factual information established during the evidence collection phase, was released on 30 April 2026 - see below.
The final report has been drafted and is undergoing internal review to ensure the report adequately and accurately reflects the evidence collected, analysis, and agreed findings.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Preliminary report
Report release date: 30/04/2026
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 13 March 2026, the pilot of a Robinson R44 II helicopter, registered VH-TCF, planned to conduct a private flight from Gold Coast, Queensland, to Mudgee, New South Wales (NSW), with an intermediate stop at Armidale, NSW, to refuel (Figure 1).
Figure 1: Map showing accident site and key locations
Source: Google Earth, annotated by the ATSB
At about 0834 Eastern Standard Time (EST),[1] the helicopter departed from a private helipad on the Gold Coast. The pilot was the sole occupant of the helicopter.
NSW Police advised that an automated emergency message associated with activation of the pilot’s iPhone crash alarm was received at 1046 Eastern Daylight-saving Time (EDT),[2] about an hour and a quarter after the aircraft departed. In response, a formal search was commenced by NSW Police.
The wreckage was located at 1113 EDT on 14 March 2026 in dense bushland near Paddy’s Flat, 46 km north-east of Tenterfield, NSW. The helicopter was destroyed and the pilot sustained fatal injuries.
Context
Pilot information
The pilot held a Private Pilot Licence (Helicopter) and a single‑engine helicopter class rating. The pilot also held a class 2 aviation medical certificate valid to 6 September 2026 with the following limitations:
Must use [continuous positive airway pressure] CPAP in sleep period prior to exercising privileges of medical certificate.
Reading correction to be available whilst exercising the privileges of this licence.
Records obtained from the CPAP provider showed that the pilot was regularly using the CPAP machine and that sleep apnoea was controlled.
As of 7 March 2026, the pilot’s logbook showed they had accrued 1,264.6 hours total flight time.
Aircraft information
VH-TCF was a Robinson R44 II helicopter, manufactured in the United States in 2007 as serial number 11912 and first registered in Australia in 2007. The helicopter was powered by a Textron Lycoming IO-540-AE1A5 engine. VH-TCF was being maintained in accordance with the Robinson R44 maintenance manual and the Lycoming IO-540 engine manual. According to the maintenance release, on the morning of 13 March 2026, the helicopter had a total time in service of 2,104.7 hours. There were no defects recorded.
Site and wreckage information
The accident site was located about 46 km north-east of Tenterfield Airport in a densely vegetated area to the west of Cataract National Park. It was situated on the southern side of a steep slope, at an elevation of about 870 m (2,850 ft).
The wreckage trail was approximately 12 m long in a westerly direction, across and down the slope as shown in Figure 2. It consisted of an initial impact point, followed by a trail of debris that led to the fuselage, engine and main rotors, much of which were consumed by a post-impact fire. The aft section of the tail cone assembly had separated from the fuselage and was located approximately 20 m from the fuselage across the slope.
Figure 2: Accident site
Source: ATSB
Significant damage was evident on 2 trees located near the initial impact point, indicating the helicopter had collided with trees in a near vertical descent. A bag found in the tree canopy, and various other parts from the helicopter, were located around 20 m up the slope from the initial impact site.
The instrument panel and other debris were found further down the slope away from the fuselage location. A fuel jerry can, which had been filled at the helicopter’s departure location, was found onsite. The contents were tested for presence of water, which returned a negative result.
Recorded data
Although the pilot was reportedly using the Oz Runways electronic flight bag software, no track data was transmitted to the service provider.
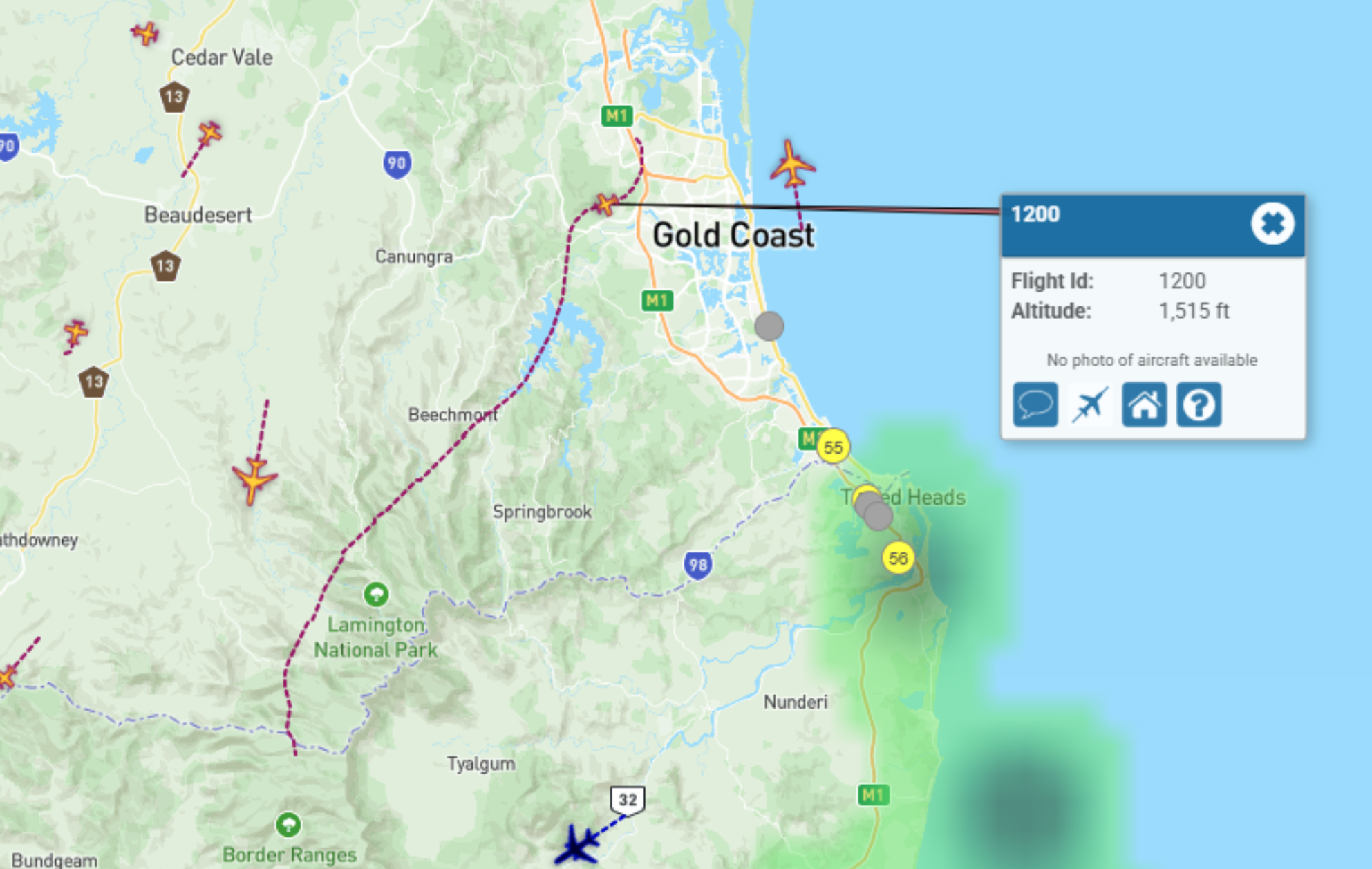
VH-TCF was identified on WebTrak[3] around Gold Coast Airport. It showed that the helicopter tracked roughly south-west before crossing the NSW border at 0854. This service then stopped recording the helicopter’s position (Figure 3).
Figure 3: Aircraft track from departure to the NSW border
Source: Airservices Australia WebTrak
National aeronautical information processing system (NAIPS) records showed that weather information was accessed by the pilot’s account at 0740 and 0745 on 13 March 2026. The requirements of the Aeronautical Information Publication (AIP) ENR 1.10 Flight Planning stated that a pilot must obtain current weather reports and forecasts for the route to be flown, then plan the flight having regard to that information.
Weather information
Forecasts
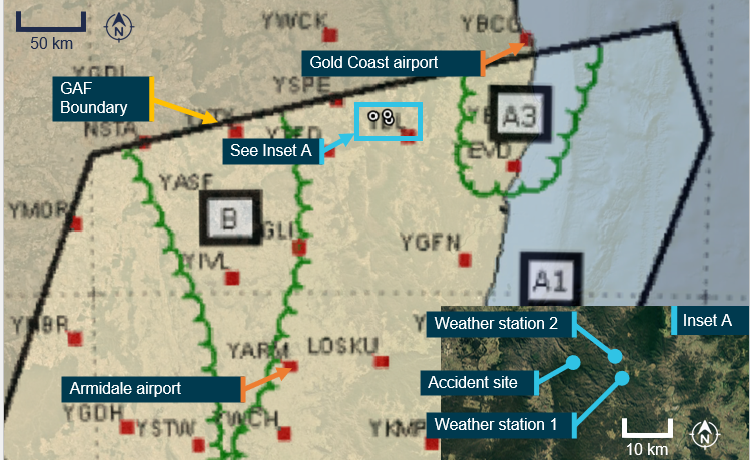
The Bureau of Meteorology graphical area forecast (GAF),[4] issued at 0809 EST on 13 March 2026 for the area encompassing the flight path south of Gold Coast to the accident site (Figure 4), included:
visibility greater than 10 km with broken[5] stratus with bases at 1,500 ft and tops at 2,000 ft and broken stratocumulus with bases at 2,000 ft tops to 9,000 ft
visibility 4,000 m in isolated[6] showers of rain with broken stratus with bases at 1,000 ft and tops at 2,000 ft, and broken cumulus/stratocumulus with bases at 2,000 ft and tops to 9,000 ft
visibility 3,000 m in isolated drizzle with broken stratus with bases at 800 ft and tops at 2,000 ft, and overcast stratocumulus with bases at 2,000 ft and tops to 9,000 ft
in a small coastal area just south of Gold Coast, isolated thunderstorms and rain were forecast, reducing visibility to 2,000 m with associated cumulonimbus with bases at 2,000 ft and tops above 10,000 ft, broken stratus with bases at 500 ft and tops at 2,000 ft, and broken cumulus/stratocumulus with bases at 2,000 ft and tops above 10,000 ft.
Figure 4: Geographical area forecast and additional weather stations
Source: Bureau of Meteorology and Google Earth, annotated by the ATSB
The previous GAF issued at 0226 on the morning of 13 March contained the same information without the forecast small area of thunderstorms. An AIRMET[7] valid from 0624 to 1024, was also issued for isolated thunderstorms in that area.
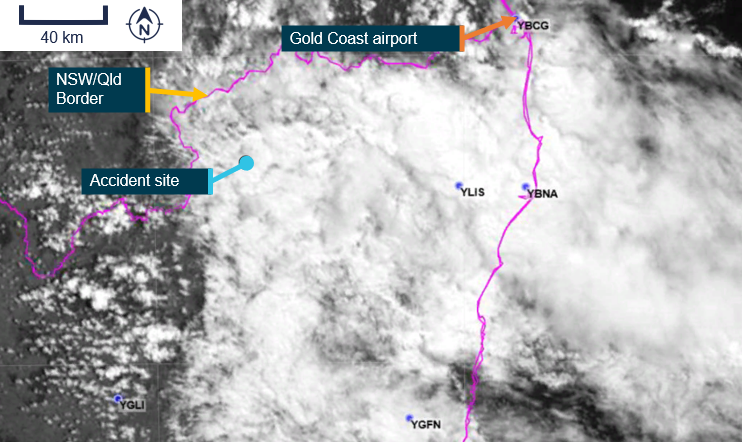
High resolution visible satellite imagery shows cloud extending inland to the NSW/Queensland border, including at the accident site (Figure 5).
Figure 5: Satellite cloud imagery at 1000 EST (14 minutes after the accident)
Source: Satellite image processed by the Bureau of Meteorology from the geostationary meteorological satellite Himawari-9, operated by the Japan Meteorological Agency, annotated by the ATSB
The aerodrome forecast (TAF)[8] for the pilot’s first intended stop at Armidale Airport, NSW, issued at 0422 EDT and valid 0600–1900 on 13 March included:
wind from 080° at 8 kt
visibility greater than 10 km
cloud broken at 400 ft (TAF cloud heights above aerodrome elevation).
During the period 0900–1100:
wind from 100°at 12 kt
visibility greater than 10 km
light showers of rain
scattered cloud at 3,000 ft
temperature 16°C at 0600 and 19°C at 0900
QNH 1,016 hPa at 0600 and 1,019 hPa at 0900.
Weather stations
The ATSB also obtained weather data from 2 Weather Underground[9] stations close to the accident site (inset Figure 2):
Site 1: 12.64 km 106° from the accident site at an elevation of about 530 m (Table 1)
Site 2: 10.67 km 084° from the accident site at an elevation of about 200 m (Table 2).
The ultraviolet (UV) index is a simple way of describing the level of UV radiation and can be affected by the amount of cloud cover. According to the Bureau of Meteorology, ‘thick unbroken clouds and rainfall can reduce UV, as thick clouds reflect and absorb more UV that thin cloud cover.’ The UV Index has 5 categories:
low (1–2)
moderate (3–5)
high (6–7)
very high (8–10)
extreme (11 and above).
The weather stations also measured solar irradiance, which is the power of electromagnetic radiation received from the sun, measured in watts per square metre. According to the National Environmental Satellite, Data and Information Service:[10]
When sunlight hits low clouds, a lot of that light – and heat – is reflected back into space. When sunlight hits clouds that are high in the atmosphere, those clouds reflect less sunlight energy. However, these high clouds also trap more heat.
The UV and solar irradiance[11] values from 13 March indicated that there was substantial cloud coverage at both locations on 13 March between 1004–1104 (Table 1 and Table 2). By comparison, on 15 March 2026, when the ATSB attended the accident site and observed a clear day, at 1119, the solar irradiance was recorded at 923 W/m2 and the UV index was 9.
Table 1: Five-minute weather data, site 1
Local time (EDT)
Temp (°C)
Dew point (°C)
Hum.
%
Wind dir.
Wind (kt)
Gust (kt)
Rain mm
Rain mm/hr
UV
Solar (W/m2)
1004
20.8
20.6
99
ENE
4.8
5.6
0
0
1
95.5
1009
20.9
20.7
99
E
3.1
4.5
0
0
1
94.4
1014
20.9
20.7
99
ESE
4.3
5.7
0
0
1
113.1
1018
20.9
20.7
99
E
3.5
4.8
0
0
1
136
1024
21.1
20.8
99
ESE
4.4
5.6
0
0
1
170
1029
21.1
20.8
99
ESE
3.9
5.0
0
0
1
131.6
1034
21.1
20.9
99
E
4.1
5.1
0
0
1
123.9
1039
21.1
20.9
99
E
4.3
4.9
0
0
1
121
1044
21.1
20.8
99
ESE
5.3
6.3
0
0
1
182.3
1049
21.1
20.8
99
ENE
3.0
4.6
0.05
1.27
1
94.3
1054
20.8
20.6
99
E
4.8
6.6
0.1
2.54
1
127.8
1059
20.8
20.6
99
ESE
3.3
5.0
0.1
2.54
1
102
1104
20.5
20.3
99
E
4.9
7.9
0.05
1.27
1
100.5
Table 2: Five-minute weather data, site 2
Local time (EDT
Temp (°C)
Dew point (°C)
Hum.
%
Wind dir.
Wind (kt)
Gust (kt)
Rain mm
Rain mm/hr
UV
Solar (W/m2)
1004
24.0
20.9
83
SSE
2.5
3.0
0
0
1
95.5
1009
23.8
20.9
84
WSW
1.8
2.4
0
0
1
94.4
1014
24.1
20.9
83
ENE
1.1
1.4
0
0
1
113.1
1019
24.3
20.9
82
NW
1.3
1.8
0
0
1
136
1023
24.5
21.0
81
ESE
2.1
3.1
0
0
2
170
1029
24.5
20.8
80
NNE
2.6
3.6
0
0
2
131.6
1034
24.8
20.9
79
ESE
2.0
2.9
0
0
2
123.9
1039
24.6
20.8
80
W
3.5
4.8
0
0
1
121
1044
25.3
21.1
78
NNE
1.7
2.3
0
0
2
182.3
1049
25.6
21.1
77
ENE
2.1
3.2
0
0
2
94.3
1054
25.4
21.1
77
NNW
2.3
3.0
0
0
2
127.8
1059
25.1
20.9
78
ENE
2.4
4.2
0
0
1
102
1104
24.7
21.1
81
ENE
1.9
3.4
0
0
1
100.5
Visual meteorological conditions
For flights under the visual flight rules (VFR),[12] the Civil Aviation Safety Regulations Part 91 Manual of Standards specified criteria for visual meteorological conditions (VMC)[13] in terms of visibility and distance from cloud. The criteria for all aircraft operating in Class G (non‑controlled) airspace were:
At or below whichever is the higher of 3,000 ft AMSL and 1,000 ft above ground level (AGL):
visibility 5,000 m
clear of cloud
aircraft must be operated in sight of ground or water.
For helicopters (rotorcraft) operating below 700 ft over land in non‑controlled airspace (and not within 10 NM of an aerodrome with an instrument approach procedure), the criteria were:
flight visibility 800 m
clear of cloud
by day
at a speed that allows the pilot to see obstructions in sufficient time to avoid a collision.
Witness information
Several witnesses located near the accident site (Figure 6) stated that they observed a helicopter flying very low, ‘before lunchtime’ on the day of the accident. All witnesses reported that it was unusual to see a helicopter in the area, but this one was particularly unusual due to its low altitude.
All witnesses reported very low cloud and drizzle on the morning of the accident. One witness stated that the helicopter seemed to be stuck below cloud and remarked to their partner that it ‘looks like it’s trying to find a way out’. Another witness recalled waving at the helicopter and stated that it passed them twice before heading west.
Figure 6: Witness locations
Source: Google Earth, annotated by the ATSB
Further investigation
To date, the ATSB has
examined the site and wreckage
retained drive shaft components and warning light bulbs for examination
interviewed witnesses and involved parties
obtained recorded flight data
obtained aircraft and operational information
obtained meteorological information.
The investigation is continuing and will include further review and examination of:
the mapped accident site and helicopter wreckage
aircraft and operational documentation
meteorological information.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB acknowledges the assistance of New South Wales Police, in particular the Lismore Search and Rescue unit.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Eastern Standard Time (EST): Coordinated Universal Time (UTC) + 10 hours
[2]Eastern Daylight-saving Time (EDT): Coordinated Universal Time (UTC) + 11 hours
[3]WebTrak uses information from air traffic control secondary surveillance radars to display aircraft movements.
[4]In a graphical area forecast (GAF), all cloud heights are above mean sea level (AMSL).
[5]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky, ‘broken’ indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
[6]Weather coverage is given as isolated if it consists of individual features which affect, or are forecast to affect, an area with a maximum spatial coverage of up to 50%.
[7]AIRMET provides information of certain meteorological phenomena that are not contained in the current area forecast.
[8]A TAF is a coded statement of meteorological conditions expected at an aerodrome and within a radius of 5 nautical miles of the aerodrome reference point.
[9]Weather Underground provides local and long-range weather forecasts, weather reports, maps and tropical weather conditions for locations worldwide.
[10]The National Environmental Satellite, Data, and Information Service (NESDIS) manages the United States environmental satellite programs, and manage the data gathered by the National Weather Service and other government agencies and departments.
[11]Solar irradiance is the power per unit area or electromagnetic radiation received from the sun, measured in Watts per square metre.
[12]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[13]Visual Meteorological Conditions (VMC): an aviation flight category in which visual flight rules (VFR) flight is permitted – that is, conditions in which pilots have sufficient visibility to fly the aircraft while maintaining visual separation from terrain and other aircraft.
Occurrence summary
Investigation number
AO-2026-067
Occurrence date
13/03/2026
Occurrence time and timezone
10:59 Australian Eastern Daylight Time
Location
About 46 km north-east of Tenterfield Airport
State
New South Wales
Report release date
30/04/2026
Report status
Preliminary
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Internal review
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R44 II
Registration
VH-TCF
Serial number
11912
Aircraft operator
Tasklake Pty Ltd
Sector
Helicopter
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Sport and pleasure flying / Pleasure and personal transport
The Australian Transport Safety Bureau has commenced a transport safety investigation into an accident involving a Robinson R44 helicopter in the Cataract National Park near Tenterfield, NSW.
The helicopter, which was operating a private flight from the Gold Coast to Armidale, was reported missing on Friday night and was discovered by search and rescue on Saturday.
ATSB transport safety investigators from Canberra and Brisbane are deploying to the accident site, where they are expected to arrive on Sunday. Over coming days they will conduct a range of evidence-gathering activities including site survey, wreckage examination, and retrieval of relevant components for further examination and analysis at the ATSB’s Canberra technical facilities.
As well as on-site activities, investigators will also interview involved parties and any witnesses, obtain pilot and aircraft maintenance records, and collect any available recorded flight tracking data as well as weather information.
The ATSB asks anyone who witnessed the accident, including ear witness, or anyone with video footage of the aircraft at any stage of its flight, to make contact via the witness form on our website - atsb.gov.au/witness - at their earliest opportunity.
The ATSB anticipates publishing a preliminary report, detailing factual information about the circumstances of the accident, in about 8 weeks.
A final report detailing findings and the analysis to support those findings will be released at the conclusion of the investigation. However, if the investigation identifies a critical safety issue at any time the ATSB will immediately inform relevant stakeholders.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the early morning of 15 February 2026, a Kavanagh Balloons E240 hot air balloon with a pilot and 10 passengers aboard was conducting a scenic flight over the inner eastern suburbs of Melbourne, Victoria. After launching from Mayer Park, Thornbury, the balloon followed a predominantly southerly track, and after around 40 minutes of flight, was approaching a landing at Fawkner Park, South Yarra. Describing the approach as stable at 100 ft on a track of 195 degrees towards the targeted landing point at the northern end of the park, the pilot reported noting that several other balloons had already landed in that area, so elected to extend towards the park’s south-west.
On final approach, the balloon encountered an abrupt wind direction change, with the track shifting right to 214 degrees. Judging that a landing was still possible ahead of the new direction of travel, the pilot transitioned to a landing, however there was insufficient space available to accommodate the balloon’s envelope, which contacted and became entangled with a tree as it deflated upon landing (Figure 1).
Neither pilot nor passengers were injured during the landing, however the envelope sustained substantial damage from the tree contact, with several fabric panels punctured and torn around the equatorial region.[1]
Figure 1: Entangled balloon envelope after landing
Source: Witness, annotated by the ATSB
Safety message
The ATSB SafetyWatchhighlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is Reducing passenger injuries in commercial ballooning operations.
Commercial ballooning operations was added to SafetyWatch after the ATSB identified a trend toward a heightened exposure to risk in the sector, as compared to other forms of charter aviation.
This occurrence reinforces the need for all hot air balloon pilots to be prepared to discontinue a landing approach if changing conditions result in an increased risk of contact with ground obstacles and hazards in the direction of flight.
The risks associated with landing profiles can change markedly with varying wind conditions. Pilots must plan onboard fuel loads and projected downwind tracks to ensure options remain open and viable for continued safe flight and subsequent landing/s, should an initial landing be rejected for any reason.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Balloon envelope equatorial region: the band of fabric panels extending around the circumference of the balloon envelope at its widest point.
The ATSB is investigating an inadvertent restraint release involving Avions Mudry & Cie CAP 10B, VH-YAO, 29 km north-north-west of Edinburgh Airport, South Australia, on 4 February 2026.
During flight training with an instructor and a student, the instructor demonstrated a split S manoeuvre from inverted flight. At that time the instructor's centre harness buckle released unexpectedly. The instructor was lifted out of the seat and struck the overhead canopy.
This resulted in a brief release of the flight controls before the instructor regained control and recovered the aircraft. The aircraft sustained minor damage from cracking to the windscreen and partial detachment of the canopy. The aircraft landed without further incident. The student was uninjured and the instructor sustained minor injuries.
The ATSB has completed the evidence collection and analysis phases of the investigation and is drafting the final report.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Occurrence summary
Investigation number
AO-2026-066
Occurrence date
04/02/2026
Occurrence time and timezone
19:34 Central Australia Daylight Time
Location
29 km north-north-west of Edinburgh Airport
State
South Australia
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Drafting
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Furnishings & fittings, Loss of control
Occurrence class
Serious Incident
Highest injury level
Minor
Aircraft details
Manufacturer
Avions Mudry & Cie
Model
CAP 10B
Registration
VH-YAO
Serial number
266
Aircraft operator
Flight Training Adelaide Pty Ltd
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Activity
General aviation / Recreational-Instructional flying-Instructional flying - dual
An ATSB preliminary report outlines the order of events leading up to the grounding of the cruise ship Coral Adventurernear a remote port on the north-east coast of Papua New Guinea in December.
The ATSB launched a transport safety investigation after the 93-metre Australian-flaggedshipgrounded on the morning of 27 December 2025, with 80 passengers and 44 crew on board.
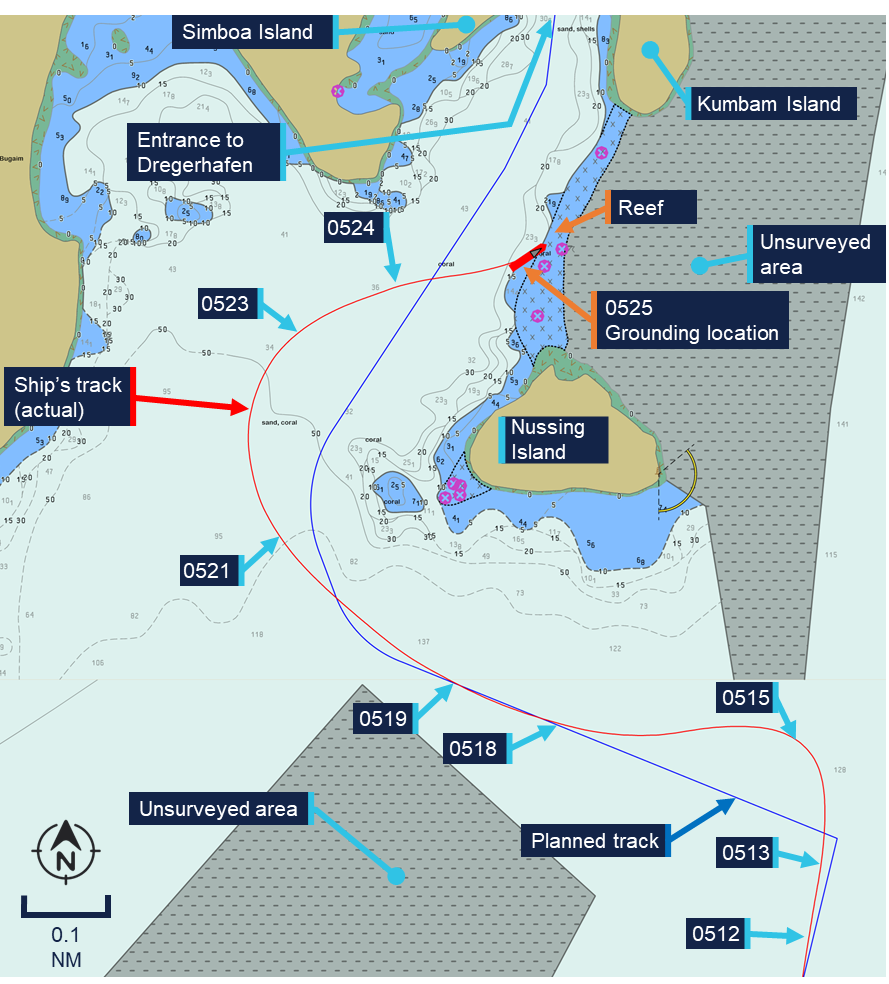
The cruise, which had left Cairns 10 days earlier, had visited several sites in Papua New Guinea, with passages between them generally conducted overnight. On the morning of the accident, the ship was towards the end of one such overnight passage, from Lababia to Dregerhafen.
The planned route to enter Dregerhafen involved first turning to port, so the ship could pass south of Nussing Island, and then turning to starboard, to continue towards the harbour entrance.
During the night, the chief mate had made a small change to this route in the ship’s Electronic Chart Display and Information System (or ‘ECDIS’, the ship’s digital navigation system), intending to smooth out the second turn.
At about 0512, as the ship approached Dregerhafen, the chief mate attempted to select this modified route in the ECDIS, but found it would not load until a ‘route safety check’ had been performed via the ECDIS’s route editor function.
While the chief mate was addressing this issue, the ship travelled past its first waypoint for the planned turn to port.
After resolving the ECDIS issue and realising the waypoint had been missed, the chief mate switched the steering from autopilot to manual, to expedite the turn to port and quickly regain the planned track.
“During this hard manual turn, the ship slowed considerably, to 3.8 knots,” ATSB Chief Commissioner Angus Mitchell said.
“The chief mate, perceiving the loss of speed was due to a strong current, increased the RPM setting of both Azipull thrusters.”
At about 0518, the ship had returned to the planned track, and the chief mate switched the steering mode back to autopilot. Speed had now increased to around 8 knots, 2.5 knots higher than planned.
As the ship arrived at the wheel over point for its second turn, the chief mate altered course to starboard but the ship did not turn as quickly as anticipated, resulting in a wider than planned turn.
With the ship now travelling at 8.5 knots and roughly 200 m west of its planned track, the chief mate switched back to manual steering and increased the rate of turn.
“At this point, in dark conditions and without navigational aids or lights ashore, the chief mate reported being unable to visually identify the surrounding topography in relation to what was being shown on the ECDIS,” Mr Mitchell explained.
The preliminary report notes the master arrived on the bridge around this time, however the ship continued past the planned track and grounded on a reef about 160 m east of it.
Coral Adventurer came to rest and was heeled over about 6 degrees to port. There were no reported injuries to those on board. The ship sustained hull indentation damage, and some structural deformation.
After initial refloating efforts were unsuccessful, all passengers were disembarked on 30 December 2025. The ship was refloated a short time later, and navigated to a safe anchorage for further assessment.
ATSB investigators attended Coral Adventurer while at anchor to collect relevant recorded data, documentary evidence, and to interview members of the ship’s crew.
Mr Mitchell said collection of other relevant evidence is being progressed, and the investigation was continuing, with analysis and findings to be developed for publication in a final report.
“As the investigation progresses, it will consider the data captured by the ship’s voyage data recorder, as well as available CCTV footage,” Mr Mitchell said.
“Investigators will also analyse human factors considerations, and will review the ship and its operator’s passage planning and navigation procedures, including resource management.
“There will also be a review of the ship’s emergency response procedures, and overall safety oversight.”
If a critical safety issue is identified during the investigation, Mr Mitchell said the ATSB would immediately notify relevant parties.
“The final report will contain analysis and findings, as well as any safety actions taken, or our recommendations for such actions to be taken,” he concluded.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On the morning of 18 January 2026, the pilot of a RotorWay Exec 90 amateur-built light helicopter was conducting a local flight from a private property near Tamborine, Queensland, with one passenger on board. The pilot reported that during the hover, in preparation for landing, they experienced a sudden loss of tail rotor authority, followed by the onset of uncontrolled yaw[1] and rotation. To counter, the pilot lowered the collective[2] and set the helicopter down, however the helicopter’s rotation as it contacted the ground caused it to roll over and sustain substantial damage. Neither the pilot nor passenger were injured.
Figure 1: Damaged helicopter after recovery
Source: Operator supplied
Engineering information
The RotorWay Exec 90 is a kit-produced light utility helicopter manufactured by the RotorWay Helicopter Manufacturing Company (formerly RotorWay International) and intended for amateur construction. As-designed, the helicopter has a maximum take-off weight (MTOW) of 680 kg (1,500 lb) and is powered by a horizontally opposed 4-cylinder piston engine delivering 112 kW (150 hp).
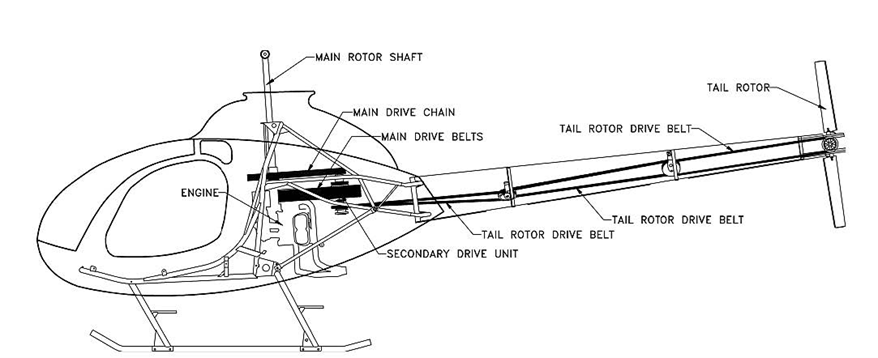
The Exec 90 powertrain employed a v-belt system that transferred drive to the tail rotor through a series of 3 belts and 2 idlers, extending from the secondary drive unit adjacent to the engine, through the tail boom, to the tail rotor pulley (Figure 2).
Source: UK Air Accidents Investigation Branch report AAIB-27186 (AAIB Bulletin 8/2022)
At the time of the accident, the helicopter had accumulated 64 hours total time in service. Upon inspection after the accident, evidence of the failure of the centre tail rotor belt was found within the tail boom structure – consistent with the loss of tail rotor effectiveness experienced by the pilot prior to the ground contact. The pilot reported that the tail rotor belt had operated for approximately 30–40 hours since new.
Figure 3: Remnants of a loose / fractured tail rotor drive belt found within the tail boom
Source: Operator supplied, annotated by ATSB
Inspections and service bulletins
The pilot reported that tail rotor belt tension had been checked with the manufacturer’s recommended tool before the flight, and noted that there were no indications of imminent belt failure leading up to the loss of tail rotor drive.
Section 3 (D) of the RotorWay Exec 90 flight manual requires a pre-flight inspection of the tail rotor drive components, including the condition and tension of the drive belts, and includes the caution:
IMPORTANT: New belts will tend to stretch and become loose. Belt tension must be monitored and adjusted frequently until stretching has stopped.
Further, the helicopter kit manufacturer has published several mandatory and advisory service bulletins applicable to the Exec 90 helicopter tail rotor drive system.
Bulletin number
Publication date
Subject
M-07 (mandatory)
8 September 1992
Prohibition of certain tail rotor belt makes
M-20 (mandatory)
4 April 2002
Inspection for proper tail rotor belt routing
A-20 (advisory)
28 November 1994
Inspection and importance of tail rotor belt tension
A-21 (advisory)
12 May 1995
Tail rotor belt inspection, tensioning, and temperature monitoring
A-25 (advisory)
21 December 1995
Cold weather inspection of tail rotor belt tension
A-36 (advisory)
4 April 2002
Inspection for proper tail rotor belt routing
Most of these bulletins centred on the importance of regular inspection and checking of tail rotor belt tension, and bulletin A-21 further noted:
Advisory Bulletin A-20 (dated November 28, 1994) stressed the importance of checking the condition and tension of the belts before every flight. Although this may be time consuming, these pre-flight checks are essential to the continued safe operation of your helicopter.
Safety message
RotorWay Exec 90 helicopters (and related types with belt-driven tail rotor systems) have an established sensitivity to tail rotor belt tension, with an operational history of failures associated with improperly tensioned belts.
Pilots, owners and operators of these helicopters are reminded to ensure that all applicable checks, inspections and maintenance activities are carried out on the tail rotor drive system, with particular attention to the tension, condition and service life of the belts.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Yaw: the motion of an aircraft about its vertical or normal axis.
[2]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 24 January at 0900 local time, the pilot of a Robinson R22 Beta helicopter was conducting cattle mustering operations at a private property near Theodore, Queensland.
During a low-level manoeuvre, the pilot attempted to block a herd of cattle running alongside a fence line when the helicopter’s tail rotor contacted the top wire of the fence, resulting in the helicopter rotating rapidly. The pilot observed an immediate lack of tail rotor authority[1] and estimated the helicopter rotated 2 or 3 times. With insufficient height to recover the helicopter safely, the pilot conducted a forced landing next to the fence line. To reduce the severity of the helicopter’s rotating motion during the forced landing, the pilot closed the throttle and applied cyclic[2] to keep the helicopter level while descending. Prior to contact with the ground, the pilot raised the collective[3] to try to soften the landing. The helicopter landed hard resulting in the skids splaying outwards. The main rotor subsequently contacted the tail boom and the cockpit windscreen shattered (Figure 1). The pilot extracted themself from the helicopter and waited nearby for assistance.
Figure 1: Forced landing site
Source: Operator
As a result of the accident, the pilot sustained several fractured vertebrae. At the time of the occurrence, the pilot was wearing a flight helmet.
Safety message
Helicopter mustering is an operation that carries increased risk, particularly when manoeuvring at low level. Ground obstacles are hazards that pilots must actively monitor to ensure adequate separation from the aircraft. An inadvertent collision with an obstacle at a low level limits the available safety margins for recovery or time to execute emergency procedures.
In the case of this occurrence, the pilot’s immediate response followed the Robinson R22 emergency procedure for a loss of tail rotor effectiveness as stated in the R22 Pilot’s Operating Handbook. These actions likely reduced the severity of the accident and the injuries sustained by the pilot.
A similar occurrence the ATSB investigated into a Tail rotor strike involving Robinson R22 Beta II, VH-HGE, 58 km north-west of Anthony Lagoon, Northern Territory, on 1 July 2025 (AO-2025-035) discusses the benefits of conducting recency training for emergency procedures.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Lack of tail rotor authority: a lack of thrust produced by the tail rotor to counter the torque produced by the main rotor.
[2]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[3]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.