
Foreign object debris involving Airbus A380, VH-OQK, Sydney Airport, New South Wales, on 9 January 2026
Summary
The ATSB is investigating an occurrence where a tool was located inside the left wing of a Qantas Airbus A380, registered VH-OQK, on 9 January 2026. The aircraft had flown 2 sectors prior to the tool being located.
In the course of the investigation, the ATSB has identified potential limitations in risk controls relevant to the occurrence. Examination of these factors represent an increase in the scope of this investigation, and it has been upgraded from Short to Defined as a result (the ATSB's different levels of investigation are detailed here).
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
| Investigation number | AO-2026-004 |
|---|---|
| Occurrence date | 09/01/2026 |
| Occurrence time and timezone | 15:00 Australian Eastern Daylight Time |
| Location | Sydney Airport |
| State | New South Wales |
| Report status | Pending |
| Anticipated completion | Q3 2026 |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Internal review |
| Investigation status | Active |
| Mode of transport | Aviation |
| Aviation occurrence category | Foreign object damage / debris |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Airbus |
|---|---|
| Model | A380-842 |
| Registration | VH-OQK |
| Serial number | 0063 |
| Aircraft operator | Qantas Airways Limited |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Activity | Commercial air transport-Scheduled-International |
| Departure point | Dallas/Fort Worth International Airport, United States of America |
| Destination | Sydney Airport, New South Wales |
| Injuries | None |
| Damage | Nil |
Hard landing and runway excursion involving a Cessna 150H, West Sale Airport, Victoria, on 22 December 2025
What happened
On 22 December 2025 at 1640, a pilot was conducting circuit operations with one passenger on board a Cessna 150H at West Sale Airport, Victoria.
In contrast to the recorded weather conditions, the pilot identified a left-hand crosswind via the aerodrome windsock for the one runway available. Alternate grass runways were unavailable due to rain in the preceding 24 hours.
During landing in the crosswind on runway 27, the pilot ‘crabbed’ by yawing[1] the nose of the aircraft into the wind to prevent the aircraft from drifting off the centreline. The pilot assessed that the approach was stable and proceeded to touch down. During rollout, after the flare, the aircraft encountered a gusting wind, resulting in the aircraft ballooning[2] and yawing to the right. In response, the pilot attempted to counteract with a left yaw. However, the conditions exceeded the aircraft’s capabilities and the aircraft was carried to the right, and the right wheel contacted the runway surface. The right main landing gear collapsed, and the right wing tip struck the ground before the aircraft veered off the runway.
The pilot and passenger exited the aircraft without injuries, and the aircraft was substantially damaged (Figure 1).
Figure 1: Damage to the Cessna 150H right landing gear

Source: Aircraft owner
Safety message
Crosswind gusts during the later stages of landing can present challenges for pilots. Depending on the magnitude and direction of the gust, there may be insufficient time to apply corrective controls before the aircraft deviates from the intended path.
Once the aircraft wheels touch down, it's important to remain focused and use your rudder to keep the aircraft straight, even after you have touched down, to retain control and stability.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2026-001 |
| Occurrence date | 22/12/2025 |
| Location | West Sale Airport |
| State | Victoria |
| Occurrence class | Accident |
| Aviation occurrence category | Control issues, Hard landing, Runway excursion |
| Highest injury level | None |
| Brief release date | 23/01/2026 |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 150H |
| Sector | Piston |
| Operation type | Part 91 General operating and flight rules |
| Damage | Substantial |
Forced landing after engine failure in Piper Cherokee
A Piper Cherokee conducted a forced landing on a Sydney golf course after an exhaust valve broke in the aircraft’s engine, resulting in a rapid loss of power, an ATSB investigation has found.
The accident occurred during a 17 August 2025 navigation training flight, which had taken off from Wollongong (Shellharbour) Airport with a student pilot and an instructor on board.
While around 1,600 ft above the coast north of Sydney, the crew heard unusual noises and observed a rapid drop in engine RPM.
“Fortunately, the instructor was proactive in maintaining an awareness of potential landing sites throughout the flight,” ATSB Chief Commissioner Angus Mitchell said.
The report notes the instructor initially wanted to reach Long Reef golf course, with fewer trees, but maintained awareness of Mona Vale golf course being closer in case engine performance worsened.
“About six minutes into the occurrence, as the engine RPM progressively decreased, the instructor was able to determine that the safest option would be to conduct a landing on the Mona Vale golf course,” Mr Mitchell said.
During the final stages of the approach, however, the pilot realised they had positioned the aircraft such that they could not safely land straight ahead, and so made a right turn to avoid the golf course facilities.
During the turn the right wing dropped. The aircraft subsequently landed heavily, resulting in substantial damage, and minor injuries to the student pilot.
Nonetheless, Mr Mitchell said, the pilot’s prompt identification of a suitable forced landing site meant a worse potential outcome was avoided.
“This investigation highlights the importance of effective decision-making skills in emergency situations,” he said.
The source of the engine failure was found to be the exhaust valve of the engine’s number 3 cylinder, which broke away from its stem and caused extensive damage to the internal surfaces of the cylinder, its piston and spark plugs.
In this case, the cause of the exhaust valve failure could not be determined. However, the ATSB’s final report notes the engine’s manufacturer, Textron Lycoming, has provided maintenance practices to reduce the possibility of valve sticking.
“Operators and maintainers should be aware the risk of valve sticking is increased for engines operating in hot ambient conditions, and where engines are regularly shut down before they have cooled sufficiently,” Mr Mitchell concluded.
After the accident, the training operator undertook several safety actions, including revising its emergency briefing content, completing a review of competency in conducting engine failure procedures for its instructors, and commencing a process to check students’ post-engine failure competencies.
Read the final report: Loss of power and forced landing involving Piper PA-28, VH-BUN, 32 km north-north-east of Sydney Airport, New South Wales, on 17 August 2025
Cressy level crossing collision
A transport safety investigation has been launched into a collision between a utility vehicle and a freight train at a level crossing in western Victoria on Tuesday morning.
The collision occurred around 10:15 am local time at the Reddies Road passive level crossing at Cressy. Tragically, two people in the utility vehicle were fatally injured. The train drivers were not physically injured, and the train remained on the tracks.
The independent, ‘no blame’ transport safety investigation will be conducted by Victoria’s Office of the Chief Investigator under a collaboration agreement with the Australian Transport Safety Bureau.
A team of investigators arrived on site on Tuesday afternoon to commence the investigation.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the investigation, relevant parties will be notified immediately, so that appropriate safety action can be taken.
Background: The Office of the Chief Investigator (OCI) is the operational office of the Chief Investigator, Transport Safety, a statutory position established in the Transport Integration Act 2010 (Vic) to provide independent, no blame investigation of transport safety matters in Victoria.
OCI can investigate rail occurrences in Victoria under the Transport Safety Investigation Act 2003 (Cth), under a collaboration agreement with the Australian Transport Safety Bureau.
The ATSB is Australia’s national transport safety investigator, and conducts no blame aviation, rail and marine transport safety investigations to help prevent the occurrence of similar future accidents.
Runway excursion and collision with terrain involving an Air Tractor AT-802A, 82 km north-west of Hopetoun, Victoria, on 4 December 2025
What happened
On 4 December 2025, at 1720 local time, an Air Tractor AT-802A was preparing to conduct aerial firefighting operations from Linga Airbase, Victoria. Before departure the pilot briefly consulted electronic maps for Linga Airbase, however, did not observe that runways 17 and 19 were 2 separate runways with runway 19 commencing at the end of runway 17 rather than a single longer runway (Figure 1). After loading the aircraft with fire retardant, the pilot commenced taxi for runway 17, believing they were backtracking to use the entire length of runways 17 and 19. The pilot completed their take-off checks and commenced the take-off roll.
The pilot reported that during the take-off run, due to the upslope on runway 17, they were unable to see the threshold of runway 19 until the aircraft had crested the rise towards the end of runway 17. Unaware of the 20° right turn, on becoming visual with runway 19, the pilot assessed the turn was too sharp to navigate and the aircraft was travelling too fast to stop and not yet fast enough to become airborne.
Figure 1: Linga Airbase, Victoria

* Wind direction was recorded 82 km away at Hopetoun, Victoria. Source: Google Earth, annotated by the ATSB
The pilot maintained the runway 17 heading, and the aircraft overran the end of runway 17 into a field, impacting a fence, before becoming airborne. The pilot intended to release the load of fire retardant to reduce weight, however, due to their unfamiliarity with the location of the load release switch in that aircraft, instead activated the aircraft lights, before locating the correct switch and dumping the load. Images show the left-wing tip dragged along the surface of the field while the load was dumped. A witness reported the aircraft briefly became airborne with a nose high attitude and left wing down in a left turn before the left wing again contacted the ground and pulled the aircraft to the ground before coming to a stop (Figure 2).
Figure 2: Occurrence aircraft impact marks and final position
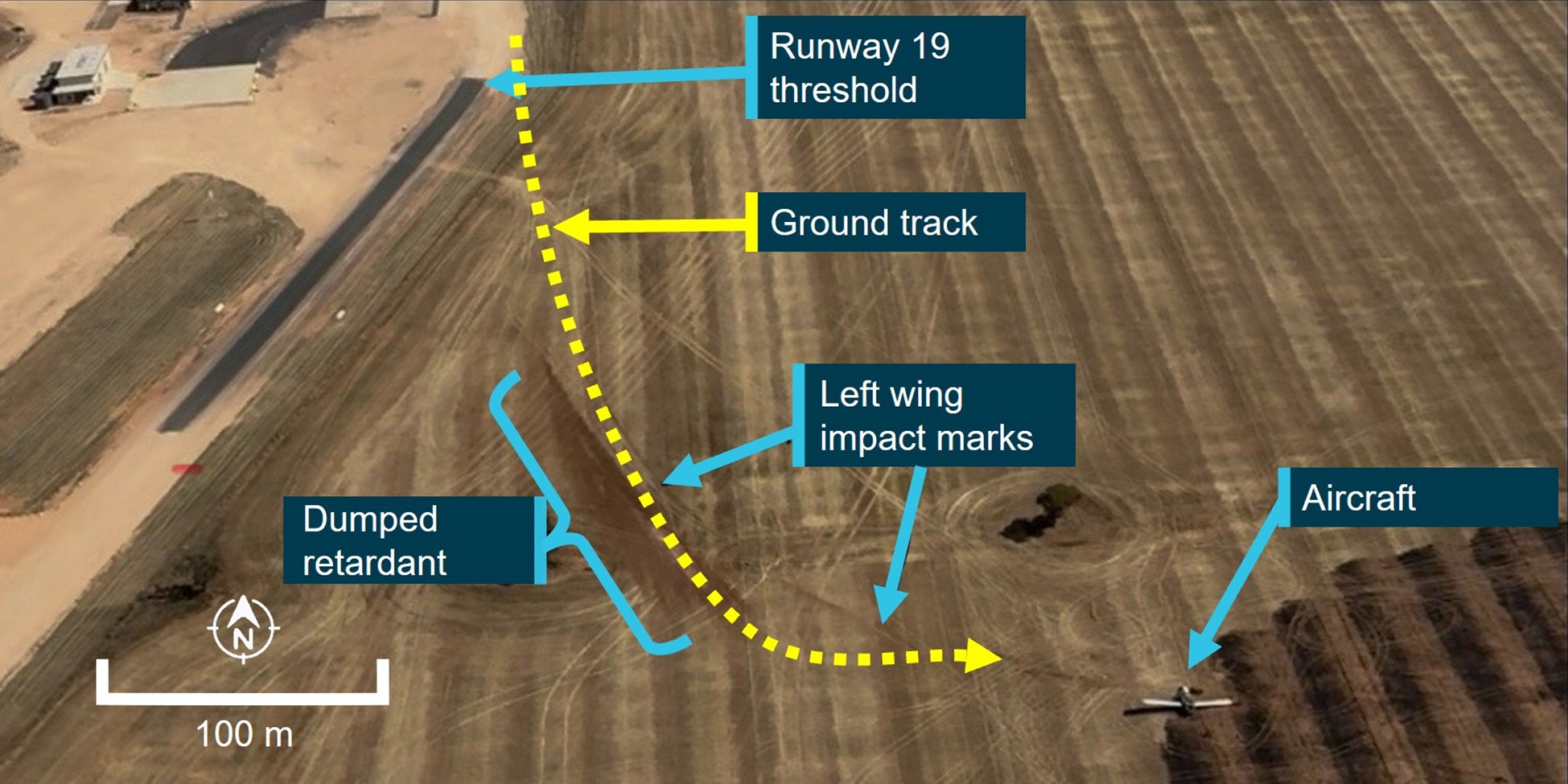
Source: Operator, annotated by the ATSB
The impact was sufficient to liberate the engine and propeller from the aircraft which subsequently set fire to the field (Figure 3). The local airbase manager and 2 other state government employees attended the scene and were able to put the fire out in the vicinity of the aircraft and were then able to assist the pilot to egress the aircraft.
The pilot sustained minor injuries and was admitted to Mildura hospital. The aircraft was substantially damaged.

Source: Operator
The pilot reported that they had not previously operated from Linga Airbase, and earlier when arriving in the circuit they joined a midfield crosswind leg for runway 01 before landing, and had not observed the angle of the adjoining runways from the air.
The airbase manager reported other firefighting aircraft had been using runway 19 throughout the day. Linga Airbase runway 17 was about 660 m in length and joined the northern end of runway 19 which measured about 1,000 m in length. The aircraft was loaded with retardant to the western side of where runways 17 and 19 met.
The pilot reported the wind direction during the take-off roll was a crosswind. Conditions around the time of the occurrence recorded at Hopetoun, Victoria indicated temperature of 38°C with winds gusting between 16–33 kt from the north-west.
The aircraft loading log for the day of the occurrence indicated it was loaded with about 2,300 L of fire retardant. This gave the aircraft a take-off weight of about 6,900 kg, which was below the aircraft’s maximum take-off weight for the conditions. The operator reported the aircraft’s performance in the hot conditions required a take-off ground roll distance of about 1,000 m.
Although they were an experienced agricultural pilot, they had not previously operated from that airbase. Although the pilot observed other aircraft depart using runway 19 while reloading, they assumed they were not using the entire length of the runway, and by taxiing and backtracking to the threshold of runway 17 believed they were increasing their take-off roll distance. Performance calculations indicated that due to the air temperature, weight of the aircraft and wind conditions, the aircraft would have required the full length of the longer runway 19 to become airborne.
Safety message

The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing the severity of injuries in accidents involving small aircraft. As a result of the aircraft’s sudden stop the pilot’s flight helmet was damaged in the occurrence and they suffered a laceration to their head. Therefore, it was likely the pilot’s helmet prevented a more serious head injury.
Thorough pre-flight planning is essential to safe flight and is especially important when operating from unfamiliar airports. A clear understanding of the take-off distances available and runway configuration improves pilots’ situational awareness, reducing the possibility of the unexpected during higher risk stages of flight such as take-off and landing.
Aerial firefighting operations are often conducted in conditions of extreme heat and wind; accurate performance calculations including take-off weight and available runway distance are essential for safe operations in challenging conditions.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2025-065 |
| Occurrence date | 04/12/2025 |
| Location | 82 km north-west of Hopetoun |
| State | Victoria |
| Occurrence class | Accident |
| Aviation occurrence category | Collision with terrain, Runway excursion |
| Highest injury level | Minor |
| Brief release date | 21/01/2026 |
Aircraft details
| Manufacturer | Air Tractor Inc |
|---|---|
| Model | AT-208 |
| Sector | Turboprop |
| Operation type | Part 138 Aerial work operations |
| Damage | Substantial |
Non-specific pre-flight inspection procedures contributed to pitot covers incident

Poor visibility, an incorrect assumption, and non-specific operator procedures contributed to a Metroliner freight aircraft taking off from Townsville with both of its pitot tubes still covered, an ATSB final report details.
The incident occurred at night, in heavy rain on 10 February 2025, when the Fairchild SA227 twin turboprop was being prepared for a freight flight from Townsville to Brisbane, Queensland.
The same aircraft had been flown into Townsville by the same captain and first officer on the morning of the incident. After landing in Townsville around 0800, the flight crew had conducted a terminating check and installed engine bungs, static port covers, and pitot tube covers, before ending their duty and spending the day resting.
After coming back onto duty shortly after 1800, the flight crew began to prepare the aircraft for its return trip to Brisbane.
The first officer removed the engine bungs and static port covers, but was unable to reach the pitot tube covers, so asked the captain to remove them. The captain said they would remove the tube covers but subsequently forgot.
The first officer incorrectly assumed the captain had removed the covers, and the flight crew proceeded to taxi for take-off.
Due to the conditions, neither crew could see the pitot tube covers on the nose of the aircraft during their taxi.
“The flight crew recognised slowly rising airspeed indications during the take-off roll but did not identify that this was symptomatic of blocked pitot tubes,” ATSB Director of Transport Safety Stuart Macleod said.
Observing the aircraft’s groundspeed on a separate GPS unit, and uncertain if there was sufficient runway in wet weather to safely stop, the captain elected to continue the take-off.
During the climb, the flight crew became aware the pitot covers had been left installed on the pitot tubes. The crew was then able to return to Townsville for an uneventful landing.
“This occurrence highlights the importance of conducting an airspeed check early in the take-off run and recognising if something is not as expected, so the take-off can be safely rejected,” Mr Macleod said.
He said the occurrence also highlighted a discrepancy between the operator’s expectations and what was detailed in its procedures.
“When the flight crew began their evening shift shortly after 1800, the captain did not believe a daily inspection was required, as one had already been completed earlier that day,” Mr Macleod explained.
“They also believed a crew change inspection was not required, as the crew had not changed.”
The aircraft operator, Sharp Airlines, stated it expected a full daily inspection of the aircraft was required after termination checks had been completed, but this was not stated in its procedures.
Further, the final visual check conducted by the first officer prior to closing the doors, as stated in the procedures, did not include checking the pitot covers had been removed.
Sharp Airlines has advised it is reviewing the standard operating procedures to ensure clarity of process for pre-flight inspections.
“This scenario illustrates the importance of procedures clearly stating what inspections are required, and when,” Mr Macleod said.
“Flight crew pre-flight inspections are an important risk control, but if they are not done correctly, it increases the risk of defects not being identified, and/or the aircraft not being correctly configured for flight.”
Read the report: Unreliable airspeed indication on take-off involving Fairchild SA227, VH-UZN, Townsville Airport, Queensland, on 10 February 2025