
Final report
Report release date: 04/06/2026
Investigation summary
What happened
On the morning of 5 June 2025, the pilot of a Piper Chieftain PA-31, registered VH-PGO and operated by Shine Aviation, was conducting a multi-leg return passenger transport operation from Geraldton Airport via Carnarvon Airport and Meekatharra Airport, Western Australia. After refuelling in Carnarvon, VH-PGO departed for Meekatharra with the pilot and 2 passengers on board.
The flight was being conducted under instrument flight rules. During the instrument approach to Meekatharra, the right low fuel flow warning light illuminated. Shortly after, the right boost pump inoperative warning illuminated, and the right engine commenced surging with associated aircraft yaw. The pilot performed the engine failure checks, feathered the propeller, and continued the approach. The aircraft landed without further incident.
What the ATSB found
The ATSB found that the pilot did not check that the fuel caps were secured after refuelling, as required by the pilot’s operating handbook and company procedures. This resulted in the aircraft departing with the right inboard fuel cap incorrectly secured. The incorrectly secured fuel cap led to fuel siphoning overboard in flight. Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in the fuel tank quantity gauge overreading its contents.
The ATSB also found that the pilot was unaware of the actions to be taken on illumination of the right low fuel flow warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach.
Additionally, the ATSB found that Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light.
What has been done as a result
Following the occurrence, Shine Aviation reminded company pilots of the significance of the PA-31 low fuel flow warning and associated procedures. The operator also revised its training programs to strengthen coverage of abnormal and emergency scenarios, with particular emphasis on fuel system management. This included increasing the number of questions in the PA-31 theory examination. In addition, the general competency training syllabus was updated to expand instruction on fuel loading and verification processes, in‑flight fuel management practices, and aircraft type-specific emergency procedures, including detailed guidance on PA-31 annunciator panel warning lights and their operational significance.
Following a repeat incorrect cap fitment in October 2025, Shine Aviation elected to replace the fuel cap as a precaution, with no further incidents reported.
Safety message
An unsecured or incorrectly installed fuel cap can result in significant fuel loss in-flight, potentially leading to an abnormal or emergency situation. Checks of fuel system security including fuel caps should be conducted by the pilot during pre-flight, turnarounds and after refuelling to ensure correct fitment. Fuel cells will collapse if tanks are not sufficiently vented when in use; a collapsed fuel cell can result in a fuel quantity gauge overreading and providing a false indication to the pilot.
Civil Aviation Safety Regulations require pilots to be competent to the standards specified for the aircraft they are operating. This includes being able to conduct all normal, abnormal and emergency flight procedures. An awareness and understanding of cautions, warnings, and limitations contained in the pilot’s operating handbook enables pilots to identify and respond to any problems that may arise, prior to them escalating further. In this case, had the pilot taken the documented action in response to the warning, it would have prevented an emergency situation arising. However, when the engine stopped during approach while in cloud, the pilot took immediate action to feather the propeller and ensure a safe landing.
Operators also play an important role in pilots achieving the competency requirements. This includes ensuring pilots receive comprehensive training that develops and reinforces aircraft specific system knowledge, particularly regarding manufacturer warnings and cautions, and decision-making skills.
CASA Advisory Circular 91-25 Fuel and oil safety provides advice and guidance on procedures and practices to ensure the safety of fuelling operations. Included in this guidance are recommendations associated with fuel caps and vents to prevent in‑flight fuel loss and starvation.
Summary video
The occurrence
On 5 June 2025, the pilot of a Piper Chieftain PA-31-350, registered VH-PGO and operated by Shine Aviation, was conducting a multi-leg passenger transport operation under the instrument flight rules.1 At 0650 local time, the aircraft departed Geraldton Airport, Western Australia (WA), with the pilot and 3 passengers on board, and all 4 fuel tanks full – left and right, inboard and outboard. Stops were planned at Carnarvon and Meekatharra, WA, where the pilot planned to refuel, before a return flight to Geraldton (Figure 1).
Figure 1: Flight path of VH-PGO

Source: Google Earth, annotated by the ATSB
At 0817, the aircraft landed at Carnarvon Airport. The pilot then escorted the 3 passengers to the terminal building, where one passenger left the airport. The pilot returned to the aircraft to supervise refuelling and conduct a post-flight, external visual inspection of the aircraft. The local fuel supplier, on the pilot’s request, filled VH-PGO to full and then replaced the fuel caps on all 4 tanks. The refueller informed the pilot that a total of 240 L had been added to the aircraft. The pilot calculated, from the previous flight’s fuel usage, that the total fuel on board was now 688 L, which was consistent with full fuel tanks. The pilot recalled that they visually inspected but did not physically check the fuel caps for security after refuelling, and that all fuel cap latches appeared ‘down’ and in the ‘locked’ position.
The pilot assisted the 2 remaining passengers to board the aircraft, removed the chocks and then boarded the aircraft. As the pilot climbed onto the left wing to enter the aircraft, they reported giving the fuel caps ‘one last look’ and noted that they appeared correctly installed.
At 0851, VH-PGO departed Carnarvon Airport. The pilot selected the inboard fuel tanks for departure as per company and the pilot’s operating handbook (POH)2 procedures. The aircraft climbed to 9,000 ft above mean sea level (AMSL), where the pilot selected the outboard fuel tanks for the cruise to Meekatharra. At that time, the pilot calculated a fuel total of 636 L, using the onboard digital fuel flow indicator (see the section titled Fuel flow indicators). The fuel consisted of a combined 348 L in the inboard tanks and 288 L in the outboard fuel tanks. The pilot recalled that the fuel quantity gauges were indicating expected fuel quantities and fuel flow to both engines was stable throughout the take-off, climb, and into the cruise phase of flight.
During the cruise, the pilot obtained the weather at Meekatharra Airport via the aerodrome weather information service3 over VHF radio. The pilot noted that the wind was from 210° at 10 kt, cloud was overcast with a base of 800 ft above ground level (AGL), and visibility was 25 km, with no significant weather present. Based on this information, the pilot planned to conduct a landing on runway 27.4
The pilot selected the inboard tanks prior to the top of descent, in accordance with procedures. The pilot noted that the fuel quantity indication for the right inboard fuel tank was reading slightly lower than the left gauge but reported that they considered it ‘within an acceptable discrepancy for the PA-31’. The pilot calculated that 348 L remained in the inboard tanks and 118 L of fuel remained in the outboard tanks, totalling 466 L of fuel remaining on board.
The pilot descended the aircraft to 1,700 ft AGL and levelled off in accordance with the instrument approach procedure, before commencing the final approach to runway 09 with the intention of conducting a circling approach to runway 27. During this segment the R LOW FUEL FLOW warning light illuminated on the annunciator panel (see Figure 2 and the section titled Fuel system).
Figure 2: Right low fuel flow annunciator illumination during approach to Meekatharra

Source: Pilot, annotated by the ATSB
The pilot scanned the engine indications and noted they were normal, with no discrepancies between the engines. The pilot reported observing that the left and right fuel flow gauges were stable and indicating similar values, the fuel pumps were selected on, the engine mixtures were set to full rich, and the fuel boost pump circuit breakers were in and not tripped. The pilot also checked the fuel quantity gauges and stated that, while they did not recall the exact readings, nothing appeared abnormal or suggested that a tank was empty. The pilot continued the approach to Meekatharra. On the final approach segment, the aircraft entered instrument meteorological conditions (IMC).5 After entering IMC, the R FUEL BOOST INOP warning light (see the section titled Fuel system ) illuminated, followed by the right engine surging and associated aircraft yaw.
The pilot conducted their memory item initial engine failure checks and feathered the right propeller. At this time, the aircraft exited IMC and was about 800 ft AGL. The pilot elected to abandon the planned circling approach to land on runway 27 and instead accepted a 5 kt tail wind to conduct a straight-in approach to runway 09, landing without further incident.
Context
Pilot information
The pilot held a Commercial Pilot Licence (Aeroplane) and an instrument rating. The pilot also held a class 1 aviation medical certificate, valid until February 2026. At the time of the occurrence, the pilot had a total flying time of 1,381 hours, with 104 hours on the PA‑31 aircraft type. The pilot had flown 47.8 hours in the last 90 days which included 45.4 hours on PA‑31 aircraft.
The pilot commenced work with the operator in January 2025 and since then, had flown approximately 250 hours, including 220 hours in multi-engine aeroplanes, prior to the occurrence.
Aircraft information
General information
VH-PGO was a Piper Aircraft Corporation PA‑313‑50, twin‑engine, 10‑seat aircraft manufactured in the United States in 1978 and first registered in June 1979. The aircraft was powered by 2 Textron Lycoming engines: a TIO‑540‑J2BD on the left and an LTIO‑540‑J2BD on the right, each driving a Hartzell 3‑bladed constant speed propeller.
Fuel system
In PA-31 aircraft, fuel is stored in 4 flexible fuel cells, 2 in each wing. The fuel cell is attached to the upper inside of the wing by a cord running around the top section of the cell (Figure 3). The inboard cells hold 212 L each and the outboard cells hold 151 L each, totalling 726 L, of which 689 L are usable fuel.6
Figure 3: Right inboard fuel cell
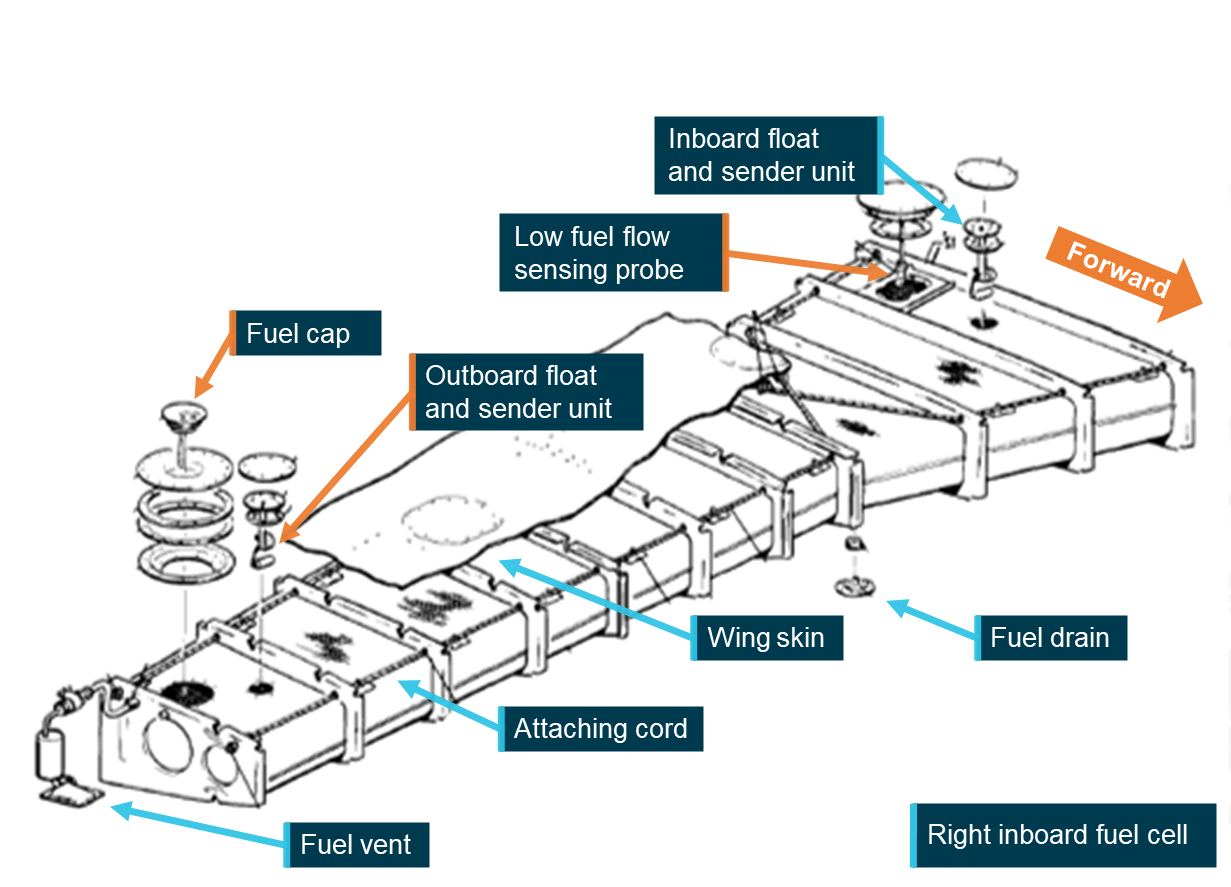
Source: Operator, annotated by the ATSB
A fuel vent is located on each cell and is designed to maintain each tank at atmospheric pressure by allowing air to enter the tanks as fuel is consumed and as fuel volume changes with temperature and altitude. This is designed to prevent the development of a vacuum in the tanks and ensures a continuous and reliable supply of fuel to the engines. The vent also provides for slight positive pressure in flight. A restriction or blockage of the vent system can result in reduced fuel flow and fuel starvation despite usable fuel remaining in the tanks.
The fuel control panel is located at the base of the central control pedestal and contains the fuel tank selectors, fuel shutoffs and crossfeed controls. During normal operation each engine is supplied with fuel from its own respective fuel system. The fuel controls on the right control the fuel from the right cells to the right engine and the controls on the left control the fuel from the left fuel cells to the left engine. In emergencies, fuel from one system can supply the opposite engine through a crossfeed system.
Fuel is routed from the fuel cells to the selector valves where, dependent on valve position, fuel from either the inboard or outboard tank is routed to the engine. Fuel leaving the selector travels through a fuel filter, a fuel boost pump, the emergency fuel pump, a firewall shutoff valve, and then to the engine-driven fuel pump and engine fuel system.
The emergency fuel pumps are installed for emergency use in case of an engine-driven fuel pump failure. They are also used for take-off and landing and, when necessary, to prime the engines. Control switches for the emergency fuel pumps are located on the overhead switch panel to the right of the fuel gauges.
Two electric fuel quantity gauges are also mounted on the overhead switch panel (Figure 5). These indicate the fuel tank level from float-style sender units in each tank. The gauges indicate left inboard or outboard tank, and right inboard or outboard fuel tank quantities dependent on selector valve position. The inboard tanks contain 2 sender units each, one near the wing root and one near the filler cap (Figure 3).
The fuel boost pumps are operated continuously and are provided to maintain fuel under pressure to the engine‑driven fuel pump. There are no fuel boost pump control switches or pressure gauges.
Each tank has a separate Shaw-style fuel cap for servicing (Figure 4). The inboard tank caps are located on the upper centre section of each wing and the outboard tank caps are on the upper outboard section of each wing. The right inboard fuel cap is not visible from the pilot’s seated position. The fuel caps are installed on the filler neck of each tank and utilise a twist‑to‑lock cam mechanism. As the latch is rotated, the upper and lower sections are drawn together, compressing the O‑ring seal against the filler neck to form a secure, fuel- and water-tight closure. The lower cap lugs engage under the filler neck flange to hold the cap in place against vibration, pressure changes, and airflow that is encountered in flight. The caps are also attached to the wing by a lanyard.
Figure 4: Shaw-style fuel cap
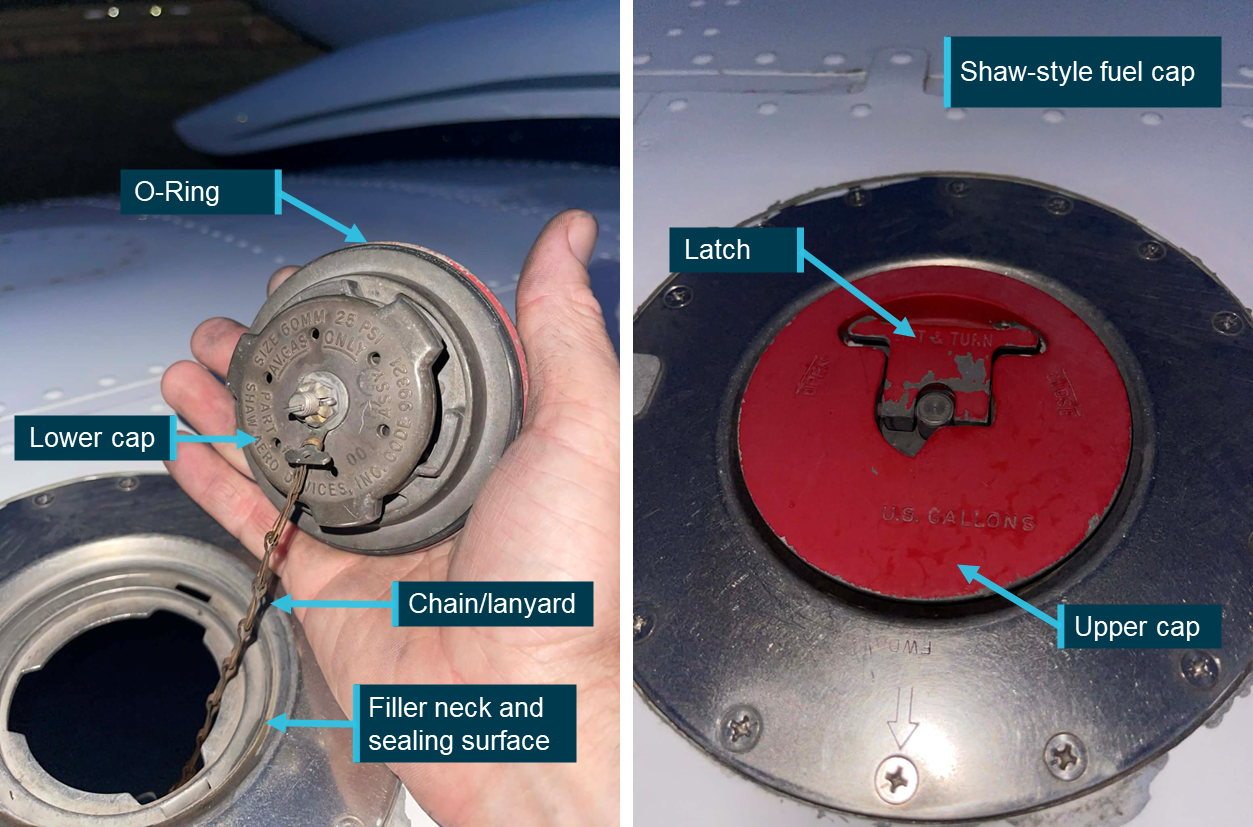
Source: Toby Dorn, annotated by the ATSB
Fuel flow indicators
Analogue fuel flow gauges located on the instrument panel indicate fuel flow to the engines in US gallons per hour. An FS-450 fuel flow indicator is also located on the instrument panel and digitally displays real-time fuel flow in litres per hour, fuel used, fuel remaining, and time-to empty. It is used to assist pilots in fuel management, however, it records fuel flowing through the fuel flow indicator transducer into the engine fuel system and would not detect a leak upstream such as a fuel tank leak.
Fuel system warning lights
Right and left fuel flow warning lights are mounted on the annunciator panel and illuminate to warn the pilot of an impending fuel flow interruption from the inboard tanks. The lights are activated by a probe that is mounted near each inboard fuel tank outlet (Figure 3). In the event of the fuel level near the tank outlet dropping to a point where a fuel flow interruption could occur, the LOW FUEL FLOW warning light will illuminate.
The pilot’s operating handbook contains the following warning:
WARNING
If either the right or left fuel flow warning light illuminates and the fuel gauge indicates fuel remaining in the corresponding inboard tank, this will indicate a malfunction of the flapper door in the inboard tank. Immediately select the outboard tank or select crossfeed to avoid fuel flow interruption.
This warning indicates a possible flapper door malfunction within the inboard fuel tank.7 In this condition, the fuel flow warning light may illuminate despite sufficient fuel remaining in the affected tank, as the malfunction may restrict fuel flow to the tank outlet. The procedure directs the pilot to immediately select the outboard tank or crossfeed to maintain fuel supply and prevent fuel flow interruption.
Left and right FUEL BOOST PUMP INOP warning lights are also mounted on the annunciator panel, and they illuminate when the fuel boost pressure to the associated engine fuel pump is less than 3 PSI. An illumination of a fuel boost pump inoperative warning light will occur immediately prior to that engine being starved of fuel.
Post‑occurrence
Pilot actions
After landing and shutting down the left engine, the pilot escorted the passengers to the terminal, reported the occurrence to Shine Aviation, and then returned to the aircraft. The pilot then applied battery power and noted that the right inboard tank fuel quantity gauge was indicating just above a quarter full, and the left inboard tank fuel quantity gauge was indicating half a tank (Figure 5). The pilot recalled that this was unusual and was more significant than the minor discrepancy observed at the top of descent.
Figure 5: Inboard tank quantity discrepancy after landing

Source: Pilot, annotated by the ATSB
The pilot then conducted a visual inspection of the right wing area and noted blue fuel streaks behind the right inboard fuel cap (Figure 6). After attempting to drain fuel out of the right inboard fuel tank without success, the pilot then removed the right fuel cap to see if any fuel was present. The pilot noted that the fuel cap latch was ‘extremely’ difficult to unlatch and required the use of both hands. Upon looking in the tank, the pilot observed that it was empty, and the bottom of the fuel cell had been sucked up towards the fuel filler area. The pilot then reinstalled the cap, commenting that the cap latched normally and without difficulty.
Figure 6: Fuel staining aft of right inboard fuel cap
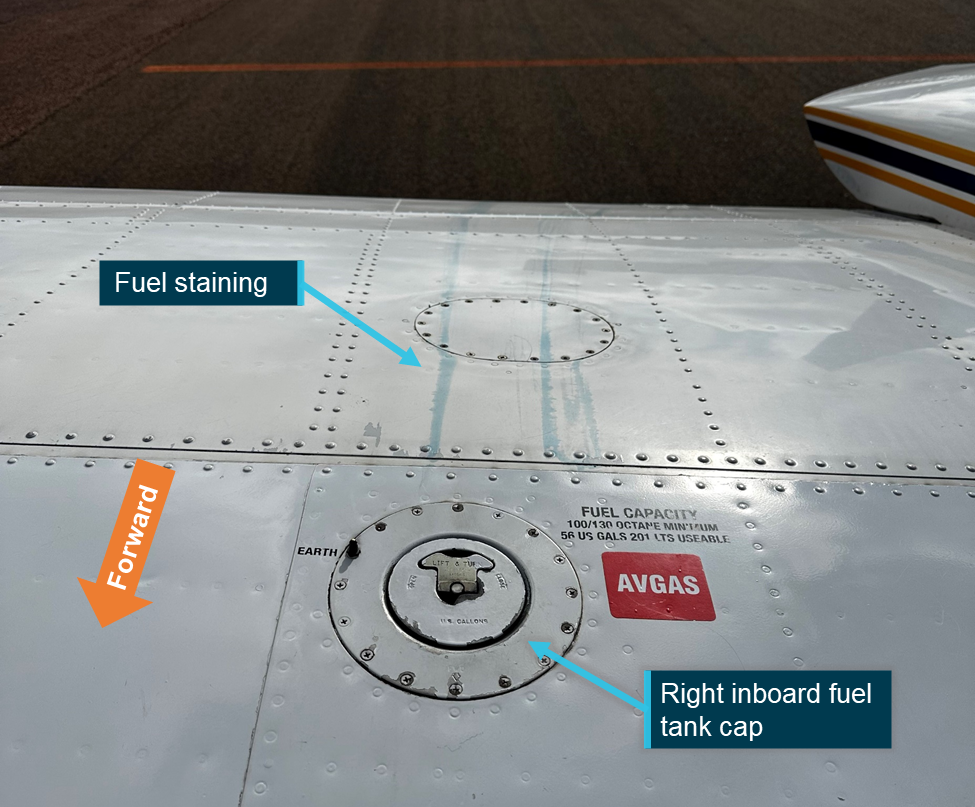
Source: Pilot, annotated by the ATSB
At hourly intervals, the pilot reapplied battery power noting that it took 2.5 hours after landing for the right inboard tank fuel gauge to read zero.
Engineering inspection
The company’s chief engineer arrived about 3.5 hours after the occurrence to commence troubleshooting. They reported that there was no evidence of a leak source around the right inboard fuel tank aside from the fuel staining aft of the fuel cap. Although the pilot had already removed and refitted the fuel cap, an inspection of the fuel cap was conducted with no defects noted including the O‑ring being found serviceable. The chief engineer replaced the cap O‑ring seal and re-tensioned the cap’s latch mechanism as a precaution. They also commented that there was a possibility of the fuel cap lanyard interfering with the cap’s fitment however no damage to the cap or the lanyard was identified.
The chief engineer observed that the bottom of the fuel cell had been drawn up towards the fuel cap and required manual reseating. They filled the inboard tanks to maximum capacity; 67 L was required to fill the left inboard tank, and 204 L was required to fill the right inboard tank. The chief engineer stated that they were satisfied that the fuel cell had reseated correctly within the fuel tank cavity.
The engines had been operated alike up to the right engine starvation. The ATSB estimated that the left engine consumed 6 L of fuel after the right engine stopped. Therefore, about 131 L had been siphoned and lost overboard from the right tank through the fuel cap during flight.
During the draft report review process, the ATSB was informed of a repeat incorrect fitment of VH-PGO’s right inboard fuel cap that resulted in fuel leaking during flight. The operator advised that this occurred on 6 October 2025, 4 months and an estimated 60–70 refuels after the initial occurrence. However, the chief engineer was able to observe the cap in its incorrectly fitted state where they determined that the cap had not been seated correctly prior to being latched. This resulted in the upper and lower portions of the cap clamping on the filler neck of the wing (Figure 7). Following the second occurrence, the chief engineer elected to replace the fuel cap as a precaution.
Upon receipt of the new fuel cap the chief engineer noted that a skirt had been incorporated into the design of the replacement cap therefore limiting the ability of the upper and lower portions of the cap to clamp on the filler neck of the wing (Figure 7). The ATSB contacted the manufacturer for further information on the apparent design change. However, at the time of publication no response had been received.
Figure 7: Incorrect fitment on 6 October 2025
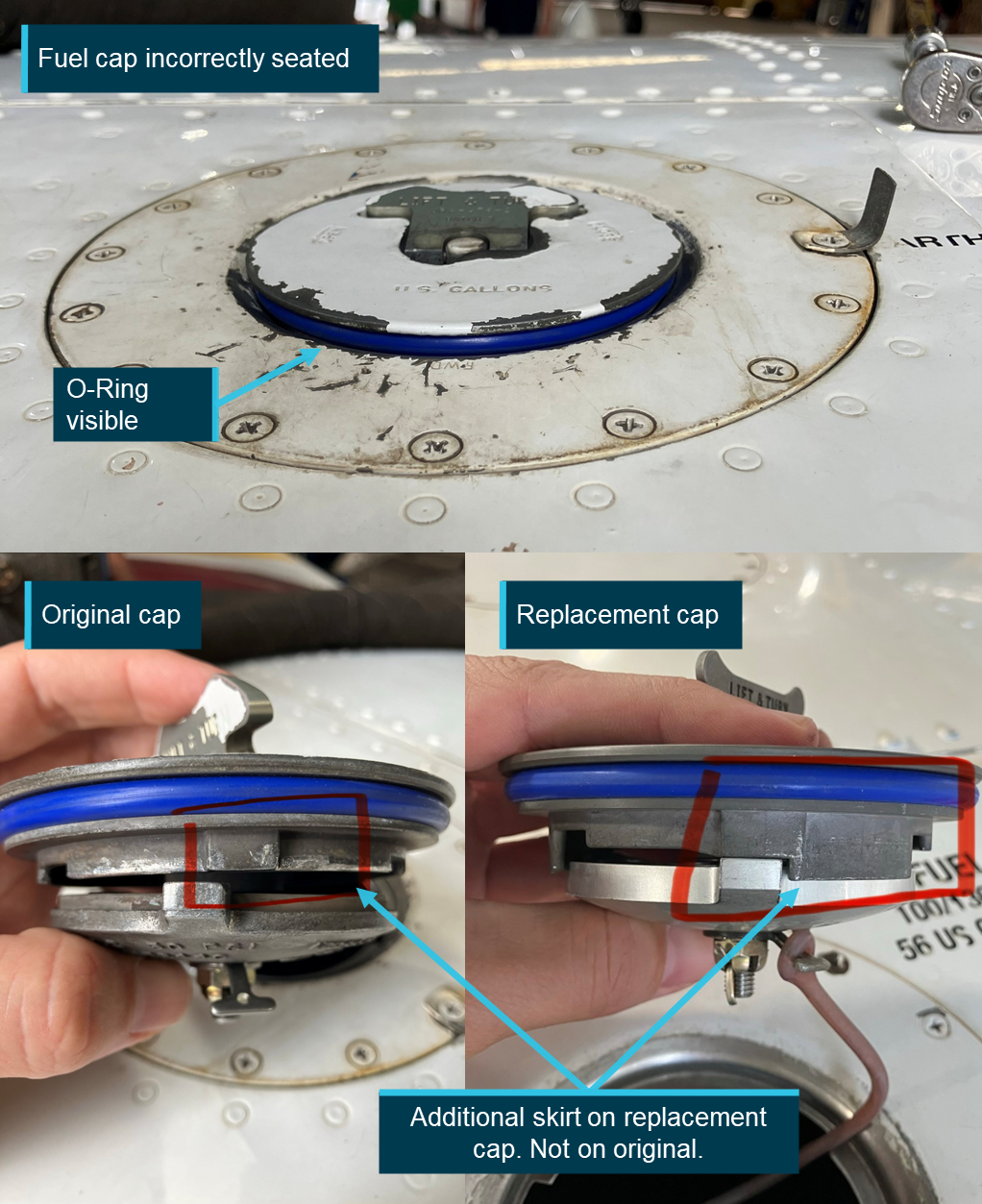
Source: Operator, annotated by the operator and the ATSB
Flight testing
Following the inspection, the aircraft was ferried back to Geraldton (without passengers) by the head of flying operations, with the chief engineer seated in a position that allowed full view of the right inboard fuel tank cap.
During climb out of Meekatharra Airport, they observed that the FS-450 fuel flow indicator for the right engine was displaying a significantly lower fuel flow than expected for the selected power and mixture setting, and it was lower than the corresponding analogue fuel flow gauge. The FS-450 indicated approximately 70 L/h, compared to the expected value of about 120‑L/h. However, the right engine exhaust gas temperatures, oil temperature, manifold pressure and cylinder head temperature were within normal limits for that power setting and comparable to the left engine. On that basis, they assessed that the FS‑450 indication was erroneous and not representative of the actual fuel flow to the engine, with the chief engineer stating that the engine would not be able to run with that fuel flow for that power setting. The engineer advised the head of flying operations to use the analogue fuel flow gauges for engine management for the remainder of the flight.
The occurrence pilot reported that they had not observed any irregularities with any of the engine indications prior to the occurrence. This was supported by a review, conducted by the operator’s head of safety and quality assurance, of VH‑PGO’s previous 8 flight logs, which found that fuel usage data was normal and within acceptable parameters for the PA‑31‑350.8 In addition, a review of the flight logs for flights conducted after the occurrence identified no abnormalities.
The chief engineer later commented that the FS‑450 unit’s calibration may have been inadvertently altered by the occurrence pilot after the event during their initial troubleshooting.
During the return flight to Geraldton, the chief engineer did not observe any fuel leaking from the right inboard fuel tank cap, and a post‑flight inspection confirmed that no fuel leakage was present. The aircraft was subsequently flown that evening and the following morning, with no further leaks or related issues identified.
Refueller
The refueller who uplifted fuel to the aircraft at Carnarvon and secured the fuel caps before the occurrence flight later recalled that the right inboard fuel cap was slightly difficult to close. However, based on their familiarity with the aircraft, they believed the cap was properly secured. They also stated that if they had any concerns about the aircraft, they would have informed the pilot.
Pre-flight and refuelling
The pre-flight inspection detailed in the POH stated that the fuel supply should be checked visually, and a check was required to ensure the fuel caps are securely in place. To visually check the fuel supply, the cap would have to be removed and therefore a physical check of security is performed when the caps are installed.
Shine Aviation’s Policy and Procedures manual provided instructions regarding refuelling and fuel caps, additional to the POH procedures. The instructions included:
When fuelling is complete, sufficient airspace must remain in each fuel tank to allow for anticipated fuel expansion, and the PIC must ensure that all fuel and oil tank caps have been securely refitted.
PA-31 training
Regulatory requirements
Shine Aviation operated as a Civil Aviation Safety Regulation (CASR) Part 135 operation (Australian Air Transport Operations - Smaller Aeroplanes) and held a Part 135 Air Operator’s Certificate (AOC). Section 12.05 of the Part 135 Manual of Standards stated the following:
• The flight crew member must have successfully completed the operator’s conversion training, and flight crew member proficiency check, for the aeroplane.
• The training must deal with the following:
- training in the duties and responsibilities for the flight crew member’s position;
- training in the standard operating procedures for the type or class of aeroplane used for the flight;
- training in the normal, non-normal and emergency procedures for an aeroplane of that type or class;
- training in any flight procedures or manoeuvres, conducted in an aeroplane of that type or class, for which the operator holds an approval under regulation 91.045, or 135.020, of CASR;
Note: Examples of approvals issued under regulation 91.045, or 135.020, of CASR include approvals to conduct low visibility operations and flights using certain PBN navigation specifications.
- training in the procedures for any other operations conducted by the operator in an aeroplane of that type or class that the flight crew member has not previously experienced, for example, precision runway monitor operations or land and hold short operations.
Under CASR Part 61.385 Limitations on exercise of privileges of pilot licences – general competency requirement, a pilot may only exercise the privileges of their licence if they are competent to the standards specified for the relevant aircraft they are operating. This includes being able to conduct all normal, abnormal and emergency flight procedures for that aircraft.
Company flight training
Shine Aviation was approved by CASA as a CASR Part 141 training organisation, enabling it to conduct in-house pilot training and competency assessments in support of pilot qualification for operations under the organisation’s Part 135 Air Operator’s Certificate.
Pilots underwent conversion training onto company aircraft in 2 parts: a ground-based theory component, followed by a flying component. The ground-based theory component consisted of self-paced study of the POH prior to undergoing a multiple-choice theory exam. The theory examination consisted of 25 PA-31 specific questions, automatically generated from a question bank of 82, including topics relating to weight and balance, aircraft performance, and systems knowledge.9
The flying component involved the pilot conducting 2 non-revenue (no passengers) training flights with a company flight instructor. Shine Aviation’s General Competency Training syllabus included the following competencies for the pilots to demonstrate:
- departure and arrival (including appropriate engine management for turbocharged aircraft)
- stalling
- steep turning
- different cruise configurations
- upper air asymmetric where applicable
- normal circuit
- flapless circuit
- crosswind circuit
- engine failure on take-off
- engine failure elsewhere in circuit
- single engine go‑around
- discussion on differences in standard practice between engine models (oil uplift, engine monitoring etc)
- any other multi engine or single engine class rating competencies as deemed necessary by instructor.
Although this syllabus contained specific competencies for other types of aircraft Shine Aviation operated, it did not contain any specific PA-31 competencies. However, it did contain an ‘underpinning knowledge’ section in which ‘Instrument failure and warning systems fitted to the aeroplane’ was listed.
Following satisfactory demonstration of the required flying competencies, the pilot was required to act as a copilot for approximately 30 hours of normal company operations prior to conducting single pilot operations.
The pilot in this occurrence completed their ground component and 2 non-revenue training flights, involving 3 hours of flight and 4 hours of briefing time, in January 2025. The pilot then conducted approximately 30 hours of flying as a copilot in the PA-31, including 13.5 hours in VH-PGO, prior to being assessed and approved for single pilot operations. The pilot completed an instrument proficiency check in January 2025 in the PA-31 with a company examiner.10
In May 2025, the pilot successfully completed 2 recurrent flight training exercises in the company’s approved synthetic training device.11 These exercises involved various emergency and abnormal scenarios consisting of adverse weather, engine failures, single engine approaches, instrument failures and flight planning exercises.
Training regarding low fuel flow warning light
The theory examination contained the following question related to the LOW FUEL FLOW warning light:
Illumination of a LOW FUEL FLOW annunciator:
a) Indicates that outboard fuel quantity has decreased to a point where engine power loss could occur
b) Indicates low fuel quantity in the inboard tanks
c) Indicates that a fuel boost pump has failed
d) a and c
The correct answer is (b), however this question pertains to the function of the warning light but does not cover the published warning or the actions to be taken by the pilot upon its illumination (see the section titled Fuel system warning lights). Regardless, the theory examination that was generated for the occurrence pilot did not include this question.
Shine Aviation’s head of training for the PA-31 stated that the LOW FUEL FLOW warning light was likely discussed during the flight training component when the annunciator panel was covered. However, they also stated that not every annunciator panel indication was examined in detail.
The incident pilot advised that the LOW FUEL FLOW warning light was not specifically addressed during initial or copilot training and that, although they understood that it related to a fuel flow issue to the affected engine, they were not aware of, or could not recall, the required immediate actions that are directed by the warning in the POH.
Related occurrences
Excluding the incident flight, the ATSB occurrence database contained 49 reported occurrences of fuel leaking or venting from a fuel cap on non-jet aircraft between 2014 and 2025. Of those occurrences, 8 resulted in fuel starvation or fuel exhaustion. Those numbers likely under‑represent the total number of incidents of this type, as the ATSB only required instances of fuel leaking/venting or missing/insecure fuel caps to be reported for commercial passenger transport operations.
ATSB occurrence brief AB-2021-009 was published following a fuel starvation event involving a PA-31-350 in 2021:
On 21 March 2021 a Piper PA-31-350 aircraft was operating a scheduled freight flight from Moorabbin, Victoria to Devonport, Tasmania. During approach, the low fuel flow and low boost pump warning lights illuminated. The right engine stopped shortly after. The pilot in command confirmed the fuel selector was in the correct position and observed that the fuel gauges indicated three-quarters full, which was as expected. The pilot then attempted to cross-feed fuel from the left engine, which was unsuccessful. By this time, the aircraft was on mid-final and, once assured of making the runway, the pilot stopped troubleshooting and concentrated on landing the aircraft.
After landing, the pilot inspected the fuel cap, which appeared to be secured correctly. However, blue stains were evident on top of the wing consistent with fuel venting out of the fuel cap. The fuel system was subsequently inspected by maintenance personnel with nil defects found with the fuel cap and no blockages in the fuel tank vents.
The pilot later advised that the rubber bladder containing the fuel within the tank was sucked up against the top of the wing as the tank emptied, providing a false indication of the fuel remaining in the tank.
ATSB occurrence investigation AO-2024-008 was published following a fuel exhaustion event in 2024:
On 8 March 2024, the pilot of an Aero Commander 500-S, registered VH-MEH and operated by GAM Air, was conducting a return cargo transport operation from Bankstown Airport to Parkes Regional Airport, New South Wales with one intermediate stop outbound, and 2 intermediate stops on return.
After landing on the first sector, the pilot found the fuel cap was off and secured only by a retention chain. The pilot re-secured the cap but after landing at Parkes on the second sector, they again found the fuel cap off. They arranged an inspection by a maintenance engineer, where a fault was found that prevented the fuel cap from locking and rectified it.
Later that day, the pilot commenced the return sectors to Bankstown. Shortly after departing Bathurst for the final sector, both engines lost power, and the pilot conducted a forced landing in a field. The aircraft was undamaged and the pilot was uninjured.
The ATSB found that the fuel cap retention chain had lodged within the fuel tanks anti siphon valve. This allowed fuel to be siphoned overboard during flight.
CASA Advisory Circular 91-25 Fuel and oil safety, section 6, highlighted recommendations associated with fuel caps and vents. In particular, the circular advised of the possibility of fuel siphoning overboard due to a cap attachment chain or lanyard becoming trapped across a fuel cap seal. The advisory circular also identified that an insufficiently vented tank may collapse the fuel bladder and exaggerate indications of fuel within the tank.
Safety analysis
Introduction
On 5 June 2025, the pilot of a Piper Chieftain PA-31, registered VH-PGO, and operated by Shine Aviation, was conducting a passenger transport operation from Carnarvon to Meekatharra, Western Australia. During the approach to Meekatharra Airport, the R LOW FUEL FLOW warning light illuminated, followed shortly by the R FUEL BOOST INOP warning light and surging of the right engine. The pilot conducted their memory item initial engine failure checks and feathered the right propeller. The pilot continued the approach and landed without further incident.
Fuel siphoned overboard
Photographs taken by the pilot after landing at Meekatharra Airport show fuel staining immediately aft of the right inboard fuel cap, consistent with fuel leaking from the cap in flight. This staining, in conjunction with the pilot’s observation that the right inboard tank was emptied earlier than expected based on calculated consumption, and that the tank cell collapsed upwards towards the cap, all indicate that fuel had likely been siphoned through the cap in flight. The pilot also reported that the fuel cap latch was difficult to lift, suggesting the cap may not have been correctly seated.
During the post-occurrence inspection, the chief engineer found no evidence of any other fuel leaks around the right inboard tank. The pilot had removed and reinstalled the cap prior to this inspection, therefore the chief engineer could not determine exactly how the cap was incorrectly fitted. The chief engineer was also unable to reproduce an incorrect installation. However, the chief engineer considered it likely that the fuel cap had been incorrectly secured, including the possibility of the attaching lanyard interfering with the cap and seal. No damage was observed to the cap, seal, or lanyard and the chief engineer replaced the O-ring on the cap as a precaution, although they considered the removed O‑ring serviceable. Subsequent flights, including the immediate post‑occurrence flight with the chief engineer observing the cap, did not reproduce the leak. As the leak did not recur, it was almost certain the fuel cap was incorrectly secured in Carnarvon.
As part of the troubleshooting, the chief engineer refuelled the right inboard tank with 204 L, while the left tank required only 67 L to fill. Given that both tanks had been selected for use at similar times during the flight, and accounting for fuel used by the left engine after the right had stopped, the discrepancy indicated that approximately 131 L of fuel had been lost through the fuel cap from the right inboard tank.
Contributing factor The fuel cap on the right inboard fuel tank was almost certainly incorrectly secured which led to fuel being siphoned overboard in flight. |
Fuel cap installation
Shine Aviation’s Policy and Procedures manual required the pilot in command to ensure that fuel caps were securely fitted. While this did not explicitly require the pilot to remove and reinstall the caps, the pilot’s operating handbook specified that the pilot in command must visually check the fuel supply and confirm that the fuel caps are secure. Checking the fuel quantity required the pilot removing the caps and physically handling the fuel caps to verify correct fitment.
Although the pilot stated that they visually inspected the fuel cap, a closer inspection or physical check of the cap would likely have aided the pilot in identifying the incorrect installation. Consequently, the pilot did not detect that the right inboard fuel tank cap was incorrectly secured.
Contributing factor The pilot did not check that the fuel caps were secured as required by the pilot’s operating handbook and company procedures, resulting in the aircraft departing with the right inboard fuel cap almost certainly incorrectly secured. |
False gauge reading
During flight, the rate of fuel being siphoned through the fuel cap was likely sufficient to overcome the vent’s ability to equalise pressure in the fuel tank. This resulted in negative pressure collapsing the fuel cell as observed by both the pilot and the chief engineer during their post-occurrence inspections. As the fuel cell was secured by a single cord around the upper perimeter, the collapse of the fuel cell resulted in the base of the cell lifting towards the filler port.
As one of the right inboard fuel tank float-style sender units was located near the fuel filler port, it is likely that the upwards lifting of the fuel cell floor toward the filler port, raised the outboard sender unit’s float. This resulted in an overreading of the cockpit fuel quantity gauge. ATSB occurrence brief AB-2021-009 identified a similar failure mechanism where the fuel cell collapsed resulting in the fuel gauge overreading its contents. The Civil Aviation Safety Authority’s advisory circular (AC) 91-25 Fuel and oil safety, section 6, also contained information about collapsing fuel cells interfering with the accuracy of fuel gauge readings.
During the subsequent flight, the onboard fuel flow indicator was incorrectly and significantly underreading the right engine fuel flow. However, the pilot reported it was functioning normally during the flight to Meekatharra. Engineers assessed the instrument had probably been inadvertently recalibrated during post-incident fault finding.
When the pilot changed from the outboard tanks to the inboard tanks at the top of descent, they noticed that the right inboard tank quantity gauge was reading a slightly lower quantity than the left inboard, however they assessed that this was an acceptable discrepancy related to VH-PGO. It is likely that the right inboard tank was almost empty at that stage of flight as the R LOW FUEL FLOW warning light illuminated shortly after.
Contributing factor Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in that fuel tank quantity gauge overreading its contents. |
Response to warning
The warning in the pilot’s operating handbook (POH) stated that if the right or left LOW FUEL FLOW warning light illuminated, and the fuel gauge indicated fuel remaining in the corresponding inboard tank, this indicated a malfunction of the flapper door in the inboard tank. The prescribed action was to immediately select the outboard tank or select crossfeed to avoid fuel flow interruption. While a flapper door malfunction did not occur in this instance, compliance with the warning actions would likely have restored fuel supply.
The pilot was unaware of the required immediate actions and therefore did not respond to the R LOW FUEL FLOW warning light as directed by the POH. The pilot was also unaware that a fuel starvation event was developing, until the subsequent illumination of the right FUEL BOOST INOP warning light and associated engine surging.
The sequential activation of the R LOW FUEL FLOW warning followed by the right FUEL BOOST INOP warning was a progressive indication that fuel flow to the right engine would be interrupted. As the pilot did not restore fuel flow following either warning, the right engine became starved of fuel, resulting in the engine surging and a corresponding yaw of the aircraft.
Contributing factor The pilot was unaware of the actions to be taken on illumination of the LOW FUEL FLOW warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach. |
Training regarding low fuel flow warning light
As part of the Civil Aviation Safety Regulations (CASR) limitations on the privileges of a pilot licence, pilots were required to be competent in conducting all normal, abnormal and emergency flight procedures for the aircraft. This required the pilot to be aware of the POH warnings and associated instructions included in emergency procedures. Additionally, under CASR Part 135, operators were also required to ensure that flight crew were trained in the normal, non-normal and emergency procedures for the aircraft they were operating.
Shine Aviation PA-31 pilots independently studied the POH and subsequently undertook a theory examination. This examination consisted of 25 PA-31 specific questions that were automatically generated from a question bank of 82. Although there was one question regarding the illumination of the LOW FUEL FLOW warning light, this question did not evaluate the immediate response required. Furthermore, this question was not included in the occurrence pilot’s automatically generated examination.
Shine Aviation’s head of PA-31 training advised that the LOW FUEL FLOW annunciator and associated warning were likely addressed to some extent during practical line training. However, the occurrence pilot did not recall this topic being covered. Shine Aviation’s General Competency syllabus required a general knowledge of the warning systems, however, it did not specifically require demonstration of the appropriate response to a LOW FUEL FLOW warning. In this case, the training was ineffective at ensuring the incident pilot was competent in responding to the warning.
Contributing factor Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light. (Safety issue) |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the fuel starvation involving Piper PA-31, VH-PGO, 28 km west of Meekatharra Airport, Western Australia, on 5 June 2025.
Contributing factors
- The fuel cap on the right inboard fuel tank was almost certainly incorrectly secured which led to fuel being siphoned overboard in flight.
- The pilot did not check that the fuel caps were secured as required by the pilot’s operating handbook and the company procedures, resulting in the aircraft departing with the right inboard fuel cap almost certainly incorrectly secured.
- Fuel siphoning overboard by airflow caused the fuel cell to collapse, resulting in that fuel tank quantity gauge overreading its contents.
- The pilot was unaware of the actions to be taken on illumination of the LOW FUEL FLOW warning light and therefore did not switch tanks or crossfeed as required by the pilot’s operating handbook. This resulted in the right engine being starved of fuel during approach.
- Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow warning light. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Low fuel flow warning light and subsequent actions not highlighted in training
Safety issue number: AO-2025-026-SI-01
Safety issue description: Shine Aviation's training for the PA-31 did not specifically highlight the warning in the pilot’s operating handbook or address the actions required by the pilot on the illumination of the low fuel flow annunciator light.
Glossary
| AMSL | Above mean sea level |
| AGL | Above ground level |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| IFR | Instrument flight rules |
| IMC | Instrument meteorological conditions |
| POH | Pilot’s Operating Handbook |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot
- the operator of VH-PGO
- Civil Aviation Safety Authority
- Airservices Australia.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the pilot
- the operator of VH-PGO
- Civil Aviation Safety Authority.
Submissions were received from:
- the pilot
- the operator of VH-PGO.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
- ^ Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
- ^ Pilot’s operating handbook: a manufacturer-produced manual that provides pilots with all the essential information needed to safely operate the aircraft.
- ^ Aerodrome weather information service (AWIS): actual weather conditions, provided via telephone or radio broadcast, from Bureau of Meteorology (BoM) automatic weather stations, or weather stations approved for that purpose by the BoM. Winds are in degrees magnetic.
- ^ Runway number: the number represents the magnetic heading of the runway to the nearest 10 degrees.
- ^ Instrument meteorological conditions (IMC): weather conditions that require pilots to fly primarily by reference to instruments, and therefore under instrument flight rules (IFR), rather than by outside visual reference. Typically, this means flying in cloud or limited visibility.
- ^ Usable fuel: the amount of fuel in a fuel tank that can reliably be supplied to the engine in all operating conditions. This excludes fuel that cannot be used due to aspects such as tank geometry and fuel pickup locations.
- ^ A flapper door is installed in each inboard tank to keep fuel around the tank outlet by preventing it from flowing away during manoeuvring, climb, descent, turbulence, or uncoordinated flight.
- ^ The pilot records fuel quantity prior to start, fuel quantity used via the FS-450, and fuel quantity after shutdown for each sector in a flight log. This allows the operator to monitor fuel usage for individual aircraft.
- ^ Following the occurrence, Shine Aviation increased the number of questions in the PA-31 theory examination to 30.
- ^ Instrument proficiency check (IPC): A required annual flight test to ensure that a pilot maintains the necessary skills and knowledge to safely operate an aircraft under instrument flight rules (IFR). It involves demonstrating competency in tasks such as navigation, communication, and handling the aircraft in various conditions, all while relying on instruments rather than visual references.
- ^ Recurrent training: Shine Aviation conducts recurrent training for all its instrument rated pilots every 6 months. Training is delivered in a synthetic flight training device and consists of simulated IFR flights that include operational and decision-making scenarios tailored to the individual pilot. This recurrent training is in addition to regular instrument proficiency checks as required every 12 months under CASR Part 61.
Occurrence summary
| Investigation number | AO-2025-026 |
|---|---|
| Occurrence date | 05/06/2025 |
| Occurrence time and timezone | 1031 Australian Western Standard Time |
| Location | 28 km west of Meekatharra Airport |
| State | Western Australia |
| Report release date | 04/06/2026 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Fuel starvation |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Piper Aircraft Corp |
|---|---|
| Model | PA-31-350 |
| Registration | VH-PGO |
| Serial number | 31-7852109 |
| Aircraft operator | Shine Aviation |
| Sector | Piston |
| Operation type | Part 135 Air transport operations - smaller aeroplanes |
| Activity | Commercial air transport-Non-scheduled-Passenger transport charters |
| Departure point | Carnarvon Airport, Western Australia |
| Destination | Meekatharra Airport, Western Australia |
| Injuries | None |
| Damage | Nil |