The ATSB has released a preliminary report detailing an engine malfunction incident during a Qantas A330 passenger flight between Los Angeles and Brisbane on 4 December 2024.
The preliminary report summarises evidence gathered so far in the ATSB’s ongoing investigation. It does not contain analysis or findings, which will be published at the conclusion of the investigation.
The preliminary report notes that, while the Airbus A330‑200 was cruising at about 34,000 ft after departing Los Angeles, the flight crew received a passenger report of sparks emanating from the right engine observed during the climb.
After conducting a number of checks and considering alternate airports, the flight crew opted for a return to Los Angeles, and descended the aircraft to 31,000 ft to reduce load on the engine.
By the time the aircraft reached this altitude, the intermittent sparks were observed to have stopped.
“Later, as the aircraft was descending to land in Los Angeles, three loud bangs were heard, and there was a right engine compressor stall indication,” ATSB Chief Commissioner Angus Mitchell said.
“In response, the flight crew operated the engine at idle for the rest of the descent and landing.”
A post-flight inspection of the right engine identified a missing high-pressure compressor blade that had separated at its root, another high-pressure compressor blade fractured about half-way up, and damage to the tips of several other blades.
A variable stator vane was also found to be out of alignment, and there was metal debris in the engine’s exhaust.
The aircraft was subsequently grounded, and the right engine replaced.
The preliminary report details that, on the aircraft’s previous flight into Los Angeles, the flight crew had observed a high N2* vibration advisory.
During the turnaround in Los Angeles, two maintenance engineers troubleshooted the N2 vibration issue, during which they observed particles in the right engine exhaust.
“The ATSB’s ongoing investigation is considering the communications between involved personnel during this troubleshooting, including communications between staff in Los Angeles and at the Qantas maintenance operation centre in Sydney,” Mr Mitchell said.
The troubleshooting culminated in the aircraft being released to service with its N2 vibration sensor inoperative in line with minimum equipment list (MEL) requirements, meaning N2 vibration readings were not available to the flight crew on the incident flight.
“Flight crew for the incident flight told the ATSB they were not aware that particles had been observed during the examination prior to their flight,” Mr Mitchell noted.
As well as the communications and maintenance during the turnaround in Los Angeles, the ATSB’s ongoing investigation will examine the recorded data, maintenance procedures and records, and the outcomes of the material failure analysis being conducted by GE Aerospace on relevant components of the engine.
A final report will be released at the conclusion of the investigation, including findings, and any identified safety issues.
“Should a critical safety issue be identified during the course of the investigation, the ATSB will notify relevant parties immediately so appropriate and timely safety action can be taken,” Mr Mitchell concluded.
* N2 refers to the rotational speed of a jet engine’s high-speed spool, which consists of the high-pressure compressor and the high‑pressure turbine connected by a concentric shaft.
At about 1620 local time on 6 February 2025, a bulk carrier vessel arrived at Newcastle pilot boarding ground Bravo, New South Wales (Figure 1) from Rayong, Thailand to board a harbour pilot for the inbound transit to M4 berth. In accordance with the pilot’s requirement, the ship’s crew prepared the pilot ladder on the port side, positioned 2 m above the water line, with 2 manropes[1] also rigged.
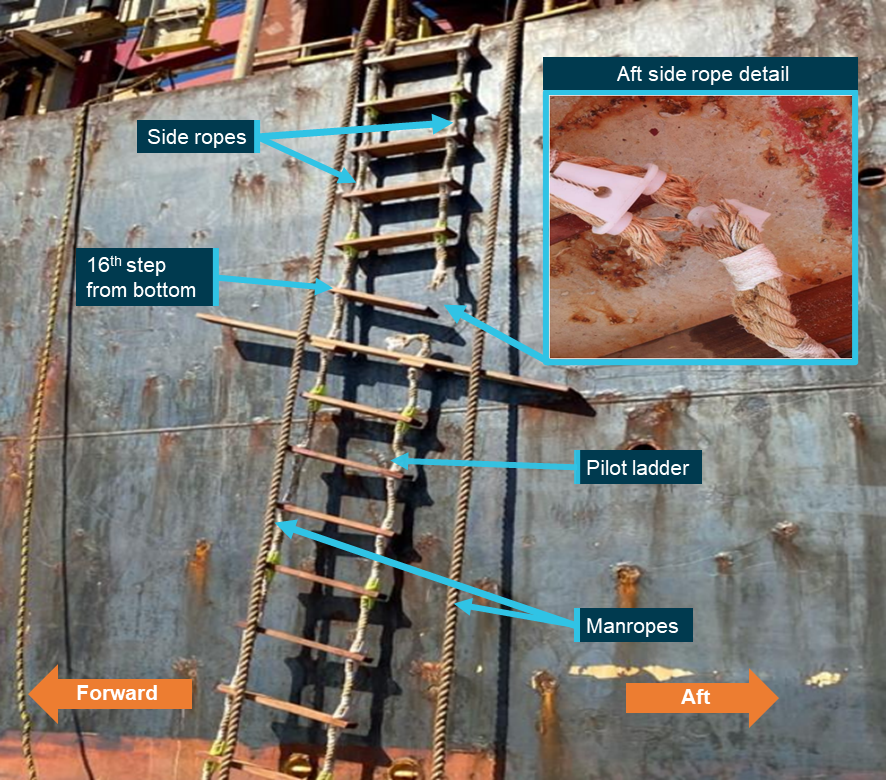
A few minutes later, the pilot vessel arrived at the pilot boarding ground. It was an approximately 8 m climb[2] from the pilot vessel to the ship’s main deck. As the pilot started ascending the pilot ladder, the aft side rope of the pilot ladder parted at the sixteenth step (Figure 2).
Figure 2: Failed pilot ladder with close-up detail
Source: Vessel operator, annotated by the ATSB
The pilot managed to support their weight with their arms and quickly moved to the step above and then onto the main deck of the vessel without injury. The pilot reported the matter to the ship’s master, who was conning[3] the vessel from the wheelhouse. On completion of the primary task of the inbound pilotage, and once the ship had been safely made fast alongside its berth, the master and pilot inspected the pilot ladder. The matter was also reported to the Australian Maritime Safety Authority (AMSA).
Pilot ladder particulars
The pilot ladder was 9 m in length and comprised 27 steps. It was supplied to the vessel on 1 February 2024 and accompanied by a certificate indicating a manufacture date of 15 January 2024. The certificate also stated that the pilot ladder complied with the following standards:
EU Regulation 2023/1667, item no. MED/4.49
SOLAS 74 as amended, regulation V/23 and X/3
IMO Resolution A.1045(27)
IMO MSC.1/Circ.1428
ISO 799-1.
On board storage
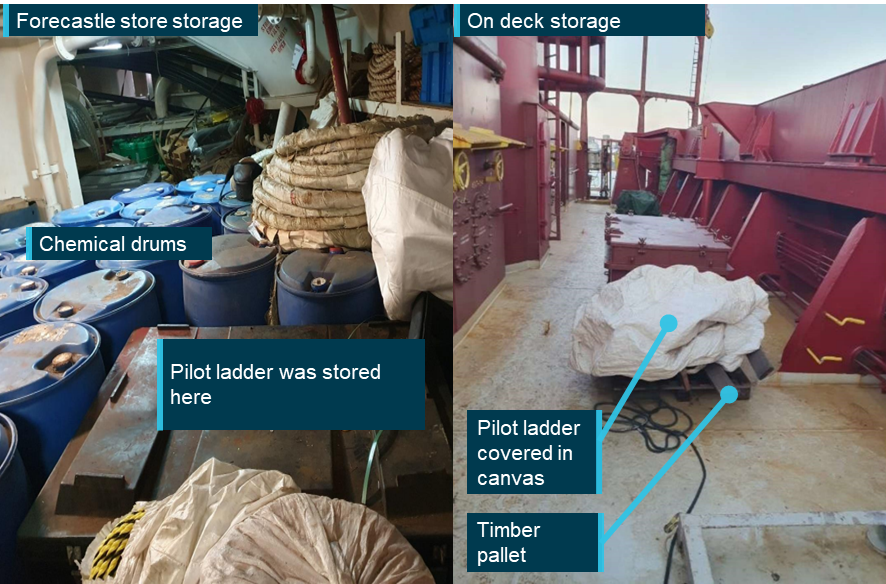
At the time of receipt, the pilot ladder was maintained in the ship’s spare inventory and was stored in the forecastle store, in the immediate vicinity of several sealed drums containing corrosive chemicals intended for cargo hold cleaning operations.
In order to be put into service, the ladder was removed from storage on 14 January 2025, covered with canvas and placed on top of a timber pallet on the ship’s main deck, pending its use during pilot boarding operations (Figure 3).
Figure 3: Pilot ladder onboard storage arrangements
Source: Vessel’s operator, annotated by the ATSB
Prior to the ladder’s first use at the port of Newcastle on 6 February 2025, the ship’s crew reported they undertook a visual and limited physical examination of the ladder.
Operator’s investigation
Following the incident, the damaged pilot ladder was sent to an independent testing facility in Brisbane, Queensland for failure analysis. The investigation identified the following:
the manila side rope had degraded due to several factors, including pre-existing damage, poor quality rope, chlorine contamination, and improper storage
at the time of inspection, the ladder did not comply with the breaking strength requirement of the ISO 799-1:2019(E) standard
the step fixtures (chocks) had steel fixing screws embedded within, which appeared to have chafed against the side ropes
the most severe failure occurred at the sixteenth step from the bottom of the ladder, where the rope had parted completely – this was where a steel fixing screw had been embedded (Figure 4)
a partial failure occurred between steps 22 and 23, where one of the 2 supporting ropes had broken
minor failures of the side rope occurred throughout the ladder, primarily where securing steel screws were embedded in the plastic components
moisture retention and significant chlorine contamination[4] of the rope fibres
corrosion deposits on the maker’s steel identification plate that was affixed to the ladder’s step.
Figure 4: Step fixtures with steel fixing screws embedded
Source: Vessel operator, annotated by the ATSB
Safety action
The vessel’s operators have implemented the following safety actions to prevent recurrence of such incidents:
A fleet-wide safety bulletin and circular have been issued, highlighting the precautions of pilot ladder use and mandating the immediate use of ladders from a globally reputed manufacturer.
The company's safety management system procedure for maintaining pilot boarding arrangements was updated to include instructions on proper storage of pilot ladders to prevent their degradation.
Fleet-wide changes to the planned maintenance system mandating the inspection, maintenance and storage of in-use and spare pilot ladders.
Pre-joining briefing of shipboard management personnel, emphasising safe pilot boarding arrangements.
Fleet-wide dissemination of this incident’s findings.
Safety message
Pilot ladders are typically manufactured from manila rope, which is a natural fibre. While natural fibre ropes have properties that make them ideal for use in many marine applications, they are also susceptible to damage and loss of strength from UV exposure, dirt and chemicals. Rope ladders should be adequately covered and not be stored together with acids, detergents or paint as these products and their fumes may cause the fibres to deteriorate prematurely.
Vessel operators and crew should not assume that new and unused rope ladders will be free from damage. Although the surface of the rope may appear to be in satisfactory condition, natural fibre ropes can self-abrade from the inside. It is therefore essential to open the lay of the ropes and check the strands for any internal deterioration. Regular onboard inspections, comprising visual and physical examinations, are required to ensure that the ladders are stored and maintained in a suitable environment.
Ideally rope ladders should be stored in a cool, dry and well-ventilated compartment, or if kept on the exposed deck area of ships, ranged at regular intervals to facilitate drying between uses.
Marine Notice 04/2023[5] provides guidance on pilot transfer arrangements and highlights the issues due to regular non-compliance with these arrangements. The notice stated that since November 2017, multiple separate incidents involving the failure of a pilot ladder securing point or manropes had been reported.
The International Maritime Organization Sub-Committee on Navigation, Communications and Search and Rescue (NCSR) finalised the draft amendments to SOLAS Regulation V/23 and associated instruments to improve the safety of pilot transfer arrangements. These amendments are expected to enter into force from 1 January 2028. Vessel operators and managers are urged to heed the relevant requirements and, where possible, implement the measures on a proactive basis.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Manropes are 2 ropes of not less than 28 mm and not more than 32 mm diameter secured to the ship in addition to the pilot ladder if required by the pilot. They are placed either side of the pilot ladder and fixed at the rope end to a ring plate fixed on the ship’s deck.
[2]The ship’s freeboard was reported as 7.8 m and therefore a combination ladder (pilot ladder used in conjunction with accommodation ladder) was not required.
[4]In addition to potential saltwater exposure while stored on deck, the ladder was stored in an environment exposed to chemical mixtures comprising hydrochloric acid in the forecastle store for approximately one year.
A GA8 Airvan operating a scenic flight in Queensland’s Whitsunday region overran the runway after the pilot did not initiate a go‑around when the aircraft was above profile with a high airspeed during approach, an ATSB investigation report details.
The aircraft, operated by Wave Air and with a pilot and seven passengers on board, was landing at Whitsunday Airport at Shute Harbour at the conclusion of a scenic flight on 2 November 2024.
After overrunning the runway, the Airvan travelled briefly across grass before entering marshy ground and coming to a stop in a ditch. While the aircraft was substantially damaged, the pilot and passengers were uninjured.
Multiple onboard passenger videos aided the ATSB investigation in determining the aircraft’s flightpath and speed during the approach and landing.
“The aircraft’s approach was above profile with a high airspeed,” Director Transport Safety Stuart Macleod explained.
“Subsequently, the landing was beyond the planned touchdown point.”
The report details that the aircraft passed over the displaced threshold of the runway at approximately 100 ft AGL. The pilot commenced the flare about 300 m beyond the displaced threshold, at an airspeed of approximately 90 kt. The aircraft then floated for about 640 m before touching down at a groundspeed of 65 kt with 370 m of runway remaining
“While landing beyond the planned touchdown point, there was adequate landing distance remaining, however the pilot did not apply sufficient braking to stop the aircraft departing the runway.”
The investigation determined the pilot had an incorrect understanding of the required approach speed. It also found that the pilot’s initial training was not fully completed, and that Wave Air’s training, supervision and checking flights did not identify the pilot’s approach speed was routinely excessive.
“For pilots, this accident should demonstrate the importance of accurate knowledge of your aircraft’s reference speeds, and always being prepared to promptly execute a go‑around if an approach for landing does not proceed as expected,” Mr Macleod noted.
“In addition, routinely practicing go‑arounds will ensure the manoeuvre can be performed safely when needed.”
While not determined to have contributed to the accident, the investigation also found Wave Air’s weight and balance system used an incorrect figure to calculate the aircraft’s centre of gravity, and passengers were not weighed in accordance with the operator’s procedures.
Additionally, it was found the operator’s stabilised approach criteria included a decision height which was too low.
Since the accident Wave Air has taken several safety actions including updating its training and checking manual, appointing a new head of training and checking, updating pilot training, reviewing procedures and errors in the weight and balance system, and revising its stabilised approach criteria.
On 8 February 2025, the pilot of a Bell Helicopter 206B was conducting a scenic flight from Cairns Airport, Queensland (Figure 1). The passengers comprised 2 adults and 2 children, with 1 child placed in the front left seat and the remaining passengers in the rear of the helicopter.
Figure 1: Bell Helicopter 206B with incident location (inset)
Source: Operator and Google Earth, annotated by the ATSB
Approximately 12 minutes into the flight, the pilot contacted the operator over the company radio and expressed concern about the operation of the flight controls. The control issues were similar to a previously reported occurrence from approximately a month earlier, where the pilot had experienced an aft ‘kick’ in the flight controls, followed by stiffening of both the cyclic and the collective controls. On this occasion, the pilot also experienced the cyclic control moving to the right.
Following the previous occurrence, the operator conducted a technical assessment of the aircraft’s hydraulic system, but no abnormalities were detected, and the precise cause of the issue was not identified.
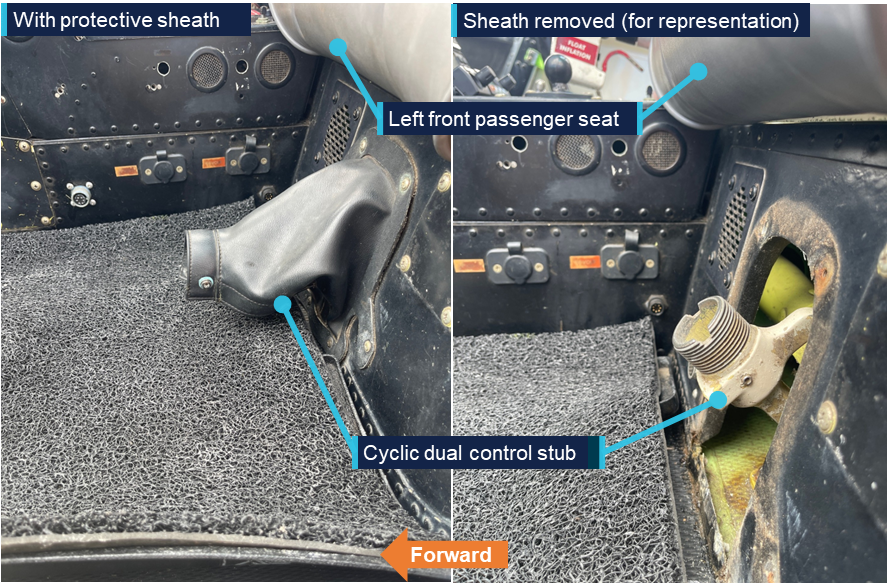
On this occasion, on being notified of the issue by the pilot during flight, the operator immediately advised the pilot to check the front seat passenger’s feet position. The pilot observed that the passenger’s feet were interfering with the copilot cyclic[1] control stub. The stub was a small moveable part that remained on the floor of the helicopter under the seat, after the copilot cyclic control stick had been removed (Figure 2).
Shortly after, the pilot reported to the operator that they had moved the passenger’s feet, resulting in normal operation of the controls. The operator provided the pilot with the option to return to the airport at their discretion, but the pilot elected to continue the flight.
On arrival back at Cairns Airport, the operator and pilot discussed the occurrence in further detail. During the debrief, the operator deliberately manipulated the copilot cyclic stub to allow the pilot to feel the corresponding effect on the flight controls. The pilot confirmed that the stiffening of the controls was similar to that experienced in flight.
In the absence of any fault with the hydraulic system and the near-identical symptoms experienced in both occurrences, the operator determined that the likely cause of the previous month-old occurrence was also due to the same reason.
The ATSB was advised that the operator purchased the helicopter around late-November 2024 and thereafter installed the left side copilot controls for pilot training flights.
Bell Helicopter Textron Inc. Service Instruction BHT-206-SI-67 Service instruction for dual controls, quick disconnect provided procedures to install left side controls. In reference to this incident, the Service Instruction required the installation of a cyclic cover following the removal of a copilot cyclic control stick.
The ATSB identified that the operator had not installed a cover on the left side copilot cyclic control stub following the removal of the cyclic control stick. Similarly, it was identified that a protective cover for the collective control stub had not been installed by the operator, which increased the risk of accidental flight control interference.
Safety action
Following the incident, the operator advised of the following safety action:
metal cover has been installed on the left side copilot cyclic control stub
a cover has been ordered for the left side copilot collective control stub and will be installed as soon as it is received
they will inform all pilots of the risk of inadvertent passenger interference of the flight controls
remind all pilots of the requirement to adhere to aircraft flight manual procedures in the event of an abnormal situation being encountered
review relevant Safety Instructions and Safety Bulletins issued by the aircraft manufacturer.
Safety message
Where removable flight controls are utilised, aircraft operators must ensure the personnel installing/removing the flight controls are appropriately trained to do so. Installation/removal should also be conducted in accordance with the manufacturer’s instructions, including any associated safety precautions.
In addition, the pilot’s pre-flight safety briefing to passengers must clearly emphasise the importance of avoiding contact with any flight controls.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
At about 2005 local time on 26 November 2024, a Piper Aircraft PA-28R departed Archerfield Airport runway 10L, for night VFR[1] solo circuit training under the supervision of a ground instructor. All aircraft around the aerodrome were operating under common traffic advisory frequency (CTAF) procedures as it was outside of air traffic control tower hours.
Turning onto the circuit base leg, the pilot made a radio call, advising of their position and intent to conduct a touch-and-go. The aircraft subsequently turned onto final for runway 10L at about 500 ft AGL.
At around the same time as the Piper was turning onto final, the pilot of a Vulcanair P.68B operating under IFR[2] made a radio call to advise they were inbound on an area navigation (RNAV) approach to runway 10L. This prompted the pilot of the Piper to make a radio call advising they were on final for runway 10L. Both aircraft continued their approaches and made a series of radio calls to determine their respective positions. When the pilot of the Piper became aware that the 2 aircraft were likely in close proximity, they discontinued the approach and conducted a go‑around. The Vulcanair pilot continued the approach and landed without further event.
The Vulcanair pilot advised they had received a traffic report on the Piper conducting circuits when they became visual with the aerodrome but reported that they did not attempt to establish communication with the Piper before continuing the final stages of the approach.
Recorded ADS-B data showed that the 2 aircraft came within about 37 m horizontally and 50 ft vertically, before the Piper discontinued the approach. Neither pilot reported establishing visual contact with the other aircraft.
Safety message
This incident highlights the importance of situational awareness and effective communication when making and monitoring radio calls over the CTAF, to coordinate separation with others during times of aerodrome tower closure.
The Civil Aviation Safety Authority’s AC 91-10 v1.3 provides further guidance on procedures that, when followed, will improve situational awareness and safety for all pilots flying in the vicinity of non-controlled aerodromes or outside of air traffic control tower hours.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Visual flight rules (VFR): A set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2]Instrument flight rules (IFR): A set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-048
Occurrence date
26/11/2024
Location
Archerfield Airport
State
Queensland
Occurrence class
Serious Incident
Aviation occurrence category
Near collision
Highest injury level
None
Brief release date
05/05/2025
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-28R-200
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
The ATSB is investigating a collision with water involving Robinson R44, VH-CTT, 13 km east of Barwon Heads Airport, Victoria, on 2 May 2025.
The final report has been drafted and is undergoing internal review to ensure the report adequately and accurately reflects the evidence collected, analysis, and agreed findings.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2025-022
Occurrence date
02/05/2025
Occurrence time and timezone
09:43 Australian Eastern Standard Time
Location
13 km east of Barwon Heads Airport
State
Victoria
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Internal review
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Abnormal engine indications, Collision with terrain, Engine failure or malfunction, Loss of control
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R44 II
Registration
VH-CTT
Serial number
12599
Aircraft operator
Helicopter Adventures Pty Ltd
Sector
Helicopter
Operation type
Part 133 Air transport operations - rotorcraft
Activity
Commercial air transport-Non-scheduled-Joyflights / sightseeing charters
Departure point
Barwon Heads/Geelong Aircraft Landing Area, Victoria
Destination
Barwon Heads/Geelong Aircraft Landing Area, Victoria