
Final report
Report release date: 02/04/2026
Investigation summary
What happened
On 2 separate occasions in 2025, the Gate 82 aerobridge at the Brisbane International Airport Terminal collided with 2 narrow-body Boeing 737 aircraft, registrations VH-VZG (18 June) and DQ-FAE (26 July 2025).
The aerobridge operators, from 2 separate airlines, intended to drive the aerobridge parallel to the parked aircraft on the bay from the aerobridge home position prior to docking. However, the aerobridge moved diagonally towards the aircraft until the bottom right corner of the aerobridge impacted the aircraft and broke through the aircraft cockpit windshield. The collisions resulted in minor damage on both occasions with no recorded injuries.
What the ATSB found
Visibility of narrow-body aircraft was restricted from the aerobridge home position due to the required parking location of narrow-body aircraft, to the far right of the aerobridge home position. In addition, the design of the aerobridge cab walls, which lacked viewing windows installed in some other aerobridges at the airport, also limited direct visibility.
Both operators did not have visual reference of the aircraft prior to the collisions but expected to gain visibility following aerobridge extension. This expectation was reinforced by previous successful operations and was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft.
Both operators had moved the joystick to a 3 o’clock position and believed they were moving the aerobridge parallel to the aircraft. However, the aerobridge moved diagonally towards the aircraft. Both operators had rotated the cab left and were unaware that this orientation changed the direction of travel of the aerobridge. The operators were not alerted to the diagonal movement because they could not see the aircraft and perceived no other information to challenge their spatial orientation.
The ATSB identified that Brisbane Airport Corporation’s training material and in-cab instructions did not provide direction to operators to gain and maintain visibility of the aircraft from the home position, before moving the aerobridge.
Safety features designed to prevent collisions and damage to aircraft did not activate due to the approach angle of the aerobridge.
In the first occurrence an engineer on the ground activated the aerobridge emergency stop button to prevent further damage to the aircraft.
What has been done as a result
Following the occurrences in August 2025, Brisbane Airport Corporation (BAC) disseminated a safety notice to all operators that emphasised the requirement to rotate the cab towards the aircraft, always maintain positive line-of-sight with the aircraft, and cease operations if visual reference is lost.
BAC also reviewed the operator training material and identified gaps and an opportunity to be more specific in the process to safely attach aerobridges (similar to aerobridge 82) to aircraft. The training was updated in January 2026. Obsolete and inconsistent in‑cab instructions are in the process of being removed and will not be replaced in the aerobridge cabs.
BAC also created a new role focused on airside performance of assets and operators, including aerobridges, and all supporting infrastructure tools the operators use. Quality assurance activities have commenced with the role in place.
An aerobridge replacement program will renew 8 aerobridges at Brisbane Airport, including the aerobridge at Gate 82, commencing in 2026 at the International Terminal. BAC will review safety features and narrow-body visibility will be reviewed as part of this program. BAC is also planning to trial automated docking of aerobridges in the first half of 2026.
Fiji Airways has temporarily introduced a second operator as a ‘spotter’ at Gate 82 pending the release of this report.
Safety message
There are many risk controls in place at airports and within ground handling companies and airlines to help minimise the hazards associated with airport ground operations.
Visibility of aircraft is critical for safe aerobridge operations. Aerobridges should be designed to maximise visibility and aerobridge training should reinforce visibility as a critical step in safe operations.
Aerobridge training and operational documentation should also highlight the mental rotation required for operators when joystick movement is relative to the orientation of the cab and not fixed to the direction of the aerobridge tunnel, or other stationary visual references outside the aerobridge.
The occurrences
Aerobridge operation – both occurrences
On 2 separate occasions, during aircraft arrival at the bay at night, prior to passenger disembarkation, the aerobridge at Gate 82 of the international terminal at Brisbane Airport collided with 2 different aircraft, resulting in minor damage to the cockpit windshields.
The first aircraft was a B737-838 narrow-body operating as Qantas flight QF186 (VH‑VZG), from Queenstown, New Zealand, on 18 June 2025.
The second aircraft was a B737-8 MAX narrow-body operating as Fiji Airways flight FJ923 (DQ-FAE), from Nadi, Fiji, on 26 July 2025.
On both occasions, the aircraft were correctly parked in the designated marshaller’s position[1] for a Boeing 737 (Figure 1), in line with the visual docking guidance system (VDGS).
Figure 1: Overview of aerobridge operational area

Source: Brisbane Airport Corporation
On both occasions, the aerobridge was operated at night (Figure 2). Rain was present in the area prior to the second event on 26 July 2025, with water visible on the ground (Figure 2, right).
After receiving visual confirmation from ground staff to indicate the wheels were chocked and the park brake was released, both operators activated the aerobridge by swiping their security identity card at the operator console and then initiated movement from the default home position (Figure 2).
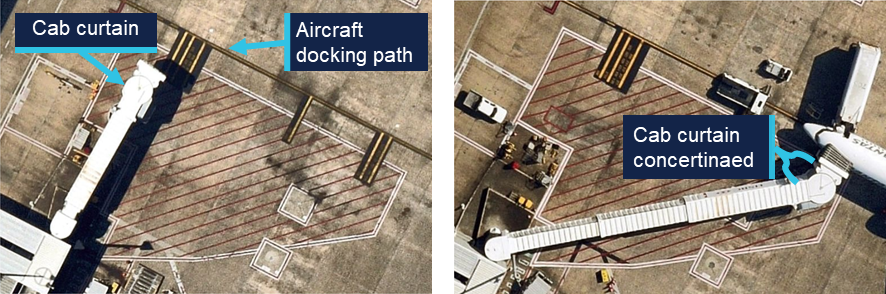
Figure 2: Home position of aerobridge with parked QF186 (left) and FJ923 (right)

Source: Brisbane Airport Corporation
Closed circuit television (CCTV) showed that at about 30 seconds into the aerobridge extension (halfway through), and while moving diagonally, the aerobridge cab was rotated to the left as identified by contraction of the concertinaed side curtain (Figure 3).
Figure 3: Left orientation of cab at 1845, 18 June 2025 (left) and 2304, 26 July 2025 (right)

Source: Brisbane Airport Corporation, annotated by the ATSB
During this time, the aerobridge continued to move diagonally towards the aircraft before the bottom right corner of the aerobridge impacted the aircraft windshield.
Both operators expected to gain visibility of the aircraft from the cab window during the aerobridge extension from the home position. They both reported previous successful operations where gaining visibility of the aircraft was delayed, but always occurred, and both stated that they were surprised by the unexpected collision.
While glass fragments entered the cockpit, and a jolt occurred, no injuries resulted to crew or passengers on either occasion. The aircraft windshields were subsequently replaced, and pressurisation was checked before both aircraft continued operations. The aerobridge was also assessed, however no faults were identified, and a return to service check was conducted before further operations on each occasion.
Occurrence 1 details
At 1845 on 18 June 2025, aerobridge 82 was being operated by a Qantas customer service agent (Operator 1) to disembark QF186 (VH-VZG), a B737-838 narrow-body aircraft after arrival from Queenstown, New Zealand.
At 1846 the right aircraft windshield was impacted by the front right aerobridge corner (Figure 4, left). A licensed aircraft maintenance engineer (LAME) was on the ground assessing the aircraft following a potential bird strike. They detected abnormal operation of the aerobridge and attempted to alert the aerobridge operator by hand gestures before activating the on-ground emergency stop at the same time as the impact.
From the cockpit, 2 flight crew members noticed the aerobridge approaching the aircraft from a high angle and further towards the nose of the aircraft than usual. The captain pressed the ground call switch on board to contact engineering or other ground staff to advise them of their urgent concern that the aerobridge was likely to impact the aircraft.
The crew were unable to make contact with engineering or ground staff before the aerobridge collided with the first officer’s windshield, shattering the glass (Figure 4, right). Although the glass fragments landed on the first officer, they were uninjured. The flight crew reported a jolt at impact, however, no passengers or cabin crew were injured.
Figure 4: Collision and damage to QF186

Occurrence 2 details
At 2304 on 26 July 2025, aerobridge 82 was being operated by a Fiji Airways customer service agent (Operator 2) to disembark FJ923 (DQ-FAE), a B737-8 MAX narrow-body aircraft after arriving from Nadi, Fiji.
At 2305 the left aircraft windshield was impacted by the front right aerobridge corner (Figure 5, left). From the cockpit, 2 flight crew members noticed the unusual movement of the aerobridge towards the aircraft, aligned with the windshield (rather than the side of the fuselage). They expected the movement to stop, but it continued until impact.
Although glass fragments and the corner of the aerobridge partially entered the cockpit (Figure 5, right), the captain was able to move out of their seat and they were uninjured. The flight crew reported a jolt at impact; however, no passengers or cabin crew were injured.
Figure 5: Collision and damage to FJ923

Source: Brisbane Airport Corporation
Context
Personnel information
Both aerobridge operators were airline customer service agents employed directly by airlines. Their normal tasking involved customer-facing pre-flight and post-flight services as well as ground operations support.
Operator 1 (Qantas) was certified in January 2024, and Operator 2 (Fiji Airways) was certified in June 2024, both were certified to operate international aerobridges, including aerobridge 82. At the time of the occurrences Operator 1 had 17 months experience and Operator 2 had 13 months experience in operating aerobridges.
Operator 1 had controlled aerobridge 82 within 3 months of the occurrence and Operator 2 had controlled aerobridge 82 within 2 months of the occurrence.
Both operators reported adequate prior sleep and recalled feeling fully alert at the time of the occurrences.
Aircraft information
Both aircraft were Boeing B737 narrow-body aircraft. VH-VZG (QF186) was a Boeing 737‑838 and DQ-FAE (FJ923) was a B737-8 MAX.
Meteorological information
Dark night conditions were present in both occurrences, and the operational area was illuminated with bright lights (Figure 2).
No significant weather was recorded prior to the first occurrence on 18 June 2025. In contrast, rain occurred at Brisbane Airport on 26 July 2025, and precipitation was present in the area prior to the second occurrence.
Aerobridge information
An aerobridge (or passenger boarding bridge) is an enclosed, elevated passageway which extends from an airport terminal gate to an aircraft.
Five types of aerobridges were in operation at Brisbane Airport across the international and domestic aprons, these ranged from fixed or pedestal aerobridges to moveable or apron drive aerobridges.
Aerobridge 82
The aerobridge at Gate 82 of the Brisbane international terminal was a Jetway Apron Drive Aerobridge. It was installed in 1995 and was in continued service for 30 years at the time of both occurrences.
As a telescopic bridge, aerobridge 82 was used for a wide range of aircraft and parking positions. The aerobridge could swing up to 180 degrees (clockwise and counterclockwise) across the bay and extend, raise or lower depending on the aircraft size. Fiji Airways used aerobridge 82 mostly for narrow-body aircraft, while Qantas used aerobridge 82 for mostly wide-body aircraft, and narrow-body aircraft on occasion.
- A prime factor determining the parking position of the aircraft and therefore the required orientation and extension length of the aerobridge was maintaining aerobridge slope as close to the design limit of 1:14. For example, if the aerobridge was to rise 1 m, then it also needs to extend by 14 m to maintain suitable slope.
Another factor determining the parking position of the aircraft was the aircraft length forward from the wings (Figure 6):
- Wide-body aircraft fuselage length from the wings forward is relatively long. The designated parking position provided sufficient clearance for the wings from the aerobridge passenger tunnel. When in the designated parking position, the left‑front door lined up with the aerobridge and the required aerobridge extension was minimal.
- Narrow-body aircraft fuselage length from the wings forward is relatively short and require parking further from the aerobridge home position to maintain clearance of the left wing and the aerobridge passenger tunnel. The aerobridge required further extension to the right to line up with the left-front door of the aircraft for aerobridge attachment.
Figure 6: Schematic drawing showing aerobridge movement in relation to a wide-body and narrow-body aircraft

Source: Brisbane Airport Corporation, modified by the ATSB
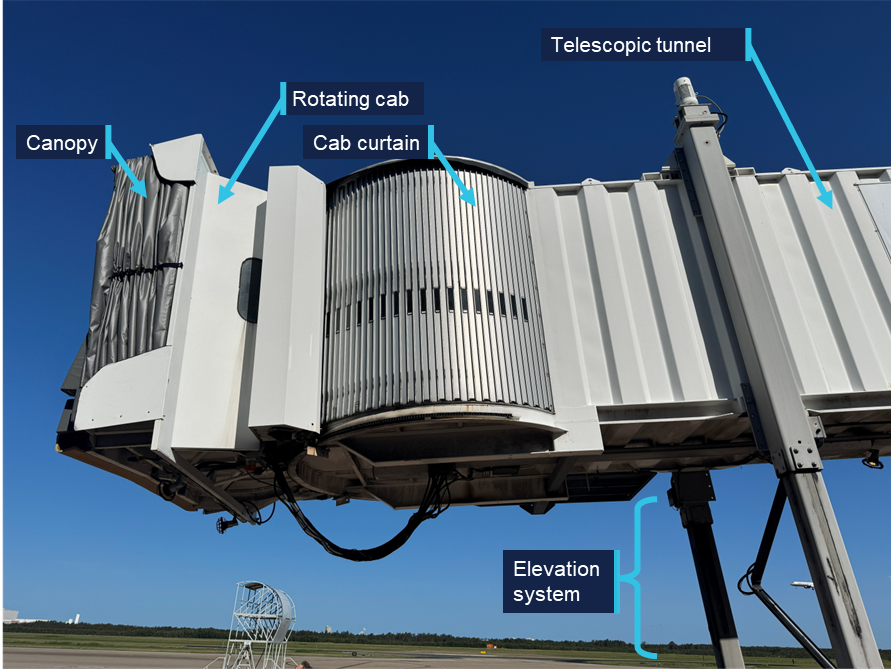
The aerobridge was formed by the following main elements (Figure 7 and Figure 8):
- rotunda with column
- canopy (which closes on to aircraft once the aerobridge is docked)
- bumper with bumper proximity switches
- slow down sensor located under the cab floor
- rotating cab and cab curtain
- telescopic tunnels (which extend and retract)
- elevation and traveling systems.
Figure 7: Front view of aerobridge 82 in the home position

Source: ATSB
An external/on ground emergency stop button was located above the aerobridge wheels (Figure 7).
Figure 8: Side view of aerobridge 82 in the home position
Source: ATSB
Home position
Before and after aerobridge operations, the aerobridge returned to a default home position (Figure 7) where the:
- wheels faced forward within a red home position box marked on the ground
- telescopic tunnel retracted and sat perpendicular to the passenger walkway
- rotating cab faced directly forward
- height was set to 3.57 m.
The home position ensured safe clearance for parking aircraft wing tips, engines and fuselage. Pre-positioning of aerobridge 82 prior to aircraft arrival was previously considered by BAC, however, was removed following safety concerns.
Operator console
The aerobridge was operated using controls mounted on a console on the left side of the cab (Figure 9). The console was positioned and orientated to provide the operator a clear view of aircraft in front during final aerobridge manoeuvring and docking. The operator stood on a slightly raised step below the console.
The step and the console moved together left or right as the cab was rotated, while the circular cab floor remained stationary,[2] and the cab side curtains concertinaed (folded in) or expanded (folded out).
Figure 9: Example operator standing at operator console
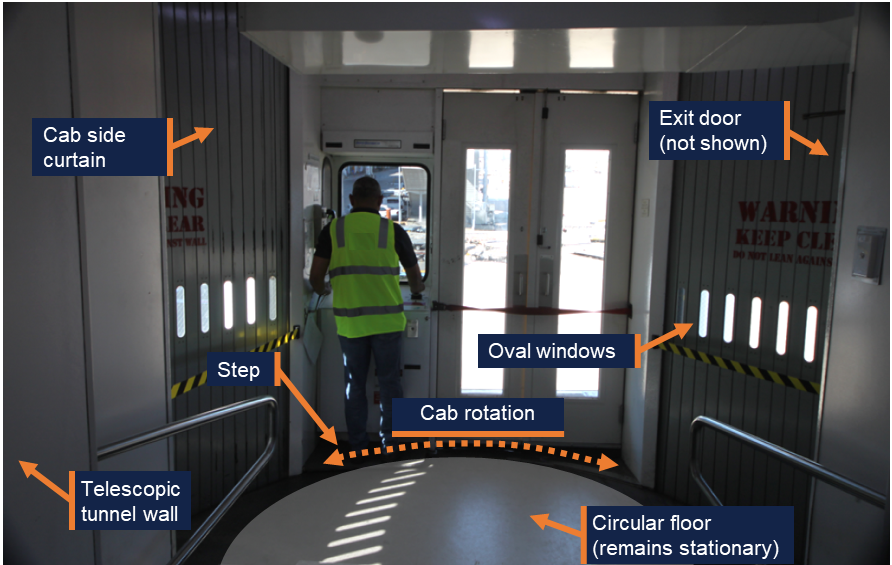
Note: The footprint of circular floor has been exaggerated by the ATSB to illustrate cab rotation around the stationary floor. Source: ATSB
Visibility of narrow-body aircraft
From the home position, wide-body aircraft were visible to aerobridge operators standing at the operator console (Figure 6). However, narrow-body aircraft fell outside the operator’s field of view at the console as the designated parking position was to the far right of the aerobridge. The operator’s view of narrow-body aircraft was blocked by protruding walls inside and outside the right side of the cab (Figure 7 and Figure 9).
For aerobridge 82, oval shaped windows interspersed on the right curtain below the operator’s eye height provided very limited visibility unless the operator left the operating console and bent down to establish visibility directly through the section of window. However, full visibility was not possible while operating the aerobridge and manoeuvring to narrow-bodied aircraft (Figure 9).
Similarly, the operator could exit the cab to view the aircraft via a service door on the far‑right of the cab. This was done on occasion to obtain visual confirmation from the ground crew prior to operation, but the operator could not operate the aerobridge unless they returned to the console.
Some other aerobridge types had been designed with large windows on the right side of the cab at eye level and below, such as the aerobridge at Gate 44 of the Brisbane Domestic terminal (Figure 10).
Figure 10: Right side windows on aerobridge at Gate 44 of the Brisbane Domestic terminal

Source: Brisbane Airport Corporation
Control panel
The control panel contained the required switches, buttons and control sticks to operate the aerobridge (Figure 11). By design, operators could rotate the cab, adjust the height, and move towards the aircraft with simultaneous actions to align with the aircraft door. Operators reported it was normal practice to do so.
Figure 11: Aerobridge control panel
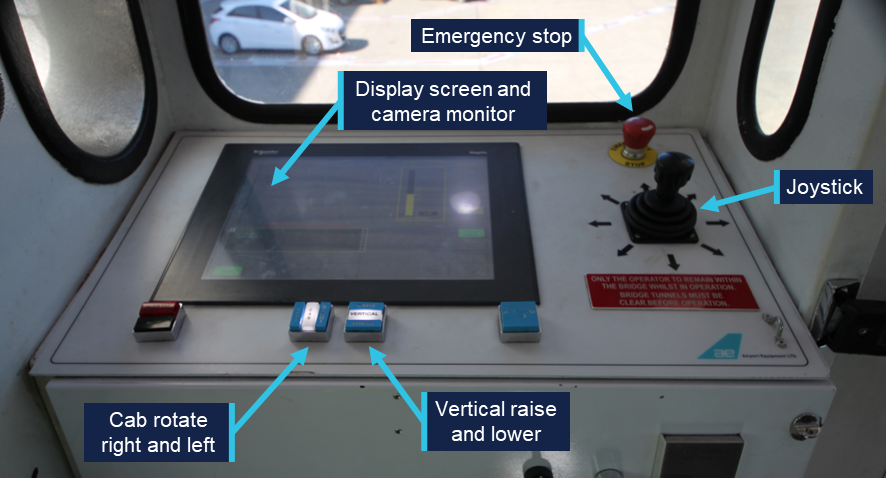
Source: Brisbane Airport Corporation, annotated by the ATSB
Vertical control
Aerobridge height could be adjusted via the vertical raise and lower buttons (Figure 11) to meet the height requirements of each aircraft type. The current height of the front bumper was displayed to the operator via a height gauge on the display screen (Figure 12). The gauge also showed 8 different aircraft types for reference.
Figure 12: Display screen and camera monitor
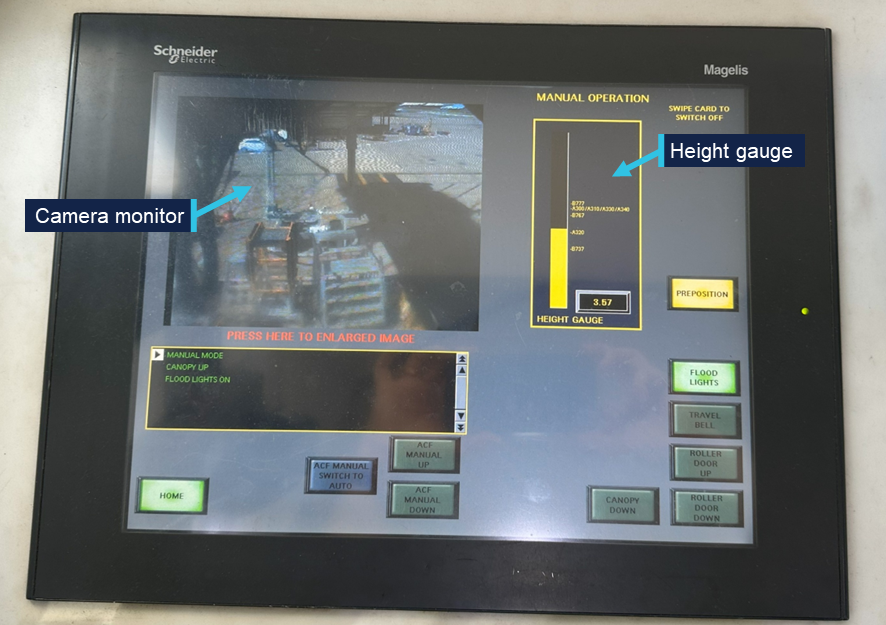
Source: ATSB
The default home height of 3.57 m was suitable for attaching aerobridge 82 to the door of an Airbus A320 aircraft, however the aerobridge needed to be lowered to meet the door height of a Boeing 737.
Cab rotate right and left
To attach the aerobridge to the aircraft door, operators were required to orient the rotating cab, using the left and right buttons (Figure 11) to ensure the cab was parallel to the fuselage (or the aircraft docking path). As the home position of the cab faced directly forward, the cab also needed to be rotated left to attach to a 737 (Figure 13), demonstrated by the concertinaed cab curtain.
Operators reported it was normal technique to pre-emptively rotate the cab to the left while moving the aerobridge horizontally or laterally.
Figure 13: Aerobridge in home position (left) and correctly attached to a 737 (right)
Source: Qantas
Joystick
The joystick controlled the aerobridge’s direction of travel and could be moved 360 degrees about its central point (Figure 11). The aerobridge drive wheels oriented to the desired direction of travel when the operator pushed the joystick in the required direction.
Speed of aerobridge movement and extension was controlled by the amount of pressure the operator applied to the joystick. The further control input, the faster the aerobridge would move. Movement stopped when the operator released the joystick (following a short delay which was perceived as a minor jolt to operators) and the joystick returned to the central neutral position.
The joystick was designed to move relative to the orientation of the cab. Specifically, relative to the forward-facing window (and therefore the direction the operator was normally facing) and not the direction of the tunnel. If the orientation or rotation of the cab changed, so did the direction of travel.
From the home position, the operator could move the joystick to a 3 o’clock direction, and the wheels would orient to travel right (Figure 14, left), and the aerobridge would travel to the right, parallel to the parked aircraft.[3]
If the operator rotated the cab slightly left from the home position (Figure 14, right), and pushed the joystick to a 3 o’clock position, as the movement of the aerobridge would be relative to the direction the cab was orientated, the aerobridge would travel diagonally towards the parked aircraft.
Figure 14: The operator’s 3 o’clock direction from home position (left) versus the operator’s 3 o’clock direction when the cab rotated slightly left (right)
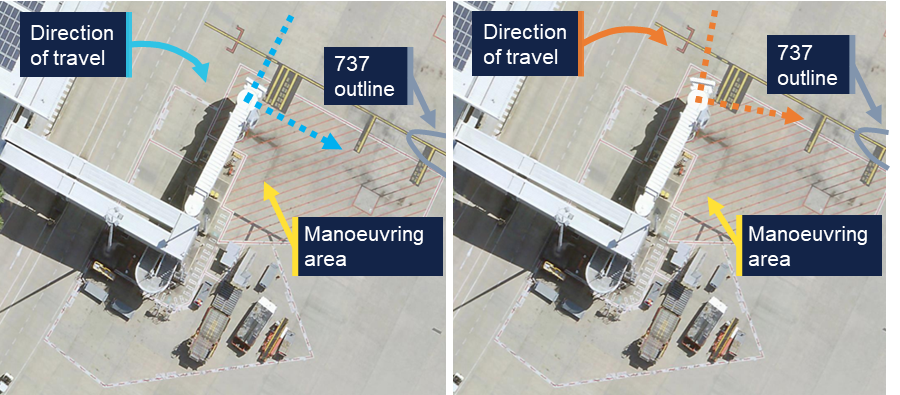
Note: Right image was edited to replicate left cab rotation. Source: Brisbane Airport Corporation, annotated by the ATSB
To anticipate the direction of travel, operators were therefore required to mentally rotate[4] the direction of travel relative to the orientation of the cab. Visible stationary references outside the cab would likely aid operators to orient the direction of travel during aerobridge movement (and correct any potential orientation errors).
Camera monitor
A front facing CCTV view of the area underneath the cab (around the wheels) was presented to the operator as a safety control to prevent contact between the elevation and travel systems (Figure 7) and any person or object inside the aerobridge manoeuvring area marked by red hatching (Figure 14).
Operators reported, and the ATSB observed, that perceptibility of the CCTV could be reduced by glare and shadows (Figure 12).
The aerobridge operator of the second occurrence reported additional blurriness on the monitor, potentially due to condensation following rain in the area prior to the event.
Safety features
The following safety features were installed on aerobridge 82 to prevent collisions with aircraft:
- A slow down sensor (or slow down beam) located under the cab floor was used to detect aerobridge proximity to the aircraft fuselage. When the ultrasonic sensor detected an obstruction directly in front of the cab, the horizontal speed slowed.
- Four bumper switches (or bumper proximity switches) located in the bumper of each aerobridge were designed to detect when the aerobridge bumper contacted an aircraft. Four spring loaded probes stopped bridge extension if activated by forward touch, while the outer 2 probes also prevented cab rotation if activated by forward touch.
Neither proximity nor bumper switches activated during the 2 occurrences.
More sophisticated anti-collision systems were installed on 7 multi-bridge[5] aerobridges at Brisbane Airport. These anti-collision systems were designed to avoid collision with other aerobridges or aircraft in front of, and either side of, the aerobridges. However, these were not equipped on single aerobridges like aerobridge 82.
Separate to the camera monitor which showed the wheel area, no other CCTV cameras were installed. Additional camera views had been discussed and considered by Brisbane Airport Corporation (BAC) for aerobridge 82, however were not installed. Further, these camera views were for inside the cab to view operator functions, not as additional visibility for the operator.
While alarms (and alerts via the display screen) were frequently presented to operators of aerobridge 82 to help operators troubleshoot common faults or issues, no alarms or alerts activated prior to the collisions.
Maintenance
Aerobridge 82 was maintained by a third party service provider, Alstef Group on behalf of BAC.
Onsite technicians responded to phone calls and callouts to address issues, faults and alarms that could not be addressed by aerobridge operators. Operator training highlighted the reporting process (and 24/7 phone number) for faults, error messages and persistent alarms. A phone was installed on the wall near the operator console for maintenance provider contact.
Preventative maintenance inspections were carried out at 3, 6, and 12 months in line with the Operating and maintenance manual[6] using standardised checklists. Weekly inspections were conducted as an additional control for aerobridge serviceability and operation. A weekly cab curtain serviceability check was also added following a fall from height occurrence at Sydney Airport in 2025.
Return to service inspections were conducted following both occurrences, with no significant damage and no faults identified.
Aerobridge operator training
BAC was responsible for the aerobridge operations at Brisbane Airport. BAC held the responsibility for operator training, operational procedures and instructions and governed user access. However, the day-to-day operation was performed by airline staff or contracted to third party service providers (e.g. ground handlers).
Certification
BAC required aerobridge operators to be trained and certified for the appropriate aerobridge type. Training involved e-learning modules, in-person demonstrations and assessment by certified aerobridge trainer/assessors for competency.
E-learning
Operators were required to successfully complete a general aerobridge e-learning module (updated in June 2022) and at least one other aerobridge specific e-learning module for each aerobridge type.
The specific module that was applicable to aerobridge 82 was the Jetway Apron Drive (International) module (updated in September 2023). The training content of this module was relevant to 3 different Jetway Apron Drive aerobridges in use at Brisbane Airport, with different control panels, but similar functionality. The training material broadly covered operations for both wide and narrow-body aircraft but did not specify individual instructions for different aircraft types.
Both the general and specific modules included online assessments that required a 100% pass mark. Ten questions were provided for the general module and 5 questions for the Jetway Apron Drive (International) module.
The training content was based on Airport Equipment (New Zealand) Limited Operation and Maintenance manuals, particularly the standard operating procedures for manual docking.
The training modules contained clear safety messages about the operation of aerobridges. Safety risks (and controls) were emphasised for:
- movement of aircraft once docked (use of auto lever and safety shoe)
- contact with the elevation and travel systems (visual check of the control area to ensure no person or obstruction is present)
- injury due to moving machine parts (one operator permitted in cab (unless training))
- risk of falls from height (use of safety straps and curtain gap checks)
- loss of control during operation (emergency stop button).
The general module also contained case studies of previous safety occurrences to communicate safety lessons.
The BAC docking procedure detailed in the training module (Figure 15) instructed operators to:
- first use the joystick to drive towards the aircraft door until approximately 500 mm (Step 4)
- then use the cab rotate buttons to ensure the bumper was parallel with the aircraft (Step 5)
- then use the joystick to extend further (Step 5)
- further adjust the cabin height and angle to align the with the aircraft door (Step 5).
Figure 15: Docking procedure from the Jetway Apron Drive (International) module
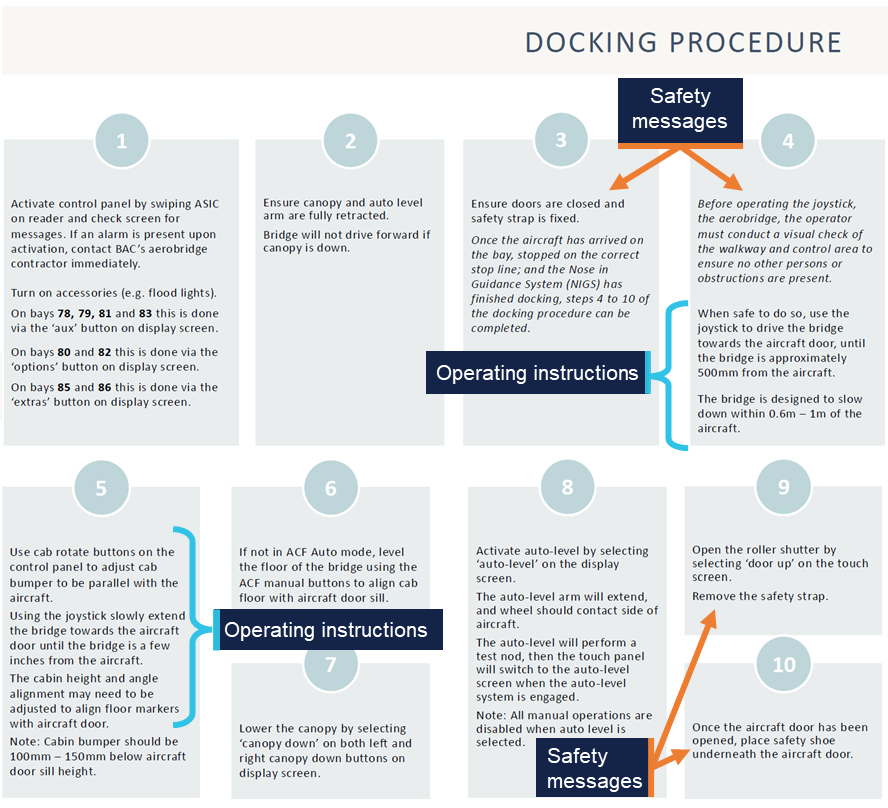
Source: Brisbane Airport Corporation
The docking procedure did not detail rotation of the cab to obtain visibility of the aircraft prior to movement, or to stop movement if visibility was lost. Also, visibility of aircraft was not explicitly mentioned elsewhere in the 2 modules or online assessments.
ATSB review of available training material from other airports showed that at least one other Australian international airport emphasises visibility in aerobridge operator training and assessment material.
Interviews with involved personnel (including Operator 1 and 2) did not highlight that joystick operation was relative to the operator’s front facing window. The operator training and instructions were also silent on this feature of the joystick.
Train-the-trainer
BAC provided train-the-trainer service to designated airline staff (such as experienced airline aerobridge operators), who would then internally train and assess airline aerobridge operators. The train-the-trainer service was provided by a third party contractor, Aviator Operator Solutions, which was contracted by Airport Equipment (New Zealand) Limited, which in turn was contracted by Alstef, on behalf of BAC.
Trainers completed a train-the-trainer session every 2 years to maintain approved trainer/assessor status.
The training involved 2 days of classroom theory and concluded with an in-person demonstration and assessment.
Both operator 1 and 2 received in-person practical training and assessment by trainer/assessors from their company airline.
Operator assessment
Assessment was conducted by an approved trainer/assessor using the BNE Operator Practical Assessment form (updated on 1 July 2022).
An operator was deemed competent once 14 steps were observed by the trainer/assessor. Each step contained several sub-steps, however full competency was recorded (yes or no) for the full step (Figure 16).
Figure 16: BNE Aerobridge Operator – Practical Assessment
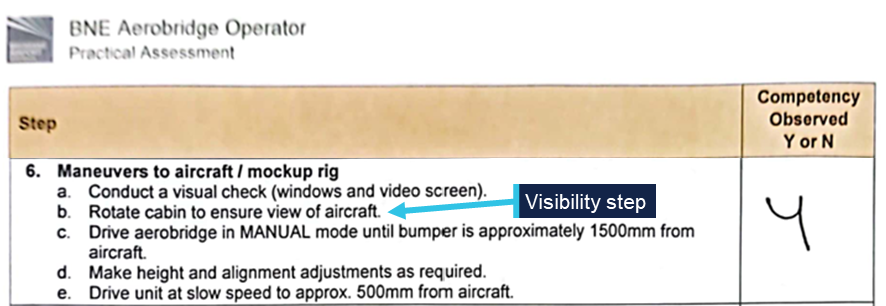
Source: Supplied
One item, step 6b, of the assessment form required operators to rotate the cab to ensure view of the aircraft (Figure 16).
Once assessed as competent under the BNE Operator Practical Assessment, competency was valid for a maximum of 2 years before the operator would need to be reassessed.
Operator recency
Where an operator had not operated an aerobridge for 6 months, e-learning refresher training was required. The BAC security card system would automatically revoke the operator’s access if operator recency was not up to date.
Aerobridge operating instructions
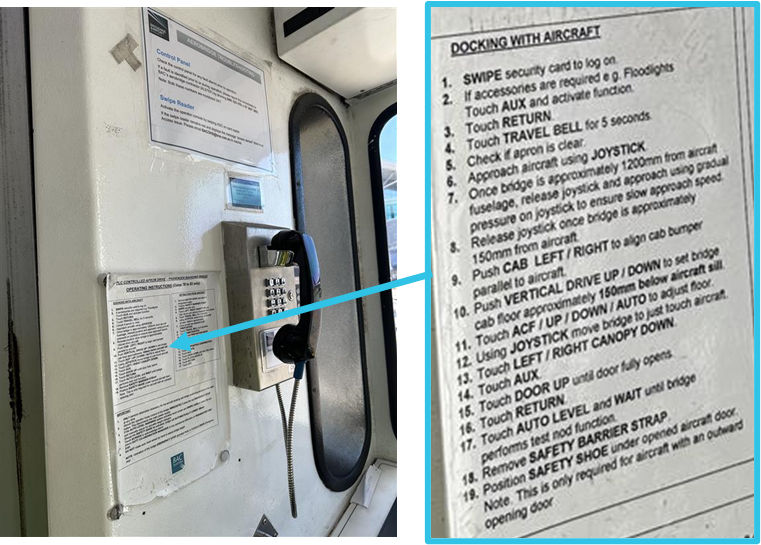
Laminated operating instructions were stuck to the cab wall next to the operator console (Figure 17). Step 6 of the instructions stated: ‘approach aircraft using joystick’ and steps 7–12 contained instruction to continue docking with control movements once the aerobridge was within 1.2 m of the aircraft.
These instructions did not require operators to obtain visibility of the aircraft, rotate the cab prior to movement or to stop movement if visibility was lost.
Figure 17: Laminated operating instructions
Source: ATSB
Visibility requirements for safe operation
Interviews with involved personnel (including Operator 1 and 2) revealed that rotating the cab to ensure visibility was not widely understood as a critical safety step prior to the occurrences.
Both operators reported multiple previous successful aerobridge dockings, including at aerobridge 82, where they did gain visibility of the aircraft prior to docking, but not prior to initial aerobridge movement.
Insufficient visibility from the driving or operating position is recognised as an ergonomic hazard in the European design standard used for Australian aerobridges (EN 12312‑4:2024).
External visual reference points
While not formally documented or trained, both operators reported using alternate visual reference points. Operator 1 reported using the CCTV camera monitor (Figure 12) briefly to view the nose of the aircraft prior to the collision. Operator 2 reported using the ‘red line’ aircraft docking path (Figure 13) to help orient their direction of travel on occasion during normal operations, but not on this occasion. The height of the cab during operation may restrict visibility of these ground reference points, depending on the position of the aerobridge and the height of the operator.
Recorded information
BAC automatically recorded each time an operator swiped their aviation security identity card (ASIC) to activate an aerobridge at Brisbane Airport.
BAC also recorded Gate 82 aerobridge operations from a CCTV camera mounted on the terminal building (view shown in Figure 2 and Figure 3).
No cameras were installed inside the aerobridge cab and the CCTV camera monitor showing the underneath wheel area of the aerobridge was not recorded. The aerobridge 82 control system did not log or record specific user actions or system output while the bridge was in operation.
Regulatory information
The Civil Aviation Safety Regulations (CASR) Part 139 (Aerodromes) Manual of Standards 2019 (the Part 139 MOS) required aerodrome operators to ensure that the apron safety management procedures were followed by any organisation that conducts operational activities on the apron. Where operations on an apron are controlled by third parties, such as airline operators, ground handling agents or other parties, the responsibility of apron safety remains with the aerodrome operator. Further guidance is available at Advisory Circular 139.C-13 v1.0.
Related occurrences
Two similar occurrences have been recorded at Brisbane International Airport Gate 82, occurring on 3 March 2011 and 19 February 2012.[7]
On 3 March 2011, the lower, right-hand corner of the aerobridge contacted the nose cone of a Boeing 737-800 during aerobridge docking. An internal investigation by the aircraft operator identified several contributing factors, including:
- The aerobridge operator’s visual reference was impeded.
- The slowdown sensors fitted to the aerobridge did not detect/sense the aircraft due to the approach angle of the aerobridge.
On 19 February 2012, the lower, right-hand corner of the aerobridge contacted the forward upper fuselage of a Boeing 737-800 aircraft during docking, penetrating the skin forward of the windscreen. The internal investigation by Brisbane Airport Corporation identified an option of determining via a risk management process whether retrofitting the existing aerobridges with extra sensor equipment at the side will minimise future impacts with aircraft fuselage.
Safety analysis
Introduction
On 2 separate occasions in 2025, the Gate 82 aerobridge at the Brisbane International Airport Terminal collided with 2 narrow-body Boeing 737 aircraft, registrations VH-VZG (18 June) and DQ-FAE (26 July 2025).
The aerobridge operators, employed by 2 separate airlines, intended to dock with the parked aircraft on the bay. However, the aerobridge collided with the aircraft cockpit windshield resulting in minor damage on both occasions with no recorded injuries.
This analysis will explore the visibility of narrow-body aircraft, the training provided to operators, the design of the joystick operation, the required mental rotation for operators to orient movement, and aerobridge safety features.
Visibility of narrow-body aircraft
From the home position, with the default home cab orientation, operators standing at the operational console have clear visibility directly in front via the front-facing cab windows. As such, there was good visibility of wide-body aircraft parked to the right of the aerobridge. However, due to the parking location of narrow-body aircraft on the bay and the design of the aerobridge 82 walls and windows, there was limited visibility of narrow‑body aircraft for an aerobridge operator at the control console prior to aerobridge movement.
Aerobridge 82 also lacked viewing windows that were available on some other aerobridges at Brisbane Airport. Such windows may have given the operators visibility towards aircraft parked in the narrow-body parking position. Without such windows, the operator was effectively restricted to seeing only what was in front of the cab.
This created a hazard for the safe operation of the aerobridge and increased the risk of an aerobridge collision with narrow-body aircraft.
Contributing factor The aerobridge home position and cab orientation, and lack of side-viewing windows, provided limited outside visual reference to narrow‑body aircraft along the docking path, limiting the safe operation of the aerobridge. |
Normal operations
While not explicitly emphasised in their training, both aerobridge operators understood that visibility of the aircraft prior to docking was required for safe operation. They reported that gaining visibility was immediate for wide-body aircraft from the home position and normally delayed for narrow-body aircraft. Both operators expected to gain visibility of the narrow-body aircraft following aerobridge movement. Their normal steps included simultaneous actions of rotating the cab, lowering the bridge, and moving toward the aircraft.
Both operators did not expect their actions to result in a collision and they did not believe their technique was incorrect or that it differed from other aerobridge operators.
The operators understood they were required to rotate the cabin left to dock successfully and likely pre-emptively rotated the cab left while moving the aerobridge, further reducing visibility. They did not believe that rotating the cab (to the right) to gain and maintain visibility was a critical step before moving from the home position. While there was an opportunity for the operators to become aware of the critical step when they completed their practical assessment, the step was not explicitly trained or emphasised via in-cab instructions.
Contributing factor It was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft, and both operators operated without visual reference prior to the collisions. |
Object orientation and mental rotation
The aerobridge operators believed that they were extending the aerobridge parallel to the aircraft. However, it is certain that both operators rotated the cab left from the home position during aerobridge extension, and this changed the aerobridge travel direction from parallel to diagonal towards the aircraft.
Due to the design of the joystick, cab rotation required operators to mentally rotate, and account for, the expected aerobridge movement. Both operators were unaware that their 3 o’clock frame of reference had rotated (after rotating the cab left) and did not perceive other visual information to make them aware of the diagonal movement.
The operators reported that the movement did not feel different to normal, and that they expected to gain visibility of the aircraft imminently.
However, in the absence of any contradictory feedback, the operators proceeded with an incorrect awareness of the aerobridge directional movement. It was likely that the complexity of the mental rotation required, was not widely understood by the operators and that the task complexity likely increased prior to both collisions because the cab was simultaneously orientated to the left during aerobridge extension, further blocking the operator’s already limited view of the aircraft on the bay.
Contributing factor Both operators rotated the aerobridge cab left, the orientation of the cab changed the relative joystick direction creating a complex mental rotation task. |
Diagonal movement
Both operators reported pushing the joystick right (to a 3 o’clock position) to move the aerobridge parallel to the aircraft and did not perceive any conflicting information (in what they heard, saw, or felt).
Following the occurrences, one operator believed that the aerobridge system had performed an incorrect movement and was faulty (whereby the operator’s action of pushing the joystick right did not match the system behaviour). However, the system did not record user input (or system output) and no relevant pre-occurrence faults were recorded. Post-occurrence return to service inspections also found no faults.
CCTV footage of the occurrences shows that the aerobridge moved diagonally from the home position towards the aircraft at a 2 o’clock angle. The operators did not gain visibility of the aircraft because the cab had been rotated left (away from the aircraft), and because they did not perceive conflicting information, they were unaware of the parallel movement toward the aircraft.
Contributing factor The aerobridge extended diagonally towards the aircraft, in a direction that did not provide visual reference to the aircraft, and the operators were unaware of the diagonal movement, increasing the risk of aircraft collision. |
Operator training and instruction gaps
Operator training material and in-cab instructions contained clear safety messages regarding the operation of aerobridges. The operator training material also included case studies of previous safety occurrences to communicate safety lessons. However, the importance of initial visibility was not highlighted in the safety messages and the case studies did not mention limited visibility operations, particularly due to the parking position of narrow-body aircraft at Gate 82 and some other international gates at Brisbane Airport.
By design, operators could rotate the cab, adjust the height, and move towards the aircraft with simultaneous actions. The operator training material and in-cab instructions provided specific instructions for how to operate the aerobridge to successfully dock with aircraft, however omitted instructions to gain and maintain visibility of the aircraft as a critical first step.
While gaining and maintaining visibility of the aircraft may not be explicitly trained or emphasised via instructions, there was an opportunity for the step to be raised with operators at the time they were assessed. The practical operator competency assessment required operators to ensure aircraft visibility from the home position, before moving the aerobridge.
However, interviews with involved personnel (including Operator 1 and 2) revealed that rotating the cab to ensure visibility was not understood as a critical safety step prior to the occurrences and it was normal to rotate the cab left while moving the aerobridge horizontally and laterally.
Contributing factor The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge. (Safety issue) |
Safety features
The slow down and bumper contact sensors installed on the aerobridge were designed to aid docking and prevent damage to the aircraft when the aerobridge approached the aircraft from a forward direction (normal operations). The sensors would either slow or stop movement. There were no similar sensors installed on the side of aerobridge 82, therefore no sensors activated prior to the collisions when the side of the aerobridge and the corner of the cab approach the aircraft windshields.
Further, no alarms or alerts were presented to the users prior to the collisions, and no side cameras were installed to aid outside visibility of the aircraft blocked by the right side of the cab.
Contributing factor Available safety features did not activate as they were not designed to work when the aerobridge approached the aircraft from the side. |
Emergency stop
An engineer on the ground at the time of the first occurrence detected the abnormal operation of the aerobridge and immediately attempted to alert the aerobridge driver (via hand signals) before activating the ground emergency stop button. Activation of the emergency stop button was a positive action to prevent further damage to the aircraft.
Other finding In the first occurrence a licensed aircraft maintenance engineer activated the aerobridge emergency stop button to prevent further damage to the aircraft. |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the Ground handling events involving Boeing 737-838, VH-VZG, and Boeing 737-8 MAX, DQ-FAE, at Brisbane Airport, Queensland, on 18 June and 26 July 2025.
Contributing factors
- The aerobridge home position and cab orientation, and lack of side-viewing windows, provided limited outside visual reference to narrow‑body aircraft along the docking path, limiting the safe operation of the aerobridge.
- It was common practice for operators to begin the extension of the aerobridge without visual reference to the aircraft, and both operators operated without visual reference prior to the collisions.
- Both operators rotated the aerobridge cab left, the orientation of the cab changed the relative joystick direction creating a complex mental rotation task.
- The aerobridge extended diagonally towards the aircraft, in a direction that did not provide visual reference to the aircraft, and the operators were unaware of the diagonal movement, increasing the risk of aircraft collision.
- The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge. (Safety issue)
- Available safety features did not activate as they were not designed to work when the aerobridge approached the aircraft from the side.
Other findings
- In the first occurrence a licensed aircraft maintenance engineer activated the aerobridge emergency stop button to prevent further damage to the aircraft.
Safety issues and actions
Training gap
Safety issue number: AO-2025-047-SI-01
Safety issue description: The Brisbane Airport Corporation training material and in-cab instructions did not state that operators must gain and maintain visibility of aircraft from the home position, before moving the aerobridge.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Additional safety action taken by Fiji Airways
Fiji Airways temporarily introduced a second operator as a ‘spotter’ at Gate 82 pending the release of this report.
Glossary
| ASIC | Aviation security identify card |
| BAC | Brisbane Airport Corporation |
| BNE | Brisbane |
| CASA | Civil Aviation Safety Authority |
| CCTV | Closed-circuit television |
| LAME | Licensed Aircraft Maintenance Engineer |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Brisbane Airport Corporation
- the aerobridge operators and aerobridge trainer/assessors
- Qantas Airways
- Fiji Airways
- Civil Aviation Safety Authority
- Airport Equipment (New Zealand) Limited
- video footage of the occurrences and other photographs and videos taken on the day of the accident
- recorded data from the aerobridge access security card system.
References
CASA (Civil Aviation Safety Authority), (2023), Part 139 Apron safety management, Advisory Circular AC 139.C-13 v1.0, CASA
European Committee for Standardisation, (2024), Aircraft ground support equipment - Specific requirements - Part 4: Passenger boarding bridges (European standard EN 12312-4:2024). CEN.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Aerobridge operator 1
- Aerobridge operator 2
- Brisbane Airport Corporation
- Qantas Airways
- Fiji Airways
- Civil Aviation Safety Authority
- Airport Equipment (New Zealand) Limited
- National Transport Safety Board.
Submissions were received from:
- Brisbane Airport Corporation
- Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The marshaller’s stop line indicates the designated position where the aircraft’s nose wheel must stop.
[2] The circular cab floor remained stationary unless the bridge was moving horizontally or laterally at the same time (separate operations to cab rotation).
[3] If the operator continued with the cab in the home orientation, with no rotation, and continued to hold the joystick at 3 o’clock, the aerobridge would continue to arc around to the right.
[4] The cognitive ability to rotate 2-dimensional or 3-dimensional mental representations of objects in one’s mind.
[5] Feature multiple and independent walkways, tunnels or arms that connect to an aircraft at different doors simultaneously.
[6] Jetway Systems Apron Drive 2 & 3 tunnel computerized smart bridge manual, June 1994.
[7] Note that the incident described in this report as ‘Occurrence 1’ was originally published as an ATSB Occurrence Brief (AB-2025-025).
Occurrence summary
| Investigation number | AO-2025-047 |
|---|---|
| Occurrence date | 26/07/2025 |
| Location | Brisbane Airport |
| State | Queensland |
| Report release date | 02/04/2026 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation phase | Final report: Dissemination |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Ground handling |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-838 |
| Registration | VH-VZG |
| Serial number | 34201 |
| Aircraft operator | Qantas Airways Limited |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Queenstown International Airport, New Zealand |
| Destination | Brisbane Airport, Queensland |
| Damage | Minor |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-8 MAX |
| Registration | DQ-FAE |
| Serial number | 64309 |
| Aircraft operator | Fiji Airways |
| Sector | Jet |
| Operation type | Part 129 Foreign air transport operators |
| Departure point | Nadi International Airport, Fiji |
| Destination | Brisbane Airport, Queensland |
| Damage | Minor |