
Corporate Plan 2025-26
It is my pleasure to present the Australian Transport Safety Bureau’s corporate plan for the period of 2025‑26 to 2028-29, in which we outline our priorities and key activities to deliver on our purpose. It also sets out the broader environment we operate in, our risks and capabilities, and how we will measure our performance.
Our primary focus is to improve transport safety through the independent investigation of accidents and incidents in aviation, marine and rail. We prioritise investigating accidents or incidents that occur in these modes that are most likely to provide the greatest public benefit.
When determining investigations that will provide the greatest public benefit we consider:
- the safety of passengers and crew on an aircraft, train, or ship
- significant damage to public infrastructure
- impact on the national economy.
We have a small but dedicated workforce with specialist knowledge and skills that allow us to fulfil our role as Australia’s national transport safety investigator. We will continue to invest in the capability of our staff, and improving the systems and technology that support them.
Due to our independence, the ATSB plays a unique role in the transport sector. Through our investigations we can take a holistic view of systems and processes and identify key systemic issues relevant across industries. Our independence from regulators and policy makers means we do not have the power to enforce action. Instead, we influence safety action through:
- our reputation as a world-leading investigative agency
- engaging with our stakeholders
- communicating our findings
- fostering awareness of safety issues and concerns.
Our ability to influence safety action is dependent on our expertise, our relationships with stakeholders, and our effective communication of safety issues and outcomes. As such we will continue to work collaboratively with industry stakeholders and representative bodies to raise awareness and encourage actions that address identified safety issues. Such actions reduce the likelihood of future incidents and accidents. We will also continue to prioritise raising public awareness of our investigations and outcomes to support ongoing confidence in Australia’s transport sector.
Statement of preparation
I, Angus Mitchell, as the accountable authority of the Australian Transport Safety Bureau (ATSB), present the ATSB Corporate Plan 2025-26 for the period 2025-26 to 2028-29, as required under section 35(1)(b) of the Public Governance, Performance and Accountability Act 2013 (PGPA Act).
Angus Mitchell
Chief Commissioner and Chief Executive Officer
Publication details
| Publication type | Corporate Plan |
|---|---|
| Publication mode | Corporate |
| Publication date | 29/08/2025 |
Ground strike involving Air Tractor AT-802, 20 km north-north-east of Thessaloniki Airport Makedonia, Greece, on 30 July 2025
What happened
On 30 July 2025, at 0741 local time, an Australian-registered amphibious Air Tractor AT‑802, configured for firefighting and with 2 crew members on board, departed from Thessaloniki Airport Makedonia, Greece. The aircraft, along with 2 other company aircraft, was headed to a fire located about 40 km north of the airport. At about 20 km south of the fire location, all 3 aircraft commenced water scooping operations at Lake Koroneia.
The amphibious aircraft was designed to scoop water by lowering a retractable intake hole underneath the aircraft while skimming the surface of a body of water at high speed, using the forward motion to force water into the onboard tanks. Prior to scooping operations, pilots will conduct a visual inspection of the proposed scooping area to look for obstacles both on top of and submerged in the water.
The pilot conducted a water inspection and recalled that the water appeared murky and was difficult to see through. During water uplift, the crew of the aircraft reported hearing an impact and immediately initiated a climb to gain height.
The 2 accompanying aircraft flew alongside the Air Tractor to conduct a visual inspection and reported that the right float had dislodged from its mounts. All 3 aircraft made the decision to return to Thessaloniki Airport, with the pilot of the Air Tractor notifying air traffic control and declaring an emergency.
At 0817 the Air Tractor landed on runway 34, however the damaged right float struts were unable to support the weight of the aircraft, and it collapsed onto the right float after landing (Figure 1). The aircraft was subsequently stranded on the runway and emergency services attended. The crew members evacuated the aircraft without injury.
Following the accident, the pilot reported that all 3 aircraft had successfully completed water uplifts from the same location on the previous day. On this occasion, the pilot reported that the glassy water conditions[1] made it difficult to establish the aircraft's height above the water's surface, and the aircraft had hit a submerged object during the scooping run. Due to the risk of unknown hazards at this location, the operator sent a direction to all crew to suspend scooping operations from Lake Koroneia until further notice.
Figure 1: Damaged float struts led to collapse on landing

Source: Operator
Safety message
In murky water, obstructions may not always be visible and the potential for hitting submerged or partly submerged debris is an ever‑present hazard for such operations. Overflying the intended scooping area to scan for such obstacles is always good practice.
In this case, the crew’s quick actions to discontinue operations and pre‑organise emergency services at the airport for their arrival, decreased the risk of injury during their emergency landing.
The hazards that exist in conducting low‑level operations over water have long been recognised (ATSB, 2012) and include the risks of visual illusion and altered depth perception. These factors can make it difficult for pilots to accurately judge the height above water, especially over featureless or reflective surfaces. Flying over calm, glassy water is particularly dangerous, but even choppy water with a constantly varying surface interferes with normal depth perception. Regularly checking the altimeter and establishing smooth descent rates for water alighting during such operations can assist in raising safety margins.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report and allow for greater industry awareness of potential safety issues and possible safety actions.
[1] Glassy water can be present across a broad spectrum, from a mirror-like surface to rippled or wavy water, which reflects a distorted image. The reason it presents a challenge for pilots is that without texture on the surface of the water, it is more difficult to judge height.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2025-036 |
| Occurrence date | 30/07/2025 |
| Location | 20 km north-north-east of Thessaloniki Airport Makedonia |
| State | International |
| Aviation occurrence category | Collision with terrain, Diversion/return, Ground strike, Landing gear/indication |
| Highest injury level | None |
| Brief release date | 29/08/2025 |
Aircraft details
| Manufacturer | Air Tractor Inc |
|---|---|
| Model | AT-802 |
| Sector | Turboprop |
| Operation type | Part 137 Aerial application operations |
| Departure point | Thessaloniki Airport Makedonia, Greece |
| Destination | Thessaloniki Airport Makedonia, Greece |
| Damage | Substantial |
Continued unstable approach into Darwin
A continued unstable approach into Darwin by an Embraer E190 has resulted in Alliance Airlines clarifying its stabilised approach criteria and amending the applicable stabilisation height, an ATSB investigation final report notes.
The aircraft, with 2 flight crew, 2 cabin crew and 49 passengers on board, was approaching Darwin at the conclusion of a scheduled flight from Cairns on 12 February 2025, the report details.
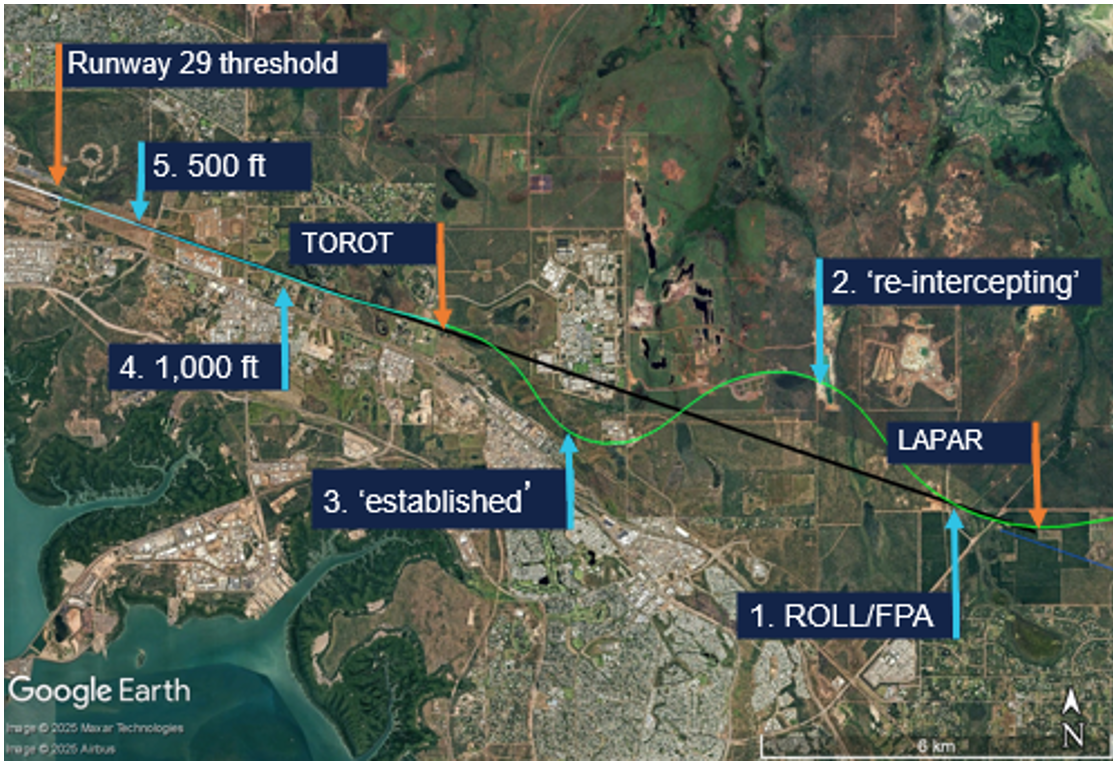
Passing the initial approach fix for the ILS (instrument landing system) approach to runway 29, the aircraft’s auto‑flight system approach mode unexpectedly disarmed and reverted to basic flight director (roll and flight path angle) modes, due either to a system synchronisation issue or the pilot flying inadvertently disarming the approach mode.
“Following this unexpected change, the pilot flying did not re-engage approach mode, or disconnect the autopilot, and the aircraft deviated right and then left of the ILS course, before intercepting the lateral course again at about the final approach fix,” ATSB Director Transport Safety Stuart Macleod said.
The deviation took the aircraft outside the required lateral tolerance of the approach below the minimum safe altitude, while in instrument meteorological conditions.
Additionally, as the aircraft descended through 1,000 ft, it was above the glideslope, at a high rate of descent and a high airspeed.
“The flight crew did not discontinue the approach at this time, because they had become visual, and incorrectly assessed they could therefore continue to 500 ft with multiple stabilised approach criteria unmet,” Mr Macleod said.
As the aircraft continued through 500 ft, the flight crew incorrectly assessed they were now stable, although still too fast. They were also unaware that the pilot monitoring had inadvertently selected an incorrect flap setting.
The pilot monitoring subsequently identified that the flaps were not in the landing configuration and selected the correct position. The flight crew continued the approach and conducted an uneventful landing.
Mr Macleod noted data showing more than 97% of unstable approaches in large air transport operations are continued, and the vast majority result in an uneventful landing.
“This reinforces bad practice, given the highest risk factor for a runway excursion is an unstable approach,” he said.
The ATSB’s investigation identified Alliance’s standard operating procedures were unclear about the criteria for continuing an unstable instrument approach to 500 ft when the aircraft entered visual conditions.
In response, Alliance issued an operations notice intended to improve clarity and compliance with the stabilised approach criteria. As detailed in the notice, Alliance also amended its stabilisation height to 1,000 ft (above aerodrome altitude) for 3‑dimensional and 2‑dimensional instrument approaches and straight‑in visual approaches, and the 500 ft stabilisation height applied only to a visual circuit or circling manoeuvre approaches. The notice also reiterated the operator’s ‘non punitive go‑around policy’, and the requirement for all unstable approaches to be reported.
Mr Macleod said the incident also demonstrated how important continuous attention to automatic flight system modes on the primary flight display is to the maintenance of situation awareness.
“It also illustrates the need for effective flight crew monitoring, which can be improved by standard operating procedures, increased emphasis, and practice,” he concluded.
Read the final report: Unstable approach involving Embraer E190, VH-UYO, near Darwin Airport, Northern Territory, on 12 February 2025
Uncommanded engine acceleration events on single-engine PT6A powered aircraft
Safety Advisory Notice
To operators of single-engine PT6A powered aircraft
Increased awareness and training for pilots in uncommanded engine acceleration events involving PT6A engines will improve outcomes for such malfunctions.
What happened
On 8 January 2024, a Cessna 208B Grand Caravan, departed Lizard Island Airport, Queensland on a flight to Cairns with the pilot and 9 passengers on board. During the climb, the pilot observed the aircraft’s speed and thrust increase uncommanded, and some engine parameters were exceeded or were not indicating. The pilot returned to land but due to the uncontrollable excessive engine power, they conducted a high-speed approach, touched down long on a short runway, overran the end, and the aircraft flipped over. All occupants received minor injuries.
Why did it happen
The ATSB’s examination determined that the uncommanded engine acceleration was very likely associated with an engine fuel control unit (FCU) malfunction. It was identified that there was no documented procedure or troubleshooting information available in the aircraft flight manual and there was limited industry awareness of this type of event and how it should be managed in-flight.
Safety advisory notice
AO-2024-001-SAN-001: In the absence of a flight manual procedure and with limited industry awareness, the ATSB encourages operators of single-engine PT6A powered aircraft to consider potential responses to an uncommanded engine acceleration event for different phases of flight, and to document and train pilots on appropriate actions to ensure operations are performed correctly and consistently.
Awareness and training
Many single-engine PT6A powered aircraft have a procedure for when the engine rolls back to idle power. Some aircraft also have a manual override or emergency power lever to handle this situation and pilots are trained in this. However, there was no such procedure for when the engine accelerated to, or beyond, engine limitations, which occurred more often than any other type of FCU malfunction. Without a formal procedure, pilots are required to exercise judgement based on their experience, skills and knowledge.
ATSB consultation with Cessna Caravan training organisations found that there was limited awareness of such an event. While not as immediately dire as an engine failure or roll back to idle event, an uncommanded engine acceleration is alarming and requires prompt action to control the aircraft and prevent overstress of the engine and airframe. Awareness and training of this type of event will prepare pilots and should result in a better outcome.
Read more about this ATSB investigation: Engine malfunction and runway overrun involving Cessna 208B, VH-NWJ, Lizard Island Airport, Queensland, on 8 January 2024
Publication details
| Investigation number | AO-2024-001 |
|---|---|
| Publication type | Safety Advisory Notice |
| Publication mode | Aviation |
| Publication date | 22/08/2025 |
Aircraft preparation event involving a Van’s RV-8, Halls Creek Airport, Western Australia, on 31 July 2025
Summary video
What happened
On 31 July 2025 at about 1100 local time, the pilot of a Van’s RV‑8 planned a private flight with one passenger on board from Halls Creek to Broome, Western Australia. The passenger also held a pilot’s licence. Prior to departure, the pilot conducted a pre‑flight inspection of the aircraft. Believing that the aircraft was prepared for flight, the pilot proceeded to taxi the aircraft to the runway for take‑off.
During the take-off roll, the pilot did not detect any abnormalities with the airspeed but reported that they were looking outside of the aircraft and not at the airspeed indicator. The aircraft rotated[1] successfully, at which point the pilot then observed airspeed fluctuations, and with no other indications in the cockpit, quickly determined that there was likely a blockage or issue with the pitot tube.[2] The pilot conducted a left turn joining the circuit, returning the aircraft to Halls Creek.
After landing and taxiing back to the runway threshold, the passenger exited the aircraft, conducted a brief external inspection and confirmed that the pitot cover had not been removed prior to take‑off. Once removed, the passenger returned to the aircraft and the pilot recommenced the take‑off roll without further incident.
Safety message
This incident highlights the importance of pre‑flight preparation and planning with a high level of attention required when conducting visual inspections of critical aircraft systems. Pilots must ensure that all pre‑flight checks and procedures are carried out systematically as detailed in the aircraft’s flight manual.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2025-037 |
| Occurrence date | 31/07/2025 |
| Location | Halls Creek Airport |
| State | Western Australia |
| Occurrence class | Incident |
| Aviation occurrence category | Aircraft preparation |
| Highest injury level | None |
| Brief release date | 28/08/2025 |
Aircraft details
| Manufacturer | Van's Aircraft |
|---|---|
| Model | RV-8 |
| Sector | Piston |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Halls Creek Airport, Western Australia |
| Destination | Brome Airport, Western Australia |
| Damage | Nil |