
Final report
Report release date: 30/09/2025
Investigation summary
What happened
On the morning of 12 June 2025, a Virgin Australia Airlines Boeing 737‑800, registered VH‑YIL, operated a passenger transport flight from Brisbane, Queensland, to Sydney, New South Wales.
As the aircraft descended towards Sydney, air traffic control provided clearance for the crew to conduct a visual approach to runway 34 left. During the approach, the speed brake was not armed, and the final flap selection was not completed until 875 ft above the airport elevation (AFE). The operator’s procedures required that both items be completed before the aircraft descend below 1,000 ft above the airport elevation.
As the aircraft later descended through about 500 ft AFE, the captain checked the aircraft configuration and identified that the speed brake was not armed. The captain then armed the speed brake as the aircraft descended below 405 ft AFE. The approach continued and the aircraft landed without further incident.
What the ATSB found
The ATSB found that after air traffic control provided clearance for the crew to conduct a visual approach, a required autopilot altitude selection was not completed. As a result, the aircraft later deviated above the desired approach path.
The crew immediately recognised the deviation and, in response, the captain disengaged the autopilot and auto thrust to manually re‑establish the approach descent profile, without informing the first officer. This led to an unexpected increase in flight crew workload. Then, in attempting to re‑establish the desired approach path, the crew did not fully complete the landing procedures and associated checklist before descending below the stabilisation criteria check altitude. Subsequently, the flight crew did not perform the required missed approach but instead continued the approach and landing.
Safety message
Unstable approaches continue to be a leading contributor to approach and landing accidents and runway excursions. This incident highlights how quickly a small oversight can disrupt an otherwise standard approach. If the disruption leads to a breach of the stabilised approach criteria, early recognition of the situation and prompt execution of a go‑around, rather than continuing the approach, will significantly reduce the risk of approach and landing accidents.
This incident also highlights that when crews are faced with the unexpected, effective crew resource management, with clear communication between the crewmembers, is essential. This ensures effective teamwork when responding to disruptions. Additionally, effective flight crew monitoring in a multi‑crew environment is paramount to aircraft safety. Bringing deviations to the attention of the pilot flying ensures that the aircraft remains on a safe flight path and is correctly configured for the relevant phase of flight.
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the morning of 12 June 2025, a Virgin Australia Airlines Boeing 737-800, registered VH‑YIL, operated a passenger transport flight from Brisbane, Queensland, to Sydney, New South Wales.
As the aircraft descended towards Sydney in day visual meteorological conditions and with the autopilot engaged, air traffic control provided clearance for the crew to conduct a visual approach to runway 34 left. At that time, an altitude of 2,000 ft was set in the altitude window of the autopilot mode control panel (MCP). After receiving clearance for a visual approach, operational procedures required that the pilot flying[1] select an altitude equivalent to 500 ft above the airfield elevation (in this case 500 ft, as the airport was close to sea level) in the MCP altitude window (see the section titled Approach procedures). However, the captain, acting as pilot flying, inadvertently did not make this selection and the first officer, acting as pilot monitoring, did not identify that this altitude selection had not been completed.
As the aircraft descended toward 2,000 ft above mean sea level (AMSL) (Figure 1), the aircraft intercepted the final approach track. The crew expected the descent to continue, but the aircraft began automatically levelling off to capture the 2,000 ft altitude set in the MCP altitude window, taking the aircraft above the desired approach descent profile.
The crew immediately recognised the deviation and identified that the incorrect altitude was entered into the MCP altitude window; to continue the descent, but without verbalising the action, the captain entered 500 ft in the altitude window. Shortly after, the captain recognised that this selection would not re‑establish the required approach path, so, without first alerting the first officer to their intentions, disengaged the autopilot and auto thrust to manually re‑establish the approach descent profile.
Figure 1: Overview of the approach
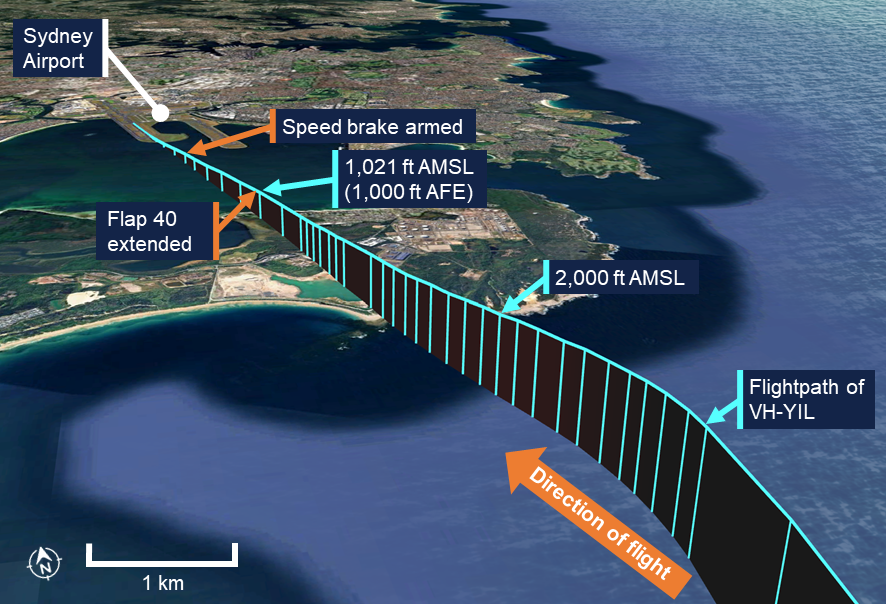
Source: Google Earth, recorded flight data and ATSB
As the crew worked to re-establish the desired approach path while completing the pre‑landing procedures, the speed brake was unintentionally not armed, and the final flap selection (flap 40) was not made until 939 ft above the airport elevation. These items, and the associated landing checklist, were required to be completed before the aircraft passed 1,000 ft as set out in the operator’s procedures (see the section titled Stabilised approach).
The captain did not recognise that the checklist was not complete and believed that the stabilised approach criteria had been met. The first officer, acting as pilot monitoring, did not identify that the speed brake was not armed, but did identify that the required final flap selection and the landing checklist had not been completed in time. However, the first officer noted that the approach path, speed and descent rate were within the criteria and announced that the approach was stable.
As the aircraft descended through about 500 ft AMSL, the captain checked the aircraft configuration and identified that the speed brake was not armed. The captain then armed the speed brake as the aircraft descended below 426 ft AMSL (405 ft above the airport elevation). The approach continued without further incident and the aircraft landed at 0905 local time.
After landing, the captain discussed the incident with the first officer and assessed that a missed approach should have been conducted.
Context
Pilot details
The captain held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The captain had 14,975 hours of flying experience, of which 10,081 hours were on the Boeing 737 aircraft type, with 127 hours accrued in the previous 90 days.
The captain held additional non‑flying duties in the organisation with 50% of their time spent in normal flying duties. The captain also stated that in their experience of regular flying operations, visual approach clearances were unusual.
The first officer held an air transport pilot licence (aeroplane) and class 1 aviation medical certificate. The first officer had about 28,000 hours of flying experience, of which about 14,000 hours were on the Boeing 737 aircraft type, with 117 hours accrued in the previous 90 days.
The ATSB found no indicators that the flight crew were experiencing a level of fatigue known to adversely affect performance.
Approach procedures
Visual approach
The operator’s flight crew operations manual (FCOM) for the Boeing 737‑800 aircraft included the following visual approach procedure:
When cleared for a visual approach, the MCP altitude should be selected to 500 ft above field elevation, however this does not preclude setting an intermediate level‑off altitude if desired.
Stabilised approach
The operator’s policy and procedure manual provided the following stabilised approach policy that included:
All approaches must be stabilised by 1000 ft above field elevation.
An approach is stabilised when the following criteria are met:
- Briefings and normal checklists are completed
- Aircraft is in the correct landing configuration
- Aircraft is on the correct lateral and vertical flight path
- Sink rate, no greater than 1,000 feet per minute.
The policy also noted that if the stabilisation criteria were exceeded for other than momentary periods at any time below the stabilisation height, the pilot monitoring must call "NOT STABLE”, and the pilot flying must initiate a missed approach.
The FCOM also stated that a missed approach shall be executed whenever required visual reference is not obtained or maintained or when an approach is not stabilised at 1000 ft above the airport elevation.
Meteorology
The approach was conducted in visual meteorological conditions.
At 0900, 3 minutes before the incident, the Bureau of Meteorology automatic weather station at Sydney Airport recorded the temperature as 12°C and the wind as 13 kt from 247° magnetic. Cloud cover was recorded as few[2] at 3,521 ft above mean sea level (AMSL). Visibility was recorded as greater than 10 km with no recorded precipitation.
Recorded data
Virgin Australia provided the ATSB with the aircraft’s quick access recorder data which captured the incident approach.
The recorded data (Figure 2) showed that the landing flap selection (flap 40) was completed 3 seconds after the aircraft descended below 1,000 ft above the airport elevation (AFE), at 939 ft AFE (960 ft AMSL). The flaps then completed moving to that extension as the aircraft descended below 875 ft AFE (896 ft AMSL). The speed brake lever was moved to the armed position as the aircraft descended below 405 ft AFE (426 ft AMSL).
Figure 2: Graphical representation of the recorded quick access data
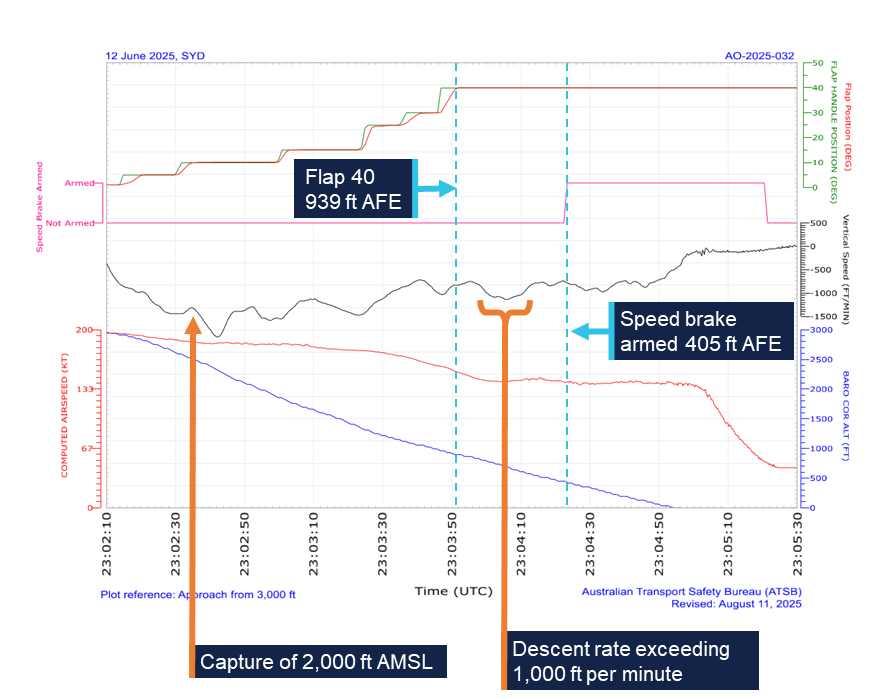
All times are coordinated universal time (UTC). Local time was Australian Eastern Standard Time (EST), which was UTC +10 hours. Source: Quick access recorder from VH-YIL, annotated by the ATSB
After descending below 1,000 ft, the aircraft maintained an appropriate speed and flightpath. The rate of descent exceeded the 1,000 ft per minute stabilised approach criteria limit for a 9 second period between 0904:02 and 0904:11. During this period, the aircraft descended from 747 ft AFE to 587 ft AFE, and the maximum recorded descent rate was 1,136 ft per minute at 0904:07.
Safety analysis
As the aircraft descended towards Sydney, the crew were provided with a visual approach clearance which the captain reported was unusual. After receiving the clearance, the captain unintentionally did not make the required 500 ft selection in the altitude window of the mode control panel. The first officer, as the pilot monitoring, did not identify that this omission had occurred. Consequently, as the aircraft descended to 2,000 ft the autopilot began to level off rather than continuing the descent to 500 ft, which took the aircraft above the desired descent profile. The captain responded with an unplanned manual intervention without alerting the first officer to their intention while the flight crew were also attempting to complete the final landing procedures. This led to an unexpected increase in flight crew workload and reduced the first officer’s situation awareness.
Workload has been defined as ‘reflecting the interaction between a specific individual and the demands imposed by a particular task. Workload represents the cost incurred by the human operator in achieving a particular level of performance’ (Orlady and Orlady, 1999). A discussion of the effect of workload on the completion of a task requires an understanding of an individual’s strategies for managing tasks.
An individual has a finite set of mental resources they can assign to a set of tasks (for example, performing an approach and landing). These resources can change given the individual’s experience and training and the level of stress being experienced at the time. An individual will seek to perform at an optimum workload by balancing the demands of their tasks. When workload is low, the individual will seek to take on tasks. When workload becomes excessive the individual must, as a result of their finite mental resources, shed tasks.
An individual can shed tasks in an efficient manner by eliminating performance on low priority tasks. Alternatively, they can shed tasks in an inefficient fashion by abandoning tasks that should be performed. Tasks make demands on an individual’s resources through the mental and physical requirements of the task, temporal demands and the wish to achieve performance goals (Hart and Staveland, 1988, and Lee and Liu, 2003).
In this case, likely in response to increased workload and the absence of crew coordination, they missed required checklist items (the final flap and speed brake selections). The stabilised approach criteria required that the aircraft be in the final landing configuration by 1,000 ft above the airport elevation. The landing flap selection was made 3 seconds after descending below this height, although the captain believed that the flap selection had been made in time to meet the stabilised approach criteria requirements. However, the flaps did not reach the required position until the aircraft descended through 875 ft above the airport elevation.
The first officer identified that the flap selection was made late and that, therefore, the stabilised approach criteria had not been met. However, as the descent rate, speed and profile were within the criteria, they announced that the approach was ‘stable’ instead of making the required ‘not stable’ announcement. Consequently, the required missed approach was not commenced, and the approach was continued. The first officer did not identify that the speed brake landing procedure action was not completed.
As the approach continued, the descent rate exceeded the stabilised approach criteria for a period of 9 seconds. This exceedance was momentary and not excessive and therefore it did not require the commencement of a missed approach.
When the unarmed speed brake was later identified by the captain, this should have acted as a further trigger for the commencement of a missed approach. Instead, this missed action was quickly rectified by the captain and the approach continued.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the unstable approach involving Boeing 737, VH-YIL, near Sydney Airport, New South Wales, on 12 June 2025.
Contributing factors
- After air traffic control provided clearance for the crew to conduct a visual approach, a required autopilot altitude selection was not completed. As a result, the aircraft later deviated above the desired approach path.
- While re-establishing the approach path, the crew did not complete required landing procedures until after the aircraft descended below the stabilisation criteria check altitude. Subsequently the flight crew did not perform the required missed approach, instead continuing the approach and landing.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Airservices Australia
- Bureau of Meteorology
- recorded data from the quick access recorder from VH-YIL
- the flight crew
- Virgin Australia Airlines.
References
Orlady, HW & Orlady, LM 1999, Human factors in multi-crew flight operations. Ashgate, Aldershot, p. 203.
Hart, SG & Staveland, LE 1988, ‘Development of NASA-TLX (Task Load Index): Results of empirical and theoretical research’, In PA Hancock & N Meshkati (Eds.), Human Mental Workload. North Holland Press, Amsterdam.
Lee, YH & Liu, BS 2003, ‘Inflight workload assessment: Comparison of subjective and physiological measurements’, Aviation, Space, and Environmental Medicine, vol.74, pp. 1078- 1084.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Civil Aviation Safety Authority
- the flight crew
- Virgin Australia Airlines.
No submissions were received.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky was covered.
Occurrence summary
| Investigation number | AO-2025-032 |
|---|---|
| Occurrence date | 12/06/2025 |
| Location | Sydney Airport |
| State | New South Wales |
| Report release date | 30/09/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Aircraft preparation, Unstable approach |
| Occurrence class | Incident |
| Highest injury level | None |
Aircraft details
| Manufacturer | The Boeing Company |
|---|---|
| Model | 737-8FE |
| Registration | VH-YIL |
| Serial number | 38713 |
| Aircraft operator | Virgin Australia Airlines Pty Ltd |
| Sector | Jet |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Brisbane Airport, Queensland |
| Destination | Sydney Airport, New South Wales |
| Damage | Nil |