The pilot of a Cessna 150 light aircraft which collided with terrain near Ogilvie, in mid-west WA, likely experienced an incapacitating medical event prior to the aircraft entering a spiral dive, an ATSB investigation has determined.
On 21 March 2025, the single-engine Cessna 150M collided with terrain next to Ogilvie Road, about 84 km north-west of Geraldton. The pilot, the aircraft’s sole occupant, was fatally injured.
The aircraft had earlier taken off from Geraldton Airport for a planned ferry flight to Shark Bay.
There was no available radar or ADS-B recording of the flight, but the ATSB was able to recover data from a damaged Garmin 296 GPS which was fitted to the aircraft.
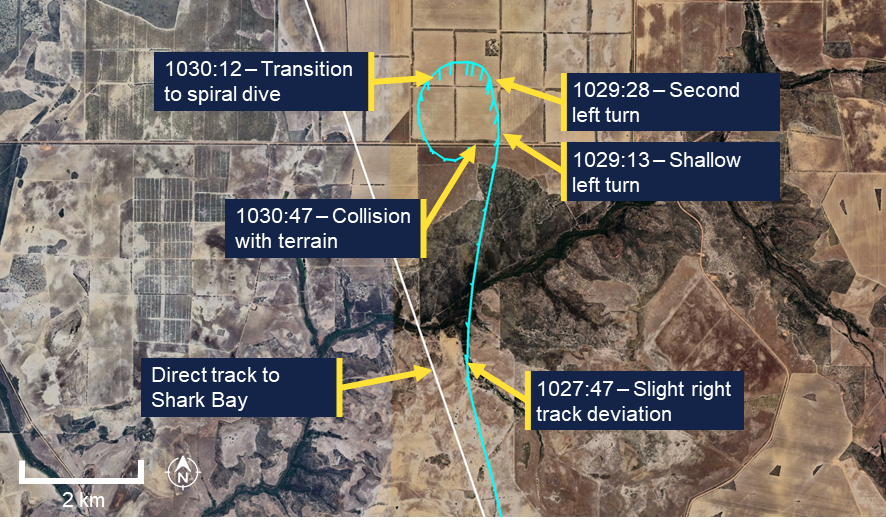
That data indicated that about 30 minutes into the flight the aircraft had briefly deviated right of its track, then entered a shallow left turn which transitioned into a spiral dive, before the collision with terrain about three minutes after the initial deviation.
“Wreckage examination found no evidence of any in-flight failure of the airframe or flight controls, and the engine was producing power throughout the descent,” ATSB Chief Commissioner Angus Mitchell said.
The ATSB’s final report notes the pilot was acutely unwell in the days preceding the accident, and was very likely still symptomatic during the flight.
“Based on the pilot’s significant aviation experience and medical history, and the established sequence of events, it was determined the pilot likely experienced an incapacitating medical event resulting in a deviation off track and the uncorrected spiral dive,” Mr Mitchell said.
The ATSB consulted with an independent medical professional and the Civil Aviation Safety Authority, as well as the pilot’s general practitioner, next of kin, and designated aviation medical practitioner (DAME), to consider possible medical events which could have incapacitated the pilot, including cardiovascular conditions and acute gastroenteritis.
“While it is very likely the pilot experienced an incapacitation event, the evidence available did not allow the exact nature of the incapacitation to be determined,” Mr Mitchell said.
The investigation’s final report advises pilots to ensure they conduct the ‘IMSAFE’ checklist prior to every flight.
The checklist, created by the US Federal Aviation Administration, prompts pilots to consider whether factors such as illness, medication, stress, alcohol, fatigue or emotion could affect their performance and compromise flight safety.
“Pilots are encouraged to integrate this checklist into their pre-flight routine, no matter how routine the flight,” Mr Mitchell said.
“Prioritising personal fitness for flight duty helps reduce risk, not only for the pilot, but for passengers, crew and the public.”
UPDATED 10AM 13 OCTOBER: The ATSB is conducting a transport safety investigation into an accident involving a Piper Cherokee Lance aircraft at Shellharbour Airport on Saturday morning.
The aircraft was departing from runway 26 when soon after take-off flight tracking data shows it deviating to the left and impacting the end of the intersecting runway. Despite a timely response from first responders the aircraft was consumed by a post-impact fire and the three occupants were fatally injured.
The ATSB deployed a team of 4 transport safety investigators from its Canberra and Melbourne offices, specialising in aircraft operations, maintenance and engineering, to the accident site.
Arriving on site on late Saturday afternoon, investigators undertook an initial site assessment.
Returning to the site on Sunday morning they began conducting a range of evidence-gathering activities, with their initial focus on surveying the accident site including mapping with a drone, and documenting witness marks and the location and condition of the aircraft wreckage before allowing the wreckage to be removed from the runway so that it could reopen later on Sunday.
Further examination of the wreckage is taking place in the hangar as investigators seek to establish any evidence of pre‑existing aircraft faults, continuity of flight controls and engine issues.
Investigators have also begun interviewing involved parties and witnesses, and are collecting relevant recorded information including flight tracking data, airport radio calls and CCTV footage, as well as pilot and aircraft maintenance records, and weather information.
The ATSB anticipates releasing a preliminary report detailing factual information established in the investigation’s evidence-gathering phase in about two months.
A final report, detailing findings and the analysis to support those findings, will be published at the conclusion of the investigation.
However, should a critical safety issue be identified at any stage during the investigation, the ATSB will immediately notify relevant parties so safety action can be taken.
On 8 October 2025 at about 0719 local time, a Robinson R44 Raven I helicopter, registered VH-XSO and operated by GBR Helicopters, departed Thursday Island, Queensland, with 2 passengers on board to conduct work related to their employment on Coconut Island (Poruma), 55 NM (102 km) north-east of Horn Island.
While en route at about 600 ft above sea level, the low rotor RPM horn sounded, and the pilot reacted by immediately lowering the collective lever and entered autorotation. The pilot suspected a total engine power loss and transmitted a MAYDAY call, deployed the emergency pop-out floats and instructed the passengers to brace.
The helicopter landed on the water and immediately began to roll onto its left side as the left side float detached from the helicopter’s skid tube. The pilot instructed the passengers to evacuate, with the rear seat passenger and pilot egressing on the right side and the front left passenger egressing from their left door, under water.
The 3 occupants were able to inflate their lifejackets and climb on board the partially submerged helicopter.
An emergency locator transmitter activation was received by the Joint Rescue Coordination Centre who initiated a rescue. The pilot’s MAYDAY call was also heard by the pilot of another helicopter in the area that diverted to the accident location and provided updated information on the welfare of the occupants.
The rescue helicopter arrived about 50 minutes after the ditching and winched the 3 people on board before transferring them to Thursday Island Hospital. During the winching operation, one of the people being rescued impacted the submerged wreckage, fracturing a rib.
The pilot and passengers received serious injuries from chemical burns from exposure to aviation gasoline in the water while waiting to be rescued. Subsequently, the helicopter sank and was not able to be located or recovered.
What the ATSB found
During the cruise at about 600 ft while operating over the ocean, the helicopter engine had a total power loss, forcing the pilot to conduct a forced landing onto the ocean surface.
The pilot transmitted an effective MAYDAY call, activated the pop-out floats and instructed the passengers to brace prior to ditching. This improved the occupants' survivability during and after the ditching. Further, the operator’s use of constant wear lifejackets likely increased the ease and speed of use by the occupants (compared to pouch-worn lifejackets), enhancing their survivability post-accident.
Although the passengers flew regularly as part of their employment, on this occasion the pilot did not provide the passengers with information on the appropriate brace position during the pre-flight safety briefing. Subsequently, when the pilot instructed them to brace for impact, both passengers adopted inappropriate brace positions that increased the risk of injury.
During the ditching, the left pop-out float detached causing the helicopter to roll in the water. This reduced the likelihood of timely emergency egress and exposed the occupants to fuel in the water that resulted in chemical burns.
GBR Helicopters did not provide company pilots with a survival emergency locator transmitter for all overwater flights. Although it did not influence the outcome on this occasion, it had the potential to reduce the post‑impact survivability of a ditching event by relying on the onboard automatic emergency locator transmitter.
Queensland Department of Education employees who regularly flew over water in helicopters as passengers were not provided with helicopter underwater escape training (HUET) which increased the risk of drowning in the event of a ditching.
One of the occupants of the ditched helicopter likely sustained an additional serious injury after impacting the wreckage while being winched during their rescue.
Safety message
Passengers, who regularly fly in helicopters for their employment, are not always provided with aviation‑specific training including helicopter underwater escape training (HUET).
Research has shown that disorientation, entanglement with debris, unfamiliarity with seat belt release mechanisms and difficulty locating or opening exits, are commonly cited as hazards when attempting to escape from a helicopter following an in-water accident. HUET provides participants with familiarity with the crash environment and improves occupant confidence in their ability to manage an in-water emergency egress situation. Individuals and organisations whose employees regularly travel in helicopters over water are encouraged to consider the potential life-saving benefits of HUET for their employees in otherwise survivable helicopter accidents.
The accident highlighted the importance of an effective MAYDAY transmission. With limited time before landing on the water, the pilot’s broadcast alerted other aircraft to their identity and approximate location, resulting in another helicopter arriving at the accident site about 11 minutes after the ditching. Situations requiring a MAYDAY call are often intense and time‑limited, and calculation of an accurate position may not always be possible. The ATSB reminds pilots that, as in this situation, an accurate location, transmitted effectively during an emergency, will likely reduce response time during a rescue and increase the survivability of occupants.
Summary video
The occurrence
Departure and cruise
On the 8 October 2025, at about 0705 local time, the pilot of a Robinson R44 Raven I helicopter, registered VH-XSO, operated by GBR Helicopters Pty Ltd, ferried the helicopter from Horn Island Airport, Queensland, to Sadie’s Helipad on the south-eastern side of Thursday Island, Queensland, about 4 NM north-west of Horn Island Airport.
On arrival at Sadie’s Helipad the pilot shut down the helicopter and commenced a safety briefing for 2 passengers employed by the Queensland Department of Education. Both passengers were familiar with the R44 helicopter, having flown in the model numerous times as part of their employment. The pilot assisted the passengers to board the helicopter, seating one passenger in the rear right seat, behind the pilot and the other in the front left seat.
The non-scheduled air transport passenger flight was planned from Thursday Island (Figure 1) direct to Coconut Island (Poruma), about 55 NM (102 km) north-east of Horn Island Airport, where the passengers were to conduct duties related to their employment before the flight continued to Warraber Island and then return to Thursday Island.
At 0719, the helicopter became airborne from Sadie’s Helipad and climbed to an altitude of about 600 ft above sea level. Once they had passed over Wednesday Island, the pilot recalled they conducted a ‘CLEAR-OFF’1 check to assess the helicopter’s performance and position, the check indicated the helicopter was operating normally and on track for its destination.
Figure 1: VH-XSO flight track
Source: Google Earth, annotated by the ATSB
Ditching
After the completion of the check, the pilot considered that they had reached a sufficient distance that would no longer impede traffic approaching to land at Horn Island Airport and they planned to commence a further climb. The pilot reported at this time the low rotor RPM horn activated. They rapidly lowered the collective2 to preserve the rotor RPM and entered autorotation.3 They then observed the engine RPM reducing through about 50% before the engine then completely stopped.
Preparing for a ditching,4 the pilot broadcast a MAYDAY5 call on the local common traffic advisory frequency (CTAF). The transmission included the helicopter’s position relative to Horn Island and that they were ditching into the ocean. The pilot inflated the emergency pop-out floats and instructed the passengers to brace. Prior to contact with the water, the pilot adjusted the helicopter’s heading to the right to align the helicopter more into wind.
Recorded data showed that at 0730:15, the helicopter’s altitude was at sea level. The pilot described the contact with the water as ‘upright’ between an airspeed of 5–10 kt. One passenger described the landing as ‘pretty hard’ and that the water covered the windscreen on impact. The pilot then instructed both passengers to evacuate and recalled that the helicopter rolled immediately on its left side. The pilot and rear right passenger were able to egress via their doors to the right side of the helicopter, which was not submerged, and inflated their lifejackets. The front left passenger, positioned on the lower side (left side) of the rolled helicopter egressed using their low side (left) door, reporting that they struggled to open the door due to the pressure of the water. Once the door was opened, the passenger exited and surfaced near the main rotor blades. While attempting to return to the cabin, they struck their head twice on the helicopter’s main rotor blade. They reported feeling heavy in the water and had difficulty maintaining buoyancy until the other passenger instructed them to inflate their lifejacket.
All the occupants were subsequently able to climb onto the partially submerged helicopter (Figure 2). The pilot observed that the left float, still inflated, had detached from the skid tube and had become entangled around the helicopter’s rotor hub.
Figure 2: VH-XSO shortly after ditching
Source: GBR Helicopters, annotated by the ATSB
Unsure if other aircraft had heard the pilot’s MAYDAY transmission, the occupants attempted to call for help using their phones, however due to water ingress were unable to place any calls. Assisted by the passengers, the pilot entered into the submerged cabin of the helicopter to ensure the emergency locator transmitter (ELT) had been activated. They entered the cabin a second time, shortly after, to retrieve the helicopter’s survival kit and satellite phone. The satellite phone, which had also been submerged, did not work.
All 3 occupants later reported that after a period of time on the submerged helicopter, they noticed a burning sensation, mostly on their legs as they were submerged and presumed this was from fuel in the water. The occupants were individually swept off the helicopter on several occasions as a result of the sea state6 conditions and were assisted by the others to climb back onto the helicopter.
Rescue
The Joint Rescue Coordination Centre (JRCC) received an ELT activation detection in the Torres Strait at 0731.
The pilot of a second R44, operated by another helicopter company based in the Torres Strait, heard a broken transmission of the pilot’s MAYDAY call including the registration and that they were ditching. The second pilot was able to contact the operator of VH‑XSO’s base manager who advised the last known position of the aircraft using company aircraft tracking software. The airborne R44 pilot was then able to track to the location, alerting other airborne fixed wing traffic, who also diverted to the location. About 11 minutes after the ditching, the R44 pilot located the ditched helicopter and relayed, via a fixed wing aircraft that also began orbiting above the site, the ditching location and state of the occupants to Brisbane Centre air traffic control. The helicopter pilot flew above VH-XSO to ensure the occupants were not separated from the ditched helicopter until remaining fuel required them to continue their flight to Horn Island. A company helicopter arrived at the location shortly after and continued monitoring the occupants in the water.
The Horn Island rescue helicopter crew, operating a Leonardo Helicopters AW139, received notification of the task at 0741 and after a reconfiguration for water winching, started engines at 0758 and were airborne at 0804. On board were the aircraft captain, air crew officer (winch operator) and rescue crew officer. The rescue helicopter arrived at the location of the ditched helicopter at 0819, about 50 minutes after the ditching.
A rescue crew officer descended into the water via the winch about 20 m from the wreckage to reduce the effects of the rescue helicopter’s downwash. They approached the wreckage toward the tail of the helicopter and recalled being about 2–5 m from the wreckage when, due to debris and the potential to snag the winch cable on the wreckage, they requested the 3 people to be rescued to enter the water. The rescue crew officer individually winched each person using a rescue strop7 and accompanied each person during the winch.
One rescued person later recalled that once in the winch rescue strop, as the winch cable tightened, they were immersed underwater and impacted the tail of the partially submerged wreckage on the right side of their chest. Neither the rescue crew officer who accompanied the person on the winch, nor the aircrew officer operating the winch, observed the impact with the wreckage nor did the person advise the crew of the impact following the winching.
Once all 3 people had been winched from the water, the rescue helicopter tracked to Thursday Island Hospital and arrived there at 0841. The rescue crew officer recalled during the flight, the survivors advised they were suffering from a burning sensation on their legs and they assisted to rinse the affected areas with water.
Injuries and damage
Medical records indicated all 3 occupants of the ditched helicopter received chemical burns due to their exposure to aviation gasoline. Two of the occupants suffered chemical burns to 14% of their total body surface area (TBSA) while the third suffered burns to 21% of their TBSA. One occupant also suffered a minor head injury, likely from impact with the wreckage following their egress.
The third occupant also received a fracture to a right-side rib. This was reported to medical staff and the ATSB as being a result of the rescue operation where after being attached to the rescue strop, they impacted the tail of the partially submerged wreckage.
Occupants were treated for chemical burns and kept under observation for about 6 hours at Thursday Island Hospital before being discharged later the same day.
In addition to the occupants of the ditched helicopter, the rescue crew officer was kept under observation at the hospital for chemical burns, however reported they were uninjured and also released the same day.
VH-XSO was later reported to have sunk and was not able to be located or recovered.
Context
Personnel information
Pilot experience
The pilot held a commercial helicopter pilot’s licence issued on 22 April 2025 and a current low-level rating valid until 30 March 2027. They had accumulated about 210 hours total time flying helicopters.
They also held an unrestricted Class 1 aviation medical that was valid until 1 November 2026.
Training
The pilot had last completed an operator proficiency check on 20 June 2025 which included emergency autorotations and they were deemed competent by the operator.
The pilot had completed helicopter underwater escape training (HUET) and survival on 20 July 2023 that was valid for 3 years. The pilot later stated that they felt their HUET training was ‘instrumental’ in their efficient egress from the helicopter.
Fatigue
The pilot recalled they had slept well and felt rested and that the early flight did not require a change to their usual sleep pattern. They were rostered the day prior to the occurrence for an 8‑hour duty period, however were not required to fly and had last flown 5 days earlier on 3 October 2025.
The ATSB considered that it was unlikely that fatigue affected the pilot’s performance on the day of the occurrence.
Aircraft information
General information
The Robinson Helicopter Company R44, Raven I is a 4‑place, light helicopter, powered by a Lycoming O-540-F1B5, 6-cylinder, horizontally-opposed piston engine. It has a 2‑bladed main rotor system and a conventional 2‑bladed tail rotor.
The manufacturer advised that the most recent calculation for R44 helicopter engine power loss events indicated a failure rate of 0.37 events per 100,000 flight hours.
VH-XSO was manufactured in the United States as serial number 0817 in 2000 and had flown a total of 3,253.7 hours prior to the occurrence flight. Nautilus Aviation had been the registration holder since January 2024 and cross-hired the helicopter to GBR Helicopters.
Emergency pop-out floats
VH-XSO was fitted with emergency pop-out floats (Robinson Helicopter Company part number C-950). The pilot operating handbook (POH) pop-out float supplement stated that they were ‘intended for safety during overwater flight’ and that the ‘pop-out floats were not certified for ditching’. The supplement did however provide a procedure for practise autorotations onto water, directing pilots to conduct autorotations as per the basic manual with the addition of ensuring a slight nose high attitude.
Following inflation, the POH supplement indicated the emergency pop-out floats would remain inflated for at least one hour and typically maintained shape for several hours.
The R44 type certificate data sheet (H11NM) provided the certification basis for the helicopter and included certification of ‘emergency pop-out floats’ under US Federal Aviation Administration (FAA) Title 14 Code of Federal Regulations (CFR) Part 27. The emergency pop-out floats were certified under Part 27.521 - float landing conditions.
CASR Part 133 Manual of Standards Division 12, section 11.51 stated:
(2) Subject to subsection (3), the rotorcraft must be fitted with emergency flotation equipment if one or more of the following applies to the flight:
(a) the flight:
(i) is to, or from, a helideck on a vessel or other offshore facility; and
(ii) will have an approach and landing or baulked landing stage, or a take‑off and initial climb stage, over water;
(b) the rotorcraft will be flown further over water from land than the distance in which, with 1 engine inoperative, the rotorcraft could reach a suitable forced landing area, for the flight, on land.
(3) Despite paragraph (2)(b), the flight over water is permitted without having to fit emergency flotation equipment if:
(a) it is in a rotorcraft access lane mentioned in the AIP; or
(b) both:
(i) it is to comply with an ATC instruction; and
(ii) it is for no longer than 2 minutes at normal cruising speed in still air.
The R44’s pop-out floats are bolted to the helicopter skid tubes and featured 6 individual chambers per float, the R44 POH described the system:
The pop-out float system consists of inflatable floats stowed in protective covers along the skid tubes, a pressure cylinder located in the compartment under the left front seat, flexible hoses from the cylinder to the floats, an inflation lever located on the pilot’s collective, and an additional stabilizer installed at the base of the lower vertical stabilizer.
The cylinder was filled with helium, with the required operating pressure indicated on a placard on the cylinder and actual pressure was displayed on a gauge at the top of the cylinder.
Squeezing the inflation lever (required about 9 kg of force) caused a spring-loaded pin to puncture a metal sealing disk and allowed the helium to fill the floats.
The POH provided a caution to pilots:
Do not inflate floats above 80 KIAS [knots indicated airspeed]. Do not exceed 80 KIAS with floats inflated.
During the autorotation the pilot reported they reduced the helicopter’s airspeed below the 80 kt limit and then inflated the floats. The pilot also suspected that the left float may have detached or partially detached while the helicopter was descending as they recalled hearing a flapping noise from the left side of the helicopter. However, the R44 POH also contained a note to state:
Some flapping of float covers during flight with floats inflated is normal……
Images of the helicopter in the water showed the left float completely detached from the skid tube and caught on the hub of the main rotor (Figure 3) which prevented the helicopter rolling fully inverted.
Figure 3: VH-XSO ditched
Source: GBR Helicopters, annotated by the ATSB
The manufacturer advised that the floats may be susceptible to damage if:
deployed above the 80 kt airspeed limit
there is a higher than normal vertical impact
there is high forward airspeed
allowing the nose to drop when contacting the water, which could cause the float to separate from the skid and may start as a partial separation before fully detaching.
The manufacturer conducted tests using a 1/7 scale model of the Robinson R66 model equipped with identical floats as used on the R44. These tests were conducted in conditions that simulated uniform waves per the sea state 48 definition and demonstrated that the R66 would remain upright.
Robinson Helicopter Company advised that additional unofficial testing of the R66 in irregular wave conditions peaking at sea state 4 levels, also demonstrated it would remain upright. Although model testing was limited to the R66 configuration, the manufacturer advised that the results extended to the R44 6‑chamber floats by analysis to substantiate European Union Aviation Safety Agency (EASA) requirements for overwater commercial operations. The R44 emergency pop-out float supplement contained a limitation saying the following for normal operations on water:
Safe operation on water has been demonstrated in waves up to 1 foot (0.3 M) (trough to crest) Maximum recommended water taxi speed is 5 kt. Some application of collective is required.
However, the R44 POH did not contain any limitations on the maximum sea state stability of the helicopter to remain upright.
Recent maintenance
The operator advised that prior to the ditching, recent maintenance was completed on VH-XSO following identification of an unserviceable main rotor gearbox pinion and swashplate,9 which was found to be ‘noisy, rough and rusty’. The operator replaced the main rotor gearbox assembly and swashplate. At the completion of the maintenance on 24 September 2025, 2 maintenance test flights were conducted that totalled about 36 minutes and the aircraft was then released into service.
After release to service, a company pilot further reported that the left skid tube on VH‑XSO was cracked. The skid was replaced with one from another R44 helicopter undergoing maintenance at the time. This included the removal of the left side emergency pop-out floats and reattachment to the replacement skid tube, which was completed on 30 September 2025.
VH-XSO then operated on 1 and 2 October 2025 which totalled 4.8 hours of flying over the 2 days and was not flown again prior to the occurrence flight on 8 October.
As VH-XSO sank and was not recovered, the ATSB was unable to determine if recent maintenance may have contributed to either the total loss of power or the left emergency pop-out float separation from the skid tubes.
Fuel
The pilot stated that they departed Horn Island with about 150 L of fuel on board. The R44 helicopter uses about 60 L per hour during normal flying operations and had flown for about 12 minutes before the low rotor RPM warning, including the ferry flight to Thursday Island.
As a result of the helicopter rolling 90° on its left side and the swell of the ocean causing movement, it was likely that this caused fuel to leak from a vent located in the R44’s mast fairing.
Due to the presence of fuel in the ocean following the ditching, the ATSB concluded it was unlikely that fuel exhaustion was a factor.
Carburettor heat
The R44 Raven I is equipped with a carburettor that delivers a fuel air mixture to the engine. A gauge in the helicopter’s cockpit displays the air temperature inside the carburettor and features a yellow caution arc between −17°C and 3°C.
Pressure drops and fuel evaporation inside the carburetor cause significant cooling. Therefore, carburetor ice can occur at OATs [outside air temperatures] as high as 30˚C. Even in generally dry air, local conditions such as a nearby body of water can be conducive to carburetor ice and apply carb heat as required.
The pilot reported that they observed low cloud during the flight and that they had mostly flown fuel‑injected variants of the R44 previously, so were particularly conscious to regularly check the carburettor temperature gauge in VH-XSO. The pilot recalled the carburettor temperature was about 10° before they applied about half carburettor heat early in the flight, while abeam Horn Island, to increase the temperature and reduce the possibility of carburettor ice build-up.
Meteorological information
One minute recorded meteorological data from Thursday Island indicated that the outside air temperature had been a consistent 28°C from 0700 local time with a mean sea level pressure of 1010 hectopascals. One minute meteorological data from Horn Island Airport, about 13 NM (24 km) south-west of the accident location, from 0700 until the time of the occurrence showed wind strengths of 10–19 kt from a consistent east‑south‑east direction.
The ATSB was unable to obtain data from a nearby Queensland Government wave measuring device, however the European Centre for Medium-Range Weather Forecasts (ECMWF) forecast the following ocean conditions in the area:
wave height: 0.82 m (steady)
sea temperature: 27.3°C (steady)
wave period: 3.55 seconds (steady)
wave direction: 115°(ESE)
swell height: 0–0.2 m (steady).
The passengers described windy conditions and being ‘smashed’ by the swell and on several occasions were washed off VH-XSO and were required to assist each other to get back onto the partially submerged helicopter.
Operational information
Overwater flights
The operator’s rotorcraft exposition for both their Civil Aviation Safety Regulation (CASR) Part 133 (air transport operations - rotorcraft) and Part 138 (aerial work operations) for flights over water, detailed that the rotorcraft must be fitted with emergency pop-out floats and that one or more suitable forced landing areas must be available at all times during flight.
The exposition detailed the requirements of a suitable forced landing area in relation to ditching as:
the rotorcraft must be able to ditch in the area of water with a reasonable expectation that there would be no injuries to persons in the rotorcraft or on the water. Company policy is that this is only viable in sea states of less than 2 metres.
CASR Part 133.010 provided the definition of a suitable forced landing area:
Areas of ground
(1) An area of ground is a suitable forced landing area for a flight of a rotorcraft if the rotorcraft could make a forced landing in the area with a reasonable expectation that there would be no injuries to persons in the rotorcraft or on the ground.
Areas of water
(2) An area of water that meets the requirements mentioned in subregulation
(3) is a suitable forced landing area for a flight of a rotorcraft if the rotorcraft:
(a) is equipped with emergency flotation equipment; or
(b) has a type certificate or supplemental type certificate for landing on water.
(3) For the purposes of subregulation (2), the requirements are the following:
(a) the rotorcraft must be able to ditch in the area of water with a reasonable expectation that there would be no injuries to persons in the rotorcraft or on the water;
(b) there must be a reasonable expectation that persons in the rotorcraft would survive in the area of water for the time that it would take to rescue the persons;
(c) if the flight is a passenger transport operation or a medical transport operation—the area of water must be:
(i) adjacent to land; or
(ii) adjacent to an offshore installation with search and rescue capabilities; or
(iii) in a location, set out in the rotorcraft operator’s exposition, that has search and rescue capabilities.
(4) Factors that affect whether there is a reasonable expectation about the matters mentioned in paragraphs (3)(a) and (b) include the following:
(a) the surface condition of the area of water, including the wave height, wind conditions and swell;
(b) the limits of the capability of the rotorcraft’s emergency flotation system to stay upright and floating in certain sea states.
Survivability
Operator’s procedures
For overwater flights, the pilot was required to leave a search and rescue time (SARTIME) with company operations that detailed the commencement and completion times of the intended flight. The pilot reported that they left SARTIME details with company operations and that the flight was also being monitored by aviation tracking software that recorded the helicopter’s position, altitude and performance every 2 minutes.
Helicopter underwater escape training
Fear, anxiety, panic and inaction are the common behavioural responses experienced by occupants during a helicopter ditching. The initial impact, in-rushing water, disorientation, entanglement with debris, unfamiliarity with seatbelt release mechanisms and an inability to reach or open exits have all been cited as problems experienced when attempting to escape from a helicopter following an in-water accident (Rice and Greear, 1973).
Helicopter underwater escape training (HUET) involves a replica of a helicopter cabin and fuselage being lowered into a swimming pool to simulate the ditching of a helicopter. The cabin can rotate upside down and focuses participants on bracing for impact, identifying primary and secondary exit points, opening an exit, releasing harness, egressing the wreckage and surfacing. HUET is normally part of a program of graduated training that builds in complexity, with occupants utilising different seating locations, exits and visibility. This training is conducted in a controlled environment with safety divers in the water.
The CASR Manual of Standards (MOS) Part 133, Chapter 12, section 12.04 discusses the requirements for flight crew general emergency training. The section included that training must cover ditching procedures, including in-water practical training, underwater escape and the use of lifejackets when lifejackets were required to be carried on the flight.
The operator’s risk assessment for an aircraft emergency while over water included a mitigating control that all pilots conducting overwater flight had currency in HUET. The pilot recalled that the techniques learnt during HUET assisted with their efficient egress.
Neither passenger had ever completed HUET, nor was there any regulatory requirement for them to do so.
The passenger in the rear right seat stated they initially attempted to egress the helicopter while wearing their seatbelt. They stated they were panicked and took 2 attempts to then unbuckle their seatbelt.
The front left passenger described ‘fumbling’ during their egress and stated they had difficulty opening their door due to the force of the water, and similar to the other passenger, they also attempted to egress with their seatbelt still fastened.
The Australian Transport Safety Bureau advises helicopter operators involved in overwater operations of the importance of undertaking regular HUET for all crew and regular passengers to increase their survivability in the event of an in-water accident or ditching.
The ATSB contacted 2 large organisations with employees who regularly flew as passengers in light helicopters over water as part of their employment. One of the organisations required that employees who flew 2 or more return flights per year underwent HUET, the other required HUET when employees flew 3 or more return flights per year. As part of a separate ATSB investigation, passengers from a third organisation with employees who regularly flew in the Torres Strait reported they were also provided HUET by their employer.
The Queensland Department of Education stated they did not provide any aviation training to their employees, nor was there a regulatory requirement for the passengers to conduct HUET.
Survival emergency locator transmitter
For all air transport flights, the operator required their aircraft to be fitted with a serviceable automatic emergency locator transmitter (ELT).10 The operator’s exposition also stated:
For any flights where a safe landing may not be possible in the event of an emergency, the PIC [pilot in command] should also carry a survival ELT.
The operator did not require nor did they provide a survival ELT11 to the pilot for the occurrence flight.
ATSB aviation research AR-2012-128A review of the effectiveness of emergency locator transmitters in aviation accidents(2013) found that automatic ELTs functioned as intended in about 40 to 60% of accidents in which their activation was expected and that automatic ELT activation accounted for the first notification in only about 15% of incidents. The research report safety message stated:
Pilots and operators of general aviation and low-capacity aircraft need to be aware that a fixed fuselage mounted ELT cannot be relied upon to function in the types of accidents in which they were intended to be useful. The effectiveness of ELTs in increasing occupant safety and assisting SAR efforts may be enhanced by using a GPS-enabled ELT, using an ELT with a newer 3-axis g-switch, ensuring it is installed correctly, ensuring your beacon is registered with AMSA and pre-emptively activating the beacon if a forced landing or ditching is imminent. Additionally, carrying a personal locator beacon in place of or as well as a fixed ELT will most likely only be beneficial to safety if it is carried on the person, rather than being fixed or stowed elsewhere in the aircraft.
CASA Part 133 MOS Chapter 11.50 required that a life raft fitted with a survival ELT be carried in single-engined rotorcraft if flights were conducted over water at a distance greater than 25 NM (46 km) from a suitable forced landing situated on land.
GBR Helicopters’ operations manual advised that flights were not conducted at distances over water where a life raft was required to be carried.
During the course of other ATSB investigations, it was identified that at least 2 other helicopter operators that conducted regular overwater flights with multiple helicopters, required their pilots to carry a survival ELT in addition to the helicopter’s automatic ELT.
Lifejackets
The operator’s exposition required occupants to wear lifejackets during overwater flight. For Torres Strait operations, passengers were provided with aviation‑approved constant wear vest style lifejackets with a single inflation cord that activated 2 gas cylinders that inflated the jacket. The lifejacket was worn over the head with a single strap fastened across the lower back (Figure 4).
The pilot wore a similar style lifejacket that was fastened at the front with a buckle and zip and featured pockets and dual toggles that individually inflated the 2 gas cylinders separately.
Both the pilot and passengers did not report any difficulty using or inflating the lifejackets.
Figure 4: Lifejackets provided for the occupants by the operator
Source: Red Barron ALSE, annotated by the ATSB
These lifejackets allow the wearer to inflate with a single movement. In comparison, pouch style lifejackets, common in overwater helicopter passenger operations and worn around the waist, required the lifejacket to be pulled from the pouch and then physically placed over the head prior to inflation. They are designed to be donned using one arm to allow the other arm to assist with buoyancy.
Survival kit
The operator advised that survival kits were located in all helicopters operating from its Horn Island base, serviced annually and stowed in an area where they were easily accessible but would not affect the operation of the helicopter. The operator’s exposition stated the minimum contents for their survival kits:
• survival manual
• 2 rations barley sugar
• 13 m light rope
• 2 water purifier tablets
• 1 knife
• 1 box of waterproof matches
• 2 space blankets
• 1 orange plastic sheet
• 1 compass
• 2 containers of water
• 1 signalling mirror
• 1 can opener.
One passenger stated the kit was also equipped with a small torch, however it was not bright enough to attract the attention of the pilot of the R44 helicopter who located the ditched helicopter.
The pilot reported that flares and sea dye were also available at the Horn Island base, however, were not part of the survival kit, were not required to be carried under the regulations or the operator’s exposition and that the pilot had not carried them on the flight.
Brace position
As of 1 December 2022, CASR Part 133 MOS chapter 7 section 7.01– Safety briefing card required that an operator supply a safety briefing card to all passengers specific to the helicopter type and model, which should include detail on how to assume the emergency brace position.
Section 7.02 –Safety briefings, instructions, or demonstrations, before take-off (9)(p) required that a safety briefing addresses when, and how, to assume the brace position.
Both passengers received a safety briefing from the pilot prior to their departure. The pilot recalled they had shown the passenger the operation of the doors, alternative exits and discussed the operation of the lifejackets. During interview the passengers were asked to recall the details of the safety briefing. Neither passenger reported receiving instruction of the brace position.
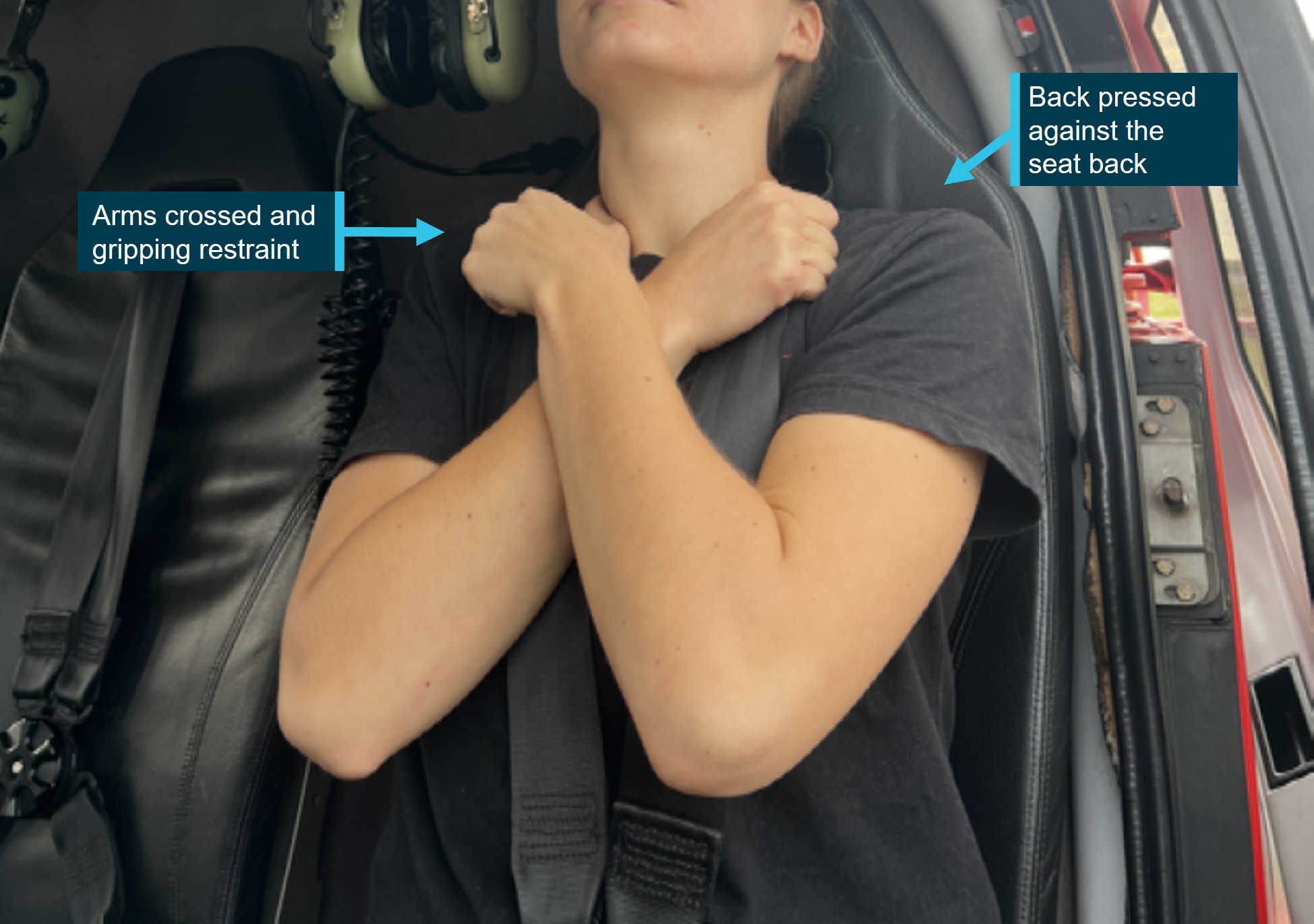
The operator had produced a specific briefing card for R44 helicopters. The card was available for each passenger in the helicopter, as required. The operator’s briefing card advised passengers the brace position was leaning back into the forward-facing seat while gripping the upper part of the harness for both the lap and sash style seatbelt fitted in VH-XSO and double shoulder harness as pictured (Figure 5). One of the passengers stated they were not aware of the safety briefing card in the helicopter.
Figure 5: GBR Helicopters R44 helicopter emergency brace position
Source: GBR Helicopters, annotated by the ATSB
During the emergency, when the pilot instructed the passengers to brace, the front left passenger stated that they sat upright in their seat and placed one hand on the pilot’s arm, the second passenger reported they gripped the crossbar on the back of the pilot’s seat and held the position until water impact.
Recorded information
Aviation planning software from the pilot’s electronic flight bag (EFB) recorded data every 5 seconds in increments of 100 ft altitude. The recorded data identified that the helicopter became airborne from Sadie’s Helipad, Thursday Island, at about 0719:50 and initially climbed to about 500 ft above sea level. At 0729:45 the helicopter was recorded at 600 ft and 83 kt ground speed. The data then showed a rapid descent (Table 1).
Table 1: VH-XSO last 5 recorded data points
Local time
Height above sea level (ft)
Ground speed (kt)
Heading (Magnetic)
0729:45
600
83
060˚
0729:50
500
75
059˚
0729:55
300
65
061˚
0730:00
200
56
082˚
0730:05
100
49
088˚
Separate aircraft tracking software, used by the operator to monitor aircraft position, recorded the helicopter’s last known position at about 600 ft and 90 kt ground speed and identified that the engine was ‘off’.
Related occurrences
A search of the ATSB occurrence database showed 7 other Australian registered helicopters had ditched into the ocean since 2011. The pilots of 6 of those occurrences had sufficient time to deploy the emergency pop-out floats, and 3 of the 6 helicopters involved rolled shortly after landing on the water.
Engine flame-out and ditching involving Bell LongRanger, VH-RHF, Cone Bay, approximately 98 km north of Derby, Western Australia (AO-2013-097)
On 8 June 2013 VH-RHF, was conducting an aerial survey flight with 4 passengers in the Buccaneer Archipelago area north of Derby, Western Australia. The helicopter was being flown at about 1,000 ft to a planned fuel stop on an island in Cone Bay and was over water when the engine flamed out. The pilot entered autorotation to glide towards land but was unable to reach it. During the glide the pilot deployed the helicopter’s pop-out floats in preparation for an emergency ditching. Shortly after touchdown the helicopter rolled inverted. The pilot and the 4 passengers exited without injury.
Ditching – Robinson R44, VH-HOT, 2 km east of Cairns, Queensland (AO-2011-001)
On 3 January 2011, VH-HOT departed Cairns Airport, Queensland, for a 30-minute charter flight. On board the helicopter was the pilot and 3 non-English speaking passengers. About 25 minutes into the flight, at about 400 ft above sea level, the engine failed and the rotor low rpm horn sounded. The pilot broadcast a MAYDAY and entered autorotation. During the descent he deployed the inflatable floats, however the right float did not fully inflate. The pilot assisted the passengers to egress the helicopter and inflated their life preservers. They were rescued from the water by fishermen in a small boat.
Abnormal engine indications and ditching involving Bell 206L-3, VH-LMW, 6.5 km west of Horn Island Airport, Queensland (AO-2026-003)
On 6 January 2026 during climb, the pilot and only occupant observed uncommanded yaw and fluctuating torque indications. The pilot received a low rotor alert and conducted an autorotation before activating the floats and ditching the helicopter which subsequently inverted. The pilot escaped the wreckage uninjured.
At the time of publication of this report this investigation was ongoing.
Safety analysis
Introduction
On 8 October 2025 a Robinson R44 Raven I, registered VH-XSO and operated by GBR Helicopters, departed Thursday Island, Queensland, with the pilot and 2 passengers on board. During cruise at about 600 ft above sea level the low rotor RPM horn activated and the pilot entered an autorotation. The pilot conducted a ditching and the helicopter immediately rolled onto its left side resulting in the front left seat passenger egressing the helicopter underwater. The 3 occupants were seriously injured from chemical burns from the fuel in the water while waiting for rescue, and one was additionally injured from an impact with the wreckage during the rescue winching.
This analysis will explore the operational considerations related to factors that affected the survivability of the occupants during an overwater emergency.
Total power loss
The pilot reported while in the cruise at about 600 ft, that the low rotor RPM horn activated and the helicopter engine RPM reduced before the engine completely stopped prior to ditching into the ocean. The last recorded data point from the operator’s flight tracking software for VH-XSO also indicated ‘engine off’.
The helicopter subsequently sank and was not able to be located or recovered. Consequently, the ATSB was unable to determine the likely cause of the engine power loss.
Contributing factor
For reasons undetermined, the helicopter engine had a total power loss during the cruise at 600 ft while operating over water, requiring the pilot to conduct a ditching.
Briefing of the brace position
Although the passengers had flown in helicopters in the Torres Strait regularly, and were familiar with the R44, the pilot of VH-XSO provided a pre-flight safety briefing which included operation of the doors as an emergency exit and alternative exits if a door was blocked, and the use of the lifejackets.
However, on this occasion, the pilot did not brief the passengers on how to adopt the correct brace position as required by the operator’s manual and the regulations. Although the pilot advised both passengers to brace during the autorotation, the front left passenger grabbed the pilot’s arm and sat back in their seat, while the rear seat passenger braced themselves using the cross bar on the back of the pilot’s seat. Both brace positions increased the risk of injury to the passengers and had the potential to interfere with the pilot’s ability to control the helicopter during the emergency.
The operator advised that VH-XSO contained safety briefing cards that depicted the brace position for the lap and sash harness fitted to VH-XSO. However, one passenger was not aware of the location of the safety briefing card.
Not being briefed on adopting the appropriate brace position increased the risk of injury to both occupants which may have further hindered emergency egress from the helicopter or affected the pilot’s ability to control the helicopter during the emergency.
Other factor that increased risk
The pilot did not provide the passengers with information on the appropriate brace position during the pre-flight safety briefing.
MAYDAY transmission and emergency response
Realising they were forced to ditch the helicopter, the pilot transmitted a MAYDAY call that alerted another helicopter that they intended to ditch in the ocean. The second helicopter diverted to the ditched helicopter, and in conjunction with a nearby fixed wing aircraft, were able to communicate the emergency to Brisbane Centre air traffic control, providing their location, which reduced the response time of the search and rescue aircraft in locating the occupants, and additional information on the survivor’s welfare.
Although the automatic emergency locator transmitter (ELT) had alerted the Joint Rescue Coordination Centre (JRCC) to the aircraft’s last known position, past studies have shown that the activation and transmission of ELTs is not always certain. Had the ELT not been activated, the pilot’s MAYDAY call was likely to have been the initiation of the emergency response.
Following their MAYDAY call, the pilot was able to deploy the emergency pop-out floats in preparation for the water landing; this very likely prevented the helicopter from rapidly sinking and allowed the occupants time to egress. Although the helicopter rolled shortly after ditching, the partially submerged helicopter provided some refuge from the ocean conditions and made visual identification for first responders easier. The helicopter’s ELT had also been activated, alerting rescuers to its location. However, had the helicopter sunk, ocean currents and wind would have carried the occupants away from their last known position.
The pilot also advised the passengers to brace prior to the water impact, and even though they had not been advised of the appropriate brace position, it is likely that this gave the passengers additional time to prepare and consider possible egress options.
Other finding
The pilot transmitted an effective MAYDAY call, activated the pop-out floats and instructed the passengers to brace prior to ditching. This improved the occupants’ survivability during and after the ditching.
Emergency pop-out floats
On landing, the left side emergency pop-out float detached from the skid and the helicopter rolled onto its left side. The detached float then became entangled in the rotor assembly, providing some buoyancy to the mast and preventing the helicopter from becoming inverted. The manufacturer advised that the floats may be susceptible to damage as a result of high forward airspeeds or impact forces.
The helicopter’s left skid had also recently been replaced due to an identified crack. The replacement of the skid meant that the emergency pop-out floats were reattached to the replacement skids. The operator advised that the skid replacement and emergency pop‑out float attachment was completed in accordance with the manufacturer’s maintenance manual.
The helicopter’s roll to the left resulted in the front left passenger egressing through their door while under water. Had the emergency pop-out float not lodged around the helicopter’s main rotor hub it is likely that all 3 occupants would have been required to egress from an inverted helicopter, increasing the risk of disorientation during escape.
The Robinson Helicopter Company advised that the R44 would likely remain stable in sea states of up to 2.4 m, which was above the forecast wave heights of about 0.8 m on the day of the accident. Following the egress, the 3 occupants then sought refuge on board the partially submerged helicopter. However, their legs were mostly submerged and they were often swept off the helicopter entirely. This exposed them to the leaked aviation gasoline and resulted in serious injuries to all 3 occupants. Without the detachment of the emergency pop-out float it was likely the helicopter would have remained upright and the occupants could have remained on board until their rescue with significantly less time exposed to the leaked fuel in the water.
Both the helicopter and the detached left emergency pop-out float were not recovered, and the cause of the detachment could not be accurately determined.
Contributing factor
For reasons that were undetermined, during the ditching, the left float detached causing the helicopter to roll in the water. This reduced the likelihood of a successful emergency egress and exposed the survivors to fuel in the water leading to chemical burn injuries.
Survival emergency locator transmitter on overwater flights
GBR Helicopters did not provide company pilots with a survival ELT for all overwater flights, nor were they required to unless the flight involved a distance from a suitable forced landing area that required the carriage of a life raft.
The single-engined Robinson R44 helicopter VH-XSO was fitted with emergency pop-out floats, certified for water landing, however they were not certified for ditching, resulting in a greater risk of float damage and therefore capsize during a ditching event.
The ATSB considered that during the ditching, the attached remaining emergency pop‑out float could have been damaged or detached, which may have resulted in the helicopter sinking immediately after impact. In such circumstances, had the occupants successfully egressed they would have been subject to wind and current and likely drifted from the last known position, increasing the search area, reducing the likelihood of timely detection and increasing the occupants’ exposure time in the water.
Carriage of a survival ELT by the pilot would have provided an additional layer of safety, if carried on their person, via timely and accurate location for search and rescue focus, increasing post‑impact survivability.
Other factor that increased risk
GBR Helicopters did not provide company pilots with a survival ELT for all overwater flights. This reduced the post‑impact survivability of a ditching event. (Safety Issue)
Helicopter underwater escape training
It is a regulatory requirement for pilots conducting overwater flight to conduct helicopter underwater escape training (HUET) every 3 years, although there is no regulatory requirement for passengers who travel regularly in helicopters over water to conduct the training.
Both passengers had flown regularly in helicopters over water as part of their employment with the Queensland Department of Education during the 12 months preceding the occurrence flight and had never undertaken HUET.
HUET is considered to provide individuals with familiarity with the crash environment and confidence in their ability to cope with the emergency situation (Ryack et al., 1986). Interviews with survivors from helicopter accidents requiring underwater escape frequently mention that they considered that HUET was very important in their survival. Training assists by providing reflex conditioning, a behaviour pattern to follow and reducing confusion and panic (Hytten, 1989).
Passengers stated they fumbled and felt panicked, both attempting to egress while still wearing their seatbelts. Therefore, it was likely the passengers’ egress would have been more efficient and reduced the risk of drowning had they completed HUET.
Other organisations whose employees travelled numerous times per year in helicopters over water arranged HUET for these employees. However, Queensland Department of Education employees were not provided with any aviation‑specific training. HUET training provides the opportunity to develop a behavioural pattern for underwater emergency helicopter egress and has been shown to increase post‑impact survivability and decrease the risk of drowning.
Other factor that increased risk
Queensland Department of Education employees who regularly fly over water in helicopters were not provided with Helicopter Underwater Escape Training which increased the risk of drowning. (Safety Issue)
Lifejackets
GBR Helicopter’s Horn Island operation provided passengers with constant wear, vest style, lifejackets and required that they be worn at all times for overwater flights.
The front seat passenger described ‘feeling heavy’ in the water and had difficulty staying buoyant, compounded by the constant swell, until they were instructed to inflate their lifejacket. The wearable vest style life jacket was able to be immediately inflated post‑accident, without requiring it to be donned while attempting to remain afloat in the water.
Had any of the occupants lost consciousness while awaiting a rescue, a first responder need only inflate the passenger’s lifejacket, removing the additional step of donning the jacket from a pouch for a person requiring assistance.
The quick inflation of the lifejacket provided rapid buoyancy and increased their post‑accident survivability.
Other finding
The use of constant wear, vest style lifejackets likely increased the ease and speed of use, enhancing the survivability of occupants.
Rescue
Following the arrival of the rescue helicopter on site, the rescue crew officer was winched into the water to retrieve the people one-by-one via the winch with themselves also attached. During one winch recovery, the person being rescued reported they impacted the wreckage of the helicopter while being dragged through the water, likely resulting in the fracture to their rib. Environmental conditions on the day likely increased the difficulty for the rescue, with the wind and sea state moving the rolled and partially submerged wreckage. This likely increased the difficulty of identifying their proximity to the wreckage, especially sections of the helicopter that were submerged, and increased the risk of impact and therefore injury.
Neither the rescue crew officer or the aircrew officer observed the impact with the wreckage and were not advised by the injured person during the transfer to Thursday Island Hospital.
Although it was considered possible that the rib injury was sustained during the ditching sequence or subsequent egress, the elapsed time between the ditching and rescue was likely sufficient for the injured individual to have recognised the presence of a fracture injury. In the absence of any reported awareness of such an injury before the rescue, it is therefore more likely that the fractured rib was sustained during the winch recovery.
Contributing factor
One of the people being rescued likely sustained an additional serious injury after impacting the wreckage while being winched.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the power loss and ditching involving Robinson R44, VH-XSO, 24 km north-east of Horn Island Airport, Queensland, on 8 October 2025.
Contributing factors
For reasons undetermined, the helicopter engine had a total power loss during the cruise at 600 ft while operating over water, requiring the pilot to conduct a ditching.
For reasons that were undetermined, during the ditching, the left float detached causing the helicopter to roll in the water. This reduced the likelihood of a successful emergency egress and exposed the survivors to fuel in the water leading to chemical burn injuries.
One of the people being rescued likely sustained an additional serious injury after impacting the wreckage while being winched.
Other factors that increased risk
The pilot did not provide the passengers with information on the appropriate brace position during the pre-flight safety briefing.
GBR Helicopters did not provide company pilots with a survival emergency locator transmitter for overwater flights. This reduced the post‑impact survivability of a ditching event. (Safety Issue)
Queensland Department of Education employees who regularly fly over water in helicopters were not provided with Helicopter Underwater Escape Training which increased the risk of drowning. (Safety Issue)
Other findings
The pilot transmitted an effective MAYDAY call, activated the pop-out floats and instructed the passenger to brace prior to ditching. This improved the occupants' survivability during and after the ditching.
The use of constant wear, vest style lifejackets likely increased the ease and speed of use, enhancing the survivability of occupants.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.comes to hand.
Helicopter underwater escape training for regular passengers
Safety issue description: Queensland Department of Education employees who regularly fly over water in helicopters were not provided with Helicopter Underwater Escape Training which increased the risk of drowning.
Carriage of survival emergency locator transmitter
Safety issue description: GBR Helicopters did not provide company pilots with a personal locator beacon for overwater flights. This reduced the post‑impact survivability of a ditching event.
Glossary
ATC
Air Traffic Control
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
CTAF
Common terminal area frequency
EASA
European Union Aviation Safety Agency
ECMWF
European centre for medium-range weather forecasts
ELT
Emergency locator transmitter
EPIRB
Emergency position-indicating radio beacon
FAA
Federal Aviation Administration
HUET
Helicopter underwater escape training
JRCC
Joint Rescue Coordination Centre
KIAS
Knots of indicated airspeed
kt
Knots
NM
Nautical mile
SAR
Search and rescue
PLB
Personal locator beacon
POH
Pilot operating handbook
RPM
Revolutions per minute
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of the accident flight
passengers of the accident flight
the pilot of VH-WTT
recorded data from EFB and satellite tracking device
images provided by the operator
maintenance records of the occurrence aircraft
the rescue crew officer
Queensland Department of Education
Civil Aviation Safety Authority
Robinson Helicopter Company
Bureau of Meteorology.
References
Rice, E. a. (1973). Underwater escape from helicopters. In proceedings of the eleventh annual symposium, Cited in Brooks C. (1989)The human factors relating to escape and survival from helicopters ditching in water (pp. 59-60). Phoenix AZ: AGRAD.
Ryack, B. L. (1986). Surviving Helicopter crashes at sea,. Aviation Space and Environment Medicine, 57(6), 603-609.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of VH-XSO
the passengers on board VH-XSO
GBR Helicopters
the rescue helicopter operator
CASA
Bureau of Meteorology
Robinson Helicopter Company
Queensland Department of Education
Australian Maritime Safety Authority
United States National Transport Safety Board (NTSB)
Submissions were received from:
the pilot of VH-XSO
the passengers on board VH-XSO
GBR Helicopters
the rescue helicopter operator
CASA
Bureau of Meteorology
Robinson Helicopter Company
Queensland Department of Education
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
Footnotes
1
A precautionary check of the aircraft’s performance and position - compass, log, engine, altitude, radio, orientation, fuel and forced landing areas.
2
A primary flight control that collectively adjusts the pitch on the main rotor blades.
3
Autorotation is a condition of descending flight where, following an engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is driven mainly by airspeed.
4
A ditching is a controlled emergency landing of an aircraft on water.
5
MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
6
Sea state is the general condition of the free surface on a large body of water.
7
Rescue strop is designed for hoisting personnel from ships, shore and sea during helicopter operations.
8
World Meteorological Organization - Sea State 4 wave heights of between 1.25 and 2.5 metres.
9
A helicopter swash plate transmits flight control inputs to the main rotor blades allowing vertical and rotational movement.
10
Automatic emergency locator transmitter (ELT): a radio beacon that transmits an emergency signal that may include the position of a crashed aircraft, activated either manually or due to the forces of an accident.
11
A survival ELT refers to approved emergency position-indicating radio beacons (EPIRB) and personal locator beacons (PLB). They are removable from an aircraft or carried on the person, and require manual activation.
Occurrence summary
Investigation number
AO-2025-062
Occurrence date
08/10/2025
Occurrence time and timezone
07:20 Australian Eastern Standard Time
Location
24 km north-east of Horn Island Airport
State
Queensland
Report release date
07/05/2026
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Ditching, Engine failure or malfunction
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R44
Registration
VH-XSO
Serial number
817
Aircraft operator
GBR Helicopters Pty Ltd
Sector
Helicopter
Operation type
Part 133 Air transport operations - rotorcraft
Activity
Commercial air transport-Non-scheduled-Passenger transport charters
The ATSB is investigating a flight below minimum altitude involving Cirrus SR22T, VH-XXO, 10 km east of Canberra Airport, Australian Capital Territory, on 2 October 2025.
The aircraft did not adhere to the height or tracking requirements during approach and subsequently descended below the minimum safe altitude. The controller issued a safety alert, followed by a visual approach that did not meet the requirements of operations after last light.
To date, the ATSB investigation has included:
analysis of recorded and air traffic surveillance data
interviewing the pilot
reviewing weather and environmental conditions
reviewing operational documentation
reviewing related occurrences.
The final report has been drafted and is undergoing internal review to ensure the report adequately and accurately reflects the evidence collected, analysis, and agreed findings.
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
The Australian Transport Safety Bureau is currently recruiting for marine transport safety investigators.
The ATSB is completely independent of operators and the regulator, and has unique powers to gather and protect evidence under the Transport Safety Investigation Act 2003.
Our role is to help prevent future occurrences by ensuring lessons are learned and safety improvements are made through evidence-based, no-blame investigations, providing assurance that systems are operating safely.
We are looking for candidates with a good understanding of the maritime industry, ships and shipboard operations, the ability to interpret and apply legislation, regulations and standards, and demonstrable involvement and interest in marine safety and safe shipboard operations.
In particular, we are seeking candidates with at least 2 years of current or recent experience as a chief engineer or first engineer on seagoing vessels or as a ship superintendent, surveyor or similar, and who have a highly developed knowledge and understanding of the ISM Code and safety management systems.
The successful candidates will be supported in their transport safety investigator career path through a structured development and training program, including the opportunity to gain formal tertiary qualifications through our partnership with RMIT University.
As their capabilities, skills and experiences develop, investigators take on increasingly complex investigations and can lead multiple investigations at any point in time.
With on-the-job training and mentoring, they progressively become involved in larger and more systemic investigations that drive safety change – such as our recently-released reported into the near stranding of the bulk carrier Portland Bay near Sydney.
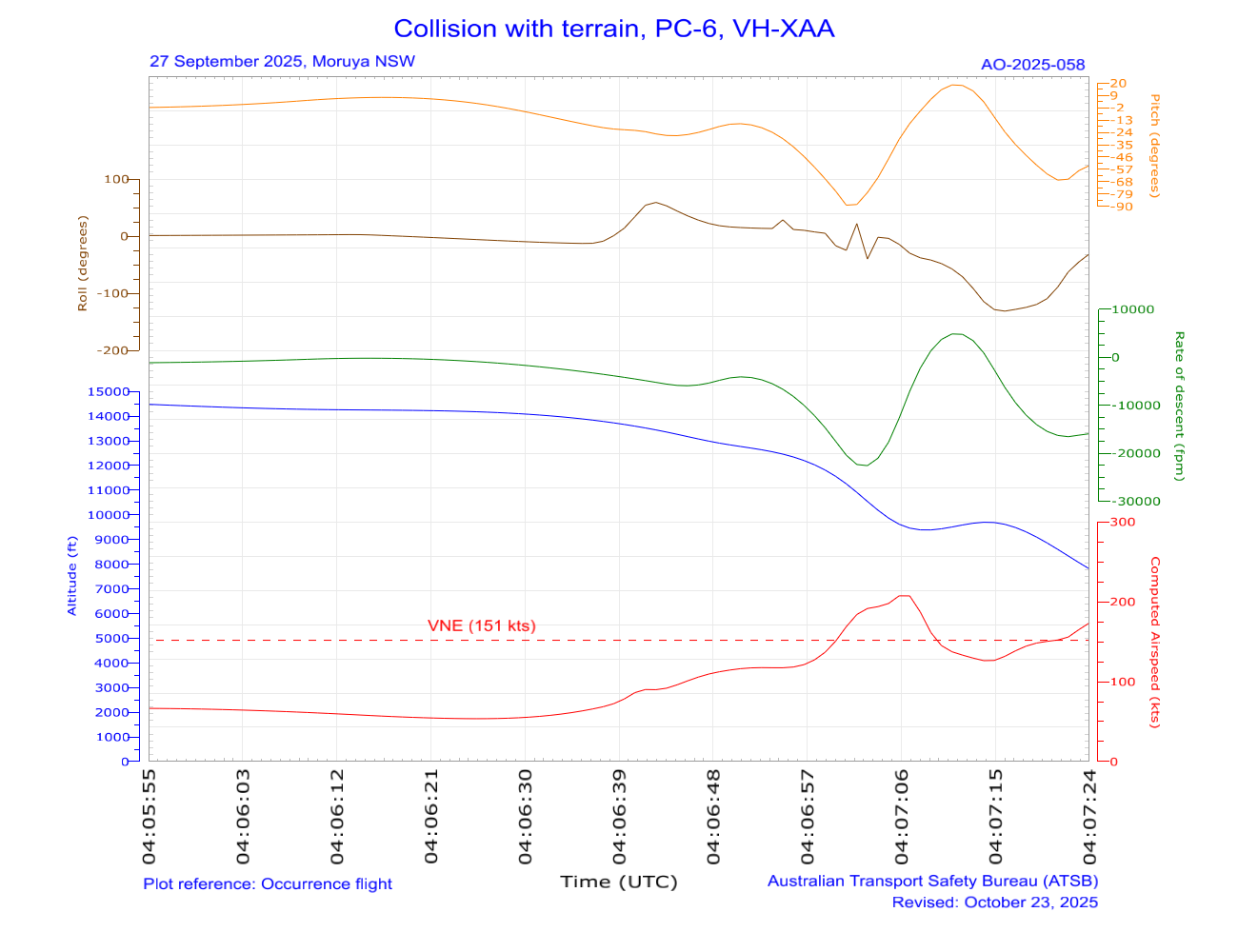
The ATSB is investigating a collision with terrain involving a Pilatus Aircraft Ltd PC-6, registered VH-XAA, 2 km north of Moruya Airport, New South Wales, on 27 September 2025.
While returning to Moruya Airport following the completion of a skydiving drop, the aircraft collided with terrain. The pilot sustained fatal injuries.
The ATSB deployed a team of transport safety investigators to the accident site with experience in aircraft operations, maintenance and engineering.
As part of the evidence collection phase of the investigation, ATSB investigators will examine the aircraft wreckage and other information from the accident site, examine operator procedures, interview witnesses and any involved parties, and examine maintenance records and any recorded data.
The ATSB released a preliminary report, which details factual information established in the investigation’s early evidence collection phase, on 12 November 2025. See below.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Preliminary report
Report release date: 12/11/2025
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Summary video
The occurrence
On 27 September 2025, the pilot and owner of a Pilatus PC-6/B2-H4 aircraft, registered VH-XAA and operated by Jump Aviation for SKYONE Moruya Heads parachuting organisation, was conducting parachute operations over Moruya Airport, New South Wales. After conducting 8 successful parachute drops, at 1348:58 local time, the pilot broadcast on the common traffic advisory frequency (CTAF)[1] that they were taxiing for runway 04[2] to conduct the next flight. On board were 8 parachutists and the pilot. The pilot was wearing the fitted 4-point restraint and an emergency parachute in accordance with company procedures.
At 1351:08, the pilot broadcast that the aircraft was airborne off runway 04, for an upwind departure and on climb to flight levels (FL)[3] for parachute operations. During the climb to the planned drop between FL 140 and 150, several parachutists reported feeling a bump and hearing the stall warning[4] activate momentarily, passing about 10,000 ft.
At 1400:52, the pilot broadcast on the CTAF that they were 4 minutes to a parachute drop, then advised the same to Melbourne Centre air traffic control. Recorded data showed the ‘jump run’ tracked in a northerly direction about 2 km west of Moruya Airport runway 36, in a gradual descent between FL 150 and 140. The parachutists reported that the jump run was normal, and all the parachutists exited successfully. At 1406:15, the pilot broadcast that the parachutists had exited and the aircraft was on descent.
Several witnesses on the ground observed the aircraft enter a steep nose-down dive, rotating left before pitching[5] up and rolling[6] right. Recorded data showed the aircraft initially descended from FL 140 at about 5,000 fpm, but approaching FL 120, the descent rate increased significantly. The last recorded automatic dependent surveillance‑broadcast (ADS-B) data position was at 1407:26 and 7,425 ft, descending at about 15,000 fpm (Figure 1). The aircraft subsequently impacted trees and terrain about 2 km north of Moruya Airport. The pilot sustained fatal injuries, and the aircraft was destroyed.
Figure 1: VH-XAA flight track and accident site
Source: Google Earth, annotated by the ATSB
Context
Pilot
The pilot held a private pilot licence (aeroplane) with the last flight review conducted in August 2025, and a class 2 aviation medical certificate, valid until June 2027. The pilot held the appropriate ratings and endorsements for the flight. In addition, the pilot held aerobatics and spin endorsements and jump pilot authorisation. At the time of the accident, they had about 11,690 hours total aeronautical experience. In the previous 90 days, they had flown 135.2 hours, most of which were conducting parachuting operations in Cessna 206 and 208 aircraft.
The pilot’s logbook recorded an endorsement for the Pilatus PC-6 (required by the then Civil Aviation Regulations) in 1998. The ATSB was unable to access some of the pilot’s logbooks to confirm how many hours they had logged flying the Pilatus PC-6 prior to purchasing VH‑XAA from New Zealand (NZ). Between 22 and 24 August 2025, the pilot and an instructor flew the aircraft from Auckland, NZ, to Dubbo, New South Wales, logging 19.5 hours of flight time. The pilot then recorded 2 hours operating the aircraft to Moruya on 12 September 2025. From 20 to 24 September 2025 inclusive, the pilot recorded 9.7 hours in the aircraft conducting parachute operations. At the start of the accident morning, the pilot had logged 31.2 hours in VH-XAA.
The pilot was an experienced parachutist and had been a member of the Australian Parachute Federation (APF)[7] since 1987. On 30 June 2025, the pilot reported having conducted 17,000 jumps. The pilot held numerous parachuting qualifications including senior instructor and a Certificate F, which was the highest certificate issued by the APF. The pilot was the senior pilot of Jump Aviation and the chief parachute instructor of the parachuting operator SKYONE Moruya Heads – a group member of the APF.
Aircraft
General information
VH-XAA was a Pilatus Aircraft PC-6/B2-H4, short take-off and landing utility aeroplane with fixed landing gear (Figure 2). It was powered by a Pratt & Whitney Canada PT6A-27 turbine engine and a Hartzell Propellers HC-B3TN-3D 3-bladed propeller. The aircraft was not approved for aerobatic manoeuvres including spins.
Figure 2: VH-XAA when operating in New Zealand as ZK-MCK
Source: Richard Currie, modified by the ATSB
It was manufactured in Switzerland in 1980 and issued serial number 809. The aircraft had been used for parachute operations in New Zealand (NZ) since 1982. As such, the passenger seats, copilot seat and copilot control stick had been removed. Additionally, a skydiving step and hand hold had been installed.
A 7,000 hour/14-year ‘complete overhaul’ maintenance activity was performed in NZ and finalised on 14 August 2025. During the maintenance activity, the horizontal stabiliser electric trim actuator was removed and overhauled by the manufacturer in the United States.
The aircraft was added to the Australian civil aircraft register on 15 August 2025, and a special flight permit[8] was issued to allow the aircraft to be flown from NZ to Australia. After the pilot ferried the aircraft to Australia, a certificate of airworthiness was issued for VH-XAA on 19 September 2025. At the time of the accident, VH-XAA had accrued 13,594.5 hours total time in service.
Doors
The aircraft had a door on each side of the cockpit for pilot and copilot access, which were fitted with a jettison system. Figure 3 shows the Pilatus PC-6 airplane flight manual[9] (AFM) procedure for emergency opening of the cockpit doors:
The aircraft cabin had a sliding door on the right side, which was used for parachutists to exit, and 2 hinged doors on the left side, which were fitted with an emergency jettison system. The sliding door had a mechanism to open it from inside the aircraft, but it could not be locked open. Parachutists reported that, on the day of the accident, the pilot had landed with the sliding door open on some flights and closed on others. Although it was not identified at the accident site, several parachutists reported that there was a fishing gaffer hook on a pole onboard the aircraft that the pilot used to close the sliding door in flight from the pilot’s seat.
stalling speeds at a gross weight of 2,800 kg, power off and 0° angle of bank including:
58 kt calibrated airspeed[12] (KCAS) with flap retracted
52 KCAS with landing flap extended.
Horizontal stabiliser electric trim system
The aircraft was fitted with a horizontal stabiliser electric trim system, designed to move the entire horizontal stabiliser to adjust the pitch trim of the aircraft and balance the aerodynamic forces to reduce the pilot control forces on the elevator. The system (Figure 4), consisted of:
a dual motor (main and alternate motors) electrically‑operated linear trim actuator
a 3-position spring-loaded trim switch, located on the control column grip
a relay located on the firewall
an interrupt system incorporating a guarded switch on the instrument panel shelf and an alternate trim control system with a 3-position spring-loaded trim switch (Figure 5)
an electrically‑operated trim position indicator on the upper left side of the instrument panel.
Figure 4: Schematic of horizontal stabiliser trim system
Source: Pilatus PC-6 Illustrated Parts Catalogue, modified and annotated by the ATSB
Figure 5: Instrument panel shelf horizontal stabiliser trim switches
Source: Supplied and Pilatus PC-6 AFM, annotated by the ATSB
The AFM included the following procedure (Figure 6) in the event of a trim runaway:[13]
Figure 6: Horizontal stabiliser trim runaway emergency procedure
Source: Pilatus PC-6 airplane flight manual
The AFM included the following procedure (Figure 7) for jammed trim actuators:
Figure 7: Jammed horizontal stabiliser trim actuator emergency procedure
Source: Pilatus PC-6 airplane flight manual
The AFM also included the following procedure (Figure 8) for loss of elevator control:
Figure 8: Loss of elevator control emergency procedure
Source: Pilatus PC-6 airplane flight manual
Beta mode
The AFM described beta mode as ‘operation of the propeller used in flight to achieve fast deceleration and high rates of descent’. The AFM stated:
In the beta range, the propeller blades are set at a low positive pitch angle to provide a braking effect for steep controlled descents. When operating in the beta mode, the propeller pitch angle is controlled by power lever movement between the lift detent and the point where constant speed operation becomes effective.
NOTE
BETA MODE is provided in descent at airspeeds below 100 KIAS [kt indicated airspeed] with the POWER lever near or at the detent. Only small movements of the POWER lever are necessary to change rate of descent or airspeed. Approaches in full BETA MODE (POWER lever at detent) are not permitted at airspeeds below 1.3 Vs.[14]
Meteorological information
The Bureau of Meteorology aerodrome forecast for Moruya Airport, issued at 1109 on 27 September 2025 included wind from 090° at 5 kt, which was expected to change to 310° and become gusty between 1200 and 1300. The grid point wind and temperature chart showed the forecast winds:
at 10,000 ft from 270° at 42 kt
at FL 140 from 270° at 51 kt.
The Bureau of Meteorology had also issued SIGMETs[15] for severe turbulence below 8,000 ft and mountain waves from 4,000 ft to FL 320 in an area that included Moruya Airport, between 1100 and 1500.
The conditions recorded in the METAR[16] at Moruya Airport at 1400 included wind from 130° at 6 kt, visibility greater than 10 km, temperature 22°C, and QNH[17] 1,007 hPa.
Recorded data
The ATSB conducted preliminary analysis of the aircraft’s 3-dimensional position information recorded in the ADS-B data for the 9 flights on 27 September 2025, the last of which was the accident flight. The positional data was interpolated between recorded positions and a trajectory analysis conducted to estimate other flight performance and handling parameters. The analysis was based on the forecast wind and an estimated aircraft weight of 1,587 kg (3,500 lb). For most of the flights, there was no recorded ADS‑B data below about 4,000 ft above mean sea level.
A comparison of the following key parameters for the 9 flights was conducted for the descent following parachute drop from about FL 140:
altitude
descent rate
estimated calibrated airspeed
estimated pitch and roll angles.
For flights 1–5, 7 and 8, the values of these parameters were similar. In those 7 flights, the descent commenced at an airspeed of about 55–70 KCAS, with an initial nose-down pitch of about 30° and either a right or left roll of about 30° (on flight 4 the roll angle was possibly up to 50°). The maximum descent rate for these 7 flights was between about 5,500 and 8,000 fpm.
On flight 6, the descent was initiated slightly slower, at about 54 KCAS, which increased within 10 seconds to about 145 KCAS, coincident with a maximum momentary descent rate of about 14,000 fpm, a steep (70°) pitch down in conjunction with a substantial roll right.
The descent on the accident flight (flight 9) was initiated at about 53 KCAS from 14,200 ft to a nose-down pitch of about 25°, with a 60° right roll. The aircraft briefly reduced pitch slightly before nosing vertically down (about 90°) in a left roll, reaching a maximum descent rate of over 20,000 fpm. The aircraft then pitched up to a shallow climb and into a roll of more than 120°. From the data it could not be confirmed whether this manoeuvre was conducted upright or inverted. Passing about 9,600 ft, the airspeed reduced to 125–130 KCAS before increasing again. The last recorded position, passing about 8,000 ft indicated the aircraft had accelerated to 173 KCAS, with a final descent rate above 15,000 fpm (Figure 9).
Figure 9: Preliminary plot of key parameters from the accident flight descent
Due to the aircraft’s manoeuvring, the roll information may be inaccurate. Local time was UTC+10 hours. Source: ATSB
Site and wreckage
The wreckage site was about 2.5 km north (and slightly west) of the northern end of the Moruya Airport runway 36. ATSB examination showed that the right wing struck a tree on the eastern side of George Bass Drive and separated from the fuselage, before the aircraft collided with trees on the western side of the road and subsequently impacted terrain in a nose-down inverted attitude (Figure 10). The outer section of the right wing landed on the road but was moved clear by members of the public shortly after the accident.
Figure 10: Overview of VH-XAA accident site
Source: ATSB
The examination identified:
there was fuel remaining and no post-impact fire occurred
all major components of the aircraft were at the site, indicating there was no in-flight breakup
the propeller had indications that the engine was producing power at impact
there were no indications of any pre-impact mechanical anomalies that would have precluded normal engine operation
the pilot’s 4-point restraint was undone, and the pilot was almost certainly not in the pilot seat at the time of impact
the horizontal stabiliser trim actuator was found in the full nose-down position (Figure 11).
Figure 11: Horizontal stabiliser trim actuator showing trim position
Source: ATSB
Further investigation
To date, the ATSB has:
interviewed witnesses and involved parties
obtained pilot and aircraft documentation
analysed recorded data
reviewed recorded audio transmissions
assessed the accident site and examined the aircraft wreckage.
The investigation is continuing and will include further examination of:
the horizontal stabiliser trim system
recorded flight data
aircraft configuration, maintenance and documentation
operational procedures and documentation
pilot training records
survivability and opportunity for egress
other similar occurrences.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB would like to acknowledge the assistance of the NSW Police Force, Fire and Rescue NSW, and first responders.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Common traffic advisory frequency (CTAF): a designated frequency on which pilots make positional broadcasts when operating in the vicinity of a non-controlled aerodrome or within a broadcast area.
[2]Moruya Airport had 2 sealed runways, 18/36 and 04/22. The runway number represents its magnetic heading.
[3]Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 140 equates to 14,000 ft.
[4]A stall warning system provides the pilot with advance warning of an impending aerodynamic stall.
[5]Pitching: the motion of an aircraft about its lateral (wingtip-to-wingtip) axis.
[6]Rolling: the movement of an aircraft about its longitudinal axis.
[7]The APF is the peak body for the administration and representation of Australian Sport Parachuting.
[8]Special Flight Permit (SFP): issued to allow the operation of an aircraft that does not meet its airworthiness requirements but under certain circumstances, and for a particular intended purpose, the aircraft may still be capable of safe flight.
[9]Airplane flight manual (AFM): a manual that is part of the certification basis of the aircraft, containing the operating limitations within which the aircraft is considered airworthy, and any other information required for the safe operation of the aircraft, including all amendments and supplements for that manual.
[10]Never exceed speed (VNE): the indicated airspeed which, if exceeded, may result in structural damage to the aircraft, normally represented by a red line on the airspeed indicator.
[11]Manoeuvring speed (VA): the maximum speed at which a pilot can make full or abrupt control movements without causing structural failure of the aircraft.
[12]Calibrated airspeed: indicated airspeed corrected for air speed indicator system errors.
[13]Pitch trim runaway is an uncontrolled movement of the aircraft’s trim system causing uncommanded nose-up or nose‑down pitch.
[14]Vs - Stall speed or minimum steady flight speed for which the aircraft is still controllable.
[15]SIGMET: a concise description of the occurrence or expected occurrence, in an area over which area meteorological watch is maintained, of specified phenomena which may affect the safety of aircraft operations.
[16]METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[17]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
Occurrence summary
Investigation number
AO-2025-058
Occurrence date
27/09/2025
Occurrence time and timezone
14:00 Australian Eastern Standard Time
Location
2.5 km north of Moruya Airport
State
New South Wales
Report release date
12/11/2025
Report status
Preliminary
Anticipated completion
Q1 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Evidence collection
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Loss of control
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Pilatus Aircraft Ltd
Model
PC-6/B2-H4
Registration
VH-XAA
Serial number
809
Aircraft operator
Jump Aviation Pty Ltd
Sector
Turboprop
Operation type
Part 105 Parachuting
Activity
General aviation / Recreational-Sport and pleasure flying-Parachute dropping
The ATSB is investigating a collision with terrain involving a Robinson R22, registered VH‑RDL, at Bankstown Airport, New South Wales, on 3 October 2025.
During training operations, the aircraft collided with terrain and was subsequently destroyed. One occupant was fatally injured and the other person received serious injuries.
The ATSB deployed a team of transport safety investigators to the accident site with experience in operations, maintenance and engineering. Several components were recovered from the accident site for more detailed examination.
The ATSB has commenced the examination and analysis of the initial evidence collected.
To date, the ATSB investigation has:
examined the aircraft wreckage and other information from the accident site
retrieved operator procedures
conducted interviews with the surviving pilot, witnesses and other involved parties.
reviewed pilot records
reviewed maintenance records and video evidence.
reviewed air traffic control communications.
The continuing investigation will include:
analysis of the audio signatures captured by the recording camera
further analysis of physical evidence retrieved from the accident site
interview with Bankstown tower air traffic control.
The ATSB released a preliminary report, which details factual information established in the investigation’s early evidence collection phase, on 17 December 2025. See below.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Preliminary report
Report release date: 17/12/2025
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 3 October 2025, a Robinson R22 Beta helicopter, registered VH‑RDL and operated by Bankstown Helicopters,[1] was conducting a training flight at Bankstown Airport, New South Wales. On board the helicopter was a flight instructor, seated in the left seat, and a student pilot in the right seat. The flight instructor was the pilot in command (PIC), however, as it was a training flight, the student pilot was in the seat normally reserved for the PIC.
The helicopter departed the main helicopter pad (Figure 1) at about 1328 local time. The plan for the flight was to conduct circuits[2] on runway 29. The student pilot stated to the ATSB that they had planned and prepared to conduct a lesson on practice forced landings. However, due to the weather, the instructor changed the lesson to circuits. Due to the windy conditions on the day, the instructor demonstrated the first circuit, with the student pilot following them on the flight controls.[3]
At about 1329, the instructor made a downwind position radio broadcast and was cleared by Bankstown Tower air traffic control for a ‘stop and go’ on the main pad. In interview with the ATSB, the student pilot recalled that, during the downwind leg of the circuit, the helicopter dropped suddenly and they noticed the revolutions per minute (RPM) reduce but could not recall if this was engine or rotor RPM (see section Helicopter information). The student also recalled hearing a whistling noise prior to the RPM reduction. Following the sudden drop and RPM reduction, the student recalled that the instructor kept their hands on the controls and continued to fly the aircraft while attempting an autorotation,[4] and they could not recall the instructor changing any switch positions.
Dashcam video taken from a parked car captured the helicopter tracking along its flight path, before conducting a turn back into wind toward the airport. The video showed that the helicopter was flared[5] as it approached the ground, likely in an attempt to reduce the rate of descent. The helicopter impacted trees, before colliding with the rear of a car and the ground, coming to rest on its left side. The instructor was fatally injured, and the student was seriously injured. The helicopter was destroyed.
Figure 1: Estimated flight path
Source: Airservices Australia, annotated by the ATSB
Context
Pilot information
The instructor held a Commercial Pilot (Aeroplane) Licence (CPL-A) issued July 1998, and a Commercial Pilot Licence (Helicopter) (CPL-H) issued July 2012. They also held a Grade 1 flight instructor rating for helicopter operations.
The instructor began employment with the operator of VH-RDL in November 2024. Paperwork completed when joining indicated that the instructor had around 877 hours experience on fixed-wing aircraft, and 1,071 hours in helicopters. The instructor’s logbook indicated that, as of September 2025, they had a total helicopter flying experience of 1,131 hours, which included 993 hours as PIC.
The instructor held a class 2 aviation medical certificate, which was current at the time of the accident. To exercise the privileges of a commercial pilot’s licence, pilots normally required a class 1 aviation medical. However, under Civil Aviation Safety Authority (CASA) General Exemption CASA EX28/23, commercial pilots with a class 2 medical certificate can fly commercial flights without passengers if the aircraft’s maximum take-off weight is less than 8,618 kg. This included flight training.[6]
Video evidence showed the instructor was completing pre-flight duties in the office at approximately 0630. Their first flight of the day commenced at 0700 with a hover lesson. This was followed by another general handling instructional flight at 0830. All flights were conducted in VH‑RDL.
The student pilot had approximately 33 hours of flight experience. They did not yet hold a pilot’s licence.
Helicopter information
VH-RDL was a 2-seat Robinson Helicopter Company R22 Beta, serial number 1498, powered by a 4-cylinder Lycoming O-320-B2C engine. The helicopter was manufactured in the United States in 1990 and placed on the Australian aircraft register on 16 April 2002. Bankstown Helicopters had been the registered operator of VH-RDL since 22 February 2024.
The helicopter had a combined engine and rotor RPM tachometer, which was positioned on the right side of the dashboard in front of the student pilot (Figure 2). The left side of the tachometer showed the engine RPM and the right side showed the rotor RPM. The position of the tachometer required the instructor to look across the dashboard to see the instrument.
Figure 2: VH-RDL engine and rotor RPM tachometer
Source: ATSB
Meteorological information
During taxi, the student pilot reported they had received information ‘golf’ from the automatic terminal information service (ATIS).[7] The information indicated that runway 29 was in use, mechanical turbulence was present on short final, the wind was 220° at 18 kt with a crosswind up to 20 kt, conditions were CAVOK,[8] the temperature was 24°C and QNH[9] 1014 hPa.
The ATSB obtained Bureau of Meteorology weather observations for Bankstown Airport taken at 1-minute intervals, which showed:
at 1328, the wind was 278° T (true) and 265° M (magnetic) at 18.1 kt
at 1329, the wind was 269° T (256° M) at 18.1 kt
at 1330, the wind was 270° T (257° M) at 16.9 kt.
The operator’s alternate chief pilot, who was also instructing that day, had cancelled their flights as they assessed the weather to be challenging for their student’s experience level and the environmental conditions would have likely not resulted in useful learning for them.
Operational information
The operator advised the ATSB that their normal pre-landing checks in the Robinson R22 Beta, performed on the downwind leg of the circuit, included the following:
warning/caution lights – out
rpm (engine and rotor) – in the green
temperatures and pressures – in the green
fuel – sufficient for go around
battery – charging
carburettor heat – on
hatches and harnesses – secure.
Wreckage information
The helicopter wreckage was contained within a relatively small accident site, with only minor wreckage spread and limited forward projection of debris. This indicated that the helicopter impacted the car and ground with a low forward speed. There was no post‑impact fire. The ATSB’s wreckage examination found that:
there was sufficient fuel on board the helicopter to sustain continued engine operation
damage identified in the main rotor system was consistent with low energy flight, as also indicated by the dashcam and the observed spread of the wreckage
there was no evidence of pre-existing defects with the flight control system
the pitot system was checked and considered to be serviceable prior to the collision with terrain
inside the aircraft, the key switches were found in the following positions:
fuel selector – on
fuel mixture – rich
carburettor heat – on
master switch – off
magnetos – off
A witness to the accident confirmed that they had switched the master to the off position to secure the helicopter and make it safe. The ATSB was unable to establish how the magnetos came to be in the off position.
It was determined by the ATSB that the engine was intact, and all components were present. Examination of the engine by the ATSB on site identified an absence of physical damage expected of an engine that was operating (rotating) at the time of impact with terrain. The engine examination also found:
Evidence of an exhaust gas leak between the exhaust riser mount flange/exhaust gasket surfaces of the no 4 cylinder. The leak was attributed to deformation of the flange that created space between the flange and the gasket (Figure 3). This leak was located directly above the carburettor heat intake scoop opening.
Deposits of exhaust gas products were present on the no 2 and no 4 cylinder ignition leads that were routed beside the no 4 cylinder exhaust riser.
Figure 3: Exhaust leak found during the onsite inspection
Source: ATSB
Survivability information
First responders and witnesses stated that the instructor and student had their seatbelts on. Neither of them was wearing a helmet and nor were they required to.
Further investigation
To date, the ATSB has:
examined the wreckage and other information from the accident site
obtained operator procedures
conducted interviews with the student, witnesses and other involved parties
reviewed the pilot records
reviewed the helicopter maintenance records
examined the dashcam video
reviewed air traffic control communications.
The investigation is continuing and will include:
an analysis of the audio signatures captured by the dashcam video
further analysis of physical evidence including the exhaust system components retrieved from the accident site
a review of the PIC’s experience performing autorotations in all helicopter types and specific to the Robinson R22 Beta
a review of both the helicopter manufacturer and operator’s procedures for conducting autorotations.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Bankstown Helicopters was operated under Civil Aviation Safety Regulation Part 141 as an approved flight training organisation based at Bankstown Airport, New South Wales.
[2]Circuits: a circuit is the specified path to be flown by aircraft operating in the vicinity of an aerodrome. It comprises upwind, crosswind, downwind, base and final approach legs. It creates an orderly flow of traffic from take-off to landing and assists pilots with positioning the aircraft on final at the appropriate altitude and distance from the landing area to make a stabilised approach.
[3]Following on the controls: it is common for students to learn by having their hands and feet on the controls while the instructor manipulates them. This can help students to learn how much input to use for certain controls and when they are appropriate. Students have their hands on the controls but are not making inputs.
[4]Autorotation: is a condition of descending flight where, following engine failure or deliberate disengagement, the rotor blades are driven solely by aerodynamic forces resulting from rate of descent airflow through the rotor. The rate of descent is determined mainly by airspeed.
[5]Flaring: the final nose-up pitch of a landing helicopter used to reduce the rate of descent and forward airspeed to about zero at touchdown, it can also increase the rotor RPM during an autorotation.
[7]Automatic terminal information service (ATIS): provides routine airport and weather information to arriving and departing aircraft by means of continuous and repetitive broadcasts. ATIS information is prefixed with a unique letter identifier and is updated either routinely or when there is a significant change to weather and/or operations.
[8]Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
[9]QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean sea level.
Occurrence summary
Investigation number
AO-2025-059
Occurrence date
03/10/2025
Occurrence time and timezone
13:30 Australian Eastern Standard Time
Location
Bankstown Airport
State
New South Wales
Report release date
17/12/2025
Report status
Preliminary
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R22 Beta
Registration
VH-RDL
Serial number
1498
Aircraft operator
Bankstown Helicopters Pty Limited
Sector
Helicopter
Operation type
Part 141 Recreational, private and commercial pilot flight training
Activity
General aviation / Recreational-Instructional flying-Instructional flying - dual
An ATSB interim report details the sequence of events leading to and following a bulk carrier’s loss of propulsion in a channel when departing Port Hedland.
The ongoing investigation’s interim report notes that the 327-m Singapore-flagged bulk carrier FMG Nicola departed its berth at Port Hedland early in the afternoon of 7 February 2025, fully laden with iron ore.
The ship was conducted out of the harbour by two harbour pilots, and four tugs were secured to assist.
About an hour into the ship’s transit of Port Hedland’s single shipping channel, travelling at about 8.3 knots with two tugs still secured and a third nearby, the ship’s main engine suddenly shut down.
The pilot informed the tug masters of the propulsion loss and directed them to help keep the ship in the channel. The pilot then notified vessel traffic service of the emergency and requested additional tugs.
“Over the next half hour, the ship neared the western, and then the eastern side of the channel, before travelling along the channel’s eastern edge as it slowed gradually,” ATSB Chief Commissioner Angus Mitchell said.
“During this sequence, four more tugs joined the three already attending, and the pilots and tug masters collectively worked to keep the ship inside the channel.”
Meanwhile, the ship’s engineers identified the engine had shut down due to a faulty switch monitoring the main engine’s lubricating oil pressure. After confirming all engine systems were operating normally, the trip lockout system was reset, and the engine was restarted at dead slow ahead.
About 35 minutes after the shutdown, the ship had been moved away from the channel side, and its main engine speed had progressively been increased to full ahead.
The tugs continued escorting the ship out of the channel towards open water, and the ship then continued its passage to Dongjiakou, China.
During the passage to China, the crew inspected all ballast tanks on the ship’s starboard side and found no physical damage.
Later inspections, including an underwater survey by divers, found no evidence of damage and that the hull paint was intact.
Mr Mitchell noted that the investigation is ongoing, but that the ATSB had released the interim report to provide timely information to industry on its progress to date.
“As it progresses the ATSB investigation will include examination and analysis of the collected evidence, including the event sequence, corroborating data, ship track and position, and the response to the incident,” he said
The investigation will also look further into the reporting of the incident to authorities.
“A full report of the incident did not reach the ATSB at the time of the occurrence, and the ATSB only became aware of its potential seriousness after media reporting in July 2025 suggested FMG Nicola had grounded while departing Port Hedland on 7 February,” Mr Mitchell said.
On the morning after the incident, the interim report details, the ship’s local agent submitted the appropriate incident reports, including to the Australian Maritime Safety Authority’s local office in Port Hedland.
“The notifications submitted by FMG Nicola’s master via the agent regarding the loss of propulsion incident did not, at that time, reach the ATSB,” Mr Mitchell noted.
A final report, to be released at the conclusion of the investigation, will detail the ATSB’s analysis and findings.
“The features of the Port Hedland channel make the risks associated with channel blockage high,” Mr Mitchell concluded.
“A disabled ship can strand on a receding tide as well as blocking the passage of other ships. Depending on departure times, separation between ships and the location of an incident, up to 3 additional ships could be committed to, or within, the channel and exposed to this hazard at a given time.”
The ATSB is investigating an engine failure during take-off involving a Rex Airlines Saab 340, VH-ZPN, at Adelaide Airport on 8 October 2025.
During take-off, the crew received abnormal left engine indications and rejected the take-off. During the rejected take-off, the left engine failed. The investigation is continuing.
The evidence collection phase of the investigation involved interviewing involved parties, examination of maintenance records, retrieving and reviewing recorded data, examining any recovered components, and the collection of other relevant information.
The ATSB has now commenced the examination and analysis of the initial evidence collected.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2025-060
Occurrence date
08/10/2025
Occurrence time and timezone
21:20 UTC
Location
Adelaide Airport
State
South Australia
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Engine failure or malfunction
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340B
Registration
VH-ZPN
Serial number
340B-384
Aircraft operator
Regional Express
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
The ATSB will investigate an engine failure on take-off incident involving a Regional Express Saab 340 aircraft at Adelaide this morning.
As reported to the ATSB, during the aircraft’s take-off roll for a scheduled flight to Broken Hill, the crew observed engine warnings for the left engine and aborted the take-off. During the aborted take-off procedure, the engine failed.
The aircraft subsequently vacated the runway and passengers and crew were able to disembark without further incident.
As part of the investigation ATSB investigators will review recorded flight data, interview the flight crew and other involved parties, and gather aircraft maintenance and other relevant records and documentation.
The ATSB asks anyone with video footage of the incident to make contact via the witness form on our website: atsb.gov.au/witness(Opens in a new tab/window) at their earliest opportunity.