A Cessna 182 struck trees while recovering from a dive after inadvertently entering low cloud, an ATSB investigation report details.
The Cessna 182T was being used for a private flight under visual flight rules from Emerald to Atherton, west of Cairns in Far North Queensland, with a pilot and passenger on board, on the morning of 16 June 2025.
About two hours into the flight the pilot decided due to cloud and reduced visibility to divert to Mareeba which, while further away than Atherton, was at a lower elevation.
Over the next 35 minutes, the pilot made multiple heading and altitude adjustments to avoid weather and higher terrain.
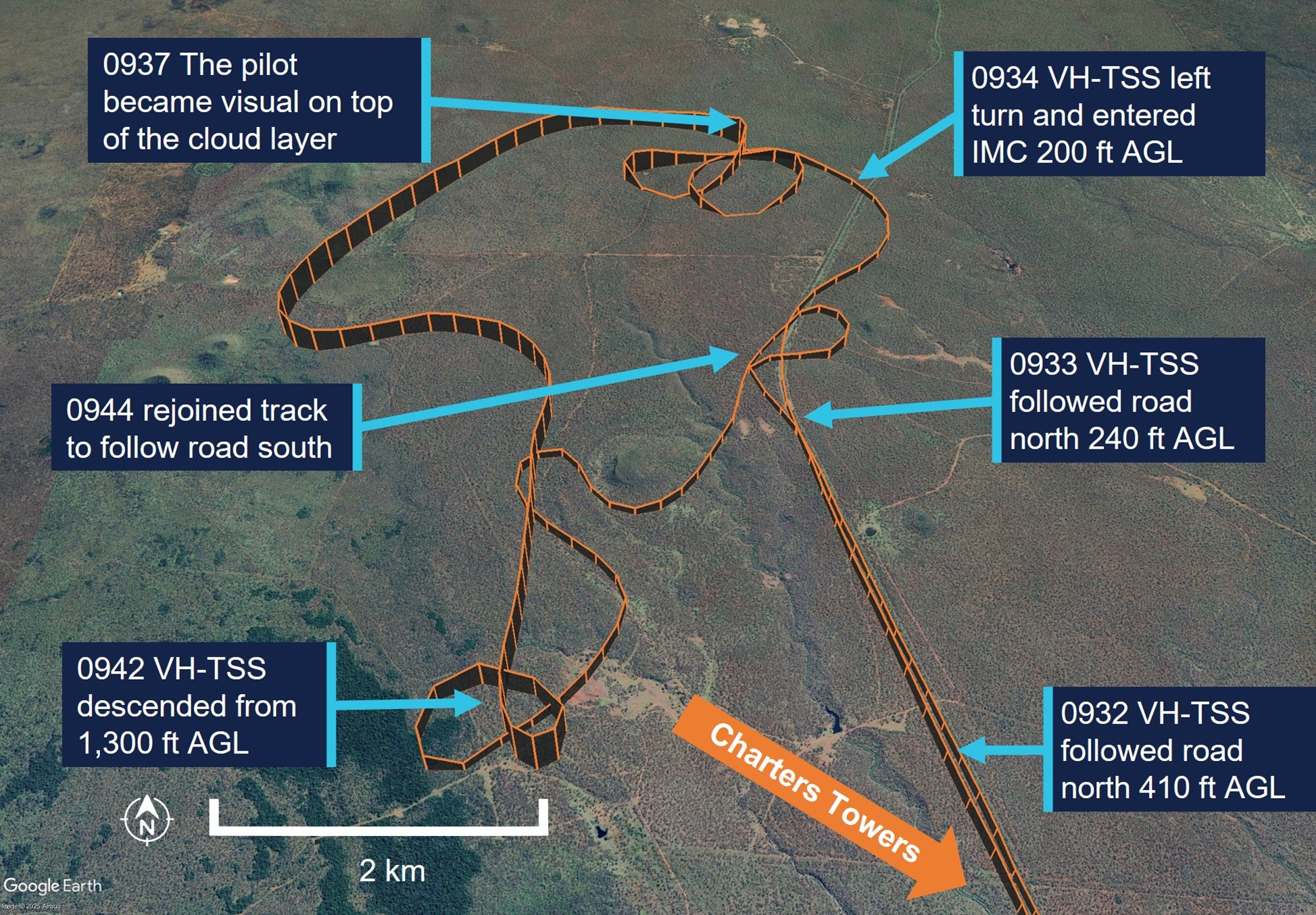
Near Mt Surprise, the pilot began following a road, flying about 530 ft above ground level, due to a low cloud ceiling and their belief the road usually avoided areas of highest terrain.
“A few minutes later the pilot lost sight of the road and reported sudden ‘white-out’ conditions ahead,” ATSB Director of Transport Safety Dr Stuart Godley explained.
“Aiming to avoid the cloud, the pilot began to turn and reduced engine power, but the aircraft entered cloud while about 200 ft above ground level, and tracking towards rising terrain.”
Recorded data indicated the aircraft conducted a full 360° left turn with several changes in altitude, and came close to terrain, before the pilot engaged the autopilot.
“Using the autopilot, the pilot then commanded a 180° left turn in an attempt to exit cloud. But, as the aircraft climbed, its airspeed dropped and it likely stalled, leading it to rapidly descend in a dive.”
In response to a terrain proximity warning from the aircraft’s Garmin G1000 avionics system the pilot immediately applied stall recovery actions, applying right rudder and attempting to level the aircraft as it descended almost to ground level.
The pilot reported becoming momentarily visual and hearing the aircraft impact trees.
After pulling back on the control column and commencing a climb, the aircraft again entered cloud. However, using the aircraft instruments the pilot was able to maintain control and became visual again on top of the cloud layer and, with the aircraft substantially damaged, diverted to Charters Towers.
The aircraft was following a road before entering cloud.
Dr Godley said the investigation found that the pilot’s pre-flight planning was not adequate for the intended flight.
“During pre-flight planning the pilot obtained weather for the destination but not for the planned track,” he said.
“Had the pilot obtained the area forecast this likely would have influenced their decision to commence the flight, or to plan an alternate route.”
Citing the ATSB’s Aviation Occurrence Database, Dr Godley noted 108 occurrences where pilots flying under visual flight rules entered instrument meteorological conditions that were reported to the ATSB in the last 10 years. Of these, 14 resulted in accidents, causing 23 fatalities.
“Given the aircraft struck trees while exiting a dive, the pilot and passenger were incredibly fortunate to avoid a catastrophic outcome,” he said.
“It is the nature of flying under visual flight rules that pilots will not always be able to reach their planned destination.
“Making an early decision to land or divert and to resist the urge to ‘press on’ may prevent flight into marginal weather conditions and ultimately disaster.”
An Air Tractor’s flight path was under two consecutive powerlines when it turned to the right and collided with terrain while spraying on South Australia’s Eyre Peninsula, an ATSB preliminary report details.
In the early afternoon of 8 September 2025, the single-seat Air Tractor AT-802A, operated by Aerotech Australia, had been spraying two fields on a property north of Cummins,the ATSB’s preliminary report from the ongoing investigation of the accident explains.
The report details the positioning of electrical powerlines about 12 m above the ground in both fields, and the poles supporting them, and how the recorded data indicates the pilot typically navigated them.
“Data from the spray runs conducted on the day of the accident showed the pilot flew mostly under the powerlines when they ran perpendicular to the spray passes,” ATSB Chief Commissioner Angus Mitchell said.
“The pilot occasionally flew over a powerline where there was a power pole, or where a wire ran adjacent to, or merged close to the edge of a field.”
The report notes the field being sprayed featured a north-south powerline, which the pilot primarily flew under, and a west-south-west powerline.
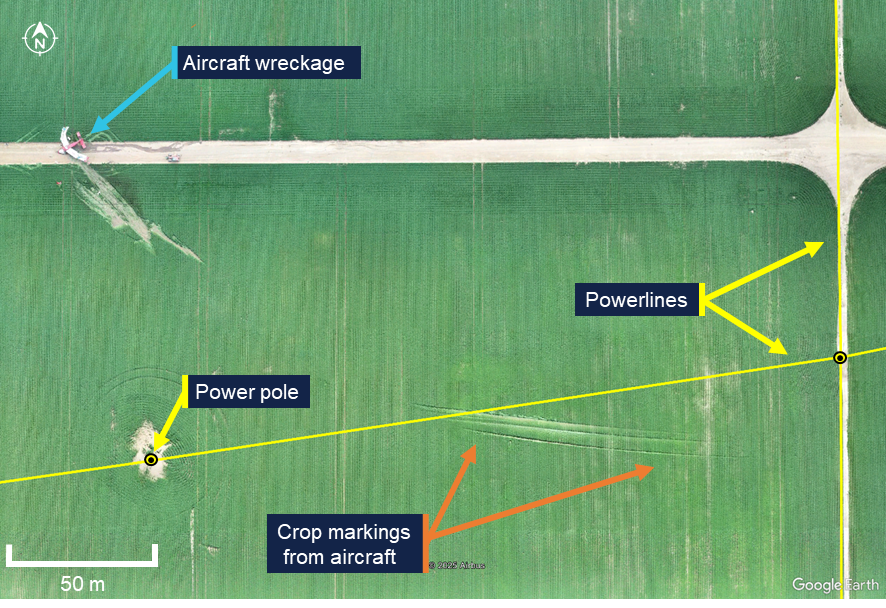
“On the accident spray run, as the pilot flew in a westerly direction under the north-south powerline, the aircraft was tracking towards a pole which supported the west-south-west powerline, about 240 m away,” Mr Mitchell said.
“Recorded data from the flight showed the pilot conducted a right turn underneath the second power line after which the aircraft collided with terrain.”
The collision activated the aircraft’s emergency locator transmitter, alerting the Joint Rescue Coordination Centre, which in turn contacted Airservices Australia and the operator.
Personnel from the operator and a local farm worker responded and found the aircraft wreckage about 15 minutes after the accident. The pilot was fatally injured and the aircraft was substantially damaged. There was no fire.
Examination of the accident site and wreckage by ATSB transport safety investigators found the aircraft had dragged a main wheel, spray boom and wingtip through the crop just prior to the impact with terrain. Numerous indicators such as debris locations and damage signatures to the airframe indicated the aircraft impacted terrain in an inverted orientation.
The report notes there was no evidence of pre-impact defects with the flight controls or aircraft structure.
As well as onsite activities, Mr Mitchell said ATSB investigators have also conducted interviews, collected documentation, and begun the analysis of recovered recorded data from the aircraft.
“As the investigation progresses, we will continue to examine several sources of recorded data, and review and analyse aircraft documentation and operational records, as well as the pilot’s medical records, qualifications and experience,” he said.
“The investigation will also consider aerial application standard practices and safety equipment.”
The ATSB will release a final report, which will detail findings and the analysis to support them, at the conclusion of the investigation.
Subsection 49(2) notice for incident in the Perth Protection Zone, Western Australia, between 31 July and 1 August 2021
The ATSB received a report that between 31 July and 1 August 2021, in the Perth Protection Zone, Western Australia, submarine cables on the seabed were damaged by a vessel dragging its anchor across the cables.
Based on the information available, the ATSB did not conduct an investigation.
For the purpose of subsection 49(2) of the Transport Safety Investigation Act 2003 (Cth) (TSI Act), I declare that any on-board recordings (as defined under section 48 of the TSI Act) (OBR) made in relation to the reported incident are not to be treated as OBR on or after 14 October 2025.
The ATSB is investigating the grounding of RSV Nuyina, off Heard Island, on 13 October 2025.
While operating off the coast of Heard Island in the Indian Ocean, RSV Nuyina contacted the seabed, resulting in damage to the ship’s retractable drop keel. The drop keel was retracted successfully and the ship relocated to safe water. The investigation is continuing.
The ATSB has commenced the examination and analysis of the initial evidence collected.
To date, the ATSB investigation has included:
interviewing the involved crew
examining available closed-circuit television (CCTV) of the occurrence
analysis of the voyage data recorder and received AIS data
examination of safety management system procedures
analysis of recorded survey data
analysis of local hydrographic data.
A review of the evidence collected to date has resulted in the investigation's scope being upgraded to the Defined level (the ATSB's different levels of investigation are detailed here).
The ATSB released a preliminary report, which details factual information established in the investigation’s early evidence collection phase, on 17 March 2026. See below.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Preliminary report
Report release date: 17/03/2026
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
Early on the morning of 12 October 2025, the research and supply vessel (RSV) Nuyina arrived off Heard Island (Figure 1) with 37 marine crew and 85 expeditioners on board, following a voyage from Casey station, Antarctica. The purpose of the visit was to support field science operations on the island as part of the Australian Antarctic Program’s (AAP) first voyage of the 2025–2026 Antarctic season, which also included visits to Casey and Davis stations in Antarctica.
During that first day, the crew carried out drills practising watercraft operations and conducted scientific operations using remotely piloted aircraft (RPA) on the north-west side of the island. After completion of these activities, Nuyina moved away from the coast and conducted planned bathymetric mapping operations overnight in an area to the east of Spit Bay (Figure 1). These survey operations were conducted using scientific acoustic instruments, including a high resolution multi‑beam echo sounder (MBES) mounted on one of the ship’s drop keels.[1]
Figure 1: Heard Island, seen from the east with Spit Bay to the right
Source: Dave Lomas, Helicopter Resources/AAD
Depth information from the MBES was received and processed by the ship’s scientific systems, with a dedicated display on the bridge also showing this information. This depth information could not be displayed on the electronic chart display and information system (ECDIS) or be used to generate navigational alarms.
The ship’s navigational echo sounders, which were the normal source of water depth information for the bridge crew, were switched off to prevent interference with the ship’s scientific acoustic instruments such as the MBES.
The plan for daytime operations for the following day included landing personnel ashore by helicopter, bathymetric surveys in nearshore waters using inflatable rubber boats[2] and aerial surveys using RPA.
RPA operations
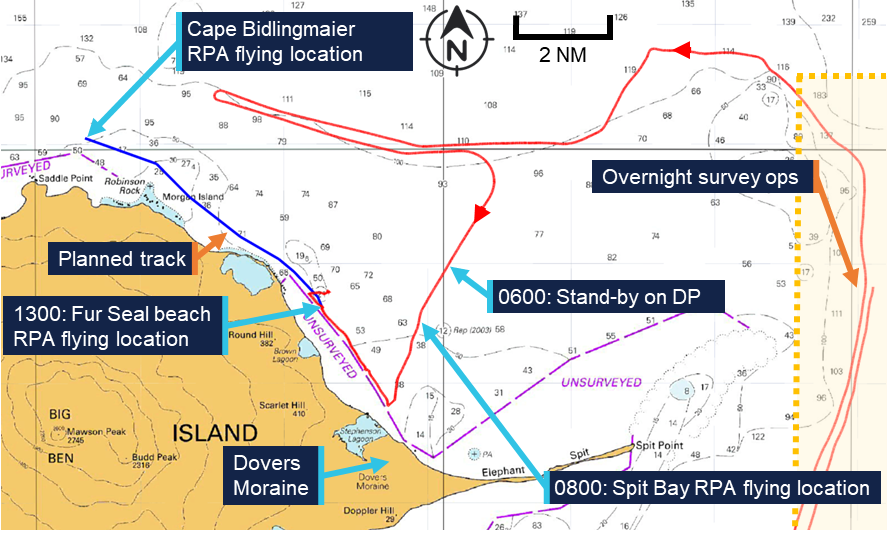
After completing overnight survey operations, Nuyina arrived at a holding position 5 miles[3] north of Dovers Moraine (Figure 2) at 0600 local time on 13 October. The bridge team engaged the ship’s dynamic positioning (DP) system[4] in auto-DP mode to maintain position while waiting for the weather to improve.
At about this time, the planned near-shore boat surveys and helicopter personnel-landing operations ashore were cancelled due to a change in the volcanic risk assessment.[5] The voyage management team then decided to focus on the scheduled RPA flights instead.
By about 0800, the weather had improved and Nuyina was moved closer inshore to a position in Spit Bay (Figure 1), in water depths of about 30 m (Figure 2). The position was close enough to shore to allow for effective RPA operations while remaining clear of the ‘unsurveyed’ area marked on the chart.
While at this location, the drop keel was retracted from its lowest working position (3 m below the keel) to its highest working position, which left it protruding 750 mm below the keel. The MBES was left switched on and continued to provide depth information.
Figure 2: Section of navigation chart AUS 605 showing operations on 13 October 2025
Source: Australian Hydrographic Office chart 605, annotated by the ATSB
At that time, the master was on the bridge and coordinated with the science team, while the officer of the watch – the third officer – manoeuvred the vessel from the DP console. Between 0800 and 1030, the ship was holding position, with small moves made to allow for a better line of sight of the RPA. At 1030, the third officer switched the DP system to joystick mode[6] and moved in a north-westerly direction, using an electronic bearing line (EBL) bearing 321° on the ECDIS as a guide (Figure 3). At 1100, the third officer switched back to auto-DP mode, with the ship still moving slowly in the direction of the EBL.
At about 1200, the second officer took over the watch while the third officer left the bridge. The master also left the bridge but returned shortly after.
The second officer continued to move the ship to the north-west, parallel to, and outside of, the unsurveyed area using the EBL as a guide. From about 1300 onwards, the ship was stopped off Fur Seal beach and held in position for further RPA flights with the ship’s heading kept into the prevailing south-westerly wind to reduce load on the thrusters.
Grounding
At about 1430, the voyage leader (VL) requested the master move the ship from its location off Fur Seal beach to a location north of Cape Bidlingmaier (around 5 miles to the north-west along the coast). The master understood that a track close to shore would be beneficial for continued RPA flights although the VL stressed that the RPAs could be retrieved if a route further away from the coast was required. The VL, master and second officer then discussed the new location while referencing the ECDIS screen. At the time, the chief officer and deck cadet were also on the bridge conducting other tasks but were not part of the bridge team.
Subsequently, the master informed the acoustics team by phone of their planned move and confirmed that the drop‑keel was still at a 750 mm extension below the ship’s nominal 9 m draft. The acoustics operator then prepared to start logging bathymetric data as the ship moved to the new location.
The master and second officer then discussed the route to the new location in more detail, after which the master constructed the route at the ECDIS planning station (located in the aft area of the bridge). The master then verified the route using the ECDIS checking functionality. After completing the route check, the master activated it for monitoring in the system.
At 1450, on request of the master, the second officer started a turn to starboard, while remaining in DP mode, from a heading of 200° toward 321° in preparation for the intended move to the new location. During this heading change, the increasing lateral and yawing forces as the wind moved from ahead to abeam and then to the port quarter resulted in an increased load on the ship’s thrusters. At 1456, the master instructed the second mate to disengage DP mode and start the transit on manual control. They briefly discussed the transit speed, with the master requesting a speed of 5 knots.
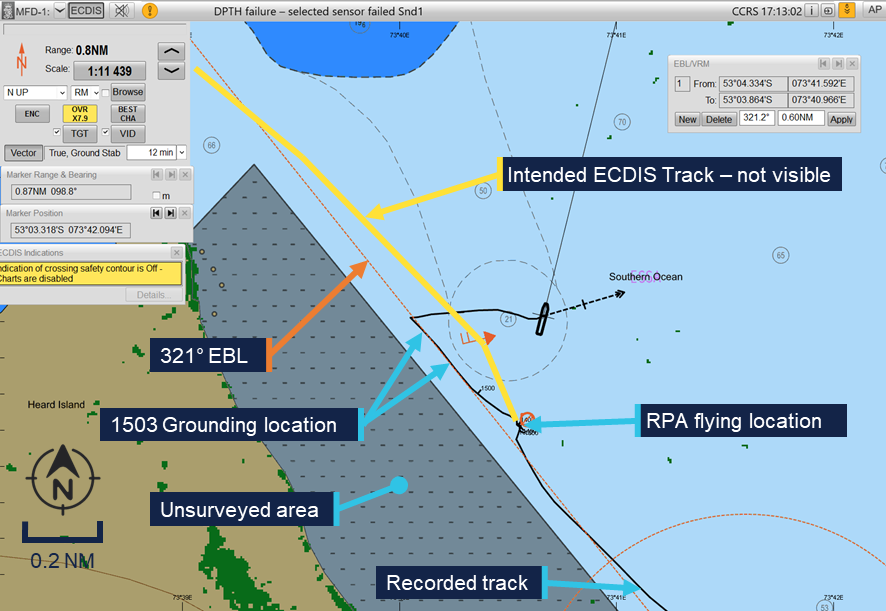
The second officer switched over to manual control and moved from the DP console to the helm controls forward. However, the planned route was not visible on the forward ECDIS. The master tried to correct this, while the second officer continued to track along the EBL which was still displayed on the ECDIS from the earlier manoeuvring and was set in a similar direction to the planned route. This track took the ship between the unsurveyed area to the west and a charted bank with an indicated depth of 21 m to the east (Figure 3).
Figure 3: ECDIS image showing planned track, EBL and grounding
Source: Serco, annotated by the ATSB
At 1500, the acoustics operator contacted the bridge by phone to confirm that the bridge MBES displays were showing the correct information. The master discussed the setup of the screens and asked for some changes. At that stage, the MBES display was showing a depth[7] of 15 m. At 1502, the master ended the call and ordered the engines dead slow ahead, immediately followed by ‘stop’, which was acknowledged and executed by the second officer. This was followed at 1503 by the order to go ‘dead slow astern’.
At about the same time, the acoustics operator noted the water depth was now indicating 13 m and that this only left 3.25 m between the MBES transducer in the deployed drop keel and the seabed. The operator called the bridge to warn of shallow water and this was acknowledged by the master who stated they were already ‘going astern’.
Nuyina then briefly grounded with the retractable drop keel initially impacting the seabed, followed by the ship’s hull.
Emergency response
Nuyina subsequently cleared the shallow water and started drifting towards the north‑east on the south‑westerly wind. The crew stopped the ship’s movement and held position in auto‑DP, assessing damage using the relevant emergency checklists.
The drop keel was retracted to its maintenance position for inspection while tanks and void spaces were sounded in accordance with the checklists.
No flooding was detected in any of the tanks or void spaces, but the drop keel was found to be substantially damaged, with mounted instruments damaged or missing. An inspection of the hull using a remotely operated vehicle (ROV) showed that damage to the hull was limited to scratches and paint damage, which was later confirmed by diving inspection after return to Hobart.
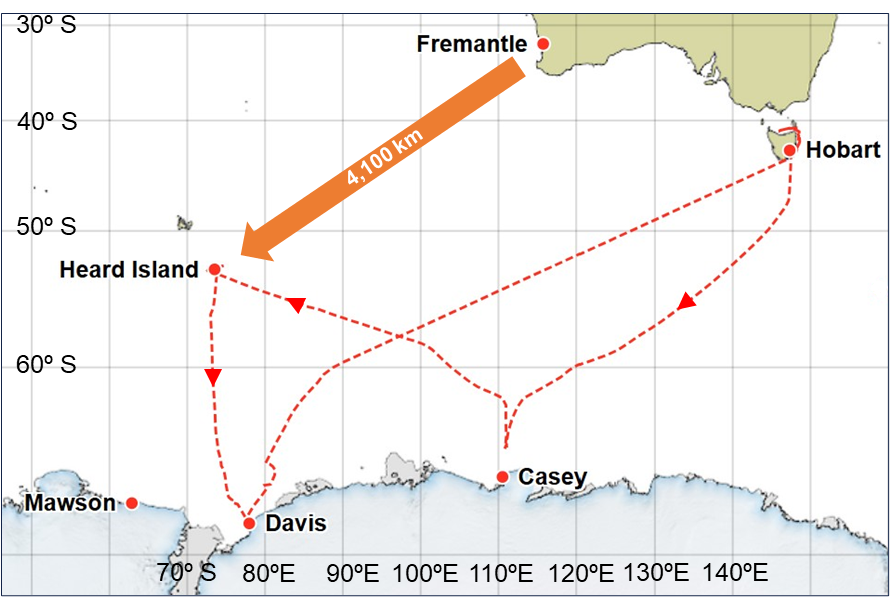
After reporting the grounding and consulting with relevant authorities and experts ashore, including the Australian Maritime Safety Authority and the ship’s classification society,[8] Lloyds Register, it was concluded that the ship could continue its operations at Heard Island as well as the scheduled resupply operations at Davis station in Antarctica before returning to Hobart, Tasmania (approximately 3,800 miles total).
Context
Nuyina
Nuyina was built by Damen Shipyards in Romania and the Netherlands as the primary research and supply vessel for the Australian Antarctic Division (AAD). The ship was owned by the AAD and managed by DMS Maritime (Serco). Nuyina was classed with Lloyd’s Register and built to the polar class 3 (PC3) standard.
As the ships manager, Serco was responsible for the day-to-day management of Nuyina. It employed the ship’s marine crew, provided technical management and was responsible for regulatory compliance.
Propulsion system
Nuyina was equipped with twin controllable pitch propellers (CPP) each driven by a MAN 16V32 main diesel engine of 9,600 kW. Alternatively, each propeller could be driven by an electric drive for a service speed up to 12 kt or by combining electrical drive and diesel engines for additional capability when engaged in icebreaking operations. When using the electric drives for transits or in DP mode, power was supplied by the ship’s diesel generators, and the main engines could be shut down.
In addition to its propellers, Nuyina was equipped with 3 tunnel thrusters at the bow and 3 at the stern which provided lateral thrust when operating in DP mode and when manoeuvring at slow speed.
On the day of the occurrence, Nuyina was operated with the CPPs engaged in electric drive mode, both during transits and while in DP.
Bridge equipment
Nuyina was fitted with navigational equipment required by the International Convention for the Safety of Life at Sea (SOLAS)[9] for a ship of its size and operations. Navigation equipment included a Kongsberg K-Bridge integrated bridge system which combined the input of various sensors and incorporated the functions of the Electronic Chart Display Information System (ECDIS), radar and autopilot using multi-function displays. To satisfy SOLAS requirements for the carriage of navigational charts, Nuyina was equipped with a dual ECDIS displaying approved electronic navigational charts.
Nuyina was equipped with a Consilium MK2 voyage data recorder (VDR). The VDR recorded bridge audio, screenshots of the ECDIS and radar displays as well as navigation and engineering parameters. VDR data relevant to the investigation was obtained by the ATSB.
Nuyina was equipped with a Kongsberg KPOS-21 DP system, which uses a combination of position and heading reference systems to provide station and track keeping capabilities using the ship’s main propulsion and rudders as well as the 6 tunnel thrusters. The DP system was class certified as DP 2, which – in certain defined configurations – guaranteed a level of redundancy, allowing the ship to stay under DP control in case of the complete failure of any single active component.
Safety management system
Serco had implemented a safety management system (SMS) as required under the ISM code.[10] This SMS consisted of policies, procedures and manuals covering different aspects of the ship’s operation and included a:
safety management manual
Nuyina operating manual
navigation manual
science operations manual.
The science operations manual provided information for the master and crew about the scientific equipment on board Nuyina. It included procedures for the operation and maintenance of scientific equipment, introduced relevant supporting checklists and outlined how Serco expected research operations to be carried out.
Acoustic equipment
As part of its navigational equipment, Nuyina was fitted with 2 class-approved dual‑frequency echo sounders, which also incorporated doppler speed logs. The Nuyina operating manual stated that: ‘An echo sounder must be always running …’.
To support science operations, Nuyina was fitted with a suite of acoustic subsea sensors including 2 MBES, operating on various frequencies. The echo sounders included in the suite of science instruments were not intended or approved for navigation use, though a dedicated display was provided on the bridge as an additional source of information.
To prevent interference when using multiple instruments simultaneously, a synchronisation trigger system was fitted to optimise and deconflict acoustic sensor use. However, the navigational echo sounders were not included in this system, and the science operations manual noted that:
The navigation echosounders must be turned off while the science echosounders conduct measurements.
Crew
Nuyina had 37 marine crew and 85 expeditioners on board at the time of the occurrence.
The 85 expeditioners included staff bound to or from Antarctic research stations, voyage management staff and science and logistics personnel. They were considered ‘special personnel’[11]under the Navigation Act 2012.
The 37 marine crew reported to the master through their respective department heads while the expeditioners reported to the AAD ‘voyage leader’ (VL). The master had the final authority over matters of safety on board the ship.
All marine crew had joined the ship during its port call in Hobart, Tasmania, between 17 and 19 September 2025.
Master
Nuyina’s master held a valid Australian master’s certificate of competency, with about 35 years of experience at sea, of which approximately 25 years involved working in polar waters. They had served as master on board Nuyina’s predecessor Aurora Australis for 3 years and had been master of Nuyina since the ship’s delivery in 2021.
Second officer
The second officer held a valid Australian certificate of competency as officer in charge of a navigational watch. They had about 14 years of experience at sea, working as second and third officer for a total of 10 years. They had first joined Nuyina as third officer during the ship’s construction in 2020.
Australian Antarctic Program
The Australian Antarctic Program (AAP) was established in 1947 as the Australian National Antarctic Research Expeditions. The program comprised a range of activities, interests and capabilities, including scientific research, logistics, transport and administration of the Australian Antarctic Territory.
The Australian Antarctic Division (AAD) is a division of the Australian Government’s Department of Climate Change, Energy, the Environment and Water, based in Kingston, Tasmania, and it leads, coordinates and delivers the AAP.
Australia maintains 3 year-round research stations in Antarctica – Casey, Davis and Mawson – and one sub‑Antarctic station on Macquarie Island. The population at each station varies between 40 and 100 expeditioners over summer, and between 15 and 20 over the winter months. The AAD utilises air and sea transport to get expeditioners to and from the research stations.
Flights carrying passengers and cargo operate from Hobart, Tasmania, to Wilkins Aerodrome, near Casey station, each summer and smaller fixed wing aircraft and helicopters enable travel within the continent. However, shipping is the primary means by which personnel, equipment, fuel and supplies are transported to and from Antarctica. In addition, ships are used as platforms to conduct scientific research as well as coastal and sub-sea surveys.
2025 Voyage 1
RSV Nuyina was conducting the AAP’s first voyage of the 2025–2026 Antarctic season (Figure 4), with a planned itinerary including helicopter operations at Casey station, a scientific field campaign on and around Heard Island followed by over-ice supply operations at Davis station.
The Heard Island campaign was the AAP’s first dedicated environmental management visit to Heard Island in more than 20 years. It included planned landings by scientists, using helicopters and small craft to check on the state of the island’s unique flora and fauna as well as small scale ROV operations and mapping the bathymetry around the island.
Figure 4: Voyage 1 overview
Source: AAD, modified by the ATSB
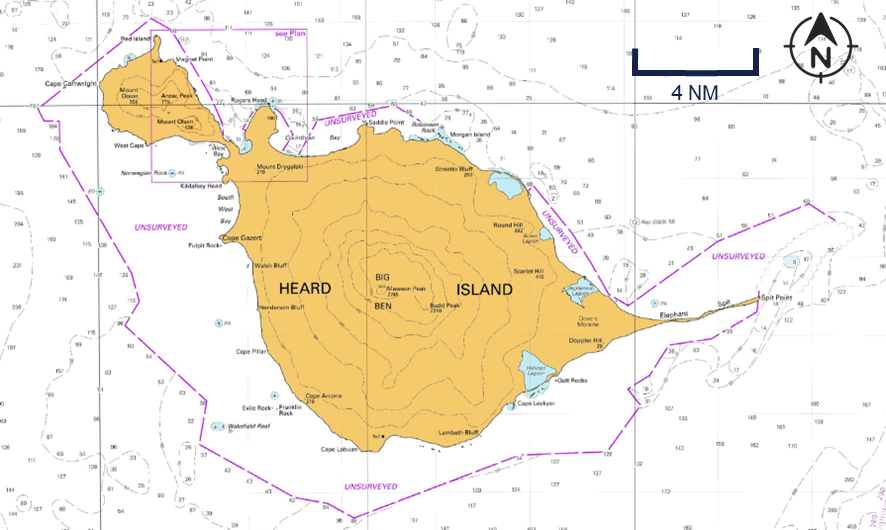
Heard Island
Heard Island (Figure 5) is part of the Australian external territory of Heard Island and McDonald Islands. Located in the Southern Ocean about 4,100 km south-west of Fremantle, Western Australia, it is home to Australia’s only active volcano, as well as 12 major glaciers. It is uninhabited by humans. The island is home to penguin and seal colonies dotting the coastline, as well as an important breeding location for Southern Ocean seabirds. The island’s location at a latitude of 53° south exposes it to persistent strong westerly winds with precipitation and poor visibility common year-round.
Due to the island’s remote location and low volumes of shipping traffic, the waters around Heard Island have not been systematically surveyed. Instead, charts are based on limited data available from passage soundings, mostly obtained by earlier expeditions by the AAP and its predecessors. The charted soundings for the area around Spit Bay were based on data from passage soundings obtained in 1948 and 1990 as well as from a more comprehensive 1999 survey.
In electronic navigational charts, information to evaluate the relative accuracy of the chart data is provided by assigning a ‘category of zone of confidence in data’ (CATZOC). Areas of the chart are assigned to one of 6 categories and allocated a CATZOC value (A1, A2, B, C, D and U). The area around Heard Island (including the location of the ship’s grounding) was assessed in the lowest assessed category (CATZOC D), indicating poor seafloor coverage and accuracy where large depth anomalies may be expected. Additionally, extensive coastal areas were marked as ‘unsurveyed’ with no depth information presented.
Figure 5: Section of navigation chart AUS 605 showing Heard Island
Source: Australian Hydrographic Office, modified by the ATSB
Safety actions
Following the incident Serco and the AAD implemented several safety actions:
New measures addressing the hazards of operations in low CATZOC areas were introduced including the development of a detailed risk assessment, revision of the master’s standing orders to prioritise use of the navigational echo sounders and the use of the science tender to support mapping operations.
A review of passage planning processes in the SMS, including the navigation manual, procedures and supporting forms. This also included instructions on ECDIS management and troubleshooting as a specific procedure.
The development of a Heard and McDonald Islands navigation decision support guide and the acquisition of sufficient multi beam data to identify safe transit corridors around Heard Island.
Further investigation
To date, the ATSB has:
interviewed key personnel
recovered and examined recorded data
recovered and reviewed CCTV footage
obtained operational documentation
obtained historic and recorded bathymetric data.
The investigation is continuing and will include further review and examination of:
operator procedures
recorded data
bathymetric data.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Nuyina was equipped with 2 retractable drop keels, which allowed scientific instruments to be lowered up to 3 m below the keel to reduce hull interference, be retracted to avoid damage in ice and be recovered on board for servicing.
[2]Nuyina could also carry a dedicated science tender; however, this was not embarked for this voyage.
[4]Dynamic positioning is a vessel capability where a set heading and position can be maintained by an automated system controlling the vessel’s rudders, propellers and thrusters.
[5]Heard Island is home to Australia’s only active volcano. The volcanic risks to aircraft and landing parties were assessed by geologists in Kingston, Tasmania, where the Australian Antarctic Division is headquartered, based on observations from the ship.
[6]In joystick mode the operator could manually control heading and/or selected longitudinal or transverse axis of motion using a joystick integrated in the DP system.
[7]The displayed MBES data was shown as total water depth and to obtain the under-keel clearance the draft of the ship had to be deducted.
[8]Classification societies are recognised organisations which are authorised to issue statutory certification on behalf of the flag State.
[9]International Maritime Organization, 2024, The International Convention for the Safety of Life at Sea (SOLAS) 1974, as amended, IMO, London.
[10]International Maritime Organization, 2018, International Management Code for the Safe Operation of ships and for Pollution Prevention (ISM Code) as amended, IMO, London.
[11]As defined in the Navigation Act 2012: ‘Special personnel’, in relation to a special purpose vessel means a person who is carried on board the vessel in connection with the special purpose of the vessel. They are not passengers or part of the ship’s crew.
Occurrence summary
Investigation number
MO-2025-011
Occurrence date
13/10/2025
Occurrence time and timezone
09:02 UTC
Location
off Heard Island, Territory of Heard Island and McDonald Islands
State
External Territory
Report release date
17/03/2026
Report status
Preliminary
Anticipated completion
Q4 2026
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Examination and analysis
Investigation status
Active
Mode of transport
Marine
Marine occurrence category
Grounding
Occurrence class
Serious Incident
Highest injury level
None
Ship details
Name
RSV Nuyina
IMO number
9797060
Ship type
Special-purpose vessel
Flag
Australia
Classification society
Lloyd's Register
Manager
DMS Maritime
Departure point
Casey Station, Australian Antarctic Territory
Destination
Heard Island, Territory of Heard Island and McDonald Islands
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 22 September 2025, at 1747 local time, the pilot of a Robinson R22 helicopter was conducting mustering operations on a cattle station near Century Mine, Queensland. Weather conditions were clear with a 10–15 kt wind from the south.
After a short stop in a designated take-off and landing location, in a dry creek bed to allow cattle to cross, the pilot commenced lift-off. The pilot reported that the wind conditions at this time became ‘quite gusty’.
While the helicopter was in the hover at 35 ft, the pilot observed a small limb of a nearby tree moving toward the helicopter in the wind. Attempting to avoid the tree limb, the pilot manoeuvred the helicopter to the left, however the tree limb contacted the tail rotor. The helicopter subsequently conducted two 360° spins and collided with a nearby wire fence, resulting in a roll over to the right (Figure 1). The helicopter was substantially damaged in the accident, with damage to the right skid, tail boom, main and tail rotor systems and fuselage. The pilot sustained serious injuries.
Figure 1: Damage to helicopter
Source: Operator
Safety message
Helicopter pilots conducting mustering operations will often conduct multiple landings for short durations for various reasons, such as allowing cattle to cross in this occurrence. Frequent monitoring of environmental conditions such as changing wind conditions is necessary to ensure a safe take-off, particularly in confined areas.
Although the site was familiar to the pilot, operations in confined areas present challenges and increased risks for operating crew. The physical characteristics of a confined area site not only increase the risk of controlled flight into obstacles but limit the options available to the pilot in the event of a loss of performance during critical phases of flight.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
The ATSB is conducting a safety study into aviation safety management systems.
A safety management system (SMS) is a systematic process-based approach to the management of risk. Within the aviation context, the implementation and operation of an SMS is widely credited with improvements in safety performance through effective risk-based decision-making. However, several recent systemic aviation investigations have identified significant issues associated with the implementation and utilisation of SMS functions.
The purpose of this study is to discover and document common deficiencies and system interdependencies with current SMS implemented in aviation. The results could be used to improve existing systems and enhance future guidance material.
A final report will be published at the conclusion of the study. Should any safety critical information be discovered at any time during the study, the ATSB will immediately notify operators and regulators so appropriate and timely safety action can be taken.
On the morning of 11 October 2025, a Piper PA-32R-300 Cherokee Lance, registered VH-JVA, commenced a take-off from runway 26 at Shellharbour Airport, New South Wales, for a private instrument flight rules flight to Bathurst Airport, with a pilot and 2 passengers on board.
After a ground roll of 410 m, the aircraft abruptly pitched up, yawed left and became airborne. The aircraft then climbed away from the runway in a nose high attitude while skidding and rolling left. It then followed a left-turning flight path and reached a maximum recorded altitude of about 50 ft above ground level (AGL) before it began descending. As the aircraft descended, it appeared to stall, the angle of bank increased, and the descent rate increased rapidly. The aircraft collided with terrain and came to rest at the threshold of the intersecting runway (runway 34). The pilot and passengers were fatally injured in the accident, and the aircraft was destroyed.
What the ATSB found
The ATSB found that during the take-off roll, the horizontal stabilator moved to a full, or near-full, nose up deflection and very likely remained in this position for the entire flight. The reason for the control deflection could not be determined.
The ATSB also found that at the time of the accident flight, required scheduled instrument and avionics maintenance inspections had not been completed. While not contributory to the accident, that reduced the assurance that these systems were functioning accurately.
What has been done as a result
In response, the aircraft maintainer advised that they had automated the tracking and alerting of aircraft maintenance requirements to ensure that all required items were completed.
Safety message
If not rapidly corrected, an uncommanded pitch up during take-off can lead to a stall and a loss of control. This is not a scenario typically included in training and a pilot confronted with this scenario faces an unexpected and challenging situation. If control cannot be quickly regained by pushing forward on the control column, engine power should be promptly reduced and control maintained as best as possible to attempt a landing.
Inspections of aircraft instruments and avionics are vital to ensure these systems operate correctly and present accurate and reliable information. While the overdue inspections did not contribute to the accident, pilots can be entirely reliant on these systems to ensure the safety of a flight. Therefore, both pilots and maintainers should ensure required inspections are completed prior to a flight.
Summary video
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the morning of 11 October 2025, a Piper PA-32R-300 Cherokee Lance, registered VH-JVA, taxied for a private flight from Shellharbour Airport to Bathurst Airport, New South Wales. The flight was being operated under the instrument flight rules1 with the pilot and 2 passengers on board.
At 0956 local time, as the aircraft approached runway 26, the pilot announced on the Shellharbour common traffic advisory frequency (CTAF) that the aircraft was entering the runway and lining up to depart. The pilot then taxied the aircraft onto the runway starter extension2, lined up and conducted pre‑take‑off checks and engine run ups. While VH‑JVA was lined up, a Cessna Caravan taxiing behind VH‑JVA stopped at the holding point at the runway 26 threshold. The pilot of VH‑JVA invited the pilot of the Cessna to depart ahead of VH‑JVA and the Cessna took off shortly after.
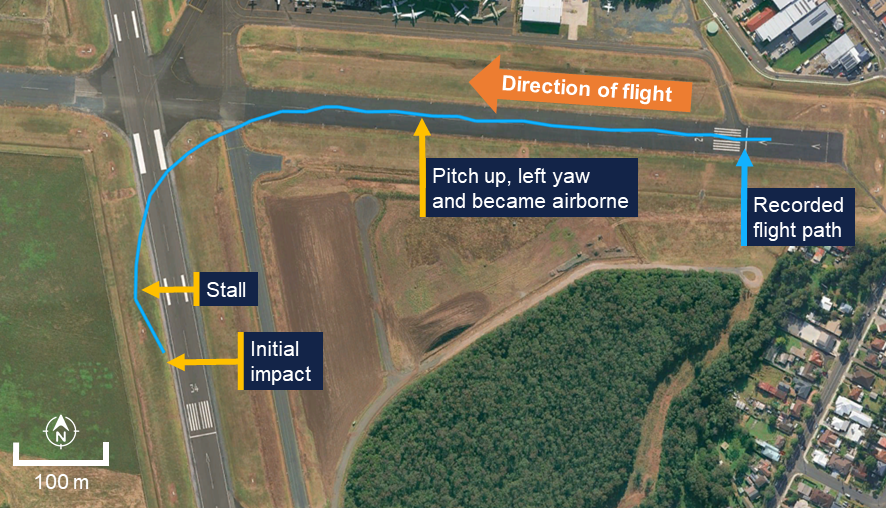
About a minute after the Cessna departed, VH-JVA began a take-off from runway 26. Following a ground roll of about 410 m, VH-JVA abruptly pitched up and yawed left as it became airborne. The aircraft then climbed away from the runway in a nose high attitude while skidding3 and rolling left (Figure 1 and Figure 2).
Figure 1: Composite image of recorded security camera footage of the flight
Source: Supplied, annotated by the ATSB
Figure 2: Composite image of recorded security camera footage of later part of the flight
Source: Shellharbour Airport, modified and annotated by the ATSB
The angle of bank then appeared to stabilise briefly as the aircraft followed a left-turning flight path (Figure 3). As it turned to a heading of about 200° magnetic (M), it reached a maximum recorded altitude of about 50 ft above ground level (AGL) and then began descending. Three seconds after reaching 50 ft AGL, the aircraft appeared to stall, the angle of bank increased, and the descent rate began increasing rapidly. As the descent rate increased, engine power reduced before the aircraft collided with terrain.
Figure 3: Flight overview
Source: Supplied, annotated by the ATSB
A post-impact fire commenced and the aircraft came to rest at the threshold of the intersecting runway (runway 34). The pilot and passengers were fatally injured in the accident, and the aircraft was destroyed.
Context
Pilot details
The pilot held a Private Pilot Licence (Aeroplane) and the required class rating and endorsements to operate the aircraft. The pilot also held a private instrument rating and Class 2 aviation medical certificate, which were both current at the time of the accident.
The pilot’s logbook was reported to be in the aircraft during the accident flight. However, the cabin area of the aircraft was extensively fire damaged following the accident and the logbook could not be located.
At the pilot’s last aviation medical examination, the pilot had declared a total of 1,015 hours of aeronautical experience. Maintenance release entries showed that since that medical examination, the pilot had flown 27.1 hours in the aircraft. Of these, 4.6 hours were in the 90 days before the accident and none in the 30 days before the accident.
The ATSB found no indicators that the pilot was experiencing a level of fatigue known to adversely affect performance.
Medical details
A review of medical records and post‑mortem examinations of the pilot and passengers identified no pre‑existing conditions that were likely to adversely impact their actions or behaviours. Similarly, the toxicological examinations did not identify any substances, including carbon monoxide concentration, that could have impaired the pilot’s performance or adversely impacted the passengers’ actions or behaviours.
Aircraft details
General information
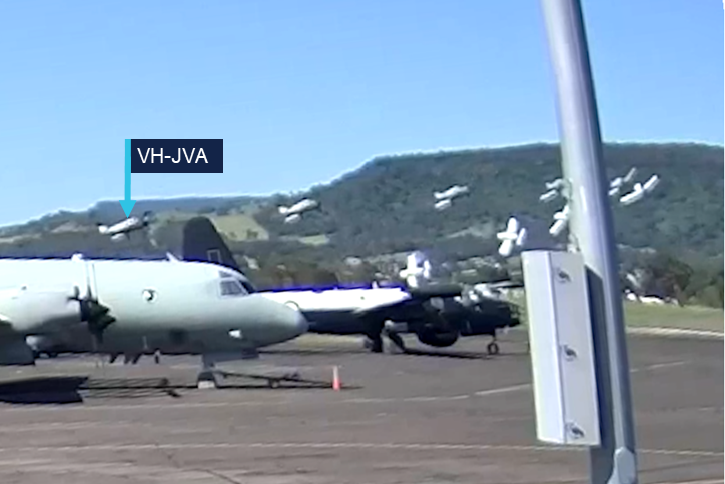
The Piper PA-32R-300 Cherokee Lance is a single-engine, low-wing, retractable-tricycle landing gear aircraft. The Lance is powered by a Lycoming IO-540 fuel-injected, horizontally-opposed piston engine driving a 3-blade, variable-pitch propeller. VH‑JVA (Figure 4), serial number 32R-7680030, was manufactured in the United States in 1975 and first registered in Australia in 1985. The maintenance release stated that the aircraft was approved for IFR, visual flight rules4 (VFR) night and VFR day operations.
Prior to the accident flight, the aircraft was last flown on 12 September 2025 and, at the completion of that flight, the aircraft had accumulated 3,915.5 hours total time in service. At the time of the accident, the engine had accumulated 2,043 hours in service since its last overhaul in 1991.
The aircraft was configured with 7 seats (all forward facing) and equipped with dual flight controls. The aircraft was not fitted with aileron trim and was equipped with a Century IIB autopilot, which incorporated a servo on the aileron control system only. In the event of a malfunction, the autopilot servo was designed to allow a pilot to manually override the system.
Figure 4: VH-JVA
Source: Clinton J Down Photography, modified by the ATSB
Horizontal stabilator
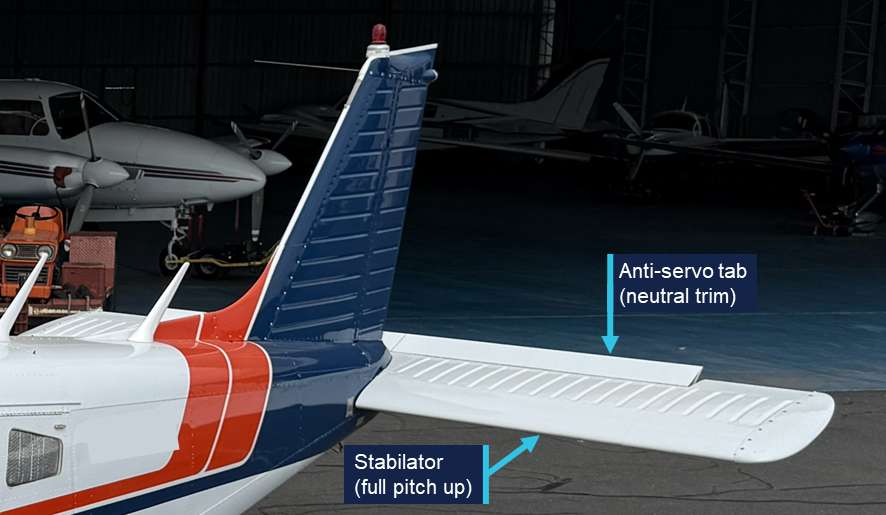
The aircraft was fitted with a horizontal stabilator (Figure 5), sometimes referred to as an all-moving tail. A horizontal stabilator is a fully movable aircraft horizontal stabiliser in which the entire horizontal tail surface is responsive to control column inputs.
Figure 5: Horizontal stabilator
The figure shows the stabilator of a representative Piper Lance (not VH-JVA). Source: ATSB
The stabilator was fitted with an anti-servo tab (Figure 6), a small, hinged surface set into the trailing edge of the stabilator. As the stabilator deflected from the trim position, the tab moved in the same direction, but further than the stabilator, to provide an opposing force.
Figure 6: Stabilator and anti-servo tab
The figure shows the stabilator of a representative Piper Lance (not VH-JVA). Source: ATSB
Maintenance
The aircraft was maintained in accordance with the Civil Aviation Safety Authority (CASA) maintenance schedule, which required a periodic inspection every 100 hours or 12 months, whichever came first. The CASA maintenance schedule for periodic inspections is divided into airframe, engine, electrical, instruments and radio sections. For aircraft operating only under the visual flight rules (VFR), these inspections could be certified by an ‘airframe’ licenced aircraft maintenance engineer (LAME). For IFR approved aircraft, the radio section contained additional requirements that could only be certified by a suitably-endorsed avionics LAME.5
The logbook for VH-JVA indicated that a periodic inspection had been completed on 14 May 2025 at 3,898.2 hours in service. However, the logbook entry by the aircraft’s current maintainer (who was not an avionics LAME) did not specify which elements of the maintenance schedule had been completed. Logbook entries for previous periodic inspections conducted by other maintenance organisations specifically noted where the VFR-required inspections had been completed, with a separate entry certifying the completion of the IFR requirements.
The current aircraft maintainer advised that all logbook entries reflected inspections and maintenance completed as specified in work packages.6 The maintainer also advised that for several aircraft, including VH-JVA, the completed work package documents had been inadvertently disposed of, or destroyed by recent flooding of their premises. Therefore, the ATSB could not verify which elements of the VFR maintenance schedule had been completed by the maintainer under their airframe licence. The instrument and radio system inspections for IFR flight (required to be certified by an avionics LAME) were not completed during the May 2025 inspection or at any subsequent time before the accident flight.
Further to the periodic inspections, CASA Civil Aviation Order (CAO) 100.5 General requirements in respect of maintenance of Australian aircraft set out additional maintenance requirements for specific systems that were not covered in the maintenance schedule. The aircraft logbook recorded the following CAO 100.5 instrument and radio inspections as being last completed on the dates listed in Table 1.
Table 1: CAO 100.5 instrument and radio inspections
Inspection item
Required frequency
Most recent logbook entry
Next inspection due (IFR flight)
Pitot-static systems
24 months
17 April 2023
17 April 2025
Pressure altimeters
24 months
17 April 2023
17 April 2025
Airspeed indicator
48 months
17 April 2023
17 April 2027
ATC transponder
24 months
17 April 2023
17 April 2025
CAO 100.5 allowed for time extensions of up to 60 days for compliance with these inspections (to 16 June 2025, except for the airspeed indicator). However, there was no record of these CAO 100.5 maintenance inspections being completed before the accident flight in October 2025.
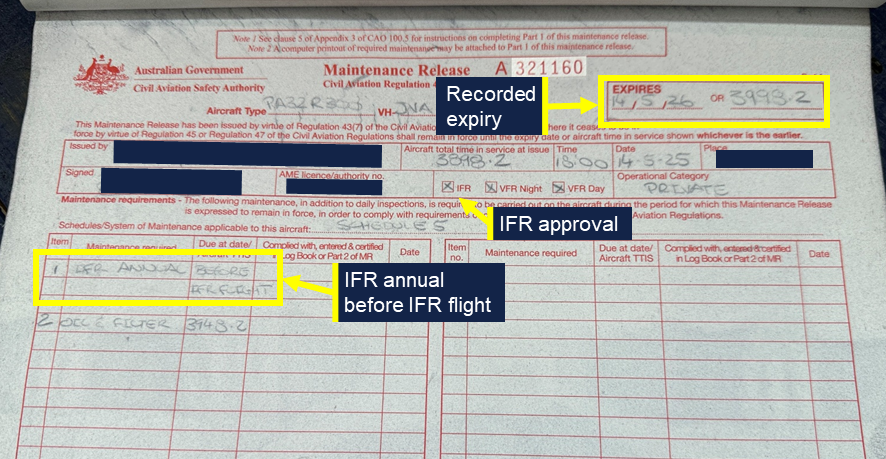
The aircraft’s original maintenance release was not found in the fire-damaged wreckage, but the ATSB viewed the carbon copy of the current maintenance release that was retained by the maintainer. The current maintenance release, issued by the maintainer, was endorsed for IFR operations and was recorded as expiring on 14 May 2026, or 3,998.2 hours in service, whichever occurred sooner (Figure 7).
Part 1 of the maintenance release included a section where any maintenance required within the validity period could be recorded. Any flight outside of the conditions endorsed in the maintenance release was not permissible until the required item had been addressed and certified by a suitably qualified person. The ‘Maintenance required’ section of the current maintenance release noted that an ‘IFR annual’ was required before IFR flight. This ‘IFR annual’ (IFR-required periodic inspections) was not completed before the accident flight. Additionally, the ‘Maintenance required’ section of the release did not contain any entry relating to the CAO 100.5 inspections required to be completed by 16 June 2025.
Figure 7: Maintenance release carbon copy
Source: Maintainer, annotated by the ATSB
Aircraft loading and take-off performance
The pilot and a passenger were in the 2 front seats while the other passenger was seated in the left seat of the second row. Witness statements and fuel records indicated that the aircraft departed with full tanks.
The purpose of the flight was an overnight stay at Bathurst before returning to Shellharbour the following afternoon. No large or heavy items were identified in the aircraft during the examination of the wreckage and the ATSB estimated the aircraft to be within weight and balance limitations for the flight.
The pilot’s operating handbook (POH) indicated that for the conditions of the accident take-off, the ground roll for a maximum performance take-off could be expected to be between about 260 m (flaps 25) and 365 m (flaps 0).
Impact and wreckage information
Overview
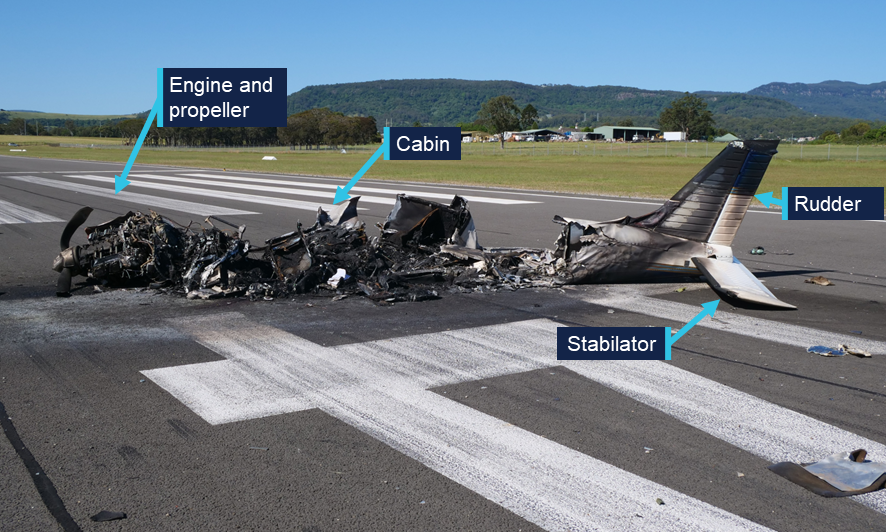
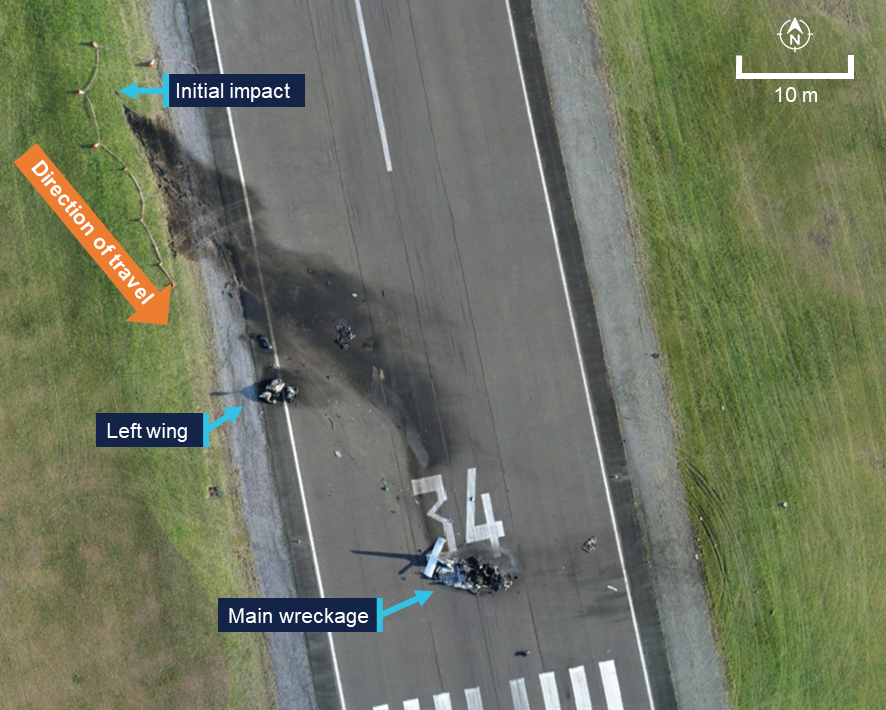
The aircraft impacted the ground to the west of runway 34 while travelling in the 138° M direction (Figure 8). The left wing tip impacted the ground first with the aircraft at or near a 90° angle of bank and with a nose down attitude. The propeller and engine then impacted the ground about 12 m from the wing tip impact. The left wing separated from the aircraft and the main wreckage continued along the ground for a further 47 m before coming to rest on runway 34 near the runway threshold. The integral fuel tanks in both wings ruptured during the accident sequence, leading to a post-impact fire that destroyed most of the fuselage (Figure 9).
Figure 8: Accident site
Source: ATSB
Figure 9: Fuselage wreckage
Source: ATSB
All major aircraft components were accounted for at the accident site. The ATSB conducted an initial examination of the wreckage at the site before moving the wreckage to an airport hangar for further examination. This examination did not identify any pre‑existing faults with the aircraft, the primary flight controls or the associated trim systems.
The landing gear was extended, and the flaps were extended to the 10-degree setting at impact. The stabilator trim was set to slightly nose up and the rudder trim was neutral (both positions were in accordance with POH guidance for take-off). Damage to the pilot’s seat rails indicated that it was locked in an appropriate position for the flight. The left (inboard) pin of the passenger’s seat was found secured in the rearmost position while the right (outboard) pin was found not secured into a position. However, there was no damage to the passenger seat rails or outboard rail stop to indicate that this seat had slid rearward.7
An inspection of runway 26 and the wreckage examination found no evidence of an animal strike.
Engine and propeller examination
The damage to the propeller indicated that the engine was driving the propeller at the time of impact. The throttle, propeller and mixture controls were all found fully forward although movement of the controls during the accident sequence could not be ruled out.
In December 2025, the engine was disassembled and examined at a CASA-authorised maintenance facility under the supervision of the ATSB. The engine condition was consistent with the engine’s recorded time in service since overhaul. No internal or external damage was identified that may have prevented the engine from operating normally prior to the accident. No defects were identified in the induction system components or engine accessories that may have affected its pre-accident operation.
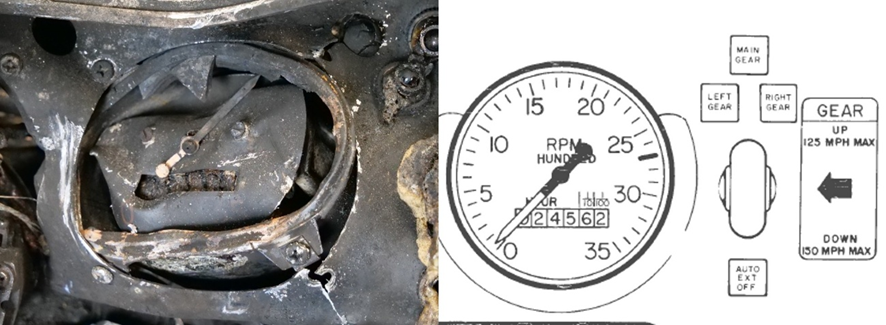
The propeller blades were all retained in the propeller hub. The blades and the spinner also exhibited signatures consistent with the propeller being driven by the engine at moderate power at the time of impact. Propeller ground scars and the tachometer needle position indicated that the engine was rotating at about 2,000 to 2,200 RPM at the time of the ground impact (Figure 10).
Figure 10: Tachometer from the aircraft (left) and an extract from the pilot’s operating handbook (right)
Source: Piper and ATSB
Recorded data
The ATSB obtained recorded automatic dependent surveillance‑broadcast (ADS-B) data for the accident flight. In addition, several security cameras captured the aircraft before and during the flight (Figure 11 and Figure 12)
Figure 11: The aircraft taxiing prior to take-off
Source: Supplied, modified by the ATSB
Figure 12: Flight path and recorded data
All speeds are groundspeed, and the altitude is above ground level. Source: Google Earth, Bureau of Meteorology, Avdata and publicly available ADS‑B data, annotated by the ATSB
A witness also captured 2 photographs of the aircraft while airborne (Figure 13 and Figure 14). From the security camera footage, photographs and ADS-B data, the ATSB was able to establish that:
the primary flight controls were not locked
during the initial take-off ground roll, the stabilator was in a neutral position
the initial take-off ground roll appeared normal
the recorded groundspeed at the time the aircraft became airborne was 61 kt
the groundspeed increased to 64 kt as the aircraft commenced turning left and then remained between 60–61 kt as the aircraft turned through 180° M. As the turn continued and with an increasing tailwind component, the groundspeed increased to the recorded maximum of 70 kt immediately before impact
in the second photograph (Figure 13), taken just before impact, the propeller was rotating at about 2,700 RPM
there was no evidence of an animal strike
all cabin and baggage compartment doors appeared to be correctly secured
in the 2 photographs, the rudder was at a near-neutral position, the stabilator was at a full, or near-full, nose up deflection and the ailerons were partially deflected to the right
in the first photograph (Figure 14), the stabilator trim anti-servo tab was deflected up (the tab is not visible in the second photograph)
the security camera footage was not of sufficient resolution to determine control deflections during the flight.
Figure 13: Photographs of the aircraft during the accident flight
Source: Ari Bone and Google Earth, modified by the ATSB
Figure 14: Enlargement of first photograph
Source: Ari Bone, modified and annotated by the ATSB
A Garmin 750 navigation unit was recovered from the aircraft wreckage, but the installed software version did not record track logs.
Shellharbour Airport CTAF recordings captured no further broadcasts from the pilot of VH-JVA following those made prior to take-off.
Meteorological information
Shellharbour
The terminal area forecast valid for Shellharbour Airport at the time of the accident indicated winds of 10 kt from 260° M. Severe turbulence8 was also forecast below 5,000 ft above mean sea level (AMSL). From 1000, the winds were forecast to increase in strength to 15 kt, gusting to 25 kt.
At 0959, as the aircraft departed runway 26, the Bureau of Meteorology automatic weather station at Shellharbour Airport recorded the temperature as 27°C and the wind as 12 kt from 278° M. There was no recorded cloud, and visibility was recorded as greater than 10 km.
The pilot of the preceding Cessna reported that during their departure, the winds were gusty with light windshear and moderate turbulence. This pilot also stated that this was common for Shellharbour Airport with strong westerly winds. The accident pilot and aircraft were based at Shellharbour Airport, and the pilot was reported to be familiar with mechanical turbulence associated with strong westerly winds at the airport.
En route and Bathurst
The flight plan indicated that the pilot intended to climb to 6,000 ft AMSL for the flight to Bathurst. The graphical area forecast valid for the flight to Bathurst included a visibility of greater than 10 km with scattered9 stratocumulus cloud between 4,000 ft AMSL and 8,000 ft AMSL. The terminal area forecast valid for the estimated time of arrival at Bathurst included winds of 12 kt from 260° M, with the ceiling, visibility and weather forecast to be OK (CAVOK).10
For the return flight planned for 1600 the following day, the terminal area forecast, valid for Bathurst Airport, included light showers of rain, winds of 10 kt from 250° M, scattered cloud at 3,435 ft (1,000 ft above the airport elevation) and visibility greater than 10 km. This forecast also included periods of up to 30 mins (INTER) with rain showers, wind of 20 kt gusting to 35 kt and a variable direction. These periods also forecast broken cloud at 3,235 ft (800 ft above airport elevation), scattered towering cumulus cloud at 5,435 ft (3,000 ft above aerodrome elevation) and 4 km visibility.
The graphical area forecast for this flight included a general visibility greater than 10 km but reducing to 7 km in scattered light rain showers and 3 km in isolated rain showers. Scattered cumulus cloud was forecast extending from 5,000 ft AMSL to above 10,000 ft AMSL. The scattered light showers were associated with scattered stratocumulus cloud between 4,000 ft AMSL and 8,000 ft AMSL and broken altocumulus/altostratus cloud from 8,000 ft AMSL to above 10,000 ft AMSL. The isolated rain showers were associated with isolated towering cumulus cloud from 6,000 ft AMSL to above 10,000 ft AMSL and broken stratocumulus and cumulus cloud from 2,000 ft AMSL to above 10,000 ft AMSL.
Safety analysis
Stabilator deflection
The aircraft started the take-off roll with the stabilator in a near-neutral position. However, during the take-off roll, the horizontal stabilator moved to a full, or near-full, nose up deflection.
The reason for the stabilator deflection could not be determined. The selected stabilator trim was correct and examination of the flight control and trim systems did not identify any pre-accident defects. Furthermore, neither control seat slid rearward, the aircraft was not equipped with an autopilot servo on the stabilator control and the observed stabilator anti-servo tab position during the flight indicated that the tab was operating correctly. In addition, the aircraft did not appear to be subjected to an external influence such as an animal strike or environmental effect. There was also no evidence to indicate that the stabilator deflection resulted from any intentional or inadvertent action or a medical episode of the pilot or passengers.
When the stabilator moved to the nose up deflection, the aircraft pitched abruptly nose up, yawed left and became airborne. The aircraft’s propeller rotated right (clockwise) when viewed from the cabin, generating a torque effect and a spiralling slipstream acting on the left side of the vertical stabiliser. These forces result in the aircraft yawing left with an associated rolling tendency. These left-turning tendencies are particularly apparent at high engine power settings and low air speeds, such as those experienced by the aircraft as it became airborne and are primarily corrected using right rudder input.
Photographs taken during the flight showed the rudder was maintained in a neutral position. The left yaw and roll and left turning flightpath likely occurred because of the aircraft’s left turning tendency not being corrected with rudder input. However, the right aileron input during the flight and the engine power reduction just before impact indicated attempts to correct the flightpath and reduce the severity of the impact.
The photographs and flight path indicate that the stabilator very likely remained in the nose up deflection for the entire flight. Late in the flight, as the aircraft began descending, it stalled, the angle of bank increased, and the descent rate increased rapidly before the aircraft collided with terrain.
Overdue instrument and radio inspections
The aircraft logbook last recorded specific instrument system inspections required under Civil Aviation Order 100.5 as being completed on 17 April 2023 and, with the exception of the air speed indicator, these inspections needed to be completed again no later than 16 June 2025 (3 months before the accident).
On 14 May 2025, the maintenance release was issued with an expiry date or time of 14 May 2026, or 3,998.2 hours in service, whichever occurred sooner. This maintenance release included a statement in the ‘Maintenance required’ section noting that an ‘IFR annual’ inspection was required before an instrument flight rules (IFR) flight. However, the IFR annual instrument and radio system inspections were not completed before the accident flight that was conducted under the instrument flight rules. Additionally, the maintenance release did not state that certain CAO 100.5 inspections for visual flight rules flight were also due during the period of the maintenance release validity (16 June 2025). The aircraft logbook had no record of these inspections being completed prior to the accident flight. Therefore, the maintenance release should have ceased to be valid as of 16 June 2025.
The forecast weather conditions for the flight to Bathurst and particularly the return flight on the following day indicated a high likelihood of encountering cloud with associated reduced visibility. During these periods, the pilot would have been solely reliant on the aircraft’s instrument and radio systems to ensure the safe completion of the flight. The overdue inspections for these systems reduced assurance that the indications provided by these systems were accurate and therefore increased risk to the flights.
While these inspections were not completed prior to the flight being conducted, they did not relate to the stabilator or its control systems. Therefore, the absence of these inspections did not contribute to the accident.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Piper PA-32R-300, VH-JVA, at Shellharbour Airport, New South Wales on 11 October 2025.
Contributing factors
During the take-off roll, the horizontal stabilator moved to a full, or near-full, nose up deflection and very likely remained in this position for the entire flight.
Following the significant stabilator movement the aircraft pitched abruptly nose up, yawed to the left and became airborne. The aircraft then followed a left turning flight path until it stalled and collided with terrain.
Other factors that increased risk
At the time of the accident flight, required instrument and avionics maintenance inspections had not been completed, reducing the assurance that the indications provided by these systems were accurate.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence
Safety action by maintenance organisation
In response to the accident, the maintainer advised that they had automated the tracking of aircraft maintenance requirements to ensure that all required items were completed during maintenance events.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Civil Aviation Safety Authority
Airservices Australia
New South Wales Police
New South Wales Health
Shellharbour Airport
Piper Aircraft
the maintenance organisation for VH-JVA
the aircraft co-owner
witnesses
security camera footage and photographs of the accident flight
Bureau of Meteorology.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Civil Aviation Safety Authority
United States National Transportation Safety Board
Piper Aircraft
the maintenance organisation for VH-JVA
the aircraft co-owner.
A submission was received from:
the maintenance organisation for VH-JVA
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
^The runway starter extension is additional runway length available for take-off (not landing) before the runway threshold.
^A skidding turn is an uncoordinated turn where the fuselage of the aircraft is not aligned with the airflow. In a skid the tail of the aircraft follows a path that is outside of that followed by the nose.
^Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to fly using external references and without relying on instrument indications.
^‘Avionics’ LAME relates to where specialist knowledge, techniques and equipment is required by LAMEs for specified electrical, instrument and radio systems maintenance.
^Work packages are documents which define a set of maintenance tasks that are to be performed on an aircraft during an inspection. These contain notes of test results, certification for the completion of maintenance tasks and records of parts removed/installed.
^The seat rail stops limit the fore/aft seat movement, ensuring that the seat feet remain attached to the rails.
^Moderate turbulence is usually associated with small changes in airspeed and moderate changes to aircraft attitude and/or altitude, but the aircraft remains under positive control. Severe turbulence is associated with large changes in airspeed and abrupt changes to aircraft attitude and/or altitude; in severe turbulence the aircraft may be out of control for short periods.
^Scattered cloud indicates that cloud is covering between a quarter and a half of the sky. Broken cloud indicates that more than half to almost all the sky is covered, and ‘overcast’ indicates that all the sky is covered.
^CAVOK indicated that the following conditions were forecast simultaneously: visibility is 10 km or more, no cloud below the higher of 5,000 ft or the highest 25 nm minimum sector altitude, no cumulonimbus or towering cumulus cloud types, and no other weather of significance to aviation.
Preliminary report
Report release date: 14/11/2025
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Summary video
The occurrence
On the morning of 11 October 2025, a Piper PA-32R-300 Cherokee Lance, registered VH-JVA, taxied for a private flight from Shellharbour Airport to Bathurst Airport, New South Wales. The flight was being operated under the instrument flight rules[1] with the pilot and 2 passengers on board.
At 0956 local time, as the aircraft approached runway 26, the pilot announced on the Shellharbour common traffic advisory frequency (CTAF) that the aircraft was entering the runway and lining up to depart. The pilot then taxied the aircraft onto the runway starter extension[2] and lined up. While VH-JVA was lined up, a Cessna Caravan taxiing behind VH-JVA stopped at the holding point at the runway 26 threshold. The pilot of VH-JVA invited the pilot of the Cessna to depart ahead of VH-JVA and the Cessna took-off shortly after.
About a minute after the Cessna departed, VH-JVA began a take-off from runway 26. Following a ground roll of about 410 m, VH-JVA abruptly pitched up and yawed left as it became airborne. The aircraft then climbed away from the runway in a nose high attitude while skidding[3] and rolling left (Figure 1 and Figure 2).
Figure 1: Composite image of recorded security camera footage of the whole flight
Source: Supplied, annotated by the ATSB
Figure 2: Composite image of recorded security camera footage of later part of flight
Source: Shellharbour Airport, annotated by the ATSB
The angle of bank then appeared to stabilise briefly as the aircraft followed a left-turning flight path. As it turned to a heading of about 200° magnetic (M), it reached a maximum recorded altitude of about 50 ft above ground level (AGL) and then began descending. Three seconds after reaching 50 ft AGL, the angle of bank and descent rate began increasing rapidly before the aircraft collided with terrain, coming to rest at the threshold of the intersecting runway (runway 34). The pilot and passengers were fatally injured in the accident, and the aircraft was destroyed.
Context
Pilot details
The pilot held a private pilot licence (aeroplane) and the required class rating and endorsements to operate the aircraft. The pilot also held a private instrument rating and Class 2 aviation medical certificate, which were both current at the time of the accident.
The pilot’s logbook was reported to be in the aircraft during the accident flight. The cabin area of the aircraft was extensively fire damaged following the accident and the logbook could not be located during the wreckage examination. At the pilot’s last medical examination, the pilot had declared a total of 1,015 hours aeronautical experience. Maintenance release entries for VH-JVA showed that since that medical examination, the pilot had flown 27.1 hours in the aircraft. Of these, 4.6 hours were in the 90 days before the accident and none in the 30 days before the accident.
Aircraft details
The Piper PA-32R-300 Cherokee Lance is a single-engine, low-wing, retractable tricycle landing gear aircraft. The Lance is powered by a Lycoming IO-540 fuel-injected, horizontally opposed piston engine driving a three-blade variable-pitch propeller and is fitted with dual controls. VH-JVA (Figure 3), serial number 32R-7680030, was manufactured in the United States in 1975 and first registered in Australia in 1985. The most recent periodic inspection was completed on 14 May 2025, at 3,898.2 hours total time in service. At the time of the accident, VH-JVA had accumulated 3,915 hours in service.
Figure 3: VH-JVA
Source: Clinton J Down Photography, modified by the ATSB
Aircraft loading
The pilot and a passenger were in the 2 front seats while the other passenger was seated in the second row. Witness statements and fuel records indicated that the aircraft departed with full tanks.
The purpose of the flight was an overnight stay at Bathurst before returning to Shellharbour the following day. No large or heavy items were identified in the aircraft during the examination of the wreckage and the ATSB estimated the aircraft to be within weight and balance limitations for the flight.
Meteorological information
The terminal area forecast valid for Shellharbour Airport at the time of the accident included winds of 10 kt from 257° M. Severe turbulence[4] was also forecast below 5,000 ft AMSL. From 1000, the winds were forecast to increase in strength to 15 kt with gusts to 25 kt.
At 0959, as the aircraft departed runway 26, the Bureau of Meteorology automatic weather station at Shellharbour Airport recorded the temperature as 27°C and the wind as 12 kt from 278° M. There was no recorded cloud, and visibility was recorded as greater than 10 km.
The pilot of the preceding Cessna reported that, during their departure, the winds were gusty with light windshear and moderate turbulence. This pilot also stated that this was common for Shellharbour Airport with strong westerly winds. The accident pilot and aircraft were based at Shellharbour Airport, and the pilot was reported to be familiar with mechanical turbulence associated with strong westerly winds at the airport.
Impact and wreckage information
The aircraft impacted the ground to the west of runway 34 while travelling in the 138° M direction (Figure 4). The left wing tip impacted the ground first with the aircraft at near 90° angle of bank and a slightly nose down attitude. The propeller and engine then impacted the ground 12 m from the wing tip and ground scars consistent with propeller strikes were indicative of engine rotation. The left wing separated from the aircraft and the main wreckage continued along the ground for a further 47 m before coming to rest on runway 34 near the runway threshold. The integral fuel tanks in both wings ruptured during the accident sequence, leading to a post-impact fire that destroyed most of the fuselage.
Figure 4: Accident site
Source: ATSB
The ATSB conducted an initial examination of the wreckage at the accident site before moving the wreckage to an airport hangar for further examination. All major aircraft components were accounted for at the accident site. The damage to the propeller indicated that the engine was driving the propeller at the time of impact. The landing gear was extended and the flaps were extended to the 10-degree setting. The stabilator trim was set to slightly nose up and the rudder trim was neutral. Damage to the pilot’s seat rails indicated that it was locked in an appropriate position. The left pin of the passenger’s seat was found secured in the rearmost position while the right pin was found not secured into a position. There was no damage to the outboard passenger seat rail stop to indicate that this seat had slid rearward.[5]
Recorded data
Recorded automatic dependent surveillance broadcast (ADS-B) data and a number of security cameras captured the flight (Figure 5). A witness also captured 2 photographs of the aircraft while airborne (Figure 6). The data showed that:
during the take-off ground roll, until the nose wheel lifted from the runway, the take-off appeared normal and the stabilator was in a neutral position
the recorded groundspeed at the time the aircraft became airborne was 61 kt
the groundspeed increased to 64 kt as the aircraft commenced turning left and then remained between 60–61 kt as the aircraft turned through 180° M. As the turn continued and with an increasing tailwind component, the groundspeed increased to the recorded maximum of 70 kt immediately before impact
all doors appeared to be correctly secured.
Figure 5: Flight path and recorded data from flight
All speeds are groundspeed, and the altitude is above mean sea level (equating to about 50 ft above ground level). Source: Google Earth, Bureau of Meteorology, Avdata and publicly available ADSB data, annotated by the ATSB
Figure 6: Photographs of VH-JVA during the accident flight
Source: Ari Bone and Google Earth, modified by the ATSB
A Garmin 750 navigation unit was recovered from the aircraft wreckage and retained by the ATSB for further investigation.
Shellharbour Airport CTAF recordings captured no further broadcasts from the pilot of VH-JVA following those made prior to take-off.
Further investigation
To date, the ATSB has examined the site and wreckage, conducted interviews and collected documentation and recorded data relating to the accident flight.
The investigation is continuing and will include further review and examination of:
recorded data
aircraft documentation
aircraft maintenance records
recovered aircraft components
pilot medical records, qualifications, and experience.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB would like to acknowledge the assistance of New South Wales Police, Shellharbour Airport, and the airport hangar operator during the onsite stage of the investigation.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[2]The runway starter extension is additional runway length available for take-off (not landing) before the runway threshold.
[3]A skidding turn is an uncoordinated turn where the fuselage of the aircraft is not aligned with the airflow. In a skid the tail of the aircraft follows a path that is outside of that followed by the nose.
[4]Moderate turbulence is usually associated with small changes in airspeed and moderate changes to aircraft attitude and/or altitude, but the aircraft remains under positive control. Severe turbulence is associated with large changes in airspeed and abrupt changes to aircraft attitude and/or altitude; in severe turbulence the aircraft may be out of control for short periods.
[5]The seat rail stops limit the fore/aft seat movement, ensuring that the seat feet remain attached to the rails.
On the evening of 9 October 2025, a Robinson R22 Beta II helicopter, registered VH‑LYD, was being operated by MDH Pty Ltd (MDH) 25 km south-south‑east of Kowanyama, Queensland.
The helicopter left Rutland Plains at around 1845 to guide ground vehicles tackling a bushfire. At around 1920 the pilot told the ground crew that it was getting too dark and set off to return to Rutland Plains Station.
Staff at the station lit the helipad for the arrival of the pilot. When the pilot did not return to the station, staff raised the alarm.
The following morning, the helicopter wreckage was found. The helicopter had collided with terrain. The pilot of VH-LYD was fatally injured in the accident, and the helicopter was destroyed.
What the ATSB found
The ATSB found that the pilot operated the helicopter at night. The helicopter was not equipped, and the pilot was unqualified, for flight at night. However, it was normal for company R22 pilots to exceed the limits of last light.
Instead of observing the legal limits, pilots chose their own limits, despite none of the company’s R22 pilots being qualified for night flight and none of its R22 helicopters being equipped for night flight. ATSB analysis of historical flight tracking data showed that on 39 occasions in the previous 6 months MDH pilots had flown beyond the legal minimums into night. Flying after last light was a tolerated and unmanaged risk on MDH properties.
In addition, the ATSB found that MDH did not require pilots to formally assess risk and did not provide tools or training to do so. This limited the ability of the company and its pilots to identify and understand operational hazards and their consequences.
What has been done as a result
MDH now requires its pilots to determine the official time of last light and has made it a clear responsibility of the pilot and the station manager to ensure aircraft are on the ground before last light.
Additionally, pre-flight planning now includes consideration of fatigue, including rest and duty times, and consideration of risk assessment criteria.
MDH has also implemented a pilot mentoring scheme to assist, mentor and supervise MDH pilots during aerial mustering operations. This includes a pre-season low level risk assessment and standardised mustering workshop, the first of which took place in March 2026.
Safety message
This accident is the fourth fatal accident of this type in the last 5 years. Flying after last light without appropriate equipment and qualifications is an unsafe practice. The acceptance of this activity is leading pilots to fatal accidents.
The ATSB’s Avoidable Accidents No 7 - Visual flight at night accidents provides further discussion about these practices and how they have contributed to accidents. The requirement to operate under daylight conditions, and plan to land 10 minutes before last light, provides a reliable method for ensuring there are sufficient external visual references available to safely operate an aircraft.
Pilots and the companies or landowners they work for, or contract to, must work together to avoid flight at night by unqualified, unequipped pilots. Development of risk management practices in any organisation should be an ongoing activity. It should develop an ability across all parties to document operational risks and codify learnings from operations.
The occurrence
On the evening of 9 October 2025, a Robinson R22 Beta II helicopter, registered VH‑LYD, was being operated by MDH Pty Ltd (MDH) at Rutland Plains, a cattle property in northern Queensland on the Gulf of Carpentaria (Figure 1).
Figure 1: Area of operation
Source: Queensland Globe
The pilot started the day’s flying just after 0600, aerial mustering in an area about 40 km south‑west of another company‑owned property, Dunbar Station, Queensland. In the afternoon, the pilot travelled to Rutland Plains to collect a colleague and conduct aerial reconnaissance for another muster planned for the following day. After leaving their colleague, the pilot flew to a nearby location to collect parts for equipment needed for the planned muster at Rutland Plains.
At around 1730, on the way to collect the parts, the pilot spotted a bushfire around 25 km south-south‑east of Rutland Plains station. The pilot advised crew at the station via radio and ground vehicles were dispatched to control the fire. Crew at the station recalled that after returning to Rutland Plains with the parts, the pilot flew to the fire to assist in guiding the ground vehicles through tracks and fences to the flame front.
The pilot and helicopter were limited to daytime operations. The pilot departed Rutland Plains for the fire at around 1845. The time of last light (the beginning of nighttime) at Rutland Plains on 9 October was 1852.
At around 1920, the pilot was providing airborne assistance to ground crew controlling the fire. Around that time the pilot announced over the radio that it was getting too dark, and the pilot needed to return to Rutland Plains. Hearing this, the crew at the station lit the helipad with the headlights of a vehicle to assist the pilot on their return.
At around 1935, crew at the station checked to see if the pilot had landed. Discovering that the helicopter had not returned, they tried contacting the pilot by radio. When radio contact was unsuccessful, they escalated the non-arrival within the company and sought information from a satellite tracking system on board the helicopter to establish its location. Tracking had stopped at 1929 around 7.5 km south-south‑east of the station (Figure 2).
Figure 2: Fire location and VH-LYD track
Source: Google Earth, BoM and SPOT Trace tracking data
Station crew conducted a ground search while company management contacted emergency services and the Joint Rescue Coordination Centre. A coordinated air search began just after midnight.
The following morning, helicopter wreckage was found by a station crew member from Rutland Plains and a helicopter pilot from a neighbouring property. VH-LYD had collided with terrain around 1.5 km north of the last satellite tracking point. The pilot was fatally injured in the accident, and the helicopter was destroyed by impact forces.
Context
Pilot information
The pilot held a valid Private Pilot Licence (Helicopter) (PPL(H)), which was issued in February 2023 and a mustering endorsement issued in April 2023. The pilot held a class 2 medical certificate which was valid to 31 August 2026.
The pilot commenced work in ground-based cattle operations with MDH Pty Ltd (MDH) in 2017 and transitioned to an aerial mustering role. The pilot had accumulated around 2,000 to 2,500 hours of flight time.
In November 2024, the pilot attended a Robinson Helicopter Company safety course. On 16 January 2025 they underwent a biannual helicopter flight review. In March 2025 the pilot attended an MDH leadership conference. In June 2025 the pilot completed refresher training and check flights in mustering techniques. There was no record of the pilot being trained or qualified to operate under night visual flight rules (NVFR) [1],[2] (see Night flight regulatory requirements).
It could not be determined if the pilot experienced a level of fatigue that would have impaired performance or decision‑making at the time of the accident (see Fatigue).
Helicopter information
VH-LYD was a Robinson Helicopter Company R22 Beta II helicopter, serial number 4471 (Figure 3). It was powered by a Textron Lycoming, O-360-J2A, 4-cylinder piston engine. VH-LYD was manufactured in the United States on 12 February 2010 and first registered in Australia on 19 May 2010. It was equipped and maintained to a day VFR standard. Its last 100-hourly maintenance was conducted on 24 September 2025. At the time of the accident VH-LYD had accumulated approximately 14,645 hours total time in service.
Figure 3: Exemplar Robinson Helicopter Company R22
Note: This exemplar image has been digitally altered by the ATSB. Source: MDH Pty Ltd
The R22 had 2 seats, with the pilot flying from the right seat, and each seat was fitted with a seatbelt and inertia reel shoulder strap. VH-LYD did not have doors fitted at the time of the accident.
Maintenance records and wreckage inspection both showed that VH-LYD was not equipped with instruments necessary for flight at night (see Night flight regulatory requirements).
Recorded information
The helicopter was not fitted with a flight data recorder or a cockpit voice recorder, nor was it required to be. During the accident flight, data was transmitted from a SPOT Trace[3] satellite tracking unit fitted to the helicopter, which could be used by MDH personnel to track the location of the helicopter during flight. The unit provided 5-minute time-stamped updates on the helicopter’s location, speed and altitude. The recorded data captured the accident flight until shortly before the impact with terrain.
The SPOT Trace units were fitted to all MDH R22 helicopters, and the ATSB sourced the preceding 6 months of fleet data for analysis purposes. The data covered 596 days of helicopter operation across 4 helicopters (see Night flight data analysis).
Wreckage and impact information
The ATSB did not attend the accident site. The site was mapped, documented and assessed by a team from the forensic crash unit of the Queensland Police Service (QPS). QPS recovered the wreckage of VH-LYD to a secure location in Cairns, Queensland, where it was examined by 2 ATSB investigators.
Site photographs and wreckage inspection indicate that VH-LYD was moving at high speed, around 90 degrees off track, at the time of the collision with terrain (Figure 4). The helicopter was significantly damaged by tree and ground impacts with the main rotor and transmission assembly separating from the helicopter. There were no pre-accident defects identified, and the engine was driving the main and tail rotor system at the time of the collision. The impact with terrain was not considered to be survivable.
Figure 4: VH-LYD accident site
Source: Queensland Globe, Queensland Police Service, annotated by the ATSB
Meteorological and environmental information
Weather
A Bureau of Meteorology (BoM) aviation weather forecast for Kowanyama Airport (located around 20 km north‑west of Rutland Plains) for 9 October related the possibility of thunderstorms. Meteorological conditions recorded by the BoM weather station at Kowanyama Airport included distant lightning from around 1530, indicating that thunderstorms were reported within 30 NM (55 km) but not at the airport. Cloud developed through the day, with periods of scattered to broken cloud between 6,000 ft and 9,000 ft. No cloud was detected at Kowanyama Airport at the time of the accident.
No rainfall was detected throughout the day, and the wind had shifted from a variable easterly in the morning to a south-westerly wind of 6 kt from around 1730. Around that time the accident pilot reported to a colleague at Rutland Plains that dry storms[4] were building in the area, and that there was smoke, indicating a bushfire.
A witness who heard the departure of VH-LYD stated that on last light, shortly after the time the pilot departed Rutland Plains for the fire, cloud covered the area though there was still a visible horizon.
Light
The period between sunset[5] and the geometric centre of the Sun’s disk reaching 6° below the horizon is called civil twilight (Figure 5). The end of civil twilight is otherwise known as last light. For aviation purposes last light is the boundary between night and day. The period when the geometric centre of the Sun is between 6° and 12° below the horizon is called nautical twilight. After that time, it is ordinarily, for all practical purposes, dark. This is especially so in areas devoid of artificial lighting.
Figure 5: Limits of day and night relative to the position of the Sun
Source: Geoscience Australia, ATSB
The time of last light was readily available for any location in Australia from Airservices Australia’s national aeronautical information processing system (NAIPS). It could also be calculated using tables published in the aeronautical information package (AIP) at GEN Section 2.7 – First light and last light computations(Airservices Australia, 2024) or via Geoscience Australia’s calculator on its website.
On 9 October 2025 at the location of the accident near Rutland Plains Station, Queensland, sunset was 1831, the end of civil twilight was 1852 and the end of nautical twilight was 1917. Celestial illumination would have been limited by cloud and there was no moonlight as a waning gibbous[6] moon would not rise until 2045.
Smoke
The 6 kt (10.8 km/h) south-westerly wind, though light, is likely to have kept smoke away from the pilot’s return track to Rutland Plains Station. Moreover, the pilot was unlikely to have approached the fire through smoke, and the pilot departed the fire on a reciprocal track.
Operational information
Operator overview
MDH Pty Ltd was one of Australia’s largest beef cattle operations. It was a family business that owned 14 properties covering 3.36 million hectares. MDH’s aircraft and pilots were spread over Queensland and managed from Brightlands Station just south of Cloncurry, Queensland.
At the time of the accident MDH owned and operated 4 Robinson R22 helicopters, 1 Robinson R44 helicopter and 6 fixed wing aircraft. It had operated Robinson R22 helicopters since 1985. The chief pilot stated that at the time of the accident none of its R22 helicopters were equipped for night flight.
MDH had 4 helicopter pilots flying the R22s. Three of the pilots had Private Pilot Licences (Helicopter) and one had a Commercial Pilot’s Licence (Helicopter). All were endorsed for low‑level flight and mustering and none held a night visual flight rules rating.[7]
The helicopters were being operated by paid employees, aerial mustering for commercial beef cattle operations. As the helicopters were company‑owned, and were being operated over private land, those operations were conducted as limited aerial work operations under Part 138 of Civil Aviation Safety Regulations (CASR), which do not require the issue of an aerial work certificate by CASA. Part 91 of the Civil Aviation Safety Regulations (CASR) (2025b) also applied unless a specific requirement of Part 138 disapplied it. This meant MDH had to comply with the requirements of CASR Part 138 with respect to pilot fatigue and risk management of operations.
Operator procedures and oversight
MDH did not have, and was not required to have, a CASR Part 138 aerial work certificate for the R22 operations. Therefore, it was not required to provide the Civil Aviation Safety Authority (CASA) with a complete operations manual covering all requirements of the regulations for its proposed operations.
Instead of an operations manual detailing how operations were to be conducted, MDH had limited manuals and procedures for helicopter operations. An induction handbook for pilots carried information on administration and basic instructions with respect to flight operations. A statement at the head of the document required pilots to observe all applicable laws and rotorcraft flight manual limitations.
Pilots stated that the document matched their operations, and that the expectation of pilots not breaching regulations was observed. MDH held pre-season[8] safety meetings with the pilots. The last was 21 March 2025 in Brightlands. The meetings would cover operational elements, as well as a review of the pilot induction material to refresh procedures.
MDH had a senior pilot who was positioned in the induction handbook as the chief pilot. They were to be contacted for aircraft and pilot issues. The chief pilot stated that oversight of the pilots was conducted, when possible, by the chief pilot or another senior manager, though they were most often not co-located with the pilots.
The chief pilot would roster pilots by date, helicopter and location and build in rest days. They would also ensure that pilots’ tasks remained solely associated with flying. Ordinarily pilots would start at first light, but it was left to the pilots as to when their duty would end. Days rostered were documented and retained by the company, but duty hours worked by pilots were not.
The chief pilot acknowledged that there were occasions whereby pilots would have to use the helicopter for as long as possible and into twilight. They stated that they expected pilots to minimise their exposure to flight at night by landing near vehicles to get a lift home, or by staying at alternative accommodation. The chief pilot provided an example of setting this expectation to a pilot in mid-August 2025 after they exceeded last light by 35 minutes.
They also stated that pilots would assess whether there was enough light to continue flight, and the decision was at the sole discretion of the pilot. MDH’s pilots concurred with this, and all stated that the pilot in command was solely responsible for the operation of the helicopter and had final say in all decisions related to the operation of their helicopter.
There was one mention of daylight in the MDH induction handbook for pilots which concerned ferrying of aircraft. It stated:
A decision has to be made by the pilot if the daylight does not permit making the scheduled property in the afternoon to stay at a property and notify [management] that they did not make it.
Flight at night
Night flight AIP instructions and CASA guidance material
The CASA (2025f) Visual flight rules guide carried information on the regulations and requirements pertaining to night visual flight rules. It was a useful starting point for pilots and operators to ensure night flight was appropriately managed. In addition, advisory circular (AC) 61-05 Night VFR rating (CASA, 2022) was an important supporting document to the regulations and related notable hazards of night flight.
Untrained (and therefore unauthorised) pilots were not allowed to conduct flight at night. AIP ENR Section 1.2 – Visual Flight Rules, paragraph 1 Flight Rules, sub paragraph 1.1 The Visual Flight Rules (VFR), sub sub paragraph 1.1.2 stated:
1.1.2 Unless the pilot in command is authorised under CASR Part 61 to conduct a flight under the IFR or at night under the VFR and the aircraft is appropriately equipped for flight at night or under the IFR, a VFR flight must not be conducted at night.
The appropriate equipment mentioned was listed in CASR Part 91 manual of standards (MOS) (CASA, 2021). This included specific equipment such as:
equipment for displaying the rotorcraft’s attitude
radio communications system equipment
navigation systems equipment, such as an approved GNSS
navigation and cockpit lighting.
Furthermore, there were rules about fuel reserves, alternate aerodromes, and calculating and flying above lowest safe altitudes. Additionally, AC 139.R-01 v3.1 (CASA, 2024a) carried guidelines for helipad dimensions and markings for night operations which were in excess of those required for operations by day.
AIP ENR Section 1.2 – Visual Flight Rules, paragraph 1 Flight Rules, sub paragraph 1.1 The Visual Flight Rules (VFR), sub sub paragraph 1.1.3 stated:
1.1.3 For pilots not authorised to fly at night, it is recommended that they plan to arrive at the later of the destination aerodrome or alternate aerodrome at least 10 minutes before last light (allowing for any required holding).
The AIP instructions and associated CASA guidance material clearly indicate that the regulations precluded an untrained or unequipped pilot from flying at night. Additionally. there was a clear intention that pilots aim to land at least 10 minutes before last light (10 minutes before end of civil twilight).
Operator’s night flight practices
The ATSB interviewed 3 company R22 pilots and the chief pilot about practices related to night flight.
MDH did not roster pilots to fly after last light. To do so was against regulations. However, pilots reported that the requirement to land before last light was not always observed. They stated that while they would not plan to land after last light, at times, operational needs led them to do so.
On occasion, depending on the location and behaviour of the cattle, a muster could take longer than planned. In some locations where a holding yard was available, it was possible to re-plan and stop work without losing effort. Additionally, the option existed to land at the yards and return to the station in a vehicle rather than flying back to a station in fading light. However, that could delay the start of the following day’s muster and leave less time to manage overruns the next day.
In locations where cattle could not be held, ending the job before cattle were yarded up could lead to the loss of a day’s work. While there was no reported pressure on pilots to continue, pilots reported that they would do so rather than undo a day’s work. Exceeding last light was an accepted part of operations and pilots could make their own decisions about whether the light remaining was enough to finish the job and fly home.
The actual time of last light and 10-minute buffer was not used in pilot assessments, and pilots did not use the time of last light to delineate between night and day. Instead, pilots would weigh environmental factors such as sunset, cloud and available horizon against their own tolerance for risk. The distinction became one between dark with a discernible horizon and fully dark.
From time-to-time emergencies, such as fires, could crop up and require input or oversight from a pilot in a helicopter. There was no expectation on the part of MDH that pilots would fly after last light, no matter the reason. At the same time, it was reported that in an environment where the pilots were most often unsupervised, no-one would prevent a pilot from doing so. Individual accountability in pilot decision‑making was reported to be the only determining factor.
Night flight data analysis
The SPOT Trace data for MDH’s 4 R22 helicopters for the 6 months preceding the accident was analysed by the ATSB to identify night flight practices. The data was pruned to remove any points that did not indicate flight, then differenced with the time of civil twilight for that location. Matches close to last light were further refined by measuring the distance to the next spot and calculating time available to destination.
The tracking data (Figure 6) showed that in the 6 months preceding the accident, the 4 company helicopters operated on 596 days. Of the 596 days of operation, company helicopters were flown after last light on 39 occasions, around 6.5% of days of operation across the 4 helicopters. The level of exceedance ranged from under a minute up to 1 hour 34 minutes, with the average exceedance being 17 minutes. Eight of the late flights, including the accident flight, extended beyond nautical twilight.
Figure 6: Latest time flown after last light for 39 flights in company R22 helicopters
Source: SPOT Trace data
The largest exceedance of around 1 hour 34 minutes after last light took place in July 2025 in the vicinity of Mount Windsor Station, Queensland. While cloud cover is not known, the moon rose at 1404 and was approaching three quarters full at an altitude of 70° when the helicopter landed.
Operational risk management
Risk management regulatory requirements
MDH, as a limited aerial work operator, was required to comply with CASR 138.370 which required risk assessment and mitigation.
MDH had to ensure that, before beginning a task, a pilot had assessed the risk of an operation (Part 138 MOS 13.05). The pilot had to ensure that the operation could be conducted without unacceptable safety risk (Part 138 MOS 13.02).
Part 138 MOS at 13.04 instructed pilots to take specific notice of:
(a) the operation and its particular characteristics;
(b) the location of the operation and its particular characteristics;
(c) the aircraft to be used in the operation, its particular characteristics, and its performance;
(d) the qualifications and experience of the crew members to be used in the operation;
(e) the hazards, external to the aircraft, that may be met in the course of the operation.
Advice on risk management was available to operators in AC 138-05 v3.0 Aerial work risk management (2025a). It stated:
For limited aerial work operations, a risk assessment and mitigation process must be undertaken by the pilot in command (PIC) before an operation is conducted…
It is incumbent upon the operator … to ensure these procedures are carried out.
Annex A to AC 138-05 v3.0 was titled Sample risk assessment process - limited aerial work operator. It explained how to implement risk management to meet the requirements of the Part 138 Manual of Standards.
Operator’s risk management practices
MDH’s primary use of helicopters was aerial mustering. This activity was supported by training and operational documents. MDH provided training in aircraft knowledge, operational techniques and safety, which was suitable for conduct of its operations.
It had also outlined a pre-mustering assessment which pilots could use to discuss and manage mustering operations. The document contained some collected knowledge of hazards and prompts to identify powerlines and brief ground crew on safety around helicopters. However, it was essentially a task management document and did not address identification and management of risk.
The flight planning section of the pilot induction handbook also prompted identification of threats with respect to reconnaissance of known local hazards such as powerlines and dead trees. While this applied to managing safety during a flight, it did not constitute risk management. Risk management was where a pilot and organisation could decide if an operation could be conducted within the organisation’s safety performance criteria (CASA, 2025d).
The pilot induction handbook also contained a section called risk management which was a high-level outline of the pilots’ responsibilities with respect to weather, fatigue, mustering, aircraft handling, and sightseeing. It outlined some associated hazards but did not discuss risk management as an activity and no risk management plans were present. Specifically, there were no defined limits or organisational tolerance for risk. Additionally, there were no apparent tools or support for company pilots to formally identify and manage risks, to ensure that an operation could be conducted without unacceptable safety risk. This limited the guidance and support available to pilots undertaking novel or infrequently encountered activities such as fire spotting.
Fatigue management
Fatigue management regulatory requirements
As a limited aerial work operator CASR 138.150 required MDH to have a system for managing crew fatigue that met the requirements of the Part 138 Manual of Standards. The Part 138 MOS at 6.02 required compliance with an element of Civil Aviation Order 48.1. That element at paragraph 16.1 of CAO 48.1 put the onus on a pilot to not carry out a task if at any point during that task, they were likely to be fatigued.
The requirement for MDH was then to ensure that pilots had knowledge and frameworks to understand and measure fatigue and to support pilot decision‑making around fatigue.
While MDH was not required to comply with the rules for daylight aerial work operations from appendix 5A of CAO 48.1, it serves as useful guidance. CASA CAO 48.1 plain English guide (CASA, 2025c) stated:
• The maximum flight duty period (FDP) that can be assigned in 1 day is 14 hours.
• Following an FDP, you must be off duty for at least 10 hours.
• You cannot be assigned an FDP that starts 30 minutes before the start of morning civil twilight (MCT) or that ends later than the end of evening civil twilight (ECT).
• An FDP cannot be extended beyond the end of ECT, unless it is necessary to complete the duties associated with the last daylight flight.
The final provision was to allow a pilot to complete ground-based work after landing, not to continue flight.
3.1.1.3 Reduced alertness may impact judgement. To manage the potential for poorer judgment and decision making associated with a fatigued FCM, CASA recommends involving a non-fatigued individual along with multiple methods for measuring alertness to assist the FCM when assessing fitness to fly.
Operator’s fatigue management practices
The pilot induction handbook contained advice to pilots on fatigue and stated:
Fatigue, or tiredness, can often be an issue in mustering operations where early mornings and long days are involved. Fatigue can have a profound effect on the performance of the mustering crew. Due to the high level of concentration required by the PIC, fatigue can set in earlier for the PIC than for the other crew members.
The accident pilot’s flight and duty times for the 7 days leading up to the accident are captured in Table 1.
Table 1: Pilot’s previous 7 days flight and duty
Date
Activity
Duty [1]
Flight Hours [2]
Start
End
Total Hours [2]
3/10/2025
Time off
4/10/2025
Travel
10:00
15:30
5.5
4.1
5/10/2025
Time off
6/10/2025
Muster
6:36
18:27
11.9
5.2
7/10/2025
Muster
5:54
14:56
9.0
8.2
8/10/2025
Muster
5:45
19:47
14.0
10.3
9/10/2025
Muster / Fire
5:42
19:29
13.8
11.3
Totals
54.2
39.1
[1] A record of duty time was not available for the pilot. Duties have been calculated by adding 30 minutes to the beginning and end of flight time to allow for pre and post flight activities.
[2] Total duty hours and flight hours are related in decimals of an hour
Source: Pilot’s roster and satellite tracking data from VH-LYD
In the 72 hours prior to the accident the pilot had flown 29.8 hours and completed an estimated 36.8 hours of duty. In the 2 days leading up to the accident the pilot had flown 21.6 hours and conducted an estimated duty of 27.8 hours. On both days the pilot’s duty exceeded daylight hours, with flight on 8 and 9 October being conducted at night. Additionally, the rest period between the duties was likely less than 10 hours.
While the fatigue regulations of an aerial work certificate holder did not apply to MDH, by way of example, this was outside of the fatigue limits for aerial work under day visual flight rules documented in Appendix 5A of CAO 48.1.
It was reported that the pilot’s accommodation was suitable for rest. Although the pilot had worked 2 long days leading up to the accident, the rest period earlier in the week potentially protected the pilot from an accumulation of fatigue. It is not possible to determine whether the pilot experienced a level of fatigue that would have impaired performance or decision‑making at the time of the accident.
Human factors
Fatigue
Fatigue can impact pilots in various ways. It can affect decision‑making, and CASA (2025e) states that fatigue at the end of a day, shift or flight, can lead people to persevere with a chosen course of action or ignore information which could contradict a decision to continue. Fatigue can diminish the ability of the eye to focus (Robson, 2008). It can also increase the risk of spatial disorientation, and lead to delayed response times as well as a range of pilot errors (ATSB, 2013).
Spatial disorientation
For day VFR pilots, spatial orientation is being aware of how they are orientated and moving in space with reference to external objects such as the surface of the Earth (Young, 2003). Spatial disorientation is loss of that awareness, ordinarily due to a loss of visual information, leading to an inability to correctly interpret aircraft attitude, altitude or airspeed in relation to the Earth or other points of reference (ATSB, 2013).
The mechanisms of spatial disorientation and dangers of flight at night, which by its very nature reduces available visual information, is discussed in detail in ATSB report Avoidable Accidents No.7 Visual flight at night accidents: what you can’t see can still hurt you (AR-2012-122) (ATSB, 2013).
Young (2003) describes the sensory systems that support spatial orientation. They include:
The visual system (sight) tells us where things are and what is present. It makes use of peripheral vision to detect self-motion relative to objects and the ground. The central vision can detect objects of known size and character to provide distance and closing information.
The vestibular system (balance and orientation organs in the ears) is the primary system for sensing body motion relative to gravity and acceleration. It supports the muscle commands that keep our eyes and head stable and keep us upright relative to gravity.
Proprioception (the sense of movement) helps to sense orientation and acceleration through pressure on the skin. It will also generate an accurate estimate of the current position of the body to plan movements and predict the outcome of future actions (Tuthill & Azim, 2018).
Sight provides around 80% of the information, and the balance organs and sense of movement, providing around 10% of the information each, are prone to illusions and misinterpretation.
Poor visual cues are a feature of almost all spatial disorientation accidents. There are several well-known illusions that can affect pilots at night (ATSB, 2013):
Somatogravic, the brain cannot differentiate between acceleration and a pitch-up event. In the absence of visual cues, the pilot can easily confuse the two states. A pilot response to an incorrect sensation can increase the confusion.
Somatogyral, the pilot’s vestibular system responds to angular acceleration. Without visual cues, this can lead to an incorrect understanding of an aircraft’s angle of bank in a turn or level flight. In the absence of external visual cues, successful orientation relies on the use of appropriate flight instruments.
Autokinesis is the phenomenon of a single point of light (a star or light from a distant station) appearing to move randomly in the visual field.
Blackhole approach involves an approach to land at night where there is nothing to see between the aircraft and the intended landing site. The absence of peripheral visual cues, especially below the aircraft, can lead pilots to perceive the aircraft is high and initiate an aggressive descent to correct their perceived approach path. The result can be landing short or impacting terrain.
The helicopter manufacturer also highlighted the dangers of disorientation specific to rotary wing operations. Safety notice SN-18 in the Robinson Helicopter Company Pilot’s Operating Handbook for the R22 stated:
Flying a helicopter in obscured visibility due to fog, snow, low ceiling, or even dark night can be fatal. Helicopters have less inherent stability and much faster roll and pitch rates than airplanes. Loss of the pilot’s outside visual references, even for a moment, can result in disorientation, wrong control inputs, and an uncontrolled crash.
Related events
Accidents involving flight at night in an unequipped Robinson R22 by pilots unqualified for night flight are frequently repeated in Australia. Common features related in the accident investigation reports in Table 2 are summarised below.
Table 2: Investigations into similar events
Investigation number
Title
AO-2023-058
VFR into smoke on a dark night and collision with terrain involving Robinson R22, VH‑DLD
AO-2022-057
Collision with terrain involving Robinson Helicopter Company R22 Beta, VH‑LOS
AO-2021-006
Collision with terrain involving Robinson R22 Beta II helicopter, VH‑HKC
AO-2016-031
Collision with water in dark night conditions involving Robinson R22, VH‑YLY
AO-2014-144
Collision with terrain involving Robinson R22, VH‑YPC
AO-2011-087
Collision with terrain, VH-YOL
AO-2011-051
Controlled flight into water, VH‑RUR
All these events involved pilots who were not qualified to fly at night. In addition, in all but one accident (AO-2014-144), the helicopters were unequipped for night flight. There was a general acceptance by pilots involved in these accidents that being unqualified and unequipped was not an impediment to flying at night.
One investigation report (AO-2014-144) noted that the pilot planned on landing with sufficient sunlight. In all other cases the flights were intentionally conducted after last light, or pilots did not discontinue the flight when presented with an opportunity to do so. In 2 accidents (AO-2023-058 and AO-2021-006), pilots departed locations with available accommodation into dark night conditions.
Many of the investigations related to hazards that would be easily detected or inconsequential in daytime but become difficult to detect and far more serious at night. Environmental conditions such as smoke (AO‑2023‑058) and cloud and rain (AO‑2022‑057, AO‑2021‑006, AO‑2016‑031, and AO‑2011‑051) were common features. Furthermore, in 3 of the accidents (AO‑2011‑087, AO‑2014‑144, and AO‑2016-031), lights inside the cabin from sources such as GPS, instrument lights and warning lights, were noted to interfere with vision outside of the helicopter by producing glare on the windscreen.
Several workarounds to support these activities were implemented by the pilots involved. These included turning off equipment to reduce glare (AO-2016-031 and AO-2014-144), flying at low level in an attempt to find ground references (AO-2023-061, AO-2021-006, and AO-2011-087), and lighting the helipad with vehicle headlights in anticipation of a late arrival (AO-2023-058).
All of the accidents took place while travelling between locations, as opposed to while conducting aerial work. All resulted in a high-speed collision with terrain or water and all but one of the accidents (AO-2011-051) resulted in fatal injuries.
Safety analysis
Flight at night
Witness statements and tracking data for VH-LYD on the night of the accident showed it was moving after last light and beyond nautical twilight. The last movement of VH-LYD was recorded at 1929, 37 minutes after last light (end of civil twilight at 1852) and 12 minutes after nautical twilight (1917) (Figure 7). Moonrise would not happen until 2045. The combination of cloud obscuring celestial light from stars, no artificial lighting on the ground, and no moonlight meant it was almost certainly very dark. This made the pilot susceptible to spatial disorientation and loss of control of the helicopter.
Figure 7: VH-LYD night flight
Source: SPOT Trace, ATSB
The pilot of VH-LYD did not have a night rating, and while there was evidence of the pilot previously operating at night, the pilot had not demonstrated competence or capability as part of a flight review or flight test.
The wreckage inspection showed it was highly unlikely that any mechanical failure of the helicopter contributed to the accident. The inspection also showed that VH-LYD did not have equipment required for flight at night such as an artificial horizon.
The extra risks inherent in visual flight at night are from reduced visual cues, and the consequent risk of spatial disorientation (ATSB, 2013). The accident site analysis showed that VH-LYD collided with a tree at high speed while travelling perpendicular to the direction required to reach Rutland Plains. While it is not possible to determine the exact nature of the disorientation affecting the pilot, being off track and too low at high speed indicated that the pilot was very likely disorientated and without visual references at the time of collision with terrain.
Contributing factor
The pilot flew at night but was not qualified to fly at night and the helicopter was not equipped to be flown at night.
Contributing factor
It is very likely that the pilot became spatially disorientated, resulting in collision with terrain.
Organisational acceptance
Risk management and decision‑making
The Civil Aviation Safety Regulations (CASR) Part 138 manual of standards explained that MDH Pty Ltd (MDH) had to ensure the pilot assessed that the operation could be conducted without unacceptable safety risk for the pilot and people on the ground in the context of the task. The accident occurred on the transit back from fire spotting and directing ground crew at night.
There was no evidence of a risk assessment being conducted or of risk assessment tools or training being made available to the pilot. To align with the manual of standards, the assessment would have had to include the aircraft used in the operation and the qualifications of the pilot. MDH did not have trained pilots or suitably equipped helicopters available. Had a risk analysis been conducted, mitigating the risk of the operation involving an untrained pilot in an unequipped helicopter at night was not possible without cancelling the flight.
Company pilots were making decisions about operations without input from the organisation, peers or risk management tools. The high level of pilot autonomy was reflected in interviews with the chief pilot, company pilots and employees. The consensus was that it was a pilot’s decision to fly and there was a position amongst pilots that it was not the place of others to tell a pilot to fly or not fly.
While the pilots reported no pressure to fly after last light, they stated that they would fly beyond last light to complete a task and not lose a day’s work for a mustering team. Pressure on decision‑making can come from various sources without being overt. Bearman and Bremner (2016) wrote that:
Situational pressure can lead people to pursue a particular goal.
People internalise values of the organisation they work for and value decisions that benefit the organisation.
Social pressure can influence decisions to optimise the impression we present to others.
Perhaps due to situational and social pressure, the pilot of VH-LYD elected to use the helicopter to support fire operations after last light, and that was accepted by the pilot’s colleagues. This was consistent with accepted practices within their working environment.
Other factor that increased risk
MDH did not require its R22 pilots to formally assess risk and did not provide tools or training to do so. This limited the ability of the company and those pilots to identify and understand operational hazards and their consequences. (Safety issue)
Awareness of flight after last light
In MDH’s environment of animal management in remote areas, teams need to be flexible and be able to improvise solutions. Autonomy of crew is a large part of that. They also need to make best use of the resources available, and a helicopter is a valuable resource. Practices such as flying beyond last light, which is an unsafe practice, can develop to become normal operations. Especially if it provides positive outcomes without negative repercussions (CASA, 2017).
Analysis of 6 months of tracking data for 4 company R22 helicopters showed that over a combined total of 596 days of operation, on 39 occasions pilots landed after last light. There was evidence of exceedances in all company R22 helicopters. The average exceedance was just over 15 minutes. Combining the tracking data with pilot rosters showed that 3 of the accident pilot’s colleagues had flown after last light, reportedly for operational reasons.
The company was aware that the pilots were not trained nor equipped for flight at night and aware that last light was not always observed. The chief pilot stated that there were times that helicopters would be needed to be used as long as possible. Instead of observing the limits of last light, pilots would judge the available light by sight and operate to their own level of comfort.
Relying on individual pilot decision‑making is reflective of the Part 91 flight operations, however, the context for these flights were primarily aerial mustering and related aerial work activities for commercial cattle farming.
While these were considered limited aerial work operations by the regulations, MDH had the ability to influence pilots and set an organisational tolerance for risk. By ignoring an actual time for last light, a distinct and easy to measure limit became ambiguous and inconsistent. The company limit was not that pilots should observe last light, rather that they should not push on into the dark. However, MDH did not provide oversight or definition of this and expected pilots to manage it themselves.
Not preventing the activity normalised the deviation from a safe envelope of operations and indicated an acceptance of flight after last light. The only limit to the non-compliance became an individual pilot’s tolerance for risk. This meant the practice could easily extend to later times and different activities.
For the pilot of VH-LYD on 9 October 2025, flying at night to assist in firefighting was likely an easy step to take, especially in the absence of a formal consideration of risk. It is not possible to discern the factors that combined in the pilot’s decision‑making about the flight. Neither is it possible to separate that decision‑making from the general acceptance of flight after last light or the influence of the operating environment.
Within the operation, limited oversight and the absence of risk management, combined with an acceptance of flight after last light, created an increased and unmitigated risk of an accident at night by an untrained pilot in an unequipped company helicopter on MDH properties.
Contributing factor
Flying after last light by pilots without night ratings, in R22 helicopters not equipped for night flight, was a tolerated and unmanaged risk on MDH properties. This increased the risk of an accident in a company R22 at night. (Safety issue)
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain at night involving Robinson R22 Beta II, VH-LYD, 25 km south-south-east of Kowanyama, Queensland, on 9 October 2025.
Contributing factors
The pilot flew at night but was not qualified to fly at night and the helicopter was not equipped to be flown at night.
It is very likely that the pilot became spatially disorientated, resulting in collision with terrain.
Flying after last light by pilots without night ratings, in R22 helicopters not equipped for night flight, was a tolerated and unmanaged risk on MDH properties. This increased the risk of an accident in a company R22 at night. (Safety issue)
Other factors that increased risk
MDH did not require its R22 pilots to formally assess risk and did not provide tools or training to do so. This limited the ability of the company and those pilots to identify and understand operational hazards and their consequences. (Safety issue)
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies.
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report.
All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out or are planning to carry out in relation to each safety issue relevant to their organisation.
Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action.
Safety issue description: Flying after last light by pilots without night ratings, in R22 helicopters not equipped for night flight, was a tolerated and unmanaged risk on MDH properties. This increased the risk of an accident in a company R22 at night.
Safety issue description: MDH did not require its R22 pilots to formally assess risk and did not provide tools or training to do so. This reduced the ability of the company and those pilots to identify and understand operational hazards and their consequences.
Glossary
AC
Advisory circular
AIP
Aeronautical information publication
CAAP
Civil Aviation Advisory Publication
CAO
Civil Aviation Order
CASA
Civil Aviation Safety Authority
CASR
Civil Aviation Safety Regulations
FCM
Flight crew member
FDP
Flight duty period
MOS
Manual of standards
NVFR
Night visual flight rules
PIC
Pilot in command
QPS
Queensland Police Service
VFR
Visual flight rules
Sources and submissions
Sources of information
The sources of information during the investigation included:
MDH Pty Ltd
employees of MDH Pty Ltd
accident witnesses
Civil Aviation Safety Authority
Queensland Police Service
Robinson Helicopter Company
maintenance organisation for VH-LDY
Bureau of Meteorology
recorded data from tracking units on company aircraft.
CASA. (2025e). Safety behaviours: human factors for pilots 4th edition Resource booklet 9 Human information processing. Civil Aviation Safety Authority.
Flight Safety Foundation. (2025). Operational Risk Assessment. In Basic Aviation Risk Standard Aerial Mustering. Flight Safety Foundation.
Liu, Y., Tian, J., Martin-Gomez, A., Arshad, Q., Armand, M., & Kheradmand, A. (2024). Autokinesis Reveals a Threshold for Perception of Visual Motion. Neuroscience, 543, 101-107. https://doi.org/10.1016/j.neuroscience.2024.02.001
Robson, D. (2008). Night Flight (2nd ed.). Aviation Theory Centre.
Young, L. R. (2003). Spatial orientation. In P. S. Tsang, Vidulich, M.A. (Ed.), Principles and practice of aviation psychology (pp. 69-113). LEA Publishers.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
MDH Pty Ltd
Cloncurry Air Maintenance
Civil Aviation Safety Authority
Bureau of Meterology
Queensland Police Service
Submissions were received from:
MDH Pty Ltd
Civil Aviation Safety Authority
Bureau of Meterology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]A night VFR rating ensures a pilot has the knowledge and skills necessary to safely operate and navigate an aircraft under visual flight rules at night.
[2]Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[3]The SPOT Trace system allowed users to set tracking intervals and view the tracker’s GPS coordinates online in real time.
[4]A dry storm is a thunder storm that produces lightning but precipitation does not reach the ground.
[5]Geoscience Australia defines sunset as the instant in the evening under ideal meteorological conditions, with standard refraction of the Sun's rays, when the upper edge of the Sun's disk is coincident with an ideal horizon.
[6]A waning gibbous moon phase is the period between full moon and half-moon.
[7]A night VFR rating ensures a pilot has the knowledge and skills necessary to safely operate and navigate an aircraft under visual flight rules at night.
[8]In the north of Australia, cattle mustering ordinarily takes place in the dry season, from around April to November.
Occurrence summary
Investigation number
AO-2025-063
Occurrence date
09/10/2025
Occurrence time and timezone
19:29 Australian Eastern Standard Time
Location
25 km south-south-east of Kowanyama
State
Queensland
Report release date
06/05/2026
Report status
Final
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain
Occurrence class
Accident
Highest injury level
Fatal
Aircraft details
Manufacturer
Robinson Helicopter Co
Model
R22 Beta
Registration
VH-LYD
Serial number
4471
Aircraft operator
MDH Pty Ltd
Sector
Helicopter
Operation type
Part 91 General operating and flight rules
Activity
General aviation / Recreational-Aerial work-Observation and patrol
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 13 September 2025, the pilot of a Eurocopter AS 350 B2 helicopter was conducting aerial fire suppression operations over an active grass fire in regional North Queensland. The helicopter was about 500 ft above ground level, with about 50 kt airspeed and a laden water bucket. At about 1220 local time, the helicopter completed a turn and the pilot reported feeling a jolt and observed, via an external mirror, the water bucket and attached line falling from the helicopter. The bucket and line impacted the ground causing significant damage to the bucket but no other damage or injuries.
The pilot recalled that, at the time the bucket released from the helicopter, their hands were clear of the cyclic cargo release button and manual release handle. The pilot landed the helicopter immediately and advised the helicopter operator of the incident.
Shortly after landing the pilot conducted a post-flight inspection. There was no damage to the helicopter, however the pilot was able to replicate the cargo hook unintentionally opening by moving the assembly in certain directions (Figure 1 shows the type of cargo hook fitted). The pilot later determined that the manual release cable had been incorrectly rigged. They observed a loop in the manual release cable prior to the cable entering the cargo hook assembly that caused the cable to tension and triggered the opening of the cargo hook.
Figure 1: Cargo hook used by the operator’s AS350
Source: Onboard Systems, annotated by the ATSB
Safety message
The uncommanded release of an underslung load has the potential for fatal consequences, damage to property and the load itself. Another occurrence of an underslung load being released without pilot input from a Eurocopter AS 350 helicopter as a result of the incorrect rigging of the cargo hook manual release cable has been detailed by the ATSB (AB‑2024‑033).
Although the rigging mechanism of the manual release cargo hook cable is not visible to the pilot during a pre-flight inspection, pilots intending to conduct underslung operations are encouraged to check for correct rigging and, if possible, simulate the full range of cargo hook movement prior to flight to observe any abnormalities.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
The Australian Transport Safety Bureau has published the final report from its investigation into an accident involving a Cirrus SR22 light aircraft near Gundaroo, north of Canberra, which fatally injured four people.
The four-seat, single-engine aircraft had taken off from Canberra Airport on 6 October 2023 with a pilot and three passengers on board, for a planned flight to Armidale, NSW, operating under instrument flight rules.
About 12 minutes after take-off, the aircraft aerodynamically stalled and departed from controlled flight. It then entered a high vertical descent which developed into a spin, before impacting the ground.
The aircraft came to rest in an open field adjacent to a farm dam wall and was consumed by a post‑impact fire.
ATSB Chief Commissioner Angus Mitchell said extensive damage from the collision and post‑impact fire limited the ATSB’s ability to determine the circumstances preceding the accident.
“The lack of available evidence made this investigation extremely challenging and, unfortunately – particularly given the tragic loss of four lives – limited the findings the ATSB could make,” Mr Mitchell said.
Flight data showed that, at about 8,000 ft, the aircraft began to deviate from its track, with heading, altitude and airspeed deviations. Then, when approaching 10,000 ft, the aircraft’s climb rate increased significantly and its airspeed decreased, resulting in the aerodynamic stall and departure from controlled flight.
The investigation found no evidence of any recovery actions being conducted after the aircraft stalled, and that the ballistic recovery parachute – an emergency parachute that when activated by the pilot supports and lowers the aircraft to the ground – was not deployed.
Additionally, no radio broadcasts were heard from the pilot during the accident sequence, or to indicate any issues prior to the stall.
“The ATSB considered several scenarios to establish the reason for the deviations in flight track, the subsequent stall, the absence of any recovery actions, and the non-deployment of the aircraft’s parachute system,” Mr Mitchell said.
“These included in-flight icing, pilot incapacitation, and technical issues with the aircraft, but the lack of available evidence could not definitively support or dismiss any of these hypotheses.”
The investigation report notes it was likely the aircraft, which was not fitted with an anti-icing system and was prohibited from operating in icing conditions, had encountered icing conditions prior to the stall.
Moderate icing conditions were forecast along the aircraft’s flight path from 7,000 ft to 10,000 ft when in cloud.
But the ATSB was unable to determine if these conditions were sufficient to have adversely affected the aircraft’s performance and/or handling, and icing would not prevent the deployment of the aircraft’s parachute system.
Meanwhile, an independent forensic pathologist did not identify any underlying medical conditions, natural disease or toxicological abnormalities that could have led to an incapacitation event. However, the report notes that medical incapacitation can result for reasons that may not be detectable.
Finally, to the extent possible, an inspection of the remaining aircraft structure and flight controls did not identify any pre-accident anomalies.
“Unfortunately, due in part to the significant post-impact fire limiting the collection of evidence, the circumstances preceding the stall and this tragic accident could not be conclusively determined,” Mr Mitchell said.