The ditching of an R22 helicopter during a Queensland flood rescue highlights the importance of pilots and operators carefully considering risks and alternatives when conducting a mercy flight, an ATSB investigation report details.
On 27 March 2025, mustering company Channel Country Helicopters was requested to assist with the flood evacuation of the town of Adavale, in south-west Queensland, deploying three two-seat R22 light helicopters in response.
After arriving overhead the town, the pilot of one of the helicopters spotted a person stranded on the roof of a demountable building that had a strong flood current flowing around it and, assessing the situation as critical, landed on a flat roof section to pick them up.
Once on board the rescued passenger, who was wearing wet clothing and carrying essential medical gear, put the helicopter about 46 kg over its maximum take-off weight.
That meant that as the helicopter took off and left ground effect, it had insufficient performance available to climb or maintain altitude.
“This was an unfamiliar and demanding rescue operation for the pilot, who, under time pressure due to the perceived imminent risk of a roof collapse, did not assess available performance after boarding a heavier than expected passenger and committed to the rescue with an immediate take-off,” ATSB Chief Commissioner Angus Mitchell said.
“The operator and pilot felt an understandable and commendable moral obligation to conduct a rescue operation, but they were neither trained nor equipped for such scenarios, and the pilot attempted a take-off with the helicopter significantly overweight.”
Mr Mitchell noted the pilot’s subsequent actions contributed to a controlled ditching that allowed both occupants to safely exit the helicopter.
“The pilot correctly followed the procedure for low rotor RPM, and made a controlled ditching in the only sheltered area available, in the lee of a building about 60 metres away, allowing the helicopter to remain upright in the otherwise fast-flowing water,” he said.
After exiting into chest deep water, the passenger avoided the strong current by standing close to the helicopter, but sustained chemical burns from fuel seeping out of the helicopter’s tank.
The pilot, meanwhile, attempted to return to the take-off site to retrieve a ladder, but was swept away by the current before finding shelter in a tree about 900 metres downstream.
The pilot was subsequently rescued by a larger helicopter and the passenger was rescued by a police officer, who had commandeered a small motorboat.
Mr Mitchell acknowledged the important role volunteers play in emergency response in Australia, including through mercy flights, which by definition are outside the scope of normal operations for pilots and operators.
“Mercy flights can save lives when dedicated, trained assistance is not available,” he said.
“This investigation should not deter pilots and operators from conducting mercy flights, but rather highlight that when responding to an emergency it is important to stop and take a moment to assess risk to the rescuers before assisting others.”
The Australian Transport Safety Bureau (ATSB) has launched a transport safety investigation into a collision with terrain accident involving a Robinson R22 helicopter just outside Bankstown Airport, in Sydney’s south-west, on Friday.
The piston engine helicopter had been conducting a training flight with an instructor and student pilot on board when it collided with terrain and was destroyed.
The ATSB is deploying a team of transport safety investigators from its Canberra office, specialising in operations, engineering and maintenance.
Planned activities include site and wreckage examination, mapping of the site, and recovery of any helicopter components for further examination at the ATSB’s technical facilities in Canberra.
Investigators are also collecting relevant recorded information including any flight tracking data, weather information, and pilot and helicopter maintenance records.
The ATSB asks anyone with video footage of the helicopter at any phase of the flight, or in the immediate aftermath of the accident, to make contact via the witness form on our website: atsb.gov.au/witness at their earliest opportunity.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
At about 0625 local time on 6 September 2025, the pilot and sole occupant of a Robinson R22 helicopter departed Cloncurry Airport, Queensland, to conduct commercial aerial mustering operations about 100 km north of Cloncurry. At about 0830 the pilot identified a small mob of cattle under trees in a dry creek bed. Attempting to move the stock, the pilot turned the aircraft downwind and recalled the aircraft descended during the turn. While attempting to arrest the rate of descent the pilot increased power as they attempted to avoid a dead tree which they estimated was about 6–8 m high. However, as the aircraft was already at maximum power the pilot was unable to gain sufficient height and the helicopter collided with the tree.
The pilot recalled the tree penetrated the windscreen and that the helicopter began to rotate. The helicopter then impacted terrain on its left side, temporarily rendering the pilot unconscious. The aircraft came to a stop in a dry creek bed about 20 m from the impact tree. The helicopter sustained substantial damage: the tail rotor and horizontal stabiliser separated from the main fuselage during the accident sequence and were located in close proximity to the tree (Figure 1).
Figure 1: Occurrence aircraft
Source: LifeFlight, modified by the ATSB
After regaining consciousness, the pilot recalled they were held in their seat by the seatbelt and freed themselves from the wreckage. They contacted nearby ground crew on motorcycles via two-way radio to request assistance. The operator advised that the onboard tracking and phone records showed the pilot then called the operator about 15 minutes after the impact with the tree.
The pilot had been wearing a helmet which sustained minor damage. The pilot sustained serious injuries that included cracked vertebrae and was airlifted to Mount Isa hospital later that morning.
The 2014 CASA aerial mustering sector risk profile identified some of the key risks during aerial mustering operations stating:
The aerial mustering sector is hazard rich due to the inherent characteristics of the operation, such as very low level flying, high workload, negative effects from weather, obstacles such as power lines, trees, and terrain, pilot distraction, small power margins, and extended time operating within the shaded area of the height/ velocity diagram (‘deadmans curve’). In some parts of Australia, military aircraft may intrude into airspace above cattle stations which could cause airborne conflict. Pilot training, supervision and mentoring play an important role in developing pilot skills to manage aerial mustering manoeuvres.
Safety message
Aerial stock mustering involves operating in an inherently hazardous environment – aircraft are manoeuvred at very low level, close to obstacles. Low‑level operations in small helicopters often result in minimal available power margins because reduced airspeeds and abrupt manoeuvring of the helicopter both require additional power. When the helicopter’s power required is greater than the power available, the aircraft is unable to maintain height and can cause the pilot to attempt to apply additional collective[1] pitch. The result is a reduction in rotor RPM and therefore further loss of altitude. Also, low‑level flight reduces the time available for pilots to apply corrective techniques to restore rotor RPM and level flight.
Several Robinson Helicopter Safety Notices discuss the risks involved with low rotor RPM and are available on its website robinsonheli.com.
Operators and pilots of Robinson R22 and other smaller helicopters, especially those used for low-level aerial work such as mustering, are encouraged to review the causes, effects and recovery techniques for low rotor RPM and ensure they avoid low rotor RPM situations at low level in environments where obstacles may present a significant hazard.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]The collective control changes the pitch angle of all main rotor blades.
A preliminary report has been released from the ongoing transport safety investigation into the derailment of a suburban passenger train at Clifton Hill, in Melbourne’s north, in July.
The report details the series of events prior to, during and after the derailment, based on evidence gathered to date in the investigation being conducted under a collaboration agreement with the Australian Transport Safety Bureau (ATSB) by the Office of the Chief Investigator (OCI)*.
The derailment occurred on the evening of 13 July 2025, when a Metro Trains Melbourne (MTM) X’Trapolis train was conducting a passenger service from Mernda to Flinders Street station.
After departing Rushall station towards Clifton Hill, the train initially accelerated to about 38 km/h, before the driver reduced the speed in preparation for the right curve over the High Street bridge.
The train was proceeding through the curve at about 28 km/h, below the 40 km/h permitted speed, when the leading wheelset of the first bogie of the train’s fifth car derailed on the bridge.
“Witness marks show the left wheel of this wheelset climbed over the left rail, towards the outside of the right curve,” Chief Investigator Mark Smallwood said.
“As a result of the leading wheelset moving to the left, the right wheel dropped to the inside of the right rail.”
“Initially the derailed wheels moved along the sleepers in close proximity to the rails,” Mr Smallwood stated.
“However, once off the bridge deck, the path of the derailed wheelset began to move further to the left until the front left corner of the fifth car and its first bogie struck a stanchion, part of an overhead wiring gantry.”
The impact of the bogie with the stanchion further rotated the bogie in an anticlockwise direction, derailing its trailing axle. The stanchion was substantially damaged by the impact, which caused the overhead wire that supplied electrical power to trains to move and lose tension.
This resulted in electrical arcing between the overhead wire and the train.
Alerted by the electrical arcing and overhead wire movement, the drivers made a brake application to stop the train. In total the train travelled about 120 m in a derailed state.
The train, track and overhead infrastructure were damaged in the derailment, but none of the approximately 30 passengers, nor the two drivers, were injured.
After the derailment, passengers were moved into the leading car of each three-car set (the first and fourth cars of the train) to wait until it was safe to detrain. Detraining was completed about 3 hours after the derailment.
Said ATSB Chief Commissioner Angus Mitchell:
“As the ‘no blame’ investigation continues, it will include analysis of factors potentially related to the nature of the derailment, including rolling stock wheel and suspension component condition, track condition and maintenance, and wheel to rail contact conditions.
“The investigation will also consider the emergency response to the derailment and overhead damage,” Mr Mitchell said.
A final report will be released at the conclusion of the investigation.
“Should a critical safety issue be identified prior to the conclusion of the investigation, relevant parties will be notified immediately so appropriate and timely safety action can be taken,” Mr Mitchell concluded.
* OCI is the operational office of the Chief Investigator, Transport Safety, a statutory position established in the Transport Integration Act 2010 (Vic) to provide independent, no blame investigation of transport safety matters in Victoria.
Under the collaboration agreement with the ATSB, OCI staff exercise powers and perform functions under the Transport Safety Investigation Act 2003 (Cth), and reports are approved for release under the TSI Act by the ATSB Commission.
The pilot of a Pilatus PC-12 was likely affected by sun glare when the aircraft was aligned to land on a taxiway at Launceston Airport, before manoeuvring at low level to align with the runway and then going around, an ATSB final report details.
The single-engine turboprop aircraft was operating a charter flight from Essendon, Victoria, to Launceston, Tasmania, with a pilot and four passengers on board, on 13 June 2025, the report details.
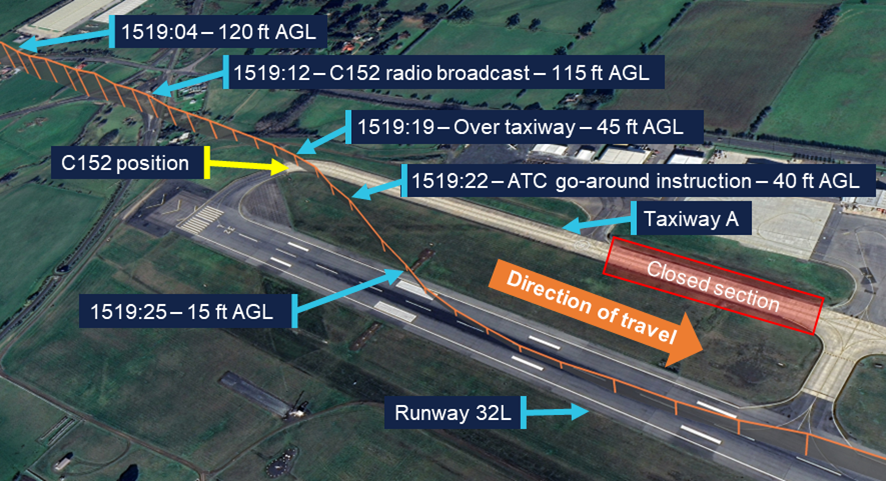
As the aircraft was on approach to Launceston Airport’s runway 32L in clear conditions with the sun low in the sky and 10° to the left of runway heading, the pilot misidentified the parallel taxiway as the runway, and aligned the aircraft with the taxiway’s extended centreline.
When at a low level, the pilot became aware they were approaching the taxiway.
They then conducted a low-level right then left turn to realign with the runway, before commencing a missed approach. After a visual circuit the aircraft landed without further incident.
During the approach to the taxiway, a Cessna 152 was waiting at a holding point with an instructor and student pilot on board.
The Pilatus passed 15 m behind the holding point approximately 45 ft above ground level. The pilot later reported they were not aware of the Cessna at the holding point at the time of the incident.
While landing on the taxiway would likely have resulted in the PC-12 passing over the Cessna, it would probably have resulted in a collision with airport construction works obstacles further down the taxiway.
“The final approach was conducted in clear conditions almost directly into the sun, exposing the pilot to glare,” ATSB Director Transport Safety Stuart Macleod said.
“When flying visually in such conditions, pilots should crosscheck against available flight and navigation instruments in conjunction with external indicators, such as airport lighting, to verify that the aircraft is on the intended flight path.”
The investigation also found that once they identified they were approaching the taxiway, the pilot corrected the aircraft’s flight path at a low level, rather than conducting an immediate missed approach.
“If a discrepancy is identified below an appropriate stabilised approach height, an immediate missed approach should be conducted,” Mr Macleod noted.
Following the occurrence, the aircraft operator, Armada Aviation, made changes to its operating procedures, including updating the final decision to proceed to landing to include a requirement that the runway was confirmed and clear by 400 ft above ground level, or the approach minima.
A discrepancy in the training and guidance provided to the pilot of a Cessna Citation contributed to a runway overrun in wet conditions at Bankstown Airport, an ATSB investigation has found.
On 11 January 2025, the Citation Mustang light jet was conducting a medical transport flight from Narrandera to Bankstown, New South Wales, with a pilot, a flight nurse and a patient on board.
While landing on Bankstown’s runway 11C, the pilot experienced reduced braking performance and the aircraft overran the end of the runway by about 30 m, coming to a rest in muddy ground. The occupants were uninjured, and the aircraft undamaged.
An investigation by the ATSB identified several factors contributed to the serious incident.
There was likely standing water on the runway, and the aircraft’s main landing gear tyres were worn to limits. The aircraft had also encountered an undetected tailwind on approach, raising the groundspeed above the minimum aquaplaning speed.
Encountering braking issues during the landing, the pilot cycled the anti-skid system, which likely further decreased braking performance.
The investigation also found when determining the required landing distance at Bankstown, the pilot had applied an incorrect landing distance factor, which was prescribed by the operator, AirMed.
“AirMed required, and its associated type rating training provider Air Link taught, pilots to apply an 80% landing distance factor when determining the distance required at a destination aerodrome, rather than the 60% figure required in the relevant regulations,” ATSB Chief Commissioner Angus Mitchell said.
“This reduced the safety margin when determining the required landing distance.
“Furthermore, AirMed’s procedures were unclear on how the factor should be applied, when the assessment should be conducted, and how runway surface conditions should be considered.”
In response, both AirMed and Air Link have updated relevant material to correct the landing distance factor. The operator also introduced the requirement to conduct a landing distance calculation both before take-off, and prior to landing.
In addition, while not directly relevant to the investigation’s findings, Bankstown Airport has amended the runway 11C/29C longitudinal slope information in the aerodrome manual to align with the En Route Supplement Australia slope values, and the Civil Aviation Safety Authority has amended the performance section of the Part 121 guidance material as part of its continuous improvement process.
Mr Mitchell acknowledged the safety action taken by multiple parties since the incident.
“The use of safety margins on top of calculated take-off and landing distances provides mitigation for a wide range of issues that can impact performance, including unexpected environmental conditions,” he said.
“As this occurrence demonstrates, there are limitations on accurate and timely reporting of runway surface condition – particularly after intense rainfall, given only 3 mm of standing water is required for a runway to be considered contaminated.”
The crew of a Boeing 737 continued an approach and landing at Sydney Airport despite the aircraft not meeting the stabilised approach criteria before it descended below the relevant altitude, an ATSB investigation report details.
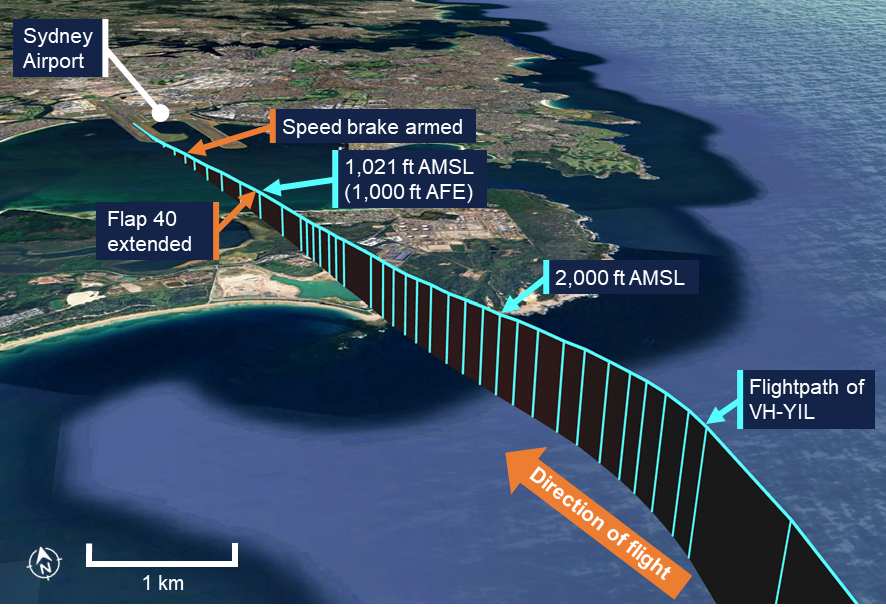
The Virgin Australia Boeing 737-800 was on descent to Sydney at the end of a flight from Brisbane on 12 June 2025 when air traffic control provided clearance to conduct a visual approach to runway 34 left.
At this time, a required autopilot altitude selection was not completed and, a short time later, the aircraft deviated above the desired approach path.
“The captain, who was pilot flying, responded by disengaging the autopilot and auto thrust to manually re‑establish the approach descent profile, but without alerting the first officer to their intention,” Director Transport Safety Stuart Macleod explained.
“This led to an unexpected increase in flight crew workload and reduced the situation awareness of the first officer, who was pilot monitoring.”
The crew subsequently missed 2 required checklist items: the speed brake was not armed, and the final flap selection was not made before the aircraft descended below 1,000 ft above the airport elevation.
“This meant the operator’s stabilised approach criteria were not met, and as such the flight crew should have conducted a go-around,” Mr Macleod said.
The correct landing flap selection was made three seconds after the aircraft passed through the 1,000 ft stabilised approach criteria altitude.
Later, the captain identified the unarmed speed brake, and armed it as the aircraft descended through 405 ft.
After landing, the captain discussed the incident with the first officer and assessed that a missed approach should have been conducted.
Mr Macleod noted unstable approaches are a precursor to approach and landing accidents and runway excursions.
“A small oversight can quickly disrupt an otherwise standard approach, leading to a breach of the stabilised approach criteria,” he said.
“Early recognition of an approach becoming unstable and promptly executing a go-around significantly reduces the risk of approach and landing accidents.”
Mr Macleod noted that the incident demonstrates the importance of effective crew resource management, particularly when crews are faced with the unexpected.
“Effective flight crew monitoring is paramount to aircraft safety,” he said. “Bringing deviations to the attention of the pilot flying ensures that the aircraft remains on a safe flight path and is correctly configured for the relevant phase of flight.”
On the evening of 8 September 2025, a Cessna T210M, registered VH-LLM, was conducting night take-offs and landings at Darwin Airport, Northern Territory. On board was an instructor from a training organisation and a student who was doing their first night training flight and owned the aircraft. After completing several take-offs and landings, the instructor directed the student to conduct a go-around. Shortly after turning downwind, the aircraft lost power. The student handed control of the aircraft to the instructor and made a MAYDAY call.
The instructor initiated troubleshooting checks and determined that the fuel selector was set on the right tank and was likely empty. The instructor activated the electric fuel pump before selecting the left tank which restored engine power and the aircraft was recovered into a climb. The student resumed control and proceeded to land safely at Darwin Airport.
What the ATSB found
Fuel was not selected to the fullest tank during multiple circuits resulting in a loss of power.
The student did not effectively conduct the pre-landing checks to monitor the fuel state of the aircraft. This was likely due to an increased workload during their first night flight in controlled airspace. In addition, the configuration of the primary flight display was changed to show airport maps, resulting in a smaller fuel gauges display in a different location, unfamiliar to the student.
The instructor had identified that the student had not changed tanks during previous circuits (a requirement to land on the fullest tank) and had intended to discuss this. However, the instructor later became focused on monitoring the student’s performance and forgot to brief the student on changing to the fuller tank.
In addition, before the flights, the student did not visually inspect the quantity of fuel on board the aircraft prior to departure and relied on the instructor’s recollection the aircraft had adequate fuel for the training session.
Safety message
Fuel starvation occurrences can often be prevented by conducting thorough pre-flight fuel quantity checks combined with in‑flight fuel management.
Although pre-landing checks are routine, they must never become perfunctory. Pilots must understand the purpose behind each check, ensuring the aircraft is properly configured for landing according to the aircraft guidance.
Pilots are reminded to independently visually check fuel quantities prior to departure and use a known calibrated instrument such as a dipstick in addition to fuel gauge readings.
Pilots should familiarise themselves with the Civil Aviation Safety Authority, Advisory Circular AC 91-15v1.1 Guidelines for aircraft fuel requirements, which provides further guidance for in‑flight fuel management.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the evening of 8 September 2025, a Cessna T210M, registered VH-LLM, was being used to conduct night visual flight rules (NVFR) training circuits[1] at Darwin Airport, Northern Territory. The student was a licensed pilot who owned VH-LLM, and also on board was an instructor from the training organisation, Flight Standards.
The day before the flight, the student refuelled the aircraft to capacity and flew it from Emkaytee aerodrome, Northern Territory, to Darwin Airport. On the morning of the training session, the instructor, who had not previously flown a turbo Cessna 210, took the aircraft for a familiarisation flight, accompanied by Flight Standards’ chief flying instructor. The student reported that they had given permission for the flight but were unaware of the route taken or the amount of fuel used.
The instructor recalled dipping the fuel tanks after completing the familiarisation flight that morning, recording a total of about 55 L in the left tank and 75 L in the right tank. The instructor assessed that the total remaining fuel quantity was sufficient for the planned night circuit training session.
The student arrived at the airport at about 1800 local time[2] and conducted a pre-flight check with the instructor. The student asked whether there was sufficient fuel in the aircraft for the flight and received confirmation from the instructor that there was sufficient fuel. Subsequently, no visual inspection of the aircraft fuel quantity was carried out by the student.
For the flight, the student occupied the left seat with the primary flight display (PFD) directly in front of them and the instructor sat on the right. The student reported noticing that the instructor had altered the configuration of the PFD from their normal set up of engine instruments, to a split screen with a map of Darwin Airport taxiways on the right of the screen.
As this was the student’s first night flight the instructor reported spending additional time briefing the student on night circuits after engine start, which included aircraft lighting and other general information for night flying, before the student conducted engine run-ups at about 1914. During this time, the fuel selector was positioned on the left tank.
The aircraft pilot operating handbook (POH)[3], as well as the training organisation’s flight crew operating manual (FCOM), stated that it was a requirement to take off and land on the fullest tank. The student reported that at the beginning of the flight, this was the right tank. Before handing control to the instructor to demonstrate the first circuit, the student switched from the left to the right tank.
After completing the demonstration, while on the runway, the instructor briefed the student on the focus of the next circuit before the student took control from the left seat.
At about 1952, on completion of the student’s first landing, the instructor noticed that the student had conducted the pre-landing fuel check using a non-standard mnemonic checklist and identified that the student did not turn on the landing lights and that the flaps were not at the correct position. The student did not change the fuel selector from the right tank. As the instructor believed there was more fuel in the right tank at that time, they were comfortable with the student’s actions and did not direct them to change tanks before continuing with the next circuit. The instructor reported they debriefed the student on checklist discipline.
The fuel selector was not changed on the student’s second or third circuit. The instructor noted that the student’s use of a mnemonic checklist was not completely effective in ensuring that the actions in the checklist were completed for landing. In particular, this included that the student’s checklist did not cover the challenge/response to the fuel check as per the POH to ensure that the fuel selector was set to the fullest tank. The student reported their increased concentration on flying the aircraft at night detracted from monitoring the fuel gauge in the altered position. The instructor reported they had planned to request the tanks be changed on the next downwind leg.
At about 2030, during the student’s fourth circuit, the instructor directed the student to conduct a go-around[4] while on the final approach due to an aircraft behind them. The instructor recalled that the go-around was not completed proficiently and mentally noted to brief the student at the next opportunity to change the fuel selector to the left tank.
At 2032:57, recorded data showed that the right fuel tank indicated zero fuel before conducting the go-around, but the aircraft engine continued running using fuel in the lines and header tank (Figure 1).
At 2037:32, after turning onto the downwind circuit leg, the engine began to lose power and, realising that a return to the airport was not achievable, the student handed control to the instructor. The instructor conducted troubleshooting while the student declared an emergency to air traffic control (ATC).
The instructor identified that the aircraft fuel selector was positioned on the right fuel tank and realised that the tank, which had not been changed since beginning the circuits, was likely empty. They followed the POH procedure to change tanks, activated the auxiliary fuel pump and changed the fuel selector to the left tank. This restored engine power and they initiated a climb. The aircraft was at 600 ft above ground level at this time, and the crew heard an alert from ATC. The student responded and cancelled the emergency with the tower.
Once established in the climb, the student assumed control, recovered the aircraft back into the circuit and landed safely at Darwin Airport without further incident.
Post-flight inspection by maintenance personnel reported no mechanical defects with the aircraft fuel system or engine.
Figure 1: Graphical depiction of the occurrence circuit
Source: Google Earth, annotated by the ATSB
Context
Pilot information
Instructor
The instructor attained their Commercial Pilot Licence (Aeroplane) in 2021 with class ratings for single and multi-engine aircraft. They completed their Grade 2 instructor qualifications in December 2024. They held an NVFR endorsement and had a total of about 1,270 flying hours, of which about 800 hours were instructional. The instructor reported that at the time of the occurrence they had accrued 27.6 hours of night flight experience. Their most recent night flying activity prior to the occurrence was a flight instructor rating flight test conducted on 28 July 2025. The instructor was subsequently approved by the operator to carry out instructional flights at night, and the occurrence flight was the first instance of this.
The instructor had about 70 hours experience in non‑turbocharged models of Cessna 210 aircraft. The instructor held a current Class 1 medical certificate.
They reported sleeping for 8 hours the night before the occurrence and identified that they had slept for about 4 hours that afternoon. They reported their level of alertness as a ‘3‑ Okay somewhat fresh’ on a scale of 1–7 where, 1 is fully alert and 7 is completely exhausted.
Student
The student held a Private Pilot Licence (PPL) for a single‑engine aeroplane issued in 2018, held a current Class 1 medical certificate and had a total experience of about 412 hours of which 123.5 hours were completed in VH-LLM. They had completed 2 NVFR training sessions in the Flight Standards’ simulator prior to the occurrence. The student had flown day VFR for several years and wished to obtain a NVFR endorsement along with practice in procedures for Class C controlled airspace.
The student reported having a normal amount of sleep the night before and following their usual routine of breakfast and a light lunch. They worked a busy but uneventful day from about 0800 before arriving at the airport for the lesson at 1800. The student indicated they were fully alert on a scale of 1–7, where 1 is fully alert and 7 is completely exhausted.
Aircraft information
The aircraft was a Cessna Aircraft Company T210M, 6‑seat, high-wing aircraft manufactured in 1977. It was powered by a Teledyne Continental Motors Inc TSIO-520 turbocharged, fuel‑injected piston engine driving a 3-bladed, constant-speed McCauley propeller. The cockpit consisted of side-by-side seating for the pilot/student on the left and instructor/passenger on the right. The aircraft was initially registered on 6 June 1989 and then transferred to the current owner on 27 March 2023.
Glass cockpit
The cockpit of VH-LLM had been retrofitted with a customisable Garmin G3X suite (GI 275) glass cockpit.[5] The student reported that on the night of the training session the instructor had changed the screen from the configuration that the student was previously used to. This included a change to the location of the fuel gauge which was positioned at the far left of the screen rather than on the right (Figure 2).
Figure 2: Photograph of VH-LLM Garmin G3X screen configuration changes
Source: Aircraft owner, annotated by the ATSB
The instructor reported that there were no audio or visual fuel‑related alerts associated with low fuel quantities or reminders to switch the fuel tank selection in the display. The instructor reported that the location of the fuel gauge was difficult to see from their seat position on the right-side of the aircraft.
Both the student and instructor reported that the fuel gauge was less visually prominent in the new screen configuration and more difficult to monitor.
Fuel
The Cessna 210 fuel system consists of 2 main fuel tanks, 1 in each wing. Each tank has a capacity of 171 L, of which 169 L is usable. The fuel selector valve had 3 positions – left, right and off. Fuel could only be drawn from either the left or right tank during normal operations. The fuel system has an engine-driven fuel pump and an electrically‑driven auxiliary fuel pump. The pilot operating handbook (POH) stated:
If it is desired to completely exhaust a fuel tank quantity in flight, the auxiliary fuel pump will be needed to assist in restarting the engine when fuel exhaustion occurs.
The POH stated that a final 45 L reserve fuel should be available for operations. The chief pilot observed that 47 L remained in the left tank after landing.
Training organisation’s procedures for flight planning and fuel usage
The instructor reported that the training organisation’s fuel management guidance for circuit operations stated that circuit flights must plan to land with greater than final fuel reserve.[6]
The training organisation’s FCOM for the Cessna 210 (Section 2.5) stated that it was a requirement to take off and land on the fullest tank, with guidance in Section 7.1 stating:
For take-off and the first 30 minutes of flight, the fullest tank is selected and then tanks are cycled every 60 minutes thereafter, with the fullest tank selected for landing.
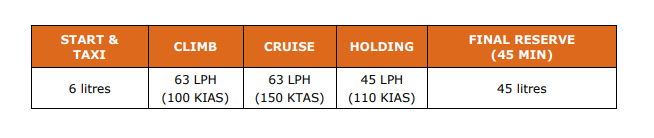
Section 5.3 provided typical fuel usage guidance in a table for fuel planning purposes (Figure 3).
Figure 3: Table provided for fuel management from the operator’s Cessna 210 FCOM
Source: Operator
The instructor commented that they were aware that the turbocharged 210 model had a slightly higher fuel burn, but they considered the amount of fuel available as adequate for the planned training session.
Meteorological information
The weather forecast for Darwin Airport indicated good flying conditions with no significant weather, no cloud below 5,000 ft, and visibility greater than 10 km. The automated observation at Darwin Airport for 2030 reported no cloud detected, visibility greater than 10 km, north‑easterly winds at 5 kt, temperature of 27°C and no rainfall.
Airport information
Darwin Airport is a joint civil and military facility. It services domestic and international air traffic and has 2 runways. The airport has an elevation of 103 ft above mean sea level (AMSL). The control tower provides a Class C controlled airspace around the airport, while outside of this area is class G uncontrolled airspace.
Recorded information
Flight data
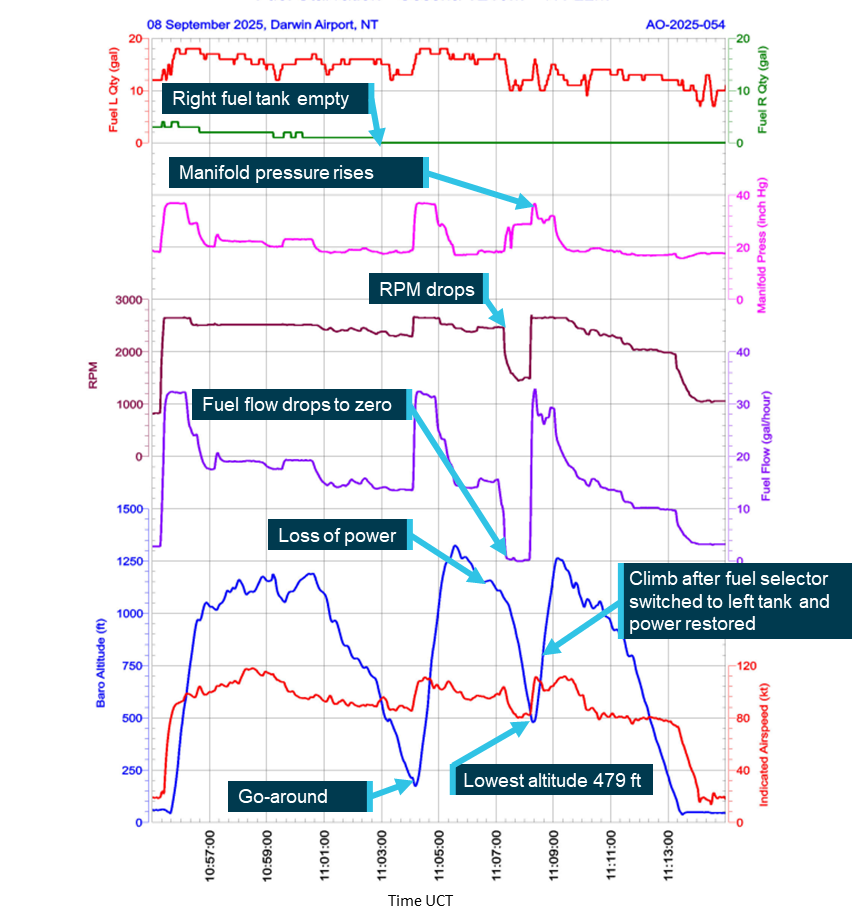
The Garmin G3X avionics suite recorded to a secure digital (SD) card which was analysed by the ATSB (Figure 4).
Recorded data indicated that during the last circuit, the aircraft had descended from about 1,200 ft to 479 ft AMSL before then climbing.
Figure 4: Data obtained from the VH-LLM Garmin G3X SD card
Source: ATSB
Fuel data
The recorded fuel data identified that fuel from the right tank had been fully used at 2032:57, prior to commencement of the go-around. Due to the residual fuel in the system and header tanks, the engine power loss occurred about 5 minutes later at 2037:32. After conducting engine troubleshooting, the power was restored at 2038:11.
Fuel starvation
Fuel starvation refers to where the fuel supply to the engine is interrupted, although adequate fuel remains on board the aircraft. Fuel exhaustion refers to where the aircraft has depleted all useable fuel.
An ATSB study Avoidable Accidents No. 5 Starved and exhausted: Fuel management aviation accidents (AR-2011-112) regarding fuel starvation accidents found that in addition to accurate knowledge of fuel quantity at the start of a flight, the risks for fuel starvation are increased when pilots forget to change tanks during periods of low workload, or when pilots forget to select the appropriate tank prior to the approach to land. Although tank selection for approach and landing is often specified in the aircraft flight manual, following this procedure will only be successful if the pilot has also ensured that there is sufficient fuel in the required tank for landing.
Cognitive resources
Cognitive ability is a finite resource to pilots, and the limit of its availability plays a role in determining how effectively a pilot maintains adequate performance. Workload is a term used to describe the ‘cost’ for a human to fulfil certain task requirements. This cost can be reflected in the depletion of cognitive resources, the inability to conduct additional activities, emotional stress, fatigue or decreased performance (de Souza Borges and others, 2023). Workload and performance are intricately related as task demands are actively managed through resource allocation and strategy change (Loft and others, 2023).
An intention to perform a task at some future time is known as a prospective task. Prospective memory involves remembering, and sometimes forgetting, to perform tasks that must be deferred (Dismukes, 2010; Harrison and others, 2014).
In aviation, individuals typically must manage several concurrent tasks and consequently are often forced to postpone or interrupt tasks and attempt to remember to perform the deferred tasks later. A significant issue in prospective memory is not retention of the content of intentions, but retrieval of those intentions at the appropriate moment, which is often vulnerable to failure. Typically, if queried after forgetting to perform an action, an individual can recall what they intended to do.
Related occurrences
Fuel starvation occurrences highlight the critical importance of proper fuel management and pre‑flight planning. Fuel management and fuel starvation incidents and accidents have regularly occurred with single and twin-engine aircraft. Examples of other similar ATSB investigations include:
Fuel starvation and forced landing involving Piper PA-28, VH-BDB, 15 km west‑south‑west of Bankstown Airport, New South Wales, on 19 September 2017 (AO‑2017‑094).
Fuel starvation event involving Cessna 310, VH-JQK, near Sunshine Coast Airport, Queensland, on 18 August 2022 (AO-2022-040).
Fuel starvation and forced landing involving Pilatus Britten-Norman Islander BN2A, VH‑WQA, Moa Island, Queensland, on 3 October 2022 (AO-2022-046)
Fuel starvation and forced landing involving Piper PA-31-350, VH-HJE, 11 km south of Archerfield Airport, Queensland, on 7 April 2023 (AO-2023-017).
Fuel starvation and ditching involving Piper PA-28, VH-FEY, 15 km north-west of Jandakot Airport, Western Australia, on 20 April 2023 (AO-2023-021).
Fuel starvation and forced landing involving Cessna 310R, VH-DAW, about 5 km south-east of Derby Airport, Western Australia, on 20 June 2023 (AO-2023-029).
Fuel starvation involving Cessna T210M, VH-MYW, 4 km north-west of Bankstown Airport, New South Wales, on 26 May 2024 (AO-2024-033).
Safety analysis
The flight crew of VH-LLM experienced a loss of engine power during a night training flight. The instructor took command of the aircraft and quickly diagnosed that the fuel selector was on the right-wing tank and had not been changed for the duration of the circuits. The instructor activated the electric fuel pump and changed to the left tank which restored fuel and engine power to the aircraft.
This analysis will look at the use of appropriate checklists and the management of fuel prior to and during flight.
Fuel management
Student
The student did not visually verify the fuel quantity in the aircraft when conducting pre‑flight checks, instead they relied on the instructor’s confirmation that the aircraft had sufficient fuel on board but without informing the student how much fuel was in each of the tanks.
The student reported not monitoring the fuel gauge (which had been relocated on the primary flight display) due to the screen configuration change from the display that they normally used. Although the student used a mnemonic for pre-landing checks which included the fuel, the check was not completed with the required response that the fuel selector was set to the fullest tank in accordance with the pilot operating handbook.
In addition, the student reported the fuel gauge checks were a consequence of their need to concentrate on flying the aircraft in the night environment. Night flying increases cognitive and perceptual workload due to the decreased visual cues, the requirement for increased instrument monitoring and the risk of spatial disorientation (Biernacki and others, 2024). Further, this was the first time operating at night in controlled airspace for the student. The additional workload likely limited the student’s capacity for systematic visual scanning of cockpit instruments.
Instructor
The instructor reported noticing the student not switching tanks for the first circuit but was satisfied with the student’s decision as the tank in use was the fullest tank at that point. The instructor intended to monitor this on further landings and brief the requirement if it continued. However, during subsequent circuits, their focus shifted to monitoring the student’s performance and other demands such as other aircraft and the execution of the go-around.
As this was the instructor’s first instructional flight at night, this would have increased the demands on their ability to effectively monitor all aspects of the flight and student. The focus on monitoring other aspects of the student’s performance led them to forget to brief the student on switching to the fullest fuel tank as they had intended. Research on attention (Harrison and others, 2014) indicates that demands of competing tasks can narrow attention to the task perceived as most important at the time, reducing the likelihood of recalling or completing other intended actions.
The instructor reported that their ability to monitor the fuel status was influenced by their restricted view of the fuel gauge which was not clearly visible during a normal visual scan.
Missed opportunities by the crew to effectively monitor the fuel status led to fuel starvation and engine power loss beyond glide range of the airport. This increased the risk of having to conduct an off airfield forced landing at night.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation event involving Cessna T210M, VH-LLM, near Darwin Airport, Northern Territory, on 8 September 2025.
Contributing factor
Fuel was not selected to the fullest tank at all during multiple circuits resulting in a loss of power.
The student did not effectively conduct the pre-landing checks to monitor the fuel state of the aircraft, likely due to an increased workload during their first night flight in controlled airspace and the change in configuration of the primary flight display.
The instructor identified that student had not changed tanks during previous circuits however became focused on monitoring the student’s performance and did not brief the student on changing to the fuller tank.
Other factors that increased risk
The student did not conduct a visual check of the fuel quantity prior to departure, relying instead on the instructor’s recollection of sufficient fuel being available.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Biernacki, M. P., & Lewkowicz, R. (2024). The role of visual conditions and aircraft type on different aspects of pilot workload. Applied Ergonomics, 118, 104268.
de Souza Borges, S. F., de Morais, P., Bovo, M. G., Castilho, D. S., & Junior, M. M. C. (2023). Evaluation of workload for operators in the aeronautical sector. Proceedings of the 33rd European Safety and Reliability Conference (ESREL 2023) Edited by Mário P. Brito, Terje Aven, Piero Baraldi, Marko Čepin and Enrico Zio
Dismukes, R. K. (2010). Remembrance of things future: Prospective memory in laboratory, workplace, and everyday settings. Reviews of human factors and ergonomics, 6(1), 79-122.
Loft, S., Tatasciore, M., & Visser, T. (2023). Managing workload, performance, and situation awareness in aviation systems. In Human factors in aviation and aerospace (pp. 171-197). Academic Press.
Harrison, T. L., Mullet, H. G., Whiffen, K. N., Ousterhout, H., & Einstein, G. O. (2014). Prospective memory: Effects of divided attention on spontaneous retrieval. Memory & Cognition, 42(2), 212-224.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the instructor
the student
the operator
Civil Aviation Safety Authority
Bureau of Meteorology.
Submissions were received from:
the instructor
the student
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Circuit: a standard flight path that aircraft follow when taking off and landing at an airfield, ensuring safe and orderly aircraft management.
[2]Local time was Australian Central Standard Time (ASCT) which is Coordinated Universal Time (UTC) + 9.30 hours.
[3]Pilot Operating Handbook: contains specific information about a particular aircraft, such as the equipment installed and weight and balance information. Manufacturers are required to include the serial number and registration on the title page to identify the aircraft to which the manual belongs
[4]Go-around: a manoeuvre where a landing approach is discontinued followed by a climb for another approach.
[5]The term ‘glass cockpit’ refers to a flat panel LCD display system that replaces the conventional analogue flight instruments in an aircraft. In this system primary flight information is presented on one or more integrated electronic flight displays.
[6]Usable fuel to reach the destination and then fly for at least 45 minutes after, at normal cruising power.
Occurrence summary
Investigation number
AO-2025-054
Occurrence date
08/09/2025
Location
Near Darwin Airport
State
Northern Territory
Report release date
28/01/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Engine failure or malfunction, Fuel starvation
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
T210M
Registration
VH-LLM
Serial number
21061937
Aircraft operator
Howard Springs Veterinary Clinic Pty Ltd
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into an accident involving a turboprop Pilatus Porter aircraft near Moruya, NSW, on Saturday afternoon.
As reported to the ATSB, the aircraft was returning to Moruya airport after conducting a skydiving drop when it collided with terrain. The pilot, the sole occupant on board, was fatally injured.
The ATSB is deploying a team of transport safety investigators from its Canberra and Brisbane offices, specialising in aircraft operations, maintenance and engineering, to the accident site.
Once on site on Sunday morning, investigators will conduct a range of evidence-gathering activities including site survey with a drone, wreckage examination, and recovery of any aircraft components for further examination at the ATSB’s technical facilities in Canberra.
Investigators will also seek to interview involved parties and witnesses, and collect relevant recorded information including flight tracking data, pilot and aircraft maintenance records, and weather information.
The ATSB asks anyone with video footage of the aircraft at any phase of the flight, or in the immediate aftermath of the accident, to make contact via the witness form on our website: atsb.gov.au/witness at their earliest opportunity.