Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
At 1241 local time on 14 September 2025, a Kawasaki Heavy Industries Ltd BK117 C‑1 helicopter with a crew of 3 lifted off from the operator's base in La Perouse, New South Wales, for a local search and rescue flight. Shortly after lift-off, at a height of around 50 ft, the cabin sliding crew door separated from its lower track while the rescue crewmember was holding on to the internal door handle. The door remained in position against the airframe and the crewmember continued to hold the door handle while notifying the pilot of the situation. The pilot immediately commenced a right orbit, climbing clear of the take-off zone before descending and returning to the base for an uneventful landing at 1242.
After the helicopter was secured on the ground, the rescue crewmember was able to re‑seat the door in position on its tracks, and after confirming it was properly closed, the flight resumed the intended mission at 1250.
Door information
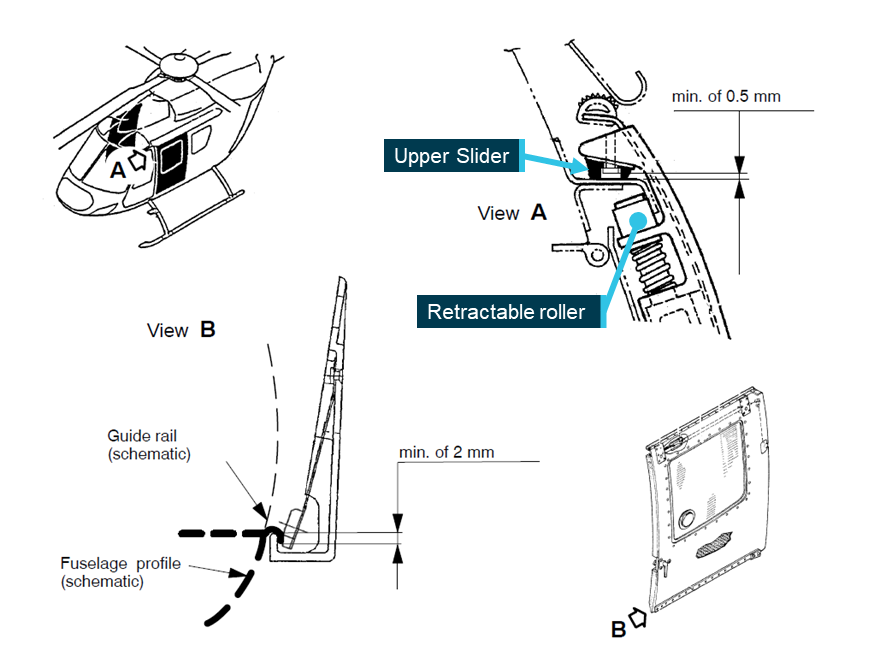
The BK117 crew cabin sliding door operates on upper and lower tracks (Figure 1), with front and rear sliding elements running along an upper recessed track. At the door base, front and rear guides engage with an inverted lip and are held in position with sliders on flexible plates.
The crew door is designed to be jettisoned from the helicopter in emergency situations – this is achieved by an internal actuating handle which retracts the 2 upper track rollers, freeing the door from the upper track and allowing it to move outward and downward away from the airframe.
Figure 1: BK117 crew door track detail
Source: Section of Figure 4 from Eurocopter Alert Service Bulletin ASB-MBB-BK117-20-111, annotated by the ATSB
Engineering inspection
The operator reported that an engineering examination of the door mechanism and tracks had found the door sliders and guides to be in a serviceable condition, with no wear exceeding permissible limits. The 2 upper track rollers were found with localised surface wear (flat spots), however, due to the design of the track, this damage would not have affected the door’s security.
The operator’s internal investigation concluded that the door’s emergency jettisoning mechanism had not been activated, however the factors contributing to the door separation had not been identified.
Safety message
Accidents and serious incidents have resulted from the separation of the BK117 crew access door, with the potential for door impact with the main and/or tail rotor assemblies presenting a serious risk to the safety of flight.
Operators and crew of BK117 helicopters and other aircraft with jettisonable doors must ensure that the jettison mechanisms are protected from inadvertent activation during flight.
Periodic inspection of the door operating and jettisoning mechanisms must be conducted in line with the manufacturer's published documentation and service bulletins.
Specific attention is drawn to European Union Aviation Safety Agency (EASA) airworthiness directive AD No. 2011-0107 and Eurocopter (Airbus Helicopters) Alert Service Bulletin ASB-MBB-BK117-20-111 (and related documents) for issues and actions relating to the security of the sliding cabin door.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 8 October 2025, around 2340 local time, as the vessel was engaged in an offshore construction operation a fire was detected in the laundry on the main deck. The Chief mate immediately went to the area and, after confirming that the fire was in the laundry, pressed the emergency stop button for the laundry equipment.
The fire alarm was raised and, in accordance with procedures, the vessel was stopped and the ongoing operation ceased. The crew were mustered and firefighting teams were dispatched to the laundry.
The fire was sourced to a faulty clothes dryer (Figure 1) and subsequently extinguished.
The likely cause of the fire was determined to be overheating of an electrical component of the dryer, most probably the transformer.
Figure 1: Fire damage to dryer
Source: Vessel operator
Safety message
Clothes dryer fires are common and can pose a serious safety hazard, especially on a ship. Various sources indicate that most dryer fires are caused by:
spontaneous combustion of residual soils, paint, oils, etc.
Confirming that everyone understands that they should raise the alarm before attempting to tackle a fire.
Ensuring systems for fire prevention, detection, protection and extinguishing, are communicated to all crew during vessel inductions and regularly reinforced thereafter.
Ensuring that the design of the tumble dryer filters, drums and exhaust ducting enable sufficient access to allow for cleaning and removal of build-up of material.
Ensuring all personnel are familiar with operations, maintenance and emergency procedures for equipment and machinery they are operating.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
A study into Australia’s growing hot air balloon sector advises pilots and operators on key areas of focus to improve safety, and recommends the use of a structured Safety Management System to identify and manage risk.
The ATSB conducted the safety study in line with one of its SafetyWatch priorities, Reducing passenger injuries in commercial ballooning operations, and after identifying a serious incident and accident rate in balloon operations around 10 times that of charter operations in aeroplanes and helicopters, on a per flight basis.
ATSB Chief Commissioner Angus Mitchell noted the sector’s overall exposure to risk had also increased recently with an increase in larger balloons, capable of carrying the maximum passenger limit of 24 per flight, on the Australian register.
While no fatal accidents occurred in the sector during the study period, from 2014 to 2022, the study did find ballooning carried a higher risk to fare paying passengers than similar operations in small aeroplanes and helicopters.
“On a per-flight basis, ballooning was more likely to have a serious incident or accident, and more likely to have a passenger injury, than equivalent operations in small aeroplanes and helicopters,” Mr Mitchell said.
Injuries, serious incidents and accidents were more likely to occur during landing than any other phase of flight, the study found.
“Balloons are distinct from other aircraft in that they travel by moving with the wind, with pilots achieving directional control by using differing wind directions at different altitudes,” Mr Mitchell said.
Of the 79 balloon occurrences reported to the ATSB during the study period, 35 cited wind as a safety factor, resulting in 8 serious incidents and 5 accidents.
15 of the occurrences attributed assessing and planning as a safety factor, resulting in 7 serious incidents and 3 accidents.
The study, available here, advises balloon pilots to use all available information sources, including approved Bureau of Meteorology products, to ensure they understand the weather, particularly the wind, and its influence on flight safety.
“Accurate weather assessment is critical for safe go/no-go decisions,” Mr Mitchell continued.
“Pilots should also apply threat and error management by anticipating risks such as powerlines and poor visibility, and prioritising safety over logistical pressures in adverse conditions.”
The study also urges balloon operators to consider implementing a Safety Management System.
“Although not required by legislation for balloon operators, implementing a Safety Management System provides a structured approach to identifying and managing risks,” Mr Mitchell said.
Beaudesert incident a case study
An ATSB occurrence investigation, released alongside the safety study, details an accident involving a large balloon during a morning scenic flight near Beaudesert, Queensland, on 7 July this year.
The final report notes the balloon, with 20 passengers and the pilot on board, encountered fog after clearing a ridge line.
During the approach to land in low visibility, an unexpected low-level wind shift diverted the balloon away from the preferred clear landing area.
The pilot then selected an alternate, unplanned landing site in the final stages of landing and, due to reduced visibility from fog, was unable to see obstacles in the final landing area.
On landing, the balloon basket was carried forward with momentum, skipping several times before coming to a stop. The balloon’s envelope collided with a dead tree during the landing, resulting in minor damage.
“This serious incident demonstrates the unique challenges faced by balloon pilots, dealing with dynamic and changing weather conditions,” Mr Mitchell said.
“It also demonstrates some of the safety steps operators can take to reduce risk.”
The final report notes comprehensive passenger safety briefings meant passengers adopted brace positions before the landing, which likely prevented injury.
“This accident highlights the importance of effective safety briefings and how passengers adopting the correct body position during landing – the most common phase of flight for serious incidents and accidents – substantially reduces the likelihood and severity of injury.
“We encourage all ballooning operators and pilots to review this material from the perspective of their operations, and consider how they can best ensure the safety of their passengers and aircraft,” Mr Mitchell concluded.
This interim report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Interim reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this interim report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
The occurrence
On 24 November 2025, hot and humid weather conditions prevailed over South East Queensland. Occurring during most of the month of November, these conditions were conducive to the formation of thunderstorms and had resulted in several significant storms developing across the region. These included storms affecting the Gold Coast and its hinterland, to the south of Brisbane, on 23 November. The Bureau of Meteorology (BoM) marine forecast for Moreton Bay for 24 November, issued at 0300, again warned of a chance of a thunderstorm during the afternoon or evening.
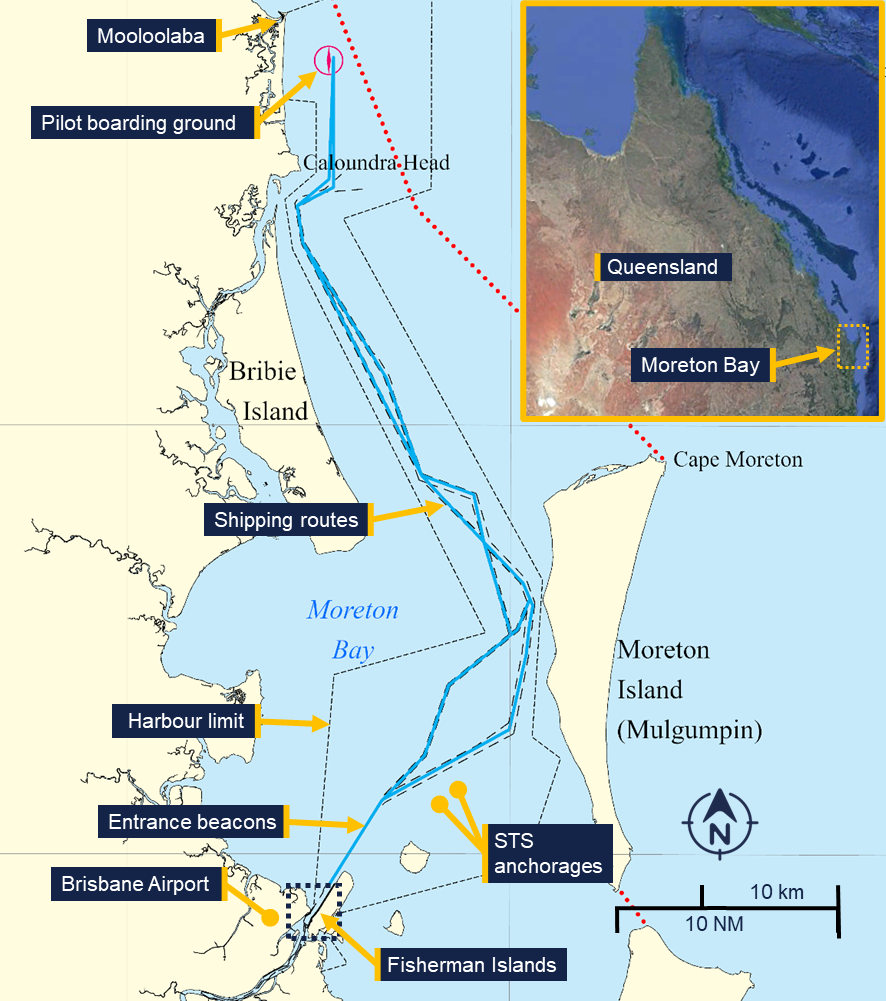
At 0930 the car carrier Viking Passama was inbound to the Port of Brisbane, preparing to embark a pilot at the Mooloolaba pilot boarding ground for its transit of Moreton Bay. It was following the oil tanker Cielo di Cagliari which had embarked a pilot at 0900 (Figure 1). Gas tanker Gaschem Iliad was anchored at ship-to-ship (STS) anchorage 1, waiting to enter the port following Viking Passama’s arrival, destined for an upriver berth.
Figure 1: Moreton Bay shipping routes, berths and anchorages
Source: Maritime Safety Queensland and Google Earth, annotated by the ATSB
The container ships MSC Barbara, Medkon Ten, Wide India and Volans had arrived in the Port of Brisbane in the preceding days. The ships were moored at the container berths of Fisherman Islands and were loading and unloading containers. As part of these routine cargo operations, hatch covers from Wide India and MSC Barbara were offloaded onto the berth.
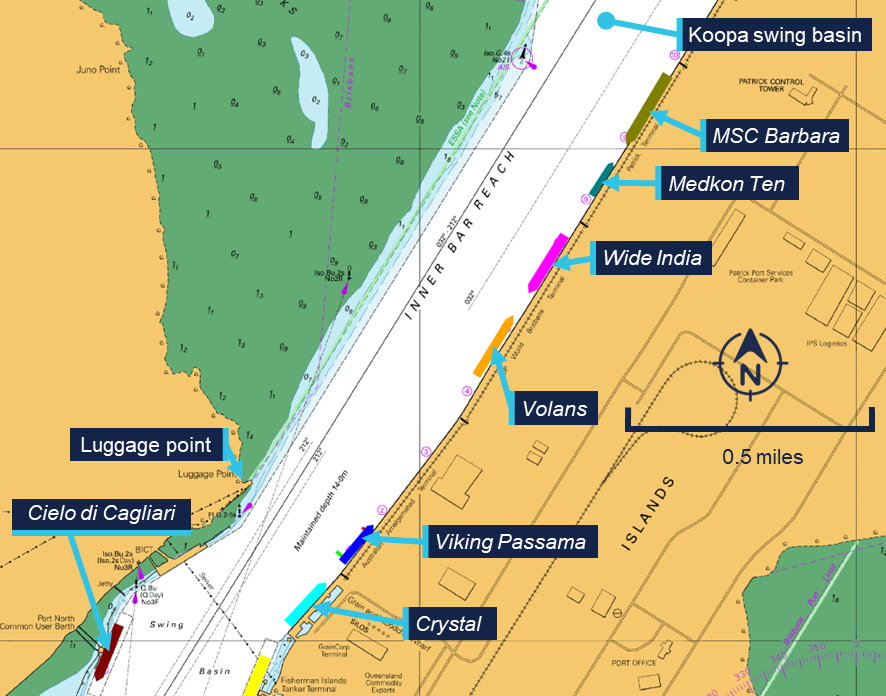
Additionally, the woodchip carrier Crystal was moored at the Fisherman Islands grain and woodchip wharf just south of Fisherman Islands berth 1 (Figure 2).
Figure 2: Mooring locations at Fisherman Islands preceding the storm
Source: Australian Hydrographic office, annotated by the ATSB
At 0945, the regional harbour master (RHM) for the Brisbane region received a BoM severe weather briefing from the state disaster coordination centre. It warned of ‘Potential isolated “very dangerous” thunderstorms with locally destructive winds and giant hail around South East Queensland during this afternoon and evening’. This was followed at 1022, by a weather update from Brisbane city council disaster operations that indicated the possible formation of storms in the Brisbane area in the late morning and afternoon. It also noted that severe storms were ‘possible to likely’ in the afternoon, and warned that isolated, very dangerous thunderstorm activity could not be ruled out, especially over the city’s western suburbs.
The RHM relayed the warnings to the Brisbane vessel traffic service (VTS) for distribution to port stakeholders and requested that ships moored at the Fisherman Islands container berths lower their outboard anchor and add extra mooring lines where possible. Brisbane VTS subsequently passed on the warnings to the various stakeholders in the port. This included a vessel traffic service operator (VTSO) contacting the operators of the container berths by telephone. The terminal operators then informed the crew on board the ships alongside and reported back to VTS that precautions had been taken as requested.
At 1045, Viking Passama embarked a pilot at the pilot boarding ground, inbound to the vehicle terminal at Fisherman Islands berth 1.
Viking Passama’s pilot had prepared for the pilotage early in the morning using the port’s proprietary planning software. The pilot noted that a weather front with up to 40 knots of wind was forecast to pass the Port of Brisbane at about 1400, coinciding with the expected arrival time of the ship. In response they requested a second tug to assist with berthing, with the understanding that these tugs would likely come to Viking Passama after being released from the preceding Cielo di Cagliari.
At about 1100, after discussing the forecast with the ship’s master during the master-pilot information exchange (MPX), the pilot made VHF radio contact with VTS. Concerned that a late release of the tugs could leave the ship in the narrow channel without assistance, the pilot requested separate tugs for the ship’s arrival at berth 1.
The duty VTSO acknowledged the request, and their colleague contacted the port’s towage provider to check for tug availability. The planner at the towage company informed VTS that only 2 tugs were available for the afternoon, as the crew for the stand‑by tug was on their break and would be available from 1730.
At 1124, the VTSO informed the pilot that no extra tugs were available for the scheduled arrival time. Instead, they requested the that the pilot postpone Viking Passama’s arrival until after Cielo di Cagliari had berthed. In response, the pilot slowed the ship to about 7 knots, adjusting the arrival time to 1500.
At 1243, the first of a series of severe thunderstorm warnings was issued by the BoM. The first warning detailed the development of severe thunderstorms in northern New South Wales, tracking towards the southern part of the Gold Coast in a north-easterly direction.
At 1244, the pilot on board Cielo di Cagliari reported to VTS that the ship was passing the entrance beacons and enquired about the BoM warning they had received on their phone. The duty VTSO replied that the BoM was reporting severe thunderstorms over the New South Wales border ranges, possibly impacting Brisbane later that afternoon.
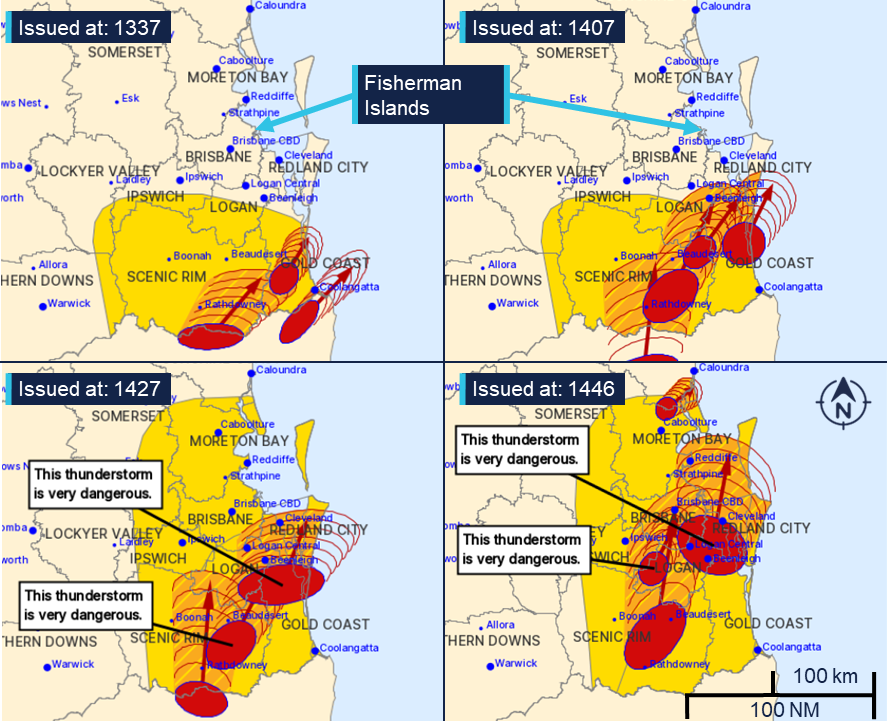
Updated warnings were issued by the BoM at 1310 and 1337, with observations and short-term forecasts nowshowing storms in the Gold Coast area tracking north-east (Figure 3). At 1407, an updated warning predictedstorms tracking further north, potentially passing close toBrisbane port.
Figure 3: Storm warnings 1337 to 1446
Source: Bureau of Meteorology, annotated by the ATSB
At 1410, Cielo di Cagliari’s pilot contacted the pilot on Viking Passama directly on VHF, reporting that the ship had nearly completed berthing and that the tugs would be released in 5 to 10 minutes. Viking Passama’s pilot confirmed the message. Following this Viking Passama increased speed to 11 knots and at 1412, it passed between the entrance beacons, committing to its approach.
At 1419, the pilot on board the Gaschem Iliad called VTS andreported heaving anchor at the STS anchorage. The pilot also gave 30 minutes’ notice of the ship’s arrival at the entrance beacons in anticipation of its inbound transit, following Viking Passama.
At 1427, a severe thunderstorm warning classified 2 storms as ‘very dangerous’, with the northernmost storm tracking towards Moreton Bay and expected to impact Cleveland (about 20 km to the south-east of the port) at 1520. An updated warning, issued at 1446, showed a large thunderstorm tracking towards the Port of Brisbane, noting (in part):
The Bureau of Meteorology warns that, at 2:40 pm, VERY DANGEROUS THUNDERSTORMS likely to produce large, possibly giant hailstones, damaging, locally destructive winds and heavy rainfall that may lead to flash flooding were detected near Beenleigh, Logan Central, Cleveland and Greenbank. These thunderstorms are moving towards the north to northeast. They are forecast to affect Redbank Plains, Wacol and Archerfield by 3:10 pm and Brisbane CBD, Redcliffe and Point Lookout by 3:40 pm.
The warning was relayed by the duty VTSO via an all-ships safety broadcast,1 on the port VHF working channel at 1448.
In reply, the pilot on board Gaschem Iliad requested a second tug for its berthing manoeuvre. However, at 1451, the pilot informed VTS that they would instead delay the ship’s entry into the port as wind speeds were exceeding 30 knots.
At about the same time, cargo operations on board Wide India, MSC Barbara and Volans were stopped by the respective terminal operators and stevedores disembarked the ships.
Storm arrival
The master of Wide India later reported that they did not receive the 1448 VTS warning broadcast on the port VHF working channel. Instead, the chief officer was warned by the departing stevedores. The master and chief officer reported that at this time, the storm was visibly approaching from the south (Figure 4). The master urgently requested the duty engineer to make the ship’s main engine and bow thruster ready for manoeuvring.2
Figure 4: View of approaching storm from Wide India at 1503
Source: Chief mate of Wide India, modified and annotated by the ATSB
The crew of MSC Barbara could also see the approaching storm and its master reported that they requested the engineers to bring the ship’s bow thruster online to assist in keeping the ship alongside its berth.
At 1500, the assistant regional harbour master, who was the designated duty harbour master for the day, was called to the VTS control centre to support the VTSOs in dealing with the emerging situation.
At the same time, Volans’ master ordered the ship’s engine and bow thruster to be made ready for manoeuvring and the gangway to be lifted to deck level.
Viking Passama
At 1503, the storm was approaching the port while Viking Passama was in the process of being moored at Fisherman Islands berth 1, assisted by the tugs Bullara and Svitzer Newstead. The pilot instructed both tugs to ‘lift’ (pull back on their towlines) slowing the ship’s movement towards the berth caused by the strong northerly wind (Figure 4, inset).
At 1505, wind speeds briefly subsided to calm conditions for about 2 minutes before increasing and abruptly changing direction to the south-east. In response, Viking Passama’s pilot ordered the tugs to push the ship alongside (Figure 5) and at 1510, it came to rest on the shore fenders. The crew passed mooring lines ashore while the rapidly increasing wind was pushing the ship off the berth. The chief mate reported wind speeds of over 60 knots on the bridge anemometer, and the master and pilot had to take shelter against the accompanying rain and large hail stones.
Meanwhile, on the aft mooring station, the second mate reported to the bridge that the ship was moving away from the berth but was advised by the master that the tugs were already pushing at full power. The mooring party noticed the extreme tension on the spring lines and moved to a safe position. At about 1515, both aft spring lines parted, snapping back across the deck. The lines impacted the protective cage around the winch controls and severed the aft winch hydraulic control pipes, disabling the aft mooring winches. At the same time, the pilot called VTS to request an additional (third) tug, as an emergency measure.
At 1516, the pilot again called VTS informing the VTSO that the ship was now being held in a stable position, just off the berth, by the 2 tugs. The VTSO replied that they had requested additional tug assistance and that a windspeed of 60 knots was being recorded at the entrance beacons.
The ship was slowly blown further off from the berth, despite both tugs pushing at full power and, at 1517, the remaining lines parted.
At 1519, the VTSO called the Viking Passama and informed the pilotthat the tugs were needed to assist other ships. The pilot replied that they had parted all lines and that the ship would be grounded in minutes if they released the tugs. Eventually, Viking Passama was blown approximately 120 m off its berth before the wind abated sufficiently to enable the tugs to push it back.
Figure 5: View from Wide India at 1510
Source: Chief mate Wide India, modified and annotated by the ATSB.
Volans
At about 1515, the rapidly increasing wind on Volans’ stern caused its aft mooring lines to part due to the increased strain. The ship’s unsecured stern was pushed off the berth.3 (Figure 6)
Volans’ master subsequently requested tug and pilot assistance from VTS at 1517 and was informed that tugs would be underway to them as soon as possible.
The ship then continued to swing around its bow which was still connected to the berth by 2 headlines and held by its port anchor. Eventually rotating about 135°, with its bow now facing into the wind and its stern impinging into the adjacent channel. The crew lowered the starboard anchor to assist in holding the ship in position but were unsuccessful at deploying additional mooring lines.
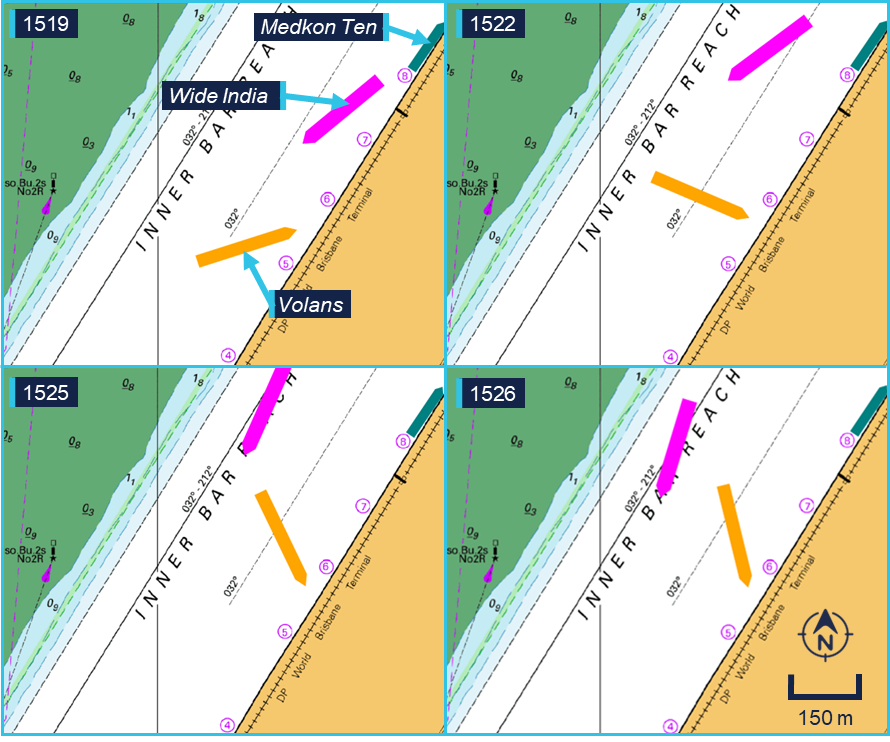
Figure 6: Volans’ and Wide India’s movements
Source: Australian Hydrographic Office, annotated by the ATSB
Wide India
As the storm hit, Wide India’s mooring lines came under increased strain. Its crew attempted tightening the winch brakes to prevent them slipping, before seeking shelter away from the mooring lines, which were parting or paying out violently. By 1519, the ship had broken free of its berth and was drifting across the channel.
The master started the main engine, to prevent the ship from drifting astern into Medkon Ten. The duty VTSO radioed the ship and gave the master permission to use the ship’s engine to manoeuvre. The masterreplied that they were already underway as all lines had parted, after which the VTSO informed them that tugs were some time away and requested them to ‘manoeuvre and handle your situation the best you see fit’. Wide India moved slowly upriver, maintaining steerageway4 as the master dredged5 the ship’s starboard anchor and used the bow thruster to maintain heading control. At 1526, Wide India passed closely around the stern of Volans (Figure 7).
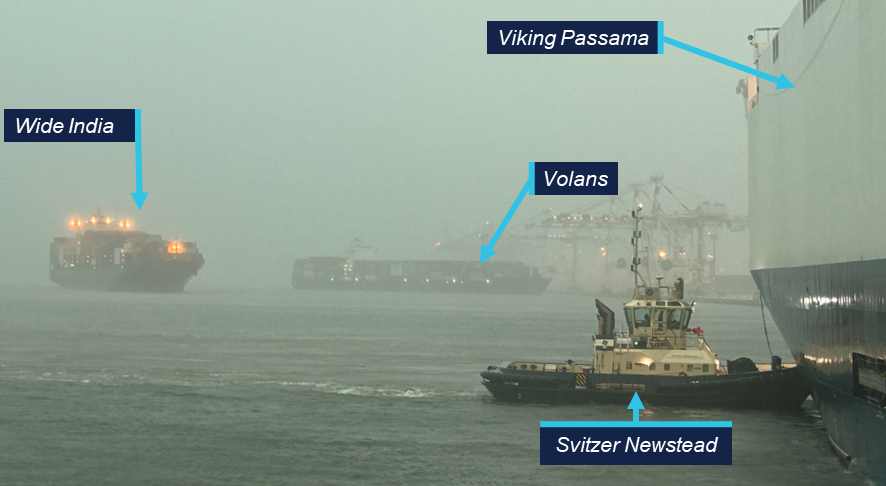
Figure 7: 1532 view from Bullara
Source: Master Bullara, annotated by the ATSB
MSC Barbara
At about 1520 the wind force on MSC Barbara moorings caused its winch brakes to render. As the wind pushed the ship further off the berth, its mooring lines eventually ran off the winch drums. The lines were still connected to the shore mooring bollards and streamed across the channel. At 1523, its master requested tug assistance on the port VHF working channel. The VTSO then informed the master that tugs were ‘a short time away’ and that the RHM had given permission to manoeuvre.
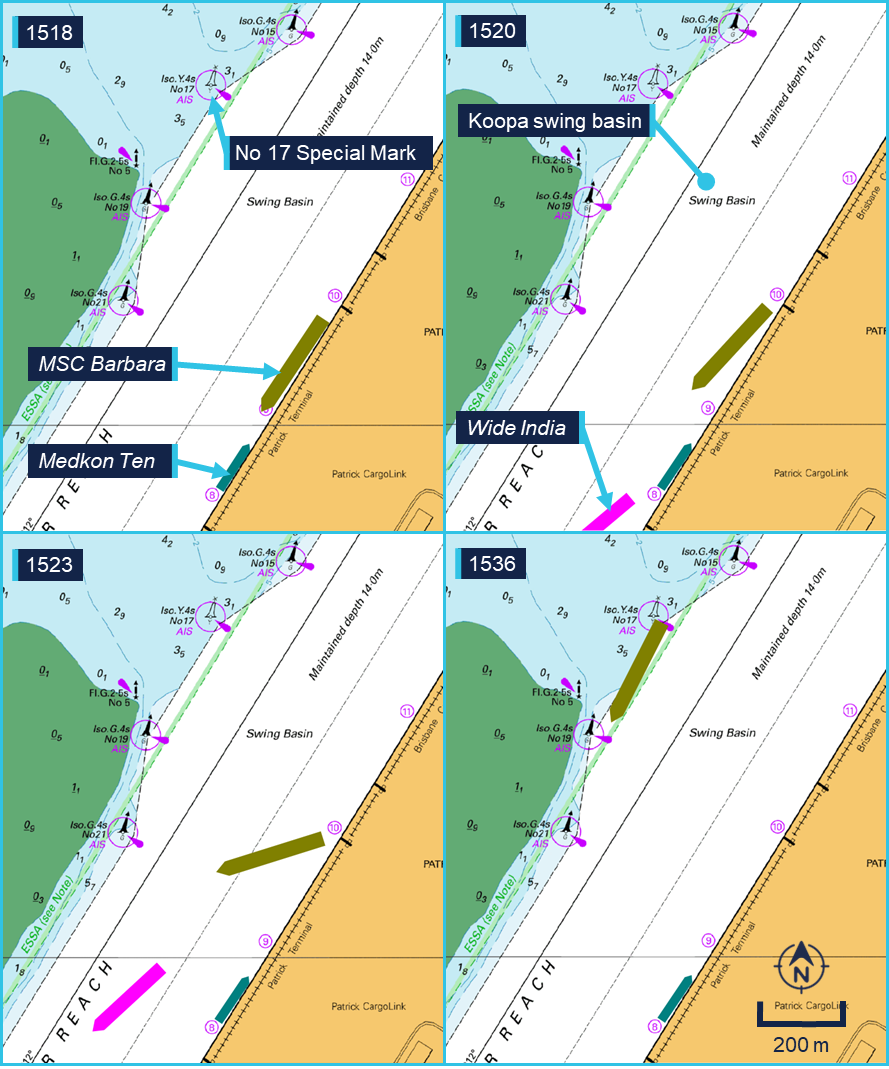
However, the ship’s main engine was not ready to manoeuvre, leaving the ship without propulsion. The master utilised the ship’s bow thruster to provide limited heading control, attempting to maintain its heading into the wind. The strong winds pushed the ship in a northerly direction and it ran aground on the opposite side of the channel, on the side batter of the Koopa swing basin (Figure 8).
Six of the ship’s hatch cover pontoons, which had been offloaded ashore as a routine part of cargo operations were left behind on the berth.
Figure 8: MSC Barbara’s movement across the channel
Source: Australian Hydrographic Office, annotated by the ATSB
Other ships
At 1528, Crystal, moored at the grain and woodchip wharf just south of Viking Passama, reported to VTS that it was coming off the berth and requested tug assistance. The VTSO replied that no tugs were available and that the crew could use their engine and thrusters if needed. Though affected by the storm, its moorings held and the crew successfully returned the ship alongside using its winches.
The 148 m container feeder Medcon Ten was moored at Fisherman Island berth 8, between Wide India and MSC Barbara, its crew did not report any damage and the ship stayed alongside during the storm.
Recovery
As the impact of the storm became clear, VTS personnel started activating emergency response procedures. This included contacting the RHM and communicating with the pilotage provider, harbour tug operators, terminal operators, ship’s agents and internally within Maritime Safety Queensland to coordinate a response.
Several pilots, along with launch and towage crew, made their way to the port to assist – either after being called out, or after reporting in while off-duty. Their response was initially hampered by the weather conditions, as road traffic en route to Brisbane port was severely affected by falling debris, poor visibility and large hail.
At 1512 and 1514, a VTSO phoned both towage operators in the port, requesting they start mobilising crews to provide emergency assistance. Additional tugs became available between 1640 and 1752, as crewmembers made their way to the tug bases.
At 1604, the first pilot arrived near Fisherman Islands on board a police boat. They had requested assistance at the Lytton water police station, after being unable to cross the river to reach the pilot base at Pinkenba. This pilot boarded Wide India, which was assessed as the highest priority by the RHM.
At about 1600, a pilot launch departed from its Pinkenba berth with 3 pilots on board. One pilot boarded Volans at about 1620, while the other 2 made their way to the grounded MSC Barbara and boarded at about 1625.
The port launch Moggill was mobilised to assist in recovering ropes from the water and relocating a buoy away from MSC Barbara’s rudder.
Viking Passama
As the storm cleared the area and wind speeds subsided, Viking Passama was pushed back by its assisting tugs and, at 1543, was again alongside. Once the forward lines had been secured, the forward tug (Svitzer Newstead) was released at 1559.
However, the aft lines could not immediately be deployed due to the damage to the winch controls. This meant the aft tug (Bullara) had to be kept pushing up on the stern, while the ship’s engineering crew made emergency repairs to the aft winches (Figure 9). On completing the repairs, Bullara was released at 1644 for tasking to another ship.
Figure 9: Viking Passama winch control emergency repair
Source: ATSB
Wide India
Meanwhile, Wide India had slowly made its way upriver to the end of the Fisherman Islands berths, approaching Viking Passama (Figure 10) before coming to a stop and backing away. As Wide India could not turn unassisted in the narrow channel its master kept it underway at slow speed, against the south-easterly wind and ebb current, to maintain steerage until a tug was available.
Figure 10: 1554 Wide India approaching Viking Passama
Source: Master Viking Passama, annotated by the ATSB
At 1600, the tug Svitzer Newstead approached and its master formally offered assistance, informing Wide India’s master that the tug’s ‘owner reserved the right to negotiate the terms of engagement’. Wide India’s master did not directly answer the request, and VTS then informed the tug’s master to standby, awaiting the pilot, who was en route on a police boat.
The pilot boarded Wide India, arriving on the bridge at 1614. The pilot then coordinated with Svitzer Newstead to secure a tow line and assisted the ship turning in the channel (Figure 11).
Figure 11: 1614 WideIndia and Volans
Source: Pilot MSC Barbara
At about 1635, the ship had swung around to starboard and was heading down river (Figure 12). At 1703, the pilot reported passing the entrance beacons outbound, heading for the STS anchorage where it anchored at 1757. After inspection of the ship’s mooring equipment and respooling its mooring lines at the anchorage, Wide India returned to its berth on 25 November to complete cargo operations and recover its hatch covers.
Figure 12: 1628 WideIndia swinging in fairway
Source: Port of Brisbane CCTV, annotated by the ATSB.
Volans
Once the storm cleared, Volans was secured to the berth with its 2 remaining headlines, with additional support from both its anchors. Its exact position was determined by the wind and current, with its stern protruding into the channel. Lines from both Volans and Wide India were in the water around the ship, causing a possible navigational hazard to assisting tugs (Figure 13).
Figure 13: 1618 Volans secured with 2 headlines
Source: Pilot MSC Barbara, insert Australian Hydrographic Office, insert crew Volans, annotated by the ATSB
At 1620, a pilot boarded from the pilot launch, followed at 1645 by the arrival of the tug Svitzer Olivia. Though the ship had originally been moored on its starboard side, the pilot and master decided to use the tug to push the ship alongside on the port side first – clearing the channel for other traffic until a second tug was available to swing the ship. Meanwhile, the port tender Moggill assisted with recovery of the mooring lines from the water.
At 1720, with the additional assistance of SL Fitzroy, Volans was swung in the channel and returned to its original berth, where it was alongside by about 1755. However, mooring operations were slow, as the recovered lines had to be passed from the quayside and resecured onto the ship’s winches. Volans was finally safely moored at 1854.
MSC Barbara
After embarking the pilot on Volans, the launchproceeded to MSC Barbara, which was grounded on the bank of the Koopa swing basin (Figure 14).
Figure 14: MSC Barbara aground
Source: Master Svitzer Newstead, modified by the ATSB
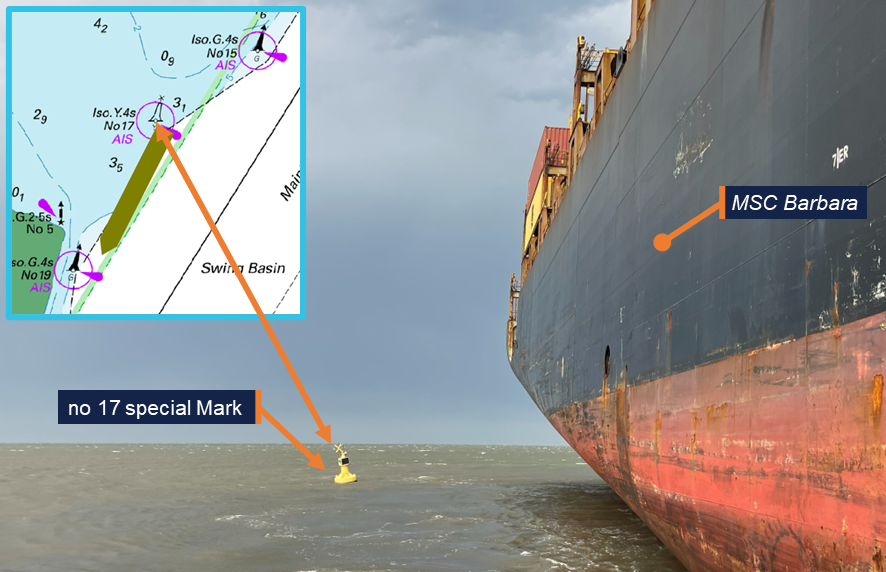
The 2 assigned pilots first assessed the situation before boarding. They observed MSC Barbara heeled over slightly to port on the falling tide and at close distance from the no 17 special mark buoy (Figure 15). The ship’s starboard anchor was run out to port, with the chain leading over the bulbous bow. The pilots agreed on the division of their roles, with one pilot conning the ship and controlling the tugs and the other handling communication, both on board and with parties ashore.
Figure 15: MSC Barabara’s stern and no 17 special mark
Source: Pilot MSC Barbara
The pilots boarded MSC Barbara at 1624 and conducted the MPX with the master, which was also attended by an on-board company superintendent. The MPX was interrupted several times by calls from the ship’s manager, MSC, but the pilots and master agreed on a strategy to refloat the ship using the tugs assisted by heaving of the anchor. At 1645, the tug Svitzer Newstead arrived, followed at 1654, by Bullara and SL Murrimbidgee. Additionally, port tender Moggill moved the no 17 buoy away to avoid it fouling the ship’s hull or propeller. Under the direction of the conning pilot, the tugs then proceeded to refloat the ship. The main engine was not used due to concerns about possible damage to the propeller.
At 1713, the pilot reported to VTS that they were starting to move and, at 1716, the ship was afloat. It was then moved into the channel by the 3 tugs where its engine was tested and the anchor cable heaved in. It was found that the anchor had fouled the bulbous bow, which took some time to clear.
MSC Barbara’s master, on request of the ship’s manager, insisted on bringing the ship back alongside the berth. Several phone calls between the master, the managers, the ship’s agent and the RHM were made to discuss the situation.
Eventually, the RHM issued a formal direction to the ship to depart, first at 1750 and then again at 1810. At 1815, the ship started its transit to the STS anchorage to assess damage to the hull and mooring systems. It was safely anchored in the STS-1 anchorage at 2024. After assessment of the damage and respooling of the mooring lines at the anchorage, MSC Barbara returned to the terminal on 28 November, where it completed its scheduled cargo operations and recovered its hatch covers.
Context
Port of Brisbane
The Port of Brisbane is located at the mouth of the Brisbane River and is Queensland's largest general cargo port with 30 berths. Port throughput in 2024–25 exceeded 34 million tonnes. The Brisbane port limits encompass a significant area of Moreton Bay and extend to the northern end of the bay, with about 45 miles from the pilot boarding ground to the river entrance beacons.
The port was privatised in 2010 and was managed and developed by the Port of Brisbane Pty Ltd (PBPL) under a 99-year lease with the Queensland Government. Maritime Safety Queensland retained responsibility for certain aspects of port management.
Maritime Safety Queensland
Queensland’s maritime legislation was administered by Maritime Safety Queensland (MSQ), a state government agency within the Department of Transport and Main Roads. As such, MSQ was responsible for safety oversight of pilotage, pollution protection services, vessel traffic services (VTS) and the administration of all aspects of ship registration and marine safety in the state of Queensland.
The day-to-day management of shipping activities and port safety were subject to the directions of a regional harbour master (RHM). The Brisbane RHM’s area of responsibility extended beyond the port limits to include areas of other commercial and recreational activities, including Moreton Bay, the Brisbane River upstream of the port and the coastal sea area to about 45 miles further north of the port limits.
As part of its role in maritime safety MSQ was also responsible for the management of maritime emergencies, including those caused by extreme weather events. MSQ procedures stated that in the event of an emergency the duty harbour master would take the role of incident controller (IC), with VTS noted as one of the main triggers for identifying emergencies and activating the response. On 24 November the assigned duty harbour master was the assistant RHM (ARHM) – who arrived at the VTS control centre at 1500, within a minute of being called by the duty VTSO.
For larger emergencies the IC was supported by the maritime emergency management team (MEM), consisting of senior MSQ managers. On this occasion, the MEM was activated at 1530, and its members arrived at the VTS control centre at 1645.
Under section 86 of the Queensland Transport Operations (Marine Safety) Act 1994, the RHM or the duty harbour master as their delegate, could issue ‘general’ directions applicable to all ships, or ‘particular’ to an individual ship. For example, a general direction closing and reopening the port or a direction for a ship to proceed to anchorage.
Vessel traffic service
A vessel traffic service (VTS) was provided by MSQ for the Port of Brisbane and the waters of Moreton Bay in accordance with the Australian Maritime Safety Authority’s Marine Order 64.6 The VTS monitored and communicated with ships in its area of responsibility to improve navigational safety. It also coordinated the allocation of tugs and pilots.
A vessel traffic management system (VTMS) was used by the vessel traffic service officers (VTSO) to maintain a traffic image of vessels moving through the area. This data was then used by the VTSOs to provide traffic information, maritime safety information and navigational support to individual vessels.
The location, heading and speed of ships displayed on the VTMS could be derived from radar and automatic identification system (AIS) information. Radar data was not dependent on ships’ equipment or transmissions but was subject to coverage limitations. During the storm the radar was unreliable due to rain clutter caused by the strong precipitation. While AIS data was available throughout the storm, position update frequency was limited by the transmission interval. The ships that had broken away from their moorings at the container berths had their AIS status set to ‘moored’. This meant that as long as their speed was below 3 knots, positions were only updated every 3 minutes.
Under normal circumstances, the VTS was crewed by 3 VTSOs working 12-hour shifts. Two VTSOs managed traffic and operated the radio, while the third VTSO handled scheduling of pilots, tugs and coordination with the terminals.
The VTS control centre was located on the ground floor of MSQ’s Pinkenba building, which did not provide the VTSOs with an outside view over the river. Instead, they had access to several CCTV cameras around the port to improve their situational awareness.
Pilotage
For the Port of Brisbane pilotage was compulsory for ships with an overall length of more than 50 metres. The pilotage area covered most of Moreton Bay, with pilots boarding inbound ships by launch, at the pilot boarding ground, 2.5 miles south-east of Point Cartwright, Mooloolaba.
Ships with an overall length of more than 300 metres were considered ‘oversize’ and procedures required them to be piloted by 2 pilots, which in this incident applied to MSC Barbara.
Pilotage was provided on behalf of MSQ by Poseidon Sea Pilots (PSP) which operated a base and several launches both in Pinkenba, on the Brisbane River, and in Mooloolaba at the northern end of Moreton Bay.
Fisherman Islands terminals
Several terminals operated on Fisherman Islands transhipping various commodities, including containers and vehicles as well as liquid and dry bulk goods. The terminal operators leased their terminals from PBPL, that in turn managed maintenance of both quayside infrastructure and waterways. Both PBPL and the individual terminals operated CCTV cameras around the port. Video recordings from these cameras were provided to the ATSB for analysis.
The Fisherman Islands berths consisted of a concrete deck supported by pillars bordering a rock wall abutment. Vertical rubber fenders were fitted at regular intervals to the wharf face and crane tracks ran on either side of the deck supporting several gantry cranes.
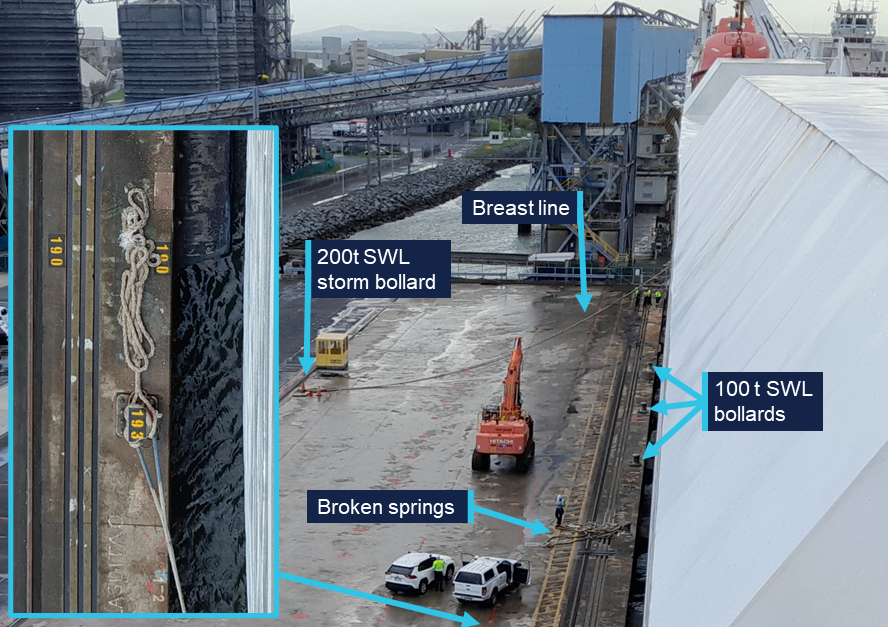
Vehicle berth 1, used by Viking Passama, was operated by Australian Amalgamated Terminal (AAT). Its mooring arrangements comprised 100 t safe working load (SWL) mooring bollards at intervals of 16 metres along the edge of the quay. Additionally, a limited number of 200 t SWL recessed storm bollards were located about 29 metres from the wharf face (Figure 16).
Figure 16: Berth 1 mooring arrangements
Source: Master of Viking Passama, annotated by the ATSB
The container berths 4 to 7, used by Volans and Wide India, were operated by DP World Brisbane. MSC Barbara was moored at berths 9 and 10, operated by Patrick Terminals. These berths were fitted with upgraded 150 t bollards, 18 metres apart (Figure 17). Although 200 t SWL storm bollards on the far side of the quay deck were included in the original design of the berth, these were either not installed or not accessible.
Figure 17: Mooring arrangements at Fisherman Islands berths 4 to 11
Source: ATSB
Harbour towage
Two companies provided harbour towage services in the Port of Brisbane. The largest operator was Svitzer towage, which operated 5 tugs. Of these tugs, 2 were crewed by alternating 12‑hour day and night shifts and available for use at any time. An additional secondary crew was kept on stand-by at 90 minutes’ notice and was available subject to work and rest hour restrictions.
At the time of the occurrence, Svitzer Newstead and Bullara were crewed by the day shift, with the secondary shift crewing SL Murrumbidgee. The secondary crew had reached their work hour limit earlier in the day and was not available for routine operations. However, they were mobilised on an emergency basis after a request for emergency assistance by VTS at 1514 and departed the tug base at 1650.
Two crews, who were scheduled as primary crew for the night shift, were called out to start their shift early. They departed, at 1732 and 1752, on board the tugs Beltana and Svitzer Colmslie. They took over the duties from the day shift crews on Bullara and Svitzer Newstead, who had reached the end of their shifts.
Additionally, Boluda towage, formerly Smit Lamnalco, also operated 2 harbour tugs in the port: SL Fitzroy and Svitzer Olivia. These tugs were operated on a single shift of 12 hours per day and were not crewed during the incident. They were mobilised on an emergency basis after a phone call by VTS at 1512, with Svitzer Olivia departing at 1622, followed by SL Fitzroy at 1648.
Ships
Viking Passama
Viking Passama was a Marshall Islands registered car carrier, built in 2012 at Yangfan Shipyard, Zhoushan, China, and classed with Det Norske Veritas (DNV).
The 47,053 gross ton ship had a capacity of 5000 RT,7an overall length of 183 metres and a summer draught of 9.1 metres. It was propelled by a single MAN 9S50MC-C7 2‑stroke main engine, producing 14,220 kW and driving a fixed pitch propeller. To assist manoeuvring, it was equipped with a 1,100 kW bow thruster.
The shipwas equipped with an Intershalt G4e voyage data recorder (VDR). The VDR recorded bridge audio, ECDIS and radar display information as well as navigation and engineering parameters. The VDR data relevant to the investigation was downloaded on board the ship by the ATSB.
At the time of the incident, Viking Passama was owned by Gram Car Carriers and managed by Reederei F.Laeiz of Hamburg, Germany. It had a crew of 22 Russian, Estonian and Filipino nationals.
The ship was equipped with 2 loading ramps for the loading and discharging of its vehicle cargo. One ramp was mounted on the starboard quarter and the other in the starboard side shell. In line with these asymmetric cargo arrangements, its mooring arrangements were primarily designed to moor the ship starboard side alongside.
Its forward mooring arrangements consisted of 2 windlasses, each driving 2 mooring drums and a warping drum. A single drum winch was fitted between the windlasses in the central position. Additionally, several mooring bitts with an SWL of 335 kN (34 t) were fitted.
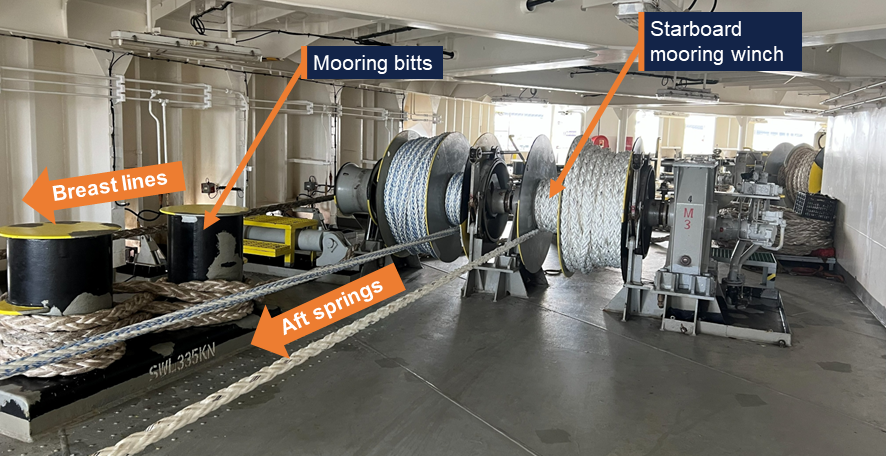
The aft mooring station was equipped with one double drum mooring winch on its port side and a single drum centre winch, that were normally used to deploy stern lines. A double drum winch fitted on its starboard side, forward of the stern-ramp recess, was normally used to deploy the aft springs (Figure 18). Additional 335 kN (34 t) mooring bitts were also fitted and typically used to set breast lines on storm bollards.
During the incident, 2 aft- and one fore-spring had been secured ashore, while the aft mooring crew were in the process of running the stern lines. The mooring plan also included 2 breast lines to be secured to the storm bollard on the quay, that were to be run from the fixed bitts on the aft mooring station.
Figure 18: Starboard-aft mooring station on board Viking Passama
Viking Passama’s aft mooring station seen from the location of the starboard winch control (Figure 9). Source: ATSB
MSC Barbara
MSC Barbara was a Panamanian registered cellular container ship, built in 2002 at Ulsan, Korea, and classed with DNV.
The 73,819 GT ship had a capacity of 6,720 TEU8 and an overall length of 304 metres. It was propelled by a single MAN-B&W Hyundai 10K98MC‑C 2‑stroke engine producing 57,700 kW and driving a fixed pitch propellor at maximum 80 RPM. To assist with manoeuvring, it was equipped with a 2,500 kW bow thruster.
The ship was equipped with a Danelec DM200 simplified voyage data recorder9 (S‑VDR). The S-VDR recorded bridge audio, radar display information and limited navigation parameters. S-VDR data relevant to the investigation was downloaded on board the ship by the ATSB.
At the time of the incident, MSC Barabara was owned by Compania Naviera Dunrobin and managed by MSC Shipmanagement in Cyprus. It operated on a fixed route between Australian and Asian ports for the Mediterranean Shipping Company and had a crew of 25 Ukrainian, Romanian, Filipino, Moldovan and Indian nationals. During the incident the ship also carried a company superintendent, who was not signed on as crew.
The ship’s forward mooring station was equipped with 2 windlasses, used for anchoring and each driving a single mooring drum and warping drum. Four additional single drum winches and 4 sets of 100 t SWL mooring bitts were also installed. The ship’s aft mooring station was equipped with 6 winches, each equipped with a single mooring drum and a warping drum (Figure 19) and 4 sets of 100 tonne SWL mooring bitts.
Figure 19: MSC Barbara aft mooring station, looking to starboard
Source: ATSB
On arrival, the ship was initially moored using 4 headlines, 4 stern lines and 2 forward and 2 aft springs, all on the winch drums. After receiving the weather warning from VTS via the terminal safety officer, the crew rigged an extra fore spring and headline as well as an aft spring and stern line, secured on the bitts.
Volans
Volans was a Liberian registered cellular container ship, built in 2010 at the Zhejiang Shipbuilding yard in Ningbo, China, and classed with DNV.
The 41,225 GT ship had a capacity of 4,254 TEU and an overall length of 265 metres. It was propelled by a single MAN 8K90MC-C 2-stroke main engine producing 36,560 kW and driving a fixed pitch propeller. It was additionally equipped with a 1,600 kW bow thruster for manoeuvring.
The ship was equipped with a Furuno VDR. The VDR recorded bridge audio, ECDIS and radar display information as well as navigation and engineering parameters. VDR data relevant to the investigation was downloaded by the crew and was obtained by the ATSB.
At the time of the incident, Volans was managed by Oltmann Schiffarhtgesellschaft, Germany. It operated on a fixed route between Asian, Australian and New Zealand ports.
The ship’s forward mooring arrangements consisted of 2 windlasses and one centre mooring winch, fitted with 2 mooring drums each. Its aft mooring station was equipped with 3 double drum mooring winches. Both mooring stations were further equipped with several mooring bitts with an SWL of 60 t that could be used to secure additional lines.
On arrival at Brisbane, the ship was moored using 4 headlines and 2 springs forward and 4 stern lines and 2 springs aft. After receiving the warning in the morning, the crew lowered the starboard anchor and secured an additional stern line aft and an additional headline and spring forward. After the storm passed the ship remained secured to the berth by 2 headlines from the port windlass mooring drums. (Figure 20)
Figure 20: 1640 Volans forecastle looking aft
Source: Crew Volans
Wide India
Wide India was a Marshall Islands registered cellular container ship built in 2015 at Hanjin Heavy Industries in Subic Bay, Philippines, and classed with DNV.
The ship measured 51,872 GT, had a capacity of 5,466 TEU and an overall length of 255 metres. It was propelled by a single MAN-B&W 6G80ME-C producing 24,680 kW and driving a fixed pitch propellor. It was additionally equipped with an 1,800 kW bow thruster to assist in manoeuvring.
The ship was equipped with a Furuno VDR which recorded 12 hours of bridge audio, ECDIS and radar display information as well as navigation and engineering parameters. The data on the VDR was not secured and subsequently overwritten before the ATSB could attend.
At the time of the incident, Wide India was managed by Danaos Shipping, Greece. It operated on a route between Tanjung Pelepas, Singapore, Brisbane and Sydney for Hapag Lloyd. The ship had a crew of 21 Ukrainian, Russian, Ghanese and Tanzanian nationals, as well as 3 Korean supernumerary service engineers. During the incident the ship also carried a company superintendent, who was not signed on as part of the crew.
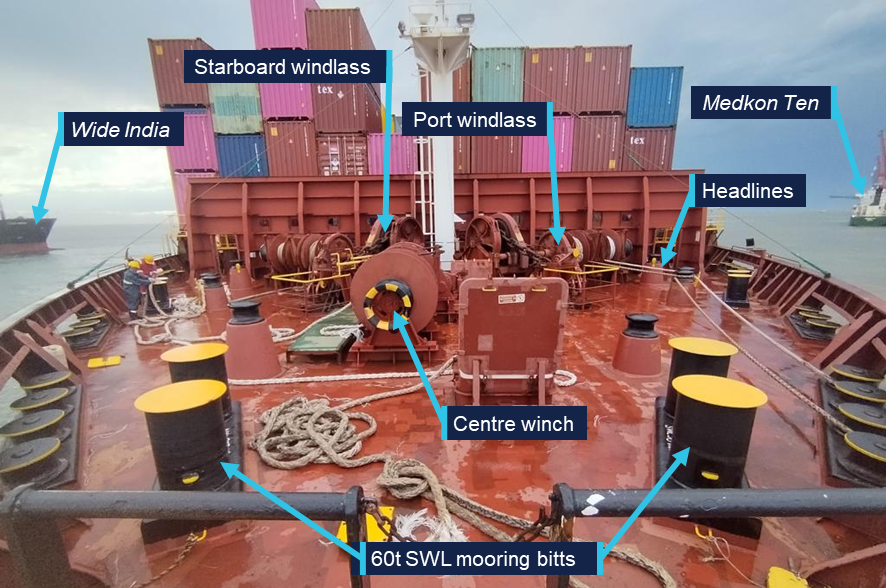
The ship’s forward mooring arrangements consisted of 2 windlasses and one centre mooring winch, fitted with 2 mooring drums each. Its aft mooring station was equipped with 3 double drum mooring winches. Both forward and aft stations were equipped with 6 sets of mooring bitts with an SWL of 100 t (Figure 21). On arrival at Brisbane, it was moored using 4 headlines and 2 springs forward and 4 stern lines and 2 springs aft. After receiving the warning from the terminal, the crew lowered the starboard anchor but did not deploy extra lines.
Figure 21: Wide India forecastle looking aft
Source: ATSB
Meteorology
South East Queensland is particularly susceptible to severe thunderstorms, especially during the summer months. Such storms have a much smaller footprint than tropical storms and are generally short-lived. However, they move fast and may contain severe gusts as well as large, damaging hail. Accurate predictions in the hours preceding impact are often limited by the complex and chaotic atmospheric environment.
In the past 4 decades, multiple high-impact storms have affected the greater Brisbane area, with major damage occurring in 1985, 2008 and 2014. The highest recorded wind gust, of 184 km/h, was recorded at Brisbane Airport during the 1985 event.10
November 2025 had been warmer and wetter than usual in South East Queensland, with multiple severe thunderstorm events. The marine weather forecasts for the 3 days leading up to 24 November indicated a chance of thunderstorm development on each day.
The 24 November storm caused widespread damage to buildings and infrastructure, including widespread electrical power outages. The maximum windspeed observed at Brisbane airport during the storm was 96 km/h. At the Port of Brisbane entrance beacons, a maximum gust strength of 132 km/h was recorded.11
Bureau of Meteorology
The Bureau of Meteorology (BoM) provides several relevant products to assist seafarers, government organisations and the public to assess and prepare for thunderstorms and general weather hazards. These included:
meteorological warnings and forecasts through METAREA X, as part of the Global Maritime Distress and Safety System (GMDSS)
coastal waters forecast for Moreton Bay
severe weather briefing for Queensland
general area forecasts available through the BoM website and app
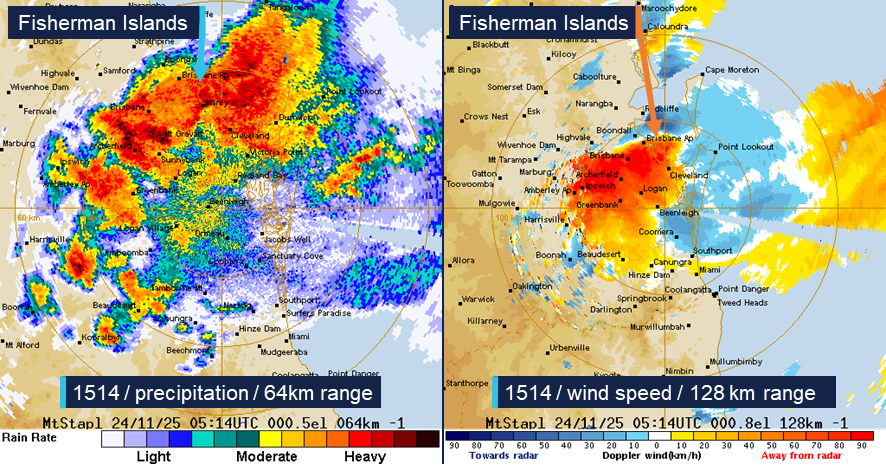
weather radar information including precipitation density and doppler windspeed to and from the radar (Figure 22).
Figure 22: Mount Stapleton weather radar at 1514 on 24 November
Source: Bureau of Meteorology, annotated by the ATSB
Proprietary weather information
A version of the Nonlinear Channel Optimisation Simulator (NCOS) was operated by PBPL. This software provided a near real-time, 7-day forecast of environmental conditions and a ship’s under keel clearance (UKC) through a web interface, accessible to the port’s stakeholders to aid ship scheduling. Though it was primarily designed as a tool for managing UKC, it also included weather prediction data, which was available to the pilots.
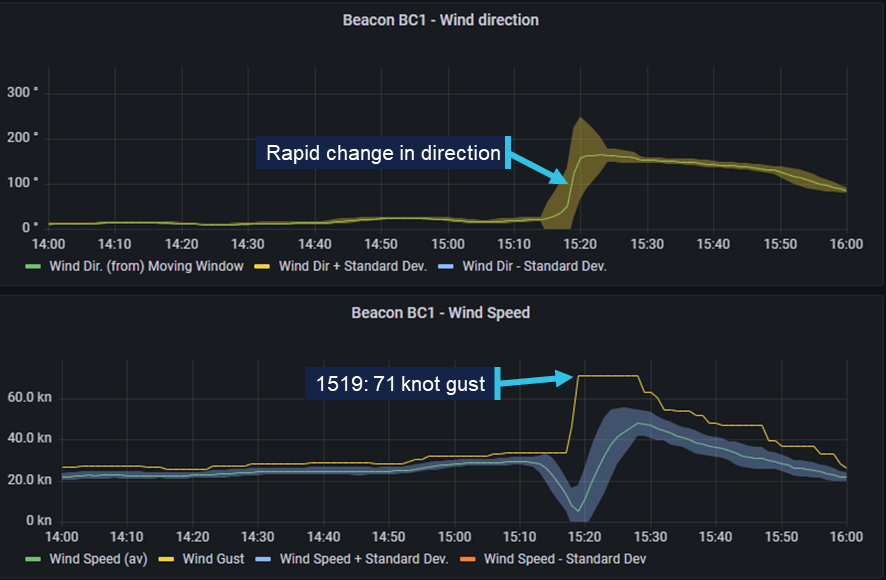
Maritime Safety Queensland also operated an online weather dashboard, called ‘PortWeather’. This provided live weather, tidal and current observations for ports around Queensland. It was available to VTS, pilots and other local stakeholders for different locations in the port and its approaches. The system’s meteorological instrumentation located on the port channel entrance beacon (BC1) recorded a maximum gust speed of 71 knots during the incident (Figure 23).
Figure 23: MSQ port weather dashboard data from beacon BC1 (1400 to 1600)
Source: MSQ, modified and annotated by the ATSB
Further investigation
The ATSB attended Wide India and MSC Barbara in Brisbane, and Viking Passama in Melbourne, to collect relevant evidence and interview the masters and relevant crew.
VDR data was received from Volans and recovered by the ATSB from Viking Passama and MSC Barbara.
The ATSB attended the Port of Brisbane to collect relevant evidence and interview directly involved individuals. Additionally, meteorological information was provided by the Bureau of Meteorology.
The investigation is continuing and will include analysis of:
meteorological and climatological data
shipboard and shore-side mooring arrangements
harbour towage
emergency arrangements on board and ashore
effectiveness of the port procedures and operational guidance.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^The prefix ‘securite’ is used for navigation or meteorological safety broadcasts.
^Wide India, Volans, MSC Barbara and Viking Passama were each fitted with reversible two-stroke engines. As these engines are directly connected to a fixed pitch propellor, they cannot run idle and are only started when thrust is needed. However, several auxiliary systems, e.g. auxiliary blowers, cooling, lubrication oil and fuel oil systems had to be brought online for the engine to be ready (or ‘stand-by’) for immediate use.
^Movement and location information has been obtained from voyage data recorder for Volans, and from Automatic Identification System (AIS) data for Wide India. The AIS transceiver on board Wide India was set to ‘moored’ which meant their position was only transmitted every 3 minutes as long as its ground speed was below 3 knots.
^Steerageway: the minimum required speed through water to permit a ship to be manoeuvred.
^Dredging anchor: the towing of an anchor at a short stay to assist in heading and speed control during a manoeuvre.
^Australian Maritime Safety Agency, 2022, Marine Order 64 (Vessel traffic services), AMSA, Canberra. Available at https://www.amsa.gov.au
^The nominal size of car carriers is expressed in RT, or the number of 1966 RT43 Toyota Coronas that it can carry.
^Twenty-foot Equivalent Unit, a standard shipping container. The nominal size of a ship in TEU refers to the number of standard containers that it can carry.
^The voyage data recorder for a cargo ship larger than 3,000 gross tons, constructed before July 2002 may be an S‑VDR.
^Soderholm, J.S. Turner, K.I. Brook, J.P. Wedd, T. & Callaghan, J. (2019). High-impact thunderstorms of the Brisbane metropolitan area. JSHESS 69(1), 239-251. Available at Journal of Southern Hemisphere Earth Systems Science.
^The higher speeds observed on board the ships and by sensors operated by PBPL cannot be directly compared to BoM data. BoM measurements are normalised to indicate windspeeds at 10 metres above ground level.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 21 October 2025, a Robinson R22 helicopter with one pilot on board was conducting a private flight from Jimboomba to Southport, Queensland.
Prior to departure, the pilot loaded a box of freight, approximately 1,000 mm long, 350 mm wide and 400 mm deep, weighing 10 kg, onto the passenger seat and secured it by wrapping the seatbelt around the box. The flight departed Jimboomba at 1033 local time with a flight time of approximately 12 minutes.
As the pilot turned onto the base leg for final approach to runway 01 at Southport, the box on the passenger seat shifted and interfered with the cyclic[1] control resulting in the helicopter being unable to turn left. The helicopter then veered to the right and as the pilot focused their attention on moving the box, they lost control of the helicopter which came into contact with trees before colliding with terrain, resulting in substantial damage (Figure 1). The pilot sustained serious injuries in the accident.
Figure 1: Post-impact damage
Source: Queensland Police, annotated by the ATSB
Safety message
Pilots must adhere to CASA Regulation 91.610 (2) (b) Carriage of cargo – unoccupied seats, which states that the cargo, and the means of restraint of the cargo, must not interfere with the safe operation of the aircraft.
The ATSB has had 3 occurrences reported in a 15-year period involving Robinson R22 helicopters carrying cargo on the passenger seat which has interfered with the helicopter’s flight controls. All 3 of these occurrences resulted in a collision with terrain and substantial damage.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-057
Occurrence date
21/10/2025
Location
Southport Aerodrome
State
Queensland
Occurrence class
Accident
Aviation occurrence category
Collision with terrain, Flight control systems, Loading related, Loss of control, Unrestrained occupants/objects
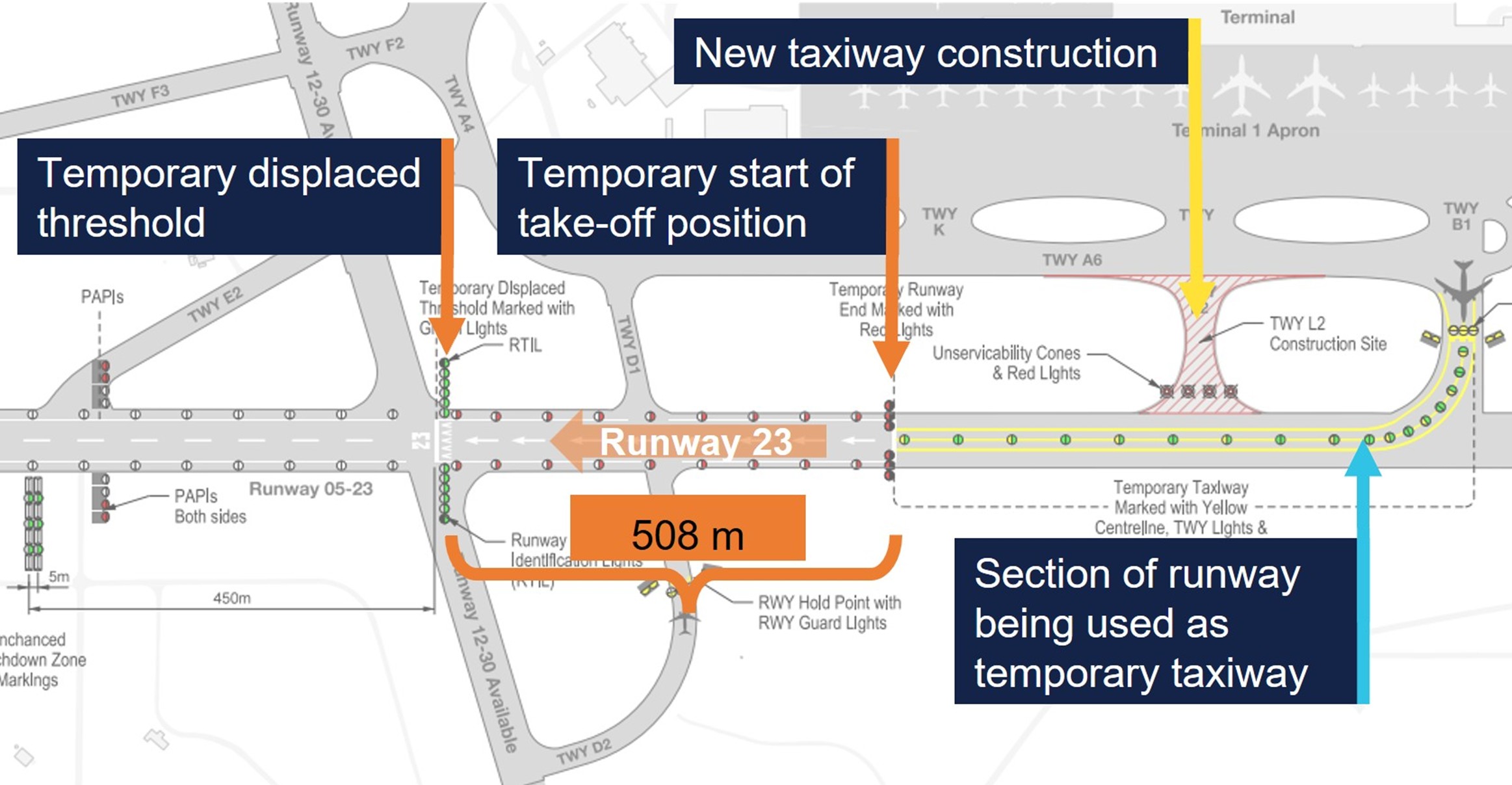
Confusing markings and lights contributed to several passenger aircraft taking off with less runway remaining than the flight crews had used for performance calculations, during taxiway construction works at Adelaide Airport earlier this year.
From 31 March to 20 May 2025, taxiway construction works took place at Adelaide Airport, an ATSB investigation report details.
Due to the works, the eastern end of the runway was being used as a taxiway, with the start of take-off position for runway 25 (and end of runway 05) displaced 650 m.
For aircraft landing on runway 23, a displaced landing threshold was 508 m beyond the temporary SOT position.
During the works period, 13 occurrences were identified, in both day and night operations, where flight crew mistakenly commenced the take-off on runway 23 from the displaced landing threshold, rather than the temporary SOT position.
“This meant the flight crews of multiple aircraft used performance parameters for a longer runway than was used, increasing the risk of a runway overrun, especially if a high speed rejected take-off had been required,” ATSB Chief Commissioner Angus Mitchell said.
The ATSB report notes the initial notice to airmen (NOTAM) released at the start of the runway works used inconsistent terminology and did not refer to the SOT markings being used.
For one of the reported occurrences, it was also identified that air traffic control did not challenge two incorrect readbacks of displaced threshold instead of displaced runway end by the flight crew.
One safety issue consistently identified across the occurrences was that lights and markings in use during the construction works were confusing, despite being in accordance with the standards specified in the relevant Civil Aviation Safety Regulations.
“The relevant manual of standards for aerodromes did not recommend or provide standardised options for movement area guidance signs, or other visual aids, to draw flight crews’ attention to the temporary SOT position, especially when that position was distant from a displaced threshold, and not coinciding with a taxiway or runway intersection,” Mr Mitchell explained.
“This investigation highlights how visual cues for the SOT position may be more difficult to identify than those for aircraft landing on a displaced threshold.”
Mr Mitchell noted the Australian standards for aerodrome signs, markings and lighting are based on the International Civil Aviation Organization (ICAO)’s existing standards, but do not include conspicuous visual cues for a displaced start of take-off position. The next amendment of the relevant ICAO Annex will incorporate construction signage, including for a temporary start of take-off position and stating the take-off run distance available.
The Australian Civil Aviation Safety Authority plans to consider inclusion of this signage in future amendments to the aerodrome manual of standards.
“It remains essential for pilots to review all available information before flight, to understand the visual cues necessary to identify both the threshold and SOT positions,” Mr Mitchell said.
“However, runway safety during runway works requires a system-wide approach, including flight crew, airport and aircraft operators, air traffic service providers, and regulators.”
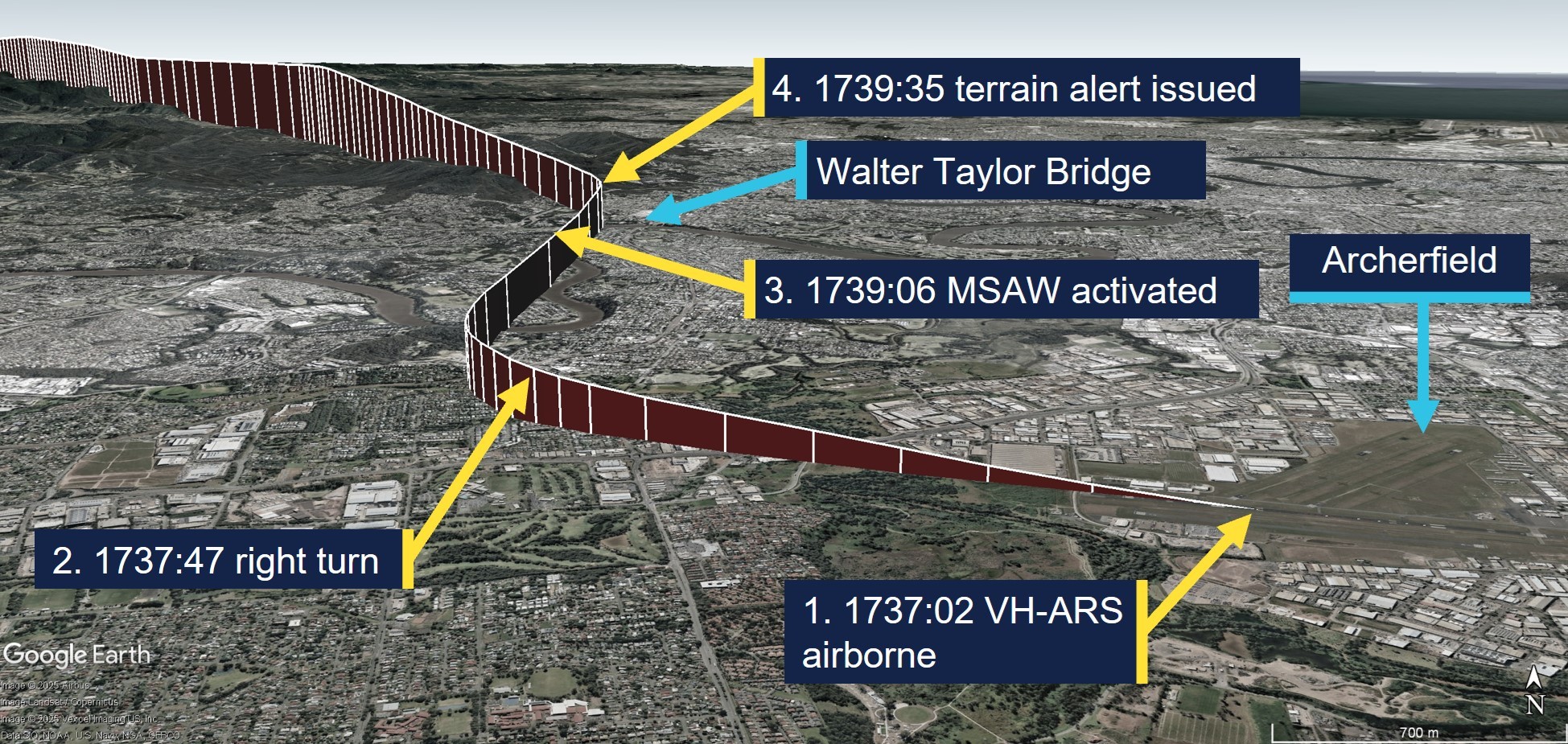
A Cessna 206 triggered an air traffic control terrain alert after conducting a visual flight rules take-off from Archerfield close to last light, an ATSB short investigation report details.
On 24 July 2025, the Cessna 206G was preparing for a training flight under instrument flight rules from Archerfield to Rockhampton. On board was an instructor and a pilot under training for a private instrument rating.
An instrument flight rules (IFR) flight plan was submitted with a departure time of 1730, prior to last light at 1739. CTAF procedures were in place after the Archerfield tower had closed at 1700.
However, the take-off occurred seven minutes later than planned, just two minutes prior to last light, and the instructor elected to conduct a visual flight rules departure, instead of an IFR departure.
This meant when last light occurred shortly after take-off, the aircraft was below the 2,900 ft minimum altitude when it left the circling area, triggering a minimum safe altitude warning at Brisbane Centre ATC.
ATC requested the pilots expedite their climb to at least 3,000 ft, which they did. The flight then continued without further incident.
“Despite the IFR plan, the instructor elected to conduct the VFR Northern departure instead of conducting an IFR departure,” ATSB Director of Transport Safety Stuart Macleod said.
“While it was feasible that the aircraft would reach the required minimum altitude before last light based on their flight plan departure time of 1730, take-off actually occurred 7 minutes later than what was flight planned.”
Mr Macleod said the incident highlights the importance of planning, particularly around times of day when rules change, such as the transition from day to night.
The final report notes the instructor opted for a VFR departure for the IFR flight because they believed it was the preferred method for Brisbane ATC traffic management.
In line with this, during the investigation the ATSB became aware of a potential conflict point over Archerfield Airport, for IFR departures from Archerfield and IFR arrivals into Brisbane Airport runway 01R.
“IFR arrivals to Brisbane runway 01R pass overhead Archerfield at 3,000 ft, which is the same altitude ATC needs IFR departures from Archerfield to climb to in the circling area before departing, creating a potential traffic conflict point for ATC to manage,” Mr Macleod explained.
“This concern is understood by the parties involved, and a project is underway to develop a procedural instrument departure from Archerfield Airport.”
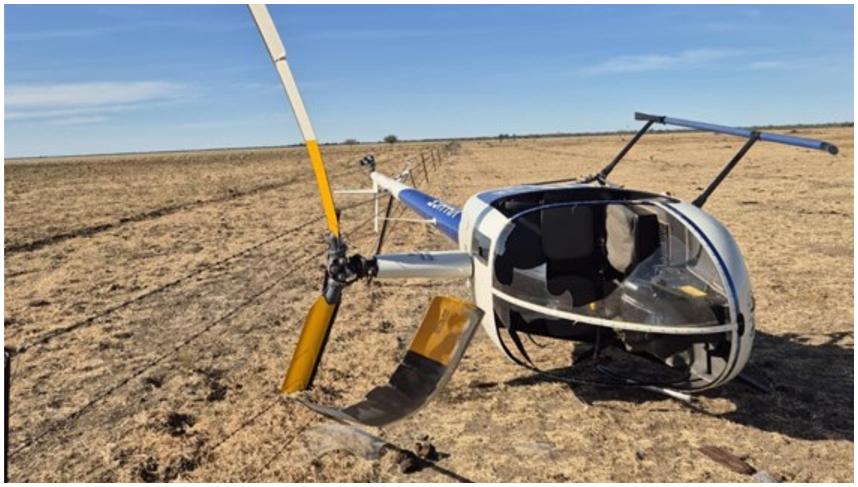
A mustering pilot was uninjured in a tail strike accident in a Robinson R22 after they immediately applied the correct tail rotor failure technique, as had been included in a recent proficiency check, an ATSB final report details.
The helicopter was one of two being used for mustering cattle on a property in eastern Northern Territory on 1 July 2025 when, as it was working an animal towards a holding yard, the animal baulked and turned away from the mustered direction.
“With limited time to react, the pilot attempted to stop the animal changing direction but, with a tailwind present, did not anticipate the additional power required to flare the helicopter,” ATSB Director of Transport Safety Dr Stuart Godley said.
The helicopter descended in a tail low attitude before the tail rotor struck the ground.
The R22 subsequently began to rotate and the pilot, assessing there was a tail rotor failure, reduced the throttle to decrease the torque, and increased the collective to cushion the aircraft onto the ground.
The pilot estimated that the helicopter had completed 2 or 3 full rotations, and still had some rotation when the right skid made contact with the ground, causing the helicopter to roll over to the right.
The main rotor blades then impacted the ground and the helicopter came to a stop on its right side, resulting in substantial damage.
“The pilot had recently conducted a proficiency check which included simulated tail rotor failures,” Dr Godley said.
“This likely allowed them to react quickly, and correctly apply the emergency technique, avoiding a more serious accident.”
The pilot was able to exit the helicopter, uninjured, once it came to a rest, and later stated that their wearing of a flight helmet had prevented a head impact during the accident sequence.
“Aerial mustering is a high-risk activity involving low flying, often near obstacles, powerlines and stock,” Dr Godley concluded.
“This accident highlights the benefit of recent emergency training, which in this case likely helped the pilot to react to the tail rotor failure with the correct technique before the helicopter became uncontrollable.”
An ATSB final report details how features of the airport runway and taxiway contributed to three separate misaligned take-off incidents before first light from Perth Airport’s runway 06.
On 12 June 2023, a Virgin Australia Boeing 737-800 entered Perth’s runway 06 via taxiway V from the south, the investigation report details. As the aircraft turned onto the runway, the crew inadvertently went past the centreline and aligned with the left-hand runway edge lighting.
After this, in two occurrences on 10 August 2023 and 4 April 2024, a Cessna Conquest 441 charter aircraft also entered runway 06 via taxiway V, but from the north. It also turned beyond the centreline, aligning with the right-hand runway edge lighting.
No damage was reported in the first incident involving the 737. During the take-off roll, the crew identified they were misaligned, and manoeuvred to the centreline, continuing the take-off and flight to Sydney without further incident.
During the second incident, the Cessna 441 pilot detected an impact with the aircraft and returned to land in Perth. Subsequent inspection found no aircraft damage, but several damaged runway edge lights.
In the third incident, the Cessna 441 pilot – a different pilot to the prior occurrence but in the same aircraft – heard an unusual noise, but believed it originated from outside the cabin, so continued their take-off and flight to Southern Cross. A runway inspection later that morning found several damaged runway edge lights and, after returning to Perth, the pilot identified minor damage to the aircraft’s right engine propeller.
ATSB Director Transport Safety Kerri Hughes said in all three incidents there were common contributing factors that increased the risk of misaligned take-offs.
“All three occurred before first light, exacerbated by factors specific to runway 06/24, which unlike Perth’s main runway, does not have centreline lighting,” Ms Hughes noted.
“There was also an unlit and unmarked pavement area on each side of the runway, making it appear wider, and the lead-on lights from taxiway V continued across the taxiway to the other side, meaning there was limited guidance when taxiing to the runway centreline.”
After the first two occurrences, Perth Airport submitted a notice to Airservices Australia requesting an update to the Aeronautical Information Publication to highlight the misaligned take-off risk on runway 06. This update was made effective in November 2023.
The airport has also painted chevrons on the extra pavement on either side of runway 06 to delineate this area from the useable runway.
Ms Hughes noted one factor specific to the first incident involving the 737, was the flight crew reported their attention was diverted to completing pre-take-off tasks and their take-off clearance, while lining up on the runway.
Following that occurrence, Virgin Australia revised its before take-off procedure to reallocate tasks earlier in the taxi to reduce flight crew workload during line-up.
The airline also added caution notes to its Perth Airport supplementary port information about centreline misidentification on runway 06, and developed case studies involving this event, which were incorporated into non-technical skills training.
The operator involved in the latter two occurrences, Western Sky Aviation, distributed notices to its flight crew, including strategies to check runway alignment prior to take-off.
“The features of airport runways and taxiways can vary, and at times the combination of these features can increase the risk of runway misalignments,” Ms Hughes said.
“This can be exacerbated at night-time, when the amount of visual information available is markedly reduced. These reduced visual cues can affect pilots even when they are familiar with an airport.”
The ATSB’s final report also encourages pilots to report any circumstances where they believe they may have conducted a misaligned take-off, to limit the risk to their aircraft and others subsequently using the same runway.
“This would also allow aerodrome operators to identify any trends or emerging misaligned take-off hotspots, and consider mitigations,” Ms Hughes concluded.