A gas tanker had just left its berth at the Port of Brisbane when it lost propulsion for two minutes as two of its three electrical generators were not properly configured, an ATSB final report explains.
On 15 March 2025, the 100-metre, Liberian-flagged Gaschem Homer departed the BP Products berth in the Port of Brisbane, under the conduct of a harbour pilot.
While it was being turned towards the port’s entrance, it experienced an electrical blackout, resulting in the total loss of all propulsion and steering control.
Power was able to be restored after about two minutes, during which time the pilot used the assisting tug to keep the ship within the shipping channel.
An ATSB investigation identified two of the ship’s three auxiliary diesel generators had been incorrectly left in manual mode for the departure.
This meant that when the bow thruster, an auxiliary propulsion unit, was engaged during departure, the resultant surge in electrical load led to an overload of the only generator providing power, and the subsequent tripping and blackout.
“No injuries or damage occurred in this case, but a loss of propulsion and steering for a ship in a confined area like the Brisbane River is a serious incident,” Chief Commissioner Angus Mitchell said.
Looking beyond this individual occurrence, the ATSB’s investigation identified Gaschem Homer’s safety management system did not have adequate controls to manage the risk of a complete power failure due to generators being inadvertently left in manual mode during manoeuvring operations.
Specifically, the ship operator’s safety management system had generic engine room operational procedures for its fleet. This meant Gaschem Homer’s safety management system did not consider the specifics of its systems.
“Industry practice dictates that a procedure should provide sufficient detail as to how a task is carried out, including when and by whom, while a checklist is typically purposed as a memory aid, itemising key actions to ensure nothing is overlooked,” Mr Mitchell said.
“In this serious incident, the pre-departure checklist was purposed as a substitute for a detailed procedure, but provided little in the way of specific and usable task descriptions. Consequently, the crew had to rely on memory and experience to complete critical tasks, which increased the likelihood of an oversight.”
In response, the ship’s manager has conducted a risk assessment and established additional controls to prevent total power failures.
The shipboard safety management system was also amended to include guidelines for blackout prevention and procedures requiring generators to be set for automatic load sharing before manoeuvring.
Pre-departure and arrival checklists have also been amended, and a power demand matrix has been developed.
The company has also introduced targeted training for watchkeeping engineers on critical power management and monitoring tasks.
“These safety actions adequately addressed the safety issue identified by the ATSB’s investigation,” Mr Mitchell said.
“But for all operators, this incident should highlight the importance of ensuring all risks associated with shipboard operations and critical equipment are identified, assessed and effectively controlled.
“A safety management system should encompass up-to-date and usable ship-specific procedures, as well as any additional technical controls if procedural barriers alone are insufficient to mitigate risk.”
The ATSB is investigating a runway incursion involving a Fairchild Industries SA227-DC, registered VH-HPE, at Mackay Airport, Queensland, on 12 November 2025.
During the take-off run, the pilot of the Fairchild SA227 observed a safety vehicle on the runway and overflew the vehicle in close proximity.
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release
The final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties, so that appropriate safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2025-067
Occurrence date
12/11/2025
Occurrence time and timezone
20:00 Australian Eastern Standard Time
Location
Mackay Airport
State
Queensland
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Defined
Investigation type
Occurrence Investigation
Investigation phase
Final report: External review
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Near collision, Runway incursion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Fairchild Industries Inc
Model
SA227-DC
Registration
VH-HPE
Serial number
DC-823B
Aircraft operator
Sharp Aviation Pty Ltd
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes
Activity
Commercial air transport-Scheduled-Scheduled freight only
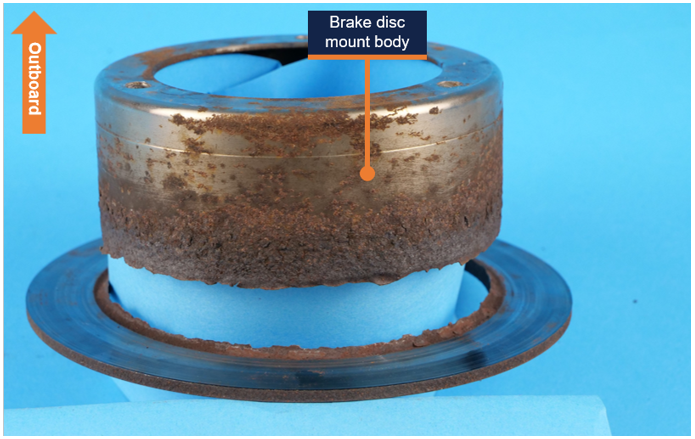
A Sling aircraft’s brake disc was severely corroded before it fractured after landing at Moorabbin Airport, an ATSB investigation has found.
The two-seat light aircraft, operated by Learn to Fly Australia, was being used for a training flight with an instructor and student pilot on board out of Melbourne’s Moorabbin Airport on 14 February this year.
After landing on runway 17R and vacating the runway via taxiway A4, there was a jolt and an unusual sound from the right side of the aircraft.
The instructor continued to taxi, and after noticing that the aircraft’s wheel brakes were less effective, brought the aircraft to a stop and conducted after-landing checks without noting anything significant.
After then taxiing to the operator’s parking area and exiting the aircraft, the instructor saw the right main landing gear brake disc had failed.
“The ATSB’s examination of the brake disc identified severe corrosion had compromised its structural integrity to the point where it failed during normal braking after landing,” ATSB Director of Transport Safety Dr Stuart Godley said.
“This corrosion was not identified by those maintaining and operating the aircraft as having progressed to a point where failure of the brake disc was possible.”
The investigation report notes the operator parked its aircraft on concrete pads in the open at Moorabbin Airport, which is about 3km away from Port Phillip Bay.
“Being parked outside and operated in the vicinity of a saltwater environment would have contributed to the corrosion development,” Dr Godley noted.
“The effect of the environment was also demonstrated by the extent of corrosion observed on the brake disc assemblies of the other 6 aircraft in the operator's fleet.”
The aircraft had been fitted with an unapproved aftermarket brake disc.
“As there was no record in the aircraft logbooks of fitment of the brake disc, the time taken for the corrosion to develop could not be established,” Dr Godley noted.
“However, there were multiple opportunities to intervene ahead of the failure, given that the aircraft was being inspected daily by pilots, and typically every 2 months by a maintenance organisation,” Dr Godley said.
“Importantly, the maintenance organisation was aware of the corrosion, but had not identified that it had progressed to a point where the structural integrity of the brake disc had been compromised, or taken any maintenance actions to limit its progression.”
The operator has subsequently replaced all corroded brake discs fitted to its entire Sling fleet with approved parts, and has amended its procedures to move aircraft onto the apron prior to boarding to allow for easier access to inspect landing gear.
“Aircraft brake system failures can result in serious outcomes such as a runway excursion or a taxiing collision,” Dr Godley noted.
“As such aircraft operators and maintainers should take timely action to prevent the progression of corrosion, and replace parts before the serviceability of an aircraft is affected,” he said.
“Operators should also give consideration to their aircraft operating environments, and whether additional maintenance can be undertaken to limit corrosion development.”
A Piper Cherokee Lance light aircraft pitched up and yawed to the left before colliding with terrain shortly after take-off at Shellharbour Airport, near Wollongong, a preliminary report from an ongoing ATSB investigation details.
On the morning of 11 October 2025, the Piper PA-32R-300 was departing from Shellharbour on a planned flight to Bathurst, NSW, with a pilot and two passengers on board.
ADS-B flight data and footage from a number of security cameras, which captured the flight has allowed the investigation to establish that as the aircraft was taking off from runway 26, it abruptly pitched up and yawed left, then followed a left turning flightpath before striking the ground and coming to rest at the threshold of the intersecting runway 34. The pilot and passengers were fatally injured, and the aircraft was destroyed.
“From the data available we can ascertain the aircraft rolled for about 410 m on runway 26 before it abruptly pitched up, yawed to the left and became airborne,” ATSB Chief Commissioner Angus Mitchell said.
“The aircraft then climbed away from the runway nose-high, while initially skidding and rolling left, before the skid reduced and its angle of bank appeared to stabilise briefly as it followed a left‑turning flight path.
“But just after reaching about 50 ft above ground level, it began to descend, and collided with terrain a few seconds later.”
Mr Mitchell noted that the ATSB is yet to determine why the aircraft pitched up and yawed before colliding with terrain.
“This preliminary report details factual information gathered during the early evidence collection phase, and does not contain findings or analysis, which will be included in a final report,” he noted.
As outlined in the preliminary report, data showed the aircraft’s groundspeed was 61 kt as it lifted off into a 12 kt headwind, increasing to 64 kt as it commenced turning left.
As the turn continued and with an increasing tailwind component, the groundspeed increased to a recorded maximum of 70 kt, immediately before impact.
All major aircraft components were accounted for during the ATSB’s examination of the accident site.
Examination of the aircraft itself, both in situ and later in a secure hangar, indicated the engine was driving the propeller at the time of impact, the aircraft’s landing gear was extended, and the flaps were extended to the 10‑degree setting.
The stabilator trim was set to slightly nose up, and the rudder trim was neutral.
A Garmin 750 navigation unit was recovered from the wreckage and retained by the ATSB for further examination.
“As the investigation continues, the ATSB continues to further review and examine the recorded data, along with consideration of aircraft maintenance records, recovered aircraft components, and the pilot’s medical records, qualifications and experience,” Mr Mitchell said.
A final report will be released at the conclusion of the investigation.
“If any critical safety issues come to light during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.”
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 17 October 2025, at 1413 local time, an American Champion Aircraft Corp 8GCBC (Scout), with 2 pilots on board, had conducted aerial observation operations before landing at Busselton Airport, Western Australia.
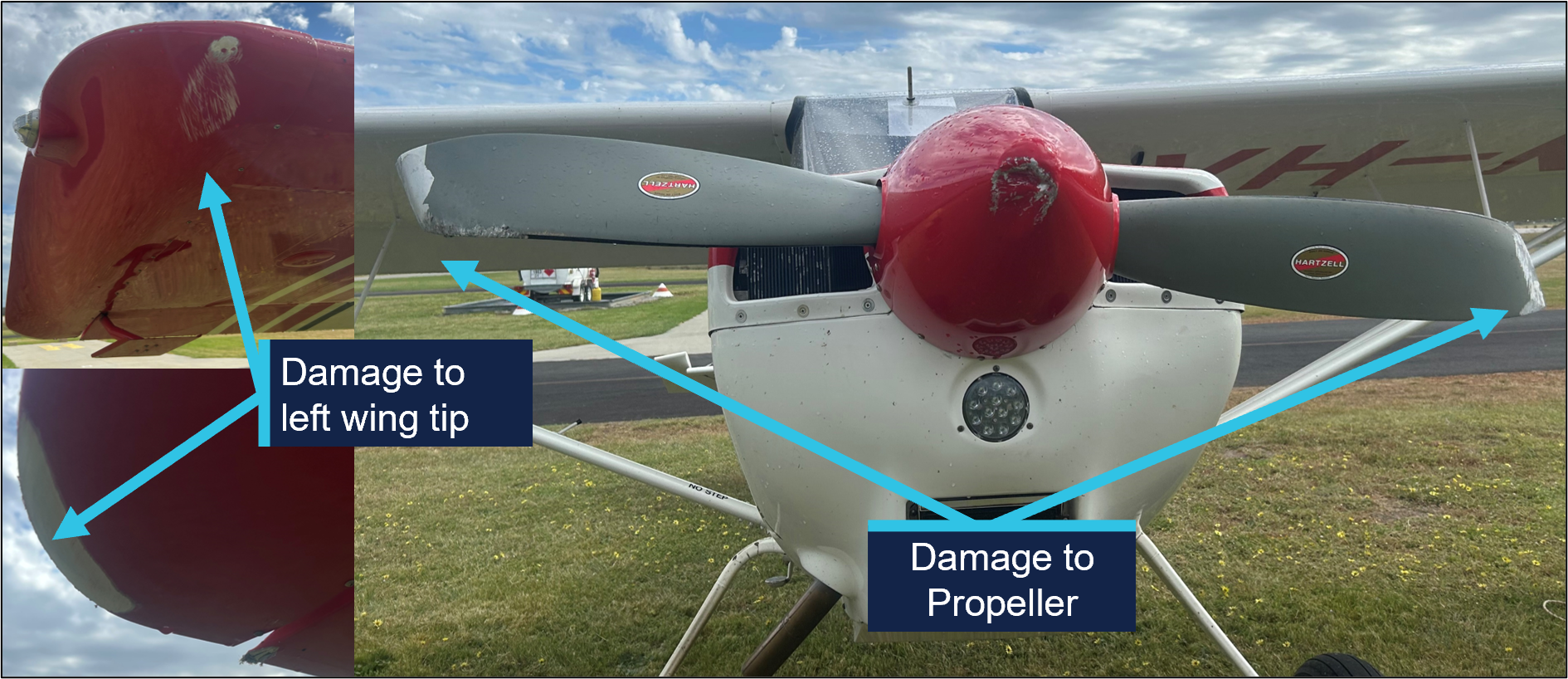
The pilot reported that during the crosswind landing, after touching down with the tailwheel still clear of the ground, the aircraft left wing lifted due to a gust and the right wing struck the runway.
The pilot also believed that whilst they were recovering using the rudder controls, the toe brakes may have been inadvertently applied. This likely caused the aircraft to pitch forward, resulting in propellor impact with the ground and the aircraft coming to rest in a nose-over position (Figure 1).
Figure 1: Aircraft post-occurrence
Source: Photo supplied by operator
Inspection of the aircraft post‑event noted damage to the aircraft, that included the right wing and the propeller (Figure 2). One of the pilots incurred minor injuries.
Figure 2: Aircraft damage
Source: Photo supplied by operator, annotated by the ATSB
The landing was on runway 03 (Figure 3). The recorded weather conditions at the time was wind at 332° at 12 kt, gusting to 15 kt.
Figure 3: Approach orientation Busselton Airport
Note: aircraft not to scale. Source: Google Earth, annotated by the ATSB
The pilot operating manual for the Scout notes a crosswind limit of 17 kts. The variable wind strength of the gusting crosswind may have been close to the maximum demonstrated limit for the aircraft.
The operator reported that the pilot flying had previously demonstrated competency in crosswinds during landing. Furthermore, in this instance, the senior pilot in the back seat did not attempt to take over control during the landing, as they felt the conditions well within both the aircraft and the pilot flying’s capabilities.
The manual describes that the technique is to place the control stick into the wind (up‑wind aileron up) and assume a tail high attitude with the elevator to prevent drift.
Safety message
This occurrence highlights the importance of exercising caution when operating in conditions that have the potential to exceed the maximum demonstrated crosswind speed of an aircraft.
It also illustrates the need for pilots to establish a personal minimums checklist that is commensurate with the flying experience of the individual. If the conditions do not meet these criteria, or if there is any doubt, pilots should not attempt the landing, consider conducting a go-around, change runways or hand control to a more experienced pilot.
Tailwheel aircraft can be susceptible to crosswind gusts during the later stages of landing. Depending on the magnitude and direction of the gust, there may be insufficient time to apply corrective controls before the aircraft deviates from the intended path.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2025-055
Occurrence date
17/10/2025
Location
Busselton Airport
State
Western Australia
Occurrence class
Serious Incident
Aviation occurrence category
Control issues, Ground strike
Highest injury level
Minor
Brief release date
17/11/2025
Aircraft details
Manufacturer
American Champion Aircraft Corp
Model
8GCBC
Sector
Piston
Operation type
Part 138 Aerial work operations
Departure point
Margaret River Aircraft Landing Area, Western Australia
Correct operation of approved mode S transponders can significantly improve situational awareness of other traffic on the ground. Electronic surveillance information is an effective trigger to alert pilots of other ground traffic. Early use of mode S transponders before taxi assists the process of ‘alerted see‑and‑avoid’ to identify and avoid traffic conflict.
What happened
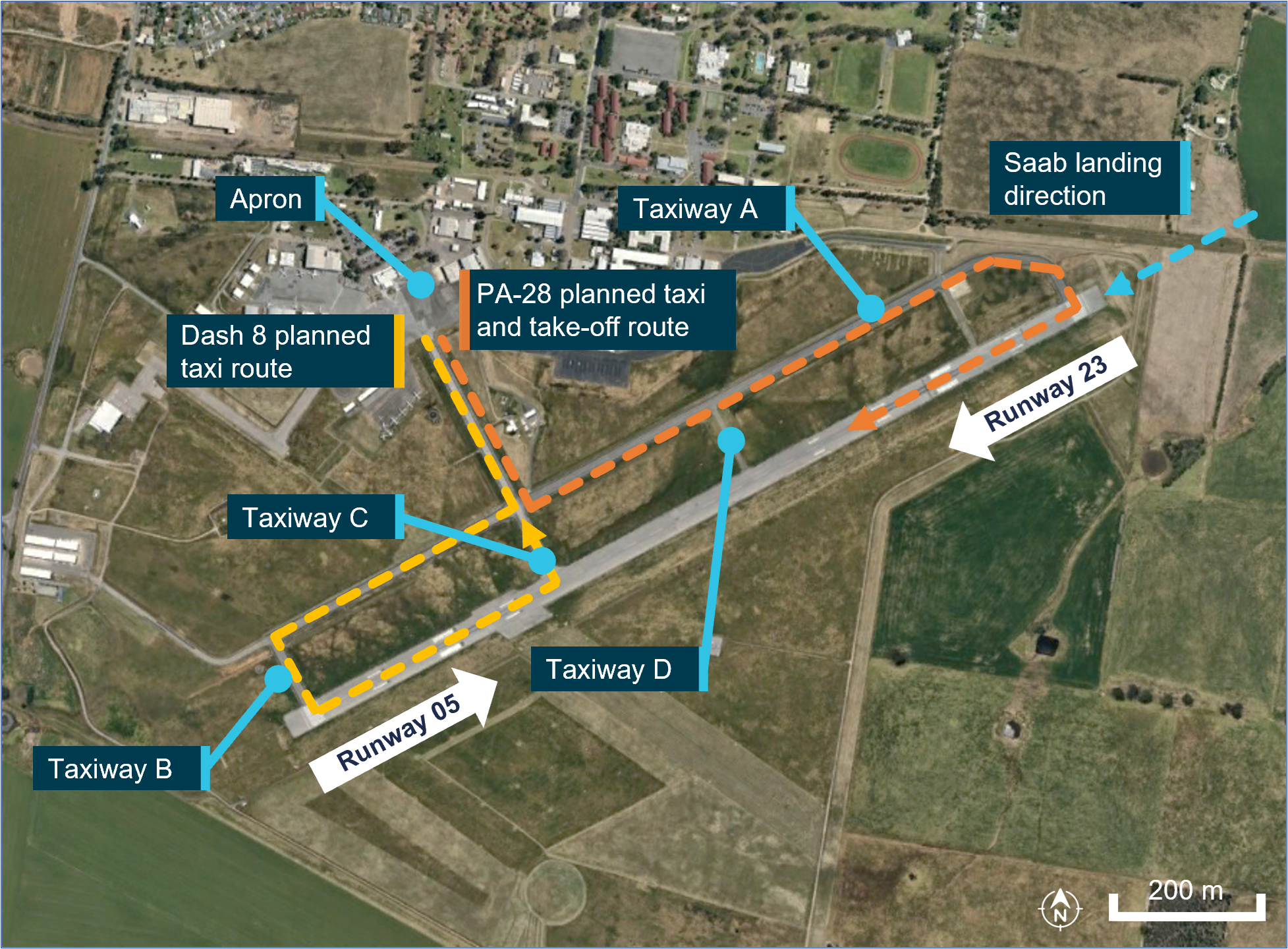
On 15 July 2024, a De Havilland Aircraft of Canada Limited DHC-8 (Dash 8), registered VH-QOD, entered runway 05 at Wagga Wagga, unaware that a Piper PA-28, registered VH-XDK, was commencing its take-off roll from the reciprocal runway 23. The Dash 8 pilots did not detect the PA-28 until the crew of a third aircraft broadcast that there was an aircraft taking off.
Why did it happen
The pilot of the PA-28 reported selecting the mode S transponder mode to ON/ALT prior to entering the runway. This was in compliance with their operations manual and standard operating procedures. However, this meant that the aircraft would not be electronically conspicuous to other traffic in the vicinity of the aerodrome, prior to entering the runway.
While not a formalised procedure for the Dash 8 crew, electronic surveillance equipment could be used as an aid to identify potential conflicting ground movements. The crew of the Dash 8 reported that transponder information was used to identify potential traffic at the time to develop their mental model.
Safety advisory notice
AO-2024-041-SAN-001: The effective use of mode S transponders from the first movement of the aircraft can serve as an effective tool in adding another layer of collision avoidance between aircraft at a non‑controlled aerodrome. Using the mode S transponder, particularly if the aircraft has ADS-B OUT capability, is the most effective way of making an aircraft electronically conspicuous and delivering maximum interoperability with other aircraft as well as the ground traffic environment. The ATSB advises pilots and operators to review their procedures to ensure that mode S transponders are on from first movement of the aircraft, particularly at non-controlled aerodromes.
Use of mode S transponders during taxi
At non-controlled airports, maintaining awareness of other traffic is critically important. Good airmanship dictates that all pilots should be looking out and using all available resources at their disposal. Pilots can guard against the issues highlighted by this incident by utilising all available tools at their disposal.
Turning your mode S transponder on prior to taxi will increase your electronic conspicuity to other aircraft, enhancing their situation awareness and alerted see and avoid practices. Likewise, using an electronic flight bag at a non‑controlled aerodrome can enhance your awareness of other traffic in the vicinity when they are using mode S transponders or ADS-B.
On 18 October 2025, a Go Ballooning Gold Coast balloon pilot and a ground crew member were preparing for a scheduled sunrise sightseeing flight near Beaudesert, Queensland. Weather forecasts indicated light winds and some clearing rain. The operator’s tour manager arrived at the launch site at about 0500 local time with 24 passengers booked for the flight. As the crew began the envelope cold inflation, a change in wind direction pushed the partially inflated balloon envelope across the field, striking 2 light posts near the road. After the crew recovered the balloon from the light posts, it was relocated with the help of the passengers. An inspection by the pilot identified a tear in one of the upper envelope panels.
The pilot, who was also the maintainer, estimated the tear to be about 45 cm and conducted a field repair using specialised adhesive tape. After checking the weather conditions were suitable for launch, the pilot assessed the repair was sufficient to continue with the proposed flight. The crew boarded the passengers, and the balloon departed the Beaudesert launch site.
During the latter part of the flight, the repair degraded, allowing air to escape from the balloon’s envelope. The pilot continued the flight to the chosen landing site as planned and landed the balloon without further incident.
What the ATSB found
The ATSB found that the position selected within the launch site did not provide sufficient clearance from nearby obstacles, which resulted in damage to the balloon’s envelope after being moved by an unexpected wind gust.
The envelope repair using adhesive tape was not conducted in accordance with the manufacturer’s requirements, and the pilot did not fully understand the manufacturer’s limits for field repairs for the tear location and did not review the manufacturer’s written requirements before proceeding with the repair.
The pilot’s decision to continue with the intended flight was likely influenced by the pilot’s perception of the expectations of the waiting passengers, along with the improvement in weather conditions and the pilot’s confidence in the repair. Subsequent in‑flight deterioration of the repair emphasised the potential risk of the tear propagating which increased the risk to occupants on board. However, the pilot continued for the remaining 5–10 minutes of the flight rather than landing immediately.
Safety message
Balloon repairs must be conducted in accordance with the manufacturer’s instructions.
Non-approved repairs that appear to work without consequence can normalise unsafe practices over time and represent a significant risk to all occupants on board. Operators and maintainers should be familiar with the approved maintenance standards and practices before commencing any repair work.
Pilots and maintainers should also be aware of external and internal commercial pressures to continue a flight without fully researching and conducting an appropriate repair.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is Reducing passenger injuries in commercial ballooning operations.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 18 October 2025, a Kubíček BB142P hot-air balloon, registered VH-RRP, was being operated by Go Ballooning Gold Coast on a sightseeing flight from Beaudesert, Queensland.
The pilot, who was also the operator and maintenance controller, obtained relevant weather information from the Bureau of Meteorology and via a phone‑based weather application, Rain Parrot, to assess the weather conditions and plan the proposed flight.
The pilot picked a familiar launch site location in a large open field adjacent to a supermarket car park, which they had operated from numerous times previously.
The pilot and a ground crew member arrived at the launch site (Figure 1) at about 0300 to unload and prepare the balloon for launch. The balloon basket was positioned close to the public road bordering the launch area. This position was within 10 m of a public road and about 20 m from nearby light posts bordering the shopping centre car park.
Figure 1: Location of balloon launch site
Source: Google Earth, annotated by the ATSB
As per Go Ballooning Gold Coast’s operational procedure the pilot released several helium pibal[1] balloons to observe wind conditions at different levels for the intended flight and confirmed the launch site suitability for the planned flight.
The pilot and ground crew member were preparing the balloon by cold inflation,[2] when the pilot described that the wind speed increased to about 6 kt and changed direction. At a time that could not be determined, the partially inflated balloon envelope moved from a north-east to a south-west position around the basket that was secured to the front of a 4-wheel drive car. The crew attempted to restrain the balloon by pulling on the crown line,[3] but were unable to stop the movement of the envelope. The balloon envelope continued to travel across the public road and struck 2 light posts (Figure 2) in the shopping centre car park. During recovery from one of the light posts, it sustained a tear to the upper section of the envelope.
Figure 2: Photograph of balloon after striking light posts
Source: Supplied, annotated by the ATSB
At about 0500 local time, the tour manager and 24 passengers, booked for the scheduled sunrise flight, arrived at the launch site on the operator’s bus.
After the crew retrieved the balloon envelope it was deflated and packed up with the assistance of some of the passengers.
The balloon was then repositioned away from the obstacles and laid out for the pilot to inspect for any damage. The pilot identified a tear in the upper section of the envelope, above the balloon equator.[4] The pilot estimated the tear to be about 45 cm in length (Figure 3), and no other damage was identified.
The pilot reported that they had previously carried out field repairs on balloons and was confident that the specialised adhesive tape provided from the manufacturer would temporarily fix the tear to allow the flight to proceed as planned.
After the pilot applied the tape, the balloon was fully inflated with hot air and was visually inspected. The pilot reported that they believed the repair was sufficient to continue with the flight. About 20 minutes after completing the repair and following an assessment that the wind speed was within the allowable limits for launch, the pilot decided to continue with the flight as scheduled. A safety briefing was given to the passengers before boarding, and the flight proceeded at about 0550.
Figure 3: Photograph of damage to balloon envelope
Source: Supplied, annotated by the ATSB
The pilot reported that after take-off, the balloon tracked in a southerly direction, opposite to the intended direction of flight for about 30 minutes. The pilot reported that about 5–10 minutes before arriving at a newly planned landing site, heat at the top of the balloon likely caused the adhesive repair tape to weaken, partially re-opening the tear and allowing a small, uncontrolled venting of air. The pilot reported not being concerned and continued to the planned landing site. The balloon landed safely at 0620 at Kerry, Queensland, about 17 km south of Beaudesert.
Context
Pilot information
The pilot was the owner and operator of Go Ballooning, operating sightseeing balloon flights and private charters in south-east Queensland, since 2015.
They held a Civil Aviation Safety Authority (CASA) Commercial Pilot (Balloon) Licence and had over 20 years of experience with 2,299 total flying hours at the time of the incident. In the previous 2 weeks the pilot had flown about 6.5 hours in VH-RRP. The pilot held a current CASA class 2 aviation medical certificate, a valid CASA maintenance authority (MA) for balloons and a valid Kubíček maintenance certificate.
The pilot reported having slept their normal 7–8 hours prior to the incident and self‑assessed as ‘1’ on a fatigue scale of 1–7 where 1 is fully alert and 7 is completely exhausted.
Balloon information
VH-RRP was manufactured in 2022 by the Kubíček factory in Czechia and could operate with a maximum of 24 passengers and 1 pilot. The balloon was registered to Go Ballooning Australia on 9 December 2022.
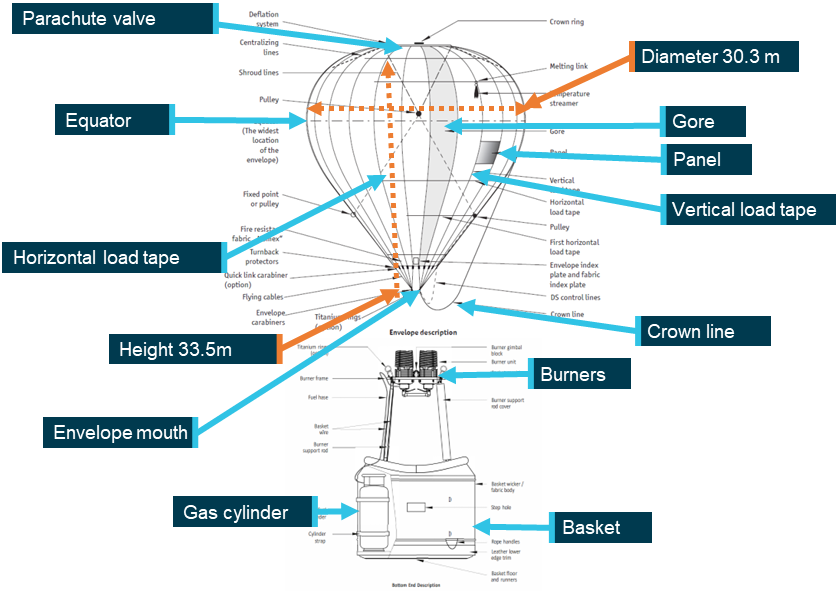
The BB142P balloon envelope had a volume of 14,158 m2 and was about 30 m in diameter and almost 34 m in height which supported a maximum take-off weight of 4,500 kg (Figure 4). The balloon envelope was constructed of 32 gores[5] and was inflated by hot air from 4 burners connected to 4 independent fuel systems.
Figure 4: Schematic of a Kubíček balloon
Envelope and basket not to scale. Source: Adapted from the Kubíček hot air balloon flight manual (section 1), annotated by the ATSB
A manned free balloon certificate of airworthiness was issued on 16 February 2023, and the balloon had accumulated a total time of 369.6 hours in service and the basket 942 hours at the time of the event.
Meteorological information
The ATSB obtained relevant weather data from the Bureau of Meteorology. For Beaudesert, observations for wind were recorded at 1-minute intervals at ground level about 3 km to the north-west of the launch site. Between 0448 and 0515, surface winds were reported as west to north-westerly at approximately 3 kt, shifting through the west to a southerly, then south‑easterly at approximately 2 kt from 0516 through to the launch time of 0550. The forecast temperature for Amberly, (about 50 km to the north-west of the launch site) at the time of the launch was around 16°C.
The pilot recalled that, at the time of preparation, forecast conditions for the time of the launch were:
light and variable winds
unrestricted visibility
no low cloud, a few scattered high-level clouds.
Regulatory oversight
Operators require a Civil Aviation Safety Authority (CASA) Air Operator’s Certificate (AOC) to conduct balloon transport operations under Part 131 of the Civil Aviation Safety Regulations (CASR).
The Part 131 Manual of Standards (MOS) sets out the specific requirements for these operations. The MOS does not specify size requirements for balloon launch sites, however an operator is required to keep records of launch and landing sites. This includes a description of each launch and landing site with maps, diagrams, and records of any hazards associated with the site and any limitations or restrictions. The documented information is required to form part of the operator’s exposition.[6]
CASA Advisory Circular (AC) 131-02 v4.0 specifies in section 8.2 Ground Handling:
Operators and PIC [pilot in command] are recommended to consider the hazards or risks to persons or property that might arise during any of the following activities:
• laying out, inflation and preparation for launch
• take-off and climb
• landing, normal deflation and pack up
• relocation of inflated balloon on the ground
• use of the handling line for hot air balloons
• use of the trail rope for gas balloons.
Pre-flight damage assessment and repair
After contact with the light posts and inspection of the envelope, the pilot identified an estimated 45 cm tear, located above the equator of the balloon in gore 22, panel 26 (Figure 5) and no other damage. The pilot, who was also a maintenance authority, applied specialised adhesive tape to the tear as they had reportedly done on previous occasions for temporary field repairs on minor fabric damage.
Figure 5: Location of tear in balloon envelope VH-RRP
Source: Photograph supplied; diagram from Kubicek maintenance manual, annotated by the ATSB
Manufacturer instructions for envelope repair
The operator’s exposition outlined the pre-flight procedures with a list of pre-flight inspections and checks for the balloon which included verifying the envelope integrity in accordance with damage limitation in the Kubíček Hot Air Balloon Flight Manual (BFM).
The BFM provides information on the damage limits applicable to various sections of the balloon. Different sections of the balloon envelope are subject to varying thermal loads, internal pressures and fabric tensions during operation. Therefore, the structural consequences of damage will differ depending on where the damage is located on the envelope. The hottest and highest structurally loaded area of the balloon envelope is above the equator.
The operator accessed the BFM and the Kubíček Maintenance Manual(BMM) for the BB142P model.
The BFM stated that repairs above the first horizontal load tape are limited to:
…small holes or tears of no more than 5 mm (1/4 in) in any direction. The integrity of the panel must not be affected by the holes or tears.
Any damage exceeding the above limits must be repaired prior the next flight according to the instructions given by the Kubicek Maintenance Manual
For damage limitation the BFM warning states:
Any damage to the fabric weakens the fabrics resistance to tear and causes localized heating of the fabric around that damage. Damage exceeding those listed above increase the potential of propagating a tear or hole and is unacceptable for flight.
The BMM (section 3.21) repair guidance for using an adhesive patch above the equator, stated:
Adhesive Patch without Overstitching:
If the damage is not more than 2.5 cm (1") in any dimension. There must be minimum of 10 cm (4") between any two damaged locations on a single panel.
Adhesive Patch with Overstitching:
If the damage is not more than 10 cm (4“) in any dimension. May not be used if the damage extends to within 2.5 cm (1“) of a load tape. There must be a minimum of 10 cm (4“) between any two adhesive patches on a single panel.
A further note also stated that:
Always check adhesion of the patch as the adhesive may adhere differently on different materials (polyester vs. polyamide, ripstop, etc.) and its adhesion may also be affected by outside temperature, age and dustyness of the fabric, and other factors. When in doubt, use sewn patch.
Balloon envelope damage
The size (45 cm) and location (above the equator) of the tear significantly exceeded the limit to use adhesive tape for repair. The BMM stated that a sewn partial panel or panel with the same material as used in the original panel was required for a tear of this size. The panel repair is designated as a category B repair which covers the common maintenance tasks that may be carried out by individuals who have undertaken a manufacturer maintenance course and hold a valid manufacturer maintenance certificate. The approved method to repair the damage, as detailed in the BMM, required the affected panel to be repaired in accordance with the manufacturer's directions before further flight.
Operational information
Launch site selection and preparation
The pilot reported that between 40 and 50 sites were used for launching and landing balloons, with agreements in place with landowners to access several private properties on the Gold Coast. The operator’s exposition included documented information for each site, including the Beaudesert launch site. The balloon basket was positioned close to the public road bordering the launch area. While this suited the southerly wind at the time for the balloon layout, it left little clearance from other obstacles in the circumstances of a wind shift.
Passenger briefings
The pilot reported that the passenger briefing was given prior to boarding the passengers. It was described as the operator’s standard briefing and included details on the brace position for landing, that passengers should not enter or exit the balloon until the pilot has given permission and that smoking was strictly prohibited.
Balloon envelope damage in-flight
The operator’s exposition referred to the manufacturer’s flight manual for emergency procedures. The Kubíček BFM stated that in the event of damage to the envelope in‑flight the balloon should be kept flying at a low altitude to avoid a hard landing and landed as soon as possible.
Safety risk
ATSB investigation 198900820 illustrated that damage to the envelope of a balloon that propagates to the point where it rapidly deflates can have disastrous implications for flight safety.
On 13 August 1988, 2 hot air balloons, VH-NMS and VH-WMS, were operating tourist flights near Alice Springs Airport. VH-WMS departed about 2 minutes ahead of VH-NMS and climbed to about 4,000 ft AMSL (2,000 ft AGL) and drifted in a westerly direction. After reaching 4,000 ft, VH-WMS commenced descending as VH-NMS climbed towards it. VH‑NMS continued climbing until its envelope collided with the basket of VH-WMS, tearing a large hole in the envelope fabric. The disruption to the envelope of VH-NMS prevented the balloon maintaining inflation and it descended uncontrolled until it collided with terrain. The pilot and 12 passengers were fatally injured.
Safety analysis
During the envelope pre-inflation for a scheduled sunrise sightseeing balloon flight, the wind suddenly increased and changed direction pushing the balloon envelope into contact with 2 nearby light posts. This caused a tear in a panel above the equator of the envelope greater than the manufacturer’s allowable limit. The pilot applied adhesive tape to repair the damage while passengers waited. After hot inflation and inspection of the repair, the pilot then decided to operate the flight as scheduled. The repair subsequently degraded in‑flight however a safe landing was made.
This analysis will explore the assessment of the launch location, damage assessment and repair, as well as factors relating to the continuation of the flight.
Launch site
The pilot selected a regular launch site and although the site had been used previously, the positioning of the basket and envelope layout for the flight did not provide sufficient available space to ensure clearance of surrounding obstacles at all times during the balloon’s preparation for flight, increasing the risk of envelope damage.
A wind change occurred at a critical part of envelope inflation, causing the envelope to contact nearby light poles. During recovery from the light pole, the envelope sustained damage.
Repair
The onsite repair did not comply with the operator’s exposition which required repairs to be conducted in accordance with balloon manufacturer’s instructions.
Although adhesive tape was allowed for smaller tears up to 10 cm in that area of the envelope, this tear was at least 45 cm. The decision to apply adhesive tape for the repair indicated that the pilot, who was also the maintainer, did not fully understand the manufacturer’s requirements relating to envelope damage limits and did not review the manufacturer’s written requirements before proceeding with the repair.
The absence of any other obvious deformation of the envelope, or further tearing after the tape was applied, was interpreted that the repair was sufficient. Previous experience repairing minor damage with the adhesive tape likely reinforced the perception that this was an adequate method for this repair, even though 45 cm was beyond admissible damage where such repair was permitted.
Had the pilot consulted the hot air balloon flight manual, a sewn panel repair would have necessitated the postponement or cancellation of the flight. The pilot’s decision to repair the tear to enable the planned flight to continue without consulting the manufacturer’s envelope repair requirements increased the risk of further in-flight envelope tear propagation, potentially leading to catastrophic envelope failure and a subsequent uncontrolled descent.
Flight continuation
Research has shown that many aviation accidents involve a ‘plan continuation bias’ or ‘plan continuation error’.[7] That is, pilots decide to continue with the original plan of action despite the presence of cues or information that suggests changing the course of action would be the safer option (Orasanu and others 2001; Orasanu 2010). Plan continuation bias is often associated with situations involving dynamically changing risk and pilots underestimating the risk level (Orasanu and others 2001; Wiegmann and others 2002).
The absence of any immediate deterioration in the tape repair after hot inflation likely reinforced the pilot's belief that the envelope was airworthy. The pilot’s expectation that the balloon was serviceable, supported the pilot’s desire to continue the flight. Improving stability in the surface wind direction and strength then provided an opportunity to launch the balloon.
With the 24 passengers already arrived and waiting, it was likely the pilot perception of the passengers’ expectations was also a strong motivator to continue and influenced the pilot’s decision to conduct the flight. The weight of the perceived passenger expectation would likely have the pilot searching for solutions to enable the flight to proceed, rather than cancelling and rescheduling the flight to conduct repairs.
The manufacturer’s flight manual instructions were to land as soon as possible following in‑flight envelope damage. While the pilot reported awareness of the tape repair degrading in flight, they did not assess the need to land earlier.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the flight with damaged envelope involving Kubíček BB142P, VH‑RRP, near Beaudesert, Queensland, on 18 October 2025.
Contributing factors
The location in the launch area did not provide adequate clearance from obstacles during inflation.
A change in the wind direction caused the partially inflated balloon envelope to move and strike 2 light posts, resulting in significant envelope damage.
The pilot identified the tear and conducted a repair not in accordance with the balloon manufacturer’s requirements, increasing the risk of in‑flight envelope failure.
The pilot continued with the intended flight, likely due to their confidence in the repair, improvement in the weather conditions and perceived passenger expectations. When the repair failed, the pilot continued for the remaining 5-10 minutes of the flight rather than landing immediately.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of the incident flight
Civil Aviation Safety Authority
Bureau of Meteorology
balloon manufacturer
witness
video footage of the accident flight and other photographs taken on the day of the accident.
References
ATSB (1989) Kavanagh Hot Air Balloon E-260, VH-NMS, 14 km SSE of Alice Springs Airport NT, 13 August 1989 198900820
Orasanu, J., Martin, L., & Davison, J. (2001). Cognitive and contextual factors in aviation accidents: Decision errors. In Linking expertise and naturalistic decision making (pp. 209-225). Psychology Press.
Orasanu, J. M. (2010). Flight crew decision-making. In Crew resource management (pp. 147-179). Academic Press.
Wiegmann, D. A., Goh, J., & O'Hare, D. (2002). The role of situation assessment and flight experience in pilots' decisions to continue visual flight rules flight into adverse weather. Human factors,44(2), 189-197.
Submissions
Submissions were received from:
the pilot of the incident flight
Civil Aviation Safety Authority
Bureau of Meteorology.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Pibal: a lighter-than-air gas‑filled small rubber balloon used to estimate wind speed and direction at the launch (take-off) site and in the first few hundred feet above the surface.
[2]Cold inflation is the initial stage of inflating a hot air balloon. Cold air is forced into the envelope prior to using the burners.
[3]Crown line: a rope connected to the top of the balloon envelope used to control the balloon’s position during inflation.
[4]The equator of the balloon is the widest part of the balloon envelope in diameter. The loss of hot air from a same size tear would be greater when the tear was higher in the balloon.
[5]A gore is a section of fabric running from the top to the bottom of the envelope.
[6]An exposition is a Part 131 document detailing an organisation's policies and processes, specific to each operator.
[7]In terms of continuing a flight to the original destination, plan-continuous bias is often known as ‘mission‑itis’, ‘get‑home‑itis’ and ‘press‑on‑itis’.
Occurrence summary
Investigation number
AO-2025-065
Occurrence date
18/10/2025
Occurrence time and timezone
04:45 Australian Eastern Standard Time
Location
Near Beaudesert
State
Queensland
Report release date
05/02/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Aircraft preparation, Airframe - Other, Collision
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Kubicek Factory
Model
BB142P
Registration
VH-RRP
Serial number
2052
Aircraft operator
Go Ballooning Gold Coast Pty Ltd
Sector
Balloon
Operation type
Part 131 Balloons and hot air airships
Activity
Commercial air transport-Non-scheduled-Joyflights / sightseeing charters
At around 0655 local time on 7 November 2025, a Cessna 172N, registered VH-SCU and operated by Consolidated Pastoral Company (CPC), departed Newcastle Waters Airport, Northern Territory, on a training flight. On board the aircraft were the pilot and an instructor. The pilot was being trained to fly at low level, with the intention of obtaining a low-level operational rating.
About one hour into the flight while flying at around 300 ft above the ground at an airspeed of 80 kts, and manoeuvring to follow a creek bed, the pilot initiated a steep turn to the right. During the turn, control of the aircraft was lost and it descended towards the ground. The instructor attempted to override the pilot’s control inputs but could not do so before the aircraft impacted terrain. The aircraft came to rest upright but was substantially damaged. The instructor received minor injuries, the pilot was uninjured.
What the ATSB found
The ATSB found that while conducting a steep turn at low level, excessive aft control input was applied which almost certainly caused the aircraft to enter an aerodynamic stall. Subsequently, inappropriate recovery control inputs by the pilot limited the instructor’s ability to intervene before the aircraft collided with the ground.
The initial excessive control input was likely a combined result of the pilot being focused on maintaining a track over the ground feature and their inexperience in handling the aircraft during low-level flight. The subsequent application of an inappropriate stall recovery technique was likely caused by the pilot reverting to instinctive rather than learned behaviour under stress.
The ATSB also found that the instructor's recovery control inputs likely prevented the aircraft from impacting terrain in a nose down attitude and reduced the severity of the collision.
What has been done as a result
The flight training provider undertook a critical review of its training practices and risk mitigation measures.
Safety message
This accident highlights the importance of understanding the relationship between the elevator control stick position and the aircraft’s angle of attack, to minimise the risk of an aerodynamic stall. The wing will stall when the control stick is moved beyond a fixed position, irrespective of airspeed and attitude. During steep turns at low airspeed, awareness of the stick position provides increased awareness of the aircraft’s performance relative to its limits. This is particularly important to consider when operating close to the ground, such as during take-off, landing, and when conducting low-level air work. Attention may become focused on positioning the aircraft relative to ground features rather than monitoring its aerodynamic performance, and the time available for recovery from an undesired state will be limited.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
At around 0655 local time on 7 November 2025, a Cessna 172N, registered VH-SCU and operated by Consolidated Pastoral Company (CPC), departed Newcastle Waters Airport, Northern Territory, on a training flight. On board the aircraft were the pilot and an instructor. The pilot was being trained to fly at low level,1 with the intention of obtaining a low-level operational rating and had completed 6 training flights with the instructor over the previous 3 days. The purpose of this flight was to consolidate the earlier training and prepare for the low-level rating flight test.
The aircraft was initially climbed to an altitude of approximately 2,000 ft above ground level (AGL), where the pilot demonstrated a sequence of flight manoeuvres. These included left and right turns at angles of bank up to 60° and minimum radius turns at angles of bank up to 45° (see the section titled Minimum radius turns). The pilot also demonstrated their ability to identify and recover from a stall during a minimum radius turn.
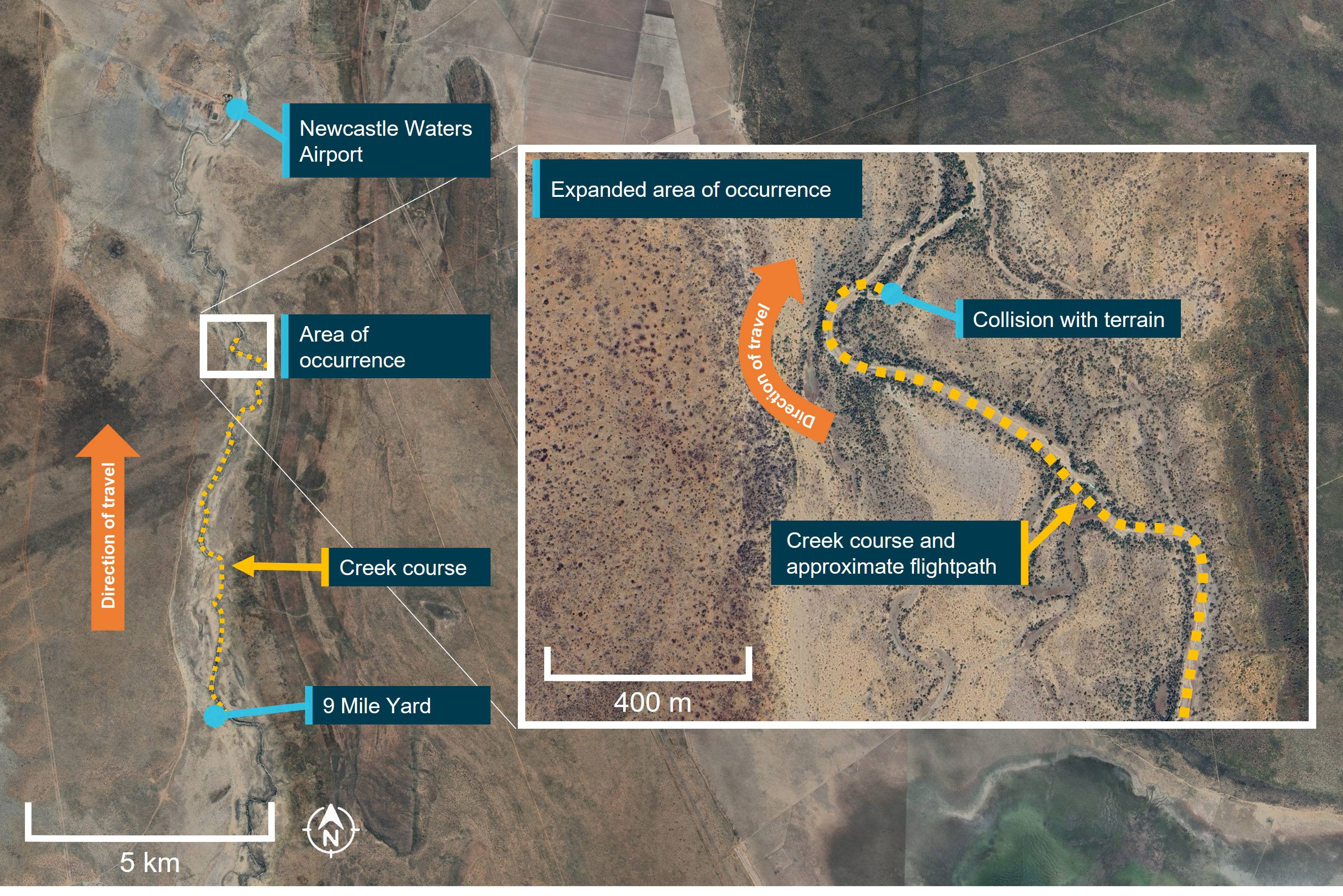
The pilot then proceeded to perform a pre-briefed low-level task, which simulated a typical airborne survey of station infrastructure. This task was flown at altitudes between 200 ft and 1,000 ft AGL and incorporated simulated contingencies such as system and engine failures. At the completion of this portion of the training flight, the aircraft was approximately 13 km south of Newcastle Waters Airport, just north of 9 Mile Yard (Figure 1).
The instructor then asked the pilot to return to the departure airport by following the Newcastle Waters Creek in a northerly direction, simulating a water course survey activity (Figure 1). The task commenced at an altitude of 300 ft and the pilot was reminded not to descend below the pre-briefed minimum altitude of 200 ft. At around 0750, a few minutes into the activity, the pilot observed that the creek bed ahead made a sharp turn to the right and they began to manoeuvre the aircraft to keep the ground feature directly below the aircraft. At the start of this manoeuvre, the aircraft was flying approximately 300 ft above the terrain at an airspeed of around 80 kt, with flaps retracted.
Figure 1: Low-level flightpath over the Newcastle Waters Creek and the location of the collision with terrain
Source: Google Earth, annotated by ATSB
The pilot rolled the aircraft right to a bank angle of around 45º. As the turn commenced, both the pilot and instructor noted that the aircraft’s nose was pitching down and the aircraft was beginning to descend. The instructor expected that the pilot would correct the pitch attitude by adding power, following the technique that had been taught and successfully demonstrated during the preceding training.
In addition to the observed descent, the pilot also noted that the aircraft was not turning quickly enough to remain above the ground feature, and in response they rapidly applied more aft control column input to tighten the turn, recalling that they also added a ‘smidge’ more power, however the instructor advised no power was added. In response, the aircraft rolled further to the right and continued to descend. Immediately, the pilot attempted to level the aircraft’s wings and arrest its descent by applying left roll control input, however they maintained aft control input. They stated they did not hear the stall warning horn activate throughout the manoeuvre.
The instructor could also not recall if they heard the stall warning, however they assessed that the aircraft was in an aerodynamic stall and attempted to intervene by making opposing corrective inputs through their own control column but they could not overcome the control forces being held by the pilot. They could not remember if they advised they were ‘taking over’ however, the pilot flying recalled that the instructor had announced that they were ‘taking over’ and they subsequently released the controls. The pilot advised that the aircraft was already below the tops of the trees before the instructor’s inputs could take effect.
The instructor stated that they judged that the aircraft would now almost certainly impact the terrain, and that the rudder pedals and throttle were the only effective control inputs available. They applied full power and right rudder with the aim of raising the aircraft’s nose and inducing further right yaw. The instructor’s intent was to prevent the aircraft from impacting terrain nose first and therefore improve the likelihood of survivability.
As the aircraft descended below the height of the treetops, its pitch attitude had almost levelled, its roll angle had reduced, and it was yawing to the right. The aircraft then impacted the trees, before coming to rest upright on its undercarriage, on relatively flat terrain. It had yawed during the impact sequence, such that it was facing back along its flightpath through the trees. The aircraft sustained extensive damage, particularly to its wings and tail section, with the latter being almost completely detached from the rear fuselage (Figure 2).
Figure 2: VH-SCU as it came to rest following impact with trees and terrain
Source: Supplied
Immediately after the aircraft came to rest, fuel began draining from a rupture in the right wing prompting the crew to exit the aircraft through the left door. During the impact, the instructor sustained minor injuries, while the pilot suffered no visible injuries but reported some neck pain.
The pilot used a mobile telephone to report the occurrence to the operator, and a ground vehicle was dispatched, which arrived at the accident site at around 0835 and subsequently transported both crew members back to the Newcastle Waters station. Following an initial examination by medical staff, both crew were conveyed to a medical clinic for treatment. The instructor was later discharged, while the pilot was transported to a hospital in Alice Springs for further assessment and monitoring. The pilot was discharged from hospital the following day.
Context
Flight crew
The pilot of VH-SCU held a Commercial Pilot Licence (Aeroplane) issued in 2024 and a class 1 aviation medical certificate. They had accumulated around 300 flight hours, mostly on single engine piston training aircraft, including the Cessna 172 and Diamond DA40. They had worked as a pilot on the station since October 2025.
The instructor held an Air Transport Pilot Licence (Aeroplane), a class 1 aviation medical, and a low-level rating, among other ratings and endorsements. They had accumulated a total of around 24,500 flying hours, with approximately 2,500 hours in the Cessna 172. They had flown 240 hours in the 90 days prior to the occurrence, with 25 of those in the Cessna 172.
Aircraft
VH-SCU was a Cessna Aircraft Company 172N manufactured in the United States in 1977 and assigned serial number 17268700. It was equipped with a Textron Lycoming O‑320‑H2AD piston engine, fixed pitch propeller, and fixed tricycle undercarriage. Maintenance records indicated that the airframe had accumulated a total flying time of 15,995 hours prior to the accident flight and the engine had 927.6 hours since overhaul. The aircraft was being maintained under the Civil Aviation Safety Authority Schedule 5 and had flown 45 hours since its most recent maintenance event, which was a 100-hour inspection performed on 23 August 2025.
The aircraft had no recording devices on board and nor was it required to.
Weather
No weather information was recorded for Newcastle Waters station, however the Bureau of Meteorology provided information for the nearest observation station at Daly Waters, approximately 123 km north. An observation issued at 0800 local time reported the temperature to be 29°, with a dew point of 21°, an atmospheric pressure of 1010 hectopascals, and a surface wind of between 8–10 kt from the north. This station did not provide a report of visibility or cloud cover.
Both flight crew provided consistent reports of the weather conditions at Newcastle Waters. They recalled a temperature of between 22–26°, winds of between 5–10 kt from the north-west, smooth air with no mechanical turbulence, and no cloud. There was light smoke haze but this did not significantly impair their visibility. The instructor estimated the density altitude2 to be approximately 3,000 ft.
Low-level training
The low-level flight training was being provided under the provisions of Part 141 of the Civil Aviation Safety Regulations (CASR). The instructor was qualified to deliver this training and had provided the same training to other pilots, employed at the station, on numerous occasions prior.
Part 61 of the CASR required an applicant for a low-level rating and aeroplane low-level endorsement to have, among other conditions:
• undertaken at least 5 hours of dual flight training in an aeroplane while receiving training in low level operations
• pass a flight test defined in the Part 61 manual of standards.
The Part 61 manual of standards prescribed a set of knowledge and flying competencies, which must be satisfactorily demonstrated during the low-level rating flight test. The specific activities and manoeuvres to be demonstrated during the flight test included:
• navigate at low-level
• conduct steep, max rate and min radius turns
• recover from approach to stalls – level and turning
• recover from unusual attitudes
• recover from wing drop at the stall
The training syllabus employed by the instructor planned for all airborne activities and manoeuvres to be taught over a period of 5 flying hours. The instructor reported that, in their experience, most students achieved competency within this period.
At the time of the accident, the pilot flying had undertaken 10.1 hours of low-level training. Training records indicated that additional flying hours were required at the start of the course for the student to demonstrate competency in some manoeuvres, including maintaining altitude during steep turns, stall recognition and recovery. However, during a period of upper air work conducted earlier in the accident flight, the student had successfully demonstrated competency in all these manoeuvres.
Aircraft stall behaviour
The angle of attack (AOA) is the angle at which the wing meets the relative airflow passing the aircraft. It is directly related to elevator position and therefore control stick position. The amount of lifting force produced by the wing increases with increasing AOA until a critical angle is reached. At the critical AOA (typically 16–18°), the wing aerodynamically stalls and lift production decreases abruptly. Recovering from a stall requires AOA be reduced below the critical angle by reducing aft control stick displacement.
Should the critical AOA be approached during a turn, using aileron to level the wings increases the AOA of the inside wing and may cause it to stall prior to the outside wing. This can result in the angle of bank rapidly increasing rather than decreasing. Instead, it is recommended that rudder is used to level the wings when a stall is encountered.
Minimum radius turns
A minimum radius turn achieves a change in aircraft direction over the smallest possible ground space. This technique is often used in low-flying operations where manoeuvring is made with respect to a ground feature and within confined terrain. Minimum radius turns are typically conducted at high angles of bank and lower airspeeds. Both conditions increase the AOA required to maintain level flight. The margin between required AOA and the critical (stalled) AOA is therefore reduced.
Adding additional aft control stick displacement during a minimum radius turn can quickly result in the wing exceeding the critical AOA and entering a stalled condition. For this reason, pilots are often instructed to correct low attitude during minimum radius turns through application of power, rather than additional aft control stick input.
Related occurrences
There have been a number of recent ATSB investigations into fatal accidents that resulted from a loss of control while manoeuvring during low-level flight.
On 27 June 2024, the pilot of a Cessna 172N, registered VH-SQO, was mustering sheep at Mulgathing Station, South Australia. The aircraft was observed to dive to an estimated height of about 50 ft above the ground before climbing rapidly, turning to the left and then descending towards the ground. The ATSB found that, while mustering without the appropriate endorsement, the pilot lost control of the aircraft leading to an aerodynamic stall and spin from an altitude that was not recoverable.
On 3 March 2022, the sole pilot of a Cessna U206G, registered VH-JVR, was conducting a low-level geophysical survey, about 120 km west of Norseman, Western Australia. At about 1430, the aircraft’s satellite tracking system stopped reporting its position. Wreckage was subsequently located 3.2 km west of the aircraft’s last recorded position. The ATSB found it was likely that, during a manoeuvre to intercept the next survey line, for undetermined reasons, control of the aircraft was lost at a height from which recovery was not possible.
On 13 April 2021, a Cessna R172K, registered VH-DLA, departed Canberra Airport, Australian Capital Territory, with a pilot and observer on board to conduct powerline survey work to the north of Sutton township, New South Wales. The aircraft was subsequently observed flying low above the trees before commencing a left turn that continued in to a steep descent and collision with terrain. The ATSB found that while manoeuvring to align the aircraft to inspect a powerline, the aircraft aerodynamically stalled and entered a spin at a height that was insufficient for recovery prior to the collision with terrain.
On 4 December 2021, the pilot of an Air Tractor AT-400 aircraft, registered VH-ACQ, was conducting aerial spraying operations on a property 75 km west-south-west of Moree, New South Wales. During a right procedure turn, the aircraft was observed to climb then descend rapidly and collide with terrain. The ATSB found that the aircraft was too close to the start of the spray run during the turn, which probably resulted in the pilot tightening the turn. This almost certainly resulted in an aerodynamic stall at a height too low to recover before colliding with the terrain.
Safety analysis
The pilot and instructor were conducting a low-level navigation exercise, tracking along a ground feature at approximately 300 ft AGL and 80 kt.
Accounts from both crew members indicated that while making a steep right turn to follow the ground feature, the aircraft’s nose dropped. Additionally, the pilot observed thatthe aircraft was not turning quickly enough to remain over the river. In response, they sharply increased their aft control stick input rather than increase the bank angle. This almost certainly placed the aircraft into an aerodynamically stalled condition rapidly increasing the rate of descent and further rolling to the right.
The pilot did not follow the recommended method to address the nose drop at low level - application of power rather than increasing pitch, which they had demonstrated successfully earlier in the flight. The ATSB could not determine why the correct recovery technique was not applied. However, human factors research (Martin, Murray, Bates and Lee 2013) noted that when faced with a sudden unexpected aircraft condition, pilots may experience a rapid increase in stress and revert to instinctive behaviour over trained behaviour.
After recognising that the pilot had applied inappropriate control inputs the instructor attempted to intervene. It is uncertain what verbal communication was made between the crew, but there was a period of confusion over who had control of the aircraft, and it is likely both crew members were making control inputs simultaneously resulting in the instructor being unable to override the control inputs of the pilot, delaying the effectiveness of the recovery actions. Due to the proximity to the ground, the aircraft descended into terrain before this confusion could be resolved. Despite this, the instructor’s inputs to the throttle and rudder likely prevented the aircraft from contacting the ground in a nose down attitude and reduced the severity of the impact.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Cessna 172, VH-SCU, about 6 km south of Newcastle Waters, Northern Territory, on 7 November 2025.
Contributing factor
While training to follow a ground feature at low level, the pilot flying applied and held inappropriate control inputs, which led to an aerodynamic stall and limited the instructor’s ability to make corrective actions, resulting in the aircraft colliding with terrain.
Other finding
The instructor's control inputs likely prevented the aircraft from impacting terrain in a nose down attitude and reduced the severity of the collision.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by flight training provider
The flight training provider undertook a critical review of its training practices and risk mitigation measures.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and instructor of the accident flight
Consolidated Pastoral Company
Bureau of Meteorology.
References
Martin, Murray, Bates, and Lee (2015) Fear-potentiated startle: A review from an aviation perspective. The International Journal of Aviation Psychology, 25(2), pp.97-107.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot and instructor of the accident flight
Consolidated Pastoral Company
Civil Aviation Safety Authority.
Submissions were received from:
the pilot and instructor of the accident flight
Consolidated Pastoral Company.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^CASA defines low-level flight operation as any flying conducted below 500 ft above ground level (AGL), other than for the purpose of take-off or landing.
^Density altitude is the pressure altitude corrected for non-standard temperature. It is the altitude at which the aircraft ‘feels’ it is flying regardless of its actual height above sea level.
Occurrence summary
Investigation number
AO-2025-066
Occurrence date
07/11/2025
Occurrence time and timezone
07:50 Central Standard Time
Location
About 6 km south of Newcastle Waters
State
Northern Territory
Report release date
20/05/2026
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Final report: Dissemination
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Loss of control
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
172N
Registration
VH-SCU
Serial number
17268700
Aircraft operator
Consolidated Pastoral Company Pty Limited
Sector
Piston
Operation type
Part 141 Recreational, private and commercial pilot flight training
Activity
General aviation / Recreational-Instructional flying-Instructional flying - dual
The ATSB has issued a safety advisory notice urging pilots to switch on their mode S transponder from engine start, after a Dash 8 entered Wagga Wagga’s main runway while a Piper Cherokee was taking off last year.
On 15 July 2024, a QantasLink Dash 8 twin turboprop was being repositioned from one bay to another at Wagga Wagga Airport, requiring it be turned around by taxiing to the western end of the main runway, backtracking up the runway, and then exiting to return to the apron.
While the QantasLink flight crew was preparing for the repositioning, a Piper PA-28 light aircraft, operated by the Australian Airline Pilot Academy (AAPA), left the apron and began to taxi to the eastern end of the runway for a training flight.
About 10 minutes later, the Piper began its take-off roll from the eastern end of the runway, and the Dash 8 entered the runway at its western end.
The Dash 8 crew was not aware of the Piper until the Dash 8 crossed onto the runway from the holding point, and was notified of the potential conflict by the crew of a third aircraft.
The crew of the Dash 8 used reverse thrust to move back off the runway. At about the same time, the student pilot in the Piper rejected their take-off, and taxied off the runway mid-runway.
The ATSB’s investigation identified several factors that contributed to the Dash 8 crew not being aware of the Piper before entering the runway, including:
The reduced strength of ground-based VHF radio calls at the eastern end of the runway and the parallel taxiway, where the Piper was located.
The Dash 8 crew making and receiving ground-based transmissions on the aircraft’s VHF COM 2, as per QantasLink procedures. The location of the VHF COM 2 antenna on the belly of the aircraft likely led to situations where other aircraft had difficulty receiving and understanding radio transmissions, and where the Dash 8 did not receive the Piper’s radio transmissions.
The Piper pilot making the recommended radio calls but not attempting to directly communicate with the Dash 8 crew to arrange separation.
The crew of the Piper not switching on the aircraft’s mode S transponder during taxi.
Unalerted to the presence of the Piper, the Dash 8 crew did not visually detect it at the other end of the runway, about 1,700 m away.
Acknowledging a series of factors had contributed to the occurrence, ATSB Chief Commissioner Angus Mitchell noted the Piper’s mode S transponder, if switched on, likely would have made the smaller aircraft conspicuous on the Dash 8 crew’s electronic flight bags.
“AAPA’s operating manual only required pilots to activate the transponder prior to entering the runway,” Mr Mitchell noted.
“The use of a mode S transponder during taxi would normally provide an additional source of positional data to other pilots, aiding visual identification and alerted ‘see-and-avoid’ to other aircraft.”
In response, AAPA has changed its PA-28 Flight Crew Operating Manual, and Quick Reference Handbook, instructing that the transponder be selected to ALT mode after engine start.
More broadly, the ATSB has issued a safety advisory notice to all pilots and aircraft operators to follow suit and review their own procedures, and encourages all pilots to ensure mode S transponders are on from the first movement of the aircraft on the ground, particularly at non‑controlled aerodromes.
“Using the mode S transponder with ADS-B OUT enabled is the most effective way to make an aircraft electronically conspicuous for other aircraft, as well as the ground air traffic management environment,” Mr Mitchell said.
The ATSB’s final report also notes the use of the Dash 8’s belly-mounted VHF COM 2 antenna, as opposed to the roof-mounted VHF COM 1 antenna, was also identified as a likely contributing factor in two other ground communication events at Mildura Airport (AO-2023-025 and AO-2023-050(Opens in a new tab/window)).
“Testing conducted during the latter of those two investigations identified reception and transmission on the lower antenna on the ground had significantly reduced strength and clarity compared to the upper antenna,” Mr Mitchell said.
Aligned to this, De Havilland Aircraft of Canada Limited has also advised the Dash 8’s VHF COM 1 may provide a better line of sight with other aircraft or ground stations possibly resulting in improved communications for both transmission and reception.
The Civil Aviation Safety Authority also released new guidance and recommendations relating to the use of radios where the antenna is mounted on the underside of the aircraft fuselage to both Advisory Circular (AC) 91-10 and AC 91-14.
QantasLink has advised the ATSB that further assessment of the use of VHF COM 1 for ground-based communications at non‑controlled aerodromes for Dash 8 aircraft is being assessed, but is not yet finalised.
“The ATSB will monitor this safety issue as this action progresses,” Mr Mitchell said.
The operation of a Pilatus PC-6 skydiving aircraft’s horizontal stabiliser electric trim system will be examined as part oftheATSB’s ongoing investigation of a fatal accident near Moruya on the New South Wales South Coast.
A preliminary report, which contains information gathered to date in the ATSB’s investigation of the 27 September accident, explains the aircraft had taken off from Moruya Airport shortly before 1400, for a parachute jump flight over the airport, its ninth of the day.
After climbing to the planned jump altitude, recorded data shows the aircraft in a gradual descent from 15,000 ft to 14,000 ft as eight parachutists jumped out. The parachutists later reported the jump was normal, and all exited the aircraft safely.
At 1406:15, the pilot made a radio broadcast on the local CTAF radio that the parachutists had exited and the aircraft was on descent.
“Several witnesses on the ground then observed the aircraft enter a steep nose-down dive, rotating left before pitching up and rolling right,” ATSB Chief Commissioner Angus Mitchell said.
The aircraft’s last recorded ADS-B data position was at 1407:26, at 7,425 ft and descending at about 15,000 ft per minute.
It collided with terrain about 2.5 km north, and slightly west, of the northern end of Moruya Airport’s runway 36. The pilot was fatally injured.
ATSB transport safety investigators’ examination of the accident site showed the aircraft’s right wing struck a tree on the eastern side of George Bass Drive, and separated from the fuselage, before the aircraft collided with trees on the other side of the road. There was no post-impact fire.
“All major components of the aircraft were at the site, the propeller had indications that the engine was producing power at impact, and there were no indications of any pre-impact mechanical anomalies that would have precluded normal engine operation,” Mr Mitchell said.
“Wreckage examination also identified that the aircraft’s horizontal stabiliser trim actuator was in the fully nose-down position.”
The preliminary report details that the PC-6 is fitted with a horizontal stabiliser electric trim system, which in response to pilot inputs moves the entire horizontal stabiliser to adjust the pitch trim of the aircraft. This reduces the control forces the pilot is required to input on the elevator with the control column.
The report also details the aircraft flight manual’s instructions to pilots in the events of trim runaways and jammed trim actuators.
“As the investigation progresses, the ATSB will further examine the horizontal stabiliser trim system, alongside recorded flight data, aircraft history and maintenance records, operational procedures and documentation and pilot training.”
Mr Mitchell also said the investigation would consider the configuration of the aircraft’s doors, and the pilot’s opportunity to egress during the accident sequence.
“Consideration will be given to survivability aspects, given the pilot was almost certainly not in their seat when the collision occurred, and they were wearing their emergency parachute,” Mr Mitchell said.
A final report, with findings and the ATSB’s analysis to support those findings, will be released at the conclusion of the investigation.