Investigation summary
What happened
On the afternoon of 11 September 2024, the pilot of a Kawasaki 47GB3‑KH4, registered VH‑BEU and operated by Katherine Helicopters, was conducting a scenic flight over Nitmiluk (Katherine) Gorge, Northern Territory with 2 passengers on board.
About 13 minutes into the flight, while entering the mouth of the gorge, the pilot reported experiencing an engine power loss and lack of response from the engine. Due to inhospitable terrain in the area, the pilot identified a clear landing spot some distance away and attempted a forced landing at that location, during which time the aircraft collided with terrain.
The pilot and both passengers were uninjured in the incident, however, the aircraft was substantially damaged.
What the ATSB found
Several possibilities were considered during the investigation in relation to the reported engine power loss. While the ATSB did not conduct a physical inspection of the engine in this instance, a post‑incident inspection revealed that a large crack had developed in the engine exhaust pipework. Being a turbocharged engine, the escape of exhaust gases through the crack during operation has likely resulted in an engine power loss during flight due to the loss of boost pressure.
The ATSB also identified that the pilot was unable to cushion the landing during termination of the autorotation, likely due to low main rotor RPM, resulting in the helicopter colliding with terrain.
Safety message
Helicopter operations over harsh terrain offer limited safe emergency landing options. Autorotation to a suitable area in such circumstances requires accurate helicopter positioning and energy maintenance (airspeed and rotor RPM). This makes thorough and regular training in emergency procedures crucial for pilots operating in these demanding environments. The prompt action taken by the pilot, in identifying a suitable landing site, was instrumental in ensuring the safety of all personnel on board.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On 11 September 2024, the pilot of a Kawasaki Heavy Industries 47GB3‑KH4, registered VH‑BEU and operated by Katherine Helicopters, was conducting scenic flights over Nitmiluk (Katherine) Gorge, Northern Territory.
During the morning, the pilot conducted the required daily checks on the helicopter and completed a passenger flight over the gorge (Figure 1). After returning to base, the pilot refuelled the helicopter and completed short, uneventful ferry flights to Katherine Museum and return.
Figure 1: Nitmiluk (Katherine) Gorge scenic flight overview

Source: Google Earth, annotated by the ATSB
That afternoon, the pilot met 2 passengers at the operator’s base, and then completed the flight manifest including the passengers’ weight details, based on verbal information provided by the passengers. The pilot carried out their pre-departure checks, including a flat‑pitch check,[1] which were all normal. A safety briefing was also undertaken with both passengers, which reportedly included:
- use of seatbelts
- in‑flight procedures
- operation of the doors and emergency exits
- actions to be taken in case of an emergency.
At around 1451 local time, the helicopter departed and after making a turn towards the north, the pilot gradually climbed to about 1,000 ft above mean sea level (AMSL), proceeding north‑easterly along the Katherine River in the direction of the gorge.
About 10 minutes later, the pilot climbed further to a height of about 1,400–1,500 ft AMSL to fly neighbourly[2] while approaching the escarpment bordering Nitmiluk National Park (Figure 2). The pilot then arranged separation with the pilot of a second helicopter in the area, using the common traffic advisory frequency (CTAF).
Figure 2: View from helicopter of Nitmiluk National Park

Source: Passenger photograph, annotated by the ATSB
Approximately 3 minutes later, as the helicopter was entering the mouth of the gorge, the pilot noticed that the engine did not respond when they increased the throttle, and that the helicopter was decelerating and losing height. Due to being overhead undulating rocky terrain, the pilot commenced a right turn in search of a suitable landing site, in case they had to conduct a landing (Figure 3).
The pilot reported that the ensuing events occurred extremely quickly. While turning around, the helicopter kept slowing and the engine did not respond to throttle movements. They noticed a significant change in the engine noise, described as a low‑pitched ‘whir’ sound, and reported feeling stiffness in the pedals. Not knowing what was wrong with the engine, the pilot lowered the collective[3] and entered autorotation (see the section titled Autorotation).
During the descent, the pilot glanced at the instruments and noted that the engine RPM needle was split[4] from the main rotor RPM needle and again tried unsuccessfully to increase the throttle. The pilot later advised that the main rotor RPM was well below the green arc on the gauge, and the engine RPM was just below idle. The pilot reported identifying a landing site in a clearing about 400–500 m to the west of their location and broadcast a MAYDAY[5] call on the CTAF.
The helicopter proceeded downwind towards the clearing, attaining a maximum groundspeed in excess of 83 kt. Given the prevailing wind, that equated to an airspeed of about 70 kt, which was higher than the recommended autorotation speed for the helicopter type (see the section titled Autorotation). However, during the final approach to the selected landing site, the groundspeed, and given the crosswind approach, also airspeed was reduced to about 50 kt.
Figure 3: Helicopter flight path with identified elevation and ground speed
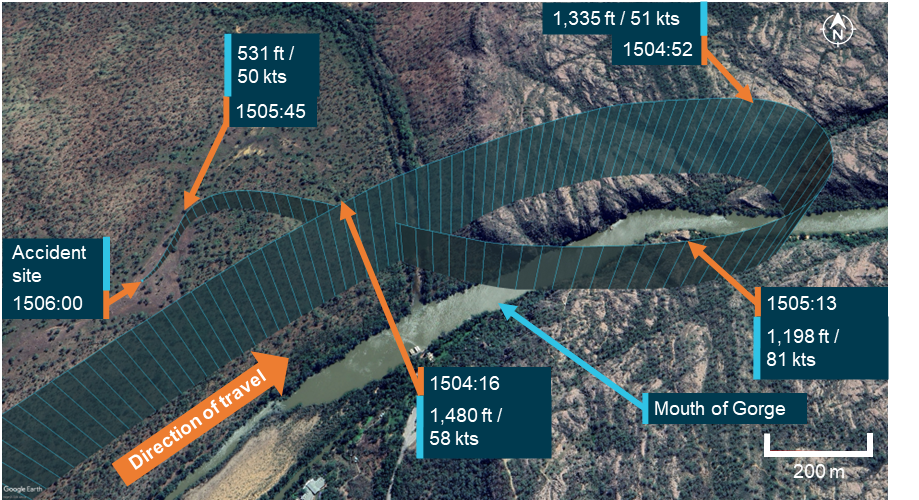
Source: OzRunways data on Google Earth, annotated by the ATSB
The passengers reported that during the descent, communication from the pilot was minimal. They were not advised by the pilot to brace for impact; however, upon hearing the MAYDAY call and seeing the pilot attempt an unexpected landing, both passengers suspected that an emergency situation had developed, and chose not to interrupt the pilot or distract them from their actions.
The pilot reported that, on nearing the landing site, they attempted to flare the helicopter but there was minimal flare effect, which they assessed was most likely due to low main rotor RPM. Consequently, the pilot attempted a run‑on landing, during which the helicopter collided with terrain, damaging its tail rotor/shaft and skids (Figure 4).
Figure 4: Helicopter accident site

Source: Operator
After landing, the pilot shut off the fuel, magnetos and battery. After checking on the passengers, the pilot disembarked the aircraft, ensured it was safe to exit with the main rotor blades still rotating, and then instructed the passengers to evacuate the aircraft. The pilot of the other helicopter operating in the area repeated the MAYDAY call on the area frequency and then circled overhead the accident site. A rescue crew arrived onsite shortly after and the pilot and both passengers were evacuated uninjured.
Context
Pilot information
The pilot held a commercial pilot licence (helicopter) and a class 1 aviation medical certificate. At the time of the incident, they had accumulated about 380 hours total aeronautical experience. All the pilot’s training and most of their flying experience has been obtained operating Robinson R44 helicopters. They had been flying for Katherine Helicopters for about 3 months.
While at Katherine Helicopters, the pilot received their Bell 47 endorsement after undergoing about 3 hours of training with an instructor that included the conduct of emergency procedures. The pilot also performed about 10 hours of in command under supervision (ICUS)[6] training with the operator.
Operator information
The operator was a helicopter tour operator based in Katherine, Northern Territory. It operated 2 Bell/Kawasaki 47 Helicopters and offered tour flights throughout northern Australia.
Previous incidents
The pilot had been involved in another engine failure incident on a second helicopter of the same type with the operator in July 2024, wherein an engine cylinder failed. The pilot completed a successful autorotation and there were no reported injuries. While this matter was reported to the ATSB, it was not investigated.
In addition to the incident above, the other helicopter operated by the operator was involved in a third off field landing, arising from an engine fault, in February 2024.
Helicopter information
The helicopter was a Kawasaki Heavy Industries 47G3B‑KH4, manufactured in 1969 in Japan by Kawasaki Heavy Industries and first registered in Australia on 20 June 1996. At the time of the accident, VH‑BEU had about 7,495 hours total time in service and had flown about 40 hours since its last periodic service inspection.
Engine and turbocharger system
VH‑BEU was powered by a Textron Lycoming TVO‑435, 6‑cylinder, vertical direct drive, horizontally opposed, turbocharged engine. The turbocharger increases the density of the carburettor inlet air to maintain the available power as altitude increases.
During operation, the exhaust gases expelled from the 3 cylinders on either side of the engine are merged into a single pipe, through which the gases are diverted either to the turbocharger or to the exhaust bypass valve (waste gate), or both (Figure 5).
As the engine power is increased, oil pressure builds up in the exhaust bypass valve assembly and the waste gate in the exhaust system is closed. This diverts the exhaust gas to the turbocharger turbine wheel, compressing the intake air and increasing the available engine power output.
Figure 5: Schematic diagram of engine and turbocharger operation
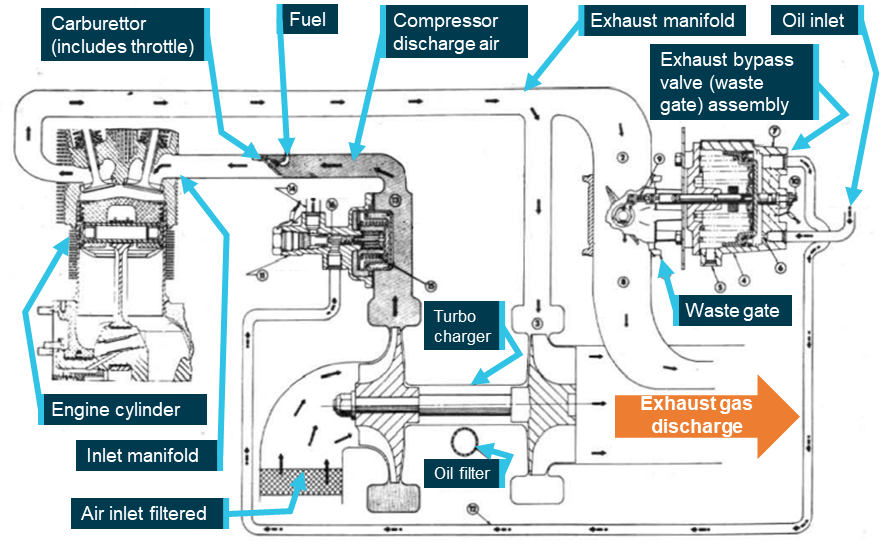
Source: Lycoming Operator’s Manual, annotated by the ATSB
Maintenance history
As part of the investigation, the ATSB requested the maintenance logs and component log cards for the aircraft. Although the provided information was incomplete, the maintenance history was able to be inferred from the supplied documents as follows:
- Lycoming engine TVO‑435, S/N: L‑751‑52 was installed February 2000 at 6,752 airframe hours. The engine component control card showed a number of zero‑hour components at the time of engine installation, indicating that this engine was likely either a new or overhauled unit. Lycoming Service Instruction No. 1009BE specified a 12‑year, 1,000 hour time between overhauls (TBO). This interval was correctly annotated in the engine log card.
- The engine was removed on 24 February 2014 (+14 years) at 7,088 airframe hours (+336 engine hours), and was bulk stripped in lieu of being overhauled, to satisfy the requirements of CASA air worthiness bulletin (AWB) 85‑5 Issue 1.[7] The same engine was refitted on 20 March 2014.
The information supplied to the ATSB showed that prior to November 2022, the aircraft flew only limited hours, having recorded 425 airframe hours in 22 years (at an average of 19.3 hours/year). Depending on how these hours were flown, the aircraft may have required special maintenance actions and/or storage procedures. If these actions were not taken, corrosion, or contamination of components may affect serviceability. No record of storage or preservation penalty maintenance was identified in the provided records.
Autorotation
When an engine failure occurs in a single‑engine helicopter such as the Kawasaki 47GB3‑KH4, the pilot must immediately lower the collective and enter autorotation to reduce rotor drag sufficiently to maintain normal rotor RPM. This is a power‑off manoeuvre wherein the engine is disengaged from the main rotor and the rotor blades are driven solely by the upward flow of air through the rotor during descent. The most common reasons for an autorotation are an engine or drive system failure. If the engine fails, the freewheeling unit[8] automatically disengages the engine from the main rotor, allowing it to rotate freely. The tail rotor, still driven by the main rotor transmission, continues to provide yaw control via the anti‑torque pedals.
The United States Federal Aviation Administration Helicopter Flying Handbook noted that the rate of descent during autorotation is influenced by various factors, including:
- bank angle
- density altitude
- gross weight
- main rotor RPM
- trim condition
- airspeed.
Pilots control the autorotative descent rate using airspeed and main rotor RPM. Airspeed is managed with the cyclic[9] pitch control, similar to normal powered flight. The descent angle can range from vertical to a minimum angle for maximum horizontal range. The rate of descent is highest at zero airspeed, reaches its minimum at approximately 50–60 kts (depending on the helicopter and conditions), and increases again at higher speeds.
During an autorotative landing, the kinetic energy associated with the helicopter’s airspeed and rotating main rotor blades are used to arrest the descent and cushion the landing. Termination of the autorotation usually involves initially flaring the helicopter to reduce the airspeed, rate of descent and, if necessary, increase the rotor RPM. The degree of flare effect is influenced by both the airspeed at the time aft cyclic is applied, as well as the rate of cyclic application.
Autorotative terminations at very low airspeeds are more challenging than those performed at the minimum rate of descent airspeed as they offer minimal flare effect. In that case, cushioning the landing using the stored rotor energy requires more precise collective application.
The Kawasaki 47G3B-KH4 flight manual stated that, in the case of an engine failure, the pilot must:
execute a normal autorotative descent and establish a level attitude prior to ground contact. At a height of approximately 10 feet above the ground, apply collective pitch in sufficient quantity to stop descent as ground contact is made. The best descent speed is 55 mph [48 kt].
Meteorological information
At the time of incident, visibility was in excess of 10 km, with scattered cloud[10] well above the aircraft operating height, no precipitation and an east‑south‑easterly wind at 11 kt.
The meteorological conditions reported by the pilot at the time of incident were consistent with the Bureau of Meteorology observations, which recorded a temperature of 36°C and dew point[11] of 11°C at the incident location.
The process of vaporising fuel in a carburetted engine can cool the airflow sufficiently to permit ice formation in the carburettor throat that restricts airflow to the engine. According to the Civil Aviation Safety Authority Carburettor icing probability chart, the probability of carburettor icing, based on the prevalent temperature and dewpoint at Katherine Gorge was on the outer limit of the ‘light icing – cruise or descent power’ zone. Of note however, the turbocharger compressor used in the Kawasaki 47G3B‑KH4 heats the inlet air to the carburettor, significantly reducing the potential for carburettor icing.
Operating weight
The passenger manifest completed by the pilot prior to take‑off recorded the empty weight of the aircraft, the pilot and both passengers, plus fuel. An allowance of 100 kg was made for the weight of fuel. The passenger weights were only verbally requested, and not physically checked by the pilot. However, the calculated total take‑off weight was well below the maximum take‑off weight so any inaccuracy in passenger weights was unlikely to have resulted in the aircraft being overloaded.
Aircraft fuel
The operator conducted an examination of the fuel in the aircraft following the incident and reported to the ATSB that there was adequate fuel remaining in the tank.
The operator also stated that the aircraft had been refuelled with premium 130 octane fuel by the pilot prior to take‑off, and that a post‑incident examination of the fuel quality did not reveal any signs of contamination or leakage.
Engine examination
Following the incident, the operator started the Lycoming TVO‑435 engine and observed that the wastegate did not operate. Thereafter, they removed the engine and delivered it to a third party maintenance facility for examination. As depicted in Figure 6, the post‑incident inspection of the engine revealed the presence of an approximately 6.5 cm crack on the right exhaust collector, with no other defects identified.
The exhaust system of the aircraft engine attains extremely high operating temperatures. The consequent widening of the crack due to heat expansion would result in the escape of exhaust gases from the defective section, resulting in inadequate drive pressure for the turbocharger compressor and reduced power output. Information provided by the engine manufacturer supported that conclusion. As such, exhaust gas bleed from the crack before the turbocharger resulted in the wastegate remaining closed.
The ATSB did not undertake a metallurgical analysis of the exhaust pipe, however, exhaust systems are generally prone to metal fatigue over time due to continuous vibration under corrosive conditions and a cyclical pattern of constant heating and cooling with extreme thermal fluctuations.[12]
While it could not be established when the exhaust crack occurred, the maintenance facility that conducted the post‑accident engine examination assessed that, based on the location and appearance of the defect, it was likely not impact‑related. They further stated that, as the helicopter did not have an engine cowl, the leaking exhaust gases would not have left a residue. This would have made the crack more difficult to detect during a pre‑flight inspection when the engine was cold.
Figure 6: Cracked exhaust collector pipe
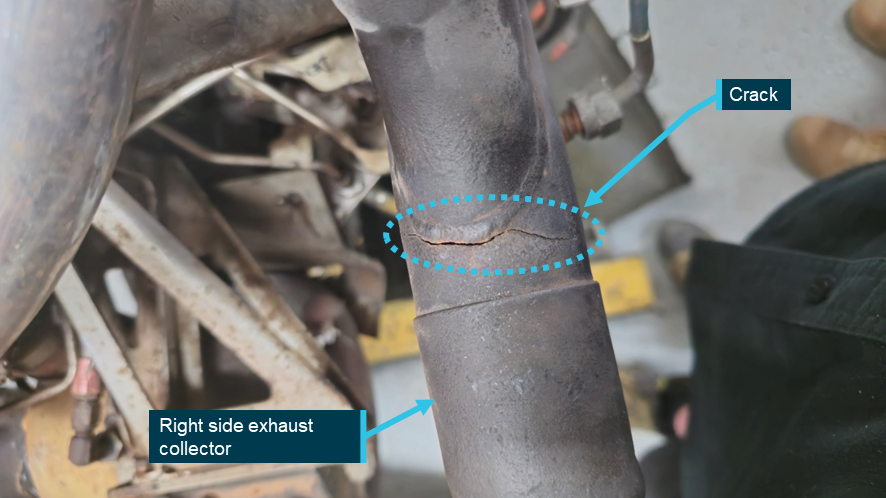
Source: the maintenance facility that conducted the engine strip down inspection, annotated by the ATSB
Safety analysis
Engine power reduction
The sequence of events described by the pilot and passengers were consistent with a loss of aircraft engine power during flight, necessitating an emergency landing. The ATSB considered the following potential reasons for the reduction in engine power:
- weather conditions, including carburettor icing
- fuel contamination or starvation
- handling‑related issues
- engine and/or associated systems defect.
The evidence gathered by the ATSB during the investigation indicated that the 3 initial possibilities were unlikely.
However, based on information from the engine manufacturer and the personnel that conducted the post‑accident engine examination, a pre‑existing crack in the exhaust collector likely reduced the engine power output during the flight.
Helicopter maintenance
The ATSB identified that low utilisation of the helicopter may have required special maintenance actions and/or storage procedures to be undertaken to prevent component corrosion or contamination. While there was no evidence that such maintenance was undertaken, it was not possible to determine whether its absence contributed to the crack in the exhaust system.
Autorotation
Analysis of flight data identified that the helicopter was over inhospitable terrain at the time of the power loss. After turning towards a suitable landing site, the pilot commenced an autorotation to that location. The helicopter proceeded downwind, initially attaining a maximum airspeed of about 70 kt. The airspeed was then reduced to close to the target minimum rate of descent airspeed of 48 kt, providing good potential flare effect to both slow the helicopter prior to touchdown and increase the rotor RPM if necessary.
Despite that, the pilot reported there was minimal flare effect when they approached the landing site, likely due to low rotor RPM. As a result, the pilot was unable to prevent the helicopter colliding with terrain during the termination. Importantly however, none of the occupants were injured.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain involving Kawasaki 47G, VH‑BEU, 24 km north of Katherine Tindal Airport, Northern Territory on 11 September 2024.
Contributing factors
- The right exhaust collector was found to have developed a significant crack, which likely resulted in engine power loss during flight.
- The pilot was unable to cushion the landing during termination of the autorotation, likely due to low rotor RPM, resulting in the helicopter colliding with terrain.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the pilot and passengers of the accident flight
- the operator
- the maintainer for VH-BEU
- Civil Aviation Safety Authority
- accident witness
- OzRunways data from the pilot’s iPad
- Bureau of Meteorology
- Kawasaki Heavy Industries
- the maintenance facility that conducted the post‑accident engine examination.
References
Lycoming Service Instruction No. 1009BE (2020).
Reciprocating engine and exhaust vibration and temperature levels in general aviation aircraft, U.S. Department of Transportation Federal Aviation Administration (1968).
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the pilot of the accident flight
- the operator
- the maintainer for VH‑BEU
- Civil Aviation Safety Authority
- Kawasaki Heavy Industries
- Textron Lycoming
- United States National Transportation Safety Board
- Japan Transport Safety Bureau
Submissions were received from:
- the pilot of the accident flight
- the operator
- Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
[1] The flat pitch is the power it takes to run the helicopter at 100% rotor RPM on the ground with the collective lever fully lowered. A helicopter flat pitch check is performed pre‑flight to identify any engine performance trends by monitoring manifold pressure.
[2] Flying neighbourly is a concept aimed at minimising the noise impact of helicopter operations on local communities.
[3] Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[4] The term used to describe the position of the 2 needles on the combined engine/rotor tachometer when the 2 needles are not superimposed. When a helicopter enters autorotation, either due to an engine failure or during practice, the needles split as the rotor system drive disengages from the engine. This indicates that the main rotor is no longer being powered by the engine and is instead being driven by the upward airflow through the rotor disc.
[5] MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[6] ICUS (In Command Under Supervision) operations enable pilots having the relevant aircraft type endorsement to gain command experience and accumulate flight hours when performing pilot‑in‑command duties under supervision.
[7] The AWB provided guidance on engine bulk strip for the purpose of extending calendar life, in instances where engine calendar life limit was reached before reaching the hourly TBO.
[8] The freewheeling unit is a mechanism that automatically disengages the engine from the main rotor when engine RPM falls below rotor RPM, allowing continued rotor rotation during autorotation.
[9] Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[10] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – scattered indicates cloud covering between a quarter and a half of the sky.
[11] Dewpoint: the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to predict the probability of aircraft carburettor icing or the likelihood of fog.
[12] US Department of Transport FAA Report No. NA‑68‑27.