Safety summary
What happened
At about 1615 on 30 October 2013, Pacific National standard-gauge freight train 3XW4 derailed at Newport, in Melbourne. The train derailed one bogie on a curve between two turnouts resulting in track damage to the mainline and an adjacent siding. There were no injuries.
What the ATSB found
The ATSB found that the track had a significant wide-gauge defect at the point of derailment. The defect had been present for more than 12 months and was at a level that exceeded the network standard. During the passage of the train, the track gauge widened further and a wheel on the inside of the curve dropped inside the rail.
The section of track was being managed by the Australian Rail Track Corporation (ARTC). The wide-gauge defect had been detected by the track geometry recording vehicle several times, although the location designated to the defect was about 58 m from its actual location. ARTC had subsequently and incorrectly attributed the wide gauge readings as being associated with the transition area in a nearby dual-gauge turnout.
The track was also subject to weekly patrols by ARTC, many conducted on foot. However, these inspections did not recognise the critical level of the wide-gauge at the derailment location and the defect remained in the track.
The ATSB also found that Pacific National freight train 3XW4 had derailed at the same location about seven weeks prior. Following that incident, ARTC did not identify the need for priority remedial works at the location and the defect remained.
What's been done as a result
Since the derailment, ARTC has introduced several measures that address identified safety issues, including:
- The development of an enhanced GPS-based defect locating system on its track geometry recording vehicle (AK Car), due for full implementation by mid-2016
- Supplementary training and audit of maintenance staff
- The introduction of a more structured Asset Management Policy and Asset Management Plan.
The ATSB has issued a recommendation to ARTC to take safety action to enhance the effectiveness of its response to a derailment event to prevent a similar incident.
Safety message
Network managers should ensure that track geometry recording machinery accurately identifies the location of track defects. Track patrols should also be vigilant in their monitoring of track conditions against network criteria.
Following a rail incident, involved parties should prioritise the identification and rectification of safety factors, including local conditions such as track defects.
Pacific National freight train 3XW4 departed Adelaide, South Australia on 29 October 2013. Its destination was Port Kembla in New South Wales via Melbourne. The train consisted of two locomotives and 29 wagons loaded with steel.
On the afternoon of 30 October, the train was passing through Newport, an inner western suburb of Melbourne. It was travelling at a speed of about 25 km/h, having slowed for a temporary speed restriction commencing just south of Newport Railway Station. At about 1615[1], on a tight left-hand curve between two turnouts, the leading bogie of the 21st wagon derailed.
The leading left-hand wheel of the lead bogie had fallen inside the common[2] rail of the dual-gauge track. On reaching the next turnout, the wheel struck the toe of the common rail point blade. The train travelled about 100 m with the bogie derailed, causing damage to the mainline track and an adjacent siding (Figure 1).
Figure 1: Derailed wagon RKOX 4072D and track damage to adjacent siding

Source: Chief Investigator, Transport Safety (Vic)
The locomotives were in power notch 2 and the train was running at about 22 km/h when the brake pipe pressure dropped as a consequence of the train parting at the leading end of the derailed wagon. After parting, the forward part of the train travelled a short distance before coming to a stand. There were no injuries.
__________
Infrastructure
Track layout
The track was part of the Defined Interstate Rail Network (DIRN) managed by the Australian Rail Track Corporation (ARTC). This section of track serviced standard- and broad-gauge freight traffic and standard-gauge Melbourne-Adelaide passenger services. The section had a line speed of 40 km/h for all trains. ARTC advised that, following the derailment on 11 September, the 25 km/h speed restriction[3] to the south of Newport had been extended to encompass the derailment location although this restriction was not reflected in published train notices.
The train was travelling on dual-gauge track and being routed from the inter/intrastate goods line through 602 and 601 turnouts towards Brooklyn. The derailment occurred between these turnouts (Figure 2).
Figure 2: Track layout, shown after restoration works

Source: Pass Assets (Vic Gov) annotated by Chief Investigator, Transport Safety (Vic)
The rail distance on the DIRN through this location was measured from a reference point located about 0.5 km to the south. At this point there was a change in the track kilometre location and a change in the direction of counting the km distance. From this reference point travelling south, the kilometre location increased from a starting point of 10.700 km. In the opposite direction towards the derailment location, the kilometre distance also increased, starting from 10.484 km.
From this10.484 km starting point, the 11 km kilometre post was located between turnouts 602 and 601 and the 12 km post was located beyond turnout 601 heading towards Brooklyn. The actual distance between the 11 and 12 km posts was 1058 m. ‘Long kilometres’ of this nature are a legacy of the network and are not uncommon.
Maintenance Responsibilities
As the accredited track manager, ARTC was responsible for track maintenance at the derailment location. From 1 January 2013 the maintenance activities were performed directly by ARTC. Prior to this, the maintenance task was contracted to Downer EDI Works.
Recent project works in area
In 2012 and prior to the end of their contract with ARTC, Downer EDI Works undertook upgrade works in the area. Turnout 602 was upgraded in November 2012 and turnout 601 upgraded in December 2012. Track within the upgraded turnouts consisted of 50 kg/m rail supported on concrete bearers and fastened using resilient clips.
The track between the two turnouts was not upgraded. Intermittent concrete sleepers had at some point been installed at the location to supplement the timber sleepers.
Derailment site information
Track detail and condition
The track between turnouts 602 and 601 had a radius of about 200 m at the point of derailment (Figure 3). There was a mix of concrete and timber sleepers (Figure 4) and the standard-gauge rail was heavily worn.
Figure 3: The approach to the left hand curve and the point of derailment

Source: Chief Investigator, Transport Safety (Vic)
Figure 4: Track construction at point of derailment

Source: Chief Investigator, Transport Safety (Vic)
At timber sleepers, rail was supported on double shouldered sleeper plates and fastened by dog spikes and screw spikes. Several dog spikes and screws were loose and ‘working’.
At concrete sleepers, a mix of resilient fastening types were used. There was a history of damaged fixings and dislodged rail spacers through the location.
Point of derailment
The point of derailment (PoD) was about 11 m before the toe of the 601 points blade. The leading left-hand wheel of wagon RKOX 4072D had dropped inside the common rail leaving a mark on the gauge face of the rail (Figure 5). The PoD was on 50 kg/m rail, just past a transition from 47 kg/m rail.
Figure 5: Point of derailment where a wheel had dropped inside the common rail
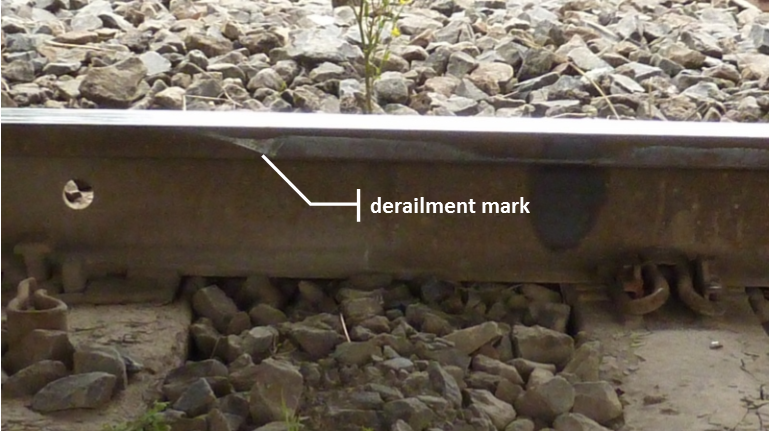
Source: Chief Investigator, Transport Safety (Vic)
Around the PoD, the ballast was fouled and the track had been pumping (Figure 6).
Figure 6: Track pumping at location of derailment

Source: Chief Investigator, Transport Safety (Vic)
The measured unloaded track gauge at the point of derailment was 1479 mm (cover photo). The maximum measured gauge just prior to the point of derailment was 1480 mm (Figure 7, ‘Gauge’), 45 mm in excess of design standard-gauge of 1435 mm. Through this location the rail on the outside of the curve was below the inside rail (Figure 7, ‘Cross level’).
Figure 7: Track measurements following derailment, noting that: (1) the point of derailment was between the two measures highlighted (2) the negative cross levels indicate that the outside rail was below the inside rail
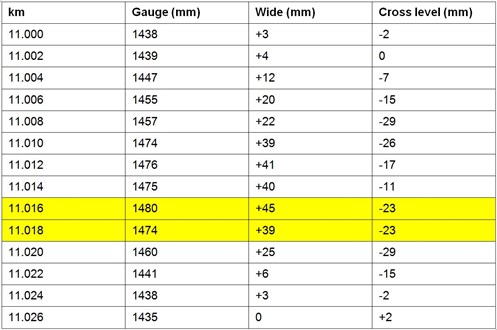
Source: ATRC
Beyond the point of derailment there were markings and fastener damage consistent with a derailed wheel travelling inside the common rail. The toe of the point blade at turnout 601 had been impacted by the wheel (Figure 8).
Figure 8: Impacted toe of the point blade at turnout 601

Source: ARTC
Track inspection regime
The ARTC inspection regime for this track included:
- Track geometry recording (4-monthly) by the track geometry recording vehicle
- Track patrol by road/rail vehicle or on-foot (at least every seven days).
Inspections of the section were consistent with this regime, with track patrols often conducted on foot.
Track geometry recording vehicle (AK Car)
The track geometry recording vehicle (AK Car) was used to measure track geometry on the DIRN. The AK Car is fitted with measuring and processing equipment and, together with other support vehicles, is hauled by locomotive around the national rail network. Technical staff ride in the train to manage the measuring and recording operations of the AK Car. This role includes ensuring that local track staff are provided with real-time system output on track geometry.
The supervisor for each track section, or their representative, normally travelled in the train to manage the response to any identified defects. On detection of a geometric anomaly by the AK Car, the system would generate an Exception Report detailing the exceedance for the supervisor to consider in real-time.
For identified geometric defects requiring an immediate response, an in-field inspector would be contacted and directed to the defect for inspection and assessment. The inspector would be provided with an approximate kilometre location to guide them to the area of the defect. An assessment of the track would be made by the track inspector and steps then taken to address confirmed defects.
Wide-gauge criteria
An ARTC network code of practice[4] specified permitted deviation from the design track geometry. Geometric limits were specified for the track under loaded conditions.
The code specified that for a wide-gauge defect of above 38 mm, an E1 response was required for all track speeds. An E1 (Emergency) response was defined as inspection prior to the next train, repair prior to the next train and if repair was not possible, passage under the control of a pilot. Assessment of the defect by a competent worker was required to determine if the train could be piloted.
For a wide-gauge of 35-38 mm on 40 km/h track, an E2 response category was specified. An E2 response was defined as inspection within two hours or prior to the next train (whichever was greater) and repair within 24 hours. Again, there were conditions allowing for trains to pass if the defect could not be repaired within the designated timeframe.
For wide-gauge defects below 35 mm, and with decreasing defect magnitude, there were a series of defect bands with responses of decreasing urgency.
Rail wear
The track recording car also recorded rail head wear. This data was generally not assessed in real time, but instead used by ARTC for longer term planning including the programming of re-railing works. A number of parameters were measured including head wear loss, and side (gauge face) wear.
An ARTC network code of practice[5] specified rail wear limits, above which certain actions were required. For 47 kg/m rail, the lighter of the rails used through this section, the code specified the following key limits applicable in this instance:
- A loss of cross-sectional head area limit of 32 per cent, above which risk controls including monitoring were required
- A condemning limit of 15 mm loss of head width, above which the rail should be replaced or train speed restricted.
Alignment of AK Car data with in-field track and infrastructure
GPS and Manual modes
In normal operation, the AK Car used GPS to track its location. ARTC advised that in this mode system accuracy was +/- 5m, with limited events +/- 20m. However, the GPS mode could not be used when:
- GPS services were unavailable, such as in tunnels and urban canyons
- There was a change in direction of the kilometre count (increasing/decreasing)
- There was a change in the reference kilometre location (a discontinuity).
When GPS could not be used, the AK Car was switched to Manual mode, and GPS disabled. In this Manual mode, the system used an ‘Auto-run’ database that would:
- Start/stop the trackcode recording
- Change trackcode, from one track section to the next
- Swap the orientation of the kilometre counting direction
- Change the kilometre reference distance at a particular location.
Mode of operation through Newport
Between Newport and Brooklyn, the AK Car was operated in Manual mode because of changes to the kilometre location and counting direction, including the change just south of Newport.
Location of track features
Track features such as turnouts were marked on various geometry measurement reports including track geometry charts. This track information was drawn from an Event database that had been populated over time by AK Car operators identifying features as they were passed. There was also a process to update the database when errors in location were identified.
Train information
Crew
The train was operated by a crew of two. Both crew members held the qualifications required for operating over this section of the ARTC network and all medicals were current.
The operation of the train was consistent with the network requirements and train handling was not considered contributory to the derailment.
Consist and loading
The wagon weights were consistent (no empty wagons) throughout the train with a maximum recorded wagon mass of 80.4 t. The Train Inspection Certificate issued at Adelaide indicated that the loading and its securement was consistent with the Pacific National and network loading requirements and that the wagons were mechanically fit for the journey.
Derailed wagon RKOX 4072D, had a length of 23.8 metres and a tare weight of 27 t. Based on the loading records, it had a payload of 49 t of structural steel beams giving it a mass of 76 t, equating to an axle load of about 19 t. The load profile was consistent with Pacific National’s loading diagram for this product and wagon type.
Bogie and wheels
The wheelset dimensions that are critical to ensure compatibility with track gauge are rim width, flange thickness and wheelset back-to-back distance (Figure 9).
Figure 9: Definition of wheelset and wheel rim dimensions
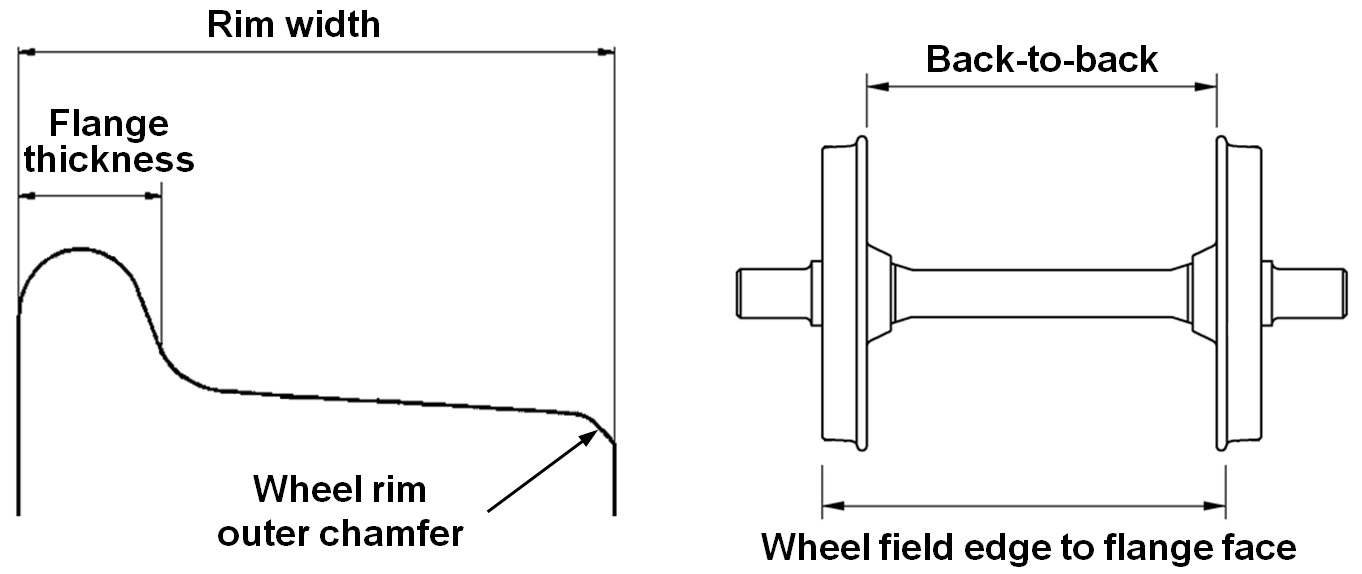
Source: ATSB
The Australian Standard[6] for railway rolling stock specified wheel rim width requirements. For the ARTC network, the standard specified a permitted rim width of 127-140 mm for axle loads of less than 25 t.
There was a range of freight rolling stock operating in Australia, and wheels generally fell into two categories, a narrower rim width within 127-130 mm, or the more common width of 138-140 mm. Both were accepted for operation on the ARTC network.
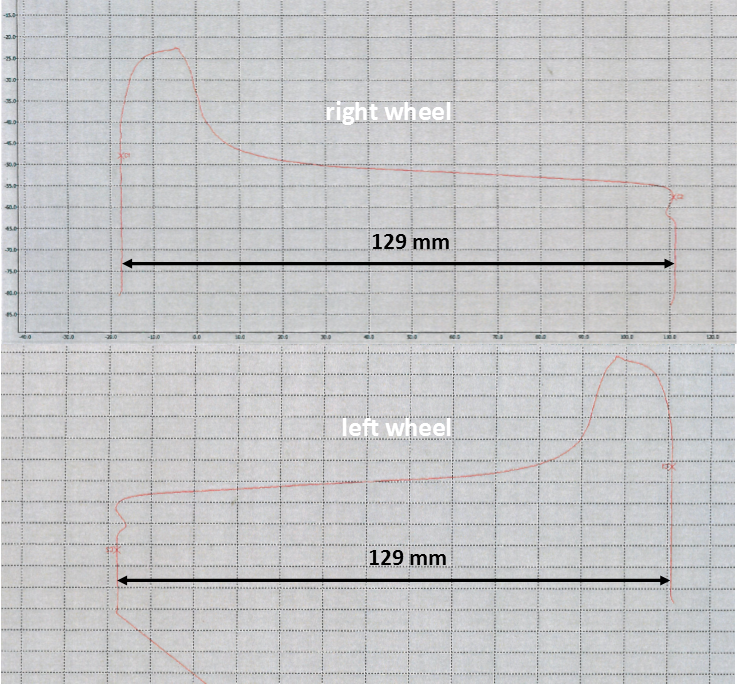
The leading wheelset of the derailed bogie was fitted with the narrower wheel type, with both wheels having a measured rim width of about 129 mm (Figure 10). Inspection of these wheels using the rolling stock operator’s field gauge found that they were more worn than others on the wagon, but that flange thickness and wheel profile met requirements. Flange thickness exceeded the operator’s permitted minimum of 19 mm.
Figure 10: Leading axle wheel profiles, right wheel (top) and left wheel (below)
Source: Pacific National
Standards[7] specify a wheelset back-to-back dimension of 1357-1359 mm for standard gauge rolling stock. A back-to-back dimension of less than 1357 mm would result in wheelsets being more prone to drop-in derailment on track with wide-gauge. In this instance, all wheelsets on the derailed wagon exceeded this minimum.
General inspection of the derailed bogie and wheels did not identify any pre-existing defect or adverse condition that may have contributed to the derailment.
Similar occurrences
About seven weeks earlier on 11 September 2013, train 3XW4 derailed two wagons at the same location while travelling in the same direction. The ATSB did not investigate the derailment, and information on the circumstances of the event were collected after the 30 October derailment.
The train was operated by Pacific National and consisted of two locomotives hauling 19 wagons loaded with steel products. Investigations conducted by Pacific National and consultants engaged by them concluded that the point of derailment (Figure 11) was between points 602 and 601.
Figure 11: Photograph from the 11 September 2013 derailment, showing marks on the rail gauge face consistent with a left hand wheel dropping inside the common rail
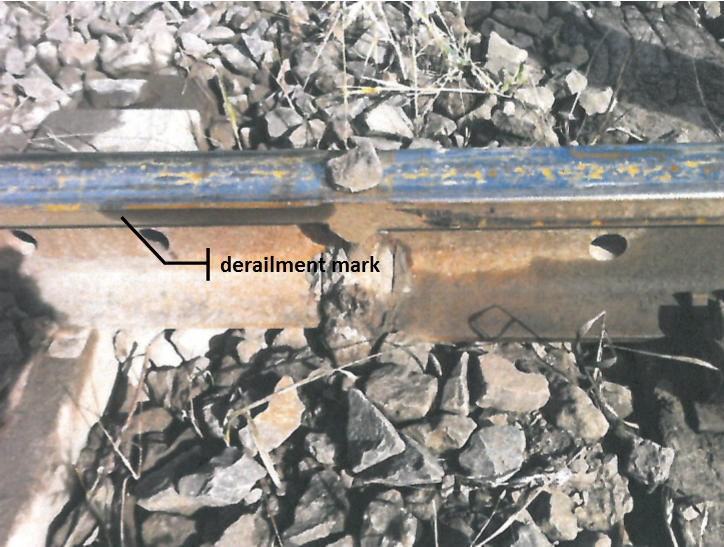
Source: Pacific National
The Pacific National report describes a wheel dropping inside the common rail on the inside of the curve before 601 points and just before a welded joint. There was also conjecture that the wheel on the outside of the curve may have climbed onto the standard-gauge rail. At the Point of Derailment, the measured static track gauge was 1477 mm (42 mm wide) and the track had a negative[8] cant of about 30 mm. Track engineering inspections indicated that spacers normally installed between the fastening shoulders on concrete sleepers, had become dislodged allowing the standard-gauge rail to move outwards, increasing the gauge. No rolling stock condition or loading condition was identified that may have contributed to the derailment.
The ATSB identified from photographic evidence that the point of wheel drop-in on 11 September was about 0.6 m before (to the south of) the point of derailment seven weeks later, on 30 October. In addition, inspection of the bogie that probably derailed first found that the wheels on that bogie were also of the 127-130 mm type.
Post-derailment works
ARTC advised that works undertaken following the 11 September derailment included:
- Replacement of sleeper pads on concrete sleepers
- Cross boring and re-spiking of 10 timber sleepers
- Realignment of track geometry with excavator tamping head.
However, AK Car measurement undertaken on 2 October 2013 confirmed that the wide-gauge defect remained after the post-derailment works.
__________
- The train was travelling at about this speed when it derailed.
- ARTC Engineering (Track & Civil) Code of Practice, Track Geometry.
- ARTC Engineering (Track & Civil) Code of Practice, Rail.
- AS 7514.2: 2010 Railway Rolling Stock - Wheels – Part 2: Freight Rolling Stock.
- At the time of reporting, the dimensional requirements were specified in Australian Standard AS7517: 2014 Wheelsets. The 1357 mm minimum requirement was unchanged from the previous standard applicable at the time of the derailment.
- The rail on the outside of the curve is lower than the inside rail.
Derailment mechanism
The left-hand wheel of the leading wheelset of wagon RKOX 4072D dropped inside the common rail. There was no identified evidence of flange climb onto the rail head opposite this point.
For the wheel to drop inside the rail, the ‘wheel field edge to flange face’ distance (Figure 9) must be less than track gauge. Post-derailment measurements indicated that for the narrow wheel type, the effective width of tread remaining on the common rail running surface at the point of derailment would have been about 20 mm in no load conditions. This assumes a reduction in effective width by the chamfer or rounding of the rim outer edge.
Additional spreading of the rails under the load of the rolling stock was required for the wheel to derail. The AK Car data points to spreading under load and combined with evidence of working fasteners at this location, the required spread could have been achieved.
Other aspects of the track geometry such as the negative cant and the slope of the standard-gauge rail gauge face are potential second order influences on the derailment.
Wide-gauge at point of derailment
Evidence supporting wide-gauge defect at point of derailment
During 2012 and 2013, the track geometry recording vehicle (AK Car) consistently identified wide-gauge around the 10.96 km mark. On each occasion, the exceedance was closed out on the basis that the flagged wide-gauge related to the transition zone within turnout 602. However, the following evidence supports the contention that the wide-gauge defect recorded by the AK Car around the 10.96 km mark, actually existed at the derailment location between 11.010 and 11.020 km:
- Post-incident measurement identified wide-gauge of up to 45 mm at the derailment location
- The magnitude and extent of the wide-gauge measured at site is consistent with the AK Car recording of wide gauge at 10.96 km
- A separate wide-gauge spike can be found for turnout 602
- There was no other wide gauge identified by the AK Car in the vicinity of the derailment
- There is a high level of correlation between the location of the recorded wide-gauge and rail wear that existed at the derailment location
- Following track repair, the wide-gauge defect was no longer identified by the AK Car.
- Each point is expanded below.
Post-incident site measurements
Post-incident measurement found that the track gauge at the derailment location was wide. The static gauge was 20 mm wide about 10 m ahead of the point of derailment and about 40 mm wide 4-6 m ahead. The wide-gauge peaked at about 45 mm just prior to the identified point of derailment. Beyond the point of derailment, gauge returned to within specified limits prior to turnout 601.
Magnitude and extent of wide-gauge
The magnitude and extent of the wide-gauge measured around the point of derailment following the incident was consistent with the AK Car record of wide-gauge at or about the 10.96 km mark.
The AK Car measured wide-gauge of 50 mm recorded four weeks prior to the derailment was consistent with the no-load measurement of 45 mm at the derailment site. The +5 mm variation under loaded conditions is considered realistic for measurement by the AK Car that has a relatively low (about 12 t) axle load. Under heavier rolling stock, greater widening would be expected.
The AK Car recorded ‘extent’ of wide-gauge was also comparable with that measured on site at the derailment location. In both the AK Car record (Figure 12) and site measurements (Figure 7), a wide-gauge of over 20 mm extended for around 15 m.
Wide-gauge spike identified for turnout 602
There was conjecture that the wide-gauge defect identified by the AK Car may have been the result of wide-gauge that existed at a transition zone within turnout 602. This transition zone was around three metres in length, and a spike can be identified with the AK Car record (Figure 12) that is consistent with this short length of wide-gauge. On the AK Car chart, this spike is about 50 m before the point of derailment. This distance was verified as being consistent with the in-field measurements.
No other wide-gauge recorded around derailment location
The AK Car did not record wide-gauge around 11.010-11.020 km (Figure 12) even though there was clear physical evidence that wide-gauge existed through this location. This indicated that there was an offset of 50-60 m between the AK Car recorded location and the actual km location.
Figure 12: Extract of AK Car chart from 2 October 2013 measurement showing: wide-gauge magnitude and extent consistent with that at the derailment site a wide-gauge spike consistent with transition zone at turnout 602 no significant wide-gauge recorded between 11-010-11.020 km
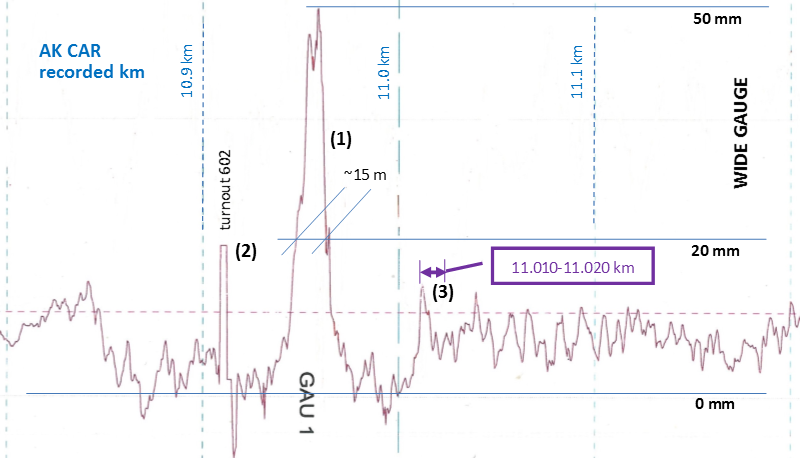
Source: AK Car chart annotated by Chief Investigator, Transport Safety (Vic)
Correlation between recordings of wide-gauge and rail wear
There was good correlation between the location of the wide-gauge and wear of the right hand rail head (Figure 13). Both the location and length of the wide-gauge was similar to that of the rail head wear that existed at and around the point of derailment.
Figure 13: AK Car data from 2013 showing correlation between location of wide-gauge and right hand rail wear. (*Note: For 6 Feb 2013, the AK Car recorded location was about 20-25 m different to other recordings through 2012-2013.)
| Date | Measure | From (km) | To (km) | Max value | Max at (km) |
| 6-Feb-13* | Wide-gauge | 10.986 | 10.977 | 43 mm | 10.985 |
| 6-Feb-13* | Rail wear | 10.987 | 10.977 | 33% | 10.987 |
| 5-Jun-13 | Wide-gauge | 10.968 | 10.959 | 48 mm | 10.962 |
| 5-Jun-13 | Rail wear | 10.971 | 10.957 | 39 % | 10.971 |
| 2-Oct-13 | Wide-gauge | 10.963 | 10.952 | 50 mm | 10.960 |
| 2-Oct-13 | Rail wear | 10.962 | 10.948 | 40 % | 10.962 |
Source: AK Car data extracted by Chief Investigator, Transport Safety (Vic)
Absence of wide-gauge defect following track repair
Once the track between 602 and 601 turnouts was renewed, the wide-gauge E fault and severe rail wear were no longer identified by the track geometry recording vehicle through the location. Comparison of charts shows that a wide-gauge peak is no longer present (Figure 14).
Figure 14: Extract of AK Car charts of track gauge on similar vertical and horizontal scales from: 2 October 2013 (top) before repair to track between turnouts 602 and 601, 11 June 2015 (below)
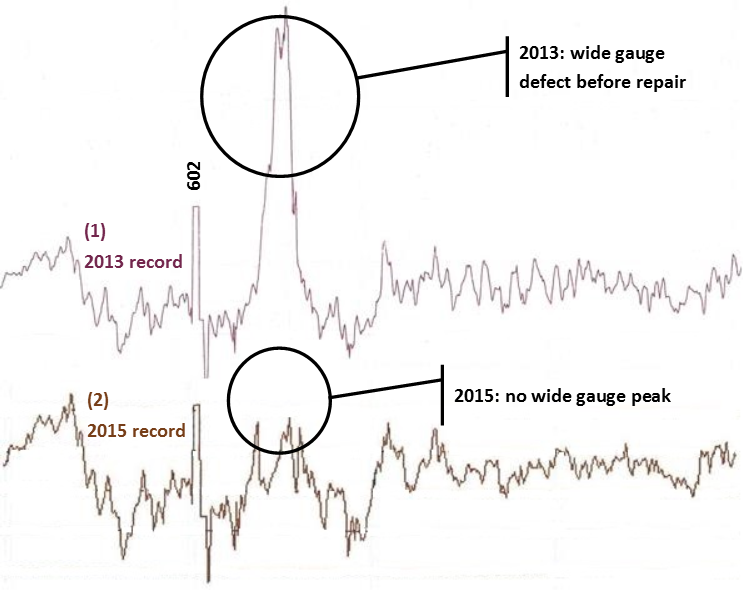
Source: AK Car chart comparison by Chief Investigator, Transport Safety (Vic)
Wide-gauge assessment against defect criterion
The network code specified a 38 mm wide-gauge limit under loaded conditions, above which an E1 (Emergency) response was required. This criterion was exceeded for both the static (no load) and loaded conditions.
No load condition
Given the measured trend in gauge on the approach to the point of derailment, and the low level of track disturbance, it is probable that the static gauge prior to the derailment was similar to that measured post-derailment. The measured track gauge of 45 mm wide exceeded the 38 mm criteria to initiate the E1 (Emergency) response specified within the network standard.
Loaded condition
The six AK Car track recordings prior to the derailment were examined. In all recordings, wide-gauge was identified by the track geometry recording vehicle for this track section. The wide-gauge exceeded the E1 limit for at least a year prior to the derailment and was trending upward (Figure 15). The track gauge was 50 mm wide when last measured by the track geometry recording vehicle on 2 October 2013, and so exceeded the 38 mm criterion.
Figure 15: Trend in measured gauge shown against E1 and E2 limits
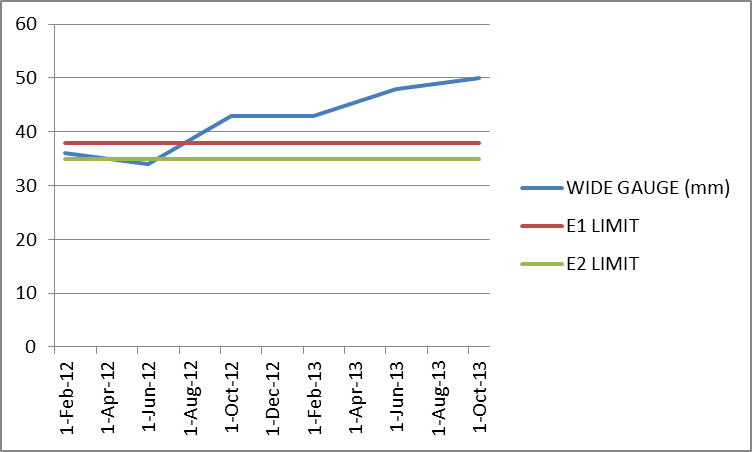
Source: Chief Investigator, Transport Safety (Vic)
Conclusion
It is concluded that a wide-gauge defect existed at the location of the derailment between turnouts 602 and 601. The magnitude of the defect was slowly increasing and had been at a level requiring an emergency response for more than 12 months.
There were a number of opportunities to identify the presence of the wide gauge between turnouts 602 and 601 prior to the 30 October derailment. Each of the following is discussed in further detail:
- AK Car track geometry recording and assessment of data
- Track patrol inspections
- The previous derailment on 11 September.
AK Car track geometry recording and assessment of data
Defect location offset
The AK Car track geometry measurements taken during 2012 and 2013 identified wide-gauge in the vicinity of turnout 602. This wide gauge actually existed between turnouts 602 and 601 about 58 m to the north of the recorded location. This offset was the result of a ‘long kilometre’ of 1058 m between the 12 and 11 km posts and the methods used by the AK Car system to identify location when the Car was being operated in Manual mode.
When operating in Manual mode, an AK Car operator, who would be located in the vehicle above the geometry measuring equipment, synchronised the location of the AK Car at each kilometre post. Until the operator synchronised at the next post or a subsequent post, the AK Car systems assumed a distance of 1000 m between each post.
Between Brooklyn and Newport, the AK Car always travelled from the 12 km post towards the 11 km. As this wide-gauge defect was just before the 11 km post, and assuming the AK Car was synchronised at the 12 km post, the defect was recorded as being around 1040 m past the 12 km post, or assuming a distance of 1000 m between the 12 km and 11 km, at a location of 11 km minus 40 m, at 10.960 km. This would occur irrespective of whether the AK Car was synchronised at the 11 km post, although if synchronised there, an anomaly indicator in the form of a ‘?’ would appear on an Exception Report for any identified defect.
Of the six AK Car recordings examined, in all but one instance the recording was not manually synchronised at the 11 km post. The Newport area is complex and observation from the AK Car confirmed that sighting of the 11 km post was difficult. In scenarios of possible confusion in sighting the km post, the AK Car operators prefer not to synchronise, as an error in manual synchronisation can introduce significant errors. Therefore, given the difficulties in sighting at this location and a potential focus on the upcoming change to kilometre counting at the 10.484 km point, it is not unexpected that the AK Car was typically not synchronised at the 11 km post. On the one occasion (February 2013) that the AK Car was synchronised at this post, the exception report annotated the location with a ‘?’, flagging a potential anomaly. There is no evidence that this annotation was questioned by track staff.
Interpretation of AK charts and exception reports
In five of the six AK Car exception reports for this location through 2012 and 2013, the wide-gauge was identified as having a ‘length’ of about 10 m. This was considerably longer than the transition zone of about 3 m in turnout 602. This difference provided an opportunity to identify the anomaly in the defect location.
Turnouts generated by the ‘Event database’ and identified on track geometry recordings were also offset from their actual location, potentially adding to the confusion.
Directing track inspectors to the location of a defect
Track inspectors reported that it was not uncommon to ‘search’ several tens of metres to locate a defect, increasing the likelihood of a defect not being correctly identified and assessed.
The technologies that were being used did not support the precise locating of a defect by track inspectors when the AK Car was in Manual mode and GPS coordinates were not available.
Track patrol inspections
This section of track was well known to the local track maintenance personnel. ARTC had been directly maintaining the section since January 2013 and most maintenance staff had also worked with the previous maintenance provider and so were familiar with the track.
While ARTC staff were generally aware of the presence of worn rail at the derailment location, there was an apparent over-reliance on the AK Car Exception Reports to trigger maintenance actions for geometric defects. There were regular patrols of this section of track that provided ample opportunity to identify the wide-gauge defect.
Gauge is defined as the rail-to-rail measurement taken 16 mm below the top surface of the rails and is normally measured by a track gauge. However, at least in some instances, gauge at this location was assessed by using the distance between the feet of the rails to estimate the gauge at the rail heads[9]. While this practice can provide an estimate of track gauge, it ignores the contribution of rail wear to gauge. This method would have estimated gauge as being 20-25 mm wide and so not requiring immediate remedial action.
Any measurements that were taken during patrols would also have been with the track in an unloaded condition. While static gauge already exceeded the network criteria, in addition it did not include the significant widening that occurred during the passage of a train as a result of the deteriorated track condition.
Actions following derailment on 11 September 2013
On 11 September 2013, seven weeks prior to the 30 October derailment, the same freight service derailed at the same location. It is probable that the mode of derailment was similar, with a wheel dropping inside the common rail due to wide-gauge.
Following the derailment on 11 September, both the network manager and the rolling stock operator initiated investigations, although neither investigation had been completed by the time of the second derailment. Nonetheless, there was sufficient information immediately available to the ARTC investigation to identify that wide-gauge was the probable cause of the derailment and that the section of track between turnouts 602 and 601 required remediation to remove the defect. However, the wide-gauge defect was not corrected and remained in track. The AK Car recording for 2 October 2013 confirms the continued presence of the defect.
Short-term post-derailment response includes both the initial investigative activity and the restoration of track. These activities are not mutually exclusive. A derailment is a significant event that should trigger the prompt identification of key causal factors (including track defects), that feeds into and supports appropriate track remediation. In this instance, the ARTC response to the derailment on 11 September 2013 was ineffective and did not prevent another derailment seven weeks later at the same location.
Rail head wear
Rail wear leads to a loss of rail strength and rail head shape. As a result the network specifies limits on rail wear. The 47 kg/m rail near the point of derailment was worn beyond the network limits (Figure 16). Specifically:
- Head loss was 39 per cent, exceeding the 32 per cent criterion that triggered risk controls
- Gauge face side wear was 23 mm, exceeding the 15 mm condemning limit.
In addition, the gauge face of the standard-gauge rail was worn to an angle of about 27 degrees, exceeding the network criterion of 26 degrees. While only just exceeding the limit, high gauge-face angles increase the potential for flange climb.
Figure 16: Rail head profile in heavily worn 47 kg/m rail, close to point of derailment
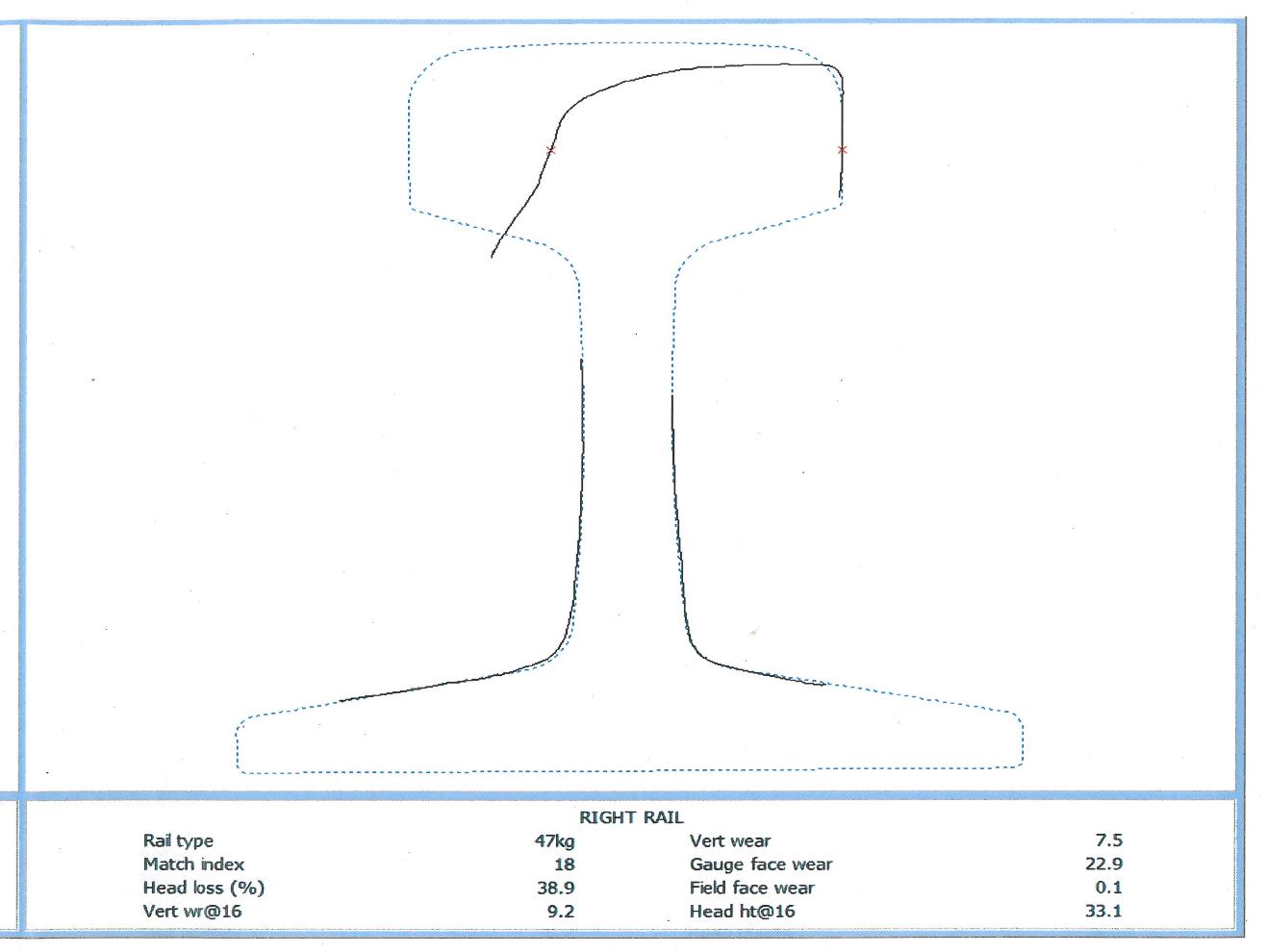
Source: ARTC
Interpretation of rail wear data
AK Car rail wear data was used for long term network planning including rail replacement works. ARTC records suggest that the rail wear flagged by the AK Car was probably not attended to because ARTC staff responsible for the long term monitoring of rail wear believed the wear was a feature of turnout 602, rather than being in plain track on the curve between turnouts 602 and 601. As with track gauge, the rail wear extended for more than 10 m and so was unlikely to be a feature of the turnout.
Locally, track staff were aware that the rail was heavily worn on this curve. However, this, local knowledge does not appear to have reached the ARTC team responsible for managing rail wear.
__________
The following findings are made with respect to the derailment of freight train 3XW4 at Newport, Victoria on 30 October 2013. These findings should not be read as apportioning blame or liability to any particular organisation or individual.
Safety issues, or system problems, are highlighted in bold to emphasise their importance. A safety issue is an event or condition that increases safety risk and (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time.
Contributing factors
- The track had a wide-gauge defect at the derailment location between turnouts 602 and 601 that exceeded the criterion for an E1 (Emergency) response. This allowed the left hand wheel of the leading wheelset of wagon RKOX 4072D to drop inside the common rail when the already wide-gauge widened further under the dynamic loading of the rolling stock.
- When the AK Car was operating in Manual mode, the methods used to identify the location of a defect and assist track staff to locate the defect could be ineffective in certain scenarios. At the derailment location, there was a consistent offset of about 58 m between the recorded location of the wide-gauge defect and its actual location due to the presence of a ‘long kilometre’. [Safety issue]
- Track patrol processes were ineffective at detecting and remedying the wide-gauge defect at the derailment location. Track patrols were overly reliant on the AK Car geometry recording vehicle to trigger maintenance action on this track geometry defect. [Safety issue]
- The ARTC response to the derailment on 11 September 2013 was ineffective and did not prevent a similar derailment at the same location on 30 October. [Safety issue]
- Despite several opportunities to identify and rectify the wide-gauge defect that existed between turnouts 602 and 601, remedial action was not taken to address the defect that was at an E1 (emergency) level for over 12 months.
Other factors that increased risk
- ARTC processes for managing the condition of the rail were ineffective despite repeated recording of rail head wear by the AK Car, and local knowledge of the worn rail. The rail was worn beyond the rail condemning limits specified within the network code of practice. [Safety issue]
Other findings
- The leading wheelset of the derailed wagon was fitted with 127-130 mm type wheels.
The safety issues identified during this investigation are listed in the Findings and Safety issues and actions sections of this report. The Australian Transport Safety Bureau (ATSB) expects that all safety issues identified by the investigation should be addressed by the relevant organisation(s). In addressing those issues, the ATSB prefers to encourage relevant organisation(s) to proactively initiate safety action, rather than to issue formal safety recommendations or safety advisory notices.
The directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation.
The initial public version of these safety issues and actions are repeated separately on the ATSB website to facilitate monitoring by interested parties. Where relevant the safety issues and actions will be updated on the ATSB website as information comes to hand.
Identification of defect location
When the AK Car was operating in Manual mode, the methods used to identify the location of a defect, and assist track staff to locate the defect could be ineffective in certain scenarios. At the derailment location, there was a consistent offset of about 58 m between the recorded location of the wide-gauge defect and its actual location due to the presence of a ‘long kilometre’.
Rail Safety Issue No: RO-2013-026-SI-01
Track patrols
Track patrol processes were ineffective at detecting and remedying the wide gauge defect at the derailment location. Track patrols were overly reliant on the AK Car geometry recording vehicle to trigger maintenance action on this track geometry defect.
Rail Safety Issue No: RO-2013-026-SI-02
Actions following derailment on 11 September 2013
The ARTC response to the derailment on 11 September 2013 was ineffective and did not prevent a similar derailment at the same location on 30 October.
Rail Safety Issue No: RO-2013-026-SI-03
Rail head wear
ARTC processes for managing the condition of the rail were ineffective despite repeated recording of rail head wear by the AK Car, and local knowledge of the worn rail. The rail was worn beyond the rail condemning limits specified within the network code of practice.
Rail Safety Issue No: RO-2013-026-SI-04
Sources of information
The sources of information during the investigation included the:
- Australian Rail Track Corporation
- Pacific National.
References
Australian Rail Track Corporation Engineering (Track & Civil) Code of Practice, Track Geometry
Australian Rail Track Corporation Engineering (Track & Civil) Code of Practice, Rail
Australian Standard AS 7514.2: 2010 Railway Rolling Stock – Wheels- Part 3: Freight Rolling Stock
Australian Standard AS 7517: 2014 Wheelsets
Submissions
Under Part 4, Division 2 (Investigation Reports), Section 26 of the Transport Safety Investigation Act 2003 (the Act), the Australian Transport Safety Bureau (ATSB) may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. Section 26 (1) (a) of the Act allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the Australian Rail Track Corporation, Downer, Pacific National, and the Office of the National Rail Safety Regulator and submissions received from those parties. The submissions were reviewed and where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2016
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |