Loss of control and collision with terrain involving Cessna 150L, VH-EYU, Bacchus Marsh aircraft landing area, Victoria, on 22 October 2024
Final report
Report release date: 10/07/2025
Investigation summary
What happened
On the morning of 22 October 2024, the pilot of a Cessna Aircraft Company 150L, registered VH‑EYU, was conducting a private flight from Bacchus Marsh aircraft landing area, Victoria. Strong and gusting winds were present. After commencing a take-off roll, the pilot rejected the take-off, before taxiing back to the same runway for a second take‑off.
On the second take-off, the aircraft became airborne and climbed to about 150 ft above the runway, before it pitched steeply nose-up, then the nose dropped suddenly, followed by the left wing dropping. The aircraft then entered a vertical descent, rotating approximately 270° before colliding with terrain. The pilot, who was the sole occupant of the aircraft, was fatally injured, and the aircraft was destroyed.
What the ATSB found
The ATSB found that shortly after take-off, in strong and gusty wind conditions, the aircraft stalled at a height too low to recover before colliding with terrain. It is probable that the aircraft was too slow on take-off into those conditions, and that inputs made to counteract the crosswind increased the angle of attack of the left wing. These factors, combined with the wind conditions, increased the risk of a quick and unrecoverable stall.
Safety message
While an aerodynamic stall can occur at any airspeed, at any altitude, and with any engine power setting, it is most hazardous during take-off and landing when the aircraft is close to the ground. When gusting conditions are present, pilots should consider waiting for more benign conditions. Guidance advises pilots to conduct their own testing in progressively higher winds to determine both their own capability and that of the aircraft.
Maintaining the aircraft’s attitude and correcting any change in attitude due to wind gusts during climb, is vital to ensure the critical angle of attack is not exceeded. Reducing the angle of attack by lowering the aircraft nose at the first indication of a stall is the most important immediate response for stall avoidance and recovery.
Pilots must understand and recognise the conditions which make stall more likely and the symptoms of an approaching stall so they can act to prevent a stall before an unrecoverable condition develops. If pilots judge the weather to be suitable, they should consider climbing out at a higher airspeed to provide a buffer above their aircraft’s stall speed for detection and correction of an impending stall.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the morning of 22 October 2024, at the Bacchus Marsh aircraft landing area (ALA), Victoria, a Cessna Aircraft Company 150L aircraft, registered VH‑EYU, was being prepared for a private flight under visual flight rules[1] to Lethbridge ALA, Victoria, about 35 km to the southwest. The weather conditions at the time were described as having strong, variable and gusty winds with a temperature of about 27°C.
Closed circuit television (CCTV) showed the pilot arriving for their flight at about 1000. Later, at about 1047, another CCTV camera located at a flying school, recorded the aircraft taxiing to the fuel bowser. After fuelling, the pilot drained a fuel sample from the aircraft fuel tanks and checked the sample. The pilot, who was the sole occupant, climbed in, then started the aircraft and taxied to a run‑up area[2] and performed engine run-up and flight control checks. They then taxied toward runway 27[3] for take‑off (Figure 1).
At about 1110 local time, a common traffic advisory frequency[4] (CTAF) recording captured the pilot stating that they were commencing their take‑off roll. Shortly after, the pilot transmitted another radio call stating that they were rejecting the take‑off. There was no further information provided by the pilot to explain why the take‑off was rejected.
The rejected take-off attracted the attention of witnesses who were now observing VH‑EYU. The pilot taxied the aircraft off the runway and returned to the end of runway 27. At 1114, the pilot commenced a second take‑off roll.
The witnesses included a flight instructor. They identified that the aircraft appeared unstable after take-off. The CCTV showed the right wing dipping twice during this take‑off, with the pilot levelling the aircraft each time. The flight instructor stated that at about 50 ft, the aircraft pitched up quickly, before the nose was pushed down again.
After the aircraft had passed the runway intersection and reached an altitude of about 150 ft, it pitched steeply upward, before the nose and then the left wing rapidly dropped. The aircraft entered a nose down vertical descent to the left, rotating approximately 270° before colliding heavily with terrain. After the collision, personnel from the flying school attended the accident site and found the pilot fatally injured. The aircraft was destroyed.
Figure 1: Bacchus Marsh ALA and VH‑EYU approximate flight path (yellow) and accident site
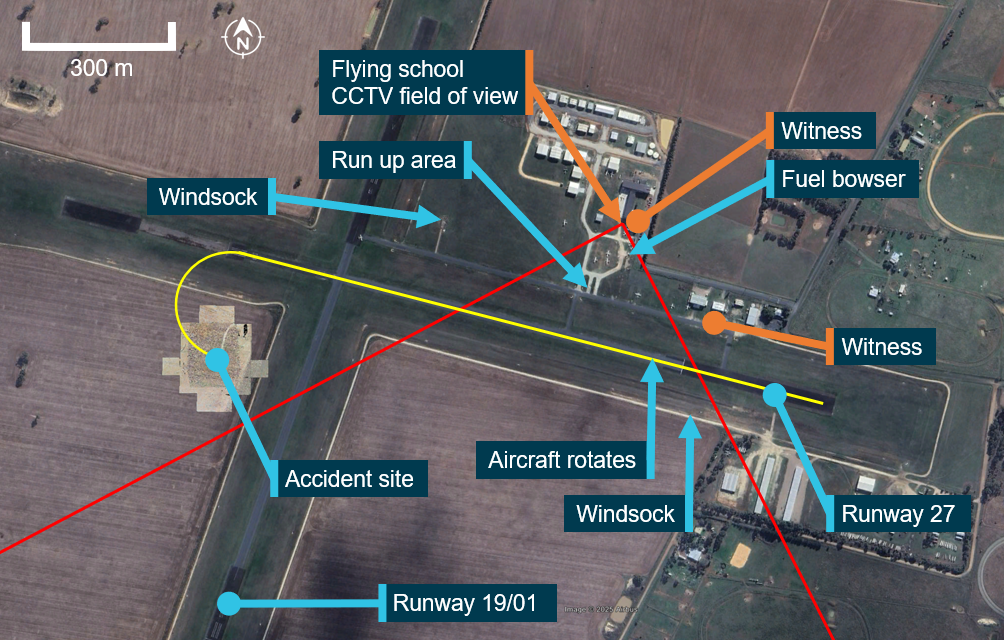
Source: Google Earth, annotated by the ATSB
Context
Pilot information
The pilot commenced their flight training in July 2019 and held a recreational pilot licence (aeroplane), which was issued on 14 November 2023. They held a single engine aeroplane class rating. The pilot also held navigation, controlled aerodrome, controlled airspace and flight radio endorsements which were issued on 19 April 2024.
Overall, the pilot had accumulated about 184 hours total aeronautical experience, of which 71.9 hours were in the Cessna 152 and 3.8 hours in the Cessna 150.
The pilot joined Bacchus Marsh Aero Club on 19 August 2024 and had completed 3 club check flights with an independent instructor during September and October 2024. Since joining the club, the pilot had flown a total of 20.1 hours in Cessna 172, Cessna 152 and Cessna 150 aircraft. They had also flown 3.3 hours in a Cessna 152 the previous day.
The pilot held a Class 2 aviation medical certificate issued by the Civil Aviation Safety Authority, without medical restrictions, which was valid until 19 March 2026.
Post-mortem examination
The post-mortem and toxicology examinations did not identify any indication of incapacitation or substances that could have affected the pilot’s capacity to perform the flight.
Aircraft information
The Cessna 150L is a high wing, all-metal, 2‑place, single‑engine aircraft with a fixed tricycle landing gear. It is powered by a 4‑cylinder Teledyne‑Continental O‑200‑A engine, driving a 2‑blade fixed‑pitch propeller. VH‑EYU (Figure 2) was manufactured in the United States in 1974 and first registered in Australia in May 1974. It had been owned by the Bacchus Marsh Aero Club since December 2023.
The aircraft was fitted with a stall warning horn on the left wing, which produces an audible signal to the pilot when the wing is approaching its critical angle of attack (AoA). The Cessna 150L’s stated stall speed in take‑off configuration with wings level was 48 kt.[5]
No crosswind limitation was published in the C150 L model owner’s manual. There was only a need for the manufacturer to demonstrate crosswind capability up to 8.5 kt (20% of the stall speed in a landing configuration). While it is possible that the aircraft may be capable of meeting the controllability standard in higher winds, this had not been established by the manufacturer.
Figure 2: VH-EYU

Source: Bacchus Marsh Aero Club
Recent maintenance history
The last 100‑hour periodic maintenance inspection was conducted on 19 January 2024. At the time of the accident, VH‑EYU had accrued a total time in service of 8,962.3 hours. Maintenance records also showed that since January, the following maintenance had been performed:
- a 50-hour/6-month oil and filter change
- the left brake was serviced
- the flap position indicator spring was replaced.
The aircraft had flown about 36.3 hours since the last scheduled maintenance which was conducted on 21 April 2024. There were no open defects recorded on the maintenance release and no outstanding or overdue maintenance was noted.
Aerodrome information
Bacchus Marsh aircraft landing area (ALA) was located about 6.5 km south of Bacchus Marsh, Victoria. It consisted of 2 sealed runways, 01/19 in a north‑south direction and 09/27 in the east‑west direction. The ALA was home to the Bacchus Marsh Aero Club, a pilot training school and several gliding clubs, as well as several privately owned aircraft.
The ALA was in non‑controlled Class G airspace. Aircraft operating in the area did not require clearance and a common traffic advisory frequency (CTAF) was available for pilot‑to‑pilot communication.
Bacchus Marsh Aero Club
Bacchus Marsh Aero Club operated several single-engine aircraft that were available to hire for approved club members, including the Cessna 150, 152, 172 and 182 models. Due to its status of being a private flying club and to satisfy insurance purposes, the club had a procedure in place for an independent flight instructor to conduct flight checks on new members prior to them being approved to fly club aircraft.
Site information
The accident site was in a barley field, 205 m south of the runway 27 centreline and to the west of runway 19/01 (Figure 1). The fuselage was orientated to the north. Ground impact marks were directly under the wreckage indicating no forward momentum. The damage signatures showed that the aircraft had impacted the field in a steep nose down attitude with the initial ground contact at the leading edge of the left wing. Severe disruption of the cockpit area, wing assembly and rear fuselage had occurred from the impact (Figure 3).
Figure 3: VH-EYU at the accident site

Source: ATSB
Wreckage examination
The ATSB’s examination of the wreckage did not identify any evidence of pre‑existing faults, flight control issues or engine issues and there was no evidence of birdstrike.
All components were accounted for at the accident site. The right fuel tank had ruptured, while the left tank remained intact. A quantity of fuel was removed from the aircraft fuel tank for onsite testing and was found to be clean and clear of contaminants. Fuel was removed from the carburettor, which was also tested with no water or contaminants found.
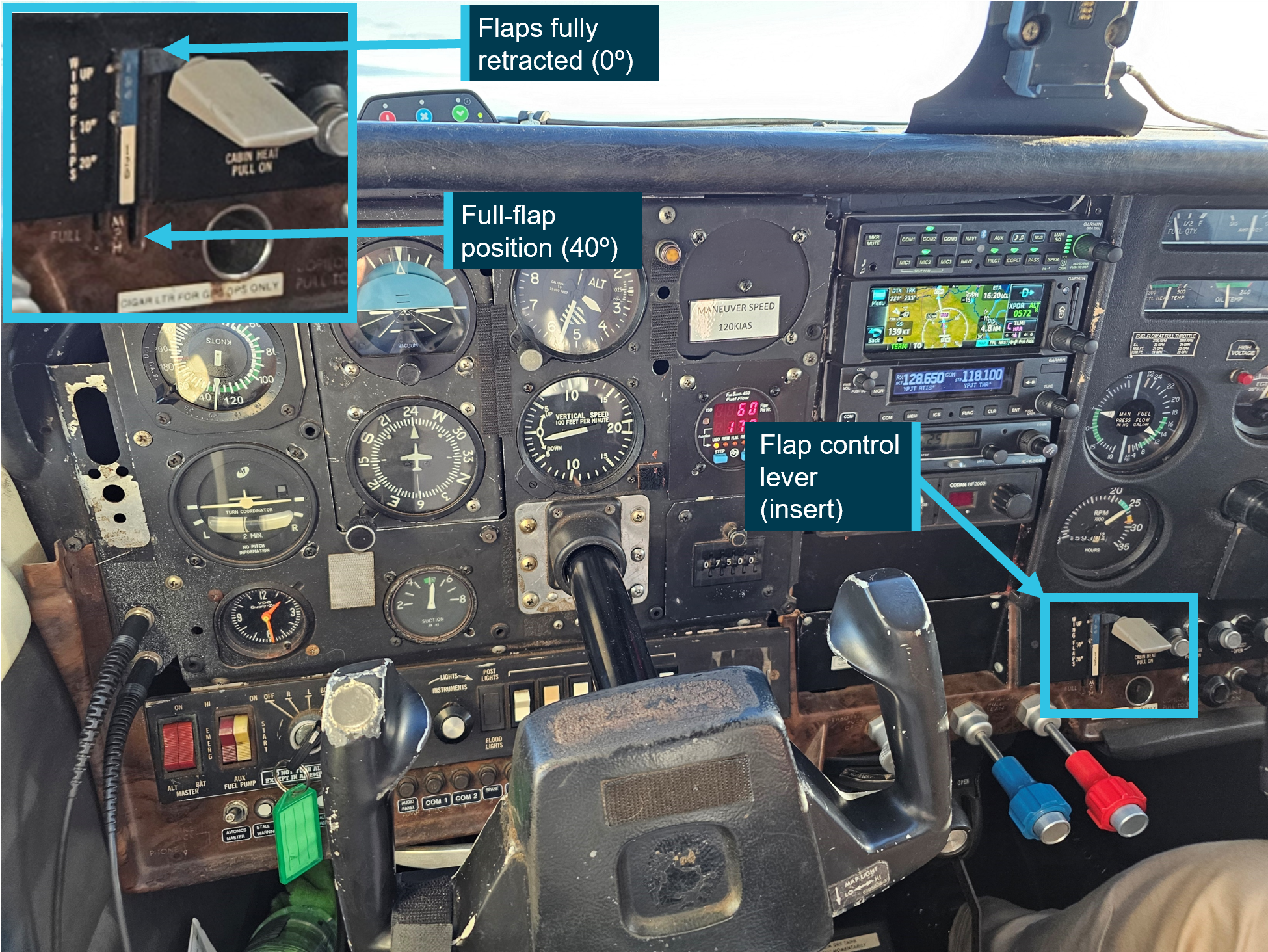
The wings and centre fuselage roof section had separated and moved forwards as a result of the impact. Portions of the airframe were removed by first responders prior to ATSB examination, and these were photographed prior to removal. The stall warning horn on the left wing was damaged in the accident sequence and could not be tested for functionality. The flaps were noted to be retracted, which is the position required in the normal take‑off checklist.
An examination of the seat rails showed that the pilot seat was locked into position and had not moved prior to the accident.
The engine and propeller displayed no pre‑existing damage. The engine was externally examined, and all components were accounted for. The engine was able to be rotated which indicated no significant internal damage had occurred.
The propeller and flange had fractured from the engine crankshaft and there was evidence of rotation on the fracture surfaces. The propeller displayed minor rotational scoring and rearward bending which was indicative of low rotational energy at the time of impact.
The throttle control in the cockpit was set at a low power position and had been bent upwards during the impact sequence.
Survival aspects
The pilot had been wearing a lap/sash seat belt during the accident flight. The extent of the damage to the occupiable space of the aircraft cabin meant that the impact was not considered survivable.
Aircraft stall and spin behaviour
Aerodynamic stalls
An aerodynamic stall is a rapid decrease in lift and increase in drag caused by the separation of airflow from the wing’s upper surface. A stall occurs when the angle of attack[6] exceeds the wing’s critical angle of attack,[7] resulting in the disruption to the smooth airflow over the wing. This can ordinarily occur at angles of around 16° (Figure 4). Due to the sudden reduction in lift from the wing and rearward movement of the centre of lift, an uncommanded nose‑down pitch ensues.
The US Federal Aviation Administration (FAA) Airplane Flying Handbook (2021) states that:
• Impending Stall—an impending stall occurs when the AOA causes a stall warning but has not yet reached the critical AOA. Indications of an impending stall can include buffeting… or aural warning.
• Full Stall—a full stall occurs when the critical AOA is exceeded. Indications of a full stall are typically that an uncommanded nose down pitch cannot be readily arrested and may be accompanied by an uncommanded rolling motion...
The FAA Airplane Flying Handbook (2021) also states that for an impending stall the pilot should:
…immediately reduce AOA once the stall warning device goes off, if installed, or recognizes other cues such as buffeting. The pilot should hold the nose down control input as required to eliminate the stall warning. Then level the wings maintain coordinated flight, and then apply whatever additional power is necessary to return to the desired flightpath.
Figure 4: Effect of increasing angle of attack leading to a stall condition
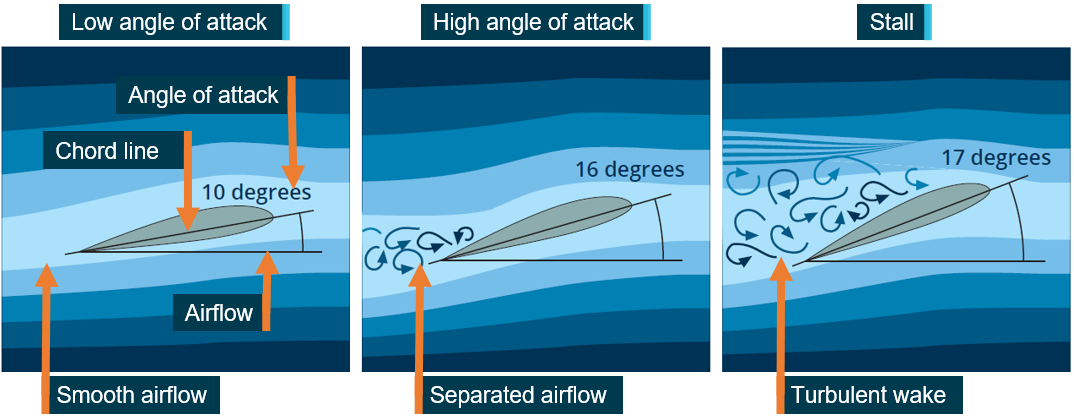
Source: CASA AvSafety, annotated by the ATSB
Aerodynamic spins
A spin can result when an aircraft simultaneously stalls and yaws.[8] The yaw can be initiated by rudder application (through manipulation of the rudder pedals) or by yaw effects from a range of factors that include aileron deflection, torque, wind and engine/propeller effects. A spin is characterised by the aircraft following a downward, corkscrew path and requires significantly more altitude for recovery compared to a wings level stall.
The spin recovery procedure stated in the Cessna 150L handbook was:
For recovery from an inadvertent or intentional spin, the following procedure should be used.
• retard the throttle to idle position
• apply full rudder opposite to the direction of rotation
• after one-fourth turn, move the control wheel forward of neutral in a brisk motion
• as rotation stops, neutralize rudder and make a smooth recovery from the resulting dive.
Application of aileron in the direction of the spin will greatly increase the rotation rate and delay the recovery. Ailerons should be held in a neutral position throughout the spin and the recovery. Intentional spins with flaps extended are prohibited.
To recover from the spin, the pilot requires sufficient height to conduct the procedure and fly away. During the initial stages of a take‑off, there is insufficient height to perform these actions.
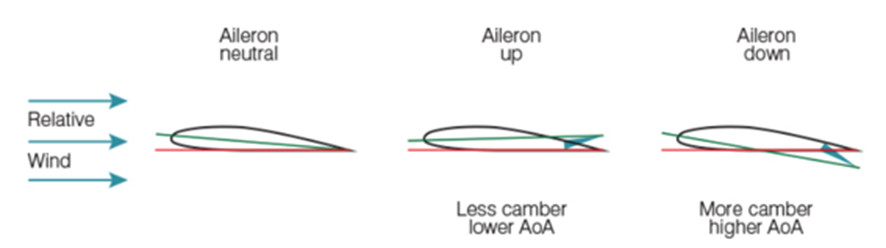
Control input in a crosswind
In a crosswind, to prevent uncommanded roll, the pilot must turn the control yoke into wind. This will move the ailerons to change the relative angle of attack of each wing (Figure 5). The aileron on the into‑wind wing (right in this case) will move up, create a lower angle of attack and produce less lift. The aileron on the downwind wing (left in this case) will move down, creating a higher angle of attack and more lift. Therefore, resisting the rolling moment created by the crosswind.
Figure 5: Effect of aileron use on angle of attack
Source: Flight Safety Australia
Guidance
The FAA Airplane Flying Handbook (2021) states for take‑off in gusty conditions that:
During take-offs in a strong, gusty wind, it is advisable that an extra margin of speed be obtained before the airplane is allowed to leave the ground. A take-off at the normal take-off speed may result in a lack of positive control, or a stall, when the airplane encounters a sudden lull in strong, gusty wind, or other turbulent air currents. In this case, the pilot should allow the airplane to stay on the ground longer to attain more speed, then make a smooth, positive rotation to leave the ground.
A Civil Aviation Safety Authority publication AC 91‑02 v1.2 – Suitable places to take‑off and land, and the FAA publication Personal minimums for wind both identify that is the responsibility of the pilot in command to consider the winds and determine if the aircraft can be operated safely in the prevailing conditions. The FAA publication advises pilots to conduct their own testing in progressively higher winds to determine both their own capability and that of the airframe.
Meteorological information
Forecast weather
The planned flight from Bacchus Marsh to Lethbridge was within the Victoria graphical area forecast (GAF)[9] region. The Bureau of Meteorology issued a GAF which included the Bacchus Marsh area, at 0900 on 22 October 2024, and was valid from 1000–1600. The forecast indicated visibility greater than 10 km and no cloud. A Grid Point Wind and Temperature Forecast was issued by the Bureau of Meteorology at 0525 on 22 October 2024. No wind and temperature was available in the Bacchus Marsh area below 5,000 ft.
The Bureau of Meteorology issued aerodrome forecasts (TAF)[10] and meteorological aerodrome reports (METAR)[11] for Melbourne, Essendon, Avalon and Ballarat airports. A special meteorological report (SPECI)[12] was also issued, which highlighted that a significant wind gust had been recorded.
There was no record that the pilot had used any personal login to access weather forecasts prior to their flight, from any official sources. It is unknown if the pilot had checked a forecast via other sources which did not require accounts for access.
Nearby airport weather
The actual weather at Bacchus Marsh ALA was not recorded and not available. However, forecasts and observation reports were available for nearby airports. Table 1 shows the recorded winds at Melbourne Airport leading up to the accident. Melbourne Airport is about 38 km on a bearing of 78° True (° T) from Bacchus Marsh.
Table 1: Wind speed and direction recorded at Melbourne Airport
| Report | Time (local) | Bearing ° T | Wind speed (kt) | Time before accident |
| METAR | 1000 | 010 | 22 | 74 minutes |
| SPECI | 1007 | 020 | 21, gusting to 32 | 67 minutes |
| METAR | 1030 | 020 | 20 | 44 minutes |
| METAR | 1100 | 010 | 20 | 14 minutes |
Source: Bureau of Meteorology
Table 2 shows the recorded winds at Ballarat Airport leading up to the accident. Ballarat Airport is about 59 km on a bearing of 293° T from Bacchus Marsh.
Table 2: Wind speed and direction recorded at Ballarat Airport
| Report | Time (local) | Bearing ° T | Wind speed (kt) | Time before accident |
| METAR | 1000 | 360 | 13 | 74 minutes |
| METAR | 1030 | 360 | 13 | 44 minutes |
| METAR | 1100 | 360 | 10 | 14 minutes |
| METAR | 1130 | 360 | 14 | -16 minutes |
Source: Bureau of Meteorology
Windsock indication
Figure 6 shows VH-EYU taxiing to the runway threshold in the opposite direction but parallel to the take‑off direction. The visible opening of the orange windsock in the background indicates headwind and crosswind components for take‑off.
Figure 6: VH-EYU taxiing prior to second take‑off

Source: Supplied
Witness observations of the weather
A number of witnesses described the temperature to be ‘very hot’ (27°C) with strong and gusting winds at the time of the accident. The winds were changing in strength (15–30 kt) and direction (between runways 27 and 01) (Figure 7). A flight instructor, who was an eyewitness to the accident stated that they had cancelled a student’s flight which was to occur later in the day due to the gusty conditions.
FlySto data from a Cessna 172
A Cessna 172 was flying nearby at the time of the accident and landed at Bacchus Marsh ALA 10 minutes after the accident. Data from the aircraft was uploaded to FlySto.[13] This data recorded the average wind from ground level up to 3,600 ft over a 40‑minute period. The wind direction varied between 262° T and 335° T and at speeds from 6–32 kt. At the time of the accident, this aircraft was located 14 km (8 NM) to the south of Bacchus Marsh ALA and had recorded a 27 kt wind from 290° T while on descent. The temperature recorded upon landing was 29°C.
A component of this data will be normal changes in wind speed and direction due to changes in altitude. For this reason, the average winds referenced in FlySto cannot be used to determine exact conditions at ground level at the time of the accident.
Figure 7: Witness observation (red arc) and recorded data from FlySto (orange arc), showing approximate wind directions and speeds around time of VH‑EYU take‑off
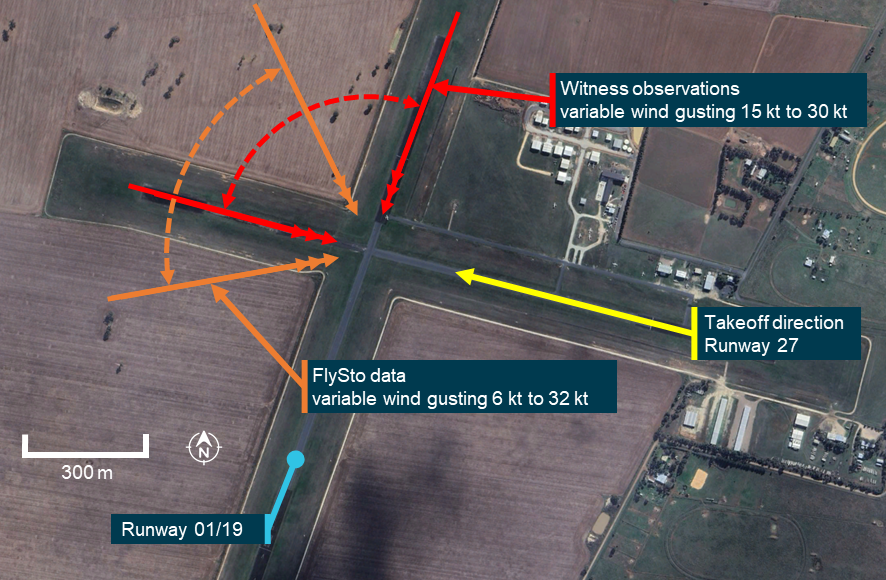
Source: Google Earth, annotated by the ATSB
CCTV and witness video
CCTV recorded the pilot’s arrival at the airport, refuelling, engine run‑up and control checks, and both take‑off runs. All videos showed evidence of strong and gusting winds creating movement in nearby trees and grass. Pitot cover flags on parked aircraft and clothing of people on the apron were observed flapping in the wind. The videos also captured wind noise varying with gusts.
A gliding club located to the east of the ALA had erected a small windsock, which was observed to be moving erratically with the varying wind strength and directions. The witness video provided, showed this windsock to be a smaller commercially available item. Due to its design, it did not meet the standards[14] for wind direction indicators and therefore was not able to provide any information of wind speed.
Recorded information
CTAF recording
CTAF recordings provided the standard radio transmissions made by the pilot. The recordings also captured the engine sounds each time a transmission was made and showed that the engine sounded normal throughout the duration of the recordings.
The pilot sounded calm during transmission and voiced no concern with the engine or aircraft after the first rejected take‑off and subsequent return for the second take‑off.
Aircraft data
The aircraft was not equipped with either a cockpit voice recorder or a flight data recorder, nor was it required to be. Further, there was no active flight tracking equipment or other devices fitted to the aircraft to provide parameters from the accident flight.
CCTV
The ATSB conducted frame‑by‑frame analysis of the CCTV of the second take‑off. This analysis showed that the groundspeed of the aircraft was 42 kt when the aircraft became airborne.
Related occurrences
AO-2014-023: Cessna 150G, VH-RXM, Loss of control during initial climb, 18 February 2014, Moorabbin Airport
An instructor and student pilot were conducting a trial instructional flight. The aircraft departed with a 3–4 kt tailwind. The student was operating the aileron and elevator controls, with the instructor operating the rudder. During the initial climb, the student continued to apply back pressure to the control column resulting in a reduction in optimal airspeed, and a higher‑than‑normal aircraft nose attitude. As the instructor attempted to rectify the aircraft’s profile, the right wing dropped, and the aircraft began to descend.
The instructor’s efforts to recover the aircraft to a normal climb attitude were not successful, and the right side of the aircraft struck the ground. The aircraft bounced, then came to a halt on its left side. The instructor and student egressed through the right door, and both sustained minor injuries. The aircraft was substantially damaged.
NTSB Docket WPR21LA255 Cessna 150L, N1972L, Collision during take‑off, 30 June 2021, Mud Lake Airport (1U2), Terreton, Jefferson County, Idaho, United States
The pilot reported that, upon landing, they saw a crop duster aircraft descending for a short base for landing on the opposite runway. The pilot initiated a go around with the flaps still extended and with a high-density altitude. The aeroplane attained an altitude of about 50 to 100 ft above ground level when the aeroplane stalled, and the left wing dropped. The pilot attempted to recover but did not have enough height before the aeroplane collided with the ground. The aeroplane nosed over and came to rest inverted. The wings and fuselage were substantially damaged. The pilot and passenger sustained serious injuries.
Safety analysis
While there was no evidence that the pilot accessed official weather forecasts on the day of the accident, the pilot may have consulted informal sources, and they were able to experience the weather at Bacchus Marsh prior to departure. Through the movement of the distant windsock, vegetation, pitot covers on parked aircraft and the clothing of people in view of CCTV and video, it was evident that strong gusting winds were present. Noise on the audio track of CCTV also showed gusts were occurring.
This supported observations of witnesses at the airfield of the conditions throughout the day and at the time of the accident. It is almost certain the wind conditions would have also been evident to the pilot at the time of take‑off. While no weather recording equipment was available at Bacchus Marsh, the evidence available allowed for an estimate of wind varying from west to north at speeds from around 10 kt gusting to 30 kt.
There was no evidence of problems with the aircraft. The CCTV showed the pilot conducting pre‑take‑off run-up and control checks prior to the first take‑off. Witnesses and analysis of engine sound from CTAF broadcasts from VH‑EYU confirmed that the engine sounded normal. Additionally, post‑accident examination of the aircraft found no evidence of pre‑accident damage which would have affected the flight.
There was no stated or discernible reason for the first rejected take‑off. The pilot gave no indication of an aircraft serviceability issue in their radio calls. They did not conduct any additional engine run‑up checks or stop the aircraft to perform any exterior airframe inspection. After exiting the runway, the aircraft was taxied without delay to runway 27 for the second take‑off.
On the second take‑off, CCTV analysis showed the groundspeed of the aircraft was 42 kt when the aircraft became airborne. Based on witness observation and the Cessna 150 measurements, the ATSB estimates the aircraft likely had an airspeed of over 50 kt, marginally faster than the 48 kt stall speed of the aircraft. At that time, crosswind was likely to be around 15 kt.
Witnesses identified and CCTV footage showed that the aircraft’s attitude was unstable after becoming airborne. This indicates that the aircraft was affected by the strong, variable and gusting headwind and crosswind components as the pilot attempted the second take‑off. These uncommanded wind‑driven movements would require constant aircraft attitude adjustments by the pilot.
The flight instructor’s observation of the steep pitch‑up and controlled lowering of the nose which occurred at around 50 ft is consistent with the pilot manipulating the controls to avoid the aircraft descending back onto the runway and to maintain a suitable airspeed and take-off profile. The second uncorrected steep pitch‑up which occurred at around 150 ft, and the subsequent dropping of the left wing and nose resulting in entry into a left incipient spin, was consistent with a fully developed stall and loss of control in flight. This, in turn, was consistent with evidence of the accident site, in which the aircraft wreckage was confined to a small area, with evidence of a high vertical impact and low forward speed.
In this accident, it is almost certain that, after take‑off and at low level, the aircraft was subjected to a strong and gusting wind. The nature of the prevailing winds increased the likelihood of a drop in airspeed during a phase of flight where the aircraft was flown at a high angle of attack, leading to an impending stall condition.
It is possible that the impending stall period was very short due to gust strength and the pitch‑up movement created conditions for aerodynamic stall. Further, as the airspeed at take‑off was likely only a few knots higher than the stall speed, there was minimal buffer to account for any sudden drop of wind strength. The evidence indicates that the angle of attack of the wings increased beyond the critical angle, the left wing of the aircraft aerodynamically stalled, and the aircraft entered the incipient phase of a spin. The stalling of the left wing indicates that the angle of attack on the left wing was higher than that on the right. This is likely due to control inputs to counteract a crosswind from the right.
The actions that take place when the aircraft enters a spin require the pilot to retard the throttle. The throttle position in the aircraft was found in a low power setting, which was likely due to the pilot responding to the aircraft entering the incipient phase of a spin. Because the aircraft stalled at a height of about 150 ft, there was insufficient height to recover before the aircraft collided with terrain.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following finding is made with respect to the loss of control and collision with terrain involving Cessna 150L, VH-EYU, at Bacchus Marsh aircraft landing area, Victoria, on 22 October 2024.
Contributing factors
- It is probable that the aircraft was too slow on take‑off for the strong and gusty wind conditions and significant crosswind, meaning there was minimal buffer to manage an impending stall. Shortly after take‑off, the aircraft stalled at a height too low to recover, resulting in a collision with terrain.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Bacchus Marsh Aero Club
- Civil Aviation Safety Authority
- Victoria Police
- the maintenance organisation for VH-EYU
- Airservices Australia
- Bureau of Meteorology
- Peninsula Aero Club
- Oxford Aviation Academy
- TVSA Pilot Training
- witnesses
- video footage of the accident flight and other videos taken on the day of the accident
- recorded CTAF communications.
References
Civil Aviation Safety Authority 2019, Strong and gusty winds, Civil Aviation Safety Authority, Canberra, ACT Strong and gusty winds | Flight Safety Australia
Civil Aviation Safety Authority 2020, Advisory Circular AC 61-16v1.0, Civil Aviation Safety Authority, Canberra, ACT, https://www.casa.gov.au/spin-avoidance-and-stall-recovery-training
Civil Aviation Safety Authority 2020, Part 139 (Aerodromes) Manual of Standards 2019, Civil Aviation Safety Authority, Canberra, ACT, Part139_(Aerodrome)_MOS.pdf pp 196-198.
Civil Aviation Safety Authority 2019, Rudder, ailerons, stalls and spins, Civil Aviation Safety Authority, Canberra, ACT Rudder, ailerons, stalls and spins | Flight Safety Australia
Civil Aviation Safety Authority 2022, Stalls in the circuit, Civil Aviation Safety Authority, Canberra, ACT Stalls in the circuit | Flight Safety Australia
Civil Aviation Safety Authority 2022, Advisory Circular AC 91-02v1.2, Civil Aviation Safety Authority, Canberra, ACT https://www.casa.gov.au/guidelines-aeroplanes-mtow-not-exceeding-5-700-kg-suitable-places-take-and-land pp21-22.
Civil Aviation Safety Authority 2024, AvSafety: Preventing a stall at low level, Civil Aviation Safety Authority, Canberra, ACT, Preventing a stall at low level
Federal Aviation Administration 2021, Airplane Flying Handbook (FAA-H-8083-3C), Federal Aviation Administration, Washington DC Airplane Flying Handbook
National Transportation Safety Board 2015, NTSB Safety Alert 19 / Prevent Aerodynamic Stalls at Low Altitude, National Transportation Safety Board, Washington DC NTSB Safety Alert 19 / Prevent Aerodynamic Stalls at Low Altitude
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the Civil Aviation Safety Authority
- the Bacchus Marsh Aero Club
- the National Transportation Safety Board.
Any submissions from those parties were reviewed and, where considered appropriate, the text of the draft report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] Run-up area: a designated area of an airfield where pilots can perform functional pre-flight checks of aircraft systems.
[3] Runway number: the number represents the magnetic heading of the runway. In this case, ‘27’ represents a magnetic heading of 270°.
[4] Common traffic advisory frequency (CTAF): radio frequency on which pilots monitor and use to make positional broadcasts when operating within a 10 NM radius of the airport.
[5] The Cessna 150L Owner’s Manual lists all speeds in miles per hour.
[6] Angle of attack: the acute angle between the chord line of the airfoil and the direction of the relative wind.
[7] Critical angle of attack. the angle of attack at which a wing stalls regardless of airspeed, flight attitude, or weight.
[8] Yaw: the motion of an aircraft about its vertical or normal axis.
[9] Graphical Area Forecast (GAF): provides information on weather, cloud, visibility, icing, turbulence and freezing level in a graphical layout with supporting text.
[10] Aerodrome Forecast (TAF): a statement of meteorological conditions expected for the specified period of time in the airspace within 5 nautical miles (9 km) of the aerodrome reference point.
[11] METAR (Meteorological Aerodrome Report) is a routine aerodrome weather report issued at half hourly time intervals. The report ordinarily covers an area of 8 km radius from the aerodrome reference point.
[12] SPECI: a special report of meteorological conditions, issued when one or more elements meet specified criteria significant to aviation.
[13] FlySto is a web-based application that allows for upload and interpretation of flight data from a range of avionics devices.
[14] The standards for windsocks are outlined in Part 139 Aerodrome Manual of Standards, which provides information for windsocks and their interpretation.
Preliminary report
Report release date: 16/12/2024
| This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003. |
The occurrence
On 22 October 2024, at about 1110 local time, the pilot of a Cessna 150L registered VH‑EYU, commenced the take-off roll on runway 27[1] at Bacchus Marsh airfield, Victoria (Figure 1). Shortly after, the pilot made a radio call stating that they were rejecting the take‑off. The aircraft was then taxied off the runway and returned to the threshold of runway 27, where at 1114 the pilot recommenced the take-off.
Several witnesses at the airfield observed the second take-off and identified that, during its initial climb, the aircraft attitude pitched steeply upward. Witnesses described that the left wing dropped rapidly. The aircraft then entered a vertical descent, rotating approximately 270° before colliding heavily with terrain. The pilot (who was the sole occupant) sustained fatal injuries and the aircraft was destroyed. There was no post-impact fire.
Figure 1: Bacchus Marsh airfield and VH-EYU accident location

Source: Google Earth, annotated by the ATSB
Context
Pilot information
The pilot held a Recreational Pilot Licence (Aeroplane) and a Class 2 Aviation Medical Certificate, valid until March 2026. The pilot held a single engine aeroplane rating, and navigation endorsement. At the time of the accident, the pilot had about 184 hours total aeronautical experience, of which 3.8 hours were in Cessna 150 aircraft.
Aircraft information
The Cessna 150L is a high wing, all-metal, 2-place, single-engine aircraft with a fixed tricycle landing gear. It is powered by a 4-cylinder Teledyne-Continental O-200-A engine, driving a 2-blade fixed-pitch propeller. The aircraft was manufactured by Cessna in the United States in 1974 and first registered in Australia in May 1974. It had been owned by the Bacchus Marsh Aero Club since December 2023 (Figure 2).
The last 100-hour periodic maintenance inspection was conducted on 19 January 2024. At the time of the accident, it had accrued a total time in service of 8,962.3 hours. The aircraft had flown about 34 hours since the last scheduled maintenance which was conducted on 21 April 2024. There no known defects documented on the aircraft maintenance release.
Figure 2: VH-EYU

Source: Bacchus Marsh Aero Club
Aerodrome information
Bacchus Marsh airfield is located about 6.5 km south of Bacchus Marsh, Victoria, Australia. It is an aircraft landing area (ALA) consisting of 2 sealed north/south (01/19) and east/west (09/27) runways. The airfield was primarily used by the Bacchus Marsh Aero Club, a pilot training school and several gliding clubs.
Bacchus Marsh Aero Club
Bacchus Marsh Aero Club operates several high wing single-engine aircraft available to hire for approved club members, including the Cessna 150, 152, 172 and 182. The pilot joined the club on 19 August 2024 and subsequently completed check rides with an instructor on 13 September, 27 September and 4 October 2024.
Site information
ATSB investigators first attended the accident site on 23 October 2024. The aircraft had impacted into a barley field 205 m south of the runway 27 centreline and was orientated toward the north. The damage signatures confirmed that it had impacted the field in a steep nose down attitude. Severe disruption of the cockpit area, the wing assembly and rear fuselage had occurred from the impact (Figure 3).
Figure 3: VH-EYU at the accident site near to the airfield runways

Source: ATSB
Wreckage examination
The ATSB conducted a preliminary examination of the aircraft wreckage in the field, then moved the wreckage to a secure hangar for detailed examination. The examinations identified:
- no evidence of pre-impact defects with the flight controls or structure
- all components were accounted for at the accident site
- the engine was able to be rotated and there were no obvious defects upon external examination
- the throttle setting was at idle position (low power)
- rotational damage signatures to the propeller were minimal which indicated a low engine power setting at the time of the impact
- the propeller and flange had fractured from the engine crankshaft.
A quantity of fuel was removed from the aircraft for onsite testing and was found to be clean and clear of contaminants.
Meteorological information
Forecast
The Bureau of Meteorology (BoM) issued a graphical area forecast that included the Bacchus Marsh area, at 0900 on 22 October 2024, that was valid from 1000–1600. The forecast indicated visibility greater than 10 km and no cloud.
Witness observations of the weather
Witnesses at Bacchus Marsh airfield described the wind at the time of the accident as strong and gusty, changing in direction and strength. A flight instructor stated that they had cancelled a student’s flight due to the increasingly gusty conditions which were present on the day.
Meteorological observations
There was no BoM aerodrome weather information specifically for Bacchus Marsh, but the ATSB obtained meteorological observations for the surrounding areas of Melbourne, Essendon, Avalon and Ballarat airports (Figure 4).
Figure 4: Location of Bacchus Marsh airfield relative to nearby aerodrome weather forecast locations

Source: Google Earth, annotated by the ATSB
Table 1 shows the recorded winds in meteorological aerodrome reports (METAR)[2] and special meteorological reports (SPECI)[3] issued between 1000 and 1200 on 22 October 2024. The wind direction is in degrees true[4] rounded to the nearest 10 degrees. The wind direction and speed are the mean values over 10 minutes, and the gust is the maximum wind speed over a 2-minute period.
Table 1: Aerodrome wind observations
| Time | Melbourne | Essendon | Avalon | Ballarat |
|---|---|---|---|---|
| 1000 | 010° 22 kt | 360° 15 kt | 020° 8 kt | 360° 13 kt |
| 1007[1] | 020° 21 kt gusting to 32 kt | |||
| 1020[1] | 360° 17 kt gusting to 27 kt | |||
| 1030 | 020° 20 kt | 360° 16 kt | 360° 10 kt | 360° 13 kt |
| 1100 | 010° 20 kt | 360° 18 kt | 330° 12 kt | 360° 10 kt |
| 1130 | 010° 19 kt | 360° 15 kt | 350° 12 kt | 360° 14 kt |
| 1200 | 010° 17 kt | 360° 15 kt | 350° 11 kt | 360° 16 kt |
[1] SPECI
Further investigation
To date, the ATSB has:
- examined the aircraft wreckage
- conducted witness interviews
- reviewed common traffic advisory frequency recordings
- reviewed CCTV footage and mobile phone footage
- obtained weather information.
The investigation is continuing and will include:
- further review of the pilot’s experience, qualifications and training
- further review and analysis of recorded CCTV and mobile phone footage
- further analysis of the weather conditions
- examination of the aircraft maintenance history.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Runway number: the number represents the magnetic heading of the runway. In this case, 27 represents a magnetic heading of 270°.
[2] METAR: a routine aerodrome weather report issued at half hourly time intervals.
[3] SPECI: a special aerodrome weather report issued only when meteorological parameters meet specific criteria.
[4] The magnetic variation at Bacchus Marsh was 11° east.
Occurrence summary
| Investigation number | AO-2024-053 |
|---|---|
| Occurrence date | 22/10/2024 |
| Location | Bacchus Marsh aircraft landing area |
| State | Victoria |
| Report release date | 10/07/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain, Loss of control |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 150L |
| Registration | VH-EYU |
| Serial number | 15075559 |
| Aircraft operator | Bacchus Marsh Aero Club |
| Sector | Piston |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Bacchus Marsh, Victoria |
| Destination | Bacchus Marsh, Victoria |
| Damage | Destroyed |