The ATSB has finalised its investigation into an accident involving a Robinson R44 helicopter which struck the roof of a Cairns hotel early in the morning of 12 August 2024.
“The investigation found that the pilot conducted an unauthorised and unnecessary flight at night, while affected by alcohol,” said ATSB Chief Commissioner Angus Mitchell.
“The pilot did not hold the appropriate endorsements to fly at night, did not have any experience flying the R44 at night, and they conducted the flight well below the 1,000 ft minimum height for flight over built up areas.”
The ATSB finalised the investigation after determining it unlikely that broader safety issues or lessons would be uncovered.
“The ATSB primarily investigates to identify industry systemic safety issues, and to then influence the adoption of targeted actions to reduce future risk,” said Mr Mitchell.
“Our final report published today provides assurance to the Cairns community and the aviation industry that after gathering and analysing the available evidence, there are unlikely to be broader transport safety issues that require addressing to reduce future risk arising from this tragic accident.”
The report details that the pilot was an employee of the helicopter operator, and had gained access to their premises after entering a code into a security door keypad, and then to the hangar and the helicopter. The pilot held valid New Zealand and Australian commercial helicopter pilot licences, and had previously flown R44 helicopters. However, they were employed by the operator as a ground handler, and were not approved to, nor employed to fly the operator’s helicopters.
“Using a combination of CCTV footage, witness accounts, GPS data from the helicopter and air traffic control surveillance radar data, the ATSB was able to develop a detailed sequence of events of the accident flight,” Mr Mitchell said.
Prior to the flight, the pilot had been socialising with friends at various venues in Cairns, where they had been consuming alcohol, the report details. They had returned to their apartment around 11 pm, with CCTV footage showing them driving away from the apartment complex at 1:09 am. CCTV footage from the operator’s hangar showed the pilot moving the helicopter outside onto a helipad just after 1:30 am.
“We know from GPS and air traffic control radar data that the helicopter departed Cairns Airport shortly before 1:47 am, while CCTV footage showed that the helicopter’s strobe lights were turned off by the pilot,” Mr Mitchell said.
After taking off, the helicopter headed south towards the Cairns city centre, flying over the pilot’s apartment building and then tracking to the northern end of the Cairns wharf complex, where it completed an orbit before heading north towards the marina and continuing along the coastline.
After crossing the coastline and flying over the pilot’s apartment a second time, the helicopter circled back towards the foreshore, following it for about 1 km.
Throughout the flight the helicopter’s altitude did not exceed 500 ft.
“Two security cameras recorded very brief portions of the final part of the flight and showed the helicopter pitching up, then almost immediately descending steeply before colliding into the roof of the hotel at about 1:51 am,” Mr Mitchell said.
“Wreckage distribution and impact marks indicate that the helicopter was inverted at impact.”
Most of the helicopter came to rest on the hotel roof and was destroyed by impact forces and a fuel-fed post-impact fire. The pilot was fatally injured.
Parts of the main rotor blade were found in the hotel rooms below the accident site, while the helicopter’s instrument panel, main rotor head and most of the main rotor blades were found within the hotel grounds. A portion of the same main rotor blade that struck the hotel windows was found in parkland across the road.
Fortunately there were no injuries to hotel guests and staff, nor passersby.
“From the available evidence there were no airworthiness factors with the helicopter that likely contributed to the accident,” Mr Mitchell said.
“The flight was a purposeful act, but there was no evidence available to explain the pilot’s intentions.”
Mr Mitchell concluded: “I would like to acknowledge that the nature of this accident is deeply distressing to the pilot’s family, and they have asked that I share with you their request for privacy at this time.”
A Socata light aircraft’s high rate of descent before impacting steep mountainous terrain was consistent with the pilot becoming spatially disoriented after flying into cloud, an ATSB investigation report details.
The five-seat, single-engine Socata TB-20 was conducting a private flight from Montpelier, near Townsville, to Palmyra, near Mackay, on 28 October 2023, with a pilot and passenger (who was also a licenced pilot, but was not current) on board.
During the flight, the pilot contacted a friend, also a licenced pilot, who was on the ground at Palmyra, to ask about the weather at the destination.
“After the friend advised of the prevailing conditions including cloud at Palmyra and blue sky to the south, the pilot replied that they would need to go through some cloud,” Director Transport Safety Dr Stuart Godley said.
Recorded data of the flight from the OzRunways electronic flight bag app being used by the pilot showed around 30 NM from the destination, shortly after commencing descent, the aircraft began a steep descending turn to the left towards mountainous terrain.
During this descent, the aircraft exceeded the airframe’s designed maximum airspeed before pitching up and passing over the top of Bull Mountain. The aircraft then entered a second steep descending turn, this time to the right, before the recorded flight path data ceased.
The aircraft collided with terrain in dense forest on the north-east face of Bull Mountain at about 1,900 ft above sea level.
“The instability of the flight path with excessive rates of descent and climb are markers of spatial disorientation where pilots are aware of a departure from controlled flight and attempt to correct the unusual attitude,” Dr Godley said.
“It is very likely the pilot had entered weather conditions not suitable for visual navigation, leading to spatial disorientation and the descent into mountainous terrain.”
The aircraft was destroyed in the accident, and both occupants were fatally injured.
The report notes the pilot, who was not qualified for flight in instrument meteorological conditions, had regularly flown between Montpelier and Palmyra, and would, according to peers, generally fly the cruise portion of the flight on autopilot and use the autopilot if they ever had to fly through cloud.
“For a non-instrument rated pilot, even with basic attitude instrument flying proficiency, maintaining control of an aircraft in IMC by reference to the primary flight instruments alone entails a very high workload that can result in narrowing of attention and loss of situational awareness,” Dr Godley said.
“While autopilot can be used to reduce workload, it is not infallible and should not be relied upon or used by VFR pilots as a risk mitigator to decide to fly into unsuitable conditions.”
Due to the limited evidence available to the ATSB, the investigation was unable to determine why the autopilot disconnected, either due to pilot action or technical failure, prior to the aircraft entering its high rate of descent.
"Appropriate pre-flight preparation and planning is the key risk control for visual flight rules pilots to avoid entering IMC,” said Dr Godley.
“While forecasts will assist in selecting the route to be flown, pilots should plan an alternate or be prepared to make necessary deviations from the planned route, should actual weather conditions indicate the possibility of not being able to remain visual.”
The investigation report also cautions against the use of unapproved mobile devices displaying charts and data as the sole means of navigation when operating under the VFR.
Tablet computers running electronic flight bag apps such as OzRunways are widely used and a useful supplement to aircraft navigation, but are not approved for use as a primary means of navigation. The accident aircraft was fitted with an approved GPS for navigation. However, the pilot was not known to program flight plans into the unit, instead relying on OzRunways running on an iPad for navigation.
“Pilots should use navigation equipment approved for aviation and maintain skills in navigating by reference to approved charts,” Dr Godley noted.
includes a selection of weather-related general aviation accidents and incidents that show weather alone is never the only factor affecting pilot decisions that result in inadvertent IMC encounters.
“These investigations consistently highlight that conducting thorough pre-flight planning is the best defence against flying into deteriorating weather.”
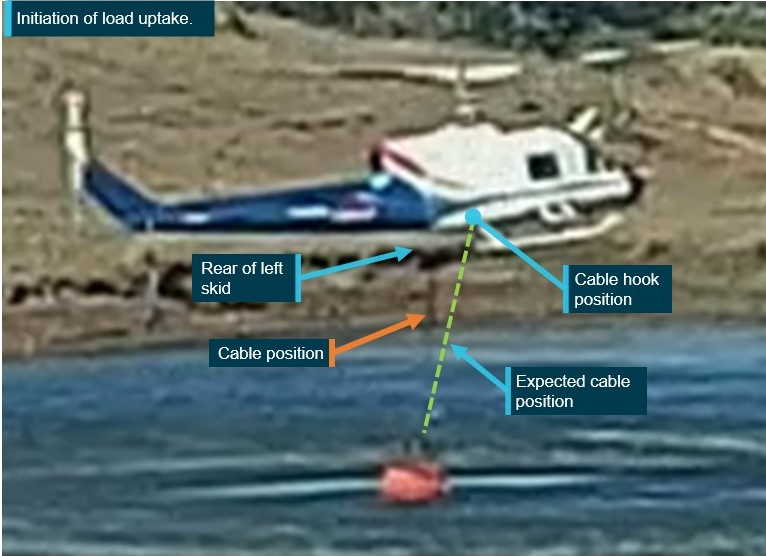
Control of a Bell 204 helicopter was lost during water uplift due to the cables attaching its firefighting bucket being captured over its left rear skid, creating a shift in the centre of gravity.
The helicopter had been tasked on firefighting operations on the afternoon of 20 September 2023 when it approached the dam on a property at Tarome, in Queensland’s south-east, the final report from the ATSB’s investigation into the accident details.
“The cables attaching the Bambi Bucket to the helicopter had been caught over the left rear skid by the time the helicopter was on approach to the dam and when it was uplifting water into the bucket,” said ATSB Director Transport Safety Kerri Hughes.
“As a result, due to the tethered weight over the left rear skid, when the pilot began lifting the bucket from the dam, the helicopter’s centre of gravity moved aft and left. This created asymmetric lift loads, resulting in the helicopter’s loss of control.”
The helicopter struck the water, and the pilot reported that it became inverted almost immediately, filled with water, and began sinking to the bottom of the dam.
The pilot initially tried escaping the sinking helicopter via the front left door. Unable to open it, they swam to the rear of cabin, by which stage the helicopter was almost fully submerged. Following attempts to open the rear right door and kicking out the windows, they escaped by opening the left rear door after applying considerable force.
“The pilot had undertaken HUET – helicopter underwater escape training – about 2.5 years prior to the accident, which increased their chances of survival when the helicopter submerged in the dam,” Ms Hughes said.
“Helicopters tend to be ‘top heavy’, thanks to their engine/s, transmission and main rotor system being above the cabin, and so can flip over quickly once hitting water. As such, this accident reinforces just how important conducting HUET is to increasing helicopter occupants’ chances of survival in the event of impact with water.”
The accident also emphasises the complex nature of conducting external load operations over water, where research has shown that the risk of an accident involving a firefighting helicopter is twice as high as private helicopter operations.
“There can be a lack of visual references, visual illusions over water, limited visibility and vertical reference of the hook and external load through mirrors and bubble windows, which all add complexity when operating helicopters with external loads over water,” Ms Hughes said.
“Fouling of external load suspension cables on the airframe can lead to rapid changes in weight distribution, asymmetric lift and loss of control.
“As Australia moves into another fire season, this accident investigation highlights how correct cable positioning is vital to the safety of external lift operations.”
The ATSB has released a preliminary report from its continuing investigation into a mid-air collision involving 2 Robinson R22 helicopters at Mount Anderson Station in Western Australia’s Kimberley region.
The report details that on the morning of 25 July 2024, 4 R22 helicopters were being prepared to take part in mustering along a section of the Fitzroy River, about a 10-minute flight from the station homestead.
The 2 accident helicopters had been parked in a grassed clearing near the homestead, while the other 2 R22s were parked about 400 m to the west.
Shortly after 0600 the 2 accident helicopters took off from the clearing and began flying to the west towards the other 2 helicopters, which were then to follow them to the muster site.
As they approached the second pair of helicopters, the airborne R22s collided. With their pilots unable to maintain control, the helicopters collided with terrain. Both pilots were fatally injured.
“The pilots of the third and fourth helicopters observed the accident helicopters flying towards them at a height of about 100 ft, with one helicopter flying behind, and below, the other,” said ATSB Director Transport Safety Dr Stuart Godley.
“Wreckage examination found damage to the right side of one helicopter which was consistent with a rotor blade strike from the other, while there was no evidence of an in-flight break-up, or any loss of flight control continuity prior to the collision.”
To date, the ATSB investigation has included examining the accident site and wreckage, collecting meteorological data and operator, pilot and aircraft-related records, and conducting interviews with involved parties.
“As the investigation continues, it will include further examination and analysis of weather conditions, helicopter components, witness information, recorded audio, electronic items retrieved from the accident site, pilot qualifications, operational documentation,” Dr Godley said.
Following the accident, the operator conducted a review of the operations manual and revised procedures for operations involving multiple aircraft and the operation in the vicinity of other aircraft, the preliminary report details.
The ATSB will release a final report, which contain findings and analysis, at the conclusion of the investigation.
“However, should we identify a critical safety issue during the course of the investigation, the ATSB will immediately notify relevant parties so safety action can be taken,” Dr Godley noted.
On the afternoon of 11 September 2024, the pilot of a Kawasaki 47GB3‑KH4, registered VH‑BEU and operated by Katherine Helicopters, was conducting a scenic flight over Nitmiluk (Katherine) Gorge, Northern Territory with 2 passengers on board.
About 13 minutes into the flight, while entering the mouth of the gorge, the pilot reported experiencing an engine power loss and lack of response from the engine. Due to inhospitable terrain in the area, the pilot identified a clear landing spot some distance away and attempted a forced landing at that location, during which time the aircraft collided with terrain.
The pilot and both passengers were uninjured in the incident, however, the aircraft was substantially damaged.
What the ATSB found
Several possibilities were considered during the investigation in relation to the reported engine power loss. While the ATSB did not conduct a physical inspection of the engine in this instance, a post‑incident inspection revealed that a large crack had developed in the engine exhaust pipework. Being a turbocharged engine, the escape of exhaust gases through the crack during operation has likely resulted in an engine power loss during flight due to the loss of boost pressure.
The ATSB also identified that the pilot was unable to cushion the landing during termination of the autorotation, likely due to low main rotor RPM, resulting in the helicopter colliding with terrain.
Safety message
Helicopter operations over harsh terrain offer limited safe emergency landing options. Autorotation to a suitable area in such circumstances requires accurate helicopter positioning and energy maintenance (airspeed and rotor RPM). This makes thorough and regular training in emergency procedures crucial for pilots operating in these demanding environments. The prompt action taken by the pilot, in identifying a suitable landing site, was instrumental in ensuring the safety of all personnel on board.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 11 September 2024, the pilot of a Kawasaki Heavy Industries 47GB3‑KH4, registered VH‑BEU and operated by Katherine Helicopters, was conducting scenic flights over Nitmiluk (Katherine) Gorge, Northern Territory.
During the morning, the pilot conducted the required daily checks on the helicopter and completed a passenger flight over the gorge (Figure 1). After returning to base, the pilot refuelled the helicopter and completed short, uneventful ferry flights to Katherine Museum and return.
That afternoon, the pilot met 2 passengers at the operator’s base, and then completed the flight manifest including the passengers’ weight details, based on verbal information provided by the passengers. The pilot carried out their pre-departure checks, including a flat‑pitch check,[1] which were all normal. A safety briefing was also undertaken with both passengers, which reportedly included:
use of seatbelts
in‑flight procedures
operation of the doors and emergency exits
actions to be taken in case of an emergency.
At around 1451 local time, the helicopter departed and after making a turn towards the north, the pilot gradually climbed to about 1,000 ft above mean sea level (AMSL), proceeding north‑easterly along the Katherine River in the direction of the gorge.
About 10 minutes later, the pilot climbed further to a height of about 1,400–1,500 ft AMSL to fly neighbourly[2] while approaching the escarpment bordering Nitmiluk National Park (Figure 2). The pilot then arranged separation with the pilot of a second helicopter in the area, using the common traffic advisory frequency (CTAF).
Figure 2: View from helicopter of Nitmiluk National Park
Source: Passenger photograph, annotated by the ATSB
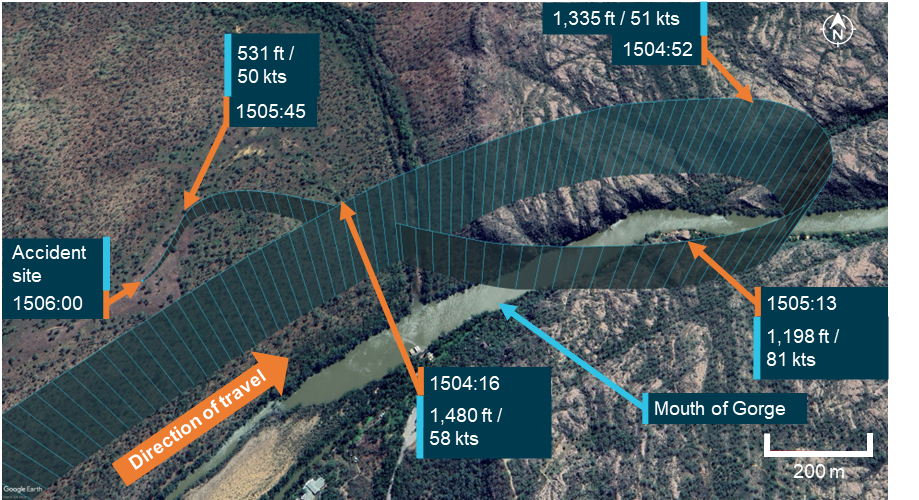
Approximately 3 minutes later, as the helicopter was entering the mouth of the gorge, the pilot noticed that the engine did not respond when they increased the throttle, and that the helicopter was decelerating and losing height. Due to being overhead undulating rocky terrain, the pilot commenced a right turn in search of a suitable landing site, in case they had to conduct a landing (Figure 3).
The pilot reported that the ensuing events occurred extremely quickly. While turning around, the helicopter kept slowing and the engine did not respond to throttle movements. They noticed a significant change in the engine noise, described as a low‑pitched ‘whir’ sound, and reported feeling stiffness in the pedals. Not knowing what was wrong with the engine, the pilot lowered the collective[3] and entered autorotation (see the section titled Autorotation).
During the descent, the pilot glanced at the instruments and noted that the engine RPM needle was split[4] from the main rotor RPM needle and again tried unsuccessfully to increase the throttle. The pilot later advised that the main rotor RPM was well below the green arc on the gauge, and the engine RPM was just below idle. The pilot reported identifying a landing site in a clearing about 400–500 m to the west of their location and broadcast a MAYDAY[5] call on the CTAF.
The helicopter proceeded downwind towards the clearing, attaining a maximum groundspeed in excess of 83 kt. Given the prevailing wind, that equated to an airspeed of about 70 kt, which was higher than the recommended autorotation speed for the helicopter type (see the section titled Autorotation). However, during the final approach to the selected landing site, the groundspeed, and given the crosswind approach, also airspeed was reduced to about 50 kt.
Figure 3: Helicopter flight path with identified elevation and ground speed
Source: OzRunways data on Google Earth, annotated by the ATSB
The passengers reported that during the descent, communication from the pilot was minimal. They were not advised by the pilot to brace for impact; however, upon hearing the MAYDAY call and seeing the pilot attempt an unexpected landing, both passengers suspected that an emergency situation had developed, and chose not to interrupt the pilot or distract them from their actions.
The pilot reported that, on nearing the landing site, they attempted to flare the helicopter but there was minimal flare effect, which they assessed was most likely due to low main rotor RPM. Consequently, the pilot attempted a run‑on landing, during which the helicopter collided with terrain, damaging its tail rotor/shaft and skids (Figure 4).
Figure 4: Helicopter accident site
Source: Operator
After landing, the pilot shut off the fuel, magnetos and battery. After checking on the passengers, the pilot disembarked the aircraft, ensured it was safe to exit with the main rotor blades still rotating, and then instructed the passengers to evacuate the aircraft. The pilot of the other helicopter operating in the area repeated the MAYDAY call on the area frequency and then circled overhead the accident site. A rescue crew arrived onsite shortly after and the pilot and both passengers were evacuated uninjured.
Context
Pilot information
The pilot held a commercial pilot licence (helicopter) and a class 1 aviation medical certificate. At the time of the incident, they had accumulated about 380 hours total aeronautical experience. All the pilot’s training and most of their flying experience has been obtained operating Robinson R44 helicopters. They had been flying for Katherine Helicopters for about 3 months.
While at Katherine Helicopters, the pilot received their Bell 47 endorsement after undergoing about 3 hours of training with an instructor that included the conduct of emergency procedures. The pilot also performed about 10 hours of in command under supervision (ICUS)[6] training with the operator.
Operator information
The operator was a helicopter tour operator based in Katherine, Northern Territory. It operated 2 Bell/Kawasaki 47 Helicopters and offered tour flights throughout northern Australia.
Previous incidents
The pilot had been involved in another engine failure incident on a second helicopter of the same type with the operator in July 2024, wherein an engine cylinder failed. The pilot completed a successful autorotation and there were no reported injuries. While this matter was reported to the ATSB, it was not investigated.
In addition to the incident above, the other helicopter operated by the operator was involved in a third off field landing, arising from an engine fault, in February 2024.
Helicopter information
The helicopter was a Kawasaki Heavy Industries 47G3B‑KH4, manufactured in 1969 in Japan by Kawasaki Heavy Industries and first registered in Australia on 20 June 1996. At the time of the accident, VH‑BEU had about 7,495 hours total time in service and had flown about 40 hours since its last periodic service inspection.
Engine and turbocharger system
VH‑BEU was powered by a Textron Lycoming TVO‑435, 6‑cylinder, vertical direct drive, horizontally opposed, turbocharged engine. The turbocharger increases the density of the carburettor inlet air to maintain the available power as altitude increases.
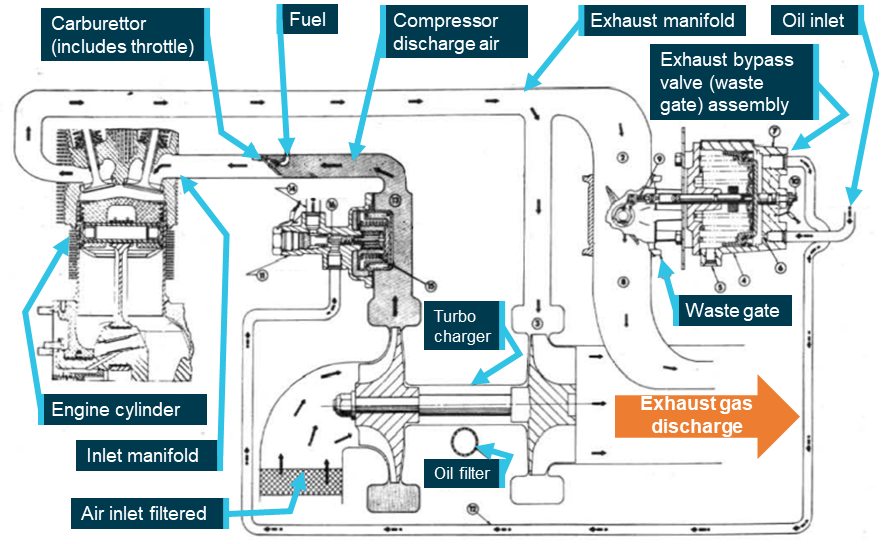
During operation, the exhaust gases expelled from the 3 cylinders on either side of the engine are merged into a single pipe, through which the gases are diverted either to the turbocharger or to the exhaust bypass valve (waste gate), or both (Figure 5).
As the engine power is increased, oil pressure builds up in the exhaust bypass valve assembly and the waste gate in the exhaust system is closed. This diverts the exhaust gas to the turbocharger turbine wheel, compressing the intake air and increasing the available engine power output.
Figure 5: Schematic diagram of engine and turbocharger operation
Source: Lycoming Operator’s Manual, annotated by the ATSB
Maintenance history
As part of the investigation, the ATSB requested the maintenance logs and component log cards for the aircraft. Although the provided information was incomplete, the maintenance history was able to be inferred from the supplied documents as follows:
Lycoming engine TVO‑435, S/N: L‑751‑52 was installed February 2000 at 6,752 airframe hours. The engine component control card showed a number of zero‑hour components at the time of engine installation, indicating that this engine was likely either a new or overhauled unit. Lycoming Service Instruction No. 1009BE specified a 12‑year, 1,000 hour time between overhauls (TBO). This interval was correctly annotated in the engine log card.
The engine was removed on 24 February 2014 (+14 years) at 7,088 airframe hours (+336 engine hours), and was bulk stripped in lieu of being overhauled, to satisfy the requirements of CASA air worthiness bulletin (AWB) 85‑5 Issue 1.[7] The same engine was refitted on 20 March 2014.
The information supplied to the ATSB showed that prior to November 2022, the aircraft flew only limited hours, having recorded 425 airframe hours in 22 years (at an average of 19.3 hours/year). Depending on how these hours were flown,the aircraft may have required special maintenance actions and/or storage procedures. If these actions were not taken, corrosion, or contamination of components may affect serviceability. No record of storage or preservation penalty maintenance was identified in the provided records.
Autorotation
When an engine failure occurs in a single‑engine helicopter such as the Kawasaki 47GB3‑KH4, the pilot must immediately lower the collective and enter autorotation to reduce rotor drag sufficiently to maintain normal rotor RPM. This is a power‑off manoeuvre wherein the engine is disengaged from the main rotor and the rotor blades are driven solely by the upward flow of air through the rotor during descent. The most common reasons for an autorotation are an engine or drive system failure. If the engine fails, the freewheeling unit[8] automatically disengages the engine from the main rotor, allowing it to rotate freely. The tail rotor, still driven by the main rotor transmission, continues to provide yaw control via the anti‑torque pedals.
The United States Federal Aviation Administration Helicopter Flying Handbook noted that the rate of descent during autorotation is influenced by various factors, including:
bank angle
density altitude
gross weight
main rotor RPM
trim condition
airspeed.
Pilots control the autorotative descent rate using airspeed and main rotor RPM. Airspeed is managed with the cyclic[9] pitch control, similar to normal powered flight. The descent angle can range from vertical to a minimum angle for maximum horizontal range. The rate of descent is highest at zero airspeed, reaches its minimum at approximately 50–60 kts (depending on the helicopter and conditions), and increases again at higher speeds.
During an autorotative landing, the kinetic energy associated with the helicopter’s airspeed and rotating main rotor blades are used to arrest the descent and cushion the landing. Termination of the autorotation usually involves initially flaring the helicopter to reduce the airspeed, rate of descent and, if necessary, increase the rotor RPM. The degree of flare effect is influenced by both the airspeed at the time aft cyclic is applied, as well as the rate of cyclic application.
Autorotative terminations at very low airspeeds are more challenging than those performed at the minimum rate of descent airspeed as they offer minimal flare effect. In that case, cushioning the landing using the stored rotor energy requires more precise collective application.
The Kawasaki 47G3B-KH4 flight manual stated that, in the case of an engine failure, the pilot must:
execute a normal autorotative descent and establish a level attitude prior to ground contact. At a height of approximately 10 feet above the ground, apply collective pitch in sufficient quantity to stop descent as ground contact is made. The best descent speed is 55 mph [48 kt].
Meteorological information
At the time of incident, visibility was in excess of 10 km, with scattered cloud[10] well above the aircraft operating height, no precipitation and an east‑south‑easterly wind at 11 kt.
The meteorological conditions reported by the pilot at the time of incident were consistent with the Bureau of Meteorology observations, which recorded a temperature of 36°C and dew point[11] of 11°C at the incident location.
The process of vaporising fuel in a carburetted engine can cool the airflow sufficiently to permit ice formation in the carburettor throat that restricts airflow to the engine. According to the Civil Aviation Safety Authority Carburettor icing probability chart, the probability of carburettor icing, based on the prevalent temperature and dewpoint at Katherine Gorge was on the outer limit of the ‘light icing – cruise or descent power’ zone. Of note however, the turbocharger compressor used in the Kawasaki 47G3B‑KH4 heats the inlet air to the carburettor, significantly reducing the potential for carburettor icing.
Operating weight
The passenger manifest completed by the pilot prior to take‑off recorded the empty weight of the aircraft, the pilot and both passengers, plus fuel. An allowance of 100 kg was made for the weight of fuel. The passenger weights were only verbally requested, and not physically checked by the pilot. However, the calculated total take‑off weight was well below the maximum take‑off weight so any inaccuracy in passenger weights was unlikely to have resulted in the aircraft being overloaded.
Aircraft fuel
The operator conducted an examination of the fuel in the aircraft following the incident and reported to the ATSB that there was adequate fuel remaining in the tank.
The operator also stated that the aircraft had been refuelled with premium 130 octane fuel by the pilot prior to take‑off, and that a post‑incident examination of the fuel quality did not reveal any signs of contamination or leakage.
Engine examination
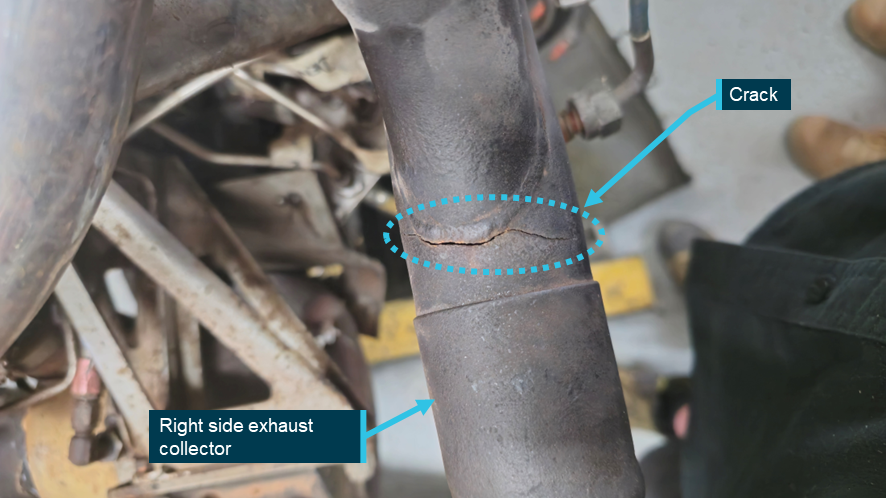
Following the incident, the operator started the Lycoming TVO‑435 engine and observed that the wastegate did not operate. Thereafter, they removed the engine and delivered it to a third party maintenance facility for examination. As depicted in Figure 6, the post‑incident inspection of the engine revealed the presence of an approximately 6.5 cm crack on the right exhaust collector, with no other defects identified.
The exhaust system of the aircraft engine attains extremely high operating temperatures. The consequent widening of the crack due to heat expansion would result in the escape of exhaust gases from the defective section, resulting in inadequate drive pressure for the turbocharger compressor and reduced power output. Information provided by the engine manufacturer supported that conclusion. As such, exhaust gas bleed from the crack before the turbocharger resulted in the wastegate remaining closed.
The ATSB did not undertake a metallurgical analysis of the exhaust pipe, however, exhaust systems are generally prone to metal fatigue over time due to continuous vibration under corrosive conditions and a cyclical pattern of constant heating and cooling with extreme thermal fluctuations.[12]
While it could not be established when the exhaust crack occurred, the maintenance facility that conducted the post‑accident engine examination assessed that, based on the location and appearance of the defect, it was likely not impact‑related. They further stated that, as the helicopter did not have an engine cowl, the leaking exhaust gases would not have left a residue. This would have made the crack more difficult to detect during a pre‑flight inspection when the engine was cold.
Figure 6: Cracked exhaust collector pipe
Source: the maintenance facility that conducted the engine strip down inspection, annotated by the ATSB
Safety analysis
Engine power reduction
The sequence of events described by the pilot and passengers were consistent with a loss of aircraft engine power during flight, necessitating an emergency landing. The ATSB considered the following potential reasons for the reduction in engine power:
weather conditions, including carburettor icing
fuel contamination or starvation
handling‑related issues
engine and/or associated systems defect.
The evidence gathered by the ATSB during the investigation indicated that the 3 initial possibilities were unlikely.
However, based on information from the engine manufacturer and the personnel that conducted the post‑accident engine examination, a pre‑existing crack in the exhaust collector likely reduced the engine power output during the flight.
Helicopter maintenance
The ATSB identified that low utilisation of the helicopter may have required special maintenance actions and/or storage procedures to be undertaken to prevent component corrosion or contamination. While there was no evidence that such maintenance was undertaken, it was not possible to determine whether its absence contributed to the crack in the exhaust system.
Autorotation
Analysis of flight data identified that the helicopter was over inhospitable terrain at the time of the power loss. After turning towards a suitable landing site, the pilot commenced an autorotation to that location. The helicopter proceeded downwind, initially attaining a maximum airspeed of about 70 kt. The airspeed was then reduced to close to the target minimum rate of descent airspeed of 48 kt, providing good potential flare effect to both slow the helicopter prior to touchdown and increase the rotor RPM if necessary.
Despite that, the pilot reported there was minimal flare effect when they approached the landing site, likely due to low rotor RPM. As a result, the pilot was unable to prevent the helicopter colliding with terrain during the termination. Importantly however, none of the occupants were injured.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Kawasaki 47G, VH‑BEU, 24 km north of Katherine Tindal Airport, Northern Territory on 11 September 2024.
Contributing factors
The right exhaust collector was found to have developed a significant crack, which likely resulted in engine power loss during flight.
The pilot was unable to cushion the landing during termination of the autorotation, likely due to low rotor RPM, resulting in the helicopter colliding with terrain.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot and passengers of the accident flight
the operator
the maintainer for VH-BEU
Civil Aviation Safety Authority
accident witness
OzRunways data from the pilot’s iPad
Bureau of Meteorology
Kawasaki Heavy Industries
the maintenance facility that conducted the post‑accident engine examination.
References
U.S. Department of Transportation Federal Aviation Administration Helicopter Flying Handbook, FAA‑H‑8083‑21B (2019).
Lycoming Service Instruction No. 1009BE (2020).
Reciprocating engine and exhaust vibration and temperature levels in general aviation aircraft, U.S. Department of Transportation Federal Aviation Administration (1968).
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of the accident flight
the operator
the maintainer for VH‑BEU
Civil Aviation Safety Authority
Kawasaki Heavy Industries
Textron Lycoming
United States National Transportation Safety Board
Japan Transport Safety Bureau
Submissions were received from:
the pilot of the accident flight
the operator
Civil Aviation Safety Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
[1]The flat pitch is the power it takes to run the helicopter at 100% rotor RPM on the ground with the collective lever fully lowered. A helicopter flat pitch check is performed pre‑flight to identify any engine performance trends by monitoring manifold pressure.
[2]Flying neighbourly is a concept aimed at minimising the noise impact of helicopter operations on local communities.
[3]Collective: a primary helicopter flight control that simultaneously affects the pitch of all blades of a lifting rotor. Collective input is the main control for vertical velocity.
[4]The term used to describe the position of the 2 needles on the combined engine/rotor tachometer when the 2 needles are not superimposed. When a helicopter enters autorotation, either due to an engine failure or during practice, the needles split as the rotor system drive disengages from the engine. This indicates that the main rotor is no longer being powered by the engine and is instead being driven by the upward airflow through the rotor disc.
[5]MAYDAY: an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
[6]ICUS (In Command Under Supervision) operations enable pilots having the relevant aircraft type endorsement to gain command experience and accumulate flight hours when performing pilot‑in‑command duties under supervision.
[7]The AWB provided guidance on engine bulk strip for the purpose of extending calendar life, in instances where engine calendar life limit was reached before reaching the hourly TBO.
[8]The freewheeling unit is a mechanism that automatically disengages the engine from the main rotor when engine RPM falls below rotor RPM, allowing continued rotor rotation during autorotation.
[9]Cyclic: a primary helicopter flight control that is similar to an aircraft control column. Cyclic input tilts the main rotor disc, varying the attitude of the helicopter and hence the lateral direction.
[10]Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – scattered indicates cloud covering between a quarter and a half of the sky.
[11]Dewpoint: the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to predict the probability of aircraft carburettor icing or the likelihood of fog.
[12]US Department of Transport FAA Report No. NA‑68‑27.
Occurrence summary
Investigation number
AO-2024-050
Occurrence date
11/09/2024
Location
24 km north of Katherine Tindal Airport
State
Northern Territory
Report release date
09/05/2025
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Engine failure or malfunction, Forced/precautionary landing
On 18 June 2024, at about 0325 local time, a Pilatus PC-12/47E was conducting a non‑scheduled medical transport flight from Newman Airport to Nullagine ALA, Western Australia. The pilot, along with 2 medical crew members and a patient, were on board.
The aircraft overflew the airport and joined upwind for a circuit to land on runway 32. Due to the flight being conducted at night, the pilot could not conduct a low level pass to ensure the runway was clear. During the landing roll, at approximately 60 kt, the pilot observed a cow to the left of the runway and applied maximum braking and reverse thrust. The pilot turned right to avoid the cow, however the aircraft struck another unobserved cow, which impacted the nose and left wing of the aircraft. The pilot secured the aircraft, ensured the crew members and patient were uninjured, and conducted an inspection. The aircraft sustained substantial damage to the propellor, engine, left wing and landing gear.
Figure 1: Aircraft damage
Source: Supplied
Safety action
The aerodrome operator has taken action to update the Nullagine entry in the En Route Supplement Australia (ERSA)[1] to include information about the risk of wildlife hazards on the runway and plans to repair damaged aerodrome fencing.
The aircraft operator has updated their Airstrip Directory for Nullagine ALA to include a note that the fencing is in a state of disrepair and the vermin risk has been elevated from medium to high with a requirement for mandatory wildlife/stock inspections day and night.
Safety message
Where an ongoing wildlife hazard to safe aircraft operations exists, aerodrome operators should include an appropriate warning in the ERSA.
Ground-based animal strikes can pose a serious safety risk for aircraft, as found in the ATSB research report, Australian aviation wildlife strike statistics(AR-2018-035). Pilots should mitigate this risk as best they can by maintaining adequate situational awareness, particularly when operating at regional strips known for significant wildlife hazards.
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]En Route Supplement Australia (ERSA): a directory for Australian aerodromes that includes details of an aerodrome and details of available air traffic and ground services, navigation aids and public facilities and any special procedures.
Occurrence summary
Mode of transport
Aviation
Occurrence ID
AB-2024-028
Occurrence date
18/06/2024
Location
Nullagine
State
Western Australia
Occurrence class
Accident
Aviation occurrence category
Animal strike
Highest injury level
None
Brief release date
20/09/2024
Aircraft details
Manufacturer
Pilatus Aircraft Ltd
Model
PC-12/47E
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
Departure point
Newman Aerodrome, Western Australia
Destination
Nullagine Aircraft Landing Area, Western Australia
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 1 June 2024, an Aerospatiale AS.350BA helicopter with a pilot and observer on board, was tasked to conduct a welfare search for some hikers in Kakadu National Park in the Northern Territory. The crew of 2 (pilot and crewman/spotter) had been briefed that 2 vehicles carrying up to 10 people had entered the park and were hiking in an area that had recently been burned as part of ongoing aerial incendiary operations.
The flight departed Jabiru Airport at 1516 local time, and the 2 vehicles and 6 hikers were located a short time later. The helicopter flew up a small valley to locate the additional hikers. Finding none, the decision was made to land and make positive contact with the hikers to determine if these 6 were the entire group or if there were others unaccounted for. The pilot identified an area on a rock shelf in a creek bed which they assessed as suitable for landing. A reconnaissance was carried out during a descending orbit, making a final approach into wind facing the nearby hikers.
Approaching the hover, the pilot noted a rocky outcrop to the right; assessing it to be far enough away to clear the main rotor the pilot then focused on the uneven touchdown area below. Just prior to touchdown there was a loud noise and a jolt followed by severe vibration. Realising that the main rotor had contacted the rock outcrop, the pilot manoeuvred the helicopter about 1–2 metres to the left and landed immediately.
The helicopter was shut down and the crewman instructed to exit once movement had stopped. The pilot then exited and, noticing that the helicopter began to rock backwards, stood on the right front landing gear skid while the crewman and hikers propped the left rear skid shoe with loose rocks to secure it (Figure 1).
There was significant damage to the helicopter tail boom and main rotor blades, as shown in Figures 2 and 3.
Following this accident, the company has implemented the following:
Review of the company operations manual (COM) procedures for the selection, assessment, and use of unprepared helicopter landing sites.
Develop a specific ‘GO – NO GO’ guidance tool for pilots to assess the urgency of landing against the complexity of the landing site available.
Develop specific advice in the COM regarding acceptable distance and buffers from obstacles having regard to the nature of the obstacle (e.g. tall grass vs. trees vs. rocks) as well as varying capabilities and experience of pilots.
Review of confined area sites used in training at the company offsite location to determine if these are adequately ‘complex’ to reflect those likely to be encountered operationally.
Incoming pilots to receive practical refresher training based on this occurrence including crew resource management.
The occurrence will be used as a flight training case study.
Safety message
This accident highlights the need tothoroughly assess the suitability of all landing sites and complete a 360° reconnaissance prior to landing. A full reconnaissance of the landing site probably would have allowed the pilot to make a better assessment of the height of the rock shelf and the limited size of the landing area.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
The ATSB has released its preliminary report from its on-going investigation into a collision with terrain involving a Cessna 172 during mustering at Mulgathing Station in central South Australia.
The preliminary report details factual information established in the investigation’s early evidence collection phase. It does not contain analysis or findings, which will be detailed in the final report to be released at the conclusion of the investigation.
The single-engine Cessna was being used for sheep spotting operations, flown by a solo pilot, on 27 June 2024.
At about 0810 local time, a witness on a motorbike about 500 m away observed the aircraft dive down on what they presumed was a mob of sheep, to an altitude of about 50 ft above the ground, before climbing rapidly, turning to the left and then nosediving towards the ground.
The pilot was fatally injured and the aircraft was destroyed in the accident.
ATSB investigators deployed to the site and found the aircraft impacted in about a 70° pitch down attitude, with ground impact marks directly under the nose showing no forward momentum.
“Investigators did not identify any pre-existing faults or pre-impact defects with the aircraft’s flight controls and structure,” Director Transport Safety Kerri Hughes said.
“Additionally, one of the propeller blades showed significant rotational abrasion damage and chord-wise twisting indicating that the engine was driving the propeller under significant power at the time of impact.”
Along with an on-site examination of the wreckage, to-date ATSB investigators have interviewed witnesses and gathered electronic devices from the accident site.
As the investigation progresses, it will include consideration of witness information, and examination of a GPS device recovered from the site, the aircraft’s maintenance history, aircraft weight and balance, performance considerations, meteorological conditions, the impact sequence and survivability.
“Investigators will also consider the conduct of similar flight operations, pilot qualifications and the regulatory requirements for fixed-wing aerial mustering,” Ms Hughes said.
“Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.”
A final report will be released at the conclusion of the investigation.
An incident in which a King Air pilot encountered instrument failure and control issues over Western Australia is a reminder of the value of aircraft system knowledge and pilot operating handbook familiarity, an ATSB final report notes.
On 25 January 2024, the twin turboprop King Air C90A aircraft departed Kalgoorlie-Boulder Airport for a charter flight to Warburton, with one pilot and two passengers on board.
About half an hour into the flight, operating in instrument meteorological conditions, the pilot was cleared by air traffic control to divert left of track to avoid a storm.
With the autopilot in heading mode, the pilot used the heading bug on the horizontal situation indicator to track left. Once past the storm, the pilot changed the heading setting to the right, to re-intercept the original track.
“Unknown to the pilot, the aircraft’s remote gyroscope had failed, resulting in erroneous indications on the horizontal situation indicator,” Director Transport Safety Stuart Macleod said.
This resulted in a sustained, uncommanded right turn.
Observing the aircraft continue to turn right through the selected heading, the pilot disengaged the autopilot and hand-flew the aircraft onto the correct heading.
During the manoeuvring, altitude variations between -400 ft and +900 ft were recorded on ADS‑B tracking services.
Having observed the aircraft deviate laterally and vertically, the monitoring air traffic controller queried the pilot’s intentions several times.
“The combination of manually flying in instrument meteorological conditions, troubleshooting and interactions from ATC resulted in a high workload situation for the pilot,” Mr Macleod observed.
A short time later, contrary to the pilot operating handbook, the pilot re-engaged the autopilot in heading mode, and made continual left inputs to the heading bug to keep the aircraft tracking left.
“This contributed to high workload and sustained control issues,” Mr Macleod said.
“Additionally, the pilot not making a PAN PAN broadcast to ATC reduced the opportunity for the controller to provide appropriate assistance.”
The pilot elected to return to Kalgoorlie, and landed without incident.
The ATSB’s final report notes the occurrence highlights the value of aircraft system knowledge and pilot operating handbook familiarity in resolving malfunctions.
“This incident emphasises the importance of pilots utilising all options to reduce their workload, including requesting assistance from air traffic services when they recognise an emergency situation developing,” Mr Macleod said.
“Controllers are also reminded that a pilot in difficulty may not immediately alert air traffic services if they are disoriented or focused on flying the aircraft. If a controller assesses they may be able to assist, this should be communicated proactively.”
On the morning of 15 September 2024, passenger train 7DA8E (also known as ‘The Ghan’) was travelling southbound on the Tarcoola–Darwin railway line toward Alice Springs, Northern Territory, with 218 passengers, 38 service staff and 4 locomotive crew on board.
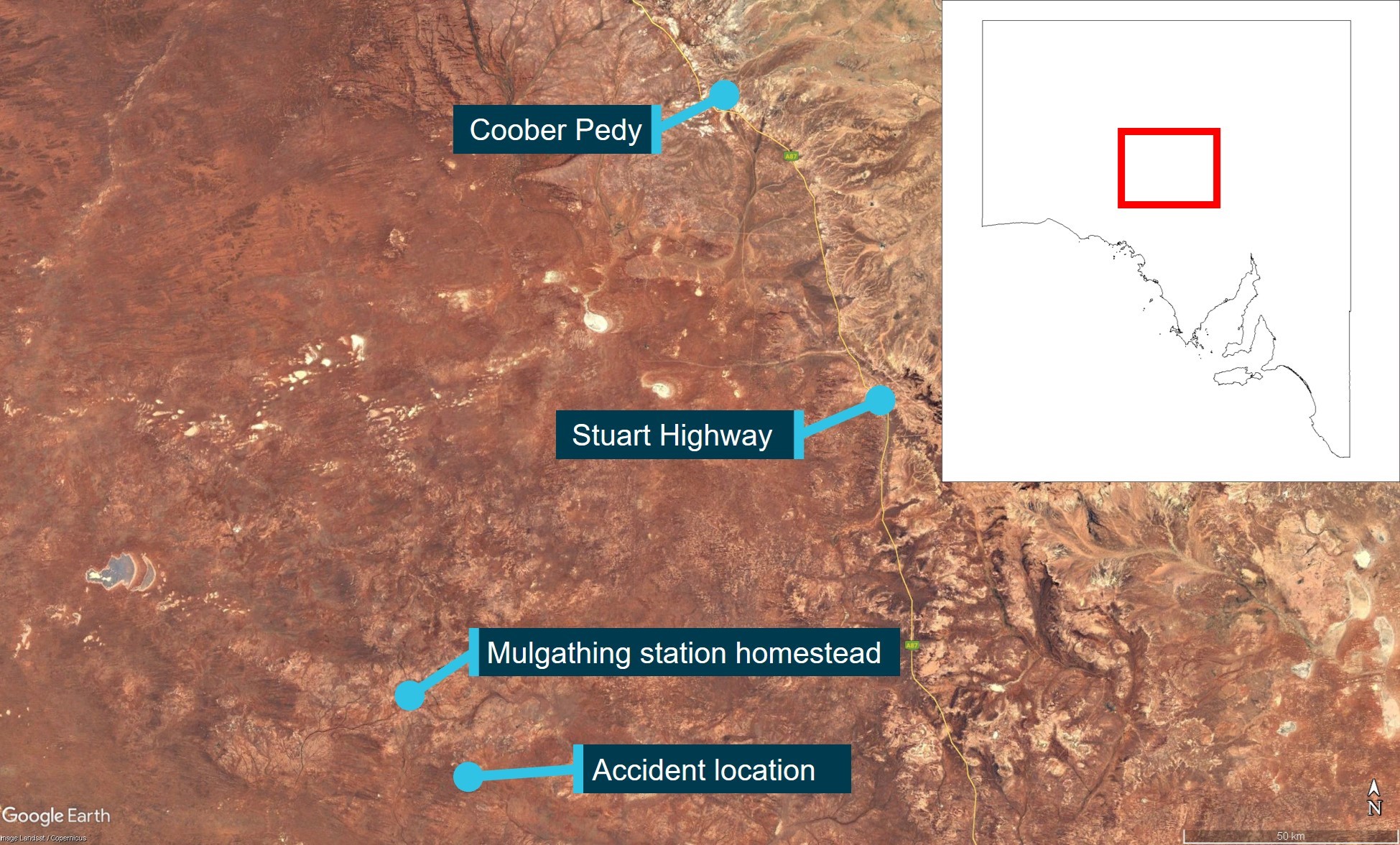
As The Ghan approached a passive level crossing where the railway line crossed with The Garden Road (about 48 km north of Alice Springs), an A-triple truck turned from the Stuart Highway onto The Garden Road and commenced driving east toward the level crossing. Advance road warnings and passive controls, including a stop sign, were installed from the highway turn‑off and along The Garden Road to alert road users of the nearby level crossing.
When The Ghan was approximately 120 m from the crossing, travelling at 108 km/h, the locomotive drivers witnessed the truck emerge from behind roadside vegetation and approach the level crossing. The driver sounded The Ghan’s horn, however, the truck did not stop, it entered the level crossing and collided with the side of the trailing locomotive. The Ghan remained upright and the truck came to rest in the field side of the track.
The truck driver sustained serious injuries and there were no injuries on board The Ghan.
What the ATSB found
The ATSB found that, as the truck was being driven along The Garden Road toward where the road crossed the Tarcoola–Darwin railway line, the truck driver did not slow sufficiently to stop prior to the level crossing, resulting in a collision with The Ghan passenger train.
The ATSB also found that, while some aspects of the level crossing controls were not as per standard or were faded, there was signage and markings for road users to be aware of the crossing and bring their vehicles to a controlled stop before entering. Once stopped, there was adequate visibility for a driver to sight a train and give way.
What has been done as a result
Following the collision, the Department of Logistics and Infrastructure within the Northern Territory Government undertook a series of safety actions at The Garden Road level crossing. The approach signage was upgraded, and the faded road line markings were refreshed. However, some of the approach signage elements remained incorrectly positioned as required by the Australian Standard AS 1742.7.
The interface agreement was revised and renegotiated with the rail infrastructure manager. They further advised that the rail infrastructure manager had committed to install updated signage (R6-25 ‘Railway Crossing’) to meet the current standards at The Garden Road level crossing, and to progressively upgrade signage at other crossings when existing signs were due for replacement.
At a broader level, the department also advised that they delivered a targeted campaign during the August 2025 National Rail Safety Week to raise public awareness of level crossing risks across the Northern Territory. The strategies used during that campaign included social media advertising, learner driver education and displays at the motor vehicle registry.
Safety message
Passive traffic controls such as signage and road markings cannot physically prevent road users from entering a level crossing. Therefore, it remains the responsibility of those users to follow these controls. When required to stop at a level crossing, drivers must stop, sight, and remain clear of all rail traffic. The maximum sighting distance along the rail corridor occurs when a vehicle is stopped at the stop line and provides road users the greatest opportunity to detect for oncoming rail traffic. This is a critical requirement to avoid a collision.
This accident also highlights the notion of heavy vehicle drivers slowly rolling though a stop sign at a level crossing. This action is illegal as stop signs require vehicles to come to a complete stop and can place them and train crew or passengers at imminent risk of significant harm should a collision occur.
The investigation
The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 14 September 2024, passenger train 7DA8E ‘The Ghan’ departed the Berrimah Passenger Terminal in Darwin, Northern Territory, on a scheduled southbound service to the Keswick Passenger Terminal in Adelaide, South Australia, using the Tarcoola–Darwin railway line. On board the train were 4 locomotive drivers, 38 service staff and 218 passengers.
The locomotive drivers were rostered to work in 7‑hour relay shifts as 2 distinct pairs, with 1 pair driving while the other pair rested in the crew cars. After departing Darwin, the train travelled to Katherine and then overnight through to Tennant Creek, Northern Territory. On 15 September, at about 0600, the train was stopped approximately 60 km south of Tennant Creek and a crew change was completed, after which the journey continued toward Alice springs.
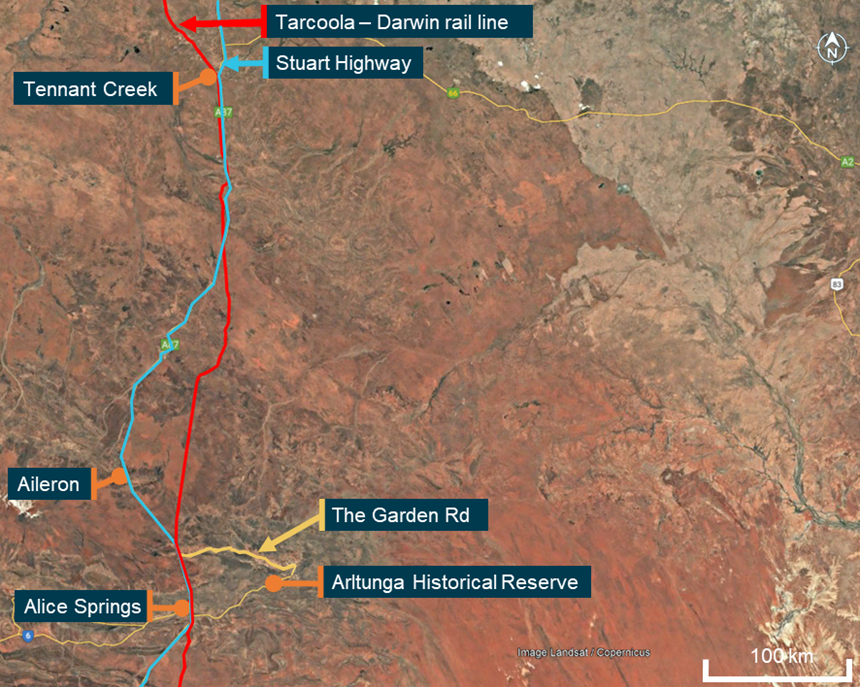
At about 0800 that same morning and 300 km south of Tennant Creek, workers at Aileron Station commenced loading cattle into the wagons of an A-triple road train (truck). The cattle were to be driven along the Stuart Highway and delivered to a remote station on The Garden Road, near the Arltunga Historical Reserve, Northern Territory. The truck consisted of a prime mover and 3 trailers. The front and centre trailers were loaded with cattle while the rear trailer remained empty. At about 0900, the truck departed Aileron and travelled south on the Stuart Highway (Figure 1).
Figure 1: Operations between Alice Springs and Tennant Creek for The Ghan and truck
Source: Google Earth, annotated by the ATSB
At about 0952, the truck turned off the highway at the intersection with The Garden Road. The driver negotiated a curved S‑bend section of the road on the western approach to the level crossing with the Tarcoola–Darwin rail line, which was located about 300 m from the highway intersection (Figure 2).
Figure 2: The Garden Road level crossing and The Ghan and truck directions of travel
Source: Google Earth, annotated by the ATSB
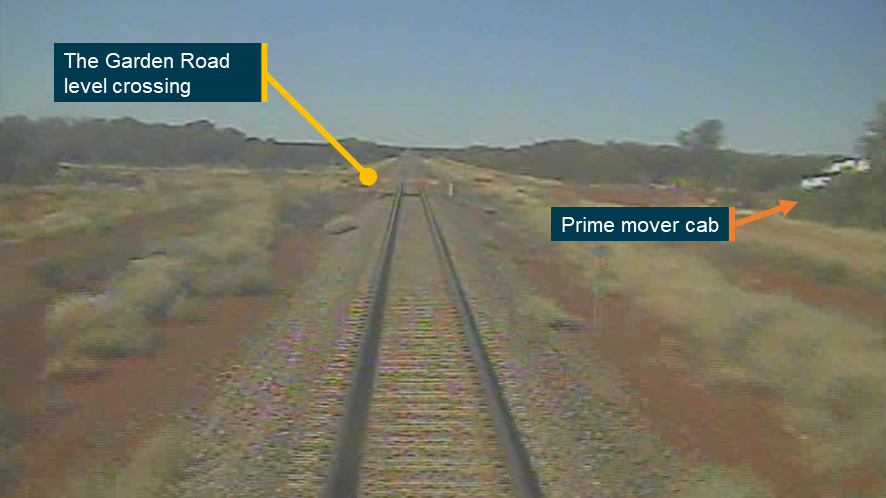
Coincident with the arrival of the truck, The Ghan was also approaching the level crossing. At 0952:44 (about 500 m from the level crossing), a track‑side whistle board[1] was passed and at 0952:53 (about 270 m from the level crossing) the locomotive driver sounded the horn for 2 seconds. When The Ghan was approximately 120 m from the crossing, the crew observed the truck come into full view from behind roadside vegetation and progress toward the level crossing (Figure 3).
A video camera system fitted to the front of The Ghan’s leading locomotive recorded the journey and at 0952:57 showed the truck appear from behind the vegetation. Audio from the recording identified that, at 0952:58, just prior to the level crossing, the driver briefly sounded the horn, and then at 0952:59, blasted it continuously as they travelled through. The truck did not stop and at 0953:02 the front end of the prime mover impacted the right rear bogie[2] of The Ghan’s trailing locomotive.
Figure 3: Field of view from the locomotive camera approximately 120 m from the level crossing showing the prime mover cab as it emerged
This image was obtained from the locomotive video camera as The Ghan travelled southward. Source: Pacific National, annotated by the ATSB
Through the collision sequence, The Ghan remained upright and neither the locomotives nor carriages derailed. At 0953:05, the driver in control of The Ghan reduced the throttle and applied the brakes. Over the next 10 seconds, they initiated a full-service brake application, and the throttle was reduced to the lowest notch. The Ghan came to a controlled stop at 0954, with the lead locomotive 1,380 m beyond the level crossing.
The prime mover of the truck came to rest on the field side of the track with engine bay components scattered along the rail corridor (Figure 4).
Figure 4: The truck at the level crossing after the collision
View looking north along the Tarcoola–Darwin railway line from which The Ghan was travelling. Source: Northern Territory Police
Post-collision management
On coming to a stand, both locomotive drivers exited the cab to assess the damage and secure the train. They subsequently telephoned network control, requested for emergency services, and maintained contact with service staff in the passenger compartments.
The truck driver was able to exit their cab unassisted, however, they had sustained serious injuries. They were attended to by service staff from The Ghan until Northern Territory Police attended the scene at 1027, followed shortly after by the ambulance service at 1029.
There were no injuries to The Ghan train crew, service staff, or passengers on board. The passengers were subsequently detrained and transferred to Alice Springs by bus service.
Context
Operation
The Ghan was a twice-weekly passenger carrying service operating from Darwin to Adelaide in both directions between April and October. The train was operated under accreditation of Great Southern Rail by Journey Beyond, which supplied and staffed the passenger cars. Pacific National supplied and staffed the locomotives. Aurizon was the rail infrastructure manager for the Tarcoola–Darwin corridor on which the train was travelling, and it owned the section of rail corridor between Alice Springs and Darwin.
Personnel information
Train crew
All locomotive drivers were employed by Pacific National. The driver in control was a qualified locomotive driver with 3 years of experience at Pacific National. They had completed their most recent competency verification in the first half of 2024. The driver assisting was also a qualified locomotive driver with over 11 years of experience at Pacific National.
Truck driver
The truck driver had been driving trucks for several years. They stated that, although it was their first time driving a loaded vehicle to the destination cattle station, they were familiar with the area and traversed the level crossing at least once a month. They had not previously encountered a train at The Garden Road level crossing.
They were unable to recall the speed they were travelling as they negotiated the S‑bend on approach to the level crossing, but indicated they would have been driving slowly as their intention was to uncouple the empty rear trailer on the other side of the level crossing. The driver had no recollection of hearing The Ghan’s horn as they approached the level crossing. On seeing the leading locomotive pass closely by the front of their cab, they recalled rapidly applying the trailer handbrake and prime mover footbrake. The truck driver reported they were aware of the stop sign at the level crossing and understood the requirement to stop behind the stop line but noted that the line was faded.
The driver did not recall any mechanical problems with the prime mover or the trailers and stated that the brakes on the truck and trailers were functional. They further stated that they would sometimes roll through level crossings as it required significantly more time and effort to stop a loaded truck and then accelerate than it did to roll through a crossing at low speed.
Vehicle information
Train
The Ghan (train 7DA8E) consisted of 2 NR-class locomotives and 29 Commonwealth Engineering stainless steel passenger and restaurant carriages. The total length of the train was 735 m and it weighed 1,418 t.
The train driver reported operations were normal throughout the journey prior to the collision. There were no mechanical problems with either the locomotives or the consist. Additionally, the locomotive headlights were operating throughout its journey and were illuminated while on approach to the level crossing.
The trailing locomotive sustained extensive damage to the air pipes, side ladder, and front cowling. The power van also received superficial body damage. There was no damage to the other carriages or the lead locomotive.
Truck
The truck was an articulated heavy vehicle, consisting of a Mack Titan prime mover and 3 Haulmark semi-trailers joined to form an A-triple consist. This configuration met the conditions of a Class 2 Road Train under the national standard and was 53.5 m long with a maximum approved weight of 115.5 tonnes.
In their examination of the truck, Northern Territory Police identified tyre skid marks from the prime mover and trailers on the road surface that each extended for approximately 2–3 m immediately leading to the crossing. Tyre defects were identified to all 3 trailers, which included several bald tyres and one shredded tyre.
The attending police also found the driver’s seatbelt was clipped into its buckle and looped back behind the seat. From that, they concluded the belt had not been appropriately fitted around the driver at the time of the collision. It was unknown to what extent the driver’s injuries were related to not wearing their seatbelt.
Recorded information
Data from the locomotive event logger recorded parameters such as throttle position, brake pressure, and speed. The event logger output was matched with the lead locomotive forward-facing video camera to correlate time, distance and speed information. No recorded data was obtained from the truck.
The locomotive camera recorded video at 15 frames per second and showed the journey along the Tarcoola–Darwin line and the arrival at the level crossing. Analysis of the video file identified a 2‑second period where the moving truck came into view. Sounding of The Ghan’s horn was audible within the recording along with the brake application by the train driver after the collision.
Using the video and georeferenced data, ATSB calculation of the vehicle closure speeds and distances showed that the truck was slowing as it approached the level crossing (Table 1). When the prime mover was 34 m from the crossing, it was travelling 30–35 km/h, and when it was 23 m from the crossing it had slowed and was travelling 22–28 km/h. At 0953:02.7, the front of the lead locomotive was approximately 30 m beyond the crossing travelling at 108 km/h[3] when the prime mover collided with the trailing locomotive.
Table 1: Calculated closure distances and speeds between the truck and The Ghan
Time (hhmm:ss.s)
Vehicle distance from the level crossing (m)
Vehicle speed (km/h)
The Ghan
Truck
The Ghan
Truck
0952:57.3
- 120
Not quantifiable
108
Not quantifiable
0952:58.0
- 90
34
108
30–35
0952:59.5
- 60
23
108
22–28
0953:02.7
+ 30
0
108
Collision
Level crossing information
The Garden Road level crossing
The Garden Road was an approved truck route and provided a thoroughfare to the Arltunga Historical Reserve. Prior to 2016, the short section of road from the Stuart Highway turn-off and beyond the level crossing was unsealed and had crossed the railway track at acute angles. In early 2016, the road was sealed and realigned with road markings and warning signs introduced on the approach to the level crossing. The realigned road section contained a dual curve (an S‑bend) and was perpendicular where it crossed the railway line. The changes in road geometry reduced the visibility angle for road users approaching the intersection, in turn increasing the opportunity for rail traffic to be sighted.
Advance warnings and road markings
Australian Standard (AS) 1742.7 (Manual of uniform traffic control devices Part 7: Railway crossings) required the use of signs, road markings and other control devices at railway crossings. The Garden Road level crossing had been constructed with passive traffic controls to protect both the eastern and western approaches. Passive level crossing controls use signage and road markings to warn road users about an approaching level crossing, but do not activate or change when a train is approaching.
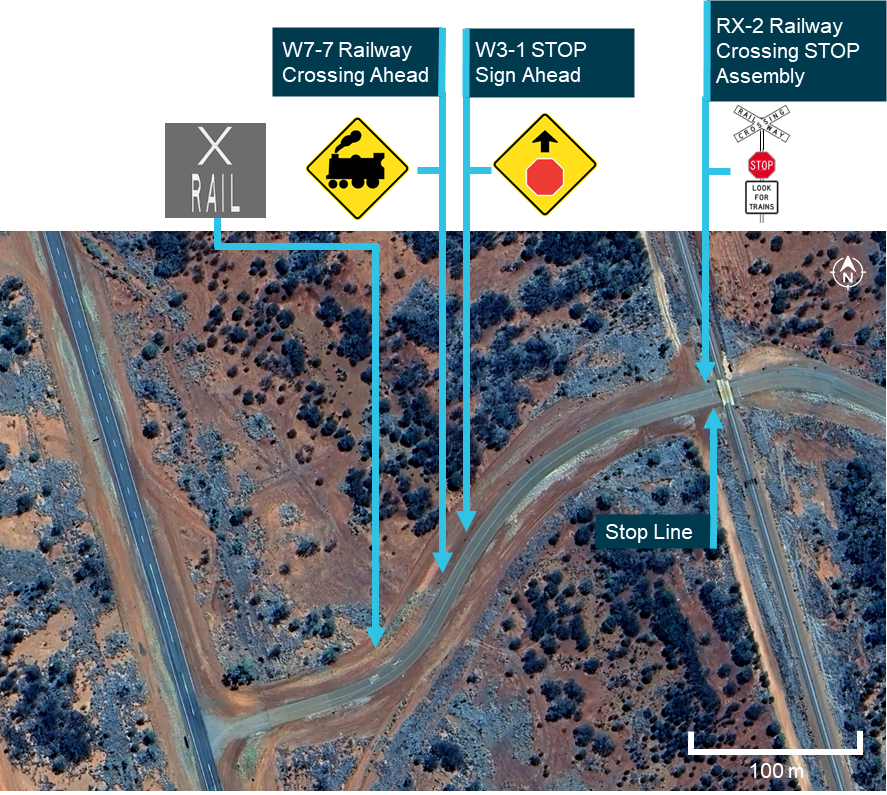
The advance warnings and markings provided along the road on the western approach to the level crossing were:
painted markings ‘RAIL’ and ‘X’ on the surface of the road with an accompanying advance warning ‘Railway Crossing Ahead’ (W7-7 L)
an advance warning ‘STOP Sign Ahead’ (W3-1).
The ‘RAIL’ and ‘X’ painted road markings were positioned approximately 225 m from the level crossing and placed at the first curve of the S‑bend. The advance warning sign ‘Rail Crossing Ahead’ (W7‑7 L) was positioned about 190 m from the crossing, and the second sign in advance of the crossing was a ‘STOP Sign Ahead’ (W3‑1) sign about 165 m from the crossing.
The passive controls installed at the level crossing were a ‘Railway Crossing STOP’ (RX‑2) sign assembly and an accompanying white painted ‘stop line’ on the road surface (Figure 5 and Figure 6). The stop line was 5.2 m from the nearest rail, which was greater than the minimum 3.5 m required by the Australian Standard.
Figure 5: Location of the advance warnings and road markings near the level crossing
Source: Google Earth, annotated by the ATSB
As the speed limit for The Garden Road was over 90 km/h, the Australian Standard required the W3-1 sign to be 180 m to 250 m before the stop sign at the crossing. The W7-7 ‘Rail Crossing Ahead’ sign had to precede the W3-1 ‘Stop Sign Ahead’ sign by a distance of 70 m due to the higher speed limit. The standard required the ‘RAIL’ and ‘X’ road marking to be placed between the W7-7 sign and W3-1 signs.
When the railway line was opened in 2004, the Australian Standard required RX-2 stop sign assemblies to have the following 3 components:
RAILWAY CROSSING (R6-24)
STOP (R1-1)
LOOK FOR TRAINS (G9-48).
In 2007, the standard was changed to allow the use of either the R6-24 crossarms or the R6-25 sign (crossarms overlaid on a red background in Figure 6). It was also added that the R6-25 sign would be the preferred design on all new and refurbished RX-2 assemblies. A further update to the standard in 2016 removed the R6-24 crossarms as an approved component for new or upgraded crossings. As indicated within the standard, the update was not intended to be retrospective and although the crossarms were outdated, they were compliant with AS1742.7 (2016).
At the time of the collision, the stop sign assemblies on both sides of The Garden Road level crossing still had the R6-24 crossarms rather than the R6-25 sign.
Figure 6: The railway crossing STOP (RX-2) sign assembly at the level crossing (left) when compared with the current Australian Standard requirements (right)
Source: Pacific National (left) and AS 1742.7-2007 (right), annotated by the ATSB
Level crossing sighting distance
The truck driver estimated that the sighting distance when looking north from the stop line along the track was 300–400 m. The Ghan driver also identified that vegetation obscured their view of road traffic when approaching the level crossing. However, they also added that, while the vegetation obscured sightlines in advance of the crossing, the crossing itself could be seen from a considerable distance away and that the clearance of the trees away from the track was ‘quite reasonable’.
Survey data within the Australian Level Crossing Assessment Model (ALCAM) report from May 2024 of The Garden Road level crossing identified that, when stopped at the stop line on the western side of the level crossing, the sighting distance when looking north along the rail corridor was 1,563 m. The view looking north from the level crossing stop line is shown at Figure 7. The sighting distance was 1,903 m when looking to the south. The sighting distance from the eastern side of the crossing in both directions was unlimited.
At a line speed limit of 115 km/h, the ATSB calculated that trains approaching from the north would become visible from the western stop line 49 seconds before the train reached the level crossing. This increased to 60 seconds for trains approaching from the south. For road users stopped at the stop line on the eastern side, there were no time limitations when approaching trains would become visible. Although the road speed limit for The Garden Road was 100 km/h, the ALCAM report identified that the average approach speed to the level crossing from the west was 60 km/h, which determined the placement of the advance warning signage.
Figure 7: View looking north along the rail corridor from the stop line at the level crossing
This image was captured on 15 September 2024. Source: Aurizon
Truck clearance times
The standard gauge track was 1.435 m wide, and the stop line on each side was 5.2 m from the nearest rail. As a result, the minimum safe distance for road users to cross the tracks and be clear of the rail corridor was about 12 m from either stop line. Accounting for the standard length of an A‑triple road train (53.5 m), the truck would have needed to travel at least 66 m from the western stop line to safely cross the tracks.
The National Heavy Vehicle Regulator required trucks (road trains) to meet level 4 acceleration capability. This was the highest of 4 capability standards, which tested the ability of a vehicle to accelerate from rest on a road with zero gradient.
To meet this capability, road trains would have to accelerate from a stand and travel 100 m on a zero-gradient road in 29 seconds (or less). Based on these requirements, the established road train clearance times on a level grade fit within the ALCAM sighting times at The Garden Road level crossing.
Interface agreement
The Rail Safety National Law required rail infrastructure managers and road managers of public roads to enter into an interface agreement to manage the risks to safety arising from their rail or road crossings. For The Garden Road level crossing, the local road manager (Northern Territory Government) was responsible for the interface boundary outside the rail corridor that included road condition, level crossing advance warning signage, road markings, and sighting along the road corridor. The rail infrastructure manager (Aurizon) was responsible for the interface boundary within the rail corridor that included: sighting along the rail corridor, track infrastructure, primary warning devices and signage at the level crossing, and the pavement at the road‑rail interface.
To assist with maintaining sighting distances, the road manager was responsible for vegetation outside of the rail corridor and the rail infrastructure manager was responsible for vegetation clearance within the rail corridor.
At the time of the accident, an interface agreement was in place between Aurizon and the local road manager. Following the collision, the interface agreement was renegotiated and signed between both parties.
Scheduled inspections
As the rail infrastructure manager, Aurizon conducted regular inspections of the Alice Springs to Tennant Creek rail corridor. This consisted of weekly visual inspections from the rail corridor to monitor track condition and known defects, and an annual ALCAM assessment from the road corridor to assess overall compliance with the Australian Standard.
The most recent visual inspection of The Garden Road level crossing had been completed on 9 September 2024. This inspection did not identify any track misalignment, defects, or faults at the level crossing prior to the collision, and no corrective maintenance was scheduled following this inspection. The next weekly inspection was scheduled for 16 September 2024, the day after the collision.
The annual ALCAM assessment for compliance with civil engineering standards was conducted in May 2024. This inspection found that vegetation obstructed advance views of the rail corridor for road users on both sides of the crossing. However, it found that this vegetation did not impact visibility and sightlines along the rail corridor when a vehicle was stopped at the stop line.
On the western side of the crossing, which was the approach direction of the truck, the ALCAM assessment made the following observations:
• Passive control required updating to current standard and maintenance
• Stop bar and centre barrier lines were faded
• Advance warning signs were incorrectly positioned for the road speed
• Advance warning road markings were faded and incorrectly spaced for the road speed.
The faded stop line is shown at Figure 8 and this was reportedly due to the effects of road resurfacing.
Figure 8: Faded stop line at the level crossing with skid marks evident from the emergency braking of the truck
Source: Pacific National, annotated by the ATSB
ATSB safety study of level crossing collisions between heavy vehicles and trains
The ATSB safety study Review of level crossing collisions involving trains and heavy road vehicles in Australia (RS-2021-001) analysed 49 collisions between trains and heavy vehicles at Australian level crossings between July 2014 and August 2022, in which 24 rail or road users were fatally or seriously injured. Records from rollingstock operators, rail infrastructure managers, police, and other organisations were obtained for each of these accidents. The aim of the study was to improve the understanding of the risks associated with level crossing collisions involving heavy vehicles. Across the study period, several correlating observations were identified:
All level crossing collisions involving heavy vehicles resulted from the heavy vehicle driver not giving way to trains. There were 3 actions associated with the collisions:
There were at least 24 collisions where the heavy vehicle did not stop prior to entering the crossing.
There were at least 11 collisions where the heavy vehicle stopped at the crossing then proceeded into the path of a train.
There were at least 13 collisions where the heavy vehicle entered a level crossing and stopped foul of the train line.
Of the 26 collisions at passive control crossings, there were at least 12 collisions where the heavy vehicle driver slowed or stopped but probably did not detect the train and entered the crossing into the path of the approaching train.
In at least 12 collisions the heavy vehicle driver had regularly used the level crossing prior to the collision with the train. The drivers' previous experience at the crossings may have led to a low expectancy for trains and contributed to them not detecting a requirement to stop and give way.
In at least 14 collisions, the heavy vehicle driver’s view of the track or level crossing protection equipment was obstructed by vegetation, the design of the heavy vehicle cab, poor crossing lighting, or sun glare.
Consistent with prior research showing that train horns have limited effectiveness for alerting road vehicle drivers approaching level crossings, in at least 25 accidents the horn was not effective at alerting the heavy vehicle driver to the presence of the train.
The report also described a ‘rolling stop’, which involved slowing a road vehicle until a decision was made to proceed into the crossing, without coming to a complete stop. When conducting a ‘rolling stop’ a road vehicle driver would spend less time at the stop point for a passive level crossing and therefore would probably employ less time scanning for oncoming trains. In turn, that increases the likelihood of an incorrect decision to proceed into the crossing when it was not safe.
Safety analysis
Truck driver actions
As the truck turned off the Stuart Highway and was being driven eastward along The Garden Road, the driver was unaware of The Ghan that was approaching southbound at 108 km/h. At the level crossing, the train would have been visible to road users that had stopped at the stop line, however, it would have been difficult to identify in advance due to the presence of roadside vegetation that obscured longer distance sighting along the rail corridor.
During its journey, the locomotive headlights of The Ghan were illuminated, and the driver had sounded the horn multiple times in close proximity to the crossing as required. The truck driver did not recall hearing the horn being sounded. This has been identified as a factor in several other accidents where a horn had limited effectiveness in alerting a heavy vehicle driver of an approaching train.
The truck was travelling at a low speed, which increased the available time and distance for the driver to see and respond to the road markings, signage and requirement to stop their vehicle. The driver reported they had no recollection of the truck’s speed, however, they did recall initiating emergency braking on seeing the passage of The Ghan immediately in front of their cab.
Remnant skid marks on the road surface were consistent with their recollection and actions. Calculations of the truck speed prior to the collision indicated that the driver had been slowing on their approach to the crossing. However, it was unlikely they were intending to bring the truck to a complete stop prior to passing the stop line as doing so would have required an emergency application of the brakes. Additionally, they acknowledged that they would sometimes roll through level crossings rather than come to a complete stop. That driving behaviour has been identified as a factor in previous collisions between heavy vehicles and trains.
From this, it can be concluded that the truck driver did not slow down sufficiently to stop at The Garden Road level crossing, resulting in a collision with The Ghan passenger train. The presence of the roadside vegetation may have contributed to restricted views of an approaching train, but if the driver had intended to stop, they would have seen the approaching train as the sighting distance from the stop line was clear and unobstructed, especially at truck cab height.
Passive level crossing
Passive controls were the primary risk control against vehicle collisions at The Garden Road level crossing. They do not activate, illuminate, or change state to indicate the presence of an approaching train. Neither did they physically prevent road users from crossing the track when a train was present or approaching the crossing. Consequently, the requirement to stop, sight, and remain clear of all rail traffic was a critical requirement to avoid a collision. It is the responsibility of the road user and in this circumstance the truck driver to stop for approaching rail traffic.
The Garden Road level crossing and its associated infrastructure largely complied with the relevant standards. All signs, road markings, and the level crossing itself, were visible from the highway intersection and in place on the day of the accident. Although it was noted that the stop sign had not been updated to the current standard, some advance warning signs were at the incorrect distances, and the stop line and other markings were partly faded. However, this did not influence the truck driver’s awareness of the requirement to stop their vehicle prior to crossing the track. The truck driver had traversed the crossing on numerous occasions and was aware of the stopping requirement.
When approaching the crossing from the west, roadside vegetation obstructed the northern view of the rail corridor until shortly before the stop line. The vegetation lined both the road and rail corridors but was set back around 20 m from the railway track. Accordingly, the vegetation did not impact the ability of road users to see the advance warnings or the passive controls, or prevent them from seeing the stop sign at the crossing. Similarly, the proximity of the S‑bend from the highway reduced vehicle approach speeds to the level crossing and improved visibility to provide additional time for drivers to observe and respond to the signs and/or road markings. As such, there was sufficient sighting distance for a driver scanning for hazards along the road ahead to react and stop in time.
While some aspects of the level crossing controls were either not as per standard, outdated or of suboptimal quality, there was signage and markings for road users to be aware of the crossing and bring their vehicles to a controlled stop before entering. Once stopped, there was adequate visibility for a driver to sight a train and give way.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision between a truck and The Ghan passenger train, at The Garden Road level crossing, 48 km north of Alice Springs, Northern Territory, on 15 September 2024.
Contributing factors
The truck driver did not slow sufficiently to stop prior to The Garden Road level crossing, resulting in a collision with The Ghan passenger train.
Other findings
While some aspects of the level crossing controls were either not as per standard or were faded, there was signage and markings for road users to be aware of the crossing and bring their vehicles to a controlled stop before entering. Once stopped, there was adequate visibility for a driver to sight a train and give way.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence
Safety action by the Northen Territory Government – Department of Logistics and Infrastructure
The Department of Logistics and Infrastructure has advised of the following safety actions since the accident:
Refreshment of the line marking and upgrading the approach signage at The Garden Road level crossing.
Negotiation of a revised interface agreement with the rail infrastructure manager (RIM), which included a commitment from the RIM to install updated signage (R6‑25 ‘Railway Crossing’) to meet current AS1742.7 standards at The Garden Road level crossing, and to progressively upgrade signage at other crossings when existing signs are due for replacement.
Continuation of the Northern Territory Level Crossing Safety Working Group with the rail industry, infrastructure managers and local government.
Continuation of level crossing assessments and line-of-sight improvements.
It also delivered a targeted campaign during the August 2025 National Rail Safety Week to raise public awareness of level crossing risks across the Northern Territory. The tactics used during that campaign included social media advertising, learner driver education and displays at the motor vehicle registry.
ATSB comment
The ATSB acknowledges the safety action completed by the Department of Logistics and Infrastructure. The ATSB notes, however, that while all physical elements of the approach to The Garden Road level crossing (road signage and pavement markings) are present or have been substantially updated, some of the approach signage elements remain incorrectly positioned, and are not in accordance with the Australian Standard AS 1742.7.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Pacific National
Great Southern Rail
Aurizon Bulk Central
the train crew
the truck driver
Northern Territory Police
Office of the National Rail Safety Regulator
Northern Territory Government – Department of Logistics and Infrastructure.
Submissions were received from:
Pacific National
Great Southern Rail
Aurizon Bulk Central
Office of the National Rail Safety Regulator
Northern Territory Government – Department of Logistics and Infrastructure.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Whistle board: when a train passes a whistle board, the train driver must sound the horn to warn workers and/or members of the public that rail traffic is approaching.
[2]Bogie: a structure incorporating suspension elements and fitted with wheels and axles, used to support rail vehicles at or near the ends of the vehicle, and capable of rotation in the horizontal plane. Bogies can have one or multiple axle sets, and can also be used as a common support for adjacent units on an articulated vehicle.