
Aircraft separation issue involving a British Aerospace Jetstream 32 and a Piper PA-28, 23 km north-east of Mudgee Airport, New South Wales, on 3 October 2024
What happened
On 3 October 2024, a British Aerospace Jetstream 32 (JS-32) was conducting a practice instrument approach procedure at Mudgee Airport, New South Wales as part of a training flight. On board were 2 flight crew members and an additional trainee captain as a passenger. Prior to descent, air traffic control (ATC) advised the crew over the area frequency of traffic for their descent, which was an aircraft inbound for the same instrument approach procedure. The crew advised that due to being in Class E airspace,[1] they did not make a general broadcast on the area frequency of their intentions.
At approximately 30 NM east of the airport, the crew of the JS-32 made an initial broadcast on the Mudgee common traffic advisory frequency (CTAF) advising of their position and intentions. Further position broadcasts were made on the CTAF during the descent, in addition to communications with the other aircraft on the approach to arrange sequencing. During the initial segment of the instrument approach, approximately 13 NM north-east of the airport, the crew observed an unknown aircraft, a Piper PA-28 (PA-28), cross below their flight path from the right, tracking towards the airport. They estimated the separation between the aircraft was less than 100 m horizontally and 200 ft vertically. The training captain advised the trainee captain to maintain their current level and subsequently commenced attempts to contact the PA-28. During these attempts, ATC contacted the crew with advice that they had observed the PA-28 on their system.
Communication was established with the PA-28 on the CTAF approximately 5 minutes after the incident. The JS-32 flight crew later reported that the PA-28 had not been detected by the ADS-B traffic display functionality of their navigation system.
The PA-28, with a student pilot and instructor on board, was conducting a training flight from Scone Memorial Airport to Mudgee Airport. The aircraft was equipped with an altitude reporting transponder and a single radio which they tuned to the CTAF at around 10 NM from the airport. They advised that they made an inbound call on the CTAF and received no response. Approximately 2 minutes later, they were contacted by the crew of the JS-32 advising them of the incident.
Figure 1: Approximate flight paths of the Jetstream 32 and Piper PA-28
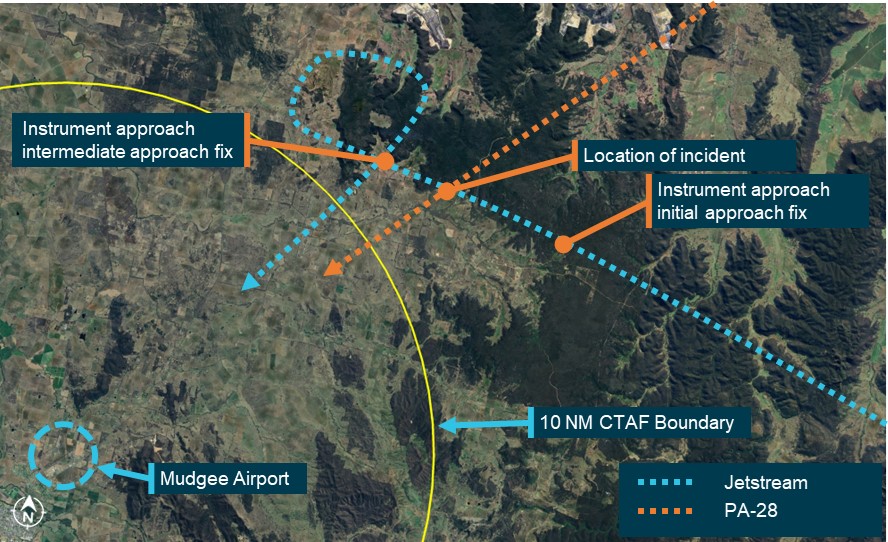
Source: Flight data overlaid on Google Earth, annotated by the ATSB
Safety message
The majority of aerodromes within Australia operate without the provision of air traffic control services. These aerodromes rely upon pilots broadcasting their positions and intentions on a common traffic advisory frequency (CTAF) and then implementing separation actions that are agreed directly between the pilots. VHF radio is the primary communication tool to provide ‘alerted see-and-avoid’, used commonly across aviation from sport and recreational flying to air transport. Listening to and broadcasting on the CTAF is mandatory within 10 NM of certified aerodromes such as Mudgee Airport.
This occurrence highlights the hazards associated with operations approaching the 10 NM CTAF boundary of non-controlled aerodromes and reinforces the importance of pilots maintaining good situational awareness and being alert to the likely traffic mix.
When conducting practice instrument approaches in visual conditions, flight crew should always maintain a vigilant lookout for other traffic as instrument approach procedures often begin outside the 10 NM CTAF area, where other aircraft may be operating while not monitoring the CTAF. Ensuring a radio broadcast is made on the area frequency, as well as the CTAF, will assist in alerting other aircraft in the vicinity. It is also important to understand the limitations of onboard traffic systems in detecting aircraft with minimal equipment, and the limitations of radar coverage in enabling air traffic control (ATC) to see and advise of traffic when operating in remote areas.
Pilots of light aircraft should consider the possibility of encountering higher performance air transport aircraft when approaching a non-controlled aerodrome, particularly when crossing the flight path of an instrument approach procedure. When equipped with more than one radio, monitoring the CTAF well before the 10 NM boundary will give more time to receive broadcasts and build awareness of traffic at the aerodrome. The ATSB also strongly encourages the fitting and use of equipment such as ADS-B transmitting devices to assist other aircraft and ATC in identifying and tracking your aircraft.
The ATSB’s publication A pilot’s guide to staying safe in the vicinity of non-controlled aerodromes outlines many of the common problems that occur at non-controlled aerodromes, and offers useful strategies to keep yourself and other pilots safe. The Civil Aviation Safety Authority's Pilot Safety Hub also has extensive information on non‑controlled operations.

The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. Two of the current safety concerns are Reducing the collision risk around non-towered airports and Encouraging the use of available technology to enhance safety.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1] The lower level of Class E airspace in this area was 8,500 ft.
Occurrence summary
| Mode of transport | Aviation |
|---|---|
| Occurrence ID | AB-2024-039 |
| Occurrence date | 03/10/2024 |
| Location | 23 km north-east of Mudgee Airport, New South Wales |
| State | New South Wales |
| Occurrence class | Incident |
| Aviation occurrence category | Aircraft separation |
| Highest injury level | None |
| Brief release date | 21/11/2024 |
Aircraft details
| Manufacturer | British Aerospace |
|---|---|
| Model | Jetstream 32 |
| Sector | Turboprop |
| Operation type | Part 121 Air transport operations - larger aeroplanes |
| Departure point | Newcastle Airport, New South Wales |
| Destination | Mudgee Airport, New South Wales |
| Damage | Nil |
Aircraft details
| Manufacturer | Piper Aircraft Corp |
|---|---|
| Model | PA-28-181 |
| Sector | Piston |
| Operation type | Part 141 Recreational, private and commercial pilot flight training |
| Departure point | Scone Memorial Airport, New South Wales |
| Destination | Mudgee Airport, New South Wales |
| Damage | Nil |
Loss of control and collision with terrain involving a Morgan Cougar Mk1 aircraft, VH-LDV, 19 km north-north-west of West Sale Airport, Victoria, on 16 November 2024
Final report
Report release date: 19/01/2026
Investigation summary
What happened
On 16 November 2024, an amateur-built experimental certificate Morgan Cougar Mk 1 aircraft, registered VH-LDV, with a pilot and 2 passengers on board, departed from West Sale Airport, Victoria for a local area flight. The aircraft collided with terrain in a paddock it was orbiting around, about 19 km north-north-west of West Sale Airport, 17 minutes after departure. The aircraft was destroyed, and the 3 occupants were fatally injured.
The pilot was operating a VH-registered aircraft with a Recreational Pilot Licence (RPL), issued by CASA in recognition of the pilot holding a Recreational Pilot Certificate (RPC), issued by Recreational Aviation Australia (RAAus).
What the ATSB found
The aircraft entered an accelerated aerodynamic stall while in a steep turn at a low speed and height from which it was too low to recover (about 220 ft above ground level). The pilot had a reported history of conducting steep turns at low heights, and on occasions at low speeds, and had low flying hours in the aircraft and no transition training. Therefore, it was likely that the pilot was not aware of the stall characteristics of the aircraft and that it might depart controlled flight in an abrupt and unexpected manner.
The pilot’s history also included several counselling sessions they had received from members of the local aviation community in response to risky flying activities. However, no official reports were submitted to authorities and therefore no follow-up action was ever initiated.
A review of the pilot’s examination history revealed several errors about aerodynamic stalling in exams conducted during 2024 and it was concluded that the pilot likely had inadequate knowledge of the relationship between angle of bank, load factor and stall speed. Additionally, the investigation found several instances of irregular practices in training and exams at the Adventure Flight Training (AFT) school, which included the pilot’s exams, and concluded that those management practices likely contributed to the pilot’s inadequate knowledge.
RAAus administered the examination system, and it was found to have inadequate controls to mitigate the practices at AFT. When RAAus uncovered the problems at AFT in 2024, they issued a safety related suspension (SRS) notice against the chief flying instructor of AFT, which resulted in the cessation of operations in August 2024.
After the accident, RAAus issued another SRS against the AFT graduates for potential knowledge deficiencies. However, when CASA were advised of this action, they did not follow-up to verify if any of those graduates also held a CASA licence granted based on holding an RAAus RPC which had been suspended. It was subsequently found that 2 members held a CASA-issued licence, granted based on their suspended RPCs.
Furthermore, the accident aircraft was found to have design deficiencies, which contributed to the severity of the occupants’ injuries. They included a lack of energy attenuation in the landing gear and seating, and the installation of a fuel tank between the engine and instrument panel that ruptured and caused the post-crash fire. In addition, it was likely that car seatbelts were fitted and the front seatbelts failed in the accident, which resulted in the front seat occupants being ejected from their seats.
Finally, it was found that the CASA advisory circular for amateur-built experimental certificate aircraft provided recommendations to address some aspects of aircraft crashworthiness, which included seatbelts. However, it did not address energy attenuation or fuel tank installation. In addition, while it provided safety recommendations for pilots conducting flight testing, it did not recommend transition training for new owners of these aircraft.
What has been done as a result
RAAus commenced a digital systems redevelopment project with scoping of user requirements completed in 2023, which includes their learning management system. This incorporates the implementation of an online exam system. RAAus are also progressing the re-drafting of several key documents in their Exposition, which includes updates to the following:
- flight operations manual to contain greater clarity around the conduct of RAAus examinations
- occurrence and complaints handling manual to include a description of the process for handling a safety related suspension for an individual if their membership has lapsed
- syllabus of flight training to include further development of the stalling element of the syllabus.
CASA has implemented a more robust process to ensure that all reports received that relate to suspension, variation or cancellation of authorisations issued by an approved self‑administering organisation will include a review of CASA records to determine if the reported individual also holds a ‘same-in-substance’ CASA-issued authorisation. If so, the holder’s qualifications will be subject to review through the CASA Coordinated Enforcement Process.
Safety message
The investigation revealed a trend in risky flying behaviour by the accident pilot, which was likely compounded by inadequate knowledge from a flight training school that had developed irregular practices in the delivery of training and had inadequate supervision. While many people knew of the pilot’s risky flying behaviour and had attempted to counsel them, there was no evidence that any of the incidents were reported to authorities, and the counselling efforts were ultimately unsuccessful.
The ATSB has previously advocated for witnesses, particularly those within the aviation industry, to report any concerns regarding unsafe behaviours through mechanisms such as confidential reporting systems (see AO-2019-027). The ATSB re-iterates this previous safety message.
CASA has published recommended guidance for amateur-built experimental certificate aircraft. While this publication is directed at those who design, build and flight test these aircraft, the safety precautions should be read by new owners and considered equally applicable to them.

The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing the severity of injuries in accidents involving small aircraft. In this accident the lack of energy attenuation and location of the fuel tank in the design of the aircraft and the likely fitment of car seatbelts all increased the risk to occupants in the event of a ground collision.
Summary video
The occurrence
At 1730 local time on 16 November 2024, an amateur-built Morgan Cougar Mk 1 aircraft, registered VH-LDV, with a pilot and 2 passengers on board, departed from West Sale Airport, Victoria for a local area flight. The pilot was seated in the front left seat, and the passengers were seated in the front and rear right seats. A review of Airservices Australia automatic dependent surveillance-broadcast (ADS-B) data identified that the aircraft conducted a left turn on departure and tracked 15 km north of West Sale Airport to the town of Maffra, where they arrived overhead at about 1736 (Figure 1).
Figure 1: Accident flightpath with key timings and locations
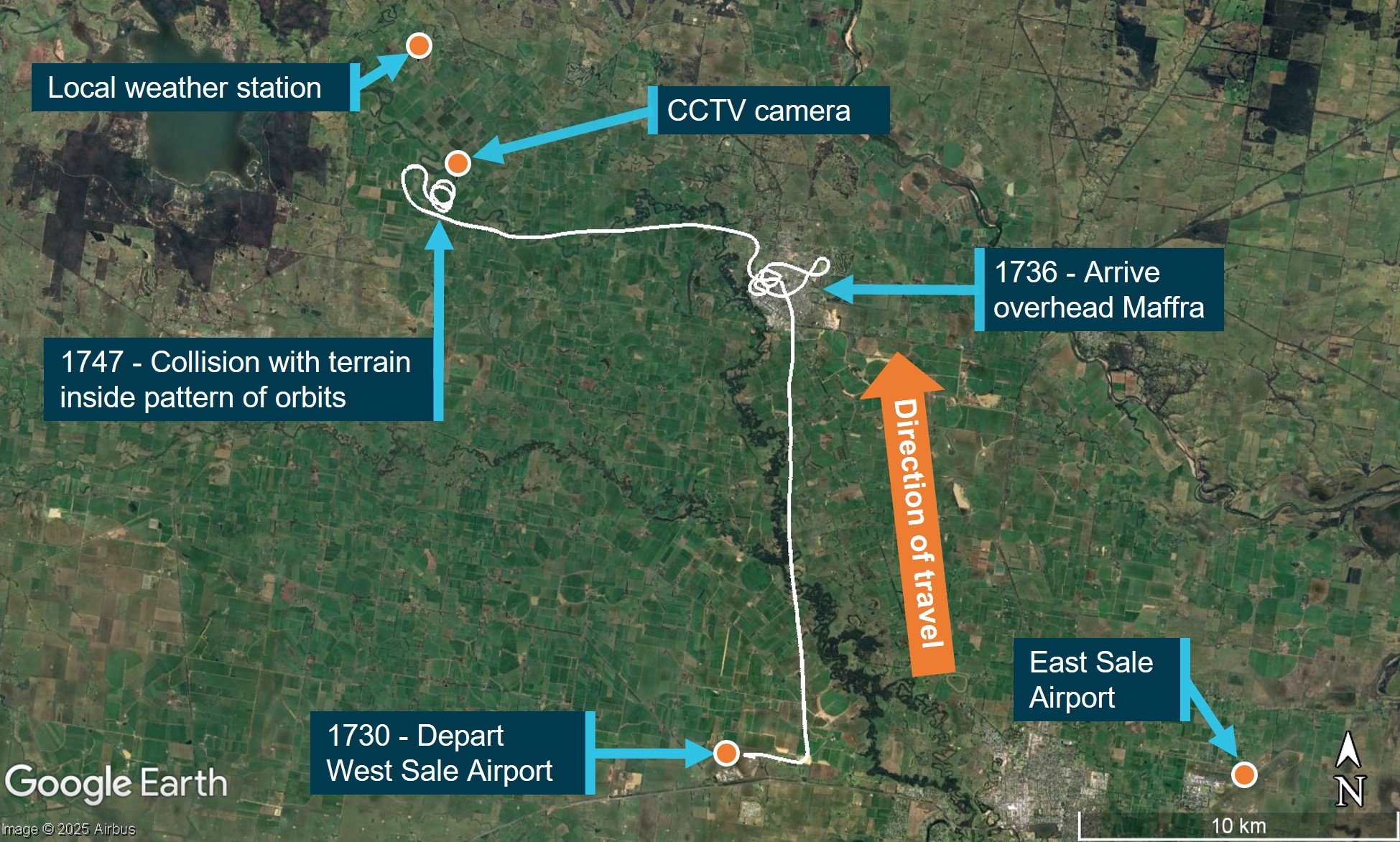
Sources: Airservices Australia and Google Earth, annotated by the ATSB
The aircraft made a series of turns overhead the town of Maffra for about 4 minutes. At 1740, the aircraft departed from overhead Maffra and tracked about 11 km west towards Tinamba West. The aircraft conducted a right-hand turn overhead a property at Tinamba West, which belonged to relatives of the aircraft occupants, before commencing a series of left-hand turns (orbits) around a point about 1 km to the south-east of the property over open paddocks (Figure 2).
On the second orbit, the aircraft made a low pass along the Macalister River, adjacent to where several witnesses, which included 2 adults, were located. The 2 adults later stated that they had witnessed the aircraft conduct 2 orbits past their location before the accident. They reported the second pass along the river was lower than the first, such that they could both see the occupant in the rear seat, and that the aircraft sounded normal.
Figure 2: Orbits and the location of witnesses

Sources: Airservices Australia and Google Earth, annotated by the ATSB
A closed-circuit television (CCTV) camera, located about 700 m north-north-east of the accident site, captured the aircraft entering a left turn towards the camera on its third orbit (Figure 3 [1]). During the turn the angle of bank increased to a steep turn attitude (Figure 3 [2]) before the nose of the aircraft pitched down and the aircraft descended in the left turn behind trees (Figure 3 [3]).
Figure 3: CCTV footage of final turn
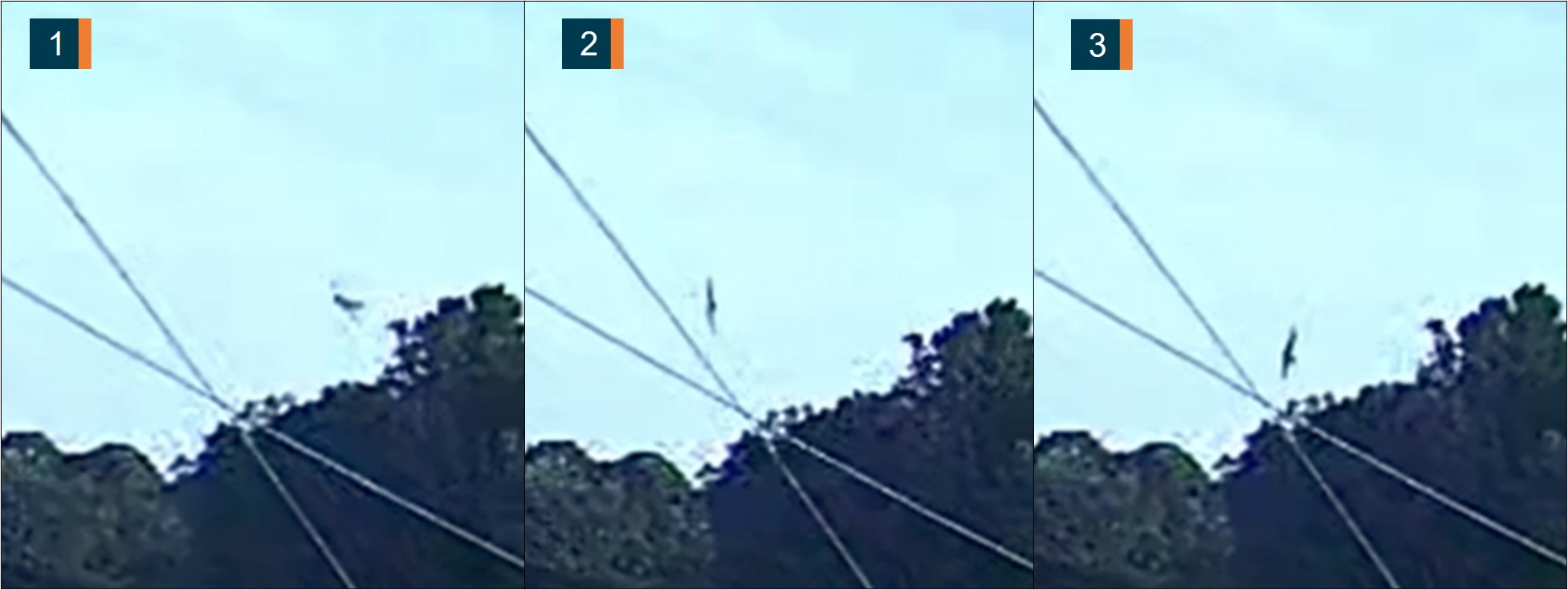
Images subject to visual distortion (fisheye lens effect). Source: Victoria Police, annotated by the ATSB
One of the witnesses reported that, as the aircraft approached them for a third pass, it did a hard left turn and then appeared to be falling and not gliding towards the ground, as though it did not have enough speed. They reported that the wings levelled after the turn and it landed very hard on its belly and immediately caught fire. The second witness saw it bank hard left and fall out of the sky but did not see the collision. The 3 occupants were fatally injured, and the aircraft was destroyed.
Context
Accident site and wreckage
Overview
The aircraft impacted flat and open terrain at an elevation of about 130 ft and produced a ground scar on a track of 315° T (Figure 4). The length of the wreckage trail was 30.3 m from the first ground scar to the propeller spinner, with the fuselage resting on a heading of 303° T. Impact analysis indicated the aircraft struck the ground in a slight left wing low and close to level pitch attitude, which was consistent with the witness report of the collision.
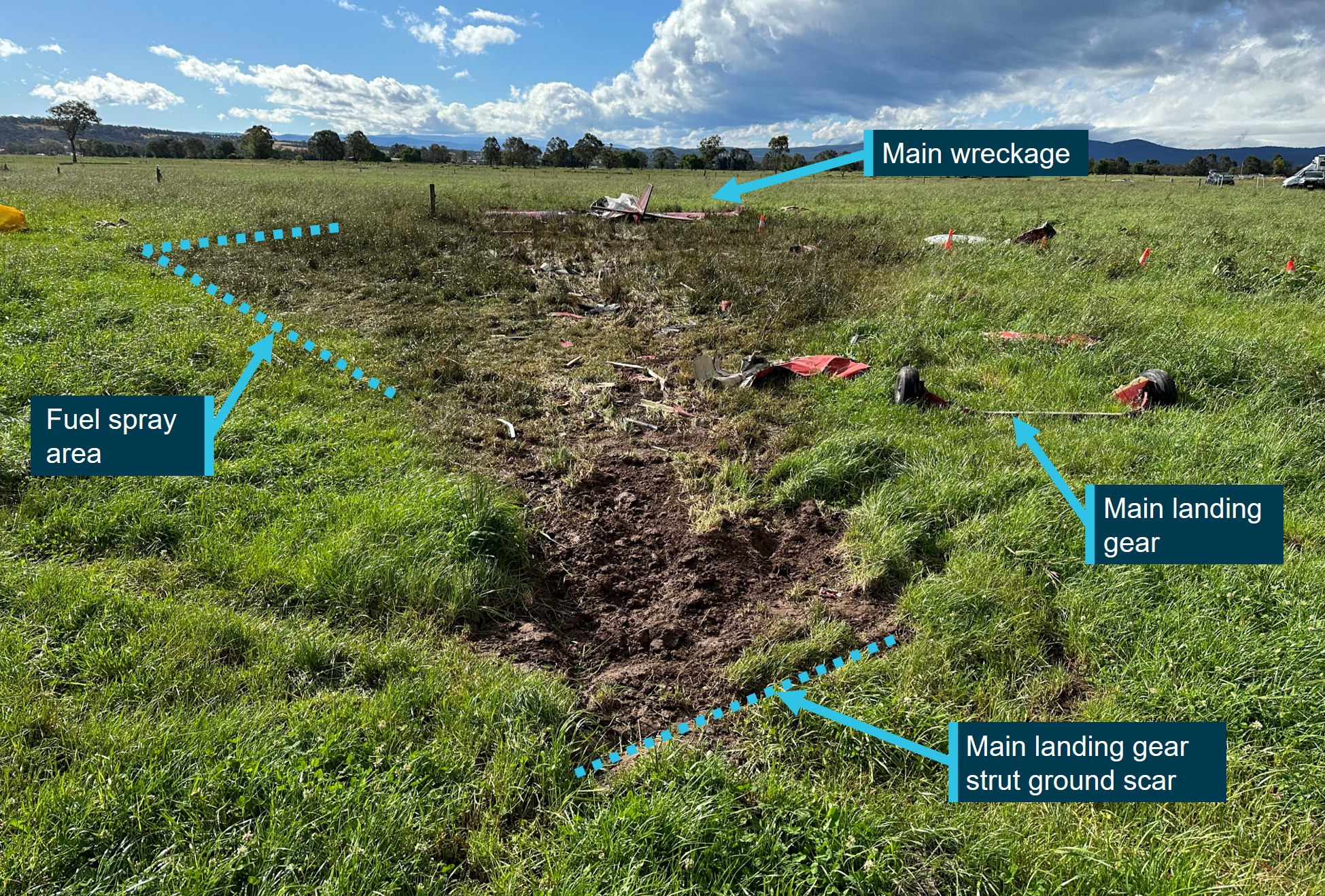
Source: ATSB
There was a delta-shaped fuel spray and debris pattern along the wreckage trail. A fuel‑fed fire occurred after the ground impact, however, most of the fire damage to the aircraft was confined to the fuselage within the area bounded by the firewall,[1] aft bulkhead (behind rear seats) and the inboard sections of the wings (Figure 5). The engine and propeller were also affected by the post‑impact fire, but to a lesser extent than the fuselage. The wings and tailplane (except the rudder) remained attached to the fuselage. The rudder was found in the wreckage trail.
Figure 5: Fire damage to the aircraft

Source: ATSB
The engine remained attached to the firewall, which had separated from the fuselage, and the 3-bladed propeller hub was attached to the engine. There was considerable disruption between the engine and airframe. One substantially fire-damaged carbon fibre propeller blade was attached to the hub and the other 2 propeller blades, which were not fire‑affected, had separated at their roots and were found fragmented within the debris field.
Aircraft inspection
Engine and propeller
The 2 witnesses to the accident sequence provided different accounts of the noise of the aircraft just prior to the collision. One reported that the aircraft sounded normal before the final turn and then went quiet, whereas the other witness reported no change in the sound of the aircraft during the accident sequence.
The intake manifolds, carburettors, drive belts, oil hoses, and fuel lines were heavily damaged by the post-impact fire. The left carburettor was damaged beyond assessment, and the right carburettor was found with the throttle valve in the idle position. However, the carburettor throttle valve is spring loaded to idle, so the as-found position was not considered a reliable indicator of its position in flight.
The number 1 cylinder head was removed for inspection and was found to be lubricated and did not exhibit any signs of distress. The other cylinders could not be accessed due to impact damage. The engine oil filter and oil sump magnetic plug were inspected, and no metallic debris was identified.
The turbocharger compressor scroll was found separated from the turbocharger and directly below the turbocharger assembly. The scroll exhibited an overstress failure, with fracture surfaces but no scoring. Several turbocharger compressor vanes exhibited bending in the opposite direction of rotation, which indicated the compressor was running at impact (Figure 6).
Figure 6: Rearward bending of turbocharger compressor vanes
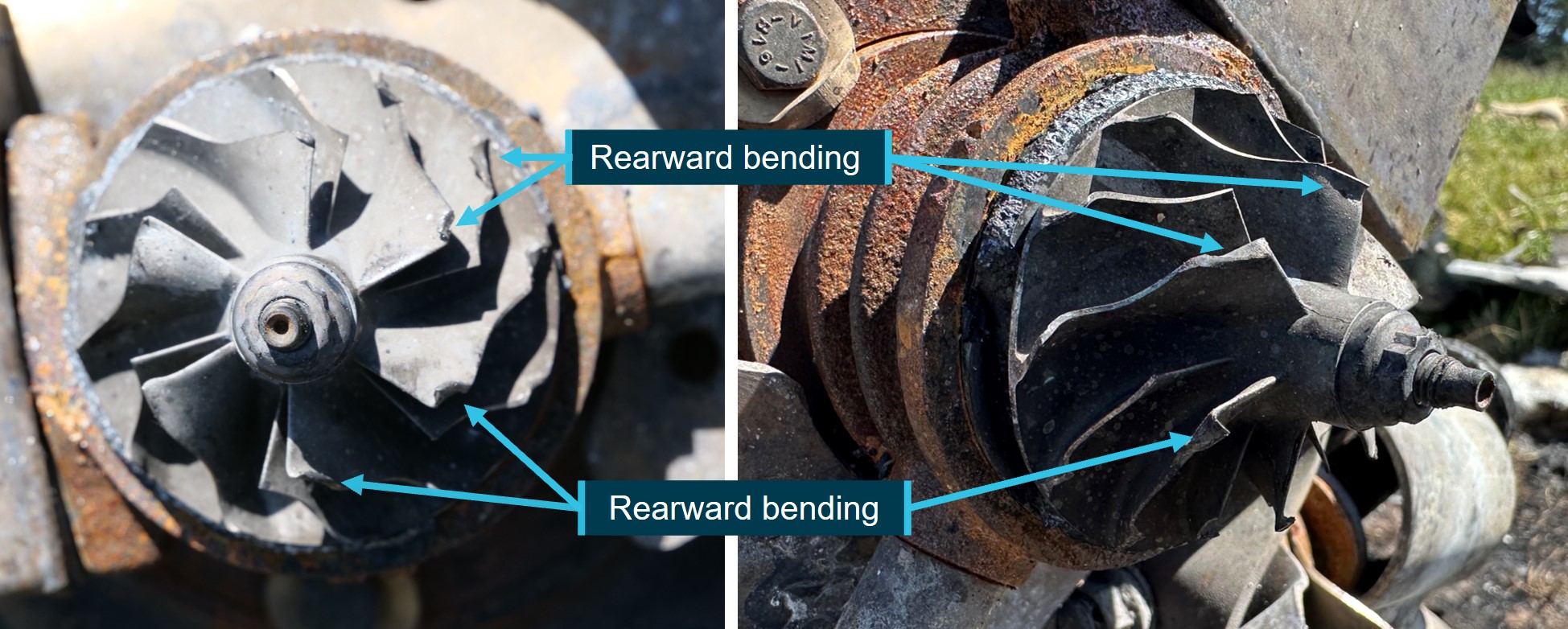
Source: ATSB
The propeller hub was secured to the engine output flange by 6 bolts and concentric locating pins. The hub was removed for inspection and very slight ovalisation of all 6 of the locating pins’ hub-side holes in the direction of rotation was noted.
Two of the propeller blades fractured at the blade root and separated from the hub, leaving the propeller root sections still clamped in the hub. The carbon fibre remnants on the root sections indicated tearing and separation of the blades in the opposite direction to rotation.
One of the propeller blade root hubs was relatively unbent and the following blade root hub (in the direction of rotation) exhibited rearward bending. This suggested a loss of propeller energy between consecutive blade ground strikes and the possibility that the first blade to separate was being driven by engine power.
The use of non-metallic propeller blades increased the uncertainty in the engine power assessment. However, in combination with the turbocharger compressor damage it was concluded that the engine was operating at impact, but the power level could not be determined.
Flight controls
Primary aircraft flight controls were of the direct acting cable, pushrod, and bellcrank type with a dual yoke control installed for elevator and aileron control. The wing flaps were electrically powered and found in the retracted position. The flaps could not be tested due to damage.
Rudder, elevator, and aileron controls were free to move about their full range. Several control cables were found severed and were inspected for signs of pre-impact failure. No wear, bird-caging, fretting, or other indications of damage were noted on the cables, and it was concluded that all these cables failed from overstress during the ground collision.
The rudder separated from the vertical stabiliser and was found in the wreckage trail. The mounting hardware was found, and the fracture surfaces of the flight control attachment points were consistent with an overstress failure.
While ATSB investigators were handling the yoke controls for inspection and photography, the chainring, which was part of the aileron control, separated under gravity from its bearings and support frame (Figure 7). However, given that they were not found separated, and that the aircraft attitude was recovered towards wings-level before the collision, it was concluded that the controls did not separate in-flight. The chainring and bearings were retained for further examination at the ATSB technical facility and details of that examination are provided in Appendix A – Examination of the flight controls.
Figure 7: Chainring separation from bearings and support frame
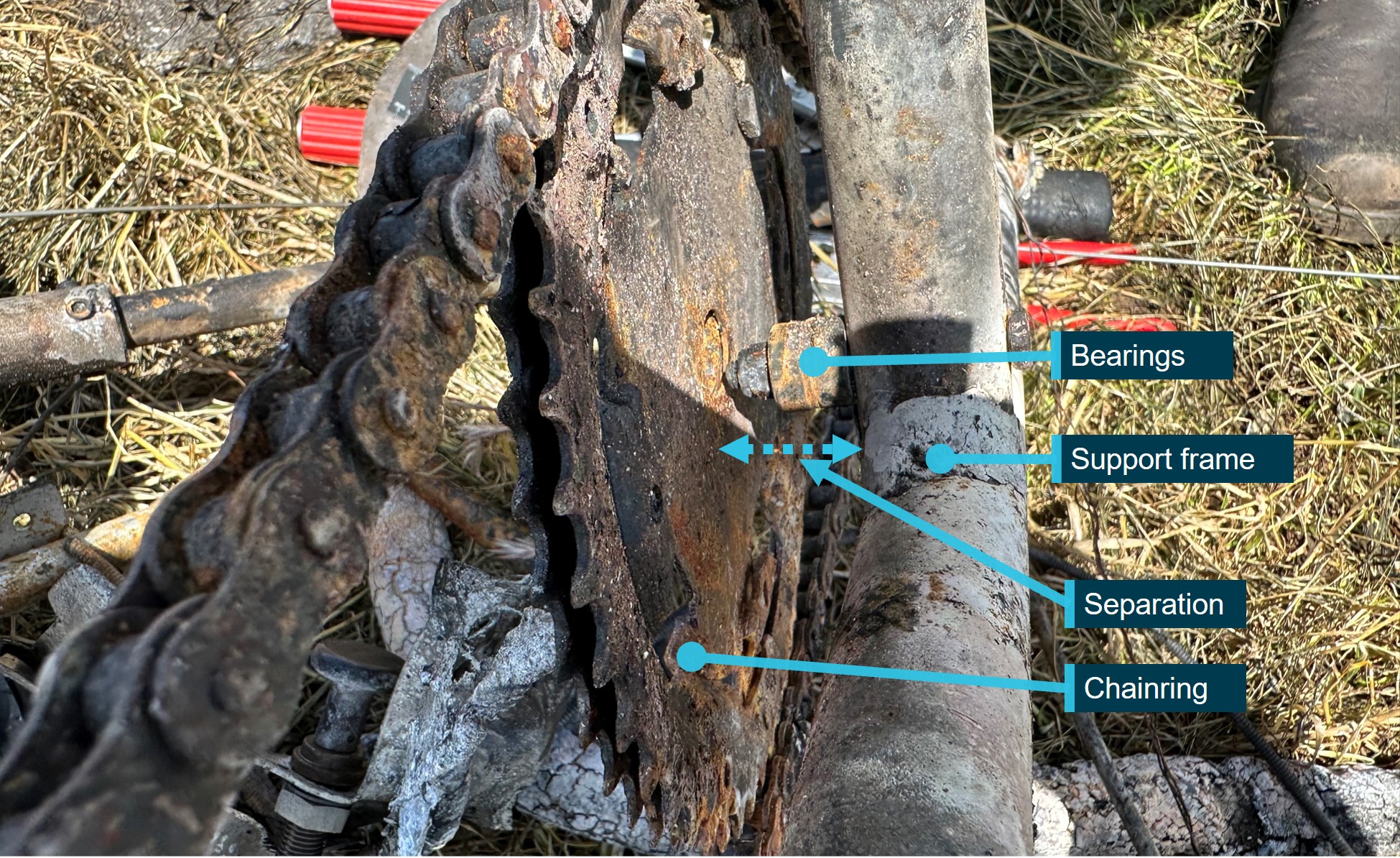
Source: ATSB
Fuel system
The aircraft fuel system consisted of a 55 L fiberglass tank in each wing, located aft of the main spar, and a 90 L fibreglass main tank between the instrument panel and the firewall. Fuel could be transferred from the wing tanks to the main tank via an electric transfer pump. The engine feed was from the main tank, via a fuel filter and 1 of 2 electric pumps.
The wing fuel tanks were found empty and relatively undamaged. The main tank was completely consumed by the impact and fire, along with significant parts of the surrounding fuselage. This was consistent with the flight fuel carried in the main tank.
Undercarriage
The undercarriage was a fixed tricycle gear, with a single-piece fibreglass strut supporting both main wheels, and a castering, spring lever nose wheel. The main and nose gear were found in the wreckage trail and their separation from the airframe was consistent with multiple overstress failures of the attachments at impact. The main gear assembly exhibited no evidence of permanent deformation or absorption of energy.
Seats and restraints
The aircraft was designed and built with 2 front seats and a 2-place rear bench-seat arrangement. The front seats were found in the wreckage, and their rear mountings were attached to the fuselage seat frame aluminium angle cross-member. The steel bolts used to mount the rear of the seats to the aluminium angle were present and fastened. The forward steel cross-member for the front seats was bowed forward (Figure 8). The right seat pan was retained by the seat back and appeared to have collapsed onto the main wing spar,[2] located underneath the front seats. The left front seat pan had separated from its seat back and was found in front of the seat frame forward cross-member.
Figure 8: Aircraft seat frame, wing spar and seats
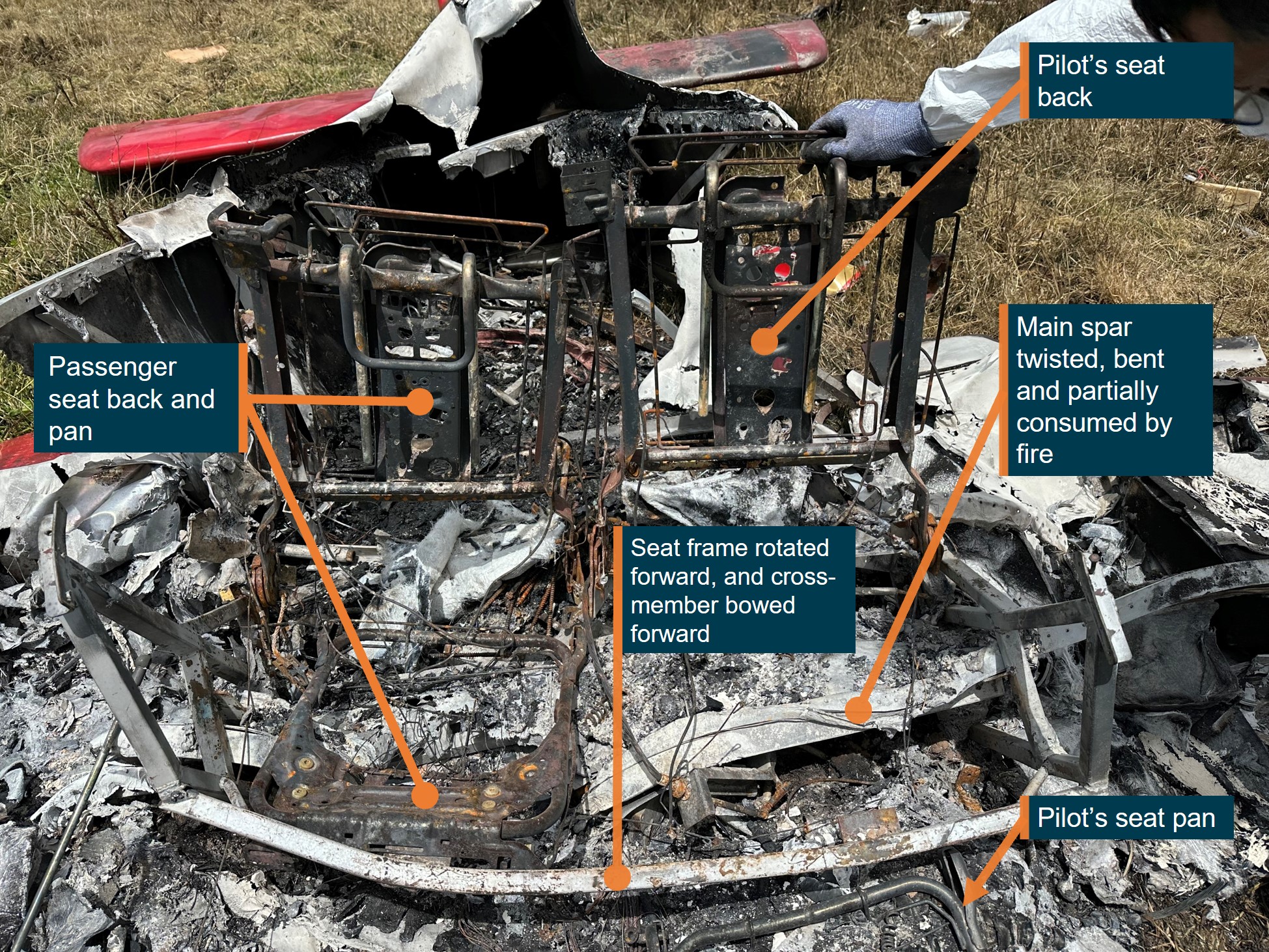
Source: ATSB
Both front seatbelt latch plates were found separated from their buckles and their associated harnesses were destroyed by the fire (Figure 9). The rear seats and seatbelts were destroyed by the post‑impact fire. However, the seatbelt latch plate for the rear seat occupant was found in its buckle.
Figure 9: Aircraft seatbelt latch plates
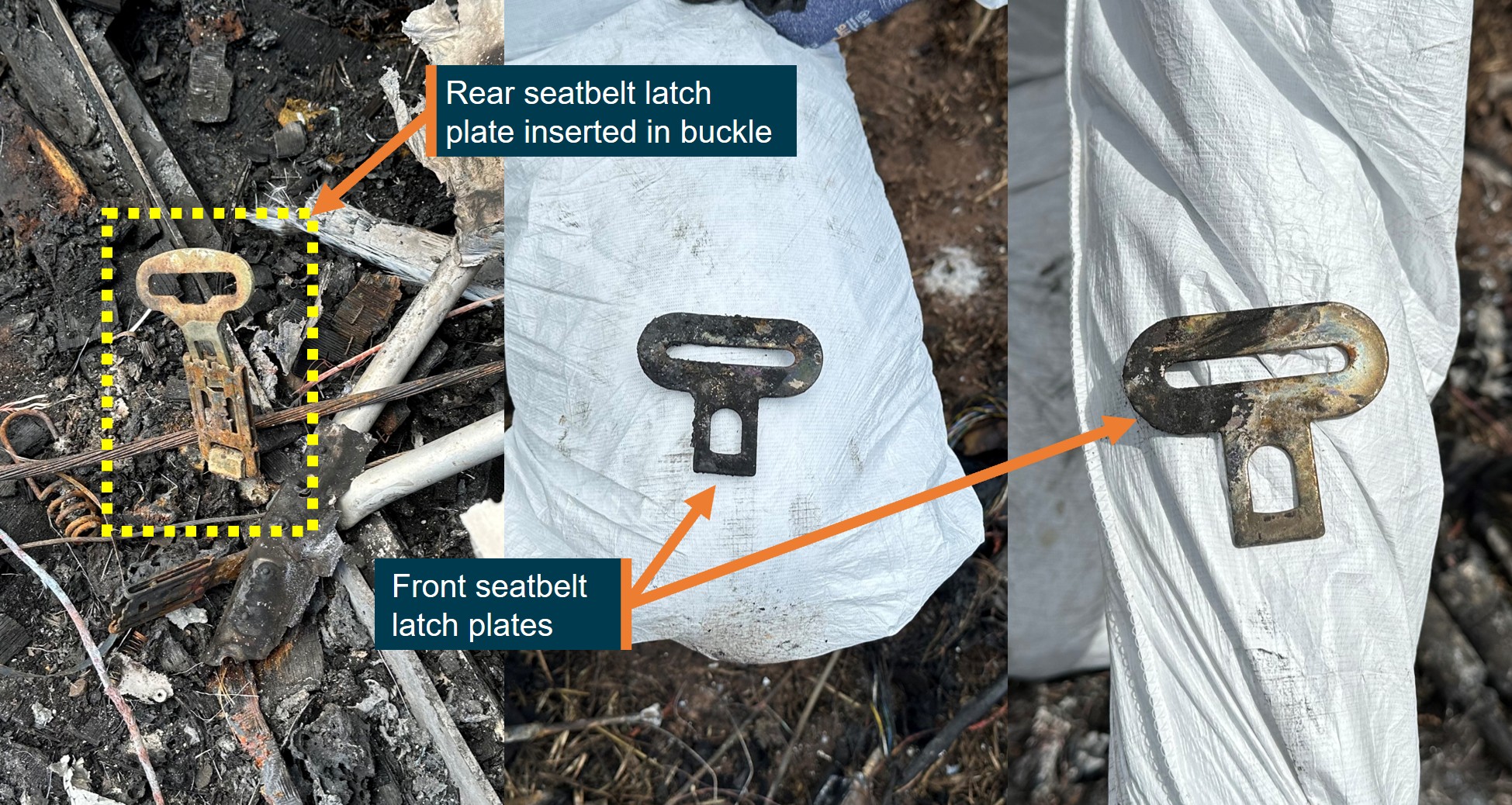
Source: ATSB
Instruments and avionics
The aircraft was fitted with:
- a Dynon Skyview SV-D1000 avionics unit, which provided a primary flight display with a navigation display and engine instruments display
- a 2-channel autopilot system
- analogue airspeed, oil pressure, altimeter, turn/slip and vertical speed instruments.
The instrument panel and instruments were found together in the wreckage, forward of the front seats and behind the engine firewall. All instruments and the panel were destroyed by the impact and fire. However, the Dynon unit was retained by the ATSB for examination (see the section titled Flight path analysis).
Meteorological information
The Bureau of Meteorology provided 30-minute METAR[3] recordings for the East Sale Airport, located about 30 km south-east of the accident site. At 1730, the temperature was 26°C and the wind was 17 kt from 090° T. The visibility was greater than 10 km and no cloud was detected. Similar conditions were recorded at 1800. A local weather station about 4 km north of the accident site recorded the weather data at 5-minute intervals. Table 1 presents the temperature, mean wind and wind gust data recorded at 1745 and 1750 by the local weather station.
Table 1: Local weather station recordings
Time | Temperature (°C) | Wind speed (kt) | Wind gust (kt) | Wind direction (°T) |
1745 | 27.5 | 6.2 | 8.0 | 124 |
1750 | 27.3 | 6.4 | 12.8 | 122 |
Flight path analysis
The aircraft was fitted with a Dynon Skyview SV-D1000 avionics unit, with the capability to record various flight path parameters. The unit was recovered from the accident site and examined at the ATSB facilities. The memory chip was recovered from the internal memory unit and read. However, due to the extensive thermal exposure beyond the specifications of the chip, the data was corrupted and not usable.
Airservices Australia ADS-B data was obtained for the flight path analysis. The data included altitude in 25 ft increments and groundspeed with timings, which were combined with the CCTV camera footage for flight path analysis. A mean wind speed of 6 kt and wind gust speed of 12.8 kt from 124° T were used to calculate a range of estimated calibrated airspeeds (CAS) for each data point.
A trend over the last 3 minutes was noted with the aircraft generally descending from a recorded altitude of 850 ft above mean sea level (AMSL) to 275 ft AMSL, with a low pass at 97 ft above ground level (AGL) during the second left orbit overhead the Macalister River. The groundspeed varied over the last 3 minutes from 103 kt to 71 kt, with a gradual and almost continuous reduction in speed below that recorded during the previous orbit speeds over the last 30 seconds of the flight.
The final turn started at 1746:52 at 64 kt (67–74 kt CAS) and 269 ft AGL. The nose drop observed in the CCTV footage during the final turn, followed by a rapid descent, was indicative of an aerodynamic stall[4] in a steep turn. The stall likely occurred at 1746:59 at 56 kt (59–65 kt CAS) and 221 ft AGL. After the stall there was an abrupt reduction in altitude and increase in speed, consistent with initiation of a stall recovery (Figure 10).
Figure 10: Plot of ADS-B data and CAS calculations
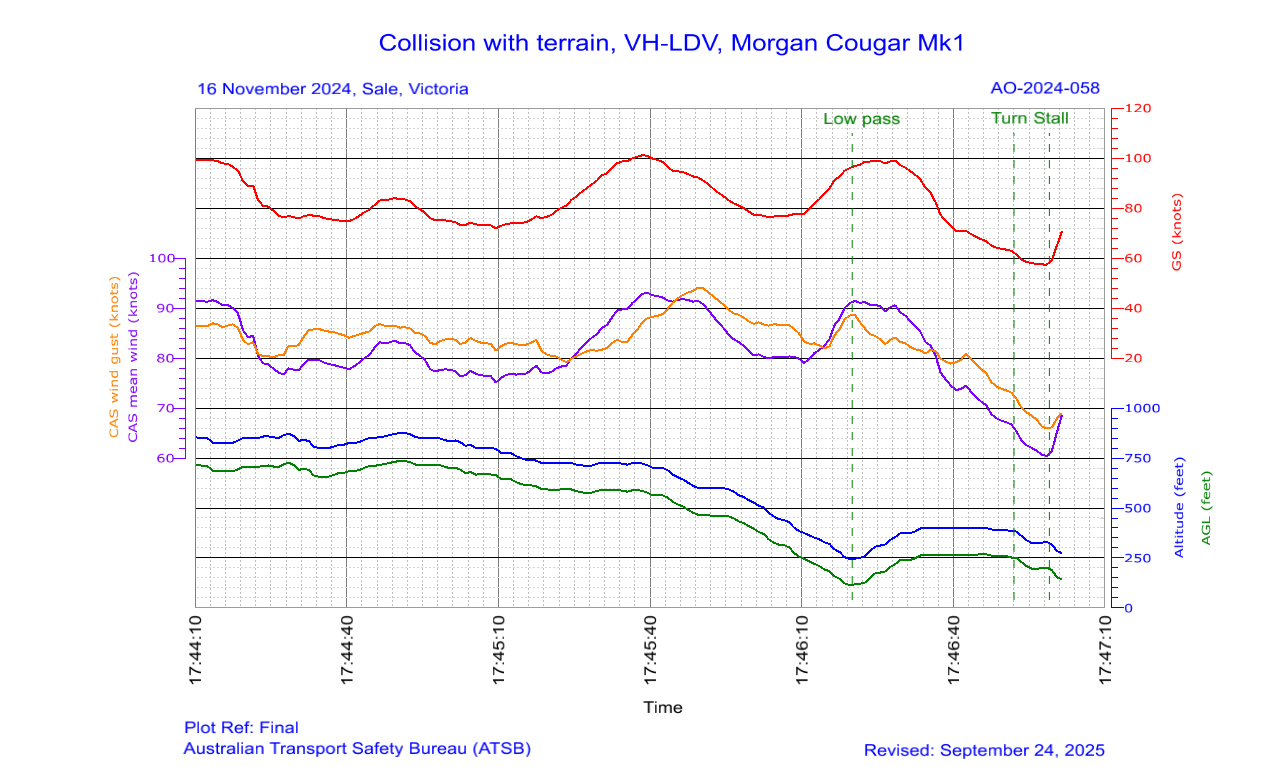
Source: ATSB
The final turn was of a tighter radius than the previous orbits and analysis of the radius of this turn indicated it was consistent with a turn to align with the Macalister River and would have required an average angle of bank of 45° in a steady coordinated turn. The turn radius appeared to reduce during the turn at a relatively constant speed, which would have required an increase in the angle of bank and load factor. For about the last minute of flight, the aircraft was operating below a height of 500 ft, which was the minimum height applicable to this portion of the flight, as prescribed in Civil Aviation Safety Regulation (CASR) 91.267. Further description of each orbit is provided in Appendix B – Flight path description.
Aircraft information
General information
The aircraft was an amateur-built Morgan Cougar Mk 1, registered VH-LDV, issued with a special certificate of airworthiness under the designation: experimental certificate. It was a 4-seat, piston-engine aircraft with a maximum take-off weight of 800 kg. The aircraft was fitted with a Rotax 912 ULS 4-cylinder turbocharged engine and 3-bladed composite (carbon fibre) propeller. The aircraft’s builder sold it to a syndicate of 3 pilots, which included the accident pilot, on 5 November 2024, with its manufacture date recorded as 2013 and with 136.9 airframe hours.
The aircraft build started in May 2013 and the experimental certificate for Phase 1 flight testing was issued by a Civil Aviation Safety Authority (CASA) delegate in December 2015. The experimental certificate for Phase 2, completion of the test flying phase, was issued by the same CASA delegate in April 2017.
Amateur-built experimental aircraft
According to the CASA advisory circular (AC) 21-10 v4.3: Experimental certificates, an experimental certificate may be issued for the purpose of operating amateur-built aircraft, and it does not attest to the airworthiness of the aircraft. CASA AC 21.4(2): Amateur-built experimental aircraft – certification (published in 2000) stated:
An amateur-built aircraft is an aircraft, the major portion of which has been fabricated and assembled by a person or persons who undertook the construction project solely for their own education or recreation.
Amateur builders should call upon persons having experience with aircraft construction techniques…to inspect particular components…prior to closure and to conduct other inspections as necessary.
The AC required an authorised person, or CASA, to only inspect the aircraft once prior to the initial test flight and the inspection should establish that:
• the aircraft is registered and marked in accordance with the requirements
• the aircraft meets the major portion rule
• the weight and balance data is available and the aircraft has been correctly weighed
• the engine(s) and flight controls operate properly
• the pitot static system and associated instruments operate properly.
• Note: The person carrying out the inspection is not responsible for the integrity of the design or construction of the amateur-built experimental aircraft, nor for the identification of any structural design or construction deficiencies — responsibility for the design, construction and integrity of the aircraft rests with the amateur builder.
In accordance with CASA AC 21.4(2), the builder maintained a build-log that detailed the progressive build of the aircraft with photographs and notes. The builder consulted with the designer during the initial build and with both the designer and the CASA delegate for subsequent modifications. The designer of the aircraft was deceased prior to the accident.
Weight and balance
The maximum take-off weight published in the aircraft logbook was 800 kg and the centre of gravity limits were between 2,263 mm and 2,537 mm aft of the datum. The aircraft was reweighed 2 days prior to the accident, which involved transferring all fuel remaining in the wing tanks into the main tank. The transfer process resulted in empty wing tanks and a full main tank.
The weight and balance for start-up and at the time of the accident were calculated and found to be within the published limits.
Builder modifications to the design
The aircraft builder reported to the ATSB that they made several modifications to the original design, consulting with the CASA delegate and designer about the changes. They reported that under the original design, aileron and elevator control was via a stick, with a linear relationship between stick and control surface movement across the full range. However, the stick control required large inputs for small movements of the control surfaces, felt sloppy and was designed with components bolted to the floor in a manner that exposed them to interference from the occupants.
After a taxiing accident in 2019, the builder incorporated modifications, which included a new engine (Rotax) and propeller, yoke controls and roller bearings to eliminate lateral movement (play) in the horizontal stabilator control tube. The builder noted improved climb and cruise performance after the modifications, but reported the greatest improvement was in flight handling.
Following the modifications, the roll, pitch and yaw motions were described as ‘smooth, linear and predictable… There was no slop in the control system and this resulted in the aircraft being responsive without being twitchy.’ The autopilot actuators provided additional resistance and a heavier feel to the original design. The builder reported no noticeable changes to the stall speed or aircraft reaction during a stall after these modifications but recovery from a stall was reported to be quicker than previous.
Aircraft stall warning and characteristics
Stall warning
While not published in the pilot operating handbook (POH), the aircraft was fitted with a stall warning system incorporated into the Dynon avionics unit. The documentation for the unit stated that it provided an audio alert as the angle of attack increased, which started as an intermittent tone and increased in frequency as the angle of attack increased, until it became a continuous tone at the critical angle of attack.[5]
There were 3 options in the settings for how early the intermittent tone activated. The ATSB could not determine what was set or if a calibration flight was conducted. The builder reported that they believed it was factory set and one of the new owners reported they believed there was an angle of attack indicator but no audible stall warning. They further stated that they had not conducted any of their own verification/calibration flights before the accident.
Stall characteristics
The stall characteristics were described in the POH as having about a 10 kt buffet warning before a slow nose drop at the stall until flying speed was regained. The POH’s published ‘straight and level’ clean indicated stall speed was 37 kt. However, after construction, the aircraft was subject to 40 hours of restricted flying operations under Phase 1 of its experimental certificate, which included stall testing. The results from Phase 1 testing were recorded in the aircraft logbook, which indicated the stall speed was found to be 38 kt.
The builder described the aircraft handling characteristics approaching the straight and level clean stall as ‘a mush’ with no sudden nose‑down pitching moment. However, they reported that during a 30° angle of bank left turn, the aircraft started to stall at about 42 kt and then suddenly pitched nose-down with a left yaw. The aircraft was quickly recovered but the builder was reportedly surprised by the different response to a stall in a turn to what was experienced in straight and level flight and hypothesised that a greater angle of bank might exacerbate the response.
The following table presents the indicated stall speeds and load factors in level coordinated turns from wings level to 75° angle of bank and up to a load factor[6] of 3.86, noting the published manoeuvring limit for the aircraft was 4G. The manoeuvring stall speed was calculated by multiplying the 1G stall speed by the square root of the load factor.
Table 2: Calculated stall speeds for increasing angle of bank and load factor
Bank angle | Load factor (G) | Stall speed (37 kt) | Stall speed (38 kt) | Stall speed (42 kt) |
0 | 1.00 | 37 | 38 | - |
30 | 1.15 | 40 | 41 | 42 |
45 | 1.41 | 44 | 45 | 46 |
60 | 2.00 | 52 | 54 | 55 |
70 | 2.92 | 63 | 65 | 67 |
75 | 3.86 | 73 | 75 | 77 |
The builder recalled discussing various types of stalls, including accelerated stalls, with the aircraft designer. However, the designer recommended against the builder testing these characteristics unless accompanied by either the designer or an experienced instructor. The builder did not conduct any stall testing additional to that detailed above.
Stall testing for amateur-built aircraft
In AC 21.4(2), CASA ‘strongly urged’ builders to ‘make detailed reference to the U.S. FAA [Federal Aviation Administration] Advisory Circular AC 90-89, “Amateur-Built Aircraft Flight Testing Handbook”, prior to their flight programs commencing, and follow the guidance provided.’ In accordance with the FAA AC, for straight and level stall testing, the aircraft should be slowed towards the expected stall speed at 1 kt per second and the stall warning should occur about 5 kt before the stall.
The FAA AC stated that a sharp wing drop during stall testing could be regarded as the onset of spin autorotation, and the recommended corrective action is reducing power, full opposite rudder, and lowering the nose to the horizon or below. The guidance for flight testing of accelerated stalls provided the following description:
An accelerated stall is not a stall reached after a rapid deceleration. It is an in-flight stall at more than 1 G, similar to what is experienced in a steep turn or a pull up.
The accelerated stall is based on a closure rate between the aircraft speed and stall speed. Standards for type certified aircraft have historically[7] used a closure rate of 3–5 kt per second for testing accelerated stall characteristics or required a minimum load factor for the test conditions (Gratton, 2015).
A turning manoeuvre is often used for the accelerated stall testing, which can affect the aircraft response. According to Gratton (2015), low wing aircraft tend to roll into the turn during a turning stall and high wing aircraft tend to roll out of the turn. Consequently, certification authorities have historically placed roll limits on the acceptable response of an aircraft during a turning or accelerated stall (Gratton, 2015). Therefore, accelerated stall flight testing may not be recommended for an amateur-built aircraft and the notes within the accelerated stall section of the FAA AC contained the following advice:
Do not attempt this or any other extreme maneuver unless the designer or kit manufacturer has performed similar tests on a prototype aircraft identical to the amateur-builder’s aircraft.
Of note, the reference from Gratton (2015) that low wing aircraft tend to roll into the turn during a turning stall, will, in combination with a nose down pitch, produce a nose low unusual attitude to the pilot. While the correct recovery technique from a conventional stall is to apply power as soon as the wings are unstalled, the standard recovery technique from a nose low unusual attitude is to close the throttle, roll wings level and then pull up (CASA, 2007).
Transition training
Purchase of the aircraft
The builder sold the aircraft due to medical issues that made it difficult for them to inspect and operate the aircraft and inhibited their ability to egress from the aircraft in an emergency. Consequently, the builder did not accompany any potential buyers on their trial flights. The inspections and trial flights of the aircraft occurred at Whyalla Airport, South Australia, and the syndicate that purchased the aircraft were the second interested buyers.
The builder reported that the first interested buyer had about 800 hours experience on slower aircraft, which included experimental kit-built aircraft. The buyer conducted a trial flight accompanied by a more experienced pilot who advised them against the purchase due to the performance difference from their previous aircraft. The accompanying pilot reported to the builder that the buyer was used to flying 80 kt aircraft, not 130 kt aircraft.
The syndicate that purchased the aircraft consisted of a recreational pilot certificate (RPC) holder and 2 Recreational Aviation Australia (RAAus) instructors. The instructors each held a CASA-issued recreational pilot licence (RPL) with navigation endorsement, and one of them was the accident pilot. They arrived together at Whyalla Airport in another light aircraft as the second prospective buyers.
The syndicate conducted several trial flights at Whyalla, and the builder briefed them on the aircraft logbook and the POH but could not recall the specific details of what was covered. The builder believed the syndicate members were going to study the POH the night before their departure from Whyalla and the builder made themselves available the following day to answer any questions but could not recall if any were asked. The syndicate members signed the sale agreement on 5 November 2024 and departed from Whyalla with the aircraft on 6 November.
The builder had no recollection of discussing the aircraft’s banked stall characteristics with them and had never received such a brief themselves in the past when introduced to a new aircraft. They did not advise the syndicate to seek transition training or recommend aerial work exercises as part of their familiarisation process. The builder was aware that 2 of the syndicate members held instructor qualifications with RAAus in addition to CASA licences. Therefore, the builder (who was not an instructor themself) did not think it was necessary to advise them about flight training matters.
One of the syndicate members was concerned about the aircraft’s centre of gravity with rear seat passengers and they agreed to have it reweighed before conducting any of their own verification flights. This was done at West Sale Airport on 14 November 2024, and no significant changes were recorded by the weight and balance organisation.
As the aircraft was in the single-engine class rating of less than 1,500 kg, the syndicate’s RPL-qualified pilots were able to fly the aircraft without additional flying training or qualifications. The ADS-B data history for the aircraft revealed about 7.7 hours were flown by the syndicate from 4 November 2024 until the accident flight, which included 4.5 hours of ferry flights from Whyalla to Moama, New South Wales, and from Moama to West Sale. There were also several check flights associated with rectifying a blocked fuel strainer. While the accident pilot had received dual transition training for other aircraft, which included the Bristell and Pitts Special, this was not undertaken on the accident aircraft.
One of the syndicate members reported that they didn’t think the pilot had the opportunity to do any aerial work exercises in the aircraft before the accident and they suspected that the pilot may not have appreciated the heavier aircraft, in which they had low flying hours. The other syndicate member reported that the pilot had limited flying experience in the aircraft and suspected that the pilot did not understand the risks of what they were doing with respect to steep turns, load factor and the associated effect on stall speed.
CASA flight testing and training advice
CASA AC 21.4(2) included recommended safety precautions for the flight-testing phase, emphasising that:
- a graduated process of familiarisation should be followed, starting with the ground handling characteristics of the aircraft before attempting flight operations
- emergency equipment and personnel should be available before the first flight
- ‘Violent or aerobatic manoeuvres should not be attempted until sufficient flight experience has been gained to establish that the aircraft is satisfactorily controllable throughout its normal range of speeds and manoeuvres.’
The minimum qualifications required for the Phase 1 flight testing was a CASA-issued private pilot licence (PPL) with the appropriate endorsements.
CASA AC 21.4(2) also stated that ‘Flight training will be permitted under certain circumstances, i.e. type endorsement training and training given in the aircraft to its owner.’ A separate section addressed the maintenance aspects for new owners, which prohibited them from certifying for maintenance, and that it must be certified by a Licenced Aircraft Maintenance Engineer (LAME) when no longer owned by the builder. However, there was no recommendation for new owners to seek transition training or for designers or builders to recommend buyers conduct transition training.
ATSB aviation research investigation
The ATSB aviation research report
AR-2007-043(2)
(4.26 MB)
Amateur-built aircraft Part 2: Analysis of accidents involving VH-registered non-factory-built aeroplanes 1988-2010, was published in 2013. It included findings related to the accident and injury rates (with implications for the crashworthiness of these aircraft) and the experience of pilots involved in these accidents, as follows:
Amateur-built aircraft had an accident rate three times higher than comparable factory-built certified aircraft conducting similar flight operations between 1988 and 2010. The fatal and serious injury accident rate was over five times higher in amateur-built aircraft, in particular due to relatively more serious injury accidents.
The pilots of amateur-built aircraft involved in accidents were significantly more experienced overall than factory-built aircraft accident pilots. However, they were significantly less experienced on the aircraft type that they were flying at the time of the accident.
A quarter of accidents were from loss of aircraft control.
The safety action section of the report included initiatives from the Sport Aircraft Association of Australia (SAAA), as follows:
Working with the Civil Aviation Safety Authority (CASA) to provide a legal framework for better training in amateur-built aircraft.
Working with CASA to allow a legal framework for suitably qualified pilots to give instruction in amateur-built aircraft both for the aeroplane flight review (AFR) and transition training for pilots (post-phase one).
The SAAA subsequently produced a Flight Training and Safety Manual supported by their Flight Safety Advisor program. However, a pilot operating an experimental aircraft needed to be a member of SAAA to access these resources.
Federal Aviation Administration advisory circular
In 2012, the United States National Transportation Safety Board published a safety study on The Safety of Experimental Amateur-Built Aircraft (NTSB/SS-12/01). Their study found that pilots who did not seek training were over‑represented in accidents, and that accidents involving loss of control could be reduced with transition training. This led to a recommendation for the FAA to develop resources for transition training and encourage builders and new owners to complete the training.
In 2015, the FAA published AC 90-109(A) Transition to unfamiliar aircraft. The purpose of the FAA AC was ‘to help plan the transition to any unfamiliar fixed-wing airplanes, including type-certificated (TC) and/or experimental airplanes.’ The AC stated that ‘accidents resulting from loss of aircraft control or situational awareness frequently result from pilot unpreparedness for challenges presented by the aircraft’ and provided recommendations for training experience based on aircraft performance and handling characteristics. It contained an extensive section on stall characteristics, which included the following points:
There are no rules for stall behavior with experimental airplanes.
Some experimental airplanes can be flown in a carefree manner with the stick all the way back, while others can depart controlled flight dramatically without any perceptible warning.
Since amateur-built airplanes are built by individuals, there can be a wide variation in the stall behavior of identical models.
Receive training in your airplane on stall avoidance and recovery from a qualified instructor, preferably with recent experience in the make and model.
Periodically practice stall avoidance, entry, and recovery at a safe altitude after you have received enough instruction to feel comfortable. Stall recognition and recovery should not be self-taught. Your first experience should not come from an inadvertent stall that catches you by surprise.
The appendices of the FAA AC provided a list of families of aircraft, based on their characteristics, with examples of experimental aircraft within each family. The accident aircraft was described to the ATSB as being responsive by the builder and very responsive by one of the syndicate members. Appendix 3 of the FAA AC was for aircraft with rapid flight control response, and it included the following information:
There are many more experimental airplanes that may look more like type-certificated (TC) airplanes, but they actually have light control forces and/or very quick maneuvering response. The hazard of light forces and rapid response is that without some level of training, the pilot may over-control the airplane.
Best Training. The best training is accomplished in the specific airplane the pilot intends to fly with a well-qualified instructor who has recent experience in the specific make and model.
In this case, the accident pilot had conducted transition training on the Pitts Special aircraft with an instructor who also had experience with the Morgan Cougar Mk 1 aircraft, though not the accident aircraft. The instructor’s experience with the Morgan Cougar included flying them and modifying them to improve their handling qualities. This offered the accident pilot an opportunity to undertake transition training for the Morgan Cougar Mk 1 that would have been consistent with the ‘best training’ model recommended in FAA AC 90-109(A).
Crashworthiness and survivability
Occupant positions and injuries
The seating configuration during the flight was the pilot in the front left seat, a passenger in the front right seat and a second passenger in the rear right seat. A full autopsy was conducted on the pilot, and a computed tomography scan and external examination was conducted on the 2 passengers at the Victorian Institute of Forensic Medicine. Toxicology analysis of blood was conducted for all occupants.
The examinations for all occupants revealed extensive non-survivable blunt force trauma injuries to the head, chest and lumbar spine. Examination of the pilot indicated that they were deceased prior to the fire. Toxicology results found no ethanol, common drugs or poisons, and carboxyhaemoglobin (an indicator of carbon monoxide exposure) was not detected.
CREEP methodology
The CREEP methodology used for analysing the crashworthiness and survivability of aircraft accidents is based on:
- Container – maintain a liveable volume
- Restraint – retain the occupants in their seats and the seats to the airframe
- Energy attenuation – minimise the transmission of forces to the occupants
- Environment (local) – minimise the lethality of the cockpit and cabin to flailing injuries
- Post-crash factors – egress and minimise the risk of drowning, fire and fumes.
Container
The occupied cabin area of the aircraft was visible, though significantly damaged from fire and the underside compromised from the ground impact. The outline of the cabin was discernible and displayed dynamic deformation of the structure supporting the front seats and the main spar located underneath the front seats, which is discussed further in the following sections.
Restraint
The pilot and front right seat passenger were ejected from their seats during the accident, and their seatbelt latch plates were found separated from their respective buckles. The rear seat occupant appeared to have remained restrained and was found in the rear right seat location with their seatbelt latch plate attached to the buckle. The pilot was seen wearing a 3-point harness in videos taken during the accident flight. Therefore, it was considered very likely that all 3 occupants were wearing their seatbelts.
According to the build log, the front seats were from a Toyota Prado motor vehicle, and the seatbelts were connected to the seat mounts and airframe with their shoulder straps extending from centre to outboard, where the buckles were located. Regarding seatbelts, AC 21-4(2) para 7.3 stated:
It is strongly recommended that US [United States] FAA [Federal Aviation Administration] Technical Standard Order (TSO) approved or equivalent seat belts be installed along with approved shoulder harnesses.
According to the build log, the builder conducted load testing of the seat belts in accordance with FAA AC 23-4 Static strength substantiation of attachment points for occupant restraint system installations. This involved the application of a simulated 4G load (400 kg) downwards and forwards to test the seats and seatbelt attachments, which they passed. The TSO specified the minimum performance standards were those in the Society of Automotive Engineers Aerospace Standard AS 8043 (1986), which included the following information:
Pelvic Restraint: A torso restraint system shall provide pelvic restraint whether or not an upper torso restraint is used. Pelvic restraint shall not incorporate emergency locking retractors (inertia reels).
Release: A torso restraint system shall be provided with a single buckle having a single motion release which is readily accessible to the occupant to permit easy and rapid egress by the occupant from the assembly. The buckle release mechanism shall be designed to minimize the possibility of inadvertent release.
A review of car and aircraft seatbelt images revealed a general difference between the design. Car seatbelt latch plates are threaded through the strap connected from the shoulder to the pelvic anchor point on the shoulder strap side. The inertia reel applies the tension, and emergency locking under acceleration, when the latch plate is inserted in the buckle on the opposite side. Therefore, the pelvic restraint (lap belt) incorporates an inertia reel because it is part of the upper torso restraint mechanism.
The aircraft builder confirmed that this was the design of the front seatbelts fitted to the aircraft and that they were probably car seatbelts. The inertia reel was located at the shoulder anchor point on the inboard side of the seats and the shoulder strap extended down to the inboard pelvic anchor point with the latch plate threaded through the strap. The inertia reels at the shoulder anchor points provided the tension and emergency locking under acceleration for the front seat occupants.
Seatbelts can fail due to overload, which is why strength tests are conducted, and they can also fail to perform a required function, such as restrain the occupant during a collision. Roberts et al. (2007) described 3 known failure modes associated with car seatbelt design as follows:
- inadvertent unlatching when the buckle is unlatched due to occupant flailing contact with the release button during an accident
- false latching when the buckle fails to engage completely, but gives the user the impression that it is properly fastened due to its partial engagement
- inertial unlatching when the buckle unlatches due to inertial forces resulting from impacts and the associated impulse accelerations during planar collisions and rollovers, which is an example of a component failing to perform a required action.
Energy attenuation
All 3 occupants had fractures of the lumbar spine and the 2 front seat occupants both had crush fractures of the fifth lumbar (L5) vertebra. According to Shanahan (2004) light fixed‑wing aircraft provide little crushable structure to attenuate collision forces. However, 2 areas where energy attenuation can be incorporated into the design are the landing gear and seating. The main landing gear for the Morgan Cougar aircraft was a rigid single-piece structure with the wheel axles attached to the structure. It separated on impact and there were no oleos for energy attenuation incorporated into the design.
The rear seats were upholstered 4 mm plywood mounted to the cross-members. The front seats were car seats, which were attached to cross-members and had the main wing spar underneath them. The front right seat pan was found collapsed onto the wing spar and the left seat pan had separated and was found forward of the front seat frame structure. None of the seats incorporated any recognisable form of energy attenuation.
According to Stech and Payne (1969), the G-loading strength of the L5 vertebra for a 160 lb (72.6 kg) male is around 25G. The 25G limit was acknowledged by Shanahan (2004) with the following caveat:
However, poorly designed seats can produce spinal fracture in impacts as low as 8-10G. Typically, spinal fractures in low to moderate velocity crashes are caused by mounting seats above rigid panels or other non-frangible objects such as batteries and from mounting relatively rigid seats directly on bulkheads or over beams. In the first case, seats collapse onto unyielding objects causing the occupants to experience excessive vertical accelerations. In the latter case, rigid bulkheads or structural members transmit excessive forces from the ground directly to the seat occupants.
According to Taylor and Moorcroft (2023) from the FAA Civil Aerospace Medical Institute, special energy attenuating seats are used to provide a controlled deceleration over a vertical stroking distance to keep aircraft crash loads within human tolerance. While there are many methods to achieve a controlled deceleration, some of the simplest and lightest methods include collapsible sheet metal boxes for the seat pan structure and/or the use of rate sensitive foams for the seat pan cushion.
CASA AC 21.4(2) para 7.3 recommended safety considerations for the design of the cockpit and seatbelts to reduce injuries to the pilot and passengers in the event of an accident. It also strongly recommended the use of FAA TSO seatbelts and shoulder harnesses. However, there was no recommendation for the designer or builder to consider energy attenuation for the occupants, specifically the energy attenuation of seating.
Environment (local)
The local environment was not considered to be a significant contributing factor in this accident due to the severity of the occupants’ spinal injuries (indicative of excessive vertical forces) and because the front seat occupants were ejected from their seats. In addition, CASA AC 21-4(2) para 7.3 recommended the ‘delethalization’ of the cockpit as follows:
The design of the cockpit or cabin of the aircraft should avoid, or provide for padding on, sharp corners or edges, protrusions, knobs and similar objects which may cause injury to the pilot or passengers in the event of an accident.
Post-crash factors
The aircraft was designed with a main fuel tank located between the engine firewall and the instrument panel. This made it susceptible to crushing forces in an impact and presented a risk of fuel spray onto the occupants and onto the engine as an ignition source, which occurred in the accident. The fire damage to the aircraft was centred on the cabin and engine area with die-back of the grass evident in a diamond pattern from the initial impact to the point of rest.
The builder modified the original design to incorporate wing fuel tanks in the design, located aft of the main wing spar. The modified wing tanks were not compromised by the collision. The importance of fuel tank location on post-crash survival was described in Johnson et al. (1980 and 1989) Aircraft Crash Survival Design Guide Volume V – Aircraft Postcrash Survival as follows:
The location of the flammable fluid-carrying tank in an aircraft is of considerable importance in minimizing the postcrash fire hazard from a tank installation. The location must be considered with respect to occupants, ignition sources, and probable impact areas.
Greater distance between occupants and fuel supply tends to increase escape time in the event of a fire because it reduces the likelihood of fuel entering the occupied area. Also, the tank should be kept away from probable ignition sources… Another important consideration is the location of tanks with respect to probable impact damage. Accident histories show repeated tank ruptures and consequent fires…, indicating the tank’s high degree of vulnerability to damage from surrounding structures.
As much aircraft structure as possible should be allowed to crush before the tanks themselves are exposed to direct contact with obstructions.
CASA AC 21.4(2) para 7.4 recommended reducing the risk of fire hazard, and the inclusion of a fireproof firewall between the engine compartment and the cabin. However, it did not recommend or advise on how to incorporate crashworthiness into the design of the fuel system.
Pilot information
Qualifications
The pilot held a:
- Recreational Pilot Licence (Aeroplane) (RPL-A), issued by CASA on 6 August 2024, with a single-engine aeroplane class rating and manual propeller pitch control endorsement
- Class 2 aviation medical certificate, issued in June 2024.
The RPL licence was granted in recognition of the pilot holding a recreational pilot certificate (RPC) with RAAus in accordance with Civil Aviation Safety Regulation (CASR) 61.480. In addition, the pilot held an RAAus-issued instructor rating and had accumulated 506.8 hours according to their last logbook entry, dated 7 August 2024.
Flight training
Recreational aviation flight training
The pilot started flying training with RAAus at Adventure Flight Training (AFT) school in Moama, New South Wales, on 11 April 2022 for their RPC. The pilot passed their RPC flight test on 20 September 2022, and was endorsed with passenger carriage later in 2022, and with navigation and formation in 2023. All flight tests and endorsements were conducted and certified by the AFT chief flying instructor (CFI).[8]
On 8 May 2023, the pilot started their RAAus instructor training at AFT and passed their instructor flight test at Bendigo, Victoria, on 7 July with an external testing officer. The pilot started delivering instructional flights at AFT on 16 July 2023.
On 19 December 2023, the pilot passed their senior instructor flight test with the AFT CFI and on 3 January 2024, the CFI endorsed the pilot’s logbook with the entry ‘meets the requirements for senior instructor rating iaw RAAus syllabus of flight.’ However, the pilot had not completed the theory exam requirement to be a senior instructor and their rating for senior instructor was not issued by RAAus.
General aviation flight training
The pilot’s logbook had entries for the following general aviation training flights in 2024:
- On 5 June, the pilot started dual flying training in the Pitts Special aerobatic biplane at Latrobe Valley and recorded 0.7 hours.
- On 6 June, the pilot successfully completed a flight review of 2.5 hours duration with a controlled airspace/aerodrome endorsement in a Cessna 152 (a flight review was required to exercise the privileges of a CASA RPL, which was issued in August).
- On 6 June, the pilot recorded a further 0.5 hours of dual flight training in the Pitts Special.
- On 1 July, the pilot recorded 3.1 hours of dual aerobatics training in the Pitts Special.
While the ATSB was informed that the pilot’s flying in the Pitts Special was for the purpose of an aerobatics endorsement, the flight training school (FTS) where the pilot conducted their RPL flight review did not have them enrolled for an aerobatics endorsement. In addition, CASA reported that they did not have an aerobatics endorsement record for the pilot. The ATSB reviewed the pilot’s flight training records for the Pitts Special and concluded that the activities were consistent with transition training onto the Pitts Special, which included stalls and spins, and not an aerobatics course.
The ATSB spoke to a member of a local aerobatics team, who knew the accident pilot, and they confirmed there had been discussions about the possible use of the accident pilot to ferry their Pitts Special aircraft to an airshow at the end of August 2024. However, the pilot did not meet the minimum experience requirements for insurance purposes and the plan was cancelled.
On 9 November 2024, a general aviation flight instructor and RAAus CFI conducted a check flight with the accident pilot at the Echuca Aero Club in the club’s Piper Archer aircraft. This was a requirement to be able to hire the aircraft. The instructor conducted a standard aerial work check flight with the pilot and did not identify any deficiencies in flying skills.
Theory examinations
Recreational aviation theory examinations
The pilot’s logbook had a record of aviation theory examinations (exams) in accordance with the following table:
Table 3: Pilot's theory exams
| Date | Theory exam |
| 31 May 2022 | Pre-solo |
| 20 June 2022 | Air legislation |
| 29 June 2022 | Basic aeronautical knowledge |
| 13 August 2022 | Radio |
| 13 August 2022 | Human factors |
| 4 December 2022 | Navigation theory [includes meteorology theory] |
| 21 May 2023 | RAA instructor rating |
The AFT CFI was recorded as the delegate for all of the pilot’s theory exams in their logbook. Another AFT instructor reviewed the exams recorded in the pilot’s logbook and reported that:
- the theory exams were conducted online and unsupervised
- the correct answers to all questions were revealed after the first attempt so that any incorrect answers could be corrected with a second attempt
- no knowledge deficiency reports were provided.
The ATSB reviewed the software used by AFT to conduct the theory exams and found that the settings allowed multiple attempts and revealed all the correct answers in a report provided to the candidate.
PPL(A)-equivalent examination
To become a senior RAAus instructor, a candidate must pass either the RAAus PPL(A) (aeroplane) equivalent exam, or the CASA PPL(A) exam. The RAAus PPL(A)-equivalent exam was a multi-choice exam in which each question had 4 options to select from.
On 3 January 2024, RAAus received the pilot’s application for upgrade to senior instructor, certified by the AFT CFI as the examiner, with a copy of the pilot’s instructor exam from 21 May 2023 attached. This exam was completed using the AFT online system. The ATSB did not find a record of the initial response to this application but based on the available evidence, it is likely that RAAus staff identified that the incorrect exam had been submitted in support of the application and reported this to the AFT CFI.
On 12 January 2024, the pilot completed the RAAus PPL(A)-equivalent exam using the AFT online system and a pass mark of 94% was recorded. However, the marking rubric for this exam had not been provided to AFT as this exam was marked by RAAus staff. As no marking rubric was provided, the AFT exam software provider had set answer ‘A’ as the default correct answer to all questions for this exam and notified the AFT CFI of this action. The accident pilot had selected answer ‘A’ to 47/50 questions.
When a copy of the pilot’s exam was provided to RAAus and re-marked it was identified that the actual result for the accident pilot’s exam was 26% (13/50).
On 29 January 2024, RAAus sent an email to the AFT CFI to report the result and express their concern about the result and the process used to mark the exam. They also notified the CFI that the pilot’s application for senior instructor would not be processed and that the pilot would:
- need to complete another PPL(A)-equivalent exam
- continue to require direct supervision (in-person) when instructing.
Re-attempt of PPL(A)-equivalent exam
On 24 February 2024, an external CFI[9] supervised the pilot’s re-attempt of the RAAus PPL(A)-equivalent exam at Moama Airfield. This CFI reported that the pilot arrived with a copy of the exam paper questions and that after the exam was completed, the CFI submitted it to RAAus for marking. They did not follow up as to how the pilot obtained a copy of the exam paper. Instead, they passed the information on to RAAus, who also did not enquire how the pilot had obtained the exam questions.
The AFT CFI reported that they believed the pilot had taken a blank answer sheet and not a copy of the exam paper to the exam. The answer sheet is a document with a table for the candidate to annotate the answer to each question. However, the pilot annotated their answer to each question on a copy of the exam paper, not an answer sheet, and it was this exam paper that was certified by the supervising external CFI and submitted to RAAus for marking.
The second exam result, marked by RAAus, was 76% (37/50), which was less than the required pass mark of 80%. This was the same exam paper, with the same questions and answers, that the pilot had previously attempted in January.
Pilot exam outcomes
The RAAus PPL(A)-equivalent exam included 3 questions about aerodynamic stalling, including about factors that change the 1G level flight stalling speed. For the pilot’s attempt on 12 January 2024, the pilot selected answer A to all 3 questions and they were all marked correct. However, 2 were correct and 1 was incorrect according to the RAAus marking rubric.
For the pilot’s re-attempt on 24 February 2024, the pilot changed all 3 answers with the result that 1 was correct and 2 were incorrect. While the pilot correctly answered one question that the stall speed increases in a steep turn, they incorrectly answered another question about the relationship between angle of bank, load factor and stall speed.
On 29 February 2024, RAAus sent an email to the AFT CFI to report the failed second exam attempt by the pilot. On this occasion they stated:
Of more concern is the type of errors made, which include several stalling questions and poor Part 91 regulatory understanding among other items. I understand you have already spoken to [the pilot] and advised [them] of this, but I will call [them] to discuss as well.
RAAus expressed concern about the reported preparation process of reviewing current exam papers which ‘could be considered an attempt at rote learning of questions rather than developing a deeper understanding of the underpinning knowledge required of a RAAus Senior Instructor.’ RAAus reiterated previous comments they had made, that the pilot should re-attempt the exam ‘only after appropriate study of aviation textbooks and regulatory references.’
The ATSB noted other incorrect questions of concern for an instructor, in addition to the questions about stalling and Part 91 regulations identified by RAAus. They included knowledge of the instruments affected by a blocked static pressure system and the interpretation of an aerodrome weather forecast. The questions about stalling and pressure instruments were in the RPC syllabus, and knowledge of weather forecasts and reports were in the navigation endorsement syllabus. At the time they were attempting the PPL(A)‑equivalent exam, the pilot was delivering instruction for both syllabi.
The ATSB queried RAAus as to whether they had considered imposing any restrictions or limitations on the pilot’s instructor rating after the second exam result, noting their concern about the pilot’s knowledge deficiencies. RAAus responded that by not processing the pilot’s upgrade to senior instructor, the pilot was required to remain under the direct supervision of a CFI, which was their risk management strategy until the pilot’s knowledge deficiencies could be addressed.
A copy of the 29 February 2024 email sent from RAAus to the AFT CFI appeared on the accident pilot’s RAAus member file. However, the pilot’s member file did not include any record of a follow-up about the exam result or progress towards completing any further attempts. Phone call records indicated that a follow-up from RAAus to the pilot did occur on 29 February 2024, but the details of the call could not be recollected.
Commercial pilot theory examinations
Instead of studying the CASA PPL theory, the pilot started studying for their CASA aeroplane commercial pilot licence (CPL-A) theory component, which consisted of 7 exams. The pilot attempted and passed their first CPL-A exam on the subject of aircraft general knowledge (CSYA) with a result of 93% on 10 July 2024. The knowledge deficiency report (KDR) had 3 items listed, which indicated a score of 37/40 questions answered correctly.
On 25 July 2024, the pilot attempted, and failed, the CPL-A aerodynamics exam (CADA) with a result of 63%. The KDR had 15 items listed, which indicated a score of 25/40. The incorrect answers were from a range of topics that included 2 questions on stalling. The 2 incorrect answers on stalling included the effect of using ailerons when approaching and during the stall, and the effect of manoeuvring on the level flight stall indicated airspeed.
On 7 August 2024, the pilot re-attempted the CPL-A aerodynamics exam and passed with a result of 75%. There were 10 items in the KDR, which indicated a score of 30/40. The 2 CPL-A aerodynamics exam KDRs included 3 errors in each of the topics of stalling, stability and control (longitudinal, lateral and directional), and control surface feature. Other items on the KDRs included:
- the lift and drag formulae
- dynamic pressure
- basic forces on an aircraft in level flight
- factors affecting turn performance
- angle of attack required for various flight situations.
Risky flying behaviour and counselling
Background
During the investigation the ATSB interviewed the AFT CFI and associates of the pilot, including:
- 2 other instructors from AFT
- 3 AFT RPC graduates from Moama
- the airport operator, who was also a local aerobatic pilot
- a local general aviation instructor and RAAus CFI.
Each of them recalled experiencing instances of risky flying behaviour involving the accident pilot, or knowledge of this behaviour and counselling. The ATSB also interviewed RAAus staff to determine if they had received any reports of the pilot engaged in risky flying behaviour.
Risky flying behaviour
A fellow AFT instructor from Moama, who was also a syndicate member in the purchase of the aircraft, reported that the accident pilot had a history of conducting low and slow steep turns. While they had steep turn flying training experience themselves, they were accustomed to entering a steep turn from cruise airspeed and were concerned about the pilot’s practice of entering steep turns at slow speed. They had experienced this personally as a passenger with the pilot, as they were co-owners of a Jabiru aircraft, and were aware of reports of similar instances from the pilot’s students.
The instructor had also witnessed the pilot conduct dumbbell turns in the circuit with students in light wind conditions. This involved the pilot conducting a reversal turn shortly after take-off to land on the reciprocal runway for student landing practice, rather than completing a full circuit between landings. They suspected the pilot had learned this from the AFT CFI as they had previously witnessed the CFI conduct this same manoeuvre in light wind conditions.
The other member of the syndicate in the purchase of the aircraft was an AFT RPC graduate from Moama in 2024. While they had conducted their RPC at AFT, they did not fly with the pilot until near the end of their flying training, at which point they were doing most of the flying. They did not observe any risky flying behaviour from the pilot but were advised by others at the school that the pilot had previously received counselling for risky flying behaviour.
Another fellow AFT instructor reported that the pilot could fly an aircraft well but ‘pushed the limits’. They recalled an example of a private flight in the pilot’s Jabiru, in which the pilot held the aircraft on the runway as it accelerated significantly beyond the take-off speed and then performed a pull-up into a steep climb. They stated that they immediately asked the pilot to lower the nose.
During the same flight, the pilot reportedly conducted low-level steep turns and a swooping manoeuvre over a friend on the ground. The instructor reported that they repeatedly verbally intervened throughout the flight, and that they didn’t like how the pilot was flying and asked them to stop and return to the airport after about 30 minutes.
Another AFT RPC graduate from Moama reported that during a local recreational flight on 1 November 2024 in the pilot’s Jabiru, which had a stall airspeed of 45 kt, the pilot conducted a low-speed steep turn overhead a friend driving a tractor. The combination of low speed and steep angle of bank made them feel uncomfortable and they assessed that the aircraft did not have sufficient lift for the manoeuvre. The pilot reportedly noticed their discomfort and told them not to worry as they were still at 60 kt (airspeed). ADS-B data recorded a minimum groundspeed of 57 kt during this turn.
The AFT graduate had previously conducted their RPC pre-check flight with the pilot in August 2023, which included stalls and steep turns in a Topaz aircraft with a stall speed of 44 kt. They reported that the steep turns demonstrated by the pilot then were at least 60° angle of bank, which made them feel uncomfortable and they noted that the pilot appeared to be pushing the aircraft to its limits in a confident manner.
Another RPC graduate interviewed by the ATSB had transferred from the CASA-issued PPL system to the RAAus-issued RPC system and completed their flying training with AFT at Moama. Three days prior to the accident, the pilot invited them on a local area private flight in the accident aircraft. During the flight, the pilot reportedly turned off the transponder and conducted a low-level, high-speed pass over a friend’s house, followed by a wingover.[10] The pilot then demonstrated the responsiveness of the aircraft by conducting a series of level steep turns. The witness reported that the angle of bank was more than 60° and felt like 70–75°, which they described as ‘knife-edge stuff’.
Counselling
The Moama Airfield operator and local aerobatic pilot knew the accident pilot from the AFT school at Moama. The operator had taken the pilot flying in their own aerobatic aircraft and found them to be a very enthusiastic young aviator. Their impression was that the pilot was attracted to the sport aviation side of the industry. In September 2024, the operator was contacted by the AFT CFI about reports of unsafe flying, which included instances of low-level flying and manoeuvring overhead a local football match.
The airfield operator investigated the reports and found that it was likely the accident pilot who had been conducting steep turns overhead the Moama football ground during a match. They approached the pilot in late September and stressed the need for them to fly respectfully and emphasised staying above the minimum requirements and not to orbit overhead properties. They thought that the pilot accepted the counselling in a positive manner.
A local general aviation instructor and RAAus CFI, who was involved in establishing an FTS near Moama, also received a report that the pilot had been observed conducting aerobatics overhead a local football match. They responded to the reporter that the pilot would not be allowed to instruct for the school with that flying behaviour. The pilot subsequently contacted the CFI and visited them on the afternoon of 1 November 2024 to discuss the reported incident. The pilot was reportedly adamant that they had not conducted aerobatics overhead the football match but acknowledged that they had conducted steep turns overhead the match.
At the time of the visit, the CFI had also heard reports that the pilot had been conducting dumbbell turns in the circuit with students. Consequently, they used the visit from the pilot as a counselling opportunity, specifically pointing out that a solo student might try to imitate the pilot’s flying and lose control of the aircraft. The CFI thought that the pilot accepted the counselling in a positive manner.
The AFT CFI reported to the ATSB that prior to the cessation of AFT operations in August 2024, they had regularly engaged in coaching and counselling sessions with the pilot. However, after they ceased AFT operations, they received multiple calls from members of the local community raising concerns about a Jabiru aircraft flying in a manner perceived to be unsafe. While the pilot was not confirmed, the context of the reports led them to believe that the flights were operated by the accident pilot.
The AFT CFI reported that several weeks prior to the accident they had a candid conversation with the pilot and urged them to continue flying safely and responsibly. They stressed that the pilot needed to be even more alert and disciplined without direct oversight. However, as they were no longer responsible for formal oversight of the pilot, they elected to contact others who could potentially mentor the pilot. This included the Moama Airfield operator.
RAAus advised the ATSB that, prior to the accident, they had not received any reports or complaints about the pilot’s flying behaviour, nor were they aware of the pilot receiving any counselling. However, following the accident, they received a report from the AFT CFI that they had been managing the pilot’s behaviour.
RAAus interrogated their occurrence management system for any complaints involving unidentified aircraft and/or pilots in the Moama region and found none. They stated that if they had received a report of an instructor involved in risky flying behaviour, there would have been a ‘fairly swift response’ because they would not want the individual working as an instructor, and potentially indoctrinating students to that behaviour.
Recreational Aviation Australia
Structure
Recreational Aviation Australia (RAAus) is a CASR (Civil Aviation Safety Regulation) Part 149 approved self-administering aviation organisation (ASAO). In 2025, RAAus had 14–15 full time employees in the following areas:
- flight operations
- maintenance and airworthiness
- safety
- finance
- information technology
- administration.
According to the RAAus website, they had 10,000+ members in 2025, and were the largest administrator of pilots, maintainers and aircraft in Australia.
RAAus were authorised by CASA to conduct their activities in accordance with their approval certificate, the Part 149 Manual of Standards and their approved Part 149 Exposition. As a sport aviation organisation, RAAus was oversighted by the CASA Sport and Recreation Aviation Branch (CASA Sport).
The structure of RAAus, with their key personnel in accordance with their Exposition, is depicted in Figure 11.
Figure 11: Recreational Aviation Australia structure
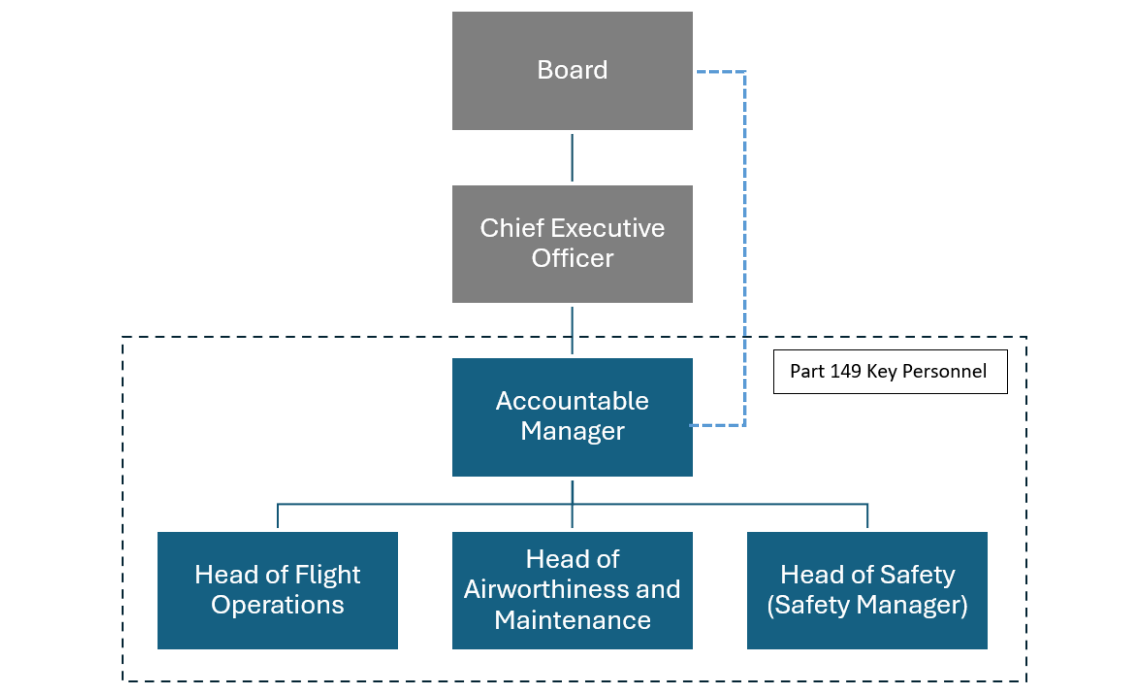
Source: Recreational Aviation Australia
The RAAus Part 149 approval certificate authorised RAAus to administer several aviation administration functions and their sub-functions. The function of relevance to the ATSB’s investigation was Part 149 Flight Training Organisations:
Administer a person that conducts flight training, or flight tests, in relation to a Part 149 aircraft.
The sub-functions were listed as follows:
1. Assessing a person’s organisation, and its procedures, practices, personnel and facilities to determine whether the person is capable of conducting flight training, or flight tests, in relation to the aircraft
2. If satisfied as mentioned in paragraph 1, issuing an authorisation to the person to conduct the activities specified in the authorisation
3. Assessing whether a person to whom the ASAO has issued an authorisation continues to be capable of conducting the activities covered by the authorisation
4. Approving aeronautical examinations that may be conducted by a Part 149 flight training organisation to assess candidates undertaking flight training.
Flight training schools
In 2025, there were about 160 RAAus flight training schools (FTSs). Student pilots, converting pilots and pilot certificate holders could only undertake flight training with an RAAus FTS approved by the RAAus Head of Flight Operations (HFO). An FTS could only operate when a CFI was approved in accordance with the RAAus flight operations manual (FOM). The FOM also required FTS instructors to be directly supervised by the CFI, or another senior instructor approved by RAAus, with indirect (remote) supervision of senior instructors permitted.
In February 2022, RAAus published version 1.1 of their Recreational Aviation Advisory Publication on instructor supervision requirements. This was published to address the enquiries RAAus had received from their members about the instructions in the FOM. Direct supervision of instructors was in-person and was required to be provided by the CFI or approved senior instructor. The intention of the direct supervision requirement was to ensure the supervisor was physically present at the location where the training was conducted to provide continuing mentoring and development for their instructors.
The CFI oversight responsibilities included 90-day check flights of their instructors and 12‑monthly check flights of their senior instructors, which were called standards and proficiency checks. To become a CFI, an individual was required to progress through the qualifications of RPC, instructor and senior instructor. A senior instructor could be appointed to supervise an FTS in the CFI’s absence if they met the requirements of the RAAus FOM and were approved by the HFO.
Flight training school exams
Each RAAus FTS qualification had a flight test and one or more associated theory exams. The theory exams were written by RAAus and sent to the FTS CFIs via email. For each exam, answer sheets were provided for the candidates to record their answers to a selection of multiple-choice exam questions. The syllabi for the theory exams were published in the RAAus syllabus of flight training.
Before accessing the exams, each CFI was required to sign a declaration acknowledging that they had read the conditions of use and would ensure the necessary processes had been implemented at their FTS. The declaration included:
Multiple Choice Examinations. These are not to be distributed and/or reproduced electronically and must be stored securely.
The FTSs were provided with the marking rubric for each exam and were responsible for marking, filing and recording of the results of each exam. The exception to this was the upgrade from instructor to senior instructor for which the exam requirement was either the CASA PPL(A) exam or the RAAus PPL(A)-equivalent exam. RAAus marked the PPL(A)-equivalent exam and did not provide the FTSs with the marking rubric for it. Prior to 2023, RAAus did not require proof of completion of any exams. In 2023, the RAAus instructor upgrade form was amended to require proof of exam completion for the upgrade to senior instructor only.
Flight training school oversight
The RAAus Exposition included an audit program to fulfill sub-functions 1 and 3 of their Part 149 Flight Training Organisations function. Sub-function 1 was for the assessment to issue FTS status while sub-function 3 was for the monitoring of the FTS, which was required to be conducted at least once in every 2-year period.
The RAAus audit activities included:
- desktop
- onsite
- special purpose audits
- health checks
- periodic reviews
- renewals.
The CFI was the only individual from the FTS who was required to be in attendance for an onsite audit and was interviewed as part of the audit process. Other staff members could be interviewed on an opportunity basis, but students were not interviewed as part of a routine audit.
Given the large number of FTSs and the limited number of RAAus staff available for oversight, RAAus developed a risk and audit matrix to determine the type and frequency of audit activity. The matrix produced a performance indicator (PI) score for each authorisation holder. The RAAus audit manual provided the following statement for FTSs assessed as higher risk:
Where resourcing permits, authorisation holders who fall within the highest 10 PI [performance indicator] scores shall only be eligible for an on-site audit and should be scheduled within the following 6 months.
When an authorisation holder within the highest 10 PI scores was scheduled for an onsite audit, the audit team would identify other authorisation holders within the local area who would also be audited during the visit.
Occurrence management system
RAAus had an occurrence and complaints management system (OCMS) database supported by an occurrence and complaints handling manual (OCHM). According to the OCHM:
Any person may report a safety concern or confidential complaint relating to an RAAus member and aircraft. A confidential occurrence may be lodged through the RAAus Occurrence and Complaint Management System (OCMS).
Apart from those OC [occurrences] that are resolved immediately by front line staff, all OC will trigger an informal assessment.
An informal assessment will be made to obtain and assess sufficient information to determine the most appropriate course of action, including the possibility of a Safety Related Suspension [SRS] if a serious safety situation is indicated.
The OCHM described the SRS as follows:
Temporary suspension of a member’s privileges, through imposing an SRS, is a risk management strategy that will be considered if:
a. the potential risk (to self, other RAAus members, members of the public, the organisation or the effective conduct of the investigation) posed by the member continuing to fly, or maintain aircraft, is significant; and/or
b. the potential risk to others posed by the member cannot reasonably be managed in any other manner.
The AM [Accountable Manager], HAM [Head of Airworthiness and maintenance] or HFO may decide to impose an SRS on a member.
The OCHM provided the following examples of an SRS:
a. enhanced supervision requirements
b. temporary suspension of certificates
c. temporary revocation or restriction of privileges.
In accordance with CASR 149.425 and the RAAus Exposition, RAAus was required to submit a written report to CASA within 7 days of taking formal compliance or enforcement action. This was described in the RAAus formal inquiry process.
RAAus advised that mandatory notification to CASA was not required following an SRS because it was part of their informal assessment process and not their formal inquiry process. However, they could notify CASA of an SRS at their own discretion if they considered it prudent, although there was no continuing reporting requirement associated with this.
The outcome from an informal assessment could include a requirement for remedial action to be completed prior to lifting an SRS. If an individual’s membership lapsed with an active SRS, the requirements remained in place, flagged in their RAAus member profile, and were to be completed prior to exercising the privileges of their RPC if they decided to reactivate their RAAus membership.
Adventure Flight Training
Background
The AFT CFI became a member of RAAus in December 2008 and was issued with an RPC in December 2009, instructor rating in April 2017 and senior instructor rating in July 2018. On their senior instructor upgrade submission to RAAus, the examiner certified that the ground theory component was satisfactorily completed, although proof of completion of the ground theory was not required and not provided. Proof of a current medical certificate was required and provided.
As previously described, the theory component for the upgrade to senior instructor could be met by either passing the CASA PPL(A) exam or submitting the RAAus PPL(A)‑equivalent exam for marking by RAAus. In the case of the AFT CFI’s senior instructor upgrade, RAAus reported that the answer sheet for the PPL(A)-equivalent exam was not received with the upgrade submission and that it was likely their administration staff believed that the CASA PPL(A) exam had been completed instead. The CFI reported to the ATSB that for their senior instructor upgrade, the RAAus PPL(A)‑equivalent exam was done, submitted and approved.
The CFI was issued with a certificate of approval for their FTS on 11 June 2019. This followed an FTS inspection report in May 2019 at the nominated location of Riddell Airfield (Riddell), Victoria, and was initially to provide training for the issue of an RPC. The first 3 RPC candidates were required to be independently assessed by an RAAus‑nominated examiner.
In October 2021, RAAus issued the CFI with temporary approval for instructor training IT(T). This required the first 3 candidates for their instructor rating to be independently assessed by an RAAus-nominated examiner before the temporary approval could be lifted. In May 2022, RAAus conducted an onsite audit of AFT at Riddell.
RAAus records indicated that on 6 March 2023, the primary location for AFT became Moama. In August 2024, RAAus imposed an SRS on the CFI, which suspended their CFI approval and senior instructor qualification. Subsequently, the CFI elected to cease the FTS operations and later sold AFT.
Practices at Riddell Airfield
As part of the investigation, the ATSB interviewed the AFT CFI, 2 AFT instructors who were peers of the accident pilot, and several AFT RPC graduates from Riddell and Moama Airfields, all of whom knew the CFI and the accident pilot.
The interviews with those who had trained at Riddell indicated that AFT operations appeared to be consistent with the RAAus Exposition for an FTS, which was the situation when AFT was audited by RAAus in May 2022. One RPC graduate from Riddell reported that it was a more positive learning environment than they had previously experienced in general aviation.
The CFI would deliver the theory during the classroom lesson, then demonstrate the manoeuvre in-flight before handing over control and directing them how to fly the manoeuvre. Theory exams were paper-based using the exam papers provided by RAAus, which were supervised, marked and debriefed by the CFI.
However, what also emerged from the interviews was a difference in the FTS practices between Riddell in the period 2019–2023 and Moama in the period 2022–2024.
Onsite audits
In May 2019, RAAus conducted an initial FTS inspection at Riddell, and an FTS inspection report was completed by the RAAus delegate. No non‑compliances or rectifications were recorded on the report. At the time, there were no satellite flight training facilities and therefore the requirement for inspections of these facilities was recorded as not applicable on the report.
The next onsite audit of AFT was conducted at Riddell by RAAus in May 2022, at which time Moama was recorded as a satellite facility. That audit only occurred by virtue of AFT being at the same airfield as another FTS at Riddell being audited due to their PI being in the top 10. RAAus reported that, prior to that audit, AFT was ranked about 20 based on their PI score.
RAAus reported that during the 2022 audit they checked the records of student exam results but would not have checked the exam papers (answer sheets) themselves. One member of the audit team recalled a discussion with the CFI about the use of an online exam system as part of a broader discussion about how to improve the administration of the FTS. They did not believe an online exam system was in use, and they did not review or approve one.
The 2022 audit report included a reference to checking exam results but no reference to the use, or discussion, of an online exam system. RAAus reported that they had declined requests by FTSs to use online systems because it conflicted with the CFI declaration to not distribute the exams in either electronic or paper form.
On review of the draft report, the CFI maintained that RAAus did approve their online exam system and that they demonstrated it to 2 of the auditors during the 2022 audit. They further reported that during the audit they reported that exams were completed and stored electronically and demonstrated this in accordance with the respective audit checklist item. However, the auditor’s annotation on the 2022 audit report next to this item indicated ‘Cloud based (Google Drive)’ and did not include reference to the online exam software platform.
The audit resulted in 2 required corrective actions and 5 observations with associated recommendations. The AFT CFI responded to the corrective actions required and observations, which were accepted by RAAus. A copy of the audit closure report with the accepted supporting evidence was sent to the CFI in August 2022.
RAAus reported that, depending on findings, an FTS did not automatically move to the bottom of the PI score list after an audit. In this instance, because of the structure of AFT and the non-compliances identified during the audit, their rank moved from about 20 to approximately 100 (of about 160 FTSs at the time).
Chief flying instructor conduct
In May 2020, RAAus investigated a close proximity event involving the AFT CFI, which their risk matrix indicated was a potentially catastrophic event. The CFI denied involvement in the event and reportedly provided RAAus with a copy of their flight path history for the day of the incident. However, the RAAus investigation confirmed it was the CFI’s aircraft and that they were aboard at the time. RAAus subsequently issued a formal letter of reprimand to the CFI for not reporting the event and denying their involvement.
In August 2020, the initial cadre of AFT RPC candidates were ready for assessment, and an independent examiner was nominated by RAAus. The examiner assessed the first candidate and reported to RAAus that the flight component of the test went smoothly but the candidate’s theory knowledge was ‘not as good as it could have been’. The examiner recommended the candidate do further theory practice exercises.
RAAus correspondence indicated that following the independent assessment of the first AFT RPC candidate, the CFI conducted the flight tests for the 2 other RPC candidates, instead of having them assessed by the nominated examiner as required. When RAAus challenged the CFI about this matter, they alleged that the examiner had lost control of the aircraft during the flight test with their candidate. This allegation was later challenged by the examiner and the CFI provided RAAus and the examiner with a retraction.
On review of the draft report, the CFI denied that they had made this allegation and reported that the student had told them the examiner was flying out of balance. Therefore, the CFI decided to request another examiner with experience on that aircraft type conduct the checks.
In December 2020, RAAus lifted the RPC testing restriction on the CFI with an administrative assessment in place. This allowed them to conduct the flight tests for the recommendation of an RPC but required them to provide RAAus with each candidate’s completed training records when the RPC recommendation paperwork was submitted.
In November 2021, about a month after RAAus issued the CFI with their instructor training temporary approval (IT(T)), the CFI advised RAAus they were starting a full-time IT course at Moama Airfield. Like the first 3 RPC candidates, the first 3 candidates for the instructor rating were required to be independently assessed.
In April 2023, the CFI reported to RAAus that their first 3 instructor candidates had been independently assessed and requested removal of their temporary IT status. However, the examiner on this occasion (different from the previous RPC examiner discussed above) reported that the candidates were not prepared for their instructor briefing session despite the preparation advice the examiner had provided to the CFI for their candidates.
The examiner also reported that there were additional administration preparation deficiencies, which led them to conclude that the CFI had not taken the time to check the process requirements. Consequently, in May 2023, RAAus notified the CFI that they would need to remain under a temporary IT approval status until a further 2 candidates could be assessed by the same examiner. The RAAus records indicate that the temporary IT approval was never lifted.
Practices at Moama Airfield
Pre-flight video briefs
The accident pilot started flight training with AFT at Moama in April 2022 with operations temporarily moving to Echuca, Victoria, during the flooding of Moama in late 2022. Staff and students interviewed by the ATSB who attended Moama from late 2022 through to the closure in August 2024 reported that no pre-flight briefings or post-flight debriefings were delivered for RPC candidates. Instead, the CFI had produced a short in-flight video for each of the RPC flight training elements, which demonstrated how the manoeuvres were to be flown, and candidates reported they had to pay a subscription fee to access AFT flight training videos for pre-flight briefing material.
On review of the draft report, the CFI reported that the videos were gradually introduced from 12 July 2023 to 22 July 2024. Therefore, the videos were not used for the delivery of training to the accident pilot, which they reported was delivered in-person.
The CFI reported that the videos were only introductory material and not the pre-flight briefing material. However, the CFI’s position was contradicted by the Moama AFT instructor staff and students interviewed by the ATSB. Additionally, the ATSB noted that the syllabus used by AFT staff included the following items:
Confirm student has watched the relevant video briefing and understood the concepts
Remind students to login to AFT members page and watch next video
According to RAAus, their Exposition did not prohibit an FTS from implementing pre-flight video briefings in lieu of in-person pre-flight briefs. However, RAAus advised being unaware of the videos prior to suspending the CFI in August 2024. RAAus learnt about the videos from interviews with AFT members about the practices at the FTS. However, they were then told by the CFI that access to the videos was no longer available and therefore, RAAus reported they were unable to assess whether the content of the videos was adequate.
The ATSB interviewed an RAAus CFI, who was also a CASA flight instructor, and who had reviewed one of the videos. They reported that they didn’t think the video met the quality required for a pre-flight brief. Another RAAus CFI, who had reviewed several of the videos for the AFT CFI, reported to the ATSB that they had been led to believe that they were the pre-flight briefing material and that they were inadequate due to deficiencies in the quality of instruction presented.
They noted that, while the AFT CFI was projecting a friendly demeanour in the videos, it was often at the expense of technical errors and an adequate demonstration. For example, the reviewer noted the stalling video did not include any reference to the effect of load factor on stall speed and reference to checks and limits were often omitted in the various videos.
The ATSB obtained copies of 12 of the AFT videos from elements of the RPC syllabus, one produced in 2020 and the remainder in 2023. This evidence was consistent with a report the ATSB received from a Moama AFT instructor that they were already receiving video briefs when they started flying training in late 2022. They ranged in length from 2 minutes and 15 seconds to 7 minutes and 30 seconds. Of specific interest to the ATSB investigation was the aerodynamic stalling video, which was of 6 minutes duration.
In that video, the CFI demonstrated the reduced effectiveness of flight controls near the stall by applying full left then full right rudder and instructed the use of rudder to level the aircraft if a wing drop occurred. The risk of inducing a spin from large rudder applications near the stall was not mentioned. By contrast, the CASA flight instructor manual for aeroplanes explained these points in its chapters on stalling and spinning as follows:
Emphasize that if a wing drops, rudder is used to prevent yaw into the direction of the lowered wing. The wing is raised with aileron when it is un-stalled.
An aeroplane is made to spin, whether accidentally or deliberately, by faulty use of the controls particularly the rudder.
During the stalling video, the CFI explained that lowering the flap for the configured stall demonstration would ‘thicken’ the wing, and that the thicker the wing, the slower they could fly. The manufacturer’s website for the demonstration aircraft stated that it had a slotted flap. A slotted flap is a design feature used to control the boundary airflow layer and increase the camber of the wing. Lowering the flap increases the maximum coefficient of lift (and drag) for the wing, thereby allowing the aircraft to fly and stall at a lower airspeed and is part of the basic lift formula.
At the start of the video, and in accordance with the RAAus syllabus of flight element of stalling, the CFI demonstrated the pre-manoeuvre checks. However, there was no reference to flap limiting speeds for the configured stall and no demonstration of post loss of control checks after recovery from any of the stalls. The RAAus syllabus of flight included ‘airframe limitations’ as a competency requirement within the element of stalling.
Demonstration of stall at greater than 1G
For the RAAus RPC syllabus, stall exercises were limited to straight and level, clean and configured stalls, with and without wing drops, which were covered in the AFT video. However, the RPC theory syllabus did require a thorough understanding of the relationship between load factor and stall speed and the instructor syllabus included demonstration of stall entry at greater than 1G (critical angle of attack exceeded at a higher airspeed). In the AFT stalling video, the CFI directed the viewer’s attention to the lower stall speed when the flap was lowered for a configured stall, but a higher stall speed, and what contributes to a higher stall speed, was not demonstrated or discussed.
The CFI reported that the demonstration of stall entry greater than 1G was conducted in training, but the 2 AFT instructors interviewed by the ATSB reported they did not conduct this manoeuvre during their training. One of the instructors reported that they were unaware of the effect of load factor on stall speed at the time of the accident and that both themself and the accident pilot were trained in stalling by the AFT CFI for their instructor course. Therefore, they believed the accident pilot would not have covered this topic either. Their main concern with the load factor applied by the accident pilot during steep turn manoeuvres was the potential for a structural failure.
While the CFI reported that the ‘greater than 1G stall manoeuvre’ was taught as a turning stall during training, they were unable to recall the parameters used for the demonstration. The AFT records for their instructor training courses included comments about clean stalls, configured stalls and wing drops. However, there were no references to a stall at greater than 1G.
The AFT RPC student records indicated that the element ‘critical angle of attack exceeded at a higher airspeed’, was assigned a competency code on 46 out of 55 occasions. This was despite it not being in the RPC syllabus and the AFT instructors interviewed by the ATSB reporting that they had never done it in training themselves or with a student. One instructor explained that the competencies for each flight were accessed during the flight with a portable electronic device, such as a smartphone, and that on a small screen, instructors might have only registered the start of the competency, which stated ‘critical angle of attack exceeded…’, without either registering or understanding the meaning of the rest of the competency, which stated ‘…at a higher airspeed’.
Online exams
The AFT instructor interviewed by the ATSB, who started flying training with AFT at Riddell Airfield, reported that they followed the RAAus paper-based exam system, as previously described, and that they had no experience with an online exam system. However, the other instructor interviewed by the ATSB, who started at Moama Airfield (Echuca during the floods), conducted their exams at home, unsupervised using their own login to the AFT online exam system. This was the same process described by the AFT RPC graduates from Moama interviewed by the ATSB.
The CFI reported that the online exam system was set up in response to the COVID lockdown period and was approved by RAAus. The setup of the system entailed the CFI providing a copy of each exam paper and marking rubric to the software platform provider for loading onto their platform. The exception was the RAAus PPL(A)-equivalent exam, which was marked by RAAus and therefore no marking rubric was provided. The CFI reported that the software provider loaded answer A as the default correct response to all questions for the PPL(A)-equivalent exam and notified them of this action.
The AFT cohort who used the online exam system paid a subscription to access the exams and were notified by the CFI or their instructor when they were due to complete an exam. The CFI was the administrator for the online system and reported that the security protocols prevented anyone else from downloading or printing a copy of an exam paper. As the administrator, the CFI included settings which allowed 2 attempts at each exam and revealed the correct answers to all questions in the exam report, provided after the first attempt.
One of the Moama RPC graduates reported there was no study direction before an online exam and that the staff expected they would pass each exam on a second attempt if required. This graduate reported there were no classroom lessons, in addition to no in‑person pre-flight briefs, and the lack of theory education caused them progression problems and learning difficulties with some of the technical aspects.
Another Moama RPC graduate, who had prior non-aviation teaching experience, believed the online exams were open-book as they were unsupervised. Consequently, they used their flight training reference books during exams, supported by online searches for any questions they could not find the answer to in their books.
They did not pass their first attempt at the basic aeronautical knowledge exam but received all the correct answers in their exam report, which they photographed and used for their second attempt. They did not receive any classroom lessons or pre-flight briefings at AFT and reported that they felt the learning experience was substandard.
The RPC graduate had 2 attempts at the basic aeronautical knowledge exam on the same day recorded in the AFT exam records, with a score of 100% for both attempts. One of the AFT instructors reported to the ATSB that the exam scores were manually entered and might not have represented the actual results. Of the 146 entries in the AFT exam records, from April 2021 to July 2024, there were no failures.
Deficient instructor supervision
As previously described, on 19 December 2023, the AFT CFI conducted the senior instructor flight test for the accident pilot and incorrectly submitted the upgrade application to RAAus with a copy of the pilot’s May 2023 instructor exam, which had been conducted online. On 3 January 2024, the CFI certified in the pilot’s logbook that they met the requirements for the senior instructor rating in accordance with the RAAus syllabus of flight. The pilot subsequently took the RAAus PPL(A)-equivalent exam online on 12 January 2024.
The pilot scored 94% (47/50), noting answer A was the default correct answer for all questions, and which the CFI reported that they were aware of. The CFI then submitted a copy of this exam to RAAus, noting that they reported that they were the only one who could download the exams from their online platform.
In late January, RAAus notified the CFI of the pilot’s failure assessment for the PPL(A)‑equivalent exam, that the pilot’s upgrade to senior instructor would not be processed and that the pilot would continue to require direct supervision as an instructor. However, in January 2024, the CFI left the FTS for extended travel around Australia throughout the calendar year 2024.
Prior to leaving, the CFI enquired with another RAAus CFI if that person could hold a temporary CFI position for them while they were away. However, they were told by that person that they could not attend the FTS in Moama and were therefore unable to comply with the direct supervision requirements for the AFT instructors. There was no reference in the AFT CFI’s RAAus member record of their absence from their FTS and RAAus reported they had no knowledge that the CFI had departed from the area and left their instructors without direct supervision.
The accident pilot’s last logbook entry was an AFT instructional flight on 7 August 2024 and their last check flight with the CFI was their senior instructor flight test on 19 December 2023. There were no entries in 2024 for a standards and proficiency check from the CFI, which was required every 90 days.
The AFT training records indicated that the CFI was at the FTS until at least 11 January 2024 and returned to deliver training for several days in February, May and June of 2024. One of the AFT instructors reported they didn’t get a check flight from the CFI during one of the visits, which concerned them as they considered themself and the other instructors at AFT to be relatively ‘green’.
The other AFT instructor reported that the flights they conducted with the CFI during this period were ferry flights between Melbourne and Moama when the CFI visited the FTS to deliver training. The 3 AFT instructors all qualified in 2023; one in early 2023, the accident pilot in mid-2023 and the third in late 2023.
Examination conduct
As previously described, the accident pilot unsuccessfully re-attempted the PPL(A)‑equivalent exam on 24 February 2024. At the end of February, RAAus emailed the CFI the result from the pilot’s second attempt at the exam and their concern about the type of errors made. They also advised the CFI that it was critical for the CFI to also complete the PPL(A) exam as they had delivered the instructor training for the accident pilot and RAAus could not confirm that the CFI had previously completed the PPL(A) exam.
In response, the CFI reported to RAAus that it was their intent to complete a PPL(A) course and the CASA PPL(A) exam. RAAus noted this but also committed to revising their PPL(A)‑equivalent exam by the end of March as an alternative pathway. In late March, RAAus requested an update from the CFI on their progress towards attempting the PPL(A) exam. The CFI reported that both they and the accident pilot were enrolled in a course but could not provide an estimated completion date.
On 2 July the CFI submitted a completed exam paper to RAAus for the same version of the PPL(A)-equivalent exam that the accident pilot had failed in February (2022 version). However, RAAus noted that their policy for exam conduct, published at the front of the exam paper, was not followed. Specifically, a supervisor for the exam was required to be appointed by RAAus, the exam answer sheet should have been used instead of the exam paper, and the supervisor should have submitted the exam to RAAus for marking, rather than the candidate (the CFI themself).
RAAus communicated the problems they identified to the CFI, and they subsequently received a copy of the exam answer sheet, with a supervisor’s signature dated 4 July. The answer sheet provided was marked by RAAus and scored as a pass (88%). RAAus prepared a knowledge deficiency report with the pass result for the CFI and annotated the exam location as ‘Supervised via zoom (possibly at Moama)’.
On 8 July, RAAus followed up with the certifying supervisor on several points, which included:
Their instructor approval had lapsed in January and therefore their supervisory privileges had also lapsed.
How were they given approval to supervise the exam as the policy document states that the RAAus HFO makes these arrangements?
Exams require direct supervision, which is in-person, whereas the use of Zoom indicated indirect supervision.
The supervisor’s certification date of 4 July was 2 days after the exam paper was submitted to RAAus.
There was no record of answers to these queries, but RAAus subsequently concluded that the CFI’s exam result was invalid. At the end of July, they communicated to the CFI that either the CASA PPL(A) or a new RAAus PPL(A)-equivalent exam needed to be taken prior to 16 August 2024.
The CFI notified RAAus on 7 August that they would attempt the PPL(A)-equivalent exam if it could be facilitated for them in Far North Queensland. This was arranged for 8 August with a copy of a new RAAus PPL(A)-equivalent exam (2024 version). The 2024 exam paper comprised 60 questions, of which 50 were the same, or similar, to the 2022 version. The CFI scored 77% (46/60), which was below the required pass mark of 80%.
The CFI reported to the ATSB that other CFIs had told them that they too could not pass the 2024 version exam paper, and the CFI did not believe the exam had been validated and therefore should not have been used. They provided a specific example of a navigation question they believed was marked as incorrect because they used a protractor rather than the ‘1-in-60’ rule to calculate their answer to a heading correction question. However, the ATSB identified that it was possible to derive the correct answer using either method.
The ATSB also noted that the CFI provided the same incorrect answer as the accident pilot to a question about the relationship between angle of bank, load factor and stall speed. They had both selected the answer with the correct stall speed but the incorrect load factor. The RAAus syllabus of flight training contained the references for the navigation and stall speed questions.
The marking of the CFI’s answer sheet revealed there were 13 incorrect answers in the first 50 questions (7 in common with the accident pilot) and 1 incorrect answer in the 10 additional questions. Consequently, if only the 50 questions from the 2022 version exam were marked, the score would have been 74% (37/50) and remained below the pass mark.
Safety related suspensions
On 9 August, RAAus notified the CFI of the failed exam result and that the exam had been crosschecked by 2 independent staff. They then issued an immediate SRS, suspending the CFI’s senior instructor rating, which was required for a CFI approval. To remove the SRS, the CFI was required to supply RAAus with evidence of a pass result for the CASA PPL(A) exam. RAAus reported to the ATSB that they were prepared to arrange for a temporary CFI for AFT in the interim, but the CFI decided to cease FTS operations and later sold AFT.
On 13 August, RAAus notified CASA of their implementation of the SRS for the AFT CFI and that the matter was currently under review. The notification to CASA included:
- RAAus identification of incorrect marking of a PPL(A)-equivalent exam for a senior instructor candidate, which raised questions about the CFI’s theoretical knowledge
- advice of the CFI’s failed attempt at the PPL(A)-equivalent exam, with a conclusion that they therefore did not meet the theoretical knowledge requirement for the senior instructor rating and would need to provide evidence of a pass for the CASA PPL(A) exam.
On 11 November, RAAus notified the AFT CFI that they had completed an informal assessment as per the OCHM and did not believe a formal inquiry was necessary. They reiterated that the remedial action required was the completion of the CASA PPL(A) exam. However, by that time the CFI’s membership had lapsed. RAAus reported to the ATSB that the remedial action requirement would remain flagged in the system in the event that the CFI elected to re-activate their membership and have their senior instructor rating reinstated.
Following the accident, on 19 December 2024, RAAus issued an SRS notice to all RPC graduates from AFT who did not hold a CASA PPL(A) licence or higher. This was due to non-compliances with the conduct and supervision of exams, which meant they could not verify that former students met the theoretical knowledge requirements for the issue of an RPC.
Civil Aviation Safety Authority
Surveillance events
The CASA Sport and Recreation Branch (CASA Sport) conducted a Level 1 surveillance event of RAAus at their premises between 12–14 April 2023, and a Level 2 surveillance event at their premises between 3–5 September 2024. Prior to 2023, the previous audit was a Level 1 surveillance event on 4 May 2019. The ATSB obtained a copy of the previous 2 audit reports (2023 and 2024) of RAAus by CASA.
The May 2019 audit resulted in 1 finding and 6 observations. The April 2023 audit resulted in 4 findings and 7 observations. The 4 findings related to the elements of airworthiness and listing of aircraft and were not relevant to the ATSB’s investigation. However, one observation of relevance from the 2023 audit was for the element of Evaluation of Authorisation Holders, as follows:
The processes for the regular evaluation of holders of certain authorisations to ensure compliance with the requirements set out in the ASAO’s policies and procedures require additional development.
As this was an observation, no response was required from, or provided by, RAAus. The September 2024 audit of RAAus followed their notification to CASA Sport of the SRS issued against the AFT CFI and the introduction to the audit report stated:
The auditors sampled the systems and elements relating to RAAus' oversight of flight training schools with the respective key personnel and the RAAus Accountable Manager. Emphasis was placed on reviewing:
• the integrity of their training/testing system which leads to the granting of pilot authorisations,
• governance and process including consistency,
• oversight of training and examining,
• safety assurance including the reliability of information provided by examiners.
CASA Sport raised 2 observations from the audit for competency-based training, and interpretation of manuals, which were both against the element of Flight Operations (Pilot Authorisations). No responses were required or provided to the observations. The observation about competency-based training had a similar theme to the 2023 audit observation about compliance issues and stated:
Current updates to the Flight Operations Manual (Version 8) places significant reliance on CFIs and Examiners applying competency-based training and testing outcomes. However, one of the highest individual non-compliances identified from the RAAus Risk and Audit Matrix Occurrence Tracker records has been deficiencies in the FTS applying and recording competency-based training outcomes (assessing and recording competence and rectifying deficiencies).
The non-compliances found by RAAus auditors during the audits of FTSs - with more than 30% of the RAAus FTS surveillance events (conducted between Dec 2021 and August 2024) showing a non-compliance in relation to assessing and recording competencies - may suggest a level of guidance regarding competency-based training for FTS may be required.
Pilot examination office
The CASA pilot online examination system is called the pilot examination office (PEXO). The key personnel in the daily operations of an examination centre are the registrar and invigilator. A registrar is responsible for making the booking of exams for candidates and an invigilator is responsible for the direct supervision of the candidates for their exams. An individual may hold both the registrar and invigilator positions.
Registrars, invigilators and examination centres must be authorised by CASA and the approval for FTSs to conduct exams is limited to PPL and the private instrument flight rating (PIFR). Therefore, a candidate for a commercial pilot licence, which is a requirement to instruct for the issue of a pilot licence, would need to pass their higher‑level theory exams at an examination centre independent of their FTS.[11]
The registrar, invigilator and candidate each have their own unique password, which limits their access within the system to their specific functions. CASA records access and usage of the PEXO system and provides an e-learning module for the system users (registrars, invigilators and candidates). They also undertake surveillance of examination centres, which may, or may not, be conducted with advance notice.
The exams are accessed by connection to the CASA server during an examination. When an exam is started, the questions and associated answers will be generated from a database of questions, and a timer will count down. The program will automatically close the exam when the time has expired or if the candidate selects ‘End’ exam and ‘logout’. After the candidate selects ‘End’ exam, it will be automatically submitted for marking and the result recorded against the candidate. The invigilator login is needed to recover the result and the associated knowledge deficiency report for the candidate.
Granting of a Recreational Pilot Licence
Under CASR Part 61.480, CASA can grant an RPL to an individual on the basis of them holding a pilot certificate, granted from certain organisations, which included RAAus. In this scenario, the applicant is taken to have passed the aeronautical knowledge examination and flight test for the licence and associated aircraft category rating issued.
The applicant is also taken to have met the requirements for the aircraft class rating and design feature endorsements for which the applicant is permitted by their pilot certificate to act as the pilot in command. However, they must successfully complete a flight review for their class rating in order to exercise the privileges of their rating. In the case of the accident pilot, this was a single-engine aeroplane class rating.
Mandatory reporting and enforcement process
Background
Under CASR Part 149.425, RAAus have mandatory reporting requirements to CASA Sport in accordance with their Exposition and the circumstances prescribed by 149.425. If RAAus reported to CASA Sport that they had revoked or suspended a member’s qualification(s), then the matter could be referred by CASA Sport to the CASA Coordinated Enforcement Process (CEP), which is described in the CASA Enforcement Manual.
Under the CEP, the matter is referred to the Coordinated Enforcement Meeting (CEM) where it is allocated to an investigator to investigate and provide a report to the CEM for discussion on whether to proceed with action. The participants in the CEM have a range of options, which include, but are not limited to, the following:
- no action
- education
- counselling
- direct the person to undertake examinations
- suspend authorisations pending completion of a practical or theoretical examination
- varying, suspending or revoking a licence, endorsement or rating.
Response to RAAus safety related suspension notices
On 19 December 2024, RAAus issued an SRS notice to all RPC graduates from AFT who did not hold a CASA PPL(A) licence or higher. The notice explanation included the following:
RAAus has identified non-compliance with respect to the conduct and supervision of exams conducted by students at Adventure Flight Training. Based on the evidence available, RAAus is unable to verify that all former students of Adventure Flight Training met the required theoretical knowledge standards required for the issue of a Recreational Pilot Certificate with RAAus.
Due to the potential for this finding to result in a risk to aviation safety, RAAus has implemented a safety related suspension (SRS) on your Recreational Pilot Certificate (RPC), effective immediately, pending the conduct of an assessment to confirm that your theoretical knowledge meets the expected standard required to maintain an RPC.
On 20 December, RAAus notified CASA Sport of the implementation of the SRS following their ongoing investigation into how AFT was being managed. Their notification to CASA did not include the names of the affected members, but did include the following explanation:
It has been identified that some students undertook RAAus exams using an online system from their home address without the supervision of an instructor. Further, it has been identified that the system used to sit exams online allowed the student to update incorrect answers and resubmit the exam to achieve a successful pass mark.
The process for the affected members to remove their SRS included passing the RAAus converting pilot exam (a requirement for a pilot licence holder applying for an RAAus RPC) under the supervision of an FTS CFI or senior instructor. The exam supervisor also had the discretion to require additional theoretical assessments and one of the AFT instructors subject to the SRS reported to the ATSB that in addition to the converting pilot exam, they were also required to complete the RAAus instructor exam. The instructor also reported to the ATSB that they held a CASA-issued RPL (issued in recognition of their RPC) but CASA had not contacted them about continued exercising of the privileges of their CASA-issued licence.
CASA reported that they recorded all information provided by RAAus in their records management system but no follow‑up was conducted with RAAus to identify the specific members affected. RAAus reported that they elected to voluntarily provide the initial SRS (August 2024) about the AFT CFI to CASA as it involved a higher approval holder. When the AFT graduates’ SRS was implemented in December, RAAus considered that it would be prudent to notify CASA due to the number of pilot certificate holders involved.
The ATSB obtained a list of the affected members from RAAus, about 7 months after the SRSs were issued, and requested CASA review it against their RPL records. It was identified that 3 affected members held a CASA-issued RPL, granted based on their RAAus RPC, which included 2 at the time the SRS was issued.
Two of those 3 members addressed the SRS within a month of its issue. The third had not addressed it and their RAAus membership had lapsed, which meant that they continued to hold a CASA RPL without restrictions, while their RPC was suspended and would not be lifted unless they re-activated their membership.
Safety analysis
Introduction
On 16 November 2024, an amateur-built experimental certificate Morgan Cougar Mk 1 aircraft, registered VH-LDV, with a pilot and 2 passengers on board, departed from West Sale Airport, Victoria, for a local area flight. The aircraft collided with terrain in a paddock 19 km north-north-west of West Sale Airport about 17 minutes after departure and shortly after commencing a series of orbits. The aircraft was destroyed and the 3 occupants fatally injured.
This analysis will discuss the factors that contributed to the accident sequence, including the loss of control and the pilot’s knowledge deficiencies and history of risky flying behaviour. It will also discuss the management of the Adventure Flight Training (AFT) school and the Recreational Aviation Australia (RAAus) examination system.
In addition, the analysis will examine the aircraft’s occupant restraints, aircraft design and guidance material from the Civil Aviation Safety Authority (CASA) advisory circular for amateur-built experimental certificate aircraft and transition training guidance for buyers of these aircraft. Finally, it will discuss the CASA Sport and Recreation Aviation Branch management of suspension notices received from RAAus.
Accident sequence
Loss of control
Analysis of the final 3 minutes of the flightpath revealed the aircraft’s speed and height were decreasing as it flew a series of turns and orbits. When the aircraft commenced the final turn, the groundspeed and height above the ground had reduced from 103 kt and 716 ft, to 64 kt and 269 ft. Using the recorded local mean and gust wind, the estimated calibrated airspeed was in the region of 67–74 kt at the start of the final turn. The groundspeed reduced to 56 kt during the final turn as the turn radius tightened and analysis of this turn indicated a steep turn with an average 45° angle of bank required for the observed flight path.
A closed-circuit television camera at a nearby farm recorded the aircraft enter the final turn with an angle of bank consistent with a steep turn manoeuvre. The aircraft then pitched nose down at an estimated airspeed of 59–65 kt and height of about 220 ft. Witnesses reported that the aircraft appeared to fall from the sky, and the recorded data indicated an abrupt reduction in altitude and increase in speed. The witness accounts, recorded data, and camera footage were consistent with a loss of control due to an aerodynamic stall.
Wreckage examination found the aircraft attitude was recovering towards straight and level just prior to impact and that the engine was operating at impact. This indicated that it was very unlikely that a mechanical fault contributed to the accident. The amount of engine power at impact could not be determined and the ATSB could not rule out the possibility that the pilot retarded the power lever towards idle in response to the loss of control, which would be the expected response to a nose-low unusual attitude.
The final turn started 7 seconds prior to the stall, at which time the aircraft was estimated to be 29–36 kt above the flight test recorded stall speed of 38 kt in straight and level flight. For a stall to occur in 7 seconds after starting the turn, it required a closure rate of 4–5 kt per second to the stall speed, which was consistent with an accelerated stall at a load factor of 2.5–3G.
The ATSB could not determine the stall warning system settings, or if an audible stall warning would have been activated prior to the stall event. However, the stall occurred in a steep turn at a height that was insufficient for recovery.
Contributing factor The aircraft entered an accelerated stall in a steep turn with insufficient height to recover, resulting in a collision with terrain. |
Knowledge deficiencies
Shortly after the accident, the ATSB was contacted by an AFT instructor who was a colleague of the accident pilot. They advised being unaware of the effect of angle of bank and load factor on stall speed. The accident pilot was trained at the same flight training school (FTS) as the reporting pilot for their recreational pilot certificate (RPC) and instructor rating, prompting an examination of the accident pilot’s knowledge of aerodynamics.
On review of the accident pilot’s last RAAus exam, the ATSB found that they failed the exam on 2 consecutive attempts. On the pilot’s second attempt, the incorrect answers included 2 questions about stalling, one of which included the relationship between angle of bank, load factor and stall speed. While the pilot’s answer had the correct stall speed for the nominated angle of bank, they had the incorrect load factor. However, it is the load factor generated by manoeuvring flight that affects the stall speed and not the angle of bank. Therefore, the pilot was missing the critical link in the relationship – how the load factor is derived from the angle of bank in a level turn, and how the stall speed is derived from that load factor.
The pilot’s incorrect answers resulted in RAAus expressing their concern about the pilot’s knowledge of aerodynamic stalling when they notified the AFT chief flying instructor (CFI) of the result. The question about load factor and stall speed in a turn was listed in the RAAus syllabus of flight as an item that required a thorough understanding at the RPC level and the exam had been submitted for the pilot’s upgrade from instructor to senior instructor. As the pilot had failed this exam twice, a new exam was required to be completed, and the pilot started a CASA commercial pilot licence theory course.
From early June to early July 2024, the pilot conducted flight training in a Pitts Special aerobatic aircraft. Several parties reported to the ATSB that this was for the purpose of an aerobatics endorsement. The syllabus for an aerobatics endorsement included the effect of load factor on stall speed. However, the flight training records indicated it was transition training and not training for an aerobatics endorsement. While an aerobatics endorsement included a list of underpinning knowledge requirements, which included the relationship between load factor and stall speed, it was not required to be taught for transition training.
In late July, the pilot failed their first attempt at the CASA commercial pilot licence aerodynamics exam, which included an incorrect answer to the effect of manoeuvring on stall speed. This indicated the pilot’s previous misunderstanding of this topic had not been corrected. However, only the knowledge deficiency reports were retrievable by CASA and not the exam questions and answers, which limited the analysis of these exams. A comparison of the 2 subjects the pilot completed revealed they achieved a high pass result for aircraft general knowledge, but a fail result followed by a low pass result for aerodynamics. This indicated that the pilot found learning the aerodynamic aspects of flight challenging, which was consistent with the concerns previously expressed by RAAus.
The RAAus syllabus for an instructor included demonstrating a stall entry at greater than 1G (critical angle of attack is exceeded at a higher airspeed), which could have addressed the misunderstandings that the pilot held from their RPC theory. While the AFT CFI reported that this training was conducted, the 2 AFT instructors interviewed by the ATSB reported that it was not done and the ATSB found no comments in any of the AFT instructor training records to indicate that it was completed. Therefore, the ATSB concluded that it likely was not done and that the pilot’s knowledge of the relationship between load factor and stall speed was likely deficient at the time of the accident, which contributed to them manoeuvring the aircraft close to the stall speed.
Contributing factor It was likely that the pilot had an inadequate understanding of the relationship between angle of bank, load factor and stall speed, which contributed to the pilot not fully understanding the risk of conducting slow steep turns. |
Pilot flying history and aircraft characteristics
The ATSB interviewed several pilots from AFT who were either colleagues of the accident pilot (fellow instructors) or were RPC graduates from the FTS. They all had experience flying with the accident pilot and 2 of them were syndicate members with the pilot in the purchase of the accident aircraft. One of the syndicate members reported they did not experience any risky flying practices with the pilot but was aware that the pilot had received counselling for such flying.
The ATSB identified that several people, including pilots, fellow instructors and CFIs had been counselling the pilot leading up to the accident, including 3 counselling sessions in the 2 months prior to the accident.
In between the counselling sessions in the last 2 months, there were 3 reported instances of risky flying activities by the pilot. It was therefore likely that no individual involved in counselling the pilot had full knowledge of their behaviour and the counselling sessions did not achieve their intended purpose.
While the safety concerns were discussed with the pilot, no reports were submitted to RAAus and therefore no official action was ever taken. It is possible that there was a reluctance to submit official reports after providing counselling, as this action could make the reporter identifiable and result in a loss of trust between the reporter and their community.
Other factor that increased risk The pilot was counselled about unsafe flying practices but was not reported to any authority and therefore no official follow-up action was ever initiated. |
Two fellow AFT instructors each had experiences with the pilot conducting low level steep turns at high and low speeds and had both advocated to the pilot to manoeuvre their aircraft less aggressively. One of the RPC graduates also experienced the pilot manoeuvring the aircraft aggressively during their pre-RPC check flight in 2023 and conducting a slow speed steep turn overhead a tractor during a private flight in November 2024, 15 days prior to the accident. These reports related to RAAus Topaz and Jabiru aircraft, which both had higher published stall speeds than the Morgan Cougar aircraft. This likely led to an expectation by the pilot that similar manoeuvres could be safely conducted in the Morgan Cougar.
The Morgan Cougar was an amateur-built experimental certificate aircraft, which was subject to a 40-hour flight testing period that included stall testing. However, the stall testing was predominantly limited to 1G clean and configured stalls. The builder was able to recollect one instance of a left turn stall at 30° angle of bank. In this case, the aircraft stalled in a sudden and unexpected manner compared with the 1G stall response, and the builder hypothesised that a stall at a greater angle of bank could exaggerate this effect.
The description provided by the builder was consistent with the warning from the United States (US) Federal Aviation Administration (FAA) that there are no rules for the stall behaviour of an experimental aircraft, and that they can depart controlled flight dramatically without any perceptible warning.
The designer of the Morgan Cougar recommended the builder not attempt accelerated stall testing alone, and this was not done, so the responsiveness of the aircraft to this scenario was unknown. However, the accident pilot invited an AFT RPC graduate for a familiarisation flight in the Morgan Cougar 3 days prior to the accident flight, which the passenger described to the ATSB as for the purpose of demonstrating the responsiveness of the aircraft. During the flight, the pilot demonstrated manoeuvring the aircraft at 70–75° angle of bank, which the passenger described as ‘knife-edge stuff’ and would have required a load factor in the region of 3–4G.
According to the FAA, aircraft with light control forces and/or rapid response are susceptible to overcontrolling by pilots who have not received any type-specific training. Furthermore, low wing aircraft tend to roll into the turn during a turning stall. A stall in a turn will increase the height loss during recovery, as the recovery requires a rolling motion followed by a pitching motion, and therefore, the further the aircraft has to be rolled to restore wings level flight, the greater the height loss.
The syndicate members signed the sale agreement on 5 November, 11 days prior to the accident. However, the builder was unable to accompany them on any familiarisation flights and did not discuss the turning stall behaviour of the aircraft with them. Furthermore, it was concluded from interviews and review of ADS-B data that none of the members had completed any transition training on the aircraft. Therefore, it was very unlikely that the pilot was aware of the specific response of the aircraft in a turning and/or accelerated stall scenario, which was very likely different to the 1G stall and different to the approach to stall and post-stall response of aircraft the pilot had delivered RPC training in at AFT.
Contributing factor The pilot had a reported history of conducting low flying and slow steep turns and was likely unaware that, while the accelerated stall characteristics of the accident aircraft were unknown, there were indications that it would be abrupt. |
Adventure Flight Training school management
Demonstration of stall at greater than 1G
The RAAus instructor syllabus module for aerodynamic stalling included a stall entry at greater than 1G sequence. This was for the instructor candidate to demonstrate exceeding the aircraft’s critical angle of attack at a higher speed than the 1G stall speed. While this was not part of the RPC syllabus, the instructor syllabus required the demonstration to be performed by the instructor to a high degree of accuracy. However, the AFT instructors interviewed by the ATSB reported that this manoeuvre was not taught on their instructor course and their training records did not include any instructor comments to indicate that it had been completed.
The AFT CFI reported that the stall entry at greater than 1G was taught as a turning stall manoeuvre but could not recall any of the performance parameters for it. Furthermore, the AFT records indicated that a competency code was routinely assigned to their RPC candidates for this manoeuvre as part of their stalling training. Once again, there were no comments within the instructor remarks to indicate that it was taught to those members who had a competency code assigned.
Based on this evidence, the ATSB concluded that this competency was likely not taught at AFT and that the competency code was probably misunderstood.
Instructor supervision
Within the RAAus FTS system, instructors required direct supervision from either their CFI or an approved senior instructor. The purpose of this was to provide continuing mentoring and development of the FTS instructors. The level of supervision could be reduced to indirect (remote) for a senior instructor. However, except for the CFI, none of the AFT instructional staff had progressed to senior instructor. The accident pilot attempted to upgrade to senior instructor in early 2024 but failed the required theory exam component.
When RAAus communicated the pilot’s exam result to the AFT CFI on 29 February 2024, they included their concern about the pilot’s knowledge of aerodynamic stalling and the requirement that the pilot remain under direct supervision. However, the AFT instructors reported to the ATSB that their CFI left the FTS for a trip around Australia in early 2024, with occasional return visits. This was supported by another CFI who had been asked, but declined, to supervise the FTS by the AFT CFI in their absence.
RAAus reported to the ATSB that they were not aware of the AFT CFI’s extended absence from their FTS.
Consequently, the AFT instructors were not under direct supervision for the majority of 2024, even though they had all only received their instructor ratings in 2023. Of note, the instructor who had qualified first, in early 2023, reported to the ATSB that they were all relatively inexperienced as instructors and they did not always conduct a check flight with the CFI during their return visits. This was supported by the accident pilot’s logbook, in which there were no check flights with the AFT CFI recorded in 2024. The fact that the AFT CFI had asked an external CFI to supervise the FTS indicated they were aware of their supervision requirements but ultimately did not comply with them.
Pre-flight video briefings
The RPC graduates from AFT Moama in 2023 and 2024 reported that they did not receive any classroom tutorials or in-person pre-flight briefs. Instead, they had to pay a subscription fee to access a series of flight training videos in which the CFI demonstrated the manoeuvres to be flown for each element of the RPC syllabus. While the CFI stated that the videos were not the pre-flight briefing, the AFT instructors reported that they represented the entirety of the pre-flight briefing, with no in-person pre-flight briefs delivered.
The use of this medium was not prohibited by the RAAus Exposition, but RAAus had not reviewed the material and therefore had no knowledge of the adequacy of instruction presented. Two RAAus CFIs who had reviewed the videos reported that the quality of instruction in these videos was inadequate as the sole source of pre-flight briefing material.
Within the video sequence for stalling, the AFT CFI demonstrated large rudder inputs near the stall speed and instructed the use of the rudder to level the attitude if a wing drop occurred. The risk of inducing a spin, as described in the CASA flight instructor manual for aeroplanes, was not acknowledged.
Additionally, during the stall demonstrations, the CFI omitted flap limiting speeds for the configured stall and did not demonstrate post-loss of control checks to confirm there was no overspeed or overstress of the flap. If flap is subjected to damage from an overspeed or overstress, further damage and control problems can occur if an attempt is made to retract the flap. In the case of an aircraft with a retractable landing gear, the landing gear could become stuck if an attempt to retract it is made after overspeed damage has occurred.
The stalling video also revealed incorrect terminology by the CFI for their explanation of the effect of lowering flap. This related to the basic lift formula, which should have been taught and reinforced throughout the syllabus.
While all these discrepancies may have been low risk in the demonstration aircraft, they introduced the potential for negative learning[12] in the lesson, which could be later applied in other aircraft types. The report from one of the AFT instructors, that they believed the accident pilot had copied the CFI in performing dumbbell reversal turns upwind in the circuit to expedite practice landings with students, indicated that negative learning was likely occurring at AFT.
A component of the instructor assessment was the in-person delivery of a pre-flight brief and post-flight debrief. However, this was not practiced by the staff at Moama after they passed their instructor rating because of the use of pre-flight video. The Moama RPC graduates reported that the lack of access to in-person tutorials and pre-flight briefs contributed to learning difficulties for their flight training and theory exams. The delivery of pre-flight briefs is also important for instructor development because the practice requires them to explain how the theory of flight will be applied in the lesson, check their student’s knowledge, and answer impromptu questions about the topic. It is also the time to discuss any hazards associated with the flight and ensure the student and instructor have a shared understanding of how the lesson will be conducted.
The report from one of the instructors after the accident that they were not aware of the relationship between angle of bank, load factor and stall speed, which is part of the RPC syllabus, may have been the result of knowledge decay because they were not required to deliver briefings. The substitution of video briefs for in-person pre-flight briefs was likely at the expense of both student and instructor development.
Online exams
The AFT CFI introduced an online exam platform used at the Moama Airfield school, for which their students and staff were provided with a login. The ATSB discussed the use of online exams with an instructor and RPC graduate who completed their exams at Riddell Airfield, and they both reported they followed the RAAus paper-based exam process and had no knowledge of the online platform.
The RPC graduates from Moama were prompted by the CFI or staff when they needed to complete a theory exam, which was done online and without supervision. The CFI setup the exams so that 2 attempts could be made and the correct answers to all questions were revealed in the exam report after the first attempt. Consequently, one of the graduates who failed the basic aeronautical knowledge exam on their first attempt photographed all the questions with the correct answers identified and passed the exam on their second attempt. More generally, the online exam setup likely created an attitude from the staff at AFT that candidates would naturally pass the exam on a second attempt if needed. Significantly, there were no failure results from 146 exams in the AFT exam records over a 3-year period.
The accident pilot’s first attempt at the RAAus private pilot licence (aeroplane) (PPL(A)) equivalent exam was completed using the AFT online platform. The software provider had informed the CFI that answer ‘A’ was set as the default correct answer to all questions as they were not provided with the marking rubric. The pilot had used this platform previously for their instructor exam in May 2023 and, given that the other instructor from Moama was aware of how the system was setup, it was very likely that the pilot was also aware of the settings. Consequently, the pilot’s selection of answer ‘A’ to 47/50 questions, the majority of which were technically incorrect, indicated that they were answering to the marking system and not the questions.
The pilot’s selection of answers may have resulted from the exam report providing the correct answers after a failed first attempt or from the CFI informing the pilot of the default correct response. In either case, the CFI reported that as the administrator, they were the only person who could download a copy of the exam. Therefore, they would have known the result for the exam they submitted to RAAus was almost certainly incorrect based on the default marking.
Contributing factor The Adventure Flight Training school management practices did not provide the required level of supervision, training and assurance that their graduates had achieved the required level of aeronautical knowledge and understanding for the qualifications they received. (Safety issue) |
Recreational Aviation Australia examination system
The RAAus Exposition, approved by CASA under CASR Part 149, provided a basic overview of their examination system. Multiple-choice exams were provided and the FTSs were to store them securely and not reproduce or distribute them. The exams were distributed to the FTSs via email after each respective CFI had signed a declaration that the exams would be stored securely and not be reproduced or distributed. Candidates for theory exams were provided with an exam answer sheet on which they recorded their answer to each question. All exams were required to be supervised, marked, debriefed and the results recorded and retained by the FTS, with the exception that the RAAus PPL(A)-equivalent exam was to be marked by RAAus. There was no documented exam failure management process.
The RAAus instructor application form indicated that the upgrade to senior instructor was the only time that proof of successful exam completion was required to be provided, which was a change introduced in 2023. Prior to 2023, RAAus did not require proof of completion of any exams for the issue of a qualification or endorsement. In each case they accepted the certification from the examiner that the theory component was met. However, this did not necessarily confirm the examiner had sighted the exam and their certification could be based on the record of result provided by the FTS. The RAAus Exposition required the FTSs to be able to provide exam results on request and RAAus reported that it was the record of exam results that they inspected at audit and not the exam answer sheets.
Consequently, the AFT CFI was able to progress through their instructor and senior instructor upgrade to CFI approval and the establishment of the AFT FTS, all without providing proof to RAAus that they had completed the associated theory exams. After the FTS was established, the CFI setup a system for online exams that could be completed by AFT members as open-book assessments without supervision. Further, all correct answers were revealed after the first attempt, and the exam could be immediately retaken. This non-compliant system likely existed throughout 2023, unnoticed by RAAus, as AFT’s use of an online platform only came to their attention in January 2024. The accident pilot had used the platform for their instructor exam in May 2023, but proof of completion of the instructor exam was not required to be provided to RAAus.
The CFI’s upgrade to senior instructor was investigated by RAAus in early 2024 after they discovered the accident pilot’s PPL(A)-equivalent exam failure. They were unable to confirm with the examiner for the CFI’s senior instructor upgrade that the associated exam was done. The setup of the AFT online exam system, and the CFI’s subsequent submission of an exam and certification of remote supervision by a former instructor 2 days after the exam was submitted, all suggested a cultural malaise towards the theory examination requirements.
The ATSB’s review of the RAAus examination system and the situation that unfolded at AFT, indicated that the only risk control evident in the theory examination system was the CFI declaration to not reproduce or distribute exams. The only effective oversight of exams by RAAus was the marking of the PPL(A)-equivalent exam, as the other oversight activities appeared to be limited to the records of exam results.
The situation at RAAus contrasted with the CASA examination system, which had multiple controls in place for the access to and conduct of exams, supported by surveillance of the examination centres, which could be unannounced. CASA also had restrictions in place for the exams that could be hosted by an FTS, such that a candidate for an instructor rating would have to conduct some of their theory exams at an examination centre independent of their FTS.
In 2025, there were a significant number of RAAus FTSs and members, estimated at 160 and 10,000+ respectively based on information from their website. This presented a significant risk management challenge for the integrity of their pilot examination system, particularly noting that their pilots could use their RPC to obtain a CASA licence. Considering the size and complexity of their operation, and what unfolded at AFT as described previously, the ATSB concluded that the RAAus examination system, as described in their Exposition, did not include sufficient controls to prevent the system from being exploited.
Contributing factor The Recreational Aviation Australia pilot theory examination system did not incorporate sufficient risk controls to ensure that their examination processes were followed as intended and their members had achieved the minimum required knowledge in accordance with the syllabus of flight training. (Safety issue) |
Restraint failure
The front seat occupants were ejected from their seats in the accident and the ATSB found the seatbelt latch plates separated from their buckles. However, no evidence was found to indicate the seatbelts were susceptible to false latching, and they were subjected to load testing by the builder. Other mechanisms by which a car seatbelt can fail to perform its function include inadvertent unlatching from occupant flailing in an accident and inertial unlatching. Inertial unlatching is a known phenomenon with car seatbelts in rollover accidents, when they are subjected to vertical accelerations.
The CASA advisory circular guidance for amateur-built experimental certificate aircraft (AC 21.4(2)) recommended that seatbelts comply with the US FAA Technical Standard Order approval for seatbelts. However, the builder did not believe they complied with the recommended standard and that the design was consistent with car seatbelts.
The ATSB reviewed pre-accident photographs of the interior of the aircraft and found the design of the seatbelts was consistent with car seatbelts and inconsistent with aircraft seatbelts. While the release of the front seatbelts would have contributed to the injuries sustained by the front seat occupants, the fatal injuries were likely the result of the ground impact.
Other factor that increased risk The aircraft’s front seats were likely fitted with car seatbelts, which unlatched in the accident and resulted in the front seat occupants being ejected from their seats. While this exposed them to additional injuries, the fatal injuries were likely from the aircraft-ground impact. |
Aircraft design and guidance
Energy attenuation
The pathologist reported that all occupants experienced non-survivable, blunt-force trauma injuries. However, the front seat occupants had a common vertebral crushing injury that was not found on the rear seat occupant. A likely source of the discrepancy between the front and rear seat occupant injuries was the location of the front seats above the main wing spar, as per the original design.
There are different mechanisms in which energy attenuation can be incorporated into design, but light aircraft are generally limited to the landing gear and seating. Poorly designed seats can produce spinal fractures in ground impacts as low as 8–10 G. In this situation, an unyielding structure, such as a main wing spar, can transmit a force to the occupant of the seat in excess of the ground impact force and the occupant will suffer injuries greater than those expected from the impact.
Neither the landing gear nor seating of the accident aircraft appeared to include consideration of crashworthiness in the design. The landing gear separated at impact and did not incorporate any stroking mechanism to absorb vertical energy, and the seating did not incorporate energy attenuation into the design. These 2 design deficiencies contributed to the severity of injuries to the occupants. However, the injuries indicated a minimum force experienced by the occupants and not the actual force they experienced. Therefore, it could not be concluded if a design change would have reduced the forces experienced to a survivable level. Despite that, the ATSB noted that similar accident scenarios in type-certified aircraft have been survivable.
Energy attenuating seat designs, such as stroking mechanisms, deforming box structures and rate-sensitive seat bottom cushions can all play a role in reducing the lumbar load experienced by the occupant in an accident. While there is no requirement for amateur-built aircraft to address this issue, it may be feasible for energy absorbing features to be incorporated into the design of some aircraft.
The CASA advisory circular guidance for amateur-built experimental certificate aircraft (AC 21.4(2)) recommended the delethalization of the cockpit and installing approved seatbelts but was silent on the issue of energy attenuation for the landing gear and seating. However, a 2013 ATSB aviation research report on amateur-built aircraft accidents found they resulted in a higher rate of fatal and serious injuries than factory‑built and certified aircraft. This indicated that the amateur-built industry could benefit from additional guidance in this area. However, as the CASA AC is guidance material and the recommendations may not be practicable for all builders to implement, it has not been raised as a safety issue.
Crashworthiness of the fuel system
The pathologist’s examination of the pilot indicated they were deceased prior to the post‑crash fire. However, the wreckage examination revealed a near total destruction of the cabin area by fire, while the extremities of the aircraft were relatively undamaged by fire. This was despite the collision occurring in a relatively level attitude in an open paddock with no penetrating objects.
The main fuel tank was carrying the flight fuel, and it was installed between the instrument panel and the engine firewall, as designed. This made it susceptible to rupturing in a collision and spraying fuel over the engine and occupants, which occurred in the accident. However, the wing fuel tanks installed aft of the main spar, which were a builder modification, were found intact and provided greater separation of the fuel load from the engine and occupants than the main tank.
The susceptibility of fuel tanks to rupturing in an accident is not new and there have been published recommended design standards to address this for light aircraft since at least 1980 (Johnson et al. 1980 and 1989). They included guidance for the location of fuel tanks, which should consider the location of occupants, ignition sources and probable impact areas. They recommended fuel tanks be located such that as much aircraft structure as possible can crush before the tanks are exposed to direct contact with obstructions.
The CASA advisory circular guidance for amateur-built experimental certificate aircraft (AC 21.4(2)) recommended reducing the risk of fire hazard. However, the specific design recommendations were limited to the inclusion of a fireproof firewall between the engine compartment and the cabin. It did not recommend or discuss how to incorporate crashworthiness into the design of the fuel system, and specifically the considerations for the location of fuel tanks.
Given the susceptibility of aircraft fuel tanks to rupturing and the detrimental effect that it can have on post-crash survival, the ATSB concluded that the amateur-built industry could benefit from additional guidance in this area. However, as discussed previously, the CASA AC for amateur-built experimental certificate aircraft is guidance material and the recommendations may not be practicable for all builders to implement. Therefore, it has not been raised as a safety issue.
Other factor that increased risk The aircraft design did not incorporate energy attenuation in the landing gear and seating and located the fuel tank between the engine firewall and instrument panel, which resulted in a post-crash fire. While these factors increased the severity of the injuries to the occupants, it could not be determined if design changes would have made them non-fatal. |
Other factor that increased risk The Civil Aviation Safety Authority guidance material for amateur-built experimental aircraft did not recommend consideration of the crashworthiness of seating and fuel tank installation. These characteristics within the design of the aircraft increased the risk of occupant injuries in an accident. |
Transition training guidance
The accident pilot was a member of a syndicate of 3 pilots who purchased the aircraft on 5 November 2024, 11 days before the accident. While the pilot and another member of the syndicate held instructor ratings, they were for RAAus-registered aircraft, which were 2‑seat aircraft with a maximum take‑off weight of 600 kg. The accident aircraft was a 4‑seat amateur-built experimental certificate aircraft on the CASA register with a maximum take‑off weight of 800 kg.
None of the syndicate pilots were qualified to instruct on this aircraft and none of them met the minimum licence requirements to conduct Phase 1 flight testing, which required a PPL(A) as a minimum. However, they could pilot the aircraft with an RPL as the Phase 1 flight testing of the aircraft was completed by the builder before they purchased it.
In the 11 days after the syndicate purchased the aircraft, ADS-B data recorded 7.7 hours of flying, the majority of which were ferry flights. While the accident pilot likely did most of the flying in the aircraft, the other syndicate members reported that it was unlikely that any aerial work training flights were conducted. One of the syndicate members was concerned about the weight and balance of the aircraft and they had agreed not to conduct any verification flights before the aircraft could be reweighed, which occurred 2 days prior to the accident. In addition, the builder had not conducted any familiarisation flights with them and had not recommended any aerial work exercises for them. Therefore, the ATSB concluded that the pilot had not received any transition training in the aircraft.
A 2013 ATSB aviation research report on amateur-built aircraft accidents found the pilots involved in accidents were significantly more experienced overall than factory-built aircraft accident pilots. However, they were significantly less experienced on the aircraft type that they were flying at the time of the accident, and a quarter of the accidents were from loss of control.
Previously, in 2012, the US National Transportation Safety Board published a report, which found that pilots who did not seek training for their experimental amateur-built aircraft were overrepresented in accidents. They reported that accidents involving loss of control could be reduced with transition training, which led to a recommendation to the FAA to develop resources for transition training and encourage builders and new owners to complete the training.
The FAA published AC 90-109(A) Transition to unfamiliar aircraft, in 2015. The AC stated that ‘accidents resulting from loss of aircraft control or situational awareness frequently result from pilot unpreparedness for challenges presented by the aircraft’ and provided recommendations for training experience based on aircraft performance and handling characteristics. The AC included an extensive discussion about the variety of stall characteristics that amateur-built aircraft can exhibit and recommended stall avoidance and recovery training from a qualified instructor.
The FAA AC included a ‘Best Training’ recommendation, which is accomplished in the specific aircraft the pilot intends to fly with a qualified instructor who has recent experience in the same make and model. The accident pilot had previously conducted transition training on the Pitts Special aircraft with an instructor who also had experience with the Morgan Cougar Mk 1 aircraft. Therefore, the ‘best training’ model recommended by the FAA in their AC was an option the syndicate could have pursued.
The CASA advisory circular guidance for amateur-built experimental certificate aircraft (AC 21.4(2)), included recommended safety precautions for the flight-testing phase, which emphasised a graduated process. The purpose of this was for the pilot to learn the behaviour of the aircraft near the centre of the flight envelope before pushing the aircraft out towards the predicted boundary of the envelope. As stated in the AC, ‘Violent or aerobatic manoeuvres should not be attempted until sufficient flight experience has been gained to establish that the aircraft is satisfactorily controllable throughout its normal range of speeds and manoeuvres.’ Despite these recommended precautions for pilots in the flight-testing phase, there were no recommendations for new owners to seek transition training or for sellers to recommend buyers conduct transition training.
The recommended precautionary approach to the flight testing in Phase 1 could equally apply to a new owner of an amateur-built experimental certificate aircraft. Therefore, the ATSB concluded that the amateur-built industry could benefit from further guidance in this area. However, the CASA AC for amateur-built experimental certificate aircraft is guidance material, which may not be practicable to follow in all circumstances, such as a single-seat unique design aircraft. Therefore, it has not been raised as a safety issue.
Other factor that increased risk The pilot had not conducted transition training and the Civil Aviation Safety Authority guidance material for amateur-built experimental aircraft did not include a recommendation for new owners to receive transition training. |
Civil Aviation Safety Authority management of suspension notices
An individual must be a member of RAAus to exercise the privileges of their RPC. Pilots can then use their RPC, issued by RAAus, to obtain a CASA-issued RPL without completing either a CASA pilot exam or flight test, although a CASA flight review was required to exercise the privileges of the RPL. RAAus is an approved self-administering aviation organisation under Civil Aviation Safety Regulation (CASR) 149, which imposes reporting requirements to CASA under CASR 149.425. The reporting line is from RAAus to the CASA Sport and Recreation Aviation Branch (CASA Sport).
The RAAus mandatory reporting requirements to CASA are detailed in their Exposition, specifically in their occurrence and complaints handling manual (OCHM) under the Formal Inquiry process. However, the RAAus Exposition has a safety related suspension (SRS) notice as a risk management tool within the Informal Assessment process. As the SRS sits within the Informal Assessment process, and is not enforcement action, it does not require notification to CASA. However, RAAus, at their own discretion, can notify CASA that they have issued an SRS where they believe the circumstances warrant such notification.
In August 2024, RAAus elected to notify CASA of the SRS issued against the AFT CFI because of the position the person held within RAAus. In December 2024, they notified CASA that an SRS was issued against the graduates of AFT because of the number of pilot certificate holders involved. However, the accident pilot had never been issued with an SRS despite their previous exam failures and flying history, and therefore, there was never any cause for CASA to receive a notification about the pilot.
On receipt of the RAAus AFT SRS notifications, CASA Sport entered the details into the CASA records management system, but no further action was taken. CASA had a process for follow-up of notifications, which was their Coordinated Enforcement Process (CEP), detailed in their enforcement manual. Within the CEP an investigator could be appointed to make preliminary enquiries and report findings to the Coordinated Enforcement Meeting for consideration.
After the ATSB received the details of the persons affected by the SRS issued to the graduates of AFT and their CASA licence status, it was found that 2 members also held RPLs at the time their SRSs were issued. In both cases, their RPL was granted based on their RPC which was subsequently suspended by the SRS. The ATSB spoke to one of those individuals, who reported that nobody from CASA had contacted them, but they had acted immediately to complete the remedial actions to have their SRS lifted. However, the second individual’s membership with RAAus had lapsed and they had not had their SRS lifted when the ATSB received the list of affected persons about 7 months after the SRSs were issued. RAAus confirmed that in this case the individual’s membership profile is flagged to address the remedial action if they re-activate their membership and that there were no continuing reporting requirements to CASA beyond the initial notification.
Consequently, an individual could continue to exercise the privileges of a licence issued by CASA based on holding an RPC while their RPC was suspended. This revealed a missing link within CASA’s internal process for handling the notification of an SRS, with no mechanism in place to ensure CASA Sport forwarded relevant information from the SRS to the CASA CEP for review.
Other factor that increased risk The Civil Aviation Safety Authority (CASA) Sport and Recreation Aviation Branch did not have a process in place to verify if individuals subject to a suspension from a self-administering organisation held a CASA licence and to ensure the information was provided to the CASA Coordinated Enforcement Process for review. (Safety issue) |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the loss of control and collision with terrain involving a Morgan Cougar Mk1 aircraft, registered VH‑LDV, 19 km NNW from West Sale Airport, Victoria, on 16 November 2024.
Contributing factors
- The aircraft entered an accelerated stall in a steep turn with insufficient height to recover, resulting in a collision with terrain.
- It was likely that the pilot had an inadequate understanding of the relationship between angle of bank, load factor and stall speed, which contributed to the pilot not fully understanding the risk of conducting slow steep turns.
- The pilot had a reported history of conducting low flying and slow steep turns and was likely unaware that, while the accelerated stall characteristics of the accident aircraft were unknown, there were indications that it would be abrupt.
- The Adventure Flight Training school management practices did not provide the required level of supervision, training and assurance that their graduates had achieved the required level of aeronautical knowledge and understanding for the qualifications they received. (Safety issue)
- The Recreational Aviation Australia pilot theory examination system did not incorporate sufficient risk controls to ensure that their examination processes were followed as intended and their members had achieved the minimum required knowledge in accordance with the syllabus of flight training. (Safety issue)
Other factors that increased risk
- The pilot was counselled about unsafe flying practices but was not reported to any authority and therefore no official follow-up action was ever initiated.
- The aircraft design did not incorporate energy attenuation in the landing gear and seating and located the fuel tank between the engine firewall and instrument panel, which resulted in a post-crash fire. While these factors increased the severity of the injuries to the occupants, it could not be determined if design changes would have made them non-fatal.
- The aircraft’s front seats were likely fitted with car seatbelts, which unlatched in the accident and resulted in the front seat occupants being ejected from their seats. While this exposed them to additional injuries, the fatal injuries were likely from the aircraft‑ground impact.
- The Civil Aviation Safety Authority guidance material for amateur-built experimental aircraft did not recommend consideration of the crashworthiness of seating and fuel tank installation. These characteristics within the design of the aircraft increased the risk of occupant injuries in an accident.
- The pilot had not conducted transition training and the Civil Aviation Safety Authority guidance material for amateur-built experimental aircraft did not include a recommendation for new owners to receive transition training.
- The Civil Aviation Safety Authority (CASA) Sport and Recreation Aviation Branch did not have a process in place to verify if individuals subject to a suspension from a self-administering organisation held a CASA licence and to ensure the information was provided to the CASA Coordinated Enforcement Process for review. (Safety issue)
Safety issues and actions
Adventure Flight Training school management
Safety issue number: AO-2024-058-SI-01
Safety issue description: The Adventure Flight Training school management practices did not provide the required level of supervision, training and assurance that their graduates had achieved the required level of aeronautical knowledge and understanding for the qualifications they received.
Recreational Aviation Australia examination system
Safety issue number: AO-2024-058-SI-02
Safety issue description: The Recreational Aviation Australia pilot theory examination system did not incorporate sufficient risk controls to ensure that their examination processes were followed as intended and their members had achieved the minimum required knowledge in accordance with the syllabus of flight training.
Civil Aviation Safety Authority management of suspension notices
Safety issue number: AO-2024-058-SI-03
Safety issue description: The Civil Aviation Safety Authority (CASA) Sport and Recreation Aviation Branch did not have a process in place to verify if individuals subject to a suspension from a self‑administering organisation held a CASA licence and to ensure the information was provided to the CASA Coordinated Enforcement Process for review.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Additional safety action by Recreational Aviation Australia
- The draft rewrite of the Recreational Aviation Australia (RAAus) occurrence and complaints handling manual (OCHM) has been updated to include a description of the process for handling a safety related suspension (SRS) for an individual whose membership has lapsed.
- The draft rewrite of the Recreational Aviation Australia (RAAus) syllabus of flight training has been updated to include further development of the stalling element of the syllabus.
Glossary
| AC | Advisory circular |
| ADS-B | Automatic dependent surveillance-broadcast |
| AGL | Above ground level |
| AFT | Adventure Flight Training |
| AMSL | Above mean sea level |
| CAS | Calibrated airspeed |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| CCTV | Closed-circuit television |
| CEP | Coordinated enforcement process |
| CFI | Chief flying instructor |
| FAA | Federal Aviation Administration (United States) |
| FOM | Flight operations manual |
| FTS | Flight training school |
| KDR | Knowledge deficiency report |
| NTSB | National Transportation Safety Board (United States) |
| OCHM | Occurrence and complaints handling manual |
| OCMS | Occurrence and complaints management system |
| PEXO | Pilot examination office. The CASA online theory examination system. |
| PI | Performance indicator |
| POH | Pilot operating handbook |
| RAAus | Recreational Aviation Australia |
| RPC | Recreational Pilot Certificate |
| RPL | Recreational Pilot Licence |
| SRS | Safety related suspension |
| US | United States |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- accident witnesses
- the aircraft builder
- Airservices Australia
- Bureau of Meteorology
- chief flying instructors from Recreational Aviation Australia
- Civil Aviation Safety Authority
- the former chief flying instructor from Adventure Flight Training
- former instructors and pilot graduates from Adventure Flight Training
- Recreational Aviation Australia
- Victorian Institute of Forensic Medicine
- Victoria Police
- video footage of the accident flight.
References
Australian Transport Safety Bureau (2013)
AR-2007-043(2)
(4.26 MB)
(AR-2007-043(2)), accessed 30 May 2025.
Civil Aviation Safety Authority (2000) Amateur-built experimental aircraft – certification (Advisory Circular 21.4(2)), accessed 13 May 2025.
Civil Aviation Safety Authority (2007) Flight instructor manual: aeroplane, accessed 26 March 2025.
Civil Aviation Safety Authority (2022) Experimental certificates (Advisory Circular 21-10 v4.3), accessed 13 May 2025.
Federal Aviation Administration (1986) Static strength substantiation of attachment points for occupant restraint system installations (Advisory Circular 23-4), accessed 24 June 2025.
Federal Aviation Administration (1993) Technical Standard Order: C22g, safety belts (TSO C22g), accessed 24 June 2025.
Federal Aviation Administration (2015) Amateur-built aircraft and ultralight flight testing handbook (Advisory Circular AC 90-89B), accessed 20 May 2025.
Federal Aviation Administration (2015) Transition to unfamiliar aircraft(Advisory Circular 90-109(A)), accessed 3 July 2025.
Society of Automotive Engineers (1986) Aerospace standards: Torso restraint systems (SAE AS 8043), accessed 24 June 2025.
Taylor AM and Moorcroft DM (2023) Seat and occupant response in energy absorbing seats (Civil Aerospace Medical Institute DOT/FAA/AM-23/17), accessed 22 May 2025.
Gratton G (2015) Initial airworthiness: determining the acceptability of new airborne systems, Springer, London.
Johnson NB et al. (1989) Aircraft Crash Survival Design Guide Volume V – Aircraft Postcrash Survival (USAAVSCOM TR 89-D-22E), accessed 3 July 2025.
National Transportation Safety Board (2012) The Safety of Experimental Amateur-Built Aircraft (NTSB/SS-12/01), accessed 28 March 2025.
Payne R and Stech E (1969) Dynamic models of the human body (Aerospace Medical Research Laboratory AMRL-TR-66-157), accessed 3 July 2025.
Roberts et al. (2007) ‘Failure analysis of seat belt buckle inertial release’, Engineering failure analysis, 14(6):1135-1143.
Shanahan DF (28-29 October 2004) Basic Principles of Crashworthiness: Pathological Aspects and Associated Biodynamics in Aircraft Accident Investigation. Madrid, Spain: RTO-EN-HFM-113, accessed 3 July 2025.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- the aircraft builder
- Civil Aviation Safety Authority
- the former chief flying instructor from Adventure Flight Training
- Recreational Aviation Australia.
Submissions were received from:
- Civil Aviation Safety Authority
- the former chief flying instructor from Adventure Flight Training
- Recreational Aviation Australia.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Appendices
Appendix A – Examination of the flight controls
Introduction
Examination of the flight control system chainring and bearings included a photographic review of the chainring at the wreckage site and as installed in the aircraft pre-accident, which was behind the instrument panel (Figure 12).
Figure 12: Location and movement of chainring
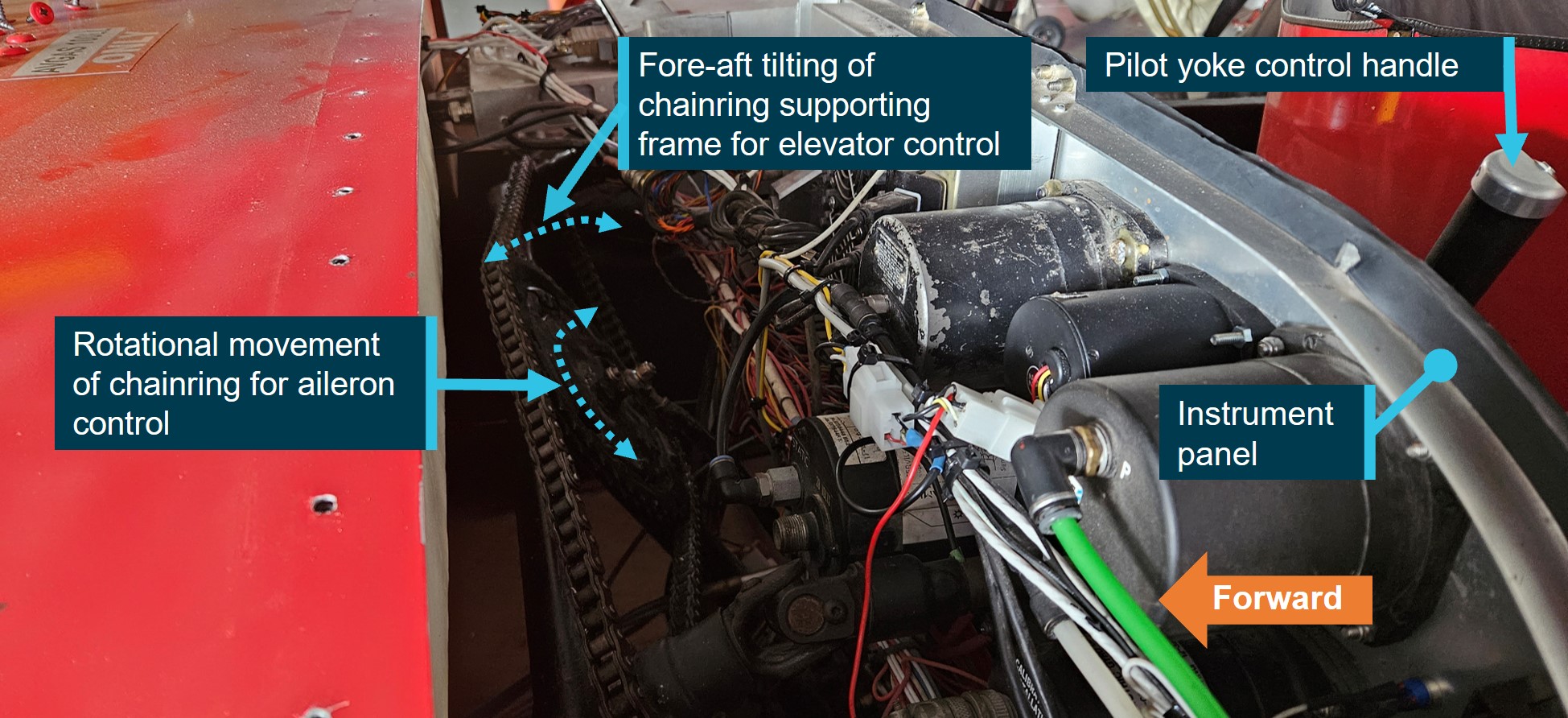
Source: ATSB
The part that transmitted roll control from either yoke to the ailerons consisted of 2 chainrings welded together around a hexagonal nut to form one part, hereafter referred to as the ‘chainring’ (Figure 13). The chainring was supported by an inner and outer bearing attached to a support frame. Two grub screws located in threaded holes through the nut were present to secure the chainring to a bearing.
Figure 13: Front chainring facing pilot (left) and rear chainring facing engine (right)
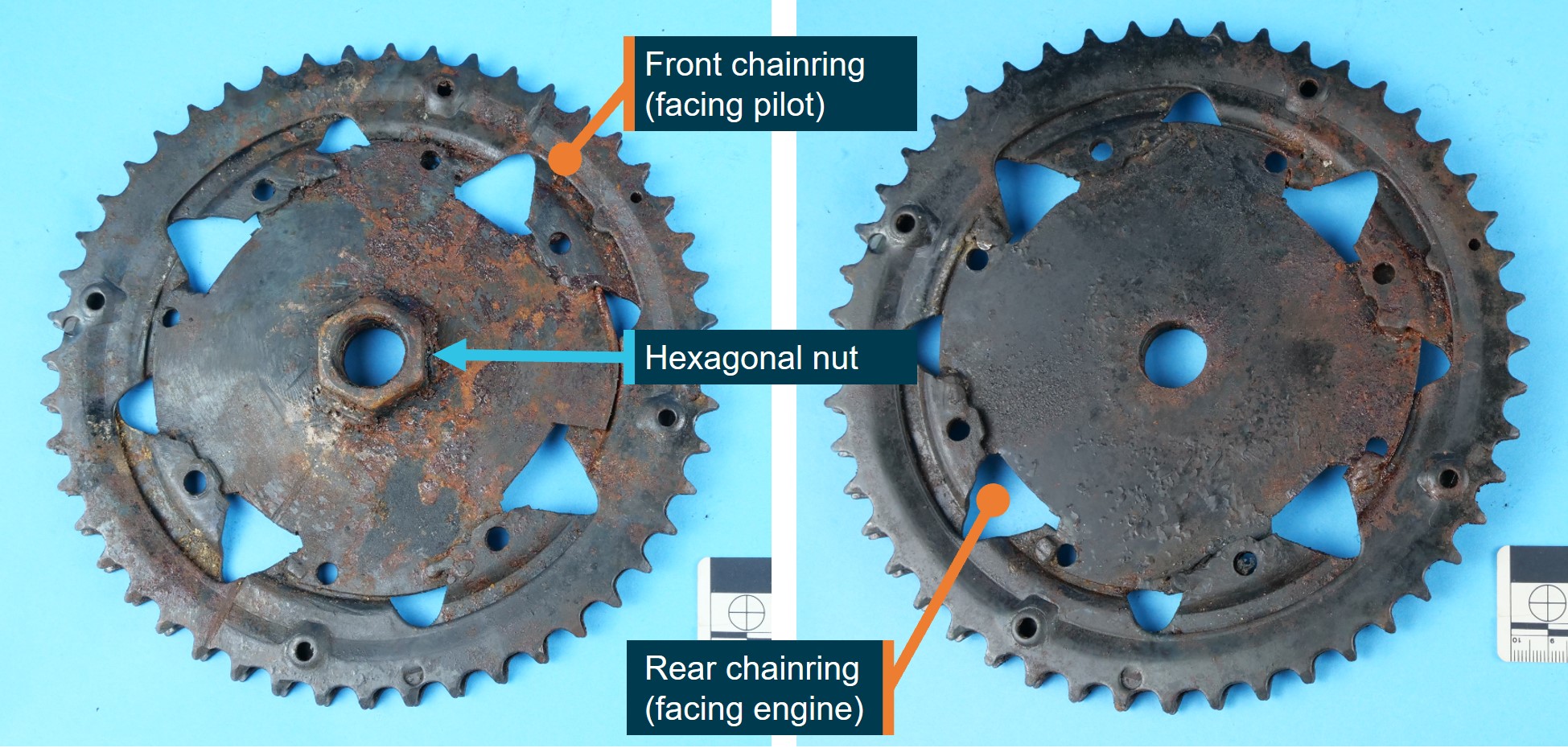
Source: ATSB
Examination and findings
It was noted that the chainring hexagonal nut appeared to be centrally located on the bearings (Figure 14 left) before the controls were disturbed for onsite examination and that the chainring only separated from the bearings when it was disturbed. Pre- and post‑accident photographs of the flight controls and measurement of the clearance between the chainring and the support frame indicated that the 2 grub screws could only have engaged with the outer bearing (Figure 14 right).
Figure 14: Location of bolt relative to hexagonal nut (left) and bearings (right)

Source: ATSB
The examination found that the 2 grub screws were not proud of the hexagonal nut inner diameter (Figure 15 [1, 2]) and they had an angular separation of 117° (Figure 15 [3]). The inner bearing and the outer bearing (Figure 15 [4]) were examined, cleaned and re‑examined. No witness marks from the grub screws were identified. The grub screws (Figure 15 [5, 6]) were examined, cleaned and re-examined and no bearing witness marks were identified. Therefore, ATSB examination could not confirm that the grub screws retained the chainring to either bearing.
Figure 15: Condition of grub screws and outer bearing

Source: ATSB
Appendix B – Flight path description
Introduction
The end-of-flight analysis was divided into sections based on the manoeuvring of the aircraft, which have been annotated on the supporting figures. It started with a right turn, followed by a reversal into a left turn followed by 2 full orbits. A third left orbit commenced inside of the second orbit, which led to the stall and collision with terrain. Airservices Australia ADS-B data was used, and altitudes are recorded in 25 ft increments. The last 3 data points, considered unreliable, were inconsistent with the observed CCTV and were potentially predicted points that were not updated prior to the collision.[13] The calibrated airspeed (CAS) range was calculated by the ATSB using a 6 kt mean wind and 12.8 kt wind gust from 124° T recorded at a local weather station 4 km north of the accident site.
End of flight description
With reference to Figure 16:
- At the start of the right turn (RH turn – yellow) at 1744:17, the aircraft recorded a groundspeed of 98 kt (87–91 kt CAS) and an altitude of 825 ft (683 ft AGL). Altitude was maintained through the turn, but groundspeed (and estimated CAS) reduced.
- The first orbit (First orbit – blue) started at 75 kt groundspeed (78–85 kt CAS) and an altitude of 825 ft (689 ft AGL) and the aircraft descended about 250 ft during the orbit.
- The second orbit (Second orbit – orange) started at 82 kt groundspeed (84–89 kt CAS) and an altitude of 575 ft (442 ft AGL). During the orbit, the aircraft descended and conducted a low pass (Low pass) at 97 kt groundspeed (89–92 kt CAS) and an altitude of 225 ft (97 ft AGL).
- A brief straight section (cyan) started at 69 kt groundspeed (72–79 kt CAS) and an altitude of 400 ft (267 ft AGL) and reduced to 64 kt groundspeed (67–74 kt CAS) at the start of the final turn (Turn – magenta) at 1746:52.
- In the final turn at 1746:59 (Stall), the groundspeed reached a minimum of 56 kt (59–65 kt CAS) at an altitude of 350 ft (221 ft AGL) as the turn radius tightened and an average of 45° angle of bank was required for this turn radius.
- The last reliable data point was recorded at 1747:02 and indicated a groundspeed of 71 kt (69 kt CAS) at an altitude of 275 ft (143 ft AGL). The abrupt descent and increase in speed were consistent with a conventional stall response.
In the accompanying Figure 17, the start of the right turn (RH turn), start of the first orbit (First orbit), start of the second orbit (Second orbit), low pass (Low pass), start of the final turn (Turn) and stall (Stall) are annotated. The lowest speeds were recorded on the segment from the final turn to the stall, which was also the segment with the smallest turn radius.
Figure 16: Accident flight path
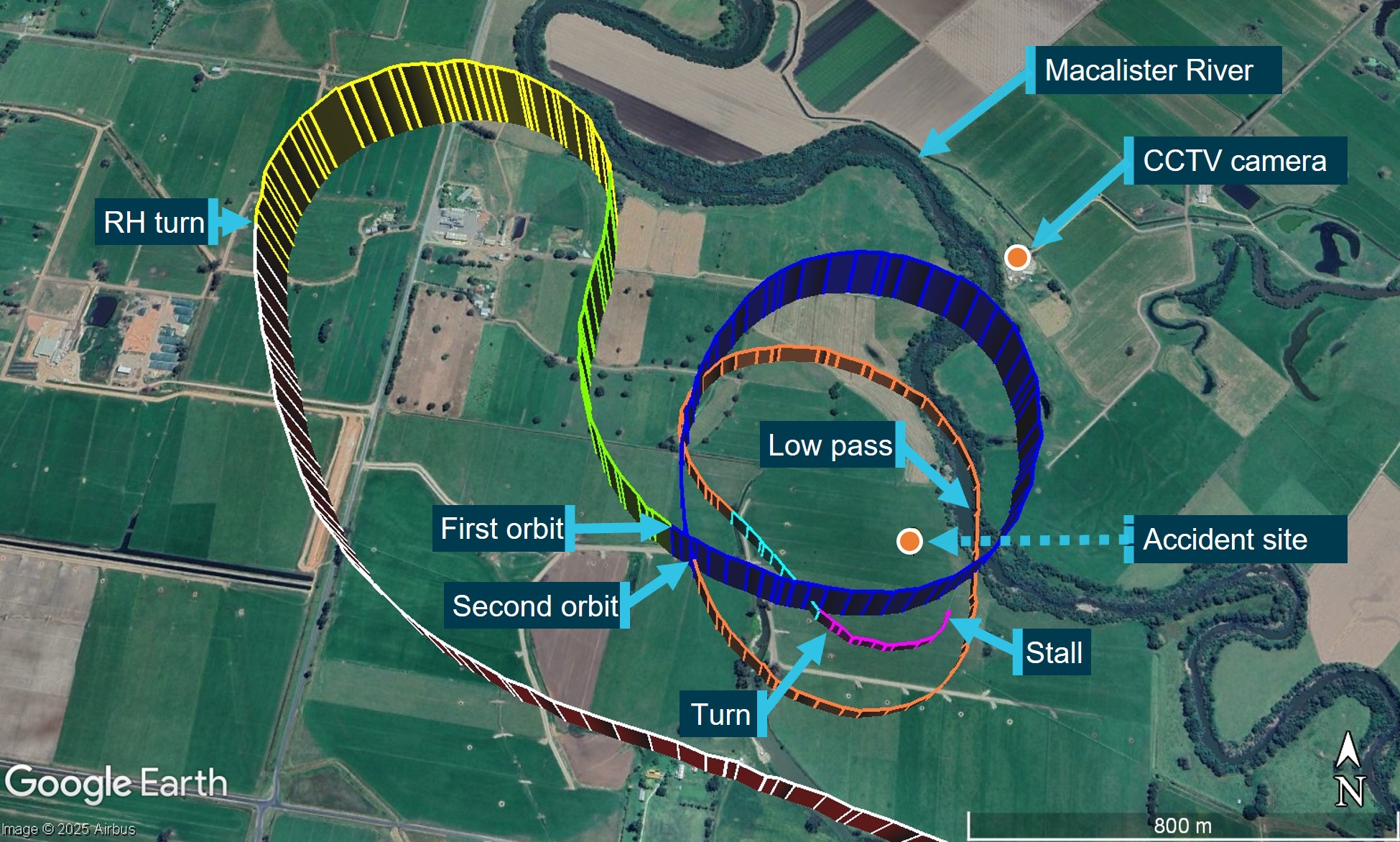
Source: Airservices Australia, annotated by the ATSB
Figure 17: Plot of ADS-B data and CAS calculations with the start of each orbit
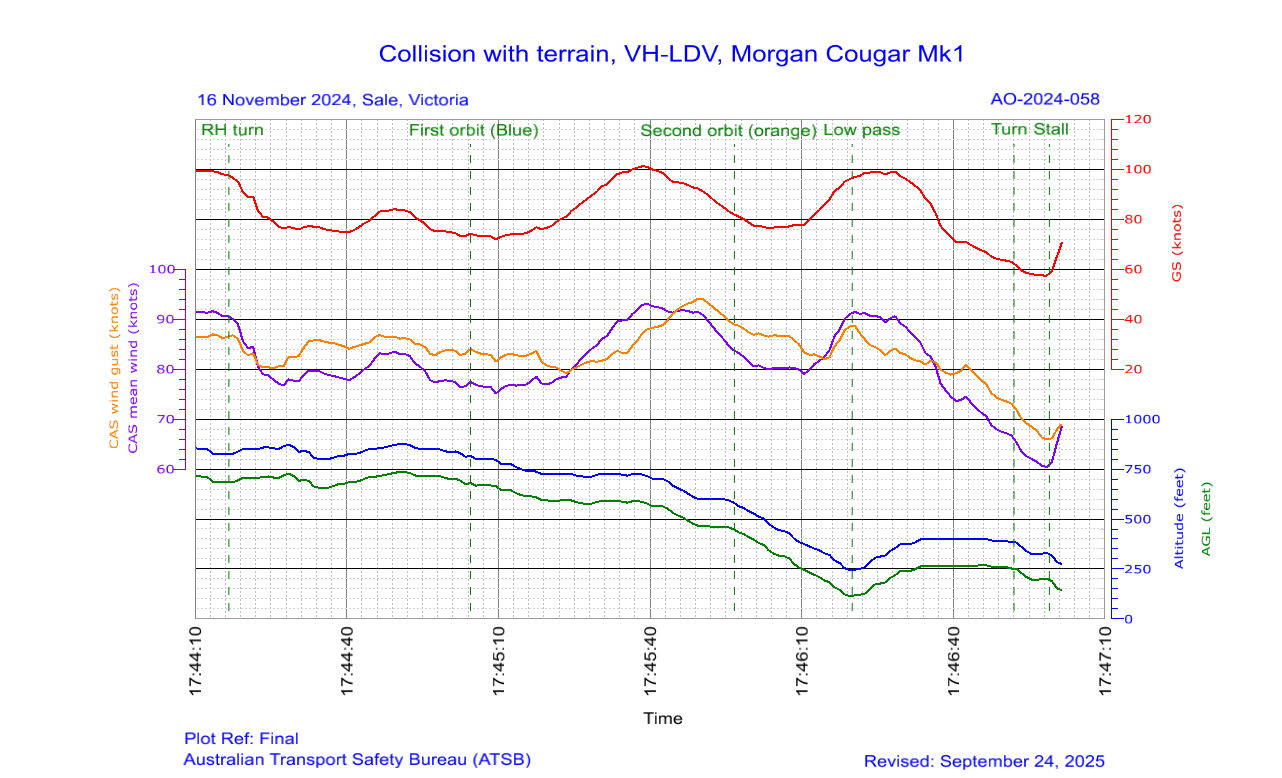
Source: ATSB
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2026 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Firewall: a fire-resistant bulkhead that separates the engine compartment from the cockpit or cabin area.
[2] There was a main spar for each wing, which were bolted together underneath the seats to form one continuous main spar.
[3] METAR: a routine report of meteorological conditions at an aerodrome. METAR are normally issued on the hour and half hour.
[4] Aerodynamic stall: occurs when airflow separates from the wing’s upper surface and becomes turbulent. A stall occurs at high angles of attack, typically 16° to 18°, and results in reduced lift.
[5] Maximum coefficient of lift prior to the wing stalling.
[6] Load factor is the ratio of the lift of an aircraft to its weight and is also referred to as the G load.
[7] Reference has been made to historical standards as they were prescriptive and in some cases these standards are now performance-based, which can make current standards more difficult to use for comparisons.
[8] The Adventure Flight Training school ceased operations in August 2024 and was later sold. All references to the AFT CFI in this report are to the CFI from the inception of the school in June 2019 to August 2024.
[9] This was a different CFI to the CFI who conducted the pilot’s instructor flight test.
[10] A coordinated positive G pitching and rolling manoeuvre.
[11] The reference to independence assumes the FTS and examination centre are independent businesses.
[12] For this report, negative learning is the interference of new leaning with the correct knowledge and/or skills to perform a task and can be detrimental to future task performance compared with no learning.
[13] The Kalman Filter algorithm used in global navigation satellite systems uses past data to predict future positions.
Preliminary report
Report release date: 18/12/2024
| This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003. |
The occurrence
At 1730 local time on 16 November 2024, an amateur-built Morgan Cougar Mk 1 aircraft, registered VH-LDV (LDV), with a pilot and 2 passengers onboard, departed from West Sale Airport, Victoria for a flight over the local area. Flightradar24 data indicated the aircraft conducted a left turn on departure and tracked 8 NM (15 km) north of West Sale Airport to the town of Maffra. The aircraft arrived overhead Maffra shortly after 1736 where LDV made a series of turns overhead the town for about 4 minutes. At 1740, the aircraft departed from overhead Maffra and tracked about 6 NM (11 km) west-north-west towards Tinamba West (Figure 1).
The aircraft conducted a right-hand turn overhead a property at Tinamba West, which belonged to relatives of the aircraft occupants, before commencing a series of left-hand turns (orbits) around a point about 1 km to the south-east of the property over open paddocks. The last data point was at 1747, after LDV had commenced a third left-hand orbit, which recorded the aircraft at an altitude of 450 ft at a groundspeed of 60 kt on a track of 073° True (T).
A closed-circuit television (CCTV) camera, located about 700 m north-north-east of the accident site, captured LDV in a left turn towards the camera. Subsequently, the nose of the aircraft pitched down and the aircraft descended in the left turn behind trees (Figure 2). About 14 seconds later a plume of dark smoke rose up above the trees. The 3 occupants were fatally injured in the accident and the aircraft was destroyed.
Context
Local weather data
A local weather station, about 4 km north of the accident site, recorded the following temperature and wind velocity information at 1745 and 1750 on the day of the accident:
Table 1: Local weather data
Time | Temperature (°C) | Wind speed (kt) | Wind gust (kt) | Wind direction (°T) |
1745 | 27.5 | 6.2 | 8.0 | 124 |
1750 | 27.3 | 6.4 | 12.8 | 122 |
Accident site
The aircraft impacted flat and open terrain at an elevation of about 130 ft and produced a ground scar on a track of 315° T (Figure 3). The length of the wreckage trail was about 30 m from the first ground scar to the propeller spinner, with the fuselage resting on a heading of 303° T. There was a diamond-shaped fuel spray and debris pattern along the wreckage trail.
Fuel was ignited after the ground impact, however, most of the fire damage to the aircraft was confined to the fuselage within the area bounded by the firewall, aft bulkhead (behind rear seats) and the inboard sections of the wings. The wings and tailplane (except the rudder) remained attached to the fuselage. The engine was attached to the firewall and the 3-bladed propeller was attached to the engine. One propeller blade was attached to the hub and the other 2 propeller blades had separated at their roots but were found within the debris field.
Figure 1: Accident flightpath with key timings and locations

Source: Flightradar24 and Google Earth, annotated by the ATSB
Figure 2: CCTV footage of final turn
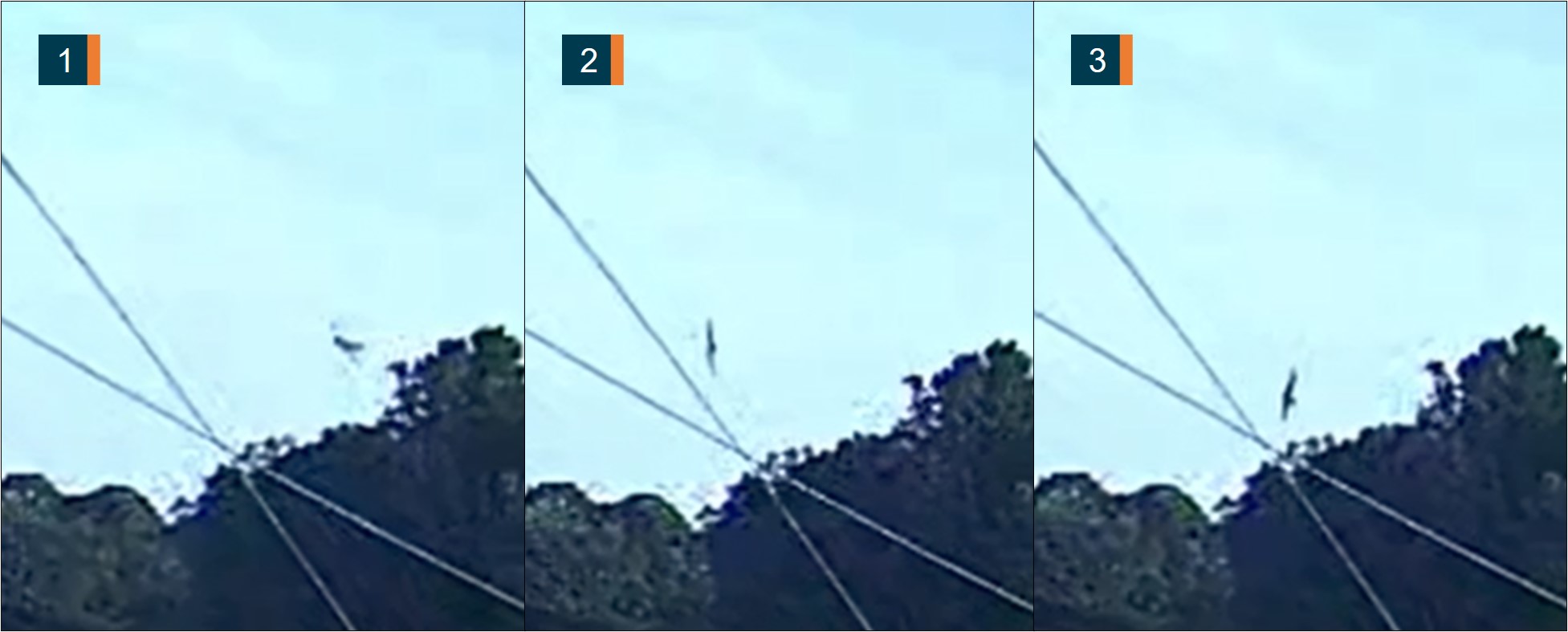
Images subject to visual distortion (fisheye lens effect).
Source: Victoria Police, annotated by the ATSB
Figure 3: Accident site

Source: ATSB
Further investigation
To date, the ATSB has:
- examined the accident site
- retrieved hardware and avionics from the wreckage
- collected witness statements, CCTV and drone footage, local weather data, pilot licencing and medical information and aircraft records.
The investigation is continuing and will include:
- examination and analysis of the avionics unit and aircraft hardware
- a review of aircraft records, including design and certification standards
- a review of witness reports
- interviews with key personnel.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Acknowledgements
The ATSB acknowledges the support provided by Victoria Police during the onsite investigation phase.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
Occurrence summary
| Investigation number | AO-2024-058 |
|---|---|
| Occurrence date | 16/11/2024 |
| Location | 19 km north-north-west of West Sale Airport |
| State | Victoria |
| Report release date | 19/01/2026 |
| Report status | Final |
| Investigation level | Systemic |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain, Loss of control |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | Amateur Built Aircraft |
|---|---|
| Model | Morgan Aero Works Cougar Mk1 |
| Registration | VH-LDV |
| Serial number | 6 |
| Sector | Piston |
| Operation type | Part 91 General operating and flight rules |
| Departure point | West Sale Airport, Victoria |
| Destination | West Sale Airport, Victoria |
| Damage | Destroyed |
Fuel management, unsecured cap risk highlighted

The pilot of an Aero Commander had to land the aircraft in a field after fuel siphoned overboard due to an incorrectly installed fuel cap, an ATSB investigation has concluded.
On 8 March 2024, the twin-engine Aero Commander 500-S was conducting a return freight flight from Bankstown to Parkes, with multiple stops each way.
Upon landing after the first sector of the day, the pilot found the aircraft’s fuel cap was off and secured only by a retention chain.
The pilot re-secured the cap, but found the cap off again after the second sector, after landing in Parkes.
“For the two sectors from Bankstown to Parkes, the fuel cap had been incorrectly installed with the retention chain lodged in the fuel tank’s anti-siphon valve, resulting in the cap dislodging in flight, and fuel being siphoned overboard,” ATSB Director Transport Safety Stuart Macleod explained.
An inspection and rectification conducted at Parkes by a maintenance engineer fixed the issue.
“However, the pilot identified an unexplained discrepancy between expected fuel remaining and gauge quantity indication, but did not refuel to a known quantity, or amend the flight log,” Mr Macleod noted.
“This meant the aircraft left Parkes without enough fuel to complete the remaining sectors on its return trip back to Bankstown.”
After departing Parkes, the pilot likely did not monitor the fuel gauge, continued fuel calculations based on an incorrect fuel quantity, and did not refuel the aircraft to a known quantity when they landed at their final interim location, Bathurst.
Subsequently, shortly after take-off for the final sector to Bankstown, both engines lost power due to fuel exhaustion, and the pilot conducted a forced landing in a field. Fortunately, the aircraft was undamaged, and the pilot uninjured.
“A missing or unsecured fuel cap should be treated as an emergency, and if detected pilots should immediately divert to the nearest suitable aerodrome,” Mr Macleod said.
Since the incident, the operator, GAM Air, published a notice to pilots reinforcing fuel management procedures. It also commenced periodic auditing of pilot fuel calculations.
Additionally, in response to an ATSB finding that its Quick Turn Around – Pre-Start checklist did not include a fuel quantity check before start, the operator has announced the intention to discontinue using this specific checklist.
“Pre-flight fuel quantity checks should use at least two different verification methods to determine the amount of fuel on board,” Mr Macleod said.
“When using computed fuel on board and comparing against gauge readings, it is important that calculations are accurate. If any discrepancy is detected between the two methods, another method such as filling to a known quantity is required.”
Read the final report: Fuel exhaustion involving Aero Commander 500-S, VH-MEH, 6 km east of Bathurst Airport, New South Wales, on 8 March 2024
Tinamba West aircraft accident
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into an accident involving an amateur-built light aircraft at Tinamba West, Victoria, on Saturday.
As reported to the ATSB, the aircraft collided with terrain in a paddock and was destroyed in a post impact fire.
The ATSB is deploying to the accident site a team of transport safety investigators from its Canberra office, specialising in aircraft operations and maintenance.
Investigators will conduct a range of evidence-gathering activities on site, including wreckage examination and recovery of any relevant aircraft components for further examination at the ATSB’s technical facilities in Canberra.
Investigators will also seek to interview any witnesses and collect relevant recorded information including any flight tracking data, as well as pilot and aircraft maintenance records, and weather information.
The ATSB asks anyone who may have witnessed or has photos or video footage of the aircraft at any phase of the flight to make contact via the witness form on our website: atsb.gov.au/witness at their earliest opportunity.
The ATSB anticipates publishing a preliminary report, detailing the information collected in the investigation’s early evidence gathering phase, in about six to eight weeks.
Tool left in A380 engine highlights importance of tool control
An A380 operated multiple flights with a tool inside one of its engines, after maintenance engineers did not commence the lost tool procedure prior to the aircraft being released to service, an ATSB investigation report details.
The 1.25 m long nylon tool, used to turn the engine’s intermediate‑pressure compressor during borescope inspections, was found wedged against the low-pressure compressor outlet guide vanes during a scheduled maintenance check at Los Angeles on 1 January 2024.
It was determined that that the tool had been left in the engine during previous scheduled maintenance in Los Angeles on 6 December 2023.
Between the two maintenance checks, the Qantas aircraft had flown 34 cycles, totalling 294 hours, with the tool in the engine. Although the tool was found to have been deformed by high energy airflow, there was no damage observed to the engine itself.
“The ATSB investigation found that maintenance engineers did not notice the tool had been left in the engine’s low-pressure compressor case when conducting checks for foreign objects at the completion of the borescope inspection task,” ATSB Chief Commissioner Angus Mitchell said.
“Further, maintenance engineers did not commence the lost tool procedure once the tool had been identified as missing, and the certifying engineer released the aircraft for service with the tool unaccounted for.”
After the tool was discovered, Qantas Engineering immediately briefed staff on the importance of ensuring all tooling is returned and actioned by tool store personnel.
The operator also completed an internal investigation, which resulted in an internal safety directive regarding complying with company tool control requirements.
“Foreign object debris and damage can pose a significant threat to the safe operation of aircraft, which is why regulations, procedures and training are in place to limit the risk of foreign object damage, especially from introduced objects during maintenance,” Mr Mitchell noted.
“Correctly applying tool control is fundamental to mitigating against any human errors that may arise.”
Read the final report: Foreign object debris event involving Airbus A380, VH-OQI, at Los Angeles International Airport, United States, on 1 January 2024
King Air wheels-up landing after nose gear fracture

A King Air’s nose landing gear became jammed during retraction after take-off when a fatigue crack in the steering link fractured, necessitating a wheels-up landing, an ATSB investigation found.
On 13 May 2024, the Beechcraft King Air B200 had departed Williamtown Airport, Newcastle on a charter flight to Lord Howe Island via Port Macquarie, with a pilot and two passengers onboard.
As the pilot retracted the landing gear during the initial climb, mechanical crunching noises were heard, and the pilot saw that the red indicator lights on the landing gear control handle remained illuminated. An air traffic controller subsequently visually confirmed that the nose landing gear was only partially retracted.
“Unable to extend the gear following emergency extension procedures the pilot held for approximately four hours to burn fuel, before conducting a wheels-up landing at Williamtown with emergency services standing by,” ATSB Director Transport Safety Stuart Macleod said.
The aircraft sustained minor damage in the landing, but the pilot and passengers were uninjured.
“Detailed examination of the steering link at the ATSB’s technical facilities in Canberra, including with the use of a scanning electron microscope, identified a pre-existing fatigue crack on the fracture surface, which had initiated from a surface flaw,” Mr Macleod explained.
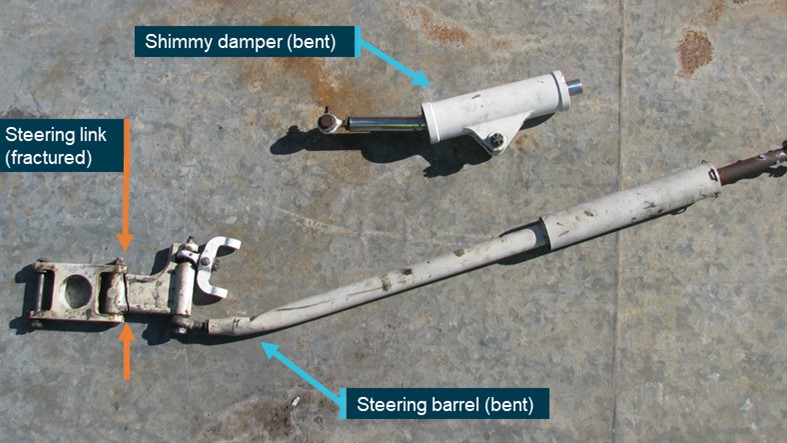
“When the steering link fractured, either during take-off or the gear retraction sequence, the nose wheel was able to rotate beyond its normal operational limits, and a significant left rotation led the nose gear shimmy damper to become jammed against a door hinge within the nose wheel well.”
During the course of the investigation, the aircraft manufacturer advised the ATSB that it was not aware of other instances of this specific malfunction, and nor did a review of the ATSB database identify any similar previous occurrences involving Kings Airs.
“Nonetheless, King Air B200 operators and maintainers should be aware that while scheduled maintenance inspections require general inspection of the nose wheel steering parts, they do not call for a detailed inspection for cracks – such as the one which precipitated this failure,” Mr Macleod said.
The incident highlights the value of aircraft system knowledge, and resource management in resolving malfunctions and in-flight emergencies, Mr Macleod observed.
“The pilot managed fuel considerations to reduce the risk of fire, engaged company personnel and air traffic control for assistance, liaised with emergency services and prepared the passengers for the wheels-up landing, minimising the risk of injury and ensuring the evacuation was conducted safely.”
Read the final report: Wheels-up landing involving B200 King Air, VH-XDV, at Williamtown Airport, New South Wales, on 13 May 2024