An aerobridge at Brisbane Airport’s international terminal collided with parked Boeing 737s on two occasions last year, an ATSB investigation final report details.
In the first incident, on 18 June 2025, the Gate 82 aerobridge shattered the right windshield of a Qantas 737-800. Glass fragments landed on the first officer, but there were no injuries.
Just over a month later, on 26 July, the same aerobridge also shattered the left windshield of a Fiji Airways 737-8 MAX. Glass and the corner of the aerobridge entered the cockpit, but the captain was able to move out of their seat before impact, and there were no injuries.
In each incident the aircraft was correctly positioned at the gate, and the aerobridge operator was an employee of the respective airline.
“The ATSB’s investigation identified safety factors common to both occurrences, finding that both aerobridge operators could not see the parked aircraft when they began to extend the aerobridge,” ATSB Chief Commissioner Angus Mitchell said.
The investigation report notes Gate 82 catered for both wide-body and narrow-body aircraft, and that the parking position for a 737 was to the far right of the aerobridge home position, meaning the aerobridge operator had restricted visibility of the aircraft from the aerobridge home position.
“Narrow-body aircraft, such as the 737, sit lower to the ground than wide-body aircraft,” Mr Mitchell explained.
“As a result, to minimise the slope of the passenger tunnel, at Gate 82 they park further from the aerobridge home position than would be the case for wide-body aircraft, or at a gate designed only for narrow-body aircraft, such as many domestic terminal gates.”
This meant the Gate 82 aerobridge had to extend much further, and almost parallel to a narrow-body aircraft, in order to attach to it.
“In addition, this aerobridge lacked side viewing windows, as installed in some other aerobridges at the airport, limiting the visibility of narrow‑body aircraft along the docking path,” he said.
The investigation found it was accepted practice for operators to extend the aerobridge without first being able to see the aircraft, with an expectation it would come into view during the extension.
“This expectation was reinforced by successful operations in the past,” Mr Mitchell noted.
“But during the collision events, each aerobridge operator moved the joystick to a 3 o’clock position after rotating the cab left, unaware that this orientation would change the aerobridge’s direction of travel.”
Consequently, as it extended, the aerobridge moved diagonally towards the aircraft, rather than parallel to it, while the aerobridge operator did not have visual reference.
The ATSB identified aerobridge training and in-cab instructions did not direct operators to gain and maintain visibility of the aircraft before moving the aerobridge.
Brisbane Airport Corporation has subsequently disseminated information to all operators emphasising the requirement to rotate the cab towards the aircraft, and to maintain positive line-of-sight during aerobridge operations.
It has also reviewed operator training manuals and identified gaps and opportunities to be more specific in the process to safely attach aerobridges to aircraft.
The airport has also created a new quality assurance role focused on airside performance of assets and operators.
“Aerobridges should be designed with visibility of aircraft in mind, and training should reinforce the importance of maintaining visual reference while operating an aerobridge,” Mr Mitchell said.
Brisbane Airport says a program to replace eight aerobridges, including Gate 82, will include a review of safety features and narrow-body aircraft visibility.
08/03/2017: A story on ABC’s 7.30 program (7 March 2017) and an article on the ABC news website, “Air safety watchdog clearly failing”, contains inaccurate and misleading claims that require correction.
Firstly, the reports quote Mr Neil Hansford as saying:
"Until a case is resolved, there can be no remedial action taken by the relevant authorities, CASA (Civil Aviation Safety Authority) or the Department of Transport or even private airport operators."
In fact, the ATSB does not wait for an investigation to be completed to bring safety matters to the attention of operators and authorities.
When the ATSB discovers critical safety issues during an investigation, it immediately brings them to the attention of relevant authorities and organisations to be addressed.
Mr Hansford also claimed that the ATSB's failure to meet its investigation targets was linked to its role in the search for Malaysia Airlines Flight MH370.
The search for MH370 has not affected the ATSB’s core functions. Additional funding was provided by the governments of Malaysia, the People’s Republic of China and Australia to assist the ATSB lead the search for the missing aircraft.
Australian aviation safety has not been compromised by the ATSB’s lead role in the search for MH370.
The ABC also quotes Mr Ben Morgan as saying “We cannot have scenarios where we're waiting five and seven years to wrap up an investigation”.
In fact, excluding delayed investigations beyond the control of the ATSB, the average time the ATSB takes to complete its reports is 14 months. The ATSB is seeking to improve its efficiency in meeting its self-imposed target of complex investigation reports published in 12 months.
Occurrence Briefs are concise reports that detail the facts surrounding a transport safety occurrence, as received in the initial notification and any follow-up enquiries. They provide an opportunity to share safety messages in the absence of an investigation. Because occurrence briefs are not investigations under the Transport Safety Investigation Act 2003, the information in them is de-identified.
What happened
On 28 February 2026, a pilot was conducting a private flight from Orange, New South Wales, to a privately‑owned, unsealed airstrip near Louth, New South Wales, with one passenger on board. During approach, the pilot observed gusting winds and localised whirlwind activity in close proximity to the runway.
As the aircraft decelerated through approximately 30 to 25 kts during the landing roll, the aircraft yawed to the left with an increasing gust of wind. The pilot applied right rudder in an attempt to arrest the yaw, however a stronger second gust occurred, increasing the pressure on the rudder and pushing the aircraft further into a left yaw.
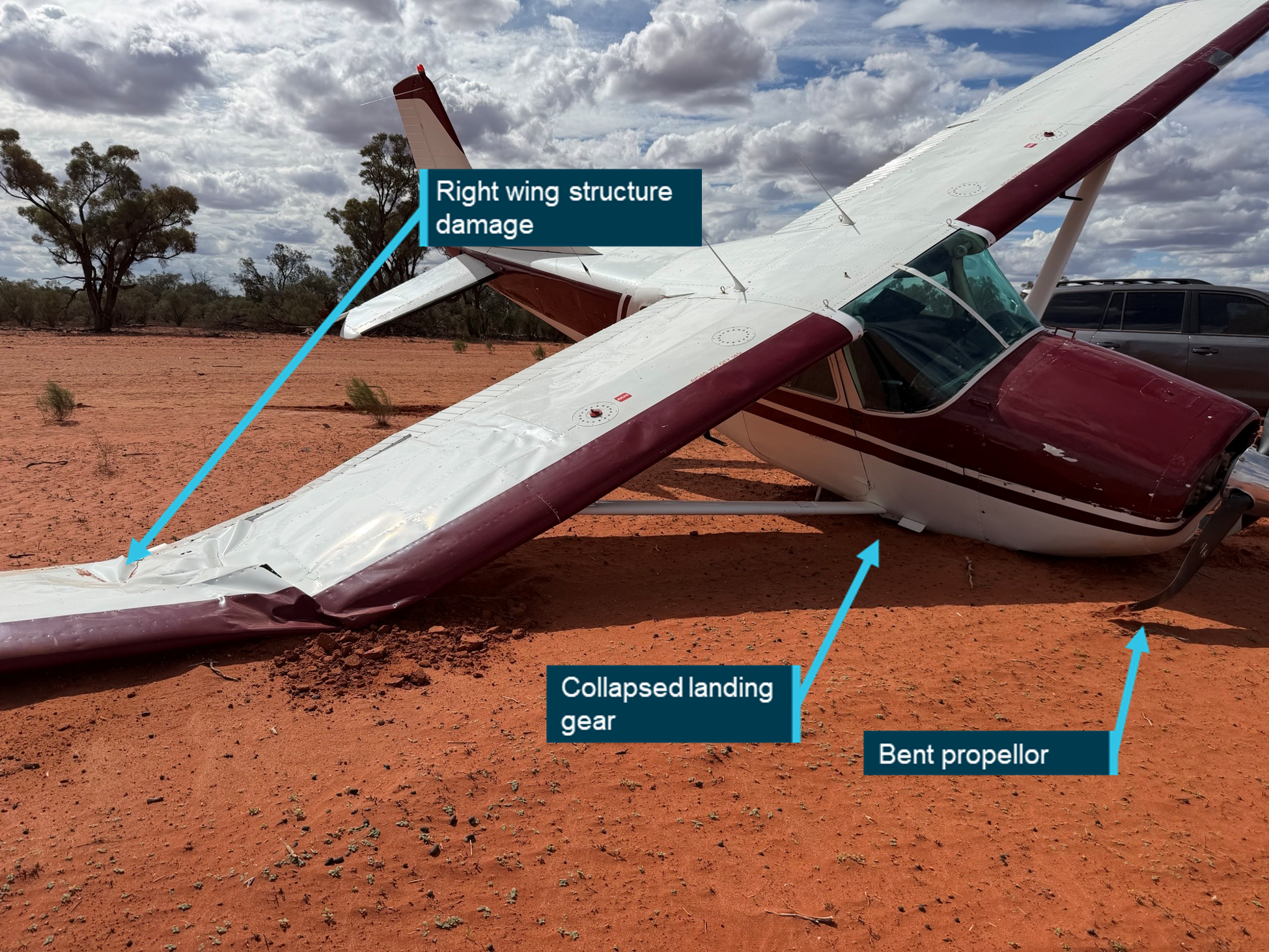
With full brakes applied and rudder authority reduced, the aircraft’s left main wheel sank into soft ground at the runway edge and the aircraft ground looped[1] to the left. The right landing gear collapsed and the right wing and propeller impacted the ground resulting in substantial damage to the wing, landing gear and propeller.
Figure 1: Aircraft wreckage
Source: Airstrip owner, annotated by the ATSB
Safety message
Pilots must ensure that the weather conditions surrounding the selected landing area are continuously assessed visually throughout the approach phase of flight. Should there be any unfavourable weather conditions that may impact the aircraft’s stability and controllability, conducting a go-around will allow time to plan for how to manage the landing conditions.
The ATSB also reminds all pilots of the importance of planning, and evaluating the local weather conditions, prior to departure. A comprehensive assessment of the weather conditions at the intended point of landing is encouraged.
About this report
Decisions regarding whether to conduct an investigation, and the scope of an investigation, are based on many factors, including the level of safety benefit likely to be obtained from an investigation. For this occurrence, no investigation has been conducted and the ATSB did not verify the accuracy of the information. A brief description has been written using information supplied in the notification and any follow-up information in order to produce a short summary report, and allow for greater industry awareness of potential safety issues and possible safety actions.
[1]A term used to describe a loss of directional control where the aircraft rotates around the yaw axis.
Video and audio from separate CCTV cameras will be analysed as part of the evidence gathered during the ATSB’s ongoing investigation of a light aircraft accident near Heck Field in South East Queensland.
Both the pilot and passenger were fatally injured when the amateur-built Van’sRV-8Acollided with terrain soon after take-off in the early morning of 27 January 2026, a preliminary report details.
The preliminary report notes that earlier on the morning of the accident, the pilot lodged a plan for a private flight to Barraba, in Northern NSW.
“CCTV from the airfield showed the aircraft accelerating for take-off on runway 28,” ATSB Chief Commissioner Angus Mitchell said.
“After lifting off, it can be seen initially flying just above the runway, before sinking briefly and then climbing with wings level.”
As the aircraft travelled beyond the end of the runway, it stopped climbing and began to descend, before its right wing dropped, and it impacted the ground.
“The aircraft wreckage was found in line with the runway, 360 m beyond its end, inverted and facing in the opposite direction to the flight path,” Mr Mitchell explained.
“An immediate, fuel‑fed, post‑impact fire had destroyed the aircraft, limiting the extent to which it could be examined, but all major components were accounted for at the site.”
Damage to the propeller blades indicated the engine was operating at impact, and an examination of the engine – which was extensively damaged by the fire – found no obvious sign of malfunction.
The preliminary report notes the aircraft’s engine was a 4‑cylinder, horizontally opposed Subaru EJ25 engine modified for aircraft use.
An earwitness at Heck Field during the accident flight reported their attention being drawn to what they described as abnormal engine noises developing during the aircraft’s take‑off run.
“Airfield CCTV did not have audio, but the ATSB has been provided footage from another nearby camera which caught audio of the accident flight off camera,” Mr Mitchell said.
“The engine could be heard for around 40 seconds of that audio and indicated engine RPM fluctuating periodically for that time.”
Mr Mitchell noted the preliminary report outlines evidence gathered to date during the investigation, but does not contain analysis or findings, which will be outlined in a final report to be released at the conclusion of the investigation.
“Further video and audio analysis will be conducted as the investigation progresses,” he said.
“Investigators will also review aircraft maintenance and pilot documentation, other recorded data, and the post‑mortem information and survivability factors.”
This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003.
Summary video
The occurrence
On 19 March 2026, a Cessna 441 Conquest aircraft, registered VH-LBZ and operated by Skippers Aviation, was being utilised for a non-scheduled passenger air transport flight from Broome Airport to Mungalalu‑Truscott aerodrome, Western Australia. The flight was being operated by 2 pilots – a pilot in command under supervision1 (pilot flying), seated in the left seat and a training captain in the right seat. There were 5 passengers on board.
The aircraft had a permissible unserviceability, under the minimum equipment list (MEL)2 applied for the right engine fuel control computer. The MEL deferred defect log stipulated that both engines be operated in manual mode for take-off, using a specific procedure. The training captain, in consultation with the pilot flying, requested that they be assigned VH‑LBZ for training purposes, to cover the manual mode procedure. In preparation, the pilot flying reviewed the manual mode procedure both the night before and on the morning of the flight. This was in addition to having talked through and observed the training captain perform the procedure about 2 weeks prior.
The pilot flying arrived at the airport at about 0900 local time, about 40 minutes prior to the scheduled sign-on time, to prepare for the flight and to participate in a briefing with the training captain. The briefing was reported to be normal except that it included the procedure to operate the aircraft’s engines in manual mode, with the pilots referencing the flight manual.
The flight was scheduled to depart at 1030. Both pilots prepared the aircraft for departure and at about 1035 all 5 passengers had checked in and were escorted to the aircraft. The passengers received a safety briefing from the training captain at the aircraft.
The aircraft start was as per the manual mode procedure and, at 1058, Broome tower air traffic control (ATC) provided a clearance and the aircraft taxi was commenced. During the taxi to the runway holding point, the pilots completed their take-off brief, where they again discussed differences related to operating in manual mode. This included an earlier decision speed3 of 105 kt, setting an engine torque limit of 1,500 ft-lbs per side and that manual fuel enrichment using the START buttons may be required during the take‑off roll.
At about 1115, after waiting for traffic, VH-LBZ was cleared for take-off. The aircraft was lined up on runway 10 and the pilot flying moved the power levers up for a normal take‑off. The pilot flying noted that the engine torque increased to about 650 ft-lbs per side, below the target of 1,500 ft-lbs. In response, the pilot flying pressed the START buttons as per the procedure, alternating between left and right to enrich with fuel, reaching 1,450 ft-lbs engine torque before rotation.4
After take-off, both pilots recalled that, just after they had completed the after-take-off checks and at about 500 ft above mean sea level, with the autopilot engaged, the pilot flying verbalised their intention to enrich again as the torque was at 1,450 ft-lbs, and they wanted to increase it to 1,500 ft‑lbs. The pilot flying pressed what they believed to be the left and right START buttons (without looking at the panel).
At about 1117, immediately following the enrichment, the pilot flying recalled a change in engine sound, feeling the aircraft yaw slightly and an absence of thrust. The training captain also reported an immediate sound change and seeing the engine torque reduce asked the pilot flying if they had pressed the STOP buttons. The pilot flying was unsure, however, immediately lowered the nose to maintain airspeed.
The training captain called for an ‘air start’ and instructed the pilot flying to press the START buttons again. The training captain pulled the power levers back to where they believed the air start zone was, however, with limited time available to restart the engines, they decided to conduct a forced landing. At 1117:12, a MAYDAY5 call was made, and the pilot flying handed over control to the training captain. Broome tower ATC activated the crash alarm at 1117:18.
The decision was made by the training captain to land in the mangroves, relatively straight ahead of the aircraft track. The landing gear was extended as instructed by the training captain, and the pilot flying called for the flaps down, which the training captain actioned. The passengers were instructed to brace for impact.
The training captain conducted a controlled descent and moved the condition levers to shut-off just before the aircraft impacted terrain at 1117:54, at a ground speed of 76 kt (141 km/h) (Figure 1). As a result of the impact, one passenger was seriously injured and the 2 pilots and 4 passengers received minor injuries. The aircraft was substantially damaged.
Figure 1: Flight track and location of accident site
Source: ATSB
The aircraft emergency locator transmitter activated on impact and the training captain attempted to contact Broome tower ATC via radio, however, was unsure if the radio was working, as they did not receive a response.
Broome tower ATC attempted to contact the aircraft operator to confirm the number of people on board, and if there were any dangerous goods, but was unable to do so. This information was instead obtained through contact with the training captain on their mobile phone.
The occupants commenced exiting the aircraft and the training captain was the last to egress, taking the fire extinguisher. The pilot flying applied first aid to the seriously injured passenger.
A search and rescue helicopter was dispatched at about 1141, arriving on site at 1210. Western Australia police arrived at about 1213. The seriously injured passenger was airlifted from the accident site and transported to hospital by ambulance. The flight crew and remaining passengers were assisted by police and the Department of Fire and Emergency Services to walk from the accident site and were met by ambulances.
Context
Personnel information
Pilot in command under supervision
The pilot in command under supervision held a Commercial Pilot Licence (Aeroplane), issued in 2018 and with class ratings for multi- and single-engine aeroplanes. They had accumulated 1,256.8 total flight hours, with 56.6 hours on the Cessna 441 aircraft type. The pilot held a current instrument rating, with their last proficiency check completed in January 2026, and a current class 1 aviation medical certificate (valid until April 2026) with no conditions. The pilot reported being well rested and fit to fly.
Training captain
The training captain held a Commercial Pilot Licence (Aeroplane) issued in 2022 and with class ratings for multi- and single-engine aeroplanes. They had accumulated 1,764.7 total flight hours, with 1,080.9 hours on the Cessna aircraft 441 type. They held a current instrument flight rating, with their last proficiency check completed in November 2025, and a current class 1 aviation medical certificate (valid until November 2026) with no conditions. The training captain reported being well rested and fit to fly.
In addition to their position as training captain, they also held the roles of Broome senior base pilot and the Cessna 441 fleet manager for the operator.
Aircraft information
General
The Cessna 441 Conquest is a pressurised, low‑wing aircraft, with seating for up to 2 pilots and 10 passengers. However, the Skippers Aviation operations manual limited the number of passengers that could be carried to 9.
VH-LBZ was powered by 2 Honeywell International Inc TPE331-10N-531S turboprop engines, fitted with Hartzell HC-B3TN-5 propellers. Both pilot seats were equipped with flight controls, however, single‑pilot line operations were flown from the left seat. The right pilot seat would normally only be occupied by a second pilot for training and checking, although for this flight the operator’s client had stipulated via policy that 2 crew would be carried.
The accident aircraft, serial number 4410038, was manufactured in the United States by the Cessna Aircraft Company in 1978 and registered in Australia as VH-LBZ in July 1984. At the time of take-off, the aircraft had a total time-in-service of 29,267.9 flight hours. The aircraft was operating under a Civil Aviation Safety Authority supplemental type certificate that, with specific maintenance requirements, permitted operators to continue operating the Cessna 441 past its service life of 22,500 flight hours to 40,000 flight hours.
Aircraft maintenance
The aircraft was maintained in accordance with the Skippers Aviation Cessna 441 maintenance program, which incorporated the requirements of the life extension program, permitted by the supplemental type certificate.
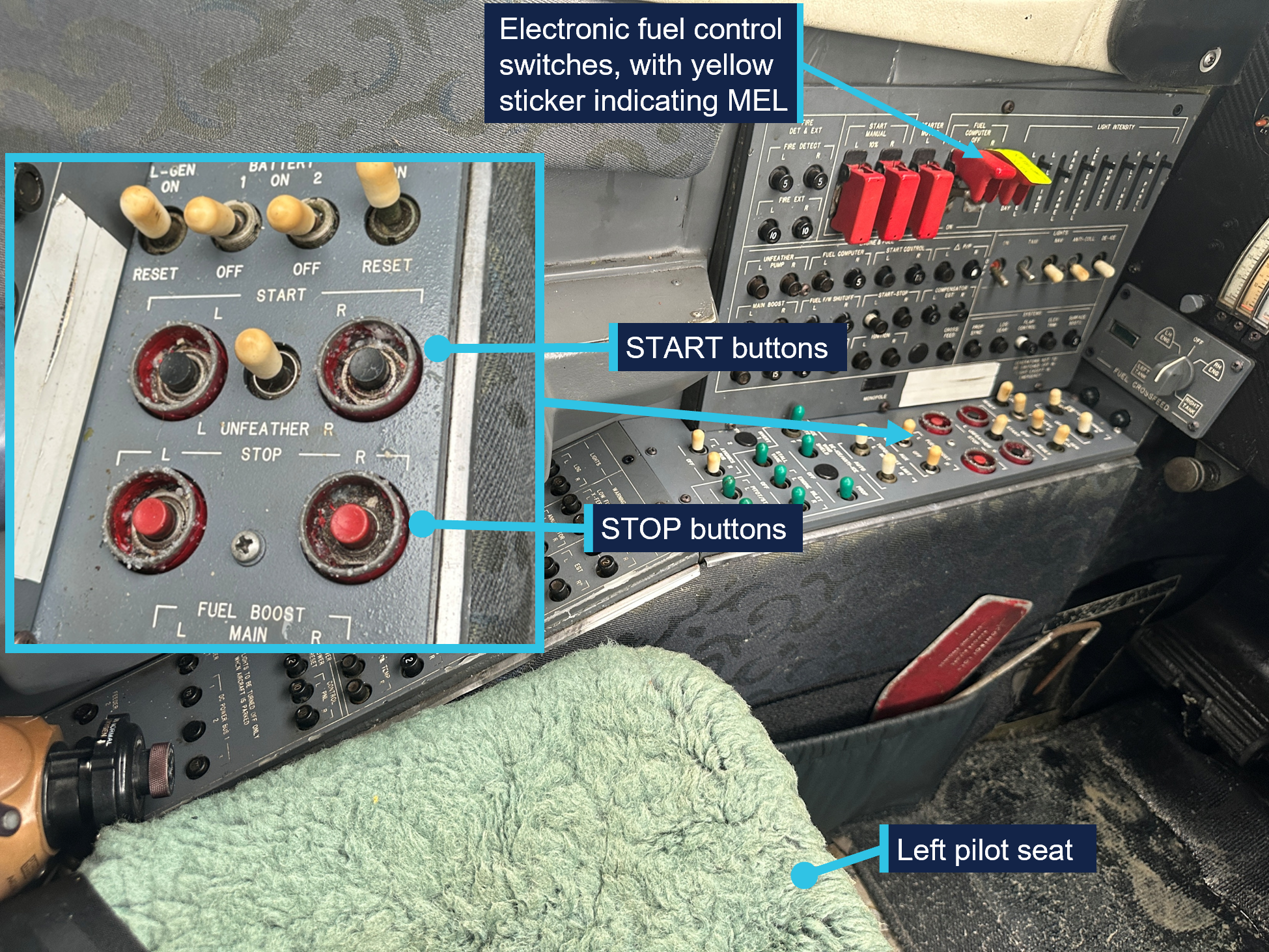
The aircraft had a deferred defect log6 entry dated 16 March 2026, which showed that the right engine fuel control computer was unserviceable. A yellow sticker was affixed to the right fuel control computer switch located on the left vertical panel inside the aircraft to identify the unserviceability (see START and STOP buttons). This was a permissible unserviceability in accordance with the aircraft’s MEL. As this was a category C defect,7 the aircraft was permitted to operate for a maximum of 10 days, with one or both fuel computers unserviceable, provided certain limitations were adhered to. Those limitations were:
manual mode (see Engine fuel control system) procedures in the airplane flight manual were followed
manual mode performance charts in the airplane flight manual were used
propeller reversing was not to be used for the engine operating in manual mode
propeller synchrophasing8 was inoperative.
The airplane flight manual procedures recommended that, where one fuel computer was inoperative, both engines were to be in manual mode for take-off. The operator’s deferred defect log included the MEL requirements and added that both engines were to be in manual mode for take-off and landing. Further, the operator required that the abovementioned specific MEL requirements be covered in line training for take-off and landing.
Engine fuel control system
Normal mode operation
Each engine was equipped with an electronic fuel control system (normal mode operation), which included an electronic fuel computer for regulating fuel flow and engine speed. The system automatic functions included:
automatic engine starting
fuel enrichment and optimum fuel scheduling
calculating a single red line exhaust gas temperature to assist the pilot with managing engine power
limiting engine torque and temperatures to prevent exceedance
the engine revolutions per minute (RPM) automatically changed with the condition lever selection9
electronic underspeed governing of the propeller.10
Manual mode operation
The electronic fuel control system was also fitted with a manual backup system (manual mode operation), which was to be used when the electronic fuel computer became inoperative for any reason. When operating in manual mode, among other reductions in certain system functions:
fuel enrichment required for take-off and engine acceleration was achieved by pressing the engine START button
the engine starting functions were to be performed manually by the pilot
the condition lever did not control the engine speed
the propeller synchroniser was inoperative
engine torque and temperature were to be monitored and manually adjusted by the pilot to prevent engine damage as the limiting functioning was inoperative
engine response to power lever advances was slower
aircraft performance was changed
propeller reversing was not permitted.
START and STOP buttons
The aircraft was fitted with START (black) and STOP (red) buttons for the left (L) and right (R) engines. Slightly recessed, the buttons were located in proximity on a horizontal switches panel to left of the left pilot seat (Figure 2). The START button was pressed momentarily to initiate the start sequence, in normal and manual modes.
When the STOP buttons were pressed, this activated the electrical fuel shutoff valve initiating an immediate cessation of fuel flow. When using the STOP buttons for a normal shutdown, the airplane flight manual advised that the buttons were to be pressed and held for 5 seconds to allow for any remaining fuel in the system to be purged.
Figure 2: Location of START and STOP buttons and electronic fuel control switches
Source: ATSB
Use of the START button for fuel enrichment
The fuel enrichment valve, part of the fuel control assembly,11 permitted fuel enrichment during engine start, primarily to accelerate the engine smoothly to operating speed. The electronic fuel computer controlled the fuel enrichment for acceleration while simultaneously ensuring that the exhaust gas temperature remained within limits. In manual mode, the pilot provided fuel enrichment by pressing and holding the START button, after fuel flow had been established. The procedure for manual mode starting included the START button could be pushed ‘as required for fuel enrichments to assist engine acceleration to 85% RPM’. The pilot must monitor exhaust gas temperature to remain within limitations.
The airplane flight manual further stated that the START button could be used as required to aid engine acceleration to 100% RPM during the take-off roll, however, did not mention the use of the START button for enrichment during any other phases of flight.
Meteorological information
The aerodrome forecast for Broome Airport, valid from 1000 on 19 March 2026, indicated the wind was 100° at 14 kt, and CAVOK12 conditions. The forecast temperature was 34°C.
Wreckage and impact information
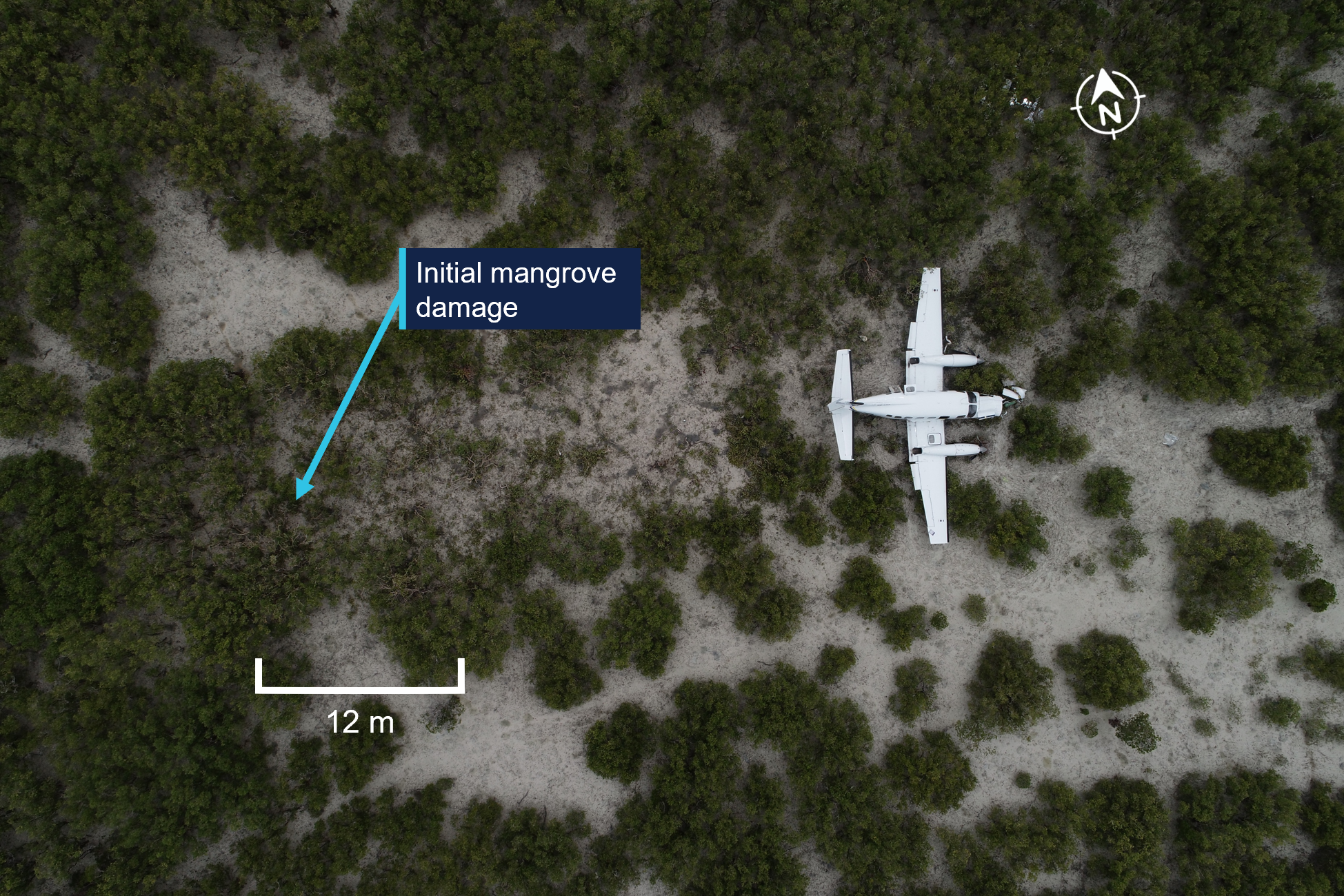
The forced landing area was in mangrove swampland about 3.6 km east of Broome Airport, in-line with the aircraft’s approximate take-off track. The flight path angle was about 9° nose down and the distance between the initial contact with mangrove trees and the wreckage was about 30 m (Figure 3).
Figure 3: Overhead view of aircraft accident site
Source: ATSB
The ATSB’s onsite examination identified that:
The aircraft was relatively intact with the landing gear down and the flaps partially extended. The aircraft rapidly decelerated once the landing gear had contacted the muddy terrain.
There was fuel in the left and right wing tanks and clean fuel in the left and right engine‑driven fuel pump filter bowls.
Examination of the left and right engine turbines viewed through the exit ducts did not show any observable damage.
Damage to the left and right propeller showed back bending and limited rotational abrasion damage, which indicated the engines were not driving the propellers at the time of the impact (Figure 4).
Figure 4: Aircraft wreckage showing propeller back bend
Source: ATSB
Recorded information
The ATSB recovered 3 Garmin electronic recording devices from the aircraft:
G600 TXi flight display
GI 275 attitude indicator
GTN 650Xi GPS, navigation, communications and multifunction display.
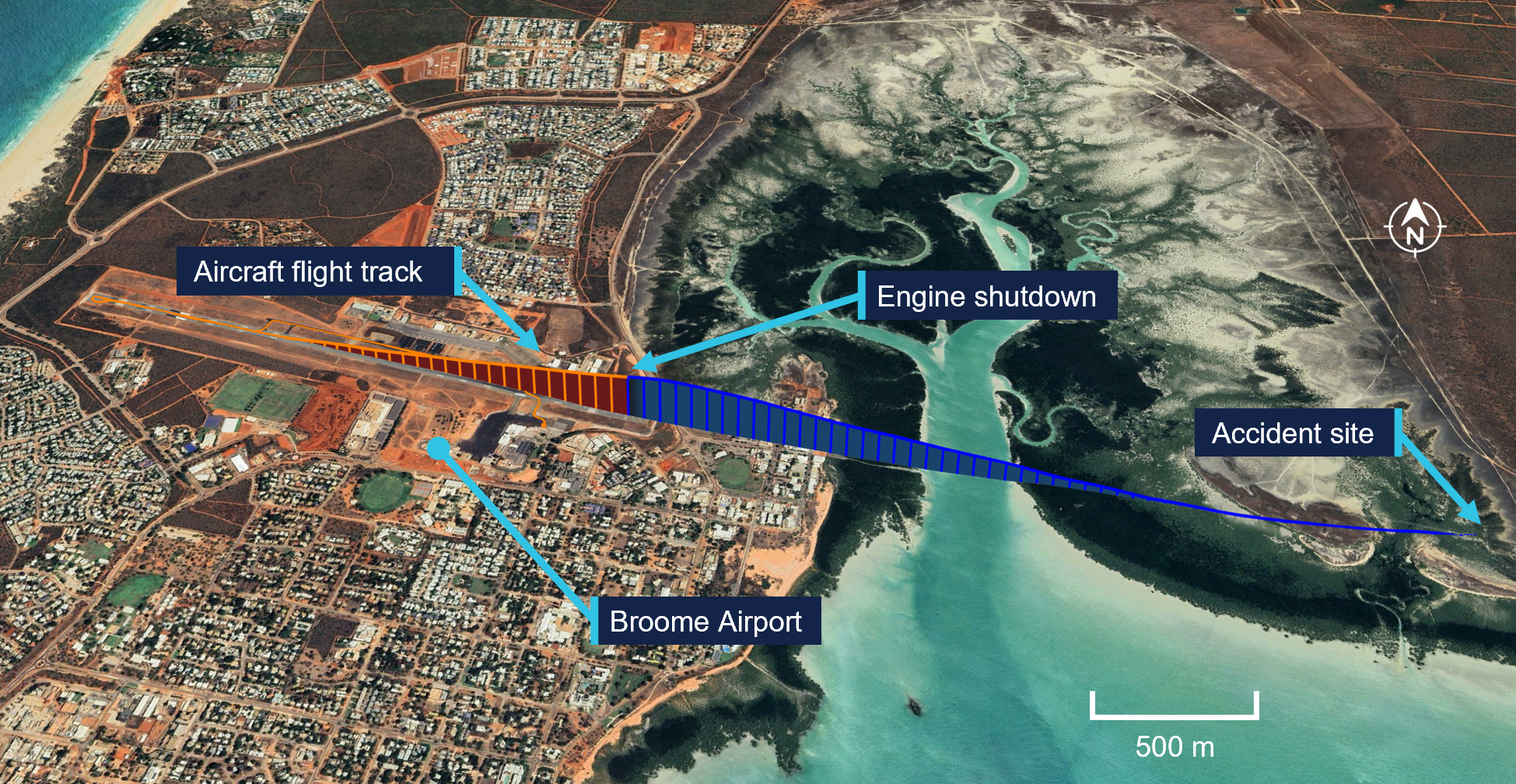
While there were no parameters on the devices recovered that directly pertained to the engines, the GI 275 recorded the system voltage (aircraft power). The data retrieved from this unit showed a drop in the system voltage beginning at 1116:59, from 27.7 volts direct current (VDC) to 26.8 VDC within 1 second, then slowly decreased to 24.5 VDC over the next 17 seconds. The base system voltage was nominally 24 VDC, however, would be about 28 VDC when the generators13 were on. Therefore, a drop in voltage was consistent with the generator speed reducing as the engines shut down. In addition, there was also a rapid decrease in longitudinal acceleration at the same time.
The data retrieved also indicated that, at 1116:59, the aircraft (Figure 5):
was at an altitude of 490 ft above mean sea level
had an indicated airspeed of 141 kt (261 km/h)
was climbing at 1,225 ft/min
had about 9° nose-up attitude and 4° left roll
was on a heading of about 107°.
At 1117:54, the impact occurred at an indicated airspeed of about 82 kt (152 km/h) and a ground speed of 76 kt (141 km/h) coming to a stop by 1117:58.
Figure 5: Location of aircraft engine shutdown
Orange section is with power available, blue section is following the engine shutdown.Source: ATSB
Survival aspects
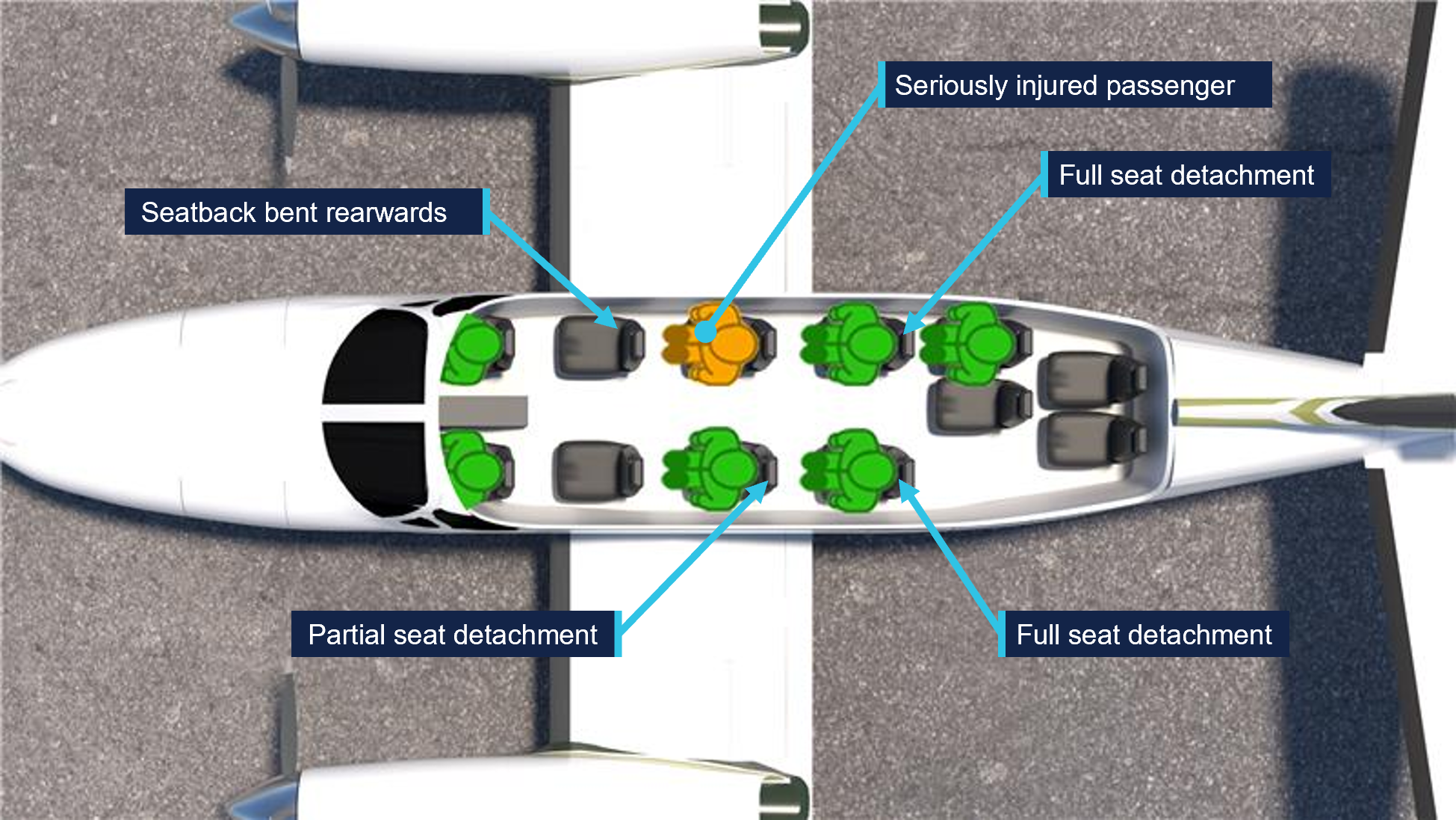
The liveable space within the aircraft cabin was maintained, and the exits were tested by the ATSB and found to function correctly. However, there was significant disruption to the cabin interior including displaced equipment, deployed oxygen masks and the complete detachment of 2 passenger seats from their seat tracks, with some of the floor structure lifting. An additional seat had partially detached and the seat behind the right pilot was significantly distorted, with a backward bend of almost 45° (Figure 6).
Figure 6: Aircraft cabin immediately after the accident
Source: Pilot of VH-LBZ
In addition, a passenger seated on the right side of the second row of passenger seats reported that their seatbelt failed during the impact, throwing them forward into the back of the seat ahead before coming to rest between the 2 pilots. This passenger received serious injuries. Figure 7 shows the location of the full and partially failed seats, and where the seriously injured passenger was seated. All other passengers and the pilots received minor injuries.
Figure 7: Location of seat failures and seriously injured passenger
Source: ATSB
Related occurrence
A previous ATSB investigation (200601053) involving a Cessna 441 Conquest, VH-LBA, 40 km north-west of Callion, Western Australia, on 27 February 2006, found that the pilot in command inadvertently shut down the left engine in-flight by pressing the STOP button. The investigation noted that:
…Prior to the event, the flight crew were discussing the use of the Start Button Guard Plate which was in place over the engine START buttons.In the course of explaining to the second pilot the use of the Start Button Guard Plate, the PIC inadvertently depressed the left engine STOP button...
Safety action
The Civil Aviation Safety Authority (CASA) issued a safety alert to Skippers Aviation Pty Ltd to prevent the use of Cessna 441 Conquest aircraft that have an MEL applied that requires the use of manual mode. The safety alert advised:
Skippers must not dispatch a flight where an MEL involving the use of manual mode is in force in any C441 Conquest operated by them until CASA has approved amendments to the Exposition and the Training and Checking manual that detail the use of manual mode and Skippers has conducted the appropriate training and checking of the flight crew assigned to the flight.
Skippers Aviation Pty Ltd advised that it has taken the following safety action, which addressed the safety alert issued by CASA and included additional actions:
Immediate grounding of the Cessna 441 Conquest fleet.
Issuance of a companywide ‘Memorandum to All Staff – The use of MEL 76-00-01 Fuel computers is Prohibited’.
Completion of a risk review of Cessna 441 Conquest operations which encompassed procedures, training, maintenance, workload, safety and staffing. The review determined that, while the operator considered all controls were compliant, multiple challenges existed and a decision was made to cease all Cessna 441 Conquest revenue operations permanently.
A cost benefit analysis was completed, and Broome operations were considered no longer feasible.
A review of companywide procedures and training is in progress, including all procedures related to the management of MELs.
Further investigation
To date, the ATSB has:
examined the wreckage and accident site
examined recorded data from the Garmin G600 TXi, GI 275 and GTN 650 devices
interviewed the pilots and passengers
collected radio communication, aircraft traffic surveillance data, and navigational application data
collected aircraft, pilot, crew and operator documentation.
The investigation is continuing and will include further review and examination of:
operational procedures and training
aircraft maintenance and MEL practices
crashworthiness and survivability aspects
aircraft design features (including the START/STOP buttons).
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
The ATSB would like to thank the Department of Biodiversity, Conservation and Attractions for its assistance in facilitating access to the aircraft accident site.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
About ATSB reports
ATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines.
Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner.
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence.
The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau.
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
^In-command under supervision allows a pilot to perform all duties and functions as a pilot in command under the supervision of a pilot in command appointed for that purpose.
^Minimum equipment list (MEL) is a list that provides for the operation of aircraft, subject to specified conditions, with particular equipment inoperative.
^An engine failure below the decision speed should result in a rejected take off; above this speed the take-off should be continued.
^Rotation: the positive, nose-up, movement of an aircraft about the lateral (pitch) axis immediately before becoming airborne.
^MAYDAY is an internationally recognised radio call announcing a distress condition where an aircraft or its occupants are being threatened by serious and/or imminent danger and the flight crew require immediate assistance.
^The deferred defect log identified the system affected, date and aircraft hours when logged, any limitations and deferral expiry date, a copy of which was in the flight log available to the pilots.
^Minimum equipment lists and repair categories are explained in Civil Aviation Advisory Publication (CAAP) 37-01 v5.1.
^Propeller synchronising and synchrophasing provide a means to match the RPM of both engines and establish a blade phase relationship between the left and right propellers to reduce vibration and cabin noise.
^The condition lever controlled engine speed (RPM) and fuel flow while the power lever adjusted the engine torque and propeller speed.
^The electronic underspeed governor is primarily to control fuel flow to maintain engine RPM during ground operations. It differs in operation to the propeller governor that directs oil to, or from, the propeller to maintain selected propeller/engine RPM.
^The fuel control assembly regulates fuel flow to the engine and contains a mechanical fuel shutoff valve and an electrical fuel shutoff valve.
^Ceiling and visibility okay (CAVOK): visibility, cloud and present weather are better than prescribed conditions. For an aerodrome weather report, those conditions are visibility 10 km or more, no significant cloud below 5,000 ft, no cumulonimbus cloud and no other significant weather.
^A combination starter-generator was mounted on each engine. The units operated as a starter during ground starts and were the aircraft’s primary power source.
Occurrence summary
Investigation number
AO-2026-068
Occurrence date
19/03/2026
Occurrence time and timezone
1117 Australian Western Standard Time
Location
3.6 km from Broome Airport
State
Western Australia
Report release date
02/06/2026
Report status
Preliminary
Anticipated completion
Q3 2026
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation phase
Evidence collection
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Collision with terrain, Forced/precautionary landing
Occurrence class
Accident
Highest injury level
Serious
Aircraft details
Manufacturer
Cessna Aircraft Company
Model
441 Conquest
Registration
VH-LBZ
Serial number
4410038
Aircraft operator
Skippers Aviation Pty Ltd
Sector
Turboprop
Operation type
Part 135 Air transport operations - smaller aeroplanes
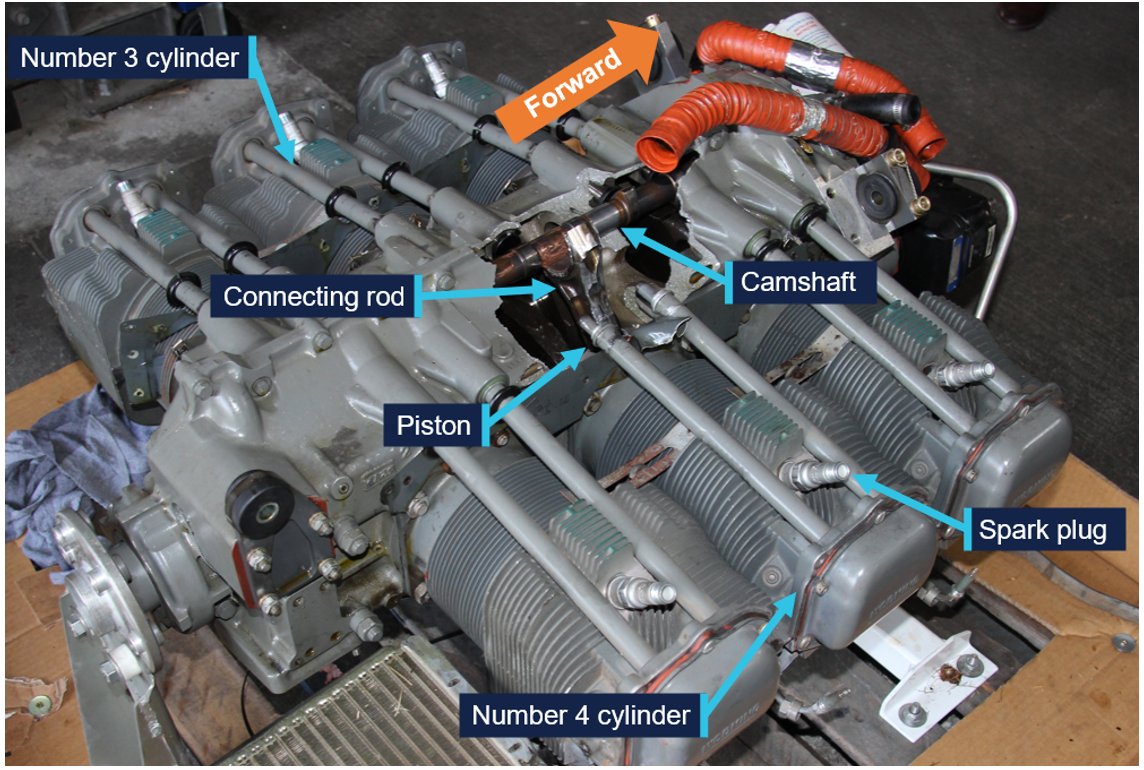
A Robinson R44 helicopter pilot’s timely actions in conducting a forced landing after a connecting rod separated from the crankshaft while in flight near Tindal in the Northern Territory ensured a safe outcome, an ATSB investigation report highlights.
The R44 sustained minor damage during the 11 June 2025 incident, after its pilot encountered severe airframe vibrations during a personal transport flight from Daly Waters to Wally’s Airstrip. Fortunately, both pilot and passenger were uninjured in the hard forced landing into an area of open farmland.
The ATSB’s investigation established that the engine’s number 4 connecting rod had separated from the crankshaft after the nuts connecting it loosened while the helicopter was in use.
While several scenarios for this in-service loosening were considered, including abnormal loading or vibration, variation in thread condition and lubrication, improper or defective parts, microscopic deformation, and inadequate installation torque, the specific cause could not be determined.
The investigation did find that during the most recent overhaul of the engine, the independent inspection of the relevant section did not involve a physical torque check of the connecting rod nuts – although there was no indication that this contributed to the engine failure.
“While such a check was not a regulatory requirement, this did represent a missed opportunity to positively verify the installation torque,” ATSB Director of Transport Safety Dr Stuart Godley said.
Separately, the engine examination identified the helicopter’s maintenance provider had not used new gaskets when refitting the spark plugs, as required by the engine and spark plug manufacturer.
“While not found to have contributed to this incident, this observation led to the discovery of an inconsistency in Civil Aviation Safety Authority guidance,” Dr Godley said.
CASA’s airworthiness bulletin for spark plug care, AWB 20-001, stated annealed gaskets could be used during spark plug fitment, while an airworthiness bulletin specific to piston engine spark plug insulator cracking, AWB 85-023, stated new gaskets must be used in all circumstances.
“This inconsistency could have led to incorrect procedures being performed which were not in accordance with spark plug maintenance requirements,” Dr Godley said.
CASA has advised that AWB 20-001 will be cancelled, and AWB 85-023 will be amended to reflect current recommendations.
In addition, the helicopter maintainer advised new spark plug gaskets are now fitted each time spark plugs are reinstalled.
Dr Godley said the successful outcome after the unexpected engine failure event highlighted the importance of managing inflight anomalies through a comprehensive understanding of systems, and the correct application of emergency procedures.
“The pilot’s timely actions following the onset of the vibrations ensured a safe outcome,” he said.
“The incident also emphasises the importance of independent inspection of completed work to provide additional assurance that manufacturer requirements have been adhered to when installing aircraft components.”
Friction locks fitted on the Beechcraft King Air series aircraft require careful adjustment to prevent the power levers migrating rearwards to the idle position, particularly during take-off.
What happened
On the night of 19 August 2021, the pilot and medical crew of a Hawker Beechcraft King Air B200C aircraft, registered VH‑VAH, departed Essendon Fields Airport, Victoria on a patient retrieval flight. During the take-off, there was a loss of left engine power and an uncommanded left yaw. The pilot initially managed the situation as an engine power loss situation. However, shortly after, they identified that the left engine power lever had migrated rearwards to the idle position. The pilot moved the power lever back to take-off power and adjusted the friction lock to prevent further movement. The flight continued without further incident.
Power levers and friction locks
(Source: Operator, modified by the ATSB)
Why did it happen
The left engine power lever had migrated rearwards as the friction lock had not been sufficiently adjusted during pre-flight checks.
The cockpit to engine nacelle power lever control cables in King Air series aircraft were spring loaded towards idle. This was to protect the engines in the event of any power lever cable issues, and to reduce the effect of hysteresis (or backlash) in the system. The effect of the springs migrating the power levers was managed by adjusting the friction locks. The left engine was more susceptible to power lever migration as its cable connecting it to the engine was shorter when compared with the right engine.
When correctly set, the friction locks provided adequate resistance for the power levers to remain in position. However, if not adequately set, power lever migration could occur. This was typically experienced when the pilot removed their hand from the levers during take-off and could lead to the aircraft yawing towards the engine experiencing the power lever migration, a significant reduction in power, and the auto‑feather system disarming.
A characteristic of the King Air friction locks was that they required careful adjustment as some aircraft had a narrow range between no friction and too much friction. In addition, the desired resistance could be inconsistent between power levers in the same aircraft and other aircraft, and this could change over time due to wear. This characteristic has been experienced among different King Air operators and pilots and has also been considered as a potential factor in several fatal accidents.
Safety advisory notice
AO-2021-034-SAN-01:
The Australian Transport Safety Bureau advises pilots and operators of the King Air series aircraft (c90, 200, and 300) that the power lever friction locks require careful adjustment to prevent power lever migration towards the idle position, particularly during take-off. Inadvertent migration of one power lever towards idle can result in power reduction and yaw that, when occurring at low height, can result in catastrophic outcomes. Operators should ensure pre-flight checks provide opportunities to confirm friction lock settings before the take-off run, and ensure pilots have adequate knowledge of friction lock sensitivity to help prevent and recover from inadvertent power lever migration.
Expectation bias and a lack of effective risk controls contributed to a passenger train travelling through a turnout near Blacktown Station at four times faster than the posted speed limit, a transport safety investigation report details.
On 21 April 2024, the driver of a Sydney Trains Waratah passenger train was thrown from their driving position when the train travelled at 101 km/h through a turnout with a posted speed limit of 25 km/h.
Fortunately, the train did not derail, no passenger injuries were reported, and the driver was able to safely stop the train at Blacktown Station.
The serious incident was investigated by the Office of Transport Safety Investigations (OTSI), which investigates rail occurrences in NSW under a collaboration agreement with the ATSB.
The investigation found the driver, who had been based at Blacktown Depot for around seven years, did not react to and slow the train in response to signals ahead of the turnout.
“The driver was familiar with taking a different route and did not expect to go through a turnout,” OTSI Chief Investigator Jim Modrouvanos said.
“This turnout was among several identified four years earlier by Transport for NSW as representing a ‘not tolerable’ risk of overspeed and derailment,” he said.
A project to incorporate Automatic Train Protection (ATP) technology at these locations was downgraded in scope, the investigation found.
Sydney Trains therefore did not have effective controls for overspeed where high risk turnouts had been identified.
After the incident, Sydney Trains lowered speed limits at high-risk turnout locations, including at this turnout, and developed a plan to implement ATP at these locations.
Sydney Trains also developed a response procedure for this type of overspeed incident, after it was identified that the train was not stopped for inspection after the occurrence.
“Overspeed carries a high risk of train rollover and the potential for multiple fatalities,” Mr Modrouvanos said.
“So, the overspeed risk controls should be reviewed regularly to make sure they are still effective, and to see if there are any practical ways to further reduce or eliminate risk.
“Near-miss events like this one present an opportunity to revisit safety controls and make safety changes to further protect the travelling public.”
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into the accident involving a Cessna 441 Conquest twin turboprop aircraft near Broome Airport, in northern WA.
As reported to the ATSB, shortly after the aircraft took off from Broome’s runway 10 it encountered a loss of engine power.
The ATSB is deploying a team of transport safety investigators, specialising in aircraft operations and engineering, and accident survivability, to the accident site from its Perth, Canberra, and Brisbane offices.
Once on site on Friday the investigation team will conduct a range of evidence-gathering activities, including aircraft examination and site mapping, and will recover any aircraft flight recorders or other components of interest for further examination at the ATSB’s technical facilities in Canberra.
Investigators will also interview flight crew, passengers, and any witnesses, and collect relevant recorded information including flight tracking data and CCTV footage, as well as pilot and aircraft maintenance records, and weather information.
The ATSB asks anyone with video footage of the accident flight, or its immediate aftermath, to contact us via the witness form on our website: atsb.gov.au/witness at your earliest opportunity.
The pilot of a Piper PA-28 that flew into the path of two F-35 fighter jets while approaching to land at RAAF Base Tindal, in the Northern Territory, was unable to communicate with air traffic control due to a loss of electrical power, and entered controlled airspace without a clearance.
An ATSB final report into the 28 August 2025 occurrence details that the single-engined Piper, with a pilot and passenger on board, was participating in the Outback Air Race.
Earlier on the day of the incident, when preparing the aircraft for the Daly Waters to Tindal race leg, the pilot detected a tripped circuit breaker.
The pilot requested assistance from a licensed aircraft maintenance engineer (LAME) who found the alternator was unserviceable – meaning the battery could not be charged by the engine. The LAME advised they could not fix it at Daly Waters, but further maintenance could be provided at Tindal.
“The LAME subsequently charged the aircraft’s battery and encouraged the pilot to conduct the flight, without assessing the time the battery could supply the aircraft with electrical power,” ATSB Chief Commissioner Angus Mitchell said.
“Further, despite the heightened potential for a loss of electrical power, the pilot did not conduct contingency planning prior to taking off for Tindal,” Mr Mitchell added.
En route to Tindal, the aircraft lost electrical power and the pilot was unable to communicate using the aircraft’s radio. In addition, the aircraft’s transponder ceased transmitting, and could no longer be detected by air traffic control.
The pilot and passenger also reported being unable to call air traffic control on a mobile phone, due to noise levels in the cockpit, however they were in communication with members of an air race group chat using a mobile device.
The report details communications on the group chat, and how other members made contact with Tindal air traffic control, which advised it was unsafe for the PA-28 to land at Tindal due to the level of traffic, and that the PA-28 should hold outside controlled airspace or land at the nearby Homebush Park airfield.
However, the PA-28 occupants responded in the group chat that they were not landing at Homebush Park and instead were tracking direct to Tindal.
In a subsequent exchange on the group chat, a different member of the chat asked if the PA-28 occupants wanted them to declare a PAN, to which the PA-28 responded that they did. The PA‑28 pilot later advised that as they considered that a PAN had been declared on their behalf, they thought that other traffic would be cleared from their planned flight path.
However, none of the Tindal air traffic controllers recalled a PAN being declared on behalf of the PA-28.
“The investigation found that the pilot did not divert to the closest airport or follow advice to remain outside controlled airspace, and instead the aircraft was climbed into controlled airspace without the required clearance, and continued to land at Tindal,” Mr Mitchell said.
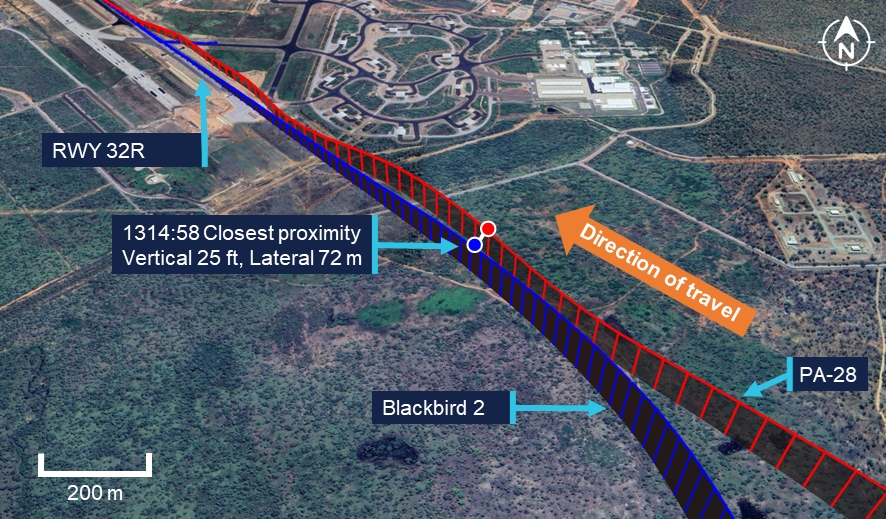
As the PA-28 was approaching Tindal, two RAAF F-35 jets were returning to Tindal in formation, with their pilots unaware of the PA-28.
“When the second F-35 turned onto final approach, the PA-28 also joined final in close proximity, with separation between the 2 aircraft reducing to 72 m laterally and 25 ft – about 7.6 metres – vertically.”
The PA-28 pilot then manoeuvred their aircraft to the right to increase separation, while continuing towards the runway. Both aircraft landed without further incident.
“This incident serves to highlight the importance of pilots conduct contingency planning prior to flight if there is an increased risk of an abnormal event and, in the case of such an event, to follow published emergency procedures to ensure their actions align with air traffic control expectations,” Mr Mitchell said.
The investigation report also stresses the importance of clear communication between maintenance personnel and pilots – and noted the LAME had not recorded the alternator issue or maintenance activity on the aircraft’s maintenance release.
“Recording of defects and subsequent maintenance actions on the maintenance release is central to ensure all parties share a common understanding of identified faults, the possible or anticipated in-flight effects, and their impact on the overall airworthiness of the aircraft,” Mr Mitchell said.