Safety summary
What happened
During the night of 25 March 2021, the pilot of a Leonardo Helicopters (formerly Finmeccanica) AW139 helicopter, registered VH-TJH, was performing aerial work near Katoomba, New South Wales, approximately 80 km west-north-west of Sydney. The task, conducted with the aid of night vision goggles (NVG), involved finding an injured bushwalker and winching in a paramedic and doctor.
While established in the hover at about 85 ft and facing cliffs near the Three Sisters, the aircrew officer started winching the paramedic down. The aircraft then stared drifting to the right towards rising terrain. The drift continued and a bank angle warning sounded as the aircraft rolled about 30° to the right. As the pilot corrected the drift the nose of the aircraft pitched up to about 51°. During the recovery manoeuvre an engine over torque occurred. After control of the aircraft was regained, the paramedic was retrieved, and the aircraft returned to Bankstown. None of the crew sustained injuries during the occurrence and a subsequent engineering inspection did not reveal any fault or damage to the aircraft.
What the ATSB found
The ATSB found that the external white lighting on the aircraft provided insufficient illumination for the pilot to maintain adequate visual references. It was also found that the lighting requirements specified by regulations provided no guidance or minimum requirements regarding the specifications or power output of the external white lights.
The ATSB also found that the operator provided insufficient guidance for the in-flight risk assessment specific to night vision imaging system (NVIS) winch operations. This led to the crew not evaluating or discussing components of the winch site that may have identified elements that made this winch site highly challenging.
It was also found that the operator’s currency requirements for NVIS winch operations did not provide the currency necessary to maintain competency in complex NVIS winch scenarios. The lack of recency in complex NVIS winch environments likely contributed to the pilot experiencing a high workload during the hover phase. This, in combination with the lack of visual cues probably led to the pilot becoming spatially disorientated and temporarily losing control of the aircraft.
It was also found that, despite being requested by the ATSB, the audio recording from the solid‑state multi-purpose flight recorder was not quarantined by the operator. This reduced the information available to the investigation team.
What has been done as a result
The operator advised the ATSB that they have updated their entire fleet with high powered Trakka searchlights, thus ensuring adequate lighting is available to illuminate the terrain at the required operating height during NVIS winching. Additionally, the operator has updated their NVIS winching recency requirements, with the addition of six-monthly recency requirement for NVIS winching in complex terrain, one of which is supervised by a Training and Checking pilot.
Furthermore, the operator has made significant changes to their winching procedures. The changes include additional guidance regarding risk management, pre-mission and pre‑winch risk assessment, as well as specific guidance to confirm and maintain adequate visual references during winch operations.
The Civil Aviation Safety Authority (CASA) have also advised that they will review the NVIS recency requirements. Consideration will be given to aligning with instrument flight recency (3 iterations in 90 days) and look at operational recency for winching and overwater SAR which will most likely require 3 iterations in 90 days. CASA have also made substantive changes to version 1.2 of the NVIS Multi-Part AC 91-13. These changes include guidance on the type of searchlight fitted and quantitative guidance regarding their capabilities.
Safety message
Inflight decision making, particularly involving pilots flying with reduced visual reference remains an ongoing safety concern. While flying visually at night it is crucial that pilots have sufficient visual reference to see and avoid obstacles. Visual cues are also required to maintain orientation so pilots know which way is up and can maintain control of their aircraft.
NVG provide a useful tool to supplement visibility for flying in low light conditions, however it is important to understand their limitations. Pressing on into conditions of reduced visual reference carries a significant risk of severe spatial disorientation due to powerful and misleading orientation sensations with reduced visual cues. Disorientation can affect any pilot, no matter what their level of experience.
Operators are reminded that regulations only set out the minimum requirements. As such, they are encouraged to assess the risks of their operations and modify their procedures, manuals, and risk assessments accordingly. Operators are also reminded that it is a requirement under the Transport Safety Investigation Act 2003 to quarantine evidence, including flight data recorders and cockpit voice recorders, when requested by the ATSB. Flight data and audio recorded during an occurrence can often be some of the most useful and compelling evidence in an investigation and can assist in finding safety factors and ultimately benefitting safety.
The occurrence
On 25 March 2021 the crew of a Leonardo Helicopters (formerly Finmeccanica S.p.A) AW139 helicopter, registered VH-TJH (TJH) were performing aerial work near Katoomba, New South Wales (NSW), approximately 80 km west-north-west of Sydney (Figure 1).
Figure 1: Occurrence location
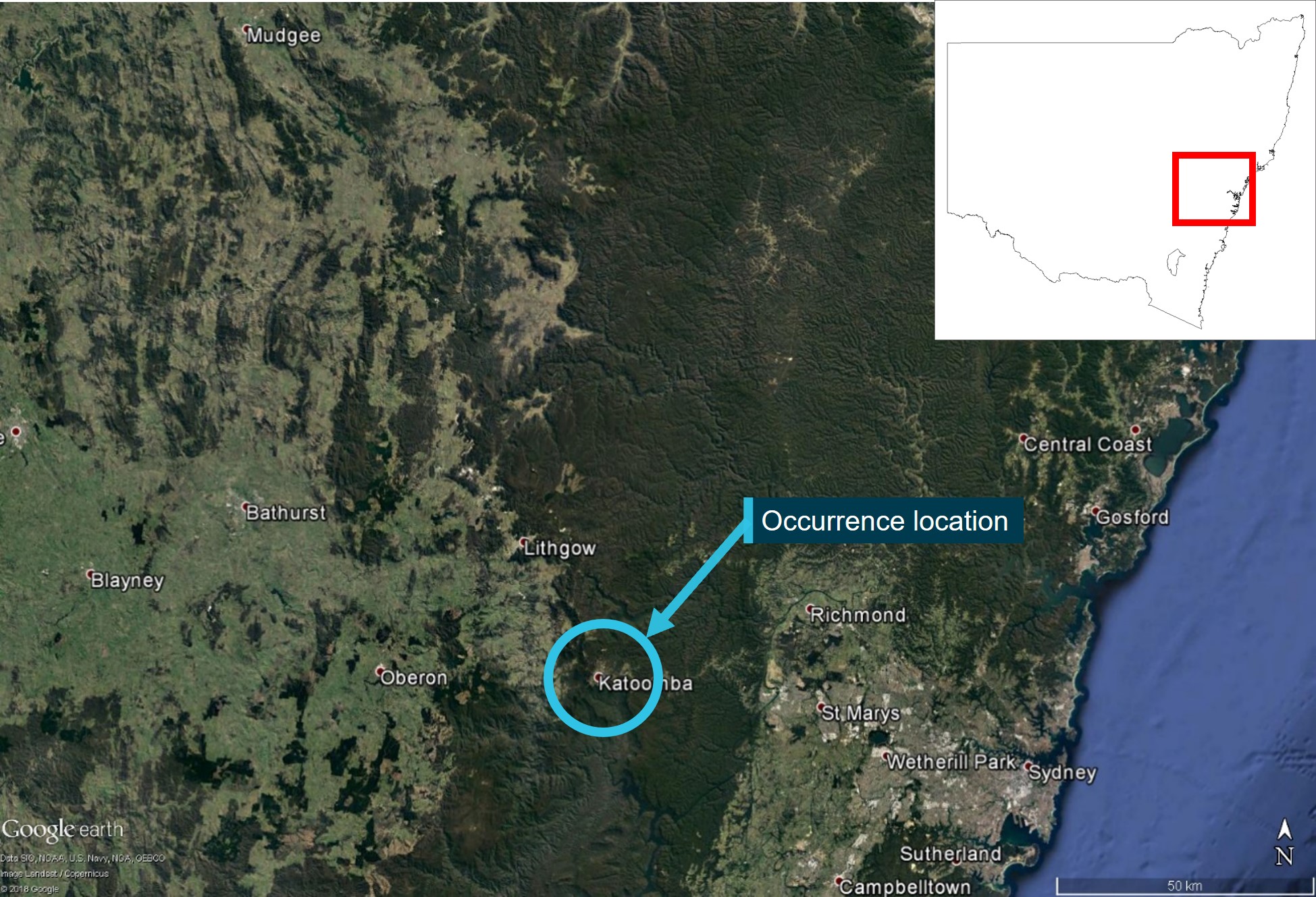
Source: Google Earth, annotated by the ATSB.
The helicopter operator had been tasked to locate and extract an injured bushwalker from the Blue Mountains National Park. The bushwalker had reportedly fallen near the base of the Giant Stairway near the Three Sisters rock formation (Figure 2).
Figure 2: Location of bushwalker at the base of the Giant Stairway near Katoomba, NSW

Source: Google Earth, annotated by the ATSB.
The task involved flying TJH from its base at Bankstown Airport, NSW, to the vicinity of Katoomba, NSW (about 65 km) to locate the injured bushwalker. The flight was conducted under the night visual flight rules, with the assistance of night vision goggles (NVG). On board was the pilot, an aircrew officer (ACO), a paramedic and a doctor. Once located, the paramedic, doctor and an equipment bag were to be lowered to the bushwalker in 3 individual winch insertions. The paramedic and doctor would then assess the patient and devise an appropriate extraction plan.
The crew shift started at 1930 on the evening on 25 March. The shift began routinely with a debrief and hand-over with the crew from the previous shift. This was followed by a check of the aircraft and equipment, including the NVG system and a review of weather conditions. Later in the shift, shortly before 2200, the pilot was notified of a possible task in the Blue Mountains, and they began some initial preparations. At 2241 the formal tasking for the job was received and preparations continued, including a pre-departure risk assessment. The helicopter departed from Bankstown Airport at 2329 and transited to Katoomba (Figure 3).
Figure 3: Flight data for VH-TJH on 26 March 2021
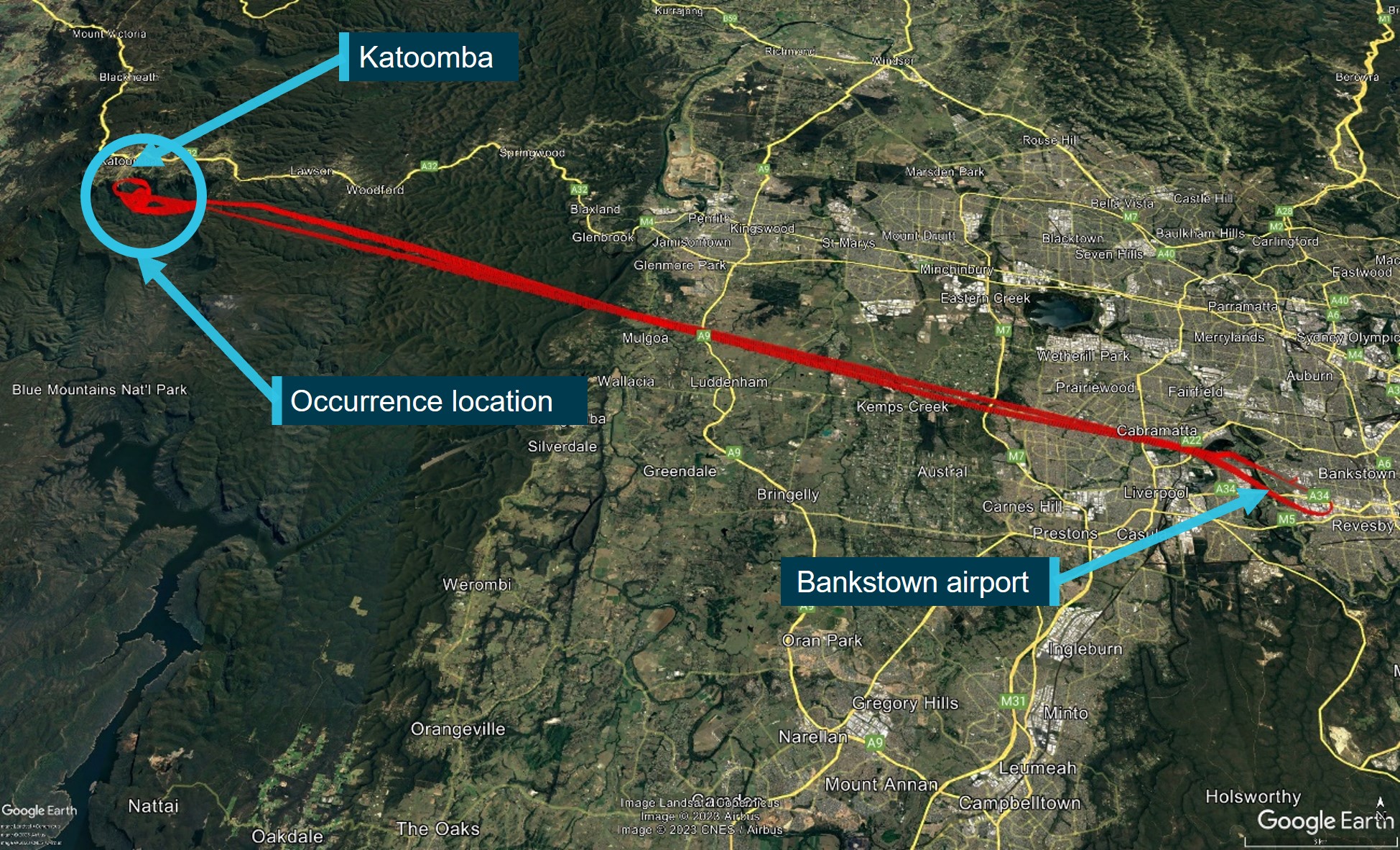
Source: Google Earth, annotated by the ATSB.
Approaching Katoomba at about 2355, the pilot identified the location of the bushwalker via a first responders’ strobe light. They then overflew the pre-determined staging point, a car park at Echo Point at the top of the mountain that could be used as a landing site if required (Figure 4).
Figure 4: Flight data showing VH-TJH overflying the bushwalker and staging point before approaching the winch location
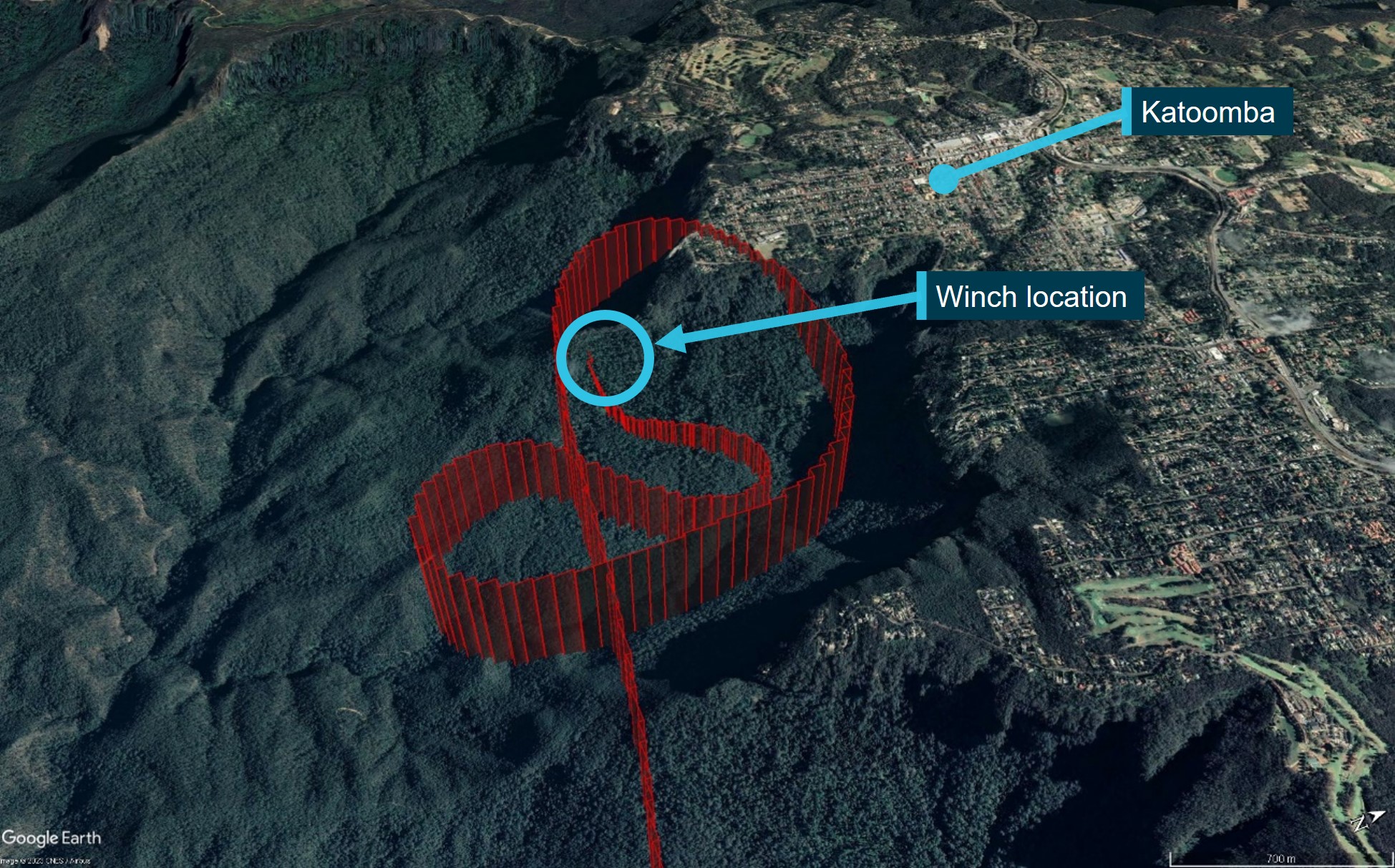
Source: Google Earth, annotated by the ATSB.
The pilot then manoeuvred the aircraft into the winch position, initially placing the aircraft in a high hover at about 400 ft above ground level, abeam the strobe light with the nose of the aircraft pointing out towards the valley to aid emergency egress if necessary.
Prior to establishing the helicopter into the final winch position the pilot and ACO conducted a brief on-site risk assessment in accordance with the operator’s standard practice. It was identified that the pilot would have better visual hover references if the aircraft was placed with the nose towards the cliff. It was recognised that this orientation came at the cost of an emergency flyaway option down the valley, but it was assessed that improved hover reference was more desirable. After this conversation the pilot moved the aircraft to the right, towards the winch site, and descended to about 85 ft. The nose of the aircraft was also repositioned to face directly towards the cliff.
Concurrently, the ACO opened the rear right sliding door and the paramedic removed their NVG in preparation for winching. With the aid of a downward facing winch light and a handheld search light, the ACO sighted the bushwalker and gave voice commands to the pilot to guide them into position.
With the helicopter facing the cliff, the pilot positioned the 2 moveable landing lights to aid visibility. The right light was placed in the one o’clock position, and the left one was angled in the 11 o’clock position. They then used NVG to identify a large dead tree on the slope of the cliff directly in front of the aircraft to use as a hover reference point. Additionally, looking down underneath the NVG, the pilot identified a bush on the slope in the lower 2 o-clock position which was illuminated with the white light of the landing light. Using these 2 points as reference, the pilot scanned their eyes between the dead tree in the 12 o’ clock position (though NVG), the bush on the ground in the 2 o’clock low position (underneath the NVG) and then to the flight instruments (also underneath the NVG). These visual references were used to maintain the hover while the ACO provided verbal feedback and commands to the pilot to assist maintaining position.
Once established in the winch position, and after a final scan for obstacles, the ACO started winching the paramedic down. With about 12 ft of cable payed out, the paramedic’s head was just past the level of the flight step, underneath the rear sliding door. At this point, during one of their scans while checking the engine torque, the pilot detected movement of the helicopter and looked up. About the same time, the ACO also noticed the aircraft had moved out of position and called to the pilot ‘you’re drifting right, you’re drifting right’, ‘hold’, hold’. Despite this command, the helicopter continued moving to the right and forwards towards rising terrain. The ACO then called ‘You’re going to crash, you’re going to crash, move back and up’, and a ‘bank angle’ warning sounded.
The pilot recovered control of the aircraft and climbed away from the cliff as the paramedic held onto the flight step. During the recovery, an over‑torque warning illuminated. A subsequent review of recorded flight data (Figure 5) identified that during the initial drift out of position the aircraft was banked right up to approximately 30° and during the recovery manoeuvre it was pitched nose-up to about 51°.
Figure 5: Flight data for VH-TJH showing the hover, drift and recovery
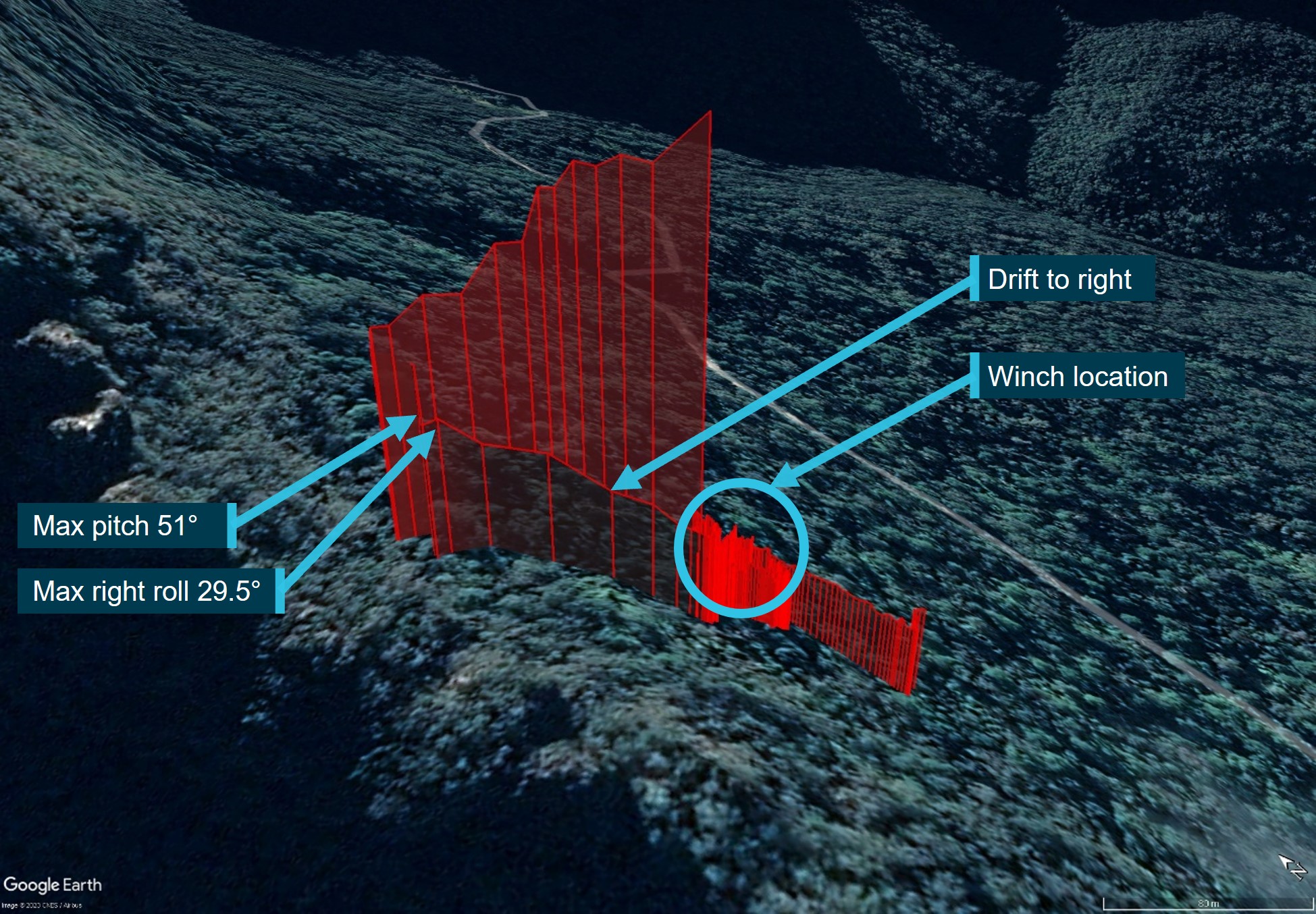
Source: Google Earth, annotated by the ATSB.
Once clear of the cliff face and in stable flight, the ACO winched the paramedic back on board and closed the rear door. The aircraft then returned to Bankstown Airport for an uneventful landing. None of the crew sustained injuries during the occurrence and a subsequent engineering inspection did not reveal any fault or damage to the aircraft. The bushwalker was winched out by another helicopter crew the next morning.
Context
Personnel information
Pilot
The pilot had over 15 years of helicopter flying experience, including military and emergency medical services (EMS) operations. They also held an Air Transport Pilot Licence (Helicopter) that was issued on 16 January 2019.
The pilot’s logbook showed a total flying experience of 3,484.1 hours to the last recorded flight on 25 March 2021. This included over 600 hours using night vision goggles (NVG). The pilot’s total flying experience on the AW139 was 338.9 hours. In the previous 90 days, the pilot had flown 70.7 hours on type, and in the previous 30 days the pilot had flown 28.4 hours on type. The pilot’s licence indicated that they had completed an AW139 flight review on 21 October 2020.
The pilot also held a Class 1 aviation medical certificate valid to 21 December 2021.
Aircrew officer
The Aircrew Officer (ACO) had over 13 years’ experience crewing helicopters. In that time, they had accumulated nearly 3,000 total hours of which about 700 involved the use of NVG.
Paramedic and doctor
The paramedic’s role included rescue crew officer duties, down‑the‑wire duties and inter-hospital operations. Given the condition of the bushwalker and their medical history, a doctor was also tasked to provide additional medical treatment. Neither the paramedic nor doctor were expected to be directly involved in the operation of the aircraft.
Aircraft information
General
The Leonardo Helicopters AW139 is a medium-sized, twin-engine helicopter powered by two Pratt & Whitney PT6C-67C engines. The combined maximum power output of both engines is greater than the main gearbox’s allowable power limit. Therefore, over torque of the transmission can occur when a pilot demands excessive engine power with both engines operative. VH-TJH was certified and maintained for both Instrument flight rules (IFR) and night vision imaging system (NVIS) operations.
Flight crew configuration
Civil Aviation Order 82.6 was in force at the time of this incident and stated that the minimum crew for NVIS operations must not be less than the highest requirement for NVFR, or IFR, specified in either:
- the aircraft’s flight manual
- the operator’s operations manual acceptable to CASA
- Australian civil aviation legislation, including this Order, that applied to the aircraft.
Flight crew configuration for EMS helicopter operations was in accordance with the approved rotorcraft manual.
Supplement 24 of the AW139 rotorcraft manual detailed the minimum flight crew required for night visual flight rules operations as one pilot, unless otherwise required by operating rules.
Supplement 60 of the AW139 rotorcraft flight manual detailed the minimum flight crew required for night vision goggle operations and was to be read in addition to supplement 24 for EMS operations. This supplement allowed for the minimum flight crew to be a single pilot and an additional NVG‑equipped crew member during take-off and landing on unimproved sites to assist with obstacle identification and clearance.
Night vision imaging system
To improve vision during night operations, the helicopter crew utilised a night vision imaging system (NVIS). The operator was experienced in the application of this technology and trained their own crews and offered NVIS training to other operators.
The operator’s NVIS comprised:
- AN/AVS-9 green phosphor NVG
- NVG-compatible cockpit and cabin lighting
- ACO‑controlled steerable winch and handheld light
- Two pilot‑steerable white landing lights on the underside of the aircraft
- Additional airworthiness requirements and NVIS specific procedures and training.
Despite the advantages provided by NVG, their application has inherent limitations including:
- Optimal performance requires accurate set-up, including inter-ocular adjustment, tilt, vertical, horizontal (eye-relief), focus and dioptre.
- The image generated by NVG is monochromatic[1] (green), resulting in a degradation in the ability to recognise objects and perceive depth (RTCA 2001b). This can result in a lack of contrast, and therefore degradation of visual acuity.[2]
- The field of view (FOV)[3] in NVG is limited to 40° horizontally and vertically (ITT Industries 2003). This compares to the FOV for normal unaided vision of about 200° horizontally and 120° vertically (Miller and Tredici 1992).
- The quality of the NVG image can be limited by environmental conditions, such as celestial illumination,[4] and weather conditions (e.g. humidity, fog, mist, cloud, precipitation) (RTCA 2001b).
For more information regarding operations with NVG see ATSB aviation research report: ATSB B2004/0152 - Night vision goggles in civil helicopter operations (April 2005)
External white lighting
Unlike military application, the use of white light was fundamental to the operator’s NVIS usage strategy. VH-TJO was fitted with the standard external AW139 lighting detailed above. The winch light pointed directly downward from the aircraft to illuminate the winch site, with illumination supplemented by the ACO’s handheld light. Low level operations (search and rescue/hover/winching) were conducted by the operator using a combination of references viewed both with and without NVG.
The pilot reported that the helicopter’s white lighting was ineffective in illuminating an area sufficient to maintain adequate visual references. The landing lights (which were also being used as search lights) were also described as being significantly less effective in comparison to the handheld light used by the ACO and also in comparison to other (purpose built) search lights used previously by the pilot with other helicopter emergency medical services (HEMS) operators.
Several other operators conducting similar night search and rescue, hover and winching operations, had modified their aircraft to include high‑powered search lights and additional external aircraft white lighting.
With regards to aircraft lighting, Civil Aviation Order (CAO) 29.11 – Air service operations – helicopter winching and rappelling operations, mandated that any helicopter engaged in winching over land by night was to be equipped with:
- 2 white lights, controllable by the ACO
- 2 white lights operable by the pilot and trainable in azimuth and elevation without removing their hands from the flying controls
- an approved inter-communication system permitting continuous communication between the pilot and ACO
Additionally, CAO 82.6 - Night vision imaging system — helicopters required that:
The operator and the pilot in command of an NVIS operation must ensure that the helicopter has a serviceable pilot-steerable searchlight, adjustable in both pitch and azimuth from the flight controls.
Finally, Appendix V of CAO 20.18 - Aircraft equipment — basic operational requirements required:
2 landing lights except that, in accordance with the provisions of regulation 308 of CAR 1988, aircraft engaged in private and aerial work operations and charter operations not carrying passengers for hire and reward are exempted from this requirement provided that 1 landing light is fitted. Note A single lamp having 2 separately energised filaments may be approved as meeting the requirement for 2 landing lights.
None of the three CAOs contained guidance or stipulation regarding the minimum intensity/performance capabilities required of the 2 white lights operated by the pilot.
The aircraft was fitted with two pilot‑steerable white landing lights on the underside of the aircraft (also being used as searchlights), as well as an ACO‑controlled steerable winch light and handheld light.
Meteorological information
Bureau of Meteorology forecasts
The flight from Bankstown Airport to the Katoomba area and return occurred in the Graphical Area Forecast NSW-E (GAF NSW-E). Within the GAF NSW-E there were 2 subdivisions affecting the flight. The departure and landing site was located in subdivision A1, and the occurrence location was in subdivision A. The GAF NSW-E was valid from 2200 local time on 25 March 2021 to 0400 on 26 March 2021, with forecast conditions including:
- average conditions of greater than 10 km visibility
- broken[5] stratocumulus[6] cloud 2,000 to 6,000 ft above mean sea level (AMSL) in A1
- scattered[7] stratocumulus cloud 2,000 to 3,000 ft AMSL
- moderate turbulence was implied in cumulous, stratocumulus and altocumulus cloud.
Automatic weather station observations
The Bureau of Meteorology’s routine report of the weather conditions at Bankstown Airport at 2330 local time (1 minute after take-off) showed a westerly wind at 4 knots, with an air temperature of 19°C and a dew point temperature[8] of 12°C. Visibility was observed to be greater than 10 km with nil clouds detected. It also showed that no rainfall had been recorded in the preceding 10 minutes and only 0.2 mm had been recorded since 0900 that morning. The QNH[9] was 1010 hPa.
Environmental observations
The pilot and ACO stated that before departure from Bankstown they had examined weather conditions en route and in the Katoomba area. No weather-related restrictions were identified. The clear skies and light variable winds were noted during the pre-flight risk assessment, as was the good visibility afforded by the roughly 80% moon phase.
Once on-site, conditions were initially observed to be good with very good visibility. However, once the aircraft was lowered into the winch position it was now positioned behind the cliff in the moon’s shadow. Additionally, the pilot reported that, with the aircraft’s nose pointed towards the cliff, they had no visual reference to the horizon. The pilot later estimated approximately a 60% reduction in overall visibility once they were in the winch position as compared to the conditions en route and at higher altitudes.
Additional information
Recorded data
VH-TJH was fitted with a Penny & Giles Aerospace Limited solid-state Multi-Purpose Flight Recorder (MPFR)[10]. The MPFR recorded over 900 flight data parameters and 2 hours of audio recordings on 4 channels.
The aircraft was also fitted with an additional video and audio recording system specifically introduced by the operator as part of the aeromedical fit out for the AW139. It consisted of 3 cameras, 2 of which were in the cabin and one fitted to the right-side fuselage below floor level and focused downward on the winch site. The rest of the system consisted of a power control module, an audio mixer and interfaces with the existing aircraft audio panels. Video and audio files were recovered from this system. Audio was recorded from several inputs, however the separate inputs were combined and recorded into one audio file.
As part of this investigation the ATSB requested both the flight data and audio recordings from the MPFR under the provisions of the Transport Safety Investigation Act 2003. Although the operator provided the flight data, the audio recordings had been overwritten. Additionally, while the operator provided video and audio from the incident from the onboard system, the operator isolated only a portion of the recordings, then reinstalled the memory card and the remaining data was overwritten. Although the audio data was not recovered from the MPFR, the recorded flight data information and time stamps from the MPFR have been used for analysis and throughout the report. Additionally, an animation was created using the flight data recorded by the MPFR.
Video 1: Animation derived from flight data from the MPFR.
Source: Cesium, annotated by the ATSB.
Operational information – Operator flight manual
The operator’s manual included a volume relating specifically to winch operations (Vol 6L, Rev 7.1). The manual included guidance on the conduct of a pre-winch brief, to be conducted with the pilot before conducting any winch task. The brief was to include:
- Emergency procedures and intended actions for loss of power / control in the hover. The crew will be informed whether the aircraft is Safe Single Engine, Flyaway or Committed
- Helicopter performance
- Relevant mission information
- Safety considerations.
The manual also included a volume relating specifically to NVIS operations (Vol 6C Rev 7.1). The NVIS operations manual provided guidance regarding pre-flight Briefing and checklist. The NVIS flight planning was to include the establishment of a range of decision points for each NVIS flight that define go / no-go criteria. The decision points included to:
- minimum weather requirements for initiating NVIS flight (illumination, visibility, cloud base)
- statement of deteriorating conditions criteria for initiating an IMC recovery (visibility, cloud base)
- the NVIS Recovery Plan.
Neither of these volumes of the operations manual contained specific guidance pertaining to hazards associated with the combined operation of winching with NVIS in the form of an on-site risk assessment. However, overarching these volumes, the operators Volume 2 Rotary wing aircraft operations manual required the maintenance of visual references during a hover, stating:
Hovering is a visual manoeuvre that requires adequate references to maintain position. Where precision hovering is required, such as during live winching, hover exit/entry, fast roping, external load operations, etc, the operation is not to commence unless adequate visual references are available and can be maintained throughout the manoeuvre. If upon termination of an approach adequate hover references are not available, a go around is to be conducted as described in section 2D1.17.
Operational information - NVIS Recency
Operator requirements
At the time of the occurrence the operator’s recency requirements for a pilot to conduct NVIS operations included:
For a pilot with more than 50 hours of NVIS flight time:
- 3 hours incorporating at least 3 take-offs, circuits and landings within the last 6 months; or an NVIS operational proficiency check (OPC) in the last 6 months.
- NVIS proficiency check (NPC): Annually after the first NPC, subsequent NPCs could be conducted within the 90 days before recency would otherwise expire.
- NVIS winch: Conducted an NVIS winch in the preceding 6 months.
CASA requirements
Civil Aviation Order (CAO) 82.6 was in force at the time of this incident and established operational and airworthiness standards and approval requirements for the use of NVG in specialised helicopter aerial work operations.[11] CAO 82.6 and regulations 61.1010 and 61.1015 of Part 61 of the Civil Aviation Safety Regulations (CASR) 1998 stated that the minimum NVIS recency check requirements for a pilot with greater than 50 hours NVIS flight time included:
- completed at least 3 hours flight time at night under the VFR using NVG within the previous 6 months; and
- conducted at least 3 take-offs and at least 3 landings at night using NVG within the previous 6 months, or
- become authorised to pilot any type of helicopter using NVG within the previous 6 months, or
- by successfully participating in an operator's training and checking system for an operation at night using NVG, and the operator holds an approval under regulation 61.040.
International requirements
The United States (US) Federal Aviation Administration (FAA) stipulated 2-month currency requirements for NVIS Helicopter emergency service (HEMS) with passengers and 4 month currency without passengers. Additionally, within the previous 2 months for operations with passengers onboard the following were required:
- 3 take-offs and landings, with each take-off and landing including a climb out, cruise, descent, and approach phase of flight.
- 3 hovering tasks.
- 3 area departures and area arrivals.
- 3 tasks transitioning from aided night flight to unaided night flight and back to aided.
- 6 night vision goggle operations for helicopter operation.
The Transportation Safety Board of Canada, stipulated 3-month recency requirements, as did the European Aviation Safety Authority. The Civil Aviation Authority of New Zealand stipulated the minimum currency requirement for a NVIS crew member of 4 months.
Pilot recency
The pilot had over 600 hours NVIS flight time experience and satisfied both their operator’s and CASA’s recency requirements. However, their last NVIS winch was conducted on 2 February 2021 as part currency training, and it was noted that this was a very benign winch environment conducted in a local area. The last complex winch the pilot had conducted was on 3 February 2020, approximately 13 months before this incident.
During interview, the pilot reported that once on-site and in the hover, they felt a sense of unfamiliarity. They reported feeling rusty and cognisant that it was over a year since they had been in a similar situation. As a result, they felt they were ‘working really hard in an environment that used to be their bread and butter’. Having done one winch in the past 6 months, they felt ‘current but not competent’.
Workload
There are 4 general factors that can directly affect workload (Jarvis 2010).
- difficulty of the task
- number of tasks running in parallel (concurrently)
- number of tasks in a series (switching from task to task)
- the time available for the task (speed of task).
Other indirect factors such as durations of task, fatigue and level of arousal can also contribute to workload (CAA, 2016). Factors affecting workload for pilots may additionally include stress, recency, and the use of NVIS.
Flying a helicopter is a cognitively complex task requiring developed psychomotor skills.[12] When manually hovering, the pilot needs to coordinate simultaneous control inputs of both hands and feet precisely, requiring constant attention. This is because helicopters are inherently unstable in the hover.
During interview, the pilot reported that they were experiencing a higher than normal workload in the lead up to the occurrence, stating that the ‘workload is high’ and they were ‘working really hard’.
Spatial disorientation
Spatial disorientation is a type of loss of situation awareness, and is different to geographical disorientation, or incorrectly perceiving the aircraft’s distance or bearing from a fixed location. Spatial disorientation occurs when pilots do not correctly sense their aircraft’s attitude, airspeed or altitude in relation to the earth’s surface. In terms of an aircraft’s attitude, spatial disorientation is often described simply as the inability to determine ‘which way is up’, although the effects can often be more subtle than implied by that description.
Spatial disorientation occurs when the brain receives conflicting or ambiguous information from the sensory systems. It is likely to happen in conditions in which visual cues are poor or absent, such as in adverse weather or at night.[13] Spatial disorientation presents a danger to pilots, as the resulting confusion can often lead to incorrect control inputs and resultant loss of aircraft control. The misperceptions can be so compelling that spatial disorientation accidents have had fatality rates of 90–91% (Gibb, Gray and Scharff 2010).
During interview the pilot reported that, while they were scanning their eyes from the 2‑o’clock low position to the engine instruments, they felt movement in the aircraft and brought their eyes up the 12 o’clock position. They then observed that the tree being used as a visual reference was no longer visible. In response, the pilot reported being both startled and confused. Additionally, they had no recollection of applying control inputs so the voice commands from the ACO announcing that they were drifting right, as well as the bank angle warning, were completely unexpected.
The pilot reported not comprehending why they were receiving the feedback from the ACO that they were drifting, nor the bank angle warning. They reported ‘the worst sense for the leans’, and a ‘horrible tumbling feeling’. Despite this, the pilot was still aware of their proximity to the cliff and the inherent danger that posed, but not their actual position in space. When the pilot pitched the aircraft up to avoid the cliffs, they caught a glimpse of a tree through the NVG on the right-hand side. At this point the pilot regained their orientation, enabling them to recover control of the aircraft.
Related occurrences
A review of Australia’s national aviation occurrence database for the 20 years leading up to this incident revealed 4 similar investigated occurrences involving the loss of control of a helicopter at night while using NVIS. Summaries of the 4 investigations are as follows.
Terrain awareness warning system alert involving Eurocopter BK 117C-2, VH-SYB, near Crookwell, New South Wales on 21 October 2016 (AO-2016-160)
Shortly after take-off, the helicopter unexpectedly encountered low cloud, and the pilot initiated the operator’s inadvertent entry into instrument meteorological conditions (IMC) procedure. While conducting the procedure, the momentum of the helicopter’s climb reduced. In response, the pilot lowered the helicopter’s nose to regain airspeed, but inadvertently overcorrected the pitch angle to 15° nose-down, as well as allowing a slight roll to the left. The resulting unusual attitude triggered a caution alert from the helicopter’s enhanced ground proximity warning system.
Loss of control in flight involving Leonardo Helicopters AW139 helicopter, VH-YHF, near Adelaide River mouth, 38 km east‑north‑east of Darwin, Northern Territory on 13 May 2018 (AO-2018-039)
During an approach to a potential EPIRB target, smoke from nearby bushfires affected visibility and the helicopter developed an uncommanded high rate of descent. The Aircrew Officer, in the rear of the helicopter, called ‘Climb! Climb! Climb!’, and the pilot regained control with a rehearsed recovery drill. During the recovery procedure, the power demand exceeded airframe limitations. This exceedance went undetected, and the helicopter was flown on a second sortie that same evening.
Main rotor blade strike involving Leonardo Helicopters AW139, VH-EGK, 21 km west‑south‑west of Caboolture Airport, Queensland on 20 June 2020
(AO-2020-031)
During night winching operations, the helicopter's main rotor blades struck a tree. The crew conducted a return to Archerfield. The post-flight inspection revealed the majority of the main rotor blades had sustained damage. One blade tip was substantially damaged. At the time of writing, this investigation was ongoing.
Loss of control and near collision with terrain, Leonardo Helicopters AW139, VH-TJO
(AO-2020-038)
On 24 July 2020, the crew of a Leonardo Helicopters AW139, registered VH-TJO, departed Shellharbour Airport, near Wollongong, New South Wales, with 4 crew onboard (including a single pilot and aircrew officer). The flight was conducted under the night visual flight rules, with the assistance of night vision goggles, to recover 2 bushwalkers from the Bungonia National Park, New South Wales.
On arrival at the search and rescue location the helicopter was descended to approximately 240 ft above ground level and the airspeed was reduced. The aircraft was then tracked over high ground past the edge of an escarpment, where the terrain dropped away to the valley floor. During this time an uncommanded, and increasing, rate of descent and lateral drift developed. This was identified by the aircrew officer, with corrective instructions provided to the pilot. During the recovery, the engine power output exceeded airframe limitations, rendering the helicopter temporarily unserviceable.
Safety analysis
Introduction
While conducting aerial work near Katoomba, about 65 km west of Bankstown Airport, New South Wales, a Leonardo Helicopters AW139 registered VH-TJH, was hovered above an injured bushwalker near the base of the Three Sisters walking trail. The aircraft was lowered to about 85 ft AGL (above ground level), about 20 ft above the treetops with its nose facing the cliff in preparation for winching. As the Aircrew Officer (ACO) started lowering the paramedic on the winch line, the aircraft started drifting to the right and towards the cliff. The ACO alerted the pilot to the drift and a bank angle warning sounded as the aircraft banked to about 30° to the right. Aware of the nearby cliffs, the pilot pitched the aircraft up and away from the cliffs, pitching the aircraft to about 51° nose up. During this manoeuvre an engine over‑torque occurred. After control of the aircraft was regained, the paramedic was retrieved, and the aircraft returned to Bankstown.
Post flight engineering inspections by the operator did not identify any damage to the aircraft. Nor were any defects identified that could have contributed to the occurrence. Additionally, no evidence was found to suggest any medical, fatigue‑related or physiological issues that would have affected the pilot’s performance on the day of the flight. Therefore, this analysis will focus on the operational and environmental factors that led to an experienced helicopter pilot temporarily losing control of their aircraft during a complex NVIS winching operation.
External aircraft white lighting
Although Civil Aviation Orders (CAO) 29.11, 82.6 and 20.18 required the aircraft to be fitted with 2 white lights operable by the pilot, there was no guidance or minimum intensity/performance capabilities specified for these lights. As a result, the operator believed they were complying with the CAO requirements by using the 2 moveable landing lights as search lights. These landing lights were described by the pilot as being ineffective in illuminating an area sufficient to maintain visual references. It was also noted that they were significantly less effective when compared to the handheld light used by the ACO and to other search lights used previously by the pilot with other HEMS operators.
The limited illumination provided by the available lights likely influenced the crew’s decision to face the aircraft relatively close, and directly towards, the cliff in order to maximise the available hover references. However, even when operating close to the cliff, the lights were still ineffective at illuminating the search area sufficiently to provide adequate visual reference for the pilot. This significantly increased the pilot’s workload during the hover phase.
Inadequate external lighting has previously been found to be a safety issue on another ATSB investigation (AO-2020-038). This occurrence also involved a loss of control and near collision during NVIS HEMS operations. It also involved the same operator, aircraft type and lighting system. That investigation found:
The external aircraft white lighting was inadequate to illuminate the terrain below and to the side of the aircraft at the required operating height. This delayed the identification and recovery from the unsafe aircraft state resulting in the pilot not identifying the developing rate of descent during the incident, delaying the recovery from the descent.
In‑flight risk assessment
During the initial positioning of the aircraft, the pilot hovered the helicopter abeam the bushwalker at about 400 ft above the ground and positioned the nose of the aircraft out towards the valley to aid egress if necessary. Before manoeuvring the aircraft into the final winch position, the pilot and ACO conducted a brief in-flight pre-winch risk assessment. It was decided to reposition the aircraft towards the cliff as they descended to about 80 ft. This decision aided visual references for the pilot at the expense of ease of egress. It also resulted in the aircraft being in the moon’s shadow behind the cliff and the pilot not having any visible horizon. Both the pilot and ACO identified the significant degradation in available illumination at the site compared to what was briefed during pre-flight risk assessment however, the implication of this was not discussed. Egress actions in the event of a goggle failure were also not discussed, nor the aircraft external lighting limitations. As the pilot became aware that their workload was unusually high, there was also no communication about this to the ACO, however that may have been influenced by the focussed attention required to control the helicopter.
Had a more effective in‑flight risk assessment been conducted, it would likely have identified the elements that made this winch site a highly challenging one, such as the low illumination and absent visible horizon. This could have allowed the pilot to more accurately assess the likely workload associated with maintaining a steady hover in those conditions. This, in turn, may have led to a conclusion that the site was unsuitable for NVIS winching.
Although operator guidance was provided for both winching and NVIS operations, as well as pre‑flight and pre-winch briefings, there was limited guidance pertaining to the risk assessment of the combined activity once on site. The inclusion of a structured on-site risk assessment process/checklist specific to NVIS winching would have emphasised the requirement to identify and assess site‑specific hazards, such as the adequacy of visual references and a safe method of recovery in the event of NVG failure.
Recency
The pilot and ACO both met the company recency requirements, as well as CASA’s, for NVIS winch currency. Despite this, the pilot found themselves in a challenging operational situation that they had not been in for over a year. This resulted in the pilot feeling a sense on unfamiliarity when they found themselves in a complex NVIS winch environment. Specifically, they reported feeling rusty and felt ‘current but not competent’. As a result, they felt they were ‘working really hard in an environment that used to be their bread and butter’.
Workload – spatial disorientation and loss of control
The pilot reported a higher‑than‑expected workload from the moment they got into the hover, combined with a feeling of unfamiliarity. In the past, the pilot had regularly flown in similar environments during military, search and rescue and HEMS operations however, at the time of the occurrence it had been over a year since their last complex NVIS winch. This likely contributed to the increased workload experienced by the pilot.
It is also likely that the lack of visual cues due to the moon’s shadow, the lack of visible horizon and the illumination provided by the external white lights as well as the pilot’s recency with complex NVIS winching, all contributed to the increased workload. These factors likely combined resulting in the pilot losing visual references during one of their instrument scans leading to the pilot becoming spatially disorientated and temporarily losing control of the aircraft. The engine over‑torque then occurred during the subsequent recovery manoeuvre.
Recovery of flight recorder audio
The ATSB requested that the multi-purpose flight recorder be quarantined for use in the investigation. Although flight data from the incident was recovered, the portion of the 2-hour audio recording that contained the incident was overwritten because power to the device was not removed while the aircraft was in transit.
Findings
|
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the loss of control and near collision with terrain, involving Augusta AW139, VH-TJH, near Katoomba, New South Wales on 26 March 2021.
Contributing factors
- The external aircraft white lighting was inadequate to illuminate the terrain below and to the side of the aircraft at the required operating height. [Safety issue]
- The pilot likely experienced a sustained higher than normal workload while operating in a reduced visual cue environment, causing a misidentification of hover references and disorientation, leading to a subsequent loss of control.
- Regulatory requirements did not ensure that aircraft lighting was adequate to conduct night vision imaging system winching operations safely. [Safety issue]
- Toll recency for night vision imaging system (NVIS) winching was insufficient to ensure that complex NVIS winching operations, such as in this occurrence, could be conducted safely. [Safety issue]
Other factors that increased risk
- Although the flight crew identified the degradation in available illumination at the winch site compared to what was briefed prior to departure, the risk posed by this hazard was not fully assessed on‑site.
- Although the operator’s procedures for winching and night vision imaging system operations included the need to have adequate hover references and a method of recovery in the event of a night vision goggle failure, there was limited guidance to ensure these requirements were confirmed by the flight crew on‑site before commencing precision hover operations. [Safety issue]
Other findings
- CVR was not recovered for this flight, however the company installed camera and audio were obtained for the period of the incident. This limited the ability of the investigation to ascertain specific information regarding the on‑site risk assessment conducted by the crew, which occurred outside the duration of the provided company footage.
Safety issues and actions
|
Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Aircraft lighting regulation
Safety issue number: AO-2021-018-SI-01
Safety issue description: Regulatory requirements did not ensure that aircraft lighting was adequate to conduct night vision imaging system winching operations safely.
External white lighting
Safety issue number: AO-2021-018-SI-02
Safety issue description: The external aircraft white lighting was inadequate to illuminate the terrain below and to the side of the aircraft at the required operating height.
TOLL recency requirements
Safety issue number: AO-2021-018-SI-03
Safety issue description: Toll recency for night vision imaging system (NVIS) winching was insufficient to ensure that complex NVIS winching operations, such as in this occurrence, could be conducted safely.
Operational in-flight risk assessment guidance
Safety issue number: AO-2021-018-SI-04
Safety issue description: Although the operator’s procedures for winching and night vision imaging system operations included the need to have adequate hover references and a method of recovery in the event of a night vision goggle failure, there was limited guidance to ensure these requirements were confirmed by the flight crew on‑site before commencing precision hover operations.
Glossary
| ACM | Air crew member |
| ACO | Aircrew officer |
| AGL | Above ground level |
| CAO | Civil Aviation Order |
| CASA | Civil Aviation Safety Authority |
| CASR | Civil Aviation Safety Regulations |
| CCTV | Closed-circuit television |
| CVR | Cockpit voice recorder |
| DAR | Digital aircraft recorder |
| EASA | European Aviation Safety Authority |
| EMS | Emergency Medical Services |
| EPIRB | Emergency Position Indicating Radio Beacon |
| FAA | Federal Aviation Administration |
| FDR | Flight data recorder |
| FOV | Field of view |
| GAF | Graphical area forecast |
| HEMS | Helicopter Emergency Medical Services |
| IAS | Indicated airspeed |
| ICAO | International Civil Aviation Organization |
| IFR | Instrument flight rules |
| NPC | NVIS proficiency check |
| NVFR | Night visual flight rules |
| NVG | Night vision goggles |
| NVIS | Night vision imaging system |
| OPC | Operational proficiency check |
| SMS | Safety management system. |
| US | United States |
| VFR | Visual flight rules |
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- pilot of the occurrence flight
- the aircrew officer of the occurrence flight
- TOLL helicopters
- Civil Aviation Safety Authority
- Leonardo S.p.A Helicopters
- Bureau of Meteorology
- video footage taken from onboard the aircraft
- recorded flight data from the MPFR.
References
RTCA 2001b, Concept of operations: Night vision imaging system for civil
Miller, R. E. and Tredci, T. J. 1992, Night vision manual for the flight surgeon, USAF Special Report No. AL-SR-1992-0002, Armstrong Laboratory, Brooks Air Force Base.
Australian Transport Safety Bureau. (2007). An overview of spatial disorientation as a factor in aviation accidents and incidents. ATSB Aviation Research and Analysis Report B2007/0063.
Australian Transport Safety Bureau. (2005). Night vision goggles in civil helicopter operations. ATSB Aviation Research and Analysis Report B2004/0152.
Civil Aviation Order (CAO) 29.11
Civil Aviation Order (CAO) 82.6
Civil Aviation Order (CAO) 20.18
Part 61 of the Civil Aviation Safety Regulations (CASR) 1998
Jarvis S (2010). Workload. Proceedings of CAA RETRE Seminar, 2010. Flight-crew human factors handbook (CAA, 2016).
Gibb, R., Gray, R. & Sharff, L. Aviation Visual Perception: Research, Misperception and Mishaps. Ashgate, 2010
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- pilot of the occurrence flight
- the aircrew officer of the occurrence flight
- TOLL helicopters
- Civil Aviation Safety Authority
- Leonardo S.p.A Helicopters
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Monochromatic: (of light or other radiation) of a single wavelength or frequency.
[2] Visual acuity: the relative ability of the human eye to resolve spatial detail and interpret an image. Any atmospheric condition, which absorbs, scatters, or refracts illumination may reduce the useable energy available to NVG.
[3] Field of View (FOV) is the maximum area that can be seen without any movement of the head or eyes. It is expressed in terms of degrees.
[4] Celestial Illumination: natural lighting from the moon, planets and stars.
[5] Broken is used to describe an amount of cloud covering the sky of between five and seven oktas (eighths). In aviation forecasts and reports it is coded as BKN
[6] Stratocumulus: A principal cloud type, forming in the low levels of the troposphere and existing in a relatively flat layer but having individual elements, from which drizzle can fall. It can form from cumulus clouds becoming more stratified when they push up into a stable atmospheric layer. In aviation forecasts and reports it is coded as SC.
[7] Scattered is used to describe an amount of cloud covering the sky of three or four oktas (eighths). In aviation forecasts and reports it is coded as SCT.
[8] Dewpoint: the temperature at which water vapour in the air starts to condense as the air cools. It is used, among other things, to monitor the risk of aircraft carburettor icing or the likelihood of fog.
[9] QNH: the altimeter barometric pressure subscale setting used to indicate the height above mean seal level.
[10] The MPFR integrates the functions of both the Flight Data Recorder and Cockpit Voice Recorder into one unit.
[11] Specialised helicopter aerial work operations and includes search and rescue, refer to CAO 82.6 (definitions)
[12] Psychomotor skills: psychological processes associated with muscular movement towards voluntary movements.
[13] More information about spatial disorientation can be found in the ATSB aviation research and analysis report
B2007/0063, An overview of spatial disorientation as a factor in aviation accidents and incidents.