Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation. The statement is published as a report in accordance with section 25 of the TSI Act, capturing information from the investigation up to the time of discontinuance.
Overview of the investigation
On the morning of 7 April 2023, a Fokker 70, registered VH-NUU, was being pushed back from a bay at Brisbane Airport, Queensland, to operate a passenger air transport flight to Roma. It was reported that during pushback at about 0640, a trail of fluid on the ground was observed and then found to be due to a fluid leak from the no. 2 (right) engine. Both engines were shut down and the aircraft was towed back to the bay.
When inspected, engineers determined there was a leak from a connection on the lower left side of the engine, between a rigid fuel line and the fuel flow regulator (FFR), and fuel had drained out of the engine nacelle through an access opening near the leak.
After removing the fuel line from the component, the source of the leak was determined to be a pair of elastomeric seals (O-rings), fitted to the fuel line, that had degraded to a point where they no longer could contain fuel under pressure. The seals were replaced, along with the FFR because of an unrelated defect. An engine ground run was carried out and the aircraft was returned to service.
After receiving notification of the occurrence on 12 April 2023, the ATSB commenced an investigation. The ATSB:
obtained maintenance records
examined maintenance information
interviewed technical specialists
obtained information from the engine manufacturer (Rolls-Royce).
During the investigation, and in consultation with the engine manufacturer, the ATSB noted that:
no reason could be established for the degradation of the seals, which occurred over a period of about 6 years since they were likely changed
maintenance records indicated that the components were installed and maintained in accordance with manufacturer requirements
there were no instances of an engine fire resulting from fuel leaks from the FFR or other components in the same area on Fokker 70 and Fokker 100 aircraft in over 26 million flying hours
the layout of the fuel lines on this engine type is routed to avoid ignition sources and there were no hot surfaces or sources of ignition in this zone
fuel leaks from this location would drain away from the engine and then out and away from the nacelle through an access opening on the bottom of the lower cowl.
Therefore, the ATSB considered it extremely unlikely that a fire would develop as a result of this type of fuel leak. Further, if a fire did occur it could be detected by on-board systems (or visually by ground crews) and extinguished (along with the fuel supply being isolated from the engine nacelle).
Reasons for the discontinuation
Based on a review of the available evidence, the ATSB considered it was unlikely that further investigation would identify any systemic safety issues or important safety lessons. The ATSB did not identify any concerns with the assessment, management, and monitoring of this type of defect. Consequently, the ATSB has discontinued this investigation.
The evidence collected during this investigation remains available to be used in future investigations or safety studies. The ATSB will also monitor for any related occurrences that may indicate a need to undertake a further safety investigation.
Occurrence summary
Investigation number
AO-2023-019
Occurrence date
07/04/2023
Location
Brisbane Airport
State
Queensland
Report release date
19/06/2023
Report status
Discontinued
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Discontinued
Mode of transport
Aviation
Aviation occurrence category
Aircraft preparation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Fokker B.V.
Model
F28MK070
Registration
VH-NUU
Serial number
11532
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
1. All non-restricted Safety Recommendations issued by the ATSB or Aviation Authority related to parking brake safety in fixed wing aircraft.
2. A copy of all non-restricted correspondence, communications, statements, reports, notes, recommendations, records exchanged between and among the ATSB and any fixed wing aircraft manufacturer, including but not limited to Textron Aviation, related to the Textron Aviation/Cessna Aircraft Citation series aircraft parking brake safety and airworthiness standards.
3. A copy of all non-restricted correspondence, communications, statements, reports, notes, recommendations, records exchanged between and among the ATSB and any other Aviation Authority related to the Textron Aviation/Cessna Aircraft Citation series aircraft parking brake safety and airworthiness standards.
All non-restricted documents relating to the aviation safety investigation and report: AO-2021-004, titled “incorrect configuration for landing involving Boeing 737 VH-XMO, near Sydney Airport, New South Wales, on 27 January 2021”.
All internal and external correspondence and records of any meetings or discussions created within the period 18 April 2020 to 17 April 2023, comprising or relating to advice given by ATSB or the ATSB’s Chief Commissioner, or advice considered to be given by ATSB or the ATSB’s Chief Commissioner even if the advice was not given, to either or both of: (1) a Minister with portfolio responsibility for the Transport Safety Investigation Act 2003 or any of that Minister’s staff; and (2) any official in the Department with portfolio responsibility for the Transport Safety Investigation Act 2003 when the costs of investigation activities by the ATSB were assessed by ATSB as likely to exceed established ATSB budget levels.
All emails, letters and other communications between the ATSB and external parties - including but not limited to DIPs - pertaining to the release of ATSB investigation AI-2018-010: The approval processes for the Bulla Road Precinct Retail Outlet Centre.
All non-restricted documents that directly relate to the derailment of freight train Y279 on 23 February 2022 for the period 11:00pm on 22 February 2022 to 3:30am on 23 February 2022.
The ATSB is investigating a long landing involving a Boeing 737-800 aircraft at Gold Coast Airport, Queensland, on 24 January 2023.
At about 1839 local time, while landing on runway 32 in poor weather conditions, the flight crew was unable to sight the touchdown markers. The aircraft was subsequently landed beyond the touchdown zone.
In early April, the operator provided the ATSB with a copy of their safety investigation report, which provided additional information regarding the incident. After obtaining this information, the ATSB decided to investigate the incident.
As part of the investigation, the ATSB has been examining the circumstances leading to the long landing and determining the contributing factors. To date, the ATSB investigation has included:
interviewing the flight crew
analysis of flight recorder and air traffic surveillance data
obtaining weather information
reviewing relevant procedures
reviewing related occurrences
collecting other evidence as required.
The draft report internal review process has been completed. The draft report has been distributed to directly involved parties (DIPs) to check factual accuracy and ensure natural justice. Any submissions from those parties will be reviewed and, where considered appropriate, the draft report will be amended accordingly.
Following the external review process, any submissions and amendments to the draft report are internally reviewed. Once approved, the final report is prepared for publication and dissemination and released to DIPs prior to its public release.
The final report will be published at the conclusion of the investigation. Should a critical safety issue be identified at any time during the investigation, the ATSB will immediately notify operators and regulators so appropriate and timely safety action can be taken.
Last updated:
Occurrence summary
Investigation number
AO-2023-018
Occurrence date
24/01/2023
Occurrence time and timezone
18:39 Australian Eastern Standard Time
Location
Gold Coast Airport
State
Queensland
Report status
Pending
Anticipated completion
Q3 2026
Investigation level
Systemic
Investigation type
Occurrence Investigation
Investigation phase
Final report: External review
Investigation status
Active
Mode of transport
Aviation
Aviation occurrence category
Runway - Other, Unstable approach
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737-8FE
Registration
VH-YQM
Serial number
41009
Aircraft operator
Virgin Australia Airlines Pty Ltd
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
On 7 April 2023, during a freight only charter flight from Bankstown Airport, New South Wales, to Archerfield Airport, Queensland, the pilot of a Piper PA-31-350, registered VH-HJE, reported a loss of power from the right engine followed soon after by the left engine. Unable to reach the destination aerodrome, the pilot conducted a gear up forced landing alongside a railway line. The aircraft struck multiple trees and was substantially damaged. The pilot, who was the sole occupant, sustained minor injuries.
What the ATSB found
Post accident inspections conducted by the operator’s engineers and an engine overhaul facility found no indication of a mechanical failure that would have caused the engines to fail.
Although the pilot reported changing from the auxiliary fuel tanks to main fuel tanks prior to descent, the quantity of fuel recovered from each tank after the accident, and fuel burn calculations, indicated that those selections had probably not been made and both engines lost power as a result of fuel starvation.
The loss of power from each engine was misdiagnosed by the pilot as a partial power loss and the engine failure procedures were not carried out. Following the first power loss on the right engine, the right propeller was not feathered. This configuration produced excessive drag, and the aircraft was unable to maintain altitude while the left engine was operating.
A review of the pilot’s sleep history found that it is likely that the pilot was experiencing a level of fatigue shown to have an effect on performance. In this case it is likely that fatigue impacted the pilot’s incorrect tank selection as well as their ability to troubleshoot the loss of power. The flight departed Bankstown at about 0350 and by the time of the accident, the pilot had been awake for almost 20 hours.
What has been done as a result
The operator issued a notice to aircrew and conducted a review of pilot training to include the recognition and management of fuel starvation. Company policy and flight planning software was reviewed to ensure consistency, and the Fatigue Management Manual was updated to include external employment and restrictions around hours of work and duty times.
Safety message
During a power loss event, pilots should take the time to determine whether a total failure has transpired or if the engine is still delivering some power. While this may not be clearly apparent in all configurations, the consequences of misdiagnosing a failed engine can be fatal. The Civil Aviation Safety Authority’s Civil Aviation Advisory Publication CAAP 5.23-1(2) Multi-engine aeroplane operations and training provides guidance on how to identify engine failures in multi‑engine aircraft.
Pilots are reminded of the importance of understanding an aircraft’s fuel supply system and being familiar and proficient in its use. Adhering to procedures, maintaining an accurate fuel record, and ensuring appropriate tank selections are made for the phase of flight will lessen the likelihood of fuel starvation.
The management of fatigue is a joint responsibility between the operator and the pilot. This accident also reinforces the importance of obtaining some sleep during the day prior to commencing operations at night during normal periods of sleep.
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is improving the management of fatigue.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 7 April 2023, the pilot of a Piper Aircraft Corporation PA-31-350 Chieftain (PA-31), registered VH-HJE and operated by Air Link, was conducting a freight charter flight from Archerfield, Queensland. The planned flight included one intermediate stop at Bankstown, New South Wales before returning to Archerfield, and was conducted under the instrument flight rules at night.
The aircraft departed Archerfield at about 0024 local time and during the first leg to Bankstown, the pilot reported an intermittent fault with the autopilot, producing uncommanded pitch changes and associated rates of climb and descent of around 1,000 ft/min. As a result, much of the first leg was flown by hand. After landing at Bankstown at about 0248, a defect entry was made on the maintenance release; however, the pilot was confident that they would be able to hand fly the aircraft for the return leg and elected to continue with the planned flight.
The aircraft was refuelled to its maximum capacity for the return leg after which a small quantity of water was detected in the samples taken from both main fuel tanks. Additional fuel drains were conducted until the fuel sample was free of water. The manifested freight for the return leg was considered a light load and the aircraft was within weight and balance limitations.
After taking off at 0351, the pilot climbed to the flight planned altitude of 9,000 ft. Once established in cruise, the pilot changed the left and right fuel selectors from the respective main tank to the auxiliary tank. The pilot advised that, during cruise, they engaged the autopilot and the uncommanded pitch events continued. Consequently, the pilot did not use the autopilot for part of the flight.
Approaching top of descent, the pilot recalled conducting their normal flow[1] checks by memory before referring to the checklist. During this time, the pilot completed a number of other tasks not related to the fuel system, such as changing the radio frequency, checking the weather at the destination and briefing themselves on the expected arrival into Archerfield. Shortly after, the pilot remembered changing from the auxiliary fuel tanks back to the main fuel tanks and using the fuel quantity gauges to confirm tank selection. The pilot calculated that 11 minutes of fuel remained in the auxiliary tanks (with an estimated 177 L in each main tank).
Around eight minutes after commencing descent and 28 NM (52 km) south of Archerfield (at 0552), the pilot observed the right ‘low fuel flow’ warning light (or ‘low fuel pressure’) illuminate on the annunciator panel. This was followed soon after by a slight reduction in noise from the right engine. As the aircraft descended through approximately 4,700 ft, the ADS-B data showed a moderate deceleration with a gradual deviation right of track. While the power loss produced a minor yaw[2] to the right, the pilot recalled that only a small amount of rudder input was required to counter the adverse yaw once the autopilot was disconnected. Without any sign of rough running or engine surging, they advised that had they not seen the annunciator light, they would not have thought there was a problem. Over the next few minutes, the pilot attempted to troubleshoot and diagnose the problem with the right engine.
Immediately following power loss, the pilot reported they:
switched on both emergency fuel boost pumps
advanced both mixture levers to RICH
cycled the throttle to full throttle and then returned it to its previous setting without fully closing the throttle
moved the right fuel selector from main tank to auxiliary
disconnected the autopilot and retrimmed the aircraft.
This did not alter the abnormal operation of the right engine, and the pilot conducted the engine roughness checklist from the aircraft pilot’s operating handbook noting the following:
oil temperature, oil pressure, and cylinder head temperature indicated normally
manifold absolute pressure (MAP) had decreased from 31 inHg to 27 inHg
exhaust gas temperature (EGT) indicated in the green range[3]
fuel flow indicated zero.
With no indication of mechanical failure, the pilot advised they could not rule out the possibility of fuel contamination and chose not to reselect the main tank for the remainder of the flight.
After considering the aircraft’s performance, handling characteristics and engine instrument indications, the pilot assessed that the right engine, while not able to generate normal power, was still producing some power and that this would assist in reaching Archerfield. Based on the partial power loss diagnosis, the pilot decided not to shut down and secure the engine which would have included feathering[4] the propeller.
At 0556, at about 20 NM south of Archerfield at approximately 3,300 ft, the pilot advised air traffic control (ATC) that they had experienced an engine malfunction and requested to maintain altitude. With maximum power being set on the fully operating left engine, the aircraft was unable to maintain height and was descending at about 100 ft/min. Even though the aircraft was unable to maintain height, the pilot calculated that the aircraft should have been able to make it to Archerfield and did not declare an emergency at that time.
At 0602, about 12 minutes after the power loss on the right engine, the left engine began to run rough and the pilot observed the left low fuel flow warning light illuminate on the annunciator panel. This was followed by severe rough running and surging from the left engine which produced a series of pronounced yawing movements. The pilot did not run through the checklist a second time for the left engine, reporting that they completed the remaining item on the checklist for the left engine by switching the left engine’s fuel supply to the auxiliary tank. The pilot once again elected not to change tank selections back to mains.
With both engines malfunctioning and both propellers unfeathered, the rate of descent increased to about 1,500 ft/min. The pilot advised that following the second power loss, it was clear that the aircraft would not be able to make it to Archerfield and their attention shifted from troubleshooting and performance management to finding somewhere to conduct a forced landing.
ADS-B data showed the aircraft was at about 1,600 ft when the left engine malfunctioned. The pilot stated that they aimed to stay above the minimum control speed, which for VH-HJE was 72 kt.[5] The aircraft was manoeuvred during the brief search (Figure 1), during which time the groundspeed fluctuated from 110 kt to a low of 75 kt. It was calculated that in the prevailing wind, this would have provided an approximate indicated airspeed of 71 kt; equal to the aircraft’s clean configuration stall speed.[6]
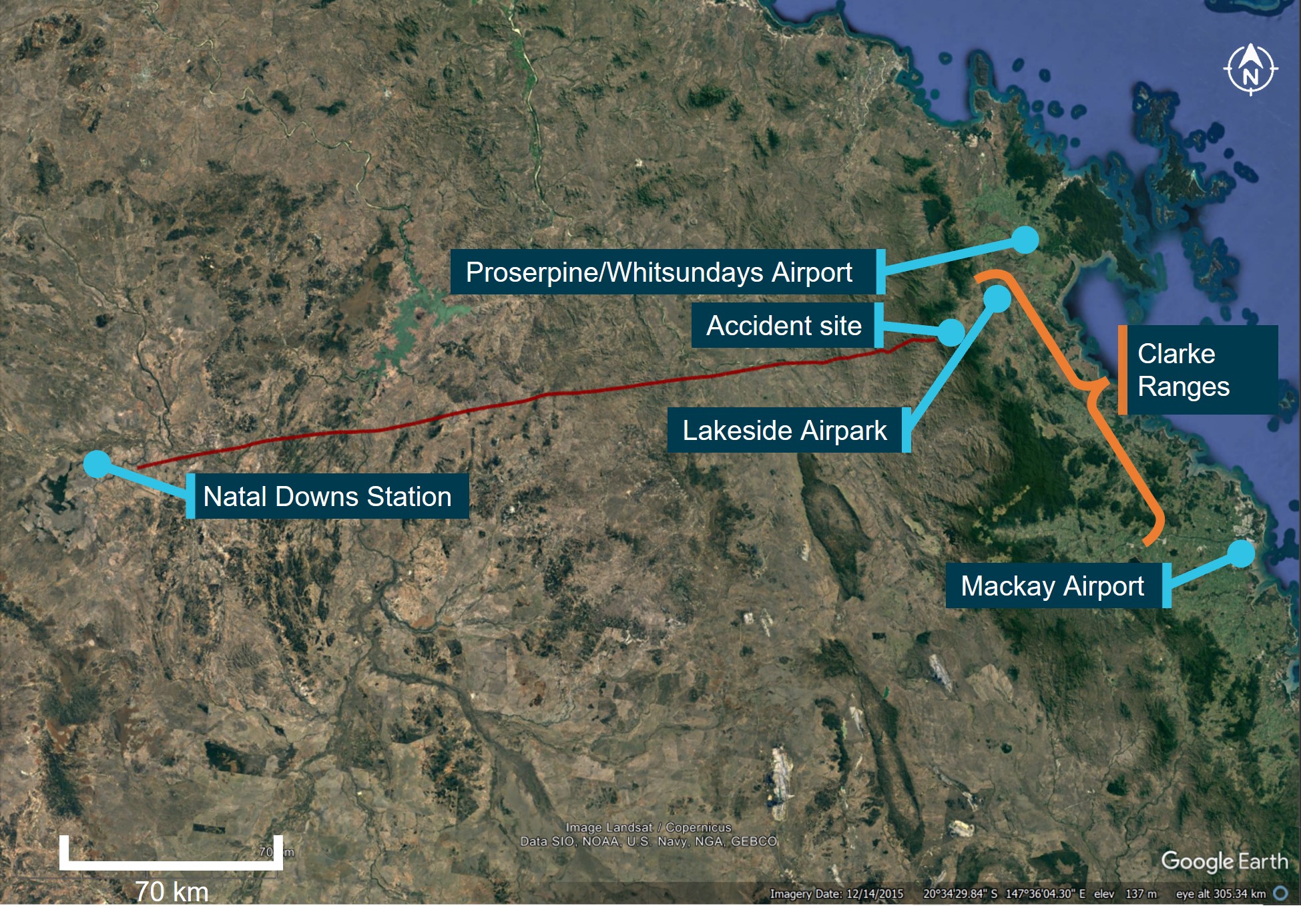
Figure 1: Flight profile showing recorded groundspeed
Source: Google Earth, annotated by the ATSB based on ADS-B data
The pilot declared an emergency and advised ATC that they were unable to make Archerfield Airport and would be conducting an off‑airport forced landing. With very limited suitable landing areas available (Figure 1), the pilot elected to leave the flaps and gear retracted to minimise drag to ensure they would be able to make the selected landing area.
At about 0605, the aircraft touched down in a rail corridor beside the railway line, and the aircraft’s left wing struck a wire fence. The aircraft hit several trees, sustaining substantial damage to the fuselage and wings (Figure 2). The pilot received only minor injuries in the accident and was able to exit through the rear door of the aircraft.
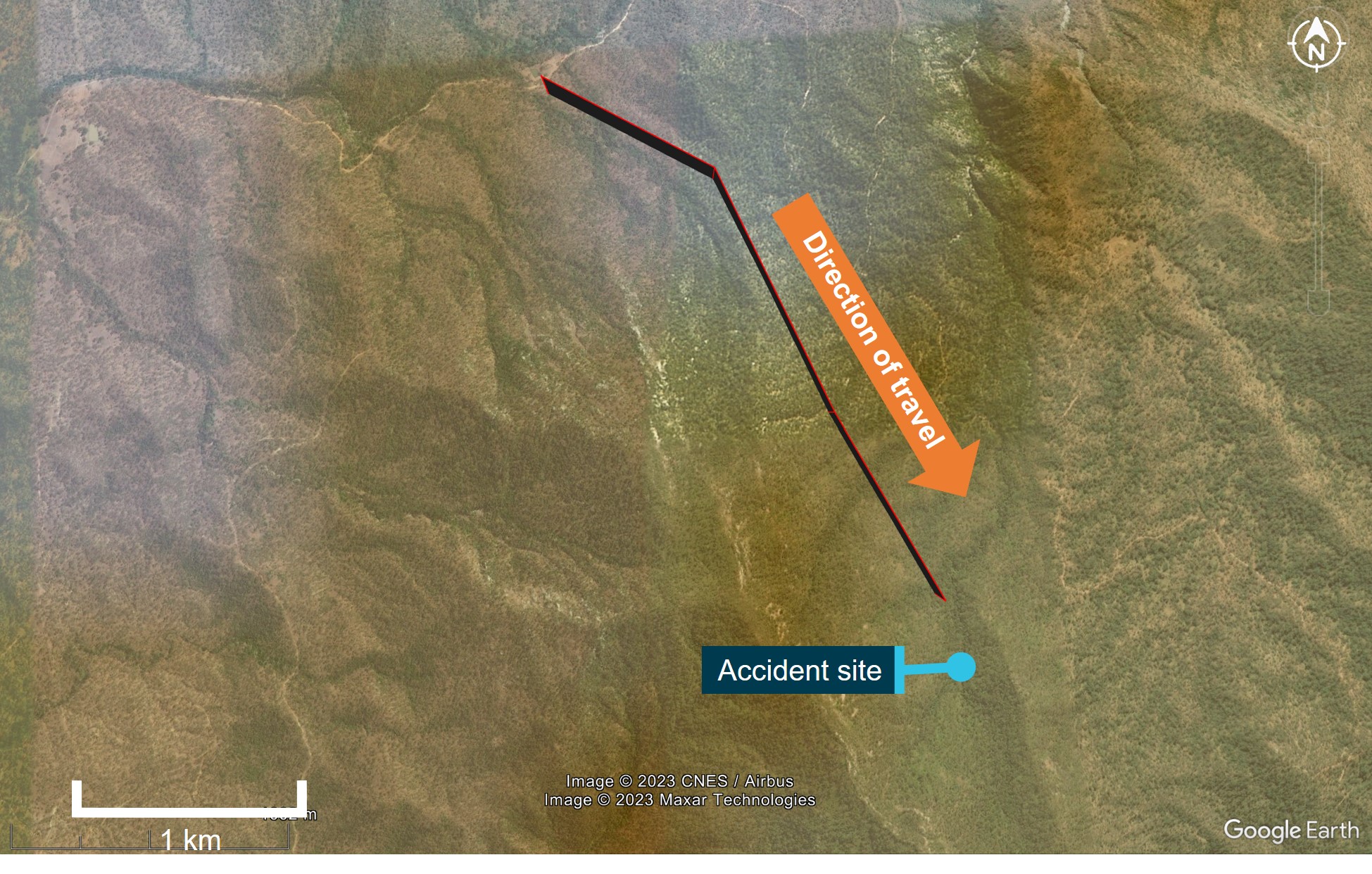
Figure 2: Accident site
Source: Queensland Police Service, annotated by the ATSB
Context
Pilot qualifications and experience
The pilot attained their commercial pilot licence (aeroplane) in 2020 and completed an instrument proficiency check on a multi-engine aircraft in May 2022. Both a line check and a proficiency check were completed with the operator on 9 January 2023, where the pilot was assessed as competent, and approved to conduct charter flights.
At the time of the accident, the pilot had 1,473 total flight hours, 233 hours on multi-engine aircraft, of which 204 hours were logged on Piper PA-31-350 type aircraft.
Aircraft information
Aircraft
VH-HJE was a Piper PA-31-350 ‘Chieftain’, light twin-engine aircraft, fitted with Textron Lycoming TIO-540 turbocharged piston engines. The aircraft was manufactured in the US in 1978 and was first registered in Australia in 1987. Air Link became the registered operator in July 2022.
The company operated 12 PA-31 aircraft. These aircraft all used the same operational data published in the operator’s piston engine aircraft flight crew operating manual. VH-HJE had been fitted with a Boundary Layers Research vortex generator kit. This kit increased the maximum permitted take-off weight, while lowering the minimum control speeds and stall speeds of the aircraft.
Operating instructions and performance figures were provided in a supplement to the aircraft’s pilot operating handbook. Discussion indicated the pilot was familiar with the supplement and its contents.
There were no on-board recording devices installed in VH-HJE that would have recorded engine indications or fuel system settings.
Fuel system
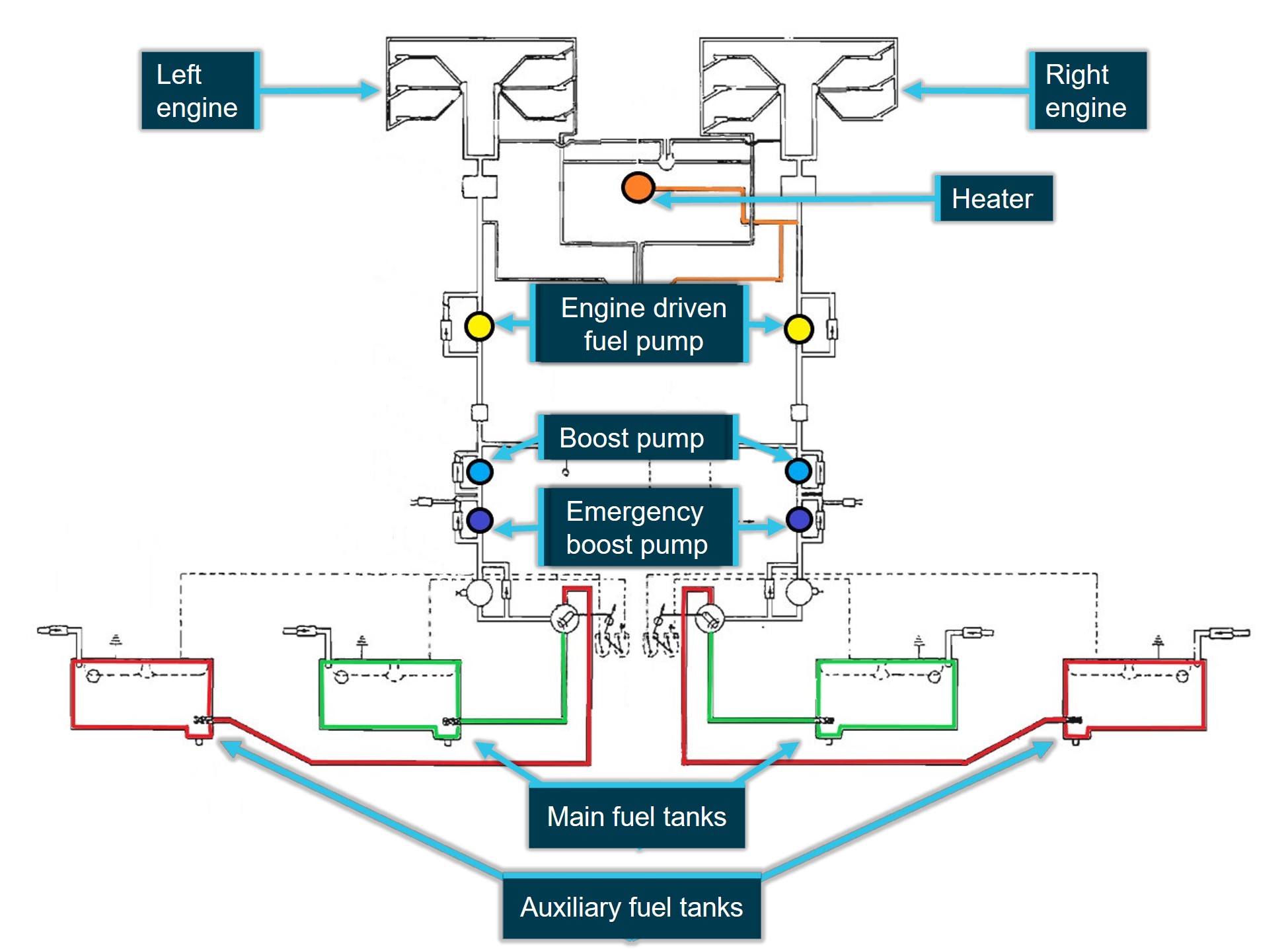
The aircraft contained 2 inboard main fuel tanks and 2 outboard auxiliary fuel tanks that provided a combined usable fuel quantity of 690 L of AVGAS. The fuel management controls were located on the fuel control panel between the front seats. The controls consisted of tank selectors, tank shutoffs and cross-feed controls.
The fuel controls in the cockpit controlled the left and right fuel tanks’ supply to their respective engines. Figure 3 shows the layout of the standard fuel system installed in the aircraft.
Figure 3: PA-31-350 Fuel system schematic
Source: Piper PA-31-350 pilot operating handbook, annotated by the ATSB
The pilot operating handbook contained operating instructions for the selection of tanks during various phases of flight. Due to the shape of the tanks and the location of the fuel outlet at the rear of the tanks, certain manoeuvres may cause the fuel to move away from the outlet increasing the likelihood of fuel flow interruption. To avoid this, the manufacturer published guidance around minimum quantities of fuel to be retained in each tank when manoeuvring. Further to this, inboard main tanks were required to be selected for take-off, climb and descent, with the auxiliary tanks only to be used during level co-ordinated flight in cruise. The operator adhered to the manufacturer’s guidance with the checklist in Figure 4 serving as a prompt to the pilot to ensure the inboard tanks were selected for descent.
The PA-31-350 was equipped with 3 fuel pumps each for the left and right fuel systems:
engine-driven fuel pump
fuel boost pump that operated when the electric master switch was turned on
emergency fuel pump that could be used in case of an engine‑driven fuel pump failure.
When fuel boost pressure was less than 3 psi, fuel boost pump warning lights located on the annunciator panel would illuminate.
Later build PA-31-350 aircraft are equipped with a left and right low fuel warning light that activates when the fuel level near the main tank outlet drops to a level where fuel flow interruption and power loss could occur. An engineering order had been obtained by a previous operator to modify the fuel system and remove these warning lights and associated hardware from VH-HJE due to the expense of replacing the fuel probes.
The engineering order included the following requirements:
amendment of the aircraft minimum equipment list to alert pilots of the system’s removal
the statement ‘Operating Procedures – During the flight, flight crew shall monitor the related fuel flow indicator’ shall remain in the minimum equipment list
a placard alerting the crew of the system’s removal shall be installed in the cockpit
this placard should be incorporated into the inspection schedule to ensure that it continues to remain legible.
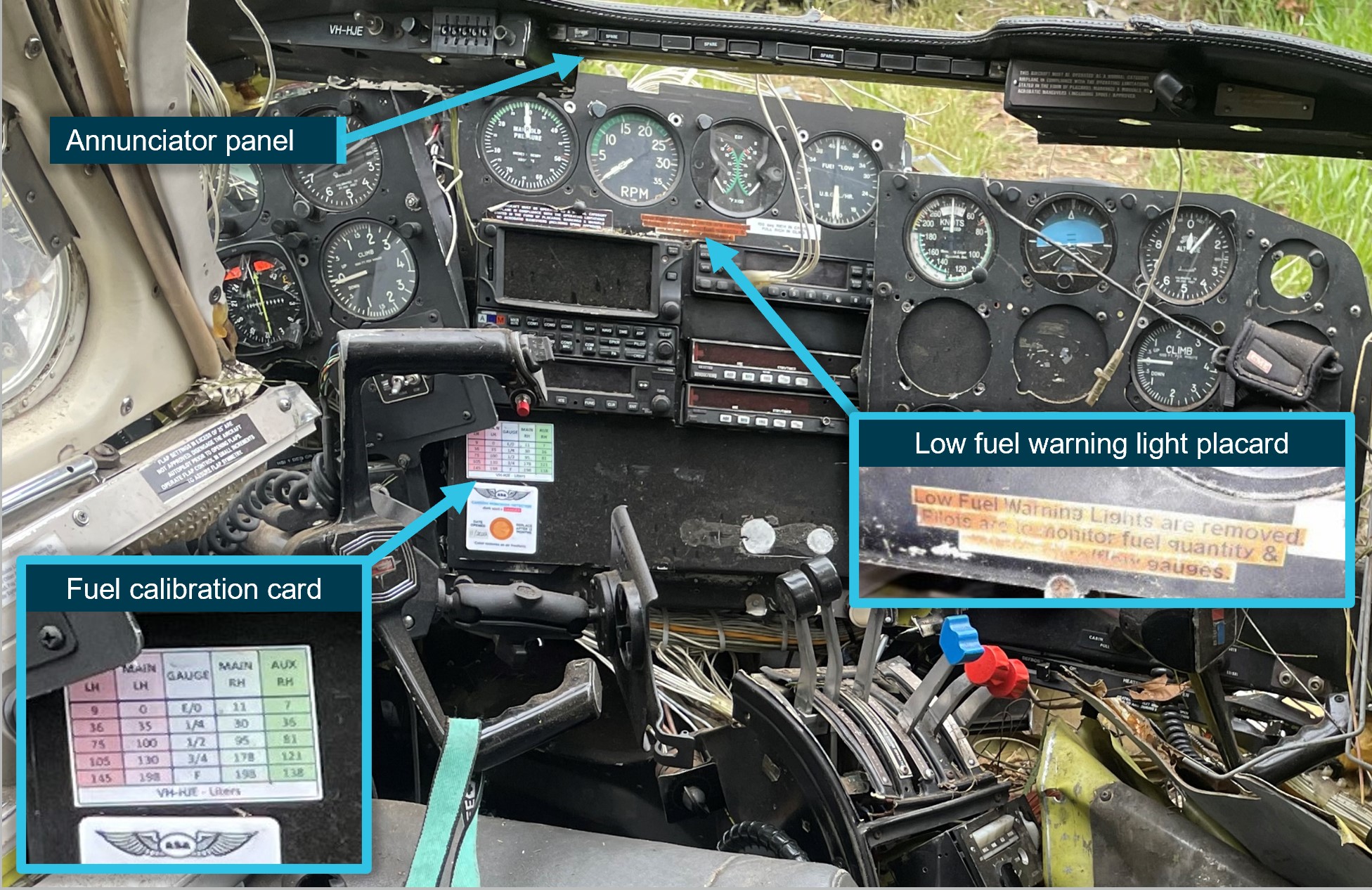
At the time of the accident, the warning system had not been reinstalled and a worn placard was installed in the aircraft (Figure 5).
This unique configuration was not reflected in the operator’s PA-31 minimum equipment list[7] where aircraft were required to have at least one low fuel warning light serviceable for flight. The only warning lights related to the fuel system on the annunciator panel in VH-HJE were the fuel boost pump warning lights that activated in response to low fuel pressure.
A fuel-burning heater was installed as part of the cabin heating, ventilating, and defrosting system. Fuel was plumbed into the heater from the selected right fuel tank. Based on pilot experience, the average consumption rate was estimated at 6 L/hr.
Figure 5: Cockpit
Image shows the low fuel warning light placard below the engine instruments, the annunciator panel that houses the light it refers to and the fuel calibration card on the instrument panel.
Source: Operator, annotated by the ATSB
Recent maintenance
VH-HJE was released from maintenance prior to the accident flight following work by engineers to rectify a defect with the autopilot. The intermittent defect produced uncommanded pitch events with significant nose-up and nose-down deviations while the autopilot was engaged in both pitch and altitude[8] modes. The autopilot received inputs from the aircraft’s attitude indicator, and during maintenance the attitude indicator was replaced. In addition to the requirements of the maintenance manual, the engineers also tested the autopilot’s response to in and out-of-level conditions prior to engine start to confirm it was performing as expected before the aircraft was returned to service.
Additionally, the right engine-driven fuel pump was adjusted following a report of the output pressure being at or near the minimum permitted for normal operations.
The operator advised that they had resting and maintenance facilities available at Bankstown airport. The pilot did not advise Bankstown engineering staff or the Archerfield base manager of the recurrence of the problem with the autopilot prior to the accident flight.
Engine-related procedures and guidance
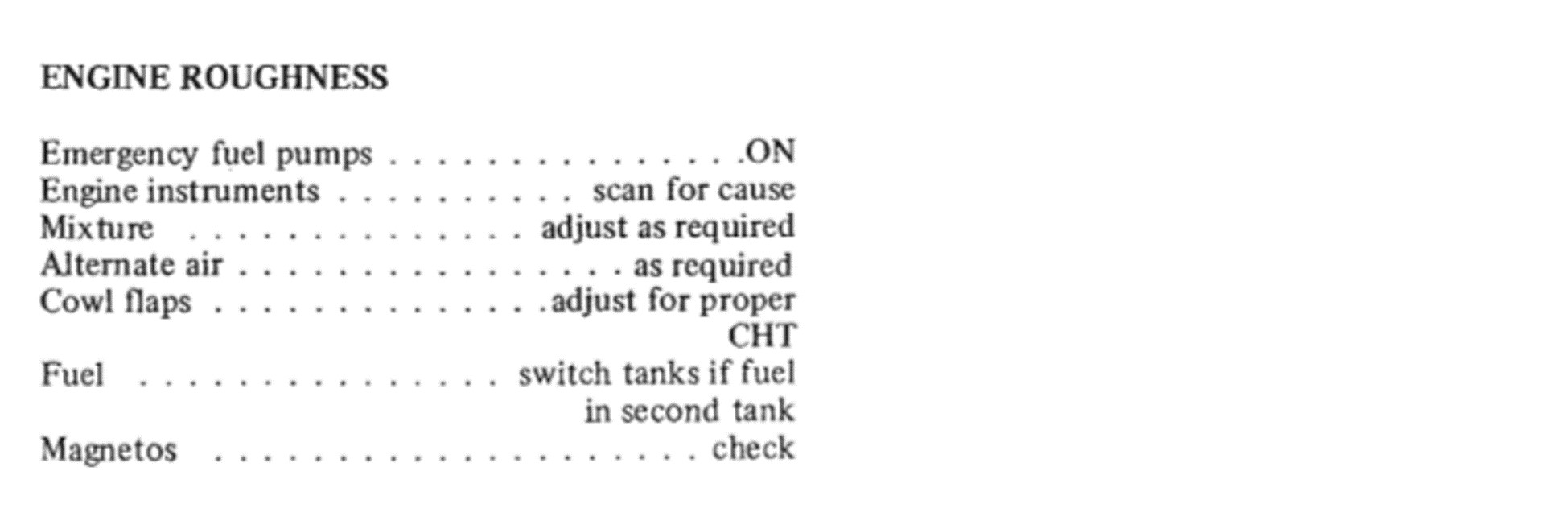
The aircraft pilot’s operating handbook (POH) contained emergency checklists including those for engine roughness (Figure 6) and an engine failure during flight (Figure 7).
Figure 6: PA-31-350 engine roughness checklist
Source: Piper PA-31-350 pilot operating handbook.
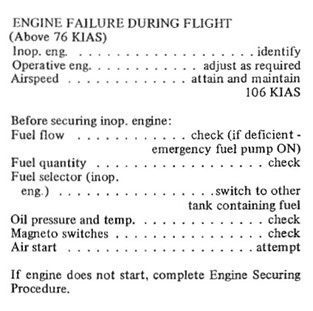
Figure 7: PA-31-350 engine failure during flight
Source: Piper PA-31-350 pilot operating handbook
If a multi-engine aircraft experiences an engine failure when airborne, there are two immediate aerodynamic effects; the yawing that occurs due to the asymmetric thrust from the engines, and the drag effect of the windmilling[9] propeller. To maintain directional control with an inoperative engine, the rudder must be deflected to counteract the adverse yaw.
The speed at which full rudder deflection can maintain a constant heading in combination with a 5 degree bank angle is defined, by regulations, as the minimum control speed and is referred to as velocity of minimum control in the air (Vmca). Vmca will vary depending on aircraft configuration. These criteria combine to give the published Vmca, which is a conservative example of when directional control will be lost (not the lowest possible speed where directional control will be lost). When Vmca occurs close to the aircraft’s stall speed, there is a reduced margin over the stall speed at which a departure from controlled flight will occur.
Examples of criteria that affect the actual minimum speed that directional control can be maintained include:
higher power settings (creates higher asymmetric forces)
windmilling propeller (increases asymmetric drag)
flap setting (likely configuration for phase of flight where potential Vmca issues are greatest and/or adds buffer over stall speed)
landing gear retracted (asymmetric drag potentially the greatest, no drag added by landing gear in accelerated airflow on the live side); and
centre of gravity (aft centre of gravity is the most unfavourable position).
The total yawing moment can be very large, particularly when the aeroplane is at high power and low speed such as during a take-off. For lower power settings and higher airspeeds, such as those used for descent, this aerodynamic effect will be less pronounced. While the drag from the failed engine remains, the thrust from the operating engine is less, and therefore the resulting yaw will be less noticeable and may reinforce the pilot’s perception of a partial power loss. Additionally, the increased airflow over the rudder surface during descent will make the rudder more effective and therefore easier to manage the adverse yaw from the failed engine.
As a rule, unless a catastrophic engine failure occurs, an engine does not just fail without warning. It should be noted that the rpm and manifold pressure gauges of a piston engine are not reliable means of identifying a failed engine, as the instrument indications may appear normal. After identifying the failed engine through, for example, the ‘dead leg, dead engine’ method, the pilot should confirm that their identification is correct. This is done by closing the throttle of the failed engine - if no yaw develops as the throttle is eased back, and the serviceable engine operates normally it confirms the identification of the faulty engine.
During an actual failure, pilots should also take the time to determine whether a total failure has transpired or if the engine is still delivering some power. If it is delivering power, use the thrust to get to a safe height before shutting the engine down to avoid further damage, unless a greater risk exists in continuing to operate the engine, such as fire, oil/fuel leaks or significant mechanical damage.
According to the POH checklist, if engine power could not be restored, the pilot was directed to the engine securing procedure. The key part of this procedure was to close the throttle of the inoperative engine and feather the propeller. On a multi-engine aircraft, feathering the propeller of a failed engine results in both a reduction in drag and a reduction in adverse yaw, vastly improving the engine-out handling characteristics and the engine-out flight performance of the aircraft. For the aircraft weight and environmental conditions, the one-engine climb performance published in the POH was a positive rate of climb of about 300 ft/min.
The engine manufacturer advised that for a windmilling inoperative engine, any change in throttle position would have an effect on indicated manifold pressure.
Closing the throttle would increase a vacuum (less MP) in the system, whereas opening the throttle plate would allow the induction system to equalise with atmospheric pressure.
At an altitude of about 3,000 ft, an indication of 27 inHg of manifold pressure is consistent with ambient atmospheric air pressure and explains the indications observed by the pilot with full throttle set.
The manufacturer advised that they did not provide any guidance for scenarios resulting from multiple simultaneous failures. The assumption being that the engines operate independently of each other with their own independent fuel systems. Both engines failing would be the result of multiple unrelated failures or the mismanagement of a common system. As such, they did not, nor were they required to, specify a power-off or recommended glide speed for the aircraft. The POH referred to power-off landings as a basic emergency procedure covered in normal flight training and recommended that these procedures were reviewed periodically to maintain proficiency.
Engineering inspection
The ATSB did not attend the accident site. Photos supplied by the Queensland Police Service and reports obtained by engineers who inspected the wreckage revealed the following:
both fuel selectors were found in the ‘auxiliary’ position
fuel selector mechanisms were serviceable
both emergency boost pumps were found in the ‘on’ position
less than 600 ml of fuel was found in each auxiliary tank that were undamaged
approximately 180 L of fuel was drained from right main tank
the left main tank drain valve was sheared off and no fuel was recovered
no residual fuel was found in the fuel system except for the airframe fuel filter
no foreign objects or debris were found in any of the fuel tanks
all fuel tanks were found to be intact with fuel tank flapper valves[10] operating freely.
Several engine components were sent away for independent testing. These included the engine‑driven fuel pumps, the emergency boost pumps, magnetos, and the fuel control units. The inspection found no evidence of a mechanical failure that would have precluded the normal operation of the engines at the time of the accident.
Additionally, engineers inspected various components with the following observations:
oil filters contained normal deposits
spark plugs were very clean indicating a potential lack of fuel
a limited internal inspection of cylinders appeared normal
right engine fuel control unit filter contained small non-magnetic slivers, possibly from one of the fuel pumps
left engine fuel control unit filter was clean
fuel nozzles were clear
both engine‑driven fuel pump drive shafts were intact
right engine turbo elbow was dislodged from the fuel control unit (suspected impact damage).
The advisory circular specified that an accurate fuel consumption rate was to be used to calculate the required fuel quantity for a flight. Aircraft‑specific data should be derived from a fuel consumption monitoring (FCM) system or the aircraft manufacturer’s fuel consumption data. The operator had an FCM system in place and monitored the fuel burn figures from in-flight trend records and flight logs against historical fuel consumption rates for the PA-31.
The operator’s fuel policy provided a consumption of 160 L/h for use across the fleet of PA-31 aircraft. This figure was derived from operational experience and considered a conservative figure to account for the various fuel consumption rates during the climb, cruise and descent phases of flight.
The operator’s flight crew operating manual (FCOM) for piston aircraft provided fuel flow figures specific to the climb, cruise and descent phases of flight. These fuel figures were taken from the POH and provided in US gallons per hour, in the same units of measurement found on the aircraft fuel gauges.
The company utilised AvPlan flight planning software. In addition to generating the flight plan based on imported weather and route details, the program also generated the fuel calculations for the flight. The program required separate fuel consumption rates for the climb and the cruise phases of flight. The operator advised that the fuel consumption rates uploaded into AvPlan were derived from company data, aircraft manual figures and trend monitoring of the aircraft fuel use, and were calculated to provide the same overall figure that would be obtained by calculations using the fuel policy fuel flow of 160 L/h for the PA-31.
The AvPlan fuel calculations for the accident flight and flight prior are provided in Table 1.
Table 1: VH-HJE flight planned fuel calculations
FROM
Archerfield
Bankstown
FUEL CALC.
Minutes
Litres
Minutes
Litres
Climb
17
62
15
55
Cruise
126
285
131
297
Altn
0
0
0
0
TRIP FUEL
144
347
147
352
Contingency
21
52
22
53
Final Reserve
45
109
45
108
Holding
0
0
0
0
Approach
0
0
Taxi
10
10
Fuel Required
210
518
213
523
Margin
81
172
77
167
ENDURANCE
290
690
290
690
Source: Data reproduced by the ATSB from the operator’s flight plan
The operator advised that all company PA-31 were equipped with a GPS featuring an in‑built fuel calculator and that this was a company‑approved means of cross-checking the quantity of fuel on board when in-flight. The pilot also confirmed that they regularly used this GPS feature and the calculator was used on the flight. This required the fuel policy fuel flow figure to be entered into the GPS fuel calculator, which then provided an estimated fuel required and fuel remaining figure in litres based on the flight time. Other means of determining fuel quantity on board when in-flight included:
calculated flight plan figures in litres
checking fuel quantity gauges against the aircraft’s fuel calibration card in gallons (Figure 5)
referencing the flight log against the aircraft fuel flow gauges presented in gallons.
Table 2 is based on the accident flight from Bankstown to Archerfield for VH-HJE on 7 April 2023. It shows the different fuel requirements when using the fuel policy consumption rate compared to the pilot’s flight plan calculated using AvPlan.
As part of the FCM system, any discrepancies greater than 3% of the planned fuel consumption were to be reported by pilots through the internal reporting system and investigated by the continuing airworthiness and maintenance manager. The operator advised that no fuel discrepancy reports had been made for this aircraft and the review process[12] had not identified any adjustment required to the PA-31 fuel consumption rate published in the fuel policy.
The ATSB conducted a review of the flights in VH-HJE between February 2023 and April 2023 for those flights where flight plans were provided by the operator. Analysis was limited to flights of the same route and of similar duration (+/- 0.1 hour flight time duration without evidence of a diversion). The AvPlan fuel calculations on the flight plans were compared to the recorded fuel burns in the company’s fuel log for VH-HJE. Of the 13 flight records of a similar duration, it was determined that 9 flights had fuel consumptions that were more than 103% of the AvPlan fuel calculation.
Fatigue
The pilot was employed by the operator on a casual basis and had recently commenced secondary ground-based employment with a different employer. The operator was aware of the secondary employment and advised this was very common, with the majority of casual pilots working a second non-aviation job. However, there was no requirement for casual aircrew to disclose secondary employment. As a result, there was no company oversight of hours worked outside rostered flight and duty times, and it was not considered when generating the pilot’s roster. The fatigue risk management manual outlined the operator’s expectation that pilots would notify the operator of a change in circumstances that may impact the pilot’s ability to meet the fatigue management obligations and that once provided with a roster, pilots would ensure they were fit for duty, making the necessary arrangements to facilitate the rostered shifts. Company pilots were provided with a roster a month in advance. A typical roster consisted of 2–4 flights per week with additional rostered duty periods for training.
Existing measures in place to ensure that fatigue was being managed included providing crew with appropriate rest opportunity prior to commencing a duty period and providing rest facilities at each base.
On the day of the occurrence the pilot reported waking at 1030 after obtaining 13 hours sleep. They worked a shift with their second employer from 1300 until 2130 before driving to the airport to prepare for the flight. The pilot advised that for the particular flight they were rostered to complete, they usually arrived at 2230 to allow time for planning and preparation. The duty period ran continuously from their arrival at 2230 until the accident at 0605 the following morning.
Using the information obtained at interview and the pilot’s roster, the ATSB conducted a fatigue analysis, including using biomathematical analysis software. From the fatigue analysis, the ATSB identified it was likely that the pilot was experiencing a level of fatigue shown to affect performance, predominately due to hours awake, sleep in the previous 24 hours and time of day. The additional employment shift was considered in the fatigue analysis to determine if it likely increased the estimated fatigue level of the pilot, and it was found to not have a significant influence.
Related occurrences
Fuel management and fuel starvation incidents and accidents continue to occur in twin engine aircraft. Examples of other ATSB investigations covering starvation related occurrences include:
Fuel starvation and forced landing involving Piper PA-31, VH-IHR, 22 km N of Mount Isa Airport, Qld, on 17 July 2008 (AO-2008-048).
Fuel starvation and forced landing involving Piper PA-28, VH-BDB, 15 km WSW of Bankstown Airport, NSW, on 19 September 2017 (AO-2017-094).
Fuel starvation involving Cessna 206, 3.5 NM NE of Aldinga, SA, on 3 February 2019 (AB‑2019-004).
Fuel starvation event involving Cessna 310, VH-JQK, near Sunshine Coast Airport, Queensland, on 18 August 2022 (AO-2022-040).
Keeping fuel supplied to the engines during flight relies on the pilot’s knowledge of the aircraft’s fuel supply system and being familiar and proficient in its use. Adhering to procedures, maintaining a record of the fuel selections during flight, and ensuring the appropriate tank selections are made before descending towards your destination will lessen the likelihood of fuel starvation at what may be a critical stage of the flight.
Safety analysis
As the aircraft was on descent into Archerfield the right engine failed. The pilot treated it as a partial power loss and continued without managing to restore power or secure the engine, and was unable to maintain altitude.
About 12 minutes later the left engine also lost power and the pilot was forced to make an off‑airport landing. Although the aircraft was seriously damaged during the landing, the pilot escaped with minor injuries.
The ATSB considered the factors that could have affected operation of both engines and pilot management of the emergency. Pilot fatigue and company procedures were also considered.
Engine power loss
In simple terms, engine power loss can occur in a PA-31-350 because of a mechanical defect, fuel contamination, or fuel exhaustion/starvation.
The operator examined the aircraft, and key engine and fuel system components were independently tested. As no defects were identified, the ATSB concluded that there was probably no mechanical factor in the loss of power to either engine.
With regard to the water identified after refuelling at Bankstown, given the fuel was drained until there was no water in the samples and the aircraft was operated on main tanks in the first part of the flight without incident, it is unlikely that fuel contamination was a factor.
Based on the fuel plan, fuel uplifted at Bankstown, and examination of the aircraft after the forced landing, there was sufficient fuel on board the aircraft for the planned flight from Bankstown to Archerfield. In that context, the ATSB considered fuel starvation.
The pilot reported operating on main tanks for take-off and climb, auxiliary tanks for cruise, then changing to the main tanks for descent. Based on the likely fuel consumed from each tank in this scenario using the company approved AvPlan generated fuel log that was available to the pilot, the ATSB calculated there would have been approximately 150 L of usable fuel in each main tank, and 15 L of usable fuel in each auxiliary tank when the engines lost power. In addition to this usable fuel, it would be expected that a quantity of unusable fuel would also be present, however, this was not consistent with the quantity of fuel recovered from the undamaged fuel tanks during the post-accident inspection. As such, if the pilot had moved the fuel tank selector back to the main tanks at the top of descent as was recalled, then there would have been sufficient fuel to complete the flight.
An alternative scenario is that the pilot overlooked changing the fuel tanks from auxiliary to main tanks at top of descent. In that case, the calculated total fuel remaining in each main tank would be approximately 175 L and there would be no usable fuel remaining in the auxiliary tanks. This is consistent with the quantity of fuel recovered from the undamaged fuel tanks. It is also consistent with the fuel system warnings and indications associated with each engine power loss.
The pilot recalled conducting the checks initially by memory and later by reference to the on-board checklist. Considering the time that passed between the check, actioning of the checklist item (fuel selectors), and the number of other tasks the pilot had to attend to, it is possible that the pilot became distracted and either missed the tank change or reversed a selection from the initial flow check.
Based on the determination that there was no fault found with the engines or fuel system that would have precluded the normal operation of both engines, it was determined to be likely that the pilot did not action the checklist items relating to the selection of main fuel tanks for descent, resulting in the change of tanks being missed and the engines being starved of fuel.
Diagnosis and management of the first engine power loss
In a fuel-injected piston engine, the key instrument indications of an engine failure are fuel pressure (if available), fuel flow, and EGT. Despite other indications that may be consistent with an operative engine, if fuel pressure, fuel flow and EGT are significantly low or zero, the engine will not be developing power. The pilot was aware that a fuel flow warning light had activated at the time of each engine power loss, and noted that fuel pressure and flow were zero, but did not appreciate the implications. Although the pilot assessed that the right engine was still producing some power, with zero fuel flow, it is almost certain that the right engine was no longer producing any power and the windmilling propeller produced significant drag for the remainder of the flight.
By continuing with an inoperative unfeathered engine, the pilot was not able to extract the maximum possible performance from the aircraft with the operative engine. Had the propeller been feathered, the aircraft would have been able to maintain height or even climb. While it could not be determined if this would have guaranteed the aircraft would reach Archerfield in the context of the impending left engine failure, it would have provided additional options to the pilot.
Having assessed that the right engine was operating at reduced power, the pilot was not prompted to conduct the engine failure checklist and instead conducted the rough running checklist. That checklist was not applicable and did not assist the pilot to identify and address the engine failure. Nevertheless, the rough running checklist prompted the pilot to scan the instruments and consider switching fuel tanks if there was fuel in the other tank. The pilot was aware there was a substantial amount of fuel in the main tanks and could have confirmed that the auxiliary fuel tank was essentially empty by reference to the fuel quantity indicating system. Because of the water that needed to be drained from the main tanks before flight, and in the absence of mechanical failure, the engine power loss resulted in the pilot hypothesising that the quality of fuel in the main tanks was the cause. This also resulted in the pilot not re-selecting the main tanks at this point. Without using the correct (engine failure) checklist, and with the suspicion about fuel quality, the pilot did not identify the fuel quantities available in each tank.
The ATSB noted that the low fuel warning light system had been removed from the aircraft. This system is essentially a low fuel quantity indication for each main tank and would not have provided a warning for low fuel flow from the auxiliary tanks. Given the substantial quantity of fuel found in the main tanks, the absence of this system was not a factor in this occurrence.
Diagnosis and management of the second engine power loss
The symptoms of the second engine power loss were consistent with fluctuating fuel pressure and flow. As was the case for the right engine, the pilot could have confirmed that the auxiliary fuel tank was essentially empty by reference to the fuel quantity indicating system.
Although continuous engine power was not restored, it is not clear if the left engine failed completely. If that had occurred, feathering the propeller as part of securing the engine would have had a significant benefit to the glide performance of the aircraft.
Fatigue
The International Civil Aviation Organization (ICAO) (2016)[13] defines fatigue as:
… a physiological state of reduced mental or physical performance capability resulting from sleep loss or extended wakefulness, circadian phase, or workload (mental and/or physical activity) that can impair a person’s alertness and ability to perform safety related duties.
At the time of the accident, the pilot had obtained 5 hours sleep in the prior 24 hours and was in a period of high workload. The pilot’s workload likely unexpectedly increased due to the need to manually fly the aircraft for extended periods during the flight, and therefore this would have likely increased the level of fatigue experienced by the pilot. The pilot was also making tank selection decisions during the window of circadian low (a period of maximum sleepiness between 0300–0500).
While the pilot had obtained 13 hours sleep in the night preceding the accident shift, that sleep period ended almost 20 hours earlier with no additional rest obtained prior to commencing the overnight shift. Although the additional employment shift was found to not have had a significant influence on the pilot’s fatigue, completing this shift removed the opportunity for the pilot to obtain additional sleep (through an afternoon nap) prior to commencing their night shift.
Fatigue can affect a variety of performance factors including problem‑solving and decision‑making. In this case it is likely that fatigue impacted the pilot’s incorrect tank selection as well as their ability to troubleshoot the loss of power.
Forced landing manoeuvring speed
Following the second unresolved power loss, it was apparent that a forced landing would be required. The aircraft manufacturer did not provide a glide speed for the PA-31 and the pilot was not aware of an airspeed that would have provided the best glide range. In this case, the airspeed did not have as much effect on performance as the drag produced by the windmilling propellers.
The ADS-B data showed that the aircraft speed reduced during manoeuvring and at times provided a small margin over the stall speed. Although the pilot considered that the aircraft speed could safely be reduced to Vmca, this should be considered in conjunction with the stall speed, especially while turning.
The pilot was able to maintain control of the aircraft and decided to limit drag by not extending flap and landing gear, to maximise the options available to them. The site selected minimised the risk of damage and injury to those on the ground and the controlled touchdown maximised the chances of survivability.
Company fuel documentation
The operator’s fuel policy and flight crew operating manual provided different sources of information relating to fuel flow in the PA-31 and presented these figures in both US gallons and in litres. While intended to be consistent, calculations using the 2 different fuel consumption figures did not always yield the same results.
Due to the requirement to depart with full fuel on flights between Bankstown and Archerfield, the difference in the fuel policy and flight crew operating manual fuel consumption rates was found to be inconsequential and therefore not a contributing factor to this occurrence. Despite this, the provision of fuel‑related data that may not be consistent with established consumption rates, or that increases the likelihood of conversion errors between units of measurement, increases the risk of a fuel related calculation error.
The operator’s fuel consumption monitoring system required company pilots to monitor the fuel consumed on flights and compare these quantities to the fuel plan, reporting discrepancies in excess of 3% of the flight planned figure. However, it was found that the operator was using the block fuel figure of 160 L/h in the fuel policy as the base rate for comparison. The fuel plan generated by the AvPlan software was found to generally provide lower total consumption figures than the fuel policy block figure. As the operator was using a higher consumption rate as the reference figure, fuel monitoring practices did not detect higher fuel burns than what was specified in fuel planning data.
The requirement to depart Bankstown with full tanks ensured an excess of fuel was carried. As a result, the fuel burn for the accident flight, while outside the permitted 3% discrepancy, was determined not to be a contributing factor to this occurrence. Of importance though, operating to a consumption higher than calculated may be significant when the AvPlan software is used to determine the operational limits for the aircraft.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the fuel starvation and forced landing involving Piper PA-31-350, VH-HJE, 11 km south of Archerfield Airport, Queensland, on 7 April 2023.
Contributing factors
It is likely that the pilot did not action the checklist items relating to the selection of main fuel tanks for descent. The fuel supply in the auxiliary tanks was subsequently consumed resulting in fuel starvation and loss of power from the right then left engine.
Following the loss of power to the right engine, the pilot misinterpreted the engine instrument indications as a partial power loss and carried out the rough running checklist but did not select the main tanks that contained substantial fuel to restore engine power, or feather the propeller. This reduced the available performance resulting in the aircraft being unable to maintain altitude.
When the left engine started to surge and run rough, the pilot did not switch to the main tank that contained substantial fuel, necessitating an off‑airport forced landing.
It is likely that the pilot was experiencing a level of fatigue shown to have an effect on performance.
Other factors that increased risk
As the pilot was manoeuvring for the forced landing there was a significant reduction of airspeed. This reduced the margin over the stall speed and increased the risk of loss of control.
Operator guidance material provided different fuel flow figures in the fuel policy and flight crew operating manual for the PA-31 aircraft type.
The operator’s fuel monitoring practices did not detect higher fuel burns than what was specified in fuel planning data.
Other findings
The forced landing site selected minimised the risk of damage and injury to those on the ground and the controlled touchdown maximised the chances of survivability.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Air Link
Following this occurrence, the operator issued a notice to aircrew and conducted a review of pilot training to include the recognition and management of fuel starvation. Company policy and flight planning software was reviewed to ensure consistency, and the Fatigue Management Manual was updated to include external employment and restrictions around hours of work and duty times.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of the accident flight
Air Link
the maintenance organisation for VH-HJE
the Queensland Police Service
the Civil Aviation Safety Authority
the Bureau of Meteorology
the aircraft and engine manufacturers.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot of the accident flight
Air Link
the Civil Aviation Safety Authority
the Bureau of Meteorology
the aircraft and engine manufacturers.
Submissions were received from:
Air Link
the Civil Aviation Safety Authority.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1]Flow checks: Flight-phase related actions are performed from memory following a cockpit flow pattern. Specific critical items are checked /cross-checked using a challenge-and-response checklist, whereby the pilot reads the items to be checked and confirms the proper status/configuration of the appropriate items.
[2]Yaw: the motion of an aircraft about its vertical or normal axis.
[3]All of the indicating range below the red line was colour coded green.
[4]Feathering: the rotation of propeller blades to an edge-on angle to the airflow to minimise aircraft drag following an in‑flight engine failure or shutdown.
[5]HJE was fitted with a vortex generator kit which lowered the minimum control speed in the air from 76 kt to 72 kt, and the clean configuration stall speed from 77 kt to 71 kt.
[6]Winds obtained from the aerodrome weather information service at 0551 local time indicated winds from 280 at 5 kt. The Meteorological Aerodrome Report (METAR) at the time of the accident indicated winds of 240 at 5 kt. Following the first turn to the right, this placed the wind behind the aircraft with about 4 kt of tailwind. For the ADS-B groundspeed of 75 kt, this meant the indicated airspeed would have been approximately 71 kt.
[7]A copy of this minimum equipment list was carried in VH-HJE.
[8]Pitch and altitude modes: Both are vertical navigation modes of an automatic flight control system, also known as an autopilot. Pitch mode maintains a constant attitude where altitude mode maintains a preset altitude.
[9]Windmilling: a rotating propeller being driven by the airflow rather than by engine power, and results in increased drag at normal propeller blade angles.
[10]Flapper valves are one-way valves installed in the fuel tanks that prevent backflow in the system.
[11]AC 91-15 does not require contingency fuel for IFR below 5,700 kg. Operator fuel policy includes a 15% contingency fuel.
[12]The operator’s review process involved calculations made by the Chief Pilot where monthly total fuel usage was divided by monthly total tacho time to arrive at an average fuel consumption rate per aircraft. This was then compared to previous figures to determine if the planned fuel rate needed to be adjusted.
[13]International Civil Aviation Organization, 2016, Manual for the oversight of fatigue management approaches, 2nd Edition.
Occurrence summary
Investigation number
AO-2023-017
Occurrence date
07/04/2023
Location
11 km south of Archerfield Airport
State
Queensland
Report release date
19/07/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Engine failure or malfunction
Occurrence class
Accident
Highest injury level
Minor
Aircraft details
Manufacturer
Piper Aircraft Corp
Model
PA-31-350
Registration
VH-HJE
Serial number
31-7852074
Aircraft operator
Air Link Pty. Limited
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
737 freighter returned to Perth after flight crew observed discrepancy between altitude and airspeed on the pilot and co-pilot’s indicators.
Investigation found that covers on the aircraft’s pitot-static probes had melted during maintenance.
Although the probes were cleaned, residue was found on probes after flight.
Incident highlights importance of maintaining high level of attention to damage and contamination when working on and inspecting these components.
The flight crew of a 737 freighter were presented with unreliable flight data information two days after the aircraft’s pitot probes were contaminated during maintenance, an ATSB investigation details.
The Airwork-operated Boeing 737 freighter, with four crew on board had departed Perth on 10 June 2022 for a freight service to Christmas Island, via Port Hedland.
As the aircraft was levelling off at 33,000 ft, the flight crew observed a 340 ft discrepancy between the altitude displayed on the captain’s altimeter, and the altitude on the first officer’s altimeter, which was connected to the autopilot.
The flight crew also observed discrepancies between airspeed and Mach numbers.
After descending to 30,000 ft and working through the relevant quick reference handbook, the flight crew established the first officer’s indications were reliable, and advised air traffic control of a need to return to Perth.
After an uneventful landing in Perth, ground crews found foreign residue adhered to the lower surfaces of all four of the aircraft’s pitot-static probes.
“The ATSB established that, during an engine ground run 2 days prior to the incident, the pitot‑static probe covers were not removed, and the automatic pitot heat was not isolated as required by the ground run procedures checklist,” said ATSB Director Transport Safety Kerri Hughes.
“As a result, the covers melted onto the probes. Although cleaned, residue remained on the probe surfaces, which had the potential to compromise the accuracy of the pitot-static instruments in-flight.”
However, as seven flights had been completed between the ground run and the incident flight with no altitude discrepancies reported during this time, the ATSB was unable to a establish a link between the remaining residue and the flight.
Irrespective, pitot probes are extremely sensitive to damage and disruption.
“Data received from an aircraft’s barometric air data sensing instrumentation components is critical for safe flight, and this incident highlights the importance of maintaining a high level of attention to damage and contamination when working on and inspecting these components.”
The ATSB report also notes the flight crew did not notify air traffic control of the altitude discrepancy of 340 ft.
“This discrepancy exceeded the 200 ft maximum allowed altimetry system error for the reduced vertical separation airspace in which they were operating,” Ms Hughes said.
“Flight crews need to advise air traffic control of altimetry system errors, so adequate vertical separation with other aircraft can be assured.”
Since the incident, the maintenance organisation has undertaken several procedural initiatives to reduce the likelihood of melted pitot-static probe covers in the future, including replacing the polyvinyl chloride covers with high temperature resistant Kevlar covers.
An overstress fracture, shortly after take-off, led to the separation of the tail rotor gearbox from the helicopter, and the subsequent separation of the aft tail section;
Pilots had previously reported experiencing vibrations in the helicopter’s tail rotor pedals;
Investigation highlights that aircraftshould not be returned to service until known issues are rectified, and that a conservative approach to troubleshooting mechanical issues and return to service should be taken to minimise risk
An ATSB investigation into a fatal helicopter accident that occurred shortly after take-off from a yard in a Broome industrial suburb highlights the crucial importance of pilots formally declaring their helicopters to be unserviceable when the source of unusual vibrations has not been identified and rectified.
On 4 July 2020, a Robinson R44 helicopter with a pilot and three passengers on board conducted a vertical departure from an industrial property at Bilingurr, 3 km north of Broome Airport, to conduct a private joyflight. As the helicopter climbed clear of obstacles and transitioned to forward flight, witnesses on the ground heard a loud bang, and observed the helicopter’s empennage and tail rotor system separate and break away.
The helicopter continued to climb and commenced rotating to the right with increasing angular velocity, before control was lost, and it impacted a road on its right side. The pilot and the passenger, who were seated on the right side of the helicopter were fatally injured. The two passengers who were seated on the left side of the helicopter sustained serious injuries.
“The ATSB found that an overstress fracture of the tail rotor gearbox’s input cartridge occurred following a period of vibration in the helicopter’s tail rotor pedals,” said ATSB Chief Commissioner Angus Mitchell.
“This overstress fracture, shortly after take-off, led to the separation of the tail rotor gearbox from the helicopter, and the subsequent separation of the aft tail section.”
The ATSB’s investigation report notes the helicopter’s two previous flights were conducted by two separate pilots (including the accident pilot, who was also the helicopter’s owner), who both reported experiencing vibration in the helicopter’s tail rotor pedals.
In response the owner requested that their local approved maintenance organisation assess the vibration. Engineers from the maintenance organisation assessed the helicopter in the yard on the afternoon of 3 July. They found the tail rotor balance to be within limits, and a close inspection of the tail cone, tail rotor and empennage of the helicopter detected no issues. Further, no vibration in the pedals was detected during ground running of the helicopter in the yard.
Nonetheless, the maintenance engineer reported wanting a pilot to fly the helicopter to determine if the reported vibration in the pedals was detectable in flight.
However, while the requirement for a maintenance check flight was not recorded on the helicopter’s maintenance release, the owner of the maintenance organisation advised the ATSB that they advised both the owner and the pilot who first detected the vibrations of the requirement to fly the helicopter to provide more information. Friends and family of the owner of the helicopter stated that no request for further flight was made.
“As the vibration was reported to only occur in flight, and no defect was identified, it was reasonable to have concluded that the problem may still be present,” said Mr Mitchell.
“As such, the safest next step, which is recommended by the helicopter manufacturer, would be to conduct a graduated flight check of hovering then re-inspection. Preferably, this would be with only a prepared pilot on board.
“Instead, the next flight, during which the accident occurred, involved the conduct of a high‑power towering take-off from a confined area with 3 passengers on board.”
The investigation report notes that the registered operator of an aircraft has ultimate responsibility for its airworthiness.
“This accident demonstrates the importance of following a conservative troubleshooting process that minimises risk.”
Mr Mitchell noted that while the source of the loading that led to the overstress fracture was not conclusively determined, the pilot’s operating handbook for the R44 helicopter states that the onset of unusual vibrations can indicate impending failure of a critical component.
“The pilot’s handbook states that pilots should land as soon as possible and formally declare the helicopter unserviceable.
“Crucially, the helicopter should not be returned to service until the source of the vibration, both on the ground and airborne, has been found and rectified.”
Mr Michell also noted that private pilots do not, unlike commercial and airline pilots, have the benefit of regular flying and frequent training and checking.
“The ATSB recommends private pilots to not rely on the minimum training and checking and training currency requirements to keep safe, and that they assess their risk profile and seek opportunities to maintain and develop their skills with a flight instructor.”
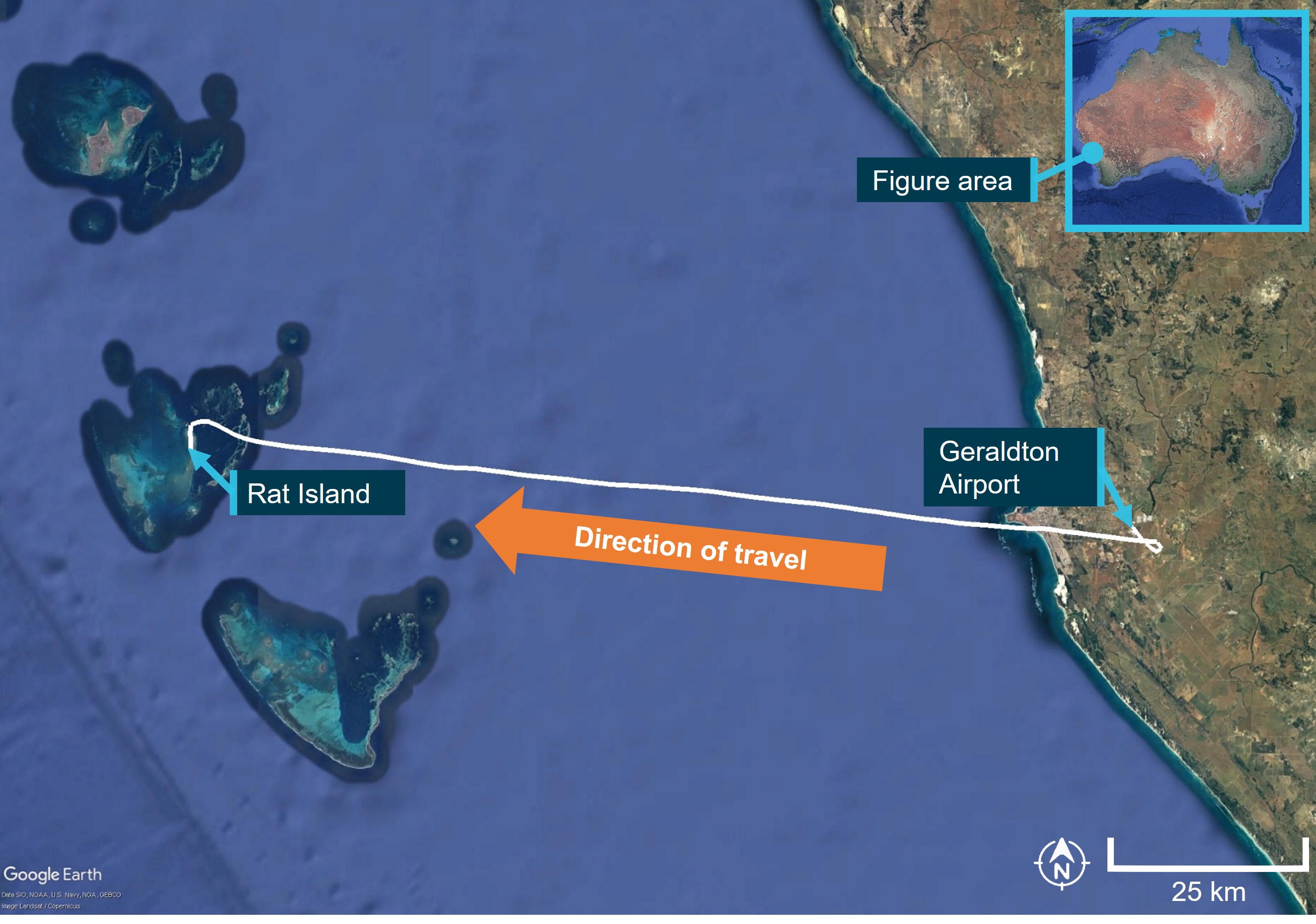
On the morning of April 6 2023, a chartered GippsAero GA8 Airvan, registered VH‑TBU and operated by Shine Aviation Services, took off from Geraldton Airport to Rat Island aircraft landing area in the Houtman Abrolhos Islands, Western Australia. A pilot and 6 passengers were on board.
During the landing on runway 18, the aircraft did not stop before the edge of the island and tipped into shallow seawater. The pilot and passengers were uninjured. The aircraft was substantially damaged.
What the ATSB found
The ATSB found that the aircraft was unstable during the approach due to excessive height and airspeed. During the landing, the aircraft floated for a significant time and touched down approximately halfway down the runway, with insufficient remaining runway to stop. While the pilot recognised opportunities to conduct a go-around when they determined they were not on the correct approach profile, this was not conducted.
Finally, the ATSB found that the pilot was possibly experiencing fatigue at a level known to affect human performance, due to a combination of restricted sleep and insufficient sustenance.
What has been done as a result
Shine Aviation Services has taken safety action to improve pilot landing and late‑stage go‑around training for their single‑ and multi‑engine piston aircraft. An increased oversight program has also been implemented to provide more regular mentoring for junior flight crew.
Safety message
This incident highlights how an unstable approach can contribute to the risk of a runway excursion. Pilots should be prepared to conduct a go-around if the stabilised approach criteria are not met. The later the decision to go-around is made, the more likely that additional hazards will be present for pilots to manage.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 6 April 2023, a GippsAero GA8 Airvan registered VH-TBU and operated by Shine Aviation Services was being used on a chartered passenger flight. The aircraft departed Geraldton, Western Australia at 0814 local time on a flight to Rat Island in the Houtman Abrolhos Island chain, Western Australia (Figure 1). Onboard were the pilot and 6 passengers.
Figure 1: Flight track of VH-TBU
Source: Google Earth and flight track, annotated by ATSB.
After cruising at 2,600 ft, the aircraft approached Rat Island and joined an extended base leg of the circuit for runway 18.[1] The pilot made a left turn onto final and extended the flaps to 38°.[2] Coming out of the final turn, the pilot noticed that the aircraft was higher than normal. Consequently, they reduced the engine power to idle and lowered the nose of the aircraft to intercept the normal approach profile. The pilot advised the aircraft’s airspeed increased to approximately 85 kt at this stage, before reducing to a little higher than normal over the threshold (see the section titled Stabilised approach criteria).
During the landing, the aircraft floated significantly more than the pilot expected, with the aircraft touching down about 247 m beyond the threshold (Figure 2). The pilot recalled ‘jumping on the brakes’ as soon as they touched down, and then realised that the aircraft could not be stopped before the runway end. In response, they applied left rudder in an attempt to avoid entering the water in the overshoot. The aircraft traversed the runway overshoot area, coming to rest on the island’s edge, before tipping forward into shallow seawater at about 0841 (Figure 3).
Figure 2: Rat Island runway and flight path of VH-TBU
Source: Google Earth and flight track, annotated by ATSB.
Water entered the cockpit to about ‘shin-height’ and the passenger seated in the rear left seat opened the emergency exit upon recalling the instructions from the safety briefing. All 6 passengers evacuated the aircraft through the rear left door. The pilot evacuated through the left cockpit door, walking across the wing strut onto land (Figure 3).
Neither the pilot nor 6 passengers were injured during the landing or evacuation. The aircraft sustained substantial damage to the nosewheel, propellor, right landing gear and cargo pod, and remained partially submerged for several days before being airlifted back to Geraldton.
Figure 3: VH-TBU accident site
Source: Shine Aviation Services, annotated by ATSB.
Context
Pilot information
The pilot held a commercial pilot license (aeroplane) with an instrument rating, and a class 1 aviation medical certificate. They had a total of 789.7 hours flying experience, of which 157.4 hours were operating the GA8 Airvan. The pilot had experience flying a variety of single‑ and multi-engine piston aircraft during island operations. They had been flying for the operator for about 12 months and had flown to Rat Island many times.
The pilot had passed an instrument proficiency check (IPC) in February 2023 and operator proficiency check (OPC) in September 2022, which included satisfactory results in conducting a missed approach/go‑around. [3]
Aircraft information
The GA8 Airvan is a single engine aircraft manufactured by GippsAero[4] of Victoria, Australia. It is fitted with a Textron Lycoming IO-540-K1A5 piston engine and can seat up to 8 people, including the pilot. VH-TBU was manufactured and registered in 2002. It was owned and maintained by the operator.
The aircraft was maintained in accordance with the GA8 service manual and had a current maintenance release. The last periodic inspection was in March 2023, and the aircraft had accumulated about 3,256.7 total hours in service.
The aircraft’s maintenance records showed an open observation recorded 2 weeks prior to the occurrence that the pilot seat was difficult to adjust. Prior to the flight, the pilot had detected this and decided it would not affect their ability to control the aircraft. During the flight, the seat was set fully aft, 1–2 increments further back than the pilot’s normal seat position. They later observed that, with the seat further rearward than normal, they could not fully depress the brake pedals.
After the accident, the ATSB received photographs of the aircraft and identified evidence of previous low hydraulic fluid in the left brake master cylinder. This was recorded to have been topped up 3 weeks prior to the occurrence, after a report of sponginess [5] on the left brake. It was unclear if this was the case at the time of the accident, although evidence of wheel skidding was observed on the runway surface after this occurrence.
Rat Island aircraft landing area
Rat Island aircraft landing area (ALA) was managed by the Western Australian Department of Biodiversity, Conservation and Attractions (DBCA). It had one unsealed runway aligned 180/360° and was about 517 m long and 30 m wide, with no significant slope. The windsock was located at the northern end, and there was a 20 m rocky overrun area at the end of runway 18. DBCA reported that improvements had been made to the overrun surface area in August 2022. The airstrip was suitable for GA8 operations.
Meteorological information
Rat Island did not have a dedicated Bureau of Meteorology (BOM) weather station. Weather observations at North Island weather station, about 50 km north of Rat Island, showed that 10 minutes prior to the runway excursion, winds were 110°, varying between 9 to 13 kt.
The pilot reported that the conditions on Rat Island favoured runway 18 with a slight headwind, which was usual for this area. They were unable to recall the direction of the windsock, and it was not captured on the passenger video recording (see the section titled Recorded data). The runway was dry.
Stabilised approach criteria
The operator required that if a VFR aircraft was not stable by 500 ft above the touchdown point a go‑around was to be conducted. The following stabilised criteria was outlined in their policy and procedures manual:
the aircraft is on the correct lateral and vertical flight path
descent rate is less than 1,000 ft per minute
bank angle is less than 10°
the aircraft is in the correct landing configuration
the aircraft is at approach speed (Vref to Vref +10) [6]
power setting is appropriate for the configuration
conditions landing checklist has been completed
The operator’s policy and procedures manual also stated:
If at 50 ft altitude, the aircraft airspeed is in excess of the planned threshold speed plus 10 kts then a go-around is mandatory.
The GA8 flight manual noted that for approach and landing:
Excessively high approach speeds will result in prolonged floating and increased landing distance.
The pilot reported being familiar with the stabilised criteria, and a general rule of thumb to conduct a go-around if the wheels had not touched down by the first third of the runway when using a shorter runway.
The standard approach into Rat Island for the GA8 at maximum take‑off weight was a standard approach angle of 7° at idle power. Pilots were instructed to employ a short-field landing to cross the threshold at a maximum airspeed of 70 kt, and upon touchdown, retract the flaps, applying firm brake application and back pressure on the control column to allow the full weight of the aircraft onto the runway for maximum braking effectiveness. Calculations for the distance required to land a GA8 aircraft with a 3 kt headwind indicated that from 50 ft overhead the threshold, it would need 410 m of runway to stop, including a ground roll of 170 m.
Recorded data
The operator supplied flight data and a passenger took a video recording of the landing and runway excursion on their mobile phone. This passenger was sitting in the front right seat, and primarily videoed in the direction of travel out the lower right corner of the windscreen. This information was used to conduct a flight path analysis of the approach and landing. The flight analysis revealed that from the start of the video recording to the 50 ft point on the approach, the average approach angle was about 10º.
At 50 ft altitude on final, and about 70 m from threshold, the aircraft was travelling at a groundspeed of 88 kt. At the runway threshold (about the landing aim point), the aircraft was about 21 ft above ground level (AGL) and was travelling at a groundspeed of 86 kt. After the flare, the aircraft floated for about 170 m, and touched down approximately 247 m beyond the threshold, travelling at a groundspeed of 77 kt. It was at this point that the pilot reported that the airspeed was slightly below the aircraft’s Vref speed of 70 kt. The aircraft exited the overrun area at a groundspeed of about 43 kt. Full flaps remained deployed during the landing sequence.
Work schedule
The pilot was rostered for a flight duty period (FDP) [7] between 0530–1800, with a split-duty rest period from 1000–1400 for sleep at home, which was 15 minutes commuting time away. They were to then sign on again at 1530. They had flown a return trip from Geraldton to East Wallabi Island earlier that morning, and had flights scheduled at 1600 and 1700 later that day. They were working their third day after 3 days off.
Fatigue
The pilot reported waking at 0400 that morning after about 5.5 hours of sleep, and about 11 hours of sleep in the previous 48 hours. The pilot had been awake for about 5 hours prior to the occurrence. Usually, they would be asleep by 2200 for this sort of work schedule, but they reported that on that night they struggled to fall asleep until about 2230.
The pilot reported their mental fatigue at the time as ‘a little tired, less than fresh’, and that while they had packed a banana and muesli bar to eat that morning during their shift, they had left them behind. They reported having had their last meal around 1700 the day before.
Previous similar occurrences
There have been 62 runway excursions in the last 4 years at ALAs across Australia. 11 of these occurrences resulted in 14 injuries: 9 minor injuries to crew, 1 serious injury to a passenger and 4 minor injuries to passengers. Of these, 2 occurrences were at the Abrolhos Islands.
The ATSB investigated 6 of these 11 occurrences.
Safety analysis
Despite the pilot identifying that the approach profile was steeper than normal and taking action to remedy the situation, flight analysis indicated that the aircraft arrived at the threshold both high and fast. The ATSB considered whether the seating position may have affected the pilot’s approach perspective. However, given they identified the steep profile, any significant effect was considered unlikely. The aircraft then touched down well into the runway at a recorded groundspeed of 77 kt, with the pilot recalling that the aircraft’s airspeed was slightly below Vref (70 kt). This indicated that the landing was conducted with a tailwind component.
It was considered unlikely that the braking capacity of the aircraft was affected by the seating configuration or low hydraulic fluid in the brake master cylinder. There were skid marks along the runway surface where the brakes had been applied and locked the wheels. While this indicates that full brake application was available, the locked wheels would have provided less stopping effectiveness than if the braking had been modulated to remain on the threshold of locking and the flaps retracted on touchdown. These elements, in combination with the long landing and groundspeed detailed above, meant that the pilot was unable to stop the aircraft before it entered the water.
There were opportunities to conduct a go-around prior to landing and during touchdown. The pilot recalled considering a go-around as they pushed the nose down to intercept the approach profile and the speed increased more than expected, however they advised that they expected to regain the correct profile and airspeed prior to landing. They also considered conducting a go‑around as the wheels made contact with the runway. However, having assessed that the airspeed was below the take-off speed of 70 kt, they were concerned that there was a risk of stalling over the water.
Fatigue is a known factor that can impair decision making and reduce reaction time. There was evidence that the pilot was possibly experiencing mild to moderate acute fatigue at the time of the occurrence. This was due to a combination of some restricted sleep in the previous 24 and 48 hours, and lack of sustenance that morning. However, it is difficult to conclude whether fatigue impaired the pilot’s actions in response to identifying the unstable approach and electing not to conduct a go-around. The ATSB reviewed the operators’ procedures for sleep arrangements during split shift duty periods and found that sign-on and sign-off times accounted for commuting time and aircraft preparation between scheduled departures.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the runway excursion, involving GippsAero GA8 registered VH-TBU, that occurred at Rat Island, Western Australia on 6 April 2023.
Contributing factors
The aircraft was unstable during the approach and landed approximately halfway down the runway with insufficient remaining runway to stop.
The pilot did not conduct a go-around, as required by the operator, when they identified the aircraft was not stabilised during the latter stages of the approach.
Other findings
The pilot was possibly experiencing fatigue at a level known to affect human performance, due to a combination of restricted sleep and insufficient sustenance.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Shine Aviation Services
As a result of this occurrence, the operator has advised the ATSB that they have taken the following actions:
implemented late stage go-around training for pilots operating to the Abrolhos Islands
implemented an increased oversight program for junior pilots and reviewed the non-technical skills syllabus
amended training packages to clarify the aircraft flap retraction policy upon landing
implemented anti-skid training into an appropriate location within training material
included aircraft performance items into the line training syllabus for their single‑ and multi‑engine aircraft
reviewed average pilot commuting times to improve the scheduling of rest periods and sleep periods for split duty times
improved operational procedures to clearly define minimum turnaround times, minimum sign‑on and sign-off times
reviewed the aircraft performance manual to ensure referenced material was up to date
Sources and submissions
Sources of information
The sources of information during the investigation included:
the pilot of the accident flight.
a passenger of the accident flight.
video footage of the accident flight and other photographs and videos taken on the day of the accident.
recorded data on the aircraft.
Shine Aviation Services.
Bureau of Meteorology (BOM).
References
Gippsland Aeronautics (2019). GA8 Flight Manual. CASA Amendment 54. C01-01-03
Gunston, B. (2004). The Cambridge aerospace dictionary. Cambridge University Press.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the pilot
Shine Aviation Services
Civil Aviation Safety Authority
United States National Transportation Safety Board
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Runway number: the number represents the magnetic heading of the runway.
[2] This was the full flap setting required for the GA8 to achieve the factored landing roll required for Rat Island at the maximum landing weight of 1,814 kg.
[3] Go-around: A standard aircraft manoeuvre that discontinues an approach to landing.
[4] The manufacturer was previously known as Gippsland Aeronautics.
[5] Compressibility within the braking system requiring greater‑than‑expected pedal application to achieve effective braking.
[6] Vref: the reference landing approach speed. For the GA8 at idle power and full flap this was 70 kt.
[7] Flight Duty Period (FDP): A period of time that starts when a person is required, by an operator, to report for a duty period in which they undertake one or more flights as part of an operating crew and ends at the later of either the person’s completion of all duties associated with the flight, or the last of the flights; or 15 minutes after the end of the person’s flight, or the last of the flights.
Occurrence summary
Investigation number
AO-2023-016
Occurrence date
06/04/2023
Location
Abrolhos Rat Island
State
Western Australia
Report release date
25/10/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway excursion
Occurrence class
Accident
Highest injury level
None
Aircraft details
Manufacturer
Gippsland Aeronautics Pty Ltd
Model
GA-8
Registration
VH-TBU
Serial number
GA8-02-011
Aircraft operator
Shine Aviation
Sector
Piston
Operation type
Part 135 Air transport operations - smaller aeroplanes
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation. The statement is published as a report in accordance with section 25 of the TSI Act, capturing information from the investigation up to the time of discontinuance.
Overview of the investigation
The occurrence
On 3 April 2023, the ATSB commenced a transport safety investigation into a fatal accident involving a Piper Aircraft Corp PA-28-180 aircraft, registered VH-PXR, about 26 km west of Lakeside Airpark, Queensland.
On 2 April 2023, at about 1530 local time, the pilot and passenger departed Natal Downs Station for a private flight to the Lakeside Airpark (Figure 1). The automatic dependent surveillance-broadcast data recorded the aircraft climbing to, and cruising between 6,000 ft and 6,500 ft above mean sea level while tracking easterly towards the Clarke Ranges. At about 1633, the aircraft was descended and then maintained an altitude between 2,000 ft and 2,500 ft. At about 1651, when in the vicinity of high terrain, the aircraft was turned onto a south-easterly direction for 1 minute. The final recorded position was about 250 m north-north-east of the accident site at about 2,150 ft (about 250 ft above ground level) (Figure 2).
Figure 1: Map with key locations and flight path (red)
Source: Google Earth and Airservices Australia, annotated by the ATSB
Figure 2: Last recorded flight path
Source: Google Earth, annotated by the ATSB
When the aircraft did not arrive at the Lakeside Airpark at the expected time, a search and rescue operation commenced. The following day, the aircraft wreckage was located on a steep slope at 1,913 ft. The pilot and passenger were fatally injured and the aircraft was destroyed.
Pilot information
Experience and qualifications
A review of records established that the pilot did not hold a Civil Aviation Safety Authority (CASA) aeroplane pilot’s licence (either a Recreational Pilot Licence or Private Pilot Licence) required to conduct the flight. The pilot also did not hold a Recreational Aviation Australia pilot certificate.
Records from the flying school where the pilot trained showed that they had completed 30.4 hours of flight instruction (25.4 hours dual and 5.0 hours solo) between November 2021 and November 2022. This included 2.9 hours on the Piper PA-28-180 aircraft type. During this time, the pilot completed the practical requirements to obtain a CASA recreational pilot licence but had not completed the flight or theory tests required to have the licence issued. It was reported by the flying school that the pilot intended to continue with training to attain a CASA Private Pilot’s Licence (Aeroplane), and this was the reason no testing had been completed. The training records also showed that the pilot had completed one navigation theory lesson towards this licence. No further records of flying training or other flying experience was available.
The pilot became the registered owner of VH-PXR in November 2022. The ATSB could not determine how many hours experience the pilot had in the aircraft. Information obtained by the ATSB detailed that the pilot had flown around the area around Natal Downs station in the aircraft. In addition, the automatic dependent surveillance-broadcast data recorded a previous return flight in the aircraft from Natal Downs Station to Lakeside Airpark about 1 week prior to the accident.
In suitable weather conditions, the planned flight from Natal Downs Station to Lakeside Airpark could have been flown in visual flight rules[1] conditions by a pilot holding a CASA Recreational Pilot Licence with a navigation endorsement.
Medical information
The pilot was issued with a Class 2 Aviation Medical Certificate in January 2023. The ATSB reviewed the pilot’s aviation medical records, which noted that they had previous, and ongoing medical conditions. The ATSB corresponded with CASA, who advised that they had considered this information in the issue of the pilot’s medical certificate. They had also conducted a post‑accident review of the pilot’s medical records and remained satisfied that the pilot met the requirements for the issue of the certificate.
Aircraft information
VH-PXR was a Piper Aircraft Corp PA-28-180 Cherokee aircraft, first registered in Australia in August 1968. A periodic inspection was carried out and a maintenance release issued on 24 October 2022 at 10,861.6 hours’ time-in-service. The aircraft was approved for instrument flight rules[2] operation, however, at the time of the accident it was restricted to day visual flight rules only until instrument lighting and glideslope defects were rectified.
The ATSB acquired evidence the pilot had completed maintenance on the aircraft’s pitot-static mast in February 2023 to clear blockages. They did not hold an aircraft maintenance engineer licence or authorisation to perform or certify for maintenance on the aircraft. This type of maintenance could lead to erroneous indications of the airspeed indicator, altimeter, and vertical speed indicator. It could not be determined if this contributed to the accident.
Meteorological information
The flight departed in good conditions suitable for visual flight. However, as was forecast, the conditions deteriorated as the aircraft approached the Clarke Ranges. Information from the Bureau of Meteorology for the accident area (within the Clarke Ranges) indicated that the forecast for all heights above mean sea level was:
generally broken cloud[3] between 2,000 ft and 6,000 ft
scattered showers of rain with broken cloud base of 1,000 ft and visibility reducing to 3,000 m
isolated thunderstorms with bases of 1,000 ft and visibility reducing to 1,000 m.
The conditions over these ranges and toward the coast included significant low cloud, rain, and thunderstorms. All these phenomena led to reduced visibility. Immediately prior to the accident, the weather radar recorded rain in the area.
Images and video taken during the flight showed broken cloud ahead, with the base below the altitude of the aircraft. The ranges where the accident site occurred were obscured by low cloud, with rain visible (Figure 3).
Figure 3: Image taken in-flight of the weather conditions ahead
Source: Supplied
Terrain
The flight was initially conducted over the relatively flat terrain of inland Queensland, with elevations generally ranging between 500 ft and 1,500 ft. The Clarke Range separated the inland areas from the low and flat coastal plains near the destination, Lakeside Airpark, for about 55 km along the intended route. Within the Clarke Range, the topography was substantially more rugged and elevated than the coastal or inland areas, rising in excess of 3,200 ft. The accident occurred within this area at an elevation of 1,913 ft.
Site and wreckage information
Due to the terrain, the ATSB did not attend the accident site. However, photographs and videos were obtained from Queensland Police and the Australian Maritime Safety Authority Joint Research Co-ordination Centre, and examined by the ATSB (Figure 4). Observations of the accident site included:
About 80 m prior to the wreckage, a number of trees sustained damage. This damage was shown to have an increasing angle down towards the wreckage.
The aircraft collided with terrain on a steep slope, and the wreckage was observed to be inverted. It was unknown if the aircraft collided with terrain inverted or became inverted during the accident sequence.
There was minimal spread of the wreckage, and the wings, fuselage, and tail were in their expected positions relative to the structure of the aircraft.
The leading edge of the right wing sustained damage consistent with a tree strike.
The forward fuselage was destroyed by fire.
The propeller was found intact, and showed impact marks and bending consistent with the engine producing power at the time of impact.
Consideration of these factors suggested that an in-flight break-up, engine failure or fuel exhaustion were unlikely to be contributory to the accident. The relatively contained wreckage was representative of a low speed, high angle of attack impact with the ground.
Figure 4: Aircraft wreckage
Source: Queensland Police Service
Safety message
This accident highlights the importance of following the standards for the operation and maintenance of aircraft to ensure the safety of flight. It further demonstrates that weather continues to remain one of the most significant causes of accidents in general aviation. The often‑fatal outcomes of these accidents are usually all the more tragic as they are avoidable. Despite the dangers of visual flight rules pilots flying into instrument meteorological conditions being well recognised, this continues to be a recurring factor in aircraft accidents and has been the focus of numerous previous ATSB reports and publications.
The ATSB publication Avoidable Accidents No. 4, Accidents involving Visual Flight Rules Pilots (VFR) in instrument Meteorological Conditions (IMC) found that weather alone is never the only factor affecting pilot decisions that result in these events. Investigations consistently highlight that conducting thorough pre-flight planning is the best defence against flying into deteriorating weather. The ATSB encourage all pilots, no matter what their experience level, to develop the knowledge and skills required to avoid unintentional operations into adverse weather. This could be aided by having alternate plans in case of unexpected changes in weather, making timely decisions to turn back, divert or hold in an area of good weather, and using a ‘personal minimums’ checklist to help clearly identify risk factors.
Reasons for the discontinuation
The Civil Aviation Safety Authority have put in place regulations designed to ensure pilots are properly trained and qualified to manage challenges likely to be encountered during flying operations. This includes training intended to teach pilots to identify and manage situations presented by adverse weather, both at the pre-flight planning phase and during flight. However, when pilots operate outside these rules, they remove the built-in safety defences. On that basis, the ATSB determined that there was limited safety benefit in continuing to direct resources at this investigation when compared with other priorities and elected to discontinue this investigation.
[1] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft in instrument meteorological conditions (IMC), which have much lower weather minimums than visual flight rules (VFR). Procedures and training are significantly more complex as a pilot must demonstrate competency in IMC conditions while controlling the aircraft solely by reference to instruments. IFR-capable aircraft have greater equipment and maintenance requirements.
[3] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘broken’ indicates that more than half to almost all the sky was covered.
The following statement can be attributed to ATSB Chief Commissioner Angus Mitchell:
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into a runway excursion involving a single-engine passenger aircraftwith a pilot and six passengers on board at Rat Island, Western Australia, on Thursday morning.
During landing at Rat Islandit was reported that the GA8 Airvanlanded long, exited the runway and came to rest in the water, resulting in substantial damage to the aircraft.No injuries werereported.
ATSB investigators will collect and examine relevant evidence, including interviewing the pilot, analysing relevant weather data, photographs, aircraft operator procedures and maintenance records.
The ATSB will publish a final report, detailing contributing factors and any identified safety issues, at the conclusion of the investigation.
However, should any critical safety issues be identified at any stage during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.
Section 21 (2) of the Transport Safety Investigation Act 2003 (TSI Act) empowers the ATSB to discontinue an investigation into a transport safety matter at any time. Section 21 (3) of the TSI Act requires the ATSB to publish a statement setting out the reasons for discontinuing an investigation.
Overview of the investigation
Just after midnight on 5 April 2023, a Boeing 737-838, registered VH‑VXH, was being operated by Qantas on a passenger air transport flight from Darwin, Northern Territory to Melbourne, Victoria. An Airbus A320, registered VH-VGV, was being operated by Jetstar on a passenger air transport flight from Sydney, New South Wales, to Darwin.
A temporary restricted area (TRA) was in place between 2130–0530 each night due to Royal Australian Air Force (RAAF) air traffic control services not being available in the airspace around Darwin Airport below 8,500 ft. As a result, aircraft flight crews were required to coordinate their own separation when arriving and departing the airport. Flight crews were also required to gain permission from the RAAF Darwin flightwatch prior to operating within the TRA. With the TRA in place, Airservices Australia was responsible for managing the airspace above 8,500 ft through its Brisbane Centre.
At 0009:56, the 737 first officer (FO) contacted the Darwin flightwatch and received permission to operate within the TRA. Darwin flightwatch also advised of opposite direction traffic inbound to Darwin (this referred to the A320 and another subsequent flight).
At 0013:43, the 737 FO contacted Brisbane Centre and advised that the aircraft was taxying at Darwin Airport and would depart using runway 11. The Brisbane Centre controller acknowledged the FO’s radio call and advised of the 2 inbound aircraft, giving details of the arrival routes (both were VEGPU SEVEN standard arrivals from the south-east and landing on runway 29). The A320 was due to land at Darwin Airport at about 0027:00.
The flight crew of the 737 recalled considering the inbound traffic and believed there was sufficient spacing to safely depart ahead of the A320 using runway 11 (the reciprocal to runway 29).
At 0016:16, the 737 flight crew commenced the take-off from runway 11 and, at 0018:04, the captain made a departure call on the Darwin flightwatch frequency. Shortly after, the Darwin flightwatch controller queried when the 737 would commence a turn and stated the A320 was now 30 NM to the south. At 0018:37 the 737 captain responded they were conducting the PALGA SEVEN standard instrument departure and they would contact Brisbane Centre shortly to get a clearance to enter the overlaying airspace.
At 0019:22, and climbing through 4,500 ft, the 737 captain contacted the A320 flight crew directly on the Darwin flightwatch frequency and offered to level off at 7,000 feet to maintain separation. By this time, the flight crew of the A320 had the 737 displayed on the aircraft’s Traffic Collision Avoidance System (TCAS) and believed the aircraft did not present a conflict. At this time, the aircraft were about 26 NM apart on converging courses, with the A320 at 8,500 ft. The A320 FO replied on the Darwin flightwatch frequency that the 737 could continue the climb.
At 0019:42, the 737 captain contacted Brisbane Centre to advise the aircraft had departed Darwin. The Brisbane Centre controller informed the 737 captain they could expect a clearance to enter the overlaying airspace on a heading of 060° and further stated, ‘suggest left heading 060 now’. The 737 captain confirmed the heading. The 737 commenced a left turn onto a heading of 060° at about 0020:00, with the aircraft about 20 NM apart. The tracks diverged and the aircraft crossed the same level a few seconds later.
At about 0022:06, the lateral separation between the 737 and the A320 decreased to its closest point of approach of about 10.6 NM, with vertical separation reducing to about 4,500 ft (Figure 1).
Figure 1: 737 and A320 locations at 0019:46, 0021:06 and 0022:06
Source: Airservices Australia, annotated by the ATSB
The ATSB received an initial occurrence report on 5 April 2023 and commenced an investigation on the same date. As part of the investigation, the ATSB interviewed the 737 flight crew, A320 flight crew, and the Brisbane Centre air traffic controller, and reviewed:
data from the 737 and A320 quick access recorders
weather information
recorded air traffic control audio and surveillance data
information provided by the aircraft operators and air traffic control services.
The investigation identified the following:
The practice of activating daily TRAs at Darwin Airport commenced in July 2022 due to controller availability preventing the delivery of a continuous approach control service. The RAAF advised that daily TRAs were planned to continue to be utilised at Darwin Airport until approximately the first quarter of 2024.
Both flight crews described an increased level of workload associated with the Darwin Airport TRA that was similar in complexity to common traffic advisory frequency (CTAF) procedures.
Although experiencing increased workload the crews felt that there was no concern regarding separation in this instance.
The 737 flight crew elected to depart from runway 11 for noise abatement and operational reasons, believing there would be adequate separation between the 737 and the arriving A320.
At the time the 737 departed, the automatic terminal information service for Darwin Airport stated the preferred runway was runway 29. The windspeed and direction recorded at the time was 2-3 kts from between 150–191° magnetic, which favoured runway 11.
The A320 and 737 flight crews coordinated their separation on the Darwin flightwatch frequency and were sufficiently aware of each other’s position, level and track to maintain separation.
Neither the 737 or A320 flight crew received a TCAS alert or advisory.
The Brisbane Centre controller recalled having concerns about the proximity of the 2 aircraft; however, the controller recalled not knowing the actual separation between the 2 aircraft due to the scale of the display.
The Brisbane Centre controller’s decision to turn the 737 was to provide increased separation; however, this purpose was not communicated to the 737 flight crew.
The lateral and vertical separation between the 737 and A320 at the closest point of approach met the separation standards required had the airspace been controlled at the time. It is probable the same separation standards would have been met had the 737’s flightpath continued without the turn.
Reasons for the discontinuation
Based on a review of the available evidence, the ATSB considered that there was no safety-related separation issue in this instance and it was unlikely that further investigation would identify any systemic safety issues or important safety lessons. Consequently, the ATSB has discontinued this investigation.
The evidence collected during this investigation remains available to be used in future investigations or safety studies. The ATSB will also monitor for any related occurrences that may indicate a need to undertake a further safety investigation, noting the potential for increased risk in terminal airspace that is made non-controlled for certain periods.
Occurrence summary
Investigation number
AO-2023-015
Occurrence date
05/04/2023
Location
Near Darwin Airport
State
Northern Territory
Report release date
29/06/2023
Report status
Discontinued
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Discontinued
Mode of transport
Aviation
Aviation occurrence category
Separation issue
Occurrence class
Incident
Aircraft details
Manufacturer
The Boeing Company
Model
737-838
Registration
VH-VXH
Serial number
33478
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Departure point
Darwin Airport, Northern Territory
Destination
Melbourne Airport, Victoria
Aircraft details
Manufacturer
Airbus
Model
A320-232
Registration
VH-VGV
Serial number
4229
Aircraft operator
Jetstar Airways Pty Ltd
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes