Brief, loud grinding noises precipitated the failure of a Bell 505 helicopter’s tail rotor driveshaft, an Australian Transport Safety Bureau report details.
On 15 July 2022, the Bell 505 was being used for a scenic flight from Cairns, Queensland, with a pilot and two passengers on board.
About 30 minutes into the flight, near Double Island, the pilot heard two brief, loud grinding noises, and elected to return to Cairns Airport.
Over the airfield, the grinding noise returned, and after 10-12 seconds, while approximately 10 ft off the ground, the pilot heard 2 loud bangs.
“In response, the pilot moved the throttle to idle, which stopped the yaw,” ATSB Director Transport Safety Stuart Macleod explained.
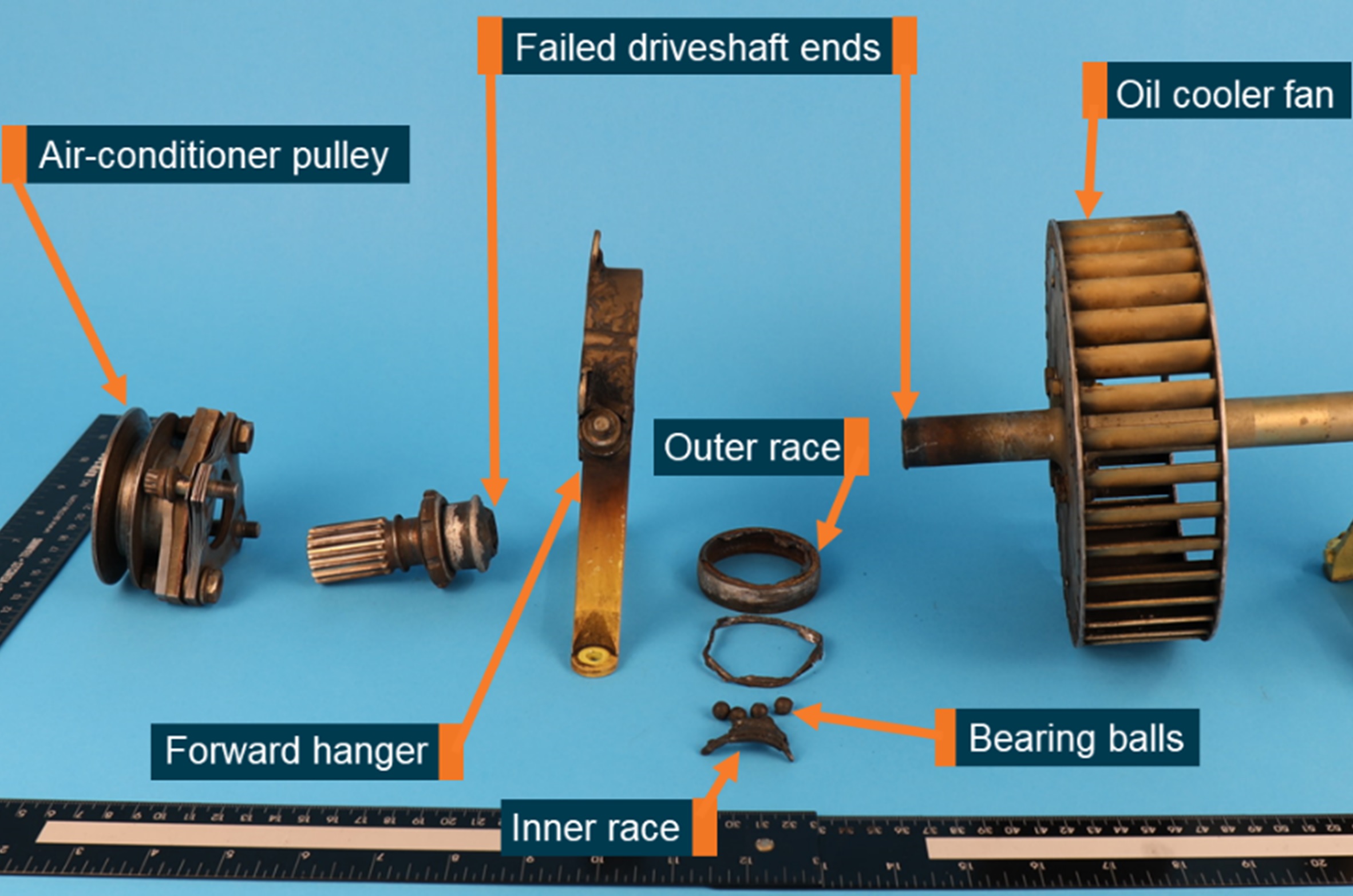
A run-on landing was performed on the grass short of the assigned helipad, and a subsequent inspection of the helicopter revealed the tail rotor driveshaft had failed.
“The ATSB determined that during landing, a combination of heat and torque due to a seized forward fan shaft bearing resulted in failure of the fan shaft just aft of that bearing,” Mr Macleod said.
Due to the amount of damage on the failed bearing, the ATSB was not able to identify the reason for the seizure, and the manufacturer, Bell Textron, advised the ATSB that it was not aware of any previous instances of bearing failure in 505 fan shaft bearings.
“Unusual sounds and responses from an aircraft can be an indication of an imminent system failure,” Mr Macleod continued.
“In this instance, the pilot’s decision to return to Cairns was probably influenced by the initial short duration of the unusual noises and overwater operation. While a safe landing on an airfield resulted, the occurrence also illustrates how quickly failures can occur.”
Mr Macleod noted pilot’s decision to adopt a shallow approach, and to reduce throttle immediately following the shaft failure, both assisted in controlling the helicopter following the uncommanded yaw, and allowed for a safe landing.
“This incident does highlight that pilots experiencing any unusual vibration or noise should land as soon as possible and have the aircraft inspected prior to further flight,” he said.
“If an immediate landing is not possible then pilot should be prepared to conduct an emergency landing or ditching if the situation deteriorates.”
On 12 May 2023, an instructor and student pilot in a Magni M16C Tandem Trainer gyroplane, registered G1850, were conducting wheel balance exercises on runway 07 at Lake Macquarie Airport, New South Wales. Following the sixth of these exercises, the student made a radio broadcast while the instructor turned the gyroplane around and taxied on the runway toward the runway 07 threshold at the western end to repeat the exercise. Meanwhile, the pilot of an Extra EA 300L, registered VH-IOG, taxied from the apron for a scenic flight with one passenger. The Extra pilot made 2 radio broadcasts before entering the runway near the eastern end and taxied towards the runway 07 threshold. At about this time, the gyroplane commenced another exercise and accelerated down runway 07 towards the Extra. As the gyroplane approached the runway midpoint, the instructor and student observed the Extra about 20 m ahead. The instructor manoeuvred to avoid a collision, banking right before colliding with terrain resulting in substantial damage to the gyroplane. The instructor was seriously injured, with the student sustaining minor injuries. The Extra was not damaged, and its occupants were uninjured.
What the ATSB found
The ATSB found that neither aircraft’s pilots heard each other’s radio broadcasts and consequently, aircraft separation became reliant solely upon visual acquisition. The investigation found that the Extra pilot did not see the gyroplane before entering the runway, and subsequently taxied towards it. Also, while accelerating on the runway, the instructor and student in the gyroplane did not see the Extra taxiing towards them until a collision was imminent.
There were several factors that likely reduced the ability of the pilots to identify each other, including the small angular size of each aircraft, the complex background features with low relative contrast, and minimal relative movement between the aircraft.
Additionally, the tailwheel configuration of the Extra limited the pilot’s forward visibility and sun glare likely also affected the pilot’s ability to detect the gyroplane. The gyroplane pilots were likely also influenced by the higher workload associated with the training exercise which probably reduced their available attention for identifying conflicting aircraft.
What has been done as a result
The airport operator released a bulletin to all operators based at Lake Macquarie Airport highlighting the importance of a visual lookout in addition to radio discipline. A runway hold point line was repainted, and radio recording equipment will be purchased to allow radio communications to be periodically reviewed.
The operator of VH-IOG updated operational procedures to require a ground employee to have a hand-held radio switched on and in reach for all operations, and to monitor all departure and arrival radio calls. Pilots are now also required to stop at a hold point line before entering the runway for departure at Lake Macquarie Airport.
The Australian Sport and Rotorcraft Association (ASRA) advised the ATSB of its intent to replace the one-off human factors exam, completed as a requirement of the ASRA pilot certificate, with a recurrent exam, to be completed as part of each biennial flight review.
Safety message
The ATSB SafetyWatch highlights the broad safety concerns that come out of our investigation findings and from the occurrence data reported to us by industry. One of the safety concerns is reducing the collision risk around non-towered airports. This accident highlights the limitations of unalerted see-and-avoid in such an environment. Pilots are reminded of the importance of effective radio communications to increase traffic awareness and to ensure an effective visual scan to identify conflicting traffic.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On the afternoon of 12 May 2023, an instructor and student pilot in a Magni M16C Tandem Trainer gyroplane, registered G1850 and operated by Airborne Flight Training, were planning to conduct wheel balance training exercises (see the section titled Operational information) at Lake Macquarie Airport, New South Wales. The airport was located within class G, non‑controlled airspace and had a designated common traffic advisory frequency (CTAF) on which pilots made positional broadcasts to coordinate aircraft separation.
At about 1537, the student and instructor pilots, seated in the front and rear seats respectively, taxied the gyroplane onto the runway near the runway 25[1] threshold and then backtracked[2] towards the runway 07 threshold (Figure 1) to commence the wheel balance training. The training exercise involved the student accelerating the gyroplane on the runway while balancing on the main landing gear until the gyroplane lifted off the ground briefly. The student then handed control to the instructor who would land on the runway, turn the gyroplane around and backtrack towards the 07 threshold before handing control back to the student and repeating the exercise.
At about 1542, the student pilot reported making a ‘rolling' radio call on the CTAF to indicate they were commencing the first wheel balance exercise. About 30 seconds later, after accelerating along the runway and briefly becoming airborne, the gyroplane landed about half-way down runway 07 and turned around. During this turn, the student reported making another radio call to indicate they were backtracking towards the runway 07 threshold.
At about 1543, the pilot of an Extra EA 300L, registered VH-IOG and operated by Inverted Downunder, walked towards the aircraft, which was located on the airport apron near the eastern end of the runway, to prepare for a scenic flight with one passenger. This was to be the pilot’s fifth flight of the day in the Extra.
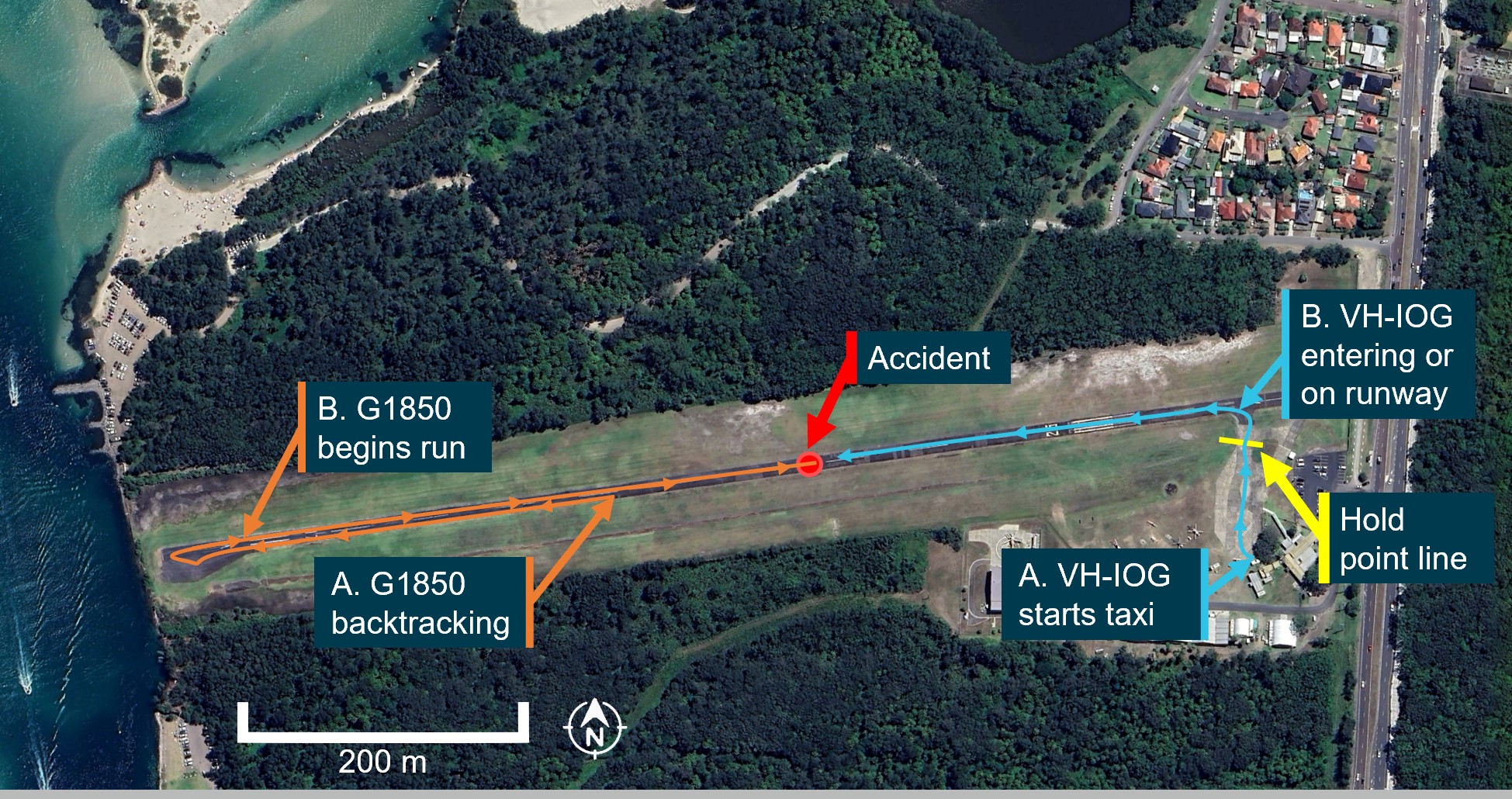
Figure 1: Lake Macquarie Airport showing G1850 estimated ground track and VH-IOG location
G1850 track estimated using CCTV footage and pilot statements. VH-IOG location based on CCTV footage.
Source: Google Earth, annotated by ATSB
At about 1544, the gyroplane’s student pilot commenced a second wheel balance exercise from the runway 07 threshold. While the gyroplane was undertaking this exercise, airport video footage showed that the pilot of the Extra stepped onto the parked aircraft’s wing to prepare the front seat for the passenger. By about 1545, the gyroplane had travelled towards the end of runway 07, adjacent to the apron area and was slowing down to turn around (Figure 2). The student recalled that during the turn, a backtracking radio call was made. At about the same time, the video footage showed the Extra’s pilot, who was still on the wing, appear to look up for about a second toward the gyroplane. Shortly after, the passenger climbed into the front seat of the Extra, while the gyroplane backtracked towards the runway 07 threshold.
Over the next 8 minutes, the Extra’s pilot secured the passenger in their seat, provided a pre-flight briefing, and then climbed into the rear seat, putting their seatbelt and helmet on. During this time, the instructor and student pilot performed a further 4 wheel balance exercises, with the gyroplane turning around at different locations along the runway (Figure 2), but none as far as during the second wheel balance exercise (near the airport apron). The student pilot and instructor recalled radio calls being made prior to the commencement of, and during the turnaround at the end of, each wheel balance exercise.
Figure 2: G1850 turnaround locations
Source: Google Earth, annotated by ATSB
At 1554:05, a few seconds after turning around following the sixth wheel balance exercise, the Extra’s pilot started the aircraft’s engine and conducted pre-flight checks which included switching on the aircraft’s radios.
At 1554:39, the Extra’s pilot began to taxi towards the runway while the gyroplane was backtracking along runway 07. At about 1554:53, the Extra’s pilot reported making a radio call on the CTAF that the aircraft was taxiing for runway 07.
At about 1555:09, and for about the next 10 seconds while taxiing, the Extra pilot reported visually looking for aircraft on final approach for runways 25 and 07, and for aircraft on the runway. The pilot recalled that most of their attention during this visual lookout was towards the ‘bad lighting’ at the runway 07 threshold and they recalled not seeing any aircraft. During this time, the Extra pilot made another radio call advising they were entering and backtracking runway 07. Shortly after, the aircraft crossed the hold point line without stopping and turned left onto the runway (Figure 3). The pilot stated that they did not usually stop at this line because they had unobstructed views towards the runway 07 threshold and final approach to runway 25 before this point. At a similar time, the student commenced the seventh wheel balance exercise from the runway 07 threshold. Both gyroplane pilots recalled that they did not see any aircraft on the runway at this time, nor could they recall making a ‘rolling’ radio call prior to this exercise.
As the Extra backtracked runway 07, the student was accelerating the gyroplane along the runway. About 30 seconds later, as the gyroplane approached the midpoint of the runway, the instructor and student observed the Extra about 20 m ahead and backtracking towards them. The instructor took control and banked the gyroplane right to avoid a collision. The rotor blades impacted the runway surface before the gyroplane veered off the runway and collided with terrain, coming to rest on its side. The gyroplane sustained substantial damage to the rotor blades, propeller blades, and landing gear. The instructor was seriously injured, with the student sustaining minor injuries. The Extra pilot saw the gyroplane veer off the runway to the left, stopped their aircraft and exited to provide assistance. The Extra was not damaged and its occupants were uninjured.
Figure 3: G1850 and VH-IOG ground tracks before accident
Labels ‘A’ and ‘B’ are timestamps for the approximate locations of each aircraft.
Source: Google Earth, annotated by ATSB
Context
Pilot information
G1850 pilots
The instructor pilot held an Australian Sport Rotorcraft Association (ASRA)[3] pilot certificate and was approved by ASRA as a chief flying instructor (CFI). They had accrued 2,254 hours of flying time in gyroplanes and about 751 hours on the Magni M16 and Magni M16C Tandem Trainer gyroplane, with 43 of those hours flown in the previous 90 days.
The student held an ASRA pilot certificate and a Private Pilot Licence (aeroplane). The student had accrued about 330 hours of flying time in aeroplanes, and 60 hours in gyroplanes, 10 of which were on the Magni M16C Tandem Trainer gyroplane in the previous 90 days.
VH-IOG
The Extra pilot held a Civil Aviation Safety Authority (CASA) Commercial Pilot Licence (Aeroplane). They had accrued 7,800 hours of flying time, with about 600 hours on the Extra EA 300L, of which 18.5 hours were flown within the previous 90 days.
Aircraft information
G1850
The Magni M16C Tandem Trainer is a 2-seat gyroplane with fixed tricycle landing gear (Figure 4). A 4‑cylinder piston engine drives a 3-bladed pusher propeller, with an unpowered rotor to develop lift. The gyroplane has a pre-rotation system linking the engine to the rotor which, when engaged, can drive the rotor to start it spinning without needing forward motion.
The Magni M16C is 4.7 m long, 2.7 m high (fuselage about 1.5 m high), and 1.8 m wide, with a rotor diameter of about 8.5 m. An external landing light was fitted to the front of the fuselage with strobe lights fitted to each side of the fuselage and one on the rear of the mast.
The front seat was instrumented for the pilot in command and was occupied by the student. The rear seat was not fitted with instrumentation but had flight controls, and was slightly higher than the front seat to improve forward visibility. Both seats were fitted with 4-point harnesses and both pilots were wearing them at the time of the accident.
Figure 4: G1850
Source: Airborne Flight Training
VH-IOG
The Extra EA 300L is a low-wing, 2-seat aerobatic monoplane with fixed tailwheel landing gear and the rear seat was instrumented for the pilot in command. A 6-cylinder piston engine drives a 3-bladed tractor propeller. VH-IOG was manufactured in Germany in 1999 and first registered in Australia in June 2005 (Figure 5).
The aircraft is about 7 m in length and 1.8 m high while on the ground with a wheel track of 1.8 m and a wingspan of 8 m. External navigation and strobe lights were fitted to the wingtips.
Figure 5: VH-IOG
Source: Inverted Downunder
Operational information
The gyroplane instructor planned for the student to perform several wheel balance exercises to teach the student the correct pitch attitude for take-off, and the exercise included many similar aspects of a normal take-off. The United States Federal Aviation Administration (FAA) Rotorcraft Flying Handbook[4] described a normal gyroplane take-off as follows:
The normal takeoff for most amateur-built gyroplanes is accomplished by prerotating to sufficient rotor r.p.m. to prevent blade flapping and tilting the rotor back with cyclic control. Using a speed of 20 to 30 m.p.h., allow the rotor to accelerate and begin producing lift. As lift increases, move the cyclic forward to decrease the pitch angle on the rotor disc. When appreciable lift is being produced, the nose of the aircraft rises, and you can feel an increase in drag. Using coordinated throttle and flight control inputs, balance the gyroplane on the main gear without the nose wheel or tail wheel in contact with the surface. At this point, smoothly increase power to full thrust and hold the nose at takeoff attitude with cyclic pressure. The gyroplane will lift off at or near the minimum power required speed for the aircraft.
The instructor stated that if the student obtained the correct pitch attitude, the gyro would lift‑off briefly, before the instructor would take control and land on the runway, turn around, backtrack towards the runway 07 threshold, and repeat.
The instructor also stated that during the acceleration phase of the wheel balance exercise, the workload was high due to the multi-tasking required in monitoring the gyroplane’s attitude, the student’s flight control inputs, and the gyroplane’s response.
The student stated that during the acceleration phase of each wheel balance exercise, they glanced down occasionally to look at the cockpit instrumentation, but their focus was primarily on looking out of the aircraft and monitoring the gyroplane’s pitch attitude.
Meteorological information
The weather at Lake Macquarie Airport at the time of the accident was good with a light easterly wind, visibility greater than 10 km, and no cloud over the airport.
At the time the Extra’s pilot was taxiing towards the runway from the apron (heading north), the sun was positioned at about the 10 o’clock (300°) position,[5] at an elevation of about 12°. This would have placed the sun in the pilot’s field of view while looking towards the runway 07 threshold (Figure 6). It is likely that the gyroplane would have been illuminated by the sun at this time. The Extra pilot stated that as there was a light wind, a take-off from runway 07 was preferable since the sun was getting low in the west making it difficult to look in that direction. The pilot stated that they were wearing a tinted helmet visor, which would have reduced sun glare.
Figure 6: VH-IOG turning left to backtrack runway 07
Source: Airport operator
While the gyroplane was accelerating towards the Extra on runway 07 during the seventh and final wheel balance exercise, the sun was positioned behind the gyroplane at about the 8 o’clock position. The Extra was likely illuminated by the sun while backtracking along the runway towards the gyroplane.
Airport information and procedures
Lake Macquarie Airport was an aircraft landing area,[6] located about 20 km southwest of Newcastle, New South Wales. It had an elevation of 5 ft above mean sea level, and a single, sealed 880 m long and 11 m wide runway designated 07/25, with trees lining each side.
As a non-controlled airport, separation between aircraft was maintained by ‘alerted see-and-avoid’ principles guided by Civil Aviation Safety Authority (CASA) advisory circulars[7]. Unalerted see‑and‑avoid relies on a pilot or crew visually detecting other aircraft without the assistance of other aids or information. This visual detection can be improved through pilots being alerted to an aircraft’s presence by radio, electronic systems, or other means (alerted see‑and-avoid).
At Lake Macquarie Airport, the carriage and use of a radio was required by the airport operator for all operating aircraft. Pilots were required to broadcast their position and intention so that nearby traffic would have an awareness of their aircraft and be able to plan or act accordingly.
All 3 pilots were familiar with the airport operations and had operated at Lake Macquarie for many years. Both aircraft were on the correct CTAF frequency before the accident, with all pilots having 2-way communications with other aircraft. None of the pilots reported hearing the other aircraft’s radio calls. The gyroplane pilots could not recall whether they had made a rolling call at the start of the final wheel balance exercise.
The Extra pilot reported that once they had taxied clear of the apron toward the hold point line, there was nothing obstructing their view of the runway 07 threshold other than the lighting conditions. The gyroplane instructor similarly reported no limitations with visibility of the entire runway when viewed from the runway 07 threshold.
The Extra pilot stated that there had been historically poor radio usage at the airport, and that they needed to use visual lookout ‘aggressively’ and not rely on radio communications. The gyroplane instructor considered radio to be a secondary means of collision avoidance to visual lookout.
Limitations of see-and-avoid
The see-and-avoid principle has been an effective defence in preventing aircraft collisions, but has several limitations (ATSB, 1991).
Workload
See-and-avoid can only be effective when the pilot is looking outside the cockpit. However, many tasks require pilots to direct their attention inside the aircraft, particularly when conducting operations and tasks that involve a high workload.
There was an opportunity for the Extra pilot to become aware of the gyroplane while they were on the Extra’s wing preparing the passenger’s seat, when they looked up briefly toward the gyroplane turning around on the runway. However, the Extra’s pilot recalled being unaware of any other operations being conducted at the airport while on the apron preparing the passenger for the flight. It is possible that the pilot’s focus on preparing the aircraft and passenger for flight resulted in them not detecting the gyroplane despite appearing to look towards it.
Although the Extra had occupied the runway for about 30 seconds before the gyroplane pilots saw the aircraft, the gyroplane pilots’ focus on other traffic in the runway environment was probably limited due to the complex training exercise being conducted. The instructor and student’s attention was primarily focused on the gyroplane’s motion and attitude to ensure the exercise was being conducted appropriately.
Visual search
In daylight, a pilot must look almost directly at an object to see it and it is possible for a pilot to look past an object if they do not see it directly. An FAA advisory circular recommended scanning the entire visual field outside the cockpit with eye movements of 10 degrees or less, with about a second spent on each 10 degree sector, to ensure effective detection of conflicting traffic.[8]
It was estimated that the Extra pilot would have spent about 10 seconds on their visual lookout which included viewing both ends of the runway and associated approaches. While the Extra’s pilot was approaching the runway from the apron, the runway 07 environment would have been captured in a sector about 30 degrees horizontal by 10 degrees vertical. This suggests that the Extra pilot would have required at least 3 seconds for an effective visual scan of the runway (without accounting for any other factors). While the pilot probably spent at least that length of time viewing the runway 07 environment, there were other factors that likely affected their visual scan and their ability to detect the gyroplane in that time.
Cockpit visibility
Items such as window pillars, sun visors, and front seat occupants may impact on the pilot’s ability to see an aircraft. The FAA Airplane Flying Handbook[9] described the reduced forward visibility of tailwheel aircraft:
In the normal nose-high attitude, the engine cowling may be high enough to restrict the pilot’s vision of the area directly ahead of the airplane while on the ground. Consequently, objects directly ahead are difficult, if not impossible to see...In taxiing such an airplane, the pilot should alternately turn the nose from one side to the other (zigzag) or make a series of short S-turns. This should be done slowly, smoothly, positively, and cautiously.
The pilot reported that the Extra EA 300L had limited visibility from inside the cockpit between 11‑1 o’clock directions while on the ground. Their usual procedure at Lake Macquarie Airport was to undertake a ‘zig-zag’ manoeuvre at the half-way point of the runway to allow them to see the runway environment and ensure the final approach was clear of traffic. The manoeuvre was only performed once as the narrow runway required the aircraft to slow down significantly. On this occasion, the accident occurred before the Extra had reached the half-way point on the runway.
Threshold for acuity
The eye’s ability to recognise an object also depends on the relative size of the object and an approaching aircraft might be too small to be seen. Studies have estimated the size an object needs to be for it to be sighted, with estimations of visual angle varying from about 0.02° to detect features of an alphabet letter (Howett, 1983), to at least 0.2° (NTSB, 1988) to reasonably detect an overall object. However, visual acuity varies widely across the retina of the eye and therefore, these values are only of relevance when looking directly at an object. Additionally, these observations were conducted under certain conditions, for example high object contrast with the background and moderate illumination (Howett, 1983), while the particular conditions experienced by the pilots involved in this occurrence were likely different.
With the Extra’s pilot at the hold point line and the gyroplane at the runway 07 threshold lined up with the runway, the estimated angular size of the gyroplane’s fuselage including landing gear would have been between 0.11° (height) and 0.14° (width). If the gyroplane pilots were at the runway 07 threshold and looked towards the runway 25 end with the Extra facing them on the runway, the estimated angular size of the Extra’s fuselage would have been about 0.14° (height and width). While the angular size of the Extra’s wingspan and the gyroplane’s rotor would be larger, these were both thin making them difficult to detect at such a distance compared to each aircraft’s fuselage.
Background features
Detecting an aircraft can become more difficult against a complex background that has different colours, contours, and objects. Aircraft are more easily spotted if they have a high contrast with their background. Images taken from around the midpoint on the runway about 20 minutes after the accident (Figure 7) provided some indication of the background features present at the time of the accident:
The background behind the runway 07 threshold end had some small dark areas of shrub where the gyroplane’s white fuselage illuminated by the sun would have provided good contrast. However, the fuselage and background area covered by the shrub were small, and the light blue of the lake, and lighter terrain areas covered with haze in the distance, would have a presented a lower contrast difference with the white fuselage.
Behind the runway 25 threshold was a highway at the same elevation as the runway, which video footage showed was busy with traffic around the time of the occurrence, with trees illuminated by the sun behind the highway. Although the Extra’s yellow nose and spinner would have been illuminated by the sun during the wheel balance exercise, the background behind the Extra had the sideways motion of traffic at the same level as the Extra creating a more complex scene. In addition, the trees in the background were also illuminated by the sun potentially reducing the contrast of the nose and spinner as the Extra moved closer to the gyroplane.
Figure 7: background features at runway ends
Source: Inverted Downunder
Other factors affecting visibility
In regard to aircraft lighting, research has shown that lights are generally ineffective in daylight at making an aircraft more visible, especially against bright sky backgrounds and can be less conspicuous than the aircraft itself, but may make aircraft more visible against terrain or in conditions of low light. The Extra’s strobe lights were off while the aircraft was backtracking runway 07. The gyroplane strobe lights were on at the time of the accident and the landing light was off.
Glare occurs when unwanted light enters the eye. Glare can come directly from the light source or can take the form of veiling glare, reflected from crazing or dirt on the windscreen. The Extra’s pilot reported that the cockpit canopy was cleaned between flights and had some scratches as it was the original canopy fitted from manufacture. Although the pilot was wearing a sun visor to reduce glare, the sun would have been in the pilot’s field of view while looking towards the runway 07 threshold before entering the runway. The associated glare, which may have been exacerbated by the cockpit canopy, would have probably reduced the pilot’s ability to detect the gyroplane.
Additionally, it is difficult to see another aircraft when there is little relative motion between one aircraft and the other, such as when they are moving towards the same location in space. There was little relative movement between the 2 aircraft while (a) the gyroplane pilots were accelerating towards the backtracking Extra and (b) the gyroplane was positioned near the runway 07 threshold while the Extra pilot was visually looking towards that location before turning onto the runway.
Recorded data
Airport video footage from several locations captured the Extra pilot’s pre-flight activities, taxi, and backtrack towards the runway 07 threshold. The footage also showed segments of the gyroplane’s wheel balance exercises when in view from around the middle of the runway towards the runway 25 threshold. Footage of the runway 07 threshold up to the runway midpoint was not captured by any available video camera.
CTAF radio broadcasts were not recorded at Lake Macquarie Airport. Of the airports that operated on the same CTAF, Warnervale Airport (28 km south-west of Lake Macquarie Airport) was the only airport that recorded radio transmissions. Due to distance and line-of-sight limitations, radio calls on or near the ground at Lake Macquarie were not normally received at Warnervale Airport. The ATSB reviewed recorded radio calls from Warnervale while both the Extra and gyroplane were operating at Lake Macquarie Airport, however, no radio calls from either aircraft were recorded. No recorded data was available from either aircraft.
Safety analysis
Radio alerting
The gyroplane student pilot recalled making backtracking radio calls when turning around at the end of every wheel balancing exercise. However, the final backtracking call was made before the Extra pilot had turned the aircraft’s radio on, and therefore, they would not have heard this radio call. Additionally, the gyroplane pilots could not recall making a rolling call at the commencement of the final wheel balancing exercise prior to the accident, and there were no other sources of evidence to assist in establishing whether this call was made. In any event, the Extra pilot reported that they did not hear any call.
The Extra pilot reported making 2 radio calls before entering the runway. However, for reasons that could not be determined, the gyroplane pilots reported that they did not hear these calls. Consequently, neither aircraft’s pilots were alerted to the other’s presence over the radio and therefore, aircraft separation became solely reliant on each aircraft’s pilots seeing each other.
Visual search
The gyroplane was operating on the runway for about 11 minutes while the Extra pilot was on the apron preparing for the flight. During this time, the gyroplane was primarily on an area of the runway some distance from the pilot and not directly in sight, limiting the Extra pilot’s ability to detect it during this time.
The Extra pilot did not sight the gyroplane before entering the runway. The gyroplane pilots also did not sight the Extra at the start of their seventh and final wheel balance exercise, or while accelerating on the runway until a collision was imminent. While the reasons for this could not be determined, there were likely many common factors that reduced the ability of the pilots to identify each other such as the small angular size of each aircraft, the complex and cluttered background with reduced contrast difference, and the minimal relative movement between each aircraft.
The effectiveness of the Extra pilot’s visual scan was likely also affected by sun glare before entering the runway, and the tailwheel configuration of the aircraft which limited forward visibility while backtracking. The gyroplane pilots were likely also influenced by the higher workload associated with the training exercise, which probably reduced their available attention for identifying conflicting aircraft.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the collision with terrain involving Magni M16C Tandem Trainer gyroplane, G1850, while avoiding Extra EA 300L, VH‑IOG.
Contributing factors
Before entering the runway, the pilot of VH-IOG did not see G1850 occupying the runway and subsequently backtracked towards G1850. As VH-IOG was a tailwheel aircraft, the pilot was unable to sight G1850 while backtracking.
While accelerating on the runway, the instructor and student in G1850 did not see VH-IOG backtracking towards them until a collision was imminent. While manoeuvring to avoid a collision, G1850 collided with terrain.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Lake Macquarie Airport
In May 2023, the airport operator released a bulletin reminding all operators based at Lake Macquarie Airport of several aspects of safe operational practice highlighted by this event, including that:
aircraft should stop forward motion at the hold point line (or equivalent for helicopters) to ensure a good lookout prior to entering the runway environment
pilots are to ensure they know and use correct radio terminology while operating at the airport and to broadcast their intentions
although radio discipline was required, it cannot be relied upon for safety, and that the visual lookout was paramount
for operations involving a backtrack for runway 07, aircraft should turn through 90° in the turning node at the far end, stop to lookout, then broadcast a radio call on lining up
the runway should only be occupied for the minimum time required to either taxi, take off, or land.
The airport operator also advised that:
the hold point line at the apron end of the runway (near the runway 25 threshold) had been repainted and a hold line also painted at the runway 07 end
CTAF radio recording equipment was purchased and anticipated to be installed in February 2024. This will ensure all communications can be reviewed periodically, and in the event of an incident.
Safety action by Inverted Downunder
The operator of VH-IOG advised the ATSB that operational procedures were updated to include requirements for:
a ground employee to have a hand-held radio, switched on and in reach for all operations, and to monitor any departure and arrival radio calls
pilots to stop at the hold point before entering the runway for departures.
Safety action by Australian Sport Rotorcraft Association
The Australian Sport Rotorcraft Association (ASRA) advised the ATSB that, in response to this accident and other previous sport rotorcraft accidents, ASRA intends to replace the one-off human factors exam, which is completed as a requirement of the ASRA pilot certificate, with an updated exam to be completed recurrently as part of each biennial flight review.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
pilot and passenger of the VH-IOG
instructor and student of G1850
VH-IOG operator photos
New South Wales Police Force photos
CCTV footage from Lake Macquarie Airport and Westpac Rescue Helicopter Service
Howett, G. L. (1983), Size of letters required for visibility as a function of viewing distance and observer visual acuity (National Bureau of Standards Technical Note 1180).
National Transport Safety Board (1988), Aircraft Accident Report - Midair Collision of Skywest airlines Swearingen Metro II, N163SW, and Mooney M20, N6485U, Kearns, Utah, January 15, 1987.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Pilot of VH-IOG
instructor and student of G1850
operators of VH-IOG and G1850
Lake Macquarie Airport
the Australian Sport Rotorcraft Association (ASRA)
the Civil Aviation Safety Authority (CASA).
Submissions were received from:
instructor and student of G1850
operator of G1850.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Runway numbers represent the magnetic heading closest to the runway orientation (for example, runway 25 is oriented 250° magnetic while the reciprocal runway 07 is oriented 070º magnetic).
[2] An airport ground procedure which involves the use of any portion of a runway as a taxiway for an aircraft to taxi in the opposite direction from which it will take off or has landed.
[3] ASRA is a national sport and recreational association, representing people with an interest in building and flying gyroplanes. Under Civil Aviation Safety Authority (CASA) accreditation, ASRA administers sport gyroplanes through the certification of pilots and the listing of gyroplanes in Australia.
[5] O’clock: the clock code is used to denote the direction of an aircraft or surface feature relative to the current heading of the observer’s aircraft, expressed in terms of position on an analogue clock face. For example, twelve o’clock is ahead while an aircraft observed abeam to the left would be said to be at 9 o’clock.
[6] An aircraft landing area is an airfield that has not been certified by CASA. These airfields are non-controlled, unregulated facilities. It is the responsibility of pilots and operators to determine whether these airfields are suitable for use.
Parking brake likelywasn’t fully released prior to taxiing for departure.
Residual pressure in the braking system led to heat build-up and further application of the brakes.
The flight crew’s swift decision to reject the take-off demonstrated their effective monitoring of the aircraft’s performance.
The flight crew of a Saab 340 rejected the take-off after experiencing handling and acceleration issues likely due to the parking brake not being fully released, an ATSB investigation details.
The Pel-Air operated Saab 340B, with 2 pilots, a cabin attendant and 25 passengers on board, was departing Flinders Island for Wynyard, Tasmania, as part of a multi-flight charter tour on 4 November last year.
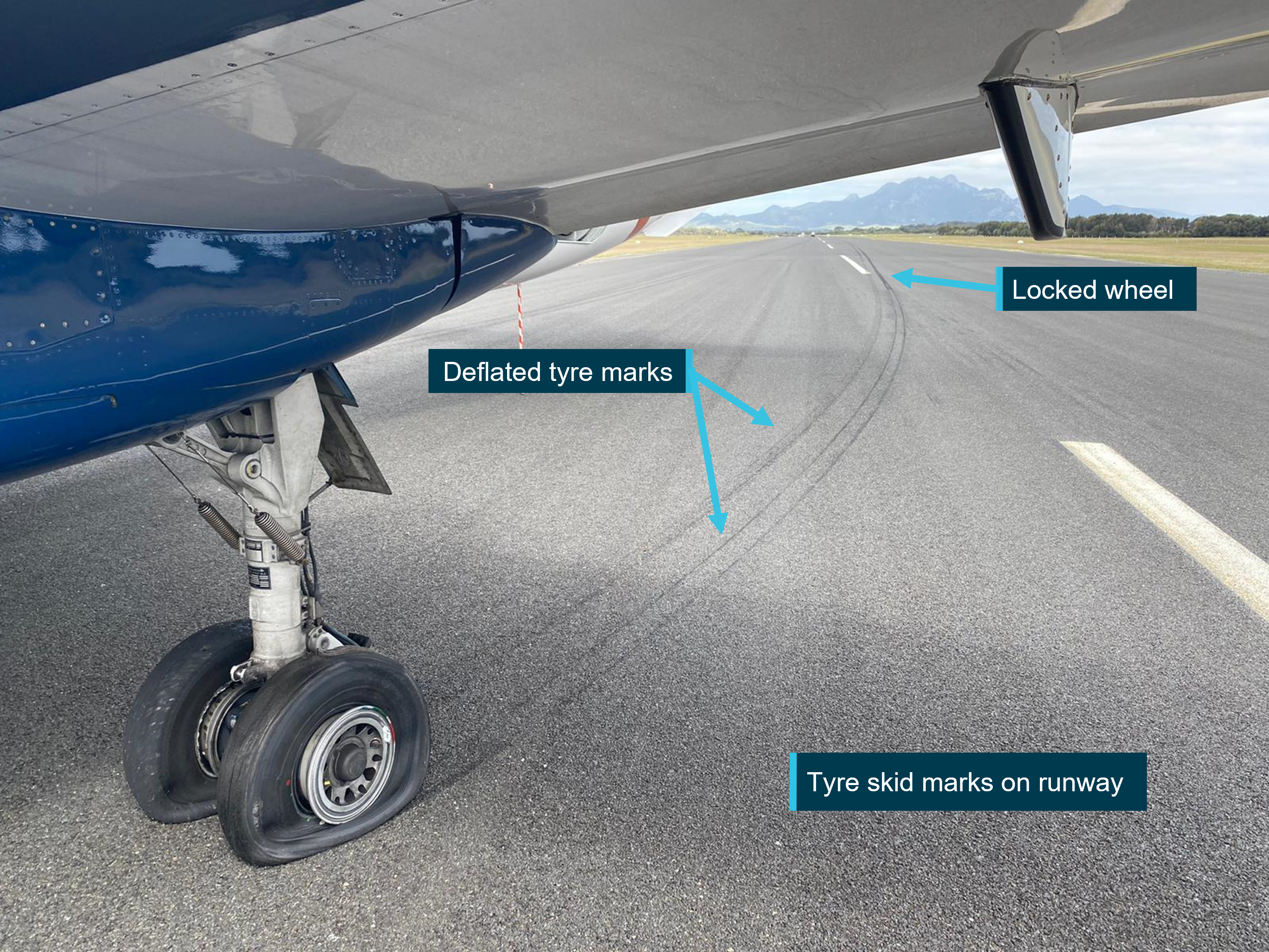
As it accelerated, the aircraft veered to the left of the runway centreline and the crew detected a decrease in acceleration before rejecting the take-off.
Afterwards, the pilots observed significant tyre marks on the runway, a flat spotted tyre, and that all main landing gear tyres were flat.
“The ATSB investigation found that the parking brake handle had likely not been completely seated in the panel when released by the pilot, resulting in residual pressure remaining in the brake system,” ATSB Director Transport Safety Stuart Macleod said.
During the taxi to the runway, the residual pressure provided a partial application of the brakes, which allowed heat to generate within the brake system, resulting in further increased pressure and a continual increase in brake application.
“As the aircraft accelerated for take-off, this heat generation increased significantly, resulting in further application of the brakes.”
Since the occurrence, the operator has taken a number of safety actions to prevent a reoccurrence, including disseminating a Notice to Aircrew to its pilots with detailed information of the operation of the parking brake.
“This occurrence demonstrates the importance of completing routine tasks in accordance with manufacturer’s instructions,” Mr Macleod said.
“The outcome of this event, no passenger injuries and minimal aircraft damage, was a result of the flight crew’s effective monitoring of the aircraft’s performance and prompt action to reject the take-off when the expected performance was not achieved.”
A 737 freighter aircraft failed to pressurise after a cargo depressurisation switch was left on during preflight preparations, an Australian Transport Safety Bureau report details.
The Boeing 737-36E SF (an aircraft built as a passenger airliner but subsequently converted to a freighter) was being operated by Airwork on a flight from Darwin to Brisbane on 4 November 2021.
After take-off, the flight crew observed the aircraft did not pressurise as expected. After stopping the climb at 11,000 ft, the flight crew began to descend to 10,000 ft, during which time a cabin altitude warning alert occurred.
Once at 10,000 ft, the crew completed required checklist actions, but were unable to establish control of the pressurisation. Subsequently the equipment cooling fan failed, the electronic flight information system reverted to a monochrome display output, and the weather radar failed.
The crew made the decision to return to Darwin for an uneventful landing.
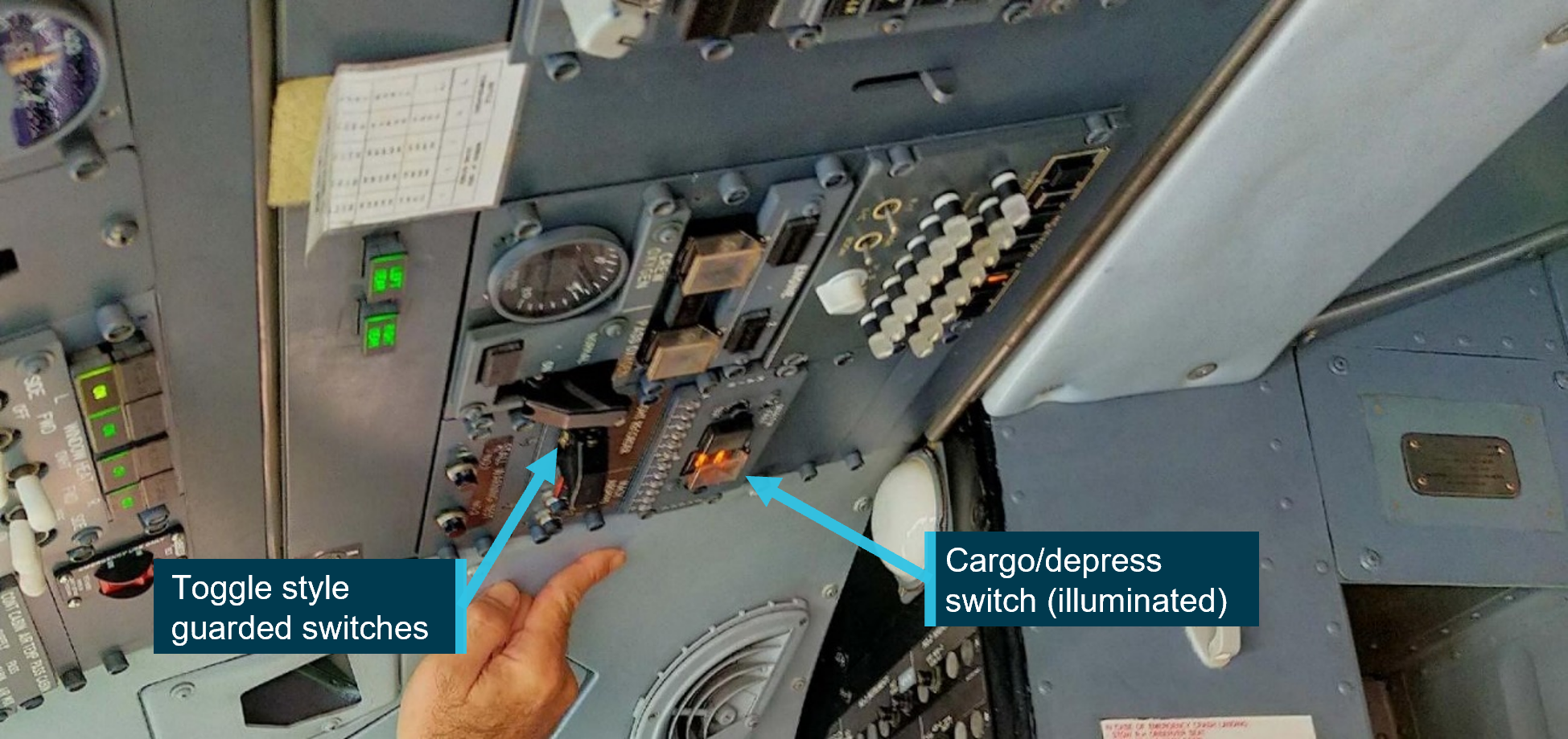
“On arrival it was identified that the guarded cargo/depress switch was on,” ATSB’s Dr Michael Walker said.
“This switch was normally only used in the event of a main cargo deck smoke event, when it will depressurise the aircraft to assist smoke removal.”
The ATSB found the switch had been turned on by a maintenance engineer during pre-flight preparation, in an attempt to cool the flight deck. The engineer omitted to turn the switch off prior to completing their duties, and this was not identified by the flight crew.
“Using the switch in this manner was not authorised, but it had become normalised by the operator’s staff in Darwin, where there was no ground support equipment to provide external cooling,” Dr Walker said.
“Even though this practice had become normalised, there were insufficient risk controls in place to ensure that the aircraft would be returned to the correct configuration prior to departure.”
Additionally, the ATSB investigation found a pre-flight check of the switch was not incorporated into the operator’s flight crew operating manual, despite the aircraft’s cargo conversion operations manual stipulating it as a requirement.
Since the incident, the operator issued communications to its staff to immediately cease the unauthorised practice, and remind staff to only operate equipment in accordance with approved documentation.
Additionally, the operator commenced a review of operational documentation and completed incorporating the requirements of the operations manual supplement.
“This incident highlights the risks associated with undertaking unauthorised practices and using equipment in a manner other than for its intended purpose,” Dr Walker said.
“Without formal assessment of its efficacy or its potential for unintended consequences, combined with no documentation of training, there is no assurance that an unauthorised practice would be carried out consistently or safely.”
Sun glare and a required radio frequency change meant it was unlikely that the pilot of a LongRanger helicopter saw or had time to avoid a wedgetail eagle before the helicopter struck the bird, an ATSB investigation details.
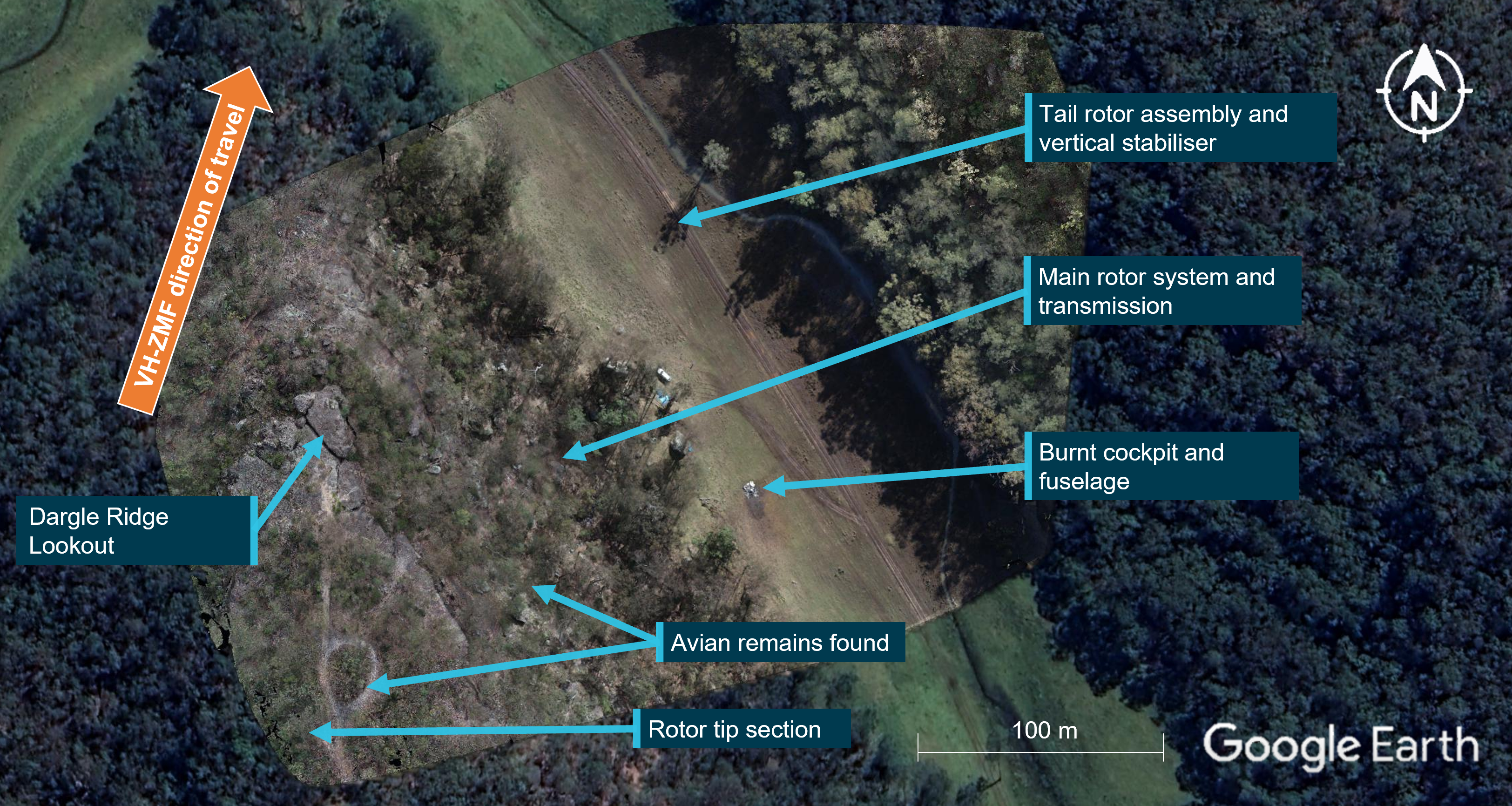
The Bell 206L-1 LongRanger helicopter had departed a private property at Cattai, north-west of Sydney, for a short flight north to nearby St Albans on the morning of 9 July 2022. About 9 minutes into the flight, as the helicopter crossed Dargle Ridge at a height of about 500 feet above the ground, the helicopter struck a wedgetail eagle just below the front left windscreen.
“The pilot was likely startled by sighting the bird or the helicopter striking the bird, reacting via abrupt control inputs,” said ATSB Director Transport Safety Dr Stuart Godley.
“Unfortunately, these inputs led to the main rotor striking and severing the tail boom, and the helicopter breaking up in flight.”
Several witnesses described seeing the helicopter enter into a rapid banking turn to the right while pitching up, and hearing several rotor beats change tone before a final louder noise.
Witnesses then recalled the helicopter pitching and rolling while descending, with one witness describing separation of the main rotor blades from the helicopter.
The main fuselage subsequently impacted the ground below the ridge in an area of open farmland. The pilot was fatally injured and the helicopter was destroyed by a post-impact fire.
Footage taken from a media helicopter, which was in the area filming flooding and had landed near the accident site to render assistance, showed biological matter on the accident helicopter’s left nose cowl before the wreckage was consumed by the fire. Other bird matter and biological tissue was recovered from the accident site.
Subsequent testing of the specimens by the Australian Centre for Wildlife Genomics confirmed them as being from an Aquilaaudax, or wedgetail eagle.
At the time of the accident the weather conditions were described as sunny, with light winds, blue skies and little cloud. However, an assessment of the time of day (about 1145am) and sun position relative to the aircraft’s altitude and track direction indicated that the helicopter was flying directly into the sun.
Further, due to the size and shape of the helicopter’s windscreen, the sun was almost directly at the top of centre of the pilot’s field of view.
The accident also occurred as the helicopter approached the control boundary for airspace surrounding the nearby Richmond air base, requiring the pilot to change radio frequencies. This meant the pilot needed to shift their vision and attention from outside of the cockpit to inside the cockpit to change the frequency on the radio.
“It was unlikely that the pilot saw or had time to avoid the wedgetail eagle due to sun glare and the required radio frequency change.”
Dr Godley noted that birdstrikes are a common occurrence in aviation. In the 5 years between 2018 and 2022, 212 birdstrikes involving helicopters were reported to the ATSB, however only one of those, the accident flight, resulted in the loss of the helicopter.
More broadly, over the 15 years between 2008 and 2022, 24,106 birdstrikes were reported to ATSB for all sectors of aviation.
“Birdstrike is sometimes an unavoidable and relatively common hazard for all aviation operations, one which is more prevalent at lower altitudes,” Dr Godley said.
“A sound lookout and visual scanning processes, as well as avoidance of low-level flight and expected areas of large concentrations of birds are key to reducing the likelihood of birdstrike.”
On 7 May 2023, the pilot of a Diamond Aircraft Industries Inc. DA 40, registered VH-ERE and operated by Flight Training Adelaide, was conducting a solo training flight from Sunshine Coast Airport, Queensland to Brisbane West Wellcamp Airport, Queensland.
At about 1328 local time, the DA 40 entered the runway 31 strip without a clearance resulting in a Boeing 737 aircraft that had been cleared to land conducting a go around.
What the ATSB found
The ATSB found that the pilot incorrectly thought they were holding at a taxiway intermediate holding position due to the distance from the holding point to the threshold and this was reinforced due to misunderstanding of a required instruction from the air traffic control to hold short at runway 31. As a result, they crossed the holding point in anticipation of there being a second holding point closer to the runway.
The ATSB also found that due to the angle of the taxiway in relation to the runway, it would have been difficult for the pilot to have seen the 737 aircraft on final. It is also likely that the crew of the 737 would not have seen the aircraft cross the holding point as it was obscured. Further, although not required to, the information in the Airservices Australia Departure and Approach Procedure charts and the Enroute Supplement did not indicate the holding point locations. Finally, while the Civil Aviation Safety Authority Manoeuvring map for the Sunshine Coast Airport did include the occurrence holding point, neither it nor the runway were accurately depicted.
What has been done as a result
The operator conducted an internal investigation into the runway incursion and has taken the following safety actions:
a NOTAC[1] was issued to address landings in controlled zones, at airports other than home base, and solo flights to controlled zones
a qualified flight instructor (QFI) meeting was conducted to communicate the importance of students understanding the signs, markings, lights and phraseology particularly when at a controlled aerodrome
a student meeting was conducted to reiterate the points outlined in the QFI meeting.
the results of class G and class C & D airspace quizzes appear in the monthly students reports to QFIs
existing tutorials for class D, class C, Sunshine Coast Airport, Archerfield Airport, and Gold Coast Airport were reviewed and updated
an exam and quiz specifically for Sunshine Coast Airport has been created
quizzes for Sunshine Coast Airport, Archerfield Airport, and Gold Coast Airport have been made mandatory for all students before visiting these airports.
The operator is also in the process of reviewing the:
requirements for solo flights to controlled zones, including the requirement for dual flight before any solo flight to any of the training controlled zones
forms used by QFIs for issuing flight plans in controlled zones.
Sunshine Coast Airport, through its safety management process, carried out a review of the occurrence and has undertaken the following safety actions:
Requested an update to the CASA manoeuvring map to correctly identify the runway length, location of displaced threshold and holding point Foxtrot.
The airport has changed the information provided to Airservices Australia in relation to the Aeronautical Information Package (AIP) Enroute Supplement (ERSA) and the Departure and Approach Procedure (DAP) to reflect the runway 31 available take-off distance. Additionally, they have added the distance between holding point Foxtrot and the runway to the additional information section in the ERSA.
The Civil Aviation Safety Authority (CASA) will provide further clarification on the terminology and definition of runway starter extensions and clarity around the runway shading on ERSA and DAP diagrams. CASA has also recommended and supported a runway hotspot depiction at taxiway Foxtrot at the Sunshine Coast Airport to be added to the ERSA and DAP. Finally, the Sunshine Coast manoeuvring map, produced by CASA, has been upgraded to accurately reflect the airport layout.
Safety message
Runway incursions and other runway separation issues are one of the most significant risks to safe aviation operations and are a key global safety priority. This occurrence serves as a reminder to pilots that they should study the most up to date airport information using all available resources if they plan to land at an unfamiliar airport.
In addition, they should never hesitate to ask ATC for clarification if they are unsure or confused about instructions, as it helps prevent potential errors or worse. Common contributory factors and methods of safety controls have been published by Air Services Australia in Runway Incursions at Metro D Aerodromes.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 7 May 2023, a pilot of a Diamond Aircraft Industries Inc. DA 40, registered VH-ERE (ERE) and operated by Flight Training Adelaide, was conducting a solo training flight from Sunshine Coast Airport, Queensland to Brisbane West Wellcamp Airport, Queensland.
At 1322 local time, while parked at the general aviation area on the airport, the pilot contacted air traffic control (ATC) requesting a departure to the south‑west. ATC instructed the pilot to ‘taxi via Foxtrot to holding point[2] Foxtrot runway 31’[3] (Figure 1) and cleared them to depart for Wellcamp via Esk at 4,500 ft. The pilot readback ‘taxi via Foxtrot, use runway 31 and cleared to Esk at 4,500’. ATC reiterated ‘taxi to holding point Foxtrot’ to which the pilot apologised after reading back ‘taxi to holding point Foxtrot’.
Figure 1: VH-ERE taxi path
Source: Google Earth annotated by the ATSB
ATC then turned their attention to a Boeing 737 (737), which was on final for runway 31, and an airport safety car that was escorting an aircraft under tow to the general aviation parking area. At 1327:25, while the 737 was on final approach, ATC cleared it to land on runway 31.
At 1327:40, ERE stopped at holding point Foxtrot and 20 seconds later the pilot radioed ATC and advised ‘holding short of Foxtrot’. ATC observed ERE stationary at the holding point and instructed the pilot to ‘hold short runway 31’ to which the pilot responded ‘Wilco’. ATC then requested a specific readback of the instruction to hold short runway 31 however, the pilot did not respond. Following a second request from ATC, the pilot responded with ‘Hold short runway 31’.
Ten seconds later, while ATC was completing a departure clearance for another aircraft on the ground and updating flight progress strips,[4] ERE proceeded to cross the holding point without a clearance. The pilot later advised misunderstanding the instruction to hold short of runway 31 as they thought they were holding short of taxiway Foxtrot and that there was a second holding point closer to the runway. The driver of the safety car, who could see ERE and had heard the exchange between the pilot and ATC, notified ATC that ERE had ‘gone onto the runway’ as soon as there was a break on the radio. ERE had travelled approximately 74 m in this time.
Figure 2: Location of VH-ERE to inbound aircraft
Source: Sunshine Coast Airport annotated by the ATSB
The controller immediately instructed the 737, which was now on late final about 250 ft above the runway, to conduct a go around. One second after the go around instruction was given, ERE stopped. The pilot advised that as they were nearing the intersection with the runway and after hearing ATC instruct the approaching aircraft to go around, they stopped as they could not see a second holding point. The crew of the 737 advised that they had seen ERE stationary at holding point Foxtrot, however due to the high nose attitude of the aircraft, they lost sight of it under the aircraft’s nose as they continued the approach.
At 1329, ATC advised the 737 to make a left circuit and 20 seconds later instructed ERE to make a right turn and vacate the runway at Foxtrot. The pilot turned the aircraft around and taxied back on taxiway Foxtrot and after passing the holding point, was instructed by ATC to turn around and hold position. The 737 landed on runway 31 uneventfully 6 minutes later.
At 1337, ATC advised ERE to taxi ahead and hold short of runway 31 on Foxtrot. The pilot taxied on Foxtrot and just prior to reaching the holding point, ATC advised the pilot that they were at the holding point and described the markings.
At 1341, ATC instructed ERE to line up on runway 31, however, before they entered the runway ATC confirmed with the pilot that they were okay to continue the flight, to which the pilot replied, ‘all good’. ATC then cleared ERE for take-off and the pilot conducted an uneventful take-off and flight to Brisbane West Wellcamp Airport.
Context
Pilot
The pilot held a student pilot licence. They commenced training on 12 September 2022 at Brisbane West Wellcamp Airport. At the time of the occurrence, they had a total flying experience of 132.5 hours, of which 33.7 hours had been in the previous 30 days.
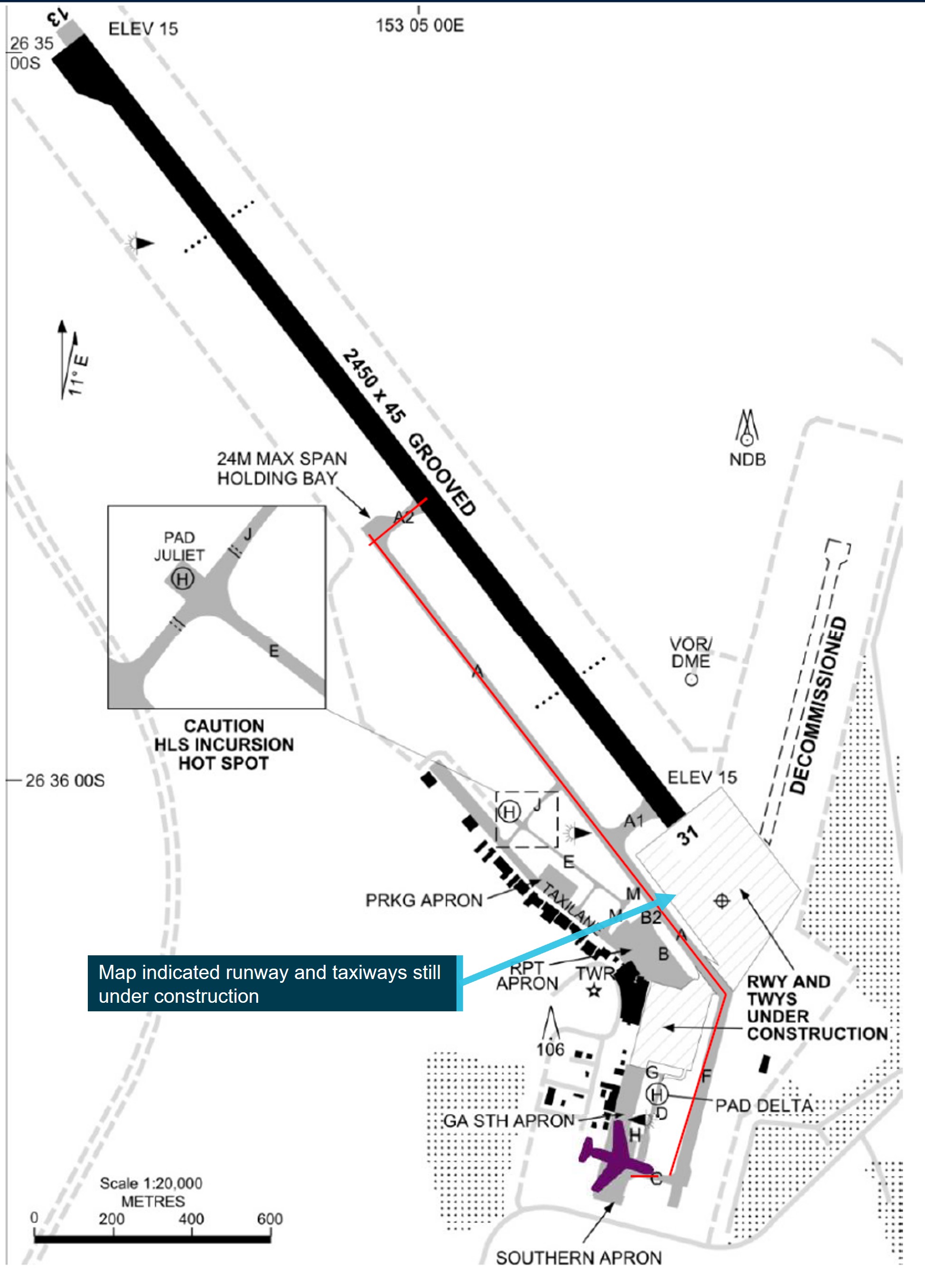
Runway and taxiway information
In June 2020, stage 1 construction of a new runway was completed and officially handed over to the Sunshine Coast Airport for operation. Stage 2, which included the completion of the displaced threshold, was completed in December 2020. The runway has an orientation of 128 degrees/308 degrees magnetic, giving the runway its 13/31 designation. The runway length is 2,800 m, which includes a 175 m permanently displaced threshold for runway 31 and a 170 m starter extension.[5] The airport operates within Class D airspace.
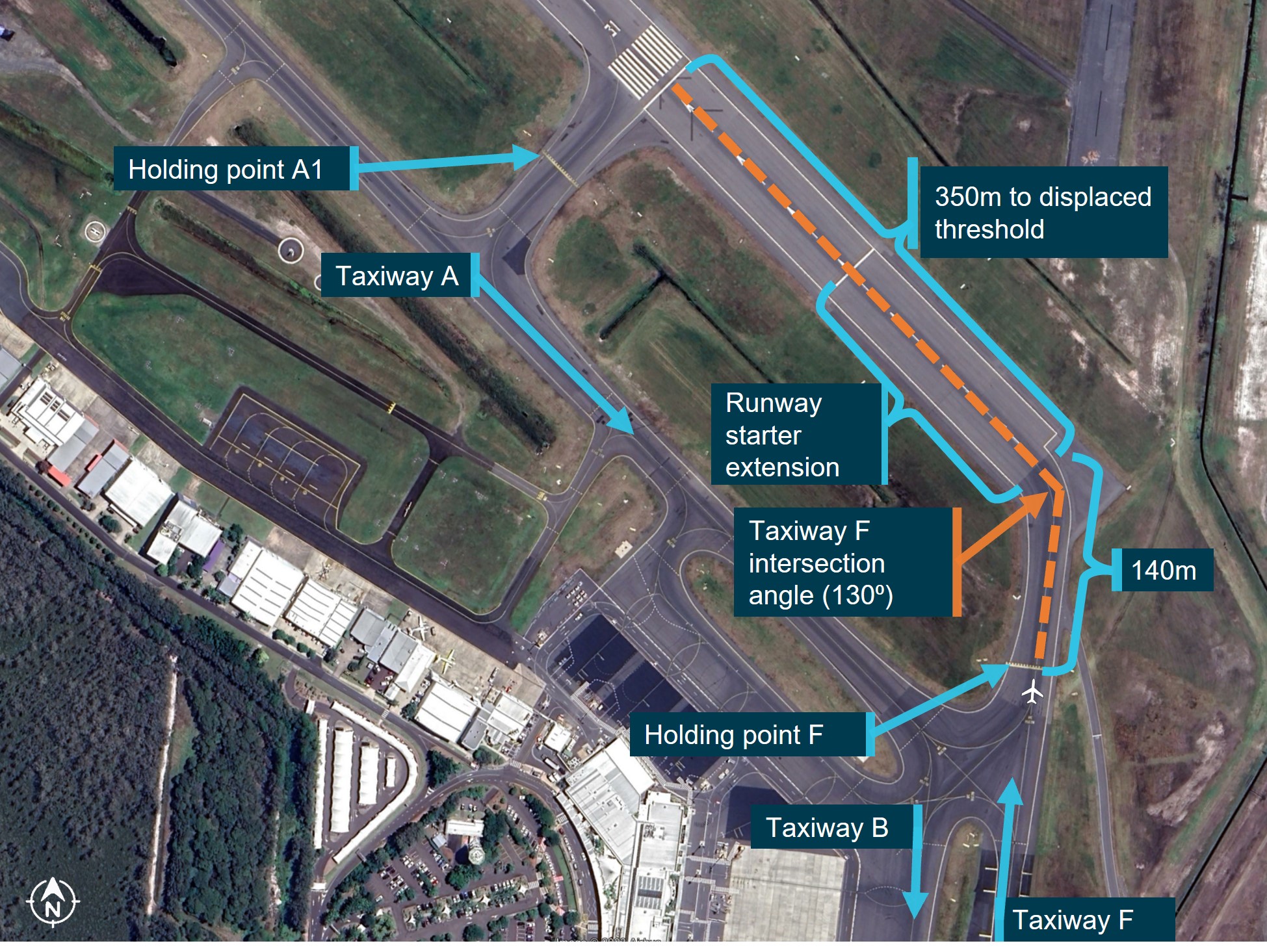
Taxiway Foxtrot is the repurposed southern end of the decommissioned runway 18/36. Due to the angle between the taxiway and runway 31 (approximately 130⁰ - Figure 3), there is approximately 140 m of taxiway from holding point Foxtrot to the intersection with runway 31 required to ensure that the holding point remained outside of the runway strip. Once reaching the intersection, there is approximately 350 m to the displaced runway threshold.
Figure 3: Taxiway Foxtrot in relation to the runway and other taxiways
Source: Google Earth annotated by the ATSB
Airport diagrams
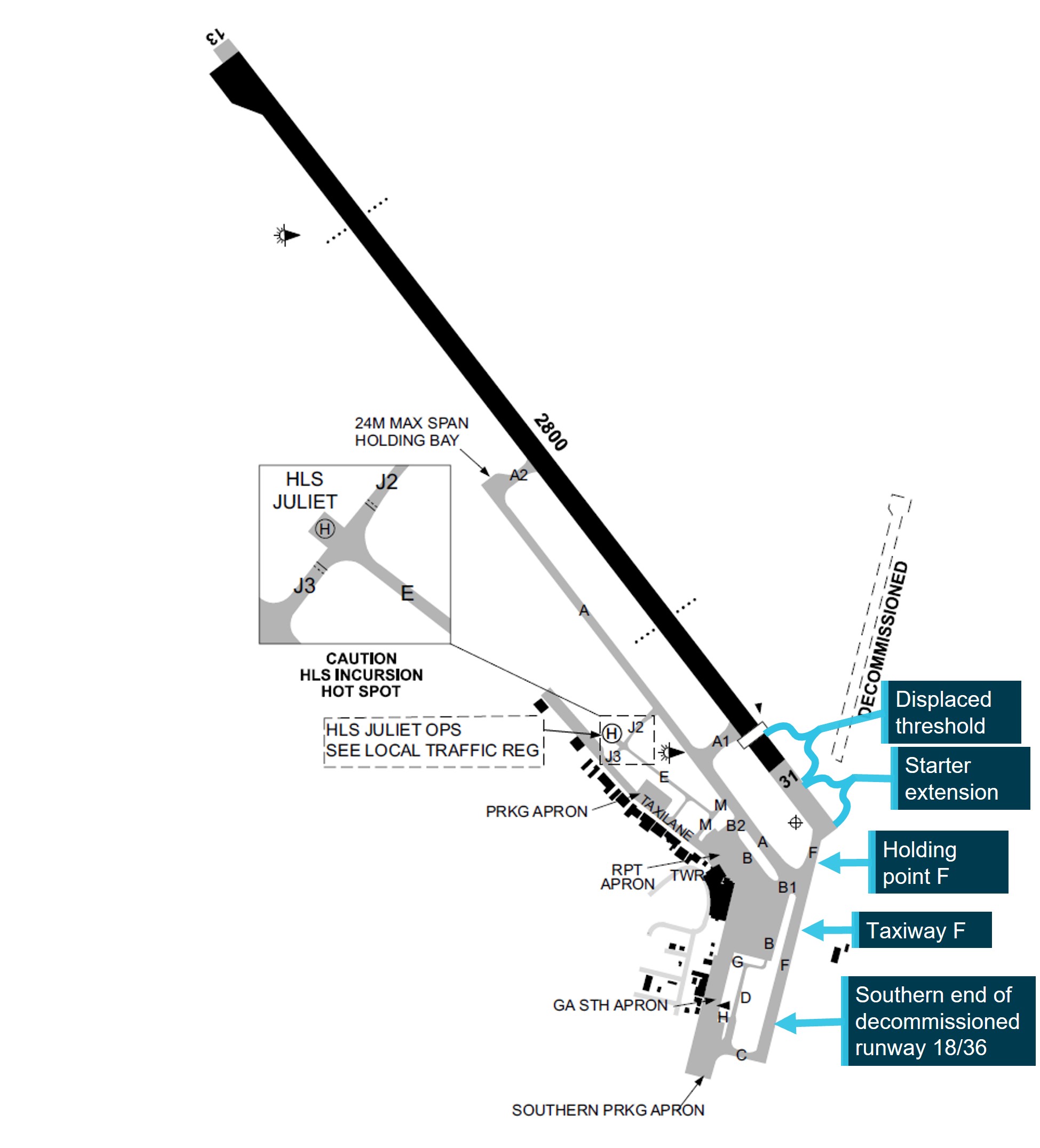
The airport diagram for the Sunshine Coast Airport in the Aeronautical Information Publication (AIP) Enroute Supplement (ERSA) (Figure 4) and the Departure and Approach Procedure (DAP) chart did not indicate any specific holding point locations. In the additional information section in the ERSA, it did not indicate the distance from the holding point to the runway junction. In addition, the ERSA did not indicate the full length of the runway (2800 m) in black shading, which is used to depict the length of runway available for take-off.
The information in these charts is supplied to Airservices Australia as the publishing body, by the Airport owner. The Civil Aviation Safety Regulations Part 139 Manual of Standards (MOS) Chapter 5 Division 2 Standards for information stipulates what information is required to be presented in the AIP documents. This did not require that holding points be depicted in the diagrams. However, International Civil Aviation Organisation Annex 4 Aeronautical charts section 13.6 (g) required that runway holding positions be marked. Australia had filed a difference with ICAO in relation to this requirement.
In addition, Part 139 MOS did not have a definition of a runway starter extension and did not outline the runway shading requirements when a runway starter extension was present.
Figure 4: ERSA Sunshine Coast airport diagram
Source: Airservices Australia annotated by the ATSB
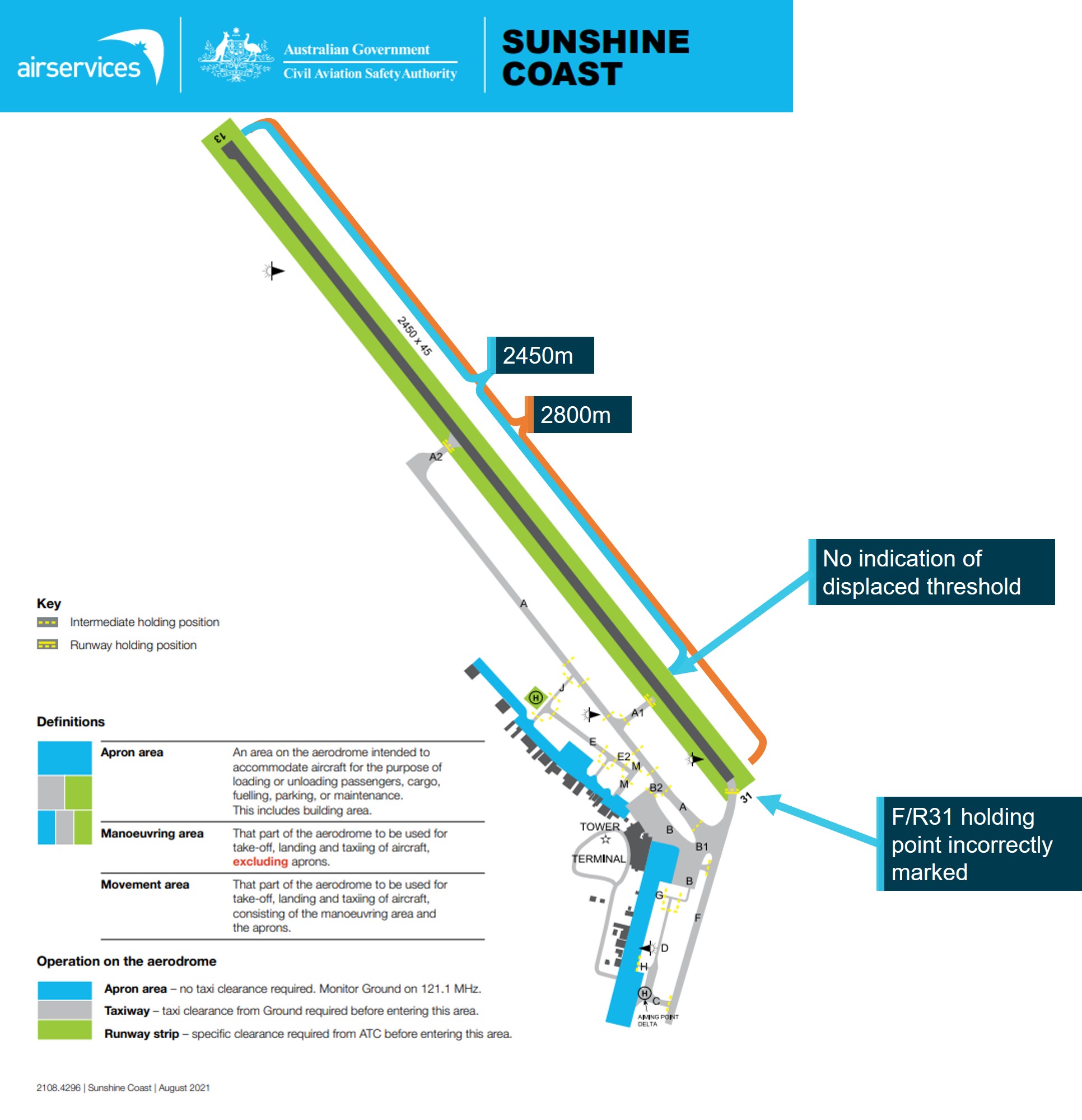
The Civil Aviation Safety Authority (CASA) aerodrome manoeuvring map for Sunshine Coast Airport (Figure 5) indicated that the entire length of the runway was 2,450 m and did not display the extra 350 m of displaced threshold. Additionally, the placement of holding point Foxtrot was not accurately depicted, with it being shown approximately 110 m closer to the intersection of the taxiway and extended runway. The map did not show the decommissioned runway.
Figure 5: Aerodrome Manoeuvring Map for Sunshine Coast
Source: CASA Aerodrome Manoeuvring Map for Sunshine Coast annotated by the ATSB
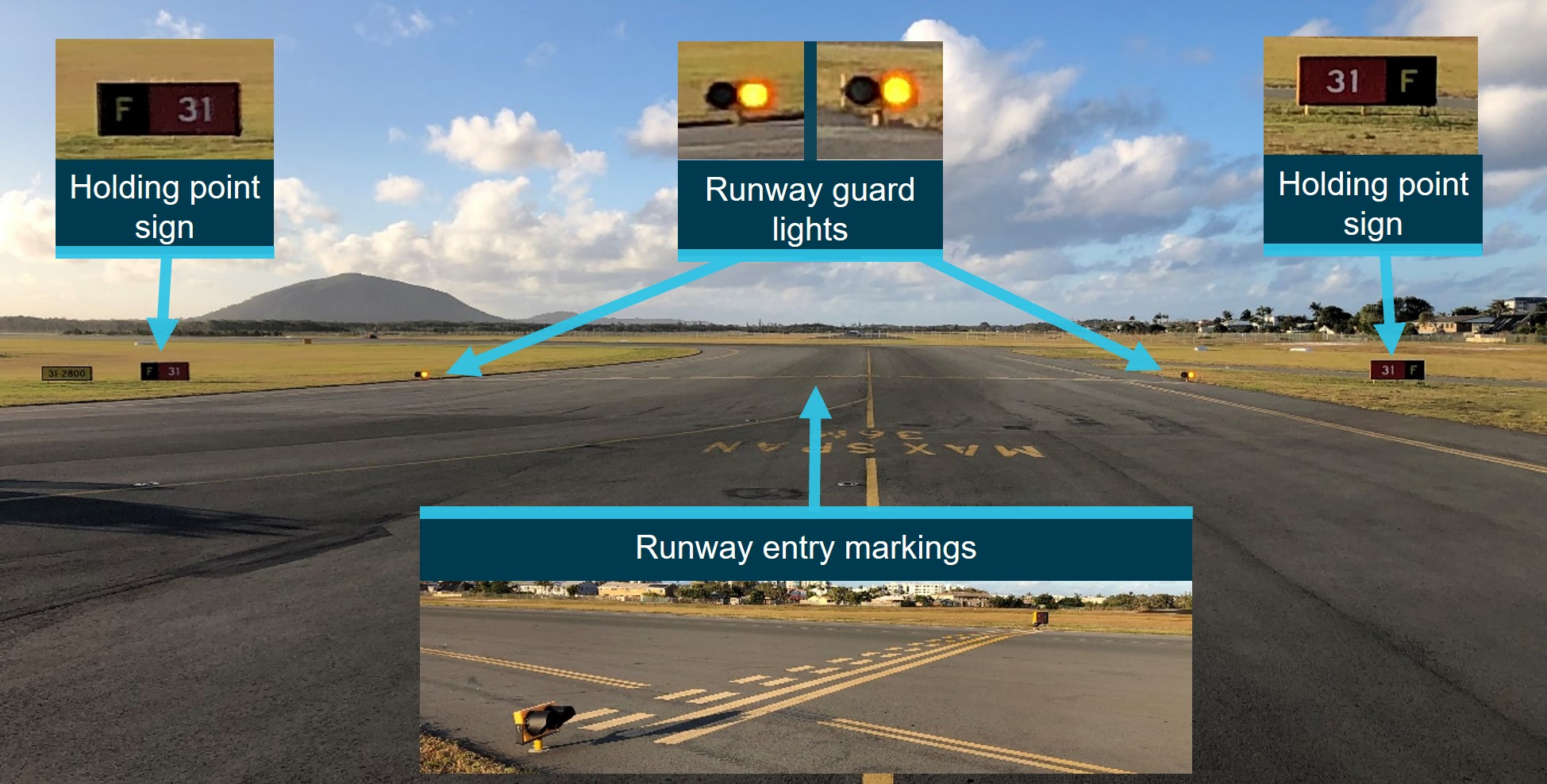
Holding point Foxtrot
Holding point Foxtrot was equipped with signage and ground markings to provide flight crews with visual cues indicating their position and proximity to the runway strip (Figure 6). The holding point was also equipped with runway guard lights which sat 30 cm above the ground on either side of the taxiway. These were bright yellow, and flashed when the runway was in operation.
The gable markers at the intersection between taxiway Foxtrot and runway 31 were in an irregular configuration to delineate the extent of the graded runway strip. Due to the location of the taxiway intersecting at the corner of the runway strip, flush rather than raised gables were provided at the taxiway shoulder. The gable that would be within the taxiway has been omitted. These differences were conducted under CASA approval.
Figure 6: Holding point markings, signage and lights
Source: Sunshine Coast Airport annotated by the ATSB
From the control tower, which is approximately 400 meters from holding point Foxtrot, the entire length of taxiway Foxtrot, the holding point and the displaced threshold of runway 31 are visible.
Figure 7: View of holding point Foxtrot from the Sunshine Coast Airport control tower
Source: Air Services annotated by the ATSB
Training and briefings
The operator had multiple training documents on runway markings and signs. Students were also taught ground basics at the commencement of their training. Prior to flying solo to any airport in Class D airspace, the operator required that they complete a competency check. They also had a guidance section which included that ‘the student must first have demonstrated competence on two visits to the same aerodrome without instructor takeover’.
The training school records indicated that the pilot had completed the required competency check for operating to a Class D airspace on 18 April 2023, flying into Archerfield Airport, Queensland. The pilot had also completed 3 training flights to Sunshine Coast Airport, 2 flights with an instructor on 28 March and 4 April 2023, and a solo flight on 5 May 2023. None of these flights had required the use of holding point Foxtrot.
The operator had a briefing for Sunshine Coast Airport that contained:
communication frequencies for the airport and surrounds
reference points for training flights
inbound and outbound information
ground information.
The information relating to the runways and taxiways contained a graphic of the runway and taxiways at Sunshine Coast Airport (Figure 8) prior to the runway extension and taxiway Foxtrot completion in 2021. The map showed only 2 runway holding points: A1 and A2.
Figure 8: Sunshine Coast Airport map used in the operator airport briefing for students.
Source: Flight Training Adelaide annotated by the ATSB
Pre-flight briefing
On the occurrence flight, the student used the current ERSA for planning and runway information, and the departure and approach procedures (DAP) available at the time for ground information while taxiing at the airport. The student’s instructor reported that prior to the flight, when a briefing of the airport layout was conducted with the student, only holding points A1 and A2, and the location of general aviation parking were discussed.
Other occurrences
The ATSB has investigated previous runway incursions at various locations throughout Australia, including:
Runway incursion involving Beech Aircraft Corp. 58, VH-NSK Bankstown Airport, New South Wales, on 26 October 2021 (AO-2021-046)
Runway incursion involving a SAAB 340B, VH-ZRH Carnarvon Airport, Western Australia, on 31 August 2020 (AO-2020-045)
Runway incursion involving Sling 2, VH-ZSD Moorabbin Airport, Victoria, on 23 July 2020 (AO‑2020-037)
Runway incursion and communication issues involving Bombardier Dash 8, VH-LQJ, Gladstone, Queensland, on 17 March 2020 (AO-2020-019)
Runway incursion involving Boeing 737, VH-XZM, resulting in a rejected take-off involving Boeing 737, VH-VZL, Perth Airport, Western Australia, on 28 April 2018 (AO-2018-032)
Safety analysis
The pilot was familiar with the runway configurations at Sunshine Coast Airport having flown to the airport previously. However, having never used taxiway Foxtrot, they were unfamiliar with the length of taxiway from holding point Foxtrot to the intersection with the runway associated with the oblique angle between them, and the displaced threshold on runway 31. Due to this distance of almost 500 m, they incorrectly assessed that they were holding at a taxiway intermediate holding position, despite the visible difference between the marking of runway and intermediate hold points and the correct lighting and signage at the holding point. This error was reinforced when the pilot received instructions to ‘hold short runway 31’, as the change in terminology from ATC led them to believe there was an additional holding point closer to the runway. At this point, and while unsure where any additional holding point might be located, the pilot did not ask ATC for clarification on the instructions and instead proceeded to cross the holding point. As the pilot did not expect to enter the runway strip, they did not scan for incoming aircraft. While they had heard an aircraft being cleared to land, they were unaware of the aircraft’s proximity to the runway.
The controller had given the 737 clearance to land prior to ERE reaching the Foxtrot holding point. At that stage, the landing path for the 737 was clear. The controller visually confirmed ERE had stopped at the holding point and had ensured they had read back that they were to ‘hold short runway 31’ prior to turning their attention to another aircraft. The controller was not required to check the landing path for the 737 again until immediately before the aircraft crossed the threshold.
Due to the angle of taxiway Foxtrot to the runway, a pilot in the left seat of an aircraft would need to scan for landing aircraft at an angle of 125–130⁰ from directly ahead. As explained in ATSB report AS-2022-001, a normal field of view is approximately 190° (95° either side of the forward view). This would have placed the approaching 737 outside the normal field of view of the pilot of ERE. It is also likely that the pilot was concentrating to the front of the aircraft as they were looking for a holding point. In addition, the pilot was sitting on the left side of the aircraft and so their view would also have been blocked by aircraft structure. This would have required them to move forward in the seat to have visibility of an aircraft on final approach.
The crew of the 737 did not know ERE had crossed the holding point as their view was obscured by the nose of the aircraft. As such, they were unaware of the runway incursion and would likely not have taken evasive action if they had not been instructed to conduct a missed approach. The aerodrome reporting officer (ARO) proactively alerted ATC to the incursion and reduced the likelihood of a serious incident.
The ERSA and the DAP diagrams for the Sunshine Coast Airport did not include holding point locations. While the ERSA was not required to show the locations of holding points, inclusion of this information reduces the potential for confusion or ambiguity around their position. Also, the marking used on the runway diagram to depict the take-off distance available was not accurate. Additionally, the CASA aerodrome manoeuvring map for Sunshine Coast Airport did not give an accurate representation of the holding points or the runway and, if compared to the ERSA, would increase confusion for pilots.
The operator’s briefing documentation on the layout of Sunshine Coast Airport was also not current and did not provide the correct information to students. However, this was found not to have contributed to the pilot’s lack of understanding of the airport taxiway layout and markings as the pilot was using the ERSA for pre-flight planning and the DAP as a location reference while at the airport, and so had the latest available information about the runway layout at the airport.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the Runway incursion involving Diamond Aircraft Industries Inc. DA 40, VH-ERE that occurred at the Sunshine Coast Airport, Queensland on 7 May 2023.
Contributing factors
The student misinterpreted the instruction given by ATC and their location in relation to the runway, resulting in their aircraft entering the runway strip while a Boeing 737 was on final approach.
The Airservices Australia‑published Departure and Approach Procedure chart (DAP) for the Sunshine Coast Airport did not indicate the position of the holding point on taxiway Foxtrot, which added to the confusion of the pilot when instructed to hold short of runway 31.
Other factors that increased risk
The oblique angle of the taxiway to the runway meant that the pilot of the DA 40 would not have had the Boeing 737 within their normal field of view and the 737 pilots on final would not have seen the Diamond as it was obscured under the nose of the aircraft while on final approach. This limited both crew's ability to react without intervention from a third party.
The Civil Aviation Safety Authority (CASA) Sunshine Coast manoeuvring map did not accurately depict the position of holding point Foxtrot and the large runway displacement.
Other factors
The aerodrome reporting officer (ARO) proactively alerted ATC to the incursion and as such reduced the likelihood of a serious incident.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action by Flight Training Adelaide
Flight Training Adelaide conducted an internal investigation into the runway incursion and has actioned the following safety actions:
A notice to crew (NOTAC) was issued to address landings at controlled zones, airports other than home base, and solo flights to controlled zones.
A qualified flight instructor (QFI) meeting was conducted to communicate the importance of students understanding the signs, markings, lights and phraseology, particularly when at a controlled aerodrome.
A student meeting was conducted to reiterate the points outlined in the QFI meeting.
The results of class G and class C & D airspace quizzes appear in the monthly students reports to QFIs.
Existing tutorials for class D, class C, Sunshine Coast Airport, Archerfield Airport, and Gold Coast Airport were reviewed and updated.
An exam and quiz specifically for Sunshine Coast Airport has been created.
Quizzes for Sunshine Coast Airport, Archerfield Airport, and Gold Coast Airport have been made mandatory for all students before visiting these airports.
The operator is also in the process of reviewing the:
requirements for solo flights to controlled zones, including the requirement for dual flight before any solo flight to any of the training controlled zones
forms used by QFIs for issuing flight plans in controlled zones.
Safety action by Sunshine Coast Airport
Sunshine Coast Airport, through its safety management process, carried out a review of the occurrence and has undertaken the following safety actions:
Figure 9: New runway holding point markings at Sunshine Coast Airport
Source: Sunshine Coast Airport
Requested an update to the CASA manoeuvring map to correctly identify the runway length, location of displaced threshold and holding point Foxtrot.
Changed the Aeronautical Information Publication (AIP) Enroute Supplement (ERSA) and the Departure and Approach Procedure (DAP) to reflect the full length of runway 31. Additionally, the distance between holding point Foxtrot and the runway has been added to the additional information section in the ERSA.
Safety action by the Civil Aviation Safety Authority
The Civil Aviation Safety Authority (CASA) has taken the following safety actions:
provided clarity around the runway shading on ERSA and DAP diagrams
upgraded the Sunshine Coast manoeuvring map to accurately reflect the airport layout.
recommended and supported the addition of a runway hotspot depiction at taxiway Foxtrot at the Sunshine Coast Airport to the ERSA and DAP.
CASA further advised that clarification on the terminology and definition of runway starter extensions will be added to the Part 139 MOS. They are also in the process of transferring the Aeronautical Information Package to digital form, which includes transferring all runway maps to digital versions. This will allow a more detailed map to be available.
Sources and submissions
Sources of information
The sources of information during the investigation included:
the involved pilots and air traffic controller
Airservices Australia
Flight Training Adelaide
References
Australian Transport Safety Bureau (2022). AS-2022-001 - Aircraft performance and cockpit visibility study supporting investigation into the mid-air collision involving VH-AEM and VH-JQF near Mangalore Airport, Victoria on 19 February 2020. Canberra: Australian Transport Safety Bureau
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the involved pilots and air traffic controller
Sunshine Coast Airport
Flight Training Adelaide
Qantas
Civil Aviation Safety Authority
Airservices Australia
Submissions were received from:
the air traffic controller
Sunshine Coast Airport
Flight Training Adelaide
Civil Aviation Safety Authority
Airservices Australia
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] NOTAC: The purpose of the NOTAC is to communicate information on new or changed policies and procedures and matters of an urgent or safety related nature affecting the proper and legal flying operations of the operator.
[2] Holding point: Signifies the entry to the runway environment.
[3] Runway number: the number represents the magnetic heading of the runway.
[4] Flight progress strip: Controllers use fight progress strips to maintain situation awareness of ATC operations and traffic. Standard annotations (such as recording the departure runway/location) provide information to assist with the correct execution of the controller’s plan and the early detection of any errors that may occur.
[5] Starter extension: an additional runway length made available for take-off, prior to the normal runway end at the commencement of the take-off run.
Occurrence summary
Investigation number
AO-2023-023
Occurrence date
09/05/2023
Location
Sunshine Coast Airport
State
Queensland
Report release date
27/10/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Runway incursion
Occurrence class
Serious Incident
Highest injury level
None
Aircraft details
Manufacturer
Diamond Aircraft Industries
Model
DA40
Registration
VH-ERE
Serial number
40.736
Aircraft operator
Flight Training Adelaide Pty Ltd
Sector
Piston
Operation type
Part 142 Integrated and multi-crew pilot flight training
Departure point
Sunshine Coast Airport, Queensland
Destination
Wellcamp Airport, Toowoomba, Queensland
Damage
Nil
Aircraft details
Manufacturer
The Boeing Company
Model
737-838
Registration
VH-VYD
Serial number
33992
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
In the evening of 29 April 2023, 2 Qantas Boeing 737-838 aircraft were undertaking operations from runway 16L at Sydney Airport, New South Wales. VH-VZW was on final approach to land while VH-VZM was preparing to take off. Shortly after VH-VZM commenced the take-off roll the aerodrome controller identified the spacing between the 2 aircraft had reduced to a distance that could result in compromised runway separation and instructed the crew of VH-VZW to go-around. During the missed approach, the separation between the 2 aircraft reduced to 0.8 NM (1.5 km) horizontally and 330 ft vertically as they climbed away from the runway.
What the ATSB found
The ATSB identified that the go-around instruction issued by the aerodrome controller was delayed by about 12 seconds due to an inadvertent interjection by the tower shift manager. The ATSB also found that the instruction issued to the crew of VH-VZW by the aerodrome controller subsequent to the go-around was interpreted as a cancelation of the published missed approach procedure. Consequently, the crew did not turn left at 600 ft as required by the procedure and instead continued on the runway track.
What has been done as a result
Airservices Australia advised that in response to the occurrence it would, among other actions:
conduct an analysis of landing runway occupancy times at Sydney Airport
add defensive controlling techniques and minimum assignable altitudes for go-around scenarios
conduct an assurance review of go-arounds at Sydney involving a second aircraft requiring controller intervention
add night-time go-around scenarios to compromised separation training.
Safety message
Aerodrome controllers are required to maintain an orderly flow of air traffic, with minimal delays, while ensuring safe separation between arriving and departing aircraft. This complex operation requires controllers to exercise their professional judgement when applying visual separation standards in a variety of environmental and procedural scenarios. In such a setting, it is inevitable that errors will be made by controllers and pilots alike. Consequently, the sociotechnical system within which these activities take place should be designed to be resilient of these errors and reduce the impact individual actions can have on the overall safety of operations.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
In the evening of 29 April 2023, 2 Qantas Boeing 737-838 aircraft were using runway 16L at Sydney Airport, New South Wales:
VH-VZW on final approach to land
VH-VZM awaiting clearance to enter the runway to take off.
VH-VZW was conducting a scheduled air transport flight from Auckland Airport, New Zealand to Sydney Airport, with 2 flight crew, 5 cabin crew and 100 passengers on board. VH-VZM was conducting a scheduled air transport flight to Brisbane Airport, Queensland, with 2 flight crew, 4 cabin crew and 52 passengers on board.
Air traffic control was being provided to both aircraft by the aerodrome controller east (ADCE) in the Sydney Airport tower (see Sydney Airport air traffic control). The wind at the time was 202°–228° at 11–14 kt, the cloud cover[1] was few at 1,500–2,800 ft and scattered at 2,400–4,900 ft, and it was night.
At 1745:39, as a landing Cessna Citation Mustang passed the runway 16L threshold, the ADCE instructed the crew of VH-VZM to line up and wait on runway 16L with an assigned departure heading of 140°. The crew of VH-VZM acknowledged the instruction and taxied the aircraft onto the runway. The crew then waited for take-off clearance. At 1746:07, the ADCE saw that the Mustang was taking longer than anticipated to vacate the runway and instructed the crew to expedite the exit. In total, the Mustang took 73 seconds from landing to vacating the runway, about 23 seconds longer than the ADCE expected.
At 1747:03, the ADCE issued a take-off clearance to the crew of VH-VZM. At this time VH-VZW was about 2.4 NM (4.4 km) from the threshold of runway 16L on approach to land. The crew of VH-VZM pushed the thrust levers forward and waited for both engines to stabilise. This process took about 4 seconds longer than normal due to a permissible unserviceability[2] affecting the performance of one of the engines. At 1747:18, the flight crew pressed the take-off go around (TOGA)[3] button and commenced the take-off.
Meanwhile, VH-VZW was now about 1.7 NM (3.1 km) from the threshold of runway 16L. The captain of VH-VZW, who was pilot monitoring (PM),[4] assessed that the spacing between VH-VZM and VH-VZW had reduced to a distance that would likely result in a ‘go-around’.[5] Consequently, the captain instructed the first officer (FO), who was pilot flying (PF), to mentally prepare for a possible go-around.
The ADCE, also aware of the reduced spacing between the 2 aircraft (see Runway separation standard) and the potential for compromised runway separation, decided to issue a go-around instruction to the crew of VH-VZW and alerted the tower shift manager (TSM) of the situation (see section titled Sydney Airport air traffic control). The TSM moved to look at the runway and began assessing the traffic scenario.
At 1747:22, the ADCE contacted the crew of VH-VZW to issue the go-around instruction. However, before the ADCE issued the instruction itself, the TSM said ‘wait’. The ADCE hesitated for a moment and, having initiated contact and needing to complete the communication, instructed the crew of VH-VZW to continue with the approach to land. The TSM later recalled that they had inadvertently spoken, but their intention was for the ADCE to continue with the go-around instruction. The ADCE then waited for further advice from the TSM, but the TSM did not say anything (the TSM recalled gesturing for the ADCE to continue). The ADCE recalled informing the TSM that they would proceed with the go-around instruction.
At 1747:34, the ADCE instructed the crew of VH-VZW to conduct a go-around. The instruction was acknowledged by the crew of VH-VZW which was now about 1.1 NM (2.0 km) from the runway 16L threshold. At 1747:36 the crew of VH-VZW initiated the go-around from an altitude of about 450 ft. (The ATSB determined that, had the go-around instruction been issued at the original intended time, VH-VZW would have been about 0.5 NM (0.9 km) further from the threshold and 160 ft higher than when the actual instruction was issued.)
At 1747:38, the ADCE issued a further instruction to the flight crew of VH-VZW, stating ‘passing 2,100 turn left heading 090’. The ADCE stated that they were aware of a requirement not to issue a turn instruction to VH‑VZW until it had reached the minimum sector altitude (MSA) of 2,100 ft (see Turn instructions at night below the minimum sector altitude).
Although the flight crew heard the instruction, they did not acknowledge it immediately due to the workload associated with the go-around procedure. They interpreted it as an amended missed approach instruction. As a result, the crew continued to fly the runway track as the aircraft climbed, rather than turning left onto a heading of 125° at 600 ft as was required by the published missed approach procedure (see Missed approach).
Meanwhile, VH-VZM was accelerating along the runway and had passed 87 kt. The captain of VH-VZM heard the go-around instruction issued to VH-VZW and they expected the aircraft to fly the published missed approach procedure and that this would provide sufficient spacing between the aircraft. The captain then monitored the traffic collision avoidance system (TCAS)[6] which displayed a ‘proximate traffic’ indication[7] 600 ft above VH-VZM (which was VH-VZW).[8]
At 1748:03, the ADCE asked if the crew of VH-VZW had received the instruction to turn left onto a heading of 090° on passing 2,100 ft, to which they responded that they had. The ADCE and the TSM visually observed the 2 aircraft as they climbed away from the runway. They also had a surveillance display showing the dispositions of aircraft in the vicinity of the airport. During this time the TSM no longer felt ‘comfortable’ with the separation between the 2 aircraft. As a result, the TSM recalled advising the ADCE that they should issue a safety alert and turn VH-VZW away from VH-VZM (see Reduced separation and safety alerts).
At 1748:17, the ADCE issued a safety alert to VH-VZW stating ‘safety alert traffic 12 o'clock low heading 140 if you're visual turn left now’. At 1748:24, the crew of VH-VZW initiated a left turn while climbing through 1,533 ft. The TSM recalled further stating to the ADCE that the aircraft needed to be turned further onto a heading of 060°.
At 1748:32, when VH-VZW was at an altitude of 1,710 ft and not climbing as fast as the ADCE expected, the ADCE issued a further instruction to the crew to turn left onto a heading of 060° to put the aircraft onto diverging flightpaths sooner. The ADCE determined that such an instruction carried less risk than permitting the scenario to continue until VH-VZW had reached the MSA. While VH-VZW was below the MSA when issued the instruction to turn, the ADCE was confident that the aircraft was above the highest obstacles in the vicinity. This instruction was acknowledged by the flight crew and the aircraft continued the left turn onto the new heading.
At 1748:38, the closest slant range between the 2 aircraft occurred, with separation reducing to 0.8 NM (1.5 km) horizontally and 330 ft vertically (Figure 1). Neither crew had visual contact with the other aircraft and no TCAS resolution advisory[9] or traffic advisory[10] was triggered. The controllers had both aircraft in sight throughout the occurrence, and the ATSB later assessed that the visual and surveillance information available to the controllers in the tower, accounting for the possibility of visual errors, was sufficient for visual separation[11] to be maintained.
Figure 1: Overview of aircraft flight paths
White lines link the locations of the two aircraft at the same point in time.
Source: Google Earth, annotated by the ATSB
With VH-VZW continuing to turn towards the east-north-east, the 2 aircraft began to diverge. At 1749:03, the ADCE transferred VH-VZM to the departure controller and the aircraft continued to its destination. At 1749:44, the ADCE transferred VH-VZW to the Sydney Airport director and the aircraft later landed on runway 16R.
Context
Personnel information
VH-VZM flight crew
Both flight crew held an air transport pilot licence (ATPL) aeroplane and Class 1 aviation medical certificate. The captain had a total of 12,413 hours of aeronautical experience, including 2,301 hours on 737 variants. The captain reported feeling ‘okay, somewhat fresh’ at the time of the occurrence. The first officer had 11,700 hours of aeronautical experience, including 7,800 hours on 737 variants. The FO reported feeling ‘very lively, responsive, but not at peak’ at the time of the occurrence.
VH-VZW flight crew
Both flight crew held an ATPL aeroplane and Class 1 aviation medical certificate. The captain had a total of 13,220 hours flight time, with 9,430 hours on 737 variants. They reported feeling ‘fully alert’ at the time of the occurrence. The FO had a total of 8,100 hours flight time, with 2,650 hours on 737 variants.
Aerodrome controller east
The ADCE had about 14 years experience as an approach and tower controller with the Royal Australian Air Force and then Airservices Australia. They had been operating in the Sydney Airport tower for about 3 years and held endorsements for the aerodrome controller and coordination roles. The ADCE’s last performance assessment (check) prior to the occurrence was completed on 2 March 2023 and they were assessed as competent. They reported feeling ‘alert’ at the time of the occurrence.
Tower shift manager
The TSM had about 10 years’ experience as an enroute and tower controller with Airservices Australia. They had been operating in the Sydney Airport tower for about 5 years and held endorsements for the aerodrome controller, surface movement controller, airways clearance delivery, coordination, and TSM roles. They had been a TSM for about 1 year. The TSM’s last performance assessment prior to the occurrence was completed on 17 March 2023 and they were assessed as competent. They reported that they had slept well and ‘felt fine’ at the time of the occurrence.
Fatigue analysis
Analysis indicated that the ADCE, TSM, and the flight crews of VH-VZM and VH-VZW were probably not experiencing a level of fatigue known to have an adverse effect on performance.
Sydney Airport
Syndey Airport has 2 parallel runways oriented 155°/335° magnetic (16L/34R and 34L/16R) and another runway oriented 062°/242° (07/25). At the time of the occurrence, the airport was operating in parallel runway mode with aircraft taking off and landing on runways 16L and 16R. The elevation of terrain to the east of runway 16L within a radius of 10 NM (18 km), is about 150‑350 ft.
Sydney Airport air traffic control
General information
The Sydney tower was located to the east of runway 16R/34L and south of runway 07/25. There were 8 Airservices Australia[12] personnel located within the Sydney tower at the time of the occurrence. This included the ADCE, who was responsible for providing traffic management to aircraft taking off and landing on runway 16L, and the TSM, who was responsible for the overall operation of the tower. According to Airservices procedures, the TSM was also responsible for the ‘supervision’ of controller activities and held ‘operational command authority’ (OCA) for the Sydney tower.
Supervision and operational command authority
The Airservices Australia National ATS administration manual (NAAM) outlined the procedures associated with the TSM’s supervision and operational command authority responsibilities.
Within the NAAM, the stated purpose of supervision was to ‘provide tactical management of risks while maintaining efficient air traffic operations’ and involved the ‘observation of air traffic service delivery and, where necessary, supporting, intervening, or directing activities within the area of responsibility’.
However, the procedures contained within the NAAM relating to the TSM’s operational command authority (OCA) responsibilities stated:
OCA does not give the holder the authority to instruct an operational controller to take certain actions such as directing a controller to issue an operational control instruction. The operational controller is always responsible for traffic separation but may accept advice from the OCA holder.
The operational command authority held by the TSM gave the role the ‘authority to make decisions on behalf of a unit’ (in this instance the Sydney tower). This authority was described by the TSM as involving a ‘duty of care’ for the overall safety of aircraft traffic managed by Sydney tower.
The NAAM required the TSM to 'initiate and manage necessary short-term mitigation actions’ when a situation occurs that ‘has or may cause a risk to the continued safe operation’ of the airways. These mitigations included workload management, reduction in task complexity, and additional support, observation or supervision. The controllers involved in this occurrence stated that, if the situation necessitated it, it was acceptable for a TSM to issue an instruction to a controller to deconflict an impending or actual unsafe scenario.
Air traffic separation
Visual separation
Throughout the occurrence, the ADCE was providing visual separation to VH-VZW and VH‑VZM. This form of separation required the controller to visually observe the aircraft under their control and apply an azimuth (horizontal) spacing between aircraft.
The Airservices Manual of air traffic services (MATS) stated:
When applying visual separation, consider.
a) aircraft performance characteristics, particularly in relation to faster following
b) aircraft and closure rates;
c) position of the aircraft relative to each other;
d) projected flight paths of the aircraft;
e) possibility of an ACAS [airborne collision avoidance system] RA [resolution advisory] due to closer proximity of operation;
f) known weather conditions; and
g) the possibility of visual errors.
Turn instructions at night below the minimum sector altitude
Aerodrome controllers providing visual separation at Sydney Airport at night or during instrument meteorological conditions were restricted from issuing turn instructions (vectors) prior to an aircraft having reached a minimum sector altitude (MSA)[13] of 2,100 ft.
This restriction was further communicated to Sydney Airport controllers in Airservices Australia standardisation directive DIR_22_0036 (issued 10 June 2022, expired 9 September 2022). This directive referenced the MATS which stated controllers were to ‘assign levels no lower than the applicable LSALT [lowest safe altitude][14] unless the pilot has accepted responsibility for terrain clearance’. The purpose of the requirement was to ensure the controller maintained responsibility for terrain clearance as pilots may not be able to see terrain and obstacles.
Separately, the MATS stated:
Do not allow anything in these instructions to preclude you [the controller] from exercising your best judgement and initiative when:
a) the safety of an aircraft may be considered to be in doubt; or
b) a situation is not covered specifically by these instructions.
Reduced separation and safety alerts
Airservices had a compromised separation recovery training package, which defined compromised separation as occurring when ‘an aircraft is, or without controller intervention will be, in unsafe proximity or at risk of a collision with another aircraft’. In situations where an unsafe proximity existed, a controller was required to issue a safety alert to draw a flight crew’s attention to the traffic scenario. A safety alert was required to be issued as a priority unless the flight crew had advised that action was being taken to resolve the situation or that the other aircraft was in sight.
The ADCE had undergone compromised separation recurrency training in May 2022. The purpose of the recurrency training was to ‘refresh the knowledge and skills’ of the controller to effectively identify and recover a compromised separation scenario. The training was required to be undertaken every 3 years and comprised a computer-based training module, which was generic to all locations, and 4 simulator sessions that involved scenarios specific to the Sydney Airport environment. The ADCE was assessed as competent during these simulator sessions.
Runway separation standards
Runway separation standards ensure sufficient separation between aircraft using the same runway. For an aircraft taking off ahead of an aircraft that is on final approach to land, as was the case for VH-VZM, the standard defined in MATS did not permit a take-off clearance to be issued until:
the arriving aircraft is sighted by the controller and is reasonably assured of landing; or
separation can be assured if the arriving aircraft conducts a missed approach.
For an aircraft landing behind a preceding aircraft that was taking off, as was the case for VH‑VZW, the standard defined in MATS did not permit the landing aircraft to cross the runway threshold until the departing aircraft was airborne and:
had either commenced a turn; or
was beyond the point on the runway at which the landing aircraft could be expected to complete its landing roll and there was sufficient distance to enable the landing aircraft to manoeuvre safely in the event of a missed approach.
Go-around and missed approach
A go-around refers to the action of aborting a landing from final approach or during the touchdown.
A missed approach procedure provides instrument flight rules[15] aircraft with terrain and obstacle clearance along the missed approach path during a go-around. The flight crew of VH-VZW were flying a GBAS landing system (GLS) approach for runway 16L. In the event of a go-around, the missed approach procedure required a flight crew to initially climb to 600 ft and then execute a left turn onto a heading of 125° (Figure 1). The crew were then required to climb to 3,000 ft or as directed by air traffic control.
Figure 2: Sydney GLS runway 16L approach chart with missed approach requirements (blue box)
Source: Airservices Australia, annotated by the ATSB
Related occurrences
ATSB study on loss of separation occurrences in Australian airspace (AR-2012-034)
The ATSB’s study on loss of separation events involving aircraft in Australian airspace (January 2008 – June 2012) found that ‘assessing and planning’ or ‘monitoring and checking’ errors were involved in the majority of individual controller actions that contributed to loss of separation occurrences. This involved the ineffective management of compromised separation before it became a loss of separation event, and controller actions associated with maintaining awareness of traffic disposition.
Unsafe proximity and radar vector below minimum vector altitude involving a Boeing 777‑31HER, A6-EBU, and two 737-838s, VH-VXS and VH-VYE, Melbourne Airport, Victoria, on 5 July 2015 (AO-2015-084)
On the evening of 5 July 2015, land and hold short operations (LAHSO) were in effect at Melbourne Airport, Victoria. During these operations, an Emirates Boeing 777 was cleared for an immediate take-off from runway 34 while 2 Qantas Boeing 737s were on approach to runways 34 and 27. This resulted in the crew of the Boeing 737 on approach to runway 27 initiating a missed approach, followed by the crew of the Boeing 737 on approach to runway 34 being instructed by air traffic control (ATC) to go-around. The Boeing 737 on approach to runway 34 was then radar vectored by ATC below the minimum vector altitude.
The ATSB found that:
The hazard associated with the inability to separate aircraft that are below the appropriate lowest safe altitude at night was identified but not adequately mitigated. This resulted in a situation where, in the event of a simultaneous go-around at night during land and hold short operations at Melbourne Airport, there was no safe option available for air traffic controllers to establish a separation standard when aircraft were below minimum vector altitude.
Airservices subsequently provided training in night operations during land and hold short operations at Melbourne Airport, and introduced a stagger strategy for Melbourne arrivals.
Close proximity involving Boeing 737, VH-VZO and Airbus A330, VH-EBJ at Sydney Airport, New South Wales, on 5 August 2019 (AO-2019-041)
In the evening of 5 August 2019, a Boeing 737 was on approach to land on runway 34R at Sydney Airport while an Airbus A330 had commenced a take-off from the same runway. Shortly after the A330 was cleared for take-off, the ADCE identified that the runway separation standard could not be assured and they instructed the crew of the 737 to go-around. During the subsequent missed approach and turn to the right, the 737 came into close proximity with the A330. Among other findings, the ATSB found that controllers had no procedural controls to draw upon to separate aircraft following similar outbound tracks when they were below the minimum vector altitude, and there were no compromised separation training scenarios involving aircraft below this altitude at night.
Following the occurrence, Airservices included compromised separation scenarios in the Sydney tower controller instructor guide, where an aircraft is operating below the minimum vector altitude at night, and in 2023 Airservices advised that the training program also now included a missed approach with a preceding departure in instrument meteorological conditions.
Safety analysis
The aerodrome controller east (ADCE) instructed the crew of VH-VZM to line up and wait on runway 16L. A take-off clearance could not be issued until a landing aircraft had vacated the runway. This aircraft took about 23 seconds longer to exit the runway than the ADCE had originally anticipated. This extra time meant VH-VZW, which was on final approach to land, was about 2.4 NM (4.4 km) from the threshold when the crew of VH-VZM was issued clearance to take off.
On receipt of the take-off clearance, VH-VZM took about 14 seconds to commence the take-off roll due, in part, to a permissible unserviceability affecting one engine’s performance. This delay further compressed the spacing between the 2 aircraft. Shortly after VH‑VZM commenced the take-off roll, the ADCE identified the spacing between the 2 aircraft had reduced to a distance that meant VH-VZW needed to go around to maintain the runway separation standard. The ADCE also had the option to not issue take-off clearance to the crew of VH-VZM or cancel it during the 14 seconds it took for the aircraft to commence the take-off roll, and this would have prevented the complication of having one aircraft taking off while another was going around.
Having decided to issue a go-around instruction to the crew of VH-VZW, the ADCE’s initial communication was inadvertently interrupted by the tower shift manager (TSM) who said ‘wait’. The TSM later stated that they did not intend to verbalise anything, and they meant for the ADCE to issue the go-around instruction. This verbal slip likely occurred at a time of high workload as the TSM attempted to assimilate the information associated with the traffic scenario.
The verbalisation of ‘wait’ by the TSM interrupted the ADCE’s management of the traffic scenario. While the TSM did not have the authority to direct the ADCE to issue a control instruction, the TSM was able to provide advice to the ADCE. Consequently, the ADCE deferred the go-around instruction for 12 seconds while they waited for the TSM to provide further guidance, which did not eventuate. This 12-second delay meant VH-VZW was 160 ft lower and 0.5 NM (0.9 km) closer to the threshold (and to VH-VZM) by the time the go-around instruction was finally issued.
Four seconds after instructing the crew of VH-VZW to go-around, the ADCE issued further instructions to the crew that required them to turn onto a heading of 090° at 2,100 ft. These instructions were provided to the crew at a time of high workload when VH-VZW had not yet reached 600 ft when they were meant to turn left onto a heading of 125° in accordance with the missed approach procedure. Consequently, the crew misinterpreted the instruction as cancellation of the missed approach procedure and they did not turn at this altitude. The timing of the additional instruction likely added workload compared with letting the crew undertake the go‑around manoeuvre, and the turn at 600 ft, before issuing any further turn instructions.
The TSM and ADCE monitored the 2 aircraft as they climbed away from the runway. During that time the ADCE issued a safety alert to the crew of VH-VZW to advise of the traffic ahead and then vectored the aircraft while it was below the minimum sector altitude. Although contrary to the Airservices Australia standardisation directive, the issuance of this instruction likely reduced the risk associated with the separation occurrence.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the separation occurrence involving Boeing 737, VH-VZM, and Boeing 737, VH-VZW, at Sydney Airport, New South Wales on 29 April 2023.
Contributing factors
The go-around instruction issued by the aerodrome controller was delayed by about 12 seconds due to an inadvertent interjection by the tower shift manager.
The instruction issued to the arriving 737 flight crew by the aerodrome controller subsequent to the go-around was interpreted by the flight crew as an instruction to cancel the published missed approach procedure and continue on the runway track before turning at 2,100 ft. Consequently, the 737 flight crew did not turn left at 600 ft as required by the procedure.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. All of the directly involved parties are invited to provide submissions to this draft report. As part of that process, each organisation is asked to communicate what safety actions, if any, they have carried out to reduce the risk associated with this type of occurrences in the future. The ATSB has so far been advised of the following proactive safety action in response to this occurrence.
Safety action
Airservices advised that it had or would undertake the following safety actions in response to this occurrence:
conduct a detailed analysis of landing runway occupancy times at Sydney, and possibly other major aerodromes, to determine expected runway occupancy times for different types of aircraft (including operator) and conditions (runway direction/wind/time of day/surface condition). This data to be disseminated to ATC [air traffic control] to assist when managing runway separation standards
Sydney tower to add defensive controlling techniques and minimum assignable altitudes applicable to go around scenarios, in particular at night or in IMC [instrument meteorological conditions]
conduct an assurance review examining go arounds at Sydney involving a second aircraft and requiring controller intervention. Specifically, analysing how separation and terrain clearance is being managed and possible reasons behind any unfavourable trending
standardisation directive disseminated to Sydney tower referring to MATS [manual of air traffic standards] 9.4.1.2.1 and outlining the importance of using the MSA [minimum sector altitude] of 2100 ft as the standard at night or in IMC as applicable to go around scenarios
standards to add night-time go around scenarios to compromised separation training
standardisation directive ATS_DIR_23_0037 disseminated to Sydney Tower referring to the NAAM [national air traffic services administrative manual] initial occurrence response requirements to be followed, and the importance of taking steps to assess the risk associated with the potential safety occurrence.
Sources and submissions
Sources of information
The sources of information during the investigation included:
captain and first officer of VH-VZW
captain and first officer of VH-VZM
aerodrome controller east
tower shift manager
flight data from VH-VZM and VH-VZW
air traffic control audio recordings and radar data
Airservices Australia
Qantas Airways
Civil Aviation Safety Authority.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
captain and first officer of VH-VZW
captain and first officer of VH-VZM
aerodrome controller east
tower shift manager
Qantas Airways
Civil Aviation Safety Authority
Airservices Australia.
Submissions were received from Airservices Australia. The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Cloud cover: in aviation, cloud cover is reported using words that denote the extent of the cover – ‘few’ indicates that up to a quarter of the sky is covered, ‘scattered’ indicates that cloud is covering between a quarter and a half of the sky.
[2] An item of equipment that may be inoperative for a limited period until repairs can be made.
[3] The TOGA button changes various autopilot, autothrottle, and flight director settings to initiate a take-off or missed approach.
[4] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[6] Traffic alert and collision avoidance system (TCAS): a type of airborne collision avoidance system that interrogates nearby aircraft and uses this information to calculate the relative range and altitude of this traffic. The system provides a visual representation of this information to the flight crew as well as issuing alerts should a traffic issue be identified.
[7] Proximate traffic: an alert issued when an aircraft is within a range of less than 6 NM and 1,200 ft, or a range of 6 NM if the traffic is not transmitting altitude information.
[8] There were no other aircraft in the immediate area.
[9] Resolution advisory (RA): a manoeuvre, or a manoeuvre restriction, calculated by an airborne collision avoidance system to avoid a collision. Pilots are expected to respond immediately to an RA unless doing so would jeopardise the safe operation of the flight.
[10] Traffic advisory (TA): an alert issued by an airborne collision avoidance system when the detected traffic may result in a conflict. Pilots are expected to initiate a visual search for the traffic causing the TA.
[12] Airservices is Australia's principal provider of air traffic services for civil airports and airspace.
[13] Minimum sector altitude (MSA): the lowest altitude which will provide a minimum clearance of 1,000 ft above all objects in an area. Separately, the minimum vectoring altitude (MVA) was the lowest altitude a controller may assign to a pilot in accordance with a radar terrain clearance chart (RTCC), which was 1,500 ft in the area of the occurrence. In this context, the tower controllers used MSA as the minimum assignable altitude.
[14] The lowest altitude which will provide safe terrain clearance at a given place. LSALT includes MSA.
[15] Instrument flight rules (IFR): a set of regulations that permit the pilot to operate an aircraft to operate in instrument meteorological conditions.
Occurrence summary
Investigation number
AO-2023-022
Occurrence date
29/04/2023
Location
Sydney Airport
State
New South Wales
Report release date
31/01/2024
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Loss of separation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
The Boeing Company
Model
737
Registration
VH-VZM
Serial number
34192
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
Departure point
Sydney Airport, New South Wales
Destination
Brisbane Airport, Queensland
Damage
Nil
Aircraft details
Manufacturer
The Boeing Company
Model
737
Registration
VH-VZW
Serial number
39359
Aircraft operator
Qantas Airways Limited
Sector
Jet
Operation type
Part 121 Air transport operations - larger aeroplanes
A recent incident in which the pilot’s seat of a Sling 2 light aircraft moved fully aft during the take-off roll highlights the importance of ensuring seat mechanisms are free of defects, and that seats are properly locked into position prior to take-off.
As reported to the ATSB by the operator, a student pilot was conducting their first solo flight in early April when, as they began to accelerate for take-off, the fore/aft seat locking mechanism unlatched, and their seat moved fully rearwards, resulting in the pilot being unable to reach the rudder pedals.
Fortunately, the pilot was able to close the throttle, apply the hand brake, and bring the aircraft to a stop on the runway.
A maintenance assessment later found a defect in the seat securing mechanism, and the aircraft was grounded so the issue could be rectified.
“Seat movement during take-off is a dangerous occurrence, and has been a factor in fatal accidents and other serious incidents in the past,” ATSB Director Transport Safety Stuart Macleod said.
In March 2014, a Cessna 206 stalled shortly after take-off and collided with terrain at Caboolture, Queensland, fatally injuring the pilot and four passengers on-board.
“It was likely that the pilot seat rear rail stop was not fitted at the time of the accident,” Mr Macleod said.
“This increased the risk of the seat feet disengaging from the rear of the seat rails if the primary locking pins were not secure or failed, and an uncommanded rearward movement of the seat and subsequent in-flight loss of control.”
In 2018, CASA issued an airworthiness bulletin (AWB 25-032) to single-engine Cessna operators and maintainers highlighting the importance of meticulous inspection and timely maintenance to ensure pilot seats, adjustment mechanisms and seat track locking mechanisms are secured correctly to prevent inadvertent seat movement, particularly during critical phases of flight.
“While the recent incident did not involve a Cessna, the AWB is a pertinent message for operators and maintainers of all aircraft types,” Mr Macleod said.
“The proper fitment and good condition of aircraft seats and their adjustment mechanisms is crucial for safe operation.”
Read the ATSB’s investigation into the 2014 accident here.