A fractured axle was found on a wagon which derailed during a rail accident south of Rockhampton, Queensland, in January;
The ATSB’s preliminary report outlines information gathered during the investigation’s early evidence collection phase;
The investigation will examine maintenance records, procedures and practices.
The Australian Transport Safety Bureau is continuing to undertake a detailed material analysis of rolling stock components after a fractured axle was at identified at the site of a freight train derailment south of Rockhampton, Queensland.
An ATSB preliminary report from the on-going investigation details that, on the evening of 29 January 2023, a Pacific National freight train was travelling west near Marmor at about 100 km/h, when the third bogie on its sixth wagon derailed.
The emergency brake was applied and the train stopped 1.1 km from the initial point of derailment. Several of its multi-pack wagons had derailed, significantly damaging points, crossings, level crossing equipment, and overhead wiring stanchions.
At about the same time, the crew of an Aurizon coal train, travelling on the parallel track in the opposite direction, noticed a cloud of dust emanating from the freight train, and began to apply their own emergency brake.
“The coal train collided with a container from the freight train which was fouling the opposite track,” ATSB Director Transport Safety Kerri Hughes said.
“Fortunately, the coal train stopped before reaching the main portion of the freight train wreckage, at the Bills Road level crossing.”
The coal train sustained impact damage to the driver’s side of the cabin. No injuries were reported in the accident.
Investigators from the ATSB attended the accident site, and found an axle from the sixth wagon had fractured.
“This correlated with marks found on the rail head at the point of derailment,” Ms Hughes noted.
Along with site inspections, investigators have so far interviewed the crew of both trains, received evidential material including recorded data, and conducted a detailed examination of rolling stock components.
“This preliminary report summarises information from the early evidence-gathering phase of its investigation into the derailment, and as such contains no analysis or findings, which will be presented in a final report,” Ms Hughes explained.
“As the investigation progresses, the ATSB will continue a detailed material analysis of specific rolling stock components, as well as examining maintenance records, procedures, and practices.”
Investigators will also review similar occurrences, and any other relevant evidential material available, before preparing a final report for release at the conclusion of the investigation.
“However, should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely action can be taken,” Ms Hughes concluded.
An S-2R aerial application aircraft experienced a ground loop after part of its left shock assembly suffered an overstress failure;
The ATSB determined it was highly likely the component was not replaced or modified to comply with a service bulletin issued by the manufacturer in 1994;
The ATSB strongly encourages compliance with service bulletins related to aircraft safety.
A ground strike accident involving an Ayres S2R aerial application aircraft at Trangie, NSW, on 31 August 2022 highlights the importance of aircraft operators ensuring all relevant service bulletins have been addressed.
The aircraft was about 100 m into its take-off roll, when its left main landing gear shock assembly failed, with the left wing hitting the ground, resulting in a ground loop. The pilot was uninjured.
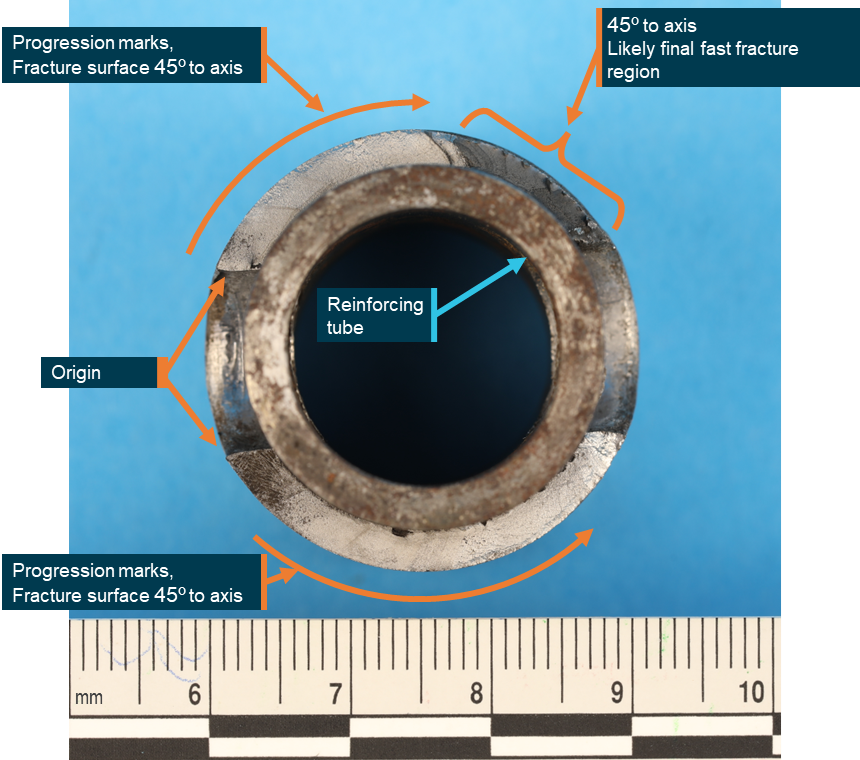
An Australian Transport Safety Bureau short investigation subsequently identified the lower tube of the left shock strut assembly had failed at a fatigue crack.
Examining the damaged strut assembly at its technical facilities in Canberra, the ATSB determined the fatigue crack had initiated from the hole where the lower tube attached to the slider plate, and had propagated around the circumference of the tube.
“It is very likely this lower tube was a part that Thrush Aircraft – then Ayres Corporation – had instructed owners and operators to replace or modify in 1994, in accordance with a service bulletin,” ATSB Director Transport Safety Stuart Macleod said.
Thrush Aircraft informed the ATSB that writing on the lower tube which fractured was consistent with a part from pre-1994, and that the failure in this accident was consistent with the failures which prompted the service bulletin.
“Manufacturers issue service bulletins to inform owners and operators about critical and useful information on aircraft safety, maintenance, or product improvement,” Mr Macleod said.
The reason the part was not replaced or modified on the accident aircraft, in accordance with the service bulletin, was not identified.
Mr Macleod said the ATSB strongly encourages compliance with service bulletins that effect aircraft safety.
“Additionally, on acquisition of an aircraft, it is important to review maintenance documentation to determine whether all the appropriate manufacturer issued instructions have been addressed,” he concluded.
On 4 April 2023, the pilot of a Robinson R44 Raven II helicopter, registered VH-WLH, was conducting aerial mustering operations on at Bingegang, Queensland (about 60 km south-east of Middlemount). The pilot was the only person on board.
While the pilot was reportedly flying to look for straggling cattle the helicopter struck an aerial powerline and collided with terrain. The pilot was fatally injured and the helicopter was destroyed by post-impact fuel-fed fire.
What the ATSB found
The pilot had an operational reason to be in the area at low level at the time of the accident. There was no evidence of pre-existing helicopter defects and the terrain was generally suitable for a landing had an in-flight emergency arisen.
The pilot was reportedly familiar with the property and knew that there was a powerline running across it, although it was not possible to conclusively determine the level of awareness they had of the wire’s presence and location during the flight. The ATSB concluded that the pilot likely lost awareness of, and did not see, the unmarked aerial powerline during low-level aerial mustering.
The powerline was not marked and nor was there a requirement to do so. The helicopter model was not able to be fitted with wirestrike protection equipment.
Safety message
This accident provides another reminder of the dangers posed by aerial powerlines during low-level mustering. There are limits to the extent to which operators can mitigate the risk of wirestrike during low-level operations near powerlines. Helicopter wirestrike protection (WSPS) can provide a last line of defence in the event of a wirestrike. Some aircraft selected for aerial agriculture operations can be configured to include WSPS. However, this technology is not currently available on smaller helicopters such as the Robinson R44.
The ATSB has released, in association with the Aerial Application Association of Australia (AAAA), an educational booklet, Wirestrikes involving known wires: A manageable aerial agriculture hazard (AR-2011-028). This booklet contains numerous wirestrike accidents and lessons learned from them.
Electrical power and telecommunications companies in Australia can mark powerlines that are identified as a hazard for low-level flying operations and some have a safety scheme to reduce the costs to property owners.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 4 April 2023, the pilot of a Robinson R44 Raven II helicopter, registered VH-WLH, was conducting cattle mustering operations on a private property at Bingegang, Queensland (about 60 km south-east of Middlemount), owned and operated by the pilot’s family business. The pilot was the only person on board and was reported to be familiar with the property. The weather was clear.
Mustering commenced early in the morning and according to witnesses the pilot took a 60–90 minute break before recommencing at about 1000. At about 1110, after mustering a large mob of cattle into a holding paddock, the pilot flew back to one corner of the lot to look for stragglers. The pilot then radioed for workers on the ground to help with further mustering.
As the workers approached, they saw a plume of smoke and were unable to contact the pilot via radio. They then saw that the helicopter had struck a single-strand aerial powerline and collided with terrain. The wreckage was on fire. The pilot was unresponsive and the workers were unable to remove the pilot due to the increasing intensity of the fire.
The pilot had been fatally injured and the helicopter was destroyed by post-impact fire.
Context
Personnel information
The pilot held a private pilot licence with a class rating for single-engine helicopters and a helicopter low-level operational rating. The pilot held a class 2 civil aviation medical certificate which included the requirement for distance vision correction lenses to be worn and reading correction lenses to be available. It was reported that the pilot always wore glasses, was wearing them on the day of the accident, and that they knew of the presence of the powerline on the property.
Aircraft information
The helicopter was a Robinson R44 Raven II, serial number 14253, manufactured in the United States in 2018 and registered in Australia on 30 October 2018. It was issued with a certificate of airworthiness in the normal category on 16 November 2018.
The R44 is a single-engine, light utility and training helicopter with a semi-rigid, two-bladed main rotor, a two-bladed tail rotor and skid type landing gear. It has an enclosed cabin with two rows of side-by-side seating for a pilot and three passengers. The pilot sat on the right side, and extensive windows at the front of the helicopter afforded generally excellent visibility ahead. The accident helicopter was being flown with the doors fitted.
A wirestrike protection system (WSPS) was not fitted to the accident helicopter. In general, smaller helicopters such as Robinson R22 and R44 series had no structural hard points to fit a wirestrike protection system, were too light, and in many instances travel too slowly for a WSPS to be effective.[1]
Site information
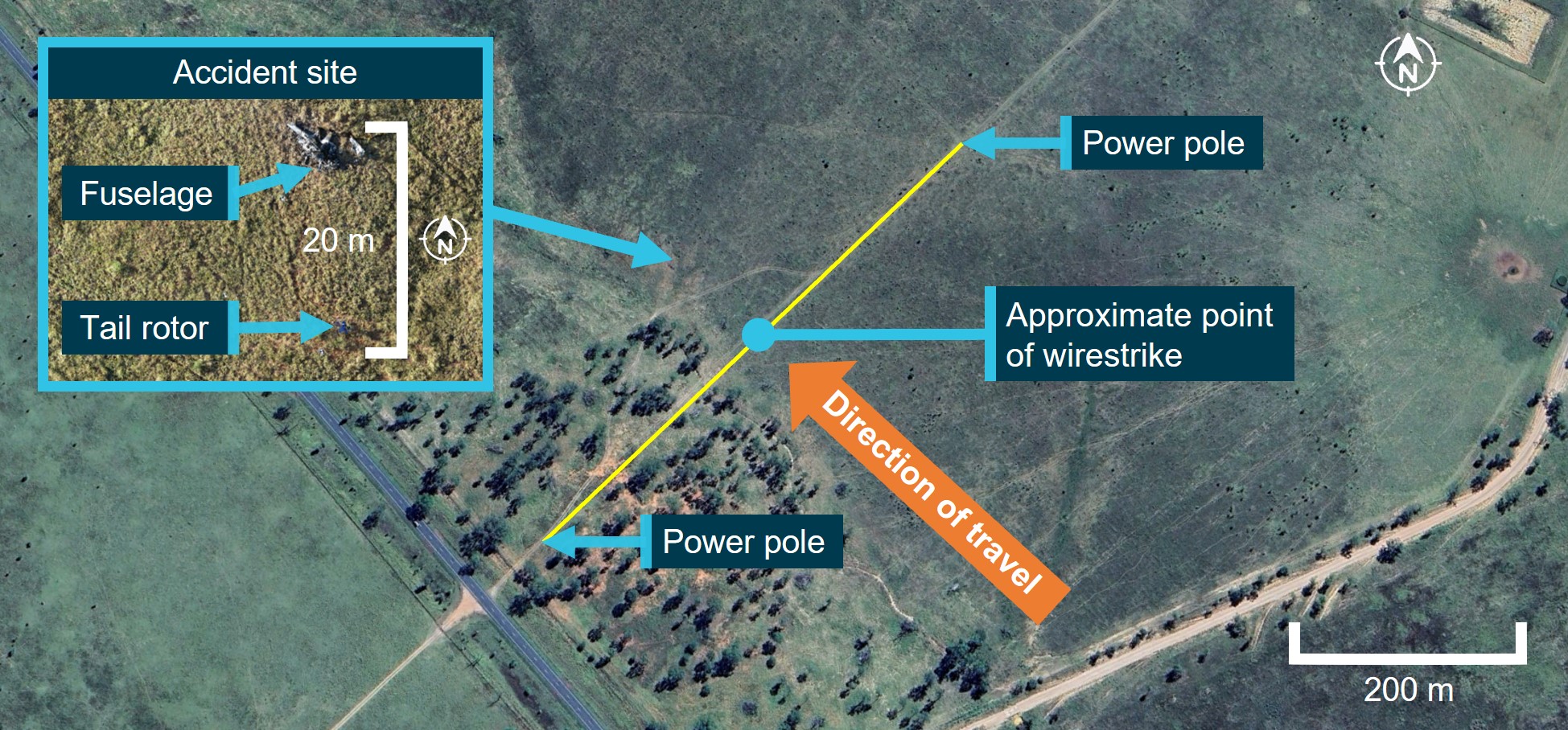
Figure 1 shows an overview of the accident site. The powerline, a single-wire earth return (SWER) wire that ran across the property, was not marked and there was no requirement within the applicable aviation regulations, Australian Standards or elsewhere to do so. The wire was estimated to be at a height of 5.6 m at the point of impact.
The terrain was clear to the right of the helicopter’s flightpath, and there were trees taller than the wire height that would have obscured the wire and pole on the left side.
Figure 1: Accident site
Source: Google, Queensland Police. Annotated by the ATSB
The helicopter impacted terrain left side down and yawing to the right about 90 m beyond the point of contact with the wire and facing back towards the wire. There was insufficient evidence available to determine the angle and speed of impact with the ground.
Visibility of powerline
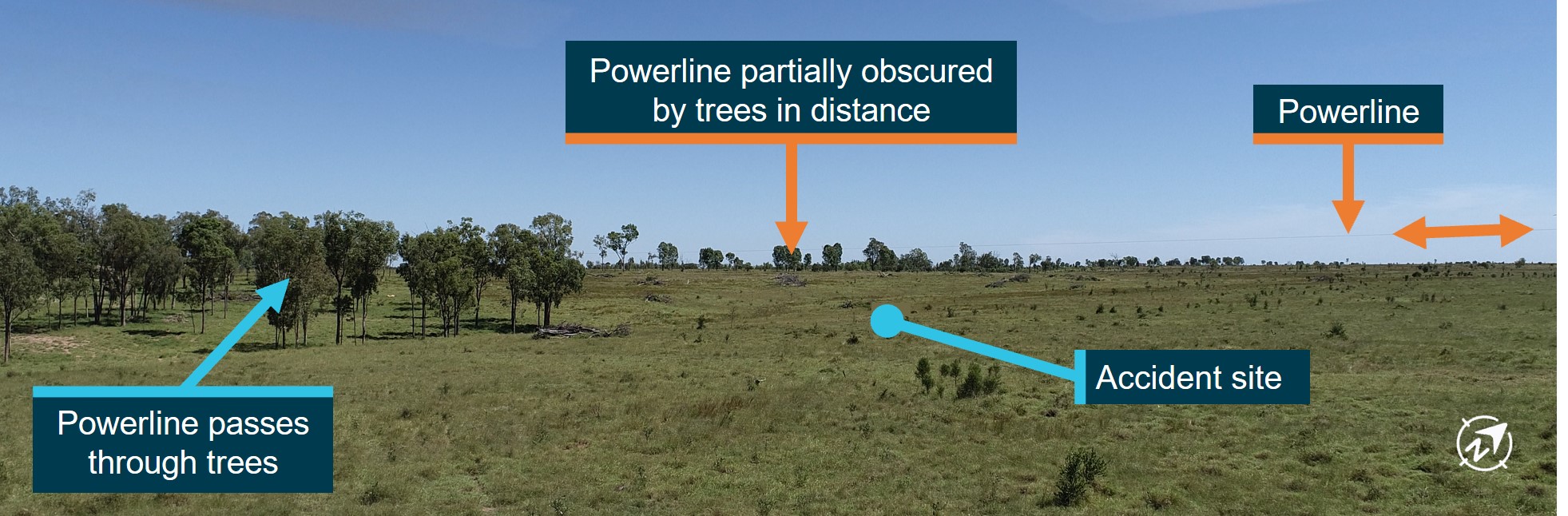
Queensland Police officers later returned to the accident site to conduct a simulation using a remotely piloted aircraft system (RPAS) of the helicopter’s approximate flight path and height prior to striking the powerline assuming that it had not turned. The simulation was conducted in conditions similar to those on the day of the accident. Images from the RPAS simulating what the pilot would have seen when approaching the wire showed the wire was difficult to distinguish from the background and the left pole was obscured by trees (Figure 2).
Figure 2: RPAS simulation of flight path
Source: Queensland Police, annotated by the ATSB
Wreckage information
The ATSB examined the aircraft wreckage after it was moved to a secure facility by Queensland Police.
The examination of the wreckage indicated that the impact with terrain was likely not survivable. The helicopter’s cockpit, systems and engine were severely damaged by the impact and post-impact fire. Within the limitations of the available evidence, there were no indications of pre-flight defects, in-flight fire or birdstrike.
The examination found that the wire was struck between the helicopter’s nose and the upper surface of the skids. Additionally, the wire marks on the upper surface of both skids were similar, and in conjuction with the position of the wreckage indicated the helicopter was travelling about perpendicular to the wire.
During the accident sequence, the rotor struck and separated the tail boom. The nature of this damage, and other evidence, indicated that the rotor had high energy at the time.
Marks on the left oil cooler indicated that the engine and ring gear were rotating at the time of impact. Other impact marks indicated that the engine stopped rotating during the impact sequence.
The helicopter’s warning light filaments, including a carbon monoxide warning, were consistent with them not being illuminated at impact.
The helicopter was fitted with a bladder fuel tank, which was breached during the accident sequence. Due to the intense fire, it was not possible to assess how the tank was breached.
Maintenance information
The helicopter’s most recent periodic (100-hourly) inspection was carried out on 6 September 2022, at 660.6 hours in service, after which a maintenance release was issued. A review of all previous maintenance releases identified no discrepancies or significant defects. The most recent maintenance (a tail rotor blade inspection) was carried out at 674.1 hours, on 6 January 2023.
At each periodic maintenance inspection, engine cylinder compression checks were carried out. The tests resulted in satisfactory compression. However, during the most recent test (at 660.6 hours in service), the variation in compression levels was at the lower limit (10–15 psi) of where a re-test should be made within 10 engine operating hours (no later than 670.6 hours in service). There was no record that this was carried out, however, the time in service at the time of the accident could not be determined as the maintenance release was not found and was likely destroyed in the post-impact fire.
Medical and pathological information
A toxicological examination showed the pilot did not have elevated levels of carbon monoxide at the time of the accident and tests for other substances likely to have an effect on performance were negative.
Witnesses reported that the pilot was wearing the helicopter’s three-point harness. The pilot was not wearing a helmet.
A final post-mortem examination report was not available at the time of publication, however, the autopsy certificate for the pilot recorded the cause of death as chest injuries resulting from the accident.
Safety analysis
Within the limitations of the available evidence, there were no indications of pre-impact defects, in-flight fire or birdstrike. Damage to the wire and helicopter were consistent with a wirestrike at a height of about 5.6 m.
The pilot had an operational reason to be in the area at low level at the time of the accident. The pilot was reportedly familiar with the property, which was also owned and operated by the pilot’s family business, and knew that there was a powerline running across it, but it was not possible to conclusively determine the level of awareness they had of the wire’s presence and location during the flight. However, the wire was unmarked and would have been very difficult to see from the air as it was partially obscured by large trees to the left of the helicopter’s flight path and in the distance, and combined with the undulating terrain, deprived the pilot of critical visual cues. Further, the task of visually scanning for cattle that had been separated from the larger mob was a potential distraction. It is therefore likely that any awareness the pilot had of the wire was lost during the flight, and the pilot did not see it at all or in time to avoid the wirestrike.
Helicopter wirestrike protection (WSPS) can provide a last line of defence in the event of a wirestrike. Some aircraft selected for aerial agriculture operations can be configured to include WSPS. However, this technology is not currently available on smaller helicopters such as the R44.
Wreckage examination indicated that the fatal injuries sustained by the pilot probably would not have been prevented through the use of a helmet, and the pilot was wearing a three-point harness which reduces the likelihood of upper body injuries. However, in low-level operations where the risk of an accident is higher, options to improve accident survivability include the wearing of a helmet and the installation and use of a five-point harness.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the wirestrike and collision with terrain involving Robinson R44 II, VH-WLH on 4 April 2023.
Contributing factors
The pilot likely lost awareness of and did not see an unmarked aerial powerline during low-level aerial mustering.
Other factors that increased risk
The powerline was partially obscured by trees and terrain, depriving the pilot of critical visual cues as to its presence.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
Civil Aviation Safety Authority
Queensland Police Service
maintenance organisations for VH-WLH.
References
Australian Transport Safety Bureau 2006, Aviation Research and Analysis Report B2005/0055 Wire-strike Accidents in General Aviation: Data Analysis 1994 to 2004.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
the operator
Civil Aviation Safety Authority.
A submission was received from the operator. The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] ATSB Aviation Research and Analysis Report B2005/0055 Wire-strike Accidents in General Aviation: Data Analysis 1994 to 2004 (Re-released September 2006).
The following statement can be attributed to ATSB Chief Commissioner Angus Mitchell:
The Australian Transport Safety Bureau (ATSB) has commenced a transport safety investigation into the collision with terrain of a four-seat Robinson R44 helicopter at a station at Bingegang, 140 km west of Rockhampton, Queensland, on Tuesday.
ATSB investigators have now commenced early evidence collection and assessment activities, including gathering information from first responders and other stakeholders, to inform the scope of investigation activities.
Investigators willalso seek to obtain and review any recorded data, weather information, witness reports, andaircraft maintenance records, and will review pilotqualifications and experience.
Investigation identified fatigue cracking in R22 helicopter fanwheel, which probably led fanwheel to break-up during 60 ft hover;
Break-up created imbalance which likely led forward drive belt to migrate from drive sheaves, causing loss of rotor drive and collision with terrain;
The ATSB reminds pilots and maintainers to pay particular attention to the installation, maintenance, and ongoing inspection of critical components of R22 and R44 drive systems, and to report all defects to CASA.
An Australian Transport Safety Bureau investigation found evidence of fatigue cracking in the fanwheel assembly of a Robinson R22 helicopter, which collided with terrain after a sudden loss of rotor drive at a low altitude.
On 16 August 2020, the pilot and sole occupant of an R22 was conducting mustering at a property near McArthur River Mine in the Northern Territory.
While hovering 60 ft above the ground, the helicopter experienced a sudden loss of rotor drive, resulting in a rapid loss of height and collision with terrain. The pilot sustained serious injuries, and the helicopter was substantially damaged.
An ATSB investigation found evidence of fatigue cracking in the helicopter’s cooling fanwheel outer support ring, and in the welded region of two vanes of the fanwheel assembly.
“These fatigue cracks probably weakened the fanwheel structure sufficiently for it to break-up in flight,” ATSB Director Transport Safety Stuart Macleod said.
This caused an imbalance which likely led the forward drive belt to migrate off the drive sheaves, resulting in a loss of rotor drive.
The ATSB’s report notes cracking of Robinson fanwheels in the vane weldment has been identified to occur in a limited number of the R22 fleet, however this was the first instance where the cracking had progressed to the point of in-flight failure.
“The circumstances of this accident are an important reminder for pilots and maintainers to pay particular attention to the installation, maintenance, and ongoing inspection of critical components of the drive systems of both Robinson R22 and larger R44 helicopters,” Mr Macleod said.
The ATSB’s final report also notes that many Robinson operators are aware that cracking can occur at the welded regions of the cooling fanwheel.
“This awareness, however, is not reflected in CASA’s Defect Reporting Service data, suggesting such instances are under-reported,” Mr Macleod said.
“The non-reporting of defects prevents the sharing of knowledge to the wider aviation community and the identification of emerging issues.
“Defect reporting benefits the aviation industry. It allows CASA to create a database, which is used to identify trends in design and maintenance reliability of aircraft systems and components and is a publicly accessible service.”
Additionally, while not a contributing factor in the accident, the ATSB found the details associated with the helicopter’s emergency locator transmitter (ELT) had not been updated since the helicopter was recently purchased by the operator.
This meant that when the transmitter automatically activated during the accident sequence, the Joint Rescue Coordination Centre was delayed in confirming an accident had taken place.
“Fortunately, this accident was reacted to quickly by others involved in the mustering,” Mr Macleod said.
“But where an aircraft is operating alone, any delay to the search and rescue response could be critical to occupant survival.”
Aircraft operators should ensure details associated with emergency locator transmitters are current. (All 406 MHz ELTs are required to be registered with the Australian Maritime Safety Authority.)
A transport safety investigation has been launched into a collision between a truck and a passenger train in South Geelong, Victoria, on the morning of 3 April.
The investigation will be undertaken by the office of the Chief Investigator, Transport Safety, which conducts rail safety investigations in Victoria on behalf of the ATSB under the Commonwealth Transport Safety Investigation Act 2003.
Investigators have deployed to the site to examine the railway infrastructure, truck, and rollingstock in-situ, documenting evidence and removing any relevant components for further examination.
Likely further investigation activities will include interviewing the train driver, operations staff and any witnesses, reviewing operator procedures, analysing any recorded information, and examining relevant components.
The scope of the investigation and its timeframe will be determined as the Chief Investigator builds its understanding of the nature of the event.
Should any critical safety issues be identified at any stage during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.
The ATSB has commenced a transport safety investigation into the collision with terrain of a light aircraft near Bloomsbury, Queensland.
A search and rescue operation was launched on the evening of 2 April after a Piper Cherokee did not arrive at Lakeside Airpark, after departing a property south of Charters Towers. A wreckage site was located on 3 April, approximately 30 km south-west of Proserpine.
The ATSB is deploying a team of transport safety investigators from its Canberra, Melbourne and Brisbane offices, with experience in aircraft operations, maintenance and engineering, and human factors, to the accident site to begin the evidence collection phase of the investigation.
ATSB investigators will survey the accident site and collect any relevant components for further examination and analysis. They will also obtain and review any recorded data, weather information, witness reports, and aircraft operator procedures and maintenance records.
The ATSB anticipates publishing a preliminary report, which will detail factual information established during the investigation’s initial evidence collection phase, in approximately 6-8 weeks.
The ATSB will publish a final report, detailing contributing factors and any identified safety issues, at the conclusion of the investigation.
However, should any critical safety issues be identified at any stage during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate safety action can be taken.
On the morning of 25 March 2023, a Link Airways Saab 340B aircraft departed Canberra Airport for the first flight of the day. As the aircraft climbed towards the cruising altitude, the flight crew noticed a higher than normal cabin altitude of 6,500 ft. In response the crew descended the aircraft and remained below 10,000 ft for the remainder of the flight to Sydney Airport.
What the ATSB found
The ATSB established that a broken section of door seal seat was found after the last flight on 24 March 2023. However, due to an incorrect assessment that the broken section was simply a piece of cosmetic trim, the off-going flight crew inappropriately applied the company’s non-safety of flight defect deferral process in phone consultation with the continuing airworthiness maintenance organisation representative and a licenced aircraft maintenance engineer.
On the following morning 25 March 2023, the on-coming flight crew noted an additional section of broken door seal seat, which was misidentified as the previously deferred defect, and the aircraft was assessed as serviceable for flight.
The combined effect of the 2 sections of broken door seal seat resulted in the aircraft’s pressurisation system being unable to maintain normal cabin altitude in flight.
What has been done as a result
Following the occurrence, Link Airways provided retraining and guidance to the involved parties on the importance of accurate identification of cosmetic trim, including terminology and level of detail required when raising defects. The Link Airways internal investigation report was distributed to flight operations and maintenance personnel as a reminder to be aware of the risk of communication errors.
Safety message
Communication between aircrew and maintenance engineers is critical to the continuing airworthiness of aircraft. Despite this, issues often arise due to differences in technical knowledge or language, time pressures, and remote communications such as phone or written messages.
Aircrew and maintenance engineers should remain vigilant of the potential for misunderstanding and use confirming techniques such as follow up questioning, demonstration, or the use of photos or video to ensure accurate and effective communication.
Aircrew and maintenance engineers are further reminded to include as much detail as practical when recording defects or rectifications in aircraft technical logs to minimise ambiguity and ensure clarity of communication.
The investigation
Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities.
The occurrence
On 25 March 2023, a Link Airways Saab 340B turbo-prop aircraft, registered VH-VEZ, was being operated for commercial passenger transport between Canberra, Australian Capital Territory and Sydney, New South Wales. On board were the captain as pilot flying,[1] first officer as pilot monitoring, a cabin manager and 32 passengers.
At about 0625 local time on the climb out of Canberra, the flight crew noticed a higher than normal cabin altitude.[2] In response, they levelled the aircraft at an altitude of about 12,000 ft. They noted that the cabin altitude held at 6,500 ft. Pressurisation system fault, and cabin pressure warnings were not indicating, and that the pressurisation system was correctly configured. In addition, the cabin manager reported a loud whistling noise from the forward left door.
The crew informed air traffic control of the pressurisation issue and requested clearance for a cruise altitude of 10,000 ft. Clearance was granted, the aircraft was descended, and cabin altitude was maintained at 6,500 ft. To minimise passenger discomfort caused by the loud whistling, the flight crew elected to reduce the airspeed to a maximum of 200 kts for the remainder of the flight.
During arrival planning, the crew realised that the execution of a normal 1,500 ft/minute descent would quickly cause the cabin altitude to match the aircraft altitude. From that point onward, the cabin altitude would decrease at 1,500 ft/minute potentially causing discomfort to passengers. To minimise this potential, the crew requested, and received, clearance to conduct an early descent into Sydney at a rate of 500 ft/minute, landing at 0656.
Link Airways did not have maintenance facilities in Sydney to assess and repair the aircraft. Therefore, Canberra‑based engineering, having considered the crew’s description of the issue, assessed that the aircraft pressurisation system was operating correctly and that the degradation in cabin altitude was due to an excessive leak from the forward left door. As such, the defect was assessed as not affecting the safety of the flight and engineering approved the return passenger flight to Canberra not above an altitude of 10,000 ft. The door seal seat was subsequently repaired in Canberra and the aircraft was returned to service.
Context
Door seal system
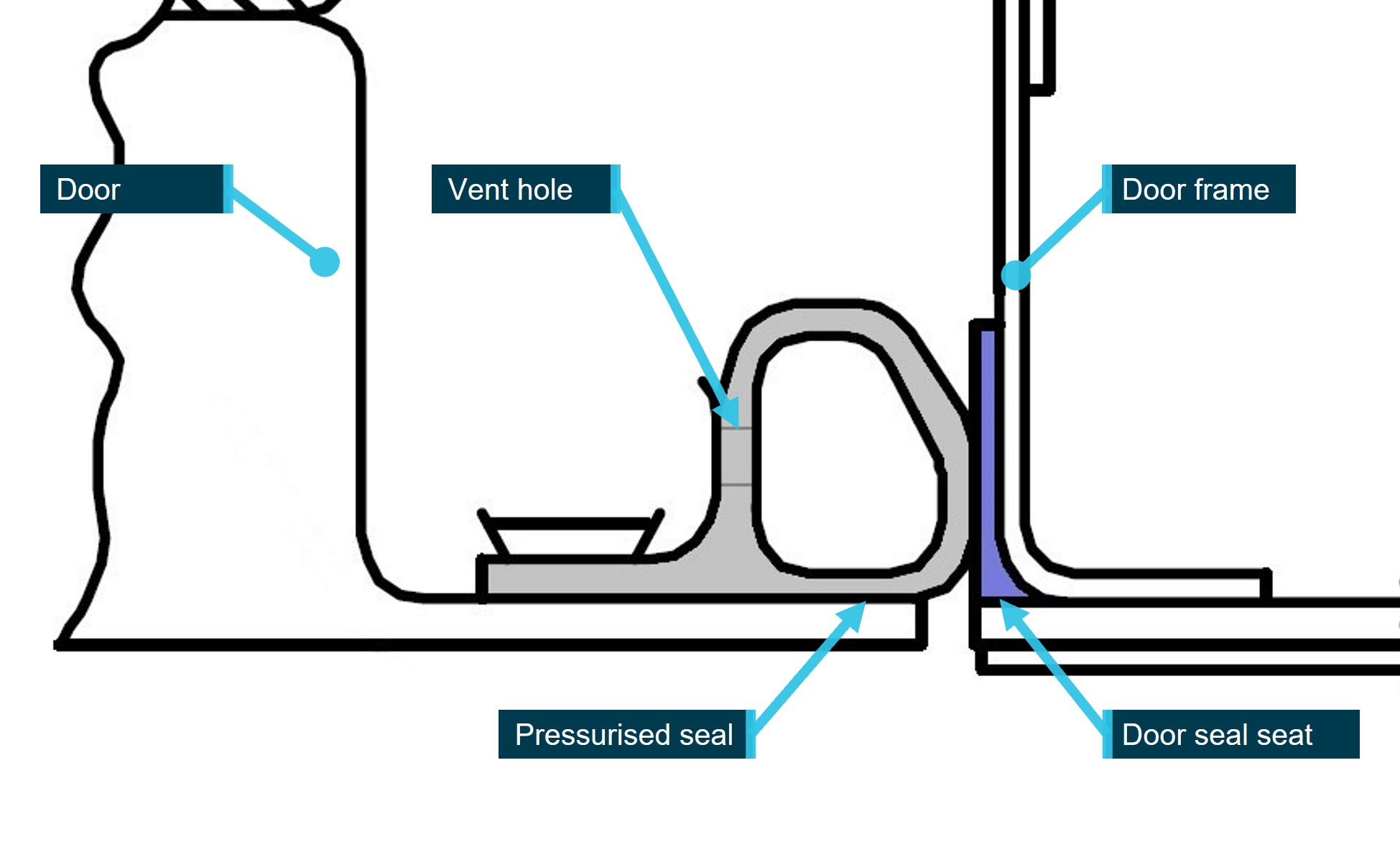
Pressurised aircraft use door seals to help maintain cabin air pressure in flight. The Saab 340B uses a pressurised hose-type seal which is attached to the door. The seal is compressed between the door and door frame when closed and small vent holes in the seal allow cabin air pressure to inflate the seal (Figure 1).
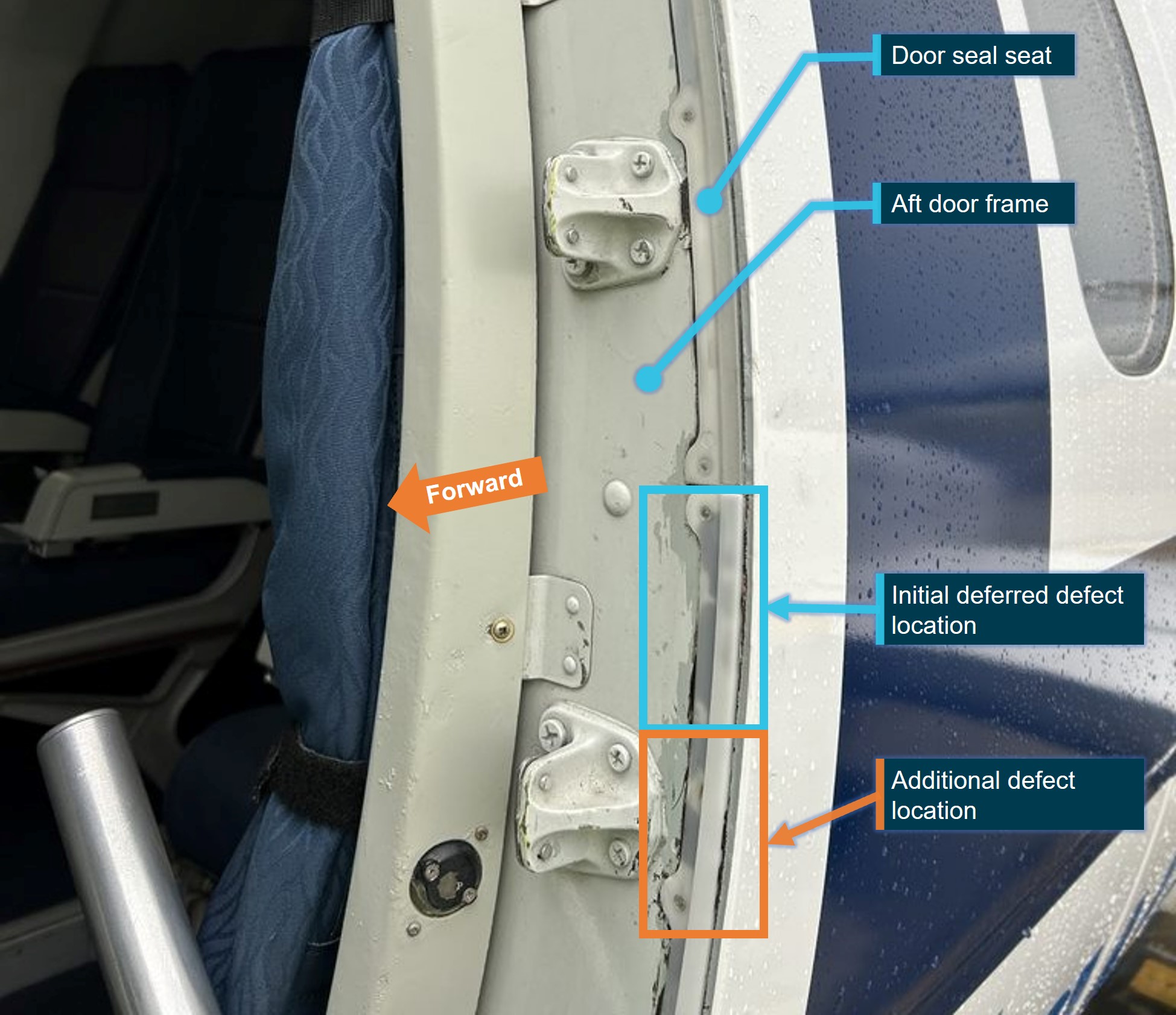
The seal seat is installed in multiple sections around the perimeter of the fuselage door frame (Figure 2). The seat provides a smooth, consistent surface for the seal to act on and assists in the sealing action of the inflatable door seal. Both defects relevant to this occurrence were in the lower, aft section of seal seat.
Figure 1: Door seal system
Source: Saab Aircraft. Modified for clarity and annotated by the ATSB
Non-safety of flight defect deferral procedure
The company’s continuing airworthiness management organisation exposition defines the non‑safety of flight defect (NSOFD) procedure, allowing the deferral of defects in accordance with Part 42 of Civil Aviation Safety Regulations.[3]
Deferral of defects under this procedure require, among other provisions, that the defect does not adversely affect the airworthiness of the aircraft and that the aircraft remains in conformance with its type certificate. Defects other than certain operational or emergency equipment[4] must be assessed by an appropriately licenced aircraft maintenance engineer.
Previous defect deferral
On 24 March 2023, VH-VEZ terminated in Canberra at about 2235. The cabin manager noticed a 15 cm section of door seal seat had broken away from its position on the aft door frame around the forward left door (Figure 2) and brought it to the attention of the terminating captain. There were no engineering staff on-site at the time to rectify the defect.
The terminating captain incorrectly identified the piece as a section of door trim rather than a section of door seal seat and contacted the company’s continuing airworthiness maintenance organisation (CAMO), by phone, to request a defect deferral in accordance with the company’s NSOFD procedure. The CAMO contacted a licenced aircraft maintenance engineer by phone and requested that they assist the terminating captain[5] in applying a NSOFD for a piece of door trim.
After discussion between the terminating captain and maintenance engineer, the terminating first officer, under supervision of the terminating captain, raised a defect in the aircraft maintenance log:
Piece of main door trim snapped off on lower right of door frame.
Rectification of the defect was deferred for a maximum of 120 days, in accordance with the company NSOFD procedure.
Pre-flight inspection
Prior to the first flight of the day on 25 March 2023, when opening the forward left door, the incident flight crew found an additional 10 cm section of broken door seal seat from the same area as the previously identified defect (Figure 2). The captain noted the NSOFD deferral in the aircraft maintenance log, assessed the second broken fragment as the previously identified and deferred defect, and therefore deemed the aircraft as serviceable for flight.
Figure 2: Exemplar image showing the location of the door seal seat defects
Source: Link Airways. Annotated by the ATSB
Safety analysis
Application of non-safety of flight defect deferral
Part 42 of Civil Aviation Safety Regulations[6] allows continued operation of aircraft with minor defects that are not immediately repairable. The operator’s non-safety of flight defect (NSOFD) deferral process was written and approved in accordance with these regulations.
The application of the NSOFD deferral process was applied by the terminating flight crew and the approving licenced aircraft maintenance engineer based on an incorrect assessment that the defect was to a piece of internal trim with no consequence to aircraft serviceability. While a piece of door cosmetic trim would be considered a deferrable defect, the door seal seat defect adversely affects aircraft airworthiness and is therefore not eligible to be deferred under the NSOFD process.
It is important that the licenced aircraft maintenance engineer accurately identifies a defect and its potential effect on aircraft systems prior to applying a maintenance deferral. In this case the use of photo or video to supplement the phone call between the involved pilot and licenced aircraft maintenance engineer would probably have enabled the engineer to identify the detached components as not eligible for repair deferral. This in turn would have resulted in the aircraft being repaired prior to further flight.
Misidentification of additional defect
The ability to defer defects on aircraft is reliant on the ability to accurately communicate the defect between aircrew and maintenance engineering as well as off going and on coming shifts.
The existence of a second defect was not understood by the on-coming flight crew and was not identified until sometime after the incident flight. The specific level of contribution of each section of broken door seal seat could not be determined, however it is likely that the combined effect of both pieces of broken door seal seat was greater than either individual piece, and resulted in degradation of the aircraft’s pressurisation system.
The United States Federal Aviation Administration Human Factors Guide for Aviation Maintenance and Inspection notes:
Effective shift turnover depends on three basic elements:
1. The outgoing worker’s ability to understand and communicate important elements of the job or task being turned over to the incoming worker.
2. The incoming worker’s ability to understand and assimilate the information being provided by the outgoing worker.
3. A formalized process for exchanging information between outgoing and incoming workers and a place for such an exchange to take place.
Where the possibility of ambiguity exists, it is important that aircrew and maintenance staff take the necessary steps to clarify the message being communicated. This will assist defect identification generally and, in this instance, would have prevented continued operation of an unserviceable aircraft.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors.
These findings should not be read as apportioning blame or liability to any particular organisation or individual.
From the evidence available, the following findings are made with respect to the pressurisation fault involving SAAB 340, VH-VEZ near Goulburn, New South Wales on 25 March 2023.
Contributing factors
The misidentification of the cabin door seal seat as door trim resulted in the company deferral process being incorrectly applied.
An additional piece of broken door seal seat was misidentified as the section deferred the previous night. In combination with the previously deferred item, this resulted in degradation of cabin pressurisation during the following flight.
Safety actions
Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence.
Safety action Link Airways
Link Airways provided retraining and guidance to the involved parties on the importance of accurate identification of cosmetic trim, including terminology and level of detail required when raising defects. The Link Airways internal investigation report was distributed to flight operations and maintenance personnel as a reminder to be aware of the risk of communication errors.
Sources and submissions
Sources of information
The sources of information during the investigation included:
Link Airways
the incident and terminating flight captains
the involved LAME
Saab Aircraft
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
Link Airways
the incident and terminating flight crews
the involved LAME
Saab Aircraft
A submission was received from:
Link Airways
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigations
The objective of a safety investigation is to enhance transport safety. This is done through:
identifying safety issues and facilitating safety action to address those issues
providing information about occurrences and their associated safety factors to facilitate learning within the transport industry.
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action.
Terminology
An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue.
Publishing information
Released in accordance with section 25 of the Transport Safety Investigation Act 2003
Ownership of intellectual property rights in this publication
Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia.
Creative Commons licence
With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence.
Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work.
The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau
Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly.
[1] Pilot Flying (PF) and Pilot Monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances; such as planning for descent, approach and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[2] Cabin altitude: altitude corresponding to the air pressure in the cabin.
[3] Part 42 of CASR Continuing airworthiness requirements for aircraft and aeronautical product. Subdivision 42.D.6.1–Dealing with defects.
[4] Operational or emergency equipment that is not required by the certification basis (type certificate) for the aircraft, or under Civil Aviation Safety Regulations for the flight.
[5] Remote assistance permitted in accordance with the company NSOFD procedure.
[6] Part 42 of CASR Continuing airworthiness requirements for aircraft and aeronautical product. Subdivision 42.D.6.1–Dealing with defects.
Occurrence summary
Investigation number
AO-2023-012
Occurrence date
25/03/2023
Location
20 km south-west of Goulburn
State
New South Wales
Report release date
10/08/2023
Report status
Final
Investigation level
Short
Investigation type
Occurrence Investigation
Investigation status
Completed
Mode of transport
Aviation
Aviation occurrence category
Air/pressurisation
Occurrence class
Incident
Highest injury level
None
Aircraft details
Manufacturer
Saab Aircraft Co.
Model
340
Registration
VH-VEZ
Serial number
340B-450
Aircraft operator
VEE H AVIATION PTY LTD
Sector
Turboprop
Operation type
Part 121 Air transport operations - larger aeroplanes