
Collision between a truck and V/Line train 7727, Barwon Terrace level crossing, South Geelong, Victoria on 3 April 2023
Final report
Report release date: 27/06/2025
Investigation summary
What happened
On 3 April 2023, at about 0636, empty V/Line passenger train 7727, running from Geelong to Waurn Ponds, Victoria was approaching Barwon Terrace level crossing in South Geelong, Victoria. At about the same time, a tip truck from a nearby heavy vehicle depot drove onto the level crossing from an unsealed side road. The side road configuration meant that vehicles could enter the level crossing between the level crossing active protection and the track.
The driver of the truck probably became aware of the approaching train and attempted to reverse their vehicle away from the track. However, the train collided with the truck before the truck was clear. The collision rotated the truck about 180° and the driver sustained fatal injuries. The train crew were uninjured.
What the ATSB found
The unsealed road access near the track had developed in recent years. CCTV footage of traffic movements in the weeks before the collision indicated that it was common practice for both light and heavy vehicles to turn right from the unsealed road onto Barwon Terrace between the level crossing protection of booms and flashing lights and the track.
Although the level crossing was inspected regularly by the rail infrastructure manager (V/Line), the inspections did not include a review of the emerging risks associated with the changing road usage and configuration at the level crossing. The safety interface agreement between rail operators and the road manager (the City of Greater Geelong) was also ineffective in triggering action by the agreement partners to monitor the road to rail interface and changing usage.
It was also found that the emerging hazard was identified by personnel from a rail infrastructure project undertaking works in the area. Although there were attempts to reduce the risk associated with the hazard by placing a sign to prohibit users from using the exit route close to the track, this proved ineffective. Signage was ignored by many users of the unsealed access road. There was a missed opportunity for identified hazards associated with the level crossing to be brought to the attention of the appropriate operational area of V/Line.
What has been done as a result
V/Line has issued a maintenance alert with actions for track inspectors to identify roads or access tracks which may be able to bypass crossing controls and raise corrective work orders and incident reports in response. In addition, V/Line advised that the Level Crossing Roadway Inspection Report form has been revised to include an assessment of hazardous access points.
The Victorian Rail Crossing Safety Steering Committee (VRCSSC) has implemented changes to the Australian Level Crossing Assessment Model (ALCAM) survey program in Victoria, that now requires contractors undertaking assessments to identify and report any road network configurations like the incident location. If reported, the rail infrastructure manager would be notified of the safety risk and further assessment and actions sought.
Safety message
Level crossing inspection regimes should include checks on any changes that may introduce new hazards and associated risks.
The occurrence
Prior to the incident
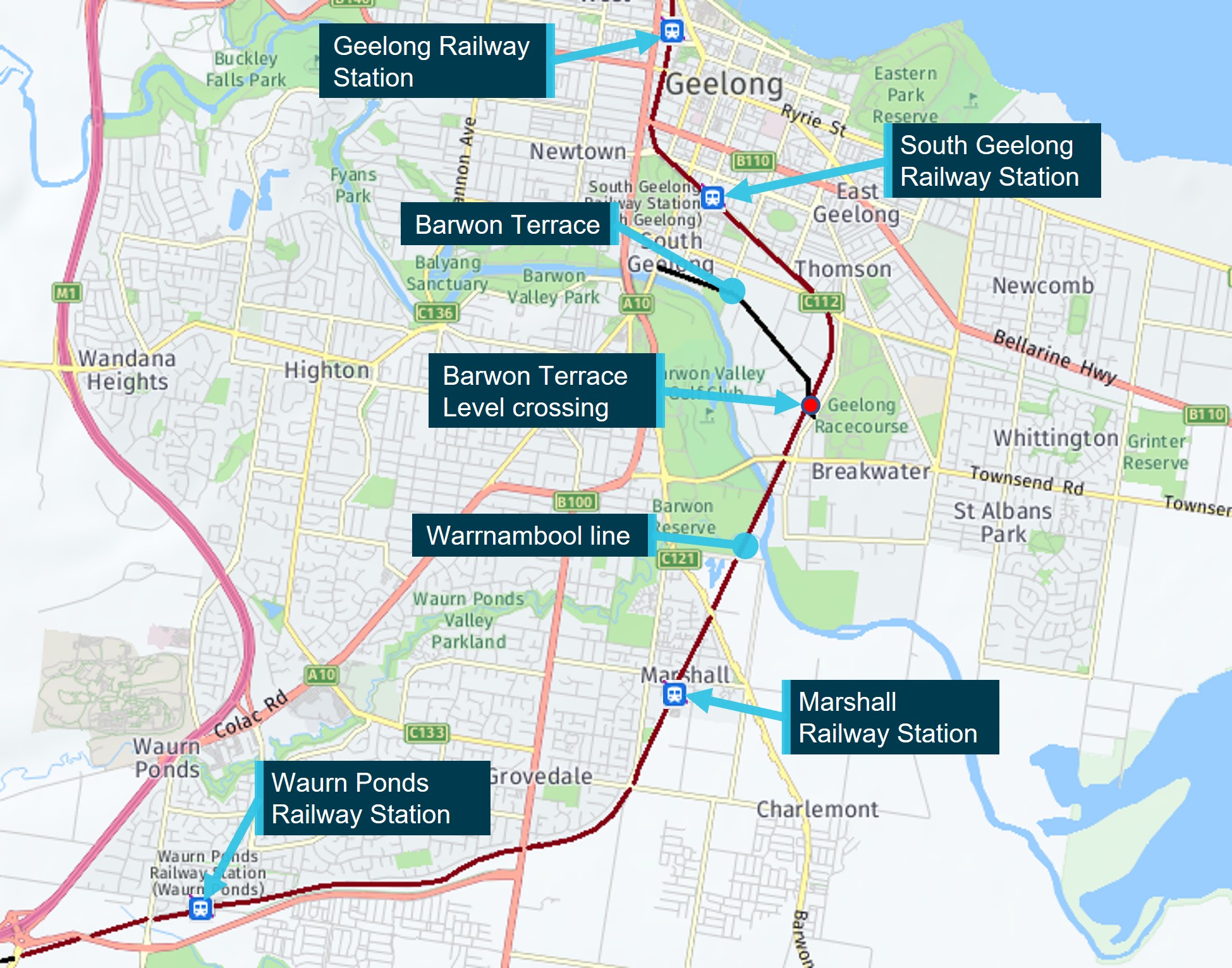
At about 0631 local time on 3 April 2023, V/Line train 7727 departed Geelong Railway Station to travel to Waurn Ponds, Victoria (Figure 1). Train 7727 was an empty, 6-car VLocity train with only the driver and conductor on board. The train was being relocated to Waurn Ponds to form the 0721 passenger service from Waurn Ponds to Melbourne. For its relocation, the train was not scheduled to stop at South Geelong or Marshall stations.
Figure 1: Train route and location of Barwon Terrace level crossing
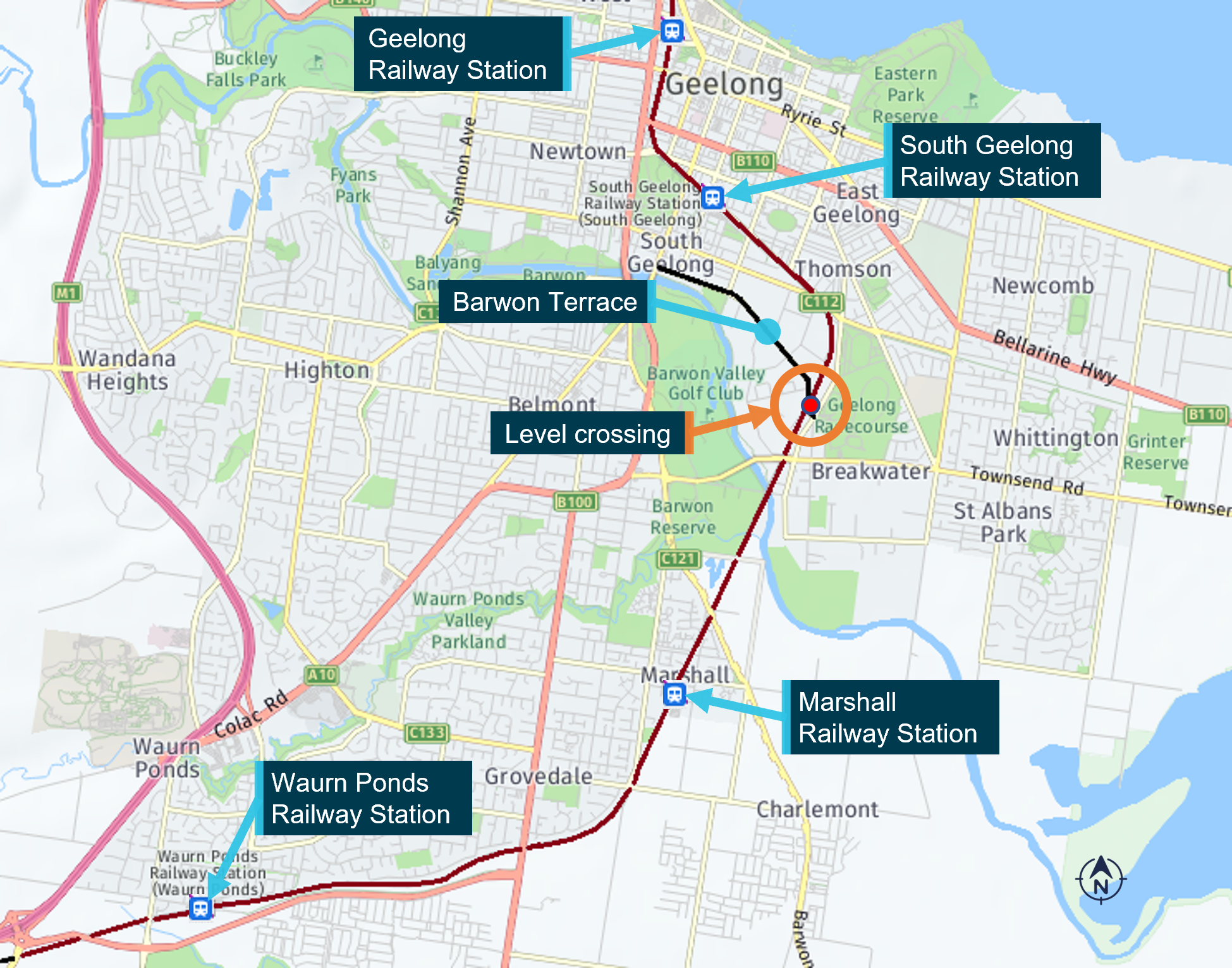
Source: Imagery © Nearmap annotated by Office of the Chief Investigator
Earlier, at about 0600, a truck driver arrived at a heavy vehicle depot adjacent to the rail corridor and began preparing a tip truck for work. The depot was located about 220 m south of the Barwon Terrace level crossing on the western side of the rail line. Access from the depot to Barwon Terrace was via an unsealed road[1] which ran parallel to the rail line and joined Barwon Terrace at the northern end of the road.
The collision
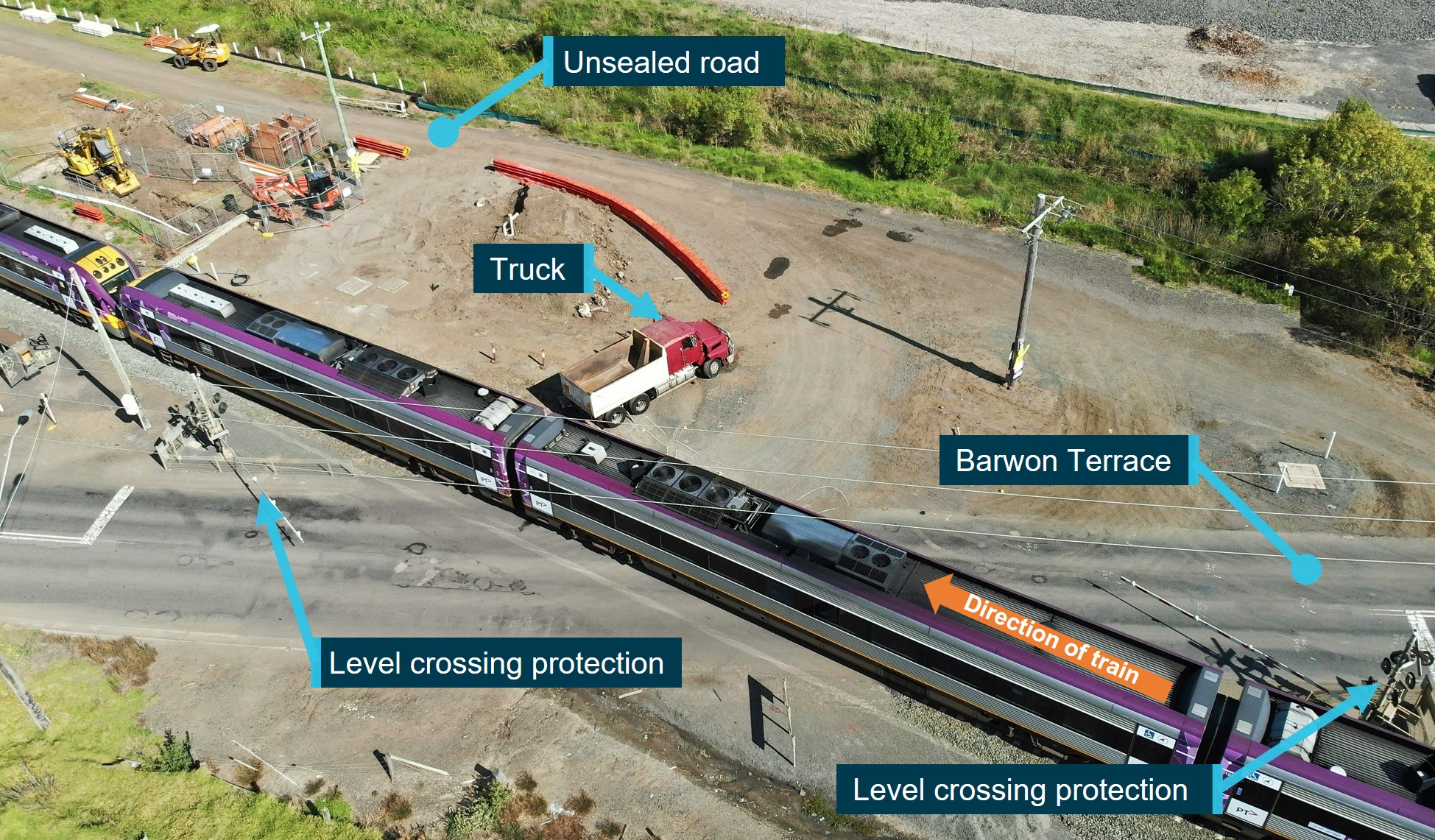
At about 0635, the truck left the depot and travelled north along the unsealed road towards Barwon Terrace. It was dawn (shortly before sunrise), overcast and dry. As the truck approached the northern end of the unsealed road, the truck turned to the right and drove slowly onto the level crossing (Figure 2). This positioned the truck between the protection equipment located on each side of the crossing. The level crossing flashing lights and bells were operating, and booms had descended. At the same time, train 7727 approached the level crossing from the north.
Figure 2: Direction of travel of train and route of truck onto the level crossing
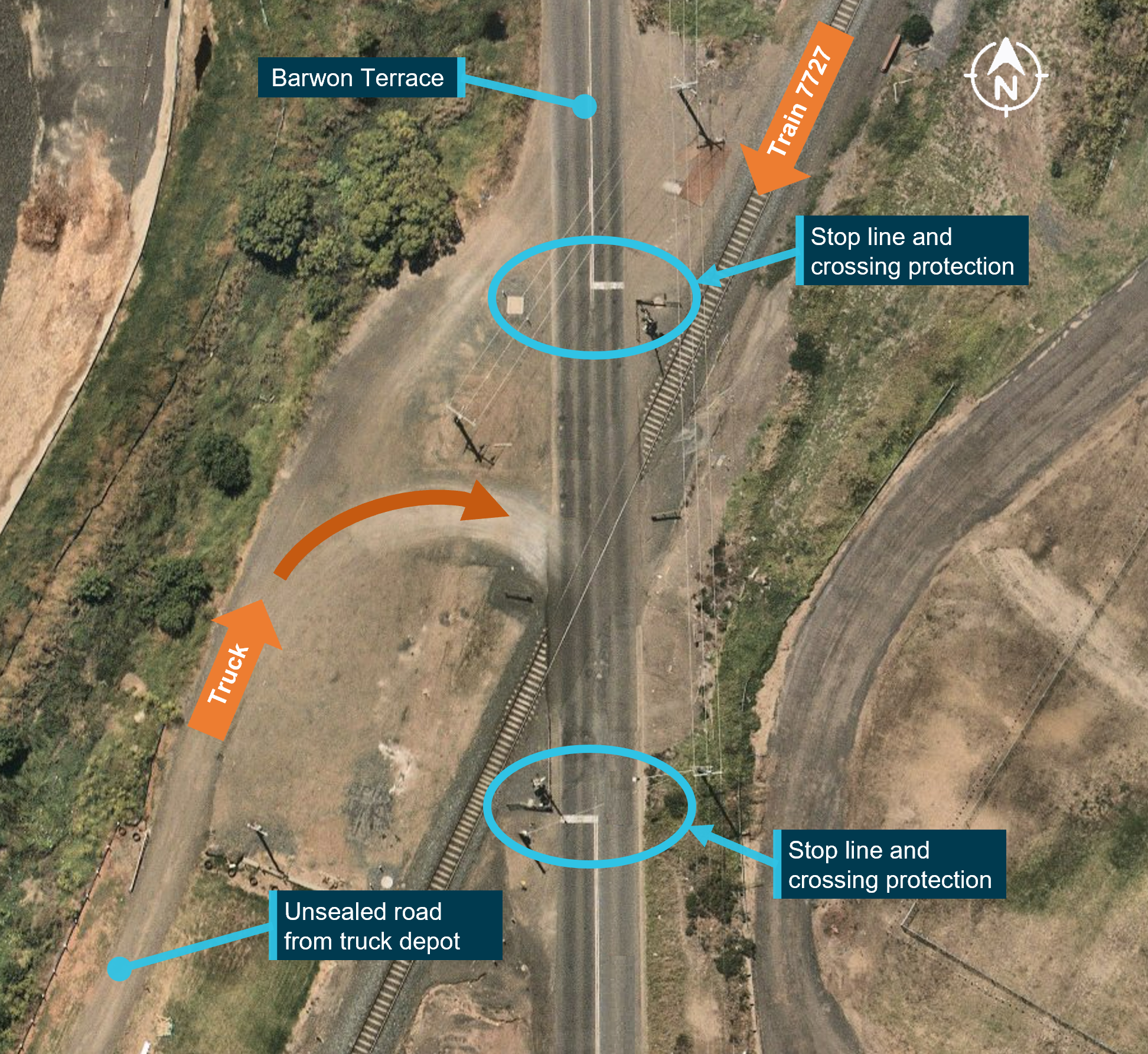
Source: Imagery © Nearmap, annotated by the Office of the Chief Investigator
Train 7727 approached the crossing with its headlights on and travelling at about 74 km/h. On observing the truck, the driver of the train commenced braking[2] and sounded the train’s horn when about 107 m from the collision point. Northbound road traffic had stopped and was queuing behind the boom barrier to the south of the crossing.
On its approach, the train was clearly visible from the level crossing from about 350 m. By either direct observation of the train or hearing the train’s horn and/or observation of the horizontal boom and queued traffic south of the crossing, the truck driver was alerted to the presence of the approaching train. The truck came to a stop. The truck then began to reverse but did not clear the track before the train collided with the left-front side of the truck. The train was travelling at about 60 km/h at the time of the collision. The impact spun the truck around in a clockwise direction and the driver was fatally injured. The train driver and the conductor were not injured.
Context
Barwon Terrace level crossing
Road – rail interface
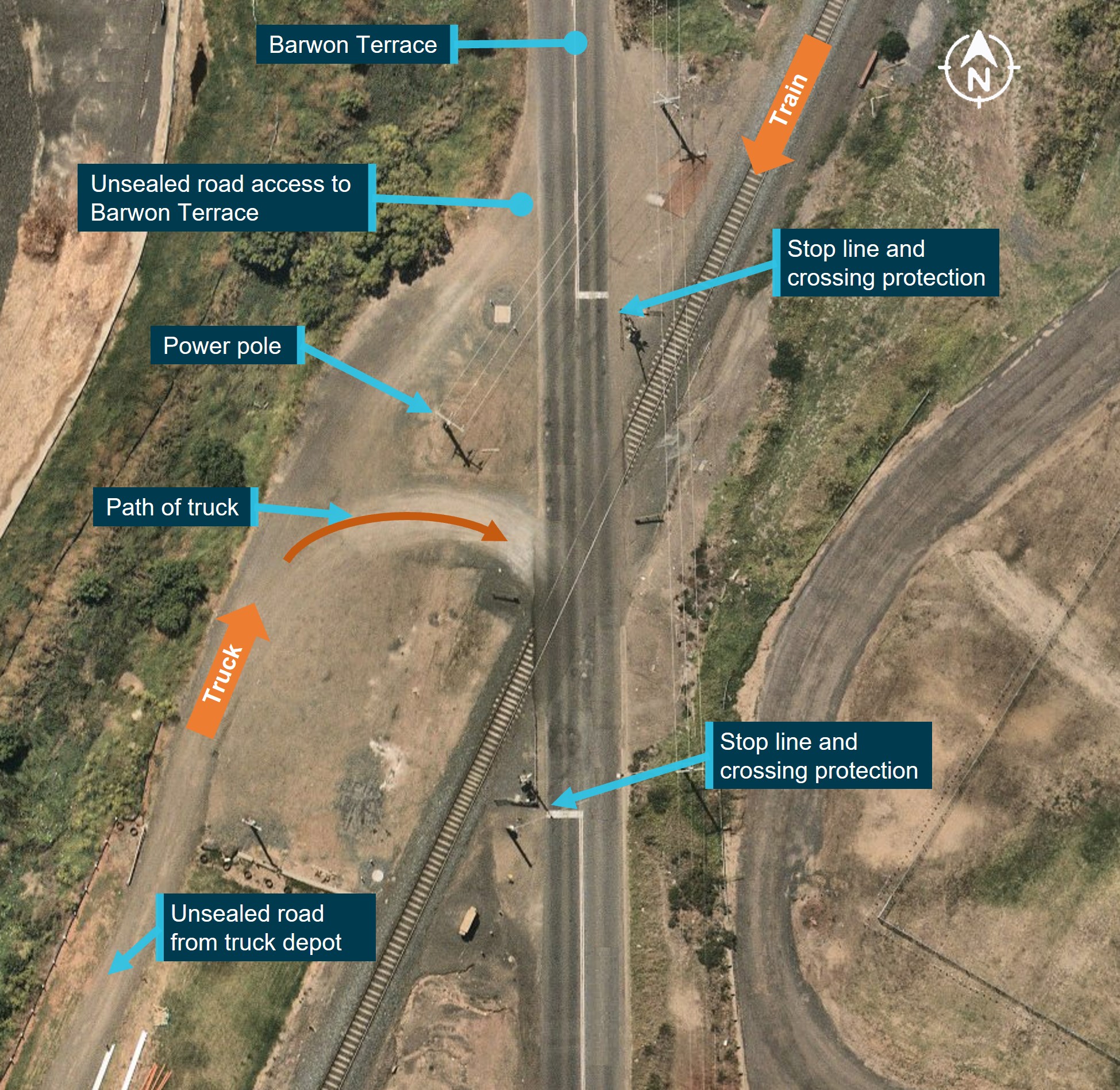
Barwon Terrace was a sealed bi-directional dual lane motor vehicle carriageway managed by the City of Greater Geelong (COGG). At its intersection with the rail line, Barwon Terrace ran in a north / south direction. Travelling south away from Geelong, Barwon Terrace intersected the rail track at the level crossing at an angle of about 25 degrees to the road user’s left (Figure 3). The maximum speed permitted on Barwon Terrace was 60km/h.
Figure 3: Barwon Terrace interface with rail line

Source: Nearmap, annotated by the Office of the Chief Investigator
Barwon Terrace level crossing was an active level crossing located on rail land leased by VicTrack[3] to Head Transport for Victoria[4] and sub-leased to V/Line. V/Line maintained and managed the level crossing.[5]
The rail line, at its intersection with Barwon Terrace, was a single bi-directional broad gauge track with concrete sleepers on a level gradient and formed part of the Warrnambool rail line. The maximum permitted speed for passenger trains travelling along that section of the rail line was 115 km/h.
Level crossing protection
Australian Standard, Manual of uniform traffic control devices, Part 7: Railway crossings (AS 1742.7 – 2016), specified the signage requirements for level crossings with active controls. Protection at the crossing was typical of an active level crossing over a single rail track and consistent with the standard. The protection consisted of boom barriers, flashing lights, warning bells and warning signage on each side of the crossing.
For road traffic approaching from the north, railway crossing warning signage included an RX-5 railway crossing flashing signal assembly,[6] a Keep Tracks Clear Sign (G9-67-1A) and a Railway Crossing with marker assembly sign (RX-9) (Figure 4).[7] There was a pair of standard flashing lights for southbound Barwon Terrace traffic and an additional flashing light directed towards the exit of the unsealed road. This single flashing light was directed to the northern access of the unsealed road and could not be clearly seen from the southern exit nearer the track crossing and used by the truck.
Figure 4: Level crossing protection for southbound traffic

The figure shows the protection equipment at the level crossing on the western side of the crossing. Source: The Office of the Chief Investigator
Inspection and maintenance
V/Line regularly serviced the level crossing and tested the crossing operability.[8] Inspection included testing the backup battery at the crossing. The crossing was serviced about 3 weeks prior to the incident and was found to be functioning as intended.
This inspection process did not include assessing the junction between Barwon Terrace and the access onto the tracks from the unsealed road.
The protection equipment at the crossing was working at the time of the incident. This was confirmed by CCTV, download data taken from the crossing equipment following the incident and eyewitnesses accounts.
ALCAM level crossing assessment
The Australian Level Crossing Assessment Model (ALCAM)[9] was an assessment tool used to identify potential risks at level crossings, to assist in the prioritisation of crossings for upgrades and support the decision-making process when determining the most cost‑effective treatments at a level crossing. The Victorian Rail Crossing Steering Committee (VRCSSC) delivered the level crossing safety strategy in Victoria and funded ALCAM surveys. Membership of this committee included the Australian Rail Track Corporation, V/Line Corporation, Metro Trains Melbourne, VicTrack, Victoria Police and the Victorian Department of Transport and Planning.
The survey of a level crossing produced an ALCAM Risk Score expressed as the expected number of equivalent fatalities at that level crossing per year. The ALCAM Risk Score was described as allowing ‘comparison of level crossings against each other within a given jurisdiction based on the level of risk’ and informed safety improvement programs.[10]
The most recent (prior to the collision) full ALCAM survey at the Barwon Terrace level crossing was conducted in July 2017 and reviewed in 2018. The assessment and review noted that flashing lights, bells and audible warning devices and the relevant level crossing signage were deployed at the crossing. The survey drawing prepared from the survey in 2017 and associated photographs at that time indicated that the used route to and from the unsealed road was on its northern interface, and not the southern access later used nearer to the track (Figure 5).
Figure 5: Junction between the access road and Barwon Terrace in 2017

In 2017, the unsealed road joined Barwon Terrace north of the level crossing. The access pathway used by the truck on the day of the incident had not yet developed. Source: ALCAM 2017 survey assessment
Activity in area
Heavy vehicle depot
The truck involved in the incident operated out of a heavy vehicle depot situated on a parcel of land located along the unsealed road south of Barwon Terrace. The land was owned by a management consulting firm and was leased to an earth moving company which based its operations at the depot. The parcel of land did not border Barwon Terrace directly. The northern end of the property was about 210 m south of the Barwon Terrace level crossing.
Several trucks operated out of the depot and undertook works for the earth moving company and regularly exited the depot using the unsealed road to access Barwon Terrace. On the day of the incident the truck drove north from the heavy vehicle depot along the unsealed road before driving onto the Barwon Terrace level crossing.
At the time of the incident, the firm that owned the parcel of land on which the heavy vehicle depot was located had not submitted the requisite planning permit to operate a contractor’s depot at the site. Between December 2020 and July 2021, the City of Great Geelong (COGG) wrote a series of letters to the firm regarding this alleged breach of the COGG Planning Scheme. The letters advised that a retrospective planning permit application was required and provided the landowner an opportunity to show why COGG should not take enforcement action for the unauthorised use and development of the land. At the time of the collision, a permit had not been issued and the matter was unresolved.
Rail corridor project
Djilang Alliance (the Alliance) was contracted to deliver a rail line duplication project between South Geelong and Waurn Ponds and was working in the area. The Alliance consortium comprised McConnell Dowell, Downer, Arup and WSP.
In the months prior to the collision, the Alliance was conducting works around Barwon Terrace level crossing. The Alliance advised that in the February prior to the collision, they began placing a temporary barrier around the Alliance worksite at the northern end of the unsealed road. The barrier was to extend out from the Alliance worksite and around to the north of the power pole and would block the unsealed road southern access route near the track. However, the owner of the land being used by the heavy vehicle depot asked that the barriers be removed to allow vehicles to access the unsealed road by turning left from Barwon Terrace when approaching from the south. The Alliance advised that their protocols[11] required that landowners not be disturbed, and the barrier was removed and repositioned more tightly around the Alliance worksite.
By the time of the collision, Alliance works near the level crossing had been completed and the works location had moved further south. Alliance activities were then at the southern end of the unsealed road, about 560 m from the level crossing. Access from the Alliance worksite onto Barwon Terrace was via the unsealed road.
The unsealed road
Overview
The road was located on Victorian government‑owned (crown) land but was not recognised as a road by COGG or the Victorian government and had not been named. The road ran in a southerly direction for about 560 m from Barwon Terrace where, at its southern end, it terminated close to the Alliance worksite and Breakwater Road in South Geelong. It did not join Breakwater Road. At its northern end, the unsealed road terminated on the western side of Barwon Terrace. The junction between the unsealed road and Barwon Terrace extended from north of the level crossing, southward to the middle of the crossing, a distance of about 40 m.
Usage
Earlier usage
The history of the unsealed road and its usage was examined. It is probable that the junction between the unsealed road, Barwon Terrace and the Barwon Terrace level crossing was not inhibited by any fencing in the years prior to the incident.[12] This absence of a physical barrier meant that road vehicles could turn left or right onto Barwon Terrace from any point along the junction with the unsealed road and adjacent land. Vehicles could also enter the area by turning left or right from Barwon Terrace.
Imagery and associated evidence indicate that the historic primary access to and from the unsealed road was around 30–40 m north of the rail track crossing and north of a nearby power pole. Over time, access had developed closer to the rail corridor and track (Figure 6).
Figure 6: Train route and location of Barwon Terrace level crossing
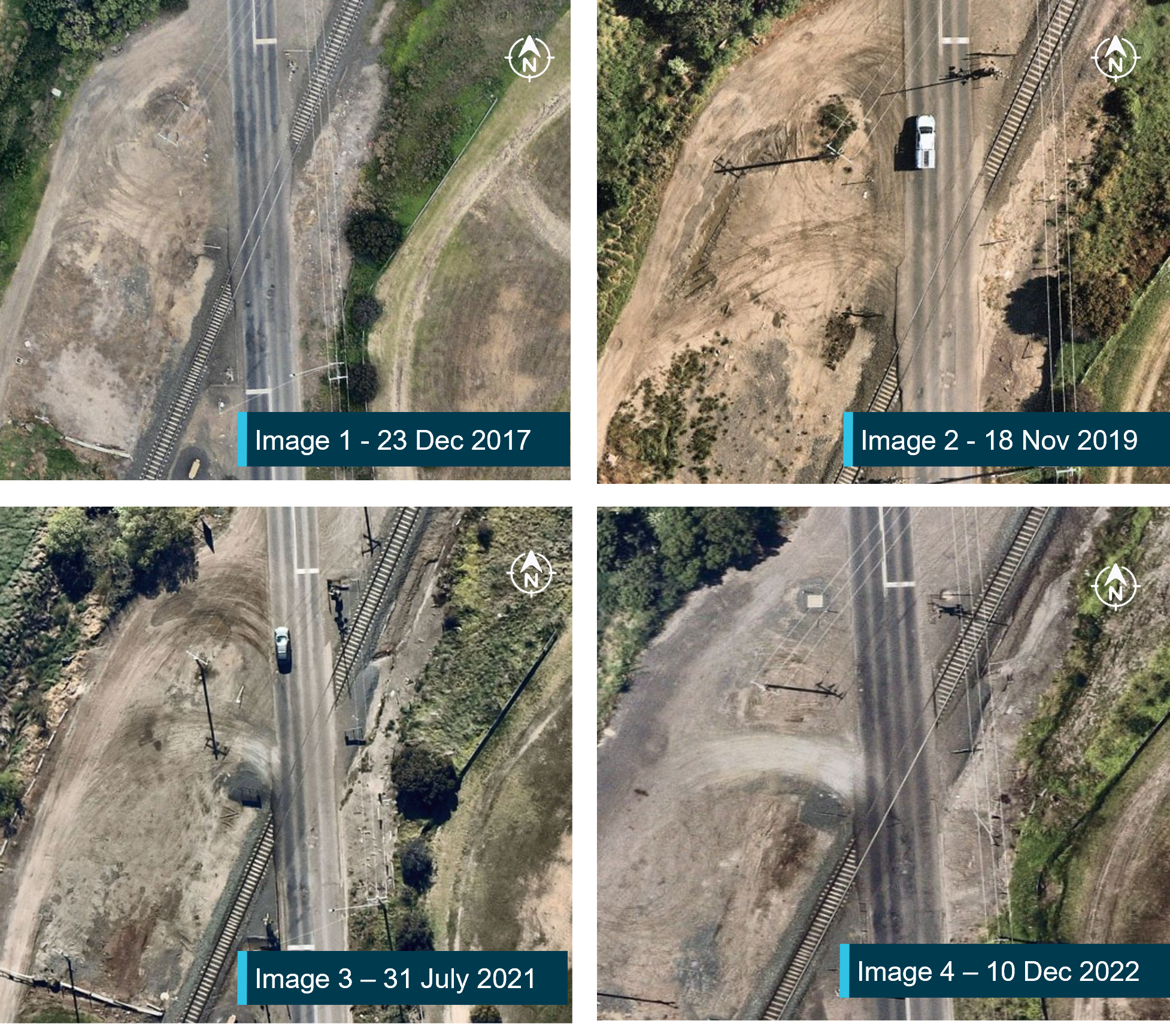
Source: Nearmap, annotated by the Office of the Chief Investigator
An overhead photograph of the intersection taken 4 months before the collision (Figure 6, Image 4) showed that use of the access near the track and south of the power pole had increased. This access was probably used by vehicles turning right from the unsealed road onto Barwon Terrace and vehicles turning left off Barwon Terrace onto the unsealed road.
Recent usage
CCTV footage, sourced from the heavy vehicle depot, showed that in the weeks prior to the incident, light and heavy motor vehicles were often driven onto the Barwon Terrace level crossing from the unsealed road. This positioned the vehicles between the protection equipment on each side of the crossing. These vehicles included flatbed light trucks, utility vehicles, four-wheel drive vehicles and tip trucks.
Footage of the previous weeks also showed that, on occasion, vehicles were driven onto the crossing moments after a V/Line train had gone through the crossing but before the boom gates had risen.
Hazard identification
On 9 March 2023, prior to the collision and after an Alliance safety officer observed an Alliance vehicle turning right onto Barwon Terrace into the middle of the level crossing, a no right turn sign[13] was affixed to the power pole (Figure 7). The sign faced south towards traffic approaching from along the unsealed road. During ‘Pre-start’ and ‘Safe Talks’ at team meetings, Alliance personnel were also advised that they were not to turn right when exiting the unsealed road onto Barwon Terrace. V/Line personnel were present at some safety meetings.
Figure 7: No right turn sign on the power pole

Photograph showing the no right turn sign on the power pole. Source: The Office of the Chief Investigator
The truck driver and truck
The truck driver had worked for the earth moving company for approximately 1 month prior to the incident.[14] They were licensed to drive the truck and had had many years of experience as a truck driver. The truck driver was fatally injured in the collision.
The truck was a 1997 International tip truck and was owned by the earth moving company (Figure 8). The truck’s dump body was empty at the time of the collision.
Figure 8: A similar tip truck to that involved in the collision

The truck involved in the incident was of a type like that at Figure 8, but red in colour. Source: Google
The train driver and train
The train driver was qualified, assessed as competent and medically fit at the time of the collision. The train sustained minor damage to its front, did not derail and was able to be driven to the Waurn Ponds stabling yard.
Passenger train 7727 was a VLocity six car set which was being relocated to Waurn Ponds railway station for a passenger service to Melbourne later that morning. The only persons on board the train at the time of the incident were the train driver and conductor. Both were unhurt.
Figure 9: Damage to the front of train 7727

The damage to the front of VLocity train 7727 following the incident. Source: The Office of the Chief Investigator
Recorded information
Recorded information was sourced from a CCTV camera positioned at the heavy vehicle depot, the train’s data logger and from the level crossing data logger. Time references were corrected, and events aligned. The key events are shown in Table 1.
Table 1: Key events in lead‑up to collision
| Time (h:m:s) | Event | Approx. train distance from level crossing (m) |
| 6:35:44 | Truck departs depot | 1350 |
| 6:36:18 | Bells and lights commence | 660 |
| 6:36:29 | Boom barriers commence to descend | 450 |
| 6:36:32 | Train passes whistle board (no horn recorded) | 400 |
| 6:36:37 | Truck commences right turn towards level crossing | 290 |
| 6:36:38 | Boom barriers reach their horizontal position | 270 |
| 6:36:45 | Train brake application commences | 120 |
| 6:36:46 | First of several train horn applications | 107 |
| 6:36:50 | Truck is stopped on level crossing | 30 |
| 6:36:51 | Truck begins to reverse away from track | 15 |
| 6:36:52 | Level crossing island track detection of train and collision | 0 |
Safety analysis
Introduction
On 3 April 2023, at about 0631, empty V/Line passenger train 7727 left Geelong to travel to Waurn Ponds. At about 0636, as the train approached the Barwon Terrace level crossing in South Geelong, a tip truck drove onto the level crossing from an unsealed side road. Moments later, the train collided with the truck and the truck driver sustained fatal injuries. The driver of the train and the conductor were uninjured.
This analysis discusses:
- the context and circumstances of the collision
- the configuration at the intersection
- risk controls at the unsealed road exit onto Barwon Terrace
- risk management at the level crossing.
The context and circumstances of the collision
Use of the unsealed road
Imagery indicated that usage of the unsealed side road had increased over recent years. This increase was probably coincidental with increased usage by vehicles from the heavy vehicle depot located about 220 m south of the level crossing. The owner of the land at the depot had not submitted a planning permit application for the land use and correspondence from 2020 and 2021 between the City of Greater Geelong and the landowner had not resolved the permit issue.
In the weeks leading up to the level crossing collision, CCTV footage showed several trucks, light commercial vehicles and cars turning right from the unsealed road onto Barwon Terrace. Based on this evidence, it was probably common practice for vehicles to use this route when leaving the unsealed road.
Other factor that increased risk It was probably common practice for both light and heavy vehicles to turn right from the unsealed road onto Barwon Terrace and between the level crossing protection of booms and flashing lights located on each side of the crossing. |
Movement of the tip truck
The truck turned right from the unsealed road onto Barwon Terrace behind the protection equipment located on the north side of the crossing. This route was probably not unusual for vehicles wanting to travel south along Barwon Terrace. For the turn onto Barwon Terrace, it is probable that the driver’s attention was directed to road traffic from both directions to assure safe entry onto the road.
The level crossing flashing lights and bells were operating before the truck commenced its turn into Barwon Terrace, and the booms were descending to their down position as the truck started its turn. All protection equipment was working correctly at the time of the incident but may not have been observed by the driver.
As the truck turned onto Barwon Terrace to travel south, cars began to queue behind the boom barrier on the south side of the crossing. The train’s horn was also sounded when the train was about 107 m from the crossing. By either observation of the queued traffic and the descended boom to the south of the crossing, hearing the train’s horn, or observation of the train, the driver was probably alerted to the presence of an approaching train. The truck was stopped on the track and its driver attempted to clear the track by reversing their vehicle. However, they were not able to clear the track before the train collided with the forward part of the truck.
Contributing factor The truck entered the level crossing between the level crossing protection equipment on either side of the track and stopped on the track. The driver probably realised a train was approaching and reversed the truck but was unable to clear the track in time. |
The sounding of the train’s horn
Train data logger records did not indicate that the train’s horn had been sounded at the whistle board which was located about 400 m before the crossing. The horn was either not sounded or was sounded for a very short period that was not recorded by the logger.
It is unknown whether the driver of the truck would have heard the train’s horn over the truck cab’s ambient noise if the horn was sounded at 400 m distance and if heard, whether the driver would have recognised the sound as a warning of an approaching train.
Other factor that increased risk The train’s horn was not sounded or only sounded for a very short period at the whistle board located about 400 m from the level crossing, removing a potential audible warning to users of the level crossing. |
The configuration of the intersection
The acute angle between Barwon Terrace and the track meant that there was about 22 m between the rail track and the stop line where the unsealed road connected with Barwon Terrace. This large distance provided an opportunity for road vehicles to turn right from the unsealed road onto the level crossing behind the northern protection equipment. There was no barrier in place to prevent this high‑risk entry of vehicles onto the level crossing.
Contributing factor The configuration of the intersection between the unsealed road and Barwon Terrace allowed road vehicles to enter Barwon Terrace between the protection equipment on the northern side of the level crossing and the track. This rendered the protection on the northern side of the crossing ineffective for these vehicles. |
Risk controls at the unsealed road exit onto Barwon Terrace
At the time of the collision, road traffic control measures at the northern end of the unsealed road where it joined Barwon Terrace included signage. The Alliance advised that a ‘no right turn’ sign had been put in place a few weeks before the collision after the Alliance identified a risk associated with Alliance vehicles turning right onto the level crossing. However, CCTV footage indicated that some vehicles continued to turn right onto Barwon Terrace after the sign was placed. The sign was ineffective in deterring some drivers from continuing to turn right from the unsealed road onto Barwon Terrace.
In addition to normal road‑facing flashing lights to warn of approaching trains, the level crossing protection on the northern side of the crossing also included a single flashing light angled towards the unsealed road. However, this warning signal was directed towards the northern exit of the intersection rather than the exit closer to the rail track. Drivers of vehicles taking this right turn, including the truck involved in the collision, would typically not see this light.
Other factor that increased risk Risk controls put in place to prevent vehicles turning right from the unsealed road onto Barwon Terrace and between the crossing’s protection equipment were ineffective. |
Risk management at the level crossing
Rail infrastructure manager
This section of the rail network including the level crossing infrastructure was managed by V/Line. V/Line routine inspection of the level crossing reviewed the functionality of crossing equipment and the condition of signage. However, the inspection regime did not extend to identifying road geometry conditions that may heighten risk. An individualised risk assessment specific to the level crossing had not been conducted and there was no clear process to identify the changing conditions at the level crossing.
Other factor that increased risk V/Line inspection regime did not identify that the interface between the unsealed road and Barwon Terrace level crossing was a safety risk. Inspections did not extend to the routine review of any change to the configuration at the interface that may heighten risk. (Safety issue) |
Safety interface agreement
The Safety Interface Agreement (SIA) between road and rail managers that covered the Barwon Terrace level crossing did not identify any specific rail or road safety hazards associated with the interface between the unsealed road and Barwon Terrace. Flagging of the specific risks in the SIA may have provided an opportunity for all parties (including the road manager) to take proactive action in monitoring and addressing risks at the crossing.
Other factor that increased risk The Safety Interface Agreement between rail and road managers did not identify potential risks associated with the Barwon Terrace level crossing nor flag any requirement for special attention of the road configuration. |
Australian level crossing assessment model (ALCAM)
The Australian Level Crossing Assessment Model (ALCAM) assessment in 2017 and review in 2018 did not identify any specific risks to road or rail traffic at the junction between the unsealed road and Barwon Terrace other than the possibility that road vehicles may be driven around the boom gates. At the time of the 2017 survey, access to and from the unsealed road was probably at its intersection with Barwon Terrace about 30–40 m north of the track and not via the access route closer to the track, the use of which probably increased substantially after the survey.
ALCAM assessment is a risk-based process against requirements of the relevant Australian Standard, and it was unclear if processes included directly flagging unusual side road access. There may be an opportunity for ALCAM survey processes to include direct flagging of unusual and potentially changed road configurations.
Other finding The unsealed road access route close to the level crossing probably developed after the 2017 survey of the Barwon Terrace level crossing using the Australian Level Crossing Assessment Model (ALCAM), and the ALCAM survey report did not identify the route. |
Hazard identification and communication
In the months preceding the incident, the risk of a collision between road and rail traffic at the level crossing was identified by safety personnel associated with rail works in the corridor. In response, a no right turn sign was erected on the power pole at the north end near the exit from the unsealed road onto Barwon Terrace.
In the weeks prior to the incident, the hazard associated with vehicles accessing Barwon Terrace by turning right from the unsealed road was again identified by onsite rail project safety personnel and raised at safety and pre-start meetings. Some of these meetings included V/Line representatives.
In addition to briefing rail project workers about the hazard, additional signage prohibiting a right turn from the unsealed road onto Barwon Terrace was erected as a risk control. However, there was a missed opportunity for the safety concerns to be raised with the appropriate operational area of V/Line, either by the rail project directly or V/Line representatives onsite.
Other finding There was a missed opportunity for identified hazards associated with the level crossing configuration to be brought to the attention of the appropriate operational area within V/Line. |
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision between a truck and V/Line train 7727 at Barwon Terrace level crossing, South Geelong, Victoria on 3 April 2023.
Contributing factors
- The configuration of the intersection between the unsealed road and Barwon Terrace allowed road vehicles to enter Barwon Terrace between the protection equipment on the northern side of the level crossing and the track. This rendered the protection on the northern side of the crossing ineffective for these vehicles.
- The truck entered the level crossing between the level crossing protection equipment on either side of the track and stopped on the track. The driver probably realised a train was approaching and reversed the truck but was unable to clear the track in time.
Other factors that increased risk
- The train’s horn was not sounded or only sounded for a very short period at the whistle board located about 400 m from the level crossing, removing a potential audible warning to users of the level crossing.
- It was probably common practice for both light and heavy vehicles to turn right from the unsealed road onto Barwon Terrace and between the level crossing protection of booms and flashing lights located on each side of the crossing.
- Risk controls put in place to prevent vehicles turning right from the unsealed road onto Barwon Terrace and between the crossing’s protection equipment were ineffective.
- V/Line inspection regime did not identify that the interface between the unsealed road and Barwon Terrace level crossing was a safety risk. Inspections did not extend to the routine review of any changes to the configuration at the interface that may heighten risk. (Safety issue)
- The Safety Interface Agreement between rail and road managers did not identify potential risks associated with the Barwon Terrace level crossing nor flag any requirement for special attention of the road configuration.
Other findings
- The unsealed road access route close to the level crossing probably developed after the 2017 survey of the Barwon Terrace level crossing using the Australian Level Crossing Assessment Model (ALCAM), and the ALCAM survey report did not identify the route.
- There was a missed opportunity for identified hazards associated with the level crossing configuration to be brought to the attention of the appropriate operational area within V/Line.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the Rail industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Monitoring level crossing risks associated with road configuration
Safety issue number: RO-2023-003-SI-01
Safety issue description: V/Line inspection regime did not identify that the interface between the unsealed road and Barwon Terrace level crossing was a safety risk. Inspections did not extend to the routine review of any changing road conditions that may heighten risk.
Safety actions not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following additional proactive safety action in response to this occurrence. |
Additional safety action by The Djilang Alliance
The Djilang Alliance advised that on completion of the rail upgrade works, the interface between the Barwon Terrace level crossing and the unsealed road was upgraded. A fence and bollards were installed which prevented motor vehicles turning right from the unsealed road onto the middle of the level crossing.
Additional safety action by the Victorian Rail Crossing Safety Steering Committee
The Victorian Rail Crossing Safety Steering Committee (VRCSSC) has implemented changes to the Australian Level Crossing Assessment Model (ALCAM) survey program in Victoria, which now requires contractors undertaking assessments to identify and report any road network configurations like the incident location. Once reported, the rail infrastructure manager would be notified of the safety risk and further assessment and actions sought. Further, the ALCAM survey program has been accelerated over the previous 3 years, and by December 2025 all public level crossings in Victoria are scheduled to have had an assessment completed within the previous 5 years.
Glossary
| ALCAM | Australian Level Crossing Assessment Model |
| Alliance | The Djilang Alliance |
| COGG | City of Greater Geelong |
| V/Line | V/Line Corporation |
| VRCSSC | Victorian Rail Crossing Safety Steering Committee |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- accident witnesses
- Australian Level Crossing Assessment Model
- City of Greater Geelong
- data download information from Barwon Terrace level crossing
- data download information from train 7727 data recorder
- Department of Transport and Planning (Victoria)
- Djilang Alliance
- Lukarna Constructions Pty Ltd
- Victoria Police
- video footage and photographs taken on days and weeks prior to the accident
- video footage of the accident and other photographs and videos taken on the day of the accident
- V/Line Corporation.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to directly involved parties. Submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] The 'unsealed road' was not recognised as a public road.
[2] The train’s emergency brake was applied immediately following the application of the train’s service brake.
[3] VicTrack was a Victorian government‑owned organisation which owned Victoria’s rail land, buildings, infrastructure and rolling stock and leased those assets to the Department of Transport and Planning (a Victorian government department). Those assets were then sub-leased to rail companies.
[4] A statutory office established under the Transport Integration Act 2010.
[5] The relevant Safety Interface Agreement and Service Level Agreement stated that V/Line was responsible for the management and maintenance of the level crossing within 3 m of the outer running rail only.
[6] The RX-5 assembly consisted of an R6-25 Railway Crossing sign and an R6-9 Stop on Red Signal sign.
[7] The RX-9 assembly consisted of an RX-9(L) sign and an RX-9(R) sign.
[8] V/Line did not undertake any assessment or testing of infrastructure outside of the area of its control.
[9] ALCAM is owned by the National ALCAM Committee. The Rail Industry Safety Standards Board helps to support the system.
[10] ALCAM in Detail – An Introduction to the new ALCAM models (2014), page 15.
[11] The Alliance advised that this protocol was an informal, unwritten protocol.
[12] Overhead images (Source: Nearmap) of the level crossing and its junction with the unsealed road spanning 10 years prior to the incident do not indicate the presence of a fence at the intersection.
[13] ‘No right turn’ sign - (R2-6(R), AS 1742.2:2022 – Manual of uniform traffic control devices, Part 2: Traffic control devices for general use.
[14] The earth moving company operated out of the depot on the unsealed road.
Preliminary report
Report release date: 28/06/2023
| This preliminary report details factual information established in the investigation’s early evidence collection phase and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003. |
The occurrence
At about 0600 local time on 3 April 2023, a truck driver arrived at a heavy vehicle depot located about 240 m south of the Barwon Terrace level crossing in South Geelong. They prepared the tipper truck for work in Point Lonsdale and departed the depot at about 0635. The truck proceeded in a north easterly direction from the depot along an unsealed road which ran parallel to the V/Line broad gauge railway track towards Barwon Terrace level crossing.
After travelling along the unsealed road towards Barwon Terrace, the truck proceeded onto the level crossing between the boom barriers and stop lines located on either side of the crossing (Figure 1).
Figure 1: Direction of travel of truck and train and location of level crossing
Source: Imagery © Nearmap annotated by Chief Investigator, Transport Safety (Victoria)
Earlier at about 0631, V/Line train 7727, an empty six-car set with only the driver and a conductor on board, departed Geelong Railway Station towards Waurn Ponds (Figure 2). The train was being taken to Waurn Ponds Railway Station for a passenger service to Melbourne. As the train was being relocated, it did not stop at South Geelong Railway Station.
Figure 2: Train route and location of Barwon Terrace level crossing
Source: Imagery © Nearmap annotated by Chief Investigator, Transport Safety (Victoria)
At about 0636 just prior to sunrise in overcast and dry conditions, train 7727 approached the Barwon Terrace level crossing from the north. The train driver reported that on observing the truck approaching the level crossing, they sounded the train’s horn and applied the emergency brake. Soon after, the train collided with the truck that was foul of the track. The train was travelling at about 65 km/h at the time of collision.
The force of impact caused the truck to spin around in a clockwise direction (Figure 3) and the driver was fatally injured. The truck sustained substantial damage.
The train sustained minor damage to its front, did not derail and was able to be driven to the Waurn Ponds stabling yard. The train driver and the conductor were not injured.
Figure 3: Location of truck and train after the collision
Source: Victoria Police annotated by Chief Investigator, Transport Safety (Victoria)
Context
Barwon Terrace level crossing
The Barwon Terrace level crossing was located in South Geelong, about 3.5 km from central Geelong. The rail infrastructure and the level crossing were managed by V/Line Corporation. The line in this section was a single bi-directional broad gauge track with a maximum permitted speed of 115 km/h for passenger trains.
Travelling by road in a south easterly direction (away from Geelong), Barwon Terrace intersected the rail line at an angle of about 25 degrees to the road user’s left and 155 degrees to the right. The unsealed road intersecting Barwon Terrace near the level crossing provided access to nearby light industry.
The unsealed road used to access the truck depot widened at its intersection with Barwon Terrace. There was evidence of at least two routes being used by road traffic (Figure 1). One route joined Barwon Terrace north of the protecting boom barrier. A second route (taken by the truck on this day) joined Barwon Terrace between the boom barriers. Tyre tracks on the unsealed road indicated that this second route was in regular use.
Level crossing protection
The protection equipment at the level crossing consisted of boom barriers, flashing lights, warning bells and warning signage on each side of the crossing (Figure 4). The warning signage consisted of a Railway Crossing combination sign (R6-25), a Stop on Red Signal sign (R6-9), a Keep Tracks Clear Sign (G9-67-1A) and a Railway crossing with marker assembly sign [RX-9(L)].
The level crossing protection was observed to be working at the time of the collision.
Figure 4 - Level crossing protection equipment at the Barwon Terrace level crossing
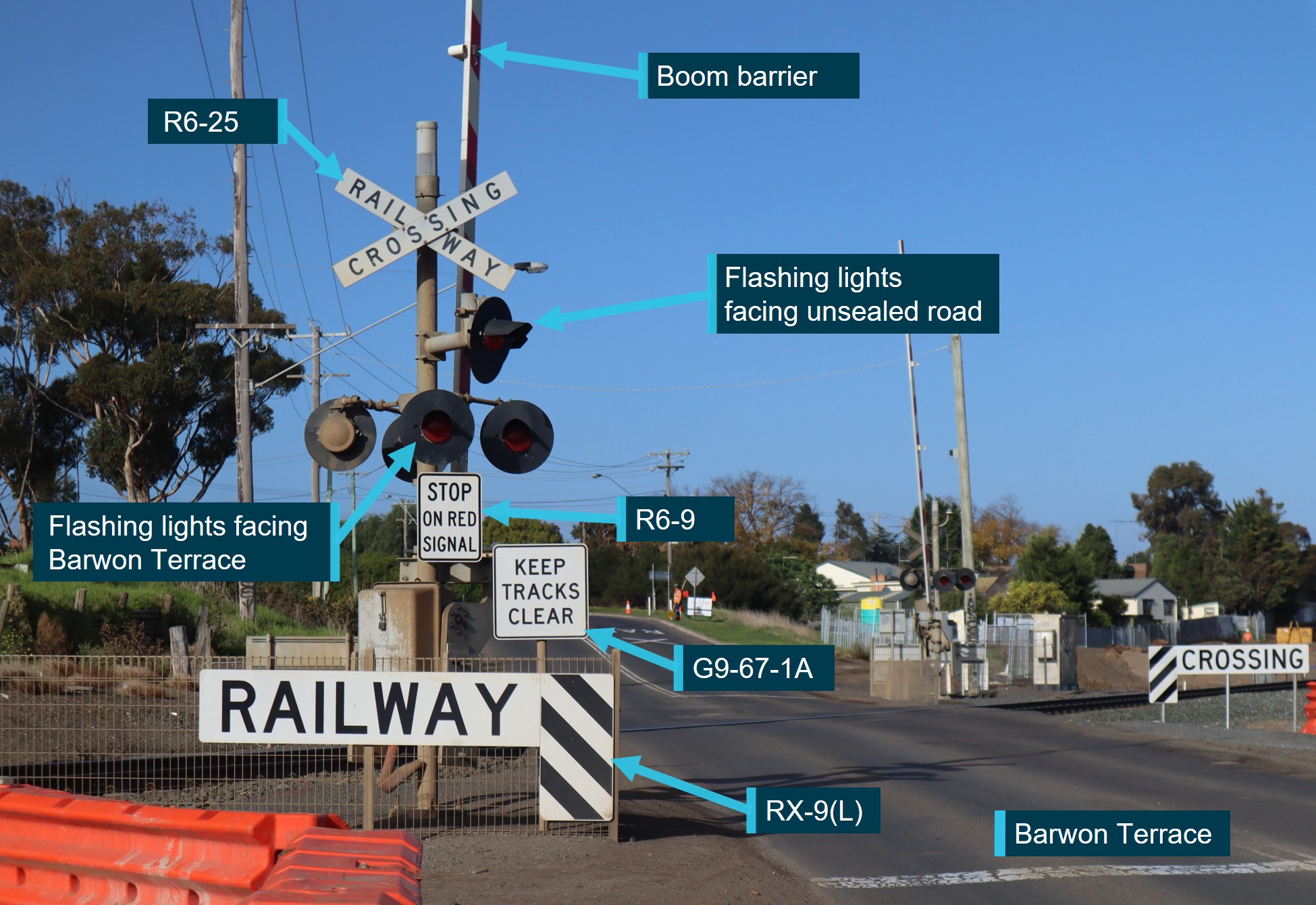
Photograph is taken from the northern approach to the level crossing, facing south.
Source: The Office of the Chief Investigator, Transport Safety (Victoria)
The level crossing warning lights at the northern end of the crossing consisted of two sets of red flashing lights. One set of lights faced north along Barwon Terrace. A second set of flashing lights faced across Barwon Terrace towards the northern end of the intersecting unsealed road.
The truck and driver
The truck was a 1997 International tip truck and was owned by an earth moving company. The truck was empty at the time of the incident. Truck drivers used the depot daily, departing and returning to the depot regularly.
The truck driver had worked for the earth moving company for approximately one month prior to the incident. The truck driver was fatally injured in the collision.
Further investigation
To date the following investigation activities have been completed:
- inspected the location of the occurrence
- examined train operational information
- examined truck operational information
- interviewed several parties
- commenced collection of other relevant information.
The investigation is continuing and will include review and examination of:
- the operation of the level crossing
- the operation of the truck and train
- the layout of the unsealed road and access to the Barwon Terrace level crossing
- a review of the traffic management in place prior to and at the time of the incident.
Should a critical safety issue be identified during the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
A final report will be released at the conclusion of the investigation.
Australian Transport Safety BureauAbout the ATSBThe ATSB is an independent Commonwealth Government statutory agency. It is governed by a Commission and is entirely separate from transport regulators, policy makers and service providers. The ATSB’s purpose is to improve the safety of, and public confidence in, aviation, rail and marine transport through:
The ATSB is responsible for investigating accidents and other transport safety matters involving civil aviation, marine and rail operations in Australia, as well as participating in overseas investigations involving Australian-registered aircraft and ships. It prioritises investigations that have the potential to deliver the greatest public benefit through improvements to transport safety. The ATSB performs its functions in accordance with the provisions of the Transport Safety Investigation Act 2003 and Regulations and, where applicable, international agreements. Rail safety investigations in VictoriaMost transport safety investigations into rail accidents and incidents in Victoria and New South Wales (NSW) are conducted in accordance with the Collaboration Agreement for Rail Safety Investigations and Other Matters between the Commonwealth Government of Australia, the State Government of Victoria, and the State Government of New South Wales. Under the Collaboration Agreement, rail safety investigations are conducted and resourced in Victoria by the Chief Investigator, Transport Safety (CITS) and in New South Wales by the Office of Transport Safety Investigations (OTSI), on behalf of the ATSB, under the provisions of the Transport Safety Investigation Act 2003. The Chief Investigator, Transport Safety (CITS) is a statutory position established in 2006 to conduct independent, no-blame investigation of transport safety matters in Victoria. CITS has a broad safety remit that includes the investigation of rail (including tram), marine and bus incidents. Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available on the ATSB website. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. |
Occurrence summary
| Investigation number | RO-2023-003 |
|---|---|
| Occurrence date | 03/04/2023 |
| Location | South Geelong |
| State | Victoria |
| Report release date | 27/06/2025 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Rail |
| Rail occurrence category | Collision |
| Occurrence class | Accident |
| Highest injury level | None |
Train details
| Train operator | V/Line |
|---|---|
| Train number | 7727 |
| Rail vehicle sector | Passenger - regional |
| Departure point | Geelong Railway Station, Victoria |
| Destination | Waurn Ponds Railway Station, Victoria |
| Injuries | None |
| Train damage | Minor |
Fuel starvation incident highlights importance of proper fuel management
Two pilots experienced engine surging and declared a mayday after inadvertently exhausting the aircraft’s auxiliary tanks, an Australian Transport Safety Bureau investigation notes.
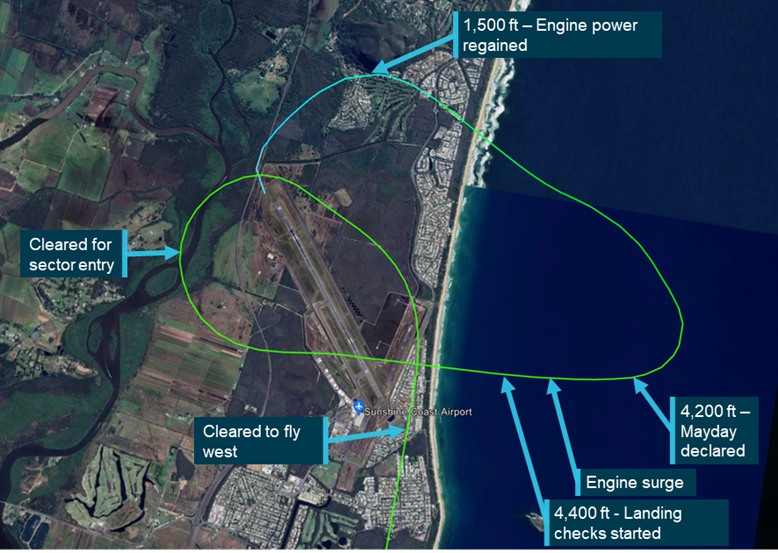
On 18 August 2022, an instructor and trainee instructor were operating a Cessna 310R during a training flight from Redcliffe Aerodrome, Queensland when the engines started surging alternatively.
The instructor declared a MAYDAY and began tracking for a forced landing at Sunshine Coast Airport, but during troubleshooting on descent, the crew switched from the auxiliary to the main fuel tanks, and the engine issues were rectified. The crew then conducted an uneventful landing.
An ATSB investigation found the auxiliary tanks had been exhausted, resulting in fuel starvation and engine surging.
“The pilots did not establish the amount of fuel on board prior to the flight, or manage the fuel state throughout the flight,” ATSB Director Transport Safety Dr Stuart Godley said.
“Both pilots were unaware of the fuel system configuration of the Cessna 310R, believing the aircraft was fitted with larger auxiliary tanks than was the case.”
The incident aircraft had a 140L usable fuel auxiliary tank capacity, but the instructor assumed it had the same 238L capacity as other Cessna 310 aircraft they had flown.
“The ATSB also found the operator had inconsistent and incomplete technical documentation for the aircraft, and the aircraft’s fuel selector plaques contained contradictory and incorrect information about the capacity of the auxiliary tanks, and in different units,” Mr Godley added.
Since the incident, the operator – Aircraft Australia – has implemented a new fuel log specific for the Cessna 310R.
Additionally, an internal memo has been distributed outlining the changes to the data sheet for the Cessna 310R to ensure all pilots and students are aware of the fuel configuration of the aircraft.
The operator has also requested fuel selector plaque replacements, to ensure the correct labels are installed.
Dr Godley welcomed the safety actions taken by the operator, but emphasised the incident’s relevance to all pilots.
“Accidents involving fuel mismanagement are an ongoing aviation safety concern, and are a reminder of the importance of monitoring fuel levels prior to, and during flight,” he said.
A selection of fuel management related incidents, and their safety lessons, have been previously published by the ATSB in the publication Avoidable Accidents No. 5.
Dr Godley also noted methods for cross-checking fuel on board before flight are published by the Civil Aviation Safety Authority in its Advisory Circular AC 91-15(Opens in a new tab/window).
Read the final report: Fuel starvation event involving Cessna 310, VH-JQK, near Sunshine Coast Airport, Queensland, on 18 August 2022
Lift-off location following a touch-and-go is more variable and complex to predict than a standing take-off
Key points
- Aircraft collided with rising terrain after conducting a touch and go from a rural property airstrip during a preparation flight for a commercial pilot licence test;
- Preflight planning was likely not performed to identify if the airstrip was suitable for flight training operations;
- Touch-and-go likely used more runway than a standing take-off, leading to the aircraft becoming airborne further along the runway, and closer to the rising terrain.
Rising terrain in the direction of take-off meant an airstrip being used for a touch-and-go was unsuitable as it exceeded the climb performance of the aircraft, an Australian Transport Safety Bureau investigation has found.
Two pilots, an instructor and student, were fatally injured when their single-engine two-seat Aquila aircraft collided with an embankment after a touch-and-go at Coombing Park airstrip in central west New South Wales, on 4 November 2020.
The flight was being conducted to assess the readiness of the student to complete a commercial pilot licence flight test. The flight had proceeded to overhead Coombing Park, where the student demonstrated the conduct of a precautionary search, to assess the suitability of conducting a landing there.
Following the precautionary search, a touch‑and‑go (landing without coming to a stop and accelerating to take-off again) was performed at Coombing Park. As the aircraft climbed through 200 ft above the lift-off point, a climbing left turn was conducted before flying straight again in the direction of a small dam, beyond which was a less wooded area. The aircraft then passed over the small dam and collided with an embankment on the far side of the dam.
“The ATSB found that pre-flight planning was likely not performed to identify if Coombing Park was suitable for flight training operations, which placed more importance on the conduct of the precautionary search to identify the rising terrain hazard in the overshoot area of the runway,” said ATSB Director Transport Safety Stuart Macleod.
“The precautionary search was conducted at a height and position that likely made assessing the hazard less effective.”
Further, the take-off was conducted on an uphill slope with a probable tailwind. A standing take-off in the more favourable reciprocal direction would likely have cleared all obstacles and terrain.
“Particularly at an unfamiliar airstrip, pilots must carefully consider the aerodrome characteristics to confirm if a touch-and-go is feasible, or if a full-stop landing and standing take-off should be completed instead,” Mr Macleod said.
“This accident demonstrates that the lift-off location following a touch-and-go is more variable and complex to predict than a standing take-off.”
The investigation also found that the aircraft operator had based its operations manual on the sample operations manual published by the Civil Aviation Safety Authority (CASA), which allowed for flight training into any aerodrome listed in the En-Route Supplement Australia (ERSA), including ALAs, although ALAs are not assured to any operational standard.
In addition, the investigation found that recommendations contained in the since-replaced CASA guidance CAAP 92-1(1) did not provide assurance that an aircraft would be able to outclimb rising terrain after take-off more than 900 metres from the runway end.
“Operators should also be aware that aerodromes meeting the recommendations in the now-obsolete CASA guidance publication CAAP 92-1(1) are not assured that an aircraft will be able to successfully climb away after take-off more than 900 metres past the runway end,” said Mr Macleod.
“The new performance-based recommendations of AC 91-02 now require operators to consider obstacle clearance beyond 900 metres.”
Flight training operators should also note that there are no standards for ALAs, even those listed in the ERSA as uncertified aerodromes.
“The published data, including obstacle information, for these uncertified aerodromes are potentially incomplete or inaccurate,” said Mr Macleod.
“This means that for take-off from ALAs, the new guidance requires pilots and operators to know the climb gradient needed to clear all obstacles by a safe margin until the aeroplane reaches the minimum height for flight,” Mr Macleod concluded.
Read the final report: Collision with terrain involving Aquila AT01, VH-OIS, Coombing Park Airstrip, 27 km south of Orange, New South Wales, on 4 November 2020
Grounding of World Diana, Port of Bunbury, Western Australia, on 22 April 2023
Final report
Report release date: 10/07/2024
Executive summary
What happened
On the morning of 22 April 2023, World Diana departed from berth no 3 in Bunbury under the conduct of a harbour pilot with 2 tugs assisting. The ship had to be manoeuvred into the inner harbour turning basin and turned to port to exit the harbour entrance. The turn did not go as planned and the ship’s bow grounded on a shallow bank to the east of the entrance.
The ship was then manoeuvred clear of the bank and departed the port. Subsequent inspections and surveys indicated minor hull damage and the ship was cleared to continue trading.
What the ATSB found
The ATSB investigation found that World Diana's turn to port was started earlier than planned, which reduced the available sea room to complete the turn. During the turn, the ship’s speed was allowed to increase until there was no room to safely turn, and the ship grounded.
The ATSB also found that bridge resource management during the pilotage was ineffective. The pilot set up the portable pilot unit but did not use the unit to its full potential. The departure plan did not provide any specific information or limits for the turn to either the ship’s bridge team or the tug masters. Nevertheless, while the tug masters had previous experience with this manoeuvre and the ship’s bridge team had further resources available no concerns were raised with the pilot until it was too late to avoid the grounding.
Finally, the investigation identified that the port had not developed adequate procedures that included arrival and departure plans for larger ships required to berth starboard side alongside berth no 3.
What has been done as a result
Southern Port Authority has updated its marine pilotage standards and procedures for Bunbury with standard procedures for departing all berths, including no 3 when berthed starboard side alongside. A maximum rate of turn for turning ships in the harbour has also been specified.
Safety message
This grounding illustrates the important part that bridge resource management plays in safe pilotage. Effective use of available resources reduces the chance of single-person errors and minimises their impact.
In this instance, proper use of the portable pilot unit, effective communication and active involvement of the World Diana’s bridge team and the tug masters would have allowed the deviation from the plan to be detected in time to prevent the grounding.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
On the morning of 22 April 2023, the bulk carrier World Diana was scheduled to depart the Port of Bunbury, Western Australia under the conduct of a harbour pilot. The ship was berthed starboard side alongside at berth no 3 (head-in) and needed to be manoeuvred into the inner harbour turning basin and then turned to port towards the harbour entrance (Figure 1). The ship was nearly fully laden with a cargo of grain and had a draught of 11.65 m forward and 11.69 m aft (a deep draught for the port).
Figure 1: Overview of Bunbury inner harbour with World Diana at berth no 3

Image source: Nearmaps, annotated by ATSB
From about 0542 local time, the pilot conducted a master-pilot information exchange (see the section titled Bridge resource management) on the ship’s navigation bridge (bridge), including discussing the departure plan. The 2 tugs allocated for the departure were made fast forward and aft on the port side. At 0620, the mooring gang arrived and began casting off the ship’s mooring lines as directed by the pilot.
At 0632, when all the mooring lines had been cast off, the pilot instructed both tug masters to ‘lift off’[1] using quarter power and, shortly after, asked them to increase to half power. By 0636, the ship had developed slight headway (0.3 kt)[2], with its main engine running dead slow ahead.
Soon after, the pilot stopped the ship’s engines and commenced turning the ship to port by directing that the aft tug stop lifting off and push at half power. The forward tug was directed to continue lifting off. At 0640, the ship’s speed had increased to 1.5 kt and the engine was ordered half astern. The ship’s rate of turn was 25°/minute and the forward tug was directed to stop (no weight on the tow line) while the aft tug continued pushing on the port side aft at full power.
As World Diana turned, its headway increased (1.6 kt) and, by 0641, the ship’s bow was closing on the shallow water on the eastern side of the harbour entrance at about 2.0 kt (Figure 5). At 0642, the forward tug master advised the pilot that the yellow buoys marking the shallow water were very close. In response, the pilot asked that the tug push with full power on the port bow to arrest the turn. At 0643, the same tug master advised the pilot that the tug could not remain in its position as it would ground, and suggested pulling back on the tow line to arrest the ship’s headway. The pilot then instructed both tugs to pull back on their lines at half power.
At 0643:30, World Diana’s bow grounded on the bank and its speed rapidly reduced to zero. The pilot then manoeuvred the ship astern using its propulsion and the tugs. Once the ship was established in the centre of the turning basin, the turn was completed. At the time of the incident, a pilot transfer vessel inspected the shallow area but did not identify any evidence of a grounding therefore it was believed to have been a near miss. Consequently, there was no inspection of the ship’s hull carried out prior to departing Australia. The pilot and ship’s master continued the departure and the pilot disembarked the ship outside the outer harbour.
Two days later, the pilot reported the incident as a near miss. A subsequent review of incident data indicated a grounding, and a survey of the seabed in the incident location was arranged. The survey identified an indentation in the soft seabed where World Diana’s bow had grounded (Figure 2).
Figure 2: Post incident survey imagery of shallow water (circled)

Image source: Survey by MNGsurvey overlay on Google Earth and annotated by the ATSB
Meanwhile, the ship was en route to its discharge port in Thailand via Singapore Strait. When the ship’s managers were made aware of the grounding, an underwater hull inspection was arranged to be done in Singapore. This inspection was conducted on 1 May and identified minor contact damage of the shell plating of the fore peak tank. The ship was cleared to continue trading with the damage to be attended at its next scheduled dry docking in 2025.
Context
World Diana
At the time of the incident, World Diana was registered in the Isle of Man, managed by OSM Maritime Group, Norway, and classed with Det Norske Veritas. It had been built by Oshima Shipbuilding, Japan, in 2020.
The ship was a Panamax[3] bulk carrier with an overall length of 229 m and breadth of 32.3 m. Propulsion was provided by a MITSUI‑MAN B&W 6S60E diesel engine driving a single, fixed‑pitch right‑hand turning propeller. The ship was fitted with a single, semi-spade conventional rudder.
World Diana’s navigation bridge was equipped with navigational equipment consistent with SOLAS[4] requirements, which included a voyage data recorder (VDR). However, data for the incident was not available to this investigation.
The ship had an appropriately qualified, multi‑national crew of 19.
The pilot
The pilot started working in the Port of Bunbury in 2007 and had completed about 4,000 pilotage movements there, including about 35 vessels of over 200 m. At the time of the incident, the pilot held a license for the movement of ships of any size permitted in the port. They were qualified to ‘assess competency as a marine check pilot’ and during the past 5 years had mostly trained new pilots.
The pilot also held an unrestricted certificate of competency as a ship’s master and had completed bridge resource management training in 2021. They had attended the Port Ash (Australia) manned model ship-handling training centre in 2022 and completed the ‘manoeuvre and handle a ship in all conditions’ training course.
In 2022, the pilot completed the Southern Port Authority manoeuvring and emergency training for the Port of Bunbury, which included a simulator exercise for ships departing berth no 3 after berthing starboard side alongside. Before the incident, the pilot had undertaken the same manoeuvre as the second pilot on one occasion and subsequently a solo pilotage of a ship of similar size to the World Diana.
The pilot had accepted the World Diana departure pilotage on the previous day and reported having had plenty of time to prepare for the pilotage and feeling well rested before the incident.
Port of Bunbury
The entrance to the inner harbour of the Port of Bunbury is about 150 m wide (Figure 3). The inner harbour has 5 berths, and a submerged rock is located within the 9 m charted depths off berth no 5 (Figure 6).
Berth no 3 is located on the western side, closest to the entrance. It is a specialised grain and woodchip loading berth, which started being used to load Panamax bulk carriers in September 2022. This larger size of ship had to be berthed starboard side alongside the berth to allow the cargo loaders to access all the ship’s cargo holds. World Diana was the 10th ship exceeding 210 m that had berthed starboard side alongside at the berth.
Pilotage is compulsory for ships with an overall length greater than 35 m. The port does not provide a vessel traffic service but can be contacted by VHF radio at all times.
Figure 3: Bunbury harbour berth layout
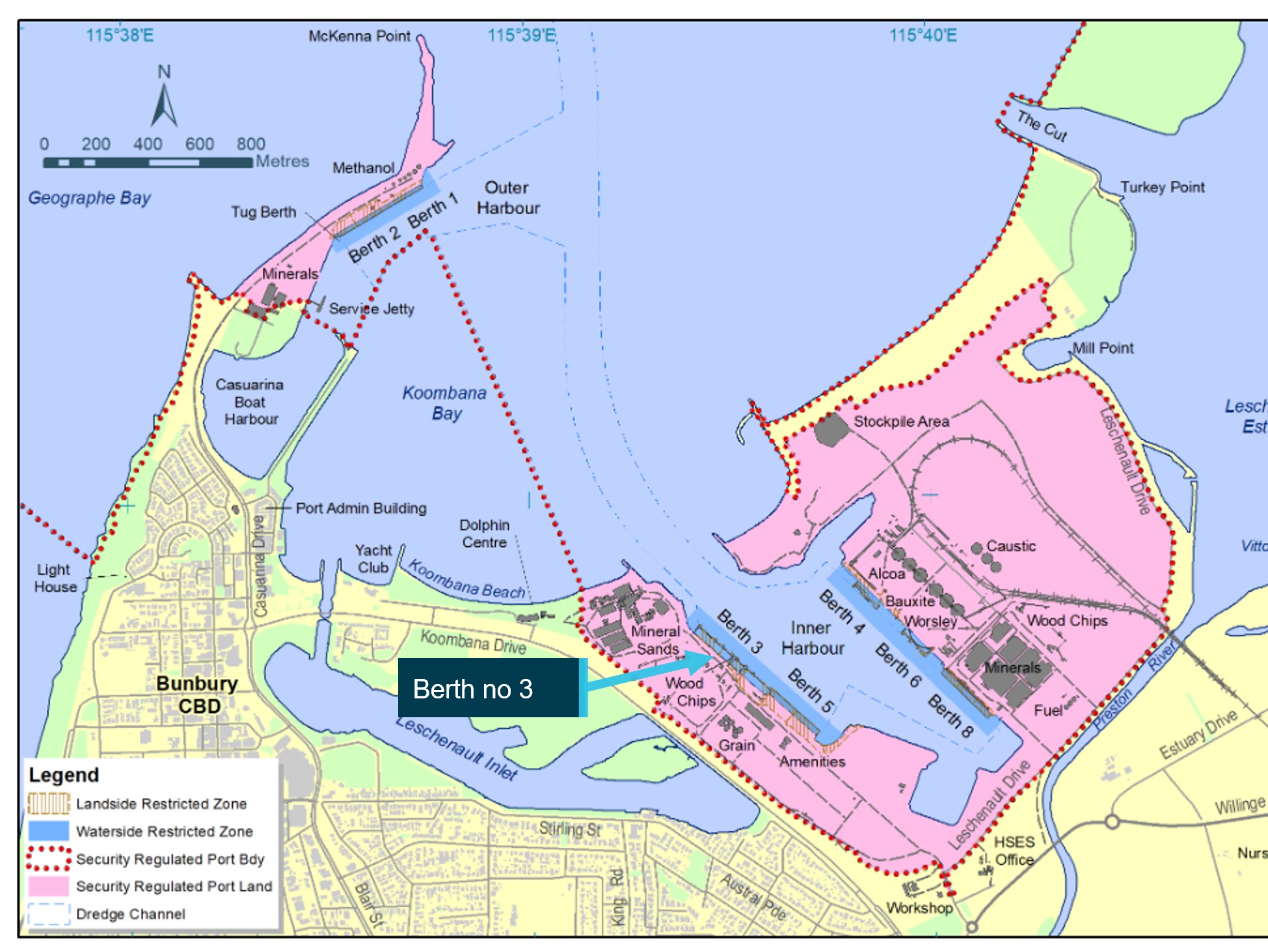
Image source: Southern Port Authority, annotated by the ATSB
Bridge resource management
Bridge resource management (BRM)[5] for World Diana’s pilotage started with a master‑pilot information exchange during which the pilot presented the departure plan (Figure 4). A hand‑drawn line on the plan indicated the approximate direction of travel, including the turn to port and the locations where the tugs would be cast off. It included the calculated static under keel clearance (1.82 m), but did not include any specific information such as ship’s speed, rate of turn and clearing distances or associated limits. There was no bridge audio data available, therefore there was no record of what was discussed during the exchange.
Figure 4: Departure plan diagram
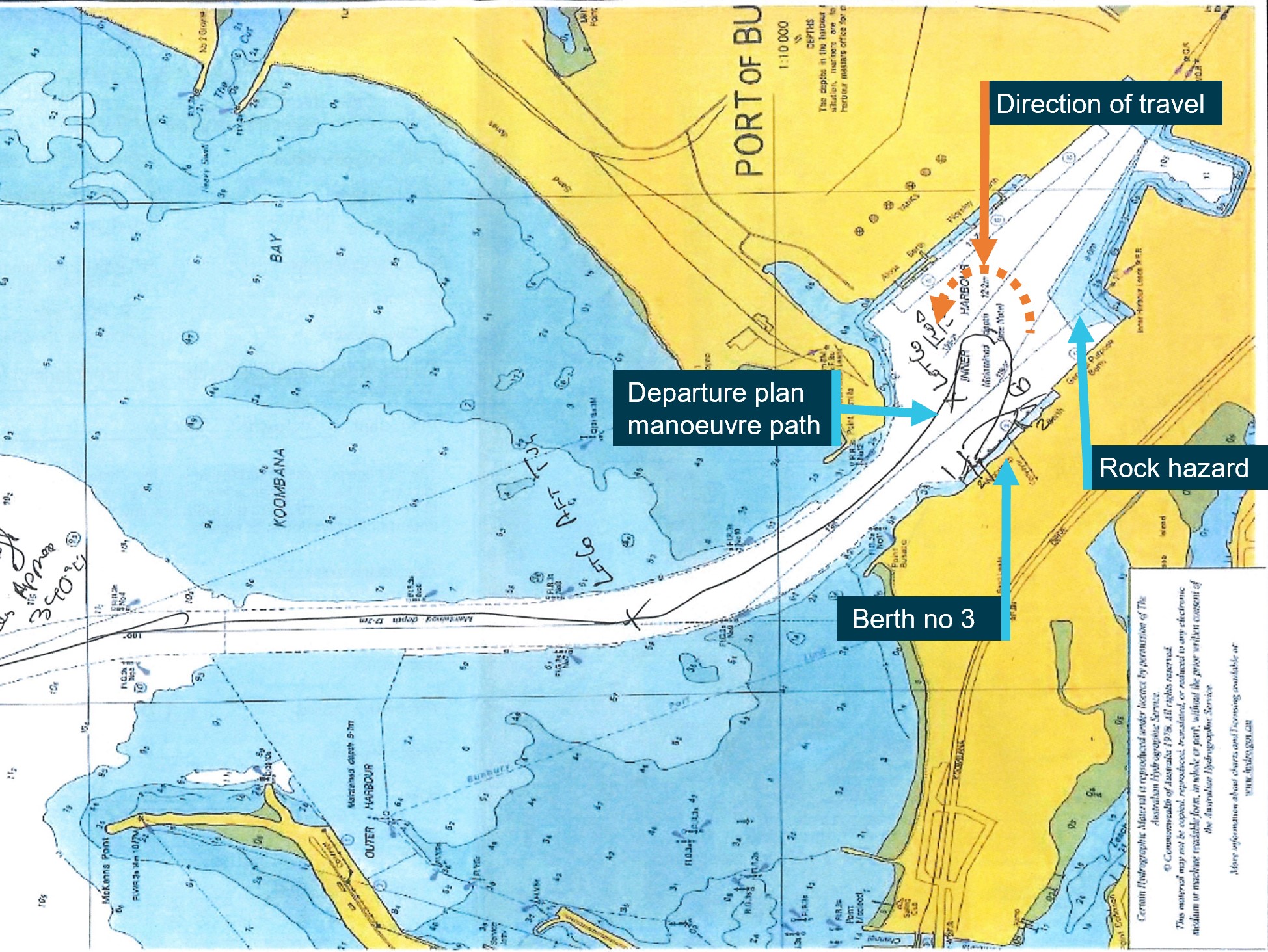
Image source: Southern Port Authority, annotated by the ATSB
The pilot reported having asked the ship master and bridge team to voice any concerns they had about the planned manoeuvre. They also stated that as the ship master was unfamiliar with the port, it was unlikely that deviations from the plan would be recognised.
The plan included using 2 tugs, each with a bollard pull of 80 tonnes. The pilot reported briefing both tug masters while waiting for the mooring gang and that both had previously participated in the planned manoeuvre.
Portable pilot unit
Before departing the berth, the pilot set up the port-supplied portable pilot unit (PPU) – an iPad application with a GPS receiver (Safe Pilot by Trelleborg). The ATSB obtained recorded PPU data, the only data available of the incident (as noted earlier, the ship’s VDR data was not saved). The PPU provided dynamic data together with a real-time display of the ship’s position, including a prediction of its trajectory.[6]
The involved pilot advised that they preferred to conduct pilotages largely by sight, using visual cues based on local knowledge and experience, and used the PPU mostly to check ship speed and rate of turn. A review of the recorded data by the ATSB identified that the PPU was showing the ship’s trajectory throughout the manoeuvring and had predicted that it was going to ground in the minutes before it occurred (Figure 5). It also showed the ship speed was 1.9 kt just prior to grounding.
Figure 5: Portable pilot unit display at 0641

Image source: Southern Port Authority, annotated by the ATSB
The manoeuvre
The pilot portable unit data was used to recreate the ship’s path (Figure 6).
Figure 6: Actual manoeuvre path
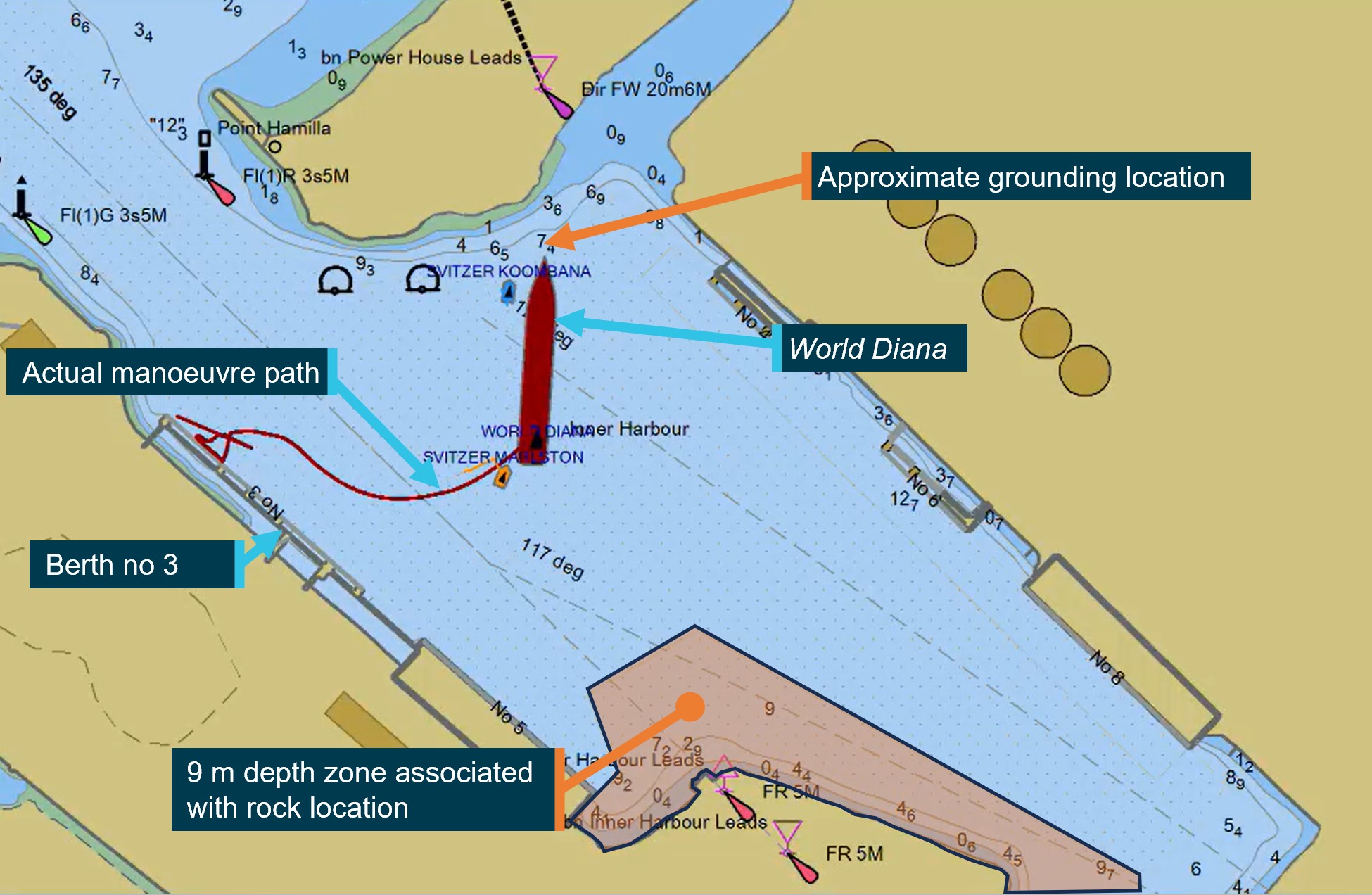
Image source: Southern Port Authority provided PPU data overlay on harbour nautical chart and annotated by the ATSB
According to the pilot, the turn was started early to keep clear of the submerged rock near berth no 5. The pilot stated that the plan was to have the aft tug push and then pull the ship back into position, but the ship's speed unexpectedly increased. The pilot attributed this to the aft tug pushing at full power at a slight angle, increasing the ship’s headway. The pilot attempted counteracting this by running the ship’s engine half astern and reported that as the rate of turn was 22˚/minute and increasing, the propeller was ineffective in arresting the headway. The pilot then resorted to using the forward tug to push at full power, but the tug had run out of sea room. Subsequently, the pilot instructed the tugs to pull back on the tow lines in an unsuccessful attempt to prevent the grounding.
The pilot further advised that the grounding could have been due to either of the following ship manoeuvring effects:
- Shallow water rudder effectiveness[7] – as the vessel swing was assisted by a fore and aft tug, it was determined that any degradation of rudder effectiveness due to low clearance with the harbour floor would have been overcome with the assistance of the tugs.
- Coanda effect[8] – this was not considered a contributing factor because the ship was pulled toward the bank by the tug and there was open water on the opposite side of the ship.
Tug master report
The ATSB reviewed the incident reports for the grounding, including one submitted by the tug master of the forward tug. In it they advised that there was a trainee manoeuvring the tug at the time. The tug master advised they thought that the turn may have been started early however, they did not advise the pilot. They instructed the trainee to be prepared to go alongside the ship to pull back. When they realised that the turn was not going to plan and the tug was running out of sea room, they took over from the trainee. As the tug closed on the yellow marker, the master advised the pilot they were unable to continue pushing and suggested they could pull straight‑back, to which the pilot agreed.
The tug master provided details of a debrief with the pilot several days after the occurrence. They advised that good communication and speaking up if the crew see any issues arising, were both raised as key learnings from this incident.
Previous manoeuvres
Pilots in Bunbury had regularly conducted ships of similar size to World Diana, with lengths up to 238 m accepted at some berths. As noted earlier, World Diana was the 10th large ship (more than 210 m) to depart berth no 3 via a turning manoeuvre to port. The first 2 departures were conducted successfully by a pilot and a safety pilot (that is, 2 pilots on the bridge). It was then decided that one pilot would conduct these pilotages.
The ATSB compared ship track PPU data from 4 of the previous departures from berth no 3 with World Diana’s track. This showed that the ship’s turn was started earlier than the others and that it was later manoeuvred further to the east of the turning basin (Figure 7). The maximum rate of turn achieved during these departures did not indicate wide variations, with World Diana’s rate of turn similar to the incident-free departures (Table 1).
Figure 7: Ship departure tracks from berth no 3
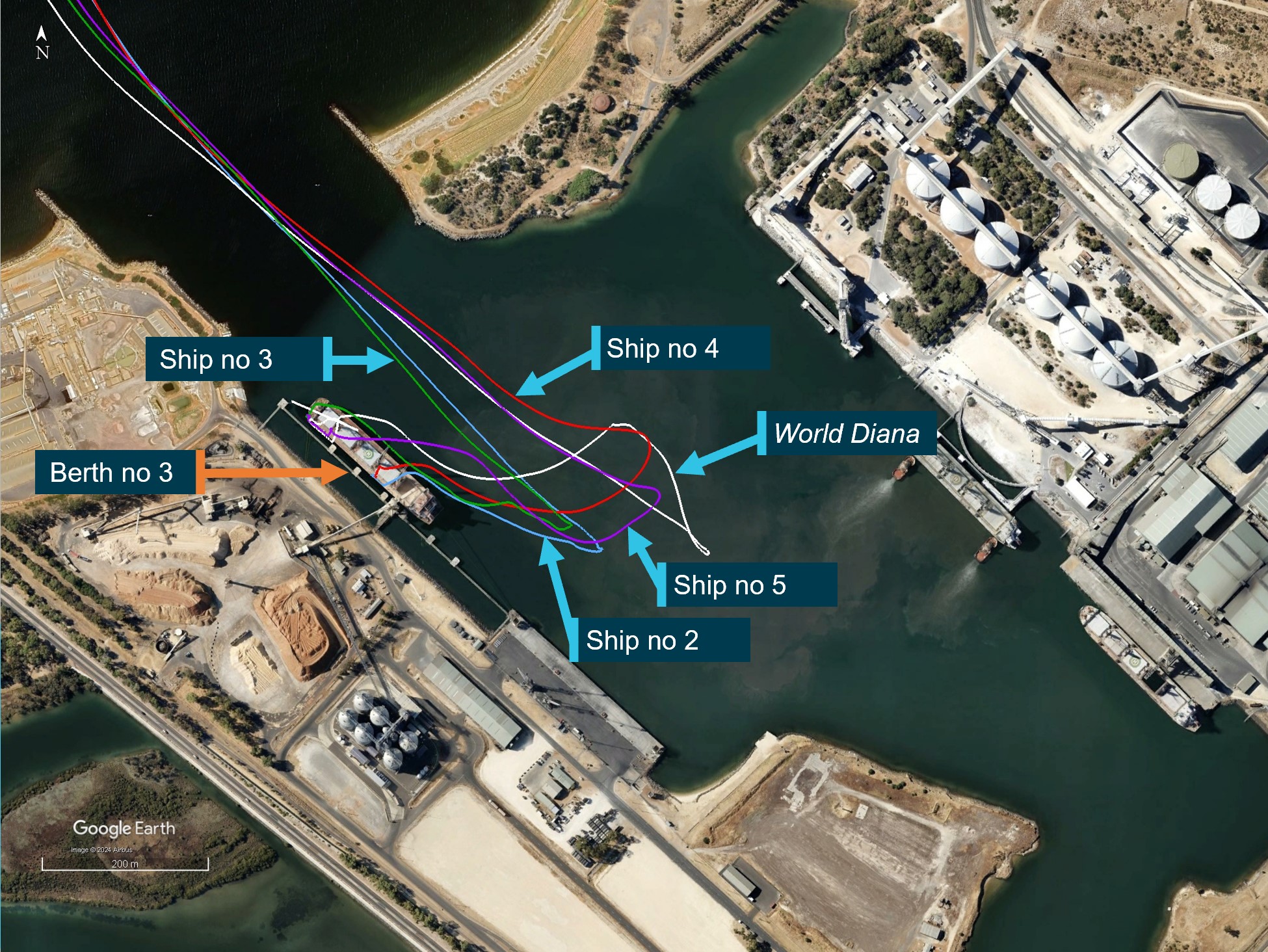
Ships referenced in image all have an approximate length of 229 m and show a different starting position due to their movement along berth no 3 used to load different hatches. The PPU data point is taken from a single position at the bridge of the ship. Labels also used as reference for Table 1.
Image source: Southern Port Authority provided PPU data overlay on Google Earth, annotated by the ATSB
Table 1: Maximum rate of turn recorded
| Ship | Size (m) | Maximum rate of turn recorded by PPU |
| World Diana | 229 | 29°/min |
| Ship 2 | 229 | 20°/min |
| Ship 3 | 229 | 25°/min |
| Ship 4 | 229 | 27°/min |
| Ship 5 | 229 | 28°/min |
Pilotage procedures
The Port of Bunbury marine pilotage standards and procedures manual stated that the PPU provided to pilots was to be used for the movements of ships with draughts exceeding 11 m. The manual stated that the PPU was 'an aid to navigation and should not be relied upon solely for the passage of the vessel’. Pilots were required to follow BRM principles, and the manual included the following instructions:
SPA [Southern Port Authority] fully endorses the principles of BRM. Pilots must:
- Make it to the bridge giving ample time for the proper exchange of information between the Master and Pilot before entering the channel.
- During the Master/Pilot exchange of information, present and discuss the intended passage plan and manoeuvre with the Master and bridge team. Information to be exchanged with the Master must include tug arrangements, prevailing weather and tidal conditions, mooring arrangements and vessel positioning. Information to be given to the Pilot should include: the vessels manoeuvring characteristics, arrival draft and the operational status of equipment and machinery. Master needs to sign the passage plan confirming the understanding of its intent.
The procedures manual provided arrival plans for all berths, including guidance for entering the harbour. These plans indicated berthing the ship head-out (that is, bow facing harbour entrance) by turning the ship either to port or starboard as shown below for berth no 3 (Figure 8). Specific ship-handling guidance such as rate of turn or speed was not provided. The manual did not include a plan to berth a ship starboard side alongside berth no 3. No departure procedure or plan was provided for any berth. In their departure plans, pilots used a copy of the chart to hand‑draw a plan, such as in this case (Figure 4).
Figure 8: Arrival procedures for berth no 3
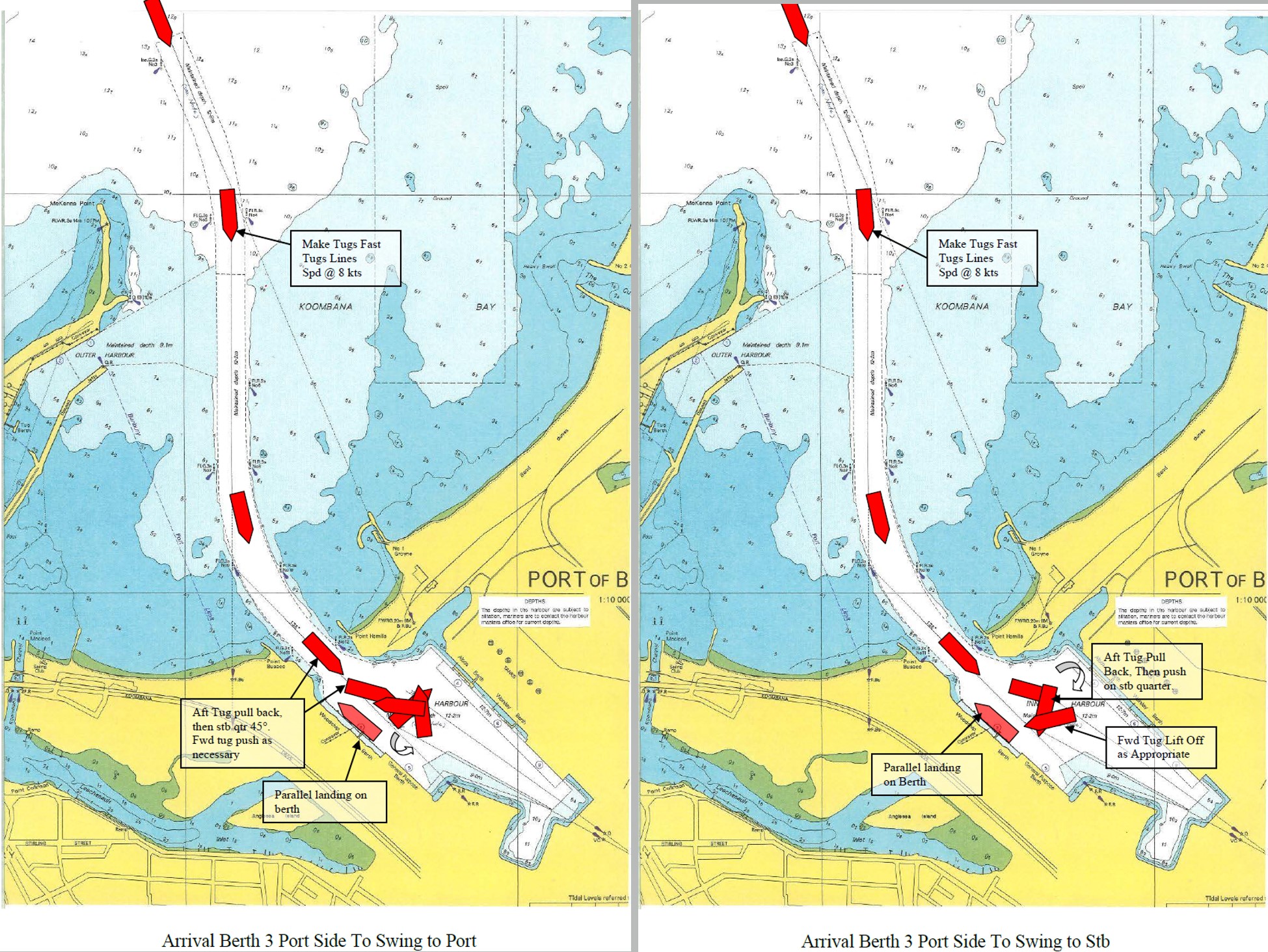
Image source: Southern Port Authority
Safety analysis
As World Diana was starboard side alongside berth no 3, its departure required the ship to be manoeuvred into the inner harbour turning basin and turned to port to exit the harbour entrance. During the master pilot information exchange on the morning of 22 April, the pilot provided a diagram of the departure plan, indicating the turn and the locations of the 2 assisting tugs. No specific information such as ship’s speed, rate of turn, clearing distances or associated limits was shown on the plan and no evidence was provided that these items were discussed.
At approximately 0632, shortly after the ship had left the berth, the pilot began turning the ship to port earlier than planned using both tugs, the ship’s main engine and steering. According to the pilot, the turn was started early to keep clear of the submerged rock near berth no 5. However, the rock was located off the farthest end of berth no 5, over a ship length ahead of the ship’s bow. Significantly, starting the turn early also reduced the sea room available to turn.
By 0636, use of the ship’s main engine had resulted in developing slight headway (0.3 kt). Four minutes later, the speed had increased to 1.5 kt and the ship was turning rapidly towards the shallow waters to the east of harbour entrance. In response to the developing situation, the pilot reversed the main engine (half astern) and instructed the aft tug to push at full power on the port side to turn the ship in the limited sea room. After a couple of minutes, the pilot realised that the turn could not be made in time to avoid the shoals and attempted to arrest the turn followed by an attempt to arrest the headway by using the tugs. These measures were unsuccessful, and shortly after 0643, the ship’s bow grounded.
The pilot’s portable pilot unit (PPU) was accurately displaying the ship’s position and progress in real time and indicating useful data, such as speed and rate of turn, to safely complete the turn. At 0641, the PPU predicted that the ship would ground. However, neither the pilot nor others on the bridge were using the PPU or paying attention to its display. Additionally, the forward tug's master identified that the ship was turned early but raised no concern with the pilot until the shallow water was extremely close, a minute before the grounding.
Overall, bridge resource management (BRM) was ineffective, most likely as specific information and limits for the departure plan were only known to the pilot, which made it difficult for the bridge team to raise concerns with the pilot. Nevertheless, had the ship’s master, being a ship-handler familiar with the ship’s manoeuvring characteristics, been actively monitoring the pilotage, the early turn and ship’s increasing headway, should have become evident on the ship’s monitors as well as the PPU. The PPU was displaying information to help avoid the grounding but this was not detected. Neither the bridge team nor the forward tug master raised any concerns with the pilot about the ship-handling errors until the grounding was imminent. In addition, when the pilot became aware of the imminent grounding, they did not make full use of the ship’s main engine, which remained at half astern (not full or emergency full astern) nor were the anchors dropped.
The investigation identified that no procedures had been developed that included arrival and departure plans for larger ships that were required to berth starboard side alongside berth no 3. This reduced the information available to pilots for these ship movements and to share with bridge teams and tug masters to ensure a common understanding of how manoeuvring would be conducted.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the grounding of World Diana when departing berth no 3 in Bunbury, Western Australia on 22 April 2023.
Contributing factors
- World Diana's turn to port to depart the inner harbour was started earlier than planned. This reduced the available sea room to complete the turn.
- During the turn, the ship’s speed was allowed to increase until there was no room to safely complete the turn and the ship grounded.
- Bridge resource management during the pilotage was ineffective. The pilot set up the portable pilot unit but did not detect the PPU projecting the ship grounding, there was no evidence that the bridge team was provided specific information or limits about the planned manoeuvre. In addition, neither the bridge team nor the forward tug masters advised the pilot of their manoeuvring concerns until the grounding was imminent.
Other factor that increased risk
- The Port of Bunbury had not developed adequate procedures that included arrival and departure plans for larger ships that were berthed starboard side alongside berth no 3.
Safety actions
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Safety action by Southern Port Authority
The Southern Port Authority has updated its Marine Pilotage Standards and Procedures Manual to include:
- standard procedures for departing all berths, including berth no 3 after berthing starboard side alongside.
- a maximum rate of turn for turning ships in the harbour of 20° per minute.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- manager of World Diana at time of incident
- pilot
- forward tug master
- Southern Port Authority
- survey completed by MCMULLEN NOLAN GROUP PTY LTD
References
Sanders, D.J. and Plumridge, M.J. (1990) The Nautical Institute on pilotage and Shiphandling. London: Nautical Institute.
Port Ash (Version 3.7 Sept 2012) Course in General Shiphandling. Australia: Port Ash
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Australian Maritime Safety Authority
- the pilot, tug masters and ship manager
- Southern Port Authority
Submissions were received from the:
- tug operator
- ship manager
- Southern Port Authority
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Lift off: pulling back on the tug’s tow line from any direction, except alongside the ship.
[2] One kt, or one nautical mile per hour, equals 1.852 kilometres per hour.
[3] A ship that is limited in size to the dimensions of the original Panama Canal locks.
[4] The International Convention for the Safety of Life at Sea, 1974, as amended.
[5] Bridge resource management can be defined as the effective management and use of all appropriate resources, including personnel and equipment, by a ship’s bridge team to complete its voyage safely and efficiently.
[6] The ship prediction is a simple iterative projection of ship’s position and heading based on its current position, course over ground, speed over ground, and rate of turn. The course and speed values are ‘smoothed’ by using a 3-second average to calculate the prediction.
[7] In shallow water the under-keel clearance affects ship turning behaviour. The hydrodynamic actions are complex, but the overall result is that in shallow water the changes in water flow round the hull have the result that a given rudder angle produces a smaller yaw angle than in deep water.
[8] The Course in General Ship Handling course notes created by Port Ash version 3.7 Sept 2012, describe the Coanda effect as an area of low pressure created between the ship and wharf which occurs when a tug is pulling a ship’s bow away from a wharf. A low-pressure area is created if part of a tug’s wash moves around the ship’s bow. The low‑pressure area attracts the ship’s bow reducing or negating the tug’s pull.
Occurrence summary
| Investigation number | MO-2023-001 |
|---|---|
| Occurrence date | 22/04/2023 |
| Location | Bunbury |
| State | Western Australia |
| Report release date | 10/07/2024 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Marine |
| Marine occurrence category | Grounding |
| Occurrence class | Incident |
Ship details
| Name | World Diana |
|---|---|
| IMO number | 9875214 |
| Ship type | Bulk Carrier |
| Flag | Isle of Man |
| Classification society | Det Norske Veritas |
| Manager | OSM MARITIME AS |
| Departure point | Port of Bunbury, Western Australia |
| Destination | Port of Koh Sichang, Thailand |
| Damage | Minor |
ATSB preliminary report details 737 large air tanker accident sequence of events
Key points
- 737 had been tasked to tag and extend a line of fire retardant which extended downslope;
- Flight data and cockpit voice recorder downloads instrumental in establishing accident sequence of events;
- Preliminary report outlines factual information collected in the on-going investigation’s early evidence collection phase.
An ATSB preliminary report details the sequence of events leading to a Boeing 737 large air tanker’s impact with a ridgeline in Western Australia’s Fitzgerald River National Park while conducting an aerial fire-fighting task on 6 February 2023.
The preliminary report outlines factual information collected in the on-going investigation’s early evidence collection phase, and details that the modified Coulson Aviation-operated 737 air tanker, callsign ‘Bomber 139’, with two pilots on board, had departed from Busselton Airport to assist fire control efforts near Hopetoun, about 600 km south-east of Perth.
“Arriving at the fire ground, the 737 crew was briefed by a bird-dog aircraft that the tasking was to tag and extend an existing retardant line,” said ATSB Chief Commissioner Angus Mitchell.
“The retardant line was to extend downslope, with the bird-dog briefing the 737 crew that their target altitude (above sea level) was 500 feet descending to 400 feet.”
Flight recorder data shows that Bomber 139 descended to about 400 ft and completed a partial drop of three-quarters of their tank before the captain, who was pilot flying, stopped the drop because their retardant line was entering a burnt area.
Bomber 139 then repositioned to commence another drop to use the remaining retardant to further extend the retardant line.
During the second drop, Bomber 139 descended through 400 ft altitude – or 80 ft above ground height – at an airspeed of 110 kt with the engines at high idle as the retardant line was extended downslope.
“Flight recorder data shows the throttles were advanced and the engines had accelerated just before the aircraft struck a ridgeline with the stick shaker activating. The aircraft then cleared a small line of foliage, before impacting the ground a second time and sliding to rest,” said Mr Mitchell.
“Fortunately, and remarkably, both pilots were able to exit the aircraft through a cockpit window, and suffered only minor injuries.”
The aircraft was subsequently consumed in a post-impact fire.
“Despite extensive fire damage, ATSB recorders specialists in our Canberra technical facilities were able to download files from both the flight data recorder and cockpit voice recorder,” Mr Mitchell said.
“As well as information from those recorders, interviews with the flight crews, a 3D map of the accident site created using a drone, and other recorded flight information will be instrumental to the ongoing investigation.”
ATSB investigators have also collected documents and recorded data from the operator as well as records from the WA Department of Fire and Emergency Services.
“The investigation is continuing and will include validation of the recorded data and reviews of the communication procedures for bird-dog and large air tanker pilots, the operator’s crew resource management procedures and practices, and standards and safety margins for 737 retardant drops.”
The preliminary report notes that following the accident, the operator increased their large air tanker minimum retardant drop heights and airspeeds.
Mr Mitchell said that a final report, containing findings and the analysis to support those findings, will be released at the conclusion of the investigation.
“However, should a critical safety issue be identified at any time during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.”
Read the preliminary report: Collision with terrain involving Boeing Company 737-3H4, N619SW, Fitzgerald River National Park, Western Australia, on 6 February 2023
Fuel starvation and ditching involving Piper PA-28, VH-FEY, 15 km north-west of Jandakot Airport, Western Australia, on 20 April 2023
Final report
Report release date: 28/11/2023
Executive summary
What happened
On 20 April 2023, a Piper PA-28-181 ‘Archer’ aircraft, registered VH-FEY, departed Carnarvon, Western Australia for a private flight with the owner-pilot and 2 passengers on board. The aircraft initially proceeded to Geraldton to drop off one of the passengers before continuing to Jandakot (Perth). Based on the conduct of previous similar flights, and the aircraft departing Carnarvon with full fuel tanks, the pilot considered there was sufficient fuel remaining for the return journey to Jandakot and did not refuel at Geraldton.
The pilot departed Geraldton and tracked to Jandakot via the generally direct route aligned with the coast, which was essentially the reciprocal of the track flown the day before. After cruising at 5,500 ft, the pilot descended to 4,000 ft then 2,000 ft, because of airspace restrictions.
At about 10 km north of Fremantle, as the pilot was tracking coastal over water, engine power subsided to idle power over a couple of seconds then recovered to cruise power. In response, the pilot selected the mixture control to full RICH and carburettor heat to ON. (The electric fuel pump was already selected ON.)
Engine power then subsided and recovered a number of times over a period of about 2 minutes. There were no indications of a mechanical failure and the pilot looked at the instruments but was unable to recall any indications after the event.
The pilot was unable to maintain height and decided to turn into wind for a forced landing on the adjacent beach but there were a number of people on the beach. Instead, the pilot decided to ditch the aircraft in the ocean as close to shore as possible.
As they were approaching the water, the pilot tried to hold the nose up as far as possible. A main wheel contacted the water and the aircraft skipped along the surface for a few seconds. Then the right wing dropped rapidly, consistent with a stall, and dug into the water, quickly stopping the aircraft. Water gushed up over the front of the aircraft and windscreen.
The pilot and passenger exited the aircraft uninjured and swam to shore.
What the ATSB found
The pilot departed Carnarvon with sufficient fuel for the intended flight to Jandakot via Geraldton but did not carry out regular fuel quantity checks in accordance with regulatory guidance or keep a written log of the fuel consumed from each tank during the flight.
During cruise at 1,900 ft, engine power subsided to low power then returned to normal power. This occurred a number of times, probably because of a lack of usable fuel in the selected (right) tank.
The pilot responded to the engine power anomalies by carrying out some of the emergency procedures but did not select the other (left) tank, which contained usable fuel. Consequently, engine power was not restored, and the pilot carried out a forced ditching into the ocean near a beach.
Prior to the first departure from Geraldton on the day of the occurrence, the pilot drained a significant amount of water from both fuel tanks (that had been refuelled to full the night before) and from the fuel strainer. The aircraft was subsequently operated for over 6.5 hrs with a refuelling at Carnarvon without any symptoms of fuel contamination and it is unlikely that there was a significant amount of water remaining in the fuel.
The engine had been in service for 28 years since overhaul and 13 years since a bulk strip, which was more than double the recommended time before overhaul of 12 years. However, given no engine defects were identified and the required maintenance was carried out, this was not identified as a factor in that occurrence.
Safety message
Fuel management
EFB and GPS technology have enhanced flight planning and navigation capability, but pilots are still required to carry out in-flight fuel quantity checks at regular intervals. These should include a cross check of all available data, including fuel quantity indications, and be recorded. For aircraft with separate tank selections, it is advisable to monitor the fuel consumed, and fuel remaining, for each tank.
Although the fuel gauges in older light aircraft can be unreliable and should not be the sole source of fuel quantity information, they are an essential component in fuel management processes. As such, they should be maintained in a serviceable condition with regular pre-flight and post-flight validation against known fuel quantities. If a fuel gauge indicates an unexpectedly low fuel quantity, the pilot should consider that to be a valid indication and act accordingly, until the anomaly is resolved.
Emergency procedures
Relative to a complete engine power loss, an intermittent or partial engine power loss is an ambiguous condition that can disrupt pilot implementation of emergency procedures. Unless there is an obvious solution, pilots should prepare for a complete engine power loss and follow the applicable procedures to optimise recovery of engine power.
If pilots might be required to ditch in case of an emergency, they should be familiar with the applicable procedures in the POH, as available, and/or generic guidance produced by national aviation authorities.
Engine time before overhaul
Although continued private operation is conditionally permitted for aeroplane engines that have exceeded the recommended calendar time before overhaul, operators should consider the length of the extension, modification status, and associated risk of failure.
The investigation
| Decisions regarding the scope of an investigation are based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, a limited-scope investigation was conducted in order to produce a short investigation report and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
The owner-pilot of a Piper PA-28-181 ‘Archer’ aircraft, registered VH-FEY, planned to conduct a flight from Jandakot to arrive in Carnarvon, Western Australia (WA) on 20 April 2023 to observe an eclipse of the sun at about 1130 local time, then return to Jandakot. This was a private operation under the visual flight rules.[1]
Previous flights
On the day before the eclipse, the pilot with one passenger on board, departed Jandakot Airport at 1416 and tracked to Geraldton Airport. The pilot landed at 1617 and parked in the general aviation area. Soon after arrival, the aircraft was attended by a refueller and Avgas tanker which replenished both fuel tanks (65 L added). The pilot and passenger then left the airport for their overnight accommodation.
At 0806 the next day, the pilot and 2 passengers arrived at the aircraft. The pilot advised that during the preflight inspection, water and a number of solid particles were visible in fuel samples drained from both tanks and the fuel strainer (gascolator). A number of fuel drains were carried out until the samples were free of water. The pilot estimated that the total amount of water drained from the aircraft fuel system was in the order of 500 ml.
Although the pilot was concerned about the amount of water that had been drained from the fuel system, they considered that the system was free of water and there should be no effect on the aircraft. The pilot conducted the usual engine run ups, did not identify any problems, and departed for Carnarvon at 0831.
The aircraft tracked direct towards Carnarvon and climbed to 6,500 ft. At about 90 NM (170 km) from Carnarvon, the pilot diverted to Shark Bay aerodrome, landing at 1020. The aircraft departed Shark Bay at 1031 and tracked to Carnarvon, landing at 1108. Engine operation during both sectors was reported as normal.
Both fuel tanks were replenished by a refueller and Avgas tanker (81 L added). The pilot and 2 passengers experienced the eclipse and obtained lunch near the airport. When the pilot carried out a fuel drain on return to the airport, there was no water found in the samples from the tanks but there was a small amount of water drained from the fuel strainer.
At 1239, the aircraft departed Carnarvon with the pilot and 2 passengers for Jandakot via Geraldton to drop off a passenger. The aircraft track was generally direct to Geraldton and the average cruise altitude was 7,500 ft. The pilot joined the circuit at 1452 and landed at 1455. Engine operation during the flight was reported as normal.
The occurrence flight
After a quick stop without refuelling, the pilot and 1 passenger boarded for the flight to Jandakot. The pilot recalled that as they advanced the throttle at the start of the take-off roll, there was an unusual ‘cough’ from the engine. Given it was a long runway and the engine reached full power, the pilot continued the take-off roll while monitoring the engine. It sounded normal and the temperatures and pressures were in the green operating ranges, so the pilot continued the take‑off.
The pilot departed Geraldton at 1513 to track to Jandakot via the generally direct route aligned with the coast, similar to the reciprocal track flown the day before. To take advantage of a forecast tailwind, the pilot climbed to cruise at 5,500 ft.
At 1559, the pilot began descent to about 4,000 ft to avoid restricted airspace near Lancelin. A further descent to 2,000 ft was initiated at 1612.
By 1632, the aircraft had reached 2,000 ft and was crossing the coast near Ledge Point (120 km north-north-west of Jandakot Airport) to track coastal over water. For the next 30 minutes the aircraft proceeded down the coast at about 2,000 ft.
The pilot advised the ATSB that they were just about to make a routine radio transmission about 10 km north of Fremantle for any traffic in the area, when engine power subsided to idle power over a couple of seconds then recovered to cruise power. (A descent, heading change, and groundspeed reduction were recorded at 1705.)
In response, the pilot selected the mixture control to full RICH and carburettor heat to ON. The electric fuel pump was already selected ON.
Engine power then subsided and recovered several times over a period of about 2 minutes. The pilot recalled there was no roughness or indications of a mechanical failure, and it seemed like the engine was responding to the throttle being moved (without any throttle movement).
The pilot tried different throttle settings for 20–30 seconds without any reported effect. The pilot recalled looking at the engine instruments and thinking of the need to look at the fuel quantity indicators but after the occurrence could not recall any indications.
At this stage, the aircraft had descended to about 1,200 ft and the pilot assessed that the aircraft would not be able to reach Jandakot Airport, which was about 18 km to the south-east. The pilot also decided against trying to reach the Swan River, which was about 4 km to the south‑south‑east and on the other side of a built-up area.
Now at about 1,000 ft, the pilot observed that they were not far from Leighton Beach. Considering that the surface wind was coming from the north-east, the pilot decided to turn into wind and land on the beach (Figure 1). During the turn however, the pilot noticed there were people all over the beach and that the plan was unworkable.
Instead, they decided to ditch the aircraft in the ocean as close to shore as possible to minimise their swimming distance. The pilot recalled trying to line up with the crest of the waves in accordance with generic ditching guidance.
At 500 ft, the pilot realised that no one had been advised of the emergency and made a MAYDAY call to Melbourne Centre. Shortly afterwards, the passenger asked if the door should be unlatched, and this was carried out.
By the time the turn had been completed, at about 300 ft, the engine had completely lost power and the propeller stopped turning shortly afterwards. The last data point was recorded at 1709.
Figure 1: Aircraft track from engine fluctuations to ditching

Source: Google Earth (Annotated by the ATSB)
The pilot recalled that as they were approaching the water, they tried to hold the nose up as far as possible to prevent the nosewheel contacting first and flipping the aircraft forward. When about 20–30 ft above the water the stall warning activated. To the pilot that meant the airspeed was probably about 50 kt or less but they were watching the water and did not look at the air speed indicator.
With the stall warning still going, a main wheel contacted the water and the aircraft skipped along the surface for a few seconds. Then the right wing dropped rapidly consistent with a stall and dug into the water, quickly stopping the aircraft. Water gushed up over the front of the aircraft and windscreen.
Figure 2: VH-FEY ditching touchdown

Source: Image extracted from Channel 9 News footage
The pilot and passenger were not injured and got out of the aircraft to stand on the wing. Some people swam out from shore to check if they were okay. When the aircraft began to sink after a couple of minutes, they swam to shore.
Context
Pilot information
The pilot began flight training in August 2020 and was issued with a private pilot licence (aeroplane) in November 2021 and a commercial pilot licence (aeroplane) (CPL(A)) in September 2022. To gain the flying experience required for a CPL(A), the pilot acquired VH-FEY in March 2022 and operated the aircraft on several long flights within WA. At the time of the occurrence, the pilot’s total flying experience was 360 hours.
The pilot held a Class 1 Medical certificate that was due to expire on 2 May 2023. This specified a requirement for the pilot to wear distance vision correction.
Meteorology
The ATSB obtained aviation meteorological information from the Bureau of Meteorology.
From the initial graphical area forecast (GAF) for southern Western Australia on the day of the occurrence (valid 1300 to 1900 local time), visibility was forecast to be greater than 10 km, except where it was 4,000 m due to isolated smoke south of Kalbarri. In a later issue of the GAF, the area of isolated smoke had contracted to potentially affect the flight south of Ledge Point, 65 NM (120 km) north of Jandakot.
The low-level grid point wind and temperature (GPWT) forecast issued at 0837 on 20 April 2023, indicated that at 1500, the following winds were expected at 5,000 ft and 7,000 ft respectively:
- Carnarvon to Geraldton from the north-east at 12 kt and 16 kt
- Geraldton to Jandakot from the north and north-west at 6 kt and 10 kt.
On 20 April 2023, at 1700 (5 minutes before the engine power loss), the automatic weather station at Swanbourne (5 km east of the engine power loss position) recorded the surface wind from the east at 5 to 8 kt. The recorded temperature was 23.8° and dewpoint 6.6°. When plotted on the Carburettor icing probability chart produced by CASA, the result was serious icing – descent power.
To ascertain the risk of water contamination due to rainfall, the ATSB accessed records of daily weather observations for Jandakot and Geraldton. At Jandakot, in the 4 weeks prior to the occurrence, a total of 67.6 mm of rain was recorded over 12 days. At Geraldton, there was no rain recorded on 19 and 20 April 2023.
Aircraft and systems
The Piper Aircraft Corporation manufactured the PA-28-181 aircraft in the United States in 1975. It was first registered in Australia in 1977.
The aircraft was powered by a Lycoming O-360-A4M piston engine and fixed pitch propeller.
A metal tank in each wing contained 24 US Gals (90 L) of usable fuel. Fuel was piped from the single outlet of each tank to a 3‑position fuel selector (OFF/LEFT/RIGHT) located on the left side‑panel (forward of the pilot’s seat), then to the fuel strainer, fuel pumps, and carburettor.
Normal operating procedures
The PA-28-181 Pilot’s Operating Handbook, issued in 1975 and last updated in 2019, advised that the fuel system should be drained daily prior to first flight and after refuelling to avoid accumulation of water or sediment. To drain the lines from the tanks, the tank selector is switched from each tank in turn, and the fuel strainer drain valve open.
In normal operation, the electric fuel pump was to be selected ON before take-off and deselected on reaching the desired altitude. Then, for approach and landing, the electric fuel pump was to be selected ON. It was also recommended that the electric fuel pump be selected ON while changing fuel tank selection. Otherwise, the electric fuel pump should normally be OFF so that any malfunction of the engine-driven fuel pump was immediately apparent.
The POH advised that, to keep best lateral trim for the flight, fuel should be used alternately from each tank at 1-hour intervals. It further recommended that one tank be used for 1 hour after take‑off, then the other tank used for 2 hours before returning to the first tank. At that point, the first tank will contain approximately 1.5 hrs of fuel and the second tank approximately 0.5 hr. There was a caution to not run tanks completely dry in flight.
To reduce fuel consumption in cruise, the POH recommended that the mixture should be leaned above 5,000 ft and at pilot discretion at lower altitudes when 75% or less power was being used. Leaning was carried out by pulling the mixture control back until the engine operation became rough then advancing it until smooth running was restored.
If an exhaust gas temperature gauge was fitted, as it was to VH-FEY, the Lycoming Operator’s Manual recommended leaning to 150°F on the rich side of peak EGT for maximum power cruise or to peak EGT for best economy cruise.
Operational practices
The pilot confirmed that their usual practice was to change fuel tank selection every hour and that this was prompted by the fuel gauge indicating 10 US Gals had been consumed. In practice, when starting with full tanks, the first and second tank changes would be when each tank indication was 20 US Gals in turn and the third and fourth at 10 US Gals.
Although the fuel gauges were calibrated a few months before the occurrence and were not reported as defective, the pilot did not rely on the gauges and considered them to only be a guide. To establish fuel on board, the pilot used a dipstick before or after flight. The pilot did not verify the accuracy of the fuel gauges by cross referencing the quantities with dipstick or refuelling figures.
The pilot advised that the mixture was left in RICH until top of climb then leaned to a setting that was slightly rich of peak EGT and was producing smooth engine operation. For descent, the pilot’s practice was to keep the mixture leaned and adjust as required to keep the engine smooth.
When the pilot operated the aircraft at higher altitudes and leaned the mixture as much as possible, the average fuel consumption rate calculated post-flight was consistently 30 L/hr. If operating at lower altitudes without leaning, the aircraft used more fuel.
The pilot reported that, based on the advice of an experienced instructor, their practice was to select the electric fuel pump ON for the entire flight to avoid any power interruptions if the engine‑driven pump failed.
Management of the flight
The pilot advised that a few days before a flight they usually used an EFB application to calculate estimates of flight times. Prior to departure from Jandakot, a flight plan was compiled manually as per their usual practice.
During the flight to Carnarvon via Geraldton and Shark Bay, the pilot did not consistently use the flight plan/navigation log or look at the map. The pilot advised that this was unnecessary because they were familiar with the route, having conducted the flight multiple times.
For the return flight to Jandakot, the pilot advised that they did not compile a flight plan or maintain a fuel log. After each of the previous flights from Carnarvon, the pilot had dipped the tanks and measured about 50–60 L remaining so expected that to be the outcome unless there was a strong headwind. As the flights from Jandakot to Carnarvon had consumed a total of 146 L, and there was no extensive ground running or stopover at Shark Bay on the return journey, the pilot expected that the fuel consumed on the return would be less than that figure. In that case, the fuel remaining on arrival at Jandakot was expected to be more than 34 L.
The pilot was monitoring progress of the flight using the EFB application.
Fuel quantity analysis
The ATSB obtained flight data that was transmitted at regular intervals from the on-board EFB application to the associated server via the mobile phone network. That data allowed for calculation of flight times[2] and in combination with refuelling records, the average[3] fuel consumption rate for the previous sectors.
On the first sector from Jandakot to Geraldton, the approximate fuel consumption rate was calculated as 32 L/hr (based on a flight time of 123 minutes and fuel add of 65 L). This flight was preceded by extended ground running so the consumption rate based on the flight time might have been marginally lower.
On the second flight from Geraldton to Carnarvon via Shark Bay, the average fuel consumption rate was calculated as 33 L/hr (based on a combined flight time of 147 minutes and fuel add of 81 L). This fuel consumption rate was applied to the return flight from Carnarvon because it was conducted in similar conditions.
The combined flight time from Carnarvon to Geraldton then to the engine power loss was 4 hrs and 15 minutes. At 33 L/hr, the estimated fuel burn was 140 L. Therefore, when the engine lost power, the estimated fuel on board was 40 L (Full fuel at Carnarvon: 180 L).
To establish the approximate distribution of fuel as the flight progressed from Carnarvon, the ATSB compiled a fuel log based on the pilot’s recollection of the fuel tank selections. From the flight data, the ATSB identified the time that the aircraft was at the pilot-nominated locations to identify an approximate time for each tank change. That data was inserted into the fuel log to retrospectively track the fuel burn and fuel on board as the flight progressed (Table 1).
Table 1: Retrospective fuel log for Carnarvon – Geraldton – Engine power loss
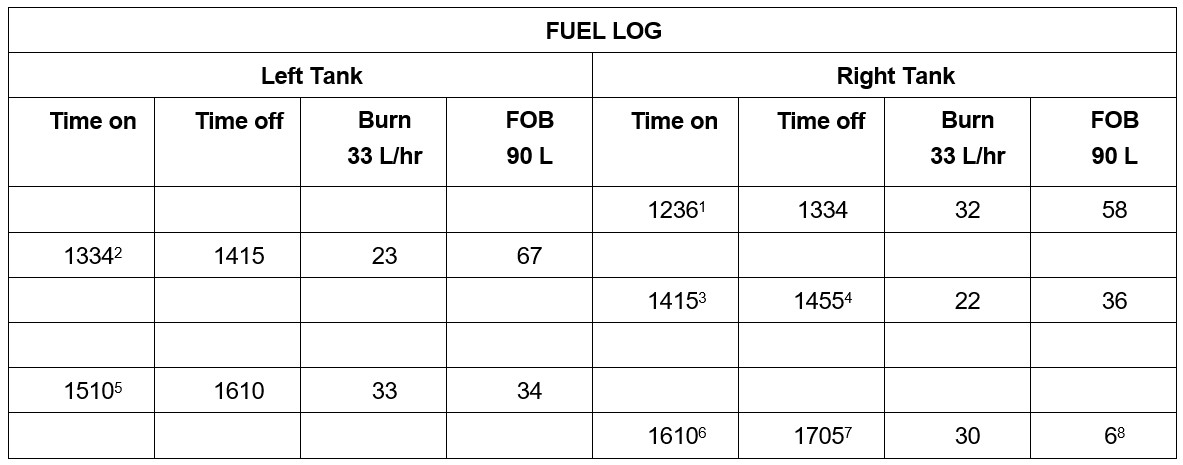
1 Take-off at Carnarvon on right tank
2 At about bottom end of Shark Bay switched to left tank
3 At about Kalbarri switched back to right tank
4 Landed at Geraldton on right tank
5 Start, taxi, and take-off at Geraldton on left tank
6 At about Cervantes switched to right tank
7 Engine power loss (right tank)
8 Estimated usable fuel remaining in right tank
The ATSB notes that the retrospective fuel log is based on an average fuel consumption rate and approximate timing of tank changes. As such, it is only indicative of the fuel on board in each tank at each change and at the time of the engine power loss. (If the left tank had been selected for 11 minutes more over the 2 periods of use, the left/right fuel balance would be 40/0 L.)
The pilot believed that the right fuel gauge was showing just under 10 US Gals remaining when it was selected before the occurrence (at 1610), but was not certain of this after the occurrence. Based on the retrospective fuel log and fuel calibration figures (Table 2), the right fuel gauge would have indicated between the 5 and 10 US Gals markings.
After the occurrence, the pilot estimated that when the engine loss occurred there was about 40 L (or 10 US Gals) in the left tank and 15–20 L in the right tank.
If the flight had continued without the engine power loss, operation for the additional flight time of approximately 15 minutes would have consumed a further 8 L (at 33 L/hr). In that case the total fuel on board after landing would have been about 32 L, which equated to an hour of flight time.
Fuel management guidance
CASA provided guidelines for aircraft fuel requirements in Advisory Circular AC 91-15 v1.1. The following information is adapted from the AC and selected for applicability to Day VFR operation of a light aircraft, such as a Piper PA-28-181.
Pilots were advised to operate in accordance with known or estimated fuel consumption data. This could be sourced from the aircraft/engine manufacturer or taken from recent historical consumption records.
The usable fuel required at the commencement of a Day VFR flight consisted of the taxi and trip fuel expected to be consumed, and final reserve fuel (30 minutes operation at 1,500 ft above aerodrome elevation) to be protected until landing. It was expected that additional fuel would be carried for contingencies.
According to the AC, the pilot must determine the amount of usable fuel on board before commencing a flight. Unless fuel quantity can be assured and verified (for example, full tanks), pilots should use the best available cross-check process. Those checks applicable to aircraft without ‘fuel consumed indicators’ were:
- after refuelling and having regard to any recorded post-flight fuel quantities, a check of the cockpit fuel quantity indications or visual readings against the refuelling uplift readings
- when a series of flights is undertaken by the same pilot and refuelling is not carried out at intermediate stops, checking of the cockpit fuel quantity indications against computed fuel on board.
The AC cautioned that fuel gauges, particularly on smaller aircraft, may be unreliable. Therefore, placing sole reliance on a fuel quantity gauge to assess fuel quantity and not cross-checking fuel quantity from a second source, increases the risk of being unable to determine actual fuel remaining should the fuel quantity indication system become faulty.
In-flight fuel management was described as continual validation of planning assumptions that influence fuel usage and required fuel reserves. As part of in-fight fuel management, the pilot must ensure that fuel quantity checks are carried out at regular intervals to:
- compare planned fuel consumption and actual fuel consumption
- determine the amount of usable fuel remaining
- determine whether the usable fuel remaining is sufficient
- determine the amount of usable fuel expected to be remaining when the aircraft lands at the destination aerodrome.
In-flight fuel quantity checks must include a reconciliation of the fuel remaining indicated from available aircraft fuel quantity indication systems and these should also be checked to confirm fuel balance and fuel tank quantity.
It was implied that the in-flight fuel checks would be recorded in some way such as flight plan or fuel log written entry, to allow a time-based reference to previous in-flight fuel checks for trend identification.
In all instances, it was highly recommended that the post-flight fuel quantity be determined and recorded.
Aircraft maintenance
The last periodic maintenance inspection was carried out in October 2022. At that time the aircraft total time in service was 7,421.3 hours.
Recent maintenance certified on 10 February 2023 included calibration of the fuel quantity indication system. The results were recorded in the aircraft logbook and on a placard above the fuel gauges (Table 2). For each increment marked on the gauges as US gallons, there is a corresponding figure for usable fuel in litres. In the brackets are the figures from the previous calibration carried out on 28 December 2018.
Table 2: Fuel calibration record VH-FEY
| Gauge (US Gals) | E | 5 | 10 | 15 | 20 | Full |
| Left (L) | 0 | 35 (35) | 60 (55) | 73 (60) | 83 (75) | 93 (86) |
| Right (L) | 0 | 26 (30) | 53 (50) | 69 (60) | 78 (70) | 89 (86) |
The ATSB notes that when each fuel gauge indicated 5 US Gals during the calibration process, the right tank contained 26 L and left tank contained 35 L. At the average fuel consumption rate of 33 L/hr (utilised in the retrospective fuel log), this equated to 47 minutes and 63 minutes flying time respectively. So, for the same fuel gauge indication of 5 US Gals, the right tank would yield 16 minutes less flying time than the left.
A review of the aircraft logbooks found 2 entries for removal and reinstallation of the right fuel tank in 1989 and 1993. These were the only records that could be associated with installation of a non‑conforming outlet fitting to the right fuel tank (see the section titled Wreckage recovery and examination).
The engine was last overhauled and installed in 1995 when the aircraft total time in service was 5,972.9 hours. As of the last periodic inspection, the engine had been operated for 1,449 hours and 28 years since overhaul.
In 2010, the engine was removed, bulk stripped, and reinstalled. Since then, and up to the last periodic inspection, the aircraft had been operated for 426 hours and 13 years.
Since the bulk strip in 2010, the carburettor had been repaired, and various components such as the engine driven fuel pump and magnetos had been replaced or overhauled.
The engine manufacturer issued a service instruction that specified time between overhaul (TBO) schedules. It included:
- All engine models were to be overhauled within 12 calendar years of the date they first entered service or of last overhaul.
- For the Lycoming O-360 type fitted to VH-FEY, the operating-hour TBO was 2,000 hours.
Although the engine had exceeded the calendar time TBO period, the registered operator (owner-pilot) of VH-FEY continued to operate the aircraft. This was permissible for private category operations when the engine was maintained in accordance with the Civil Aviation Safety Authority (CASA) ‘on-condition’ maintenance requirements. At the last annual inspection in October 2022, the maintenance organisation had fulfilled those requirements by completing a piston engine condition report that verified engine serviceability.
Wreckage recovery and examination
Prior to initiation of ATSB investigation
The aircraft was recovered from the ocean to the nearby beach by a salvage company. Disassembly of the aircraft for transport was supervised by a licensed aircraft maintenance engineer (LAME) with the support of the salvage company. They related the following details:
- both fuel tanks were full of fluid
- the fuel tank drains were not leaking
- there was a distinctive smell of Avgas when the right fuel cap was removed
- the contents of both fuel tanks were drained from each standard drain point into an empty semi-transparent intermediate bulk container (IBC)
- on completion of draining tank contents into the container there was a demarcation between the upper 25–35 mm of fluid and the remainder below
- the fluid in the upper layer was consistent with Avgas and the lower level was sea water.
Based on the estimated depth of the upper layer of fluid in the IBC, the quantity of Avgas drained from the fuel tanks was in the order of 30–42 L. It was not possible to differentiate between the amount of fuel drained from the left and right tanks. The container was subsequently used for recovery of other fluids by the salvage operator so no further information about fuel tank contents was available.
The wings and stabilator were removed and the aircraft was then transported along the beach to storage at the salvage operator’s yard.
ATSB examination
The ATSB initiated an investigation on 2 May 2023 and carried out examinations of the engine and aircraft fuel system at the storage facility. Forward of the firewall, this included:
- basic engine condition and mechanical continuity
- fuel strainer, engine driven fuel pump and carburettor
- air filter, airbox and carburettor heat mechanism
- magneto-engine timing and spark plugs
- exhaust and muffler
- oil filter
No engine defects were identified. The fuel strainer contained primarily sea water with a small amount of Avgas. The gauze filter was about 10–15% occluded by an unidentified white paste. The carburettor bowl was drained and was all sea water.
The carburettor, engine driven fuel pump, magnetos, and oil filter were removed for further examination. This was carried out and, other than saltwater residue, there were no defects or anomalies, and the components were probably serviceable at the time of the occurrence.
Examination of the aircraft fuel system was focussed on the right fuel tank assembly and fuel line to the selector. The right tank outlet fitting did not incorporate a ‘finger’ strainer, which was a non‑conformance with the fuel system data in the PA-28 parts catalogue. This outlet fitting was a different type to the conforming left tank outlet. No foreign object or evidence of contamination was found in the right tank.
Figure 3: VH-FEY Fuel tank outlet fittings - left with finger strainer and right without finger strainer

Source: ATSB
The ATSB considered the absence of a finger strainer in the only outlet from the right tank increased the risk of foreign object obstruction to fuel flow from the tank. This scenario would require an object of about the size of the internal diameter of the outlet fitting, which was stepped from 10 mm to 7 mm. Given there were no foreign objects found in the tank and no openings in the tank that would allow migration of any objects post-ditching, this scenario was considered highly unlikely. In addition, the aircraft manufacturer advised that there were no service difficulty reports or occurrences associated with the finger strainer (72091-000).
The fuel line from the right tank through the fuel selector to the fuel strainer was unobstructed. No defects were identified in the fuel selector, which was in the right tank position consistent with the pilot account.
The fuel sender unit was removed from the right tank and was in good condition. Given the immersion in sea water and removal of the wings it was not feasible to functionally test the fuel quantity indication system.
Although the wing flaps had been removed as part of the recovery operation, fuselage damage indicated the flaps were retracted during the ditching. This was consistent with the LAME’s recollection and the pilot’s account.
Geraldton Airport related
In response to the pilot account of significant water drained from the aircraft fuel system at Geraldton Airport on the morning of 20 April 2023, the ATSB sought information about possible sources of contamination at the airport.
The airport refueller advised that the usual quality checks were carried out to the tanker on the morning of 19 April 2023 and this was supported by their records. There was no report of water and the refueller advised that there was no history of this occurring.
The ATSB contacted the operator of an aircraft refuelled before VH-FEY who advised that no water had been detected from the post-refuelling fuel drains and normal operation was experienced on the subsequent flight.
Geraldton Airport is a security-controlled airport that required authorised access to airside areas. One of the CCTV cameras at the terminal was directed towards the aircraft parking area utilised by the pilot of VH-FEY.
The ATSB requested CCTV data for the period from aircraft arrival on the 19 April 2023 to departure on 20 April 2023. Due to the timing of the data recovery, data for 19 April 2023 was unavailable. The CCTV available from 0804 on 20 April 2023 showed the pilot and passengers arriving at the aircraft, some pre-flight activity, and the aircraft being taxied for take-off. Although the resolution was not high, there was evident movement that was consistent with the pilot making multiple fuel drains.
Emergency procedures – Engine power loss and forced landing
The pilot’s operating handbook (POH) for VH-FEY included emergency procedures for in-flight engine power loss and landing without engine power. There was no specific procedure or guidance in the POH for partial power loss or ditching. The text of the emergency procedures for engine power loss in flight is reproduced with revised formatting for readability in a report context:
ENGINE POWER LOSS IN FLIGHT
Fuel selector - switch to tank containing fuel
Electric fuel pump – ON
Mixture – RICH
Carburettor heat – ON
Engine gauges – check for indication of cause of power loss
Primer – check locked
If no fuel pressure indicated, check tank selector position to be sure it is on a tank containing fuel
If power is not restored prepare for power off landing.
Trim for 87 MPH IAS (76 KTS IAS)
When the pilot responded to the engine fluctuations, the first item was overlooked and the fuel selector remained on the right tank throughout the engine power loss sequence. The pilot explained that during initial flight training in a Cessna 172 they had memorised a ‘flow’ for practice forced landings that started at the centre of the aircraft (including fuel selector) then moved left. However, the pilot had not considered the implication of that method for the PA-28-181. So, in this case, the pilot had started in the middle but did not reach the left-mounted fuel selector because attention was diverted to preparing for the forced landing.
The text of the emergency procedures for a power off landing is reproduced below with revised formatting for readability in a report context:
POWER OFF LANDING
Locate suitable field
Establish spiral pattern 1000 ft. above field at downwind position for normal landing approach
When field can be easily reached slow to 76 MPH IAS (66 KTS IAS) for shortest landing
Touchdowns should normally be made at lowest possible airspeed with full flaps
When committed to landing:
Ignition – OFF
Master switch – OFF
Fuel selector – OFF
Mixture - idle cut-off
Seat belt and harness - tight
In the safety tips section of the POH, pilots were advised:
In an effort to avoid accidents, pilots should obtain and study the safety-related information made available in FAA publications such as regulations, advisory circulars, Aviation News, AIM, and safety aids.
The AIM reference in the POH safety tips was to the Aeronautical Information Manual published by the Federal Aviation Administration (FAA) in the United States. This addressed ditching procedures and is referenced in the next section.
The aircraft manufacturer advised the ATSB that they were not aware of any significant risks if pilots applied the Power Off Landing procedure in the POH to a ditching. Given the wide range of forced landing scenarios in different environments, the aircraft manufacturer considered that it was not feasible to define an emergency procedure for each one. In addition, the general information about emergency procedures in the POH indicated that emergency procedures were not intended to replace pilot training or provide information that is the same for all aircraft.
Under the certification standards[4] applicable to light aircraft such as the Piper PA-28-181, there was a requirement for information concerning normal, abnormal, emergency procedures, and other pertinent information necessary for safe operation, to be provided. In the case of single‑engine aircraft, this included the procedures, speeds, and configuration for a glide following engine failure and subsequent forced landing. There was no specific requirement for a ditching procedure.
The General Aviation Manufacturer’s Association (GAMA) issued specification No. 1 for pilot’s operating handbook released in February 1975 (the PA-28-181 POH was released in August 1975) and revised it in 1996. This document specified that procedures should be provided for forced landings under various conditions, including ‘ditching, for aircraft with extended overwater flight capability’.
Ditching guidance and training
FAA
In the emergency procedures chapter of the FAA AIM, there were various diagrams showing best heading in relation to primary swell, secondary swell, and wind. The manual specified a successful aircraft ditching was dependent on 3 primary factors in the following order of importance:
1. Sea conditions and wind
2. Type of aircraft
3. Skill and technique of the pilot
In addition to detailed guidance about evaluation of sea conditions and selection of relative heading, the manual advised that:
Touchdown should be at the lowest speed and rate of descent which permit safe handling and optimum nose up attitude on impact. Once first impact has been made, there is often little the pilot can do to control a landplane.
CASA
In the Australian context, CASA provided advice to operators of issues relevant to ditching an aeroplane through Advisory Circular 91-09 Ditching. This addressed preparation, selection of ditching area and direction of approach, and conduct of the actual ditching. The information provided was consistent with that in the FAA AIM.
If no type-specific guidance was available, the AC recommended that:
… the gear remain up, the flaps full, and speed at a minimum. In all cases, the desired configuration should be adopted at a safe height and the aeroplane trimmed to allow concentration on selection of the touchdown point.
For selection of touchdown point, the AC included the following points:
- if there is no manufacturer guidance, select an attitude for minimum sink rate
- wings level with the water surface on top of or on the back of a swell, not on the face of a swell
- no yaw if possible; straighten nose if crosswind exists, but avoid lowering a wing.
Other aircraft POH
For comparison, the ATSB reviewed the POHs for 2 light single-engine aircraft that included ditching procedures: Cessna 172 and Gippsland Aeronautics GA8. The POHs specified power (if available) to achieve 300 ft/min rate of descent, and approach direction relative to wind and sea state. Touchdown was at descent attitude, without flare and/or at slowest practical speed.
Pilot training
Pilot training in Australia was carried out in accordance with the Part 61 manual of standards (MOS). The competency standards for the ‘Manage abnormal situations – single-engine aeroplanes’ unit included elements and performance criteria for ‘Perform forced landing (simulated)’ in response to a simulated complete engine failure, and simulated partial engine failure.
For both scenarios, pilots were expected to identify the engine power loss condition, perform immediate or recall actions, and optimise aircraft performance. A landing area was to be selected, taking into account that a partially failed engine might fail completely, with an appropriate flight path. Pilots were to perform emergency procedures, as time permitted, and advise air traffic services or other agencies. If engine power was not restored, the pilot was to land the aircraft ensuring the safest outcome.
Ditching was not referenced in the elements and performance criteria, but it was listed as one of the underpinning knowledge requirements.
The pilot advised that information about ditching had been gained from flight training and reading books.
Other occurrences – Australia
Fuel starvation and forced landing
Fuel starvation and forced landing is a common occurrence type. The following occurrence was selected for the similarity of the engine power loss symptoms to the same type of aircraft.
ATSB AO-2017-094 Fuel starvation and forced landing involving Piper PA-28-181, VH-BDB, near Bankstown, New South Wales on 19 September 2017
The pilot believed that the aircraft fuel tanks were full and intended to conduct a 30–40 minute flight on the left tank. However, the aircraft had not been refuelled since the previous flight and contained about 25 L (35 minutes flying time) in the left tank and about 55 L (78 minutes flying time) in the right tank.
After about 30 minutes flight time, engine power started to fluctuate, and became progressively worse. The pilot conducted engine failure checks but did not change the fuel tank selection. Then the engine sustained a total loss of power and the pilot conducted a forced landing. There was no fuel found in the left tank.
Ditching
The ATSB carried out a search of its database for occurrences that were categorised as a ditching. The ATSB identified 78 occurrences in the previous 50 years, including 11 fatal accidents that resulted in 21 fatalities.[5]
Of the fatal accidents, 2 involved twin-engine aircraft (including Piper Chieftain, VH-MZK near Whyalla on 31 May 2000) and 2 involved loss of control of single-engine aircraft. The remaining 7 fatal accidents involved single-engine aircraft in controlled ditchings.
Apart from this occurrence involving VH-FEY, there were 5 other ditchings involving the PA-28 aircraft type, including 1 fatal ditching in a river near Bankstown in 1977. There were insufficient details to establish the method of ditching, however, the aircraft overturned on landing and sank immediately.
Extended time between overhauls (TBO)
ATSB AO-2020-060 Engine failure and collision with terrain involving S.E.D.E. Morane-Saulnier MS.893A, VH-UQI, on 6 November 2020.
During cruise, the engine began running rough then failed. The pilot conducted a forced landing in an open area but the aircraft impacted trees and caught fire. The pilot was seriously injured.
The ATSB found that the engine had sustained a catastrophic mechanical failure due to separation of a piston connecting rod. The engine had not been overhauled since 1997 and the aircraft had not been operated for an extended period, which was identified as a contributing factor.
Safety message: This investigation is a timely reminder for aircraft owners and maintainers to be cognisant of the manufacturer’s service information which ensures that the serviceability of engine and airframe systems are maintained to the highest standards. This includes strict monitoring of on-condition items, and that replacement of some parts may be warranted to ensure continued and safe operation. Consideration should also be given to preservation of the engine and its systems, should an aircraft be infrequently utilised.
Other occurrences – Outside Australia
The ATSB identified the following occurrences involving ditching of a Piper PA-28-181 aircraft:
NTSB ERA16LA109 Fuel exhaustion involving Piper PA-28-181, N29099, near Port Jefferson, New York on 20 February 2016
During a night flight with a flight instructor, student pilot, and 2 passengers on board, the engine lost power. The flight instructor diverted to land along a shoreline but, unable to see it in the darkness, decided to ditch close to where he judged the shoreline to be from house lights. The instructor held the aircraft off the water as long as possible to avoid a touchdown with excessive speed and the risk of nosing over. All of the occupants evacuated the aircraft and there were no reports of any impact-related injuries. Three of the occupants were rescued but one of the passengers did not survive.
BEA 2020-0243 Piper PA-28-181 Archer II, N5352F, off the coast of the isle of Guadeloupe on 4 July 2020
During a ferry flight the engine lost power. Although the in-flight power loss procedures was carried out, engine power could not be restored. The pilot approached without wing flaps and trimmed the aircraft slightly nose up to ditch parallel to the swell. The pilot and passenger were uninjured and were rescued by helicopter.
Safety analysis
Fuel management
Effective fuel management is a key factor in safe completion of a flight. Pilots are required to plan, uplift, then manage fuel, to ensure that an aircraft is landed with not less than the required reserve fuel on board.
For the return journey from Carnarvon to Jandakot, the pilot did not compile a flight or fuel plan. The pilot explained that the route was familiar and from experience estimated there would be about 50–60 L usable fuel (more than 1.5 hrs flying time) remaining at Jandakot. Also, the pilot expected that the fuel consumed on the return journey would be less than the total of 146 L consumed between Jandakot and Carnarvon. Based on full fuel of 180 L at Carnarvon, this equated to more than 34 L (about 1 hr flying time) remaining on arrival at Jandakot.
Although the pilot departed Carnarvon and subsequently Geraldton with sufficient fuel on board for the intended flight, the pilot did not keep a fuel log during the flight. Without progressive recording in a fuel log (or equivalent), calculation of the fuel remaining in each tank would have been based on recollection of the timing of tank changes and retrospectively calculating fuel consumed and fuel remaining in each tank.
The pilot’s practice was to change tanks using the fuel gauge indications as a prompt, which equated to 1-hour time intervals. These intervals were consistent with the POH and were generally effective at maintaining lateral balance and simplifying fuel management. However, the ATSB fuel calculations for the journey from Carnarvon show that some of the intervals were less than 1 hour and the requirement to land and take-off on the fullest tank could disrupt simple rule‑based fuel management.
In summary, EFB and GPS technology have enhanced flight planning and navigation capability, but pilots are still required to carry out in-flight fuel quantity checks at regular intervals. These should include a cross check of all available data, including fuel quantity indications, and be recorded. For aircraft with separate tank selections, it is advisable to monitor the fuel consumed, and fuel remaining, for each tank.
Engine power loss
About 15 minutes before arriving at Jandakot, engine power subsided to low power then returned to normal power. This type of fluctuation continued for about 2 minutes with insufficient power to maintain level flight. Shortly before the ditching the engine stopped completely.
The ATSB considered all of the potential reasons for the engine power loss, which can be broadly categorised as:
- engine and associated systems defect
- carburettor ice
- fuel contamination
- fuel starvation.
Although the aircraft had sustained impact damage and been submerged, the engine and associated systems were not significantly affected. The ATSB confirmed mechanical continuity of the engine and found that key engine components such as carburettor, magnetos, engine-driven fuel pump and electric fuel pump were not defective.
According to the CASA carburettor icing probability chart, the conditions were conducive to carburettor ice at descent power. Given the engine was at cruise power, carburettor icing produces a continuous engine power loss until cleared, and the pilot applied carburettor heat early in the sequence, the symptoms are not consistent with carburettor icing.
The pilot identified an unusual amount of water in the fuel during the pre-flight inspection at Geraldton on the morning of the occurrence. There was no evidence that the fuel tanker had introduced the water during refuelling the previous afternoon and there was no rain recorded at Geraldton while the aircraft was parked overnight. The ATSB was unable to resolve this anomaly.
Given the pilot had continued the fuel drains until water was no longer present in the samples and the pilot had operated for a further 6.7 hours, including another refuelling, it is unlikely that a significant amount of water was present in the tanks when the engine power loss occurred.
Submersion of the aircraft and infiltration of the fuel system by sea water prevented an accurate assessment of fuel quantity in each tank, although observations of the fluid drained from the tanks indicated there had been sufficient fuel on board for completion of the flight.
At the time of the engine power loss, the right tank was selected and the ATSB estimated that the fuel remaining in the right tank was 6 L. Due to imprecise information this was indicative and does not preclude a lower amount. In addition, there were no engine or aircraft fuel system defects, and the symptoms were consistent with other occurrences where fuel starvation was verified. Although water contamination could not be ruled out, the ATSB found that the engine power loss was probably because of a lack of usable fuel in the selected (right) tank.
This condition, categorised as fuel starvation, could have been rectified by changing the fuel tank selector from the right tank to the left tank that contained sufficient fuel to continue the flight to Jandakot.
Emergency procedures
If fuel starvation is recognised, the pilot can remedy the situation without recourse to emergency procedures. Otherwise, the pilot is required to apply the emergency procedures from memory and/or with reference to the written procedures.
The pilot responded to the engine power anomalies by selecting the mixture to RICH and carburettor heat to ON. The electric fuel pump was already selected ON because of the pilot’s method of usage and that selection was not changed. Although continuous use of the electric fuel pump was contrary to the POH, this was not a factor in the occurrence.
Those immediate actions, conducted from memory, were in accordance with the engine power loss in flight procedure in the POH. However, the pilot did not action the first item, which was:
Fuel selector - switch to tank containing fuel
The pilot attributed this to the ‘flow’ or sequence that had been learned for a different aircraft type and not adapted to the configuration of the PA-28-181, combined with limited time to complete the sequence. For pilots who fly different aircraft types, use of a checklist mnemonic that can safely be applied across those types will reduce vulnerability to negative transfer of type-specific flows or sequences. Ready access to the written procedure is an option but is often not practicable in a single-pilot time-critical context.
Compared to a complete engine power loss, an intermittent or partial engine power loss is an ambiguous condition that does not conform to standard training scenarios and can disrupt pilot implementation of emergency procedures. Unless there is an obvious solution, pilots should prepare for an imminent complete engine power loss and follow the applicable procedures to optimise recovery of engine power.
Engine power was not restored, and the pilot was required to conduct a forced landing. The pilot made a sound decision to carry out a ditching adjacent to the beach rather than landing on the populated beach with the high risk of injury.
By applying the POH guidance for a power off landing and generic ditching guidance, the pilot conducted a controlled ditching with minimal damage and no injuries. This outcome was assisted by favourable sea conditions.
The ATSB noted that the POH did not contain any procedures for ditching and considered whether this was a factor that increased risk.
For light aircraft such as the Piper PA-28-181, there was no requirement for the aircraft manufacturer to provide a ditching procedure and they advised that they were not aware of any significant risks if the Power Off Landing procedure was applied to a ditching. By contrast, some aircraft manufacturers did include ditching procedures.
As referenced in the PA-28-181 POH, the Aeronautical Information Manual published by the Federal Aviation Administration (FAA) addressed ditching procedures in some detail. And in the Australian context, CASA provided guidance in Advisory Circular AC 91-09 Ditching.
Training for ditching has obvious limitations and it was not referenced in the elements and performance criteria of the ‘Perform forced landing (simulated)’ competency standard. As one of the underpinning knowledge requirements, it is expected that on completion of pre-licence training, pilots would have an awareness of aircraft-specific and/or generic ditching procedures.
As indicated by the other occurrence information, the impact forces associated with a ditching are generally survivable, provided the pilot does not lose control of the aircraft before entering the water. As demonstrated in this occurrence, it is assumed that where there are no aircraft-specific ditching procedures, pilots conducting a ditching will apply power off landing procedures and generic training/guidance. Although aircraft-specific ditching procedures are an advantage there is no evidence that the absence of such procedures for the Piper PA-28 type significantly increases the risk of ditching.
In summary, if pilots might be required to ditch in case of an emergency, they should be familiar with the applicable procedures in the POH, as available, and/or generic guidance produced by national aviation authorities.
Extended TBO
The ATSB noted that since the last overhaul, the engine had been in service for 28 years, which was more than double the recommended time before overhaul of 12 years. This was mitigated to some extent by a bulk strip 13 years before the occurrence and various component changes.
Given there were no engine defects, and the required maintenance was carried out, the extended TBO was not identified as a factor in this occurrence.
Nevertheless, the ATSB recently found that in November 2020, a Lycoming 0-360 engine sustained a catastrophic mechanical failure due to separation of a piston connecting rod. The engine had not been overhauled since 1997 and the aircraft had not been operated for an extended period, which was identified as a contributing factor.
Although continued private operation is conditionally permitted for aeroplane engines that have exceeded the recommended calendar time before overhaul, operators should consider the length of the extension, modification status, and associated risk of failure.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the fuel starvation and ditching involving Piper PA-28-181, registered VH-FEY, on 20 April 2023.
Contributing factors
- The pilot departed Carnarvon with sufficient fuel for the intended flight to Jandakot via Geraldton but did not carry out regular fuel quantity checks in accordance with regulatory guidance or keep a written log of the fuel consumed from each tank during the flight.
- During cruise at 1,900 ft, engine power subsided to low power then returned to normal power. This occurred a number of times, probably because of a lack of usable fuel in the selected (right) tank.
- The pilot responded to the engine power anomalies by carrying out some of the emergency procedures but did not select the other (left) tank that contained usable fuel. Consequently, engine power was not restored, and the pilot carried out a forced landing/ditching into the ocean near a beach.
Other findings
- Prior to the first departure from Geraldton on the day of the occurrence, the pilot drained a significant amount of water from both fuel tanks (that had been refuelled to full the night before) and from the fuel strainer. The aircraft was subsequently operated for over 6.5 hrs with a refuelling at Carnarvon without any symptoms of fuel contamination and it is unlikely that there was a significant amount of water remaining in the fuel.
- The engine had been in service for 28 years, which was more than double the recommended time before overhaul (TBO) of 12 years. Given there were no engine defects, and the required maintenance was carried out, the extended TBO was not identified as a factor in the occurrence.
Sources and submissions
Sources of information
The sources of information during the investigation included the:
- owner-pilot of the accident flight
- maintenance organisation for VH-FEY
- aircraft manufacturer
- video footage of the accident flight and other photographs and videos taken on the day of the accident
- recorded data transmitted from the EFB application on the aircraft.
References
Advisory Circular AC 91-09 v1.0 Ditching, Civil Aviation Safety Authority, November 2021.
Advisory Circular AC 91-15 v1.1 Guidelines for aircraft fuel requirements, Civil Aviation Safety Authority, September 2021.
Pilot’s Operating Handbook Piper Cherokee Archer II PA-28-181 REPORT VB-760 Issued 15 August 1975, Revised 1 April 2019.
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- owner-pilot of the accident flight
- maintenance organisation for VH-FEY
- aircraft manufacturer
- Civil Aviation Safety Authority
A submission was received from the:
- owner-pilot of the accident flight
The submission was reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2023 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this publication is licensed under a Creative Commons Attribution 3.0 Australia licence. Creative Commons Attribution 3.0 Australia Licence is a standard form licence agreement that allows you to copy, distribute, transmit and adapt this publication provided that you attribute the work. The ATSB’s preference is that you attribute this publication (and any material sourced from it) using the following wording: Source: Australian Transport Safety Bureau Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Visual flight rules (VFR): a set of regulations that permit a pilot to operate an aircraft only in weather conditions generally clear enough to allow the pilot to see where the aircraft is going.
[2] The flight times referenced in this section are derived from the take-off and landing times recorded in the flight data. If flight times were derived from other data such as engine start to engine stop, the calculated fuel consumption rate may be different, but the results would be the same.
[3] This is sometimes referred to as block fuel consumption rate and does not identify climb or other phases of flight for calculations at different rates. In the context of the operation type and imprecision of the available data, this was considered suitable for purposes of the investigation.
[4] The Piper PA-28 type was originally certified to CAR 3 in 1956. When the PA-28-181 was certified in 1975, the CAR 3 requirements were supplemented by certain provisions of Part 23 of the Federal Aviation Regulations. So, the current version of FAR 23 was referenced.
[5] The ATSB notes that the database search was for indicative purposes only and data quality may vary over the search period.
Occurrence summary
| Investigation number | AO-2023-021 |
|---|---|
| Occurrence date | 20/04/2023 |
| Location | 15 km north-west of Jandakot Airport |
| State | Western Australia |
| Report release date | 28/11/2023 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Fuel starvation |
| Occurrence class | Accident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Piper Aircraft Corp |
|---|---|
| Model | PA-28-181 |
| Registration | VH-FEY |
| Serial number | 28-7690006 |
| Sector | Piston |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Carnarvon Aerodrome, Western Australia |
| Destination | Jandakot Aerodrome, Western Australia |
| Damage | Substantial |
Acroduster in-flight break-up highlights importance of additional inspections

Key points
- Amateur-built Acroduster aircraft broke up in-flight when the left and right eye bolts and left roll brace connecting its upper wing failed due to fatigue cracking;
- A safety advisory has been issued by the ATSB, as well as the aircraft design owner, the US Federal Aviation Administration, and the Experimental Aircraft Association;
- ATSB urges operators and maintainers of amateur-built aircraft to consider additional detailed inspections of parts of aircraft that are critical to safe flight.
The in-flight break-up of an amateur (kit) built Acroduster aircraft reinforces to operators and maintainers of these aircraft the importance of conducting additional detailed inspections of areas that are critical for flight.
On 18 August 2021, an amateur-built Stolp Acroduster II SA-750 biplane broke-up during a flight from Caboolture airfield, north of Brisbane. The pilot, who was the sole occupant, was fatally injured.
As noted in its preliminary report, the Australian Transport Safety Bureau’s technical examination determined two eye bolts, and the left roll brace, used to secure the aircraft’s upper wings, had failed due to fatigue cracking, triggering the break-up sequence.
Coinciding with the release of its preliminary report, the ATSB issued a Safety Advisory Notice (SAN) to owners and maintainers of Stolp Acroduster SA-700-750 aircraft, notifying them of the fatigue cracking issue.
“In this accident, the fatigue cracks formed in an area of the eye bolts that were obscured by the securing nuts and threads of the eye bolts,” ATSB Director Transport Safety Kerri Hughes said.
“This meant the cracks would not have likely been readily identifiable during standard maintenance inspections, without disassembling the attachment points.
“Owners and maintainers of experimental amateur-built aircraft should consider conducting additional detailed inspections that exceed the minimum standards, in areas of the aircraft that are critical to the safety of flight.”
The initial finding of fatigue cracking on the aircraft’s eye bolts was immediately shared, in August 2021, with the Civil Aviation Safety Authority, as well as the National Transportation Safety Board and Federal Aviation Administration in the United States (as the aircraft’s state of design), and the US-based Experimental Aircraft Association.
The aircraft design owner, Aircraft Spruce, was also notified.
The Experimental Aircraft Association subsequently released a notice on its website informing members of the accident, and a link to the ATSB’s preliminary report and SAN.
The Federal Aviation Administration issued a notice to more than 280,000 web subscribers informing them of the wing attachment point fatigue cracks, and also provided a link to the ATSB’s material.
Additionally, Aircraft Spruce issued a safety advisory notice to every purchaser of Starduster and Acroduster design plans since 2003.
“The ATSB welcomes these safety actions by authorities and the manufacturer in response to this accident,” Ms Hughes concluded.
Read the final report: In-flight break-up, Stolp Acroduster II SA-750, VH-YEL, 16 km north-east of Caboolture airfield, Queensland, on 18 August 2021
In-flight fire and cabin smoke involving Saab 340A, VH-KDK, 114 km east-north-east of Cobar, New South Wales, on 23 April 2023
Final report
Report release date: 20/11/2024
Executive summary
What happened
On the morning of 23 April 2023, a Saab 340A, registered VH-KDK and owned by Pel-Air Aviation, was being operated by Regional Express Airlines (Rex) for a non-revenue flight from Wagga Wagga, New South Wales, to Charleville, Queensland. While in cruise at 22,000 ft and passing to the east of Cobar, New South Wales, the flight crew received a cargo smoke indication on the central warning panel. As a precaution, the crew fitted their oxygen masks and smoke goggles. Shortly after, the cockpit filled with smoke.
The captain commenced a diversion to Cobar while the first officer made a PAN-PAN[1] call to Melbourne Centre. Thick smoke then filled the flight deck preventing the crew from effectively seeing external visual references or the aircraft’s flight instruments. While completing the emergency checklists, the crew received further warnings for avionics smoke, followed by a cabin depressurisation, and then a right engine fire detection fail indication. The crew landed at Cobar and elected to stop on the runway and evacuate the aircraft.
Shortly after landing, Fire and Rescue New South Wales personnel arrived from the Cobar station and located a heat source at the air cycle machine and in the associated wiring. After gaining access to the cabin underfloor area, the source of the heat was doused with water. An internal inspection of the aircraft found fire damage in the area around the right recirculating fan. The aircraft was substantially damaged, and the crew were not injured.
What the ATSB found
The ATSB found that a likely failure of the right recirculating fan electronic box sub-assembly resulted in an in-flight fire under the cabin floor. The fire filled the cabin with smoke, which then entered the flight deck due to a smoke barrier curtain not being fitted in place and the flight deck door being open.
When the crew fitted their oxygen masks, it was found that the first officer’s mask microphone was not working correctly, which delayed emergency checklists being actioned. The fire also caused substantial structural damage and led to a breach of the fuselage, resulting in a depressurisation of the aircraft.
It was also found that the Rex flight crew had not been trained or had knowledge of the differences in the cargo‑configured Saab 340 aircraft, leading to them having no familiarity with specific systems fitted. This prevented them from completing some of the required steps in the emergency checklists.
The flight crew did not receive training on the cargo‑configured aircraft differences prior to conducting freight operations. Further, the operator’s flight crew operating manuals did not reflect the differences in the cargo‑configured aircraft interior checklists, which may have alerted the flight crew to these differences during pre-flight preparation. Additionally, the manufacturer did not have any specific pre-flight check for correct fitment of the smoke barrier curtain for cargo‑configured aircraft preparation.
What has been done as a result
On 13 May 2023, Rex issued an Operations Notice to all pilots, highlighting the guidance on the cross-valve handle as outlined in the Saab Aircraft Operating Manual (AOM). Furthermore, this guidance has been incorporated into the Rex Flight Crew Operating Manual (FCOM).
On 13 November 2024, Rex amended the internal inspection checklist that is contained in their Saab 340 FCOM. The amendment now requires flight crews verify the position of the cross‑valve handle during the pre-flight checks.
Rex have also updated the training information delivered in their ground school to include the cross-valve system for the cargo‑configured Saab 340 aircraft into the training syllabus.
Rex indicated they are implementing a fleetwide inspection of the recirculating fan assemblies at the next aircraft heavy maintenance cycle, with a focus on the electronic sub-assembly module.
Pel-Air have included a revision to their flight crew operating manual with a caution that the smoke barrier curtain must be installed whenever combustible material is carried in the cargo compartment. Due to contract completion, Pel-Air have ceased conducting freight operations using the Saab 340 aircraft and have since sold the aircraft.
Saab has revised their preparatory and walk-around pre-flight checklists to include the fitting of the smoke barrier curtain when carrying cargo in the cargo‑configured aircraft.
Safety message
It is essential for operators to ensure that flight crew are conversant with differences in aircraft configurations when required to conduct operations on aircraft they may be unfamiliar with. It is important that information is readily available and accessible and be delivered in a manner to inform flight crews on the operational requirements of the aircraft.
Operator flight crew operating manuals need to be relevant for the aircraft configuration being utilised. Further, manufacturer checklists for pre-flight inspections are required to cover the modifications fitted, so that this is available to operators to enable them to write the appropriate documentation for their flight crews.
The occurrence
History of the flight
On the morning of 23 April 2023, a Pel-Air Aviation cargo‑configured Saab 340A, registered VH‑KDK and operated by Regional Express Airlines (Rex), was being prepared for the first stage of a non-revenue freight flight from Wagga Wagga, New South Wales, to Charleville, Queensland. The purpose of the flight was to pre‑position a Rex Saab 340 engine to Cairns, Queensland, utilising a Rex crew, consisting of a captain and first officer (FO), and operating under the Part 91 flight rules.
The crew had flown the aircraft from Cairns the previous day, and were tasked to fly the return leg, including a refuelling stop at Charleville. The flight crew arrived at the aircraft at about 0830 local time and conducted their pre-flight checks. The captain performed the interior checks while the exterior walk around checks were conducted by the FO. The aircraft departed Wagga Wagga at about 0949, tracking for Charleville, and cruising at FL 220.[1] The captain was the pilot flying (PF), and the FO was pilot monitoring (PM).[2]
In-flight fire and diversion
At about 1052, the crew was alerted by a cargo smoke detection warning[3] on the central warning panel. They began to manage the warning by identifying and cancelling the indication. The crew then donned their oxygen masks and smoke goggles. However, once fitted, the crew had difficulty communicating due to the FO’s mask microphone not functioning correctly and being very faint. A review of the cockpit voice recorder (CVR) recording showed it took another 57 seconds for the crew to establish effective communications with each other before they could commence the emergency checks.
At 1055 the crew received a right (engine) fire detection fail caution light, followed shortly after by an air conditioner caution light. This was due to the detection of a right distribution duct over temperature which automatically closed the right engine low pressure bleed valve. The crew initially detected no smoke or fumes, however within about 60 seconds, thick black smoke began filling the cockpit.
During the process of establishing the nature of the warnings, the flight crew discussed which airport would best suit their needs for the emergency, and opted to divert to Cobar, New South Wales (Figure 1). The captain had flown to this airport on several previous occasions and was familiar with it, and from their position, they could conduct a direct approach with minimal manoeuvring.
Figure 1: VH-KDK flight overview
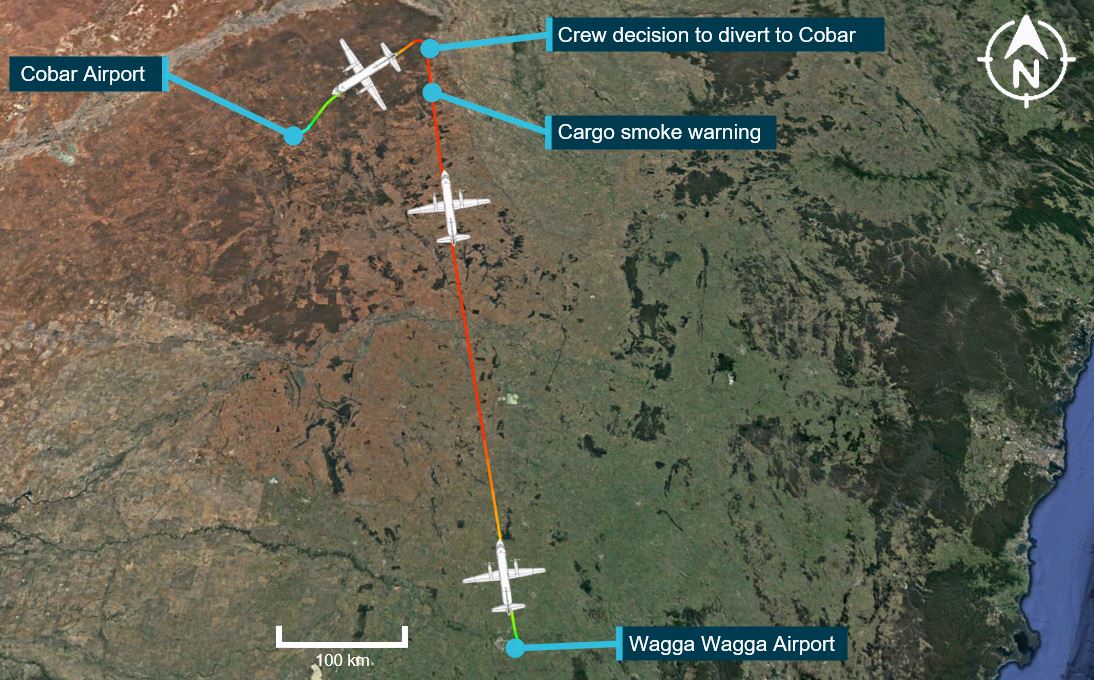
Source: Google Earth and Flightradar24, annotated by the ATSB
At 1056, the FO gave a PAN PAN[4] radio call and advised air traffic control (ATC) that they were diverting to Cobar. ATC arranged for emergency services to meet the aircraft upon arrival into Cobar. Due to the radio coverage in the Cobar area, ATC utilised an overflying aircraft to relay communications as the diversion progressed.
While descending through FL 160, the crew received a cabin pressure failure warning, indicating that the aircraft had lost pressurisation. This occurred 4 minutes after the initial warning of the cabin smoke. The cabin depressurisation led to the crew increasing their rate of descent to get below FL 100.
At approximately 1058, they commenced the ‘cargo compartment smoke’ emergency checklist. The CVR indicated the crew completed the first checklist item, which called for the left bleed valve to be closed. The checklist then called for closing the cross-valve handle, however the crew was unable to locate it, with the CVR recording indicating the crew tried to find it for 61 seconds before resuming the checklist flow without actioning the cross-valve handle closure. The crew completed the cargo compartment smoke checklist as visibility on the flight deck reduced to less than 10 cm. The captain recalled sliding their seat forward to enable them to see the instrument panel through the thick smoke.
Five minutes after the PAN PAN call, the crew commenced the checklist for ‘avionic or electrical smoke or fire’.[5] The crew then conducted the ‘smoke removal’ checklist to clear the smoke from the flight deck.
One requirement of the smoke removal checklist called for aircraft speed reduction to below 160 kt, and to open a crew hatch to aid in smoke removal. Due to the unknown severity of the on‑board fire, the crew decided to maintain their speed and not complete all the checklist items as required, enabling them to expedite their landing.
As the crew continued their approach, the volume of smoke in the flight deck began to dissipate. This allowed them to navigate using external visual cues and conduct a visual approach for the landing. Because of the unknown source of the fire, upon arrival in Cobar, the crew elected to stop the aircraft on the runway and evacuate the aircraft.
As part of the emergency evacuation procedure, the crew activated the fire extinguisher system[6] on both engines after shutting down, and then exited the aircraft. The incident had taken 22 minutes from the first smoke warning to landing.
After evacuation, the crew noted smoke to be coming from the vicinity of the right air cycle machine at the right wing root. Shortly after landing, Fire and Rescue New South Wales personnel arrived from the Cobar station and assessed the aircraft. After gaining access to the cabin underfloor area, an electrical harness was initially found melted and smoking. Consequently, the area was doused with water.
Further inspection of the aircraft found significant fire damage concentrated in the area around the right recirculating fan. The right recirculating fan was also significantly fire damaged. An assessment of the right engine found no evidence of a fire. The aircraft underfloor structure was substantially damaged, and the crew were not injured.
Context
Aircraft information
The Saab 340A[7] is a twin-engine turboprop aircraft designed and initially produced by Saab and Fairchild Aircraft. It is designed to seat 30–36 passengers in standard configuration and is powered by 2 General Electric CT7-5A2 turboprop engines.
VH-KDK was manufactured in Sweden in 1984 and first registered in Australia in February 1985. It was operated in passenger configuration by Regional Express Airlines (Rex), before being modified to cargo configuration in 2009. VH-KDK was then owned and operated by Pel‑Air Aviation.[8]
At the time of the accident,[9] VH-KDK had accrued a total time in service of 48,130.6 hours and 60,046 landings and had flown 13.5 hours since the last maintenance.
Flight crew information
Captain
The captain held an air transport pilot licence (ATPL) (Aeroplane), and a valid Class 1 aviation medical certificate. They reported a total flying time of 7,579 hours with about 5,070 of those being on the Saab 340. They had flown for the operator for about 10 years, and previously had flown for another regional airline and had operated into Cobar airport on numerous occasions.
The captain had previously flown the Saab 340A in a passenger configuration but had not flown either the Saab 340A or B variant in a cargo configuration.
First officer
The first officer (FO) held an ATPL (Aeroplane), and a valid Class 1 aviation medical certificate with a restriction for vision correction. They had reported a total flying time of about 18,297 hours, having flown about 1,480.9 in the Saab 340B. The FO had not previously flown any Saab 340 variants in a cargo configuration.
Meteorological conditions
Graphical area forecasts provided by the Bureau of Meteorology (BoM) stated that generally good weather conditions, with little cloud, and visibility greater than 10 km existed during the flight. The terminal area forecast for Cobar indicated light winds from the east at about 10 kt with the flight crew reporting CAVOK[10] conditions existing for the time of the diversion.
Cargo configuration
VH-KDK cargo conversion
The cargo conversion modification was carried out in accordance with Saab service bulletin (SB) 340-25-280. As an overview, the SB involved removal of the passenger fit‑out and replacing it with an interior cargo liner, blanked over windows, additional cargo barrier nets, and a floor roller system (Figure 2). In conjunction with this SB, other SBs were incorporated on the cargo version, which modified the air conditioning system. This was done by removing the left recirculating fan and introducing a cross-valve handle.
A removable smoke barrier curtain was added at the forward section of the cargo compartment. The fire extinguishing system for the passenger cargo area at the rear of the cabin (zones C1 and C2) was also removed, and additional smoke detectors were added to the cabin.
Figure 2: Cargo configuration modification
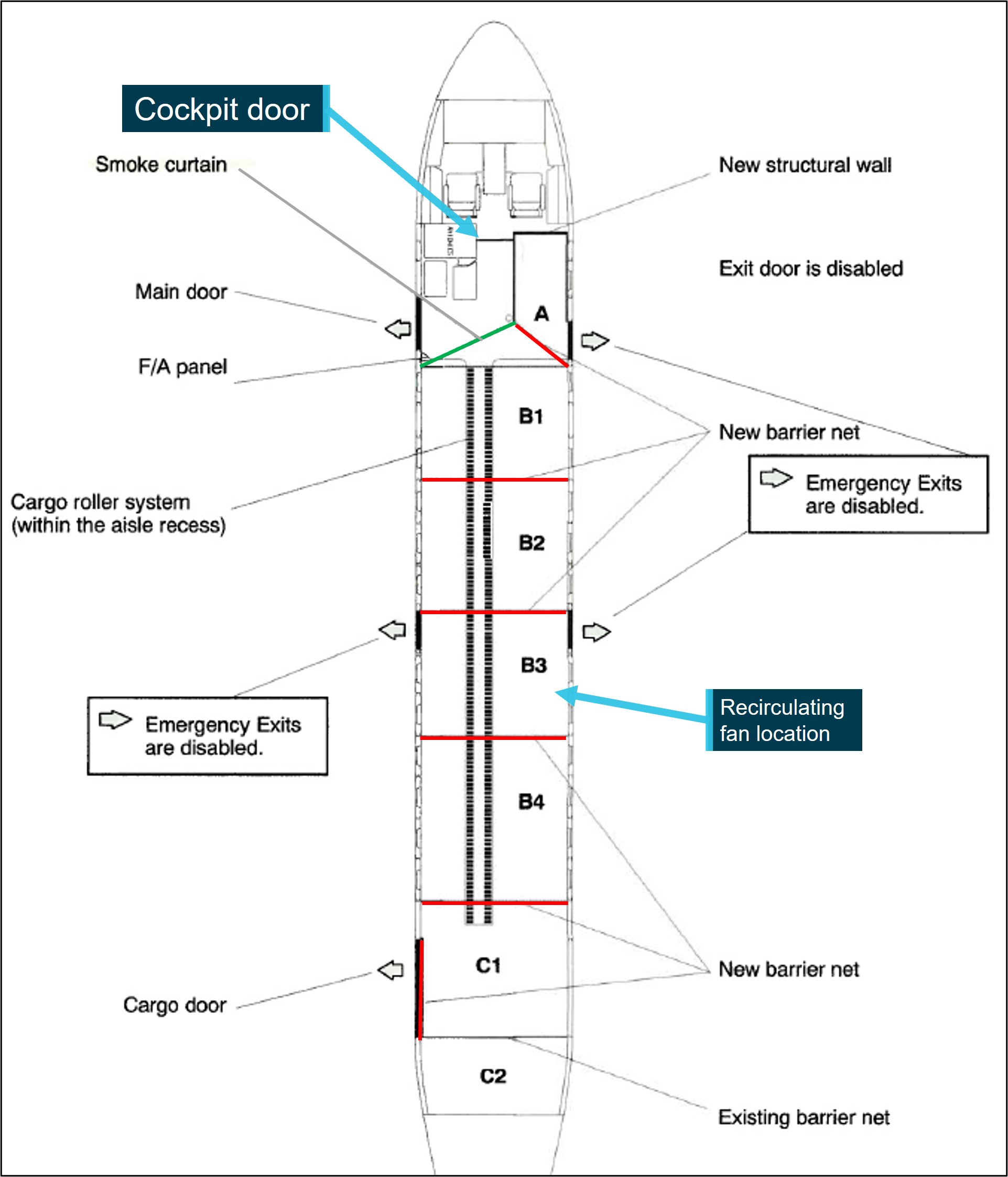
Source: Saab, annotated by the ATSB
Smoke curtain
A removable smoke barrier curtain was designed to be installed between compartment A and the front-left fuselage (Figure 2). The purpose of the curtain was to provide containment of smoke and fire within the cargo compartment in the event of an on-board fire and prevent smoke ingress to the flight deck (Figure 3). The aircraft carried a placard at the top of the entrance stairs which stated:
Smoke barrier must be installed for all cargo operation flights.
The smoke barrier was constructed of a fibreglass impregnated vinyl which was secured in place by a Velcro perimeter and metal press studs. The aircraft owner stated that the standard procedure was that it would be left attached by the left side attachment points and secured in place by the freight handlers after loading of cargo. It was then to be checked by the FO prior to flight.
During interview, the flight crew stated that they were not aware of the use of the smoke barrier, and that it had been located after the incident in compartment A of the cargo area, and that it was not in place on the left of the cabin. The ATSB did not determine why the engineers who loaded the engine into VH-KDK had not secured the smoke curtain.
Figure 3: Smoke barrier curtain location in exemplar aircraft
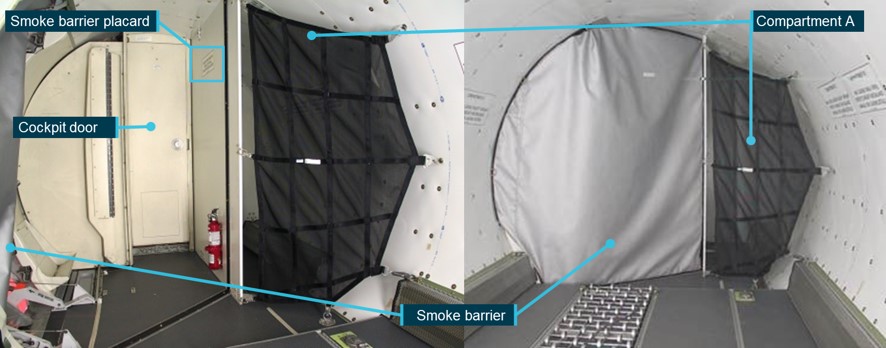
Source: Saab, annotated by the ATSB
Air conditioning system
In passenger configuration, the Saab 340 air conditioning system is comprised of a left and right air conditioning pack (ACP) which is supplied by bleed air from its respective engine. Each ACP is mounted externally under a fairing on the lower fuselage near the rear of each wing. The system has 2 recirculating fans under the adjacent cabin floor, ducting for the cabin and flight deck conditioned air supply and return, temperature sensors and controls, and cabin and flight deck air outlets.
The left and right ACPs supply conditioned air to the cabin, and a portion of the right ACP conditioned air is supplied to the flight deck. The left recirculating fan returns the air to the left ACP from the aircraft cabin, while the right fan extracted air from the flight deck. The avionics fan draws air for cooling the avionics from the cabin conditioned air supply. The air is then expelled under floor.
As part of the modification from passenger to cargo configuration, the left recirculating fan and ducting were removed. This resulted in limited extraction and recirculation of any contaminated air from the cabin interior, while the right recirculating fan would extract and recirculate air solely from the flight deck.
Cross-valve handle
In the cargo configuration, a cross-valve and handle were added to the air conditioning system ducting between the left and right ACP (Figure 4), with the manual operating handle being located at floor level, next to the FO seat. Closing of the left bleed valve and cross-valve in accordance with the emergency checklist would isolate the supply of air to the cabin in the event of cargo smoke or fire, and the right ACP would supply only to the flight deck. As part of the emergency checklist for ‘cargo compartment smoke’, the left ACP would also be isolated from supplying the cabin.
Figure 4: Schematic of modified air conditioning system
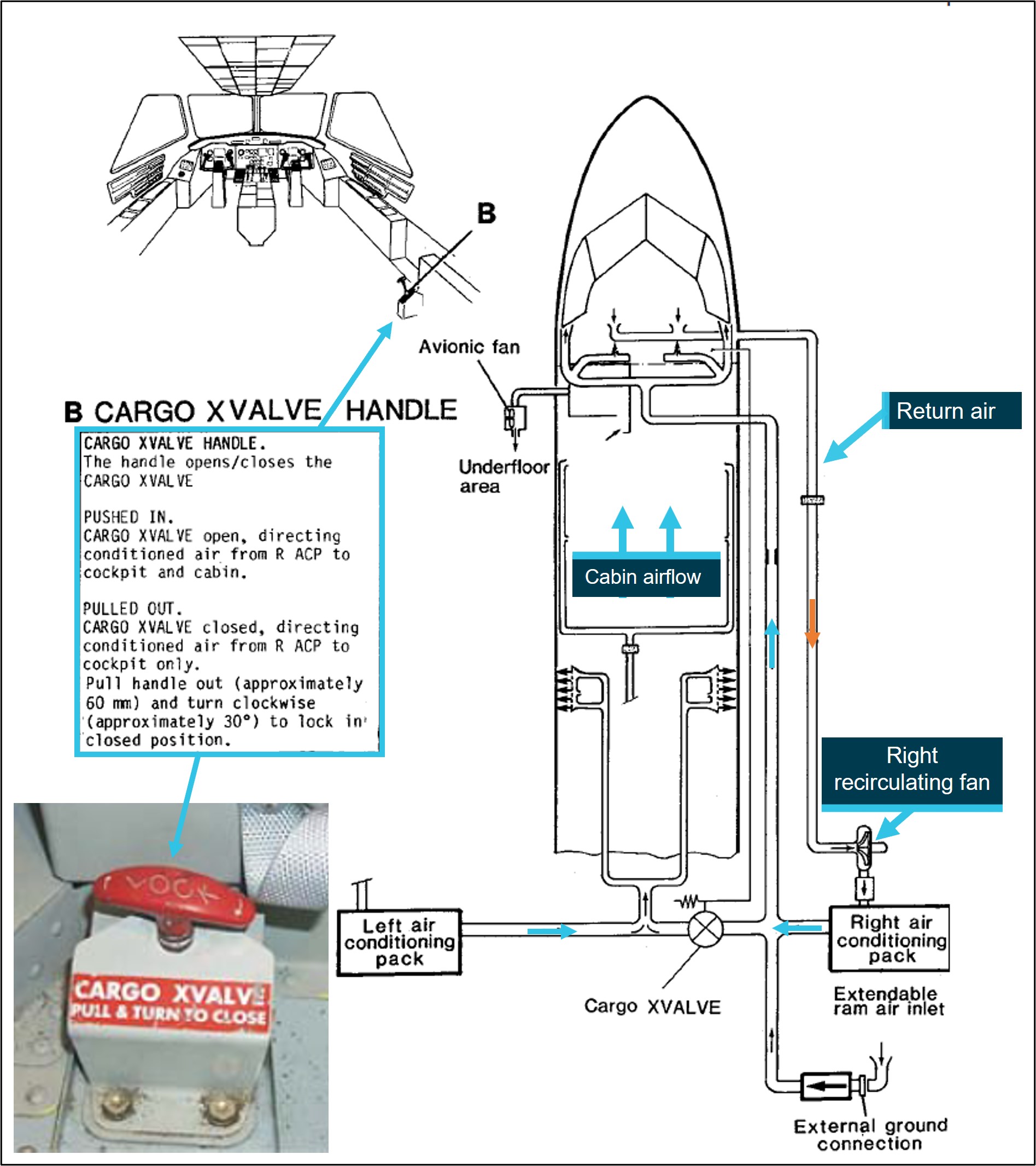
Source: Saab, annotated by the ATSB
Recirculating fan
The right recirculating fan was a centrifugal impeller type fan and was driven by an AC motor. The fan had an in‑built inverter, supplied by 28-volt DC. The majority of the electronics for the fan unit were contained in the box sub-assembly. This included the inverter, an electromagnetic interference (EMI) filter unit and the electronic card sub-assembly. The box sub-assembly controlled the fan operation, including the thermal control. Each electric motor was equipped with:
- a thermal switch[11] located in the cooler which guarded against an abnormal temperature increase. This switch would cut off the power if the motor temperature exceeded 110°C +/− 5° (230°F +/− 41°). The fan would start again when the temperature decreased to 65°C +/− 5° (149°F +/− 41°)
- a speed sensor which guarded against an abnormal decrease of nominal speed. If the speed fell below 80% of nominal speed for more than 17 seconds, the fan would be stopped.
In 1987, Saab released a service bulletin which gave operators the option to install an upgraded recirculating fan. The original fan was a brush type motor which required regular maintenance, including brush replacement when they had worn from use. Saab had received reports of smoke and burning smells which were attributed to brushes that were incorrectly installed. The brushless fans were introduced to help eliminate this issue and also required less maintenance.
The fan installed in VH-KDK was the new brushless fan, manufactured in 1990 and fitted in April 1996. The fan history prior to installation was unknown by the operator. The fan accrued 27,585 hours while fitted to VH-KDK.
Recirculating fan examination
Fire damage was found in the area around the right recirculating fan and on the fan itself (Figure 5). There were no other components in the vicinity of the fan with significant fire damage. As such, it is likely the right recirculating fan was the source of the fire.
Figure 5: Damaged recirculating fan
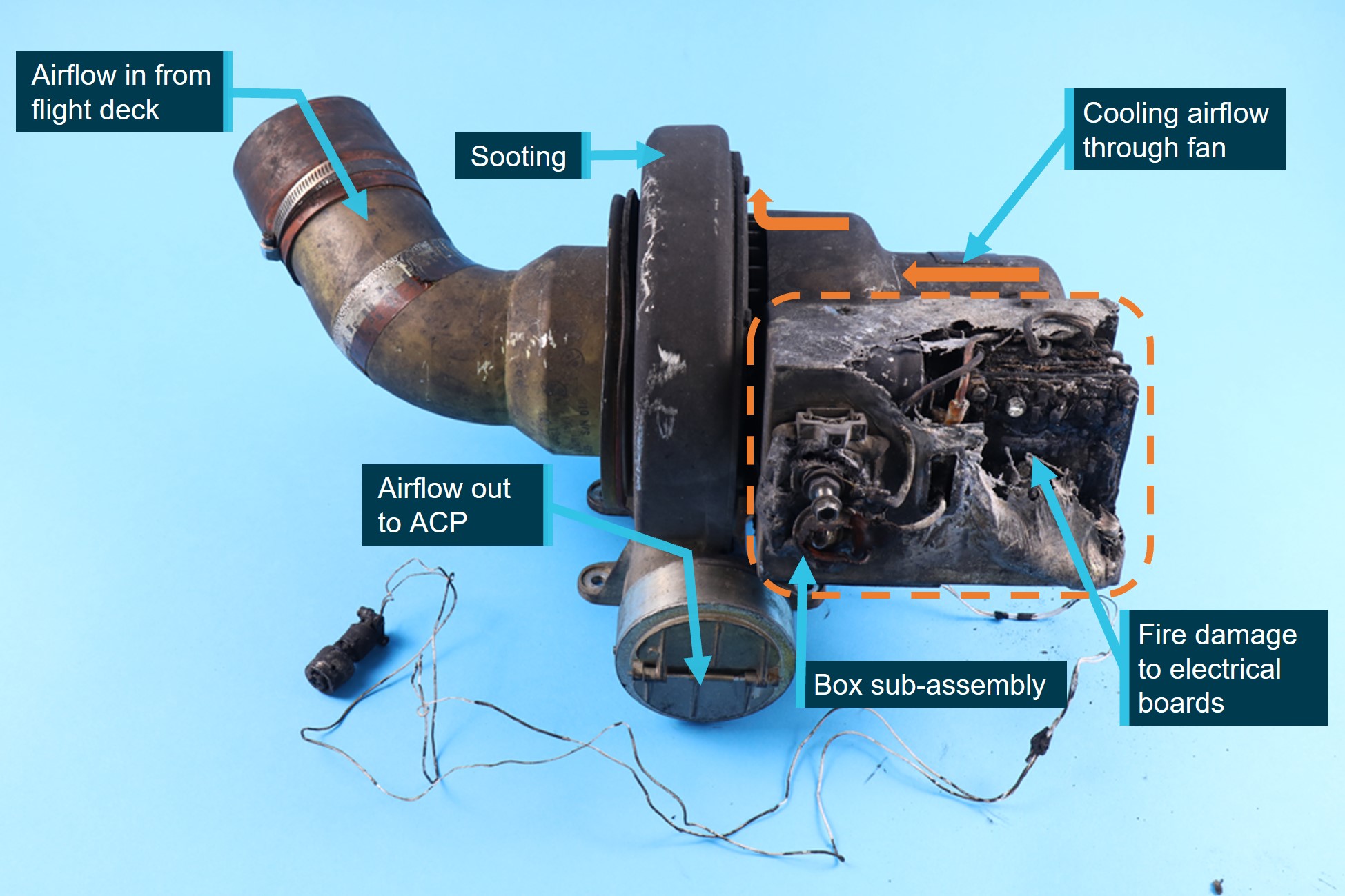
Source: ATSB
An examination of the recirculating fan was conducted at the ATSB’s technical facilities in Canberra. The examination found that the fire damage was most significant at the external box sub‑assembly which housed the EMI filter, the resistor support plates and electronic card sub‑assembly. The aluminium cover of the box sub-assembly had melted, the electrical wiring was damaged, and some terminals had disconnected as a result of the fire damage. There was heavy soot and melting of solder in the cooler assembly.
The electronic card sub-assembly was made up 3 circuit boards, mounted to the resistor support plate. The function of the circuit boards was for motor speed detection, timer control, and a logic card. The damage exhibited on the circuit boards showed significant burning, consistent with the other components within the aluminium cover.
The electromagnetic interference (EMI) filter sub-assembly had considerable damage to the filter itself and to the mounting plate with signs of melting and heat tinting of the steel plate structure, indicating a significant heat source. The heat tint was indicative of temperatures of approximately 310° to 330°C.
Of note, the fire did not appear to be associated with the motor and there was no indication of damage to the internal components of the fan and was able to rotate freely. There was carbon and soot observed on the external surface on the motor. The crew stated that there had been no circuit breakers tripped that would be associated with the failure of the electronic card sub‑assembly.
The ATSB examination of the recirculating fan could not determine the cause of the failure of the electronic components attached to the assembly.
Pressurisation system
The Saab 340 cabin is pressurised by the 2 air conditioning packs. The pressurisation system uses bleed air drawn from each engine and was either automatically controlled by a pressurisation controller, or manually controlled by a control valve operated by the flight crew from the flight deck.
Pressure is able to be regulated by the opening and closing of 2 outflow valves, located in the empennage. The primary outflow valve is electro-pneumatically operated by the pressurisation controller, while the secondary outflow valve is pneumatically controlled from the cockpit and used as a manual standby system.
When emergency pressure relief is required, the primary outflow valve is able to be opened with the emergency pressure dump switch. When the crew of VH-KDK experienced the smoke in the cabin and flight deck, dumping cabin pressure as stated in the ‘smoke removal’ emergency checklist was the method used to assist in rapid removal of the smoke.
Aircraft depressurisation
The severity of the fire resulted in significant damage to the surrounding underfloor furnishings, ducting and airframe structure. The damage was then sufficient to rupture the skin (Figure 6) and caused a subsequent depressurisation of the aircraft.
Figure 6: Underfloor fire damage showing fuselage hole
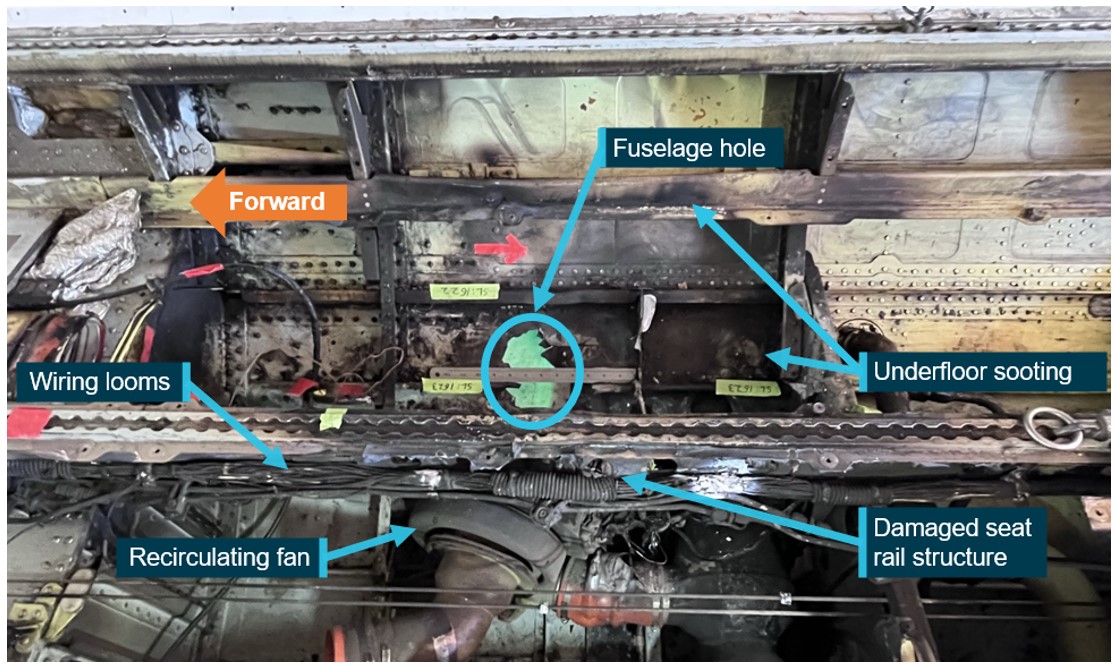
Source: Operator, annotated by the ATSB
Checklists
The pre-flight procedures for the Saab 340A aircraft, including cargo configuration aircraft, were covered by the Aircraft Operations Manual (AOM) normal procedures, produced by the aircraft manufacturer. The AOM pre-flight normal checklist contained a check of the cross-valve handle position prior to flight but did not include a specific check for correct fitment of the smoke barrier curtain.
A flight crew operating manual (FCOM) was carried on board VH-KDK which was developed by Pel-Air, based on the aircraft manufacturer’s AOM. Unlike the aircraft manufacturer's AOM, the pre-flight checks in the operator's FCOM did not contain any reference to the cross-valve handle. Consistent with the aircraft manufacturer’s AOM, the operator’s FCOM also did not include a specific pre-flight check for correct fitment of the smoke barrier curtain. The weight and balance chapter of the FCOM did show a diagram of the smoke curtain fitted but did not include a requirement to ensure the smoke curtain was in place.
The manufacturer had an airplane flight manual supplement in place, implemented as part of the cargo configuration SB, which included fitting the smoke barrier as a limitation (Figure 7 left). There were no identified interior checks in this supplement, which included the checking of the cross-valve handle prior to flight.
The aircraft manufacturer did have emergency checklists specific to cargo‑configured aircraft. These were compiled into the quick reference handbook (QRH) which was available to flight crew in the aircraft (Figure 7 right).
Figure 7: Flight manual supplement (left) highlighting smoke curtain use and QRH checklist (right) highlighting cargo cross-valve handle and cockpit door
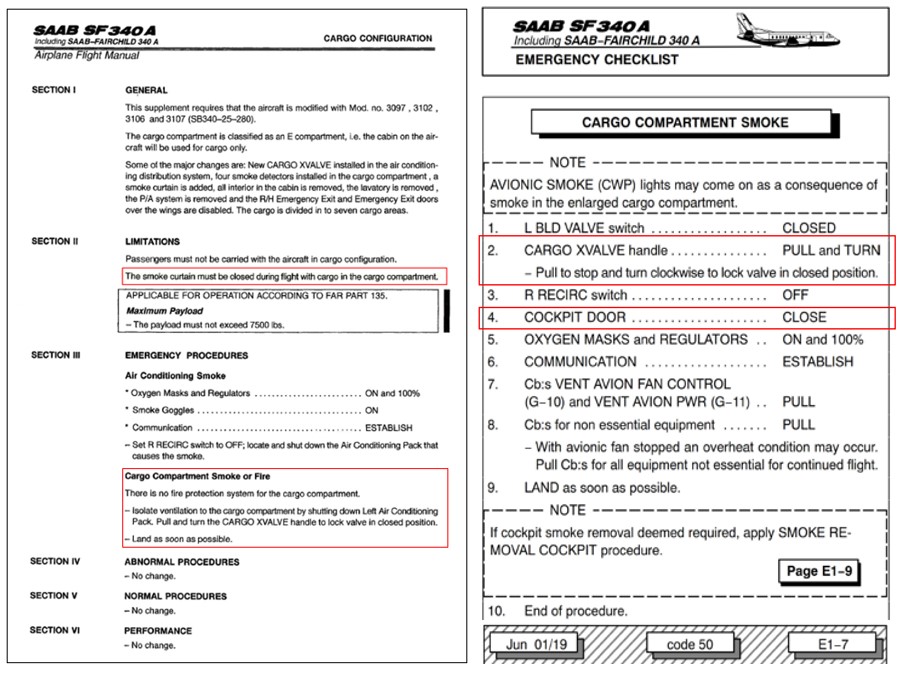
Source: Saab, annotated by the ATSB
Flight deck door
The Pel-Air FCOM stated in the Operating Limitations section that during flight, the flight deck door must be kept closed and locked at all times. It is further listed in the engine start checklist that all doors are closed before engine start.
Evidence from the accident flight, however, shows that before the fire, the crew were operating with the cockpit door open. During interview, the flight crew indicated they closed the door, whilst performing the cargo compartment smoke checklist. This was further supported by the CVR review, where the crew were heard to state the door was to be closed as per the checklist steps, which was followed by the sound of the door shutting.
Flight crew training
Rex conducted a ground school, including simulator training, for their new Saab 340 flight crew. Under a commercial agreement, Pel-Air flight crews were also trained by Rex. The ground school covered the 340 variants of A, B and B WT. The aim of the ground school was to provide pilots from both operators with the necessary knowledge to gain a Saab 340 type rating. The type rating covered all Saab 340 aircraft and did not distinguish between any variant or configuration of the aircraft.
Following the Rex ground school, Pel-Air then conducted further training through its line training program for its flight crews allocated to freight operations. Delivery of this training was in a practical environment, with pilots learning the systems and differences of the cargo‑configured Saab 340. This included the use of the smoke barrier and the operation of the cross-valve handle.
The ATSB asked what the process was for Rex pilots to receive this training and knowledge. Pel‑Air advised that a pilot employed by Rex would only receive this if they were to transition to freight operations with Pel-Air in a permanent role.
Crew familiarity of cargo aircraft
The flight crew operating VH-KDK were both Rex pilots, who were normally rostered for passenger operations. The night before the flight to Wagga Wagga, they were rostered to fly the cargo‑configured 340A. The captain recalled asking the scheduler if they needed a briefing for flying the cargo 340A, and was told that they did not, but it could be arranged if needed.
The captain decided to speak to a Rex colleague who had flown the cargo‑configured 340A several times previously. They were told there were no differences other than the removal of the seats and a freight interior being fitted and that there were no special procedures to be aware of.
Both Rex and Pel-Air advised that their respective operations could roster a crew to fly either operator’s aircraft if it was available. Crewing arrangements were such that there was never any mixing of crew, that is that the flight crew would consist of either 2 Rex or 2 Pel-Air flight crew on any flight.
Oxygen mask
The flight crew fitted their oxygen masks and smoke goggles shortly after receiving the cargo smoke warning and smelling the smoke. The FO conducted the functional tests after fitment and found their microphone was barely readable by the captain. The cockpit voice recorder (CVR) indicated that, although muffled, the speech from the FO was recorded and they were also able to be heard by air traffic control (ATC) throughout the emergency.
The pre-flight checks relating to the crew oxygen system were conducted as part of the interior checklist. The FCOM detailed the checks as:
RIGHT OXYGEN MASK .................................................................................CHECKED
Check flight crew oxygen mask and microphone in accordance with the following:
• …,
• set audio panel BOOM - MASK switch to MASK,
• increase INT/SPKR volume and knock on mask,
• speaker noise indicates proper microphone function,
• set BOOM - MASK switch back to the BOOM position, ….
The check on the left oxygen mask was to be performed in the same manner. Although not detected on the CVR, the captain advised the masks were both tested prior to departure.
Aircraft damage
The damage caused by the underfloor fire was substantial. The fire had damaged underfloor air conditioning ducting and electrical wiring (Figure 8).
Figure 8: Underfloor fire damage
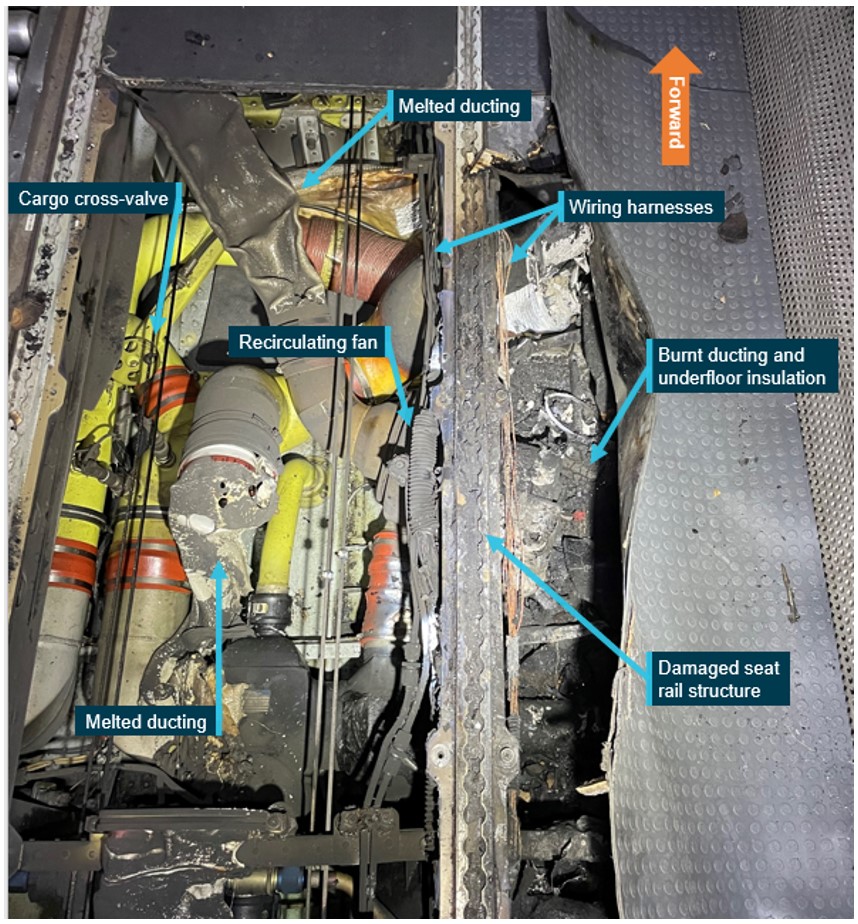
Source: Operator, annotated by the ATSB
Structural components in the surrounding area had been distorted by the extreme heat, including the floor panels, which had collapsed when fire crews entered the aircraft and inadvertently walked over the affected area. The seat track support structure had distorted, and the fuselage was weakened by the fire which breached the outer skin, preventing the aircraft from remaining pressurised (Figure 9).
Figure 9: Fuselage skin breach

Source: Operator, annotated by the ATSB
The fuselage in the immediate area above and below the cabin floor was buckled and delaminated. The heat from the fire most likely travelled between the interior panels and freight lining, leading to the damage observed (Figure 10). Following an engineering inspection of the fire damage, the aircraft was withdrawn from service and not repaired.
Figure 10: Right side delamination on fuselage
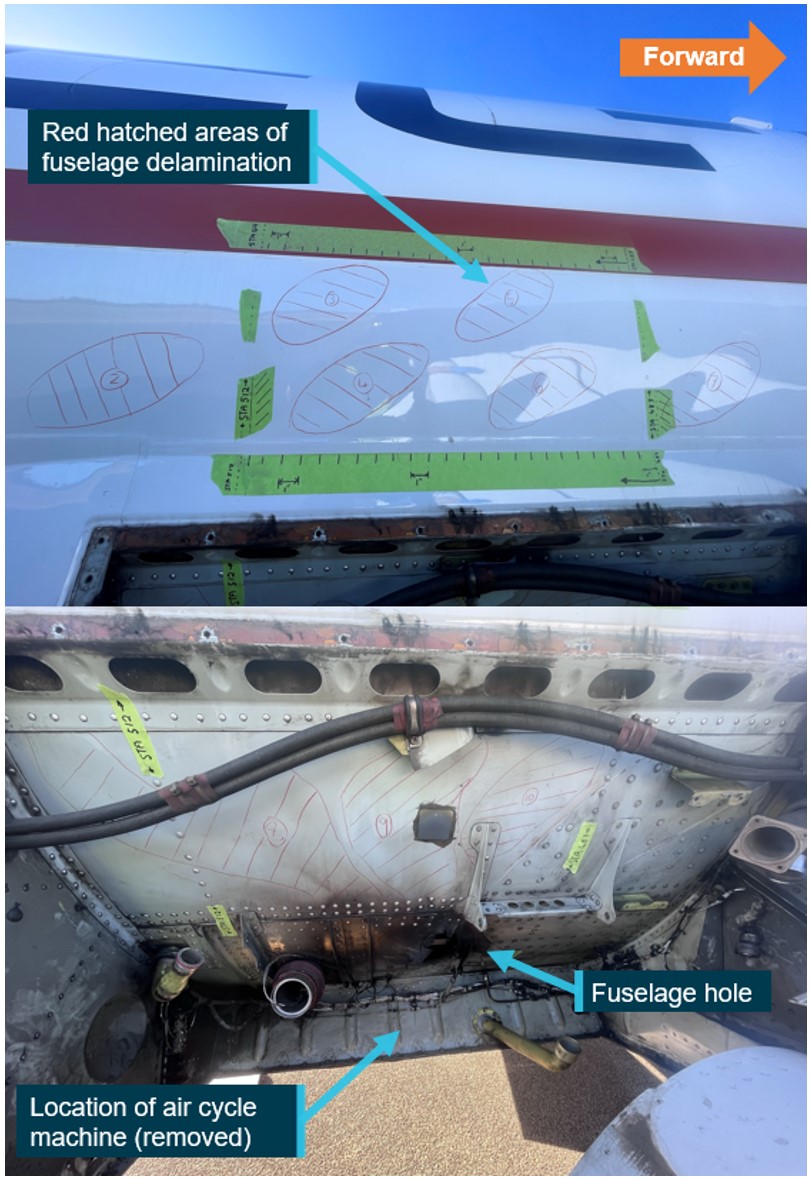
Source: Operator, annotated by the ATSB
Recorded data
The ATSB was supplied raw data by the operator from the flight data recorder (FDR). This data was analysed and was found to include the previous 4 flights.
The recorded data from the occurrence flight showed that at about 59 minutes after becoming airborne at Wagga Wagga, the FDR stopped recording. The recording stopped at about the same time as the initial smoke indication. This was most likely due to fire damage to the electrical wiring which controlled the FDR.
Flight track information was also obtained from FlightRadar24, which showed the entire flight, including the diversion and landing at Cobar (Figure 11).
Figure 11: VH-KDK flight track and diversion
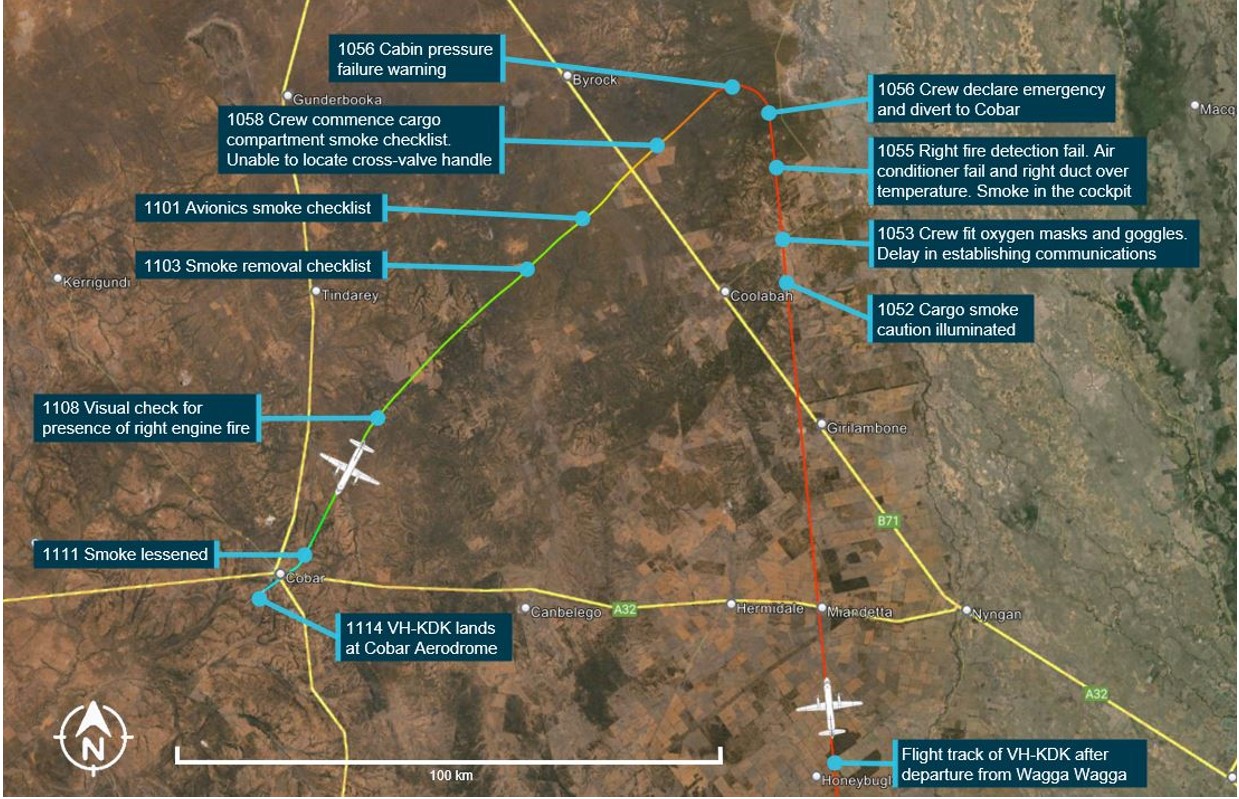
Source: Google Earth and Flightradar24, annotated by the ATSB based on CVR recordings
The CVR was removed and sent to the ATSB technical facilities in Canberra. The CVR data was downloaded, with the recovery of 4 channels of audio data of about 120 minutes duration which included the in-flight fire event. Reviewing the recorded CVR data also revealed that coincidentally, just prior to the indication of the cargo smoke caution, the flight crew had been discussing alternate airports in the area, and which one they would select if they had a need to divert.
The recording contained information from the end of the previous flight, and from the day of incident. It included the:
- flight crew’s initial reaction to the caution warning for the smoke in the cabin
- conduct of the emergency checklists
- additional warnings as they occurred
- crew intercom and communications with Melbourne Centre
- landing at Cobar and subsequent exiting of the aircraft.
The recording also revealed that while conducting the emergency checklist for ‘cargo compartment smoke’ the crew closed the cockpit door as a loud bang was heard, indicating it was open during the flight.
Safety analysis
Introduction
On 23 April 2023, the Regional Express (Rex) Airlines flight crew operating a Pel-Air Aviation Saab 340A, registered VH-KDK were conducting an internal revenue cargo flight from Wagga Wagga, New South Wales, to Charleville, Queensland. About 1 hour into the flight, the crew experienced an in-flight fire and diverted to Cobar, New South Wales. After experiencing thick smoke on the flight deck and then a cabin depressurisation, the crew performed a safe landing at Cobar. The aircraft was substantially damaged, and the flight crew were not injured.
This analysis will explore:
- origin of the in-flight fire
- aircraft preparation for the flight
- oxygen mask use and technical problem of the microphone
- cabin depressurisation
- flight crew knowledge of aircraft systems
- flight crew operating with the cockpit door open
- Pel-Air and Rex flight crew operating manual information deficiencies
- training of Rex flight crews
- Saab pre-flight inspection checklists
- Rex crew familiarity of cargo aircraft.
Origin of the in-flight fire
The source of the in-flight fire was traced to the right recirculating fan assembly. Although the fan was not damaged internally, the fire damage was most significant at the box sub-assembly, which was mounted external to the fan and housed the electrical control circuit boards. It is likely that an electrical component or components within the box sub-assembly failed, resulting in the underfloor fire. The fire damaged underfloor insulation and plastic air conditioning ducting components, which led to thick smoke filling the cabin and cockpit and aircraft structural damage.
The avionics warning received by the crew during the diversion was most likely associated with the avionics cooling air that was being drawn from the now smoke-filled cabin. This was also stated in the ‘cargo compartment smoke’ checklist.
The ATSB examination of the recirculating fan could not determine a cause for the failure in the electronic control cards which led to the fire.
When the crew received the air conditioning system right duct over temperature caution light, it was most likely due to the distribution duct over temperature being affected by the fire and the melting which occurred as a result. When the over temperature was sensed, the right bleed valve closed automatically as a function of system logic for over temperature protection.
Smoke barrier curtain
Cargo operations can have a greater fire risk than passenger operations due to the carriage of cargo that could be the source of a fire and the lack of cabin crew available to fight a fire. As such, additional protection was available to minimise flight crew exposure to cabin smoke in the form of additional smoke detectors and a smoke curtain.
However, the smoke curtain was not installed into position by anyone involved in the flight preparation. The flight crew, who normally operated the same aircraft type but in a passenger configuration, did not notice there was a placard at the aircraft entrance stating the smoke curtain was to be fitted for all cargo flights. The flight crew remained unaware of the smoke barrier curtain and its use for cargo operations. Further, the engine being transported was positioned in the cargo area of VH-KDK, on both occasions, by Rex engineers. As the curtain was usually installed by freight handlers during normal cargo operations, it is possible the Rex engineers were also unaware of its requirement to be fitted.
In this accident, the source of the fire was an aircraft component rather than the cargo being carried. If a similar fire occurs in a passenger‑configured Saab 340 aircraft, then the smoke curtain would not be in place. However, the smoke curtain was available and was required for use for this flight, so its non-use increased risk for this event.
The flight deck door was not closed during flight as prescribed in the operator’s FCOM operating limitations and checklists. Having the door closed would have likely prevented the smoke being able to flow into the flight deck.
The result of not having the smoke barrier fitted and the flight deck door closed as part of the aircraft pre-flight preparation was that smoke from the fire was not contained to the cabin area and was able to move forwards toward the flight deck.
Oxygen mask fault
The flight crew fitted their oxygen masks and smoke goggles when alerted of the presence of smoke by the central warning panel. This decision may have prevented the crew from being overcome by smoke and fumes in the cockpit in the next several minutes. However, once fitted, the crew had difficulty communicating with each other, as a result of the mask microphone being very faint and difficult for the captain to hear the first officer (FO). This appeared to be an internal fault only, as the cockpit voice recording (CVR) showed that the FO was able to be adequately heard by ATC.
This breakdown of communication delayed the crew by 57 seconds, in which emergency checks were not initiated due to the breakdown of communication. It created confusion and distraction between the crew while trying to execute the emergency checklist.
A review of the CVR captured prior to flight could not positively determine if the pre-flight check action in relation to the oxygen mask was performed. This is an important check of the emergency communication system whilst on oxygen and was designated as a mandatory check item for a daily inspection as required by the Rex and Pel-Air FCOM.
Cross-valve handle
While the flight crew were conducting the emergency checklist items for cargo compartment smoke, they were unable to locate the cross-valve handle. This was due to the combination of the thick smoke obscuring their vision and their lack of knowledge of the differences in the cargo‑configured aircraft.
Had the location and function of the cross-valve handle been known by the flight crew, the time taken to identify it during completion of the emergency checklist would have been minimised, which would have limited the delay of smoke removal from the flight deck.
In this case, the subsequent depressurisation resulted in the smoke dissipating even in the absence of the cross-valve.
Cabin depressurisation
The weakening of the fuselage structure due to the underfloor fire resulted in a breach of the fuselage skin, which led to a subsequent depressurisation of the aircraft during the descent. Although adding to another caution alert indication for the flight crew and subsequent checklist to be conducted, it also benefited in the removal of smoke from the cabin and flight deck.
At the time of the depressurisation, VH-KDK was at FL 160 and descending. The crew, when alerted to the depressurisation, increased the rate of descent to below 10,000 ft. The cabin depressurisation occurred 4 minutes after the initial smoke warning occurred.
Due to the size of the hole created, the smoke removal most likely occurred at a greater rate than using the aircraft pressurisation outflow valves alone. The resulting fortuitous reduction in the amount of smoke in the flight deck improved visibility and allowed the crew to carry out a safe landing into Cobar.
Crew familiarity of cargo‑configured aircraft
The flight crew had not flown or had any prior training on the cargo‑configured Saab 340 and were not familiar with the differences of the passenger configuration. The captain chose to liaise with a colleague to gain information on the cargo‑configured aircraft instead of accepting the company offer for a briefing.
This non-formal approach to understanding the differences between the 2 aircraft types ultimately did not pass on the required operational differences and potential safety aspects of the change of aircraft configuration.
Rex and Pel-Air manuals
Both operators (Rex and Pel-Air) manuals, which were designed to provide essential information to flight crews, did not include the required information to enable the pre-flight checks to be conducted adequately. While the weight and balance chapter of the FCOM showed the smoke barrier curtain location, there was no information on its importance to cargo operations, and as the crew had not been informed of any differences, they would not have been expecting that this section contained this information. The smoke barrier curtain installation information that was contained in the Saab service bulletin and flight manual supplement was not included in the pre‑flight checklists. As a result, the flight crew did not have awareness of its use.
The operators' manuals also did not have a check to verify the position of the cross-valve handle. As discussed above, when the checklist called for the crew to use this handle when the aircraft was already filling with smoke, the crew could not locate it.
Flight crew training
The Rex ground school provided type rating training on the Saab 340 series aircraft to both Rex and Pel-Air pilots. This training was based on the passenger‑configured aircraft. Pel-Air pilots undertook further training which gave them the knowledge and skills for the cargo‑configured aircraft.
In scheduling their flight crews to operate the cargo‑configured Saab 340, Rex did not have a process to ensure that the additional training or knowledge sharing for their crews in the differences applicable to aircraft operated by Pel-Air was delivered.
Saab pre-flight checklists
As discussed above, both operators’ manuals had no inclusion of a pre-flight interior check for the smoke barrier curtain or the cross-valve handle. Likewise, there was no pre-flight interior check for these items in the manufacturer’s documentation. Saab confirmed that there were no checks in the pre-flight checklist for the crew to specifically verify that the smoke barrier curtain was correctly fitted.
The result of the manufacturer’s pre-flight and interior checklists not detailing information for the smoke curtain was that the operator did not detail these in their own FCOM. This information was not available for the flight crew who, even without prior knowledge of the cargo‑configured variant, would have been alerted to these changes while conducting these pre-flight checks in accordance with the FCOM.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition, ‘other findings’ may be included to provide important information about topics other than safety factors. Safety issues are highlighted in bold to emphasise their importance. A safety issue is a safety factor that (a) can reasonably be regarded as having the potential to adversely affect the safety of future operations, and (b) is a characteristic of an organisation or a system, rather than a characteristic of a specific individual, or characteristic of an operating environment at a specific point in time. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the in-flight fire and cabin smoke involving a Saab 340A, VH‑KDK, 114 km east-north-east of Cobar, New South Wales, on 23 April 2023.
Contributing factors
- It was likely that an electrical component of a control circuit board on the recirculating fan failed, resulting in an in‑flight fire under the cabin floor.
- The smoke curtain was not fitted as required for the cargo configuration, and the flight deck door was open, which allowed smoke from the in‑flight fire to enter the flight deck.
- The underfloor fire caused weakening of the fuselage structure, which led to a subsequent depressurisation of the aircraft during the descent. However, the depressurisation aided in the removal of enough smoke from the flight deck on approach to allow an unhindered visual approach at Cobar.
- Crew were not familiar with the cargo configuration and were unaware of the smoke curtain requirements and location of the cross-valve handle.
- The Pel-Air and Rex Saab 340 flight crew operating manuals did not include reference to the location and operation of the cross-valve handle or the operation and use of the smoke curtain. (Safety issue)
- Rex did not ensure its flight crews received training in the differences between passenger and freight‑configured Saab 340 aircraft, prior to being scheduled to fly freight operations. (Safety issue)
- Saab did not include the smoke curtain fitment in pre-flight documentation for the cargo‑configured Saab 340 aircraft to inform flight crew of this difference from the passenger-configured version. (Safety issue)
Other factors that increased risk
- When the flight crew donned their oxygen masks, the first officer's oxygen mask microphone did not function correctly. This led to difficulty in communication between the flight crew and a delay in responding to the emergency.
- Due to the combination of the smoke density and lack of prior knowledge, the flight crew were unable to locate the cross-valve handle during the emergency, therefore delaying the removal of smoke from the flight deck.
Safety issues and actions
Central to the ATSB’s investigation of transport safety matters is the early identification of safety issues. The ATSB expects relevant organisations will address all safety issues an investigation identifies. Depending on the level of risk of a safety issue, the extent of corrective action taken by the relevant organisation(s), or the desirability of directing a broad safety message to the aviation industry, the ATSB may issue a formal safety recommendation or safety advisory notice as part of the final report. All of the directly involved parties were provided with a draft report and invited to provide submissions. As part of that process, each organisation was asked to communicate what safety actions, if any, they had carried out or were planning to carry out in relation to each safety issue relevant to their organisation. Descriptions of each safety issue, and any associated safety recommendations, are detailed below. Click the link to read the full safety issue description, including the issue status and any safety action/s taken. Safety issues and actions are updated on this website when safety issue owners provide further information concerning the implementation of safety action. |
Saab documentation for cargo configured aircraft
Safety issue number: AO-2023-020-SI-01
Safety issue description: Saab did not include the smoke curtain fitment in pre-flight documentation for the cargo‑configured Saab 340 aircraft to inform flight crew of this difference from the passenger‑configured version.
Operator documentation and crew familiarity
Safety issue number: AO-2023-020-SI-02
Safety issue description: The Pel-Air and Rex Saab 340 flight crew operating manuals did not include reference to the location and operation of the cross-valve handle or smoke curtain.
No formal company training
Safety issue number: AO-2023-020-SI-03
Safety issue description: Rex did not ensure its flight crews received training in the differences between passenger and freight‑configured Saab 340 aircraft, prior to being scheduled to fly freight operations.
Safety action not associated with an identified safety issue
| Whether or not the ATSB identifies safety issues in the course of an investigation, relevant organisations may proactively initiate safety action in order to reduce their safety risk. The ATSB has been advised of the following proactive safety action in response to this occurrence. |
Additional safety action by Regional Express
Rex advised that it is implementing a fleet‑wide inspection of the flight deck and passenger compartment recirculation fans at the next aircraft heavy maintenance visit. The inspection will be focused on the electronic sub-assembly module of the recirculation fan due to this component being identified to have the most significant fire damage on the fan assembly removed from VH‑KDK.
Glossary
| AC | Alternating current |
| ACP | Air conditioning pack |
| AOM | Aircraft operating manual |
| ATC | Air traffic control |
| ATPL | Air transport pilot licence |
| BoM | Bureau of Meteorology |
| CASA | Civil Aviation Safety Authority |
| CVR | Cockpit voice recorder |
| DC | Direct current |
| FCOM | Flight crew operating manual |
| FDR | Flight data recorder |
| FL | Flight level |
| FO | First officer |
| INT/SPKR | Intercom/Speaker |
| PF | Pilot flying |
| PM | Pilot monitoring |
| QRH | Quick reference handbook |
| SB | Service bulletin |
Sources and submissions
Sources of information
The sources of information during the investigation included:
- the crew of VH-KDK
- Regional Express Airlines
- the chief pilot of Pel-Air Aviation
- the manager training and checking and head of operations for Regional Express Airlines
- Civil Aviation Safety Authority
- Bureau of Meteorology
- Fire and Rescue New South Wales
- Saab
- Airservices Australia
- the cockpit voice recorder and flight data recorder
- recorded data from Flightradar24.
References
Australian Government 2023, Part 91 (General Operating and Flight Rules) Manual of Standards 2020, Civil Aviation Safety Authority, Canberra, ACT, viewed 30 April 2024, <Federal Register of Legislation - Part 91 (General Operating and Flight Rules) Manual of Standards 2020>
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Civil Aviation Safety Authority
- Airservices Australia
- Crew of VH-KDK
- Regional Express Aviation
- Pel-Air Aviation
- Swedish Accident Investigation Authority (SHK)
- Bureau of Enquiry and Analysis for Civil Aviation Safety (BEA).
Submissions were received from:
- the captain of the crew
- Regional Express Aviation
- Pel-Air Aviation
- Swedish Accident Investigation Authority (SHK)
- Bureau of Enquiry and Analysis for Civil Aviation Safety (BEA).
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2024 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[2] Flight level: at altitudes above 10,000 ft in Australia, an aircraft’s height above mean sea level is referred to as a flight level (FL). FL 220 equates to 22,000 ft.
[3] Pilot flying (PF) and pilot monitoring (PM): procedurally assigned roles with specifically assigned duties at specific stages of a flight. The PF does most of the flying, except in defined circumstances, such as planning for descent, approach, and landing. The PM carries out support duties and monitors the PF’s actions and the aircraft’s flight path.
[4] Warnings and cautions: give pilots aural and visual alerts for abnormal conditions. Warnings are highest priority which require immediate action. Cautions are the second priority and give advisory information to pilots.
[5] PAN PAN: an internationally recognised radio call announcing an urgency condition which concerns the safety of an aircraft or its occupants but where the flight crew does not require immediate assistance.
[6] The avionics smoke indication was a result of the avionic bay drawing in smoke from the cargo area.
[7] Activating the fire extinguisher system also closes the fuel shut‑off valves, which removes all supply of fuel to the engines. The fire bottles are then operated, extinguishing fire within the engine cowlings.
[8] Saab manufactured the 340 in A, B and B WT variants.
[9] Both Rex Airlines and Pel-Air were wholly owned subsidiaries of Regional Express Holdings Limited (REX).
[10] Although VH-KDK landed safely, the extent of the damage from the fire is classified by ICAO Annex 13 as an accident due to the nature of major repair work required to the airframe.
[11] CAVOK: Conditions and visibility good, nil significant cloud and excess of 10 kilometres visibility
[12] The thermal switch is designed to detect an overheat of the cooler only. It is not configured or located where it would detect the overheating of the electronic card sub-assembly.
[13] Quick change aircraft are designed so that they can be operated in a passenger configuration and then quickly changed to then operate in a freighter configuration, depending on operator requirements.
Occurrence summary
| Investigation number | AO-2023-020 |
|---|---|
| Occurrence date | 23/04/2023 |
| Location | 114 km east-north-east of Cobar |
| State | New South Wales |
| Report release date | 20/11/2024 |
| Report status | Final |
| Investigation level | Defined |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Air/pressurisation, Diversion/return, Emergency/precautionary descent, Fire, Smoke, Warning devices |
| Occurrence class | Accident |
| Highest injury level | None |
Aircraft details
| Manufacturer | Saab Aircraft Co. |
|---|---|
| Model | 340A |
| Registration | VH-KDK |
| Serial number | 16 |
| Aircraft operator | Regional Express |
| Sector | Turboprop |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Wagga Wagga Airport, New South Wales |
| Destination | Charleville Airport, Queensland |
| Damage | Substantial |