Collision with terrain involving Cessna 150M, VH-WWU, 40 km north-west of Northampton, Western Australia, on 21 March 2025
Final report
Report release date: 14/10/2025
Investigation summary
What happened
On the morning of 21 March 2025, a pilot was ferrying a Cessna 150M aircraft, registered VH-WWU and operated by Norwest Air Work, from Geraldton Airport to Shark Bay Airport, Western Australia.
Approximately 35 minutes into the flight, the aircraft entered a left turn that transitioned into a spiral dive. The aircraft collided with terrain, the pilot was fatally injured, and the aircraft was destroyed.
What the ATSB found
The ATSB found no evidence of any in-flight failure of the airframe structure or flight control system and the engine was producing power throughout the descent. Based on the pilot’s medical history and sequence of events, it was determined that the pilot likely experienced an incapacitating medical event of an undetermined nature, resulting in a deviation off track and the uncorrected spiral dive.
Safety message
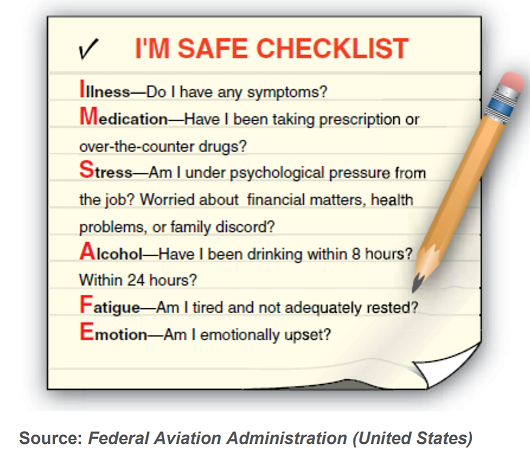
The ATSB recommends that pilots conduct the IMSAFE checklist before every flight. The checklist prompts pilots to self-assess whether factors such as illness, stress or fatigue could affect their performance and compromise flight safety.
The ATSB urges all pilots to integrate the IMSAFE checklist into their pre-flight routine, no matter how routine the flight may seem. Prioritising personal fitness for flight duty helps to reduce the risk not only to the pilot, but also to passengers, crew, and the public.
The investigation
| The ATSB scopes its investigations based on many factors, including the level of safety benefit likely to be obtained from an investigation and the associated resources required. For this occurrence, the ATSB conducted a limited-scope investigation in order to produce a short investigation report, and allow for greater industry awareness of findings that affect safety and potential learning opportunities. |
The occurrence
Overview
On the morning of 21 March 2025, a pilot was conducting 2 ferry flights of aircraft operated by Norwest Air Work. The plan was to fly from Shark Bay Airport to Geraldton Airport, Western Australia, in a Cessna 150M, registered VH‑TDZ. Once at Geraldton Airport, the pilot would swap aircraft at the maintenance hangar and fly back to Shark Bay Airport[1] in VH‑WWU, the operator’s other Cessna 150M, which had been released from maintenance on 18 March 2025.
The pilot was the sole occupant on board both flights. The operator’s senior base pilot was holding SARTIME[2] for both flights.
On the ground at Geraldton Airport
The pilot landed VH‑TDZ at 0914 local time and taxied the aircraft to the maintenance organisation’s parking bay. At 0922, the pilot sent a text message to the senior base pilot informing them of their arrival in Geraldton.
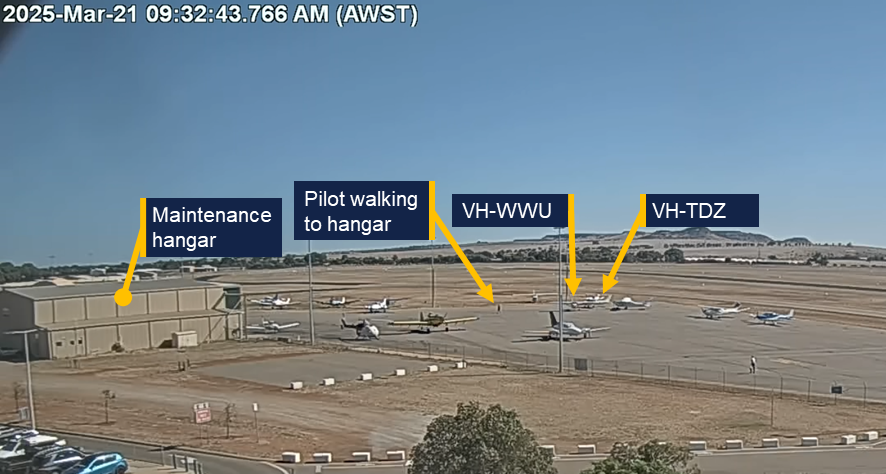
Airport CCTV footage showed that between 0925 and 0931 the pilot manually manoeuvred VH‑WWU out of its parking bay and moved VH‑TDZ into it. Once completed, the pilot walked to the maintenance hangar (Figure 1). Witnesses at the airport reported that the pilot appeared unwell and had mentioned having had severe gastroenteritis in the preceding days. Witnesses did not report any apparent speech or physical impairment. The pilot did not appear to have any difficulty walking around or moving aircraft.
At 0946, the pilot left the maintenance hangar, walked to VH‑WWU, appeared to check the oil level and enter the aircraft. The aircraft had already been refuelled that morning by the airport refueller. At about 0947, the pilot started the engine and taxied the aircraft to the centre apron.
Figure 1: Aircraft changeover
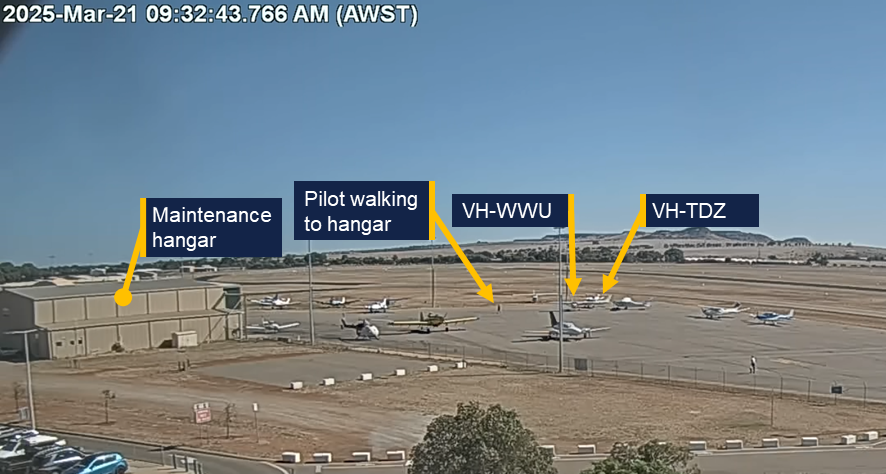
Source: Geraldton Airport, annotated by the ATSB
Geraldton to Shark Bay
At 0956, the pilot broadcast on the local CTAF[3] that they were lining up and rolling on runway 08. The aircraft lifted off the runway 40 seconds later. At 0957 the pilot broadcast they had departed the runway and were tracking out to the north climbing to 2,500 ft through 600 ft. This was the last recorded call from VH‑WWU on the CTAF.
Directly after take‑off, the pilot texted the senior base pilot with the estimated arrival time at Shark Bay of 1230. The aircraft’s flight path from Geraldton is shown in Figure 2.
At 1009, the pilot took a photo of the aircraft oil temperature gauges. Eight minutes later the pilot sent the photo to a staff member at the maintenance organisation with accompanying text stating ‘WWU flies beautiful, smooth, and tight. Oil temp a little high for a cool day so we might have to look at fitting those coolers back onto WWU. I’d hate to see the rings[4] suffer.’ The maintainer responded via text at 1018, and the message was recorded as delivered (indicating that the pilot’s phone was functional at that time). The oil temperature shown in the photo was towards the upper end of the normal range but below the 240°F maximum oil temperature limit.
Figure 2: Flight path overview

Source: Google Earth, annotated by the ATSB
At 1027:12, the aircraft crossed to the right of the direct track to Shark Bay (343°M), while maintaining a track of 347°M (Figure 3). At 1027:47, 25 seconds after crossing the direct track, the recorded data showed a right turn to a track of 011°M.
At 1028:41, while maintaining a track of 011°M, the aircraft commenced a slight descent and 22 seconds later (at 1029:13) entered a shallow left turn. The aircraft then re‑acquired the previous track of 347°M which was maintained for 15 seconds. At 1029:28, another left turn occurred as the slight descent continued. This turn transitioned into a spiral dive with the descent steepening significantly at 1030:12. The spiral dive tightened and steepened until a collision with terrain at 1030:47. The pilot was fatally injured and the aircraft was destroyed.
Figure 3: Track deviation and spiral dive

Source: Google Earth, annotated by the ATSB
At 1116:43, a call was placed to police by a member of the public stating they had come across aircraft wreckage by the side of a road as they were driving past. The wreckage was 84 km north‑west of Geraldton Airport and about 0.5 km right of the direct track. The member of the public stated that although they had been nearby, they had not seen or heard the aircraft or the impact.
Context
Pilot information
Aeronautical experience
The pilot held a commercial pilot licence (helicopter and aeroplane), with both single and multi‑engine class ratings for aeroplanes, and a single engine class rating for helicopters. They held low‑level operational ratings for sling, aerial mustering helicopter and aerial musting aeroplane operations. In addition, the pilot held a flight instructor rating with a low‑level operations training endorsement for both aeroplanes and helicopters.
The pilot most recently completed single engine aircraft and low‑level flight reviews on 12 February 2024.
The pilot’s total aeronautical experience was over 17,000 hours. In the previous 90 days the pilot had flown 28.3 hours (14.2 hours in the Cessna 172, 12.6 hours in the Cessna 206, and 1.5 hours in the Cessna 150).
Medical information
The pilot held a valid Class 1 aviation medical certificate that was revalidated in October 2024. The certificate specified that the pilot was to wear distance vision correction and a headset while flying. It also required reading vision correction to be available and no flying within 24 hours of certain types of medical treatment (which had not been recently provided in this case).
General health
At the time of the accident, the pilot was taking medication for:
- hypertension (high blood pressure) – Irbesartan
- hypercholesterolaemia (high cholesterol) / hyperlipidaemia – Atorvastatin
- gastroesophageal reflux disease, with Barret’s oesophagus – Omeprazole.[5]
All medications taken by the pilot were permissible for use by pilots in accordance with regulatory guidelines. The pilot’s designated aviation medical practitioner (DAME) and general practitioner (GP) both noted the pilot had haemochromatosis.[6]
The pilot last visited their DAME on 31 October 2024, to complete their aviation medical examination.
On 15 January 2025 the pilot completed an exercise stress ECG test. This was triggered due to a raised cardiac risk index score, which takes into account the pilot’s sex, age, blood cholesterol, blood pressure, diabetes status, smoking status and ECG interpretation. The test was valid and was reported by the supervising cardiologist as:
a normal exercise stress test with no significant ST depression during exercise and recovery.[7] Fair exercise tolerance for the patients age. Normal blood pressure at rest and normal blood pressure response to exercise.
On 25 February 2025, the pilot provided the results of a blood test for ferritin and HbA1c completed on 19 February 2025, in response to CASA letters requesting the below items for the pilot’s next medical renewal:
- the result of an HbA1c test to monitor if they had progressed from impaired glucose tolerance to diabetes mellitus
- the collated results of ferritin levels
- other clinically indicated blood tests for the preceding 12 months.
There was no information provided regarding assessment for any other tests.
A colleague at the DAME’s medical practice conducted a tele-consult on 4 March 2025 to discuss slightly raised ferritin[8] from blood samples taken on 19 February 2025 and recommended that the pilot attend their GP to consider venesection.[9] On 4 March 2025, the GP received a letter from a colleague of the pilot’s DAME to consider the venesection. The GP posted the pilot a pathology request form for therapeutic venesection on 12 March 2025. There was no evidence that this venesection was actioned by the pilot before the accident.
The GP, DAME, and pilot’s family reported the pilot was an ex-smoker, however, multiple members of the aviation community who knew the pilot, reported the pilot still smoked. The ATSB was unable to confirm the frequency with which the pilot had been smoking, however the pilot’s smoking status did not change the requirement for or the interpretation of the cardiac risk assessment.
Health leading up to the accident
The pilot’s next of kin (NOK) recalled the pilot had contracted gastroenteritis 5 days prior to the accident. The NOK recalled the pilot stating that they were feeling better the day prior to the accident (20 March) and reminding the pilot to stay hydrated.
The senior base pilot recalled that the pilot had planned to fly the same ferry route as the accident flight on 20 March. However, the pilot reported that they had gastroenteritis and were not well enough to fly.
On the day of the accident while at the maintenance facility in Geraldton, aircraft maintainers noted that the pilot’s skin appeared pale, the pilot had yellow, sunken eyes and appeared to have lost a significant amount of weight. They recalled the pilot stating they had gastroenteritis, had not been eating and had lost 4 kg of weight in the preceding days.
The pilot did not contact either their usual GP, DAME or CASA regarding the gastrointestinal illness. Symptoms usually start within 2–5 days of infection, with full recovery typically within 7–14 days. Symptoms can include diarrhoea, fever, stomach cramps, bloating, nausea and vomiting. Acute complications can include dehydration (signs include scant urine production, dark coloured or concentrated urine, dizziness or light-headedness, low blood pressure, thirst, dry mouth, loss of skin turgor, sunken eyes, acute weight loss).
Pilot health reporting requirements
CASA advised on its website[10] that if a pilot has a medically significant condition that impairs their ability to perform the duties authorised by their licence, they must ground themselves while the condition is present, and check with a DAME and/ or report the condition to CASA. These reporting requirements do not apply for ‘common medical ailments’ including gastroenteritis. It also states that if a medically significant condition lasts longer than 7 days (Class 1)[11], they must notify their DAME and ground themselves until notified by their DAME or CASA that they could continue their licenced duties.
Post-mortem examination and toxicology
Post-mortem examination of the pilot confirmed the presence of bacteria responsible for causing gastroenteritis.
Toxicology results received to date indicated nothing of concern, including that carbon monoxide levels were not significantly raised.
The post-mortem examination was consistent with the pilot wearing the lap portion of the aircraft’s 3-point restraint (see Aircraft information), however it was unable to be determined if the pilot was wearing the upper torso restraint.
Aircraft information
The Cessna 150M is a high‑wing, all-metal, 2‑seat, unpressurised aircraft with a fixed landing gear. VH‑WWU was manufactured in 1976 and first registered in Australia in 1986. It was powered by a Continental O‑200‑A reciprocating piston engine, driving a fixed-pitch propeller. The aircraft was equipped with a 3-point occupant harness.[12] The aircraft was not equipped with an autopilot.
The aircraft was operated until 2016 and then placed in storage. In January 2022, the aircraft was recommissioned which included replacement of the flight control cables and fitment of the engine, which had been overhauled. On 11 April 2024, the aircraft was issued with a maintenance release and commenced operations with Norwest Air Work. At the time, the aircraft had accrued about 13,910 hours total time in service.
A periodic and other scheduled inspections were carried out between 6–18 March 2025. The periodic inspection identified minor defects that were subsequently rectified. The aircraft’s engine reportedly had excessive oil consumption, which was addressed by honing[13] the cylinders and fitting new piston rings. Additionally, the engine ignition harness was replaced. The engine was tested by carrying out a ground run 3 days before the accident and found to be functioning correctly. At the commencement of the accident flight, the aircraft had accrued a total time in service of 14,208 hours.
Site and wreckage
The wreckage was located about 20 m south of an east‑west road. The wreckage trail extended in a north‑easterly direction, about 23 m from the initial impact point to where the main wreckage, including the wings, empennage, engine and propeller had come to rest (Figure 4). There was no fire. Fuel could be smelt in the area.
Figure 4: Overview of VH-WWU accident site

Note: Some of the aircraft had been moved by the first responders at the time this image was captured. Source: ATSB
Ground impact marks and damage to the airframe indicated that the aircraft impacted the terrain in a left wing‑low, steep, nose‑down attitude at high speed (Figure 4). All major aircraft components were accounted for at the accident site. Damage to and deformation of the propeller was consistent with the engine running at the time of impact. There were no identified pre-accident aircraft defects, although disruption to the airframe precluded a full assessment of the aircraft’s serviceability immediately prior to the accident and prevented the ability to measure remaining fuel on board.
Meteorological information
The graphical area forecast for the accident region on 21 March had clear conditions for the flight with no cloud and visibility greater than 10 km.
At 1030, the Bureau of Meteorology (BoM) automatic weather station at Geraldton Airport, 85 km south of the accident location, recorded the wind as 5 kt from 121° magnetic. There was no recorded cloud, visibility was greater than 10 km and the temperature was 34°C. Figure 1 shows the clear conditions at Geraldton during the aircraft changeover.
Recorded data
Flight track
There was no available radar or ADS‑B recording of the flight. However, the ATSB recovered recorded data from a damaged Garmin 296 GPS which was fitted to the aircraft.
From the departure at Geraldton at 0956 until 1027 the flight progressed without any significant events. The ground speeds calculated for this portion of the flight were consistent with normal cruise for a Cessna 150.
The calculated airspeed increased through the spiral dive and reached a maximum of 153 kt to the last recorded data point, which exceeded the aircraft Vne.[14] Analysis from the initial left turn until the collision with terrain indicated that the engine was producing power until impact.
Video
The ATSB obtained video recordings from Geraldton Airport and 3 cameras within the maintainer’s hangar.
The airport camera field of view (Figure 5) covered:
- both arrival (runway 14) and departure (runway 08) runways
- the parking bay for both Cessna 150s
- the maintenance hangar.
Figure 5: Geraldton Airport camera field of view

Source: Google Earth, annotated by the ATSB
Radio communication
Geraldton Airport recorded local area CTAF. At 0957:08 the pilot was heard broadcasting:
Traffic Geraldton, ah, Whisky Whisky Uniform departed runway 08, through, ah, 600. Tracking out to the north, climbing, ah, 2,500. Geraldton traffic.
This was the last call recorded.
There was no mayday call recorded on the Geraldton CTAF or the Melbourne Centre frequencies. A local pilot flying in the area at the time of the accident, stated they heard other aircraft further north of the accident site making radio transmissions on the Geraldton CTAF, however they did not hear anything further from the pilot of VH-WWU.
ATSB analysis of the radio propagation range concluded that, had the pilot made an emergency broadcast at the time of the flight path deviation, it would likely have been heard by nearby aircraft.
Survivability
ATSB analysis indicated that the deceleration forces and aircraft disruption during the collision with terrain exceeded survivability limits.
Related occurrences
Collison with terrain involving Cessna 152, N89059, Tucson, Arizona, United States on 8 February 2013 (National Transportation Safety Board WPR13FA118)
While flying the airport circuit on the base leg (prior to turning and line up for landing), several motorists observed the Cessna 152 aircraft in a steep nose-down attitude and descending rapidly. The aircraft impacted flat terrain about 1.5 miles from the airport. Examination of the airframe and engine did not reveal any pre‑impact anomalies that would have precluded continued engine operation or flight. Review of the air traffic control radar tracking data did not reveal any abnormalities with the departure or flight. The track was observed to conduct a slight right turn before a left turn steepening until collision with terrain.
The NTSB found that the probable cause was the pilot's incapacitation due to their pre‑existing cardiac disease, which resulted in degraded or complete loss of ability to control the aircraft.
Collision with terrain involving Cessna 152, N49278, Naple, Florida, United States on 13 December 1991 (National Transportation Safety Board MIA92FA045)
The Cessna 152 aircraft was observed flying westbound parallel to the runway in the opposite direction to landing. The aircraft suddenly nosed over, rotated to the left slightly, and impacted terrain in near vertical descent. There was no evidence of failure or malfunction of the aircraft structure, flight controls, or engine. The post‑mortem examination of the pilot indicated they had heart disease.
The NTSB found that the probable cause was the pilot became incapacitated due to an undetermined cardiovascular event which resulted in uncontrolled descent into terrain.
Safety analysis
Departure from level flight
Evidence from the accident site, aircraft wreckage, and flight path data identified that the aircraft collided steeply with terrain at high speed and that the accident was not survivable.
Analysis of the flight path data, combined with the aircraft’s recent release from maintenance, prompted examination of several possible factors. These included:
- airworthiness related to the post maintenance condition of the aircraft
- possibility of control jam affecting flight control functionality
- spatial disorientation impacting the pilot
- potential medical event.
Airworthiness
Examination of the aircraft’s propeller and analysis of the flight data and aircraft characteristics indicated that the aircraft’s engine was operating at the time of the accident.
Had there been an airworthiness issue with the aircraft, it would have very likely been communicated by the pilot. However, no distress calls or Mayday transmissions were recorded on the common traffic advisory frequency (CTAF), or audible to other aircraft in the vicinity on the same frequency. Analysis of the radio propagation range confirmed that any distress call, if made, would have been within range of detection by nearby aircraft.
The accident site was surrounded by expansive paddocks suitable for an emergency landing, which could have reasonably been utilised in the event of a mechanical or engine issue. The terrain was flat and largely unobstructed, providing viable options for a controlled landing. The absence of any attempt to divert to or land in these paddocks suggests that no mechanical or engine-related emergency necessitated such an action.
Control jam
A control jam in the aircraft would have limited the pilot’s ability to manoeuvre the aircraft. If a primary flight control surface, such as the ailerons, elevator, or rudder, becomes jammed or partially restricted, the pilot may have difficulty controlling the aircraft's attitude and direction. Depending on the severity and type of jam, the pilot may need to rely on secondary or alternative control methods, such as trim adjustments or differential power, to maintain control and safely land the aircraft.
However, the aircraft had been flying in level flight for over 30 minutes prior to the event, demonstrating that the controls were functioning properly during this period. Additionally, the aircraft was equipped with new control cables, and no recent maintenance had been performed on the control surfaces, significantly reducing the likelihood of errors such as improper setup or mechanical failure.
The Cessna 150’s simple design includes backup systems to allows pilots to make adjustments to maintain control even in the event of partial system issues. Although the control continuity could not be fully established at the accident site, these points strongly suggest the accident was not due to a control problem.
Spatial disorientation
Spatial disorientation refers to situation when a pilot fails to correctly sense the position, motion or attitude of the aircraft relative to the ground or the gravitational vertical. This can be particularly hazardous to aviation safety and can be affected by cloud cover, changing weather or light conditions, flight profile (e.g. dynamic high-g manoeuvres or gradual sustained turns), distraction, fatigue and medical conditions.
However, the forecasted weather was for clear flight conditions, with no cloud and visibility greater than 10 km. These favourable conditions provide visual references to the horizon and surrounding terrain minimising the chances of special disorientation.
Additionally, flight data analysis indicated the aircraft entered a left turn followed by a spiral dive, with no recorded corrective control inputs to recover from the manoeuvre. This indicates that the pilot maintained proper orientation, as disorientation typically leads to erratic or incorrect control inputs.
While the pilot is likely to have been unwell, fatigued and distracted from their acute gastrointestinal illness, it is unlikely that these conditions caused spatial disorientation.
Incapacitation event
As discussed above, the aircraft entered a left turn followed by a spiral dive with no corrective control inputs to recover. With the pilot’s significant experience, the lack of any attempt to counteract the spiral dive is highly unusual. As the aircraft was not fitted with an autopilot, no input from the pilot on the controls would likely cause the aircraft to start rolling to the left and the nose dropping causing a left turn with a possible spiral dive or spin.
Further, the absence of response to the spiral dive, in addition to the lack of distress call, are consistent with what would occur if the pilot was incapacitated, preventing them from taking corrective action.
Additionally, the flight path was almost identical to the collision with terrain involving a Cessna 152 in Tucson, Arizona, United States, which concluded a probable cause as pilot's incapacitation due to their pre‑existing cardiac disease.
Given the lack of other reasons, it is therefore likely the pilot was incapacitated.
In considering the likelihood of that incapacitating event being medically related, the ATSB engaged a medical professional to provide specialist analysis of the pilot’s medical history, specifically looking at:
- hereditary haemochromatosis
- cardiovascular
- acute gastroenteritis.
Hereditary haemochromatosis
Haemochromatosis is an inherited genetic disorder in which excess iron builds up in the body. Over time, iron overload may cause symptoms that can be a hazard to flight safety and may cause organ damage. However, the genetic profile of haemochromatosis in this case is usually not associated with significant medical complications and is typically managed with regular blood tests to monitor ferritin levels, and regular clinical assessments to observe for any complications.
There was no indication that the requested venesection was actioned prior to the accident. However, it is noted that the pilot had moderately elevated ferritin results for a long period of time but did not report any signs or symptoms of iron overload. It was not possible to discern whether the pilot’s haemochromatosis condition had any material relevance to the accident.
Cardiovascular
The pilot’s next-of-kin, general practitioner, and designated aviation medical practitioner (DAME), and the Civil Aviation Safety Authority (CASA) understood the pilot to be an ex‑smoker, however colleagues had observed the pilot smoking at times. Smoking is an independent risk factor for cancer, cardiovascular disease (higher blood pressure, heart attack, stroke), respiratory disease (chronic obstructive pulmonary disease) and other conditions which can impact fitness for flight (hypoxia, fatigue, reduced exercise tolerance, higher risk of sudden incapacitation).
The pilot’s hypertension and high cholesterol were also risk factors for cardiovascular disease. The elevated risk of major adverse cardiac event was assessed in accordance with CASA requirements (stress ECG) and the outcome was that there was no safety‑relevant coronary ischaemia detectable. The cardiac assessments do not entirely exclude coronary disease, particularly non-occlusive and non-calcified atheromatous plaque (Jennings et al 2021 and Gray et al, 2019), and it remains possible that this pilot experienced an acute cardiac ischaemic event (or other major adverse cardiovascular event) resulting in acute incapacitation.
Acute gastroenteritis
The pilot’s physical appearance, as noted by the maintenance team, was consistent with the reports that the pilot was suffering from an acute gastrointestinal infection. The fact that the pilot self-excluded from the planned flight on the day prior to the accident, was testament to the extent to which they were afflicted by the illness.
While the pilot reported feeling better ahead of the accident flight, it was very likely that they remained unwell and symptomatic. Gastroenteritis by itself does not cause sudden incapacitation, however it would have reduced the pilot’s physiological reserves and exposed the pilot to the associated complications, including dehydration and electrolyte imbalance, and fatigue. The pilot’s yellow, sunken eyes, weight loss, and reduced food intake indicated it is very likely that the pilot was moderately dehydrated at the time of the accident flight.
There is no evidence that the pilot sought any health advice or treatment from a health care provider for their acute gastrointestinal symptoms. However, for the purposes of this analysis, it could be considered most likely that the pilot continued to take their usual medications (specifically irbesartan for hypertension).
Sudden incapacitation
Dehydration from 5 days of infective gastroenteritis would have increased the pilot’s risk of low blood pressure leading to a syncopal event (faint) and may have caused or contributed to electrolyte imbalances. Additionally, the continued usage of irbesartan would have also reduced blood pressure (van Dijk et al, 2021 and Taylor et al, 2025). While seated in an upright position, a syncopal event (faint) due to low blood pressure was the most likely cause of a rapid incapacitation in this occurrence, with no prospect for timely recovery.
Alternatively, low blood pressure and electrolyte imbalances increase the risk of a major adverse cardiovascular event, such as myocardial infarction (commonly referred to as heart attack), cardiac arrhythmia or stroke, which may also cause a rapid incapacitation.
In conclusion, it is very likely that the pilot experienced an incapacitation event. However, from the evidence available, the exact nature of the incapacitation could not be determined. There were no other factors identified that were likely to have contributed to the accident.
Findings
ATSB investigation report findings focus on safety factors (that is, events and conditions that increase risk). Safety factors include ‘contributing factors’ and ‘other factors that increased risk’ (that is, factors that did not meet the definition of a contributing factor for this occurrence but were still considered important to include in the report for the purpose of increasing awareness and enhancing safety). In addition ‘other findings’ may be included to provide important information about topics other than safety factors. These findings should not be read as apportioning blame or liability to any particular organisation or individual. |
From the evidence available, the following findings are made with respect to the collision with terrain involving Cessna 150M, VH-WWU, 40 km north-west of Northampton, Western Australia, on 21 March 2025.
Contributing factors
- While in cruise, the pilot likely experienced an incapacitating medical event resulting in a deviation off track, a left-hand spiral dive and subsequent collision with terrain.
- The pilot was acutely unwell in the days preceding the accident flight, and was very likely still symptomatic during the accident flight.
Sources and submissions
Sources of information
The sources of information during the investigation included:
- Shark Bay Aviation
- the next of kin
- the senior base pilot of the operator
- witnesses who saw the pilot prior to the flight
- Civil Aviation Safety Authority
- Western Australia Police Service
- the maintenance organisation for VH-WWU
- Textron Aviation
- CCTV footage of the aircraft from Geraldton Airport
- recorded data from the GPS unit on the aircraft
- the pilot's designated aviation medical examiner
- the pilot’s general practitioner
- Royal Australian Air Force Institute of Aviation Medicine
- ChemCentre Western Australia.
References
Gert van Dijk, J., van Rossum, I A., Roland, D. Thijs,The pathophysiology of vasovagal syncope: Novel insights. Autonomic Neuroscience, Volume 236, 2021 https://doi.org/10.1016/j.autneu.2021.102899.
Gray, G, Davenport, E, Bron, D et al The challenge of asymptomatic coronary artery disease in aircrew. Heart 2019; 105: s17-s24
Jennings, G., Audehm, R., Bishop, W., Chow, K., Liaw, S., Liew, D., and Linton, S. National Heart Foundation of Australia: position statement on coronary artery calcium scoring for the primary prevention of cardiovascular disease in Australia. Med J Aust 2021; 214 (9): 434-439. doi: 10.5694/mja2.51039
Neuvonen, P., Niemi, M., & Backman, J. (2006). Drug interactions with lipid-lowering drugs: Mechanisms and clinical relevance. Clinical Pharmacology & Therapeutics, 80(6), 565–581. https://doi.org/10.1016/j.clpt.2006.09.003
Taylor K, Tripathi AK. Adult Dehydration. [Updated 2025 Mar 5]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555956/
Submissions
Under section 26 of the Transport Safety Investigation Act 2003, the ATSB may provide a draft report, on a confidential basis, to any person whom the ATSB considers appropriate. That section allows a person receiving a draft report to make submissions to the ATSB about the draft report.
A draft of this report was provided to the following directly involved parties:
- Shark Bay Aviation
- maintenance organisation for VH-WWU
- Civil Aviation Safety Authority
- Textron Aviation
- Royal Australian Air Force Institute of Aviation Medicine
- Western Australia Police Force.
Submissions were received from:
- Civil Aviation Safety Authority
- Royal Australian Air Force Institute of Aviation Medicine.
The submissions were reviewed and, where considered appropriate, the text of the report was amended accordingly.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. About ATSB reportsATSB investigation reports are organised with regard to international standards or instruments, as applicable, and with ATSB procedures and guidelines. Reports must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. An explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] Shark Bay is about 340 km north‑west from Geraldton.
[2] SARTIME (time search action required): is the time nominated by a pilot for the initiation of search and rescue action.
[3] CTAF (common traffic advisory frequency): a radio frequency used by pilots at non-towered airports to communicate with each other about their position and intentions, ensuring safe and orderly traffic flow.
[4] Likely referring to piston rings, which wear somewhat more quickly at increased temperatures.
[5] The pilot’s use of omeprazole and diagnosis with gastroesophageal reflux disease and Barrett’s oesophagus were medically significant and required ongoing surveillance as part of the medical assessment process, however they were not declared to CASA. The medication is subject to DAME approval, but must also be declared to CASA as part of the medical assessment process.
[6] An inherited genetic disorder in which excess iron builds up in the body. Over time, iron overload may cause symptoms that can be a hazard to flight safety and may cause organ damage (e.g. liver, heart, kidneys).
[7] No significant ECG changes during exercise and recovery.
[8] Ferritin is a blood protein that contains iron.
[9] Venesection, also known as therapeutic phlebotomy, is a medical procedure that involves the controlled removal of blood to reduce excess iron or red blood cells in conditions like hemochromatosis or polycythemia.
[11] A Class 1 medical certificate is required to exercise the privileges of a commercial pilot licence.
[12] A 3-point harness includes a lap belt and upper torso restraint (UTR).
[13] Honing is a process that scratches a crisscrossed (crosshatched) pattern onto the inside of the cylinder. This pattern reduces cylinder wear by allowing oil to be retained in the scratches rather than be removed by the piston rings.
[14] The aircraft’s ‘never exceed speed’ (Vne) was 141 kt. Exceedance of this airspeed may result in structural damage to the aircraft.
Preliminary report
Report release date: 28/05/2025
| This preliminary report details factual information established in the investigation’s early evidence collection phase, and has been prepared to provide timely information to the industry and public. Preliminary reports contain no analysis or findings, which will be detailed in the investigation’s final report. The information contained in this preliminary report is released in accordance with section 25 of the Transport Safety Investigation Act 2003. |
The occurrence
Overview
On the morning of 21 March 2025, a pilot was conducting 2 ferry flights of Cessna 150 aircraft that were operated by Norwest Air Work. The first flight, from Shark Bay Airport to Geraldton Airport, Western Australia, involved a Cessna 150M, registered VH‑TDZ. Once at Geraldton Airport, the pilot was to swap aircraft at the maintenance hangar and fly back to Shark Bay Airport in VH‑WWU, the operator’s other Cessna 150M which had been released from maintenance on 18 March 2025.
The pilot was the sole occupant on board both flights. The operator’s senior base pilot was holding SARTIME[1] for both flights.
On the ground at Geraldton Airport
Closed-circuit television (CCTV) showed that the pilot landed VH‑TDZ at 0914:20 local time and taxied the aircraft to the maintenance organisation’s parking bay. At 0922, the pilot texted the senior base pilot informing them of their arrival in Geraldton.
Between 0925 and 0931, the pilot manoeuvred VH‑WWU out of the parking bay and moved VH‑TDZ into it. Once completed, the pilot walked to the maintenance hangar (Figure 1). Witnesses at the airport reported that the pilot appeared unwell and had mentioned having had severe gastroenteritis in the preceding days. Witnesses did not report any apparent speech or physical impairment.
At 0945:15, the pilot left the maintenance hangar, walked to VH‑WWU and conducted a pre‑flight inspection. The aircraft had been refuelled on the morning by the airport refueller. Approximately 2 minutes later the pilot started the engine and taxied the aircraft to the centre apron.
Figure 1: Aircraft changeover
Source: Geraldton Airport, annotated by the ATSB
Geraldton to Shark Bay
At 0955:16, the pilot reported on the local CTAF[2] that they were lining up and rolling on runway 08. The aircraft lifted off the runway 40 seconds later. At 0957:08 the pilot reported they had departed the runway and were tracking out to the north climbing to 2,500 ft through 600 ft. This was the last recorded call from VH‑WWU on the CTAF. Shark Bay is about 340 km north‑west from Geraldton.
Directly after take‑off, the pilot texted the senior base pilot with the expected arrival time at Shark Bay, which was 1230.
At 1008:52, the pilot took a photo of the aircraft oil temperature gauges. Eight minutes later the pilot sent the photo to a staff member at the maintenance organisation with accompanying text stating ‘WWU flies beautiful, smooth, and tight. Oil temp a little high for a cool day so we might have to look at fitting those coolers back onto WWU. I’d hate to see the rings[3] suffer.’ The maintainer responded via text at 1018, and the message was recorded as delivered (indicating that the pilot’s phone was still functional at that time). The oil temperature shown in the photo was towards the upper end of the normal range but below the 240°F maximum oil temperature limit.
At 1116:43, a call was placed to police by a member of the public stating they had come across aircraft wreckage by the side of a road as they were driving past (Figure 2). The accident was 84 km north‑west of Geraldton Airport, and about 0.5 km right of the direct track. The member of the public stated that although they had been nearby, they had not seen or heard the aircraft or the impact.
Figure 2: Original final position of VH‑WWU at the accident site[4]
![Figure 2: Original final position of VH‑WWU at the accident site[4]](/sites/default/files/2025-05/AO-2025-014-Figure%20%282%29.png)
Source: Western Australia Police Force
The aircraft was destroyed, and the pilot was fatally injured.
Context
Pilot information
The pilot held a commercial pilot licence (helicopter and aeroplane), with both single and multi‑engine class ratings for aeroplanes and a single engine class rating for helicopters. They held low‑level operational ratings for sling, aerial mustering helicopter and aerial musting aeroplane operations. In addition, the pilot held flight instructor ratings for low‑level flight tests in both aeroplanes and helicopters.
The pilot completed single engine aircraft and low‑level flight reviews on 12 February 2024.
The pilot held a valid class 1 aviation medical certificate which was approved in October 2024. This specified a requirement for the pilot to wear distance vision correction and a headset while flying. It also required reading vision correction to be available.
The pilot logbooks were not available at the time of publication.
Aircraft information
The Cessna 150M is a high‑wing, all metal, 2‑place, unpressurised aircraft with a fixed landing gear. VH‑WWU was manufactured in 1976 and was first registered in Australia on 5 May 1986. It had a single, Continental O‑200‑A reciprocating piston engine driving a fixed-pitch propeller. The aircraft was not equipped with an autopilot.
A periodic and other scheduled inspections were carried out between 6–18 March 2025. The periodic inspection identified minor defects that were subsequently rectified. The aircraft’s engine reportedly had excessive oil consumption, and to address the issue all 4 engine cylinders were removed, honed[5] and refitted along with new piston rings. Additionally, the engine ignition harness was replaced due to it being in poor condition. The engine was tested by carrying out a ground run 3 days before the accident and found to be functioning correctly. At the completion of maintenance, the aircraft had accrued a total time in service of 14,208 hours.
Site and wreckage
The wreckage was located about 20 m south of an east‑west road. The Western Australia Police Force and emergency services attended the site on the day of the accident.
The ATSB commenced the accident site examination on the following day, 22 March. The wreckage trail extended in a north‑easterly direction, about 23 m from the initial impact point to where the main wreckage, including the wings, empennage, engine and propeller had come to rest (Figure 3). There was no fire, and fuel could be smelt in the area.
Figure 3: Overview of VH‑WWU accident site

Source: ATSB
Ground impact marks and damage to the airframe indicated that the aircraft impacted the terrain in a left wing‑low, steep nose‑down attitude at high speed (Figure 3). All major aircraft components were accounted for at the accident site. The disruption to the airframe from the impact limited the extent to which the aircraft could be examined. Of the components that could be examined, no pre‑impact defects were identified. Bending and damage to the propeller was consistent with the engine running at the time of impact.
A damaged Garmin 296 GPS receiver was recovered from the accident site. There were no available radar or ADS‑B recordings of the flight.
Meteorological information
The graphical area forecast for the accident region forecasted clear conditions for the flight with no forecast cloud and visibility greater than 10 km.
At 1030, the Bureau of Meteorology (BoM) automatic weather station at Geraldton Airport, 85 km south of the accident location, recorded the wind as 5 kt from 121° magnetic. There was no recorded cloud, visibility was greater than 10 km and the temperature was 34°C.
Further investigation
To date, the ATSB has:
- examined the wreckage and accident site
- recovered the GPS for further examination
- conducted interviews with witnesses and the maintenance organisation
- collected aircraft, pilot and operator documentation
- collected CCTV and CTAF recordings.
The investigation is continuing and will include:
- review and examination of any recovered GPS data
- collection and review of additional pilot medical information
- examination of the aircraft maintenance history.
A final report will be released at the conclusion of the investigation. Should a critical safety issue be identified during the course of the investigation, the ATSB will immediately notify relevant parties so appropriate and timely safety action can be taken.
Purpose of safety investigationsThe objective of a safety investigation is to enhance transport safety. This is done through:
It is not a function of the ATSB to apportion blame or provide a means for determining liability. At the same time, an investigation report must include factual material of sufficient weight to support the analysis and findings. At all times the ATSB endeavours to balance the use of material that could imply adverse comment with the need to properly explain what happened, and why, in a fair and unbiased manner. The ATSB does not investigate for the purpose of taking administrative, regulatory or criminal action. TerminologyAn explanation of terminology used in ATSB investigation reports is available here. This includes terms such as occurrence, contributing factor, other factor that increased risk, and safety issue. Publishing informationReleased in accordance with section 25 of the Transport Safety Investigation Act 2003 Published by: Australian Transport Safety Bureau © Commonwealth of Australia 2025 
Ownership of intellectual property rights in this publication Unless otherwise noted, copyright (and any other intellectual property rights, if any) in this report publication is owned by the Commonwealth of Australia. Creative Commons licence With the exception of the Commonwealth Coat of Arms, ATSB logo, and photos and graphics in which a third party holds copyright, this report is licensed under a Creative Commons Attribution 4.0 International licence. The CC BY 4.0 licence enables you to distribute, remix, adapt, and build upon our material in any medium or format, so long as attribution is given to the Australian Transport Safety Bureau. Copyright in material obtained from other agencies, private individuals or organisations, belongs to those agencies, individuals or organisations. Where you wish to use their material, you will need to contact them directly. |
[1] SARTIME ('time search action required'): is the time nominated by a pilot for the initiation of search and rescue action.
[2] CTAF (common traffic advisory frequency): a radio frequency used by pilots at non-towered airports to communicate with each other about their position and intentions, ensuring safe and orderly traffic flow.
[3] Likely referring to piston rings, which wear somewhat more quickly at increased temperatures.
[4] Emergency services personnel moved main sections of the aircraft when removing the pilot.
[5] Honing is a process that scratches a crisscrossed (crosshatched) pattern onto the inside of the cylinder. This pattern reduces cylinder wear by allowing oil to be retained in the scratches rather than be removed by the piston rings.
Occurrence summary
| Investigation number | AO-2025-014 |
|---|---|
| Occurrence date | 21/03/2025 |
| Location | 40 km north-west of Northampton |
| State | Western Australia |
| Report release date | 14/10/2025 |
| Report status | Final |
| Investigation level | Short |
| Investigation type | Occurrence Investigation |
| Investigation status | Completed |
| Mode of transport | Aviation |
| Aviation occurrence category | Collision with terrain |
| Occurrence class | Accident |
| Highest injury level | Fatal |
Aircraft details
| Manufacturer | Cessna Aircraft Company |
|---|---|
| Model | 150M |
| Registration | VH-WWU |
| Serial number | 15077949 |
| Aircraft operator | Norwest Air Work Pty Ltd |
| Sector | Piston |
| Operation type | Part 91 General operating and flight rules |
| Departure point | Geraldton Airport, Western Australia |
| Destination | Shark Bay Airport, Western Australia |
| Damage | Destroyed |